CHD Says Pfizer and FDA Dropped Data Bombshell on COVID Vaccine Consumers
Children’s Health Defense | March 03, 2022
Washington, DC, — In a 55,000-page set of documents released on Tuesday, the U.S. Food and Drug Administration’s (FDA’s) Center for Biologics Evaluation and Research (CBER) is for the first time allowing the public to access data Pfizer submitted to FDA from its clinical trials in support of a COVID-19 vaccine license. This follows U.S. District Judge Mark T. Pittman’s decision on January 6 to deny the request from the FDA to suppress the data for the next 75 years which the agency claimed was necessary, in part, because of its “limited resources.”
A 38-page report included in the documents features an Appendix, “LIST OF ADVERSE EVENTS OF SPECIAL INTEREST,” that lists 1,291 different adverse events following vaccination. The list includes acute kidney injury, acute flaccid myelitis, anti-sperm antibody positive, brain stem embolism, brain stem thrombosis, cardiac arrest, cardiac failure, cardiac ventricular thrombosis, cardiogenic shock, central nervous system vasculitis, death neonatal, deep vein thrombosis, encephalitis brain stem, encephalitis hemorrhagic, frontal lobe epilepsy, foaming at mouth, epileptic psychosis, facial paralysis, fetal distress syndrome, gastrointestinal amyloidosis, generalized tonic-clonic seizure, Hashimoto’s encephalopathy, hepatic vascular thrombosis, herpes zoster reactivation, immune-mediated hepatitis, interstitial lung disease, jugular vein embolism, juvenile myoclonic epilepsy, liver injury, low birth weight, multisystem inflammatory syndrome in children, myocarditis, neonatal seizure, pancreatitis, pneumonia, stillbirth, tachycardia, temporal lobe epilepsy, testicular autoimmunity, thrombotic cerebral infarction, Type 1 diabetes mellitus, venous thrombosis neonatal, and vertebral artery thrombosis among 1,246 other medical conditions following vaccination.
“This is a bombshell,” said Children’s Health Defense (CHD) president and general counsel Mary Holland. “At least now we know why the FDA and Pfizer wanted to keep this data under wraps for 75 years. These findings should put an immediate end to the Pfizer COVID vaccines. The potential for serious harm is very clear, and those injured by the vaccines are prohibited from suing Pfizer for damages.”
The U.S. government has already purchased 50 million doses of the Pfizer vaccine intended for children under five years of age to be delivered by April 30, 2022 although the FDA has yet to grant an Emergency Use Authorization (EUA) for this age group. The risk of serious injury or death from COVID to healthy children is practically nil and so far, the vaccine is not effective when used in young children.
According to The Guardian, “Pfizer made nearly $37bn (£27bn) in sales from its Covid-19 vaccine last year – making it one of the most lucrative products in history – and has forecast another bumper year in 2022, with a big boost coming from its Covid-19 pill Paxlovid.” President Biden advertised Paxlovid in his State of the Union address on Tuesday, the same day the Pfizer data was released to the public. “We’re launching the ‘Test to Treat’ initiative so people can get tested at a pharmacy, and if they’re positive, receive antiviral pills on the spot at no cost,” Biden said during his speech.
From mid-December, 2020 through February 18, 2022, the U.S. government’s database, the Vaccine Adverse Events Reporting System (VAERS), has received 1,134,984 reports of adverse events, including 24,402 deaths, following COVID vaccination. Additionally, there have been 4,021 cases of myocarditis and pericarditis in the U.S. with 2,475 cases associated with Pfizer, 1,364 cases with Moderna and 171 cases with J&J’s COVID vaccine. These include 643 reports of myocarditis and pericarditis in children aged 12 to 17.
“It would be criminal to expose infants and young children to this extremely risky product,” said Holland. “VAERS data show the catastrophic health impacts the vaccine is having on millions of people, yet Pfizer and other vaccine makers are raking in billions of dollars with no fear of being held accountable for injuries and deaths from their vaccines.”
The FDA’s attempt to suppress these data in support of the pharmaceutical industry’s bottom line isn’t a new phenomenon in this country’s public health system. For more information on pharmaceutical corruption and the tight relationship the industry has with government regulatory agencies, read The Real Anthony Fauci: Bill Gates, Big Pharma and the Global War on Democracy and Public Health by CHD Chair and lead counsel Robert F. Kennedy, Jr.
###
Children’s Health Defense is a 501(c)(3) non-profit organization. Its mission is to end childhood health epidemics by working aggressively to eliminate harmful exposures, hold those responsible accountable, and establish safeguards to prevent future harm. For more information, visit ChildrensHealthDefense.org.
Most Kids Are Already Naturally Immune to COVID. So Why Are We Vaccinating Them?
The Defender | March 1, 2022
The “majority” of children in the U.S. have already been infected with COVID-19, The Washington Post today reported, after reviewing data from the Centers for Disease Control and Prevention (CDC).
The Post’s report begs the question: If so many kids have natural immunity to the virus, and, as reported Monday, the vaccines aren’t very effective in children 5 to 11 years old, why are public health officials, schools, businesses and others pushing to vaccinate kids?

Source: Centers for Disease Control and Prevention
During a security conference in Munich on Feb. 18, Bill Gates said:
“Sadly, the virus itself, particularly the variant called Omicron, is [a] type of vaccine — that is, it creates both B cell and T cell immunity — and it’s done a better job of getting out to the world population than we have with vaccines.”
Did Gates actually admit natural immunity to Omicron is succeeding where vaccines have failed — and that he’s “sad” about that?
Gates isn’t the only one talking about natural immunity these days.
Eric Topol, executive vice president of Scripps Research last month argued for including an option of natural immunity in the definition of “fully vaccinated.”
Even vaccine advocate Dr. Paul Offit, director of the Vaccine Education Center and member of the U.S. Food and Drug Administration’s vaccine advisory committee, is going to bat for recognizing natural immunity to COVID.
During a Jan. 25 interview, Offit described a meeting with Dr. Francis Collins, then-director of the National Institutes of Health, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, Dr. Rochelle Walensky, director of the Centers for Disease Control and Prevention (CDC) and U.S. Surgeon General Dr. Vivek Murthy where Offit was asked, along with three others, whether he thought natural immunity should count as a vaccine.
Offit and one other person said yes, natural immunity should count. But they were out-voted, leading U.S. health officials to decide natural immunity should not be recognized in the U.S, as an alternative to a vaccine mandate.
To this day, the CDC maintains this position in its official guidance for the public — despite the agency’s own studies showing natural immunity against COVID is superior to the immunity provided by COVID vaccines.
Some U.S. lawmakers think the CDC is wrong, as evidenced by the introduction of two the Natural Immunity Is Real Act in the Senate (S.2846) and the House (H.R. 5590).
The bills would require “all federal agencies to acknowledge and consider natural immunity to COVID-19 when promulgating any regulation related to the COVID-19 public health emergency.
But for now, in the U.S. at least, those states, businesses and schools requiring “proof of COVID vaccination” make no exceptions for people — including kids — who recovered from COVID, and therefore have natural immunity.
UK data show most unvaccinated kids already have natural immunity
Unfortunately, the CDC doesn’t provide up-to-date seroprevalence data for children in the U.S., but UK data may shed light on children and natural immunity.
The UK Office of National Statistics (ONS) early last month reported these data based on population sampling:
“In the week beginning 10 January 2022, the percentage who would have tested positive for antibodies against SARS-CoV-2 ranged from 90.2% to 93.3% for children aged 12 to 15 years and from 63.3% to 72.7% for those aged 8 to 11 years across the UK. Estimates show the percentage of children testing positive for antibodies against SARS-CoV-2 at or above 42 ng/ml.”
In the UK, vaccines have not yet been made available for the under 12 age group (except those who are at very high risk). The 63.3 to 72.7% is thus overwhelmingly due to natural immunity and not vaccination.
Also, as noted by the ONS, individuals testing below the threshold level may also have natural immunity, presumably in the form of T cells and B cells, where the antibodies have waned. Thus these data may be underestimates of the true population-level immunity.
The UK government had previously reported:
“It is estimated that over 85% of all children aged 5 to 11 will have had prior SARS-CoV-2 infection by the end of January 2022 with roughly half of these infections due to the Omicron variant. Natural immunity arising from prior infection will contribute towards protection against future infection and severe disease.”
The UK’s Joint Committee on Vaccination and Immunisation (JCVI) on Dec. 22, 2021, authorized the vaccine only for high-risk children ages 5 to 11.
Yet despite the encouraging data on natural immunity in this age group, the JCVI on Feb. 16, in updated guidance, expanded its recommendations to include a “non-urgent offer” of the vaccine to children who are not in a clinical risk group.
To be clear, the UK government authorized an mRNA vaccine for the original SARS-CoV-2 strain, to be made available in April, to a group of 5 million young healthy children — 85% or more of whom are expected to have natural immunity.
As John Campbell, Ph.D., said, if and when a future COVID wave ever comes, any possible beneficial effect from these shots will likely have waned.
Studies may explain why children are protected from SARS-COV2
A study in 2020 reported that cross cellular immunity and immunomodulation from previous existing childhood vaccines may provide protection against COVID infections.
A more recent study of children as young as 3 years old measured spike-specific T cell responses and found they were twice as high as those in adults. The authors suggested this is in part due to pre-existing cross-reactive responses to seasonal coronaviruses.
A January 2022 study demonstrated a protective effect from high levels of pre-existing immune cells generated by other coronaviruses like the common cold, which attack the proteins within the virus (nucleocapsid), rather than the spike protein on the virus.
