Have you heard of the 7-Step Recipe for Generating Interest In, And Demand For Flu (or any other) Vaccination? Back when journalists did some real work, HuffPo’s Laurence Solomon wrote a fascinating expose on the CDC colluding with vaccine makers.
In this interview, which was initially banned by YouTube before it was even published (but now reversed), Spiro is joined by Attorney Ana Garner of New Mexico. Garner represents her client Isaac Legaretta, an officer at the Doña Ana County Detention Center and a military veteran, who is suing the county over its new policy for first responders to receive the COVID-19 vaccinations or face termination.
Attorney Garner explains the significance of this case and what is at stake, as it is the first of its kind and may set a new standard for legal precedent regarding mandatory vaccination. Garner says she is prepared to take this case to the Supreme Court if necessary.
Spiro and Ana Garner also discuss another case of hers that is ongoing currently. A case that challenges not only the Governor of New Mexico, but the emergency itself.
You can see this important interview on the free speech platform BitChute below:
Increasingly, there are serious questions being asked about the factual basis for declaring a pandemic and the growing number of mitigation policies being implemented by governments and corporations. When is a COVID-19 “case” really a case? Moreover, do the case numbers and death numbers that have been touted over the last 12 months by governments in UK, EU, USA, and numerous governments around the world, accurately reflect actual COVID cases and COVID deaths?
In fact, the World Health Organization (WHO) itself has admitted that the entire basis for collating “case” numbers since the beginning of this ‘global pandemic’ is effectively null and void. In its directive published in late January, the organization stated that medical professionals should not be using PCR Testing with high Cycle Threshold (CT) levels due to the high likelihood of generating false positives in people, and also that the PCR Test should not be used as the sole metric for diagnosing and should be accompanied by a professional clinical diagnosis. In other words: the PCR Test cannot rightly be used as a medical diagnostic tool, and yet, it has been widely used as such for the last 12 months. This admission should have grave implications for every public health official, politician and media editor on the planet, but the silence is deafening – as most are simply ignoring this fact.
Description of the problem: WHO requests users to follow the instructions for use (IFU) when interpreting results for specimens tested using PCR methodology.
Users of IVDs must read and follow the IFU carefully to determine if manual adjustment of the PCR positivity threshold is recommended by the manufacturer.
WHO guidance Diagnostic testing for SARS-CoV-2 states that careful interpretation of weak positive results is needed (1). The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient’s viral load. Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology.
WHO reminds IVD users that disease prevalence alters the predictive value of test results; as disease prevalence decreases, the risk of false positive increases (2). This means that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity.
Most PCR assays are indicated as an aid for diagnosis, therefore, health care providers must consider any result in combination with timing of sampling, specimen type, assay specifics, clinical observations, patient history, confirmed status of any contacts, and epidemiological information.
In addition, from the beginning of the ‘pandemic,’ arbitrary and broad guidelines for symptom diagnosis for COVID were being encouraged, and not surprisingly this corresponded with a complete disappearance of season influenza.
Former Minnesota state legislator, Dr Scott Jensen MD, explains why this is absolutely crucial and how we’ve all been played over the last 12 months. Watch:
At first glance, bioethics might seem like just another branch of ethical philosophy where academics endlessly debate other academics about how many angels dance on the head of a pin in far-out, science fiction like scenarios. What many do not know, however, is that the seemingly benign academic study of bioethics has its roots in the dark history of eugenics. With that knowledge, the dangers inherent in entrusting some of the most important discussions about the life, death and health of humanity in the hands of a select few become even more apparent.
For those with limited bandwidth, CLICK HERE to download a smaller, lower file size version of this episode.
For those interested in audio quality, CLICK HERE for the highest-quality version of this episode (WARNING: very large download).
TRANSCRIPT
Bioethics is the study of the moral issues arising from medicine, biology and the life sciences.
At first glance, bioethics might seem like just another branch of ethical philosophy where academics endlessly debate other academics about how many angels dance on the head of a pin in far-out, science fiction like scenarios.
PAUL ROOT WOLPE: Imagine what’s going to happen when we have a memory pill. First of all, you don’t have to raise your hand but let’s be honest: who here’s going to take it?
MICHAEL SANDEL: I’ve read of a sport—it’s a variant of polo that is I think played in Afghanistan if I’m not mistaken—where the people ride on horses. Is it horses or camels? I don’t know which. And they use a—it’s a dead goat or something—to, I don’t know, whack the polo ball or whatever it is. Now it’s a dead—I think it’s a goat. Maybe someone knows who studies sociology about this. So it’s not that the goat is experiencing pain. It’s dead already. And yet there is something grim about that practice, wouldn’t you agree? And yet it’s not that the interests of that goat are somehow not being considered. Let’s assume it was killed painlessly before the match began.
MOLLY CROCKETT: What if I told you that a pill could change your judgement of what is right and what is wrong. Or what if I told you that your sense of justice could depend on what you had for breakfast this morning. You’re probably thinking by now this sounds like science fiction, right?
But the bioethicists cannot be dismissed so lightly. Their ideas are being used by governments to assert control over people’s bodies and to enforce that control in increasingly nightmarish ways.
ARCHELLE GEORGIOU: Lithium is a medication that in prescription doses treats mood disorders in people with bipolar disorder or manic-depressive illness. And what these researchers found in Japan is that lithium is present in trace amounts in the normal water supply in some communities and in those communities they have a lower suicide rate. And so they’re really investigating whether trace amounts of lithium can just change the mood in a community enough to really in a positive way without having the bad effects of lithium to really affect the mood and decrease the suicide rate very interesting concept.
GATES: You’re raising tuitions at the University of California as rapidly as they [sic] can and so the access that used to be available to the middle class or whatever is just rapidly going away. That’s a trade-off society’s making because of very, very high medical costs and a lack of willingness to say, you know, “Is spending a million dollars on that last three months of life for that patient—would it be better not to lay off those 10 teachers and to make that trade off in medical cost?” But that’s called the “death panel” and you’re not supposed to have that discussion.
Even a short time ago, talk about medicating the public through the water supply or enacting death panels for the elderly still seemed outlandish. But now that the world is being plunged into hysteria over the threat of pandemics and overburdened health care systems, these previously unspeakable topics are increasingly becoming part of the public debate.
What many do not know, however, is that the seemingly benign academic study of bioethics has its roots in the dark history of eugenics. With that knowledge, the dangers inherent in entrusting some of the most important discussions about the life, death and health of humanity in the hands of a select few become even more apparent.
This is a study of Bioethics and the New Eugenics.
On November 10, 2020, Joe Biden announced the members of a coronavirus task force that would advise his transition team on setting COVID-19-related policies for the Biden administration. That task force included Dr. Ezekiel Emanuel, a bioethicist and senior fellow at the Center for American Progress.
JOE BIDEN: So that’s why today I’ve named the COVID-19 Transition Advisory Board comprised of distinguished public health experts to help our transition team translate the Biden-Harris COVID-19 plan into action. A blueprint that we can put in place as soon as Kamala and I are sworn into office on January 20th, 2021.
ANCHOR: We’ve learned that a doctor from our area is on the president-elect’s task force. Eyewitness News reporter Howard Monroe picks up the story.
THOMAS FARLEY: I know he’s a very bright, capable guy and i think that’s a great choice to represent doctors in general in addressing this epidemic.
HOWARD MONROE: Philadelphia health commissioner Dr. Thomas Farley this morning on Eyewitness News. He praised president-elect Joe Biden’s transition team for picking Dr. Ezekiel Emanuel to join his coronavirus task force. He is the chair of the Department of Medical Ethics and Health Policy at the University of Pennsylvania.
That announcement meant very little to the general public, who likely only know Emanuel as a talking head on tv panel discussions or as the brother of former Obama chief of staff and ex-mayor of Chicago, Rahm Emanuel. But for those who have followed Ezekiel Emanuel’s career as a bioethicist and his history of advocating controversial reforms of the American health care system, his appointment was an ominous sign of things to come.
He has argued that the Hippocratic Oath is obsolete and that it leads to doctors believing that they should do everything they can for their patients rather than letting them die to focus on higher priorities. He has argued that people should choose to die at age 75 to spare society the burden of looking after them in old age. As a health policy advisor to the Obama administration he helped craft the Affordable Care Act, which fellow Obamacare architect Jonathan Gruber admitted was only passed thanks to the stupidity of the American public.
JONATHAN GRUBER: OK? Just like the people—transparency—lack of transparency is a huge political advantage. And basically, you know, call it the stupidity of the American voter or whatever, but basically that was really critical to getting the thing to pass.
During the course of the deliberations over Obamacare, the issue of “death panels” arose. Although the term “death panel” was immediately lampooned by government apologists in the media, the essence of the argument was one that Emanuel has long advocated: appointing a body or council to ration health care, effectively condemning those deemed unworthy of medical attention to death.
ROB MASS: When I first heard about you it was in the context of an article you wrote right around the time that the Affordable Care Act was under consideration. And the article was entitled “Principles for the Allocation of Scarce Medical Interventions.” I don’t know how many of you remember there was a lot of talk at the time about [how] this new Obamacare was going to create death panels. And he wrote an article which I thought should have been required reading for the entire country about how rationing medical care—you think that that’s going to start with with the Affordable Care Act? Medical care is rationed all the time and it must be rationed. Explain that.
EZEKIEL EMANUEL: So there are two kinds of “rationing,” you might say. One is absolute scarcity leading to rationing and that’s when we don’t simply don’t have enough of something and you have to choose between people. We do that with organs for transplantation. We don’t have enough. Some people will get it, other people won’t and, tragically, people will die. Similarly if we ever have a flu pandemic—not if but when we have a flu pandemic—we’re not going to have enough vaccine, we’re not going to have enough respirators, we’re not going to have enough hospital beds. We’re just going to have to choose between people.
When the debate is framed as an impersonal imposition of economic restraint over the deployment of scarce resources, it is easy to forget the real nature of the idea that Emanuel is advocating. Excluded from these softball interviews is the implicit question of who gets to decide who is worthy of medical attention. Emanuel’s various proposals over the years, and those of his fellow bioethicists, have usually supposed that some government-appointed but somehow “independent” board of bioethicists, economists and other technocrats, should be entrusted with these life-and-death decisions.
