Bill Gates-Funded Scientists Found NO mRNA in Breast Milk a Year Ago
They Tried Hard NOT to Find Anything!
By Igor Chudov | September 28, 2022
My recent post about scientists finding mRNA nanoparticles containing Covid vaccine genetic code, in the breast milk of vaccinated mothers, and mentioning an infant documented to have died thereof, got quite a bit of traction online.

Today, I want to look at a study from a year ago that purported to NOT find mRNA nanoparticles in breast milk. We will see why exactly the team having Bill Gates and CDC-sponsored researchers, could not find what the independent scientists could find a year later!

I decided to compare the two studies (one that found mRNA in breast milk and the other that did not) very closely and compare their methodologies using the “Modern Discontent” method.
Modern Discontent has a great post about his method, but he mostly is saying “pay close attention and understand the whole f… thing”, which is basically what I usually do with something interesting and important anyway. He posted his method three days ago, and I had my substack for a while longer. So, I intuitively used many of his approaches, but he laid them out very systematically and clearly. His article is extremely useful for all people writing about biomedical science, so take a look:
At first sight, both studies, which I will call the 2022 shedding study (which I discussed two days ago) and the 2021 no-shedding study, superficially appear to be similarly designed. They took several lactating women and tested their milk. One study found shedding, while the other did not. Upon a closer look, the differences between these studies turned out to be extremely important!
Here’s a summary of their differences:

You can see that the study that found mRNA lipid nanoparticle shedding, was done more thoroughly. The shedding study had:
- More participants (11 vs 7)
- More milk samples were taken (131 vs 13!)
- Samples better preserved (frozen immediately)
- Samples were taken at varied moments post-vaccination including within mere hours, and also days
- Looked at very important Extracellular Vesicles
As a result of being more thorough and covering more cases, the shedding study found actual shedding! Surprise!
What if the women in the shedding study, getting the same vaccines, were analyzed using the poorer methodology of the no-shedding study?
I took the chart from the shedding study showing five women with milk samples positive for mRNA nanoparticles. I crossed out samples that WOULD NOT BE DETECTED, if the no-shedding study methodology was applied to the samples of the shedding study:

You can see that if the researchers in the shedding study used the crippled methodology of the no-shedding study, they would detect only two positive samples, instead of seven.
The methodology of the no-shedding study would miss all extracellular vesicle (EV) samples because they did not look at EVs. That is shown in the column on the right that is entirely crossed out.
The no-shedding study would also miss the 1 hour and three-hour samples because they did not take those samples (save for just ONE woman who happened not to be positive).
As a result, had the less thorough no-shedding study methodology been applied to the shedding study, only 2 positive samples, instead of 7, would be detected!
Since the actual no-shedding study collected only 13 samples and not 131 samples and used deficient methodology, no wonder they missed all positive instances!
It is as if the no-shedding study was intentionally designed not to find anything. Hmmm…
Let me give an analogy that many will understand — fishing using fishing nets.
Let’s say that a good fisherman (the shedding study) was asked to do his best job fishing to see if a particular lake has fish (mRNA nanoparticles). A bad fisherman, on the contrary, would be asked to design his fishing expedition to not catch any fish, so as to falsely prove that the lake has no fish. What would they do? This infographic shows the difference:

What’s up with Bill Gates and the CDC?
By pure coincidence, the study that did not find mRNA nanoparticles in breast milk (the no-shedding study), had key scientists sponsored by the Bill and Melinda Gates Foundation. They also received money from the CDC. You can see that Prof. Gaw and Dr. Flaherman were key participants, making the most important decisions and analyses!

Did these sponsorships influence the authors’ approach to designing the experiment? We cannot know this. We can only wonder.
Why would a fisherman try to NOT catch fish?
Executive Order Advances Biotech-Transhumanist Agenda
I predicted this ‘no testing required’ formula would spread beyond COVID shots, and that’s exactly what’s about to happen.
By Dr. Joseph Mercola | September 25, 2022
Scroll down for videos.
September 12, 2022, President Biden signed the “Executive Order on Advancing Biotechnology and Biomanufacturing Innovation for a Sustainable, Safe and Secure American Bioeconomy.”1
Specified in that order is the development of genetic engineering technologies and techniques “to be able to write circuitry for cells and predictably program biology in the same way in which we write software and program computers,” as well as genetic technologies to “unlock the power of biological data” using “computing tools and artificial intelligence.”
Additionally, “obstacles for commercialization” will be reduced “so that innovative technologies and products can reach markets faster.” What we have here is, in a nutshell, the creation of a fast-tracked mRNA pipeline.
When, in June 2022, the U.S. Food and Drug Administration quietly implemented a “Future Framework” scheme2 to deliver reformulated COVID boosters without additional testing, I predicted that this “no testing required” formula would spread beyond COVID shots. And, according to this executive order, that’s exactly what’s about to happen.
In early September 2022, the FDA also put out medically false and misleading COVID booster campaign messages that prove we’ve officially entered the era of transhumanism:
“It’s time to install that update! #UpdateYourAntibodies with a new #COVID19 booster.”3 “Don’t be shocked! You can now #RechargeYourImmunity with an updated #COVID19 booster.”4

Historically, gene therapies have had to jump through extra hoops, which is why so few exist on the market. As of 2021, there were 20 gene therapies commercially available.5 The world’s first gene therapy trial didn’t begin until 1990, so this is still a very new field.
The entire gene therapy field actually collapsed overnight in 1999, when a teenage trial participant died from side effects. An FDA investigation concluded research had moved too fast and that safety “had not been put first.”6 Progress, thanks to increased caution, slowed from there on.
Such caution is now being thrown to the wind, and it’s not difficult to predict there will be disastrous ramifications. Millions will die from poorly tested gene therapies and, eventually, medical research and allopathic medicine will both cease to exist, as survivors vow to have nothing to do with that murderous cabal ever again.
The only way they might be able to keep going is if they are in control of people’s brain function and/or able to force drugs under threat of death, or worse — neither of which is impossible at this point, shockingly enough. In the meantime, we’re looking at a cornucopia of mRNA shots coming our way.
Not surprisingly, mRNA flu shots are in the works.7 While we probably won’t see mRNA flu shots during the 2022/2023 winter season, there’s every reason to expect they’ll be rolled out next year.
September 14, 2022, Pfizer initiated a Phase 3 study, which will test a quadrivalent mRNA-based flu shot on 25,000 American adults.8 Pfizer is also exploring mRNA technology that uses self-amplifying RNA (saRNA), for potential use in the future.9
Moderna began its Phase 3 mRNA flu jab trial in early June 2022.10 It’s also working on mRNA shots for respiratory syncytial virus (RSV) and cytomegalovirus (CMV), which is in the herpes family, as well as a SARS-CoV-2-influenza combination shot. Ultimately, Moderna wants to create an annual mRNA shot that covers all of the top 10 viruses that result in hospitalizations each year.11
Its current flu jab candidate, mRNA-1010, encodes for the hemagglutinin (HA) glycoproteins of four different influenza strains, including influenza A/H1N1, A/H3N2, influenza B/Yamagata and B/Victoria. According to Moderna:12
“HA is a major influenza surface glycoprotein that is considered an important target to generate broad protection against influenza and is the primary target of currently available influenza vaccines.”
The Transhumanist Agenda
Over the past three years, I’ve written several articles exploring the transhumanist agenda, which all these mRNA shots and genetic technologies are part and parcel of. Basically, the goal of the transhumanist movement is to transcend biology through technology, and to meld human biology with technology and artificial intelligence.
In September 2020, I posted a video with Dr. Carrie Madej (above), in which she suggested we were standing at the crossroads of transhumanism, thanks to the fast approaching release of mRNA COVID-19 shots.
