If It’s Okay for Mice, It’s Good Enough for People, Right?
By Madhava Setty, M.D. | The Defender | August 26, 2022
Its audacity on full display, Pfizer — arguably the most criminal corporation in history — has asked the U.S. Food and Drug Administration (FDA) to greenlight its new bivalent COVID-19 vaccine that targets the Omicron BA.4 and BA.5 subvariants for people 12 and older “to help the country prepare for potential fall and winter surges of the coronavirus,” Pfizer CEO Albert Bourla said in a statement.
Bourla’s good intentions are sadly thwarted by FDA regulations that require an Investigational New Drug (IND) application be submitted and approved before a drug can be tested in humans.
Luckily, the FDA can circumvent the inconvenience of its own regulatory processes by allowing itself the ability “to authorize use of an experimental drug in an emergency situation that does not allow time for submission of an IND in accordance with 21CFR, Sec. 312.23 or Sec. 312.20.”
Section 312.20 of the Code of Federal Regulations specifies that a clinical investigation cannot commence until an IND application has been submitted and approved. Nevertheless, Pfizer on Monday submitted an IND for its new formulation.
Now that the FDA and Pfizer have crossed their Ts and dotted their Is to make sure all the rules are followed, how do we know these products are safe and will work?
This is where the rodents come in — the products seem to work on mice.
As NPR reported, “For the first time, the FDA is planning to base its decision about whether to authorize new boosters on studies involving mice instead of humans.”
Yes, it’s an unprecedented move by the FDA, but Dr. Ofer Levy, professor of pediatrics at Harvard and advisor to the FDA argues that the country has had enough experience with the vaccines at this point to be confident the shots are safe and that there’s not enough time to wait for data from human studies.
He has a point. There were still only 30,479 uninvestigated deaths reported in VAERS after administration of the shots as of Aug. 19.
In any case, why should the FDA be concerned with such things as human studies in the first place?
This maneuver by the FDA may finally unshackle the agency from its overly restrictive responsibility to fulfill its own mission and become more agile in bringing products to market.
Not to be left behind, Moderna also requested the FDA authorize its bivalent vaccine for human beings over the age of 17.
Similar to the Pfizer vaccine, Moderna’s vaccine also, for good measure, will encode for the spike protein for the original ancestral SARS-CoV-2 strain, which for all intents and purposes, does not exist on our planet any longer.
Meryl Nass, M.D., summarized it this way:
“No clinical trials. (You need to obtain an IND before you can start testing the vaccine in humans. Pfizer applied 4 days ago.)”
Taking no chances, the FDA will not convene the Vaccines and Related Biological Products Advisory Committee (just like the first time the FDA authorized boosters) and has announced this today to see how much opposition the agency gets.
Can we dispense with the pretense any of this is about health?
No sane person vaccinates the entire country with an experimental vaccine without trials — particularly since the whole country already has some immunity, the virulence is low and the evidence supports higher all-cause mortality with an increasing number of vaccine doses.
What is in the vaccine that they are desperate to inject us with?
Madhava Setty, M.D. is senior science editor for The Defender.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Norwegian Schools Are Disseminating Government-Approved Covid Misinformation

BY KATHRINE JEBSEN MOORE | THE DAILY SCEPTIC | AUGUST 26, 2022
Who needs conspiracy theorists when you’ve got school books teaching children that Covid vaccines are “95% effective”?
This autumn, a new school book was introduced for the ninth grade in Norway. Fabel 10 was revised in 2021/22, but has only now been introduced in schools across Norway. Not only does the book overstate the effectiveness of the novel mRNA vaccines, it decries anyone questioning that as conspiracy theorists.
One excerpt reads:
Since the Covid pandemic broke loose, Covid deniers and vaccine sceptics have spread disinformation about coronavirus through social media. They claimed among other things that COVID-19 was no more deadly than the flu, that the vaccine was dangerous, and that restrictions were unnecessary. On Saturday March 20th 2021, 200 Covid deniers gathered in front of the Parliament. They burnt face masks to show that they thought they were unnecessary.
This short paragraph is easily debunked. Readers of the Daily Sceptic know that Covid now has an infection fatality rate about the same as influenza. We also know that side effects from the Covid vaccines – both the mRNA and the viral vector vaccines such as AstraZeneca’s – are more common than for other tried and tested vaccines. Remember when the Pandemrix vaccine rollout was halted because of a link to rare instances of narcolepsy? Multiple studies show Pfizer and Moderna’s Covid vaccines increase the risk of myocarditis and pericarditis in especially younger males – the demographic who make up precisely half the readership of Fabel 10. The German Government even admits that as many as one in 300 doses of the mRNA jabs produce serious injury. Compared to the danger that Covid poses to most people, does that make vaccines worth having?
