Question ‘The Science’? Go To Gulag!
By Dr Ron Paul | September 28, 2020
In the Soviet Union it was forbidden to dispute the wisdom of the “party line.” That’s because Marxian communism was viewed as the scientifically inevitable progression of mankind. For Marx and Lenin, the “science was settled.” Therefore anyone speaking out against “the science” of the Soviet system must be acting with malice; must actually want destruction; must want people to die.
Anyone voicing opposition to the “settled science” of Marxism-Leninism soon found their voice silenced. Oftentimes permanently.
Ironically, just 30 years after the “science” of Marxism-Leninism imploded for all the world to see, we are witnessing a resurgence here in the US of the idea that to question “the science” is not to seek truth or refine understanding of what appears to be conflicting evidence. No, it is to actually wish harm on one’s fellow Americans.
And while we who question “the science” are not being physically carried off to the gulags for disputing the wisdom of our “betters” in the CDC or the World Health Organization, for example, we are finding that the outcome is the same. We are being silenced and accused of malicious intent. The Soviet Communists called dissidents like us “wreckers.”
Last week on my daily news broadcast, the Ron Paul Liberty Report, we reported on two whistleblowers from inside the CDC and Big Pharma who raised serious and legitimate questions about the prevailing coronavirus narrative. The former Chief Science Officer for the pharmaceutical giant Pfizer, Dr. Mike Yeadon, has stated that from his experience he believes that nearly 90 percent of positive results from the current tests for Covid are false positives. That means that this massive expansion in “cases,” used to justify continued attacks on our civil liberties, is simply phony.
As Dr. Yeadon said in a recent interview about the Orwellian UK coronavirus lockdown, “we are basing a government policy, an economic policy, a civil liberties policy, in terms of limiting people to six people in a meeting… all based on, what may well be, completely fake data on this coronavirus?”
Is Dr. Yeadon correct in claiming that based on his scientific observation there is no “second wave”? We don’t know. But we do know that his claims that the massive increase in “cases” in Europe used to justify new lockdowns are not in any way being matched with a similar increase in deaths. The EU’s own charts prove this. Deaths remain a flat line near zero while “cases” skyrocket to match the massive increase in testing.
Yet when we reported on Dr. Yeadon’s findings on the Liberty Report last week we found that for the first time ever, our program was removed by YouTube.
YouTube, owned by Google, which is firmly embedded into the deep state, was vague in explaining just where we violated their “community standards” by simply reporting on qualified scientists who happen to disagree with the mainstream coronavirus narrative.
But they did offer this shocking explanation in an email sent to us at the Ron Paul Liberty Report: “YouTube does not allow content that explicitly disputes the efficacy of the World Health Organization.”
Incredible!
It’s not the science that is settled. What appears to be “settled is the impulse to silence anyone who asks “why”?
Copyright © 2020 by RonPaul Institute.
Canada Wildfires At Lowest Level In Years
By Paul Homewood | Not A Lot Of People Know That | September 27, 2020
According to the Met Office, global warming is leading to record breaking fires in North America.
Canada, of course, is a large part of North America, so surely fires should be getting worse there too.
In fact wildfires this year are running at just 8% of the 10-year average:


https://cwfis.cfs.nrcan.gc.ca/report
All provinces are well below average:

This suggests that meteorological conditions have been responsible for both the glut of fires in the US west and the dearth in Canada.
More significant though is the long term trend in Canada:

http://nfdp.ccfm.org/en/data/fires.php
1994, 1995 and 1998 recorded the biggest wildfire acreages. But over the full period, there is no obvious trend at all.
Which all rather makes of a nonsense of the Met Office’s claim that hot dry weather conditions promoting wildfires are becoming more severe and widespread due to climate change.
CLINTEL puts hard climate questions to Bill Gates
By David Wojick | CFACT | September 23, 2020
Bill Gates is throwing several billion dollars at climate change. Mind you he is not throwing it away, because it is mostly venture capital for new energy technologies, which could pay off handsomely without climate change.
Gates can do what he likes with his riches, but he is a leading figure and lately he has become a serious climate change scaremonger. This has prompted CLINTEL to put some hard questions to him, in the form of a registered letter.
On the scaremongering side, last month Gates published an article claiming that climate change will be far worse than the present Covid outbreak. He imagines many millions dying from climate change. The press spread his doomsday words far and wide.
Here are some doomful excerpts:
“I am talking about COVID-19. But in just a few decades, the same description will fit another global crisis: climate change. As awful as this pandemic is, climate change could be worse.“
“I realize that it’s hard to think about a problem like climate change right now. When disaster strikes, it is human nature to worry only about meeting our most immediate needs, especially when the disaster is as bad as COVID-19. But the fact that dramatically higher temperatures seem far off in the future does not make them any less of a problem—and the only way to avoid the worst possible climate outcomes is to accelerate our efforts now. Even as the world works to stop the novel coronavirus and begin recovering from it, we also need to act now to avoid a climate disaster by building and deploying innovations that will let us eliminate our greenhouse gas emissions.”
“If you want to understand the kind of damage that climate change will inflict, look at COVID-19 and spread the pain out over a much longer period of time. The loss of life and economic misery caused by this pandemic are on par with what will happen regularly if we do not eliminate the world’s carbon emissions.”
According to Gates’ Energy Plan, progress is the problem. He puts it this way:
“These challenges are only getting more urgent. The world’s middle class has been growing at an unprecedented rate, and as you move up the income ladder, your carbon footprint expands. Instead of walking everywhere, you can afford a bicycle (which doesn’t use gas but is likely made with energy-intensive metal and gets to you via cargo ships and trucks that run on fossil fuels). Eventually you get a motorbike so you can travel farther from home to work a better job and afford to send your kids to school. Your family eats more eggs, meat, and dairy, so they get better nutrition. You’re in the market for a refrigerator, electric lights so your kids can study at night, and a sturdy home built with metal and concrete.
All of that new consumption translates into tangible improvements in people’s lives. It is good for the world overall—but it will be very bad for the climate, unless we find ways to do it without adding more greenhouse gases to the atmosphere.”
As a rebuttal, the CLINTEL open letter asks him these six central questions:
1. How much or how little global warming does mankind really cause on top of the natural contribution?
2. Why does projected global warming exceed observationally-derived warming by more than 200%?
3. Have the large benefits of more CO2 in the atmosphere been properly accounted for?
4. Does the cost of attempting to abate global warming exceed the benefit in the avoided cost of adaptation?
5. What of the tens of millions who die every year because they cannot afford expensive “renewable” electricity and are denied affordable, reliable alternatives?
6. Has history not shown us repeatedly that adaptation to change presents a powerful survival and evolutionary strategy?
Professor Guus Berkhout, CLINTEL President, asks a more personal question:
“CLINTEL particularly blames Bill Gates that he takes advantage of his riches-based fame to frighten the public with extreme modeling predictions (question 2), but does not reassure them with the fact that these scaring modeling results never agreed with observations in practice. ‘Why this one-sided message, Mr. Gates?’”
It will be interesting to see how Bill Gates responds. I urge others to send similar letters to the misguided billionaires who are funding the climate false change scare.
In related news CLINTEL has posted an updated listing of its 900+ international
member scientists and related professionals, all signatories to the World Climate Declaration. They are listed by nationality, with 34 countries listed to date.
David Wojick, Ph.D. is an independent analyst working at the intersection of science, technology and policy.
Open letter from medical doctors and health professionals to all Belgian authorities and media
Dr Malcomb Kendrick | September 19, 2020
In order to make you aware that there are a growing number of doctors in Europe who feel that Lockdown has been an unmitigated disaster, I have downloaded an open Letter from doctors in Belgium. It can be seen here.
Doctors in other countries e.g. Germany have done much the same thing. I am putting this on my blog so that as many people as possible read it.
Open letter from medical doctors and health professionals to all Belgian authorities and all Belgian media.
We, Belgian doctors and health professionals, wish to express our serious concern about the evolution of the situation in the recent months surrounding the outbreak of the SARS-CoV-2 virus. We call on politicians to be independently and critically informed in the decision-making process and in the compulsory implementation of corona-measures. We ask for an open debate, where all experts are represented without any form of censorship. After the initial panic surrounding covid-19, the objective facts now show a completely different picture – there is no medical justification for any emergency policy anymore.