Since these shots are designed to manipulate your biology, they have the potential to also alter the biology of the entire human race. Nearly two years later, we still don’t know the extent to which they might be doing that, yet more fast-tracked and untested gene therapies are on the way.
One reason why it’s important to know for certain whether synthetic RNA ends up creating permanent changes in the genome is because synthetic genes are patented. If they cause permanent changes, humans will contain patented genes, and that brings up very serious questions, seeing how patents have owners, and owners have patent rights.
The hydrogel used to preserve the mRNA can also contain nanobots to create a bioelectric interface capable of connecting to a smartphone or other interface. Novel technologies that measure biological data, such as blood sugar, are based on this. Such technologies will, of course, have immediate ramifications for our privacy.
Who will collect and have access to all this data? Who will be responsible for protecting it? How will it be used? Also, if your cellphone can receive information from your body, what information can your body receive from it, or other sources? Could transmissions affect your mood? Your behavior? Your physical function? Your thoughts or memories?
So far, it doesn’t appear as though the COVID shots have these kinds of capabilities built in, but we do know for a fact that militaries around the world are exploring and working toward such capabilities. In fact, it’s an arms race in its own right.
In his September 14, 2022, Substack article,13 “Human Cyborgs Are Just the Beginning,” Dr. Robert Malone reviewed several of those plans. Certain report titles alone tell the story, such as the U.S. Department of Defense (DOD) Biotechnologies for Health and Human Performance Council’s report,14 “Cyborg Soldier 2050: Human/Machine Fusion and the Implications for the Future of the DOD.” It doesn’t leave a whole lot to the imagination, does it? According to the assessment abstract:
“The primary objective of this effort was to forecast and evaluate the military implications of machines that are physically integrated with the human body to augment and enhance human performance over the next 30 years.
This report summarizes this assessment and findings; identifies four potential military-use cases for new technologies in this area; and assesses their impact upon the DOD organizational structure, warfighter doctrine and tactics, and interoperability with U.S. allies and civil society.”
Human augmentation technologies deemed technically feasible by 2050 at the latest include ocular enhancements to improve sight and situational awareness, optogenetic bodysuit to restore or improve muscular strength and control, auditory enhancements, and neural enhancement of the brain for two-way data transfers and brain-to-brain communication.
In “The Plan to Turn You Into a Genetically Edited Cyborg,” I covered another shockingly dystopian report by the U.K. Ministry of Defense and the German Bundeswehr Office for Defense Planning, published in May 2021.
That report, “Human Augmentation — The Dawn of a New Paradigm, a Strategic Implications Project,”15 reviews the scientific goals of the U.K. and German defense ministries, and they basically mirror that of the U.S. DOD. On page 12 of the report, the concept of the human body as a platform is described, and how various parts of the human platform can be augmented. For example:
- Physical performance such as strength, dexterity, speed and endurance can be enhanced, as well as physical senses. One example given is gene editing for enhanced sight
- Psychological performance such as cognition, emotion and motivation can be influenced to activate and direct desired behavior. Examples of cognitive augmentation include improving memory, attention, alertness, creativity, understanding, decision-making, intelligence and vigilance
- Social performance — “The ability to perceive oneself as part of a group and the readiness to act as part of the team” — can be influenced. Communication skills, collaboration and trust are also included here
They list several different ways to influence the physical, psychological and social performance of the “human platform,” including genetics (germ line and somatic modification), synthetic biology, invasive (internal) and noninvasive (external) brain interfaces, passive and powered exoskeletons, drugs and nano technology, neurostimulation, augmented reality technologies such as external holograms or glasses with built-in artificial intelligence, and sensory augmentation technologies such as external sensors or implants.
As noted in this report, “Human augmentation has the potential to … change the meaning of what it means to be a human.” This is precisely what Klaus Schwab, founder and executive chairman of the World Economic Forum (WEF), has stated is the goal of The Fourth Industrial Revolution.16
WEF has been at the center of global affairs for more than 40 years, and if you take the time to dive into WEF’s Fourth Industrial Revolution material, you realize that it’s all about transhumanism. It’s about the merger of man and machine.
This is a dystopian future that WEF and its global allies are actively trying to implement, whether humanity at large agrees with it or not. Importantly, the “Human Augmentation” report readily admits that human augmentation can “directly enhance behavior.”
And, if you think these reports are just brain fodder for geeks in uniforms, think again. The U.K. Defense and Security Accelerator (DASA) is currently, right now, accepting proposals for human augmentation technologies such as those listed above.17 Grants of 70,000 euros ($74,000), will be given to proposals that can provide proof of concept.
Both the DOD’s “Cyborg Soldier” report and the British/German “Human Augmentation” reports discuss the fact that human augmentation will inevitably widen already existing disparities, inequalities and inequities, and therefore, “efforts should be undertaken to reverse negative cultural narratives of enhancement technologies.”18
In other words, don’t let people come to the conclusion that human cyborgs are a bad idea, because at worst that might prevent their development, and at best, it’ll pitch regular people against the augmented elite, making their efforts to rule the plebs more difficult.
As noted by Malone, “Once again, we are being played before we even know what the playing field looks like.”19
Disturbingly, considering how nontransparent governments have been so far, it’s not inconceivable that technologies capable of influencing thoughts and behaviors would be used on populations without informing anyone, which makes the list of potential risks one takes with each new mRNA injection even longer than it already is.
But we don’t need to be genetically reengineered or have nanobots introduced into our brains to be at risk of outside manipulation. That’s already happening through noninvasive means.
In a November 2019 interview with CNN,20 history professor Yuval Noah Harari, a Klaus Schwab disciple, stated that humans are already “hackable,” meaning the technology exists by which a company or government can know you better than you know yourself, and this knowledge can be used for both good and ill.
According to Harari, the available capabilities already go far beyond Orwell’s “1984” authoritarian vision, and it’s only going to become more powerful from here.
He predicted that algorithms will increasingly be used to make decisions that historically have been made by humans, either yourself or someone else, including whether or not you’ll be hired for a particular job, whether you’ll be granted a loan, what scholastic curriculum you will follow and even whom you will marry.
To learn more about the larger issues of transhumanism and the race to merge man with machine and artificial intelligence, check out the Truthstream Media video below.
For example, there are even ongoing attempts to upload the human mind into the cloud, ultimately creating a form of “digital hive mind” where everyone communicates via “Wi-Fi telepathy.” This, despite the fact we still do not fully understand what “the mind” actually is, or where it’s located.
I don’t know what it will take to prevent the dystopian post-human world envisioned by Schwab and his technocratic minions, but I suspect education would be a cornerstone of such an endeavor. In order for there to be a resistance, enough people need to be aware of what the plan is, and where we’re actually being led with all these novel therapies and inventions.
In the shorter term, it’s crucial to realize that the fast-tracking of “genetic engineering technologies and techniques to be able to write circuitry for cells and predictably program biology in the same way in which we write software and program computers” means they’re going to cut corners. Loads of them.
Testing is basically going to be done on the population at large, just as they’ve done with the COVID jabs. The results of such experimentation are relatively predictable. People will be seriously injured and many will die. So, think long and hard before you agree to take any of these forthcoming gene therapies.
A look at the true benefits and harms of mRNA
Curing the pandemic of misinformation on COVID-19 mRNA vaccines through real evidence-based medicine

The Naked Emperor’s Newsletter – September 26, 2022
A British doctor, Aseem Malhotra, has just had a two part, peer-reviewed paper published in the Journal of Insulin Resistance. The aim of the paper was to gain a better understanding of the true benefits and potential harms of the mRNA Covid vaccines. You can read Part 1 and Part 2 in full by clicking on the links.