And as for restrictions, a new consensus is gaining momentum. Whereas back in 2021, when the book was written, it was mainly agreed that lockdowns and other Covid restrictions were necessary to halt the spread, and countries with low Covid fatalities would credit these non-pharmaceutical interventions for their comparatively low excess mortality, studies later proved them incorrect. Lockdowns and excess mortality were not correlated. Whereas back in the early days of the pandemic, only a few, brave voices spoke up about their concerns, now even Rishi Sunak, who helped implement Britain’s lockdowns, admit they were detrimental to overall health and the economy and did little to stop infection. Yet in Norway, pupils are stuck in the reality curated more than a year ago, a reality that has now been revealed to most as bonkers.
And those 200 “Covid deniers” who burnt face masks deserve praise for being a tiny minority speaking up for science at a time where “the science” became an allegory for anything the authorities wanted us to do without having to prove why.
The book also states that vaccines are “95% effective against COVID-19 infections”. This is clearly nonsense, and doesn’t need further debunking. We all know of multiple-jabbed people getting infected several times over, and that infection rates in highly vaccinated countries went through the roof after the vaccine rollout.
Perhaps the book will serve as a test to pupils old enough to gather information from multiple sources. Some might agree with what they’re presented with, while others will see through this Government-approved misinformation. But that’s not really the sort of education you want in a free, democratic country. The book doesn’t invite 14-15 year-olds to question or discuss – it presents them with all the (wrong) answers. That’s bad enough in itself, but what’s worse is it tells them to ridicule those who don’t agree. The chapter on Covid and conspiracy theories could have been a great opportunity to teach children about academic freedom, online censorship, tolerance, debate, dissent and freedom of speech. Instead, it serves straight-up, Orwellian newspeak to young minds in a way the CCP would be proud of.
DC Mayor: No vaccine passport, no education – even for virtual learners

By Ken Macon | Reclaim The Net | August 26, 2022
The District of Columbia mayor Muriel Bowser said kids who do not have a vaccine passport within the first 20 days when schools resume next week Monday will not be allowed to get educated, even for those doing virtual learning from home.
A press release on the District of Columbia Public School’s website states: “The Coronavirus Immunization of School Students and Early Childhood Workers Amendment Act of 2021, which the Council passed in 2021, requires students ages 12 and older to be vaccinated against COVID-19 in order to attend school.”
The vaccine mandate applies to staff and also private schools.
Asked by The Daily Signal what the plan was for unvaccinated students, Bowser said: “They can go to school on Monday. But they need to get their vaccinations… and their families will be alerted as to the dates.”
The Office of The State Superintendent of Education for the District of Columbia recently announced that “all students must have up-to-date immunization certification on file with the school within the first 20 school days or they will not be allowed to attend school or school activities until the immunization certification is secured by the school.”
“If the student does not come into compliance within a 20-school day period, the school must remove the student from school until the immunization certification is secured by the school,” the office added.
The vaccine mandate will likely affect the education of black students as 47% of black children aged 12-15 in DC have not received the primary vaccination needed to attend school, according to government data. And 42% of black kids aged 16 and 17 are not vaccinated.
CDC Director deflects blame for lockdowns towards predecessors

By Mike Campbell | The Counter Signal | August 25, 2022
CDC Director Rochelle Walensky admitted organizational shortcomings on Fox News while deflecting blame toward predecessors for their lockdown recommendation.
“Many of those lockdowns pre-dated me at the CDC,” she said.
Walensky, who once used ‘Trust the science’ to persuade the public, carried a humbler tone while reflecting on her organization’s decisions.
“There were important decisions that we had to make in imperfect times, with imperfect data, and we always updated those decisions as those data were evolving…”
“So, I don’t really want to re-visit the questions of lockdowns that pre-dated me, but what I will say is, we’ve updated our guidance in the context of new information, and sometimes we have to make a decision before we have all the information that we want…”
Indeed, the CDC updated guidance by removing special quarantine recommendations for unvaccinated persons, effectively admitting that vaccination status is no longer relevant when it comes to infection or spread of the Covid virus.