According to the senior author of the study:
“The spike protein is under intense immune pressure from vaccine-induced antibodies which drives evolution of vaccine escape mutants. In contrast, the internal proteins targeted by the protective T cells we identified mutate much less.
“Consequently, they are highly conserved between the various SARS-CoV-2 variants, including omicron. This suggests that the existing cross-reactive T cells may provide better protection than an mRNA vaccine that focuses only on the original variant spike protein.”
Despite these studies, the latest data on how many children likely have immunity because they’ve recovered from COVID and the well-established scientific theory that natural immunity to a pathogen is superior to vaccine-induced immunity, places like New York City continue to demand proof of vaccination for all children age 5 and over in order for them to participate in extracurricular school activities, visit museums, zoos, theaters, gyms, and restaurants.
For the most comprehensive list of 150 research articles on natural immunity visit the Brownstone Institute.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Papua New Guinea’s pandemic leadership is an inspiration to us all
Harry Dougherty Blog | February 24, 2022
When I find myself arguing with pro mandate Australians in social media comment sections (tragic, I know) I get the impression that they desperately want the last couple of years they’ve squandered to have been worthwhile.
Australia’s official Covid19 death rate happens to be low by international standards, which makes it easier for the Dan Andrews fanboys to delude themselves that the sick cruelty they inflicted on their fellow citizens was justified.
For a recap, this cruelty includes but is not limited to:
- Prolonged mass house arrest
- Vaccine Passports
- Vaccine injuries and deaths in individuals (often young and not at serious risk from Covid) who were coerced into getting it.
- The four newborn babies in South Australia who died after domestic Covid19 travel restrictions prevented them from being transferred for specialist life-saving emergency treatment in Victoria.
- In Western Australia, the prevention of unvaccinated parents from visiting their sick children in hospital.
If I was Australian Prime Minister Scott Morrison, (that snivelling, gaslighting, modern-day Pontius Pilate), I would not want to admit that pointlessly I stole two years of quality life from my citizens and presided over state policies that killed people,
“Australians have made many sacrifices during this pandemic,… together we have achieved one of the lowest death rates in the world,” he says.
Achieved? Everywhere in the Oceania region has a low death rate by global standards. When will Papua New Guinea’s PM be praised for his inspirational leadership? Don’t hold your breath, but PNG is Australia’s immediate neighbour, (and the only other country on Earth with kangaroos), yet has a lower Covid19 death rate than does oz.
Could that be because of the success of PNG’s vaccination rollout? Did they her the sheep through the gate, so to speak?
Vaccination rate for Australia (at least one dose): 85%
Vaccination rate for PNG (at least one dose): 3.4%
Since we are only allowed to compare Sweden with its neighbours, it’s only fair that the same rules must apply to everyone. I assume vaccine passports aren’t really a thing in PNG. But they seem to be coping without them.
Covid19 deaths per million for Australia: 193/1M
Covid19 deaths per million for PNG: 69/1M
Most countries in Europe have relatively high death rates, though the few nations that had extremely low death rates (Norway and Finland) did not have the strictest measures. Lockdown rejecting Sweden’s death rate is firmly in Europe’s lower half.
At present, the UK is the least restricted country in Europe, possibly in the developed world and has been since July 2021, yet our (questionably recorded) Covid19 death rate is only the 22nd highest in Europe, currently slightly lower than that of Italy, which has vaccine passports and vaccine mandates, and surgical masks remain compulsory.
What would Australia’s death rate be were it somehow squeezed into the North Atlantic or continental Europe? We cannot know.
The Nudge: Ethically Dubious and Ineffective
BY GARY SIDLEY | BROWNSTONE INSTITUTE | MARCH 1, 2022
More and more people in the US will be wising up to their government’s use of behavioural science – or ‘nudging’ – as a means of increasing compliance with Covid-19 restrictions. These psychological techniques exploit the fact that human beings are almost always on ‘automatic pilot,’ habitually making moment-by-moment decisions without rational thought or conscious reflection.
The use of behavioural science in this way represents a radical departure from the traditional methods – legislation, information provision, rational argument – used by governments to influence the behaviour of their citizens. But why expend all that time and energy when, by contrast, many of the ‘nudges’ delivered are – to various degrees – acting upon the public automatically, below the level of conscious thought and reason?
By going with the grain of how we think and act, the state-employed ‘nudgers’ can covertly shape our behaviour in a direction deemed desirable by the regime of the day – an appealing prospect for any government. The ubiquitous deployment of these behavioural strategies – which frequently rely on inflating emotional distress to change behaviour – raises profound moral questions.
The UK has been an innovator in these methods, but they are now raising widespread disquiet here. In fact serious concerns about our Government’s use of behavioural science were previously raised in relation to other spheres of government activity. In 2019, a Parliamentary report found that the distress evoked in people targeted by behavioural insights in relation to tax collection may, in some instances, have led to victims taking their own lives.
In the Covid-19 era, it appears the behavioural scientists have been given free reign. As a retired consultant clinical psychologist, I – and 39 professionals from the psychology/therapy/mental health sphere – have become so concerned we are calling on the UK Parliament to formally investigate the government’s use of behavioural science. People across the world can glean from the UK experience what may also have been done to them, and what may be next.
The Behavioural Insights Team
The appetite for using covert psychological strategies as a means of changing people’s behaviour was boosted by the emergence of the ‘Behavioural Insights Team’ (BIT) in 2010 as ‘the world’s first government institution dedicated to the application of behavioural science to policy.’ The membership of BIT rapidly expanded from a seven-person unit embedded in the UK Government to a ‘social purpose company’ operating in many countries across the world. A comprehensive account of the psychological techniques recommended by the BIT is provided in the document, MINDSPACE: Influencing behaviour through public policy, where the authors claim that their strategies can achieve ‘low cost, low pain ways of nudging citizens … into new ways of acting by going with the grain of how we think and act.’
Since its inception in 2010, the BIT has been led by Professor David Halpern who is currently the team’s chief executive. Professor Halpern and two other members of the BIT also currently sit on the Scientific Pandemic Insights Group on Behaviours (SPI-B), which advises the Government on its Covid-19 communications strategy. Most of the other members of the SPI-B are prominent UK psychologists who have expertise in the deployment of behavioural-science ‘nudge’ techniques.
‘Nudges’ of concern: fear inflation, shaming, peer pressure
The BIT and the SPI-B have encouraged the deployment of many techniques from behavioural science within the UK Government’s Covid-19 communications. However, there are three ‘nudges’ which have evoked most alarm: the exploitation of fear (inflating perceived threat levels), shame (conflating compliance with virtue) and peer pressure (portraying non-compliers as a deviant minority) – or “affect,” “ego” and “norms,” to use the language of the MINDSPACE document.
Affect and Fear
Aware that a frightened population is a compliant one, a strategic decision was made to inflate the fear levels of all the UK people. The minutes of the SPI-B meeting dated the 22nd of March 2020 stated, ‘The perceived level of personal threat needs to be increased among those who are complacent’ by ‘using hard-hitting emotional messaging.’ Subsequently, in tandem with the UK’s subservient mainstream media, the collective efforts of the BIT and the SPI-B have inflicted a prolonged and concerted scare campaign upon the UK public. The methods used have included:
– Daily statistics displayed without context: the macabre mono focus on showing the number of Covid-19 deaths without mention of mortality from other causes or the fact that, under normal circumstances, around 1,600 people die each day in the UK.
– Recurrent footage of dying patients: images of the acutely unwell in Intensive Care Units.
– Scary slogans: for example, ‘IF YOU GO OUT YOU CAN SPREAD IT, PEOPLE WILL DIE,’ typically accompanied by frightening images of emergency personnel in masks and visors.
Ego and Shame
We all strive to maintain a positive view of ourselves. Utilising this human tendency, behavioural scientists have recommended messaging that equates virtue with adherence to the Covid-19 restrictions and subsequent vaccination campaign. Consequently, following the rules preserves the integrity of our egos while any deviation evokes shame. Examples of these nudges in action include:
– Slogans that shame the non-compliant: for example, ‘STAY HOME, PROTECT THE NHS, SAVE LIVES.’
– TV advertisements: actors tell us, ‘I wear a face covering to protect my mates’ and ‘I make space to protect you.’
– Clap for Careers: the pre-orchestrated weekly ritual, purportedly to show appreciation for NHS staff.
– Ministers telling students not to ‘kill your gran.’
– Shame-evoking adverts: close-up images of acutely unwell hospital patients with the voice-over, ‘Can you look them in the eyes and tell them you’re doing all you can to stop the spread of coronavirus?’
Norms and Peer Pressure
Awareness of the prevalent views and behaviour of our fellow citizens can pressurise us to conform, and knowledge of being in a deviant minority is a source of discomfort. The UK Government repeatedly encouraged peer pressure throughout the Covid-19 crisis to gain the public’s compliance with their escalating restrictions, an approach that – at higher levels of intensity – can morph into scapegoating.
The most straightforward example is how, during interviews with the media, Government ministers often resorted to telling us that the vast majority of people were ‘obeying the rules’ or that almost all of us were conforming.
However, in order to enhance and sustain normative pressure, people need to be able to instantly distinguish the rule breakers from the rule followers; the visibility of face coverings provides this immediate differentiation. The switch to the mandating of masks in community settings in summer 2020, without the emergence of new and robust evidence that they reduce viral transmission, strongly suggests that the mask requirement was introduced primarily as a compliance device to harness normative pressure.