Dr Malhotra. a cardiologist by trade, was originally a strong Covid vaccine advocate. He volunteered in a vaccine centre, was one of the first people to be double dosed and appeared on morning television to encourage everyone to get vaccinated. He was surprised and concerned at vaccine-hesitant patients when they asked about ‘anti-vax’ propaganda.
That was until, sadly, in July 2021, his father suffered a cardiac arrest and died. His father had been the former deputy chair of the British Medical Association (BMA) and honorary vice president. The 73 year old gentleman was extremely fit and active and heart scans from a few years earlier had revealed no significant problems. Dr Malhotra was shocked to read his father’s post mortem which found that two out of three of his major arteries had severe blockages.
Aseem couldn’t explain the post mortem findings and became more concerned in November 2021 after reading a peer-reviewed abstract in Circulation Journal. In the study, the mRNA vaccine was associated with significantly increasing the risk of a coronary event within five years from 11% pre-mRNA vaccine to 25% 2-10 weeks post vaccine.
He began to question his father’s death and wondered whether the Pfizer vaccination he had received six months earlier could have contributed in some way. After six months of critically appraising the data and speaking to eminent scientists, he reluctantly concluded that, contrary to his own dogmatic beliefs, Pfizer’s vaccine was far from being as safe and effective as first thought.
Questioning the data
During his reassessment of the Covid vaccine he recalled a conversation with a cardiologist colleague who decided against vaccination due to his low personal risk and concerns about short and long term harms. His colleague was particularly alarmed that, during the trials, there had been four cardiac arrests in the vaccine group but only one in the placebo group.
Next, Dr Malhotra assessed the 95% efficacy claims. Whilst this relative risk reduction made good sales material, the true value of a treatment can only be established by looking at the absolute individual risk reduction.
This turned out to be 0.84%, in other words, in a trial of 20,000 people (10,000 in the vaccine group and 10,000 in the placebo group), 4 people in the vaccine group and 88 people in the unvaccinated group would end up testing positive for Covid. Another way to express that is that you would need to vaccinate 119 people to prevent one positive test.
This absolute risk reduction figure (0.84%) is extremely important for doctors and patients to know but how many of them were told this when they received the shot? Transparent communication of risk and benefit of any intervention is a core principle of ethical evidence-based medical practice and informed consent.
The trials did not show statistically significant reductions in serious illness or mortality and in fact there were actually more deaths (19) in the vaccine group versus the placebo group (17). Furthermore, there were only nine severe cases of Covid in the placebo group, representing 0.04%. And this was in regions specifically chosen for their high prevalence of infection.
To find protection against death, then the 119 figure above (people vaccinated to prevent one positive test) must be multiplied by the number of infections that would lead to a single death in each age group. So, Dr Malhotra calculates his rate of death from Delta was 1 in 3,000 meaning the absolute risk reduction of the vaccine protecting him from death is (1 x 3000 x 119) 1 in 357,000.
As also pointed out in a recent editorial by John Ioannidis in BMJ evidence-based medicine the inferred efficacy of the vaccine from non-randomised studies may be ‘spurious’, with bias being generated by ‘pre-existing immunity, vaccination misclassification, exposure differences, testing, disease risk factor confounding, hospital admission decision, treatment use differences and death attribution’.
What should be part of the shared decision-making informed consent discussion when any member of the public is considering taking the shot is something along these lines: Depending on your age, several hundreds or thousands of people like you would need to be injected in order to prevent one person from dying from the Delta variant of COVID-19 over a period of around three months. For the over 80s, this figure is at least 230, but it rises the younger you are, reaching at least 2600 for people in their 50s, 10 000 for those in their 40s, and 93 000 for those between 18 and 29 years. For omicron, which has been shown to be 30% – 50% less lethal, meaning significantly more people would need to be vaccinated to prevent one death. How long any protection actually lasts for is unknown; boosters are currently being recommended after as short a period as 4 months in some countries.
But how many people have had a conversation that even approaches an explanation similar to that? This is before we get into the known, unknown and as yet to be fully quantified harms.
Harms
Concerns have been raised about trial participants being limited as to the type of adverse event they could report. Furthermore, hospitalised participants were withdrawn from the trial and not reported in the final results. To make matters even worse, after two months, the FDA allowed the placebo group to be unblinded and get vaccinated, completely removing any control group with which to assess adverse events.
Dr Malhotra sticks with his field of expertise, cardiology and discusses one of the most common vaccine-induced harms, myocarditis. Whilst authorities say that myocarditis is more likely after infection than vaccination, other studies have shown the opposite. There is no evidence of myocarditis until vaccination began in 2021, a full year after millions of youngsters naturally caught Covid.
Although vaccine-induced myocarditis is not often fatal in young adults, MRI scans reveal that, of the ones admitted to hospital, approximately 80% have some degree of myocardial damage. It is like suffering a small heart attack and sustaining some – likely permanent – heart muscle injury. It is uncertain how this will play out in the longer-term, including if, and to what degree, it will increase the risk of poor quality of life or potentially more serious heart rhythm disturbances in the future.
The UK’s Yellow Card reporting system is addressed and determined to be far from adequate to cope with a rapid roll out of a brand new product. 9.7 million doses were administered before the clotting problems with AstraZeneca were detected. In Denmark, they detected the problem after only 150,000 doses.
Since the beginning of the vaccine roll-out, there have been almost 500,000 adverse events reported involving over 150,000 individuals. This shows around 1 in 120 suffer an adverse event that is beyond mild. This number is unprecedented and represents the same as the total number of reports received in the first 40 years of the Yellow Card system being active. The MMR vaccine reports around 1 in 4000 suffer an adverse event.
The paper also looks at VAERS in the US which has recorded over 24,000 deaths, 29% occurring within 48 hours of vaccination and 50% within two weeks. Before 2020 there were approximately 300 deaths recorded per year.
Of most concern is that these reporting systems are actually likely to be underestimates with one paper suggesting that only 1% of serious adverse events are ever reported to the FDA. Another analysis estimated that only 10% of serious adverse events were ever reported on the Yellow Card system.
Moreover, these reporting systems will generally miss medium and long term harms as it is more difficult to attribute to vaccination.
According to ambulance service data, in 2021 there were an extra 20,000 (20% increase) cardiac arrest calls compared to 2019 and 14,000 more than 2020 in the UK.
Similarly, a recent paper in Nature revealed a 25% increase in both acute coronary syndrome and cardiac arrest calls in the 16- to 39-year-old age groups significantly associated with administration with the first and second doses of the mRNA vaccines but no association with COVID-19 infection.
More harm than good?
One has to raise the possibility that the excess cardiac arrests and continuing pressures on hospitals in 2021/2022 from non-COVID-19 admissions may all be signalling a non-COVID-19 health crisis exacerbated by interventions, which would of course also include lockdowns and/or vaccines.
Given these observations, and reappraisal of the randomised controlled trial data of mRNA products, it seems difficult to argue that the vaccine roll-out has been net beneficial in all age groups.
Dr Malhotra concludes the first part by saying that whilst risks from vaccination remain constant, the benefits reduce over time as the virus become less virulent and variants are not targeted by outdated products. He recommends a pause and reappraisal of vaccination policies.
Pandemic of misinformation
In part 2, Dr Malhotra explores the pandemic of misinformed doctors and a misinformed and unwittingly harmed public.
According to one senior doctor in regular contact with England’s Chief Medical Officer, Chris Whitty, most of his colleagues in leadership positions influencing health policy may not have been critically appraising the evidence and were instead relying on media stories on COVID-19 and the vaccines.
