The United Nations World Health Organization (WHO) has published a new draft of its troubled pandemic agreement/accord/treaty – which the agency has complained is taking too long to finalize.
The latest draft of the negotiating text, released by the Bureau of the Intergovernmental Negotiating Body (INB) on Monday must be considered until the INB session scheduled for November 6-10, when it should be formalized.
Some of the commitments contained in this version of the document have to do with combating “false, misleading, misinformation or disinformation, including through effective international collaboration and cooperation” – which skeptics might easily dub, “cross-border censorship.”
And then there’s surveillance, too: something called One Health approach for pandemic prevention, preparedness and response, which the draft wants to see promoted and implemented. Meanwhile, One Health is a surveillance tool that is supposed to create new methods of disease control.
Yet another point from the proposal is to “develop and strengthen pandemic prevention and public health surveillance capacities.”
Critics have many concerns and misgivings about all of this, including WHO setting up what’s known as a conference of the parties – an international convention’s top governing body – around the pandemic accord.
The fear here is that it would be one more instrument taking agency and consent away from national governments and people and transferring the decision-making processes, in this case related to health, to the world organization, specifically, WHO.
However, the draft’s chapter on institutional arrangements envisages establishing just such a conference of the parties as part of the accord’s scope.
A number of advocacy organizations from around the world have already expressed their dissatisfaction with the draft from different points of view, including how the treaty, if adopted, would impact less developed countries, while the draft itself is seen as “unbalanced.”
This last objection stems from the origin of the proposal – namely the discussions between INB Bureau and Secretariat, rather than drawing from the meetings of the INB itself.
Ignoring proposals from all countries that are supposed to implement the treaty, and allowing those with the most clout (in the Bureau) to set the tone is seen as one-sided in this sense as well.
It’s happening. The manufacturers and regulators knew it was a risk, yet, like numerous aspects of the Covid vaccine mRNA technology, did not test for excretion potential of spike proteins or LNP’s.
Awareness of the Federal Regulators and Vaccine Manufacturers
The data showing the toxicity and lethality of the vaccines started within weeks of the roll-out with hundreds of thousands of adverse events and hundreds of deaths reported to VAERS in January of 2021, far exceeding previous stopping points of any new medical product or vaccine.
Although ignored (to this day), anyone paying unbiased attention could see a further mountain of evidence develop, including a skyrocketing number of newspaper and television reports of healthy athletes and young people arresting and dying while doing normal everyday activities or sports (countered by corporate/government controlled media with a plethora of fact checking articles using cherry picked data to inform the world that what they are seeing is not factually true).
Then life insurance industry data emerged showing historically unprecedented rises in death claims being paid out amongst the healthiest sectors of society temporally associated with the proliferation of Covid mRNA vaccine mandates within schools, corporations, universities, health care institutions, federal contractors etc. Most telling of the deathly impact of mandates was the fact that the largest increases among the sudden, rapid rises in excess deaths occurred among employed white collar workers.
It truly is unimaginable that we now must consider the risks (and reality) of “shedding” of the vaccine products from the vaccinated to the unvaccinated. This now has implications for nearly every human being walking the earth, vaccinated or unvaccinated (including me).
This series will explore the regulatory, scientific, epidemiological, and clinical data indicating that shedding is occurring. The health of who knows how many is now being threatened, with the extent of the risks likely both highly variable and difficult to predict, both in the short term and long term. That is unless we start to seriously study the phenomenon further. So, let’s review what is known.
Within 3 months of the rollout of the global Covid mRNA vaccination campaign, I was consulted by two different unvaccinated women in their late 30’s and early 40’s respectively, who reported that they were suffering acute menstrual abnormalities in the days following close exposure to a recently vaccinated practitioner (one visited a massage therapist and another an acupuncturist). Both had a history of highly regular, uncomplicated menstrual cycles over decades.
Since that time, at least twenty other unvaccinated and vaccinated people, both men and women, have reported to me compelling histories of typical post-mRNA vaccine adverse effects subsequent to close exposure to vaccinated family members, contacts, or friends.
Further, my partner Scott Marsland at our Leading Edge Clinic, who also specializes in treating Long Covid/Long Vax syndromes, has a growing series of detailed case histories of similar “shedding” events occurring. I will revisit this in a later post in this series, but I will briefly say here that our clinical observations conclude that symptomatic shedding events do occur. However, we have little idea of exactly how common it is occurring among the general population.
This is further complicated by the fact that even if it were occurring frequently, the vast majority of people suddenly developing typical vaccine side effects symptoms after exposure to a vaccinated person would never think to relate it to exposure to shed vaccine products. It is my belief that very few people in the general public are aware of the possibility it could occur. You know, because the regulators have assured the country that mRNA technology is “safe and effective.”
However, my general sense is that it occurs largely in people who have increased physiologic sensitivity to environmental exposures, toxins, or pharmaceuticals and that it is generally transmitted by someone recently vaccinated or someone who is producing a lot of spike protein. Note that is my “general sense.” More studies are required to fully understand both the frequency of and physiologic impacts from such events.
My ignorance as to the frequency of symptomatic shedding events is due to the fact that the concept of transmitting spike proteins (or lipid nanoparticles) from a Covid mRNA vaccinated person to another is one of the least studied and published-on aspect of the mRNA vaccine technology.
What is so shocking about that lack of research (actually nothing is shocking anymore) is that shedding has major global implications. Apparently it is not just me who thinks this because, as an expert on several aspects of Covid, I have been lecturing across the U.S, Europe, and South America in conferences, Parliamentary hearings, or invited lectures. Questions about shedding appear everywhere (in the dozens of Q & A’s that I have participated in, it is nearly always the first question. It is also a very common topic in the chat of our FLCCC weekly webinar.
Know that in this tonight’s FLCCC webinar, I will present a 15-20 minute overview of this series along with my private practice partner Scott Marsland. We expect to be deluged with questions after.
Anyway, I believe that by the end of this series on the science, epidemiology, and clinical observations of shedding, you will be convinced that it can and does occur.
What IS The Definition Of Shedding In Regards To The Covid mRNA Vaccines?
From our Federal government, in this FDA document, the term “shedding” is defined as:
“The release of viral or bacterial gene therapy products from the patient by any or all of the following routes: feces (feces); secretions (urine, saliva, nasopharyngeal fluids, etc.); or through the skin (pustules, lesions, sores).”
They forgot to mention “exhaled breath.” More on that later. The “products” they refer to that can be transmitted from a Covid vaccinated person to another include not only the genetically programmed spike protein product, but also the lipid nanoparticle (LNP) containing the mRNA that is in the injections as well as naked mRNA that can be released from the LNP. Even more worrying is the recent shocking discovery that every single Moderna and Pfizer vaccine vial is contaminated with high levels of DNA plasmids potentially capable of integrating into the human genome. Contemplating that last one is disturbing, the implications of which we will not know for some time.
Why Would The Modified mRNA Vaccine Technology Lead To The Possibility of Shedding?
“Gene therapy products are all products that mediate their effects by transcription and/or translation of transferred genetic material and/or by integrating into the host genome and that are administered as nucleic acids, viruses, or genetically engineered microorganisms.
Also note that in this European Medicines Agency (EMA) document, the mRNA vaccines also meet their definition of gene therapy medicinal products (GMTP’s).