If this idea seems familiar, it’s because it has a long and dark history that harkens back to the eugenicists who argued that only the “fittest” should be allowed to breed, and anyone deemed “unfit” by the government-appointed boards—presided over by the eugenicists—should be sterilized, or, in extreme cases, put to death.
GEORGE BERNARD SHAW: [. . .] But there are an extraordinary number of people whom I want to kill. Not in any unkind or personal spirit, but it must be evident to all of you — you must all know half a dozen people, at least—who are no use in this world. Who are more trouble than they are worth. And I think it would be a good thing to make everybody come before a properly appointed board, just as he might come before the income tax commissioner, and, say, every five years, or every seven years, just put him there, and say: “Sir, or madam, now will you be kind enough to justify your existence?”
This is the exact same talk of “Life Unworthy of Life” that was employed in Nazi Germany as justification for their Aktion T4 program, which resulted in over 70,000 children, senior citizens and psychiatric patients being murdered by the Nazi regime.
MODERATOR: So we’ll do the same format. It’ll be three minutes and then time for questions. We’ll start with Mr. Chaitkin.
ANTON CHAITKIN: [My name is] Anton Chaitkin. I’m a historian and the history editor for Executive Intelligence Review.
President Obama has put in place a reform apparatus reviving the euthanasia of Hitler Germany in 1939 that began the genocide there. The apparatus here is to deny medical care to elderly, chronically ill and poor people and thus save, as the president says, two to three trillion dollars by taking lives considered “not worthy to be lived” as the Nazi doctors said.
Dr. Ezekiel Emanuel and other avowed cost-cutters on this panel also lead a propaganda movement for euthanasia headquartered at the Hastings Center, of which Dr. Emanuel is a fellow. They shape public opinion and the medical profession to accept a death culture, such as the Washington state law passed in November to let physicians help kill patients whose medical care is now rapidly being withdrawn in the universal health disaster. Dr. Emmanuel’s movement for bioethics and euthanasia and this council’s purpose directly continue the eugenics movement that organized Hitler’s killing of patients and then other costly and supposedly “unworthy” people.
Dr. Emanuel wrote last October 12 that a crisis, war and financial collapse would get the frightened public to accept the program. Hitler told Dr. Brandt in 1935 that the euthanasia program would have to wait until the war began to get the public to go along. Dr. Emanuel wrote last year that the hippocratic oath should be junked; doctors should no longer just serve the needs of the patient. Hoche and Binding, the German eugenicists, exactly said the same thing to start the killing.
You on the council are drawing up the procedures to be used to deny care which will kill millions if it goes ahead in the present world crash. You think perhaps the backing of powerful men, financiers, will shield you from accountability, but you are now in the spotlight.
Disband this council and reverse the whole course of this nazi revival now.
It should come as no surprise, then, that Emanuel emerged last year as the lead author of a New England Journal of Medicine article advocating for rationing COVID-19 care that was later adopted by the Canadian Medical Association. The paper, “Fair Allocation of Scarce Medical Resources in the Time of Covid-19,” was written by Emanuel and a team of prominent bioethicists and discusses “the need to ration medical equipment and interventions” during a pandemic emergency.
Their recommendations include removing treatment from patients who are elderly and/or less likely to survive, as these people divert scarce medical resources from younger patients or from those with more promising prognoses. Although the authors refrain from using the term, the necessity of setting up a “death panel” to determine who should or should not receive treatment is implicit in the proposal itself.
In normal times, this would have been just another scholarly discussion of a theoretical situation. But these are not normal times. As Canadian researcher and medical writer Rosemary Frei documented at the time, the declared COVID crisis meant the paper quickly went from abstract proposal to concrete reality.
JAMES CORBETT: Let’s get back to that question about hospital care rationing, which is such an important part of this story. And it’s one of those things that when you read it at a surface level at first glance sounds reasonable enough, but the more that you look into it I think it becomes more horrifying.
And you quote, for example, specifically a March 23rd paper, “Fair Allocation of Scarce Medical Resources in the Time of Covid-19,” which was published in the prestigious New England Journal of Medicine, which calls for “maximizing the number of patients that survived treatment with a reasonable life expectancy.” Which, again, I would say sounds reasonable at first glance. Yes, of course we want to maximize the number of patients that survive. What’s wrong with that?
So what can you tell us about this paper and the precedent that it’s setting here.
ROSEMARY FREI: Well it’s all of a sudden changing the rules in terms of saying, “Well, the most important thing is that it’s the older people get a lower place in terms of triaging.”
And I point out in my article, also, that Canadians have a lot of experience with SARS because we had that—there were a significant number of deaths in Ontario because of it. And there were people from Toronto who had direct experience with SARS—which of course is (ostensibly, at least) a cousin with the novel coronavirus—who wrote triaging guidelines, or at least an ethical framework for how to triage during a pandemic—this was in 2006—they didn’t mention age at all. And here we are 14 years later, every single set of guidelines, including this really important New England Journal of Medicine paper say, “Well, age is an important criterion.” And this is what’s interesting.
So this paper is really important because—and also the Journal of the American Medical Association, which is the official organ, I would say, of the American Medical Association says the same thing: it’s age. So they’re all stepping in line and then the Canadian Medical Association said, “Oh, we don’t have time to put our own guidelines together so we’ll just use this one from the New England Journal of Medicine.” To me, that’s astonishing.
When I was a medical writer and journalist, I did some work helping various—one particular organization: the Canadian Thoracic Society, which does, you know, chest infections and stuff. I helped them put together guidelines. There’s a whole big set of organizations for every single specialty for creating guidelines. Yet, “Oh!
We don’t have time to put together this—” And also, I mean Canada had a lot of experience with SARS, so we had a lot of this background. Yet, “Oh, we can’t do so it!” So they gave totally—they, quote, they said we have to go with the recommendations from the New England Journal of Medicine.
That bioethicists like Emanuel are writing papers that are changing the rules for rationing health care in the midst of a generated crisis should hardly be surprising for someone whose brother infamously remarked that you should never let a good crisis go to waste.
RAHM EMANUEL: You never want a serious crisis to go to waste. And what I mean by that, it’s an opportunity to do things you think you could not do before.
But from a broader perspective, it is not at all surprising that the concept of “death panels” has been effectively smuggled in through the back door by the bioethicists.
In fact, when you start documenting the history of bioethics, you discover that this is exactly what this field of study is meant to do: Frame the debate about hot button issues so that eugenicist ideals and values can be mainstreamed in society and enacted in law. From abortion to euthanasia, there isn’t a debate in the medical field that wasn’t preceded by some bioethicist or bioethics institute preparing the public for a massive change in mores, values and laws.
That research into the history of bioethics leads one to the doorstep of the Hastings Center, a nonprofit research center that, according to its website, “was important in establishing the field of bioethics.” The founding director of the Hastings Center, Theodosius Dobzhansky, was a chairman of the American Eugenics Society from 1969 to 1975. Meanwhile, Hastings cofounder Daniel Callahan—who has admitted to relying on Rockefeller Population Council and UN Population Fund money in the early days of the center’s work—served as a director of the American Eugenics Society (rebranded as The Society for the Study of Social Biology) from 1987 to 1992.
As previous Corbett Report guest Anton Chaitkin has extensively documented, there is a line of historical continuity connecting the promotion of eugenics in America by the Rockefeller family in the early 20th century to the creation of the Hastings Center in the late 20th century. The Center, Chaitkin points out, was fostered by the Rockefeller-founded Population Council as a front for pushing the eugenics agenda—including abortion, euthanasia and the creation of death panels—under the guise of “bioethics.”
CHAITKIN: Eugenics practices that we saw and discussions and preparations for eugenics, which were going on in the United States in the early 1920s and earlier going back to the late 19th century—those discussions were carried over—and the same discussions and preparations in England—were carried over into Nazi Germany. After the war—after World War II—people who had participated in these movements wanted to keep the eugenics idea alive and with the backing of particularly the Rockefeller Foundation—which had backed Nazi eugenics before World War II in Europe—they set up a population control movement that overlapped with the Eugenics Society and with eugenics ideas. And out of that combination of eugenics and population control was born the institutes and programs which are today at the heart of what’s called “bioethics,” where you decide—so, supposedly decide—ethical questions in a medical practice based on supposedly limited resources.
So it’s a completely phony and morally disgusting field in general. It’s ill-born at the root of it and it’s a practice which has never confronted—in the medical community and in the academic community that has this as part of its, you know, its practice—they’ve never confronted the basis for the existence of this “bioethics.”
The history of bioethics connects the Rockefeller funding behind the first wave of American eugenics, the Rockefeller funding behind the Kaiser Wilhelm Institutes and the Nazi-era German eugenics program, and the Rockefeller funding behind the Population Council, the Hastings Center and other centres for post-war “crypto-eugenics” research. As a result, it is perhaps not surprising to find that many of the most well-known and most controversial bioethicists working today are associated with the Hastings Center.
Take Ezekiel Emanuel himself. In addition to being a senior fellow at the John Podesta-founded Center for American Progress—which was accused in a 2013 expose from The Nation of maintaining “a revolving door” with the Obama administration and running a pay-for-play operation for various industry lobbyists—Emanuel is also a Hastings Center fellow. In fact, Emanuel’s career as a bioethicist was kickstarted by a November 1996 article in The Hastings Center Report, which—after praising Daniel Callahan’s attempts to inject a debate about the goals of medicine into the discussion of health care—highlighted a point on which both liberals and communitarians can agree: “services provided to individuals who are irreversibly prevented from being or becoming participating citizens are not basic and should not be guaranteed.” For “an obvious example” of this principle in action, Emanuel then cites “not guaranteeing health services to patients with dementia.”
Just last year, The Hastings Center hosted an online discussion about “What Values Should Guide Us” when considering COVID-19 pandemic restrictions in the United States, during which Emanuel opined that big tech was not doing enough to share data about users’ movements with governments and researchers:
EMANUEL: I have to say I’ve actually found Big Tech totally unhelpful so far in this. It’s hard for me to see that they’ve done something really, really helpful in this regard when it comes to COVID-19. They have lots of capacity. Believe me: Facebook already knows who you interact with on a regular basis; how close you’ve gotten to them; when you leave your house; which stores you go into. Google does the same. And they have not used this data. Maybe they’re afraid that people are going to be all upset, but they haven’t even been willing to give it to someone else to use in an effective manner. And I think either they’re going to become irrelevant in this process or they’re going to have to step up and actually be contributory to solving this problem.
