In October 2020 Dr Andrew Hill was tasked to report to the World Health Organisation on the dozens of new studies from around the world suggesting that Ivermectin could be a remarkably safe and effective treatment for COVID-19.
But on January 18th 2021, Dr Hill published his findings on a pre-print server. His methods lacked rigour, the review was low quality and the extremely positive findings on ivermectin were contradicted by the conclusion. In the end, Dr Hill advised that “Ivermectin should be validated in larger appropriately controlled randomized trials before the results are sufficient for review by regulatory authorities.”
The researcher seeking a global recommendation on Ivermectin had instead recommended against it. A media onslaught against the medicine ensued. What were Dr Hill’s reasons for doing so? Were his conclusions justified? Or were external forces influencing his about-face?
One year on, this film recalls exactly what happened from the perspective of somebody that experienced it first hand; Dr Tess Lawrie; also featuring contributions from Dr Pierre Kory and Dr Paul Marik who worked closely with Dr Hill during the same time frame.
“Oh what a tangled web we weave, when first we practice to deceive” – Sir Walter Scott
Throughout the last two years Public Health Scotland (PHS) has punched above its weight by providing reliable data that has quantified the impact of the Scottish government’s COVID-19 response on the health of the Scottish population. In particular, it has documented the unprecedented excess death that occurred in summer and autumn 2021, prompting the establishment of an official enquiry as to the cause, and uncovered a spike in September 2021 in the number of stillbirths in Scotland that is currently under investigation.
However, in its report of 14th February 2022, PHS has declared that it will no longer publish data on COVID-19 outcomes (cases, hospitalisations and deaths) classified by vaccination status, a hitherto valuable component of the COVID-19 vaccination surveillance strategy. The reason given for making this change is that ‘PHS is aware of inappropriate use and misinterpretation of the data when taken in isolation without fully understanding the limitations’.
It is certainly true that claims have been made about the deleterious effects of COVID-19 vaccines that go well beyond what can be supported by the data published by PHS. In this case critical appraisal of these unsubstantiated claims, rather than the blanket withdrawal of valuable information, would seem the better antidote to the spread of misinformation.
However, it is important to note that implicit in the decision made by PHS is that the information they provide is above reproach, both in terms of inappropriate use and misrepresentation of the data to which they alone are privy. To investigate whether PHS analysis is indeed above reproach, we can look in a little detail at the way in which they have presented the information on COVID-19 outcomes by vaccination status in their last report of February 2022. We will concentrate on the analysis of death with COVID-19 by vaccination status, unvaccinated or booster, found in Table 15, using the data for week 29 January – 04 February 2022. The relevant data from that table is reproduced below:
No. of Deaths
Population
Age Standardised Mortality Rate per 100,000 with 95% confidence intervals
Unvaccinated
13
1,524,406
10.95 (3.40 – 18.50)
Booster
73
3,229,938
1.50 (1.15 – 1.85)
A superficial inspection of this table would suggest to the casual reader that the death rate with COVID-19 in those who have received a booster is far lower than that suffered by those who are unvaccinated when the difference in age distributions of the booster and unvaccinated populations are taken into account. Indeed, PHS draw the conclusion that ‘the death rate in individuals that received a booster or 3rd dose of a COVID-19 vaccine was between 4.6 and 9.5 times lower than individuals who are unvaccinated or have only received one or two doses of a COVID-19 vaccine’. Let us look in detail at how the data were treated to arrive at this conclusion, and ask whether this very strong affirmation of the benefits of the booster can be substantiated.
We first look at the way in which the two populations that we are comparing, unvaccinated and booster, are defined. For this we turn to Appendix 6 of the report. Here we learn that the unvaccinated population is not, as we might have assumed, those that have never been vaccinated. Instead, it also includes all those individuals who have received a first vaccine, but for whom the time since vaccination is less than 22 days. Thus, if any deaths occur within the 21 days post first vaccine, these deaths will be attributed to the unvaccinated category. This misattribution may have significant consequences because deaths from adverse vaccination reactions principally occur shortly after vaccination. This idiosyncratic classification of the unvaccinated artificially, and misleadingly, inflates the death rate in the unvaccinated population. Would it not have been better to classify the unvaccinated as those never receiving a vaccine, to preclude the introduction of such bias against the unvaccinated into the analysis?
Turning to the boosted population we find that this is not defined as the number of individuals who have received a booster, but rather the number that have received a booster at least 14 days prior to the reporting period. Therefore, if deaths of boosted individuals occur within the first 14 days of this vaccination, they will not be counted as booster deaths, but as a 2-dose death. The mortality rates given are also dependent on the size of the vaccinated population. If the addition of boostered individuals is a continuous process then, depending on accounting, the last two week cohort added to the boostered population may effectively be excluded from contributing to deaths, while the unvaccinated population during the same time period will not. PHS’s redefinition of the booster population again serves to artificially and misleadingly reduce the reported rate of deaths in the PHS booster population relative to the unvaccinated population. Would it not have been better to classify the booster population simply as those who have received a booster shot, and avoided the inevitable bias in favour of the boosted population that is introduced by the PHS redefinition?
Notwithstanding the biases introduced by PHS’s redefinition of the populations to be compared, we can now concentrate our attention on the methods they have used to correct for the fact that the age distribution of the unvaccinated is likely to be much younger than that of the boosted population. To begin our explanation, it is helpful to use the raw data provided in table 15 for week 29 January – 04 February 2022 to calculate the individual rate of death with COVID-19 per 100,000 per week without making any adjustment for differences in age distribution. This can be compared with the figures PHS calculated from the data to quantify ‘Age Standardised Mortality Rate per 100,000 per week’.
Unvaccinated
Booster
Unadjusted COVID-19 mortality per 100,000 per week
0.85
2.26
Age Standardised Mortality Rate per 100,000 per week
10.95
1.50
The comparison is illuminating and a little worrying. An unadjusted death rate 2.7 times higher in the booster population than in the unvaccinated population has been converted into an age standardised mortality rate that is now 7.3 times higher in the unvaccinated population than in the booster population. To understand what is going on we have to know both how to calculate an Age Standardised Mortality Rate per 100,000 per week, and to understand what this value actually represents.
The Age Standardised Mortality Rate is a measure of the impact, in terms of mortality, on the whole population rather than a particular age group. Rather than calculating a population Age Standardised Mortality Rate based on the age distribution of the Scottish population, Public Health Scotland used the standard WHO age distribution. In this age distribution there is a much lower representation of older people. The consequence is that a very low weight is given to deaths in older age groups and a disproportionately high weighting to deaths in young age groups. In fact, the weighting of a young death can be 10 times higher than for an old death. Through this unjustified weighting a raw mortality rate which was 2.7 times greater in the vaccinated is turned into an age standardised mortality rate which is 7.3 times greater in the unvaccinated.
The age standardised mortality does not relate to individual risk – we may have much higher risk in old age groups individually, but this translates into a very small effect on overall deaths at a population level because the percentage of old people in the population is very low. The point of calculating age standardised mortality is not to compare risks. It is designed to allow comparison of the relative burden of a disease on a population – what proportion of a population will be lost from that population by a particular disease. Its use to somehow correct for differences in age distributions on risk of death is completely inappropriate.
The important thing to note is that what has been calculated is a measure of population impact of COVID-19 in a hypothetical population; what proportion of the population die in this hypothetical population as a consequence of the disease. It is assuredly not a measure of individual mortality risk from COVID-19. As such it is completely inappropriate and misleading to use it to compare the risk of death with COVID 19 between populations of different vaccination status as has been done by PHS. Therefore, their statement that ‘the death rate in individuals that received a booster or 3rd dose of a COVID-19 vaccine was between 4.6 and 9.5 times lower than individuals who are unvaccinated or have only received one or two doses of a COVID-19 vaccine’ is utterly false and misleading and completely unsupported by the data. The simple and transparent way of comparing individual mortality risk would be to use the data in PHS’s possession to estimate individual risk of death for each age category and population, and compare these values within each age category. Rather than compare the whole population, the risk for each age group by vaccination status would provide useful information. UKHSA do provide this data but PHS never have done. The magnitude of the error in using Age Standardised Mortality Rates as a metric calls into question the competence of PHS to analyse and interpret data that are critical to the formulation of Scottish government health policy which directly impacts the wellbeing of literally millions of people.
The final point to make is that in order to receive a booster, an individual must previously have received both a first and a second dose of vaccine. There is a risk of a bias being introduced whereby only survivors, who are by definition less likely to die, are being measured. Therefore, deaths that occurred after first and second vaccinations should be included with deaths after the booster vaccination itself in order to properly assess the overall COVID-19 death rates in the vaccinated population. In other words, the appropriate comparison to make when assessing the effect of booster doses on COVID-19 mortality is between the unvaccinated population and the vaccinated population, where the latter includes anyone who has received any injection.
In conclusion, by announcing that data on COVID-19 outcomes by vaccination status will no longer be provided due to “misrepresentation and misinterpretation of their analyses”, PHS has drawn attention to their own glaring shortcomings in this area. They have been shown to introduce unwarranted bias into their analyses by manipulation of the definitions of vaccination status, and they have used a wholly inappropriate metric to compare the risk of death with COVID-19 among the vaccinated and unvaccinated in the Scottish population.
We are under siege. A nihilistic fanaticism is running free among us thanks to the emergence of a journalistic “ethos” that establishes an almost complete equivalence between the “truth” and those utterances that support the strategic goals of the great economic and digital powers of our time.
A few months ago Facebook censored an article in the British Medical Journal that highlighted serious irregularities in Pfizer’s clinical vaccine trials. Then two weeks ago, fact-checkers from the Spanish websites Newtral and Maldita burst into the public square to accuse professor of Pharmacology, renowned expert in drug safety, and ex-WHO adviser, Joan Ramón Laporte of foisting lies and disinformation onto the Spanish populace. This, in reaction to Laporte’s testimony before a Spanish parliamentary commission investigating the country’s vaccination effort.
Despite his towering credentials, his intervention was quickly tarred as problematic by the media and subsequently banned by YouTube. The crime of this new Galileo Galilei? Alerting the assembled parliamentarians to the existence of grave procedural irregularities in the trials for the vaccines, and questioning the wisdom of a health strategy that aims to inject every Spanish child over the age of six with a new, poorly tested, and largely ineffective medication.
This incident reveals that the fact-checkers will attack anyone who does not accept the truth as dictated by the great economic and government centers of the world. This is not the usual official media obfuscation to which we’ve become accustomed over the years, but rather a brazen McCarthyist intimidation device, designed to frighten citizens into submission by appealing to their lowest and most ignoble instincts, an approach lain bare in Maldita’s smug and Manichaean slogan: “Join and support us in our battle against lies.”
Under this harsh binary logic, an internationally famous scientist like Laporte is not even given the opportunity to be judged wrong or misguided in good faith. Rather, he is immediately accused of being a willful and dangerous liar who must be immediately banished from public view.
Fact-checkers as destroyers of science and the public sphere
Nowadays the word “fascist” is used so profligately that it has lost most of its meaning. But if we are really serious about describing the operational logic of fact-checking entities like Maldita and Newtral we must recur precisely to that term, adding the prefix “neo” to avoid confusion with the original version of this totalitarian sensibility.
Whereas the original model of fascism sought to enforce social conformity through physical intimidation, the new variant seeks to do so by aggressively enforcing the “acceptable” (to big power, of course) parameters of both scientific discourse and the idea of the public sphere, a direct product, like science, of the Enlightenment. Their objective is to liquidate these flawed but essential spaces of debate in all but name, and thus deprive us of two of the only remaining vehicles we have for defending ourselves against the abuses meted out by the liberal state and its corporate and military allies.
The fact-checking industry was born as a consequence of fake news, that great invented crisis whose sole objective was to provide a pretext for enhancing elite control over any democratic impulse that might arise in response to the sudden and often harsh imposition of neoliberalism and digital technologies in our lives.
But what initially began as a pathetic, overreaching and classist attempt to prevent the unwashed from even considering, say, that people in Hillary Clinton’s entourage might have prostituted minors in a pizza-house basement, quickly morphed, during the Covid era, into something much more sinister and consequential.
It is now the menacing cudgel of an ever-growing exercise in illegitimate corporate and state power, a weapon that allows elites to effectively disappear world-renowned experts like Laporte who dare to put the interests of society ahead of the economic interests and control agendas of Big Pharma and Big Tech.
These Digital Brownshirts are just the most visible and forward-leaning elements of a much broader effort to install the logic of the algorithm—a providential and vertically-imposed concept of truth that vitiates traditional fact-finding and admits neither human intelligence nor scientific debate—as a cornerstone of our human interactions and cognitive processes. Under this paradigm, a linear relationship between power and truth is presented as wholly and completely natural.
When analyzed in this light we could say that while the libels launched against Laporte by Maldita and Newtral are not strictly-speaking algorithmic in origin, they are profoundly algorithmic in spirit in that they are designed, like Neil Ferguson’s well-publicized if completely errant epidemiological models, to radically preempt the search for truth over time through empirical observation and informed debate.
The methods these fact-checkers use to dictate what is to be presented to the public as “true” operate under few, if any known, procedural standards. Rather, in forming their “arguments” it seems they simply cherry-pick the opinions of an expert or two who is known to be on board with the particular “algorithmic” project of social change or social mobilization.
This, regardless of the at times massive gap between the slim credentials and in-field experience of the project-compliant experts (not to mention the fact-checking journalists) and the demonstrated international skill and renown of the objects of their efforts in cognitive cleansing like Laporte, or earlier on in the Covid crisis, Michael Levitt and John Ioannidis.
In short, these fact-checking processes follow neither the basic principles of journalistic ethics—which requires that one enter into a given question without any unduly strong presuppositions—or the necessary back and forth of the scientific method, which insures, or is at least designed to insure, that dissident opinions be considered in the process of establishing operative, if still always provisional, notions of truth.
The only recognizable “strength” the new fact-checkers have—and here we see perhaps the clearest link to the thugs that were strategically deployed by Mussolini and Hitler— is their backing from the very highest levels of social and economic power.
The seriousness of the current situation lies in the way the fact-checkers have—before the often dumbfounded acquiescence of much of the academy itself—successfully arrogated to themselves the right, for all practical purposes, to smash the day-to-day freedom and epistemic authority of scientists, as well as the processes designed to insulate intellectual inquiry from the undue impingements of concentrated power, or to put it more simply, from the possibility that an oligarchy-sponsored mediocrity, or pack of mediocrities, can summarily cancel the widely institutionally recognized wisdom of a Joan Ramon Laporte.
The authoritarianism of the fact-checkers not only cripples science but effectively annuls the very idea of the public sphere by naturalizing the idea that the robust, and at times, conflictual exchange of ideas is in some way perverse. Is it any wonder that observing a world like this, many of our students, who should at their age be bursting with a desire for healthy conflicts in the service of growth, have confessed to us both in private how scared they are to express themselves freely and openly in class?
If the largely anonymous fact-checkers are the shock troops of this campaign to override both epistemological rigor and the idea of the public sphere, the media-anointed “science-explainers” are its field generals.
There is, of course nothing wrong with seeking to make often arcane fields of knowledge accessible to the general public. Indeed when done well by a real scientist like Carl Sagan it is a high art.
