Eight items of major concern regarding the proposed WHO treaty and IHR amendments
By Meryl Nass, MD | November 13, 2023
1. Biological warfare agent proliferation.
The treaty and the proposed amendments instruct nations that they must perform surveillance for potential pandemic pathogens, build or maintain sequencing labs, and both share actual specimens with the WHO (where a BioHub has been created for this purpose) and also share the sequences online. This demands the proliferation of biological weapons agents — which I believe is a crime (based on my interpretation of Security Council Resolution 1540 and the 1972 Biological Weapons Convention).
1 a. The June 2, 2023 “Bureau text” version of the treaty also called for nations performing Gain-of-Function research to reduce “administrative impediments” to the work. In other words, restrictions on the research should be relaxed, which would make lab leaks more likely to occur. This paragraph was removed from the October 30, 2023 version of the treaty.
2. Giving the WHO a blank check to create new rules in the future
The treaty calls for a Conference of Parties and a new WHO Secretariat to be created in the future that will make rules for how the pandemic prevention and response apparatus will work—which provides essentially a blank, signed contract to the WHO to create whatever rules it wants.
3. Liability-free vaccines developed at warp speed will be produced
The treaty calls for rapid vaccine development /production and shaving time off all aspects of vaccine development, testing and manufacture. This requires vaccines to be used without licenses, and the treaty calls for nations to have laws in place to issue Emergency Use Authorizations for this purpose, and to “manage” liability issues. See “The WHO’s Proposed Treaty will Increase Man-Made Pandemics” for more information about this. The US, EU and others have specifically called for 100-day vaccine development and an additional 30 days for production of pandemic vaccines. This would allow for no meaningful human testing.
4. Human rights guarantees have been removed in the new amendments
The amendments removed “human rights, dignity and freedom of persons” from the existing IHR language. Following complaints, this phrase was later inserted into the Treaty–but the treaty may not be accepted in 2024. Meanwhile, the amendments require only a simple majority to pass, are being written in secret, and so it is likely that the most problematic issues will be found in the amendments.
5. Social media surveillance and censorship of citizens is required
Both the amendments and the treaty call for nation states to perform surveillance of their citizens’ social media, and to censor and prevent the spread of information that does not conform to the WHO’s public health narratives. Yet the treaty also calls for citizens to be free to access information, while they are to be protected from “infodemics,” which are defined as too much information. Citizens must also be stopped from spreading mis- and disinformation.
6. We may not learn what is in the amendments until after they are passed
The amendments have been negotiated entirely in secret for the past nine months, while there have been multiple consecutive drafts of the pandemic treaty released to the public during that time. And while the negotiated amendments were to be tabled for public review in January, the WHO’s principal legal officer has provided a legal fig leaf to avoid the obligation of making them public 4 months ahead of the vote. Will the public even see the amendments before a vote on them occurs?
Why is there such secrecy regarding the proposed amendments?
7. The WHO Director-General could become your personal physician
According to the proposed amendments, the WHO D-G would be able to commandeer and move medical supplies from one country to another, decide what treatments can be used, and restrict the use of other treatments.
8. When will the WHO be able to use its newly minted powers?
The amendments will come into force after a declaration of a Public Health Emergency of International Concern (PHEIC) is made. However, a declaration of a potential PHEIC will also trigger these powers. The powers can be extended even after a PHEIC is over, as we have seen with COVID and monkeypox (MPOX) declarations by the D-G.
The treaty will be in force continuously, requiring no declaration or pandemic to confer new powers to the WHO.
See detailed report:
What does the WHO say about its power to enforce the Pandemic Treaty (and International Health Regulations)?
By MERYL NASS | NOVEMBER 12, 2023
Many people have insisted that the WHO could not make the US do anything. Let me remind those people that the US government under Biden is instrumental in pushing forward the WHO proposals, and so it will comply. Here is what the WHO says:

What is meant by a ‘convention, agreement or other international instrument’?
Conventions, framework agreements and treaties are all examples of international instruments, which are legal agreements made between countries that are binding.
Why did WHO’s Member States decide to create an accord for pandemic preparedness and response?
In light of the impact of the COVID-19 pandemic, WHO’s 194 Member States established a process to draft and negotiate a new convention, agreement, or other international instrument (referred to in the rest of this FAQ, generally, as an “accord”) on pandemic preparedness and response. This was driven by the need to ensure communities, governments, and all sectors of society – within countries and globally – are better prepared and protected, in order to prevent and respond to future pandemics. The great loss of human life, disruption to households and societies at large, and impact on development are among the factors cited by governments to support the need for lasting action to prevent a repeat of such crises.
[Ho ho ho—Nass]
At the heart of the proposed accord is the need to ensure equity in both access to the tools needed to prevent pandemics (including technologies like vaccines, personal protective equipment, information and expertise) and access to health care for all people.
[If this were true, why do the treaty and amendments only discuss health “coverage” which means health insurance, rather than health care? The WHO knows the difference, but only demands “coverage”—a sop to the insurance industry.
Furthermore, the WHO demands censorship of information not in agreement with the WHO’s narratives, not free sharing of information—so much for information equity—and its so-called expertise was used to overdose hospitalized patients with HCQ without informed consent, when these unfortunates were enrolled in the WHO’s “SOLIDARITY” trial. Its expertise led to demanding that nations stop the use of HCQ and ivermectin for COVID and administer more shots. Who needs this expertise? —Nass]
Who else is involved in the process for the accord?
Besides WHO Member States, the process for developing a possible new accord is providing extensive opportunities for engagement with relevant stakeholders, including other United Nations system bodies, and a wide range of other non-State actors in official relations with the WHO, to ensure robust and inclusive participation in the proceedings of the Intergovernmental Negotiating Body. Furthermore, WHO is seeking complementary inputs through public hearings with stakeholders including: international organizations; civil society; the private sector; philanthropic organizations; scientific, medical, public policy and academic institutions and other entities with relevant knowledge, experience and/or expertise.
[In other words, Bill Gates, who was the largest funder of the WHO the year Trump defunded the organization, gets the lion’s share of input, while we peons get none. Trump then turned around and funded Gate’s’ charity GAVI with the money, and GAVI turned around and gave it back to the WHO. That was our money, by the way.—Nass]
—There is more of this nonsense on this webpage, but you can go look it up yourself if you have the stomach for it.—Meryl
CPSO Pronounces Judgment Over Dr Trozzi
But the shots are still toxic, Pfizer committed fraud, everyone has been assaulted, and we must act now to save lives.
Dr Mark Trozzi | November 6, 2023
Health Canada recognizes that Pfizer committed fraud. The shots turn out to be even worse than I thought. They contain large quantities of DNA, and multiple genetic sequences including a very dangerous SV40 promoter sequence which promotes permanent genetic modification, disease, and cancer. Sadly, innocent people are uninformed and lining up for injections that they would never agree to if they knew what was in them and what it can do to them.
Here is my ten minute video to update you, with a focus on current priorities and strategies. Crisis is a combination of danger and opportunity. The SV40 revelation marks severe danger, but it is also an opportunity to finally set things right. This video includes genuinely kind and honest advice for the CPSO administrators and staff; and a small request for you to please share your judgement of me as a doctor with the CPSO.