In fact, on July 23, the CDC deleted a ‘fact’ from their “Facts about mRNA Covid-19 Vaccines”, and they did so without explanation. Last time I checked, facts don’t change — but apparently, they do for the CDC.
Walensky further stated that “[their] science” indicated hybrid immunity was superior to natural immunity. However, we’ve reported on a scientific study that accounted for more than 5.7 million people, which showed that natural immunity is just as effective as hybrid immunity.
To this point, Walensky’s usage of science in the possessive sense — by calling it “our science” — denotes a departure from “the science,” of which they’re either arbitrarily picking from or are completely unaware.
Between Fauci stepping down and Walenski pointing fingers, it appears the blame game has officially started.
The latest on vaccination of 5-11 year-olds
When will the onslaught on children end?
Health Advisory & Recovery Team | August 23, 2022
In February 2022, the JCVI in their wisdom, made a ‘non-urgent offer’ of Covid-19 vaccination for healthy children aged 5-11, scheduled to begin in April. It is worth reading the full statement, which hardly makes a strong case. Here are a few quotes.
- In comparison to the rest of the population / older age groups, evidence indicates that children aged 5 to 11 are at the very lowest risk from COVID-19. Rates of hospitalisation, paediatric intensive care admission and death are lower in this age group than in all older age groups. In addition, the high level of prior infection in this age group of children can be expected to contribute towards their natural immunity against reinfection. There are some data to suggest that natural immunity may last longer than vaccine-induced immunity against non-severe infection.
- The impact of vaccination on school absences was indeterminate; the balance between school absences due to reactions following vaccination versus school absences avoided due to prevention of infection is highly influenced by the uncertain timing of any future wave of infection and of the vaccination programme.
- vaccine effectiveness against symptomatic infection due to Omicron (Pfizer-BioNTech vaccine) wanes over time from around 70% shortly after 2 vaccine doses to around 25% after 10 weeks and 10% after 20 weeks.
- [myocarditis] medium to long-term (months to years) prognosis remains less certain.
- It is estimated that over 85% of all children aged 5 to 11 will have had prior SARS-CoV-2 infection by the end of January 2022
This last point makes the programme for this age group even more ridiculous – the 85% estimate of January 2022 has now risen to 99%, and is perhaps the main reason why parents have not been clamouring to get their children vaccinated (10% to date). Despite this, the government is planning an enhanced programme this September to reach all the currently unvaccinated, in particular primary school children.
Cornwall and the Isles of Scilly (NHS Kernow) are leading the way with advertisements and pop up clinics because of ‘a rise in cases’. As previously, petting dogs have been enrolled, and advertisements such as the one pictured here, are falsely claiming that somehow vaccinating small children who are already immune, will magically protect their grandparents.

Legal challenges: Meanwhile, disappointingly though not surprisingly, the Court has thrown out the request for a judicial review of the MHRA, the JCVI, and Secretary of State’s decision to vaccinate this age group and for the 12-15s another judge likewise rejected the legal challenge. A member of the legal team involved has published his response to these judgements here but in effect both judges were saying that the MHRA, the JCVI and the CMOs are self-evidently “experts”, thus the Secretary of State is clearly acting correctly to accept their advice, irrespective of whether their advice is sound. This is a bad day for UK citizens since it appears that drug regulators are now unaccountable.
The political route: The Children’s Covid Vaccines Advisory Committee (CCVAC) who helped with these cases, have recently sent a summary of all their concerns to Stephen Barclay, the latest Secretary of State for Health & Social Care. A reply has been received giving the usual bland “Vaccines are now safer than ever before.” and quoting the same data presented by the JCVI a year ago, totally failing to grasp that the current data give a very different risk:benefit balance. The CCVAC team have also drafted a letter for the new Prime Minister and they are seeking health professionals to add their signatures ready to have a very large letter to deliver to the new incumbent of No 10 in early September. The letter calls on the Prime Minister to halt the vaccination of children pending a full and independent safety review. Is there any chance that the new British Prime Minister will follow the lead taken by several Scandinavian countries? The Director of Denmark’s Board of Health for example was recently on record saying that the vaccination of children had achieved nothing. Meanwhile a report from Iceland shows that in their ~60,000 child population, serious vaccine injuries (eleven) far outweighed Covid-19 hospital admissions (zero).
Readers are invited to share this letter with any health professionals they know, including staff at their local medical centre. Letter to incoming PM: apply the precautionary principle (childrensunion.org)
Inside the mind of one of my very smart pro-vax friends
If you ask them for data to back up their claims, they stop responding.