The current crisis management has become totally disproportionate and causes more damage than it does any good.
We call for an end to all measures and ask for an immediate restoration of our normal democratic governance and legal structures and of all our civil liberties.
‘A cure must not be worse than the problem’ is a thesis that is more relevant than ever in the current situation. We note, however, that the collateral damage now being caused to the population will have a greater impact in the short and long term on all sections of the population than the number of people now being safeguarded from corona.
In our opinion, the current corona measures and the strict penalties for non-compliance with them are contrary to the values formulated by the Belgian Supreme Health Council, which, until recently, as the health authority, has always ensured quality medicine in our country: “Science – Expertise – Quality – Impartiality – Independence – Transparency”. 1
We believe that the policy has introduced mandatory measures that are not sufficiently scientifically based, unilaterally directed, and that there is not enough space in the media for an open debate in which different views and opinions are heard. In addition, each municipality and province now has the authorisation to add its own measures, whether well-founded or not.
Moreover, the strict repressive policy on corona strongly contrasts with the government’s minimal policy when it comes to disease prevention, strengthening our own immune system through a healthy lifestyle, optimal care with attention for the individual and investment in care personnel.2
The concept of health
In 1948, the WHO defined health as follows: ‘Health is a state of complete physical, mental and social well-being and not merely the absence of disease or other physical impairment’.3
Health, therefore, is a broad concept that goes beyond the physical and also relates to the emotional and social well-being of the individual. Belgium also has a duty, from the point of view of subscribing to fundamental human rights, to include these human rights in its decision-making when it comes to measures taken in the context of public health. 4
The current global measures taken to combat SARS-CoV-2 violate to a large extent this view of health and human rights. Measures include compulsory wearing of a mask (also in open air and during sporting activities, and in some municipalities even when there are no other people in the vicinity), physical distancing, social isolation, compulsory quarantine for some groups and hygiene measures.
The predicted pandemic with millions of deaths
At the beginning of the pandemic, the measures were understandable and widely supported, even if there were differences in implementation in the countries around us. The WHO originally predicted a pandemic that would claim 3.4% victims, in other words millions of deaths, and a highly contagious virus for which no treatment or vaccine was available. This would put unprecedented pressure on the intensive care units (ICUs) of our hospitals.
This led to a global alarm situation, never seen in the history of mankind: “flatten the curve” was represented by a lockdown that shut down the entire society and economy and quarantined healthy people. Social distancing became the new normal in anticipation of a rescue vaccine.
The facts about covid-19
Gradually, the alarm bell was sounded from many sources: the objective facts showed a completely different reality. 5 6
The course of covid-19 followed the course of a normal wave of infection similar to a flu season. As every year, we see a mix of flu viruses following the curve: first the rhinoviruses, then the influenza A and B viruses, followed by the coronaviruses. There is nothing different from what we normally see.
The use of the non-specific PCR test, which produces many false positives, showed an exponential picture. This test was rushed through with an emergency procedure and was never seriously self-tested. The creator expressly warned that this test was intended for research and not for diagnostics.7
The PCR test works with cycles of amplification of genetic material – a piece of genome is amplified each time. Any contamination (e.g. other viruses, debris from old virus genomes) can possibly result in false positives.8
The test does not measure how many viruses are present in the sample. A real viral infection means a massive presence of viruses, the so-called virus load. If someone tests positive, this does not mean that that person is actually clinically infected, is ill or is going to become ill. Koch’s postulate was not fulfilled (“The pure agent found in a patient with complaints can provoke the same complaints in a healthy person”).
Since a positive PCR test does not automatically indicate active infection or infectivity, this does not justify the social measures taken, which are based solely on these tests. 9 10
Lockdown.
If we compare the waves of infection in countries with strict lockdown policies to countries that did not impose lockdowns (Sweden, Iceland …), we see similar curves. So there is no link between the imposed lockdown and the course of the infection. Lockdown has not led to a lower mortality rate.
If we look at the date of application of the imposed lockdowns we see that the lockdowns were set after the peak was already over and the number of cases decreasing. The drop was therefore not the result of the taken measures. 11
As every year, it seems that climatic conditions (weather, temperature and humidity) and growing immunity are more likely to reduce the wave of infection.
Our immune system
For thousands of years, the human body has been exposed daily to moisture and droplets containing infectious microorganisms (viruses, bacteria and fungi).
The penetration of these microorganisms is prevented by an advanced defence mechanism – the immune system. A strong immune system relies on normal daily exposure to these microbial influences. Overly hygienic measures have a detrimental effect on our immunity. 12 13 Only people with a weak or faulty immune system should be protected by extensive hygiene or social distancing.
Influenza will re-emerge in the autumn (in combination with covid-19) and a possible decrease in natural resilience may lead to further casualties.
Our immune system consists of two parts: a congenital, non-specific immune system and an adaptive immune system.
The non-specific immune system forms a first barrier: skin, saliva, gastric juice, intestinal mucus, vibratory hair cells, commensal flora, … and prevents the attachment of micro-organisms to tissue.
If they do attach, macrophages can cause the microorganisms to be encapsulated and destroyed.
The adaptive immune system consists of mucosal immunity (IgA antibodies, mainly produced by cells in the intestines and lung epithelium), cellular immunity (T-cell activation), which can be generated in contact with foreign substances or microorganisms, and humoral immunity (IgM and IgG antibodies produced by the B cells).
Recent research shows that both systems are highly entangled.
It appears that most people already have a congenital or general immunity to e.g. influenza and other viruses. This is confirmed by the findings on the cruise ship Diamond Princess, which was quarantined because of a few passengers who died of Covid-19. Most of the passengers were elderly and were in an ideal situation of transmission on the ship. However, 75% did not appear to be infected. So even in this high-risk group, the majority are resistant to the virus.
A study in the journal Cell shows that most people neutralise the coronavirus by mucosal (IgA) and cellular immunity (T-cells), while experiencing few or no symptoms 14.
Researchers found up to 60% SARS-Cov-2 reactivity with CD4+T cells in a non-infected population, suggesting cross-reactivity with other cold (corona) viruses.15 Most people therefore already have a congenital or cross-immunity because they were already in contact with variants of the same virus.
The antibody formation (IgM and IgG) by B-cells only occupies a relatively small part of our immune system. This may explain why, with an antibody percentage of 5-10%, there may be a group immunity anyway. The efficacy of vaccines is assessed precisely on the basis of whether or not we have these antibodies. This is a misrepresentation.
Most people who test positive (PCR) have no complaints. Their immune system is strong enough. Strengthening natural immunity is a much more logical approach. Prevention is an important, insufficiently highlighted pillar: healthy, full-fledged nutrition, exercise in fresh air, without a mask, stress reduction and nourishing emotional and social contacts.
Consequences of social isolation on physical and mental health
Social isolation and economic damage led to an increase in depression, anxiety, suicides, intra-family violence and child abuse.16
Studies have shown that the more social and emotional commitments people have, the more resistant they are to viruses. It is much more likely that isolation and quarantine have fatal consequences. 17
The isolation measures have also led to physical inactivity in many older people due to their being forced to stay indoors. However, sufficient exercise has a positive effect on cognitive functioning, reducing depressive complaints and anxiety and improving physical health, energy levels, well-being and, in general, quality of life.18
Fear, persistent stress and loneliness induced by social distancing have a proven negative influence on psychological and general health. 19
A highly contagious virus with millions of deaths without any treatment?
Mortality turned out to be many times lower than expected and close to that of a normal seasonal flu (0.2%). 20
The number of registered corona deaths therefore still seems to be overestimated.
There is a difference between death by corona and death with corona. Humans are often carriers of multiple viruses and potentially pathogenic bacteria at the same time. Taking into account the fact that most people who developed serious symptoms suffered from additional pathology, one cannot simply conclude that the corona-infection was the cause of death. This was mostly not taken into account in the statistics.
The most vulnerable groups can be clearly identified. The vast majority of deceased patients were 80 years of age or older. The majority (70%) of the deceased, younger than 70 years, had an underlying disorder, such as cardiovascular suffering, diabetes mellitus, chronic lung disease or obesity. The vast majority of infected persons (>98%) did not or hardly became ill or recovered spontaneously.