Ethical questions
Compared to a government’s typical tools of persuasion, the covert psychological strategies outlined above differ in both their nature and subconscious mode of action. Consequently, there are three main areas of ethical concern associated with their use: problems with the methods per se; problems with the lack of consent; and problems with the goals to which they are applied.
First, it is highly questionable whether a civilised society should knowingly increase the emotional discomfort of its citizens as a means of gaining their compliance. Government scientists deploying fear, shame, and scapegoating to change minds is an ethically dubious practice that in some respects resembles the tactics used by totalitarian regimes such as China, where the state inflicts pain on a subset of its population in an attempt to eliminate beliefs and behavior they perceive to be deviant.
Another ethical issue associated with these covert psychological techniques relates to their unintended consequences. Shaming and scapegoating have emboldened some people to harass those unable or unwilling to wear a face covering. More disturbingly, the inflated fear levels will have significantly contributed to the many thousands of excess non-Covid deaths that have occurred in people’s homes, the strategically-increased anxieties discouraging many from seeking help for other illnesses.
Furthermore, a lot of older people, rendered housebound by fear, may have died prematurely from loneliness. Those already suffering with obsessive-compulsive problems about contamination, and patients with severe health anxieties, will have had their anguish exacerbated by the campaign of fear. Even now, after all the vulnerable groups in the UK have been offered vaccination, many of our citizens remain tormented by ‘COVID-19 Anxiety Syndrome’), characterised by a disabling combination of fear and maladaptive coping strategies.
Second, a recipient’s consent prior to the delivery of a medical or psychological intervention is a fundamental requirement of a civilised society. Professor David Halpern explicitly recognised the significant ethical dilemmas arising from the use of influencing strategies that impact subconsciously on the country’s citizens. The MINDSPACE document – of which Professor Halpern is a co-author – states that, ‘Policymakers wishing to use these tools … need the approval of the public to do so’ (p74).
More recently, in Professor Halpern’s book, Inside the Nudge Unit, he is even more emphatic about the importance of consent: ‘If Governments … wish to use behavioural insights, they must seek and maintain the permission of the public. Ultimately, you – the public, the citizen – need to decide what the objectives, and limits, of nudging and empirical testing should be’ (p375).
As far as we are aware, no attempt has ever been made to obtain the UK public’s permission to use covert psychological strategies.
Third, the perceived legitimacy of using subconscious ‘nudges’ to influence people may also depend upon the behavioural goals that are being pursued. It may be that a higher proportion of the general public would be comfortable with the government resorting to subconscious nudges to reduce violent crime as compared to the purpose of imposing unprecedented and non-evidenced public-health restrictions. Would UK citizens have agreed to the furtive deployment of fear, shame and peer pressure as a way of levering compliance with lockdowns, mask mandates and vaccination? Maybe they should be asked before the government considers any future imposition of these techniques.
A truly independent and comprehensive evaluation of the ethics of deploying psychological ‘nudges’ – during public health campaigns and in other areas of government – is now urgently required, not only in Britain, but in all countries where these interventions have been used.
Dr Gary Sidley is a retired consultant clinical psychologist who worked in the UK’s National Health Service for over 30 years, a member of HART Group and a founder member of the Smile Free campaign against forced masking.
Google suppresses America’s Frontline Doctors in search results
By Didi Rankovic | Reclaim The Net | February 28, 2022
More evidence is emerging of Google manipulating algorithms powering its mammoth and highly influential search service to give certain results (much) more visibility than others.
And now, reports say, Google is not even trying to hide that this is the case, as America’s Frontline Doctors (AFLDS) has been informed its reach on the internet is being artificially limited.
This organization says it is dedicated to improving doctor-patient relationships that are jeopardized by what it calls politicized science and biased information. The AFLDS would also like to provide patients with access to “independent, evidence-based information” that will inform people’s decisions regarding their healthcare choices.
Well, meeting that goal might prove to be quite difficult since Google Search, on which a huge majority of US-based users rely for their internet queries, says it is deliberately deranking information coming from the AFLDS.
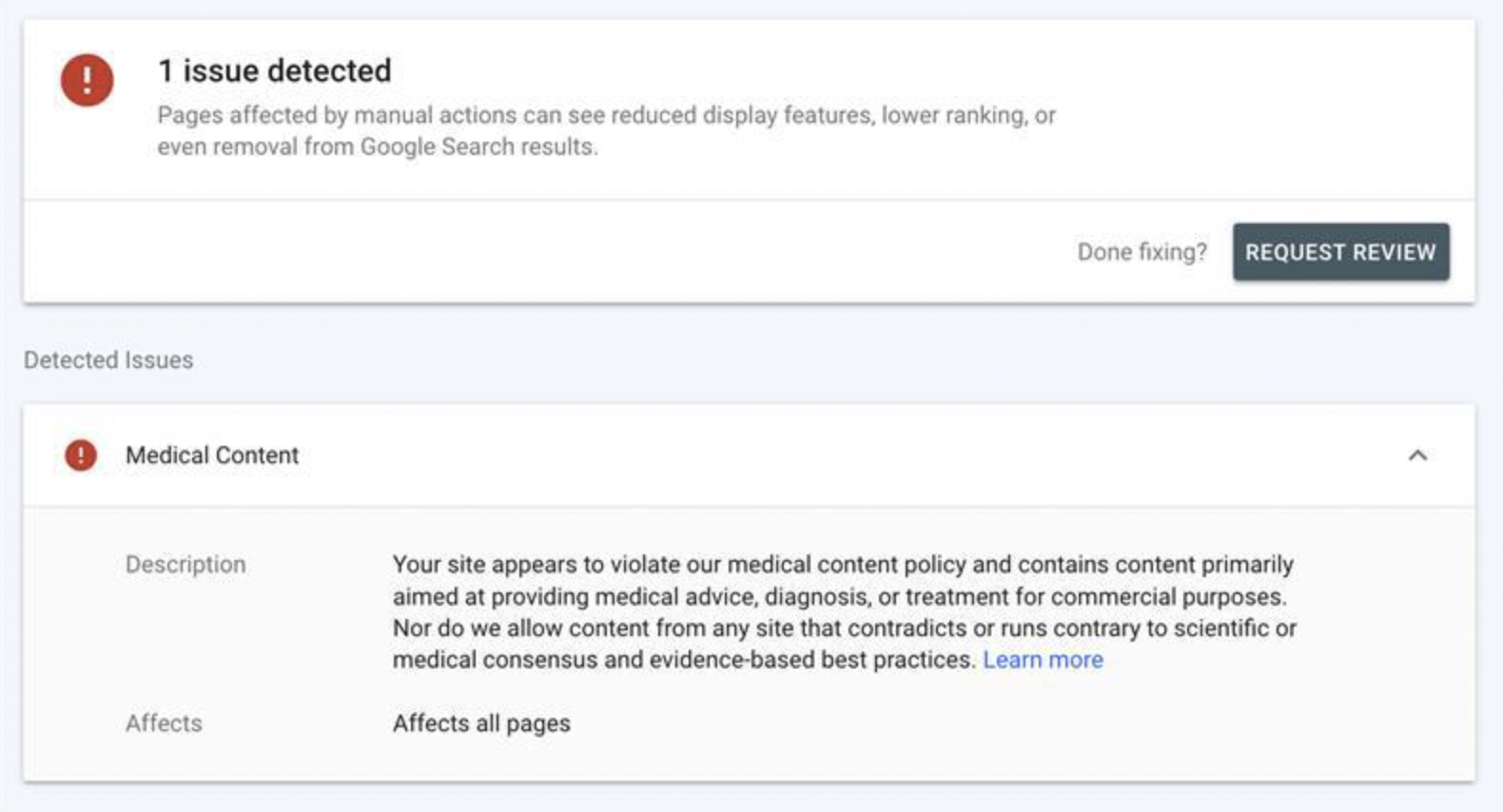
This transpires from alerts Google has been sending the organization, which state that an “issue” has been detected, which can be “fixed;” after that, the AFLDS can “request review.”
And when an “issue” has been detected, Google spells it out that “Pages affected by manual actions can see reduced display features, lower ranking or even removal from Google Search results.”
So what “issues” have been detected, you might ask next. Google’s “explanation” is the usual hodgepodge of vague language and qualifiers, in line with the giant’s now well-established censorship style.
The AFLDS is informed that its site “appears to violate” Google’s medical content policy, which is not allowed – and neither is content that “contradicts or runs contrary to scientific or medical consensus and evidence based best practices.”
That’s according to Google’s rules. What consensus, reached by who, and what best practices, determined by who, and at what time – none of this information is provided in the notices.
Google’s rigid, authoritarian style of promoting one-sided content and eliminating different arguments and positions would in this case work by first deranking (and eventually removing) AFLDS links – unless the group agrees to self-censor.
And that means deleting content from the site, and then clicking on “‘Request Review’ button which is prefaced with the question, ‘Done fixing?’,” the AFLDS explains.
The organization also takes issue with Google’s (deliberately) broad and ambiguous wording and lack of proper, or any definition of scientific and medical consensus and best practices – to ask why, “In a time when celebrities and computer programmers are allowed to express their views on virology, but actual doctors and scientists are censored, including the hundreds of doctors comprising AFLDS, such clarity is elusive.”