By Steve Kirsch | August 22, 2022
I recently talked to a friend of mine at a recent social event. We’ll call him Bob. He’s super smart about most things. But when it comes to the vaccine, he’s blind to the truth.
He was bragging about how he has been vaxxed 6 times with the COVID vax and he’s perfectly healthy. He can’t wait for SB 866 in California to pass so when his kids turn 12, they can decide to get the vaccine over their mother’s objections.
Bob thinks I’m a nut case, cherry picking data. He says I used to be respected, but after turning anti-vax, people have lost all respect for me. He said I have a religious belief about the vaccine and I’m not driven by data.
What he isn’t telling anyone is that he’s been losing his vision ever since he got his first COVID vaccine. He used to have 20/20 vision, but now he wears glasses and can’t drive at night. When I brought up the data showing the connection between the shots and vision loss, he changed the topic.
I showed him two papers showing the more you vaccinate, the sicker you get (see the two papers here). I asked, “Where are the papers that show the opposite?” He ignored my request.
He gets his belief system from the mainstream media. Full stop. He reasons that if I was correct, surely Bill Gates would agree with me and admit they goofed. It’s 100% deference to authority.
Bob will not look at the data himself and he doesn’t want to discuss it. He will not engage. He thinks that if I was right, there would be more than a handful of people speaking out. So he tallies the size of the support base on each side of an issue instead of looking at the data.
I hope this is useful in helping you understand the pro-vaxxers and how they think.
The important thing is you cannot turn these people around. Arguing with them is fruitless because they don’t want to see the data. They will only come around when the people they trust change their position.
This is why we need to focus on protecting doctors who speak out.
Perhaps a state ballot initiative in California providing that doctors cannot be retaliated against when they tell the truth (including having social media accounts taken down, having their license to practice medicine revoked, etc). That would prevent things like this from ever happening again.
Untested Bivalent COVID Jab Being Rolled Out
By Dr. Joseph Mercola | August 22, 2022
August 15, 2022, the U.K. became the first country to approve Moderna’s new bivalent COVID booster, which contains both the original concoction and mRNA to target Omicron variants. The booster has also been submitted for approval with authorities in Australia, Canada and the EU, and there’s every reason to suspect it’ll be submitted to the U.S. Food and Drug Administration as well. As reported by Sky News:1
“The booster dose, known as ‘Spikevax bivalent Original/Omicron,’ contains 25 micrograms of Omicron vaccine and 25 micrograms of original coronavirus vaccine …
The Joint Committee on Vaccination and Immunization (JCVI) has said the vaccine will be available to those aged 18 and over as part of the UK’s autumn booster program. Health Secretary Steve Barclay said those eligible will be contacted from early September.”
More Than 100 Million Doses Have Been Trashed
The approval of the new booster comes right on the heels of widespread complaints about lack of demand for the shots. Moderna recently had to throw away 30 million doses of its original COVID jab, as there was no demand for them.2
“We have a big demand problem,” Moderna CEO Stéphane Bancel said in May 2022 during a panel discussion at the World Economic Forum’s meeting in Davos, Switzerland.3 Similarly, in the U.S., pharmacies, states and federal agencies have tossed 82.1 million COVID jab doses in the trash, and for the same reason.4
Bivalent Booster Is Already Out of Date
Moderna’s bivalent booster is said to “provide a strong immune response against the Omicron BA.1 variant as well as the original 2020 Wuhan strain,” which, for the record, is extinct and no longer in circulation anywhere in the world. BA.1 is now rarely ever found, either.
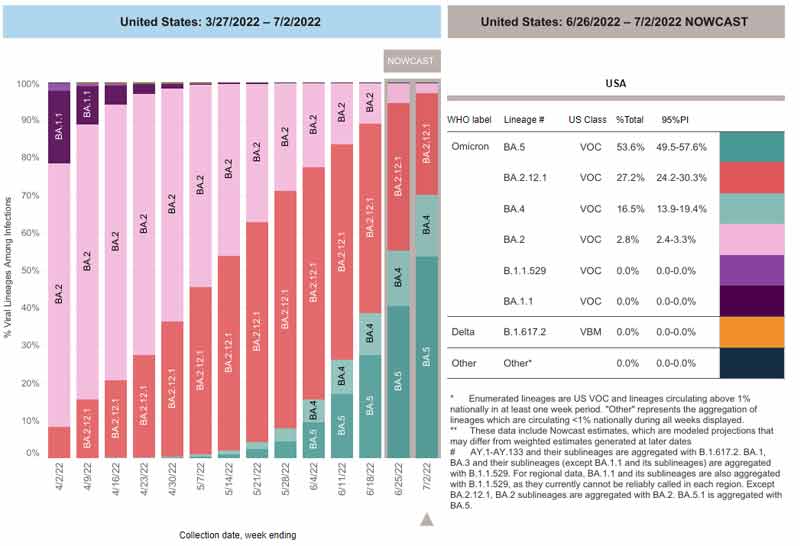
The graph5,6 below, from the U.S. Centers for Disease Control and Prevention, shows the infection ratios of common variants. As you can see, in the U.S., infections are now caused by the BA.4, BA.5 and BA.2.12.1 variants of Omicron.7 So, this booster contains two strains that aren’t even relevant anymore.