Or take Hastings Center fellow and University of Wisconsin-Madison bioethics professor Norman Fost, who, in addition to questioning whether it is “important that organ donors be dead” in the Kennedy Institute of Ethics Journal, made the case for involuntary sterilization—the hallmark of the now universally denounced American eugenics program—at a 2013 panel discussion on “Challenging Cases in Clinical Ethics.”
NORMAN FOST: On the sterilization thing, if his sexual behavior can be attenuated so that he’s not a risk of impregnating anybody that would be the best thing. But I don’t think we should rule out sterilization as being in his interest also, as well as potential victims of his sexual assault.
I think sterilization has a bad reputation in America because of the eugenic sterilization of a hundred thousand or more people with developmental disabilities, most of them inappropriate. But the overreaction to that . . . and Wisconsin leads the way at overreacting to that. We have a Supreme Court decision that says you can never sterilize a minor until the legislature gives us permission to do it and they never will and that’s not in the interest of a lot of kids with developmental disabilities for whom procreation would be a disaster—that is pregnancy or inflicting a pregnancy.
So if it’s the case that this fella is never going to be capable of being a parent . . . and I can’t tell quite that from the limited history here and it may not be the case—but I just want to say that the country’s overreaction to sterilization—like it’s wrong, it’s always terrible to involuntarily sterilized somebody—is not true and it ought to be at least on the table as something that might be in his interest.
But these discussions are not limited to the ranks of the Hastings Center.
Take Joseph Fletcher. Dubbed a pioneer in the field of biomedical ethics by both his critics and his apologists, Fletcher was the first professor of medical ethics at the University of Virginia and co-founded the Program in Biology and Society there. In addition to his position as president of the Euthanasia Society of America and his work helping to establish the Planned Parenthood Federation, Fletcher was also a member of the American Eugenics Society. In a 1968 article in defense of killing babies with Down’s syndrome “or other kind[s] of idiot[s],” Fletcher wrote:
“The sanctity (what makes it precious) is not in life itself, intrinsically; it is only extrinsic and bonum per accident, ex casu – according to the situation. Compared to some things, the taking of life is a small evil and compared to some things, the loss of life is a small evil. Death is not always an enemy; it can sometimes be a friend and servant.”
Or take Peter Singer. If there is any bioethicist in the world today whose name is known to the general public it is Peter Singer, famed for his animal liberation advocacy. Less well known to the public, however, are his arguments in favor of infanticide, including the notion that there is no relevant difference between abortion and the killing of “severely disabled infants,” positions which have driven his critics to call him “Son of Fletcher.”
Although Singer is extremely careful to frame his argument for infanticide using the least controversial positions when speaking to the public. . . .
PETER SINGER: . . . So we said, “Look, the difficult decision is whether you want this infant to live or not.” That should be a decision for the parents and doctors to make on the basis of the fullest possible information about what the condition is. But once you’ve made that decision it should be permissible to make sure that the baby dies swiftly and humanely, if that’s your decision. If your decision is that it’s better that the child should not live, it should be possible to ensure that the child dies swiftly and humanely.
And so that’s what we proposed. Now, that’s been picked up by a variety of opponents, both pro-life movement people and people in the militant disability movement—which incidentally didn’t really exist at the time we first wrote about this issue. And they’ve taken us as, you know, the stalking horse—the bogeyman, if you like—because we’re up front in saying that we think this is how we should treat these infants.
. . . his actual writings contain much bolder assertions that would be sure to shock the sensibilities of the average person if they were plainly stated. In Practical Ethics, for example, intended as a text for an introductory ethics course, Singer dispenses with arguments about severe handicaps and birth defects and talks more broadly about whether it is fundamentally immoral to kill a newborn baby, noting that “a newborn baby is not an autonomous being, capable of making choices, and so to kill a newborn baby cannot violate the principle of respect for autonomy.”
After conceding that “It would, of course, be difficult to say at what age children begin to see themselves as distinct entities existing over time”—noting that “Even when we talk with two or three year old children it is usually very difficult to elicit any coherent conception of death”—we could provide an “ample safety margin” for such concerns by deciding that “a full legal right to life comes into force not at birth, but only a short time after birth—perhaps a month.”
Singer is by no means alone in his profession in discussing this subject. In fact, he’s just part of a long line of bioethicists musing about exactly where to draw the line when discussing infanticide.
Take Alberto Giubilini and Francesca Minerva, two bioethicists working in Australia who published a paper titled “After-birth abortion: why should the baby live?” in The Journal of Medical Ethics in 2012. In that paper, they explicitly defend the practice of infanticide on moral grounds, claiming that “The moral status of an infant is equivalent to that of a fetus,” and thus “the same reasons which justify abortion should also justify the killing of the potential person when it is at the stage of a newborn.” Lest they be mistaken for forwarding the same old argument on killing severely handicapped newborn babies that bioethicists have been making for decades, the two are careful to add that their proposal includes “cases where the newborn has the potential to have an (at least) acceptable life, but the well-being of the family is at risk.”
Seemingly taken aback by the strong negative reaction to a scholarly article about the moral permissibility of killing babies, the authors of the article responded by accusing the general public of being too ignorant to understand the complex arguments made in the highly academic field of bioethics:
When we decided to write this article about after-birth abortion we had no idea that our paper would raise such a heated debate.
“Why not? You should have known!” people keep on repeating everywhere on the web. The answer is very simple: the article was supposed to be read by other fellow bioethicists who were already familiar with this topic and our arguments. Indeed, as Professor Savulescu explains in his editorial, this debate has been going on for 40 years.
Whatever else may be said about the researchers’ response, this was not a dishonest defense of their work. Julian Savulescu, the editor of The Journal of Medical Ethics that published the article, did point out in his own defense of the publication that the scholarly debate about when it is permissible to kill babies goes back to at least the 1960s, when Francis Crick—the co-discoverer of the structure of DNA and an avowed eugenicist who proposed that governments should prevent the poor and undesirable from breeding by requiring government-issued licenses for the privilege of having a baby—proposed that children should only be allowed to live if, after birth, they are found to have met certain genetic criteria.
Indeed, the pages of the medical ethics journals are filled with just such debates. From Dan Brock’s article on “Voluntary Active Euthanasia,” published in The Hastings Center Report in 1992, to John Hardwig’s 1997 article in the pages of The Hastings Center Report asking “Is There A Duty to Die?” to Hastings Center Deputy Director Nancy Berlinger’s 2008 pronouncement that “Allowing parents to practice conscientious objection by opting out of vaccinating their children is troubling in several ways,” these ethics professors toiling in a hitherto unknown and unremarked corner of academia are having a greater and greater effect in steering the policies that literally mean the difference between life and death for people around the world.
Thousands of medical ethicists and bioethicists, as they are called, professionally guide the unthinkable on its passage through the debatable on its way to becoming the justifiable until it is finally established as the unexceptionable. Those who pause too long to ponder troubling questions along the way are likely to be told that “the profession has already passed that point.” In truth, the profession is usually huffing and puffing to catch up with what is already being done without its moral blessing.
Indeed, bioethicists are not, generally speaking, trained doctors, researchers or medical workers. As academics, they are forced to take the word of doctors and researchers at face value. But which doctors? Whose research? Inevitably, it will be that of the WHO, the AMA and other organizations whose work—as even those within its ranks admit—is not solely dictated by medical need, but by the arbitrary whims of the organizations’ billionaire backers.
We are feeling the effects of this now, when these bioethics professors are held up as gurus who can not only provide medical advice, but actually lecture the public on which medical interventions they are morally obligated to undergo regardless of their own feelings about bodily autonomy.
JULIAN SAVULESCU: It’s important to recognize that mandatory vaccination would not be anything new. There are many mandatory policies, other coercive policies—taxes are a form of coercion. Seatbelts were originally voluntary and they were made mandatory because they both reduce the risk of death to the wearer by 50% and also to other occupants in the car. But importantly some people do die of seat belt injuries, but the benefits vastly outweigh the risks.
Some countries in the world already have mandatory vaccination policies. In Australia the “no jab, no pay” policy involves withholding child care benefits if the child isn’t vaccinated. In Italy there are fines. And in the US children can’t attend school unless they’re vaccinated. All of these policies have increased vaccination rates and have been implementable.
KERRY BOWMAN: Some form of vaccination passport is almost inevitable. With travel it’s virtually a given. And you look at countries like Israel is now introducing the green card. And all this is going on the assumption that people that have been vaccinated are not going to be able to spread the viruses easily, meaning they can’t transmit it and it’s kind of looking like my read on the science is it’s looking like that is the case with most of the vaccines. So that would be the question.
Now some people say we absolutely can’t do it, like, it’s just not fair in a democratic society because there’s people that refuse—don’t want vaccines—and there’s people that can’t have vaccines. But here’s the other side of the argument: Is it really fair to the Canadians that have been locked down for a year when they are vaccinated—they’re no longer a risk to other people—is it really fair to continue to limit their freedom?
So you’ve kind of got those two sides of it colliding.
From its inception, the field of bioethics has taken its moral cue from the card-carrying eugenicists who founded its core institutions. For these academicians of the eugenics philosophy, the key moral questions raised by modern medical advances are always utilitarian in nature: What is the value that forced vaccination or compulsory sterilization brings to a community? Will putting lithium in the water supply lead to a happier society? Does a family’s relief at killing their newborn baby outweigh that baby’s momentary discomfort as it is murdered?
Implicit in this line of thinking are all of the embedded assumptions about what defines “value” and “happiness” and “relief” and how these abstract ideas are measured and compared. The fundamental utilitarian assumption that the individual’s worth can or should be measured against some arbitrarily defined collective good, meanwhile, is rarely (if ever) considered.
The average person, however—largely unaware that these types of questions are even being asked (let alone answered) by bioethics professors in obscure academic journals—may literally perish for their lack of knowledge about these discussions.
All things being equal, these types of ideas would likely be treated as they always have been: as a meaningless parlor game played by ivory tower academics with no power to enforce their crazy ideas. All things, however, are not equal.