The great debate: PolitiFact vs. “the world’s top misinformation spreaders”
The request from PolitiFact to remove the fact check recording
By Steve Kirsch | February 25, 2022
Recently, I got an email from PolitiFact’s Editor-in-Chief, Angie Holan, requesting I remove the recording of my conversation with their so-called “fact checker,” Gabrielle Settles who was doing a fact check on VAERS.
I refused her request.
Gabrielle asked if she could record the call and I consented, so that entitles all parties to record the call. PolitiFact did not deny that we both consented. She wrote,
I am not in the least embarrassed by how she conducted the interview. I’m asking that you remove the video as a professional courtesy because the reporter did not consent to be recorded.
First of all, she should be embarrassed by the interview. The interviewer was clearly focused on proving an agenda and showed no interest in exploring evidence that was counter her agenda. I gave her the story of the century if she would just follow up on what I suggested she do.
Secondly with respect to permission, by asking me if it was OK to record the call, she is giving implied consent for the call to be recorded since she is doing the asking. All parties on the call consented to being recorded meaning the conversation is no longer private and all parties can record the call.
The debate challenge
I then raised the stakes: I challenged PolitiFact to a debate to settle the matter once and for all in front of a live Internet audience as to who are the liars and who are the truth tellers. Here is the email I sent on Feb 25, 2022 at 2:58pm PST:
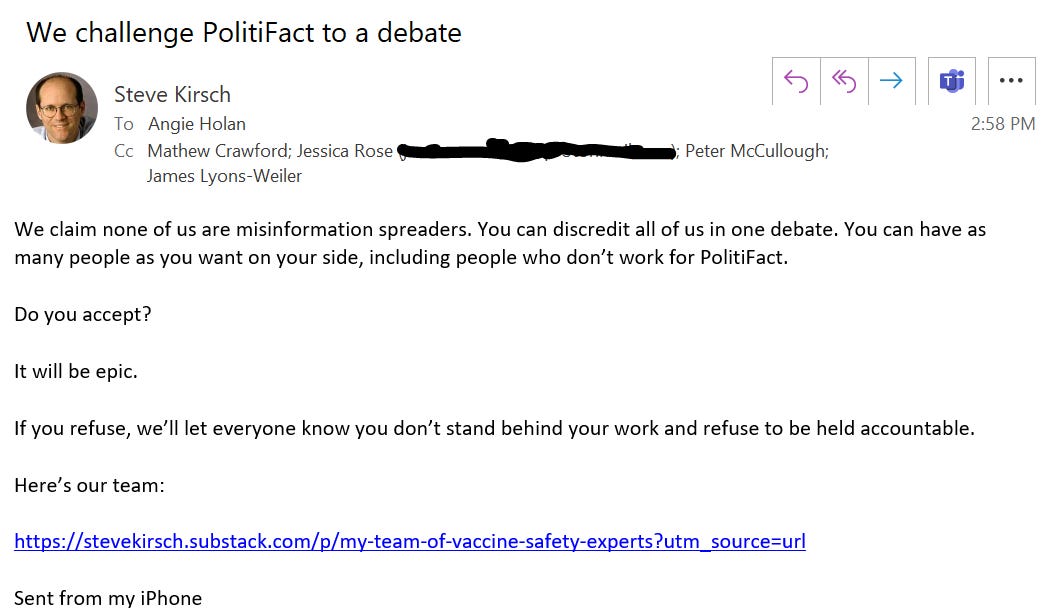
A good, old-fashioned debate.
They can have as many people as they want on their side, the more the better since it will remove all excuses when they lose.
We can use the debate rules suggested here, or anything else they are comfortable with.
The purpose is simple: to ascertain who is really spreading misinformation.
After all, the US Surgeon General has said how dangerous COVID-19 misinformation is. So has the California State Legislature: In House Resolution No. 74 of the 2021–22 Regular Session, the California State Assembly declared health misinformation to be a public health crisis, and urged the State of California to commit to appropriately combating health misinformation and curbing the spread of falsehoods that threaten the health and safety of Californians.
The fastest way to stop all COVID misinformation is to challenge the spreaders of the misinformation and discredit them in a debate
Of course, the problem with a debate is that usually one side wins. If it is the misinformation spreaders, the narrative is crushed. This is why nobody wants a debate: they can’t take the risk.
PolitiFact can’t win a fair debate. There is way too much information out now on how dangerous the vaccines are that is impossible for them to explain.
This is why I don’t think that there is a snowball’s chance in hell they will accept.
I sent the email to Angie earlier today and have not heard back. I will update this article if I do. Don’t hold your breath.
Watch the video that they don’t want you to see
The video they wanted me to remove exposes how the fact checker had absolutely no interest in exploring any of the evidence that proved that the VAERS data was correct.
In short, the video proves that these so-called fact checkers aren’t interested in the facts; they are interested in defending the false narrative.
Be sure to check out the original story (it’s point #5 in this article), and be sure to watch the video if you haven’t already. It shows just how biased these fact checkers are.
Be sure to check out the comments at Rumble on the video:
Other points about VAERS:
- The CDC warns in boldface lettering on its website, “[k]nowingly filing a false VAERS report is a violation of Federal law (18 U.S. Code Section 1001) punishable by fine and imprisonment.”
- Not only are there criminal penalties for filing false VAERS reports, but physicians or medical providers file a majority of them. Dr. McCullough says health care providers file 60 to 80% of VAERS reports. You can verify this by reading the reports.
- Whoever files the report has to have the lot number and batch number of the vaccine and it’s fairly time consuming process. McCullough says that the CDC has analysts call whoever entered the report in order to verify it. McCullough has received those calls.
- Doctors are of course not compensated for filing VAERS reports so they often don’t file them. Most are probably unaware that they are required to file VAERS reports. No one gives them training on filing VAERS reports. Hospital employees have said their hospitals don’t even know about the requirement to report VAERS injuries.
Read more about fact checkers
See this article.
In the meantime, California wants to ensure that no doctor can question whatever the government says
California just introduced a bill that would enable medical boards to take away the license of any doctor who spreads “COVID-19 misinformation.” This is a tacit admission that they can’t win on the facts, so they have to use threats and intimidation to keep the truth from emerging. Their only weapon is censorship.
Here’s the bill: AB-2098.
They define COVID-19 misinformation as anything going against the government narrative.
In short, they want to take away the free speech rights of doctors who would no longer be allowed to question anything the government says. After they do that, citizens will be next.
See this California Globe article, CA Lawmakers Propose Bill to Punish Doctors Who Speak Against COVID Treatment ‘Consensus’, for more info.
Florida is doing the opposite: Protecting the rights of doctors to speak freely
Meanwhile, Florida is doing the opposite by proposing a law that would protect the rights of doctors to speak the truth.
We live in interesting times.
Comments from my good friend Dr. Byram Bridle
Byram tried to debate the authorities in Canada, but they were a no show. He likes courts because the other party is forced to appear.
Here is what he wrote:
Hi Steve, I can’t get any of the narrative-pushers in Canada to debate the science. It would be great if you could have some success with this in the US. But, I agree with you; they almost certainly won’t. Those who don’t stand on the science will never engage in a conversation. People who love the narrative need to start asking their ‘champions’ why they keep refusing to step into the arena with the dissidents. At some point they are going to have to admit that their ‘champions’ are cowards and do nothing more than ‘talk the talk’ from behind their keyboards. A lack of scientific expertise becomes quite apparent when one has to respond off-the-cuff to another scientist in real-time. One place that the ‘experts’ for the narrative cannot hide is in court. So far, I have been seeing them crushed in this venue. This is why many court decisions are being made on technicalities; to avoid ruling on the evidence, the weight of which is not in favor of the narrative.
They are censoring doctors in the UK
From the comments:
GPs have been warned that criticising the Covid vaccine or other pandemic measures via social media could leave them ‘vulnerable’ to GMC* investigation.’1
*GMC = General Medical Council. This is the body that can strike doctors from the medical register so they cannot work as a doctor.
‘Vulnerable to GMC investigation’. What a deliciously creepy phrase that is, dripping with unspoken menace, whilst pretending to be helpful. It sounds like something the Mafia would come up with.
‘I would keep quiet about this, if I were you.’ Baseball bat tapping gently on the floor. ‘No, this is not a threat, think of it as advice from a friend. We don’t like to see anybody making themselves, or their family, vulnerable, and getting seriously injured now, would we?’
It seems that, unless you prostrate yourself before the mighty vaccine, and intone ‘Our vaccine, which art in heaven, hallowed be thy name…’ and suchlike, you will be attacked from all sides … simultaneously. Indeed, to suggest that vaccines are not perfect in every way is the twenty first century’s equivalent of blasphemy.”
See: https://drmalcolmkendrick.org/2022/02/23/a-few-thoughts-on-covid19-vaccination/
They are censoring doctors in Australia
Elizabeth Hart in the comments notes that muzzling doctors from questioning the Covid jabs is the same in Australia.
AHPRA, the regulator of ‘health practitioners’ here, issued a Position Statement dated 9 March 2021, which states: “Vaccination is a crucial part of the public health response to the COVID-19 pandemic. Many registered health practitioners will have a vital role in COVID-19 vaccination programs and in educating the public about the importance and safety of COVID-19 vaccines to ensure high participation rates.”
Health practitioners are also warned: “Any promotion of anti-vaccination statements or health advice which contradicts the best available scientific evidence or seeks to actively undermine the national immunisation campaign (including via social media) is not supported by National Boards and may be in breach of the codes of conduct and subject to investigation and possible regulatory action.” (Search for AHPRA position statement 9 March 2021 to download PDF.)
