The Politics of Natural Infection
BY JEFFREY A. TUCKER | BROWNSTONE INSTITUTE | JUNE 2, 2022
From the very outset of this pandemic, the topic of natural infection has been a taboo. To suggest that anyone might have been better off risking infection and thereby gaining immunity from a respiratorial virus rather than hiding under the sofa for two years was seen as outrageous and irresponsible.
My theory is that the reason has always been political. And that’s tragic.
Generations have gone by that have understood it. A life strategy to flee all pathogens is deeply dangerous. The immune system, in order to be trained to protect against severe disease, needs exposure. Not to all things, of course, but to many pathogens that are not finally debilitating or fatal. We’ve evolved with pathogens in what Sunetra Gupta calls a “dangerous dance.” This dance is unavoidable, especially for fast-mutating viruses like SARS-CoV-2.
And yet from the beginning, this knowledge seemed to be lost. This is gravely embarrassing since it’s been known for 2,500 years. It was worse than just lost. As a person who wrote almost daily during the pandemic, I too was careful not to discuss this topic with too much bluntness. We all felt the political pressure to stay silent or at least cloud our prose with euphemisms.
The single most controversial sentence of the Great Barrington Declaration was this one: “The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk.”
That talk about building up immunity is what drove people bonkers, as if no one was somehow allowed to utter a settled scientific truth. And yet long before Fauci began to speak as if getting infected was the worst possible fate, he was more honest.
Even I knew (from what I learned in 9th grade and what my mother taught) that the pandemic would only end with endemicity naturally earned. That is precisely what is happening. The CDC’s publication MMWR printed a seroprevalence study showing that from December 2021 to February 2022 – that period during which it seemed like everyone in the country got covid – went from 33.5% to 57.7%. In children, it went from 44.2% to 75.2%. It’s higher in both groups now.That the study got no real attention to it shows that we are fast moving toward the end, and how? Not through vaccination, which protects against neither infection nor transmission. It ends with everyone meeting the virus. There is of course some threshold of herd immunity with this virus, though it keeps rising with each mutation, requiring ever more rounds of infection to achieve it. It is surely higher than 70% but probably less than 90% depending on population mobility and other factors.We can look at that data today and wonder. What if we had never locked down? What if we had gone on with life as normally while urging those in risk categories to wait it out a bit while we achieved endemicity? How long would it have taken to get there?
Might it have been over by the summer of 2020? It is possible. It’s hard to know such counterfactuals with precision, but it does seem highly likely that the lockdowns achieved nothing good, caused tremendous damage, and also unnecessarily prolonged the pandemic. In addition, they degraded everyone’s immune system: we didn’t just avoid covid but everything else too.
And the main reason was due to the unwillingness of public health authorities to talk about actual science. When Fauci was asked about natural immunity in September 2021, he said “I don’t have a really firm answer for you on that. That’s something that we’re going to have to discuss regarding the durability of the response…I think that is something that we need to sit down and discuss seriously.”
The WHO even changed its definition of herd immunity to exclude natural infection as a factor! The whole institution gave itself over to vaccine sales based on wild exaggerations of their effectiveness while all-but-denying robust and broad immunity through exposure.
A key political factor to natural immunity is that it does not call on government to assume totalitarian controls to stop a virus. It presumes the operations of a normal society. The government wanted all power and deployed it to stop the virus. Therefore, science was out of the question, replaced by political propaganda from start to finish.
It’s not well understood that the US policy from the very outset accepted and adopted a zero covid approach. That gradually unraveled over time as unworkable. Trump’s own advisors tricked him into believing that he could achieve that just like Xi Jinping did. He fell for it, and pushed the two weeks to flatten the curve under the belief that this would make the virus go away. His rhetoric that day set the stage for more than two years of utter nonsense.
And here we are all this time later and top headlines are finally admitting what should have been obvious from the beginning. For a virus this prevalent, it ends with widespread natural immunity. Here’s the Bloomberg headline:

The rest of the article is designed to walk back that core claim. We are still not ready to face the terrible realities that the lockdowns achieved nothing and that the vaccines did not end the pandemic. The taboo subject of meeting the virus is still today what it was 30 months ago, nearly unsayable.
My theory is that this is entirely for political reasons. They hatched a wild plan to control a virus that would come and go like all such viruses in history, and so therefore they had to pretend their efforts were essential to the great task. They never were. That’s the bitter reality.
Reflecting on this topic of exposure and immunity eventually leads a person to realize that we don’t need centralized control, coercion, and dictatorial power to manage a pandemic. Pandemics are unavoidable but they largely manage themselves while the best-possible outcomes rest with the intelligence of individuals informing choices based on their own risk assessment. (I feel like I’ve been writing some version of that sentence for 33 months.)
And this speaks to the big problem we have today. The people who did this to us have not admitted error and probably won’t. Despite all the failures, these same people are gearing up for another round of lockdowns based once again on the ideology that the worst-possible fate for anyone is to face a virus naturally and bravely.
Think about this: our lords and masters are saying that our only choice in the face of any prevalent pathogen is to hunker down, don’t hold parties, don’t send kids to school, don’t go to church, don’t go work, don’t travel, and instead just wait for them to make a fancy serum to inject in our arms, which we must accept whether we like it or not.
In short, a government that seeks to control all pathogenic spread is one with totalitarian powers that knows not human rights or freedoms.
Trudeau predicts new variants, says mandates must stay
The Counter Signal | June 2, 2022
While countries around the world continue to drop their COVID mandates, Trudeau says Canada’s are here to stay due to the risk from new variants that don’t even exist yet.
“The reality is, as much as people would like to pretend that we’re not, we’re still in a pandemic,” he said.
“There are Canadians who die every single day because of COVID-19 in our hospitals.”
Trudeau adds that vaccine mandates are needed to protect against variants that do not (yet) exist.
“We are still at risk, particularly at risk, as Fall approaches, of new variants.”
“. . . What will also further damage our tourism industry is if we get another wave. If we get more serious impacts from COVID.”
This announcement comes a day after Canadian airline Westjet’s CEO, Alexis von Hoensbroech, spoke out against the mandates.
“As vaccines are not preventing the spreading of the virus since Omicron, there is no more logic to maintain it,” he said.
Indeed, most countries dropped their COVID mandates weeks, if not months ago. The latest country to do so was Italy.
Additionally, even big Pharma and Bill Gates have acknowledged the futility of the current vaccines and their mandates.