Meanwhile, there is an affordable, safe and efficient therapy available for those who do show severe symptoms of disease in the form of HCQ (hydroxychloroquine), zinc and AZT (azithromycin). Rapidly applied this therapy leads to recovery and often prevents hospitalisation. Hardly anyone has to die now.
This effective therapy has been confirmed by the clinical experience of colleagues in the field with impressive results. This contrasts sharply with the theoretical criticism (insufficient substantiation by double-blind studies) which in some countries (e.g. the Netherlands) has even led to a ban on this therapy. A meta-analysis in The Lancet, which could not demonstrate an effect of HCQ, was withdrawn. The primary data sources used proved to be unreliable and 2 out of 3 authors were in conflict of interest. However, most of the guidelines based on this study remained unchanged … 48 49
We have serious questions about this state of affairs.
In the US, a group of doctors in the field, who see patients on a daily basis, united in “America’s Frontline Doctors” and gave a press conference which has been watched millions of times.21 51
French Prof Didier Raoult of the Institut d’Infectiologie de Marseille (IHU) also presented this promising combination therapy as early as April. Dutch GP Rob Elens, who cured many patients in his practice with HCQ and zinc, called on colleagues in a petition for freedom of therapy.22
The definitive evidence comes from the epidemiological follow-up in Switzerland: mortality rates compared with and without this therapy.23
From the distressing media images of ARDS (acute respiratory distress syndrome) where people were suffocating and given artificial respiration in agony, we now know that this was caused by an exaggerated immune response with intravascular coagulation in the pulmonary blood vessels. The administration of blood thinners and dexamethasone and the avoidance of artificial ventilation, which was found to cause additional damage to lung tissue, means that this dreaded complication, too, is virtually not fatal anymore. 47
It is therefore not a killer virus, but a well-treatable condition.
Propagation
Spreading occurs by drip infection (only for patients who cough or sneeze) and aerosols in closed, unventilated rooms. Contamination is therefore not possible in the open air. Contact tracing and epidemiological studies show that healthy people (or positively tested asymptomatic carriers) are virtually unable to transmit the virus. Healthy people therefore do not put each other at risk. 24 25
Transfer via objects (e.g. money, shopping or shopping trolleys) has not been scientifically proven.26 27 28
All this seriously calls into question the whole policy of social distancing and compulsory mouth masks for healthy people – there is no scientific basis for this.
Masks
Oral masks belong in contexts where contacts with proven at-risk groups or people with upper respiratory complaints take place, and in a medical context/hospital-retirement home setting. They reduce the risk of droplet infection by sneezing or coughing. Oral masks in healthy individuals are ineffective against the spread of viral infections. 29 30 31
Wearing a mask is not without side effects. 32 33 Oxygen deficiency (headache, nausea, fatigue, loss of concentration) occurs fairly quickly, an effect similar to altitude sickness. Every day we now see patients complaining of headaches, sinus problems, respiratory problems and hyperventilation due to wearing masks. In addition, the accumulated CO2 leads to a toxic acidification of the organism which affects our immunity. Some experts even warn of an increased transmission of the virus in case of inappropriate use of the mask.34
Our Labour Code (Codex 6) refers to a CO2 content (ventilation in workplaces) of 900 ppm, maximum 1200 ppm in special circumstances. After wearing a mask for one minute, this toxic limit is considerably exceeded to values that are three to four times higher than these maximum values. Anyone who wears a mask is therefore in an extreme poorly ventilated room. 35
Inappropriate use of masks without a comprehensive medical cardio-pulmonary test file is therefore not recommended by recognised safety specialists for workers.
Hospitals have a sterile environment in their operating rooms where staff wear masks and there is precise regulation of humidity / temperature with appropriately monitored oxygen flow to compensate for this, thus meeting strict safety standards. 36
A second corona wave?
A second wave is now being discussed in Belgium, with a further tightening of the measures as a result. However, closer examination of Sciensano’s figures (latest report of 3 September 2020)37 shows that, although there has been an increase in the number of infections since mid-July, there was no increase in hospital admissions or deaths at that time. It is therefore not a second wave of corona, but a so-called “case chemistry” due to an increased number of tests. 50
The number of hospital admissions or deaths showed a shortlasting minimal increase in recent weeks, but in interpreting it, we must take into account the recent heatwave. In addition, the vast majority of the victims are still in the population group >75 years.
This indicates that the proportion of the measures taken in relation to the working population and young people is disproportionate to the intended objectives.
The vast majority of the positively tested “infected” persons are in the age group of the active population, which does not develop any or merely limited symptoms, due to a well-functioning immune system.
So nothing has changed – the peak is over.
Strengthening a prevention policy
The corona measures form a striking contrast to the minimal policy pursued by the government until now, when it comes to well-founded measures with proven health benefits such as the sugar tax, the ban on (e-)cigarettes and making healthy food, exercise and social support networks financially attractive and widely accessible. It is a missed opportunity for a better prevention policy that could have brought about a change in mentality in all sections of the population with clear results in terms of public health. At present, only 3% of the health care budget goes to prevention. 2
The Hippocratic Oath
As a doctor, we took the Hippocratic Oath:
“I will above all care for my patients, promote their health and alleviate their suffering”.
“I will inform my patients correctly.”
“Even under pressure, I will not use my medical knowledge for practices that are against humanity.”
The current measures force us to act against this oath.
Other health professionals have a similar code.
The ‘primum non nocere’, which every doctor and health professional assumes, is also undermined by the current measures and by the prospect of the possible introduction of a generalised vaccine, which is not subject to extensive prior testing.
Vaccine
Survey studies on influenza vaccinations show that in 10 years we have only succeeded three times in developing a vaccine with an efficiency rate of more than 50%. Vaccinating our elderly appears to be inefficient. Over 75 years of age, the efficacy is almost non-existent.38
Due to the continuous natural mutation of viruses, as we also see every year in the case of the influenza virus, a vaccine is at most a temporary solution, which requires new vaccines each time afterwards. An untested vaccine, which is implemented by emergency procedure and for which the manufacturers have already obtained legal immunity from possible harm, raises serious questions. 39 40 We do not wish to use our patients as guinea pigs.
On a global scale, 700 000 cases of damage or death are expected as a result of the vaccine.41 If 95% of people experience Covid-19 virtually symptom-free, the risk of exposure to an untested vaccine is irresponsible.
The role of the media and the official communication plan
Over the past few months, newspaper, radio and TV makers seemed to stand almost uncritically behind the panel of experts and the government, there, where it is precisely the press that should be critical and prevent one-sided governmental communication. This has led to a public communication in our news media, that was more like propaganda than objective reporting.
In our opinion, it is the task of journalism to bring news as objectively and neutrally as possible, aimed at finding the truth and critically controlling power, with dissenting experts also being given a forum in which to express themselves.
This view is supported by the journalistic codes of ethics.42
The official story that a lockdown was necessary, that this was the only possible solution, and that everyone stood behind this lockdown, made it difficult for people with a different view, as well as experts, to express a different opinion.
Alternative opinions were ignored or ridiculed. We have not seen open debates in the media, where different views could be expressed.
We were also surprised by the many videos and articles by many scientific experts and authorities, which were and are still being removed from social media. We feel that this does not fit in with a free, democratic constitutional state, all the more so as it leads to tunnel vision. This policy also has a paralysing effect and feeds fear and concern in society. In this context, we reject the intention of censorship of dissidents in the European Union! 43
The way in which Covid-19 has been portrayed by politicians and the media has not done the situation any good either. War terms were popular and warlike language was not lacking. There has often been mention of a ‘war’ with an ‘invisible enemy’ who has to be ‘defeated’. The use in the media of phrases such as ‘care heroes in the front line’ and ‘corona victims’ has further fuelled fear, as has the idea that we are globally dealing with a ‘killer virus’.
The relentless bombardment with figures, that were unleashed on the population day after day, hour after hour, without interpreting those figures, without comparing them to flu deaths in other years, without comparing them to deaths from other causes, has induced a real psychosis of fear in the population. This is not information, this is manipulation.
We deplore the role of the WHO in this, which has called for the infodemic (i.e. all divergent opinions from the official discourse, including by experts with different views) to be silenced by an unprecedented media censorship.43 44
We urgently call on the media to take their responsibilities here!
We demand an open debate in which all experts are heard.