Who defines what is “the best available scientific advice”? We know what a disastrous quagmire of conflicts of interest is “the best available scientific advice”…
In regards to ‘anti-vaccination’, in practice, any questioning of Covid jabs in Australia is regarded as ‘anti-vaccination’, as tennis star Novak Djokovic discovered when he tried to come here recently to participate in the Australian Open. The Immigration Minister banished Djokovic from Australia because he “has previously stated that he ‘wouldn’t want to be forced by someone to take a vaccine’ to travel or compete in tournaments”. For being an individual wanting to retain his bodily autonomy, Immigration Minister Alex Hawke considered the presence of Djokovic “may be a risk to the health of the Australian community”, presumably as Djokovic might inspire Australians to make their own informed decision about the Covid-19 jabs, counter to government diktats. (See the court judgement here: https://www.judgments.fedcourt.gov.au/judgments/Judgments/fca/full/2022/2022fcafc0003 )
What does the antagonism against Novak Djokovic mean for critical thinking Australians who have similarly made their own informed decision to refuse to consent to Covid jabs that don’t prevent infection nor transmission, injections which purportedly provide questionable ‘protection’ of very limited duration, against a disease it was known from the beginning wasn’t a serious threat to most people?
Now we have a dire situation in Australia where millions of people have been coerced to be jabbed to maintain their livelihoods under state government and business/employer mandates, this directly flouts the obligation for valid voluntary consent to be given before vaccination.
I’ve complained about this matter to medical organisations in Australia, see my email to the Medical Board of Australia, AHPRA, RACGP, RACP, AMA, 8 June 2021: https://vaccinationispolitical.files.wordpress.com/2021/06/coercive-covid-19-injections-in-australia-medical-board-of-australia-ahpra-racgp-racp-ama.pdf
After perseverance, I finally received a response from AHPRA, which confirms: “Practitioners have an obligation to obtain informed consent for treatment, including vaccination. Informed consent is a person’s voluntary decision about health care that is made with knowledge and understanding of the benefits and risks involved.” See: https://vaccinationispolitical.files.wordpress.com/2021/10/response-from-ahpra-re-informed-consent.pdf
But this isn’t happening! With so many people being coerced and manipulated into submitting to the jabs under state government and business/employer mandates, this isn’t authentic voluntary consent. The situation is really bad in Australia, which I suspect is possibly the most mandated jab country in the world.
Summary
We want to make sure people know the truth about PolitiFact. I literally handed Gabrielle Settles the story of the century and she had no interest at all in pursuing any of it.
Everyone should watch the video of how they operate.
If PolitiFact and others want to end misinformation, all they have to do is debate us. Instead, governments are passing laws to censor doctors since they don’t have the facts on their side.
All over the world, governments do not want the people to hear the fully story.
If vaccines work, then why are they bending the curves in the wrong direction?
el gato malo – bad cattitude – february 27, 2022
israel has been a good laboratory for covid intervention assessment. they are a small nation in one climate zone with a small population, good record keeping, a pretty honest set of health agencies, and modern healthcare system. they did lots of testing and they also pursued damn near every mitigation in the book from lockdowns to masking to mandating vaccines and vaccine passports. and unlike many places, they were extremely serious about compliance. they even have an very useful control group in palestine that did almost none of these things.
this provides an interesting opportunity to measure the efficacy of such interventions. at this point, it’s so well established that masking and distancing have no effect that we can more or less drop them from consideration and focus solely on vaccines. (to the extent they worked, they would drive apparent vaccine efficacy in israel anyhow).
and the two states have had remarkably similar overall outcomes and had near identical cumulative deaths per capita through 2021. however, it looks like this might be starting to diverge and this creates a useful comparison.
about three weeks ago, i left THIS POST with some questions:
we now have enough data to start to answer this.
the relative vaxx rates are very different and israel is over 50% boosted vs ~0 in palestine. so, if boosters are working, this is about as good a natural experiment setup as you could ask for.
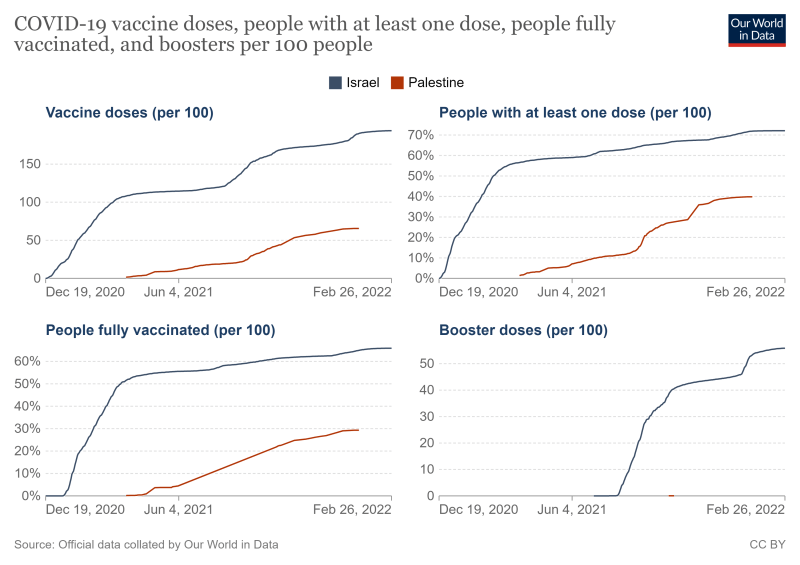
cases are a problematic metric due to variance in testing rates (and we know vaccines do not stop cases) and palestine does not report hospital data. but we can compare deaths, so this is the figure i used.
OWID is the source for all data.
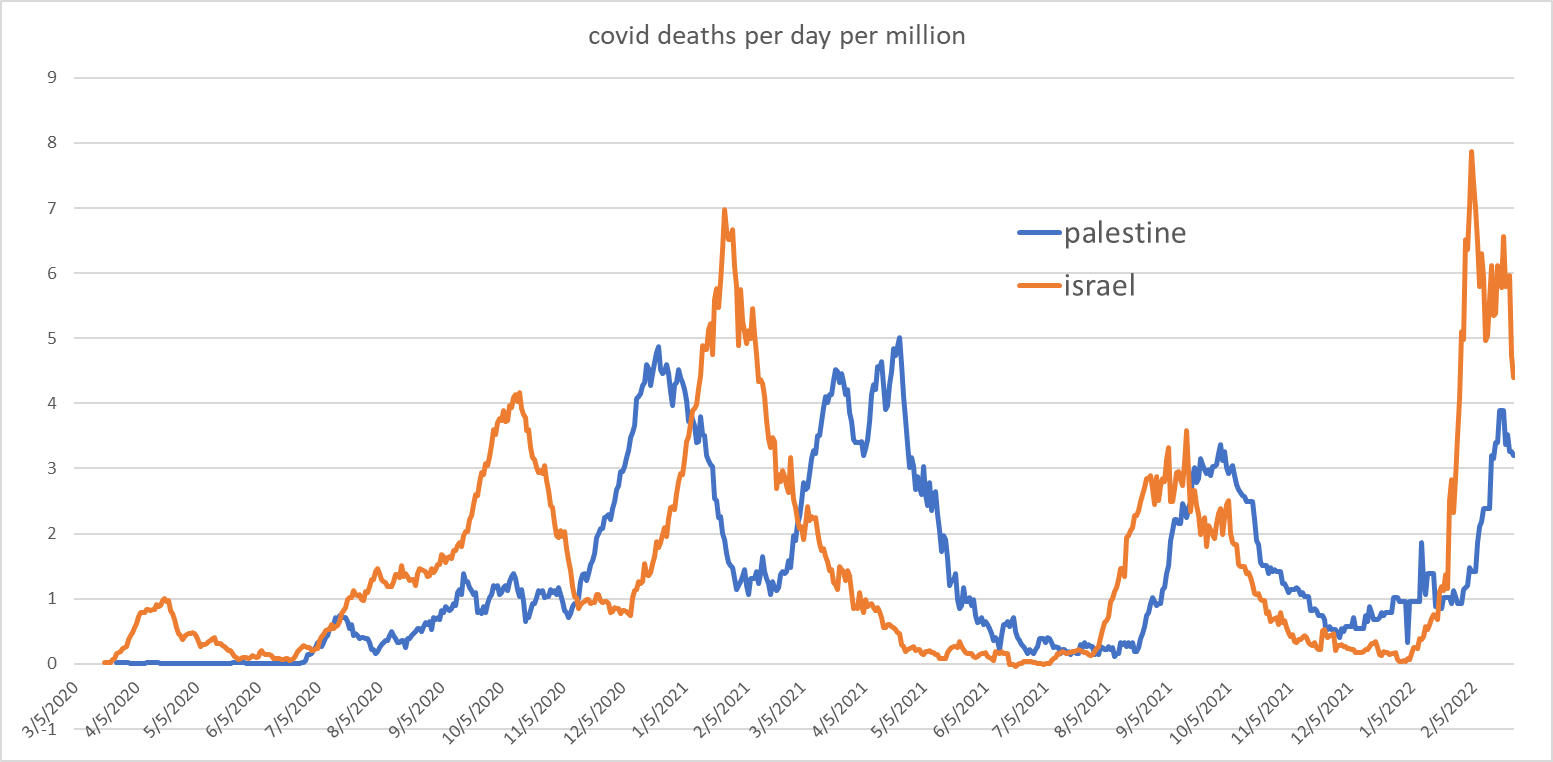
this series is striking. as has commonly been the case, palestine lagged israel by a couple weeks. (i suspect this is reporting lag, this data is day of report, not day of incidence).
assuming this peak holds, the palestine peak was 21% below winter seasonal peak last year. israel was up 13%. that’s a meaningful divergence and the israeli figure is deeply unexpected given a milder variant and 18 months of vulnerable cohort depletion.
this starts to hint at something being quite wrong and also starts to rule out “variant” as the source, because it did not drive that outcome in palestine.