The problem comes, as is so often the case today, when the popularizer lacks a grasp of the fundamental debates in the field, and from there, the ability to confidently wade into them as a participant. Painfully aware that he or she is in over his head, they will do what most people unable to compete on their own merits in the field to which they have been assigned tend to do: seek the protection in the arms of power.
This produces a perverse reality, in which the people ostensibly tasked with introducing the public to the complexity of both science and public policy, end up shielding them from an acquaintance with either. And knowing their continued prominence depends on pleasing the powers who have elevated them to the spotlight and who are seeking to destroy existing epistemologies of knowledge in order to facilitate the imposition of their algorithmic logic, they take delight in mocking those few highly accomplished people who have decided not to relinquish their principles in the face of the constant propaganda onslaught.
A good example of this practice of hooliganism in Spain is Rocio Vidal, who works for La Sexta, the country’s most-watched TV network. From a swivel chair in her home office, she ridicules anyone, from the singer and actor Miguel Bosé to the head of Allergic Diseases at Ourense Hospital in Galicia who questions the official dogma of the unprecedented virulence of Covid, and the self-evident wonders of the vaccines. The specific crime of the doctor from Galicia? Stating that the not fully tested Covid mRNA vaccines are, in fact, not fully tested and thus are by definition experimental.
What these medical influencers are doing, no doubt with the full knowledge, approval and perhaps even training of the great financial, governmental and pharmaceutical powers is to effect—under the rubric of the freedom of the press—a rapid sorpasso of the institutions that, with all their faults, have long guaranteed a more or less reliable structure for adjudication of competing claims of scientific truth. Unaccustomed to the aggressiveness, relentlessness and speed of these attacks, most doctors have, sadly, reacted like the proverbial deer in the headlights to them, hoping against hope that this plague of intellectual vandalism will somehow, someway be brought to an end. But it would appear that no such relief is in the offing.
Perhaps the most dangerous aspect of this inquisitorial logic and praxis in the long run is that it tries to make citizens believe that there is no relationship between science and politics, and that politics—the art of dissent—is a dangerous practice that must be eschewed by every conscientious citizen.
The fact-checkers as the great landowners of the new virtual world
We must face the fact that the news verification agencies are part of the global control framework set in motion by those who claim for themselves the right to be the owners of all our time and and all of our actions. Behind information verification software services like Newsguard, we find fervent defenders of illegal spying on citizens like former CIA and NSA chief and congressional perjurer Michael Hayden, and US army assassination team leader Stanley McChrystal.
The International Fact-Checking Network to which the aforementioned Spanish fact-check agencies Maldita and Newtral belong is financed in part by Pierre Omidyar, founder of eBay and a major player in, among many other shady oligarchic pursuits, the NATO-linked Allegiance for Securing Democracy.
There is nothing politically neutral about these people. Nor has any of them ever shown a great predilection or support for disinterested intellectual inquiry. What all three have shown in abundance is an abiding delight in marshaling power for the present US-led global order and the exercise of often brutally administered schemes of control over others.
The prime objective of fact-checkers—as recognized, for example, by Newtral on its website—is to use algorithms to harvest and manage citizen information, and in this way, usher in a new era in which the minds of individuals will be so seamlessly “pre-directed” to “positive” and “benevolent” ends and behaviors (as so defined by the members of the enlightened classes) that politics in all its forms will come to be seen as superfluous.
This explains why, between them, Google and Facebook currently employ 40,000 “verifiers” who exercise an invisible censorship aimed at swaying our perceptions of the world in ways deemed to be “constructive” by the controllers of those firms and those with whom they have forged political and business alliances.
These efforts lie at the core of the post-humanist gospel as preached by people like Klaus Schwab and Ray Kurzweil. Their clear message to us about the coming world is that while you might be born free, your destiny and the design of your being—and what we used to call its unique sensibilities— will be firmly entrusted to others. Like who? Like the aforementioned gentlemen and their friends who, of course, have much more far-seeing minds than your own.
But if there is one thing that the Digital Brownshirts fear more than the Wicked Witch of the West fears water, it is real politics. Thus far, these informational terrorists have been able to exploit our natural indulgence of the value of free speech for their own ends. Let’s be clear. These censors are, in effect, engaging in mass consumer fraud. And if it is illegal to sell horse meat as beef, and refined sugar as a nutritional supplement, then it should also be illegal for hired guns to arrogate to themselves the right to define truth and destroy long-standing deliberative processes and institutions.
Sadly, however, we cannot wait for our deeply compromised political classes to take the lead on this necessary criminal prosecution. Rather we, as informed citizens, must take the lead in denouncing these vandals and the powers that have cynically unleashed them upon our shared scientific and civic spaces.
In this process, we must help our ever more present-minded citizens, enslaved to the idea—so useful to the elites— that the world is fundamentally entropic, that these nihilists did not just appear on their TV screens by accident, but rather that they were placed there to do someone else’s dirty work, and that our survival as free people depends on the tenacity with which we hunt down those “someone elses” and subject them to one of the more fundamental types political action: popular justice.
David Souto Alcalde is a writer and assistant professor of Hispanic Studies at Trinity College. He is specialized in the history of republicanism, early modern culture and in the relations between politics and literature.
The “majority” of children in the U.S. have already been infected with COVID-19, The Washington Post today reported, after reviewing data from the Centers for Disease Control and Prevention (CDC).
The Post’s report begs the question: If so many kids have natural immunity to the virus, and, as reported Monday, the vaccines aren’t very effective in children 5 to 11 years old, why are public health officials, schools, businesses and others pushing to vaccinate kids?
During a security conference in Munich on Feb. 18, Bill Gates said:
“Sadly, the virus itself, particularly the variant called Omicron, is [a] type of vaccine — that is, it creates both B cell and T cell immunity — and it’s done a better job of getting out to the world population than we have with vaccines.”
Did Gates actually admit natural immunity to Omicron is succeeding where vaccines have failed — and that he’s “sad” about that?
Gates isn’t the only one talking about natural immunity these days.
Eric Topol, executive vice president of Scripps Research last month argued for including an option of natural immunity in the definition of “fully vaccinated.”
Even vaccine advocate Dr. Paul Offit, director of the Vaccine Education Center and member of the U.S. Food and Drug Administration’s vaccine advisory committee, is going to bat for recognizing natural immunity to COVID.
During a Jan. 25 interview, Offit described a meeting with Dr. Francis Collins, then-director of the National Institutes of Health, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, Dr. Rochelle Walensky, director of the Centers for Disease Control and Prevention (CDC) and U.S. Surgeon General Dr. Vivek Murthy where Offit was asked, along with three others, whether he thought natural immunity should count as a vaccine.
Offit and one other person said yes, natural immunity should count. But they were out-voted, leading U.S. health officials to decide natural immunity should not be recognized in the U.S, as an alternative to a vaccine mandate.
To this day, the CDC maintains this position in its official guidance for the public — despite the agency’s own studies showing natural immunity against COVID is superior to the immunity provided by COVID vaccines.
Some U.S. lawmakers think the CDC is wrong, as evidenced by the introduction of two the Natural Immunity Is Real Act in the Senate (S.2846) and the House (H.R. 5590).
The bills would require “all federal agencies to acknowledge and consider natural immunity to COVID-19 when promulgating any regulation related to the COVID-19 public health emergency.
But for now, in the U.S. at least, those states, businesses and schools requiring “proof of COVID vaccination” make no exceptions for people — including kids — who recovered from COVID, and therefore have natural immunity.
UK data show most unvaccinated kids already have natural immunity
Unfortunately, the CDC doesn’t provide up-to-date seroprevalence data for children in the U.S., but UK data may shed light on children and natural immunity.
“In the week beginning 10 January 2022, the percentage who would have tested positive for antibodies against SARS-CoV-2 ranged from 90.2% to 93.3% for children aged 12 to 15 years and from 63.3% to 72.7% for those aged 8 to 11 years across the UK. Estimates show the percentage of children testing positive for antibodies against SARS-CoV-2 at or above 42 ng/ml.”
In the UK, vaccines have not yet been made available for the under 12 age group (except those who are at very high risk). The 63.3 to 72.7% is thus overwhelmingly due to natural immunity and not vaccination.
Also, as noted by the ONS, individuals testing below the threshold level may also have natural immunity, presumably in the form of T cells and B cells, where the antibodies have waned. Thus these data may be underestimates of the true population-level immunity.
“It is estimated that over 85% of all children aged 5 to 11 will have had prior SARS-CoV-2 infection by the end of January 2022 with roughly half of these infections due to the Omicron variant. Natural immunity arising from prior infection will contribute towards protection against future infection and severe disease.”
The UK’s Joint Committee on Vaccination and Immunisation (JCVI) on Dec. 22, 2021, authorized the vaccine only for high-risk children ages 5 to 11.
Yet despite the encouraging data on natural immunity in this age group, the JCVI on Feb. 16, in updated guidance, expanded its recommendations to include a “non-urgent offer” of the vaccine to children who are not in a clinical risk group.
To be clear, the UK government authorized an mRNA vaccine for the original SARS-CoV-2 strain, to be made available in April, to a group of 5 million young healthy children — 85% or more of whom are expected to have natural immunity.
As John Campbell, Ph.D., said, if and when a future COVID wave ever comes, any possible beneficial effect from these shots will likely have waned.
Studies may explain why children are protected from SARS-COV2
A study in 2020 reported that cross cellular immunity and immunomodulation from previous existing childhood vaccines may provide protection against COVID infections.
A more recent study of children as young as 3 years old measured spike-specific T cell responses and found they were twice as high as those in adults. The authors suggested this is in part due to pre-existing cross-reactive responses to seasonal coronaviruses.
A January 2022 study demonstrated a protective effect from high levels of pre-existing immune cells generated by other coronaviruses like the common cold, which attack the proteins within the virus (nucleocapsid), rather than the spike protein on the virus.
According to the senior author of the study:
“The spike protein is under intense immune pressure from vaccine-induced antibodies which drives evolution of vaccine escape mutants. In contrast, the internal proteins targeted by the protective T cells we identified mutate much less.
“Consequently, they are highly conserved between the various SARS-CoV-2 variants, including omicron. This suggests that the existing cross-reactive T cells may provide better protection than an mRNA vaccine that focuses only on the original variant spike protein.”
Despite these studies, the latest data on how many children likely have immunity because they’ve recovered from COVID and the well-established scientific theory that natural immunity to a pathogen is superior to vaccine-induced immunity, places like New York City continue to demand proof of vaccination for all children age 5 and over in order for them to participate in extracurricular school activities, visit museums, zoos, theaters, gyms, and restaurants.
For the most comprehensive list of 150 research articles on natural immunity visit the Brownstone Institute.
LAST Thursday a group of senior doctors and scientists, alarmed by the Government’s deaf ear to their call for child Covid vaccination to be paused, convened a press conference to set out each and every reason, scientific and ethical, why this is so urgent. That the JCVI went into terrorist lockdown in response to four female doctors delivering yet another letter to its ‘chair’, Professor Wei Shen Lim, prior to a press conference that not one MSM health editor bothered to attend, is a scandal in itself. Far worse is the scandal of ‘guinea pig’ science that ever younger children are being subjected to, risking their health and futures for no need. This is what the press conference presentations, starting today with Dr Ros Jones’s account, make incontrovertibly clear.
Dr Ros Jones
As a retired paediatrician, I signed up for work with the General Medical Council [to assist with the Covid outbreak] back in April 2020; but actually they didn’t need me because what was very obvious early on was that the children’s ward was eerily quiet and they certainly didn’t need retired paediatricians going back to work. So that was a blessing and I went back to retirement. Unfortunately, there have been many other problems for children [arising] from the pandemic management.
It was about a year ago that I first saw advertised, on an evening BBC News, recruitment for a children’s vaccine in Oxford saying they were recruiting children aged five to 15. I was very shocked because at that stage we had no long-term adult safety data at all. I contacted Professor Pollard who was the professor leading the investigation and also, coincidentally, is [joint] chair of the Joint Committee on Vaccination and immunisation [JCVI].
I emailed him. I’ve known him through work, and he replied within the hour, saying: ‘Ooh, hi Ros, you’re quite right, we don’t know it’s safe, that’s why we’re doing the study’. He assured me it was a small pilot study, and if it was effective, then they would be looking to do a properly powered, full-size study. ‘There’s no way children will be receiving this vaccine within the year.’
I thought, Okay, but it was only two months after that that the Pfizer vaccine got its temporary authorisation in the States, and that’s when I wrote my first letter to the Government’s Medicines and Healthcare products Regulatory Agency (MHRA). We had about 60 names on the first letter, I think, and really we got that letter in before the MHRA had authorised [the vaccine for children]. They didn’t reply. They didn’t reply for ten weeks. We got a reply two hours after they had authorised the vaccine for children.
We wrote again, because every time the letters’ replies are just very bland; they don’t answer any of the individual questions that we posed about potential safety for children. They have usually been to say it’s the responsibility of the MHRA. But the MHRA, when they approved temporary authorisation for the 12s to 15s, they only looked at the Pfizer trial data. They did not look at the real world data. They said they haven’t. So they are looking at the data from a drug company that is going to be making all the profits on this.
So I thought I would start today by reminding us of the basics of how drug safety benefit works.
1. When the disease is worse than the cure, that is, when the disease is quite serious and the treatment has minimal side effects, I think we all understand that all drugs and treatments have potential side effects, but as long as the disease is worse than the cure, you’ve got a potentially useful drug.
2. When the disease more or less balances the cure, this is the next level down which is the sort of thing like you might be able to buy over the counter, but the NHS wouldn’t be spending its money on it, but at least it doesn’t do you any harm.
3. When the disease is milder than the cure. Of course, the worst situation is this, the bottom one, and that’s not a situation we want to be in. Now, obviously, [there are] quite a lot of drugs when they’re being developed, that may be discovered during the development phase, and drugs never reach the market. But it’s not uncommon for drugs to get to market where rarer side effects come to light or perhaps delayed side effects that have not been picked up on the original trials. And when that happens, then a drug gets either withdrawn completely or really restricted in its use.
So just a quick example, of course, with the AstraZeneca [vaccine] and the blood clots. At the beginning we were told, ‘Oh no, ten million doses and only ten cases,’ but when you actually looked at it, there was a very strong age stratification and it was then withdrawn for anybody under 40. So that was acting on a signal. But we turn now to Pfizer. And with the Pfizer, what seems to be the problem largely is myocarditis and that is very much age-related. So we’re in a situation where children have the least impact from Covid itself, but they have the most impact from potential side effects, particularly myocarditis.
In the US, 16-to-17-year-olds are the highest group with an incidence of 1 in 9443 for this complication. Israel, they looked a bit more systematically [and] they were the first people to spot this problem. From the moment they noticed it, they sent letters out to all their paediatricians, all their emergency departments, to tell them to look out for this. And they found [it to be] 1 in 6,230. This is young men after their second dose of Pfizer. And it’s interesting because their data – they looked at all age groups, and for the over-30s it was 1 in 72,000. So there’s a tenfold difference in risk if you are over 30 versus under 20. But the Covid risk is tenfold the other way. So your risk-benefit balance has changed by 100-fold by your age. This mantra, ‘safe and effective’, is not fit for purpose.
Hong Kong rolled the vaccine out to children a bit later, by which time they knew about myocarditis and they have just looked systematically from the beginning of the programme, and they, in fact, decided to halt the second dose when they found – for the Hong Kong 12-17s- it was 1 in 2680 getting myocarditis. And that’s just at the stage that here we went from one dose to two doses.