He says there are four key drivers and seven sins that are the root of medical misinformation:
- Driver
- Much published medical research is not reliable or is of uncertain reliability, offers no benefit to patients or is not useful for decision makers;
- Most healthcare professionals are not aware of this problem;
- Even if they are aware of this problem, most healthcare professionals lack the skills necessary to evaluate the reliability and usefulness of medical evidence; and
- Patients and families frequently lack relevant, accurate medical evidence and skilled guidance at the time of medical decision making
- Sins
- Biased funding of research (that’s research that’s funded because it’s likely to be profitable, not beneficial for patients)
- Biased reporting in medical journals
- Biased reporting in the media
- Biased patient pamphlets
- Commercial conflicts of interest
- Defensive medicine
- An inability of doctors to understand and communicate health statistics.
There are six components essential to informed decision making: (1) description of the nature of the decision; (2) discussion of alternatives; (3) discussion of risks and benefits (in absolute terms); (4) discussion of related uncertainties; (5) assessment of the patient’s understanding; and (6) elicitation of the patient’s preference.
If the administration of the vaccine did not adhere to these principles (which is likely widespread, consistent with historical evidence), then it is also a significant breach of General Medical Council duties of a doctor to ‘give patients the information they want or need in a way that they can understand’.
The paper continues to look at institutional corruption and erosion of public trust, the failure of regulation, biased reporting in the media and censorship of legitimate scientific debate.
A hard hitting, yet sensible paper which should be read by everyone, especially doctors who lost their critical thinking skills over the last few years. Dr Malhotra is a regular on TV so will this be reported in the MSM… I doubt it.
How the CDC Uses Math to Hide COVID Vaccine Harm
By Josh Mitteldorf, Ph.D. | The Defender | September 23, 2022
Last week, The Epoch Times reported that Dr. Rochelle Walensky, director of the Centers for Disease Control and Prevention (CDC), admitted the CDC had stopped monitoring the safety of mRNA COVID-19 vaccines using a method of analysis called proportional reporting ratio (PRR).
Walensky promised to resume the monitoring.
What The Epoch Times missed is that PRR is a fraudulent measure of vaccine harm, designed by the CDC expressly for the new COVID-19 vaccines to disguise the devastation the vaccines are causing.
Why? Because PRR measures the pattern of different vaccine side effects, but it is indifferent to the number of people reporting those side effects.
If some completely new vaccine side effect appears with the introduction of a new vaccine, PRR will catch that.
But the COVID-19 vaccines are associated with huge numbers of people reporting side effects on an unprecedented scale — and, by design, PRR misses this completely.
For example, if one person in a million dies from vaccine A and one person in a thousand dies from vaccine B, then vaccines A and B can have exactly the same PRR score!
PRR is a single number that compares the variety of different side effects for a new vaccine to the variety of side effects from past vaccines.
Of course, there have been many vaccines with different side-effect profiles in the past, and it is difficult to stand out among such a diversity of profiles.
Where the new mRNA vaccines do stand out is the unprecedented number of bad outcomes, including deaths, reported to the Vaccine Adverse Event Reporting System (VAERS).
Of all the reports in the 30-year history of VAERS, two-thirds of them were from the COVID-19 vaccines, introduced in the U.S. in December 2020.
This includes three-fourths of all deaths reported to VAERS and three-fourths of all hospitalizations.
Since the introduction of the COVID-19 vaccines, reports to VAERS have skyrocketed off the charts.

Credit: OpenVAERS
These numbers represent only the reports VAERS has processed and posted. Jessica Rose, Ph.D., has reported that VAERS is months behind in posting these reports because its staff has not increased, while its workload is roughly 50 times greater since the rollout of the COVID-19 vaccines.
The sheer volume of VAERS reports, including deaths, should have set off alarm bells within weeks after the vaccines were introduced.
Reporting only PRR and not the actual count provided a convenient cover for “business as usual.”
I am grateful to Mathew Crawford for pointing this out in an article last year.
Josh Mitteldorf, Ph.D., has a background in theoretical physics. Since the 1990s, he is best known for his contributions to the biology of aging, including many articles and two books.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Evidence of harm
By Steve Kirsch | September 21, 2022
A short collection of key pieces of evidence showing the COVID vaccines are not “safe and effective.” Not even close. They are the most deadly vaccines we’ve ever produced.
Here’s a high level collection of some of the most compelling pieces of evidence I’ve seen to date. This is not an exhaustive list, but just the key pieces of data that are impossible to explain if the vaccines are safe and effective.
I’ve divided the collection into sections and I’ve tried to limit each section to the most compelling data points. So don’t be disappointed if your favorite item isn’t mentioned in this article; I wanted to keep it short enough to be read..
I’ll try to keep this updated over time. It can be found in the Reference section of my Substack.
- The Pfizer trial 6 month report showed absolutely no all-cause morbidity or mortality benefit. There were no all-cause benefits at all. It was all negative. Ask your doctor why you should take a new, unproven medical intervention that is not shown to have an overall benefit. Even if there was a benefit of fewer COVID infections (which is seriously suspect due to the gaming below), the fact that the total all-cause numbers for both mortality and morbidity were negative means the intervention should not be recommended by any doctor.
- The Pfizer trial 6 month report showed that more people died (and were injured) who got the drug than who got the placebo. In other words, the cure was worse than the disease. The drug maker claimed that none of the people in the vaccine group were killed by the vaccine. They do not reveal the tests they did and explain how they were able to make that assessment. Why the secrecy here, especially in light of the study by Bhakdi and Burkhardt showing that trained medical examiners missed the causality link in 93% of the cases they looked at? The Pfizer vaccine had 4X as many cardiac arrests in the treatment group than the placebo (see page 12 of the Supplemental Appendix). This lines up very well with the numerous cardiac-related problems related to the vaccine as documented in the study by Retsef Levi and in the VAERS data which showed that the “cardiac arrest” reports were elevated by a factor of 93X higher than the annual baseline rate (VAERS reports from all vaccines combined in previous years). For some reason, the CDC wasn’t able to detect that signal (it was only 100 times higher than normal so they ignored it for some reason; they won’t let me ask them about it). In short, the claims from the manufacturer that none of the deaths were caused by the vaccine are highly suspect since all the evidence for those claims remains hidden from public view for some reason.
- The Pfizer trial 6 month report showed that at best, the drug saved only 1 COVID life per 22,000 recipients. This means that at best, after vaccinating 220M Americans, we might save 10,000 lives from COVID. But the VAERS reports show an excess death toll of well over 10,000 people and that’s before applying the minimum estimated under-reporting factor of 41. So there isn’t a mortality benefit: it’s actually the reverse. Furthermore, VAERS reports will likely only be filed for deaths in temporal proximity to the shot and is highly unlikely to report those deaths happening 5 months after the shot which appear to be the bulk of the deaths. This makes the comparison even worse. In short, we aren’t anywhere close to saving any lives at all.
- The Classen paper analyzed the clinical trial data for all three US vaccines and confirmed the lack of any overall benefit. There was an increase in morbidity which was highly statistically significant in all three vaccines. It concluded, “Based on this data it is all but a certainty that mass COVID-19 immunization is hurting the health of the population in general. Scientific principles dictate that the mass immunization with COVID-19 vaccines must be halted immediately because we face a looming vaccine induced public health catastrophe.” This is exactly right.
- The paper by Christine Stabell Benn entitled, “Randomised Clinical Trials of COVID-19 Vaccines: Do Adenovirus-Vector Vaccines Have Beneficial Non-Specific Effects?” confirmed that there was no mortality benefit by taking the COVID mRNA vaccines. “Based on the RCTs with the longest possible follow-up, mRNA vaccines had no effect on overall mortality despite protecting against fatal COVID-19.” See this article by Daniel Horowitz for more information. In other words, these vaccines have no death benefit. Period. Full stop. This is exactly what the Canadian analysis below showed.