Please Share Your Judgment of Dr Trozzi with the CPSO here:
- CPSO Compliment a physician https://www.cpso.on.ca/en/Public/Public-Information/Compliment-a-physician
- or by email direct to feedback@cpso.on.ca

CPSO v. Trozzi – Case Update – November 1, 2023
COLLEGE DENIES DR. TROZZI’S RIGHT TO FREEDOM OF EXPRESSION
We are the Administrative State and You are Not
The Ontario Physicians and Surgeons Discipline Tribunal has ruled that Dr. Mark Trozzi is guilty of professional misconduct and dishonourable conduct and is incompetent in the practice of medicine for questioning the government’s Covid-19 narrative. He was also found guilty of professional misconduct and was deemed incompetent for writing medical exemptions for Covid-19 injections in support of a patient’s right to refuse coerced medical treatment under Ontario’s Health Care Consent Act and section 7 of the Canadian Charter of Rights and Freedoms.
In 2021, the College of Physicians and Surgeons of Ontario established three Covid-19 restrictions through website statements — doctors were forbidden from: (i) making any statements that discourage anyone from following Covid-19 public policies and recommendations; (ii) prescribing alternative Health Canada approved medications for the treatment of Covid-19; and (iii) writing medical exemptions for Covid-19 injections, unless a patient had suffered a severe allergic reaction or developed myocarditis after a first shot. Based on the restrictions relating to freedom of expression and medical exemptions, the College issued investigation orders against Dr. Trozzi in 2021.
This eventually led to a five-day hearing in July of 2023 during which the College Tribunal focused its prosecution on Dr. Trozzi’s daily newsletter at drtrozzi.org, where he had supposedly caused harm by spreading “misinformation” about Covid-19 science. The College was particularly concerned with Dr. Trozzi’s view that neither Big Pharma nor Health Canada had done the due diligence required to prove the Covid-19 injections were safe and effective. The Tribunal concluded that his views were inflammatory, unprofessional and worthy of censure. On November 10th, the Tribunal will hold a penalty hearing to determine whether to revoke the licence of the 25-year ER veteran and former university professor.
Trozzi’s lawyer, Michael Alexander, commented: “The Tribunal wrote up the prosecution’s position on almost every issue. The one saving grace was the College’s acknowledgement that the right to free expression includes the right to make statements that may be wrong or mistaken. However, that position is difficult to reconcile with the Tribunal’s view that Dr. Trozzi can be punished for spreading misinformation.“
He added: “The Tribunal did not address our argument that the College lacked the authority to investigate and prosecute Dr. Trozzi since its Covid-19 restrictions were merely recommendations rather than binding rules or regulations, even though we cited the Ontario Divisional Court and the Ontario Court of Appeal in support of our position.”
Further, he stated: “The Tribunal totally ignored our cross-examination of the College’s expert witnesses, which makes the entire decision a complete travesty. On cross, the College’s main expert witness on Covid science, Dr. Andrew Gardam, admitted that he had never responded to the 41-page expert report provided by Dr. Trozzi in which he rebutted Gardam’s own 8-page expert report with 29 scientific citations. As a result, in closing submissions, we argued that Dr. Trozzi was unrefuted on Covid science; yet, the Tribunal made no mention of this fact.”
Finally, he added: “The Tribunal also paid no attention to the fact that the Supreme Court recognized an expansive right to freedom of expression as an inherent feature of parliamentary government as early as 1939, which gives the right a higher status than it enjoys under the Charter. In matters of law, we will appeal the decision to the Divisional Court on the standard of correctness.”
For media inquiries, please contact Michael Alexander by cell at 416-318-4512 and by e-mail at malexanderjd@protonmail.com.
Please support the fight to restore ethical medicine and the rule of law in Ontario and Canada.
Please sign this petition to defend my license to practice medicine in Ontario and ultimately restore Canadians’ access to many honest doctors who have been persecuted for resisting the unethical and unscientific covid agenda.
Reports about Dr Trozzi and the CPSO from others:
- Life site News: Dr. Mark Trozzi may lose medical license for defying COVID narrative
- Epoch Times Tribunal Finds Ontario Doctor Critical of COVID Measures Committed Professional Misconduct
- Derek Sloan Funding the Fight: Dr. Trozzi Latest Update – May Lose Licence Next Week
- Denis Rancourt, “In Canada, Dr Mark Trozzi has opposed the toxic death-causing vaccine in every way he can, so the CPSO @cpso has decided that he is incompetent! ( And “disgraceful, dishonourable or unprofessional”)”
Here’s a history to be proud of, and “accused” of:
- To follow Dr Trozzi’s public covid truth mission beginning January 2021 and right up until the present start here
- Or to begin with the most recent and work your way back start here
DNA Contamination/ SV40 promoter sequence/ Pfizer’s Fraud/ Health Canada
- Dr Trozzi Alert | There’s DNA in the RNA Shots. Lots! April 2023
- World Council For Health Urgent Panel of Global Experts Confirm Dangerous Criminal Undeclared DNA In Pfizer And Moderna Covid-19 “Vaccines”
- Epoch Times regarding plasmid DNA contamination and Health Canada
Cancer:
Canadian doctor sounds alarm over ‘turbo cancers’ in young people due to COVID jabs. ‘I’ve never seen anything like this,’ said Dr. William Makis regarding ‘stage four’ cancers presenting in young people and uncharacteristically aggressive leukemias.
“Game Changer for Vitamin D” – Supplementation Found To Improve Cancer Survival

BOSTON UNIVERSITY SCHOOL OF MEDICINE | OCTOBER 30, 2023
For more than 100 years, it has been believed that sunlight and vitamin D deficiency were associated with the risk for many deadly cancers including colorectal, prostate, and breast. Despite this, some scientists have remained doubtful about whether this nutrient indeed has any benefit in reducing cancer risk, morbidity, and mortality. This skepticism is bolstered by several randomized controlled trials casting doubt on the nutrient’s effectiveness.
Commentary on Vitamin D’s Effect on Cancer
However, in a new commentary published in the journal JAMA Network Open, Michael F. Holick, Ph.D., MD, professor of medicine, pharmacology, physiology & biophysics, and molecular medicine at Boston University Chobanian & Avedisian School of Medicine, explores the controversy as to whether improving vitamin D status has any benefit for reducing the risk of developing cancer as well as improving relapse-free and mortality outcomes.
He believes the results of the Kanno et al. study support the significant body of associated evidence and clinical studies concluding that improvement in vitamin D status through vitamin D supplementation can be an effective strategy for improving survival outcomes of cancers, especially of the digestive tract including colorectal cancer.
Factors Influencing Vitamin D’s Effect on Cancer
“We now recognize that there are a variety of variables that can influence how vitamin D prevents and responds to cancer. For example, being at a normal weight and taking vitamin D improves your ability to survive cancer. Other factors include the patient’s genetic makeup and how the patient utilizes and breaks down vitamin D,” explains Holick, corresponding author of the piece.