In January, Pfizer CEO Albert Bourla admitted that two doses of the vaccine “Offer very limited protection if any.” He further claimed his team was working on a new vaccine, “Version 1.1,” to effectively tackle the Omricron variant. However, to date, nothing has been produced.
And last week at the WEF conference in DAVOS, Gates admitted the vaccine wears off fast and doesn’t block transmission.
Earlier this week, Liberals, NDP, and Bloq Quebecois members of Parliament rejected a motion to lift the travel restrictions that conservative members had put to a vote.
The next day, the Trudeau government extended the current requirements until at least June 30.
But, given that future variants are always possible, Trudeauian logic implies there’s no end in sight.
They’ve officially forbidden the practice of medicine in Ontario, Canada
By Steve Kirsch | June 1, 2022
Executive Summary
They are adopting authoritarian medicine in Ontario, Canada by requiring physicians to either follow authoritarian guidelines which are not science based, or have their license to practice medicine revoked.
If you live in Canada, please contact the members of the College of Physicians and Surgeons of OntarioCollege of Physicians and Surgeons of Ontario and let them know what you think of their actions.
If you live in California, which is about to go the same way, please donate NOW to the campaigns of Michael Huang and Brian Tyson.
Introduction
Dr. Ira Bernstein who practices medicine in Ontario, Canada is about to have his license to practice medicine revoked soon. Currently he is required by the authorities to operate under the following restrictions:
- Dr. Bernstein will not provide medical exemptions in relation to vaccines for COVID-19;
- Dr. Bernstein will not provide medical exemptions in relation to mask requirements for COVID-19;
- Dr. Bernstein will not provide medical exemptions in relation to diagnostic testing for COVID-19; and
- Dr. Bernstein will not prescribe ivermectin or hydroxychloroquine.
Furthermore, Dr. Bernstein is now required to post a sign in his waiting room that says this:
Dr. Bernstein must not provide medical exemptions in relation to vaccines, mask requirements or diagnostic testing for COVID-19. Dr. Bernstein must not prescribe ivermectin or hydroxychloroquine. Further information may be found on the College of Physicians and Surgeons of Ontario website at www.cpso.on.ca
What was his crime?
None of his patients complained. None of his patients were hospitalized or died from COVID. Nobody was harmed.
What was his crime? He didn’t toe the line and treat COVID patients like the College thinks they should be treated.
The message to physicians in Canada is clear: you either treat COVID patients using methods approved by the medical authorities or they’ll take away your livelihood for the rest of your life.
If this type of authoritarian medicine can happen in Canada, it can happen everywhere else in the world. No Canadian physicians are coming to Dr. Bernstein’s defense publicly because doing so would jeopardize their license.
Who is behind this? The College of Physicians and Surgeons of Ontario. They are listed here. I’m sure they are all proud of their actions because the President wrote this (emphasis mine):
The CPSO is here to help support physicians, and in doing so, fulfill our mandate to serve the public trust in Ontario’s health care. I am proud of the CPSO’s clear messaging to its membership regarding vaccine and mask exemptions. Our role is to protect the public and that includes protection from misinformation and risk of ignoring public health policies.
These people are incompetent. Their recommendations are based on politics, not science. They are the ones that should have their licenses revoked.
For example, they think masks work even though masks have never worked to slow or stop any virus in history and the best controlled large-scale study (in Finland) showed that wearing masks resulted in higher infection rates (as UCSF Professor Vinay Prasad pointed out). That’s what the best science says.
In Ontario, a doctor faces NO professional discipline for giving hundreds of children under 5, some as young as 6 months old, the COVID jab. No matter how many die, they will not be sanctioned.
I’ve reached out to the College to see if any members will appear on our weekly VSRF calls. Don’t hold your breath on that one.
Welcome to the new world of authoritarian medicine!
California is going to be implementing similar policies. Your state is next.
We’re basically on our way to implementing the same thing in California. Check out this article:

I received this message:
I hate to tell you but there is already a bill in the California legislature that is proposing just that: either a doctor does as he/she is told or his/her license could be revoked and/or disciplinary action could be taken. My father who was a practicing physician and surgeon for the better part of 40 years told me when I worked for him told me that the insurance industry would capture the medical industry within 25 years after the institution of Medicare. That was in 1975. That has now taken place. If the proposed California legislation goes through, we can kiss traditional medicine and the conscientious practice of medicine by unfettered medical practitioners goodbye. We have to oppose the legislation in California or it will spread like wildfire throughout this country and, yes, the US will be just like Canada.
And this message:
The same criminal and idiotic medical regulations are in place in Australia, and have been since the start of the Covid 19 “pandemic”. The Canadians must be singing from the same song-sheet as AHPRA (Australian Health Practitioners Regulation Authority). I wonder who wrote the lyrics?
It’s important to memorialize statements like this in the public record to show that there were millions of critical thinkers who were being ignored.
What you can do
If you live in Ontario, Canada, you can reach out and contact the members of the College and let them know what you think of their actions. Please don’t just sit back and let this happen.
If you live in California, please make a generous contribution to red-pilled doctors running for public office such as Michael Huang and Brian Tyson.
Please donate immediately as these doctors could really use the funds and the election is days away. It is now or never. Thank you.
The FDA’s proposed “Future Framework” is the worst idea in the history of public health
If approved on June 28, all reformulated Covid-19 shots will skip clinical trials
By Toby Rogers | May 31, 2022
I. Pfizer and Moderna’s Dilemma
Pfizer and Moderna have a problem — their Covid-19 shots do NOT work. Everyone knows this. The shots do not stop infection, transmission, hospitalization, nor death. Over half a billion doses of this product have been injected into Americans in the past 17 months and these shots have made NO discernible impact on the course of the pandemic. Far more Americans have died of coronavirus since the introduction of the shots than before they were introduced.
Pfizer and Moderna are making $50 billion a year on these shots and they want that to continue. So they need to reformulate the shots. Maybe target a new variant, maybe change some of the ingredients — who knows, these shots don’t work so it’s not clear what it will take to get them to work. This is a problem because reformulated shots mean new clinical trials and new regulatory review by the FDA. There is a decent chance that any reformulated shot might fail a new clinical trial and the public is deeply skeptical of these shots so the scrutiny would be intense.
So Pfizer and Moderna have figured out a way to use regulatory capture to get their reformulated Covid-19 shots approved WITHOUT further clinical trials. Their scheme is called the “Future Framework” and it will be voted on by the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) on June 28.