It’s described as mild and it goes away. But there have been child deaths reported in the States. I’ve personally been in Zoom calls with the group of cardiologists from the States who’ve been doing cardiac MRI scans, and they found that 89 per cent of these children, whose symptoms had gone, had significant changes on the scans with swelling and potential scarring of heart muscle. And the JCVI, in the minutes of their meetings last summer, wanted to have six months to follow that up and see what’s happened to those kids over time. But that was overruled, as we know.
You can watch Dr Jones and her colleagues here in a full recording.
Throughout the Covid-19 pandemic, proponents of lockdowns, shelter-in-place orders, mask mandates and other coercive government interventions have characterized these measures as benevolently “erring on the side of caution.”
Now, as the grim toll of those public health measures comes into ever-sharper focus, it’s increasingly clear those characterizations were terribly wrong.
What’s less readily apparent, however, is how the very use of the “erring on the side of caution” framing was injurious in itself—by thwarting reasoned debate of public health policies, diverting attention from unintended consequences, and buffering the Covid regime’s architects from accountability.
To understand how the misuse of “erring on the side of caution” performed a sort of mass hypnosis that coaxed populations into two years of submission to disastrous, overreaching policies, consider how the expression is typically used.
In everyday life, one might err on the side of caution by:
Leaving for the airport an extra 30 minutes early
Carrying an umbrella when there’s a 25% chance of rain
Opting for a less-challenging ski slope
Going back into the house to make sure the iron is unplugged
Getting a second medical opinion
Generally speaking, “erring on the side of caution” in everyday life means lowering risk with a precaution that has a negligible cost.
When mandate proponents portrayed their edicts as “erring on the side of caution,” it had the effect of tacitly assuring the public—and themselves—that there’d be little or no harm associated with extreme measures like:
Shutting down businesses for months at a time
Knowingly forcing millions of people into unemployment
Halting in-person attendance at schools and colleges
Ordering people of all ages and risk profiles to wear masks
Denying people opportunities to socialize, recreate and enjoy living
That implicit low-downside assurance not only fostered unthinking support for draconian measures among citizens and experts alike, it also cultivated an atmosphere of intolerance toward those who questioned the wisdom of these interventions and predicted the great many harms that have resulted.
“Overconfident, unnuanced messaging conditioned us to assume that all dissenting opinions are misinformation rather than reflections of good faith disagreement or differing priorities,” write Rutgers professors Jacob Hale Russell and Dennis Patterson in their essay, The Mask Debacle. “In doing so, elites drove out scientific research that might have separated valuable interventions from the less valuable.”
Of course, in addition to its implicit assurance that a risk-reduction measure comes at little cost, “erring on the side of caution” conveys an assumption that the precaution will actually be effective.
Public Health Threw Out the Playbook and Threw Pandora’s Box Wide Open
The masses who’ve chanted “I trust science,” as they praise each government intervention and idolize those who impose them, are likely unaware that, before Covid-19, the well-considered scientific consensus was against lockdowns, broad quarantines and masking outside of hospital settings—particularly for a virus like Covid-19 that has a 99% survival rate for most age groups.
For example, a 2006 paper published by the Center for Biosecurity of the University of Pittsburgh Medical Center—focusing on mitigation measures against another contagious respiratory illness, pandemic influenza—reads like a warning label against many of the policies inflicted on humanity in the face of Covid-19:
“There is no basis for recommending quarantine either of groups or individuals. The problems in implementing such measures are formidable, and secondary effects of absenteeism and community disruption as well as possible adverse consequences… are likely to be considerable.”
“Widespread closures [of schools, restaurants, churches, recreations centers, etc] would almost certainly have serious adverse social and economic effects.”
“The ordinary surgical mask does little to prevent inhalation of small droplets bearing influenza virus… There are few data available to support the efficacy of N95 or surgical masks outside a healthcare setting. N95 masks need to be fit-tested to be efficacious.”
The point of that and other pre-2020 research into pandemic mitigation was to be prepared, in times of crisis, with policies that reflected a well-reasoned and dispassionate weighing of costs and benefits.
However, when the pandemic arrived, panicking public health officials and academics threw out the playbook and took their policy inspiration from the government that was first to confront the virus. Sadly for the world, that was communist China.
The breadth of the resulting harms from the ensuing plunge into public health authoritarianism is staggering. Far from erring on the side of caution…
Public health erred on the side of a mental health crisis. Anxiety and depression have surged, particularly among adolescents and young adults, where symptoms have doubled during the pandemic.
“I have never been as busy in my life and I’ve never seen my colleagues as busy,” New York psychiatrist Valentine Raiteri told CNBC. “I can’t refer people to other people because everybody is full.”
Public health erred on the side of juvenile suicide attempts. In the summer of 2020, emergency room visits for potential suicides by children leapt over 22% compared to the summer of 2019.
Public health erred on the side of drug overdoses. According to the National Institute on Drug Abuse, overdose deaths surged 30% in 2020 to a record-high of more than 93,000. Among the factors cited: social isolation, people using drugs alone, and decreased access to treatment.
Public health erred on the side of auto fatalities. Traffic deaths had been on a general downtrend since the 60s, reaching a near-record low in 2019. However, even with shutdown-lightened traffic, deaths jumped 17.5% in the summer of 2020 compared to 2019, and kept rising into 2021.
Blame increased drug and alcohol use, along with psychological fallout from people being denied life’s fundamental pleasures. University of Texas cognitive scientist Art Markman toldThe New York Times that anger and aggression behind the wheel in part reflects “two years of having to stop ourselves from doing things that we’d like to do.”
Public health erred on the side of domestic violence. A review of 32 studies found an increase in domestic violence around the world, with the increases most intense during the first week of lockdowns. “The home confinement led to constant contact between perpetrators and victims, resulting in increased violence and decreased reports,” the researchers found.
Public health erred on the side of riots, arson and looting. It’s my own conviction that 2020’s eruption of summer violence following a Minneapolis police officer’s callous homicide of George Floyd was greatly magnified by the period of forced mass confinement that preceded it.
Floyd’s death was a match dropped into a tinderbox of humanity confined to veritable house arrest. People blocked from restaurants and bars were suddenly granted a societal waiver to venture out into enormous crowds, where they found excitement, socialization and, far too often, a senselessly destructive means of venting months of pent-up energy, anxiety and frustration. It stands as the costliest civil unrest episode in American history.
Public health erred on the side of confining people where the virus is transmitted most. Lockdowns ordered people away from workplaces, schools, restaurants and bars and into their homes, where New York contract tracers found 74% of Covid spread was happening, compared to just 1.4% in bars and restaurants and even less in schools and workplaces.
Public health erred on the side of obesity. According to the CDC, “the risk of severe COVID-19 illness increases sharply with higher BMI [Body Mass Index].” Sowhat happens when public health “experts” shut down schools, workplaces and recreation options and told people to stay home to stay “safe”?
The CDC found that, in 2020, the rate by which BMI increased among 2- to 19-year olds doubled. Another study found that 48% of adults gained weight during the pandemic, with those who were already overweight most likely to add even more. Among other factors, the study pointed to psychological distress and having schoolchildren at home.
Public health erred against fresh air, exercise and Vitamin D. Governments raced to shut down playgrounds, basketball courts and other outdoor recreation facilities. In a move that’s profoundly emblematic of heavy-handed, counterproductive authoritarianism in the age of Covid, the city of San Clemente, California filled a skate park with 37 tons of sand.
Public health erred on the side of impaired child development. “We find that children born during the pandemic have significantly reduced verbal, motor, and overall cognitive performance compared to children born pre-pandemic,” say the authors of a study from Paediatric Emergency Research in the UK and Ireland (PERUKI).
“Results highlight that even in the absence of direct SARS-CoV-2 infection and COVID-19 illness, the environmental changes associated [with the] COVID-19 pandemic [are] significantly and negatively affecting infant and child development.”
Public health erred on the side of learning loss. Children are less vulnerable to Covid-19 than they are to the flu, and rarely transmit it to teachers. Unfortunately, American public health officials and teacher unions prevailed in halting in-person instruction (and socialization) in favor of “remote learning.”
It was a poor substitute that fell hardest on the youngest learners. For example, according to curriculum and assessment provider Amplify, the percentage of first-graders scoring at or above the goals for their grade in mid-school-year dropped from 58% before the pandemic to just 44% this year.
Public health erred on the side of pointlessly masking schoolchildren. When schools did open, mask mandates abounded—despite children’s relative invulnerability to the virus and the documented rarity of in-school transmission. A Spanish study showed no discernible difference in transmission among 5-year-olds—who aren’t required to mask—and 6 year olds, who are.
“Masking is a psychological stressor for children and disrupts learning. Covering the lower half of the face of both teacher and pupil reduces the ability to communicate,” wrote Neeraj Sood, director of the Covid Initiative at USC, and Jay Bhattacharya, professor of medicine at Stanford. “Positive emotions such as laughing and smiling become less recognizable, and negative emotions get amplified. Bonding between teachers and students takes a hit.”
“Most of the masks worn by most kids for most of the pandemic have likely done nothing to change the velocity or trajectory of the virus,” writes University of California associate professor of epidemiology and biostatistics Vinay Prasad. “The loss to children remains difficult to capture in hard data, but will likely become clear in the years to come.”
Public health erred on the side of giving masked people a false sense of security. As I wrote in August, “Covid-19 particles are astoundingly small. Hard as it is to imagine, the imperceptible gaps in surgical masks can be 1,000 times the size of a viral particle. Gaps in cloth masks are well larger.” That’s to say nothing of the respirated air that simply goes around the mask’s edges.
Earlier in the pandemic, questioning cloth masks triggered outrage and swift social media censorship. Now, even mandate-happy CNN medical analyst Leanna Wen has declared they’re “little more than facial decorations.” Mask skepticism is sprouting elsewhere in mainstream media; the Washington Post and Bloomberg even published an essay titled “Mask Mandates Didn’t Make Much of a Difference Anyway.”
When public health officials exaggerated the power of masks, they did more than promote pointless discomfort and a dystopian way of life. “Naively fooled to think that masks would protect them, some older high-risk people did not socially distance properly, and some died from Covid-19 because of it,” said epidemiologist, biostatistician and former Harvard Medical School professor Martin Kulldorff.
Public health erred on the side of killing small businesses. Thanks in large part to government’s targeting of so-called “non-essential businesses,” the first year of the pandemic brought an additional 200,000 business closures over prior levels.
Public health erred on the side of harming women’s careers. Women comprise a greater proportion of the sectors hid hardest by lockdowns, and the closing of schools and child care centers prompted many more women than men to put their careers on hold.
Public health erred on the side of inflation. To offset the massive economic destruction inflicted by public health shutdowns, the federal government plunged into an astounding spending spree, handing out cash to individuals, businesses and city and state governments.
It was money the government didn’t have, so the Federal Reserve essentially created it out of thin air. Pushing all that new fiat money into circulation debases the currency, fueling today’s surging price inflation—which is a stealth tax with no maximum rate, which hits poor people hardest.
Note: Lockdowns and other mandates weren’t the exclusive driver of many of the various harms I’ve described; general fear of the virus also contributed to some of them. However, it should also be noted that public health officials—and media that overwhelmingly emphasized negative stories—whipped up a level of fear that led people to overstate the level of danger actually posed by the virus.
There’s one more way in which characterizing lockdowns and other mandates as “erring on the side of caution” plays a psychological trick: Since the phrase is embedded with the notion of good intentions, it conditions citizens to be forgiving of the bureaucrats and politicians who imposed them.
Note, however, that in most everyday usage of “erring on the side of caution,” the choice to “err” is made voluntarily by individuals who bear the consequences of their own decisions—or by others, like an airplane pilot or a surgeon, to whom we’ve voluntarily and unmistakably granted control of our well-being.
The grim impacts of lockdowns and other mandates, however, were coercively imposed on society, to say nothing of the fact that so many of the edicts represented gross usurpations of power and violations of human rights.
On top of all that, the edicts were reinforced by Orwellian censorship and ostracism leveled at those who dared raise questions that have now proven valid.
So make no mistake: Overreaching public health officials and politicians—and the journalists-in-name-only who served as their mindless, unquestioning megaphones—have fully earned our withering condemnation. Indeed, holding them accountable is essential to sparing ourselves and future generations from repeating this dystopian chapter of human history.
When I find myself arguing with pro mandate Australians in social media comment sections (tragic, I know) I get the impression that they desperately want the last couple of years they’ve squandered to have been worthwhile.
Australia’s official Covid19 death rate happens to be low by international standards, which makes it easier for the Dan Andrews fanboys to delude themselves that the sick cruelty they inflicted on their fellow citizens was justified.
For a recap, this cruelty includes but is not limited to:
Prolonged mass house arrest
Vaccine Passports
Vaccine injuries and deaths in individuals (often young and not at serious risk from Covid) who were coerced into getting it.
The four newborn babies in South Australia who died after domestic Covid19 travel restrictions prevented them from being transferred for specialist life-saving emergency treatment in Victoria.
In Western Australia, the prevention of unvaccinated parents from visiting their sick children in hospital.
If I was Australian Prime Minister Scott Morrison, (that snivelling, gaslighting, modern-day Pontius Pilate), I would not want to admit that pointlessly I stole two years of quality life from my citizens and presided over state policies that killed people,
“Australians have made many sacrifices during this pandemic,… together we have achieved one of the lowest death rates in the world,” he says.
Achieved? Everywhere in the Oceania region has a low death rate by global standards. When will Papua New Guinea’s PM be praised for his inspirational leadership? Don’t hold your breath, but PNG is Australia’s immediate neighbour, (and the only other country on Earth with kangaroos), yet has a lower Covid19 death rate than does oz.
Could that be because of the success of PNG’s vaccination rollout? Did they her the sheep through the gate, so to speak?
Vaccination rate for Australia (at least one dose): 85%
Vaccination rate for PNG (at least one dose): 3.4%
Since we are only allowed to compare Sweden with its neighbours, it’s only fair that the same rules must apply to everyone. I assume vaccine passports aren’t really a thing in PNG. But they seem to be coping without them.
Covid19 deaths per million for Australia: 193/1M
Covid19 deaths per million for PNG: 69/1M
Most countries in Europe have relatively high death rates, though the few nations that had extremely low death rates (Norway and Finland) did not have the strictest measures. Lockdown rejecting Sweden’s death rate is firmly in Europe’s lower half.
At present, the UK is the least restricted country in Europe, possibly in the developed world and has been since July 2021, yet our (questionably recorded) Covid19 death rate is only the 22nd highest in Europe, currently slightly lower than that of Italy, which has vaccine passports and vaccine mandates, and surgical masks remain compulsory.
What would Australia’s death rate be were it somehow squeezed into the North Atlantic or continental Europe? We cannot know.
Two weeks ago, BKK ProVita chairman Andreas Schöfbeck caused a small uproar by writing to Germany’s vaccine regulator, the Paul-Ehrlich-Institut, to inquire about the high rate of vaccine side-effects evident from BKK billing data.
Representatives from the Paul-Ehrlich-Institut, including its president, Klaus Cichutek, had agreed to meet with Schöfbeck and other BKK officials about their concerns this afternoon. Schöfbeck’s termination was obviously timed to prevent his participation at that meeting, which will now go forward without him.