- Serious adverse reactions, including paralysis, were not reported to the FDA and there were other very serious discrepancies in the trials. For some reason, nobody seems to be interested in exploring or explaining these very serious issues. Some are very clear cut such as the case of Maddie de Garay who was one of 1,000 kids in the clinical trial. She’s paralyzed now and has to eat with a feeding tube. The FDA and Pfizer never investigated, but reported her results as mild abdominal pain in the trial results. This is fraud. Also, there were 5 times as many exclusions in the treatment arm as in the placebo arm of the trial: 311 vs. 60. Do the p-value computation on that one and you’ll find that it could not possibly have happened by chance (1e-40). It means the trial was not blinded. Why didn’t anyone in the medical community ever point this out? Nobody will tell me.
- Pfizer admitted to clinical trial fraud in federal court. Their defense was that the FDA was in on it.
- The VAERS data, which is the official adverse event reporting system used by the US government, shows that an estimated hundreds of thousands have died and millions have been injured. If these weren’t caused by the vaccine, what caused them? Why are there more adverse events reported for these vaccines than for all other vaccines in history combined? Nobody can answer that question. See this tutorial and this recent confirmation and this article on VAERS and causality. Here’s how these numbers were calculated. Here is independent confirmation of the estimates by Dr. Naomi Wolf who used different datasets. No fact checker was interested in contacting me to challenge the facts since I always insist on recording any calls. Also, the causality of events was confirmed by the Israeli safety studies, but nobody wants to look at those.
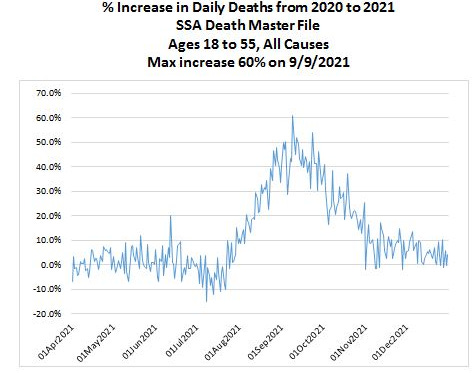
 Can you spot the unsafe vaccine? People at the CDC don’t see any problem with this mortality chart: all the vaccines look perfectly safe.
Can you spot the unsafe vaccine? People at the CDC don’t see any problem with this mortality chart: all the vaccines look perfectly safe. - The US Social Security Death Master File showed a 60% increase in the all-cause death rate in September 2021 vs. September 2020 for ages 18 to 55. According to the insurance companies, it wasn’t COVID. COVID kills only a small fraction of people in this age range so even if the COVID death rate doubled, it would be a minor blip on the all-cause death rate. A five month delay in death vs. vaccination was discovered in multiple countries, not just the US. Different studies found nearly identical delays. Also, I find it very troubling that the insurance companies aren’t asking the family of the policyholders who died whether they were vaccinated with the COVID vaccine and when. They don’t want to collect this information for some odd reason. So let’s be clear that a 60% increase in all-cause death rate makes this intervention extremely dangerous. I’m not aware of anything that comes close to killing people in such massive numbers. The CDC is silent on this. They don’t even want to show the public this chart:
- US disability rose dramatically soon after the vaccines rolled out (Y axis is Z-score). A 3 sigma increase is hard to explain.

- As of Sep 2, 2022, the vaccination rate in Israel is now just 2.4%. They used to be one of the world’s most vaccinated countries. Today, very few people in Israel are considered to be vaccinated. If the vaccines are so beneficial, why has nearly the entire country shifted from extremely pro-vax to extremely anti-vax in such a short period of time?

- The Israeli Ministry of Health revealed in a confidential meeting with scientists that the reason that they never notified the people of Israel about the safety issues from the vaccines was because of budget/staffing issues. Apparently, while they had millions of dollars to promote the vaccines as safe and effective, they forgot to budget for the possibility they were wrong.
- The Israeli vaccine safety data showed very clearly the side-effects are serious, long-lasting, and caused by the vaccines. Secondly, it showed that the Israeli authorities and the worldwide mainstream media are covering it all up. It also showed that US officials were not interested in seeing credible COVID vaccine safety that didn’t go along with the narrative. I tried to find out why, but nobody would talk to me. Harvard Professor Martin Kulldorff, a widely respected authority on vaccines, when asked why these people wouldn’t want to see the data, replied, “I don’t know.” This is the single most damaging report in the history of the COVID vaccines. Nobody wants to talk about it. They are hoping it will die. It won’t. Some people claim Israeli used a broad mix of vaccines, but that’s not true. Over 90% of the reports are from Pfizer, the bulk of the others are from Moderna. See also Israeli Investigators Find COVID-19 Vaccines Cause Side Effects: Leaked Video.
- The Canadian report prepared for the Liberal Party of Canada (Trudeau’s party) showed no benefit for infection, hospitalization, and death for those under 60. “The empirical evidence investigated in this report from PHO and PHAC does not support continuing mass vaccination programs, mandates, passports and travel bans for all age groups.” You can’t have a vaccine that doesn’t work in Canada work in other countries. The authors of the report had to hide their identities for fear of retribution. The statistics analyzed were those from Ontario which is not a small province (15M people). Naturally, the mainstream press ignored the report. Nobody has shown where the experts who wrote this made a mistake. The conclusion of the report is supported by independent analysis done by Mathew Crawford of the data from San Diego County, San Diego County Data Busts a Hole in Vaccine Efficacy Narrative. So apparently, the results are not limited to Ontario.
- The Harvard-Hopkins-UCSF study showed it is unethical to mandate vaccination for college students and anyone younger. The study clearly said, “University booster mandates are unethical.”
- The Thailand study did blood tests before vs. after the jab and determined that nearly 30% of young adults experienced cardiovascular injuries after the jab. How is that safe? And why didn’t anyone in the US ever do such a study? Do we not want to know? This was a simple blood test before and after the vaccine. Why did they not notify parents as soon as the study was published?
- The study by Bhakdi and Burkhardt showing 93% of deaths after vaccination were caused by the vaccine
- The data showing the vaccines cause prion diseases shortly after vaccination. This is impossible if the vaccines are truly safe. See the paper on ScienceOpen.com (after ResearchGate removed it).
- Determinants of COVID-19 Vaccine-Induced Myocarditis Requiring Hospitalization by Jessica Rose and Peter McCullough showing the myocarditis caused by the vaccine have distinct biomarkers.
- The Fraiman-Doshi paper looked at serious adverse event rates and found that the vaccines may not be as safe as has been claimed, but they cannot do a proper analysis because they are not allowed to see the data. “Full transparency of the COVID-19 vaccine clinical trial data is needed to properly evaluate these questions. Unfortunately, as we approach 2 years after release of COVID-19 vaccines, participant level data remain inaccessible.” You have to wonder: if the vaccine is so safe, why are the drug companies hiding the data?
- The Levi cardiac arrest rate elevation paper showed a troubling correlation between vaccine doses and increased cardiac events from January–May 2021. When they tried to get data after May 2021, they were refused access. This begs the question: if the vaccines are perfectly safe, what are they trying to hide?
- There are over 1,250 papers published in the scientific peer-reviewed literature showing the vaccines cause significant adverse events.
- The Walach paper found that the vaccines harm more people than they save.
- This news article published in the BMJ showed that 10 out of 100 deaths in elderly people they examined were “likely” caused by the vaccine. Funny, in America we think the number is 0. They can’t both be right. Someone should investigate why we have different results. This is very important. In fact, with a deeper investigation, over 90% of the deaths thought by medical examiners not to be caused by the vaccine were shown to be caused by the vaccine. This suggests that the US isn’t looking at the deaths.