The situation is exactly the same in Europe, where Omicron BA.2, BA.4 and BA.5 are the current “variants of concern.” BA.1 isn’t even a “variant of interest,” which is the next-lower categorization. It’s on the list of “de-escalated variants,” which is based on a variant meeting one or more of the following criteria:8
“(1) the variant is no longer circulating, (2) the variant has been circulating for a long time without any impact on the overall epidemiological situation, (3) scientific evidence demonstrates that the variant is not associated with any concerning properties.”
In short, BA.1 is of no concern in Europe either, as it’s not in circulation and/or because it doesn’t cause severe illness. The same goes for the original Wuhan strain, which has long since mutated out of existence.
Vaccinating Against Rapidly Mutating Viruses Is a Bad Idea
Coronaviruses mutate very rapidly in general, and the mRNA jabs are based on a surface protein (the spike protein), which is the most rapidly mutating portion of the entire virus. What happens when you vaccinate against a rapidly mutating virus? You encourage it to mutate even faster, and to develop immune-evading properties.
This is what we’ve been witnessing since the beginning of the COVID jab campaign, and at this point, there’s no hope of ever catching up with the virus. What’s worse, while variants have so far evolved into milder strains, they are in fact gaining the ability to evade antibodies, and could theoretically switch course to become more pathogenic.9
This is particularly true when a vaccine is “leaky,” meaning it doesn’t fully prevent infection (which none of the COVID shots do). Just like when you overuse an antibiotic that fails to eradicate the bacteria, which allows antibiotic-resistant bacteria to flourish, overuse of a leaky vaccine can pressure a virus to become more lethal.10,11
BA.4 and BA.5 are the most resistant to date, with BA.5 circumventing the immune systems even of those with natural immunity.12 Fortunately, it doesn’t appear to cause severe illness in most people.
The take-home here is that had natural immunity been allowed to take place without these jabs, the pandemic would be over and reinfections near-nonexistent. Instead, we’re now in a pandemic of the vaccinated, with the vast majority of serious COVID infections occurring among those who have been jabbed.13,14
We know that Pfizer was aware of this possibility, as “vaccine-associated enhanced disease (VAED)” is listed as an “Important Potential Risk” in Table 5 on page 11 of a document called “5.3.6 Cumulative Analysis of Post-Authorization Adverse Event Reports.”15 This document was part of the FOIA required and court-ordered batch released by the FDA April 1, 2022.
How Long Will the Bivalent Booster Protect You?
According to Moderna, the bivalent Spikevax “demonstrates potent neutralizing antibody response against Omicron subvariants BA.4 and BA.5.”16 They made the same claim for the original COVID jab, back in January 2021,17 and by August 2021, they admitted the neutralizing antibodies generated lasted only six months after the second dose.18
How long will the bivalent jab “be effective” (and I use that term loosely)? Who knows, but the way things are trending, six months would probably be the max. In Germany, citizens must now get a booster every three months to qualify as “fully vaccinated,”19 as rapidly waning immunity has become accepted fact, and that’s probably where we’re all headed.
Germans who haven’t received all of their boosters will be subject to mask mandates and other COVID restrictions this fall. This, despite deep criticism from businesses tasked with confirming their customers’ status. As reported by the Rise Align Ignite Reclaim (RAIR) foundation:20
“Businesses have voiced great concern about further regulatory chaos in the struggling economy. ‘The plans are simply not feasible,’ said the general manager of the German Hotel and Restaurant Association (Dehoga), Ingrid Hartges, the Handelsblatt. ‘We cannot constantly check whether our guests are vaccinated, recovered, or tested.’