Ok, now that we know what a gene therapy product is and that the Covid mRNA injection is actually a form of gene therapy (marketed to the public as a “vaccine”), what does that have to do with “shedding?” Again from the FDA document regarding the evaluation of the safety of gene therapy products, they emphasize the importance of studying shedding:
Shedding is distinct from biodistribution because the latter describes how a product is spread within the patient’s body from the site of administration while the former describes how it is excreted or released from the patient’s body. Shedding raises the possibility of transmission of virus or bacteria based gene therapy products (VBGT) from treated to untreated individuals (e.g., close contacts and health care professionals).
This guidance represents FDA’s current thinking on how and when shedding data should be collected for VBGT and oncolytic products during preclinical and clinical development and how shedding data can be used to assess the potential for transmission to untreated individuals.
So, with these findings in mind, it may be no wonder why the FDA insists on shedding studies:
Further on in the document, the FDA again emphasizes the importance of shedding studies:
Note that the FDA emphasizes the importance of doing human shedding studies and not just relying on animal studies:
To inform the design of human shedding studies, shedding data may be collected in animals following administration of the VBGT or oncolytic product. These data can help estimate the likelihood and potential shedding profile in humans, particularly when there is concern about transmission to untreated individuals. However, such data cannot substitute for human shedding studies for several reasons.
But again, no studies testing whether excretion of mRNA-containing LNPs, modified spike-encoding mRNA, or spike produced by vaccinated people have been done. Well, I shouldn’t say none, because in this paper the author cites a Pfizer document obtained by FOIA which apparently revealed that shedding was studied in the urine and feces of intra-muscular injected rats. Unfortunately, that document is no longer at the website referenced.
To summarize from the above, the FDA’s position is that:
the mRNA vaccines are gene therapy products
Gene therapy products require shedding studies in both animals and humans
Gene therapy product shedding raises the possibility of transmission from treated to untreated individuals
Note that much of the rest of this series of posts on shedding is guided by a masterful comprehensive review of the topic of gene therapy product shedding by independent researcher (by definition) Helene Banoun inInfectious Diseases Research. Hers is one of the only papers I could find that attempted to meticulously explore what is known about shedding of the mRNA gene therapy vaccines.
As already stated, an important point Banoun makes is:
There was no regulation of mRNA clinical trials prior to RNA vaccines, yet there is strict regulation of gene therapy products. It is difficult to justify that mRNA vaccines are not considered in the same way as gene therapies regarding this regulation; indeed the only difference is that they are (historically) supposed to protect against a disease and not cure it. Gene therapies are intended for a small number of people in poor health, whereas vaccines are used on a large scale on healthy people: it would therefore be wise to apply stricter rules to them.
She further points out another omission of the regulatory process:
Any experiment involving the deliberate transfer of a nucleic acid to a human must be preceded by Institutional Biosafety Committee approval (document on the regulatory standards is here), but approval was not given because of the emergency clearance given to mRNA vaccines.
Therefore, according to both the American and European agencies, mRNA vaccines are gene therapy products and should have been subjected to excretion studies of all secreted fluids (urine, exhaled droplets, saliva, sputum, nasopharyngeal fluids, semen, breast milk, feces, and sweat). Again, these studies were not done for mRNA vaccines nor for the DNA adenovirus vaccine (J&J).
So, where are the clinical human shedding studies? Well, I just learned of one that is about to be published (next ten days?) where the research team exposed a population of unvaccinated women to vaccinated individuals and their assessment outcome was the development of menstrual abnormalities. I know the results but want to respect the research teams right to present their original work. They have promised to share their manuscript with me and Paul Marik as soon as the peer-review and acceptance process is complete. I have no idea what journal they submitted to but I can be highly confident it is not the New England Journal of Medicine.
The entire reason why I did a “deep dive” into shedding science is because shedding was not studied when it absolutely should have been and I believe with near certainty that it occurs. Note my use of “near certain” is only to seem objective but it really is too late for that – both my partner Scott and I have diagnosed and successfully treated a number of shedding “victims.”
The lack of shedding studies prior to the mRNA rollout was, in my opinion, an insanely reckless and irresponsible omission (or willfully criminal, take your pick). As an evolving expert in the evaluation and treatment of Covid mRNA vaccine injury syndromes, I and others have identified thespike protein as the main component responsible for not only the pathogenicity of Covid but also of the vaccines, with this review paper proposing a new field named “spikeopathy” (study of the disease processes triggered by the spike protein).
If vaccine transcribed spike protein can be transmitted in sufficient quantity from vaccinated folks to unvaccinated ones, it stands to reason that adverse effects of the vaccine can develop in some unvaccinated people who came into contact (or close proximity) with vaccinated people.How did they get away with not studying this possibility?
An easy answer is they were doing science at “warp speed.” The more uncomfortable answer is that the “vaccines”, although meeting the definition of a gene therapy product, were actually not even legally considered a medical product at all and thus did not require a diverse range of safety studies (like on genotoxicity, reproductive risks, excretion potential etc). What? Why? How?
The reality is that the Covid vaccines, as a result of successive federal legislative actions which evolved over decades, was legally categorized as a “countermeasure” under a “public health emergency.” Such “countermeasures” require no specific regulatory approval process prior to dissemination. All a countermeasure needs is the recommendation of the Secretary of Health and Human Services that “it may be effective.”
This is the conclusion derived from the legal investigatory work of various independent and legal experts and researchers like Catherine Watts, Todd Callender, and Sasha Latypova. If interested in learning more, I would watch this lecture by Sasha Latypova (scroll down the page to find her lecture). As they have uncovered, “countermeasures” (even gene therapy ones) do not legally require studies of excretion potential, bio-distribution, pharmacokinetics, genotoxicity, insertional mutagenesis etc.
They don’t even require FDA regulated clinical trials of efficacy or safety.
So why did Pfizer and Moderna even do the efficacy trials? Latypova maintains that they did this not only to satisfy the public’s confidence to increase vaccine uptake, but also to “fool” the public into thinking these vaccines were medical products subject to standard (albeit accelerated) pharmaceutical product regulatory processes.
This obscured the reality that they were instead classified as military “countermeasures” against a perceived (if not actual) bioweapon. To wit, the COO of Operation Warp Speed was a General from the Department of Defense (DOD) and the vaccine manufacturers were under contract with the DOD to produce the countermeasure, sometimes referred to as a “demonstration (demo)” and/or a “prototype” in numerous legal documents they uncovered.
Anyway, as a result of this lack of a legal requirement to fully study these products in a public health emergency, the list and types of studies that should have been conducted (but were not) is long. Researchers and clinicians have been screaming about this since they were rolled out. These cries were met with a deafening silence by governmental health agencies across the world.
I know, it is a lot to take in.
But the latest “word on the street” is that the finance and insurance industries may finally be waking up to this fraud and its devastating impacts on U.S disability and death rates. Knowledge of these society-wide impacts largely results from the work of two different research teams led by former Blackrock portfolio manager Ed Dowd and insurance industry consultant Josh Stirling).
This article describes the reasons why Pfizer and Moderna stock are crashing of late. Put more succinctly, from what I hear it is due to the hedge fund guys shorting their stock. I believe Pfizer is in even deeper trouble now that this “forensic” paper just got published finding that they hid vaccine trial deaths which obscured a 3.7 fold increased risk of cardiac death in the vaccinated arm of their trial.
“Shedding” Part 1– Shedding of Covid mRNA Vaccine Components and Products From The Vaccinated to the Unvaccinated – Part 1
“Shedding” Part 2 – The Bio-Distribution and Excretion Potential of Covid mRNA Vaccine Products
“Shedding” Part 3 – Can You Absorb Lipid Nanoparticles From Being Exposed To a Vaccinated Person?