- My colleagues and I are not misinformation spreaders according to this paper published in a peer-reviewed medical journal.
Are the Covid mRNA Vaccines Safe? was written by Harvard professor Martin Kulldorff who until recently was on vaccine committees of the FDA and CDC. He concluded:
Fraiman and colleagues have produced the best evidence yet regarding the overall safety of the mRNA vaccines. The results are concerning. It is the responsibility of the manufacturers and FDA to ensure that benefits outweigh harms. They have failed to do so.
Canadian court decisions on the constitutionality of Covid measures are invalid due to jurisdictional errors of law reviews court decisions on COVID and emphasizes the courts’ repeated over reliance on government expert testimony. Courts are supposed to find the truth and not rely on government representations or propaganda.
- The Watson et al. “modeling study”: did “COVID vaccinations” really prevent 14 million deaths? The original paper was clearly bogus since the vaccines kill more people than they save. This article examines the paper claiming the vaccines have been ridiculously effective.
There are specialized tests required to diagnose a death from the COVID vaccine.
The CDC has never told any medical examiner in the US about these tests.
So the medical examiners aren’t implicating the vaccine in any of the deaths.
The question is we know what the tests are, we know there is solid evidence from multiple countries that the vaccine causes death, yet we refuse to even consider the possibility that the vaccine caused the deaths. Why?
This paper, A Report on Myocarditis Adverse Events in the U.S. Vaccine Adverse Events Reporting System (VAERS) in Association with COVID-19 Injectable Biological Products, was retracted because the publisher didn’t like the result. So he unilaterally decided to retract the paper. This is unethical.
Here’s the “withdrawn” notice.
Here is the backstory as well as this censorship update.
The publisher hasn’t fixed the problem in over a year despite assurances it would be quickly resolved.
Here is another retracted paper that was correct:
Why are we vaccinating children against COVID-19? by Ron Kostoff
“Compared with the 28,000 deaths the CDC stated were due to COVID-19 and not associated morbidities for the 65+ age range, the inoculation-based deaths are an order-of-magnitude greater than the COVID-19 deaths!”
That is basically what I found: the vaccines kill >10X more people than the number of COVID deaths that they save. The paper passed peer review and was published. The editor of the journal quit after he was overridden by the publisher on the retraction.
The reason cited for the retraction:
- The use of key terminology, specifically the key terms “inoculation” and “vaccination” diverges from common use and are incorrect, indicating clear evidence of bias.
- Publicly available data from the United States Center for Disease Control (U.S. CDC) were concluded by the external reviewers to be misinterpreted to make the erroneous conclusion that the vast majority of reported deaths due to COVID-19 are actually due to other comorbidities. Such an egregious misinterpretation and misrepresentation are unacceptable.
This is completely bogus for two reasons:
- The editor could have easily normalized the terminology to eliminate any perceived “bias.” They simply ask the author to do a quick search and replace.
- The vast majority of COVID-19 deaths were in fact due to other comorbidities. For example, the New Mexico death records where COVID-19 was listed as the cause of death and 5 out 6 were not consistent with a COVID death. If anyone wants to challenge me on that, I have access to the death data. In Massachusetts, only 10% to 20% of the deaths listed as COVID were actually caused by COVID. Most people don’t have access to the death data, but I do. So I wonder if the journal is interested in fixing their error?
Can anyone explain how these anecdotes are possible?
- Why don’t Dr. Paul Offit (FDA vaccine outside committee) and Professor Grace Lee (Chair, CDC vaccine outside committee) want to see the Israeli safety data? They are deliberately avoiding answering the question. Why?
- In Canada, the #1 cause of death is now “unexplained.” See Deaths with unknown causes now Alberta’s top killer: province. If it isn’t the vaccine, what is causing this?
- There is data from over 1,000 vaccine injured people where 10% of the injured report 30 or more symptoms that are unique to the vaccine injured. How is that possible if the vaccine is so safe? Marsha Gee was perfectly healthy before her COVID vaccine. Less than 1 hour after her first Pfizer shot she experienced severe symptoms and experiences 78 of symptoms common with other vaccine injured. If Marsha wasn’t injured by the COVID vaccine, what caused all these symptoms?
- Why is it illegal to analyze the vaccine vials? Why hasn’t a single medical institution done an analysis of the content of the vaccines to see if there are placebos with saline solution and the amount of mRNA degradation, rendering the vaccines useless? Why the secrecy here? If we knew what was in the vaccines would this cause harm? How?
- Why are prominent people risking their careers to obtain fake vaccine cards? We know top people at Mass General Hospital have fake vaccine cards. We’ve heard that people at the highest levels of the DoD can get fake vaccine cards. It is well known that the CEO of a large pharmaceutical company bought a fake vaccine card. Why would he risk spending years in jail if the vaccines are perfectly safe?
- The Died Suddenly group on Facebook was adding users at 20,000 per day making it the fastest growing group in Facebook history. They had to throttle the growth rate due to attempts by the British military to infiltrate the group to cause it to be shut down.
- The average age of the people reported dead in the Died Suddenly group has been trending younger and younger over time. How can you explain that? The only worldwide massive intervention that goes to younger people is the COVID vaccine.
- The embalmer data (such as The Epoch Times article and this interview). These clots are not blood clots, but they are clots embalmers never saw before mid-2021 (since they take 3 months or more to form into large sizes). If the vaccines are not causing these killer clots, what is? They can be found in up to 93% of the embalming cases.
- Insurance company data from insurance companies worldwide:
- Wayne Root’s wedding: 200 guests, half vaxxed, half unvaxxed. Only the vaxxed got injured (26%) or died (7%). I surveyed my readers and collected data from over 600 readers who collectively reported very similar stats. That’s hard to explain if there isn’t a huge effect.
- My neurologist stats: 11 years without needing to do a single VAERS report; this year, she needs to file 1,000 VAERS reports on 20,000 patients in the practice. How can anyone explain that if the vaccine is perfectly safe with mild, short term effects? This is similar to the 4.5% rate of neurological injury reported earlier by the Israeli Ministry of Health.
- The polling results using third party polling firms (so not my followers) consistently show that more people died from the vaccine than from the virus. The mainstream media refuses to do similar surveys and most survey firms refuse to even ask the questions.
- Ten different surveys I did all showed the vaccines are more harmful than helpful.
- Doctors in Canada died at a rate that was more than 10X normal after getting the fourth dose of the vaccine. And those are just the ones we know about.
- The fact that Paul Offit isn’t going to get the latest booster even though the CDC says he should. Why should any of us take the shot if Paul Offit is refusing to take the shot? He’s arguably the world’s most respected authority on vaccines and sits on the FDA outside advisory committee?
- Why are health authorities removing safety data on the latest shots? If they are so safe, why not release the data?
- Google searches show people became interested in topics related to vaccine safety before they became popular on social media
- When I ask data/statistics experts such as Joel Smalley and Professor Norman Fenton whether they’ve seen any credible data proving the vaccines are safe and effective, they are unable to cite a single reference.
- A local news station (WXYZ-TV) asked people to report on unvaxxed loved ones that became sick and died and instead they got hammered with hundreds of thousands of people saying they lost loved ones to the jab. See my video on the WXYZ-TV story and also this video.
- Woman collapses and dies 7 minutes after Booster shot… The stunning thing is the Twitter video documents that the pharmacy workers have been instructed to not bring it up when briefing patients and, if asked, not to comment on the death. Do you think they are looking out for your best interest by withholding adverse events like death 7 minutes after the shot from the public? That should never happen. Have you ever seen a video like this before the COVID vaccines rolled out? The death was ruled as “natural causes” which means it was from internal organ failure as opposed to being hit by a truck. However, the internal organ failure was due to an external event (vaccinated).