II. Doubling down on a failed strategy
Viruses vary by region. At any given time, the influenza strain circulating in England is different than it is in South Africa which is different than in southeast Asia. However, pharmaceutical companies prefer to create one-size-fits-all vaccines in order to decrease manufacturing costs and thereby increase profits. So the W.H.O. and public health agencies around the world (including FDA and CDC) have created a vast “influenza surveillance network” that identifies the different influenza strains in circulation. Then they engage in an elaborate theatrical performance called the “flu strain selection process” where they select four influenza strains that will go into the one-size-fits-all flu vaccine used throughout the world that year.
This carefully choreographed process is a complete and total failure. This is not a surprise — using a one-vaccine-fits-all approach to prevent a rapidly evolving virus that varies by region is never going to work. Lisa Grohskopf from the CDC’s Influenza Division reports that last year the flu shot was somewhere between 8% and 14% effective (based on data from seven sites that participate in the U.S. Flu Vaccine Effectiveness Network).

But a case study of a flu outbreak at the University of Michigan between October and November 2021 found that the effectiveness of the flu vaccine was literally zero.
![]()
Over the last thirty years, the federal government has paid out more compensation for adverse events in connection with the flu shot than any other vaccine — so we know that the shot comes with a high rate of harms. Given that the flu shot does not stop the flu, the harms thus outweigh the benefits.
In a sane world, the WHO, FDA, and CDC would admit that they made a strategic mistake and then change course to find better ways to support the human immune system. But we don’t live in a sane world. Instead, the FDA is proposing to take the failed flu strain selection process and apply it to future Covid-19 shots.
III. The FDA knew that Covid-19 shots would fail but they proceeded anyway
There are a quadrillion x quadrillion viruses in the world (literally more viruses on earth than stars in the known universe). Only a couple hundred of those seem to have the potential to impact human health. But some viruses make better candidates for a vaccine than others. Viruses that have been around a long time, that are very stable and evolve slowly are the best candidates for a vaccine.
Viruses that evolve rapidly are bad candidates for a vaccine. There is no vaccine for the common cold nor HIV because these viruses evolve too quickly. The SARS-CoV-2 virus is a bad candidate for a vaccine which is why all previous attempts to develop a vaccine against coronaviruses have failed (they never made it out of animal trials because all of the animals died during challenge trials or were injured by the vaccine).
What are some of the bad things that can happen when you vaccinate against a rapidly evolving virus? Original antigenic sin, antibody dependent enhancement, and the possibility of accelerating the evolution of the virus in ways that make it more virulent (and even more resistant to vaccination).
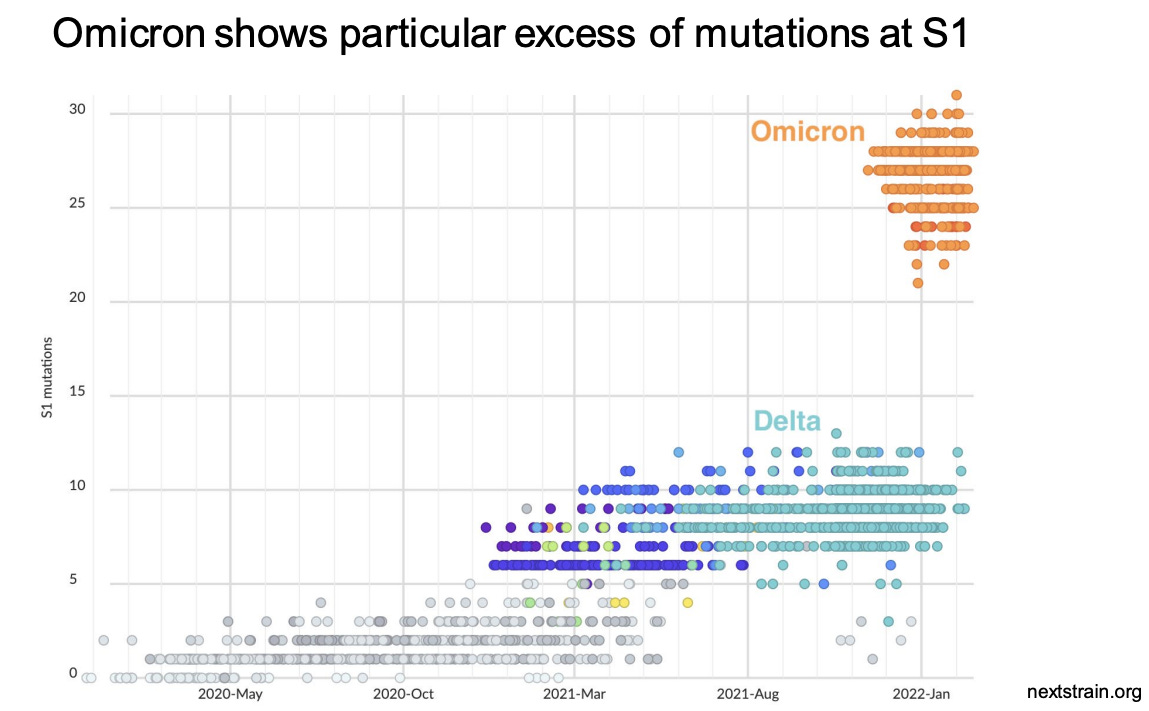
Trevor Bedford has his own lab at the Fred Hutchinson Cancer Center where he researches the evolution of Covid-19. He gave a fascinating presentation at the April 6 meeting of the FDA’s Vaccines and Related Biological Products Advisory Committee meeting where he explained that SARS-CoV-2 is evolving rapidly. He explained that SARS-CoV-2 evolves twice to ten times as fast as the flu virus and these mutations “substantially” reduce vaccine effectiveness. Following the introduction of Covid-19 vaccines, the evolution of the virus has accelerated.
Dr. Bedford’s presentation rattled some of the smarter members of the VRBPAC because his data scream — “SARS-CoV-2 is a bad candidate for a vaccine!” But FDA officials just mumbled some platitudes and then continued on with the meeting.
The only way out of the pandemic is to withdraw these vaccines from the market and pivot to therapeutics. Instead, the FDA is proposing to just hide the data from the American people.