Emergency law versus Human Rights
The general principle of good governance calls for the proportionality of government decisions to be weighed up in the light of the Higher Legal Standards: any interference by government must comply with the fundamental rights as protected in the European Convention on Human Rights (ECHR). Interference by public authorities is only permitted in crisis situations. In other words, discretionary decisions must be proportionate to an absolute necessity.
The measures currently taken concern interference in the exercise of, among other things, the right to respect of private and family life, freedom of thought, conscience and religion, freedom of expression and freedom of assembly and association, the right to education, etc., and must therefore comply with fundamental rights as protected by the European Convention on Human Rights (ECHR).
For example, in accordance with Article 8(2) of the ECHR, interference with the right to private and family life is permissible only if the measures are necessary in the interests of national security, public safety, the economic well-being of the country, the protection of public order and the prevention of criminal offences, the protection of health or the protection of the rights and freedoms of others, the regulatory text on which the interference is based must be sufficiently clear, foreseeable and proportionate to the objectives pursued.45
The predicted pandemic of millions of deaths seemed to respond to these crisis conditions, leading to the establishment of an emergency government. Now that the objective facts show something completely different, the condition of inability to act otherwise (no time to evaluate thoroughly if there is an emergency) is no longer in place. Covid-19 is not a cold virus, but a well treatable condition with a mortality rate comparable to the seasonal flu. In other words, there is no longer an insurmountable obstacle to public health.
There is no state of emergency.
Immense damage caused by the current policies
An open discussion on corona measures means that, in addition to the years of life gained by corona patients, we must also take into account other factors affecting the health of the entire population. These include damage in the psychosocial domain (increase in depression, anxiety, suicides, intra-family violence and child abuse)16 and economic damage.
If we take this collateral damage into account, the current policy is out of all proportion, the proverbial use of a sledgehammer to crack a nut.We find it shocking that the government is invoking health as a reason for the emergency law.
As doctors and health professionals, in the face of a virus which, in terms of its harmfulness, mortality and transmissibility, approaches the seasonal influenza, we can only reject these extremely disproportionate measures.
We therefore demand an immediate end to all measures.
We are questioning the legitimacy of the current advisory experts, who meet behind closed doors.
Following on from ACU 2020 46 https://acu2020.org/nederlandse-versie/ we call for an in-depth examination of the role of the WHO and the possible influence of conflicts of interest in this organisation. It was also at the heart of the fight against the “infodemic”, i.e. the systematic censorship of all dissenting opinions in the media. This is unacceptable for a democratic state governed by the rule of law.43
Distribution of this letter
We would like to make a public appeal to our professional associations and fellow carers to give their opinion on the current measures.
We draw attention to and call for an open discussion in which carers can and dare to speak out.
With this open letter, we send out the signal that progress on the same footing does more harm than good, and call on politicians to inform themselves independently and critically about the available evidence – including that from experts with different views, as long as it is based on sound science – when rolling out a policy, with the aim of promoting optimum health.
With concern, hope and in a personal capacity.
1: https://www.health.belgium.be/nl/wie-zijn-we#Missie standaard.be/preventie
2: https://www.who.int/about/who-we-are/constitution
3: https://www.who.int/news-room/fact-sheets/detail/human-rights-and-health
4: https://swprs.org/feiten-over-covid19/
6: https://www.creative-diagnostics.com/sars-cov-2-coronavirus-multiplex-rt-qpcr-kit-277854-457.htm
7: President John Magufuli of Tanzania: “Even Papaya and Goats are Corona positive” https://www.youtube.com/watch?v=207HuOxltvI
8: Open letter by biochemist Drs Mario Ortiz Martinez to the Dutch chamber https://www.gentechvrij.nl/2020/08/15/foute-interpretatie/
9: Interview with Drs Mario Ortiz Martinez https://troo.tube/videos/watch/6ed900eb-7459-4a1b-93fd-b393069f4fcd?fbclid=IwAR1XrullC2qopJjgFxEgbSTBvh-4ZCuJa1VxkHTXEtYMEyGG3DsNwUdaatY
10: https://infekt.ch/2020/04/sind-wir-tatsaechlich-im-blindflug/
11: Lambrecht, B., Hammad, H. The immunology of the allergy epidemic and the hygiene hypothesis. Nat Immunol 18, 1076–1083 (2017). https://www.nature.com/articles/ni.3829
12: Sharvan Sehrawat, Barry T. Rouse, Does the hygiene hypothesis apply to COVID-19 susceptibility?, Microbes and Infection, 2020, ISSN 1286-4579, https://doi.org/10.1016/j.micinf.2020.07.002
14: https://www.hpdetijd.nl/2020-08-11/9-manieren-om-corona-te-voorkomen/
15: Feys, F., Brokken, S., & De Peuter, S. (2020, May 22). Risk-benefit and cost-utility analysis for COVID-19 lockdown in Belgium: the impact on mental health and wellbeing. https://psyarxiv.com/xczb3/
16: Kompanje, 2020
17: Conn, Hafdahl en Brown, 2009; Martinsen 2008; Yau, 2008
19: https://swprs.org/studies-on-covid-19-lethality/#overall-mortality
22: https://zelfzorgcovid19.nl/statistieken-zwitserland-met-hcq-zonder-hcq-met-hcq-leveren-het-bewijs/
- Contradictory statements by our virologists https://www.youtube.com/watch?v=6K9xfmkMsvM
31: Security expert Tammy K. Herrema Clark https://youtu.be/TgDm_maAglM
33: https://www.technocracy.news/blaylock-face-masks-pose-serious-risks-to-the-healthy/
35: https://werk.belgie.be/nl/nieuws/nieuwe-regels-voor-de-kwaliteit-van-de-binnenlucht-werklokalen
36: https://kavlaanderen.blogspot.com/2020/07/als-maskers-niet-werken-waarom-dragen.html
37: https://covid-19.sciensano.be/sites/default/files/Covid19/Meest%20recente%20update.pdf
38: Haralambieva, I.H. et al., 2015. The impact of immunosenescence on humoral immune response variation after influenza A/H1N1 vaccination in older subjects. https://pubmed.ncbi.nlm.nih.gov/26044074/
39: Global vaccine safety summit WHO 2019 https://www.youtube.com/watch?v=oJXXDLGKmPg
40: No liability manufacturers vaccines https://m.nieuwsblad.be/cnt/dmf20200804_95956456?fbclid=IwAR0IgiA-6sNVQvE8rMC6O5Gq5xhOulbcN1BhdI7Rw-7eq_pRtJDCxde6SQI
42: Journalistic code https://www.rvdj.be/node/63
43: Disinformation related to COVID-19 approaches European Commission EurLex, juni 2020 (this file will not damage your computer)
44: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30461-X/fulltext
45: http://www.raadvst-consetat.be/dbx/adviezen/67142.pdf#search=67.142
48: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31180-6/fulltext
49 https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31324-6/fulltext
There is no revival of the pandemic, but a so-called casedemic due to more testing.
50: https://www.greenmedinfo.com/blog/crucial-viewing-understanding-covid-19-casedemic1
51: https://docs4opendebate.be/wp-content/uploads/2020/09/white-paper-on-hcq-from-AFD.pdf

Lies, Damned Lies and Health Statistics – the Deadly Danger of False Positives
By Dr Michael Yeadon | Lockdown Sceptics | September 20, 2020
I never expected to be writing something like this. I am an ordinary person, recently semi-retired from a career in the pharmaceutical industry and biotech, where I spent over 30 years trying to solve problems of disease understanding and seek new treatments for allergic and inflammatory disorders of lung and skin. I’ve always been interested in problem solving, so when anything biological comes along, my attention is drawn to it. Come 2020, came SARS-CoV-2. I’ve written about the pandemic as objectively as I could. The scientific method never leaves a person who trained and worked as a professional scientist. Please do read that piece. My co-authors & I will submit it to the normal rigours of peer review, but that process is slow and many pieces of new science this year have come to attention through pre-print servers and other less conventional outlets.