These people are exempted from the obligation to wear masks in restaurants or events under certain circumstances — if the vaccination, for example, is within the last three months. ‘But you can’t tell from the guest in the restaurant what status they have,’ says Hartges. ‘Like when he goes to the bathroom — should the staff always ask if he’s vaccinated?’ she said. ‘That’s nonsense.'”
Bivalent Jab Will Not Undergo Additional Testing
It’s important to realize that these “next-gen” boosters will not undergo any additional safety testing.21,22 They’re being rolled out under a new fast-track standard where ingredients can be swapped out without additional testing.
This is the standard protocol for seasonal flu vaccines. However, we’re now using an entirely new type and essentially untested technology. There’s no telling whether variations in the spike mRNA being injected might produce vastly differing side effects. They could potentially have differing toxicities, but that’s not being investigated.
Also, remember that the “efficacy” they’re referring to is only based on measurements of antibody titers, which tells us nothing, really, about its ability to prevent infection, severity of illness or death. Why?
Because antibodies form only a part of your immune response, and they’re not even the most important. It is far more likely that your innate immune system — your first line of defense — will destroy a virus before your adaptive immune system even has a chance to respond and create antibodies.23
It is important to understand that no vaccine improves your innate immune response. All vaccines are ever able to do is address your adaptive humoral immune system and create antibodies. Your innate immune system has T cells that can directly kill viruses. If you happen to have a vigorous T cell response, you’ll be protected even if your antibodies are low. So, antibodies are not a necessary measure of immunity.
Antibody titer levels are what’s called a “surrogate outcome.” It’s a substitute for actual clinical outcome. But it’s in no way equivalent, no matter how much the powers in control want it to be. Antibody titers may be high, but in the real world, more people may end up in the hospital and die — either from the infection or from the shot. In short, high antibody titer is not a guarantee of effectiveness — and it tells us absolutely nothing about safety.
CIA-Backed Upstart to Produce Moderna’s Bivalent mRNA
The complete absence of testing moving forward is all the more concerning when you consider who’s manufacturing the RNA for Moderna’s now-bivalent booster. In a recent Unlimited Hangout article,24 investigative journalist Whitney Webb reveals the genetic material for the reformulated booster is being exclusively manufactured by National Resilience, a relative newcomer with significant ties to U.S. intelligence agencies.
Its board of directors include In-Q-Tel CEO Chris Darby, who is also on the board of directors of the CIA Officers Memorial Foundation, and former FDA commissioner and Pfizer board member Dr. Scott Gottlieb. Not surprisingly, National Resilience promises to successfully lead its customers through the government regulatory process. As reported by Webb:25
“National Resilience was founded … in November 2020, and … plans to ‘reinvent biomanufacturing’ and democratize access to medicines,’ namely gene therapies, experimental vaccines and other ‘medicines of tomorrow’ …
In April 2021, National Resilience acquired Ology Bioservices Inc., which had received a $37 million contract from the US military the previous November to develop an advanced anti-COVID-19 monoclonal antibody treatment. This acquisition also provided National Resilience with its first Biosafety Level 3 (BSL-3) laboratory and the ability to manufacture cell and gene therapies, live viral vaccines and vectors and oncolytic viruses.
Despite being in the earliest stages of developing its ‘revolutionary’ manufacturing capabilities, National Resilience entered into a partnership with the Government of Canada in July of last year. Per that agreement, the Canadian government plans to invest CAD 199.2 million (about $154.9 million) into National Resilience’s Ontario-based subsidiary, Resilience Biotechnologies Inc.
Most of those funds are destined for use in expanding the Ontario facility that Resilience acquired last March and which is now manufacturing the mRNA for Moderna’s COVID-19 products … More recently, in 2022, the company has announced a few new clients – Takeda, Opus Genetics and the US Department of Defense …
Considering Moderna’s history and Resilience’s connections, there may be more to this partnership that meets the eye and concerned members of the public would do well to keep a very close eye on Resilience, its partnerships, and the products it is manufacturing.
Given that we now live in a world where government regulatory decisions on the approval of medicines are increasingly influenced by corporate press releases and normal regulatory procedures have fallen by the wayside for being too ‘slow,’ there is likely to be little scrutiny of the genetic material that Resilience produces for the ‘medicines of tomorrow.’
This seems to be already true for Moderna’s recently retooled COVID-19 vaccine, as there has been no independent examination of the new genetic sequence of mRNA used in the Omicron-specific vaccine candidate or its effects on the human body in the short, medium or long term.