IV. The “Future Framework” = no more clinical trials for Covid-19 shots ever again
The purpose of the “Future Framework” is to rig the Covid-19 vaccine regulatory process in perpetuity in favor of the pharmaceutical industry. If this “Future Framework” is approved all future Covid-19 shots, regardless of the formulation, will automatically be deemed “safe and effective” without additional clinical trials because they are considered “biologically similar” to existing shots.
This is literally the worst idea in the history of public health.
If you change a single molecule of mRNA in these shots it will change health outcomes in ways that no one can anticipate. That necessarily requires new clinical trials — which is what the FDA is proposing to skip.
The FDA’s “expert advisory committee” (VRBPAC) met on April 6, 2022 to discuss the “Future Framework” for the first time. All of the committee members agreed that Covid-19 shots are not working, that boosting multiple times a year was not feasible, and that the shots need to be reformulated. They also unanimously agreed that there are no “correlates of protection” that one can use to predict what antibody levels would be sufficient to prevent SARS-CoV-2 infection.
On June 28 the VRBPAC will meet once again to discuss the “Future Framework” and it will be presented as a done deal because manufacturers want a decision on vaccine strain selection by June in order to deliver shots for autumn vaccination appointments.
So if the FDA authorizes Covid-19 shots for kids on June 14 and 15 and then approves the “Future Framework” on June 28th, the shots that will be given to kids in the fall will be the reformulated shots that skipped clinical trials.
V. Monovalent Covid-19 shots failed, so maybe throwing two, three, or four variants into a single shot will make it better?
When it comes to the flu shot, the FDA tries to hedge their bets by putting four strains of the virus into a single shot (so called “quadrivalent” vaccines). As I explained above, this strategy does not work. But these people are not very clever so that’s exactly what they are planning to do with future Covid-19 shots.
Moderna is already signaling that they intend to manufacture a Covid-19 shot with the Alpha variant and then, to make it “new and improved (TM)”, they will add genetically modified mRNA targeting the Beta variant. Here’s the best part — Moderna claims that this formulation (Alpha + Beta) will somehow protect against Omicron variants — even though by the time these reformulated shots get to market, none of these variants will likely still be in widespread circulation.
There are reasons to believe that this approach will make future Covid-19 shots even less effective and more dangerous than the current failed Covid-19 shots.
Think about it. The more mRNA you put into a shot, the higher the adverse event rate (as the genetically modified mRNA hijacks the cell and starts cranking out spike proteins). So if Pfizer and Moderna put more mRNA into these shots (in order to cover multiple variants) adverse event rates will skyrocket.
But if Pfizer and Moderna put less mRNA per variant into a shot (in order to keep the total amount of mRNA at 100 mcg for Moderna and 30 mcg for Pfizer) then the effectiveness against any one particular variant will be reduced.
The Future Framework is 100% guaranteed to fail. If the “Future Framework” is approved, effectiveness of these shots will decrease, adverse events will increase, these shots will fuel the evolution of variants that evade the vaccines, and there will be no clinical trial data before these reformulated Covid-19 shots are unleashed on the unsuspecting public.
VI. Summary
The FDA’s Vaccines and Related Biological Products Advisory Committee will meet on June 28 to vote on a “Future Framework” for evaluating so-called “next generation” Covid-19 shots. The “Future Framework” is a plan to rig the Covid-19 vaccine regulatory process in perpetuity.
The “Future Framework” would take the “flu strain selection process” that fails every year and apply it to future (reformulated) Covid-19 shots. Federal bureaucrats, many of whom have financial conflicts of interests, would choose which SARS-CoV-2 variants to include in a yearly (or twice yearly) Covid-19 shot. In the process, all future Covid-19 shots will be deemed automatically “safe and effective” without further clinical trials because they are considered “biologically similar” to existing Covid-19 shots.
The “Future Framework” is the most reckless idea in the history of public health. It shows that the FDA has completely abandoned science and its statutory duty to protect the public. If the Republic is to survive, we must stop the “Future Framework” before June 28.
VII. Call to action
We have very little time and an enormous challenge in knocking this proposal down before the VRBPAC meets on June 28. So I am asking to you to contact your elected officials to tell them to reject this dangerous proposal.
Below are talking points that you can paste into an email, a script that you can use on the phone, and a tool for looking up your elected officials. I am only asking you to contact 8 officials — the President and Vice President; your two Senators and U.S. Representative; and your Governor, state House/Assembly member, and state Senator. Please be respectful but make it clear that this plan must be stopped.
Talking points (to paste into an email, letter, or fax)
Subject line: NO “flu framework” for future Covid-19 shots
The FDA and CDC are developing a “Future Framework” to authorize future Covid-19 shots without requiring additional clinical trials. This would be a public health disaster. I am asking you to contact the FDA to tell them to stop all work on this “Future Framework” immediately. If the FDA proceeds with this “Future Framework” I am asking you to eliminate all funding for the FDA in this year’s budget.
Phone script
Hi, my name is ____________. I live at __________________[address]. I’m calling because the FDA is proposing a “Future Framework” to authorize future Covid-19 shots without requiring additional clinical trials. This would be a public health disaster. I am asking you to contact the FDA to tell them to stop all work on this “Future Framework”. If the FDA proceeds with this “Future Framework”, I am asking you to eliminate all funding for the FDA in this year’s budget.
Whom to contact: 8 phones calls, letters, emails, or faxes:
President Joseph R. Biden
The White House
1600 Pennsylvania Ave NW
Washington, DC 20500
(202) 456-1111 (The White House comment line is open between the hours of 11 to 3 p.m. EST Tues.-Thurs.)
https://www.whitehouse.gov/contact/
https://twitter.com/POTUS
Vice President Kamala Harris
The White House
1600 Pennsylvania Ave NW
Washington, DC 20500
(202) 456-1111 (between the hours of 11 to 3 p.m. EST Tues.-Thurs.)
https://www.whitehouse.gov/contact/
https://twitter.com/VP
You can look up contact info for your two U.S. Senators and U.S. Representative here:
https://www.govtrack.us/congress/members/map
The message for State elected officials is slightly different:
Hi, my name is ____________. I live at __________________[address]. I’m calling because the FDA is proposing a “Future Framework” to authorize future Covid-19 shots without requiring additional clinical trials. This would be a public health disaster. If the FDA proceeds with this “Future Framework” I are asking you to nullify the actions of the FDA and reject any Covid-19 shots that have not gone through proper clinical trials.
This is a great tool to look up contact info for your Governor, state Senator, and state House/Assembly member:
That’s it, just 8 people. We want to let them know that we are watching, that we understand what they are up to, and that this wretched plan must be stopped.