“Shedding” Part 4 – Evidence of Placental and Breast Milk Transmission of Covid mRNA Vaccine Components
What is “shedding” and what are the implications for our health? Tonight, host Betsy Ashton will be joined by Dr. Pierre Kory and Scott Marsland, FNP-C for this important discussion.
My clinical practice is loaded with patients who took one or two vaccines early in 2021 and realized like most of us that the the mRNA products were not safe. A common question is: “doctor when does this shot get out of my body?”
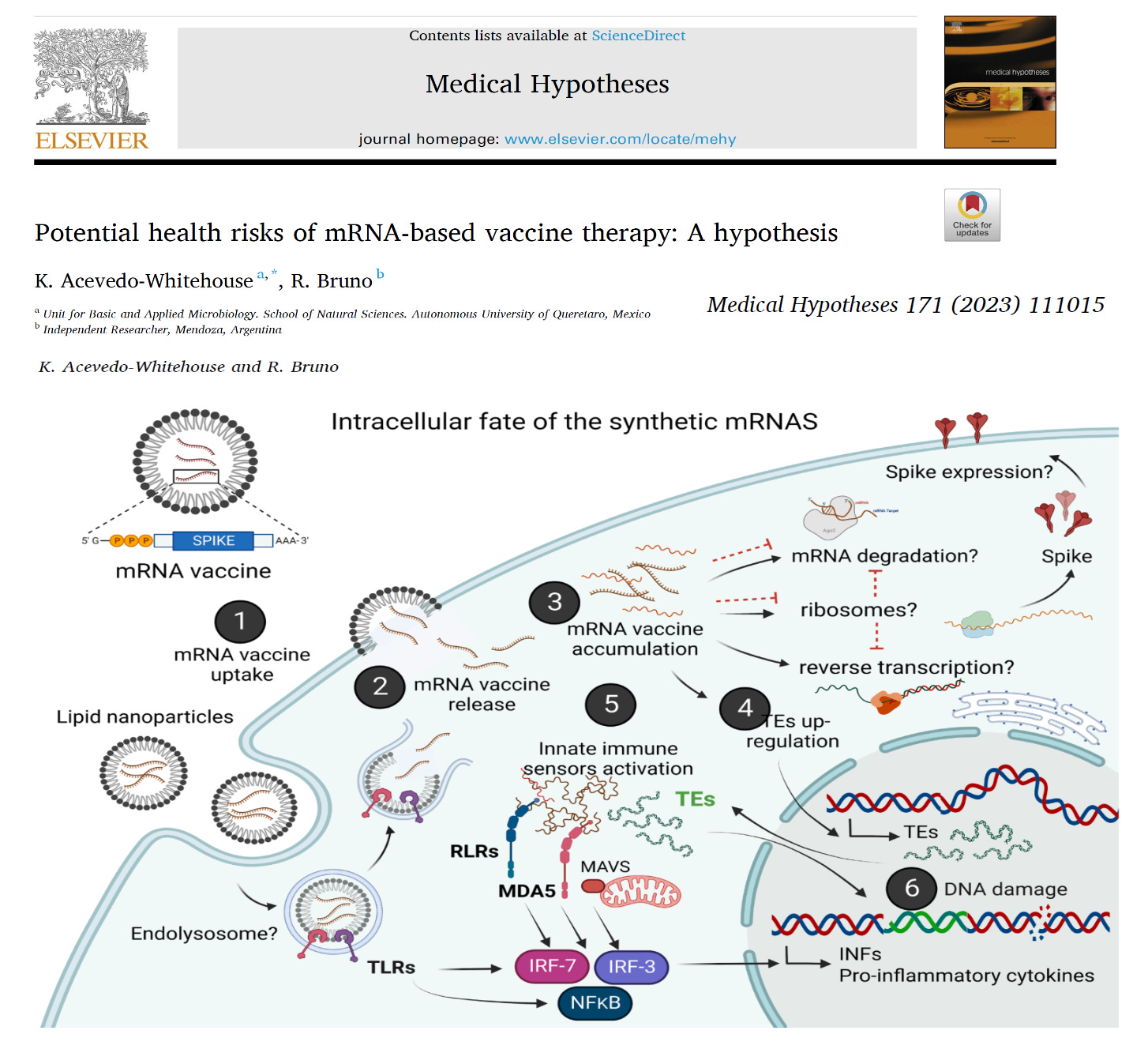
Acevedo-Whitehouse and Bruno raise this point in a recent peer reviewed publication concerning the entire mRNA vaccine product pipeline.
Therapeutic applications of synthetic mRNA were proposed more than 30 years ago, and are currently the basis of one of the vaccine platforms used at a massive scale as part of the public health strategy to get COVID-19 under control. To date, there are no published studies on the biodistribution, cellular uptake, endosomal escape, translation rates, functional half-life and inactivation kinetics of synthetic mRNA, rates and duration of vaccine-induced antigen expression in different cell types. Furthermore, despite the assumption that there is no possibility of genomic integration of therapeutic synthetic mRNA, only one recent study has examined interactions between vaccine mRNA and the genome of transfected cells, and reported that an endogenous retrotransposon, LINE-1 is unsilenced following mRNA entry to the cell, leading to reverse transcription of full length vaccine mRNA sequences, and nuclear entry. This finding should be a major safety concern, given the possibility of synthetic mRNA-driven epigenetic and genomic modifications arising.
These are stunning revelations. I have called for a halt on mRNA research development until these fundamental questions can be answered. If synthetic mRNA cannot be broken down by the human body, there were be no way to shut off potentially dangerous antigens such as the Spike protein of SARS-CoV-2, Influenza virus hemagglutinin (HA), or any other toxin produced from the genetic code. To make matters worse, it appears that all of these proteins will be expressed on the cell surface and cause auto-immunity with any new mRNA vaccine. This alone is a show stopper for me in my practice. I am advising NO mRNA vaccines for my patients.
Independent journalists Glenn Greenwald and Matt Taibbi recently had a conversation where they highlight a key point of our New Normal times – namely, that all real disinformation comes from government or mainstream media sources.
It occurs to me that our side needs to keep pounding home this point, which might resonate with enough citizens to make the proverbial difference.
What leaders on our side need to do is repeatedly point out that the real disinformation is coming from authorities and “experts.” If enough people accept this truism, the disinformation spreaders might encounter formidable obstacles as they attempt to enforce the rest of their freedom-eradicating agendas.
I’d start by simply pointing out all the allegedly true information promulgated by officials that was really false information.
Just with the categories of “settled Covid science,” most citizens in the world would probably acknowledge they’ve been sold a fraudulent bill of goods.
For example, how many adults really think the Covid “vaccines” and “boosters” prevent infections or stop or slow virus spread?
My guess: There might be 125 (?) people in world who still believe this official disinformation.
Also, if everyone was given a powerful dose of truth serum, I think everyone would admit that they know at least a few people who might have been harmed (or even died) because they received a Covid shot. So the narrative that the “vaccines” are safe or prevent “severe cases” is not really accepted by most people.
Quick thought exercise: If every person did believe the “vaccines” are safe and effective and this virus was a real threat to their health, every person would be getting the latest round of new boosters … instead of maybe five percent of the population. This means 95 percent of citizens are showing their true beliefs by what they are not doing.
This is what one might call a truth “tell.”
Poll questions that will never be asked …
It would be interesting if some well-known polling organization surveyed people and simply asked a large sample of citizens two questions:
Question 1: Do you think the Covid vaccines are “effective” at preventing new cases?
Question 2: Have you heard or read about any person who might have suffered a vaccine injury?
I just proposed two common-sense poll questions I know will never be asked by important polling organizations – because I know that every important organization is now captured. (“Every important organization” would include the important public opinion polling organizations.)