Perhaps taking a page from the notebook of his brother, Rahm, about the utility of crisis in effecting societal change, Ezekiel Emanuel declared in 2011 that “we will get health-care reform only when there is a war, a depression or some other major civil unrest.” He didn’t add “pandemic” to that list of excuses, but he didn’t have to. As the events of the past year have borne out, the public are more than willing to consider the previously unthinkable now that they have been told that there is a crisis taking place.
Forced vaccination. Immunity passports. The erection of a biosecurity state. For the first time, the eugenics-infused philosophers of bioethics are on the verge of gaining real power. And the public is still largely unaware of the discussions that these academics have been engaged in for decades.
At the very least, Bill Gates can relax now: We can finally have the discussion on death panels.
Twice in the last six weeks, warnings were issued about imminent, grave threats to public safety posed by the same type of right-wing extremists who rioted at the Capitol on January 6. And both times, these warnings ushered in severe security measures only to prove utterly baseless.
First we had the hysteria over the violence we were told was likely to occur at numerous state capitols on Inauguration Day. “Law enforcement and state officials are on high alert for potentially violent protests in the lead-up to Inauguration Day, with some state capitols boarded up and others temporarily closed ahead of Wednesday’s ceremony,” announcedCNN. In an even scarier formulation, NPR intoned that “the FBI is warning of protests and potential violence in all 50 state capitals ahead of President-elect Joe Biden’s inauguration.”
The resulting clampdowns were as extreme as the dire warnings. Washington, D.C. was militarized more than at any point since the 9/11 attack. The military was highly visible on the streets. And, described The Washington Post, “state capitols nationwide locked down, with windows boarded up, National Guard troops deployed and states of emergency preemptively declared as authorities braced for potential violence Sunday mimicking the Jan. 6 attack on the U.S. Capitol by a mob of pro-Trump rioters.” All of this, said the paper, “reflected the anxious state of the country ahead of planned demonstrations.”
But none of that happened — not even close. The Washington Postacknowledged three weeks later:
Despite warnings of violent plots around Inauguration Day, only a smattering of right-wing protesters appeared at the nation’s statehouses. In Tallahassee, just five armed men wearing the garb of the boogaloo movement — a loose collection of anti-government groups that say the country is heading for civil war — showed up. Police and National Guard personnel mostly ignored them.
All over the country it was the same story. “But at the moment that Biden was taking the oath of office in Washington, the total number of protesters on the Capitol grounds in Topeka stood at five — two men supporting Trump and two men and a boy ridin’ with Biden,” reportedThe Wichita Eagle (“With Kansas Capitol in lockdown mode, Inauguration Day protest fizzles). “The protests fizzled out after not many people showed up,” reported the local Florida affiliate in Tallahassee. “The large security efforts dwarfed the protests that materialized by Wednesday evening,” saidCNN, as “state capitols and other cities remained largely calm.”
Indeed, the only politically-motivated violence on Inauguration Day was carried out by Antifa and anarchist groups in Portland and Seattle, which caused some minor property damage as part of anti-Biden protests while they “scuffled with police.” CNN, which spent a full week excitedly hyping the likely violence coming to state capitols by right-wing Trump supporters, was forced to acknowledge in its article about their non-existence that “one exception was Portland, where left-wing protesters damaged the Democratic Party of Oregon building during one of several planned demonstrations.”
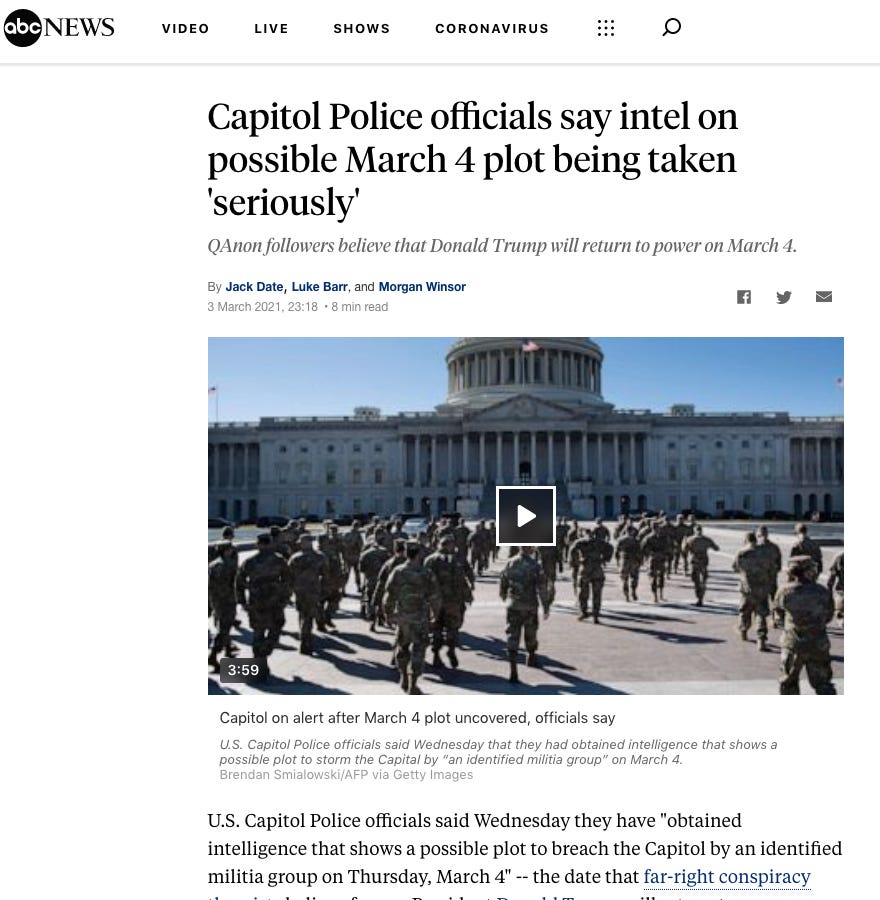
Completely undeterred by that debacle, Democrats and their media spokespeople returned with a new set of frightening warnings for this week. The date of March 4 has taken on a virtually religious significance for the Q-Anon movement, announced NBC News’ Ben Collins, who was heard on NPR on Thursday speaking through actual, literal journalistic tears as he recounted all the times he called Facebook to plead with them to remove dangerous right-wing extremists on their platform(tears commence at roughly 7:00 minutes in). Valiantly holding back full-on sobbing, Collins explained that he proved to be so right but it pains and sorrows him to admit this. With his self-proclaimed oracle status fully in place, he prophesized that March 4 had taken on special dangers because Q-Anon followers concluded that this is when Trump would be inaugurated.
This is how apocalyptic cult leaders always function. When the end of the world did not materialize on January 6, Collins insisted that January 20 was the day of the violent reckoning. When nothing happened on that day, he moved the Doomsday Date to March 4. The flock cannot remain in a state of confusion for too long about why the world has not ended as promised by the prophet, so a new date must quickly be provided with an explanation for why this is serious business this time.
This March 4 paranoia was not confined to NBC’s resident millennial hall monitor and censorship advocate. On March 3, The New York Times warned that “the Capitol Police force is preparing for another assault on the Capitol building on Thursday after obtaining intelligence of a potential plot by a militia group.” All this, said the Paper of Record, because “intelligence analysts had spent weeks tracking online chatter by some QAnon adherents who have latched on to March 4 — the original inauguration date set in the Constitution — as the day Donald J. Trump would be restored to the presidency and renew his crusade against America’s enemies.”
These dire warnings also, quite predictably, generated serious reactions. “House leaders on Wednesday abruptly moved a vote on policing legislation from Thursday to Wednesday night, so lawmakers could leave town,” said the Times. We learned that there would be further militarization of the Capitol and troop deployment in Washington indefinitely due to so-called “chatter.” NPRannounced: “The House of Representatives has canceled its Thursday session after the U.S. Capitol Police said it is aware of a threat by an identified militia group to breach the Capitol complex that day.”
Do you know what happened on March 4 when it came to violence from right-wing extremists? The same thing that happened on January 20: absolutely nothing. There were no attempted attacks on the Capitol, state capitols, or any other government institution. There was violent crime registered that day in Washington D.C. but none of it was political violence by those whom media outlets warned posed such a grave danger that Congress has to be closed and militarization of Washington extended indefinitely.
Perhaps the most significant blow to the maximalist insurrection/coup narrative took place inside the Senate on Thursday. Ever since January 6, those who were not referring to the riot as a “coup attempt” — as though the hundreds of protesters intended to overthrow the most powerful and militarized government in history — were required to refer to it instead as an “armed insurrection.”
This formulation was crucial not only for maximizing fear levels about the Democrats’ adversaries but also, as I’ve documented previously, because declaring an “armed insurrection” empowers the state with virtually unlimited powers to act against the citizenry. Over and over, leading Democrats and their media allies repeated this phrase like some hypnotic mantra:
But this was completely false. As I detailed several weeks ago, so many of the most harrowing and widespread media claims about the January 6 riot proved to be total fabrications. A pro-Trump mob did not bash Office Brian Sicknick’s skull in with a fire extinguisher. No protester brought zip-ties with them as some premeditated plot to kidnap members of Congress (two rioters found them on a table inside). There’s no evidence anyone intended to assassinate Mike Pence, Mitt Romney or anyone else.
Yet the maximalist narrative of an attempted coup or armed insurrection is so crucial to Democrats — regardless of whether it is true — that pointing out these facts deeply infuriates them. A television clip of mine from last week went viral among furious liberals calling me a fascism supporter even though it did nothing but point out the indisputable facts that other than Brian Sicknick, whose cause of death remains unknown, the only people who died at the Capitol riot were Trump supporters, and that there are no known cases of the rioters deliberately killing anyone.
(Two FBI operatives have since anonymously leaked that it is looking at a “suspect” who may have engaged with Sicknick in a way that ultimately contributed to his death. But nothing still is known; Sicknick’s mother claims he died of a stroke while his brother says it was from pepper spray; and all of this is worlds away from the endlessly repeated media claim that a bloodthirsty pro-Trump mob savagely bashed his head in with a fire extinguisher.)