Extra credit:
Here are the email addresses for all of the public health political appointees, FDA staff, and VRBPAC members who have a say in connection with the “Future Framework”. Let’s contact them as well (proposed subject line and email text below).
Subject line: The “Future Framework” is the WORST idea in the history of public health. Please vote NO.
1. The FDA must revoke the authorizations for Moderna, Pfizer, and J&J Covid-19 shots and withdraw them from the market immediately. SARS-CoV-2 was never a good candidate for a vaccine. These shots do not stop infection, transmission, hospitalization, nor death. They appear to have negative efficacy and are driving the evolution of variants that evade vaccines. The pandemic will never stop as long as the FDA and CDC are promoting shots that lack sterilizing immunity.
2. The FDA and CDC must pivot to therapeutics. This was always the answer. About twenty off-the-shelf treatments are more effective than vaccines (if used for prophylaxis or early intervention). Get these safe and effective medicines to people who need them and let doctors be doctors again and treat patients based on their own best clinical judgment.
3. Any reformulated Covid-19 shots MUST go through proper clinical trials and FDA review. That means:
• Large (50,000+ person) double-blind randomized controlled trials with inert saline placebos conducted by an independent third party;
• Safety and efficacy studies for two years prior to any application; the treatment and control groups must be followed for 20 years to monitor adverse events and all-cause mortality (no more wiping out the control group after 6 months to hide bad outcomes);
• Greater than 90% efficacy with less than 1% Grade 3 Adverse Events; and
• Proper monitoring for carcinogenesis, mutagenesis, and impairment of fertility.
sean.mccluskie@hhs.gov, commissioner@fda.hhs.gov, ashish.jha@whitehouse.gov, Aux7@cdc.gov, Peter.Marks@fda.hhs.gov, Hong.Yang@fda.hhs.gov,
Richard.Forshee@fda.hhs.gov, Huilee.Wong@fda.hhs.gov, Leslie.Ball@fda.hhs.gov, Doran.Fink@fda.hhs.gov, hanae@bcm.edu, paula.annunziato@merck.com,
adam.berger@nih.gov, hbernstein@northwell.edu, acohn@cdc.gov, anc0@cdc.gov, hjanes@fredhutch.org, hgans@stanford.edu, david.kim@hhs.gov,
asmonto@umich.edu, offit@chop.edu, spergam@fredhutch.org, Jportnoy@cmh.edu, erubin@hsph.harvard.edu, erubin@nejm.org, ashane@emory.edu,
swamy002@mc.duke.edu, fullerao@umich.edu, RandyHawkins@cdrewu.edu, officeofthepresident@mmc.edu, JYLee@uams.edu,
ofer.levy@childrens.harvard.edu, wayne_marasco@dfci.harvard.edu, cmeissner@tuftsmedicalcenter.org, mrn8d@virginia.edu,
Liberals vote to keep travel ban against unvaccinated Canadians
The Counter Signal | May 30, 2022
Members of parliament today voted 202-117 to keep the current travel ban against unvaccinated Canadians in place.
The Conservatives proposed the motion to have the current travel ban against the unvaccinated lifted.
Trudeau, Jagmeet Singh, and Travel Minister Omar Alghabra voted against the motion, as did virtually every Liberal, NDP, and Bloq Quebecois member.
Conservatives all voted to lift the ban.
“Today, the NDP-Liberal government voted against our common-sense motion that would have returned to pre-pandemic rules and service levels for travel and helped end the delays we’re seeing at airports across the country,” their Conservative’s website reads.
“As Canadian travellers are being subject to extreme delays, line-ups, bottlenecks, and missed connections because of unnecessary protocols, our allies across the world, including the European Union and the United States, have loosened rules for passengers on flights and in airports.”
“. . . Airports have directly cited the Liberals’ policies as the reason for these delays . . .”
“After two long years of the pandemic, Canadians are finally looking to return to normalcy and begin travelling again. Unfortunately, the NDP-Liberal government continues to cling to outdated and unnecessary protocols that are exacerbating delays.”
Conservative members of parliament proposed the motion on May 17. However, Charter rights – such as freedom of movement – were not leveraged to justify their call to drop restrictions.
Instead, “unacceptable wait times” at the airport (for those who are allowed to travel), labour shortages, and economic losses caused by the restrictions were cited.
However, the motion also mentioned that the restrictions were ineffective and that international allies have all dropped their restrictions.
Indeed, Canada remains one of the only countries to have a ban on unvaccinated citizens from leaving their own country, and the efficacy of the restrictions appears questionable at best.
The Trudeau Liberal government was expected to renew the federal vaccine policy eight weeks ago but has still not announced anything.
Fears of cover-up of vaccine caused deaths
Pathologist who said 30-40% of post-vaccine autopsies died of the vaccine went oddly silent and suddenly stopped carrying out autopsies
By Will Jones | The Daily Sceptic | May 31, 2022
If we are going to get to the bottom of whether and to what extent vaccines are contributing to the deaths of the vaccinated, autopsies are a crucial tool. So where are all the autopsies to help us answer these questions?
Back last summer, the Chief Pathologist at the University of Heidelberg, Dr. Peter Schirmacher, was pushing for many more autopsies of vaccinated people. His team had just finished conducting 40 autopsies of people who had died within two weeks of vaccination and concluded that 30-40% of them died from the vaccine.
Dr. Schirmacher warned of a high number of unreported deaths from vaccination and lamented that pathologists don’t notice most of the patients who die from a vaccination. The problem, he explained, is that vaccinated people do not usually die under clinical observation.
The doctor examining the corpse does not establish any context with the vaccination and certifies a natural death and the patient is buried. Or he certifies an unclear manner of death and the public prosecutor sees no third-party fault and releases the body for burial.
Dr. Schirmacher’s claims were dismissed at the time by Government scientists, but he stuck to his guns. “The colleagues are definitely wrong because they cannot judge this specific question competently,” he said. He clarified that he is in favour of the vaccines to fight Covid and has been vaccinated himself, but says the benefits and risks must be considered for each person. He argued in favour of “individual protection considerations” instead of quickly vaccinating everyone.
At the time, the Federal Association of German Pathologists was also pushing for more autopsies of vaccinated people. Johannes Friemann, head of the autopsy working group in the association, said this was the only way that connections between deaths and vaccinations could be ruled out or proven. The association had already in March 2021 sent a letter to Health Minister Jens Spahn requesting that German state governments instruct health authorities to order autopsies on site. Five months later, in August, this letter remained unanswered.