The study by Kanno et. al. provides further insight. The p53 gene produces the p53 protein to prevent cells from becoming malignant. Cancer cleverly mutates this gene and the mutated p53 protein helps the cancer to grow and become immune to cancer therapy. Kanno et. al. found that patients whose immune system is on high alert and produces antibodies to control the production and release of this mutated p53 protein were more likely, by more than 2.5 fold, to improve their chances of surviving the cancer if they also took daily 2000 IUs vitamin D3 compared to patients who had the antibodies but did not take vitamin D supplementation. Those patients who did not produce the antibodies received no survival benefit by taking the vitamin D supplement.”
Future Directions in Research
Holick believes it would be worthwhile to conduct a retrospective analysis for serum p53 antibodies and the immunohistochemical presence for p53 in histologic cancer samples of breast, prostate, and other cancer studies that found no benefit when they evaluated the potential impact of vitamin D supplementation on improving cancer survival.
More importantly, Holick believes future studies evaluating vitamin D supplementation for the prevention and improvement of cancer outcomes should now include not only many of the variables mentioned above, but also include a measurement for p53 antibodies in the blood and immunohistochemical presence of p53 in cancer tissue samples.
Dosage and Implications
According to Holick, it is important to recognize that most of the studies that have shown that vitamin D3 supplementation improves cancer survival provided patients with at least 2000 IUs vitamin D3. This amount of vitamin D3 substantially improves the vitamin D status (serum concentration of 25-hydroxyvitamin D) to a concentration above 30 ng/mL. This amount of vitamin D3 was not reported to cause any toxicity
“It is well-documented that in order to achieve a circulating concentration of 25(OH)D above 30 ng/mL requires a vitamin D intake of at least 2000 IUs daily, an amount that cannot be achieved from diet alone but requires vitamin D supplementation. Although vitamin D is the sunshine vitamin you cannot get enough vitamin D from sun exposure unless you expose more than 20% of your body surface to sunlight almost daily like the Maasai and Hazda do in equatorial Africa,” said Holick.
Reference: “The Death D-Fying Vitamin D3 for Digestive Tract Cancers—The p53 Antibody Connection” by Michael F. Holick, 22 August 2023, JAMA Network Open.
DOI: 10.1001/jamanetworkopen.2023.28883
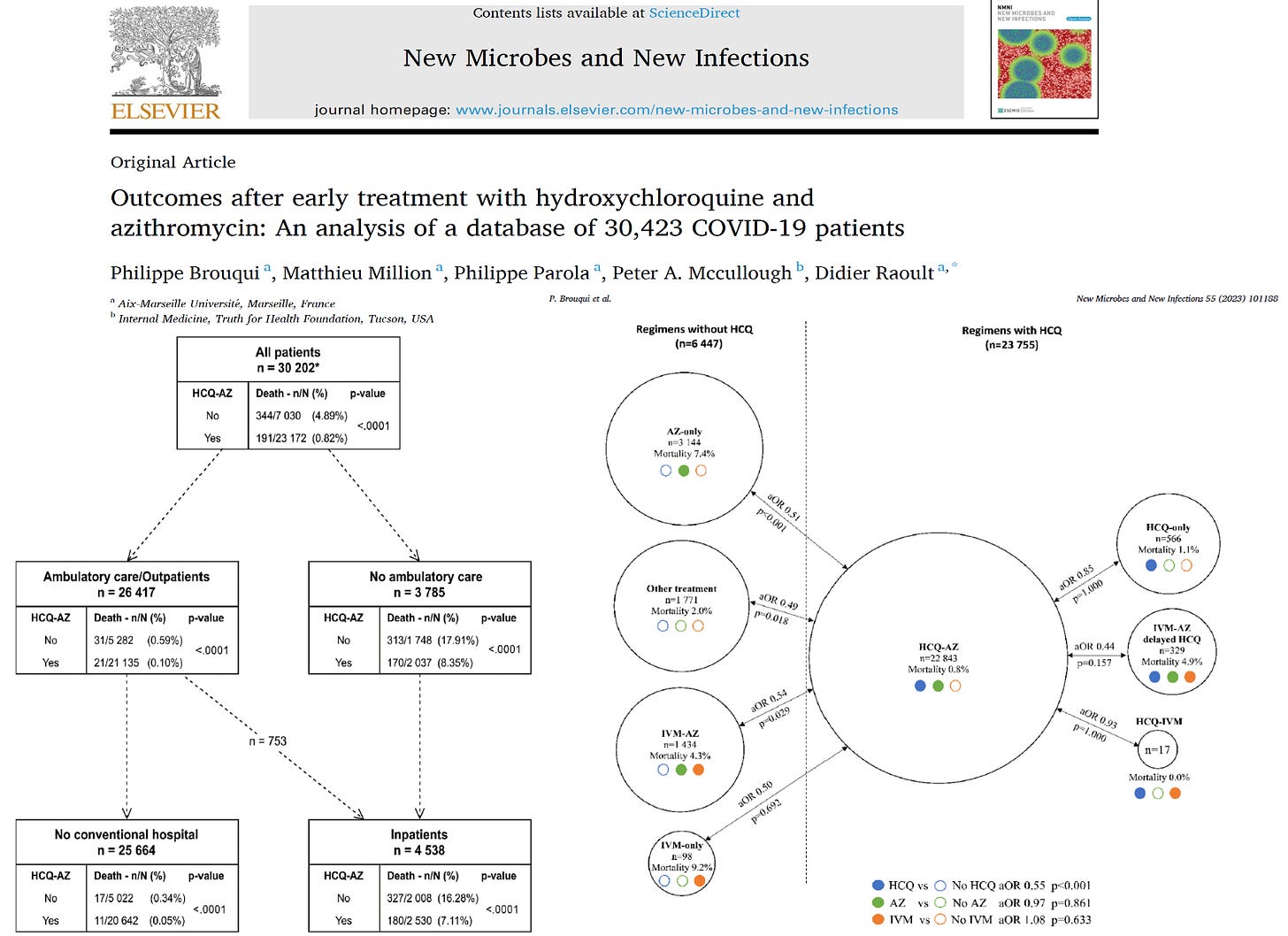
Outcomes after Early Treatment with Hydroxychloroquine and Azithromycin: An Analysis of 30,423 COVID-19 patients
By Peter A. McCullough, MD, MPH | Courageous Discourse | November 6, 2023
We perform prospective, randomized, double-blind, placebo-controlled trials to test drugs, vaccines, devices, and other products for safety and efficacy. Randomization is important since it handles: 1) selection bias, 2) all known and unknown confounders. Despite the hundreds of billions of dollars spent during the pandemic, we did not have an investment in large, multidrug prospective, randomized, placebo controlled trials or comparative studies to test the best drug regimens.
In the end, what patients care about is how they feel, function, and survive. When it came to COVID-19, whether randomized or not, if patients survived if they were in the optimally treated group. The only way to assess how a high-risk population fared in the pandemic is to report on a large sample of patients sick with COVID-19 with a large number of the outcome of of interest—death.