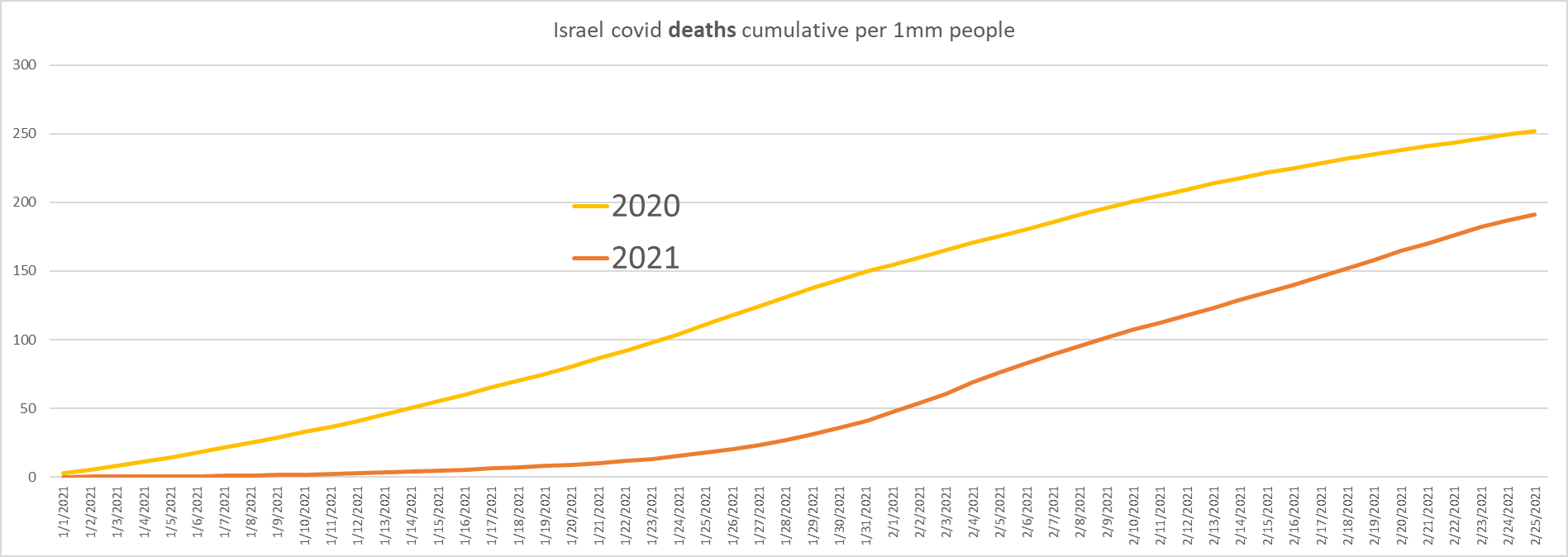
it can be notoriously difficult to eyeball area under curve, so i have plotted cumulative deaths here:
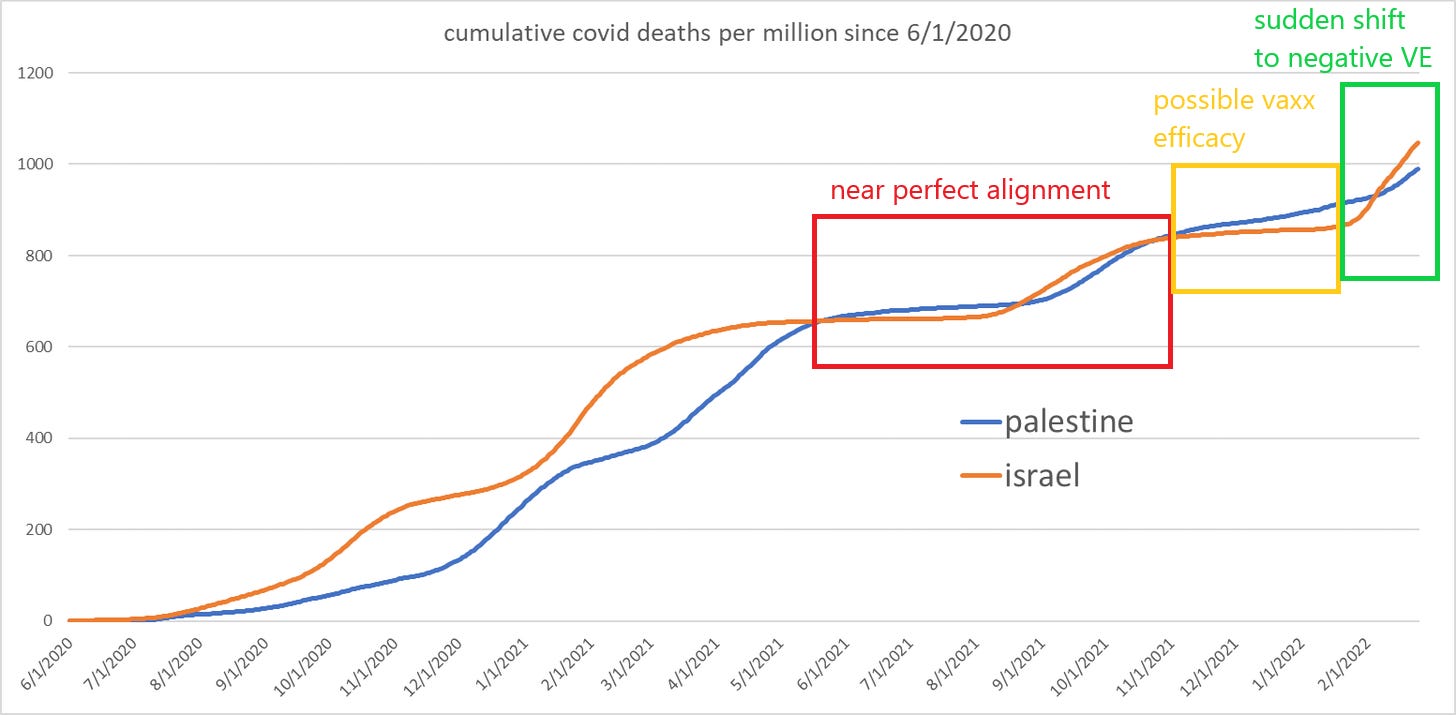
as can be seen, israel had gone pancake flat in november 2021 through jan 2022. then it inflected severely. this is omicron which hit the levant in the second half of december 2021. clinically, you’d expect about a 24 day log to show up in deaths and this tends to jibe with the data i’ve seen all over the world.
it’s possible that boosters were having some effect in bending the curve, but to the extent that they did, it was either fleeting or rapidly inverted in the face of a new variant. (or both)
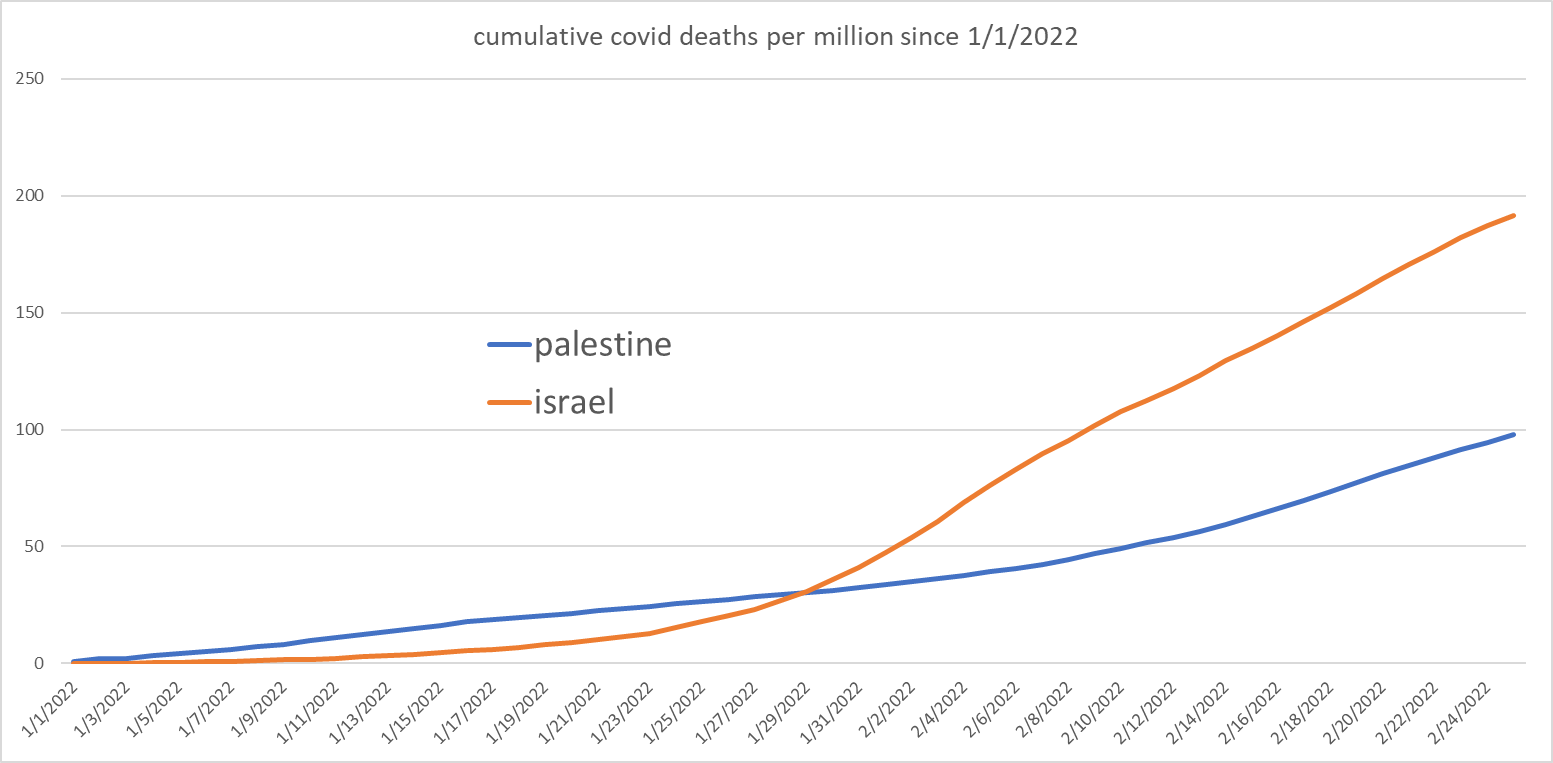
this becomes extremely easy to see when we zoom into 2022 and start a cumulative count from 1/1/2022.