This example illustrates how it’s almost impossible to prove that the government and its many cronies are trading in disinformation – because all the exercises that might prove this won’t occur.
I’ve written a thousand times that officials won’t investigate that which they don’t want to confirm. Simple opinion polls would be one example of a truth-seeking tool that can never be employed in our New Normal.
Funding and authorizing a large number of autopsies of all the people who “died suddenly” is another example of taboo investigations.
Yet another example would be all the people who have contacted mainstream media news organizations and told editors or journalists that a loved one died or was severely injured by a vaccine.
Question: How many mainstream journalists followed up on these news tips?
I’m pretty sure the answer is zero. I would also be willing to bet that every news organization in the word has received numerous news tips like this … so this is not some random, outlier anecdote.
Not only have no real investigations of vaccine injuries been performed by the so-called “watchdog” press, the public doesn’t even know how many times these requests have been ignored and dismissed.
We don’t need Covid examples to know how important disinformation is to the Establishment classes …
The reason I think the public might belatedly accept the truism that it’s officials who spread disinformation is that, by now, many members of the public understand that official narratives of the past have been debunked.
Matt and Glenn discussed one the best-known examples of bogus government-spread disinformation when they discussed the justification for America’s invasion of Iraq. The main justification was, of course, that Saddam Hussein possessed “weapons of mass destruction.”
I’m sure some people still believe this, but I would guess at least 75 percent of thinking citizens now realize this was a lie.
The good news is that many people who supported the invasion of Iraq later came to believe that Iraq didn’t have such weapons and came to believe that American citizens shouldn’t have been stressed out over an impending attack from Iraq.
My take-away, which is very germane to discussions of our Covid times, is that some lies do later get exposed as lies. People are willing to admit they no longer believe the official narrative.
Whether they know it or not, these people are admitting that they were duped by sophisticated disinformation campaigns … and the disinformation didn’t come from kooks on the Internet – it came from the “leaders” of the important organizations in the country.
Another disinformation campaign that changed the world (for the worse)
The “War on Terror” had several components, including several accepted storylines which should now be viewed as dubious disinformation.
One of these storylines is that terrorists were going to attack America with “bio-weapons,” which meant the government needed to spend billions of dollars investigating possible viruses and, most importantly, begin working preemptively on “vaccines” that would protect American citizens if and when such an attack occurred.
The terrorist attacks of 9-11 changed the world, but it might have been the anthrax letters which were mailed shortly after these attacks that changed the world even more.
The (almost-certain) disinformation at the time was that terrorists had mailed those anthrax spores.
The story that’s more likely to be true is that it was an American who mailed the anthrax (which actually doesn’t pose any great threat to the population). Also, the anthrax almost certainly came from a lab funded by American tax payers.
It didn’t really matter where the anthrax came from or who mailed it, all that mattered was that the “gain of function” research into deadly viruses proceeded at warp speed. Scientists researching possible bio-weapons received a blank check. Most significantly, the Science Industrial Complex merged with the Military Industrial Intelligence Complex.
Nobody (except maybe Ron Paul) would have guessed that 20 years later this strain of “disinformation” would lead to the whole world being locked down and then to mandatory mRNA vaccines.
It wasn’t Saddam Hussein who made sure we couldn’t go to church or could no longer go to any job deemed “non-essential.” The dictators issuing those orders worked in our own government … and were issuing orders based on their own disinformation.
The few brave contrarians who tried to warn the population what was really happening were labeled as traitors, the “enemy,” “science deniers” and disinformation spreaders.
Just like it was a coordinated effort to fool everyone into thinking Saddam Hussein was coming after grandma and our children with weapons of mass destruction, so too with the Mother of All Pandemics, which was entirely the product of government-produced disinformation.
In other words, the public shouldn’t need examples of Covid disinformation to realize the government’s been trading in disinformation for longer than most people have been alive.
And the reason the government and its partners trade in disinformation is because … this works.
If more people would just pause and use their brains, they’d probably realize it’s only an entity as powerful as the government (or the government’s shadow rulers) that can use disinformation to control the majority of the population.
Truth be told, a few contrarians on social media probably couldn’t turn the whole giant ship of state or even debunk a few bogus narratives.
However, ifthe arguments of these contrarians were persuasive enough, these contrarians’ points might spread to the masses.
This scenario no doubt identifies the real fear of our ruling class. To stop this possibility, the contrarians were labeled “disinformation” spreaders … by the very people and organizations who were spreading the real disinformation.
They don’t want us to identify them …
If a few more great communicators could simply point out who actually produces and then disseminates all the key disinformation, the world might have a fighting chance going forward.
What the world needs is some “Most Wanted” type posters that simply include the photos and job titles of the officials who are spreading the world’s important disinformation.
These posters would have to be humongous because they’d include photos of just about every key official in government and every editor and publisher of every mainstream media “news” organization.
The headline on this poster might say, “These are the people and organizations who are really spreading disinformation. These people have the means and the motives to spread dangerous disinformation. The public should quit trusting all of these people.”
I know such a project would be dangerous and wouldn’t even be “allowed” by the Censorship Industrial Complex. Still, somehow we’ve got to identify the real villains, who are the spreaders of the real disinformation.
In recent years a vast industry has been created for the “detection, management, and correction of disinformation and misinformation.” Dozens of foundations, big tech companies, and government agencies are now disbursing hundreds of millions (in aggregate) to university departments to train young people for a career in misinformation and disinformation management.
Dr. Aaron Kheriaty mentioned this to me in an interview last summer, and a few nights ago, Dr. McCullough asked me to do some research on this new industry. My inquiry has led me into a Bluebeard’s Castle of horrors.
A quick Google search of “misinformation correction” results in countless reports of grant awards in this burgeoning industry. In other words, instead of acquiring a liberal education (based on the central principle of freedom of speech and expression) an army of college students are in training to become professional censors and propagandists.
How do graduates from university censorship programs conceptualize guys like Dr. Peter McCullough and (to a lesser extent) me?
We are, in the Orwellian language of the censorship schools, “Malinformants”— that is, guys who spread “harmful” information. Because we have been designated as such, we are suitable candidates for “PreBunking.” The following video is a sort of “PreBunking” manual. Note that the technique is explicitly and favorably compared to a vaccine.
The telltales that you’ve become a “PreBunked Malinformant” is when you run afoul of internet trolls who display some or all of the following identifiers:
Express a zealous belief that vaccines are the saviors and redeemers of mankind.
Display an icon of the Ukrainian flag on their profile.
Use extremely disparaging, ad hominem, and sanctimonious language.
Characterize you of being a “grifter.”
So, how does it feel to be a “PreBunked Malinformant”? Setting aside the feeling of vexation that I’m contending with kids who possess none of my education or experience, I’m left with the emotion of total amazement that American universities now have astoundingly well-financed schools of censorship.
How could this have possibly come about in the United States of America?
The global elite plan to introduce a near-permanent “global state of emergency” by re-branding climate change as a “public health crisis” that is “worse than covid”.
This is not news. But the ongoing campaign has been accelerating in recent weeks.
I have written about this a lot over the last few years – see here and here and here. It started almost as soon as Covid started, and has been steadily progressing ever since, with some reports calling climate change “worse than covid”.
But if they keep talking about it, I’ll keep writing. And hopefully the awareness will spread.
Anyway, there’s a renewed push on the “climate = public health crisis” front. It started, as so many things do, with Bill Gates, stating in an interview with MSNBC in late September:
We have to put it all together; it’s not just climate’s over here and health is over here, the two are interacting
Since then there’s been a LOT of “climate change is a public health crisis” in the papers, likely part of the build-up to the UN’s COP28 summit later this year.