Brouqui et al reported from a French database of 30,423 COVID-19 patients of whom 535 succumbed to the illness. In great detail, the investigators report mortality according to ambulatory treatment received, hospitalization, and the course over the following six weeks.
An explosive discussion with ex-CDC scientist Norman Pieniazek
BY MARTIN NEIL, JONATHAN ENGLER, AND JESSICA HOCKETT | OCTOBER 30, 2023
Dr Norman Pieniazek is a molecular biologist, geneticist, epidemiologist with 147 publications in virology and parasitology. Before he retired, he spent 24 years working at the Center for Disease Control (CDC) in the USA. He has also spent time abroad including time working in Spain and Poland.
We met up with Norman for what was planned to be a short meeting to introduce ourselves and informally discuss common interests around covid. However, this turned into a two-hour long, wide-ranging and fascinating discussion that touched on a huge number of topics.
Early on in the meeting Norman made the wise suggestion that we record and share the discussion. So, he hit the record button on Skype and we started again. The video, accessible below, is approximately two hours long. Be aware that, given it wasn’t planned as an ‘interview’ or for broadcast, it is largely unstructured. However, for those short of time here is a synopsis of the discussion with a focus on what Norman said1:
- The bacterial pneumonia hypothesis suggests that early treatment – hydroxychloroquine, ivermectin and antibiotics address bacterial infection. Norman confirmed bacteria are everywhere in our bodies including in the lungs, creating an ever-present potentially hazardous predisposition that, given the right circumstances, might cause a deadly bacterial pneumonia infection.
- Well-understood remedies such as the stockpile of antibiotics, as recommended by Fauci, were cast aside in 2020. Bacterial infection can cause sepsis hence we need antibiotics. A Cytokine storm is caused by bacterial infection in the lungs, filling them with fluid; this lowers the oxygen level in the blood because of poor lung function.
- In-person diagnosis by a physician based on physical symptoms was largely replaced by the PCR test, and with the rise in tele-health visits, social distancing etc physicians stopped using stethoscopes to listen to a patient’s chest. This is an essential diagnostic tool to enable a doctor to audibly tell whether a patient has crossed the line into a bacterial infection which will then require antibiotics.
- Norman knew Donald Henderson who co-authored a classic work on how to best respond to a flu epidemic. Henderson and colleagues did not recommend any of the NPIs that were followed during covid because of the obvious severe health, social and economic costs. (As an aside this work was co-authored by Prof. Thomas Inglesby at John Hopkins who attended Event 201 and, oddly, recommended NPIs be used for covid – the very same ones he had rejected previously).
- Orthodox immunology was ignored – herd immunity is a fiction given there is a ‘soup’ of constantly mutating coronaviruses.
- Why didn’t scientists at the CDC question things early in 2020? Work from home restrictions meant that people at CDC couldn’t communicate and coordinate to overturn the madness being imposed from the ‘sixth floor’ top brass. You could not isolate CDC from the HHS (Health and Human Services) and it was HHS that were calling the shots.
- The Wuhan scientists were on a routine ‘fishing expedition’ for coronaviruses and unusual pneumonias. Why was this work being done in Wuhan? It is easier to do in China because it is legal and because there are lots of hospitals, in a concentrated area, where the population is in relatively poor health. Also, it is easier to get permission to perform a painful bronchial lavage procedure on patients to obtain pathogens in China; this is much harder to do in the USA. This procedure is done in the lower respiratory tract and guarantees higher quality samples than can be obtained using swabs, which really just measure the quality of the air that has entered your upper respiratory tract.
- To determine what pathogen is causing lower respiratory tract symptoms you should not use swabs and PCR. Why not? CDC acknowledges the inability of swabs to collect causative agents as reported by the EPIC study in these 2015 NEJM articles (one done on adults and one on children). Hence a positive result gained from a sample taken from the upper throat or the nose does not mean an infection is caused by the detected pathogen.


- In 2002-2004 SARS-COV was not subject to mass PCR testing, yet SARS-COV-2 was. PCR was used for SARS-COV but only on samples taken using bronchial lavage, but NOT from swab samples taken from the nose or upper throat.2
- Wu et al discovered WH-Human-1 using samples collected by bronchial lavage, and next generation sequencing of the collected genetic samples, and ultimately reported it in GenBank.
- Before reporting on GenBank they published a preprint identifying the genetic sequences3, which was appropriated and found its way into the hands of Corman and Drosten, who then decided to exploit it for personal gain (via commercial PCR testing), fabricating a story about validating it against SARS-1. It was subsequently renamed SARS-COV-2. (For a proposed timeline of events see here).
- Norman thinks SARS-COV-2 is simply a beta coronavirus (a cold), one of the many thousands of cold viruses that had remained undiscovered until 2020, but which have always been ever present in nature.
- SARS-COV-2 cannot be a novel virus created in a lab or by natural zoonotic mutation. It is simply novel to detection4. As soon as the EUA approved PCR tests started to be used the virus was simultaneously discovered in a number of disparate geographical regions. There was no evidence of sudden spread.
- In effect the results of any test are as much determined by the choice of test to apply as by the presence/absence of viruses. Norman says, “you will find whatever you want to find”. Hence people will be symptomless yet will have a lot of, whatever viruses happen to be around in their nose or throat.
- The established taxonomy of viruses is unusable simply because there are so many unknown viruses circulating in the wild.
- The mRNA vaccine technology ended in a ‘garbage heap’, because it is extremely toxic, and was rendered obsolete by protein subunit vaccines by 2019. So, the mRNA vaccines were doomed from the start. Subunit (protein-based) vaccines have been known since the late 1970s, but Moderna, Pfizer and BioNTech needed a way to realise a return on their vast investments in mRNA. Hence the pandemic.
- Novavax is a protein subunit vaccine, based on the spike protein, which was available in August 2020 but did not get approval from the FDA. Although it is protein based it will stay in the deltoid muscle injection site. It was however approved in Canada. It may not be very good for you (and ineffective against coronaviruses), but it is less dangerous than the mRNA vaccines.
- mRNA vaccines were found to be too dangerous for animals. Also, arguments that they are a safe basis for cancer drugs are based on lies. There is a competing technology called humanised monoclonal antibodies that cured President Carter from a melanoma that had migrated to his brain and there are now 500 versions of these drugs currently available.
- Norman was told that the patent on the flu vaccines, grown in eggs, expired in 2020. Hence there was little ROI in continuing with this technology.
- Viruses are in your respiratory tract and antibodies, responding to vaccines, are in your blood. These two things do not match well because the antibodies in the blood do not get into the lungs. The immune system ‘stays away’ from the complex respiratory system that deals with the thousands of pathogens we breathe in with every breath.
- Are serology studies a pointless exercise? Because of wide variation between individual’s antibody measurement only makes sense by studying change in any single individual over time.
- Testing for antibodies means nothing because antibodies in the blood cannot travel to the lungs to react.
- Testing for antigens is a cheaper and less sensitive version of the PCR test with the same limitation.
- Norman is very sceptical of a number of covid virus theories including those by Walter Chesnut and JJCoey’s infectious clone theory, though they weren’t discussed in any great detail and were probably not characterised fully (or maybe even fairly).