there is a powerful inflection in israel that does not exist in palestine and israel has seen roughly twice the cumulative per capital death rate of palestine so far this year.
if boosters are effective in preventing deaths from omicron, it sure does not show up here.
this also lets us rule out “omicron” as a source of greater underlying virulence/fatality. if this were so, it would be manifest in both places. the fact that it is not doing so supports the idea that omicron is an OAS/hoskins effect evolution taking advantage of the narrow antigenic fixation generated by mRNA and adenovirus vaccines. it also seems to show that this advantage is NOT, as many claim, limited to cases. it seems to carry through to deaths as well.
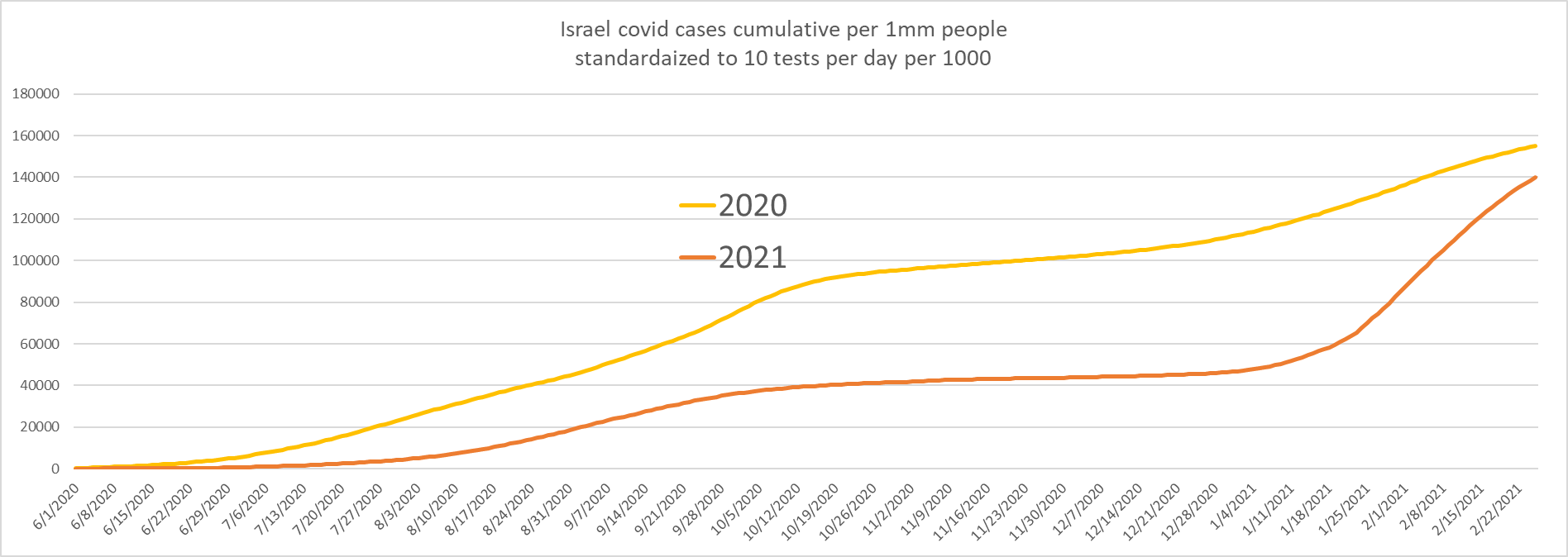
we can also compare israel to itself and see how this highly vaccinated and boosted period compares to the prior year when vaccination was zero. from this data as well, we see strong support for the OAS hypothesis.
israel had been doing better. then omi came and everything changed.
(to remove the skew from widely varying sample rate driven by big shifts in testing levels, i have normalized all cases data to 10 tests per day per 1000 population though given the absurdity of calling a high Ct PCR+ a “case” even lacking symptoms, all case data is troublesome to assess, but we work with what we have, not with what we wish we had)
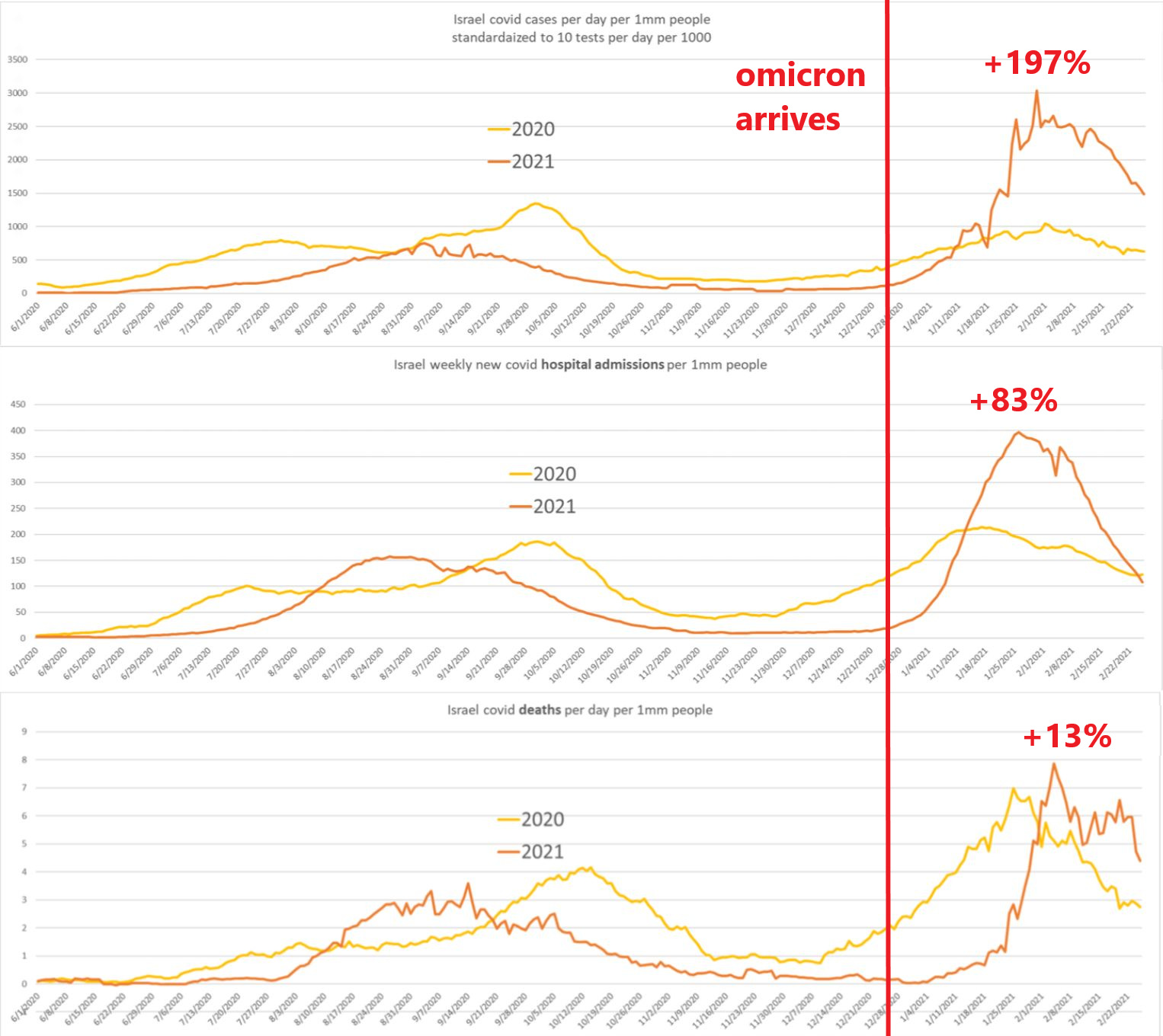
cases nearly tripled and hospitalizations nearly doubled. deaths rose 13%.