Following the reports in the media of his comments, Dr. Schirmacher fell oddly silent. Today, ten months later, no further autopsies by his group have been reported and no further calls for them have been heard. There are also no reports of autopsies being conducted specifically on those who died shortly after Covid vaccination in any other countries – save for the 15 done by Dr. Arne Burkhardt towards the end of 2021, which found “clear evidence of vaccine-induced autoimmune-like pathology in multiple organs” in 14 of 15 cases, but which were ignored by all health authorities and mainstream media.
Where are all the autopsies to investigate the role of vaccines in post-vaccine deaths, and why have Dr. Schirmacher and his colleagues gone quiet, after being so emphatic about the risks and the need?
This looks very much like a cover-up and a silencing. If it isn’t, then why don’t governments order autopsies to be carried out, to put the matter to rest? What have they got to hide?
Data shenanigans as Sweden misleads its public over vaccination-related mortality data
Health Advisory & Recovery Team | May 29, 2022
In December 2021 Norman Fenton, Martin Neil, Clare Craig, Josh Geutzkow, Joel Smalley, Scott McLachlan and Jonathan Engler published an article casting doubt on the vaccine efficacy implied by the UK’s official mortality statistics as they related to vaccination status, raising miscategorisation of vaccinated deaths soon after injection as unvaccinated as a possible significant factor.
The authors — as expected — were unable to publish this article in any mainstream journal, as anything which counters the government’s official position on anything related to the pandemic, especially vaccinations, has effectively been suppressed or censored throughout the last 2 years.
Despite repeated FOI requests by several parties, no UK government agency has ever released sufficiently granular data broken down into the necessary categories to permit any meaningful analysis of the extent (if any) of this miscategorisation issue.
Now, however, it appears that an FOI request to the Swedish Public Health Agency by 29 doctors and scientists has been successful in obtaining such data (for Sweden). They have written an article about it (in English) here.
The data is revelatory. It essentially shows that individuals dying within 2 weeks of vaccination have been classed and counted as unvaccinated. Incredibly, this applies to the 14 day period after the second as well as the first dose. The numbers involved are certainly non-trivial. In a substack blog, Jessica Rose has re-run the implied vaccine efficacy statistics in light of the new data categorizations.
In conclusion, the correct categorization turns the vaccine efficacy calculation totally on its head, suggesting a significantly increased risk of death in the vaccinated compared to the unvaccinated, rather than the vice-versa conclusion the authorities had originally touted. Whilst there is no age-breakdown, the magnitude of the reversal in the conclusions is nonetheless stark enough to conclude that there has been very serious and likely deliberate misrepresentation of what the mortality statistics truly imply about the efficacy of the vaccines against mortality.
One wonders how many other countries have played similar tricks with their data?
Post-script:
A further – anonymous – author has published an article claiming to build on Jessica Rose’s piece by calculating the mortality rates in the vaccinated and unvaccinated and comparing them to flu.
The author acknowledges the possible effect of age-confounding in the text, but in referring to it as having only a “slight” effect this understates its potential to interfere with his analysis; to draw the conclusions he /she does would in fact require a proper age breakdown of deaths month-by-month. However, if the analysis might lead to a misinterpretation of vaccine effectiveness because of the age bias then it is up to those with access to the data by age to refute the analysis.
The main take-away from the episode around this FOI is not that the vaccines are or are not efficacious (vs death), but rather that there has been a systematic miscategorization error which (1) seems likely to have been deliberate and (2) resulted in an extremely misleading picture of what the data suggests.
Such incidents – which now appear all too common in many countries – are likely to shatter the public’s trust in the institutions upon which we are supposed to rely.
Bill Gates: Next Pandemic Likely to be Caused by Climate Change

By Paul Joseph Watson | Summit News | May 30, 2022
Billionaire Bill Gates says there’s a 50 per cent chance the next pandemic will be caused by man-made climate change or be deliberately released by a bio-terrorist.
The Microsoft founder made the comments during an interview with Spanish news outlet El Diario.
Asserting that the next major pandemic is likely to occur within 20 years, Gates said, “It could be a virus made by man, by a bioterrorist who designed it and intentionally circulated it. That is a very scary scenario because they could try to spread it in different places at once.”
“Or it could be something that makes the leap from the natural world. The human population is growing and we are invading more and more ecosystems. That is why I calculate that there is a 50% chance that we will have a pandemic of natural origin in the next 20 years, as a consequence of climate change,” he added.
The prediction that climate change will cause a virus which will then require another global vaccine rollout is somewhat convenient for Gates given that he is heavily invested in both areas.
Gates reiterated the call made in his recent book to pump billions of dollars into researching future pathogens by creating a 3,000-strong team of specialists under the control of the World Health Organization, which would require a 25% budgetary increase.
Commenting on the recent outbreak of monkeypox, Gates said “there is very little chance” it will have an impact anything like coronavirus, although he cautioned that it could mutate into something significantly nastier.
Gates infamously warned of a coming super-virus five years before the emergence of COVID-19 during a 2015 TED talk.
As we highlighted earlier this month, Gates warned that COVID was not over and that there is likely to be an “even more fatal” variant of the virus coming.
During an event at the Munich Security Conference back in February, Gates said that “sadly” Omicron is a “type of vaccine” and has “done a better job getting out to the world population than we have with vaccines” by providing natural immunity.
FDA announces updated schedule for the June meetings regarding five pivotal vaccine decisions
Who needs data when you’ve got regulatory capture?
By Toby Rogers | May 29, 2022
I. The June FDA meetings
This week the Washington Post copied and pasted from a Pfizer press release to announce yet another scientific miracle(TM) that will completely fail in practice. In the process WaPo also got some quotes from the FDA who have now nailed down the schedule for the 4 meetings in June in which they intend to assemble the final pieces for Pharma’s permanent dominance over the American people.
The new schedule is as follows:
June 7, Novavax
June 14, Moderna in kids 6 to 17 years old
June 15, Moderna in kids 6 months to 5 years AND Pfizer in kids 6 months to 4 years
June 28, “Future Framework” (the plan to skip clinical trials in perpetuity)
There is a lot to parse in the WaPo’s brief article.
Contrary to the breathless headline, they still don’t have any data.