- The issue with ‘infectious clones’ is that ‘you do not know what to create’ because there are millions of sequences of coronavirus so there is no ‘clonality’ and each one has 30 thousand nucleotides and there are combinatorically infinite changes you could potentially need to consider when creating a coronavirus5. It therefore isn’t possible to know what to change, via Gain of Function (GoF), to make the virus behave in more dangerous ways.
- As part of the ‘partnership for peace’ programme in 1994 Norman hired two ex-Soviet bioweapons scientists and asked them ‘how come you worked for 20 years and didn’t create any new deadly viruses?’
- They can create thousands of virus combinations, but the problem is how to test these creations. There is no way to test the billions and billions of possible changes to a virus and identify which changes to the sequence are ‘bad’. You need the phenotype, and you cannot deduce the phenotype from the genotype. So how would GoF researchers – E.g., EcoHealth alliance – know exactly what to create?
- The claim that Saddam Hussian had biological weapons was groundless and this was confirmed to Norman by Donald Henderson who was involved at the time and who said it was not possible.
- Thus, GoF claims that changes to spike protein and furin cleavage sites make a virus more deadly are fiction. It isn’t possible and there is no proof they can produce deadly bioweapons. Those advocating this position and making these claims – EcoHealth alliance (Fauci, Baric and Duszak) should get fired by their bosses for producing “not a tiger but a kitty”.
- We discussed Gulf War syndrome. Norman said people imagine anthrax is dangerous, but the ex-Soviet bioweapons researchers said to attack New York with anthrax would need 20,000 Boeing 747s flying over the city, dropping millions of tons of anthrax spores from a low height then people spreading it with shovels. The only way to infect people with anthrax is by direct means via an oxygen line or a direct injection.
- Norman said the Tokyo gas attack was successful in Japan because the terrorist used sarin, a nerve agent. The biological agents used, botulinum and anthrax, fortunately failed.
- Within the CDC Fauci was called the ‘mean midget’ and during the AIDS epidemic he sunk Robert Gallo by inventing the story that Gallo had stolen the HIV virus from Luc Montagnier, thus destroying Gallo’s chances of being awarded the Nobel prize (he was also denied a patent).
- Fauci is “not stupid, he is mean”. Fauci wanted to get a Nobel prize, but he didn’t get a Nobel prize for AIDS, so he wanted it for the Wuhan virus. In January 2023 knowing that he wasn’t going to get the Nobel prize he “pulled the plug” and published this paper saying new types of vaccines are needed for respiratory infections, as an act of spite.
We learned a lot from Norman and are very grateful to him for giving us his valuable time. You will notice that we briefly discussed the vaccines, but you will be very pleased to hear that Norman has agreed to follow up with another meeting in early December to share his thoughts on this important topic (see here for a sneak peek)
You can access Norman’s other material on YouTube and Facebook (much of his material is in Polish and Norman speaks six languages!) His twitter handle is @normanpie.
1 Note that this synopsis is not a verbatim and true transcription of the conversation.
2 This document presents evidence PCR was used to collect samples, but no mass testing was undertaken.
3 Submitted (05-JAN-2020) Department of Zoonoses, National Institute of Communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention. The first submission to GenBank had two subsequent revisions.
4 The supposed ‘novel and deadly’ attributes of the virus are discussed extensively here.
5 See this paper. “Mammals are the reservoir hosts of the majority of emerging zoonoses (2, 3, 18). If we assume that all 5,486 described mammalian species (19) harbor an average of 58 viruses in the nine families of interest (as estimated here in P. giganteus) and that these viruses exhibit 100% host specificity, the total richness of mammalian viruses awaiting discovery exceeds ~320,000.”
Next few years will determine future world order – Biden

Joe Biden speaks about his Bidenomics agenda on November 1, 2023. © ANDREW CABALLERO-REYNOLDS / AFP
RT | November 3, 2023
The world is at a crossroads and the next few years will determine its fate for several generations to come, US President Joe Biden has claimed. His prediction comes amid Washington’s standoff with Russia over Ukraine and his country’s increasingly strained relations with China.
Speaking ahead of a meeting with Chilean President Gabriel Boric on Thursday, Biden stated that “there comes a time, maybe every six to eight generations, where the world changes in a very short time.”
The US leader further claimed that “what happens in the next two, three years are going to determine what the world looks like for the next five or six decades.”
According to a White House readout of Biden’s meeting with Boric, the pair discussed issues of shared concern, including efforts to combat climate change.
Biden also spoke last month about the need for a “new world order,” suggesting that while the post-World War II system has functioned for decades, it has “sort of run out of steam.”
However, if Americans “are bold enough and have enough confidence in ourselves, [they will have an opportunity] to unite the world in ways that it never has been,” he insisted.
Commenting on Biden’s remarks at the time, Kremlin Press Secretary Dmitry Peskov described it as a rare moment when Moscow was in complete agreement with Washington. “The world indeed needs a new order, based on absolutely new principles,” he noted.
However, Peskov suggested that Biden meant building “a world [order] revolving around the US,” insisting that “this will not be anymore.” Russia has consistently called for a multilateral world order, with President Vladimir Putin accusing the West of “a colonial approach” and bending international rules to its will.
Last month, the Russian leader also stressed that “nobody has the right to control the world at the expense of others or in their name.”
Relations between Washington and Moscow have sunk to unprecedented lows due to the Ukraine conflict, with the US sending billions of dollars’ worth of weapons to Kiev and imposing tough sanctions on Russia.
Elsewhere, relations are tense between the US and China, most notably over Washington’s support for Taiwan. The two nations are also engaged in an intense economic rivalry. China has been promoting its Belt and Road Initiative (BRI), which seeks to develop international transport infrastructure and has been supported by more than 140 countries.
Biden has signaled that the US is working with G7 members to compete with China economically, claiming that the BRI has ended up being “a noose for most of the people who have signed on.”
WHO Publishes Latest Draft of Pandemic Treaty To Combat “Misinformation”
By Didi Rankovic | Reclaim The Net | November 2, 2023
The United Nations World Health Organization (WHO) has published a new draft of its troubled pandemic agreement/accord/treaty – which the agency has complained is taking too long to finalize.
The latest draft of the negotiating text, released by the Bureau of the Intergovernmental Negotiating Body (INB) on Monday must be considered until the INB session scheduled for November 6-10, when it should be formalized.