- Turbo-cancer is being reported now. It’s impossible to explain. Never been seen before.
- A reader wrote: I work in the financial services industry in Toronto. A co-worker of mine was recently diagnosed with cancer. He has been getting treated at Sunnybrook hospital for it. The doctors there told him they’ve seen a significant spike in cancer cases well above what could be explained by people missing getting screened due to the pandemic. What’s more though is that they catalogue the vaccine status of every cancer diagnosis and the spike in the number of cases is only occurring in those who are vaccinated– apparently they are researching it to try and find out why the vaxed have seen a spike in cancers vs the unvaxed who haven’t- obviously they are not ready to go public with this but they know about it and are researching it fwiw
- Turtles all the way down: Vaccine science and myth shows the vaccines are not nearly as safe as people think. This is the most damaging book ever written showing the safety of the vaccines is highly questionable. There isn’t a single risk-benefit trial on all cause mortality and morbidity vs. placebo for any of the 70 approved vaccines even though they’ve had 60 years to do this. If the vaccines are truly beneficial, why do you think it’s never been done for any vaccine? A team of Israeli scientists wrote this book over 5 years. It was recently translated into English and is available through purchase on Amazon.
- Dissolving Illusions: the history of vaccines shows they did a lot less than people think; probably next to nothing.
- The Real Anthony Fauci: illustrates the corruption in the medical community today. For example, they created a more accurate adverse event reporting system (ESP:VAERS) system and then scrapped it after it showed all the vaccines were unsafe.
- Vaccine Secrets: a 20 minute slide presentation from CHD
- The CCCA presentations:
- My mega-presentations:
Once I established a policy of always recording calls with “fact checkers,” I’ve not had a single call from them trying to refute anything I’ve written.
None of the drug companies that make these products will refute anything I’ve written or supply a representative to debate me or any of my colleagues in a live debate. They have immunity from liability and they are not willing to be held accountable in the court of public opinion either.
- The COVID lies by Dr. Michael Yeadon
This was a very well done study, but it is of course attacked by the pro narrative people. We’d love to have an open debate about this study, but the other side doesn’t want to talk about it in a neutral forum.
A LITERATURE REVIEW AND META-ANALYSIS OF THE EFFECTS OF LOCKDOWNS ON COVID-19 MORTALITY
Masks don’t work at all. See this article which has plenty of references. If anything, masks are more likely to hurt you than to benefit you.
There is no study at all on the 6 foot distance rule. They just made that one up.
Professor Jeffrey Sachs was tasked by The Lancet to lead an independent investigation into the source of the SARS-CoV-2 virus. After he determined it came from US biotechnology, all of a sudden nobody wanted to pursue the investigation any further.
Tony Fauci gets paid every time you get a Moderna shot. He won’t disclose how much he makes and you can’t get via FOIA (it’s blacked out). If the Republicans get control of the Senate, that will change. Watch this video from Sept 20, 2022 of Rand Paul commenting on this as well as the well founded accusation that Fauci created the virus in the first place and then desperately tried to make it look like it came from nature after top scientists said it was a lab leak (watch the video at 2:00 onwards). Rand Paul called it, quite rightly, “the biggest cover-up in the history of science.”
The question you have to ask yourself is why is Fauci keeping his funding of the gain of function research and also his compensation for each vaccine dose a secret?
Tony Fauci was the primary reason that all early treatments were ignored by the government. It appears he did that because it would cut into his revenue stream.
Early in the pandemic, two physicians, George Fareed and Brian Tyson, developed a treatment protocol using a variety of safe, low cost drugs and supplements with little to no side effects that had a near 100% success track record in preventing hospitalization, death, and long haul COVID if the patient started treatment shortly after realizing they were infected. They’ve treated over 10,000 patients. They wrote a best-selling book about it.
Today, more than two years later, the FDA and the CDC have not returned their calls.
- Why can’t we have open forums where our public health officials can be challenged by experts who disagree? Is there proof that having open debate results in worse outcomes?
- Why doesn’t anyone want to see the Israeli safety data?
- Why isn’t anyone asking for Fauci’s unredacted emails?
- Is there a scientific reason that the CDC is ignoring me and all the experts I work with?
- Questions I’d love to ask Congresswoman Anna Eshoo… that she’ll never answer
- Why hasn’t anyone calculated the minimum VAERS under-reporting factor (URF)?
- Did the propensity to report change in 2021 vs. previous years. What is the new number in 2021 and 2022 compared to previous years? How did you calculate it?
- Why do John Su and Tom Shimabukuro never talk about the URF in the ACIP meetings?
- There were over 14,000 excess deaths reported in VAERS. That’s before the URF is applied. If these weren’t caused by the vaccine, what caused them?
- If these vaccines are so safe, why are there more adverse events reported for these vaccines than for all other vaccines in history combined?
- I found thousands of adverse events that are elevated by these vaccines compared to all other vaccines combined in previous years. How many adverse events did the CDC find?
- There was a dramatic rise in adverse events reported in the VAERS system for the COVID vaccines. How could this not be a serious safety concern? The propensity to report did not increase. If you believe the propensity to report did increase, what data do you have to support that?
- My neurologist has been in practice for 11 years. She has 20,000 patients in her multi-physician practice. In that time, she’s never had to report a single event to VAERS. With the COVID vaccines, she now needs to make 1,000 reports. If the vaccines are safe and effective and most all the symptoms are mild and short term, how do you explain this? Her event rate similar to the 4.5% injury rate that the Israeli MoH found. So her reporting rate is more than 10,000 times higher than for any other vaccine. Couldn’t that be the explanation for the higher rate of VAERS reports? Doesn’t this suggest that the propensity to report is much lower this year because there are so many more events and doctors simply don’t have the time to report them all?
- The NEJM pregnancy paper by Tom Shimabukuro noted that the results on safety for pregnant women was preliminary since many of the women were still pregnant. What was the final result and why wasn’t it published?
- There was an analysis of the VAERS data by Hannah Rosenblum published in the Lancet. It never goes into explaining why there were elevated reporting rates and also the nature of the reported events are not normal background events. Couldn’t the elevated reporting rates be caused by a dangerous vaccine? Does she want to look at the Israeli safety data? If not, why not? The Israeli data directly contradicts the conclusion of the paper. Shouldn’t we figure out which conclusion is correct?
- Why does Carol Crawford not answer my questions about an open discussion with the top vaccine misinformation spreaders to resolve our differences and reduce vaccine hesitancy?
- Why does Martha Sharan ignore my emails and phone messages when I attempted to ask for permission to talk to the authors of the Rosenblum paper? Can’t she reply with the reason questions are not allowed?
Questions I’d love to get the answer to. These were asked, but never answered.
- Why did the CDC never publish the follow up on the NEJM pregnancy paper by Tom Shimabukuro?
- The CEO of Moderna was asked how the 19 nucleotide sequence from a Moderna patent got into the SARS-CoV-2 genome. That sequence is never found in a virus. How did it get in this one? The CEO said he’d look into it, but never reported the explanation. I’d love to know what it was.
- Why hasn’t any Democratic committee chairman asked the NIH for Tony Fauci’s unredacted emails? Don’t we want to know the truth about whether there was a deliberate cover-up? If there was, shouldn’t Fauci be fired?
- Fauci wasn’t supposed to be funding gain of function research but he was. How is he being held accountable?
- How much is Fauci making every time someone gets a Moderna shot? He’s a public official… Why is this a secret?