What we know for sure is that no Trump supporter fired any weapon inside the Capitol and that the FBI seized a grand total of zero firearms from those it arrested that day — a rather odd state of affairs for an “armed insurrection,” to put that mildly. In questioning from Sen. Ron Johnson (R-WI) on Thursday’s hearing, a senior FBI official, Jill Sanborn, acknowledged this key fact:
(The “one lady” who died referred to by this FBI official was Ashli Babbitt, an unarmed Trump supporter who was killed when she was shot point blank in the neck inside the Capitol on January 6 by an armed Capitol Police Officer).
The key point to emphasize here is that threats and dangers are not binary: they either exist or they are fully illusory. They reside on a spectrum. To insist that they be discussed rationally, soberly and truthfully is not to deny the existence of the threat itself. One can demand a rational and fact-based understanding of the magnitude of the threat revealed by the January 6 riot without denying that there is any danger at all.
Those who denounced the excesses of McCarthyism were not insisting that there were no Communists in government; those denouncing the excesses of the Clinton administration’s attempts to seize more surveillance power after the Oklahoma City court bombing were not denying that some anti-government militias may do violence again; those who objected to the protracted and unhinged assault on civil liberties by the Bush/Cheney and Obama administrations after 9/11 were not arguing that there were no Muslim extremists intent on committing violence.
The argument then, and the argument now, is that the threat was being deliberately inflated and exaggerated, and fears stoked and exploited, both for political gain and to justify the placement of more and more powers in the hands of the state in the name of stopping these threats. That is the core formula of authoritarianism — to place the population in a state of such acute fear that it acquiesces to any assertion of power which security state agencies and politicians demand and which they insist are necessary to keep everyone safe.
There is, relatedly, a massive political benefit from convincing the population that the opponents and critics of those in power do not merely hold a different ideology but are coup plotters, insurrectionists, domestic terrorists. That is the same political benefit that accrued from trying to persuade the population that adversaries of the Democratic Party were treasonous Kremlin agents. The more you can demonize your opponents as something monstrous, the more political power you can acquire.
And as Democrats and liberals now gear up to demand a new War on Terror, this one domestic in nature, it should be no surprise that the rhetorical leaders of their effort now are the same lowlife neocon and Rovian slanderers — Bill Kristol, David Frum, Steve Schmidt, Nicolle Wallace, Rick Wilson — who demonized everyone who questioned them as part of the first War on Terror as traitors and terrorist-lovers and subversives. It is not a coincidence that neocons are leading the way now as liberals’ favorite propagandists: they are the most skilled and experienced in weaponizing and exaggerating terrorism threats for political gain and authoritarian power.
Ultimately, if this “armed insurrection” and threat of domestic terrorism are so grave, why do media figures and politicians in both parties — from Adam Schiff to Liz Cheney — keep lying about it and peddling fictions? Politicians and media figures do that only when they know that the threat, in reality, is not nearly as menacing as they need it to be to fulfill their objectives of political gain and coercive power.
The Governor of TX announced he’s opening up The Lone Star State 100%, enraging the mainstream media. The motivation may be political, but numbers don’t lie. Del breaks down the data on three key states, California, New York, and Florida, to reveal what possibly led Gov. Abbott to make such a controversial decision.
“THIS COULD HAVE SAVED 450,000 LIVES”
ER doc, Richard Bartlett, made waves last year with a viral video about his incredible success treating #Covid19 patients with a common asthma inhalant. After being vilified by the media and Fauci himself, recent studies, including one out of Oxford University, have validated his claim, stating that 90% of hospitalizations could have been avoided with this simple, early treatment.
The world has been fixated for months on novel-coronavirus PCR testing, contact tracing and vaccination.
Meanwhile, another major part of the Covid biomedical complex has received far less attention: the use of antibodies for detecting, diagnosing and treating infection with the novel coronavirus.
Hundreds of antibodies have been approved for these purposes since January 2020. And hundreds more are poised to start being marketed soon.
This is part of the biomedical gold rush: by last summer already, antibodies were on track to become the most lucrative medical product, with global revenue projected to reach nearly half a trillion dollars by 2024. Profit margins in the range of 67% aren’t uncommon.
Pharma giants such as AstraZeneca, Novartis, GlaxoSmithKline and Eli Lilly are among the companies grabbing the largest chunks of the novel-coronavirus-antibody market. And some of the most muscular government agencies, including Anthony Fauci’s US National Institute of Allergy and Infectious Diseases and the US’s Defense Advanced Research Projects Agency, are part of the action (see, for example, the second-last section of this article, on antibodies used to treat Covid).
Virtually every study and piece of marketing material related to Covid is premised on scientists having positively and correctly identified the presence of the novel coronavirus (also known as SARS-CoV-2) in the material they’re working with.
The job of that identification is usually given to antibodies that are said to bind to the novel coronavirus. The assumption is these antibodies are able to pick out the virus and only the virus from among every other organism and substance surrounding it.
Unfortunatelyit turns out that the antibodies rarely (if ever) do that. This is because of, among other things, inadequateverification of the antibodies’ accuracy in targeting the virus by the companies that manufacture and sell them. And there’s even less verification by government regulators.
Let’s take a 30,000-foot tour of a couple of the main features of the antibody-industry landscape, which is awash in complexity and cash.
Can Antibodies be Created That Only Bind to One Type of Virus or Another?
Antibodies are tiny, finely-tuned, parts of our immune system. One of their main functions is to seek out viruses and bacteria that may have the potential to cause disease. Antibodies bind to and neutralize these microbes so they can’t multiply and spread.
Humans and our ancestors have been making antibodies in our bodies to fend off infections for millions of years. Then a few decades ago companies got involved in the discovery and manipulation of antibodies, partnering with university labs.
There are two main categories of antibodies. One is ‘polyclonal’ antibodies. These are garden-variety antibodies that bind to a variety of different substances and/or organisms.
The other is monoclonal antibodies. As the name implies, cloning is involved in their creation. First an antibody that is specific to a particular amino-acid sequence (amino acids are the building blocks of proteins) of interest – for example, one from a protein on the surface of a virus or bacterium — is identified. Then the immune-system cell which produced that antibody is ‘cloned’ in the lab. As a result, each set of monoclonal antibodies binds to that particular amino-acid sequence.
I emailed one of the English-speaking world’s leading authorities on monoclonal antibodies, Harvard Medical School professor Clifford Saper, to get clarity on this. I asked him if it’s true that, as most in the antibody-commercializing arena claim, a monoclonal antibody can be created that’s specific for (that is, binds to) just one type of virus or just one other type of organism.
Saper replied [bolding and italics added by me for emphasis]: “No, there is no such thing as a monoclonal antibody that, because it is monoclonal, recognizes only one protein or only one virus. It will bind to any protein having the same (or a very similar) sequence.”
The implication of Saper’s statement is that any attempt to use a monoclonal antibody to verify the presence of the novel coronavirus will yield a large rate of false-positive results. That is, they will indicate that the novel coronavirus is detected when in fact it hasn’t been. That’s because there’s a high probability that the monoclonal antibody is binding to something else besides the virus (this is known as ‘cross-reacting’).
(I recommend this review paper by Saper, and this one and this one co-authored by Yale pathology professor David Rimm, to anyone wishing to learn about antibody validation.)
And in fact, the vast majority of antibodies and monoclonal antibodies marketed as being specific for the novel coronavirus were developed years ago fordetecting SARS-CoV-1. They were then simply repurposed for identifying SARS-CoV-2 — with very few if any checks for whether they also cross-react to other organisms or substances.
I sought confirmation of this repurposing from Zhen Lu. She’s the North American marketing manager for Sino Biological, a Beijing-headquartered company that develops and sells, among other things, hundreds of antibodies. Lu replied to me via email, “Yes, antibodies are repuposed [sic].”
I also checked and received confirmation from Pratiek Matkar, a senior staffer from BenchSci, an antibody-database company. And to see for myself, I logged into the BenchSci database (Matkar granted me a guest account), selected all antibodies for the novel coronavirus, and looked to see which organisms had been used in cross-reactivity tests for them. SARS-CoV-1 was the only one that came up in this check.
This all explains something I observed last week: Sino Biological had just changed the content of its home page for the section of their website on antibodies against SARS-CoV-2. The page now announces that they’ve introduced new “matched antibody pairs” that work better at finding the virus. The pair consists of a “capture antibody” and a “detection antibody.”
And they claim these pairs are more accurate at finding the novel coronavirus: that they “have high specificity without cross-reactivity with MERS-CoV, [or with the common human coronaviruses] 229E, NL63, HKU1, [and] OC43.”
The only way I can interpret that is they know the antibodies they’ve been marketing for months as being specific for the novel coronavirus bind to other things, such as common human coronaviruses.
How Are Antibodies Harnessed in Tests for the Novel Coronavirus?
One of the main types of tests for the virus contains antibodies that are ostensibly specific for the novel coronavirus. The way they’re designed to work is that if the virus is present in a blood sample the antibodies bind to it and, as a result, the test gives a positive signal.
The other type of test contains sequences of protein from the novel coronavirus; if antibodies to the virus are present in a blood sample, they bind to the protein sequences and produce a positive result.
The manufacturers are supposed to conduct accuracy checks of their test kits before they put them on the market. These checks largely consist of estimation of the rates of false positives and false negatives (the latter is a negative result when the antibody or protein of interest is contained in the sample being tested by the kit).
However, companies do this cursory accuracy check with only very few samples of a small number of viruses — and rarely on bacteria or any other of the millions of biological substances that can be present in the blood.
Despite this very inadequate validation and the strong incentive for the companies to make their products look good, as documented last May by David Crowe, the manufacturers often record a significant rate of false positives. The false positives areto everything from West Nile virus to various types of human coronaviruses.
Usually the companies and governments wave that off as insignificant. Occasionally though, the test kits are so bad that they’re taken off the market.
For example, an antibody-testing kit sold by a company called Chembio Diagnostics was launched on March 31, 2020. It was almost immediately granted Emergency Use Authorization (EUA) by the US Food and Drug Administration (FDA). An EUA allows companies to rush products onto the market with very minimal oversight. Brazil and the European Union also gave the nod for the Chembio test to be sold in their jurisdictions in April and May 2020, respectively.
Then in June 2020 the FDA pulled it off the market.The agency said ”this test generates a higher than expected rate of false results.” (Note that the top table on page 13 of the product insert for that “revoked” Chembio test indicates it cross-reacts to the human coronavirus 229E.)