This is the behaviour of people who have deep confidence in the safety and effectiveness of our Corona vaccines.
More evidence is emerging of Google manipulating algorithms powering its mammoth and highly influential search service to give certain results (much) more visibility than others.
And now, reports say, Google is not even trying to hide that this is the case, as America’s Frontline Doctors (AFLDS) has been informed its reach on the internet is being artificially limited.
This organization says it is dedicated to improving doctor-patient relationships that are jeopardized by what it calls politicized science and biased information. The AFLDS would also like to provide patients with access to “independent, evidence-based information” that will inform people’s decisions regarding their healthcare choices.
Well, meeting that goal might prove to be quite difficult since Google Search, on which a huge majority of US-based users rely for their internet queries, says it is deliberately deranking information coming from the AFLDS.
This transpires from alerts Google has been sending the organization, which state that an “issue” has been detected, which can be “fixed;” after that, the AFLDS can “request review.”
And when an “issue” has been detected, Google spells it out that “Pages affected by manual actions can see reduced display features, lower ranking or even removal from Google Search results.”
So what “issues” have been detected, you might ask next. Google’s “explanation” is the usual hodgepodge of vague language and qualifiers, in line with the giant’s now well-established censorship style.
The AFLDS is informed that its site “appears to violate” Google’s medical content policy, which is not allowed – and neither is content that “contradicts or runs contrary to scientific or medical consensus and evidence based best practices.”
That’s according to Google’s rules. What consensus, reached by who, and what best practices, determined by who, and at what time – none of this information is provided in the notices.
Google’s rigid, authoritarian style of promoting one-sided content and eliminating different arguments and positions would in this case work by first deranking (and eventually removing) AFLDS links – unless the group agrees to self-censor.
And that means deleting content from the site, and then clicking on “‘Request Review’ button which is prefaced with the question, ‘Done fixing?’,” the AFLDS explains.
The organization also takes issue with Google’s (deliberately) broad and ambiguous wording and lack of proper, or any definition of scientific and medical consensus and best practices – to ask why, “In a time when celebrities and computer programmers are allowed to express their views on virology, but actual doctors and scientists are censored, including the hundreds of doctors comprising AFLDS, such clarity is elusive.”
Gabrielle asked if she could record the call and I consented, so that entitles all parties to record the call. PolitiFact did not deny that we both consented. She wrote,
I am not in the least embarrassed by how she conducted the interview. I’m asking that you remove the video as a professional courtesy because the reporter did not consent to be recorded.
First of all, she should be embarrassed by the interview. The interviewer was clearly focused on proving an agenda and showed no interest in exploring evidence that was counter her agenda. I gave her the story of the century if she would just follow up on what I suggested she do.
Secondly with respect to permission, by asking me if it was OK to record the call, she is giving implied consent for the call to be recorded since she is doing the asking. All parties on the call consented to being recorded meaning the conversation is no longer private and all parties can record the call.
The debate challenge
I then raised the stakes: I challenged PolitiFact to a debate to settle the matter once and for all in front of a live Internet audience as to who are the liars and who are the truth tellers. Here is the email I sent on Feb 25, 2022 at 2:58pm PST:
A good, old-fashioned debate.
They can have as many people as they want on their side, the more the better since it will remove all excuses when they lose.
The purpose is simple: to ascertain who is really spreading misinformation.
After all, the US Surgeon General has said how dangerous COVID-19 misinformation is. So has the California State Legislature: In House Resolution No. 74 of the 2021–22 Regular Session, the California State Assembly declared health misinformation to be a public health crisis, and urged the State of California to commit to appropriately combating health misinformation and curbing the spread of falsehoods that threaten the health and safety of Californians.
The fastest way to stop all COVID misinformation is to challenge the spreaders of the misinformation and discredit them in a debate
Of course, the problem with a debate is that usually one side wins. If it is the misinformation spreaders, the narrative is crushed. This is why nobody wants a debate: they can’t take the risk.
PolitiFact can’t win a fair debate. There is way too much information out now on how dangerous the vaccines are that is impossible for them to explain.
This is why I don’t think that there is a snowball’s chance in hell they will accept.
I sent the email to Angie earlier today and have not heard back. I will update this article if I do. Don’t hold your breath.
Watch the video that they don’t want you to see
The video they wanted me to remove exposes how the fact checker had absolutely no interest in exploring any of the evidence that proved that the VAERS data was correct.
In short, the video proves that these so-called fact checkers aren’t interested in the facts; they are interested in defending the false narrative.
Be sure to check out the original story (it’s point #5 in this article), and be sure to watch the video if you haven’t already. It shows just how biased these fact checkers are.
The CDC warns in boldface lettering on its website, “[k]nowingly filing a false VAERS report is a violation of Federal law (18 U.S. Code Section 1001) punishable by fine and imprisonment.”
Not only are there criminal penalties for filing false VAERS reports, but physicians or medical providers file a majority of them. Dr. McCullough says health care providers file 60 to 80% of VAERS reports. You can verify this by reading the reports.
Whoever files the report has to have the lot number and batch number of the vaccine and it’s fairly time consuming process. McCullough says that the CDC has analysts call whoever entered the report in order to verify it. McCullough has received those calls.
Doctors are of course not compensated for filing VAERS reports so they often don’t file them. Most are probably unaware that they are required to file VAERS reports. No one gives them training on filing VAERS reports. Hospital employees have said their hospitals don’t even know about the requirement to report VAERS injuries.
They define COVID-19 misinformation as anything going against the government narrative.
In short, they want to take away the free speech rights of doctors who would no longer be allowed to question anything the government says. After they do that, citizens will be next.
Byram tried to debate the authorities in Canada, but they were a no show. He likes courts because the other party is forced to appear.
Here is what he wrote:
Hi Steve, I can’t get any of the narrative-pushers in Canada to debate the science. It would be great if you could have some success with this in the US. But, I agree with you; they almost certainly won’t. Those who don’t stand on the science will never engage in a conversation. People who love the narrative need to start asking their ‘champions’ why they keep refusing to step into the arena with the dissidents. At some point they are going to have to admit that their ‘champions’ are cowards and do nothing more than ‘talk the talk’ from behind their keyboards. A lack of scientific expertise becomes quite apparent when one has to respond off-the-cuff to another scientist in real-time. One place that the ‘experts’ for the narrative cannot hide is in court. So far, I have been seeing them crushed in this venue. This is why many court decisions are being made on technicalities; to avoid ruling on the evidence, the weight of which is not in favor of the narrative.
They are censoring doctors in the UK
From the comments:
GPs have been warned that criticising the Covid vaccine or other pandemic measures via social media could leave them ‘vulnerable’ to GMC* investigation.’1
*GMC = General Medical Council. This is the body that can strike doctors from the medical register so they cannot work as a doctor.
‘Vulnerable to GMC investigation’. What a deliciously creepy phrase that is, dripping with unspoken menace, whilst pretending to be helpful. It sounds like something the Mafia would come up with.
‘I would keep quiet about this, if I were you.’ Baseball bat tapping gently on the floor. ‘No, this is not a threat, think of it as advice from a friend. We don’t like to see anybody making themselves, or their family, vulnerable, and getting seriously injured now, would we?’
It seems that, unless you prostrate yourself before the mighty vaccine, and intone ‘Our vaccine, which art in heaven, hallowed be thy name…’ and suchlike, you will be attacked from all sides … simultaneously. Indeed, to suggest that vaccines are not perfect in every way is the twenty first century’s equivalent of blasphemy.”
AHPRA, the regulator of ‘health practitioners’ here, issued a Position Statement dated 9 March 2021, which states: “Vaccination is a crucial part of the public health response to the COVID-19 pandemic. Many registered health practitioners will have a vital role in COVID-19 vaccination programs and in educating the public about the importance and safety of COVID-19 vaccines to ensure high participation rates.”
Health practitioners are also warned: “Any promotion of anti-vaccination statements or health advice which contradicts the best available scientific evidence or seeks to actively undermine the national immunisation campaign (including via social media) is not supported by National Boards and may be in breach of the codes of conduct and subject to investigation and possible regulatory action.” (Search for AHPRA position statement 9 March 2021 to download PDF.)
Who defines what is “the best available scientific advice”? We know what a disastrous quagmire of conflicts of interest is “the best available scientific advice”…
In regards to ‘anti-vaccination’, in practice, any questioning of Covid jabs in Australia is regarded as ‘anti-vaccination’, as tennis star Novak Djokovic discovered when he tried to come here recently to participate in the Australian Open. The Immigration Minister banished Djokovic from Australia because he “has previously stated that he ‘wouldn’t want to be forced by someone to take a vaccine’ to travel or compete in tournaments”. For being an individual wanting to retain his bodily autonomy, Immigration Minister Alex Hawke considered the presence of Djokovic “may be a risk to the health of the Australian community”, presumably as Djokovic might inspire Australians to make their own informed decision about the Covid-19 jabs, counter to government diktats. (See the court judgement here: https://www.judgments.fedcourt.gov.au/judgments/Judgments/fca/full/2022/2022fcafc0003 )
What does the antagonism against Novak Djokovic mean for critical thinking Australians who have similarly made their own informed decision to refuse to consent to Covid jabs that don’t prevent infection nor transmission, injections which purportedly provide questionable ‘protection’ of very limited duration, against a disease it was known from the beginning wasn’t a serious threat to most people?
Now we have a dire situation in Australia where millions of people have been coerced to be jabbed to maintain their livelihoods under state government and business/employer mandates, this directly flouts the obligation for valid voluntary consent to be given before vaccination.
After perseverance, I finally received a response from AHPRA, which confirms: “Practitioners have an obligation to obtain informed consent for treatment, including vaccination. Informed consent is a person’s voluntary decision about health care that is made with knowledge and understanding of the benefits and risks involved.” See: https://vaccinationispolitical.files.wordpress.com/2021/10/response-from-ahpra-re-informed-consent.pdf
But this isn’t happening! With so many people being coerced and manipulated into submitting to the jabs under state government and business/employer mandates, this isn’t authentic voluntary consent. The situation is really bad in Australia, which I suspect is possibly the most mandated jab country in the world.
Summary
We want to make sure people know the truth about PolitiFact. I literally handed Gabrielle Settles the story of the century and she had no interest at all in pursuing any of it.
If PolitiFact and others want to end misinformation, all they have to do is debate us. Instead, governments are passing laws to censor doctors since they don’t have the facts on their side.
All over the world, governments do not want the people to hear the fully story.
israel has been a good laboratory for covid intervention assessment. they are a small nation in one climate zone with a small population, good record keeping, a pretty honest set of health agencies, and modern healthcare system. they did lots of testing and they also pursued damn near every mitigation in the book from lockdowns to masking to mandating vaccines and vaccine passports. and unlike many places, they were extremely serious about compliance. they even have an very useful control group in palestine that did almost none of these things.
this provides an interesting opportunity to measure the efficacy of such interventions. at this point, it’s so well established that masking and distancing have no effect that we can more or less drop them from consideration and focus solely on vaccines. (to the extent they worked, they would drive apparent vaccine efficacy in israel anyhow).
and the two states have had remarkably similar overall outcomes and had near identical cumulative deaths per capita through 2021. however, it looks like this might be starting to diverge and this creates a useful comparison.
about three weeks ago, i left THIS POST with some questions:
we now have enough data to start to answer this.
the relative vaxx rates are very different and israel is over 50% boosted vs ~0 in palestine. so, if boosters are working, this is about as good a natural experiment setup as you could ask for.
cases are a problematic metric due to variance in testing rates (and we know vaccines do not stop cases) and palestine does not report hospital data. but we can compare deaths, so this is the figure i used.
this series is striking. as has commonly been the case, palestine lagged israel by a couple weeks. (i suspect this is reporting lag, this data is day of report, not day of incidence).
assuming this peak holds, the palestine peak was 21% below winter seasonal peak last year. israel was up 13%. that’s a meaningful divergence and the israeli figure is deeply unexpected given a milder variant and 18 months of vulnerable cohort depletion.
this starts to hint at something being quite wrong and also starts to rule out “variant” as the source, because it did not drive that outcome in palestine.
it can be notoriously difficult to eyeball area under curve, so i have plotted cumulative deaths here:
as can be seen, israel had gone pancake flat in november 2021 through jan 2022. then it inflected severely. this is omicron which hit the levant in the second half of december 2021. clinically, you’d expect about a 24 day log to show up in deaths and this tends to jibe with the data i’ve seen all over the world.
it’s possible that boosters were having some effect in bending the curve, but to the extent that they did, it was either fleeting or rapidly inverted in the face of a new variant. (or both)
this becomes extremely easy to see when we zoom into 2022 and start a cumulative count from 1/1/2022.
there is a powerful inflection in israel that does not exist in palestine and israel has seen roughly twice the cumulative per capital death rate of palestine so far this year.
if boosters are effective in preventing deaths from omicron, it sure does not show up here.
this also lets us rule out “omicron” as a source of greater underlying virulence/fatality. if this were so, it would be manifest in both places. the fact that it is not doing so supports the idea that omicron is an OAS/hoskins effect evolution taking advantage of the narrow antigenic fixation generated by mRNA and adenovirus vaccines. it also seems to show that this advantage is NOT, as many claim, limited to cases. it seems to carry through to deaths as well.
we can also compare israel to itself and see how this highly vaccinated and boosted period compares to the prior year when vaccination was zero. from this data as well, we see strong support for the OAS hypothesis.
israel had been doing better. then omi came and everything changed.
(to remove the skew from widely varying sample rate driven by big shifts in testing levels, i have normalized all cases data to 10 tests per day per 1000 population though given the absurdity of calling a high Ct PCR+ a “case” even lacking symptoms, all case data is troublesome to assess, but we work with what we have, not with what we wish we had)
cases nearly tripled and hospitalizations nearly doubled. deaths rose 13%.
according to israeli authorities and hospitals, this was not driven by “the unvaxxed” but rather by the vaccinated. they seem to make up more than their share of severe outcomes though one must we wary of simpson’s paradoxes. (more HERE)
it might be possible to construct an argument whereby vaccine efficacy is claimed on any given infection (once you are sick, better to be vaxxed) but if that is, in aggregate, swamped by a rise in cases (and we knowvaccines lead to more cases, not fewer) then this is still not much of an argument. having vaccines reduce risk of hospitalization per case by 50% but tripling case risk is still a 50% rise in overall hospitalization.
the aggregate data is possibly supportive of this claim outcome, but it’s far from certain either way.
but still, if the overall outcomes are worse post vaxx in the active arm but not in control, from a public health perspective do we really care why?
cases were trending MUCH lower. then that changed in a hurry.
zooming in makes it all the more clear.
even adjusted for testing, this is a massive surge in cases.
we see the same in hospitalization.
and see the crossover to worse outcomes in 2022 when we zoom in.
overall, they are 39% higher in aggregate YTD vs prior yr.
deaths have not yet caught up, but appear likely to do so.
taken as a whole, this is pretty damning of the booster programs.
israel saw a big spike in deaths that was not present in the palestine control group.
it saw a massive jump in cases, a big jump in hospitalizations, and is rapidly converging on deaths (which will lag the others by ~3-4 weeks).
there is just no way to spin this as a win. it looks like an own goal.
this was the known and knowable outcome of widespread inoculation with a leaky vaccine. it is, in fact, WHY we do not use leaky vaccines.
they will rapidly and inevitably select for escape or vaccine enhanced variants. and now it makes you worse and worst of all, locks you into a suboptimal antigenic response pattern that may keep you from EVER generating real sterilizing immunity. the truly nasty part of this may take years to really see.
omicron was not “bad luck” it was invoked consequence of ill conceived intervention. even assuming they ever worked as claimed (dubious) these vaccines were always going to fail because that’s what leaky vaccines do.
this was known and knowable. the drug companies that made them knew it. the regulatory agencies that approved them knew it. and many, many doctors, researchers and public health officials all over the world knew it. they were silenced, threatened, and attacked for it. and this is the bitter fruit of that harvest.
in the US, the data has been manipulated and misused so badly as to render it outright fraud. it becomes obvious when one compares the US data (which calls all “unknown or undetermined” patients “unvaxxed” and used the fact that the EPIC system is awful to create a false sense of VE) with a system that keeps good records as longtime gatopal™ HOLD2, newly on substack, has done here.
like so much of the rest of the covid response, we knew better than to do this, but it was done anyway.
and now, the US is lying about it while others are, at least, coming clean.
but this truth will be too vast to hide much longer, even behind these big lies.
and american health and regulatory agencies are going to have a great deal to answer for.
dr atlas (with whom many at rational ground, including even notorious internet felines, had the pleasure to collaborate) is correct in everything he says here except in his use of the world “almost.”