For those who are skeptical of the outsized role that intelligence-linked companies are playing in the attempted technological ‘revolution’ in the medical field, it is best to consider Resilience’s role in the upcoming fall vaccination campaign and in future pandemic and public health scenarios before trying its ‘futuristic’ products.”
Was COVID Jab Intentionally Flawed?
In a June 2022 interview with British radio presenter Maajid Nawaz, Michael Yeadon, Ph.D., a former vice-president and chief scientific adviser for Pfizer and founder/CEO of the biotech company Ziarco (now owned by Novartis), explained why he believes the COVID jabs were intentionally made to be harmful and to prolong the pandemic.
For starters, it’s been known for more than 10 years that spike protein causes adverse effects in humans,26 so this could not be a design error. It must have been intentional.
As Yeadon explained, when making a vaccine, you have to be very careful about which part of the virus you use, as certain parts are more toxic and some provoke better immune responses than others. “What you would do is ask, ‘What’s the toxicity of the bit I’m going to give a person?'” he said.
Seeing how scientists have known for at least a decade that spike protein from related viruses causes blood clots through at least two different mechanism, the choice to use mRNA that programs your cells to make spike protein raised a warning flag from the start.
Nothing About the COVID Jabs Makes Sense
In addition to that, 90% of the immune response you get from natural COVID infection is in response to other parts of the virus, not the spike protein. Put another way, exposure to spike protein mounts an inferior immune response. If you’re looking to make an effective vaccine, wouldn’t you choose a part of the virus that mounts the best and most robust immune response?
By choosing the spike protein on which to base COVID-19 shots, scientists picked a protein that a) was known to be toxic to humans and b) produced an inferior immune response (compared to other parts of the virus).
On top of that, spike protein mutates rapidly, which destroys any protection the shot provides shortly after it’s given. As noted by Yeadon,27 “What you should do is pick the bits of the virus that’s genetically most stable,” but they didn’t do that. Why not? The end result is a seemingly never-ending series of boosters, and according to Yeadon, that may have been the plan from the start.
As if all of that weren’t enough, the spike protein is also similar to a variety of human proteins, which can trigger your body to mount an inappropriate immune response against your own proteins. In other words, it can cause autoimmune disease. Yet, scientists chose the spike protein anyway — even though it violated all of the accepted rules for creating a safe and effective product.
Collusion to Cause Harm
Yeadon believes the decision to use spike protein was not a mistake at all. He believes it was intentionally chosen because it has all of those ill effects. He told Nawaz:
“Again, you deselect things that are toxic in their own right, you pick things that are genetically stable, and you pick things that are most different from humans …
But guess what? Moderna picks spike protein and so does Pfizer, and AstraZeneca, and Johnson & Johnson. So, I put it to you, colleagues, any scientists out there or just logical people. How the hell would they pick [the spike protein]?
No team I was ever part of would ever have picked bloody spike protein for this vaccine. And you know what? If we did, and we have competing groups, we would not, all four of us, make the same mistake. Not possible. It’s collusion and malfeasance. The did it on purpose, knowing it would hurt you.”
Resources for Those Injured by the COVID Jabs
If you got one or more jabs and suffered an injury, first and foremost, never ever take another COVID booster, another mRNA gene therapy shot or regular vaccine. You need to end the assault on your system. The same goes for anyone who has taken one or more COVID jabs and had the good fortune of not experiencing debilitating side effects.
Your health may still be impacted long-term, so don’t take any more shots. When it comes to treatment, there are still more questions than answers, and most doctors are clueless about what to do — in part because they never bothered to give early treatment for COVID and therefore don’t understand how different medicines and supplements impact the spike protein.
So far, it seems like many of the treatments that worked against severe COVID-19 infection also help ameliorate adverse effects from the jab. This makes sense, as the toxic, most damaging part of the virus is the spike protein, and that’s what your whole body is producing if you got the jab.
Two doctors who have started tackling the treatment of COVID jab injuries in earnest include Dr. Michelle Perro (DrMichellePerro.com), whom I’ve interviewed on this topic, and Dr. Pierre Kory (DrPierreKory.com).
Both agree that eliminating the spike protein your body is now continuously producing is a primary task. Perro’s preferred remedy for this is hydroxychloroquine, while Kory typically uses ivermectin. Both of these drugs bind and thereby facilitate the removal of spike protein.