Is it identical to the rest that was so inaccurate it was pulled off the market last June? It’s hard to tell. There is no product insert for it that I could find. In fact there’s very little information about it on the webpage for the test; you have to request the information. I submitted a request on Jan. 23 and haven’t received it yet.
Two of the heads of the FDA branch that approves testing devices penned a February 18, 2021, New England Journal of Medicine article. In it, the pair admitted that the FDA’s EUAs allowed too-loose approvals for serology tests.
They indicated the FDA has tightened its criteria for approval of these tests. They also point to efforts by other government agencies to evaluate serology tests. But the pair don’t say a word about the need to move toward objective, thorough test validation. They also are mute on the fact that EUAs are still being issued.
(Also note that the FDA and Health Canada listings of the 65 serology tests approved to date in the US and 19 approved to date in Canada continue to give the sensitivity [correct identification of positive samples] of the tests by ‘positive percent agreement’ and specificity [correct identification of negative samples] by ‘negative percent agreement.’ These are relative measures of accuracy – that is, compared to other tests – rather than objective/absolute accuracy, and therefore are poor facsimiles of accuracy.)
One of the many major figures in the Covid-biomedical complex who are priming the pump of the antibody pipeline is Ian Lipkin. He’s director of the Center for Infection and Immunity at Columbia University in New York. Lipkin is involved at high levels in many global organizations including the World Health Organization and the Bill & Melinda Gates Foundation, as well in pharmaceutical companies. (And he is quoted in a ‘fact-check’ of a July 2020 article I co-authored with Patrick Corbett titled, “No one has died from the coronavirus.” Lipkin states, among other things, in the fact-check piece that “Conspiracy theorists are not persuaded by data.”)
Lipkin co-authored a Feb. 12, 2021, paper in which he and his team claimed to have identified, using a new ‘peptide-microarray’ technology they invented, 29 amino-acid sequences unique to the novel coronavirus. They assert that antibodies specific to the sequences could be created – and that these in turn could be harnessed “to facilitate diagnostics, epidemiology, and vaccinology” for Covid. (The only conflict Lipkin and some of his co-authors disclose in the ‘competing interests’ paragraph at the end of article is that they invented the peptide-microarray technology described in the article.)
Do Antibodies Used to Treat Covid Fare Any Better?
Antibodies are also being marketed to treat Covid. Some are sold singly (known as ‘monotherapy’) and others in pairs. They are deemed to confer ‘passive immunity.’
Among the most-reported-on set of antibodies for treating Covid is the Regeneron monoclonal antibodies casirivimab and imdevimab. This pair reportedly was used in October 2020 to treat then-U.S. President Donald Trump. The combo subsequently was granted an EUA by the FDA on November 21, 2020. It also is being considered for approval by Health Canada.
I’d like to focus on a somewhat lesser-known monoclonal antibody called bamlanivumab. It’s being used both singly and as one half of a pair for treatment of symptomatic Covid patients early in the course of their infection. The antibody was discovered, and clinical study of it started, by the US National Institute of Allergy and Infectious Diseases (which is headed by Anthony Fauci) and a Vancouver, British Columbia-based company called AbCellera Diagnostics. The antibody is being manufactured and sold by Eli Lilly. It costs more than $1,200 a vial.
(AbCellera also has received hundreds of millions of dollars from the Canadian government, including for building an antibody-manufacturing plant. And Peter Thiel, who co-founded both PayPal and Palantir, is a board member. So is John Montalbano, who’s also on the board of the Canada Pension Plan Investment Board and until 2015 was CEO of RBC [Royal Bank of Canada] Global Asset Management. This and significant positive media coverage helped propel the company to the biggest Canadian-biotech-company Initial Public Offering to date, on Dec. 11, 2020.)
Bamlanivumab was given an EUA by the FDA on November 9, 2020, for treatment of mild to moderate Covid. And Health Canada gave the monotherapy an interim authorization on November 17. It’snot getting much tractionin clinical practice so far in Canada, though, perhaps because of the less-than-stellar results from clinical trials (see below).
But this hasn’t deterredthe Canadian and US federal governments, which combined have purchased close to half a million of these tests. For example, most recently, on February 26, the US government bought 100,000 vials.
The only study on bamlanivimab made public prior to the November 9 FDA approval was one posted October 1, 2020, on the website of the online-only journal bioRχiv. [My Feb. 3, 2021, and Feb. 11, 2021, articles — on the new variants and the associated modelling papers, respectively – noted that the journal and its sister publication medRχiv contain only non-peer-reviewed articles and were created by an organization headed by Mark Zuckerberg and his wife.]
The study used rhesus monkeys and provided very extensive details about how the antibody was discovered and checked for specificity to the novel coronavirus. The researchers concluded that the antibody – at that time known as LY-CovV555 — has “potent neutralizing activity” against SARS-CoV-2.
On January 14 I emailed the lead author of that paper, Bryan Jones. He’s a researcher in Lilly’s Biotechnology Research Program. I asked Jones where in their paper is the proof the antibody is specific to SARS-CoV-2 (and therefore isn’t binding to something else instead of, or in addition to, the novel coronavirus).
He responded promptly, as follows [bolding added by me for emphasis]: “While we did determine that LY-CoV555 is specific to SARS-CoV-2 (and doesn’t bind to the spike protein of SARS-CoV), that is not specified or detailed in any of the figures or tables [in the paper].”
Jones pointed me to several parts of the paper and supplemental material published with it that he said show, viaindirect extrapolation, that the antibody is specific for the novel coronavirus.
That’s not exactly convincing.
Then on December 22 a study in the New England Journal of Medicine gave a thumbs-down to the usefulness of bamlanivimab in people hospitalized after receiving a Covid diagnosis. The paper noted that in late October the study was stopped because the antibody didn’t help the patients any more than did placebo.
But this didn’t deter Lilly.
On January 21, 2021, the company issued a news release about a study of bamlanivumab in residents and staff of nursing homes. They claimed their research showed that the antibody “significantly reduced the risk of contracting symptomatic COVID-19.”
However, they didn’t back this up with much information. The study hasn’t been published in a journal or presented at a scientific/medical meeting. And there’s no word on when it will be.
Despite that, on the same morning the release was sent out by Lilly, glowing articles appeared in major media outlets stating that the study showed bamlanivumab appears to significantly reduce Covid symptoms in the frail elderly.
For example a Bloomberg article was posted at 8 a.m. on Jan. 21 with the headline, “Eli Lilly Antibody Cuts Covid-19 Risk Up to 80% in Nursing Home Study.” The article was carried in many other media outlets such as the Globe & Mail.
The article quoted Lilly’s Chief Scientific Officer Daniel Skovronsky as saying, “This is an urgent situation. Where there’s an outbreak in nursing homes and people haven’t yet received the vaccine, this could be a potential way to protect them before they get it.”
And January 21 New York Times piece bysenior science journalist Gina Kolata quotes a vaccine expert at Boston Children’s Hospital, Ofer Levy, who wasn’t one of the scientists involved in the study, as saying, “I see only positives here. This is a win.”
Kolata also reported that Lilly plans to ask the FDA for an EUA for bamlanivimab for prevention of Covid in the frail elderly, focusing on those in nursing homes and long-term-care homes.
In parallel, Lilly ispivoting to using bamlanivumab in combinationwith another monoclonal antibody called etesevimab. A study on this combination in people with mild or moderate Covid was published on January 21, 2021. The results indicate it doesn’t reduce symptoms, but only lowers the viral load of people.
This didn’t deter Lilly either; it’s spinning this in the media as a very positive result. And so is the FDA:on February 9 the agency issued an EUA for the combination of the two antibodies for treating mild or moderate COVID.
Then the next twist in the plot happened, on February 16: a paper published that day in bioRχiv indicated that bamlanivumab doesn’t neutralize the South African and Brazilian variants of the novel coronavirus.
I’ll Leave the Last Words to Scott Adams
Dilbert-cartoon creator Scott Adams makes this observation on page 13 of his book Loserthink: “One thing I can say with complete certainty is that it is a bad idea to trust the majority of experts in any domain in which both complexity and large amounts of money are involved.”
This perfectly describes the situation with antibodies for the novel coronavirus.
Buyer beware, follow the money, and stay tuned.
After obtaining an MSc in molecular biology from the Faculty of Medicine at the University of Calgary, Rosemary Frei became a freelance writer. For the next 22 years she was a medical writer and journalist. She pivoted again in early 2016 to full-time, independent activism and investigative journalism. Her website is RosemaryFrei.ca.
The New York Times, WSJ and all of the media have mused about the origins of this virus – well here we explain the actual science and data, and what IT actually tells us.
NOTE: My extensive research and interviewing / video/sound editing and much more does require support – please consider helping if you can with monthly donation to support me directly, or one-off payment: https://www.paypal.com/donate?hosted_…
Professor John Edmunds, a UK scientists acting as a shill for Bill Gates appears on BBC news to promote the disgusting practice of jabbing children with a ‘vaccine’ that is more likely to harm them than help them.
This is the currently reality of the eugenicists’ culling agenda – kill the old and the young (they don’t produce, only consume) If we can’t get them all, sterilize the rest.
Should the technocrats who pushed governments to lockdown their citizens be tried for crimes against humanity?
One prominent German lawyer, who is also licensed to practice law in America, thinks they should. And he is organizing a team of thousands of participating lawyers who want to prosecute a “second Nuremberg tribunal” against a cadre of international elites responsible for what he calls the “corona fraud scandal.”
Targeting the Davos, Switzerland-based World Economic Forum and its devotees among global political leaders, attorney Reiner Fuellmich says they are guilty of crimes against humanity for their perpetration of COVID-response policies that led to forced shutdowns, destroyed businesses, impoverished families, broken lives and a spike in suicide rates.
He has formed the German Corona Investigative Committee to pursue civil charges against the main perpetrators, among them being the head of the United Nations World Health Organization Dr. Tedros Adhanom. He hopes a successful class-action lawsuit will also lead to criminal charges.
Fuellmich was on the legal team that won a major lawsuit against German automaker Volkswagen in a 2015 case involving tampered catalytic converters in the U.S. He also was involved in a lawsuit that exposed one of Germany’s largest banks, Deutsche Bank, as a criminal enterprise. The bank was recently ordered by the U.S. Justice Department to pay $130 million to resolve corrupt practices that included money laundering, bribery and fraud between the years 2009 and 2016.