Dr. Scott Atlas on the CDC data scandal: "They put forward pseudoscience trying to manipulate the public and push an agenda … Our data is simply not to be trusted because the CDC is a politicized, agenda-driven, almost disgrace to the country." pic.twitter.com/EnQOEXl2wQ
My last blog discussed the possibility that mRNA COVID19 vaccines significantly increase the risk of myocarditis. Following this, a fellow doctor reached out to tell me about what has happened to them. They too, had questioned some aspects of the safety and efficacy of the vaccines.
As a result, they have been sent two threatening letters, which are both of the ‘iron fist in a velvet glove’ variety. I asked their permission to reproduce them here. One is from the General Medical Council (GMC). The other from their responsible officer – I shall explain what this title means a bit further on.
Below is the letter from the GMC:
Dear Dr….
The GMC have received several complaints regarding your recent social media posts.
All doctors have a right to express their personal opinion regarding the Covid-19 vaccine, and while the GMC in no way supports this opinion, we don’t consider your comments are sufficiently strong to open a fitness to practice investigation at this stage.
However, we are referring this matter to your Responsible Office for your reflection through the appraisal process.
We ask that you consider what implications this complaint might have for your practise when you are discussing this with your appraiser. We would also like to remind you of GMC guidance, in particular ‘Doctors’ use of social media, and of the requirement of doctors to act with honesty and integrity to justify the public’s trust in them
What we will do now
We will share the complaint with your responsible officer for them to consider in the wider context of your practice and revalidation.
‘The wider context of your practice and revalidation.’ Which means what, exactly? I sometimes wonder if there a special training scheme where you learn to write creepy and threatening phrases that can later be denied as being creepy and threatening? ‘I was only trying to be nice. They just took it the wrong way.’
‘Your children look charming. However, you may want to consider their continued existence on the planet in the wider context of your practice.’
The GMC, as mentioned before, have the powers to investigate complaints made against doctors in the UK, and impose various punishments (they call them sanctions, which sounds far prettier). Ranging from nothing very much to permanent erasure from the medical performers list.
The latter means that you cannot work as a doctor ever again. Anywhere in the world. The GMC will communicate your erasure to other national statutory bodies, upon request. They do it gladly… and speedily.
On the face of it, in this case, the GMC have decided to do nothing. ‘We don’t consider your comments are sufficiently strong to open a fitness to practice investigation at this stage.’
Jolly good.Nothing to see here, move along. Although they add the rider … ‘at this stage.’ Well, what other stages are left, after deciding to take no action? The … I have changed my mind and I am going to have you guillotined, stage?
However, in reality they have not done nothing – have they dear reader? The GMC have decided to refer the complaint to this doctor’s responsible officer. A responsible officer is a doctor who is ‘responsible’ for ensuring that other doctors working in their area have met the necessary requirement for revalidation.
Revalidation is a five-year cycle whereby a doctor has to meet various requirements. A few hundred hours of medical education, keeping up do date with mandatory training. Carrying out an audit, and a patient satisfaction questionnaire, getting sufficient colleague feedback, and suchlike.
There is also a need to have a yearly appraisal. Which is a meeting with an allocated appraiser, to discuss how things have gone. A look through any complaints about you, work you have done, audits that have been completed, actions to take in the next year to improve your practice – a personal development plan. Release of thumbscrews – or a tightening.
If all this is done successfully, over a five-year period, the responsible officer ‘signs you off’ and you are now able to continue work. If not, you are removed from the performers list, and you cannot work as a doctor until you are successfully re-validated. No-one has ever explained to me how you actually do get revalidated. In fact, there is no system in place for this to happen.
If you manage to fulfil the re-validation cycle, and attend appraisals, in theory there can be no grounds for removal. You cannot actually ‘fail’ an appraisal. You simply have to turn up, and ‘reflect’ on your practice. I have never heard of a responsible officer stepping in to remove a doctor from the performers list any time they so wish.
Bearing all that in mind, here is the follow up letter from the responsible officer.
Dear Dr….
I have today received a communication from the GMC regarding an ‘incident that occurred on social media.’ The GMC have advised that they have reviewed the complaint and that it does not meet the threshold for investigation.
However, I understand that you have been asked to consider what implications this complaint may have for your practise and there is a requirement for you to reflect on this matter at your next appraisal meeting.
As your Responsible Officer I have a statutory duty to ensure that any concern or complaint about your practise is responded to and dealt with appropriately.
I would be grateful if you could let me have your views on this issue, by completing the attached form and returning it as a matter of urgency.
Can you also complete the attached Monitoring of Clinical Practise for your file, please.
Your co-operation with this process is vital in order for us to come to an acceptable resolution as soon as possible, minimising impact to your practice and cost in time and money.
If you have any questions regarding this process, please to contact me to discuss further.
Kind regards
Dr X
Responsible Officer for X region.
I love the ‘Kind regards’ sign off. For this is a letter dripping with unspoken menace. Just to highlight one phrase ‘An incident that occurred on social media…’ An ‘incident’. You mean, someone wrote something that someone didn’t like, they then complained about it. This was not an incident, in the sense that anyone would normally choose to use this word.
[I also note that the GMC spells practice, practice. The responsible officer spells it practise – maybe they need to reflect on their spelling between them].
If you look up the word ‘incident’ on the Cambridge Dictionary it gives an example of its use:
‘A youth was seriously injured in a shooting incident on Saturday night.’1
It does not say. ‘Someone wrote a blog post that upset someone, somewhere, for a bit. But it’s alright now, they are looking at pictures of kittens to recover.’
Words. Words, words, words. They can be used in so many different ways. Their true meaning hidden behind layers of sophistry. But we all know what the word ‘incident’ means in this case. Someone was badly damaged by your actions on that day – do not attempt to deny it, comrade.
Then we move on to the real threat. The responsible officer wants to ensure an acceptable resolution, thus … ‘minimising impact to your practise and cost in time and money.’
What the responsible officer here is saying is that I have the powers to stop you practising medicine in the UK. If I find that your answer to this complaint – which was not strong enough to open a fitness to practice investigation by the GMC – does not satisfy me. Indeed (subtext), I do not actually care what answer you give, I may remove you anyway. This will certainly maximise the impact on this doctor’s ‘practise and cost in time and money’.
If you think this is not what is being threatened. Then ask yourself what else it could mean? There is nothing that needs to be ‘resolved’. A complaint has been made, but the GMC didn’t think it was serious enough to take forward. No patient was harmed, no laws broken … no wrecks and nobody drowned, in fact nothing to laugh at, at all. (small prize for who knows where that came from).
At this point you may have begun to allow the thought to enter your mind that the GMC have quite deliberately handed this complaint down to the responsible officer to carry out the required sentence and execution. Whatever the accused doctor says, the responsible officer can simply respond. ‘Sorry, not satisfied with your answer. I am now going to stop you working – for as long as I wish.’ No hearing, no possibility of review, no accountability. Bosh.
In truth I have always known that responsible officers possess this amazing and unrestrained power. I tried, and failed, to stop this happening years ago – when I was on various British Medical Association (BMA) committees. I found it incredible that the legislation in this area was going to hand over, to one individual, the ability to destroy someone’s career, with no regard to anyone else, or anything else.
Yes, we live in a democracy that has created a form of local tyranny.
Tyranny (noun) def: government by a ruler or small group of people who have unlimited power of the people in their country or state and use it unfairly, and cruelly.
You could say that this situation suits the GMC very well … Very well indeed. Because, you see, the GMC has tried to remove other doctors from the medical register for criticising vaccination. [The medical register is not quite the same thing as the performer’s list, but you need to be on both of them to work as a doctor in the UK].
These punishments were quashed in the High Court. Here from a legal firm that works in this area:
‘On Friday, the High Court handed down a judgment quashing the GMC interim order of conditions previously imposed on a GP, Dr Samuel White, as a result of his actions arising from the pandemic. Dr White came to the GMC’s attention as a result of “spreading misinformation and inaccurate details about the Coronavirus and how it is diagnosed and treated”. His comments have included assertions that the COVID-19 vaccine “inserts a code”, masks do “absolutely nothing” and hydroxychloroquine, budesonide inhalers and ivermectin are “safe and proven treatments”.
The interesting point arising from Dr White’s High Court appeal is the technical point on which he won. The High Court found that the Medical Practitioners Tribunal Service (MPTS – the adjudication wing of the GMC) panel made an error of law in not properly considering the test required by section 12(3) of the Human Rights Act 1998 when deciding whether to impose an interim order.’2
As this company also says:
As time goes on, we’re seeing more fitness to practise cases arising from COVID-19-related activities. We’ve previously posted about the Irish GP interim suspended after describing COVID-19 as a hoax and the first UK nurse struck off by the Nursing and Midwifery Council (NMC) as a result of COVID-19 denial activities.
‘COVID denial activities’ – what a deliciously Soviet phrase.
I have to say that I very much enjoyed the lawyers’ assertion that the GMC interim order was quashed on a ‘technical point’. Namely that the GMC had failed to consider the small matter of the Human Rights Act 1998. Riding roughshod over someone’s human rights is now a technical point of law. How quaint.
However, undeterred, the GMC have not been deterred from their vital work in punishing COVID-19 vaccine deniers – to ensure that they can never work again. They have just found another, simpler, far cheaper, and far quicker route to obliterate a doctor’s career. Call the responsible officer. No-one expects the responsible officer.
Who needs time consuming and costly hearings, where you might have to bear in mind the Human Rights act 1998 – and other such woolly liberal nonsense? When you can alert the local ‘tyrant’ to a doctor’s non-comradely Soviet ‘denial’ activities. Sorry, COVID19 ‘denial’ activities.
They will know precisely what to do, and they have the powers to do it. Why on earth did the GMC not think of this of this before? I could have told them about the ridiculous, frightening, and untrammelled powers of a responsible officer, but they never asked me.
Of course, you could argue the following. If the local responsible officer does obliterate someone’s medical career and does this without paying any heed to such things as well, the law, for example, then their actions will be over-turned in court. Well, I certainly hope so, in fact I would expect so. This may act as a deterrent … maybe.
However, during the months, or years, that it takes to get such a case to court, the doctor will be out of work and unable to earn. They will almost certainly end up bankrupt, and their reputation (have been struck off the performers’ list) will lie shattered in the gutter.
As for the responsible officer. Their punishment ‘please don’t do it again,’ would just about cover it. This is very much asymmetric warfare. I can punish you, terribly, but you can do absolutely nothing to me in return.
In the financial world they call this moral hazard. A banker can bankrupt you, and your family, and half the country, making stupid and risky decisions – that will earn them huge short-term bonuses. If, as a result, their bank goes bust, the Government simply bails them out and they keep their job, and their bonus. All gain, no pain.
As a sign off, the responsible officer (washing his hands of any personal responsibility of course) wrote this ‘I have a statutory duty to ensure that any concern or complaint about your practise is responded to and dealt with appropriately.’ Kind regards … Pontius.
However, one thing that has not happened, so far, is to actually take the time and effort to forward a copy of the complaints to the doctor concerned. Still, they must be guilty of something or other. So, it is clearly critical that they respond to these unknown complaints, of some sort or another, in some-way or other. ‘Here is a bottle of whisky, and a revolver…. You know what you must do.’
What a world this has become. I had hoped I would not live to see such a time in this country, but I have.
By Lisa Pease | Consortium News | September 16, 2013
More than a half century ago, just after midnight on Sept. 18, 1961, the plane carrying UN Secretary-General Dag Hammarskjöld and 15 others went down in a plane crash over Northern Rhodesia (now Zambia). All 16 died, but the facts of the crash were provocatively mysterious. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.