Following Gate’s lead, what was once a slow-burn propaganda drive has become a dash for the finish line, with that phrase repeated in articles all over the world as a feverish catechism.
It was an editorial in the October edition of the British Medical Journal that got the ball rolling, claiming to speak for over 200 medical journals, it declares it’s…
Time to treat the climate and nature crisis as one indivisible global health emergency”
Other publications get more specific, but the message is the same. Climate change is bad for the health of women, and children, and poor people, and Kenyans, and workers and…you get the idea.
And that’s all from just the last few days.
It’s not only the press, but governments and NGOs too. The “One Earth” non-profit reported, two days ago:
Both the Red Cross and Doctors Without Borders have published (or updated) articles on their website in the last few days using variations on the phrase “The climate crisis is a health crisis.”
Local public health officials from as far apart as Western Australia and Arkansas are busy “discussing the health effects of climate change”
WHO data indicates 2 billion people lack safe drinking water and 600 million suffer from foodborne illnesses annually, with children under 5 bearing 30% of foodborne fatalities. Climate stressors heighten waterborne and foodborne disease risks. In 2020, 770 million faced hunger, predominantly in Africa and Asia. Climate change affects food availability, quality and diversity, exacerbating food and nutrition crises.
Temperature and precipitation changes enhance the spread of vector-borne diseases. Without preventive actions, deaths from such diseases, currently over 700,000 annually, may rise. Climate change induces both immediate mental health issues, like anxiety and post-traumatic stress, and long-term disorders due to factors like displacement and disrupted social cohesion.
They are tying “climate change” to anyone who is malnourished, has intestinal parasites or contaminated drinking water. As well as anyone who dies from heat, cold, fire or flood. Even mental health disorders.
We’ve already seen the world’s first “diagnosis of climate change”. With parameters set this wide, we will see more in no time.
Just as a “Covid death” was anybody who died “of any cause after testing positive for Covid”, they are putting language in place that can redefine almost any illness or accident as a “climate change-related health issue”.
Two days ago, the Director General of the World Health Organization, the UN’s Special Envoy for Climate Change and Health and COP28 President co-authored an opinion piece for the Telegraph, headlined:
Climate change is one of our biggest health threats – humanity faces a staggering toll unless we act
The WHO Director went on to repeat the claim almost word for word on Twitter yesterday:
The climate crisis is a health crisis. Air pollution and extreme temperatures are causing an increase in diseases like diabetes, cancer, cardiovascular and respiratory. People are dying prematurely, and the most vulnerable are being hit the hardest. We must prioritize healing our…
Consider, the WHO is the only body on Earth empowered to declare a “pandemic”.
Consider, the official term is not “pandemic”, but rather “Public Health Emergency of International Concern”.
Consider, a “public health emergency of international concern”, does not necessarily mean a disease.
It could mean, and I’m just spit-balling here, oh, I don’t know – maybe… climate change?
Consider, finally, that one clause in the proposed “Pandemic Treaty” would empower the WHO to declare a PHEIC on “precautionary principle” [my emphasis]:
Future declarations of a PHEIC by the WHO Director-General should be based on the precautionary principle where warranted
Essentially, once the new legislation is in place, the plan writes itself:
Put new laws in place enabling global “emergency measures” in the event of a future “public health emergency”
Declare climate change a public health emergency, or maybe a “potential public health emergency”
Activate emergency measures – like climate lockdowns – until climate change is “fixed”
See the end game here? It’s just that simple.
Oh, and we won’t be able to complain, because “climate denial” is going to be illegal. At least, if prominent climate activists like this one get their way.
That’s only a whisper in the background right now, but it will get louder after COP28, just wait.
Until then, like I said, I’m stuck here writing forever.
Dr Keith Berkowitz is a founding member, with Dr Pierre Kory, of the Front Line Covid-19 Critical Care Alliance (FLCCC). He is treating a lot of vaccine-injured patients at his practice in midtown Manhattan. Dr Berkowitz was kind enough to answer a few questions on the Covid vaccine and the vaccine injured.
***
Who is most at risk for vaccine injury?
One thought is that if someone had Covid first, and then got the vaccine after being sick, the rates of vaccine injury were higher because they already had an antibody response, their immune system was already revved up, and then they got an injection of another antigen. Another group I see is people with autoimmune disease, they seem to be more triggered. I have several cases of people who had dormant autoimmune disease, such as ulcerative colitis and rheumatoid arthritis, and post vaccine it got retriggered. What people forget about vaccines is that they have an immunosuppressive effect. So in that two- to three-week period, the immune system takes a hit, which makes the body vulnerable to other illnesses. The third group I see that are most at risk of vaccine injury are people with high histamine levels.
What are the most common symptoms of vaccine injury?
Mildest is probably loss of taste and smell, mild digestive issues, or a cough. More severe are the autoimmune responses, the neurological symptoms, like brain fog, and tinnitus (which is one of the toughest to treat), myocarditis and pericarditis (inflammation of the heart), cancer, which I would call the most severe.
Is that new cancers, or cancers that have returned?
I’m seeing both.
Which autoimmune diseases are you seeing?
First, autoimmune disease is what I’m seeing most in vaccine injury. Specifically thyroid disease, more than anything else. What’s interesting is that I’m seeing normal thyroid function, and positive thyroid antibodies. So typically we wouldn’t check for thyroid antibodies if thyroid function was normal. So that group is often missed for that reason.
Would you say any vaccine was worse than the others?
It seems to be batch-related. That’s the question. There’s a theory that 10 per cent of the batches, roughly, caused 90 per cent of the issues. If you look at the original technology, the mRNA was created at a 70 per cent purity. There’s speculation that, because of manufacturing issues, they weren’t able to create that level of purity, and achieved only 50-55 per cent purity. So does one really know if that level of purity works? Especially being that it was never tested.
Why is there so much denial around vaccine injury?
I think there was a blind trust of the government and the pharmaceutical companies, coupled with a fear aspect of Covid (remember people thought that 50 per cent of hospitalised Covid patients died, when it was more like less than 1 per cent). Fear made people not think any more, and now they’re in denial about the choice they made. Another thing I can’t figure out: If you’re vaccinated, how does an unvaccinated person put you at risk? Also, why did doctors not do their own research? It was blind faith. Medications all have side effects – why was this one different?
How do you respond to the proponents of the vaccine who say, regarding vaccine injury, correlation is not causation?
That’s true, but why are they not even looking into it? If they are so confident, then just study it. What do they have to lose? Why not disprove it? Why is disproving it a major issue for them? If you don’t agree with me, prove me wrong.
Traditionally, vaccines take 10-15 years to get approval, because all that time they are studying long-term effects. The Covid vaccine, which was administered as soon as it was created, is still only about three years old. Therefore, have we yet to see the potential damage it can cause?
Absolutely. Do you know what percentage of drugs approved by the US Food and Drug Administration are withdrawn within five years? 31 per cent. One out of three drugs are taken off the market within five years. That’s incredibly high. That tells me we’re not checking properly. Now with this vaccine, one of my biggest questions is why did we decide to use new technology? Is a pandemic the right time to test new technology? I would argue probably not. And why did some countries around the world, like China and Russia, not use this technology? And at the end of the day we have to ask, was the treatment worse than the problem? And should medical products be tied to financial incentives? That creates a huge conflict. There were incentives to use the vaccine. If a drug or a treatment was really that good, would you need to push it like that?
Any final comments?