Pfizer and BioNTech said the 80 percent efficacy finding was preliminary and based on 10 cases of Covid-19 in the study population as of the end of April. Once 21 cases have occurred, the companies will conduct a more formal analysis of efficacy… Pfizer and BioNTech said they plan to finish filing data with the FDA this week — and warned that the efficacy number was fluid because results are still arriving.
Let’s recap how we got here:
🚩 The Pfizer clinical trial in kids under 5 failed in December 2021.
🚩 So Pfizer added a third dose and that trial also apparently failed in February (which is why Pfizer was forced to withdraw its application on February 10).
🚩 Now Pfizer is describing a jerry-rigged trial of a third dose in 1,678 kids ages 6 months to four years old. Pfizer did not disclose how the kids were divided between the treatment and control group so it is impossible to run our own calculations on efficacy. Out of that sample, 10 developed Covid — although it is not clear how the 10 were distributed between the treatment and control group. (I suppose some quant on Twitter will figure out how to work backwards from Pfizer’s claims to calculate the numbers in each of these categories but needless to say, this is not the proper way to do science.) Of course Pfizer also failed to describe the contents of the “placebo.”
How exactly will Pfizer double the number of Covid-19 cases in the clinical trial in the next month given that 74.2% of kids already had natural immunity in February which means that nearly 100% of children likely have natural immunity by now?
Also, is the FDA seriously considering basing national policy, that impacts 18 million children, by relying a study with only 10 cases? It appears that the FDA is not even pretending to care about science anymore.
What little data they have will be based on antibodies in the blood, not health outcomes in the real world. That’s strange because the members of the FDA’s Vaccines and Related Biological Products Advisory Committee unanimously acknowledged on April 6 that there are “no correlates of protection” in connection with Covid-19 shots (this means that there are no valid proxy measures, such as antibody counts, that can determine whether someone who has received this shot is immune to the virus or not.)
WaPo continues:
While the adult trials recruited tens of thousands of volunteers and waited to see if vaccinated people were better protected, the children’s vaccine trials were primarily designed to measure immune responses using blood tests.
No they were not “primarily designed to measure immune responses using blood tests.” The studies were intentionally undersized to hide harms from the shots in addition to other tricks that they use to skew the results (such as kicking you out of the trial if you call 911 or go the the emergency room). But when one shrinks the sample size, surprise! it becomes impossible to detect actual health benefits from the shots (the signal would have been tiny if at all, but when one uses a sample that small then any positive signal can also disappear into statistical insignificance.)
II. The bigger picture
Tony Fauci and the NIAID funded the creation of a chimera virus that escaped a bioweapons lab and killed 6.3 million people worldwide.
Public health authorities have blocked access to safe and effective prophylaxis and early treatment throughout the pandemic in order to create the market for Covid-19 vaccines.
Covid-19 shots skipped essential safety steps (e.g. challenge trials in animals) and were rushed to market with no long term data.
In practice the mRNA shots suppress immune function for 6 weeks after the first shot, provide about two months worth of protection against coronavirus, then efficacy wanes quickly and becomes negative after six months. Meanwhile, these shots cause more side effects than any vaccine ever invented.
Popular support for the current regime has collapsed. More people have died of Covid under Mr. I Believe the Science(TM) than under Orange Man Bad. Only hypochondriacs in blue states seek out additional doses. Meanwhile Sudden Adult Death Syndrome stalks the true believers. In the past 48 hours alone actor Ray Liotta, Andy Fletcher of Depeche Mode, British drummer Alan White (from the band YES), and comedian Phil Butler were all likely killed by Covid-19 shots. It’s impossible to hide all of the bodies at this point.
The FDA seems to know that their window is closing to implement the Final Solution. So they are rushing to put the finishing touches on their plans to inject this toxic junk into the littlest kids in America. The FDA knows that these shots cannot pass proper regulatory review so they’ve developed a plan to rig the process in favor of Pharma in perpetuity. On June 28, the FDA’s “expert advisory committee” will vote on a “Future Framework” whereby all future (reformulated) Covid-19 shots will automatically be deemed “safe and effective(TM)” without any additional clinical trials, on the theory that they are “biologically similar” to existing Covid-19 shots.
What this means is that by fall, the Covid-19 shots that they will be injecting into Americans of all ages will have a new formula that skipped clinical trials altogether.
Injecting people with genetically modified mRNA that skipped clinical trials is genocide. It’s slower than the Nazi Final Solution. But it’s genocide all the same. Indeed the slower pace of the FDA Final Solution (5% to 15% increase in all cause mortality every year) might be even more lethal in the long run. It’s sinister in that they are intentionally building in plausible deniability (‘the FDA said it was safe’) to help the medical establishment feel virtuous while participating in genocide.
I’ll just conclude by saying: be careful what you wish for FDA. The tide has already turned. The American people know exactly what you are doing. We have the receipts. It will be relatively easy to secure a conviction at Nuremberg 2.0 — we literally have you on video committing crimes against humanity. As a reminder, the courts have determined that “I was just following orders” is not a valid defense.
After Summer, Europe to Target the Unvaccinated
BY ROBERT KOGON | BROWNSTONE INSTITUTE | MAY 28, 2022
Anyone who imagines that the suspension of Covid-related measures in much of Europe means that those measures, and hence the C-19 vaccination campaign, are things of the past should have a look at the recent pronouncements on the subject of the European Commission, starting with Commission President Ursula von der Leyen’s April 27 statement on the “next pandemic phase.”
While acknowledging that the “emergency” phase of the pandemic is over – but apparently not, on her account, the pandemic as such – von der Leyen warns that “we must remain vigilant. Infection numbers are still high in the EU and many people are still dying from COVID-19 worldwide. Moreover, new variants can emerge and spread fast.” “But we know the way forward,” she concluded, “We need to further step-up vaccination and boosting, and targeted testing”. The emphasis is mine.
Note that von der Leyen does not merely say that vaccination and boosting should continue – say perhaps for particularly vulnerable groups – she says rather that they have to be “further stepped-up”! This in an EU in which, according to the European Centre for Disease Prevention and Control, nearly 85% of the adult population has already been fully vaccinated!
In the Commission press release, von der Leyen’s call for “stepped-up” vaccination and boosting is the first of a series of measures that member states are called on to take “before autumn.”