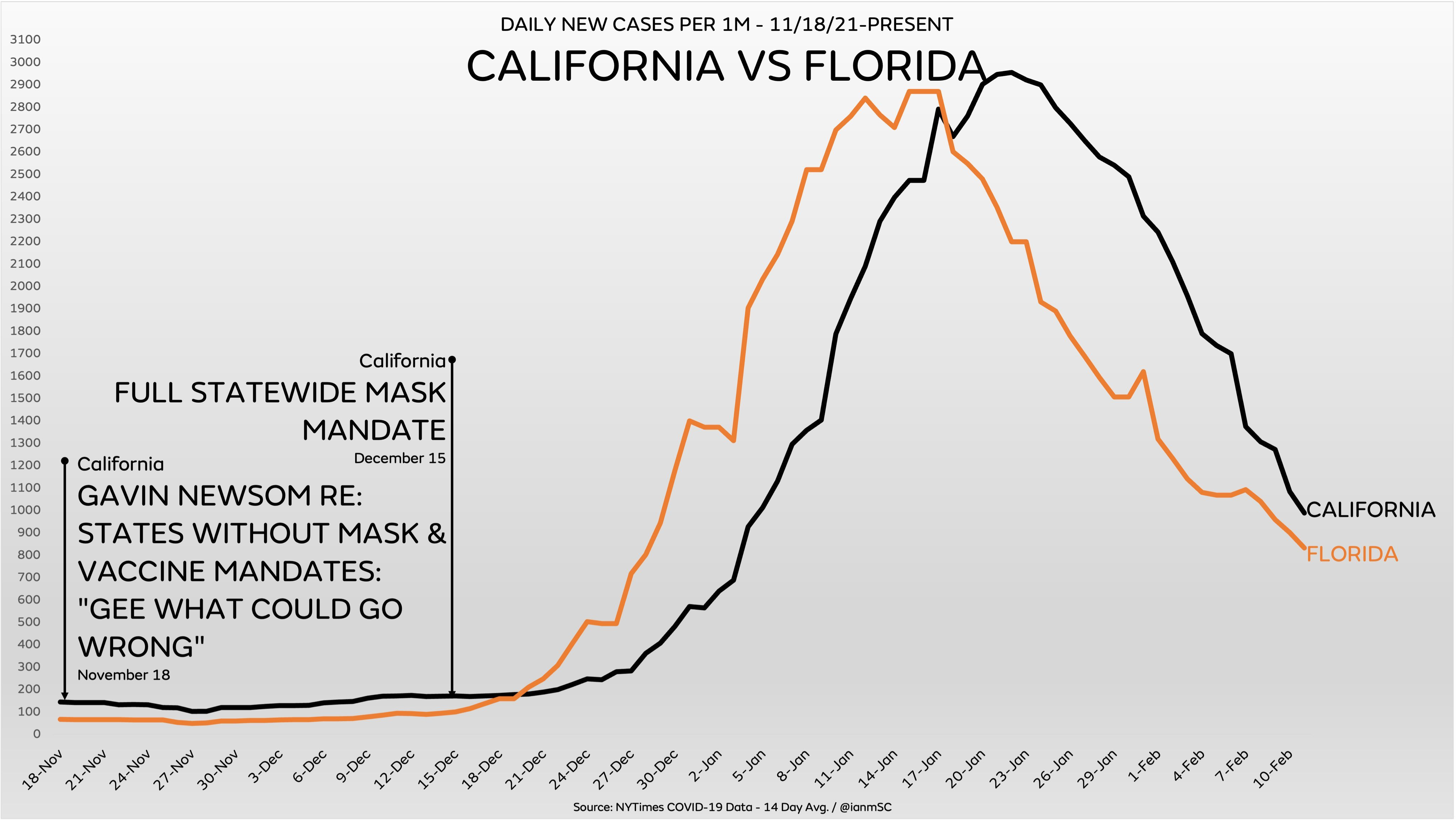
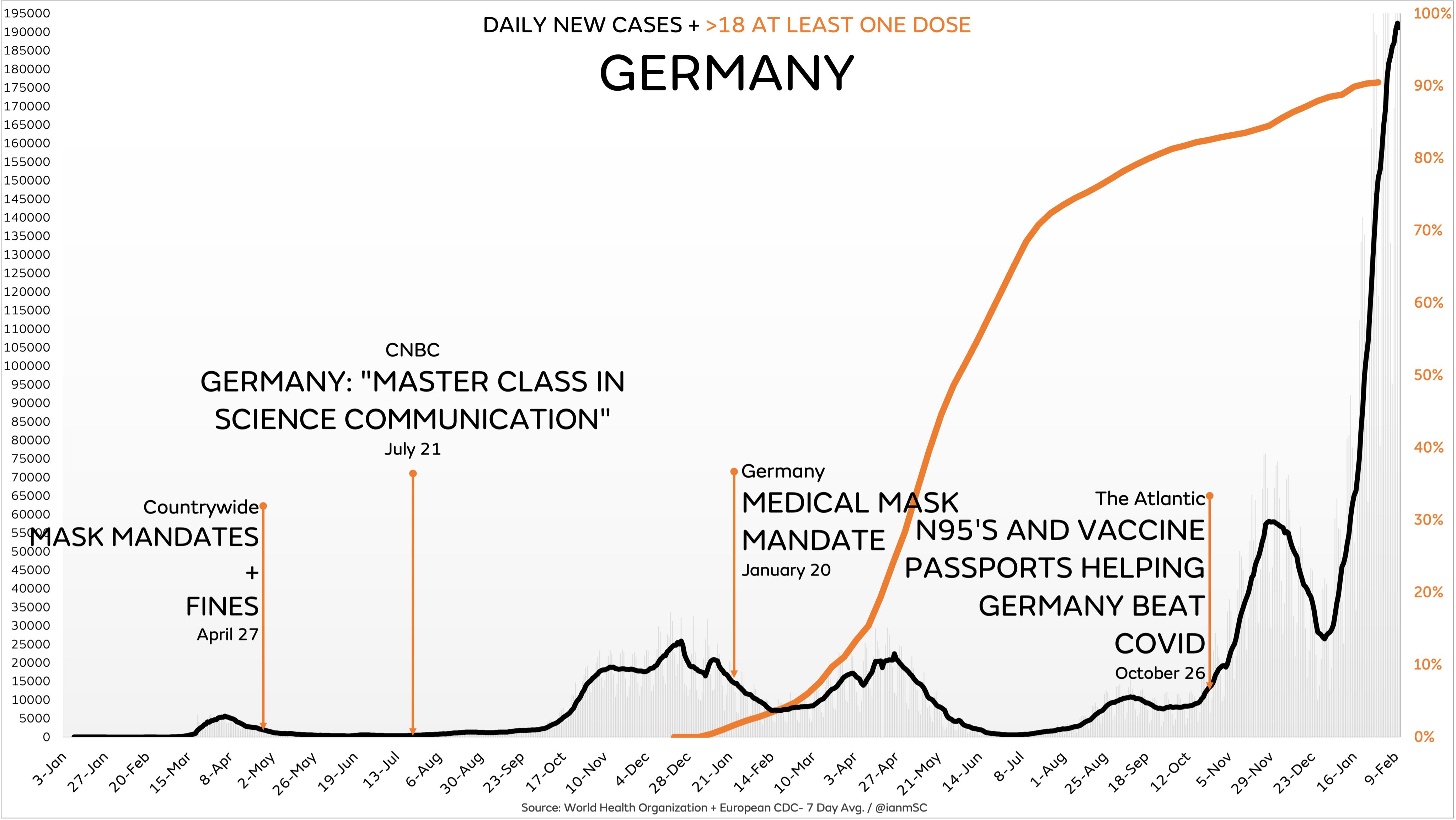
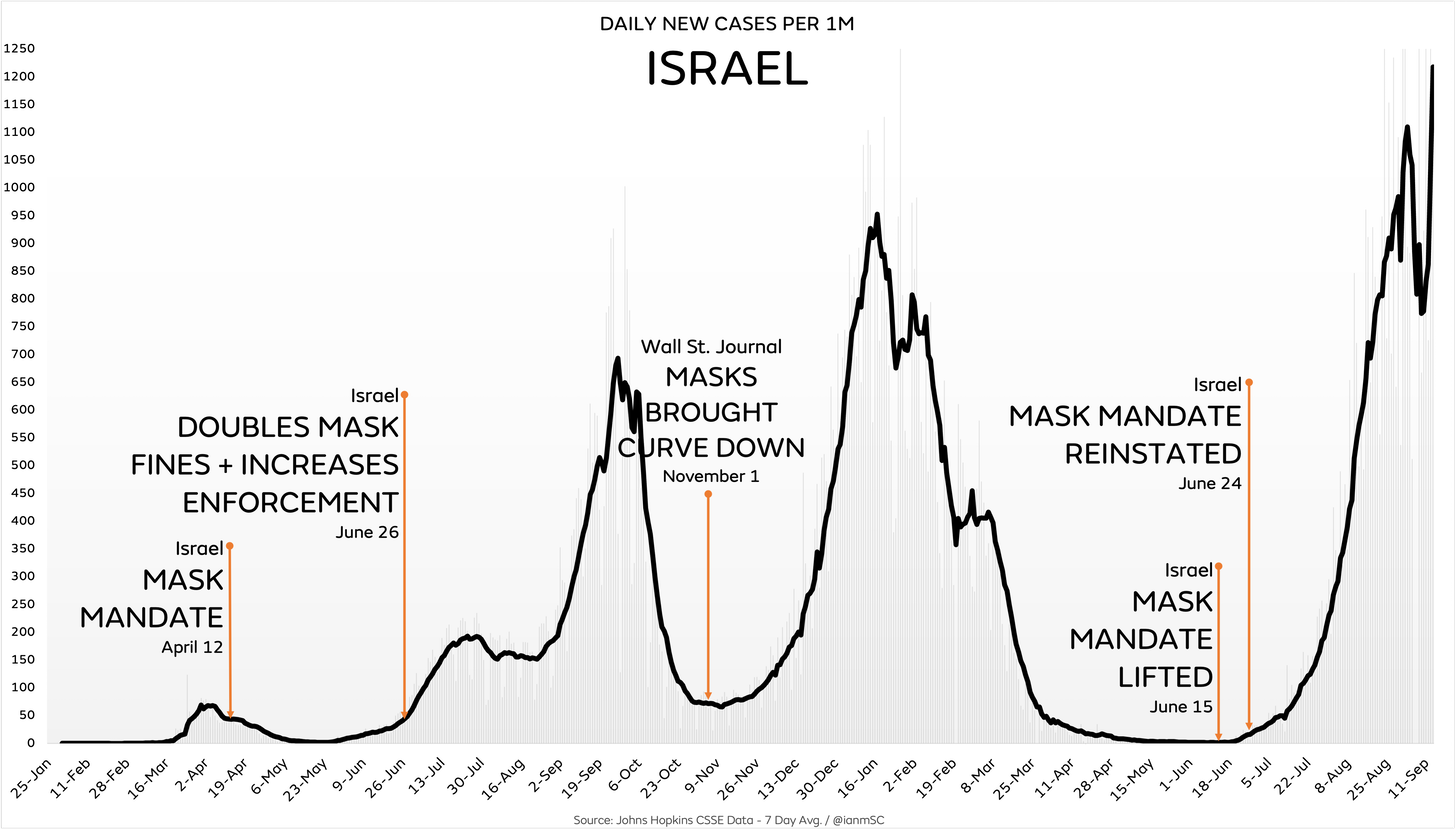

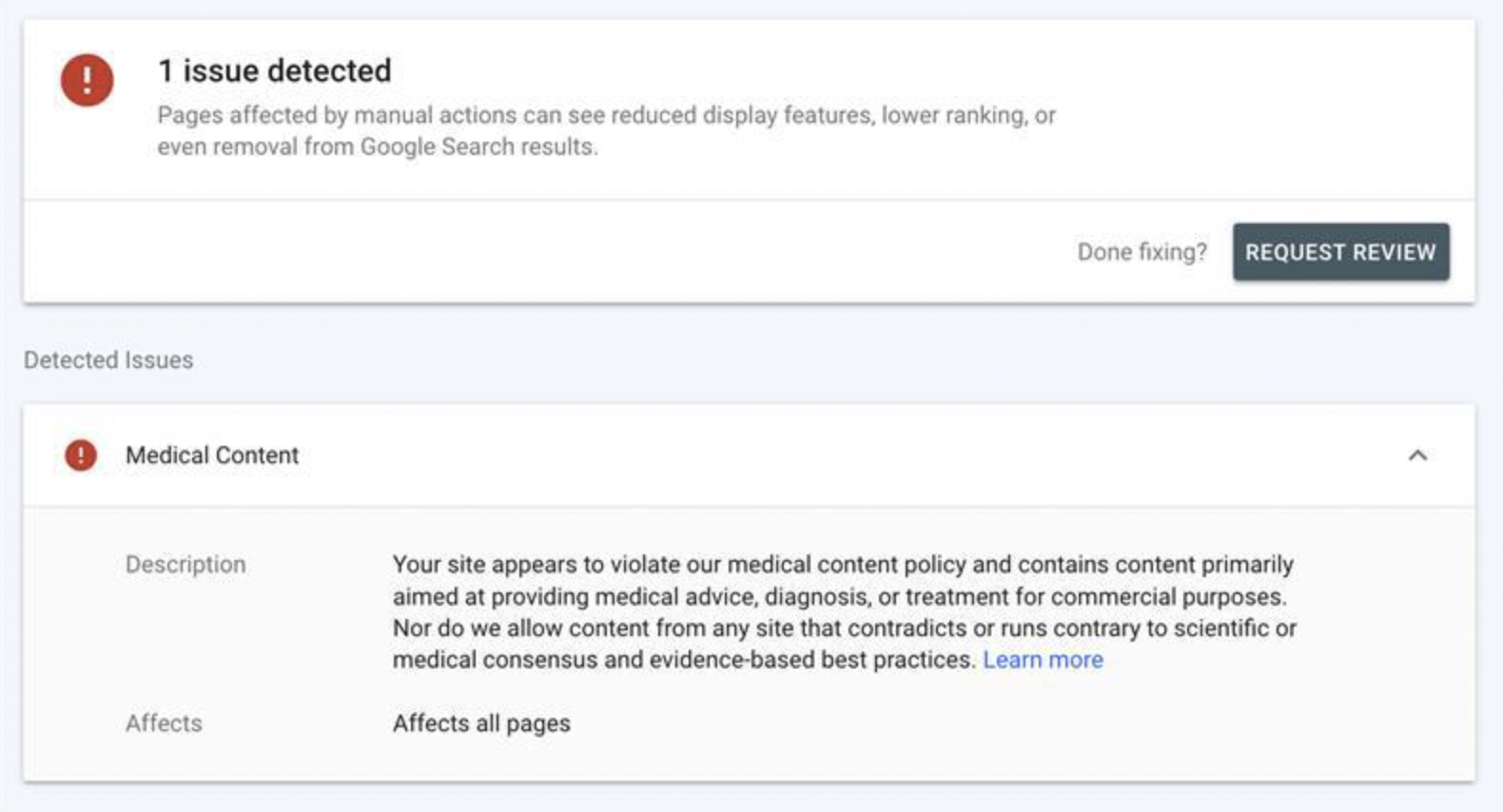
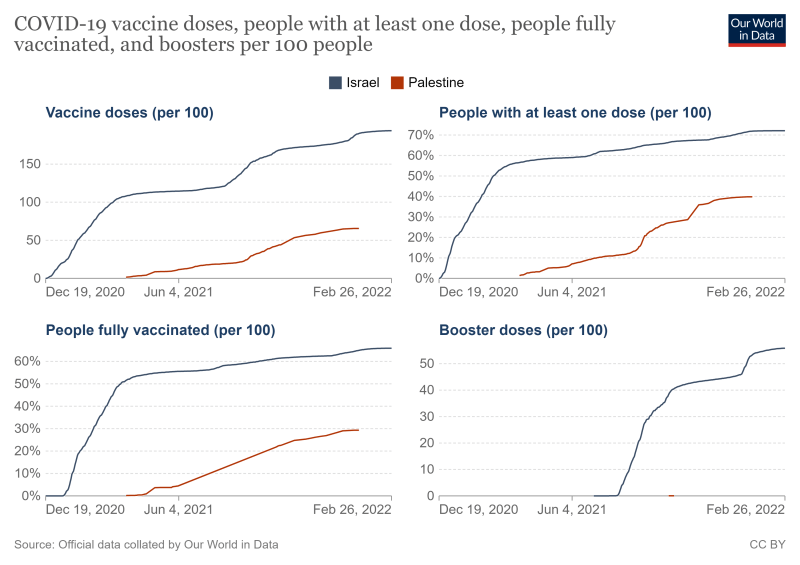