This is going to take years to figure out. It isn’t going away any time soon. I feel bad for the people who took something which they thought they were doing for the right reason, and now they are suffering. And they’re not being helped. Why does the government create a long Covid initiative, but not a vaccine-injured initiative? Why are we ignoring these patients? And why are we [in the US] approving a product for over six-month-olds when other countries are saying over 65 years? Another thing that doesn’t make sense is a study on teenagers showed that we have to vaccinate a million young men to prevent one hospitalisation. And the potential in a million doses is 1,000 with side effects. So the hospital to side effect rate is one to a thousand. It doesn’t make any sense! My worry is the trust in the medical system may never come back. And I’m not sure that it’s not deserved.
Dr. Kulvinder Kaur Gill is a pediatric allergist in Toronto. She condemned COVID rules as irrational, political, harmful, and inconsistent with scientific data. In the eyes of the College of Physicians and Surgeons of Ontario (CPSO), Gill was dangerous.
In 2021, the CPSO issued three “cautions” (formal warnings) against her. In 2022 it began disciplinary proceedings. The College alleged that she was undermining confidence in public health measures. Its senior counsel wrote that her communications were unprofessional and unbalanced. In its persecution of Gill, the CPSO has made the case for its own demise. Self-regulated monopolies do not work. The CPSO and other professional regulators need competition.
Gill’s inquisition was not an isolated case. Like other medical regulators in North America, the CPSO forbade its doctors from publicly contradicting COVID orders and recommendations. Its Discipline Tribunal revoked the licence of Patrick Phillips, one of several Ontario doctors pursued for their COVID dissent.
The Nova Scotia medical college investigated Dr. Chris Milburn for writing an op-ed on the death of personal responsibility in the criminal justice system. The Ontario College of Psychologists ordered Jordan Peterson to undergo re-education on the use of social media for tweeting about politics. The BC College of Nurses seeks to discipline Amy Hamm for believing in the biology of two sexes.
The Law Society of Ontario compelled its members to state their concurrence with the ideology of “equity, diversity, and inclusion” until a group of rebel lawyers (of whom I was one) managed to repeal it, although the agenda remains. In British Columbia and Alberta, law societies are instituting politically laden “cultural competency” requirements. Teachers, occupational therapists, engineers, and accountants cannot safely voice doubts about transgenderism or “anti-racist” agendas.
This regulatory bullying is occurring within self-regulated professions. Like “ordinary” regulation, self-regulation is coercive. The state delegates authority to their governing bodies. Some doctors rule over other doctors. A licence from the CPSO is voluntary only in the sense that a driver’s licence is voluntary. You don’t get fines or prison time if you don’t get one, but then you can’t drive or practice medicine. Gill’s livelihood was on the line.
Civil servants do not run self-governing professional bodies, but they are part of the executive branch of government nonetheless. Legislation creates them and they are subject to the constitution. Self-regulation exists only for as long as the legislature says that it does.
Legislatures delegate authority, the theory goes, because professionals have the expertise to ensure competence and ethical practice in the public interest. Your surgeon should know how to cut. Your corporate lawyer should be able to draft articles of incorporation and not skim funds off your trust account. But focusing on technical competence and honest conduct no longer satisfies professional regulatory bodies.
We live in a managerial age. As C.S. Lewis wrote:
“The greatest evil is not now done in those sordid ‘dens of crime’ that Dickens loved to paint. It is not done even in concentration camps and labour camps. In those we see its final result. But it is conceived and ordered (moved, seconded, carried, and minuted) in clean, carpeted, warmed, and well-lighted offices, by quiet men with white collars and cut fingernails and smooth-shaven cheeks who do not need to raise their voices.”
Professions have become managerial cartels. Governing bodies are their godfathers, permitting only proper people and perspectives. Their purpose is not to ensure public access to a variety of professional opinions. Instead, they seek to herd people into “correct” attitudes and behaviors. Propaganda is not evil, but merely a tool to facilitate right results.
Ironically, managerial cartels turn out to be terrible managers. They excel at exercising control but not at producing good outcomes. During COVID, even propaganda was patently incoherent. Yet Gill was one of a scant few doctors and scientists to decry the public health debacle unfolding in front of them. As her lawyer Lisa Bildy wrote in response to the College’s accusations, Gill provided the public with substantiated facts on lockdowns, masking, and COVID vaccines, relying on credible and respected scientific sources and opinions.
The College had scheduled a two-week disciplinary hearing for early 2024. But in September 2023, it abruptly cancelled the hearing with no explanation. Gill’s disciplinary ordeal had come to an end, although her formal warnings remain. Bildy will challenge their validity by judicial review in spring 2024.
Self-regulation protects professions from government interference. That is ironic, given the CPSO’s insistence that their members toe the government line. But self-regulation does not protect individual professionals from the oppression of their peers. A different model beckons: multiple, private regulators competing for members, credibility, and public trust.
Professional cartels benefit the bullies who run them. There’s no reason to grant them the power of monopoly.
Bruce Pardy is executive director of Rights Probe and professor of law at Queen’s University.
Dr. Malik writes:
My name is Ahmad Malik and I am an honest surgeon passionate about free speech and medical ethics.
I have been suspended without pay and cancelled because I dare to challenge the Government narrative, defend informed consent, oppose mandates and lockdowns, question experimental jabs and insist that there are only two biological sexes.
I am raising funds to take legal action against the hospital to lift my suspension and stop the attempts by organisations to censor me.
It will set a precedent that organisations cannot bully, harass and censor those that speak up for medical ethics, and encourage others to speak out.
I am up against large organisations and my case is complex. Legal costs will easily run into the thousands. I need a decent fighting fund which will give me the best chance of being successful.
Recently, our golden retriever, Bailey, got kennel cough. She hasn’t been in a kennel in years, but that’s what they called it: kennel cough.
Please forgive my ignorance in the matter. You see, I’m just a people-doctor. I’m not a veterinarian like, say, Pfizer CEO Albert Bourla. I can’t claim to be an expert on kennel cough.
But as far as I can tell, “kennel cough” appears to be vet-speak for a nonspecific respiratory tract infection in dogs. It seems to be a term veterinarians use much as I would “bronchitis.”
Do you know what a golden retriever with kennel cough sounds like? After all, people-doctors have historically described kids diagnosed with croup as having a “barking” cough.
Well, based on my limited experience, a golden retriever with kennel cough sounds like a Canada goose. Bailey was repeatedly emitting a medium-pitched grunt/honk, lower in register than a duck’s quack but higher than one of those old-fashioned ah-oo-ga automobile horns.
It’s kind of a Honk! Honk! Honk! with the H’s partially dropped. It’s actually quite alarming. Trust me, you don’t want to hear your golden retriever sounding like something it retrieved.
Now, Bailey is a good girl, and I love her dearly. But my wife loves that dog more than life itself. Sometimes I wonder if she’d donate her own liver if it were necessary to save her.
So my wife calls Bailey’s veterinarian, and she tells them about her symptoms.
I should mention that my wife is a doctor, too. Just a people-doctor like me, mind you, not an expert on kennel cough like Albert Bourla. But a medical case presentation is a medical case presentation, and she knows how to present a case.
So what did Bailey’s Primary Care Provider tell my wife after hearing the medical history from a fellow medical professional? Well, they told her that it sounds like kennel cough, and that they can see Bailey in 2 or 3 weeks.
Incidentally, this veterinary practice – I am not making this up – had recently been bought out by some kind of veterinary investment firm which, over the past couple of years, also bought multiple other practices in the area, including the only veterinary emergency room in town. Soon after those acquisitions, they closed down the emergency room.