While paying close attention to data, we all initially focused on the sad matter of deaths. I found it remarkable that, in discussing the COVID-19 related deaths, most people I spoke to had no idea of large numbers. Asked approximately how many people a year die in the UK in the ordinary course of events, each a personal tragedy, they usually didn’t know. I had to inform them it is around 620,000, sometimes less if we had a mild winter, sometimes quite a bit higher if we had a severe ’flu season. I mention this number because we know that around 42,000 people have died with or of COVID-19. While it’s a huge number of people, its ‘only’ 0.06% of the UK population. Its not a coincidence that this is almost the same proportion who have died with or of COVID-19 in each of the heavily infected European countries – for example, Sweden. The annual all-causes mortality of 620,000 amounts to 1,700 per day, lower in summer and higher in winter. That has always been the lot of humans in the temperate zones. So for context, 42,000 is about ~24 days worth of normal mortality. Please know I am not minimising it, just trying to get some perspective on it. Deaths of this magnitude are not uncommon, and can occur in the more severe flu seasons. Flu vaccines help a little, but on only three occasions in the last decade did vaccination reach 50% effectiveness. They’re good, but they’ve never been magic bullets for respiratory viruses. Instead, we have learned to live with such viruses, ranging from numerous common colds all the way to pneumonias which can kill. Medicines and human caring do their best.
So, to this article. Its about the testing we do with something called PCR, an amplification technique, better known to biologists as a research tool used in our labs, when trying to unpick mechanisms of disease. I was frankly astonished to realise they’re sometimes used in population screening for diseases – astonished because it is a very exacting technique, prone to invisible errors and it’s quite a tall order to get reliable information out of it, especially because of the prodigious amounts of amplification involved in attempting to pick up a strand of viral genetic code. The test cannot distinguish between a living virus and a short strand of RNA from a virus which broke into pieces weeks or months ago.
I believe I have identified a serious, really a fatal flaw in the PCR test used in what is called by the UK Government the Pillar 2 screening – that is, testing many people out in their communities. I’m going to go through this with care and in detail because I’m a scientist and dislike where this investigation takes me. I’m not particularly political and my preference is for competent, honest administration over the actual policies chosen. We’re a reasonable lot in UK and not much given to extremes. What I’m particularly reluctant about is that, by following the evidence, I have no choice but to show that the Health Secretary, Matt Hancock, misled the House of Commons and also made misleading statements in a radio interview. Those are serious accusations. I know that. I’m not a ruthless person. But I’m writing this anyway, because what I have uncovered is of monumental importance to the health and wellbeing of all the people living in the nation I have always called home.
Back to the story, and then to the evidence. When the first (and I think, only) wave of COVID-19 hit the UK, I was with almost everyone else in being very afraid. I’m 60 and in reasonable health, but on learning that I had about a 1% additional risk of perishing if I caught the virus, I discovered I was far from ready to go. So, I wasn’t surprised or angry when the first lockdown arrived. It must have been a very difficult thing to decide. However, before the first three-week period was over, I’d begun to develop an understanding of what was happening. The rate of infection, which has been calculated to have infected well over 100,000 new people every day around the peak, began to fall, and was declining before lockdown. Infection continued to spread out, at an ever-reducing rate and we saw this in the turning point of daily deaths, at a grim press conference each afternoon. We now know that lockdown made no difference at all to the spread of the virus. We can tell this because the interval between catching the virus and, in those who don’t make it, their death is longer than the interval between lockdown and peak daily deaths. There isn’t any controversy about this fact, which is easily demonstrated, but I’m aware some people like to pretend it was lockdown that turned the pandemic, perhaps to justify the extraordinary price we have all paid to do it. That price wasn’t just economic. It involved avoidable deaths from diseases other than COVID-19, as medical services were restricted, in order to focus on the virus. Some say that lockdown, directly and indirectly, killed as many as the virus. I don’t know. Its not something I’ve sought to learn. But I mention because interventions in all our lives should not be made lightly. Its not only inconvenience, but real suffering, loss of livelihoods, friendships, anchors of huge importance to us all, that are severed by such acts. We need to be certain that the prize is worth the price. While it is uncertain it was, even for the first lockdown, I too supported it, because we did not know what we faced, and frankly, almost everyone else did it, except Sweden. I am now resolutely against further interventions in what I have become convinced is a fruitless attempt to ‘control the virus’. We are, in my opinion – shared by others, some of whom are well placed to assess the situation – closer to the end of the pandemic in terms of deaths, than we are to its middle. I believe we should provide the best protection we can for any vulnerable people, and otherwise cautiously get on with our lives. I think we are all going to get a little more Swedish over time.
In recent weeks, though, it cannot have escaped anyone’s attention that there has been a drum beat which feels for all the world like a prelude to yet more fruitless and damaging restrictions. Think back to mid-summer. We were newly out of lockdown and despite concerns for crowded beaches, large demonstrations, opening of shops and pubs, the main item on the news in relation to COVID-19 was the reassuring and relentless fall in daily deaths. I noticed that, as compared to the slopes of the declining death tolls in many nearby countries, that our slope was too flat. I even mentioned to scientist friends that inferred the presence of some fixed signal that was being mixed up with genuine COVID-19 deaths. Imagine how gratifying it was when the definition of a COVID-19 death was changed to line up with that in other countries and in a heartbeat our declining death toll line became matched with that elsewhere. I was sure it would: what we have experienced and witnessed is a terrible kind of equilibrium. A virus that kills few, then leaves survivors who are almost certainly immune – a virus to which perhaps 30-50% were already immune because it has relatives and some of us have already encountered them – accounts for the whole terrible but also fascinating biological process. There was a very interesting piece in the BMJ in recent days that offers potential support for this contention.
Now we have learned some of the unusual characteristics of the new virus, better treatments (anti-inflammatory steroids, anti-coagulants and in particular, oxygen masks and not ventilators in the main) the ‘case fatality rate’ even for the most hard-hit individuals is far lower now than it was six months ago.
As there is no foundational, medical or scientific literature which tells us to expect a ‘second wave’, I began to pay more attention to the phrase as it appeared on TV, radio and print media – all on the same day – and has been relentlessly repeated ever since. I was interviewed recently by Julia Hartley-Brewer on her talkRADIO show and on that occasion I called on the Government to disclose to us the evidence upon which they were relying to predict this second wave. Surely they have some evidence? I don’t think they do. I searched and am very qualified to do so, drawing on academic friends, and we were all surprised to find that there is nothing at all. The last two novel coronaviruses, Sar (2003) and MERS (2012), were of one wave each. Even the WW1 flu ‘waves’ were almost certainly a series of single waves involving more than one virus. I believe any second wave talk is pure speculation. Or perhaps it is in a model somewhere, disconnected from the world of evidence to me? It would be reasonable to expect some limited ‘resurgence’ of a virus given we don’t mix like cordial in a glass of water, but in a more lumpy, human fashion. You’re most in contact with family, friends and workmates and they are the people with whom you generally exchange colds.
A long period of imposed restrictions, in addition to those of our ordinary lives did prevent the final few percent of virus mixing with the population. With the movements of holidays, new jobs, visiting distant relatives, starting new terms at universities and schools, that final mixing is under way. It should not be a terrifying process. It happens with every new virus, flu included. It’s just that we’ve never before in our history chased it around the countryside with a technique more suited to the biology lab than to a supermarket car park.
A very long prelude, but necessary. Part of the ‘project fear’ that is rather too obvious, involving second waves, has been the daily count of ‘cases’. Its important to understand that, according to the infectious disease specialists I’ve spoken to, the word ‘case’ has to mean more than merely the presence of some foreign organism. It must present signs (things medics notice) and symptoms (things you notice). And in most so-called cases, those testing positive had no signs or symptoms of illness at all. There was much talk of asymptomatic spreading, and as a biologist this surprised me. In almost every case, a person is symptomatic because they have a high viral load and either it is attacking their body or their immune system is fighting it, generally a mix. I don’t doubt there have been some cases of asymptomatic transmission, but I’m confident it is not important.
That all said, Government decided to call a person a ‘case’ if their swab sample was positive for viral RNA, which is what is measured in PCR. A person’s sample can be positive if they have the virus, and so it should. They can also be positive if they’ve had the virus some weeks or months ago and recovered. It’s faintly possible that high loads of related, but different coronaviruses, which can cause some of the common colds we get, might also react in the PCR test, though it’s unclear to me if it does.
But there’s a final setting in which a person can be positive and that’s a random process. This may have multiple causes, such as the amplification technique not being perfect and so amplifying the ‘bait’ sequences placed in with the sample, with the aim of marrying up with related SARS-CoV-2 viral RNA. There will be many other contributions to such positives. These are what are called false positives.