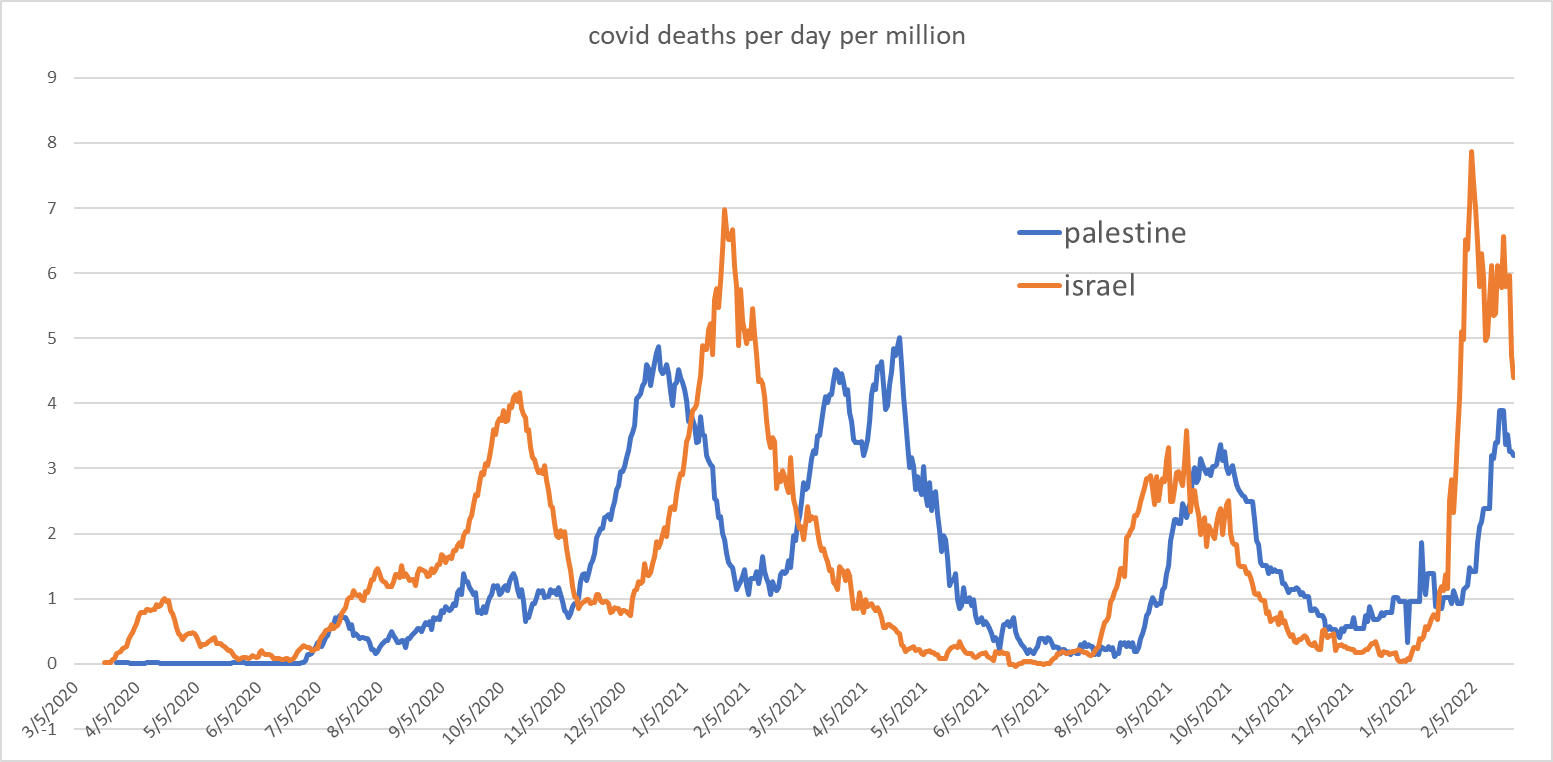
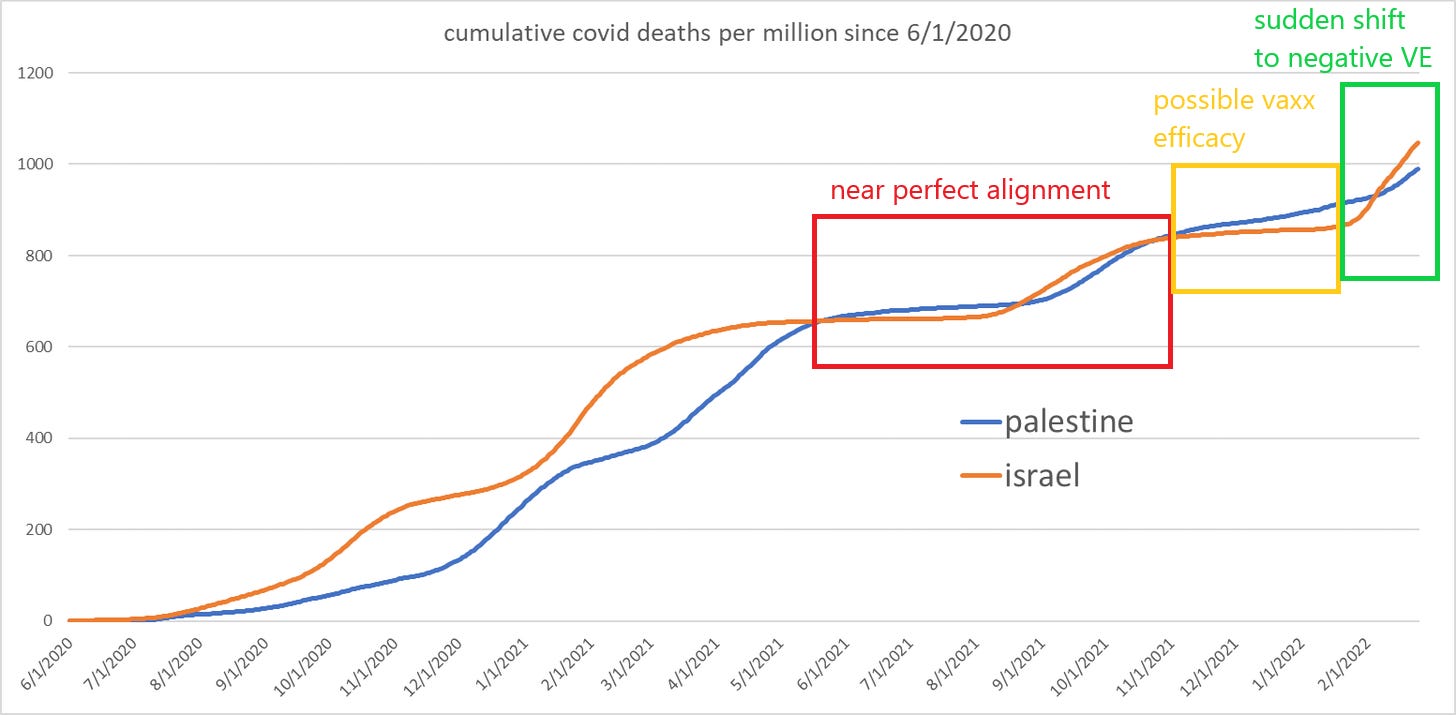
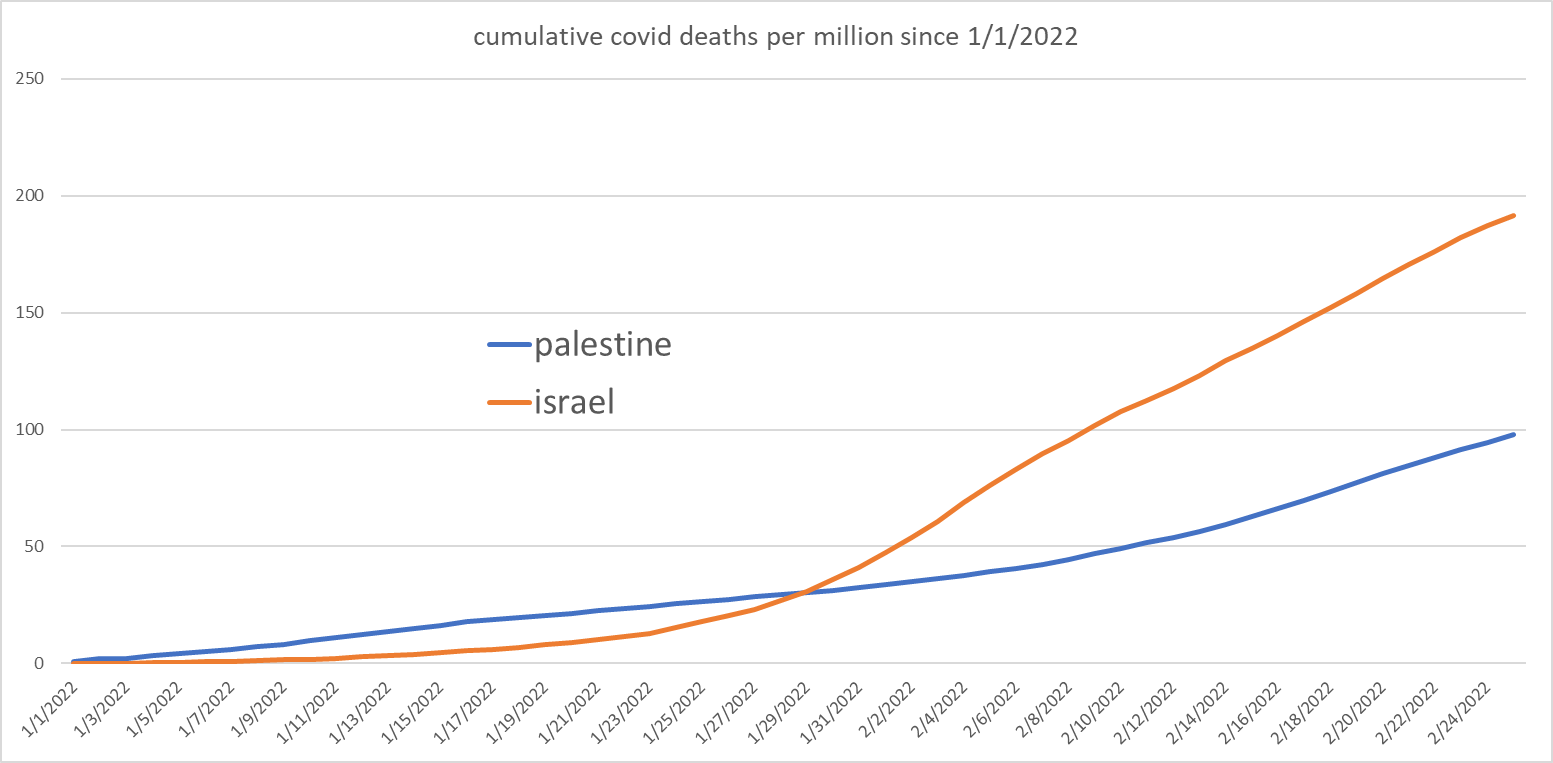
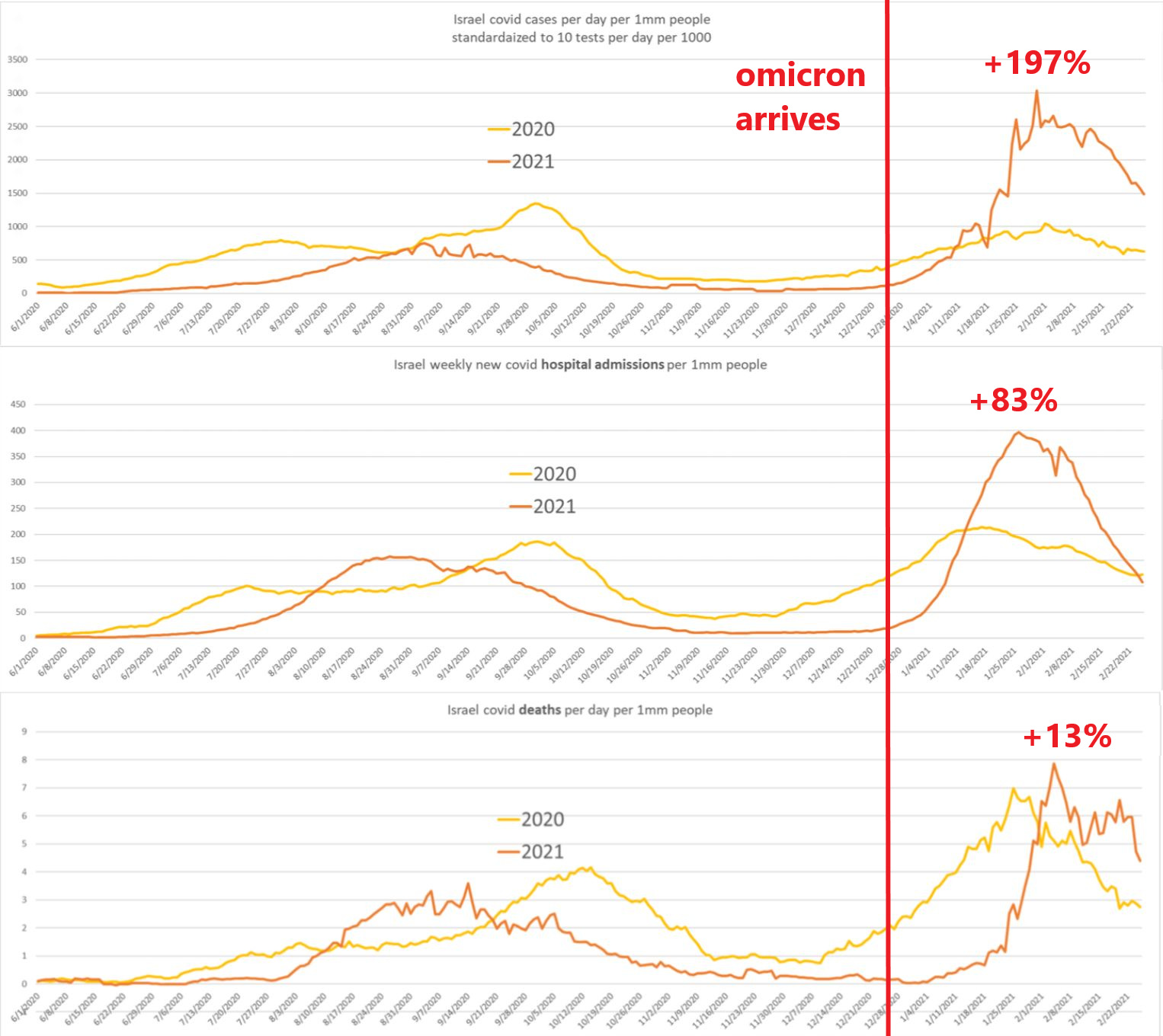
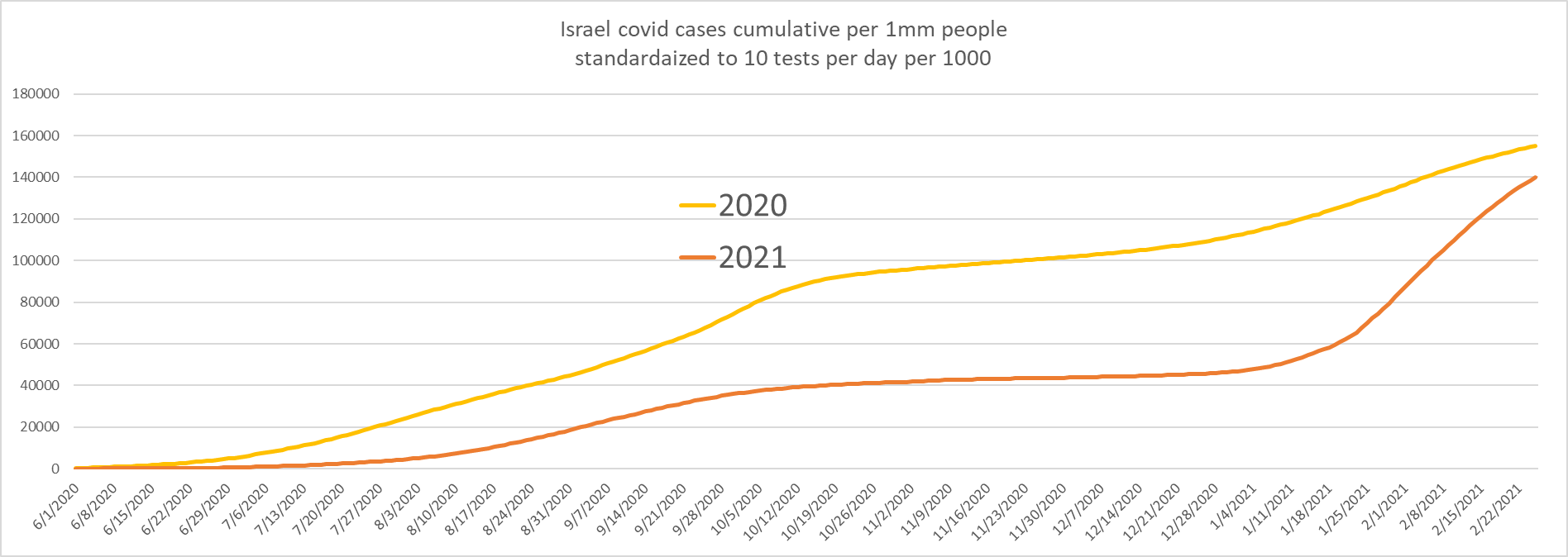