Fuellmich is licensed to practice law in Germany and the state of California.
He believes the frauds committed by Volkswagen and Deutsche Bank pale in comparison to the damage wrought by those who sold the Covid-19 crisis as the worst viral outbreak to hit the world in more than a century and used it to cause media-driven panic, government overreach and human suffering on a scale still not fully quantified.
The truth is revealed in the numbers, Fuellmich said, citing figures that show COVID-19 has not caused any statistically significant increase in the 2020 death counts over previous years.
The scam perpetrated on humanity hinged on one dirty little secret, he said – the PCR Test.
Not only are these tests not approved for diagnostic purposes but the inventor of the PCR Test, the late Kary Mullis, explicitly stated in an interview that this was never the purpose of his test.
Fuellmich explains in the video below how the coronavirus response of governments worldwide working in cahoots with the Bill Gates-funded U.N. World Health Organization “are probably the biggest crimes against humanity ever committed.”
“A number of highly respected scientists [he names several in the video including a Nobel Laurette from Stanford University] have concluded there has never been a coronavirus pandemic but only a PCR test pandemic,” he says.
“If someone tests positive it does not mean they are infected with anything, let alone with the contagious SARS-COV-2 virus,” Fuellmich says in the video.
“Based on the rules of criminal law, asserting false facts concerning the PCR tests, or intentional misrepresentation, that can only be assessed as fraud. Based on the rules of civil tort law, this translates into intentional infliction of damage.”
He said persons harmed by the PCR-induced lockdowns are entitled to full compensation for their losses.
“The crimes committed by Mr. Christian Drosten [an epidemiologist and Germany’s version of Dr. Anthony Fauci] and Mr. Lothar Wieler, a veterinarian and head of the German equivalent of the CDC, and Tedros Adhanom, head of the WHO, must be legally qualified as actual crimes against humanity as defined in Section 7 of the International Criminal Code.”
He said the class-action lawsuit is the best avenue to try the case.
In a Feb. 24 article about Fuellmich’s effort, the journal Principia Scientific International quoted him saying “this COVID-19 crisis should be renamed the ‘Covid-19 Scandal,’ and all those responsible should be prosecuted for civil damages due to manipulations and falsified test protocols. Therefore, an international network of business lawyers will plead the biggest tort case of all time, the COVID-19 fraud scandal, which has meanwhile turned into the biggest crime against humanity ever committed.”
Here is a summarized translation of the most-recent update Fuellmich put out on his German website on Feb. 15:
“The hearings of around 100 internationally renowned scientists, doctors, economists and lawyers, which have been conducted by the Berlin Commission of Inquiry into the COVID-19 affair since 10.07.2020, have in the meantime shown with a probability close to certainty that the COVID-19 scandal was at no time a health issue. Rather, it was about solidifying the illegitimate power (illegitimate because it was obtained by criminal methods) of the corrupt ‘Davos clique’ by transferring the wealth of the people to the members of the Davos clique, destroying, among other things, small and medium-sized enterprises in particular. Platforms such as Amazon, Google, Uber, etc. could thus appropriate their market share and wealth.”
Was the vaccinethe reason for the virus?
Perhaps the most egregious outgrowth of the coronavirus scam has been the fear-mongering that not only led to devastating and non-scientific shutdowns but also the rush to market of an unproven, experimental vaccine, which is now making billions of dollars for Big Pharma.
Just like the lockdowns, the vaccine is unnecessary because there are already several well-documented treatments involving long-established drugs that are proven safe and widely available. Also just like the lockdowns, this vaccine carries potentially devastating long-term effects on human health. There are questions about its effects on the fertility of men and women, and it has already led to more than 600 deaths in the U.S. and more than 250 deaths in the U.K.
To make matters worse, it is becoming plainly obvious that the intent is to make this experimental vaccine mandatory for all of humanity. It was billionaire vaccine investor Bill Gates who originally floated the idea, in April 2020, that humanity could never return to “normal” until “we have a vaccine that we’ve gotten out to basically the entire world.”
This reporter predicted last April that the vaccine would eventually be made mandatory, largely by corporations using coercive tactics.
Israel takes the lead in instituting medical tyranny
Among the nations considered to be part of the “free world,” Israel is taking the lead in pushing forward with a new type of society in which corporations and governments work together to coerce and eventually force every human being on the planet to get an injection of experimental vaccine treatments.
Not since the Nazi Third Reich has there been so little respect for citizens’ rights of individual health autonomy in a Western nation.
Whether you live in America, the U.K., Australia or Europe, if you wish to see what your future holds under the “new normal,” just look at Israel.
The Israeli government has announced that people will not be allowed to participate in a host of life functions without showing papers offering proof that they have either been vaccinated or that they have had and recovered from COVID.
A host of Israeli businesses including shops, malls, markets, pubs, gyms, museums, synagogues, hotels and libraries were allowed to reopen Sunday, Feb. 21, the Times of Israel reports. But only those Israelis who have been vaccinated or have recovered from COVID will be able to use gyms and pools, attend synagogues, sporting and culture events, board a flight or stay at hotels.
Calling the Health Ministry’s hotline and having the pass sent by email or fax.
Europe also moving toward vaccine passports
The European Union also appears to be on the cusp of embracing similar draconian measures. German Chancellor Angela Merkel stated this week that the concept of a digital vaccine passport has achieved “unanimous support within the E.U.“
“Everyone agreed that we need a digital vaccination certificate,” Merkel said last Wednesday after a meeting with European leaders.
E.U. Commission President Ursula von der Leyen also praised Israel’s new Green Pass system.
The Telegraph reports that the government of the U.K. is nearing an announcement of new rules similar to Israel’s in which no Brit will be allowed to enter pubs, gyms, large-venue events or hotels without showing their special COVID vaccine passport.
Since when do we take away freedom in order to restore it under a new set of terms defined by unelected “experts” at the United Nations World Health Organization? This is the twisted way in which the globalist technocrats think. Always perverting the language to sell their lies and enticing ill-informed masses to walk straight into their devious traps.
Forcing people to accept a medical treatment and to “show your papers” proving they have received the treatment in order to participate in society is a violation of the well-established international norms.
The Nuremberg Code came out of the Nuremberg tribunals that convicted leading German Nazis. The Code states that any experimental medical treatment must not only be voluntary but must include “informed consent,” meaning the person not only volunteered but was informed of exactly what the treatment entailed and the risks involved.
Global power elites have already used COVID as cover to clamp down on free speech, assembly, religious gatherings and small business operations, creating a world of the haves and have-nots. Big-box stores like Walmart and online retailer Amazon have thrived, raking in record profits, while small businesses are dying.
So the class-action lawsuit appears justified, at least in theory. A small cabal of globalist corporations and “experts” at the WHO created the problem, made it impossible for people to live their lives as normal human beings, leading to mass anxiety and huge spikes in suicide.
Now that everyone is miserable and desperate to get back to normal, the technocrats introduce an experimental gene therapy, the mRNA vaccine, and are holding that out as the salvation, making it oh so tempting for many to line up and roll up their sleeve.
Tempting, that is, if you haven’t done your research to find out who is promoting the vaccine, what are their long-held motives and goals, and what their previous track record has been.
Such research would lead you straight to the Bill and Melinda Gates Foundation, which has invested billions into an ever-growing lineup of vaccines through the GAVI global vaccine alliance and other organizations. Gates has bragged about the tremendous 20-to-1 “return on investment” he has reaped by investing in vaccine therapies. His net worth has increased by $17 billion since making the shift in focus from computers to vaccines.
U.S. companies bribing employees to take the shot
A number of U.S. companies are now bribing their employees, offering cash bonuses of $100 to $150 if they get the shot. Meijer, Kroger, Publix, Dollar General, Aldi, JBS Meat Processing and Trader Joe’s, among others, have all jumped on the bandwagon. They are being highly praised by “health experts” for doing this, so look for more companies to follow suit.
Those who refuse the vaccine, which is their right under the Nuremberg Codes, will become the new untouchables in a caste system that divides people along medical lines. Those getting the shot will be allowed to re-enter something closer to normalcy while those rejecting it will be left behind.
The dots are all there – with the virus, the fear-mongering, the lockdowns and mask mandates, and the coming vaccine mandates. All you have to do is connect them.
Leo Hohmann is an independent journalist whose work is 100 percent reader supported. Contributions of any size are appreciated. Send c/o Leo Hohmann, PO Box 291, Newnan, GA 30264
During the past 10 years that Health Impact News has been publishing the truth about vaccines and exposing the corruption and lies in the pharmaceutical industry and their marketing branch, the U.S. Centers for Disease Control (CDC), regarding the annual flu statistics, we have usually run stories around this time of year explaining to people that the number of people dying from the flu according to the CDC is false, and that the CDC themselves have always admitted that they do not know the exact number of people who die from the flu each year, but instead base their data on “estimates.”
For years this was published very clearly on the CDC website for all to see, at least for those who bother to “fact check” the CDC’s claims regarding annual flu deaths.
Many others over the years have exposed this scam as well.
The CDC’s decision to play up flu deaths dates back a decade, when it realized the public wasn’t following its advice on the flu vaccine.
During the 2003 flu season “the manufacturers were telling us that they weren’t receiving a lot of orders for vaccine,”Dr. Glen Nowak, associate director for communications at CDC’s National Immunization Program, told National Public Radio.
Flu results in “about 250,000 to 500,000 yearly deaths” worldwide, Wikipedia tells us.
“The typical estimate is 36,000 [deaths] a year in the United States,” reports NBC, citing the Centers for Disease Control.
“Somewhere between 4,000 and 8,000 Canadians a year die of influenza and its related complications, according to the Public Health Agency of Canada,” the Globe and Mail says, adding that “Those numbers are controversial because they are estimates.”
“Controversial” is an understatement, and not just in Canada, and not just because the numbers are estimates. The numbers differ wildly from the sober tallies recorded on death certificates — by law every certificate must show a cause — and reported by the official agencies that collect and keep vital statistics.