Think of any diagnostic test a doctor might use on you. The ideal diagnostic test correctly confirms all who have the disease and never wrongly indicates that healthy people have the disease. There is no such test. All tests have some degree of weakness in generating false positives. The important thing is to know how often this happens, and this is called the false positive rate. If 1 in 100 disease-free samples are wrongly coming up positive, the disease is not present, we call that a 1% false positive rate. The actual or operational false positive rate differs, sometimes substantially, under different settings, technical operators, detection methods and equipment. I’m focusing solely on the false positive rate in Pillar 2, because most people do not have the virus (recently around 1 in 1000 people and earlier in summer it was around 1 in 2000 people). It is when the amount of disease, its so-called prevalence, is low that any amount of a false positive rate can be a major problem. This problem can be so severe that unless changes are made, the test is hopelessly unsuitable to the job asked of it. In this case, the test in Pillar 2 was and remains charged with the job of identifying people with the virus, yet as I will show, it is unable to do so.
Because of the high false positive rate and the low prevalence, almost every positive test, a so-called case, identified by Pillar 2 since May of this year has been a FALSE POSITIVE. Not just a few percent. Not a quarter or even a half of the positives are FALSE, but around 90% of them. Put simply, the number of people Mr Hancock sombrely tells us about is an overestimate by a factor of about ten-fold. Earlier in the summer, it was an overestimate by about 20-fold.
Let me take you through this, though if you’re able to read Prof Carl Heneghan’s clearly written piece first, I’m more confident that I’ll be successful in explaining this dramatic conclusion to you. (Here is a link to the record of numbers of tests, combining Pillar 1 (hospital) and Pillar 2 (community).)
Imagine 10,000 people getting tested using those swabs you see on TV. We have a good estimate of the general prevalence of the virus from the ONS, who are wholly independent (from Pillar 2 testing) and are testing only a few people a day, around one per cent of the numbers recently tested in Pillar 2. It is reasonable to assume that most of the time, those being tested do not have symptoms. People were asked to only seek a test if they have symptoms. However, we know from TV news and stories on social media from sampling staff, from stern guidance from the Health Minister and the surprising fact that in numerous locations around the country, the local council is leafleting people’s houses, street by street to come and get tested.
The bottom line is that it is reasonable to expect the prevalence of the virus to be close to the number found by ONS, because they sample randomly, and would pick up symptomatic and asymptomatic people in proportion to their presence in the community. As of the most recent ONS survey, to a first approximation, the virus was found in 1 in every 1000 people. This can also be written as 0.1%. So when all these 10,000 people are tested in Pillar 2, you’d expect 10 true positives to be found (false negatives can be an issue when the virus is very common, but in this community setting, it is statistically unimportant and so I have chosen to ignore it, better to focus only on false positives).
So, what is the false positive rate of testing in Pillar 2? For months, this has been a concern. It appears that it isn’t known, even though as I’ve mentioned, you absolutely need to know it in order to work out whether the diagnostic test has any value! What do we know about the false positive rate? Well, we do know that the Government’s own scientists were very concerned about it, and a report on this problem was sent to SAGE dated June 3rd 2020. I quote: “Unless we understand the operational false positive rate of the UK’s RT-PCR testing system, we risk over-estimating the COVID-19 incidence, the demand on track and trace and the extent of asymptomatic infection”. In that same report, the authors helpfully listed the lowest to highest false positive rate of dozens of tests using the same technology. The lowest value for false positive rate was 0.8%.
Allow me to explain the impact of a false positive rate of 0.8% on Pillar 2. We return to our 10,000 people who’ve volunteered to get tested, and the expected ten with virus (0.1% prevalence or 1:1000) have been identified by the PCR test. But now we’ve to calculate how many false positives are accompanying them. The shocking answer is 80. 80 is 0.8% of 10,000. That’s how many false positives you’d get every time you were to use a Pillar 2 test on a group of that size.
The effect of this is, in this example, where 10,000 people have been tested in Pillar 2, could be summarised in a headline like this: “90 new cases were identified today” (10 real positive cases and 80 false positives). But we know this is wildly incorrect. Unknown to the poor technician, there were in this example, only 10 real cases. 80 did not even have a piece of viral RNA in their sample. They are really false positives.
I’m going to explain how bad this is another way, back to diagnostics. If you’d submitted to a test and it was positive, you’d expect the doctor to tell you that you had a disease, whatever it was testing for. Usually, though, they’ll answer a slightly different question: “If the patient is positive in this test, what is the probability they have the disease?” Typically, for a good diagnostic test, the doctor will be able to say something like 95% and you and they can live with that. You might take a different, confirmatory test, if the result was very serious, like cancer. But in our Pillar 2 example, what is the probability a person testing positive in Pillar 2 actually has COVID-19? The awful answer is 11% (10 divided by 80 + 10). The test exaggerates the number of covid-19 cases by almost ten-fold (90 divided by 10). Scared yet? That daily picture they show you, with the ‘cases’ climbing up on the right-hand side? Its horribly exaggerated. Its not a mistake, as I shall show.
Earlier in the summer, the ONS showed the virus prevalence was a little lower, 1 in 2000 or 0.05%. That doesn’t sound much of a difference, but it is. Now the Pillar 2 test will find half as many real cases from our notional 10,000 volunteers, so 5 real cases. But the flaw in the test means it will still find 80 false positives (0.8% of 10,000). So its even worse. The headline would be “85 new cases identified today”. But now the probability a person testing positive has the virus is an absurdly low 6% (5 divided by 80 + 5). Earlier in the summer, this same test exaggerated the number of COVID-19 cases by 17-fold (85 divided by 5). Its so easy to generate an apparently large epidemic this way. Just ignore the problem of false positives. Pretend its zero. But it is never zero.
This test is fatally flawed and MUST immediately be withdrawn and never used again in this setting unless shown to be fixed. The examples I gave are very close to what is actually happening every day as you read this.
I’m bound to ask, did Mr Hancock know of this fatal flaw? Did he know of the effect it would inevitably have, and is still having, not only on the reported case load, but the nation’s state of anxiety. I’d love to believe it is all an innocent mistake. If it was, though, he’d have to resign over sheer incompetence. But is it? We know that internal scientists wrote to SAGE, in terms, and, surely, this short but shocking warning document would have been drawn to the Health Secretary’s attention? If that was the only bit of evidence, you might be inclined to give him the benefit of the doubt. But the evidence grows more damning.
Recently, I published with my co-authors a short Position Paper. I don’t think by then, a month ago or so, the penny had quite dropped with me. And I’m an experienced biomedical research scientist, used to dealing with complex datasets and probabilities.
On September 11th 2020, I was a guest on Julia Hartley-Brewer’s talkRADIO show. Among other things, I called upon Mr Hancock to release the evidence underscoring his confidence in and planning for ‘the second wave’. This evidence has not yet been shown to the public by anyone. I also demanded he disclose the operational false positive rate in Pillar 2 testing.
On September 16th, I was back on Julia’s show and this time focused on the false positive rate issue (1m 45s – 2min 30s). I had read Carl Heneghan’s analysis showing that even if the false positive rate was as low as 0.1%, 8 times lower than any similar test, it still yields a majority of false positives. So, my critique doesn’t fall if the actual false positive rate is lower than my assumed 0.8%.
On September 18th, Mr Hancock again appeared, as often he does, on Julia Hartley-Brewer’s show. Julia asked him directly (1min 50s – on) what the false positive rate in Pillar 2 is. Mr Hancock said “It’s under 1%”. Julia again asked him exactly what it was, and did he even know it? He didn’t answer that, but then said “it means that, for all the positive cases, the likelihood of one being a false positive is very small”.
That is a seriously misleading statement as it is incorrect. The likelihood of an apparently positive case being a false positive is between 89-94%, or near-certainty. Of note, even when ONS was recording its lowest-ever prevalence, the positive rate in Pillar 2 testing never fell below 0.8%.
It gets worse for the Health Secretary. On September the 17th, I believe, Mr Hancock took a question from Sir Desmond Swayne about false positives. It is clear that Sir Desmond is asking about Pillar 2.