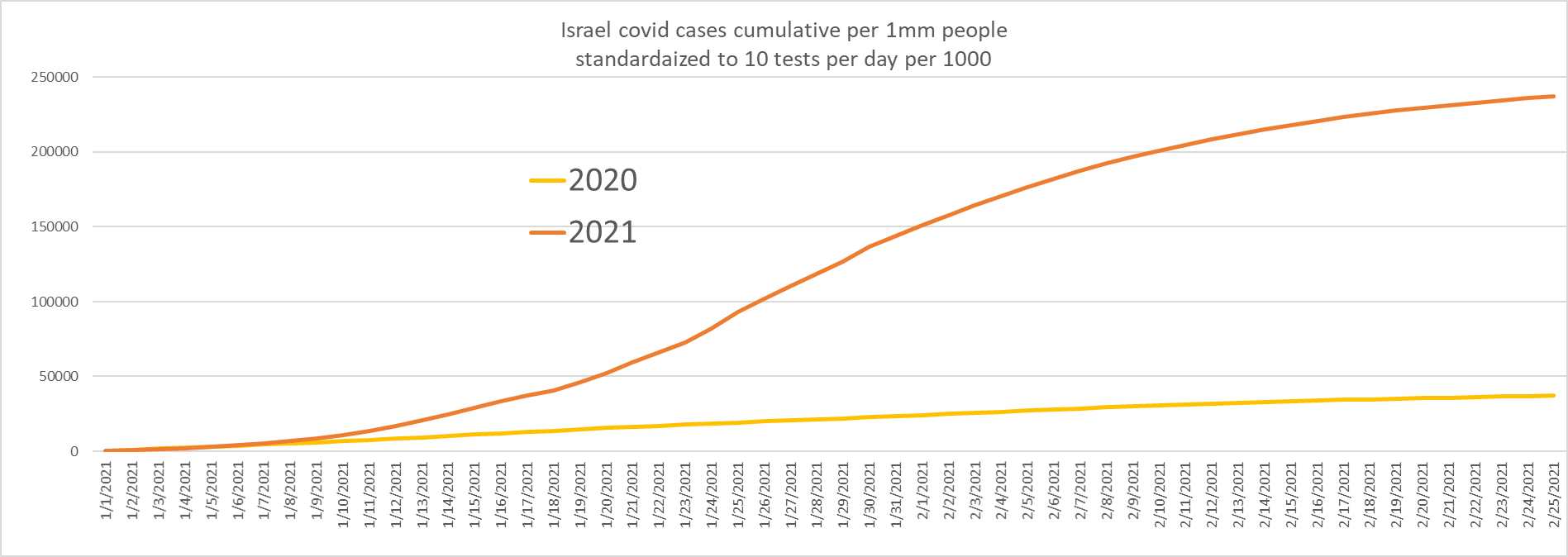

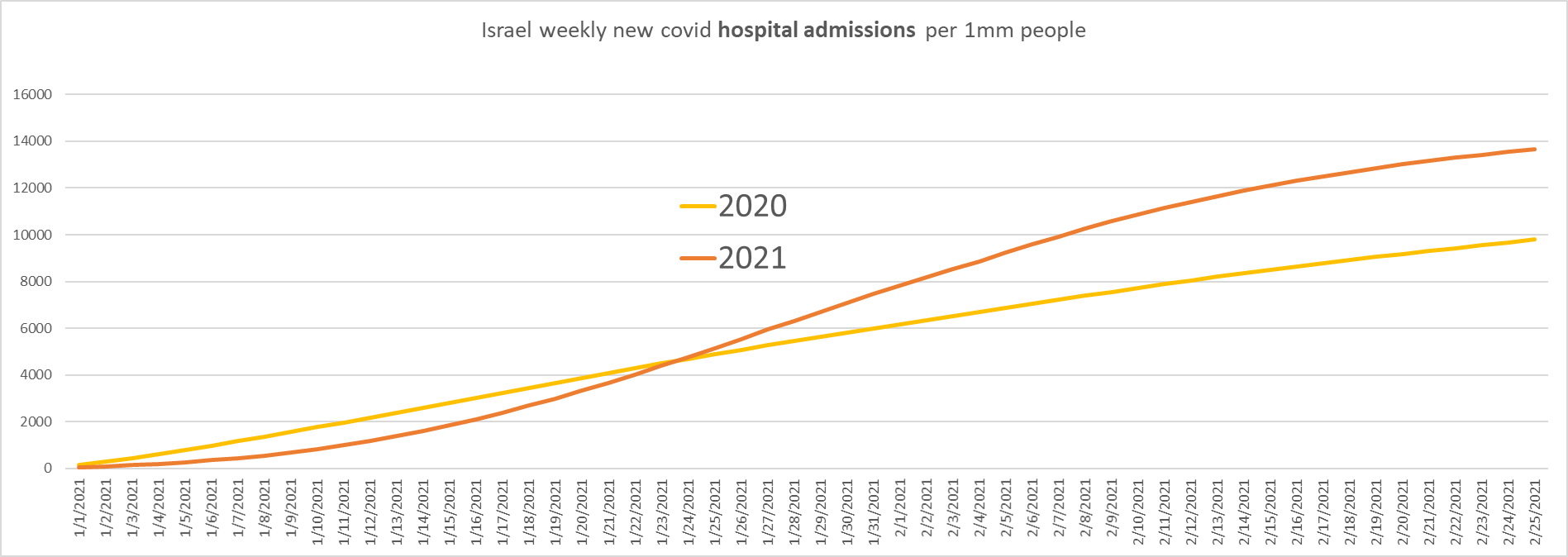
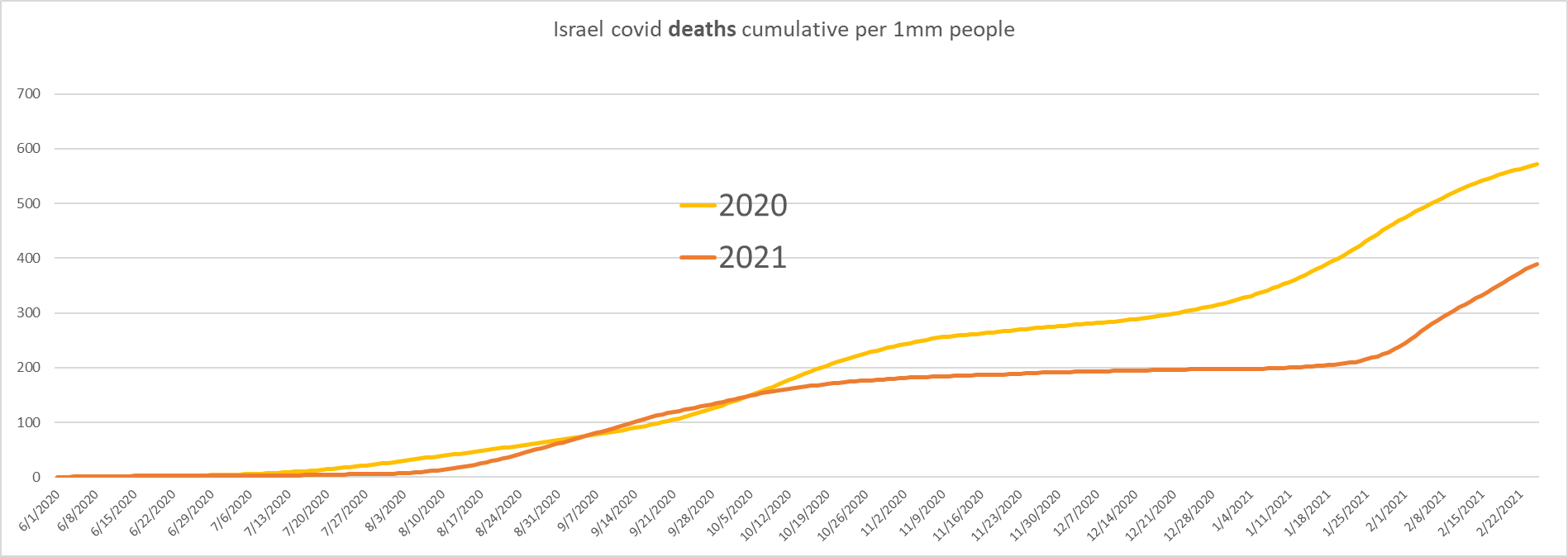
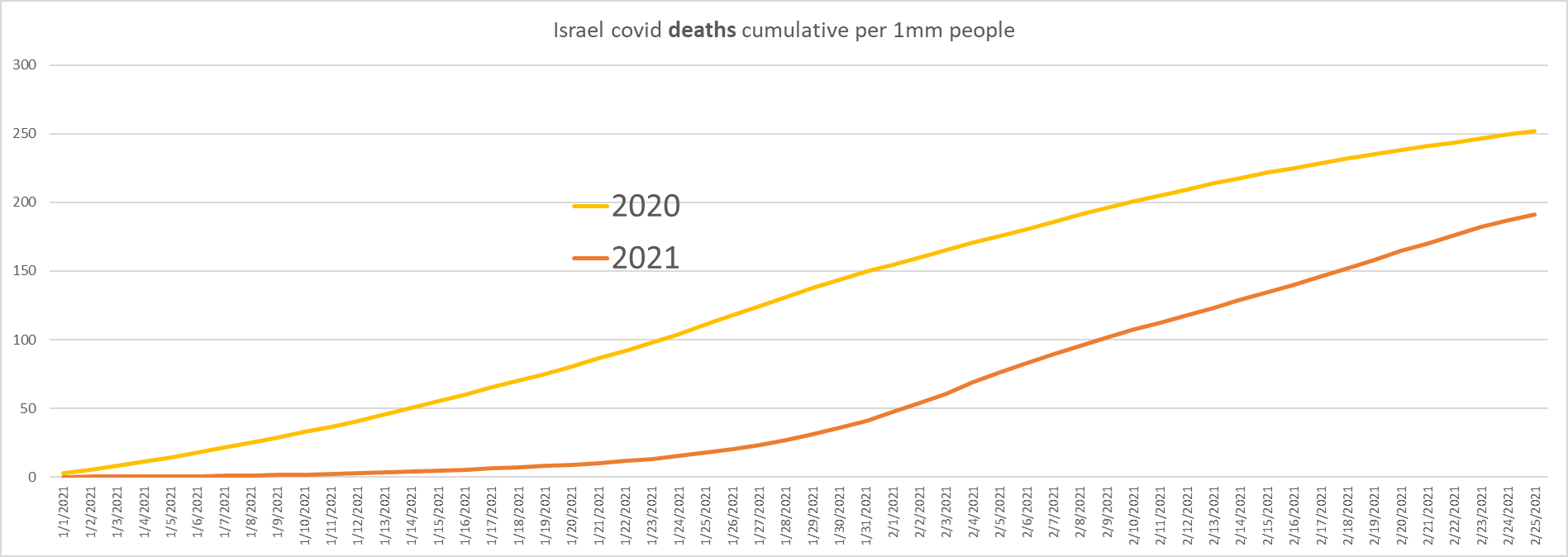

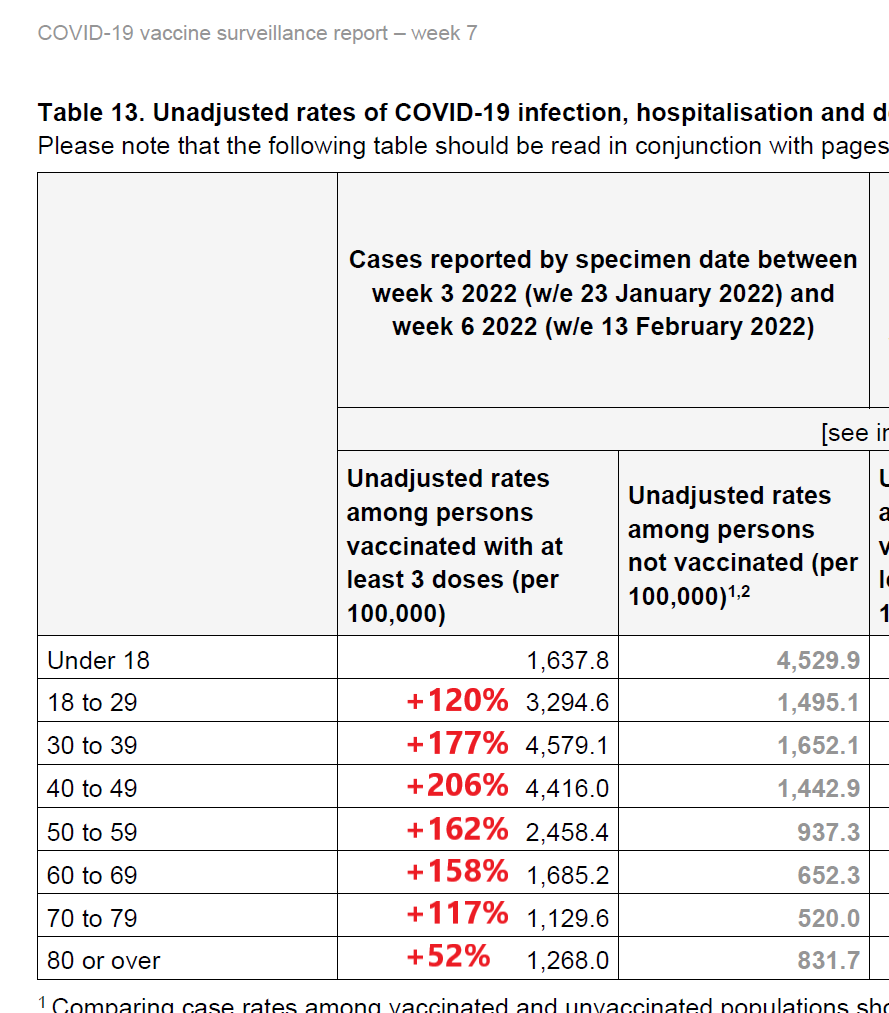{kind=link}