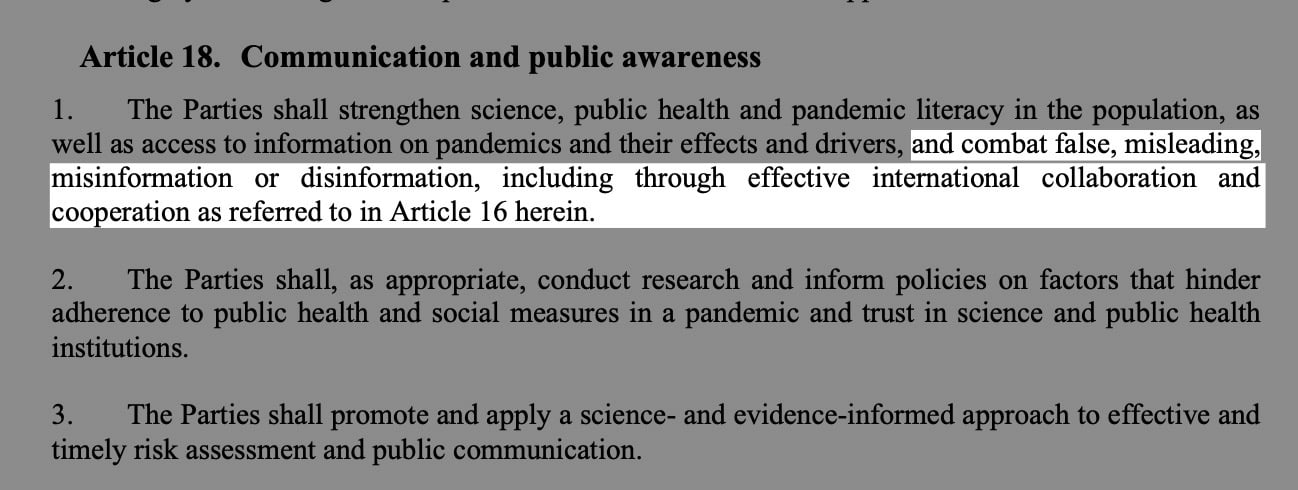
Some of the commitments contained in this version of the document have to do with combating “false, misleading, misinformation or disinformation, including through effective international collaboration and cooperation” – which skeptics might easily dub, “cross-border censorship.”
And then there’s surveillance, too: something called One Health approach for pandemic prevention, preparedness and response, which the draft wants to see promoted and implemented. Meanwhile, One Health is a surveillance tool that is supposed to create new methods of disease control.
Yet another point from the proposal is to “develop and strengthen pandemic prevention and public health surveillance capacities.”
Critics have many concerns and misgivings about all of this, including WHO setting up what’s known as a conference of the parties – an international convention’s top governing body – around the pandemic accord.
The fear here is that it would be one more instrument taking agency and consent away from national governments and people and transferring the decision-making processes, in this case related to health, to the world organization, specifically, WHO.
However, the draft’s chapter on institutional arrangements envisages establishing just such a conference of the parties as part of the accord’s scope.
A number of advocacy organizations from around the world have already expressed their dissatisfaction with the draft from different points of view, including how the treaty, if adopted, would impact less developed countries, while the draft itself is seen as “unbalanced.”
This last objection stems from the origin of the proposal – namely the discussions between INB Bureau and Secretariat, rather than drawing from the meetings of the INB itself.
Ignoring proposals from all countries that are supposed to implement the treaty, and allowing those with the most clout (in the Bureau) to set the tone is seen as one-sided in this sense as well.
“Shedding” of Covid mRNA Vaccine Components and Products From The Vaccinated to the Unvaccinated – Part 1
It’s happening. The manufacturers and regulators knew it was a risk, yet, like numerous aspects of the Covid vaccine mRNA technology, did not test for excretion potential of spike proteins or LNP’s.
Pierre Kory’s Medical Musings | November 1, 2023
Awareness of the Federal Regulators and Vaccine Manufacturers
The data showing the toxicity and lethality of the vaccines started within weeks of the roll-out with hundreds of thousands of adverse events and hundreds of deaths reported to VAERS in January of 2021, far exceeding previous stopping points of any new medical product or vaccine.
Although ignored (to this day), anyone paying unbiased attention could see a further mountain of evidence develop, including a skyrocketing number of newspaper and television reports of healthy athletes and young people arresting and dying while doing normal everyday activities or sports (countered by corporate/government controlled media with a plethora of fact checking articles using cherry picked data to inform the world that what they are seeing is not factually true).
Then life insurance industry data emerged showing historically unprecedented rises in death claims being paid out amongst the healthiest sectors of society temporally associated with the proliferation of Covid mRNA vaccine mandates within schools, corporations, universities, health care institutions, federal contractors etc. Most telling of the deathly impact of mandates was the fact that the largest increases among the sudden, rapid rises in excess deaths occurred among employed white collar workers.
The reality is that these data are still ignored by media and public health agencies across the world. Even more worrying are the more recent reports finding universal contamination of every studied vaccine vial with large magnitude, excess levels of DNA fragments and DNA plasmids. Then the discovery that the DNA plasmids used in the manufacturing process contained genetic sequences that both promote DNA integration into the human genome as well as promote the development of cancer.
It truly is unimaginable that we now must consider the risks (and reality) of “shedding” of the vaccine products from the vaccinated to the unvaccinated. This now has implications for nearly every human being walking the earth, vaccinated or unvaccinated (including me).
This series will explore the regulatory, scientific, epidemiological, and clinical data indicating that shedding is occurring. The health of who knows how many is now being threatened, with the extent of the risks likely both highly variable and difficult to predict, both in the short term and long term. That is unless we start to seriously study the phenomenon further. So, let’s review what is known.
Within 3 months of the rollout of the global Covid mRNA vaccination campaign, I was consulted by two different unvaccinated women in their late 30’s and early 40’s respectively, who reported that they were suffering acute menstrual abnormalities in the days following close exposure to a recently vaccinated practitioner (one visited a massage therapist and another an acupuncturist). Both had a history of highly regular, uncomplicated menstrual cycles over decades.
Since that time, at least twenty other unvaccinated and vaccinated people, both men and women, have reported to me compelling histories of typical post-mRNA vaccine adverse effects subsequent to close exposure to vaccinated family members, contacts, or friends.
Further, my partner Scott Marsland at our Leading Edge Clinic, who also specializes in treating Long Covid/Long Vax syndromes, has a growing series of detailed case histories of similar “shedding” events occurring. I will revisit this in a later post in this series, but I will briefly say here that our clinical observations conclude that symptomatic shedding events do occur. However, we have little idea of exactly how common it is occurring among the general population.
This is further complicated by the fact that even if it were occurring frequently, the vast majority of people suddenly developing typical vaccine side effects symptoms after exposure to a vaccinated person would never think to relate it to exposure to shed vaccine products. It is my belief that very few people in the general public are aware of the possibility it could occur. You know, because the regulators have assured the country that mRNA technology is “safe and effective.”
However, my general sense is that it occurs largely in people who have increased physiologic sensitivity to environmental exposures, toxins, or pharmaceuticals and that it is generally transmitted by someone recently vaccinated or someone who is producing a lot of spike protein. Note that is my “general sense.” More studies are required to fully understand both the frequency of and physiologic impacts from such events.
My ignorance as to the frequency of symptomatic shedding events is due to the fact that the concept of transmitting spike proteins (or lipid nanoparticles) from a Covid mRNA vaccinated person to another is one of the least studied and published-on aspect of the mRNA vaccine technology.