According to the National Vital Statistics System in the U.S., for example, annual flu deaths in 2010 amounted to just 500 per year — fewer than deaths from ulcers (2,977), hernias (1,832) and pregnancy and childbirth (825), and a far cry from the big killers such as heart disease (597,689) and cancers (574,743).
The story is similar in Canada, where unlikely killers likewise dwarf Statistics Canada’s count of flu deaths.
Even that 500 figure for the U.S. could be too high, according to analyses in authoritative journals such as the American Journal of Public Health and the British Medical Journal.
Only about 15-20 per cent of people who come down with flu-like symptoms have the influenza virus — the other 80-85 per cent actually caught rhinovirus or other germs that are indistinguishable from the true flu without laboratory tests, which are rarely done.
In 2001, a year in which death certificates listed 257 Americans as having died of flu, only 18 were positively identified as true flus. The other 239 were simply assumed to be flus and most likely had few true flus among them.
This article takes issue with the 36,000 flu-death figure commonly claimed, and with describing “influenza/pneumonia” as the seventh leading cause of death in the U.S.
As you can see from Mr. Solomon’s 2014 article, he quoted sources dating all the way back to the early 2000s where this scam was exposed. It just wasn’t published in the pharma-controlled corporate media, so those spoon-fed the propaganda from this corporate media lined up every year to get their flu shots, as Big Pharma raked in huge profits from producing over 300 million doses of the flu vaccine each year.
The Centers for Disease Control and Prevention estimated that the 2017-2018 flu season killed 80,000 and hospitalized 900,000 Americans. Of course, the mainstream media reported this as fact as shown in this September 27, 2018 article in the Washington Post.
The Powers-That-Be, including the CDC and the mainstream media, are using these estimates to promote the flu shot for the upcoming flu season.
Keep in mind, the 80,000 deaths and 900,000 hospitalizations are ESTIMATES. And, I can state, with authority, that they are very poor estimates.
You see, deaths from flu are always estimates because if the Powers-That-Be reported the true numbers of deaths from actual influenza infections, the numbers would be much lower and people would not be so inclined to receive a flu shot.
How does the CDC overestimate the number of flu deaths? The CDC accomplishes this by reporting a combined pneumonia and influenza death rate. Every time I try to analyze this data, I know I will have to spend at least an hour searching for the true number who died from influenza because the CDC tries to hide that data.
Why does the CDC do this? The answer is easy: The more people that receive the flu vaccine, the more money the CDC makes. You see, the CDC holds patents on many vaccines including the flu vaccine. (1)
Perhaps I could tolerate the CDC combining pneumonia with flu deaths IF the flu vaccine prevented both. However, the flu vaccine has never been shown to have any impact on the number of deaths from pneumonia.
In fact, for the vast majority who receive it, the flu vaccine has little impact on preventing the flu, but I digress.
In 2001 the CDC reported that 62,034 died from influenza and pneumonia. That year, I would bet that CDC proclaimed that flu killed over 50,000 Americans. After a painful hour of searching the CDCs database, I found the true 2001 numbers: 257 died from influenza and 61,777 died from pneumonia. Keep in mind, any death from the flu is tragic, but those numbers are out of a population of over 300 million. In 2010 (the latest year data are available) there were 55,227 deaths due to pneumonia and flu. Flu killed 4,605 while pneumonia killed the rest. (2)
So, let’s go back to last year’s flu season. The flu season lasts about six months. 80,000 deaths would lead one to conclude that 13,333 died per month (80,000/6 months) from the flu. If we further divide that number by 50 (the number of states), we can conclude that there were 267 people dying each month in every state from the flu. Since the internet provides 24-hour news cycles, I think we all would have heard that about 9 people (267/30 days per month) in every state dying daily from the flu. (3)
I have five practitioners in my office. We have over 100 years of experience in treating patients. None of us has can recall a single patient dying from the flu.
In fact, I can guarantee you that if 9 people were dying in my state daily from the flu, my partners and I would hear about it. In fact, there are always headlines on the internet when one person dies from the flu.
Studying the past CDC data shows that each year a few hundred to a few thousand die from the flu.
This annual flu death scam continued through 2019, as again Dr. Brownstein wrote:
The headline in the January 5, 2019 edition of the Wall Street Journal reads “Six Feet, 48 Hours, 10 Days: How to Avoid the Flu.”
This article, like nearly all main stream media flu articles was written to scare the reader into getting the flu vaccine. As with most mainstream medical articles about the flu, it is filled with fake news.
Let’s analyze the article.
The author starts off by writing,
“After a slow start, the flu season has taken off. Between Christmas and New Years Day, there was a marked rise in flu illnesses across the U.S.”
So far, no fake news to report.
However, as with most main stream media influenza stories, the writer misstates the true numbers of Americans who die from the flu.
“In a mild year, influenza, a highly contagious viral infection of the respiratory system, kills as many as 12,000 people in the U.S., and in a bad year, it could be as many as 56,000.”
I have two words to state here:
FAKE NEWS!
Folks, that is a blatant LIE. Over the last 38 years, neither twelve nor fifty-six thousand deaths from influenza infections occurred. In fact, the deaths from influenza are not even close to those numbers.
Why would the mainstream media and the Powers-That-Be continually lie about the numbers of people that die from the flu?
It is not hard to understand why—they want to scare the public in order to increase the number of people vaccinated with the flu vaccine.
The Centers for Disease Control and Prevention keeps annual death statistics. When searching through that data, it is easy to find the first Table (Table B) which lists the number of deaths from the top fifteen causes of death (https://www.cdc.gov/nchs/data/nvsr/nvsr67/nvsr67_05.pdf -page 6).
In fact, every year that the CDC reports the final data for deaths, the CDC combines influenza and pneumonia together as one of the top 15 causes of death. No other separate illnesses are combined, so why combine pneumonia and influenza which are two separate illnesses?
The answer is easy: the CDC artificially inflates the numbers of deaths from influenza to scare us into getting the flu shot. You see, if a very small percentage of Americans died yearly from the flu vaccine, why would so many of them want to get vaccinated for influenza?
The CDC has a direct financial interest in vaccinating the entire population since it holds multiple patents on vaccines including the flu vaccine.
In order to frighten the public to get the flu vaccine, the CDC’s scare tactics include annual statements that the flu kills 36,000 Americans per year.
The Great Flu Reset 2020-21: COVID Deaths Take Over to Sell New Novel COVID “Vaccines”
So now we come to the 2020-21 flu season, where we are being told the flu has “vanished.” Hardly anyone is getting the flu. Nobody is dying from the flu.
And if you still get your news only from the pharma-owned corporate media, you are being told that the lockdowns, social distancing, handwashing, and of course masks, have worked to eliminate all those horrible flu cases and deaths.
To believe this, of course, one has to overlook that these measures did nothing to slow down COVID deaths, as according to CDC statistics we have seen more COVID deaths in January and February than all the rest of the months since the “pandemic” started combined.
The “logic” of this is so absurd, that they even hired an editorialist at the New York Times to explain to people that they should not try to figure this out, because “Critical thinking, as we’re taught to do it, isn’t helping in the fight against misinformation.”
Despite all those warnings from Dr. Anthony Fauci about COVID-19 and the flu joining forces in 2020 and 2021 to create some kind of super-deadly double-whammy viral pandemic, it’s no longer a secret at this point that worries about a super-charged flu season simply never came to pass. We’ve reported on the phenomenon of falling flu cases before.
February is usually the peak of flu season, when doctors’ offices and hospitals are packed with patients. But that’s not the case this year. Instead, the flu has virtually disappeared from the US, with reports coming in at far lower levels than the world has seen in decades. Some areas, like San Diego, have seen such low numbers, health authorities have demanded audits of COVID-positive patients to see whether some might have been misdiagnosed.
According to the CDC, the cumulative positive influenza test rate from late September into the week of December 19th was just 0.2%, compared to 8.7% from a year before.
Hospitals say the expected army of flu-sickened patients never materialized, and that nationally “this is the lowest flu season we’ve had on record,” according to a surveillance system that is about 25 years old.
One source from Maine Medical Center in Portland, the state’s largest hospital, said “I have seen zero documented flu cases this winter,” said Dr. Nate Mick, the head of the emergency department.
Ditto in Oregon’s capital city, where the outpatient respiratory clinics affiliated with Salem Hospital have not seen any confirmed flu cases.
The phenomenon isn’t unique to the US.
In the UK, data released this week show that the number of active flu cases in the country has fallen to zero. (Source.)
Of course for those of us who have followed this issue for more than a decade now, we know that the flu deaths have not gone anywhere, because they were never there to begin with.
What we actually had, based on the Department of Justice quarterly reports on settlements paid out from the National Vaccine Injury Compensation Program, is many people being injured and killed by the flu shots.
The CDC simply stopped estimating and inflating the flu deaths, and concentrated on COVID deaths instead, to support the TRILLIONS spent to fast-track experimental COVID vaccines which Big Pharma is now rushing to manufacture and distribute.
So has this “Great Reset” simply replaced one scam for another one?
I’ll let Dr. Scott Jensen, a medical doctor and Senator from Minnesota, tell you in his own words:
Western media portrays Australia as a beautiful nation with independent people and a close ally of the United States. But the American Empire has no allies, only vassal states. Australia became a colony of the American empire in 1975 after an Anglo-American coup. Australians noticed nothing since Australia had been an British colony since its inception and dispatches military forces when ordered to fight empire wars.
“ALLY THIS: The CIA Subversion of Australian Democracy”; Jon Gleur; Dunemessiahdotnet; November 23, 2014; (details of the 1975 coup) https://dunemessiahdotnet.wordpress.c…
“The PM, the spy and the governor-general: what John Kerr didn’t tell the palace”; Guy Rundle; Crikey; July 17, 2020; (details about the CIA coup from the “Palace Papers” that were declassified in 2020); https://www.crikey.com.au/2020/07/17/…
I had included a short clip from this anti-China propaganda story produced by the American empire to fool Australians. “60 Minutes” objected to my “fair use” for commentary so I was forced to clip it out, resulting in an audio blip in this video.
By Lisa Pease | Consortium News | September 16, 2013
More than a half century ago, just after midnight on Sept. 18, 1961, the plane carrying UN Secretary-General Dag Hammarskjöld and 15 others went down in a plane crash over Northern Rhodesia (now Zambia). All 16 died, but the facts of the crash were provocatively mysterious. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.