Kory also believes there may be ways to boost the immune system to allow it to degrade and eventually remove the spike from your cells naturally, over time. One of the strategies he recommends for this is TRE (time restricted eating), which stimulates autophagy, a natural cleaning process that eliminates damaged, misfolded and toxic proteins. Another strategy that can do the same thing would be sauna therapy.
As a member of the Front Line COVID-19 Critical Care Alliance (FLCCC), Kory helped develop the FLCCC’s post-vaccine treatment protocol called I-RECOVER. Since the protocol is continuously updated as more data become available, your best bet is to download the latest version straight from the FLCCC website at covid19criticalcare.com28 (hyperlink to the correct page provided above).
Sources and References
- 1 Sky News August 15, 2022
- 2, 3 Washington Examiner May 26, 2022
- 4 NBC News June 6, 2022
- 5 CDC COVID Data Tracker
- 6, 7 Nebraskamed.com August 9, 2022
- 8 ECDC.Europa
- 9 geertvandenbossche.org Letter to the WHO March 6, 2021 (PDF)
- 10 PLOS Biology July 2015; 13(7): e1002198
- 11 Quanta Magazine May 10, 2018
- 12 Axios June 1, 2022
- 13 Israel National News February 3, 2022
- 14 Daily Expose April 3, 2022
- 15 5.3.6 Cumulative Analysis of Post-Authorization Adverse Event Reports, Page 11, Table 5
- 16 Moderna June 22, 2022
- 17 BioRxiv January 25, 2021; 2021.01.25.427948
- 18 Time January 26, 2022
- 19, 20 RAIR August 13, 2022
- 21 Evening Standard March 4, 2021
- 22 Evening Standard March 4, 2021 (Archived)
- 23 NCSCU.edu May 12, 2020
- 24, 25 Unlimited Hangout August 2022
- 26 Odysee, Radical w/Maajid Nawaz June 12, 2022, 1:05
- 27 Odysee, Radical w/Maajid Nawaz June 12, 2022, 1:09
- 28 Covid19criticalcare.com
Featured Video

Roosevelt’s Partnership with Stalin
or go to
Aletho News Archives – Video-Images
From the Archives
The great ADHD swindle
By Daniel Ken | TCW Defending Freedom | May 20, 2023
Over more than two decades in the classroom I’ve taught thousands of children and teenagers: some were lovely and lots were hard-working. On the other hand, quite a number were disruptive and argumentative, and a number were violently opposed to learning. But I don’t think I’ve taught more than a handful of kids who could be properly described as having the symptoms of ADHD. And that handful could just as easily have had something else wrong with them. Because here’s the thing: despite the fact that the best part of a million children are medicated for the condition, ADHD doesn’t exist.
There’s no definitive medical test for it, experts can’t agree on what it actually means, and most of the symptoms disappear if the child in question has lots of exercise, good diet and, crucially, a set of clear behavioural boundaries, preferably set early in childhood and, for the boys at least, enforced by a stable adult male living at home. … continue
Blog Roll
 Aletho News
Aletho News- Syria, Lebanon, and the limits of power
- How Multipolarity Forced Trump to Capitulate… For Now
- Switzerland confirms US-Iran talks planned for Friday are cancelled
- Iran Beat Back The Greater Israel Project
- Roosevelt’s Partnership with Stalin
- Strategic Ambiguity (If We Must)
- Finland shreds nuclear weapons ban
- Kiev turns to ‘systematic killing’ of Zaporozhye plant staff – Russia’s nuclear chief
- Censored Lavrov article Politico refused to publish (FULL TEXT)
- Israel’s censor silenced 5,700 reports in 2025
- If Americans Knew
- JD Vance speaks truth to Israel: “You can’t just kill your way out of every problem” – Daily Update
- What Ceasefire? Israel Has Now Killed Over 1,000 Palestinians in Gaza Since October
- U.S. Whole-of-Government Takeover by Israel
- Netanyahu’s Mouthpieces Turn on Trump, Revealing a Deeper Israeli Ingratitude
- Senate wants to force US to share sensitive intel with Israel
- Trump ended his idiotic Iran war. Good.
- Khanna Becomes First in Congress to Sign ‘Peace Pledge’ Promising to Reject AIPAC Funds
- Look who’s losing it over Trump’s Iran deal
- Israel has killed over 1,000 Gazans during 8-month “ceasefire” – Daily Update
- REVEALED: Former Top DEA Official Says Israel Spies on US Law Enforcement
- No Tricks Zone
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