What is so shocking about that lack of research (actually nothing is shocking anymore) is that shedding has major global implications. Apparently it is not just me who thinks this because, as an expert on several aspects of Covid, I have been lecturing across the U.S, Europe, and South America in conferences, Parliamentary hearings, or invited lectures. Questions about shedding appear everywhere (in the dozens of Q & A’s that I have participated in, it is nearly always the first question. It is also a very common topic in the chat of our FLCCC weekly webinar.
Know that in this tonight’s FLCCC webinar, I will present a 15-20 minute overview of this series along with my private practice partner Scott Marsland. We expect to be deluged with questions after.
Anyway, I believe that by the end of this series on the science, epidemiology, and clinical observations of shedding, you will be convinced that it can and does occur.
From our Federal government, in this FDA document, the term “shedding” is defined as:
“The release of viral or bacterial gene therapy products from the patient by any or all of the following routes: feces (feces); secretions (urine, saliva, nasopharyngeal fluids, etc.); or through the skin (pustules, lesions, sores).”
They forgot to mention “exhaled breath.” More on that later. The “products” they refer to that can be transmitted from a Covid vaccinated person to another include not only the genetically programmed spike protein product, but also the lipid nanoparticle (LNP) containing the mRNA that is in the injections as well as naked mRNA that can be released from the LNP. Even more worrying is the recent shocking discovery that every single Moderna and Pfizer vaccine vial is contaminated with high levels of DNA plasmids potentially capable of integrating into the human genome. Contemplating that last one is disturbing, the implications of which we will not know for some time.
First off, let’s be clear that the Covid mRNA and DNA vaccines are gene therapy medicinal products (GMTPs or GTP’s) as stated in the FDA’s 2015 document on Gene Product Shedding Studies.
“Gene therapy products are all products that mediate their effects by transcription and/or translation of transferred genetic material and/or by integrating into the host genome and that are administered as nucleic acids, viruses, or genetically engineered microorganisms.
Also note that in this European Medicines Agency (EMA) document, the mRNA vaccines also meet their definition of gene therapy medicinal products (GMTP’s).
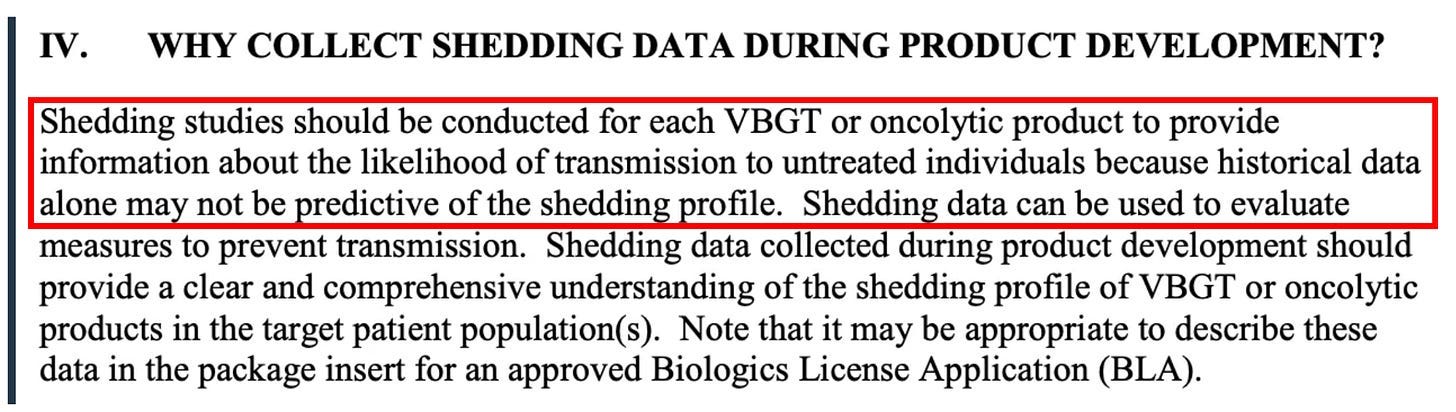
Ok, now that we know what a gene therapy product is and that the Covid mRNA injection is actually a form of gene therapy (marketed to the public as a “vaccine”), what does that have to do with “shedding?” Again from the FDA document regarding the evaluation of the safety of gene therapy products, they emphasize the importance of studying shedding:
Shedding is distinct from biodistribution because the latter describes how a product is spread within the patient’s body from the site of administration while the former describes how it is excreted or released from the patient’s body. Shedding raises the possibility of transmission of virus or bacteria based gene therapy products (VBGT) from treated to untreated individuals (e.g., close contacts and health care professionals).
This guidance represents FDA’s current thinking on how and when shedding data should be collected for VBGT and oncolytic products during preclinical and clinical development and how shedding data can be used to assess the potential for transmission to untreated individuals.
So, with these findings in mind, it may be no wonder why the FDA insists on shedding studies:
Further on in the document, the FDA again emphasizes the importance of shedding studies:
Note that the FDA emphasizes the importance of doing human shedding studies and not just relying on animal studies:
To inform the design of human shedding studies, shedding data may be collected in animals following administration of the VBGT or oncolytic product. These data can help estimate the likelihood and potential shedding profile in humans, particularly when there is concern about transmission to untreated individuals. However, such data cannot substitute for human shedding studies for several reasons.
But again, no studies testing whether excretion of mRNA-containing LNPs, modified spike-encoding mRNA, or spike produced by vaccinated people have been done. Well, I shouldn’t say none, because in this paper the author cites a Pfizer document obtained by FOIA which apparently revealed that shedding was studied in the urine and feces of intra-muscular injected rats. Unfortunately, that document is no longer at the website referenced.
To summarize from the above, the FDA’s position is that:
- the mRNA vaccines are gene therapy products
- Gene therapy products require shedding studies in both animals and humans
- Gene therapy product shedding raises the possibility of transmission from treated to untreated individuals
Note that much of the rest of this series of posts on shedding is guided by a masterful comprehensive review of the topic of gene therapy product shedding by independent researcher (by definition) Helene Banoun in Infectious Diseases Research. Hers is one of the only papers I could find that attempted to meticulously explore what is known about shedding of the mRNA gene therapy vaccines.
As already stated, an important point Banoun makes is:
There was no regulation of mRNA clinical trials prior to RNA vaccines, yet there is strict regulation of gene therapy products. It is difficult to justify that mRNA vaccines are not considered in the same way as gene therapies regarding this regulation; indeed the only difference is that they are (historically) supposed to protect against a disease and not cure it. Gene therapies are intended for a small number of people in poor health, whereas vaccines are used on a large scale on healthy people: it would therefore be wise to apply stricter rules to them.
She further points out another omission of the regulatory process:
Any experiment involving the deliberate transfer of a nucleic acid to a human must be preceded by Institutional Biosafety Committee approval (document on the regulatory standards is here), but approval was not given because of the emergency clearance given to mRNA vaccines.
Therefore, according to both the American and European agencies, mRNA vaccines are gene therapy products and should have been subjected to excretion studies of all secreted fluids (urine, exhaled droplets, saliva, sputum, nasopharyngeal fluids, semen, breast milk, feces, and sweat). Again, these studies were not done for mRNA vaccines nor for the DNA adenovirus vaccine (J&J).