My wife says to them, “2 or 3 weeks? Bailey will either be fully recovered or dead by then.”
“Well, we’ve been chronically short-staffed,” they replied. “We’re blocked up for urgent appointments…etc., etc.”
A brief, polite back-and-forth ensued, but ultimately Bailey’s “provider” didn’t offer an urgent appointment.
In their defense, this veterinary group knows what really is important. A couple of months earlier, at Bailey’s routine checkup, her doctor noted concerning “plaque buildup” on her teeth.
Do you know what Bailey’s doctor recommended? Doggie dental cleaning. Under general anesthesia. Seven hundred dollars, cash on the barrelhead.
They also have never delayed care when it comes to Bailey’s vaccines.
You see, according to the American Animal Hospital Association Guidelines (generously supported by Boehringer Ingelheim Animal Health, Elanco Animal Health, Merck Animal Health and Zoetis Petcare), all dogs should be vaccinated for:
Distemper
Adenovirus
Parvovirus
Parainfluenza
Rabies
while many or most dogs, depending on “lifestyle and risk”, should be vaccinated for
Leptospirosis
Lyme disease
Bordetella
Canine influenza
and some should even be inoculated with Rattlesnake Toxoid.
I will add, these vaccines are not one-and-done shots. Most of them are recommended to be boosted annually, or at minimum every 3 years.
But again, the experts know what is really important. For example, while Bailey has fortunately avoided any major orthopedic problems to date, we know at least one golden retriever who has had both ACLs reconstructed, and other dogs who have had total hip replacements. Advanced orthopedic surgeries, while admittedly costly, are an essential component of the golden retriever’s healthcare armamentarium.
(This probably sounds selfish, but I just hope and pray Bailey doesn’t develop gender dysphoria. I don’t think we can afford to take her down to Cornell to have them surgically construct a neophallus for her.)
Whew. Let’s step back and review. As I said, I’m no expert on these matters, like Albert Bourla. I want to make sure I’ve got all this correct.
Our golden retriever must navigate a healthcare system that cares so much for her health and well-being that it’s willing to intubate and anesthetize her for a tooth cleaning. Cha-ching!
In the name of vaccination, it will repeatedly inject her with numerous inoculations, up to and potentially including rattlesnake toxoid. Cha-ching!
It offers any number of extensive and expensive Orthopedic surgeries – as long as Bailey’s owner pays. Cha-ching!
And yet, when she gets sick with an acute respiratory infection, it tells her to stay home and wait, offers no treatment, and refuses to see her. Even though, should she become severely ill, her emergency health care system has been decimated by corporate profiteers.
Do I paint an accurate picture, or do I exaggerate?
Fortunately, Bailey’s story has a happy ending.
As so many other concerned patients and family members do, we consulted Dr. Internet. I know, I know, patients are supposed to trust the experts, and refrain from doing their own research – but you’ll have to forgive us. After all, it’s the family dog we’re talking about here. And we did discover some interesting information.
According to our research, the most common first-line treatment for kennel cough is doxycycline, an inexpensive, generic, people-antibiotic that’s been around since the 1960’s. The primary purpose of prescribing it here is to treat against Bordetella, the most common bacterial cause of the disease.
Incidentally, Bailey is up to date on all her recommended vaccines, so the fact that she got kennel cough in the first place raises its own set of questions. I won’t head down that rabbit hole here, except to ask:
If a disease doesn’t merit the patient being seen, assessed, and treated when they contract it, why is obsessive vaccination against it so necessary?
My wife called back, and in her very polite but insistent way, explained that if they weren’t going to see Bailey, we were ‘requesting’ a prescription, which in the end they wrote. I half expected them to say, “Doxycycline, but that’s human paste!” To their credit, they didn’t.
You’ll be glad to hear that after commencing empirical, early treatment with a cheap, decades-old, repurposed drug, Bailey improved almost immediately. Whether this was due to the doxycycline, her own immune system (God gave her one too, we must not forget), or both, we cannot be certain. Anyway, the goose honk is gone, her appetite is back, and she’s got the frequent zoomies again.
But the whole episode left me with a lingering, uneasy, even unhealthy feeling. It’s not exactly déjà vu, but rather the sensation that I’d been through something very similar – and similarly unpleasant – before.
Whatever could that be?
C.J. Baker, M.D. is an internal medicine physician with a quarter century in clinical practice. He has held numerous academic medical appointments, and his work has appeared in many journals, including the Journal of the American Medical Association and the New England Journal of Medicine. From 2012 to 2018 he was Clinical Associate Professor of Medical Humanities and Bioethics at the University of Rochester.
Pfizer-BioNTech delayed reporting vaccine-associated deaths among BNT162b2 clinical trial participants until after the U.S. Food and Drug Administration (FDA) issued an Emergency Use Authorization (EUA) for the product.
The vaccine makers also failed to account for a large number of subjects who dropped out of the trial.
The authors of the paper described it as a “forensic analysis,” defined by the U.S. National Institute for Standards and Technology as “the use of scientific methods or expertise to investigate crimes or examine evidence that might be presented in a court of law.”
What the analysis shows
Corinne Michels, Ph.D., retired distinguished professor of biology at Queens College, New York, led the DailyClout Pfizer/BioNTech Documents Investigations Team on what the authors claim was the first independent examination of original data from the Pfizer-BioNTech COVID-19 mRNA vaccine (BNT162b2) clinical trial.
Investigators looked at each of the 38 deaths occurring between July 27, 2020, the start of phase 2/3 of the Pfizer-BioNTech vaccine trial, and March 13, 2020, the end date culminating in Pfizer-BioNTech’s 6-month interim report.
This trial phase involved 44,060 subjects. Half received a dose of BNT162b2, half got a placebo consisting of an inactive sterile salt solution.
The trial was unusual because at week 20 after the FDA issued the EUA for the vaccine, trial subjects in the placebo group were allowed to switch to the vaccinated group and receive their first BNT162b2 shot.
Switching from the placebo to the vaccinated group — or “unblinding” — normally occurs when the benefit of the drug is so great that not treating subjects becomes unethical. For example, investigators might consider unblinding a cancer trial if at some point all untreated patients deteriorated or died but all treated patients improved.
Unblinding conditions may be specified in the study design, but they usually involve input or review from medical ethicists.
Of 20,794 unblinded placebo subjects in the Pfizer trial, 19,685 received at least one dose of BNT162b2.
Normally the decision to unblind a vaccine trial would be based on the product’s safety and effectiveness in reaching certain endpoints or objectives. Endpoints for a drug to prevent viral infections might be a positive test or self-reported COVID-19 illness (the “case” numbers that drove much of COVID-19 policy), illness requiring hospitalization or death.
But, perhaps unexpectedly, after 33 weeks the data revealed no significant difference between deaths in the vaccinated and placebo groups for the initial 20-week placebo-controlled portion of the trial.
After week 20, after most former placebo subjects had received the vaccine, deaths among those in the vaccine group continued unabated.
The authors revealed “inconsistencies” between data presented in Pfizer-BioNTech’s 6-month interim report and subsequent publications by Pfizer-BioNTech trial site administrators:
“Most importantly, we found evidence of an over 3.7-fold increase in the number of deaths due to cardiac events in the BNT162b2 vaccinated individuals compared to those who received only the placebo.”
This means that 79% of relevant deaths were not recorded in time to be included in Pfizer’s regulatory paperwork.
By not including relevant subject deaths in the case report, Pfizer obscured cardiac adverse event signals, allowing the EUA to proceed unchallenged.