People who disagree with the mainstream narrative are rewarded with censorship, permanent bans on posting on social media, demonetization of your YouTube account, revocation of your medical license, revocation of your medical certifications, loss of hospital privileges, loss of job, loss of funding, loss of friends, and a Wikipedia entry labeling you a “misinformation spreader” and/or “conspiracy theorist.”
This is a problem. I am not aware of any paper published in the medical literature that shows that such tactics result in better health decisions.
Should we use the same rules at the UN when nations disagree? Do you think that will result in better outcomes?
The way people resolve differences is by confronting the issues and talking through them. But we are not doing this:
- Why can’t we find anyone who will defend the CDC, FDA, and NIH on camera?
- Dr. Byram Bridle and 2 colleagues challenged Canada’s health authorities to a debate
- Vinay Prasad’s most important op-ed
This is objective proof of a broken system. It is indefensible. Caught on video camera. There is no reason that anyone in a position of authority on the COVID vaccines would refuse an opportunity to see the most thorough post-vaccine safety study ever done: one that shows causality of serious adverse events.
From Israeli Investigators Find COVID-19 Vaccines Cause Side Effects: Leaked Video:
Rechallenge changes a causal link “from possible to definitive,” Dr. Mati Berkovitch, head of the research team and a pediatric specialist, said at the meeting.
and
Many of the reported adverse events were found to be long-lasting, which researchers said in the meeting was surprising since the brochure handed to vaccine recipients says otherwise. They also said Pfizer officials told them that Pfizer did not know of any long-lasting symptoms.
and
In the official report later issued to the public, the MoH did not detail how researchers were caught off guard by the duration of the events and side effects. The health agency also stated that there were no new events identified.
It concludes:
The choice to omit some of the crucial findings discussed in the meeting from the public report is “a recipe to destroy” the entire vaccine program, according to Levi, an Israeli native and an expert in risk management.
“The more pro-vaccine, the more disturbed you need to be from something like this,” Levi told The Epoch Times. “And the reason is that the two most important enablers for vaccine programs … to be successful is trust and transparency, that you actually communicate to people the real risk-benefits and allow them to make choices about what they want to do. The second thing is that you take care of the people that were harmed by the vaccine because no vaccine has 100 percent safety.”
“I think we have in this example … where we violate these two very important principles,” he added. “This is a recipe to basically destroy all vaccine programs, so the more pro-vaccine you are, you should be more disturbed by this.”
How can you have the chair of a safety committee not interested in seeing important safety data? Professor Grace Lee should be removed from her position by the CDC. Why isn’t she? Does anyone care?
Why does Dr. Paul Offit ignore requests to see the same data?
According to the Epoch Times article, everyone declined to comment on the story: the scientists, the MOH officials, and the CDC’s Immunization Safety Office declined to comment on the Israeli findings.
If the above isn’t enough, there are hundreds more “hard to explain” data points.
- List of over 1,200 papers published in peer-reviewed scientific journals
- The safe and effective narrative is falling apart
- Think we got it wrong?
- How the authorities can INSTANTLY stop the spread of “COVID misinformation”
- Examining COVID Vaccine Efficacy
There is an excellent article written in August 2020 by Norman Doidge entitled “Medicine’s Fundamentalists” which talks about the “all-available-evidence approach.” It should be read by every doctor in America. This is how medical science should work.
The precautionary principle medicine seems to have been thrown under the bus during the pandemic. It says in the face of uncertainty, one should take reasonable measures to avoid threats that are serious and plausible.
For example, the Pfizer clinical trial showed the vaccine saved only one COVID death per 22,000 injected. That means we might only save around 10,000 lives if we inject 200M Americans. So if VAERS, which is at least 41 times under reported, is showing over 12,000 deaths associated with the vaccine, any reasonable person should say that killing more than 41 people to save 1 life is nonsensical… shouldn’t we put a PAUSE on this intervention until we resolve the uncertainty?
In the current system, questioning the CDC or other authorities results in serious retribution as mentioned earlier.
Is that really the right way to handle scientific dissent?
Are the vaccines “safe and effective” as claimed?
To answer this, science requires that we look at all the available data and see whether the data is more consistent with the hypothesis of “safe and effective” or “not safe and effective.”
All the data that I and my colleagues have seen end up being placed in the “not” bucket.
We are open to being shown we got it wrong on the hundreds of pieces of evidence we have examined, but nobody is willing to discuss the data with us to resolve the issue, not even for $1M dollars.
I even went to extraordinary lengths to offer the Israeli safety data to ACIP Chair Grace Lee. Her response: she called the police on me. That pretty much tells you everything you need to know: they simply refuse to look at any data that goes against their currently held beliefs. That’s the way science works.
Featured Video

Russia and China quietly take over natural gas markets in Asia, with Qatar gone
or go to
Aletho News Archives – Video-Images
Book Review
Palantir CEO Calls for Draft to Fight the Empire’s Wars
Involuntary servitude is good for business
By Kurt Nimmo | Another Day in the Empire | April 20, 2026
In 2025, Alex Karp, the CEO of government and military tech contractor Palantir, published The New York Times best-seller, The Technological Republic: Hard Power, Soft Belief, and the Future of the West. The Wall Street Journal praised the book as a cri de coeur, a passionate appeal “that takes aim at the tech industry for abandoning its history of helping America and its allies,” while Wired praised the book as a “readable polemic that skewers Silicon Valley for insufficient patriotism.”
On April 18, 2026, Palantir posted twenty-two points to social media summarizing the book. In addition to taking Silicon Valley to task for insufficient patriotism, advocating a role for AI in forever war, and denouncing the “psychologization of modern politics,” the Palantir post on X declares: “National service should be a universal duty. We should, as a society, seriously consider moving away from an all-volunteer force and only fight the next war if everyone shares in the risk and the cost.”
National conscription, a form of involuntary servitude, and the wars it portends, is good for business, especially for corporations within the orbit of the Pentagon, the CIA, and the national security state. Palantir fits comfortably within this amalgamation. … continue
Blog Roll
 Aletho News
Aletho News- Palantir CEO Calls for Draft to Fight the Empire’s Wars
- Iran War fallout: Russia and China quietly take over natural gas markets in Asia, with Qatar gone
- Hamas dismisses US-backed disarmament plan as ‘collective suicide’
- Israel’s war obsession and the urgency of Palestinian leverage
- Supply chains breaking: The hidden bottlenecks threatening to bring the global economy to a standstill
- Israel’s Expansion Means An Unraveling of Middle East Stability
- Why has Israel’s Security Doctrine begun targeting Turkey?
- US strikes vessel in Caribbean killing three, death toll reaches 180
- NATO’s Baltic Operation Aims to Curb Russian Cargo Traffic
- France’s New Nuclear Strategy to Weaken Security in Europe – Russian Foreign Ministry
- If Americans Knew
- Israel is (still) killing aid workers in Gaza
- Catholics finally splitting with Trump over Iran war and Israel
- Israel’s “Black Wednesday” Massacre Leaves Lebanese Families Giving DNA To ID Loved One’s Remains
- ‘I Felt I Was a Monster’: IDF Soldiers Talk About the ‘Moral Injury’ – and the Silence
- ‘I thought I might die’: A Palestinian mother’s account of Israeli detention
- Mom whose daughter was killed by Israeli bulldozer 23 years ago pleaded with Congress to finally stop funding
- Israeli soldier takes sledgehammer to Jesus statue in Lebanon – Daily Update
- Israel employs ‘Gaza tactics’ in Lebanon, destroying 1,000 homes per day – Daily Update
- Israel relegates another population to life in tents – Daily Update
- Senate again fails to block weapons to Israel
- No Tricks Zone
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