So, where are the clinical human shedding studies? Well, I just learned of one that is about to be published (next ten days?) where the research team exposed a population of unvaccinated women to vaccinated individuals and their assessment outcome was the development of menstrual abnormalities. I know the results but want to respect the research teams right to present their original work. They have promised to share their manuscript with me and Paul Marik as soon as the peer-review and acceptance process is complete. I have no idea what journal they submitted to but I can be highly confident it is not the New England Journal of Medicine.
The entire reason why I did a “deep dive” into shedding science is because shedding was not studied when it absolutely should have been and I believe with near certainty that it occurs. Note my use of “near certain” is only to seem objective but it really is too late for that – both my partner Scott and I have diagnosed and successfully treated a number of shedding “victims.”
The lack of shedding studies prior to the mRNA rollout was, in my opinion, an insanely reckless and irresponsible omission (or willfully criminal, take your pick). As an evolving expert in the evaluation and treatment of Covid mRNA vaccine injury syndromes, I and others have identified the spike protein as the main component responsible for not only the pathogenicity of Covid but also of the vaccines, with this review paper proposing a new field named “spikeopathy” (study of the disease processes triggered by the spike protein).
If vaccine transcribed spike protein can be transmitted in sufficient quantity from vaccinated folks to unvaccinated ones, it stands to reason that adverse effects of the vaccine can develop in some unvaccinated people who came into contact (or close proximity) with vaccinated people. How did they get away with not studying this possibility?
An easy answer is they were doing science at “warp speed.” The more uncomfortable answer is that the “vaccines”, although meeting the definition of a gene therapy product, were actually not even legally considered a medical product at all and thus did not require a diverse range of safety studies (like on genotoxicity, reproductive risks, excretion potential etc). What? Why? How?
The reality is that the Covid vaccines, as a result of successive federal legislative actions which evolved over decades, was legally categorized as a “countermeasure” under a “public health emergency.” Such “countermeasures” require no specific regulatory approval process prior to dissemination. All a countermeasure needs is the recommendation of the Secretary of Health and Human Services that “it may be effective.”
This is the conclusion derived from the legal investigatory work of various independent and legal experts and researchers like Catherine Watts, Todd Callender, and Sasha Latypova. If interested in learning more, I would watch this lecture by Sasha Latypova (scroll down the page to find her lecture). As they have uncovered, “countermeasures” (even gene therapy ones) do not legally require studies of excretion potential, bio-distribution, pharmacokinetics, genotoxicity, insertional mutagenesis etc.
They don’t even require FDA regulated clinical trials of efficacy or safety.
So why did Pfizer and Moderna even do the efficacy trials? Latypova maintains that they did this not only to satisfy the public’s confidence to increase vaccine uptake, but also to “fool” the public into thinking these vaccines were medical products subject to standard (albeit accelerated) pharmaceutical product regulatory processes.
This obscured the reality that they were instead classified as military “countermeasures” against a perceived (if not actual) bioweapon. To wit, the COO of Operation Warp Speed was a General from the Department of Defense (DOD) and the vaccine manufacturers were under contract with the DOD to produce the countermeasure, sometimes referred to as a “demonstration (demo)” and/or a “prototype” in numerous legal documents they uncovered.
Anyway, as a result of this lack of a legal requirement to fully study these products in a public health emergency, the list and types of studies that should have been conducted (but were not) is long. Researchers and clinicians have been screaming about this since they were rolled out. These cries were met with a deafening silence by governmental health agencies across the world.
I know, it is a lot to take in.
But the latest “word on the street” is that the finance and insurance industries may finally be waking up to this fraud and its devastating impacts on U.S disability and death rates. Knowledge of these society-wide impacts largely results from the work of two different research teams led by former Blackrock portfolio manager Ed Dowd and insurance industry consultant Josh Stirling).
This article describes the reasons why Pfizer and Moderna stock are crashing of late. Put more succinctly, from what I hear it is due to the hedge fund guys shorting their stock. I believe Pfizer is in even deeper trouble now that this “forensic” paper just got published finding that they hid vaccine trial deaths which obscured a 3.7 fold increased risk of cardiac death in the vaccinated arm of their trial.
“Shedding” Part 1– Shedding of Covid mRNA Vaccine Components and Products From The Vaccinated to the Unvaccinated – Part 1
“Shedding” Part 2 – The Bio-Distribution and Excretion Potential of Covid mRNA Vaccine Products
“Shedding” Part 3 – Can You Absorb Lipid Nanoparticles From Being Exposed To a Vaccinated Person?
“Shedding” Part 4 – Evidence of Placental and Breast Milk Transmission of Covid mRNA Vaccine Components
“Shedding” Part 5 – Evidence of Shedding Causing Illness In Others
“Shedding Part 6– Clinical Case Notes Describing Shedding Phenomena Among Leading Edge Clinic Patients
“Shedding” Part 7 – Shedding Via Sexual Intercourse – Clinical Reports
Featured Video
Deep Dive Intel Briefing 6/20/2026 Lt Col Daniel Davis
or go to
Aletho News Archives – Video-Images
From the Archives
As Hillary Clinton kisses up to Henry Kissinger, RT looks at 4 of his most heinous acts
RT | September 3, 2016
… While Clinton retains the ultimate warmongering seal, RT examines some of Kissinger’s most memorable acts… Read full article
Blog Roll
 Aletho News
Aletho News- Iran opens hundreds of legal cases over US, Israeli aggression: Prosecutor general
- Iran delegation protests Trump’s threat at Switzerland talks, weighs ‘proper’ response: Source
- Terms of US capitulation to Iran presage new era for the region
- Strategic Oil Reserve Nears Collapse… US Must Choose: Guns or Butter
- The Story the Media — and the Government — Don’t Want You to Hear
- Deep Dive Intel Briefing 6/20/2026 Lt Col Daniel Davis
- The Targeted Assassination of Studies Showing Vaccines Cause Injury
- BMJ Probe Into Excess Mortality Study Drags On for Two Years With No Resolution
- Securing Peace with Iran Compels Trump to Divorce Israel
- Old Iraq war architects rise up to wag finger at Trump’s Iran deal
- If Americans Knew
- JNS Policy Summit to kick off in Israel
- Fatalities From Israel’s Vast Gaza Genocide Deliberately Undercounted
- ‘Reproductive genocide’ in Gaza; death toll in Lebanon tops 4,000 (during a ceasefire) – Daily Update
- Israelis Invaded Lebanon And Then Cried Victim When Their Soldiers Got Killed
- FARA Docs: Israel is Spying On Millions Of Christian Americans In Their Churches
- Why US presidents from both parties end up cursing Benjamin Netanyahu
- Israel Asked Facebook to Censor Iran War Content, Internal Documents Show
- Deaths in Gaza undercounted, possibly by 100s of thousands; “Psychopath” Ben-Gvir talks trash – Daily Update
- UNICEF: “Trauma is woven into the very fabric of childhood in Gaza”
- 15 articles a day: The extent of the Israeli army’s media interference
- No Tricks Zone
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