How did Pfizer get around legal, ethical obligations?
The Pfizer-BioNTech data, obtained through a Freedom of Information Act lawsuit, uncovered four additional deaths in the vaccine group and one more in the placebo group — but Pfizer failed to include these data in their FDA submission despite an explicit study design requirement to do so.
These data, and how they differ from what Pfizer-BioNTech reported in their applications, are summarized in Table 3 of Michels’ study.
One case involved a 63-year-old woman who died 41 days after receiving the shot, but whose death only entered the data pool 37 days later. Another was a 58-year-old woman whose death 72 days after vaccination went unreported for 26 days.
Had Pfizer-BioNTech met their legal and ethical obligation to report all serious adverse events their data would have shown equal deaths in placebo and vaccine groups — which would have shown no clear benefit for the vaccine.
How were they able to skirt those obligations?
For one, they were able to hide behind the the 2005 Public Readiness and Emergency Preparedness (PREP) Act, which provided an almost impenetrable liability shield for vaccine manufacturers for “medical countermeasures” in response to any “public health emergency.”
Second, because COVID-19 was viewed as a national health emergency, regulators abandoned the established, patient-centered, safety-based approval process requiring years of preclinical animal testing — and Pfizer-BioNTech unsurprisingly went along.
Timing of death reports raises questions
Michels also raised issues regarding total death reports and their timing.
Since the death total from both study groups, 38, appeared “surprisingly low” to study authors — particularly during a pandemic — they undertook their own analysis based on population mortality expectations at the time.
Assuming that age-adjusted death rates for the study subjects were similar to those of the general population, they estimated that 222 subjects should have died from July 27, 2020, to March 13, 2021. The reported number, 38, is just 18% of the expected number.
Michels explained this by the large number, 4.2% of “discontinued subjects.” The most concerning of these were subjects “lost to follow-up,” which means missing scheduled visits or other required activities.
Pfizer-BioNTech tried to reach these subjects via phone, certified mail or through their emergency contact but despite their efforts could not account for 395 subjects who had dropped out.
The authors wrote:
“These are not insignificant numbers and could easily account for the low number of deaths reported in this safety period of the trial. Given the importance of knowing the status of each trial subject, there should have been greater effort to locate these individuals.
“Additionally, Pfizer/BioNTech was responsible for oversight of the trial sites. Sites with excessive numbers of lost to follow-up should have been evaluated for performance.”
Michels was also concerned over how certain trial centers had many dropped-out subjects while others had none or just a few.
Ninety-six of 153 trial sites (63%) reported 0 or 1 subjects lost to follow-up and 34 (22%) reported 2-5 dropouts. But four sites reported more than 20 subjects lost to follow-up, amounting to about 5% of all trial subjects.
Since the vaccine makers were responsible for trial site oversight, the authors wrote, “Sites with excessive numbers of lost to follow-up should have been evaluated for performance.”
Finally, based on the data, it appears Pfizer-BioNTech was in no hurry to enter death reports before the EUA submission deadline, particularly for the BNT162b2 group.
Of the 38 reported deaths only one case was added on the day the subject died. Delays of 20+ and 30+ days were common.
One death took 72 days to find its way into the database, and all were entered as occurring on the reporting day, not on the actual date of death.
Of the eight subjects in the vaccine group that should have been reported by Dec. 10, 2020, the EUA application cutoff, the average reporting delay was 17.5 days for subjects in the vaccine group, but just 5.9 days for deaths among subjects in the placebo group.
Angelo DePalma, Ph.D., is a science reporter/editor for The Defender.
In 2011, the United States experienced more than 500 deaths and over $30 billion in losses from tornadoes. As is now common, climate activists were quick to claim that the destructive tornadoes that year were due to climate change. The National Oceanic and Atmospheric Administration (NOAA) rejected such claims, advising:
[A]pplying a scientific process is essential if one is to overcome the lack of rigor inherent in attribution claims that are all too often based on mere coincidental associations.
The 2011 tornado season motivated us — Kevin Simmons, Daniel Sutter and I — to take a close look at trends in tornadoes and their impacts across the United States. The result was a peer-reviewed paper with the first comprehensive normalization of U.S. tornado losses, for 1950 to 2011.
Our results surprised even us — U.S. tornado damage and tornado incidence appeared to have decreased dramatically, contrary to conventional wisdom:
The analysis presented in this paper indicates that normalized tornado damage in the US from 1950 to 2011 declined in all three normalization methods applied (two are statistically significant one is not). The degree to which this decrease is the result of an actual decrease in the incidence of strong tornadoes is difficult to assess due to inconsistencies in reporting practices over time. However, an examination of trends within sub-periods of the dataset is suggestive that some part of the long-term decrease in losses may have a component related to actual changes in tornado behaviour. Further research is clearly needed to assess this suggestion.
You can see that we were exceedingly cautious in how we framed the possibility that things were not actually getting worse. even so, our work was ignored by the Fourth U.S. National Climate Assessment, which instead claimed the opposite, contrary to the evidence and peer-reviewed research:
[T]here is reason to expect increased tornado frequency and intensity in a warming climate
[B]oth the severity of damage from individual events and the total annual losses from tornadoes are seen to have reduced over time.
Their analysis confirms our earlier work:
[O]ur findings reiterate the results of Simmons et al. (2013) who emphasize the importance of normalizing loss data to draw adequate conclusions about the severity of natural hazards
You can see the results of their normalization for 1954 to 2018 in the figure below.
Normalized U.S. annual tornado losses, 1954-2018. Source: Zhang et al. 2023
Compare their results with ours in the figure below, which I have just updated through 2022.
Normalized U.S. annual tornado losses, 1950-2022. Source: Updated from Simmons et al. 2013.
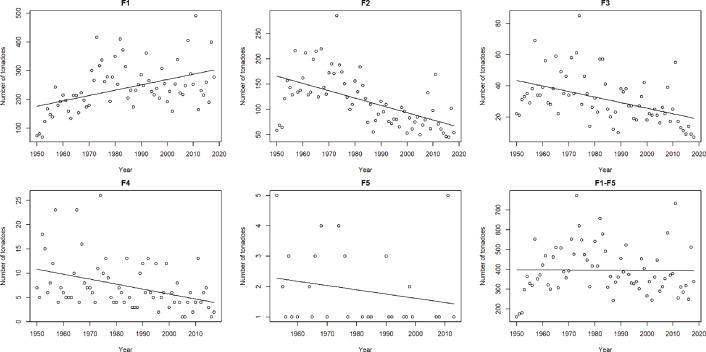
Zhang et al. also find that the strongest tornadoes have also declined appreciably since 1950. The figure below shows their presentation of trends in tornadoes of various intensities (with F1 the weakest and F5 the strongest). You can see that the incidence of tornadoes of F2 strength and stronger have decreased. In our 2013 analysis we found that ~90% of damage results from tornadoes of F2 strength or stronger.
In the 11 full years following our analysis, 9 of 11 have seen overall below average tornado incidence in the United States — 2023 will wind up slightly above average. There is simply no evidence to support claims that tornadoes are getting worse or causing more damage. In fact, the evidence indicates the opposite and peer-reviewed research is strongly in agreement.
Why has the downward trend occurred? Might climate change play a role? You rarely see such questions asked or explored in the scientific literature.
Misinformation on extreme weather and disasters sits out in plain sight, and is easily refuted — yet there seems to be exceedingly strong social norms and political pressures to simply not call things straight. It is really remarkable.
I am confident that good science will win out in the end. It just might take a while. Meantime, here at THB, I’ll keep sharing the science behind the curtain.
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.