A factsheet on “COVID-19 – Sustaining EU Preparedness and Response: Looking ahead,” which was published by the European Commission on the same day, April 27, reiterates von der Leyen’s point. The first section is entitled “Increasing uptake of COVID-19 vaccination” and the first bullet point reads:
• Member States should increase vaccination uptake and the administration of boosters and fourth doses for those who are eligible. They should also increase vaccination among children.
Here, the emphasis is in the original. The second bullet point continues:
• Member States should prepare COVID-19 vaccination strategies for the coming months taking into account the simultaneous circulation of seasonal influenza and incorporate COVID-19 vaccination into national vaccination programmes.
On May 12, The European Parliament’s recently created special committee on the Covid-19 pandemic (COVI) hosted a question-and-answer session with EU Health Commissioner Stella Kyriakides. (Full video here.) In a tweet, the French Member of the European Parliament Virginie Joron summed up the gist of Kyriakides’s remarks as follows (author’s translation):
PRIORITY: 100 million unvaccinated in EU who will have to be convinced and targeted without discriminating against them.
> combatting misinformation
> next pandemic with new variants this winter
Like Kyriakides, incidentally, the Commission press release also identifies “intensify[ing] collaboration against mis- and disinformation on COVID-19 vaccines” as one of the priority actions for the fall.
Finally, in a more recent May 17 tweet, Virginie Joron shared the below photo of a Commission document that was distributed to the EU Parliament’s Internal Market and Consumer Protection Committee and that includes, in effect, a “vaccination strategy” for the fall. This document likewise “targets” the unvaccinated, its first bullet calling on EU member states to: “Strengthen efforts to increase the uptake or completion of the primary course among the unvaccinated or partially vaccinated including by continuously monitoring and analysing vaccine hesitancy to overcome it.”

The emphasis on “targeting” the unvaccinated is particularly puzzling given how rapidly vaccine-induced protection against Covid-19 is now known to wane. In immunological terms, once it has, there is, of course, no meaningful distinction to be made anymore between vaccinated and unvaccinated. Some studies and data even suggest that the vaccinated are at this point more prone to infection. Only the very recently vaccinated may perhaps enjoy some added protection.
Numerous observational studies have demonstrated how rapidly the efficacy of the Covid-19 vaccines wanes: in particular, that of the BioNTech-Pfizer vaccine, which is by far the most widely-used vaccine in the EU. But there is no need to cite these studies here, since the very next bullet point in the Commission document tacitly acknowledges the rapid waning of vaccine efficacy, calling on member states to: “Increase efforts on the uptake of booster doses by all eligible adults, starting from three months after the primary course.” The emphasis here is again mine.
The third and last vaccine-related bullet-point specifically concerns child vaccination. It is truncated in the document photographed by Joron, but the full version is to be found in the Commission’s most complete statement of its Covid-19 strategy for the fall: a communication to the Parliament and other EU institutions that likewise dates from April 27. The full version of the recommendation reads as follows: “Before the beginning of the 2022-2023 school year, consider strategies to increase vaccination coverage rates among younger children, e.g. by working with paediatricians and other health professionals who are trusted sources of information for many parents.”
It was considerate of Kyriakides to insist that the unvaccinated should not be discriminated against, even if they need to be “targeted.” But it should be noted that the April 27 communication, as reflected in Joron’s photo, also stresses the need to “[e]nsure the adoption of the Commission proposal to extend the application of the EU Digital COVID Certificate Regulation.” The main effect and purpose of the EU Digital Covid Certificate, which has also served as framework and infrastructure for domestic “health” or “vaccine” certificates in EU member states, is, of course, precisely to reward the vaccinated and discriminate against the unvaccinated.
The European Commission’s April 27th documents thus clearly invoke a new rollout of the Covid-19 vaccination campaign in the fall, specifically targeting the hitherto unvaccinated and also children. Moreover, if the Commission gets its way – as it can be expected to – and the EU Digital Covid Certificate is indeed extended, they also raise the specter of this new rollout being combined with exactly the same coercive, discriminatory measures that turned Europe’s unvaccinated into social pariahs for much of the last year.
Robert Kogon is a pen name for a widely-published financial journalist, a translator, and researcher working in Europe. He writes at edv1694.substack.com.
Featured Video

IRAN WAR “ON PAUSE” – w/ Prof. Glenn Diesen
or go to
Aletho News Archives – Video-Images
From the Archives
Because no animal reservoir has been found for SARS-CoV-2, it cannot properly be termed a zoonosis.* Should we call it a labnosis? And what does that mean?
By Meryl Nass, MD | July 12, 2021
After a year and a half of seeking but not finding SARS-2 in any wildlife anywhere (apart from domesticated or zoo animals that appear to have caught it from humans) is it time to say, yes, it didn’t just escape from a lab. It was created, built, assembled in a lab. Or many labs
Coronavirus scientists have been constructing new viruses out of bits and pieces of other viruses for a long time.
Why did they do it? … continue
Blog Roll
 Aletho News
Aletho News- Keir Starmer arson mysteries multiply
- IRAN WAR “ON PAUSE” – w/ Prof. Glenn Diesen
- Zelensky threatens to attack Belarus
- UK to send Ukraine 150,000 drones
- ‘Biased censorship’: Iran deputy FM slams X for stripping him of blue tick
- Hezbollah lawmaker says Israel has 60 days to withdraw from Lebanon
- Iran rules out IAEA inspections of war-damaged nuclear sites
- Israeli regime’s only interest is ‘permanent war,’ Iran’s FM Araghchi says
- Syria, Lebanon, and the limits of power
- How Multipolarity Forced Trump to Capitulate… For Now
- If Americans Knew
- Deaths in Gaza undercounted, possibly by 100s of thousands; “Psychopath” Ben-Gvir talks trash – Daily Update
- UNICEF: “Trauma is woven into the very fabric of childhood in Gaza”
- 15 articles a day: The extent of the Israeli army’s media interference
- Greek Orthodox Patriarchate denounces Israeli seizure of church land in Jerusalem
- How Hillel International uses antisemitism training and ‘campus climate’ concerns to attack Palestine solidarity
- Old Iraq war architects rise up against Trump’s Iran deal
- Unmasking Axios, its Israeli ties and agenda
- Israel Is Bleeding Support in the U.S. – and Pouring Tens of Millions Into Trying to Change That
- Israeli army included on UN blacklist for 3rd year over ‘grave violations’ against children
- Trita Parsi on the Iran deal, Israel, and how Iran has been a ‘cash cow’ for AIPAC
- No Tricks Zone
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