Mr Hancock replied: “I like my right honourable friend very much and I wish it were true. The reason we have surveillance testing, done by ONS, is to ensure that we’re constantly looking at a nationally representative sample at what the case rate is. The latest ONS survey, published on Friday, does show a rise consummate (sic) with the increased number of tests that have come back positive.”
He did not answer Sir Desmond’s question, but instead answered a question of his choosing. Did the Health Secretary knowingly mislead the House? By referring only to ONS and not even mentioning the false positive rate of the test in Pillar 2 he was, as it were, stealing the garb of ONS’s more careful work which has a lower false positive rate, in order to smuggle through the hidden and very much higher, false positive rate in Pillar 2. The reader will have to decide for themselves.
Pillar 2 testing has been ongoing since May but it’s only in recent weeks that it has reached several hundreds of thousands of tests per day. The effect of the day by day climb in the number of people that are being described as ‘cases’ cannot be overstated. I know it is inducing fear, anxiety and concern for the possibility of new and unjustified restrictions, including lockdowns. I have no idea what Mr Hancock’s motivations are. But he has and continues to use the hugely inflated output from a fatally flawed Pillar 2 test and appears often on media, gravely intoning the need for additional interventions (none of which, I repeat, are proven to be effective).
You will be very familiar with the cases plot which is shown on most TV broadcasts at the moment. It purports to show the numbers of cases which rose then fell in the spring, and the recent rise in cases. This graph is always accompanied by the headline that “so many thousands of new cases were detected in the last 24 hours”.
You should know that there are two major deceptions, in that picture, which combined are very likely both to mislead and to induce anxiety. Its ubiquity indicates that it is a deliberate choice.
Firstly, it is very misleading in relation to the spring peak of cases. This is because we had no community screening capacity at that time. A colleague has adjusted the plot to show the number of cases we would have detected, had there been a well-behaved community test capability available. The effect is to greatly increase the size of the spring cases peak, because there are very many cases for each hospitalisation and many hospitalisations for every death.
Secondly, as I hope I have shown and persuaded you, the cases in summer and at present, generated by seriously flawed Pillar 2 tests, should be corrected downwards by around ten-fold.
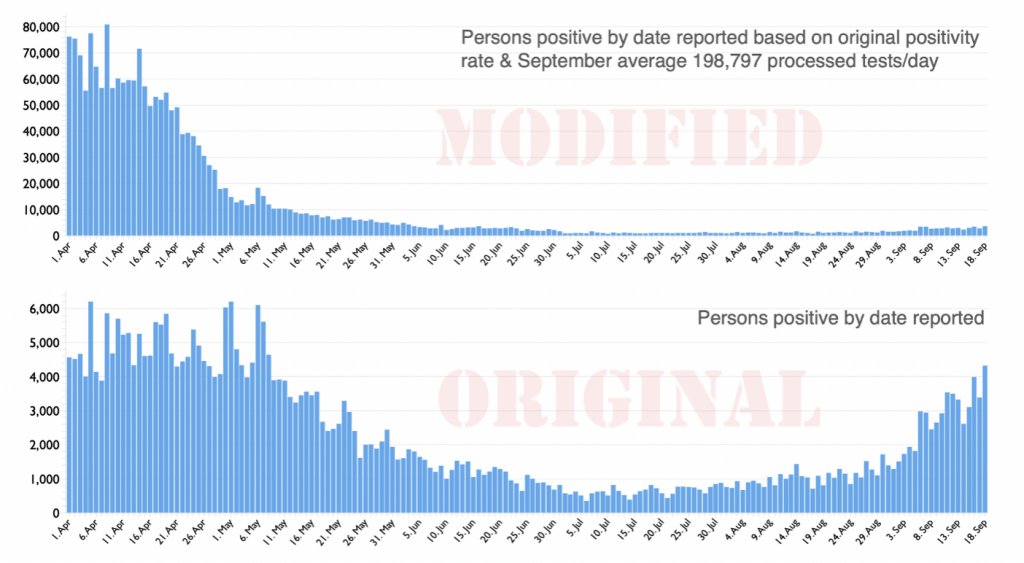
I do believe genuine cases are rising somewhat. This is, however, also true for flu, which we neither measure daily nor report on every news bulletin. If we did, you would appreciate that, going forward, it is quite likely that flu is a greater risk to public health than COVID-19. The corrected cases plot (above) does, I believe, put the recent rises in incidence of COVID-19 in a much more reasonable context. I thought you should see that difference before arriving at your own verdict on this sorry tale.
There are very serious consequences arising from grotesque over-estimation of so-called cases in Pillar 2 community testing, which I believe was put in place knowingly. Perhaps Mr Hancock believes his own copy about the level of risk now faced by the general public? Its not for me to deduce. What this huge over-estimation has done is to have slowed the normalisation of the NHS. We are all aware that access to medical services is, to varying degrees, restricted. Many specialities were greatly curtailed in spring and after some recovery, some are still between a third and a half below their normal capacities. This has led both to continuing delays and growth of waiting lists for numerous operations and treatments. I am not qualified to assess the damage to the nation’s and individuals’ health as a direct consequence of this extended wait for a second wave. Going into winter with this configuration will, on top of the already restricted access for six months, lead inevitably to a large number of avoidable, non-Covid deaths. That is already a serious enough charge. Less obvious but, in aggregate, additional impacts arise from fear of the virus, inappropriately heightened in my view, which include: damage to or even destruction of large numbers of businesses, especially small businesses, with attendant loss of livelihoods, loss of educational opportunities, strains on family relationships, eating disorders, increasing alcoholism and domestic abuse and even suicides, to name but a few.
In closing, I wish to note that in the last 40 years alone the UK has had seven official epidemics/pandemics; AIDS, Swine flu, CJD, SARS, MERS, Bird flu as well as annual, seasonal flu. All were very worrying but schools remained open and the NHS treated everybody and most of the population were unaffected. The country would rarely have been open if it had been shut down every time.
I have explained how a hopelessly-performing diagnostic test has been, and continues to be used, not for diagnosis of disease but, it seems, solely to create fear.
This misuse of power must cease. All the above costs are on the ledger, too, when weighing up the residual risks to society from COVID-19 and the appropriate actions to take, if any. Whatever else happens, the test used in Pillar 2 must be immediately withdrawn as it provides no useful information. In the absence of vastly inflated case numbers arising from this test, the pandemic would be seen and felt to be almost over.
Dr Mike Yeadon is the former CSO and VP, Allergy and Respiratory Research Head with Pfizer Global R&D and co-Founder of Ziarco Pharma Ltd.
US-based ‘creator of Novichok’ apologizes to Navalny, but Russian scientists say he wasn’t even involved in poison’s development
By Jonny Tickle | RT | September 21, 2020
US-based chemist and independence campaigner for Tatarstan Vil Mirzayanov has ‘apologized’ to Russian opposition figure Alexey Navalny, saying he considers himself indirectly responsible for his high-profile alleged poisoning.
Mirzayanov, who left Russia in the mid-1990s, has frequently claimed that he was one of the developers of Novichok. This has been rejected by other scientists known to have been on the team which created the lethal substance. In 1992, Mirzayanov leaked the structure of the poison, which resulted in Russian authorities charging him with treason, in a case that later collapsed.
Speaking to TV Rain, Mirzayanov said that he was part of the group behind the military-grade poison, which Germany claims has been found in the activist’s body. He also asserted that Navalny’s symptoms are typical of those experienced by people who have experienced exposure to Novichok.
“All the symptoms are similar,” Mirzayanov said. “Navalny will have to be patient. But in the end, he should recover.”
As none of Navalny’s associates were infected, the former scientist believes that the poison must have entered his body through his digestive tract.
However, according to Leonid Rink, a man commonly referred to in Russian media as the creator of Novichok, Mirzayanov was not involved in the development of the poison and is not an expert on its symptoms.
“He has nothing to do with biochemistry, nothing. He is an ordinary chromatographer,” Rink told Moscow news agency RIA Novosti. “He’s had nothing to do with the creation of Novichok.”
According to Rink, Navalny would not be alive if he was genuinely poisoned by Novichok.
Rink was backed up by Vladimir Uglev, another scientist known to have been on the poison’s development team, who claimed that Mirzayanov “never took part in field tests.”
Navalny, a well-known opposition figure and investigative journalist, fell ill on August 20, on a flight from Tomsk to Moscow. Following an emergency landing, he was immediately hospitalized in the Siberian city of Omsk. Two days later, after a request from his family and associates, Navalny was flown to Germany for treatment at Berlin’s Charité clinic. Over a week later, Berlin announced that the opposition figure was poisoned with a nerve agent from the ‘Novichok’ group. Contrary to German experts’ diagnoses, medical professionals in Omsk deny that any poison was found in his body.
On Saturday, a post on Navalny’s Instagram account explained that he is slowly recovering and is expected to get back to normal.
Mirzayanov has long been a vocal Kremlin opponent and Tatar activist. A member of the Presidium of the Milli Mejlis of the Tartar People in exile, he has prominently advocated for Tatarstan, a majority Muslim republic, to separate from Moscow. Back in 2008, he was declared “Prime Minister” of the region’s “government in exile”
Top UK scientists urge govt to protect most vulnerable from Covid-19 instead of carpet-bombing virus
RT | September 21, 2020
The UK should focus on helping the most vulnerable – including residents in care homes worst affected by Covid-19 – instead of pursuing an “unfeasible” goal of suppressing the virus until a vaccine arrives, top scientists urged.
British scholars penned an open letter to PM Boris Johnson, Chancellor of the Exchequer Rishi Sunak, as well as health chiefs in England, Scotland, Wales and Northern Ireland, asking them to urgently reconsider the current epidemic strategy.
Authored by Oxford professors Sunetra Gupta and Carl Heneghan, as well as Karol Sikora of the University of Buckingham and Sam Williams of the Economic Insight consultancy, the letter says the “existing policy path is inconsistent with the known risk-profile of Covid-19.” The appeal has been signed by dozens of academics from the UK’s leading educational institutions.
“The unstated objective currently appears to be one of suppression of the virus, until such a time that a vaccine can be deployed. This objective is increasingly unfeasible… and is leading to significant harm across all age groups, which likely offsets all benefits.”
The letter comes days after Health Secretary Matt Hancock pledged “to do what it takes” in order to fight Covid-19. After the UK recorded close to 4,000 confirmed coronavirus cases on Sunday, the government is considering a “circuit-breaking” period of tightened measures which could be announced later this week, UK media revealed.
Such a move could reportedly involve bringing back restrictions in public spaces for a few weeks, most of which were relaxed throughout May and June. Pubs and restaurants could be mandated to close earlier across the country, but schools and most workplaces would be kept open. Closing some parts of the hospitality industry is also one of the options.
According to the authors of the open letter, blanket measures aren’t the way to go. “Instead, more targeted measures that protect the most vulnerable from Covid, whilst not adversely impacting those not at risk, are more supportable,” they wrote.
“Given the high proportion of Covid-19 deaths in care homes, these should be a priority,” the scientists pointed out. The pandemic hit the UK’s nursing facilities exceptionally hard, claiming 19,394 lives between March and June, which accounted for 29.3 percent of all deaths in care homes during that time, according to government figures.
Last month, it emerged that care home staff were allegedly pressured by the NHS to admit coronavirus-positive or untested patients at the height of the crisis this spring. Nurses were reportedly instructed to change the status of all residents to “do not resuscitate.”
However, the government seems to have learned its lesson. Care facilities will receive £546 million ($702.5 million) to upgrade, reduce all but essential movements of staff between nursing homes to prevent the spread of the virus, and allow for the distribution of free PPE – masks and gloves – to the elderly and workers.
The UK has reported more than 394,000 coronavirus cases since the start of the epidemic, claiming close to 42,000 lives.
Featured Video

US Superpower Myth Shattered w/ Trita Parsi
or go to
Aletho News Archives – Video-Images
From the Archives
Israel Is A Genocidal Society
The Israeli Political Spectrum From The “Liberal Left” To The Far Right, Is United In Genocide
The Dissident | May 5, 2026
… The fundamental issue of Israel is not Benjamin Netanyahu, but the fact that Israel is overwhelmingly a bloodthirsty, war-ready, genocidal society.
Historian Zachary Foster has documented that the overwhelming majority of Jewish Israelis have supported every Israeli war since the 2006 invasion of Lebanon, writing:
2006
86% of the Israeli adult population justified “the IDF operation in Lebanon against Hizbollah,” or 2006 Lebanon War, in which Israel killed 1,191 people, the vast majority civilians according to HRW (Note that the % of Jewish Israelis who supported the war was even higher)2008-2009
82% of the Israeli public thought that the 2008-9 war on Gaza was justified (in which Israel killed 1,417 Palestinians, the vast majority civilians.) Note that the % of Jewish Israelis who supported the war was even higher2012
90% of Israeli Jews supported war on Gaza ( in which Israel killed 160 Palestinians, 66% civilians)2014
95% of Jewish Israelis believed the war on Gaza was justified (in which Israel killed 2,310 Palestinians, 70% civilians)2021
72% of Israelis believed the war on Gaza should continue (as of May 21) after Israel had already killed 250 Palestinians in Gaza, vast majority civilians. The % of Jewish Israelis who supported killing more Palestinians was much higher.2024
A January poll found 95% of Jewish Israelis thought the Israeli military was using either the “appropriate” amount of force or “too little” force in Gaza at a time when Israel had already killed >25,700 Palestinians in Gaza.2024
In September, 90% of Jewish Israelis supported the war on Lebanon (in which Israel killed 800+, including hundreds of civilians)2025
In March, 82% of Israeli Jews supported the forced expulsion of residents of Gaza, Israel’s main goal in it’s genocide & war on Gaza.2025
In June, 82% of Jewish Israelis supported the war on Iran known as the “twelve day war”2026
On March 4, 93% of Israeli Jews expressed support for the war on Iran. 97% of “right-wing” Jewish Israelis support it, compared with 93% in the center and 76% on the left.
The overwhelming majority of Jewish Israelis also have openly genocidal views towards Palestinians.
Polls in Israel have shown that:
- 84% of the (Israeli )public gives the IDF an excellent or very good grade regarding the moral conduct of the army
- 75% of Jewish Israelis agree with the idea that ‘there are no innocents in Gaza.’
- A vast majority of Israeli Jews – 79 percent – say they are ‘not so troubled’ or ‘not troubled at all’ by the reports of famine and suffering among the Palestinian population in Gaza.
The fundamental problem in Israel is Zionism, not Benjamin Netanyahu. – Full article
Blog Roll
 Aletho News
Aletho News- Villains of Judea: Samuel Zemurray
- Billionaires and Officials Are Just Blatantly Ignoring the Will of the People Now
- Prof Marandi Warns: Blockade stays Until Israel Withdraws!
- Iranian forces strike US vessels in swift retaliation for tanker attack: Top military commander
- Israeli ‘double tap’ strike hits paramedics in south Lebanon hours after renewed bombing of Beirut
- Occupation Bulldozes Farmland, Uproots Vineyards
- ‘Israel’ kills Azzam al-Hayya, son of Hamas chief Khalil al-Hayya
- What has Guterres supported in Gaza?
- UAE received $80m in EU farming subsidies as calls grow for sanctions over Sudan genocide
- Trump gives green light for new arms deliveries to Ukraine
- If Americans Knew
- Two Supreme Court Justices were secret agents who helped Israel cover up its attack on the USS Liberty
- Bari Weiss ‘Meddles’ With ‘CBS Sunday Morning’ Story on Palestine
- Zionists Are Gunning for Your Freedom of Speech
- The horrors in Gaza continue: Here are the facts
- Israeli General Is Running a Sophisticated, Sociological Engine of Violence
- Israel has stolen $4.8 billion from Palestinians
- The pro-Israel political consensus is collapsing in both parties
- Prominent Christian Zionist Group Is Lobbying U.S. Lawmakers on Israel—Without Revealing It’s Funded by Israel
- “Most Moral Army” caught desecrating another Christian statue, as famine looms in Gaza – Daily Update
- Israel’s subversion of Foreign Agents Registration Act
- No Tricks Zone
- New Study: Declining Trends In 1980-2023 Tropical Cyclone Frequency, Accumulated Energy
- 46 IPCC Scientists Break Rank, Publicly Challenge Long-Standing Dogmatic Climate Claims
- Another Study Links Warming To Cloud Forcing, Shortwave Radiation, Natural Atmospheric Circulation
- Wind Energy Is Toxic, Hazardous To Human Health, Scientific Review Shows
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