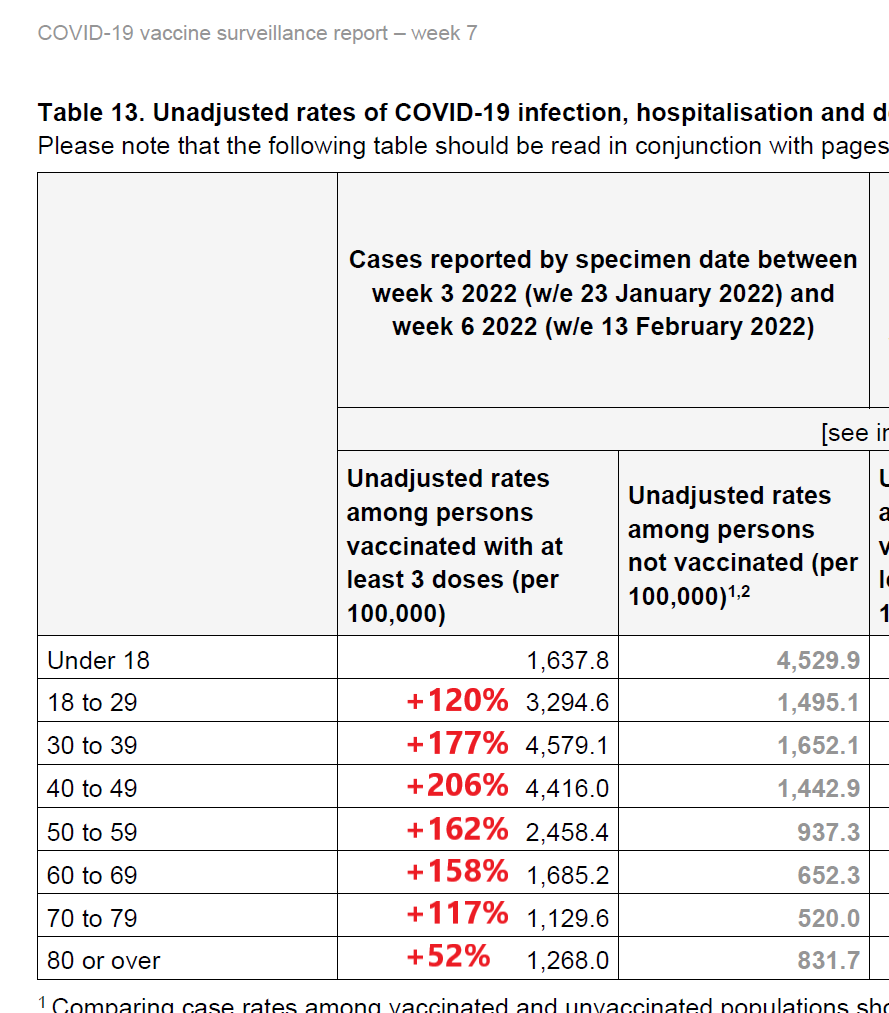
according to israeli authorities and hospitals, this was not driven by “the unvaxxed” but rather by the vaccinated. they seem to make up more than their share of severe outcomes though one must we wary of simpson’s paradoxes. (more HERE)
it might be possible to construct an argument whereby vaccine efficacy is claimed on any given infection (once you are sick, better to be vaxxed) but if that is, in aggregate, swamped by a rise in cases (and we know vaccines lead to more cases, not fewer) then this is still not much of an argument. having vaccines reduce risk of hospitalization per case by 50% but tripling case risk is still a 50% rise in overall hospitalization.
the aggregate data is possibly supportive of this claim outcome, but it’s far from certain either way.
but still, if the overall outcomes are worse post vaxx in the active arm but not in control, from a public health perspective do we really care why?
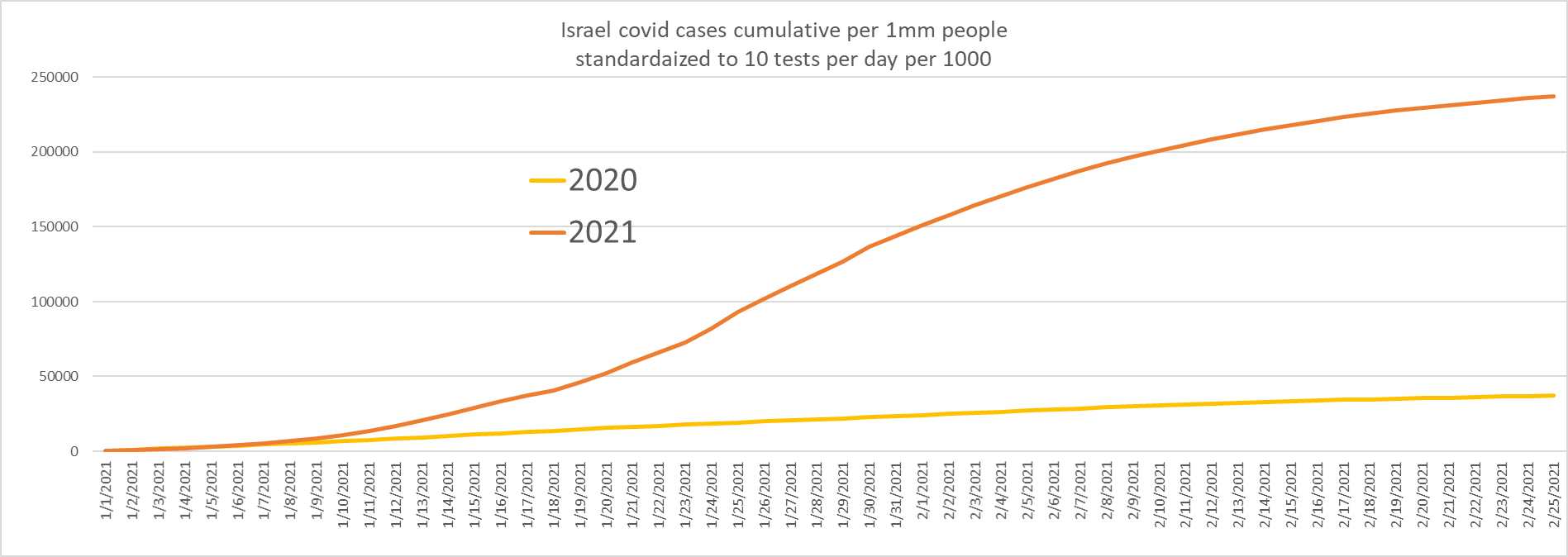
cases were trending MUCH lower. then that changed in a hurry.
zooming in makes it all the more clear.
even adjusted for testing, this is a massive surge in cases.
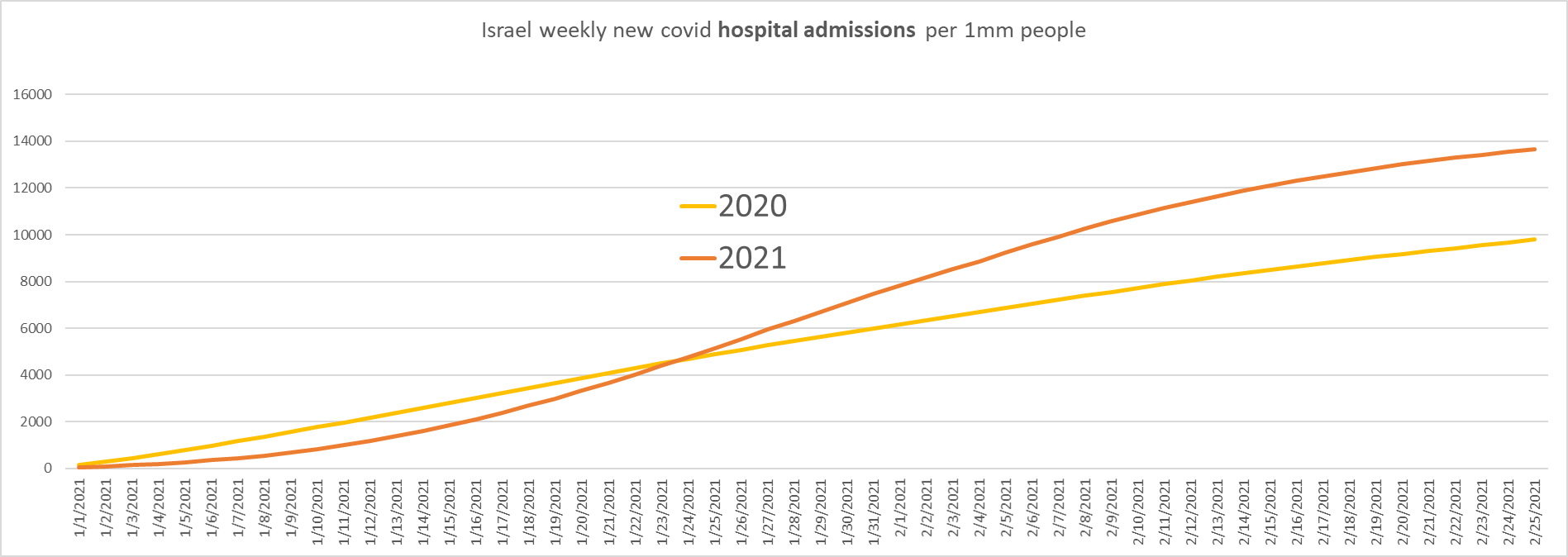
we see the same in hospitalization.

and see the crossover to worse outcomes in 2022 when we zoom in.
overall, they are 39% higher in aggregate YTD vs prior yr.
deaths have not yet caught up, but appear likely to do so.
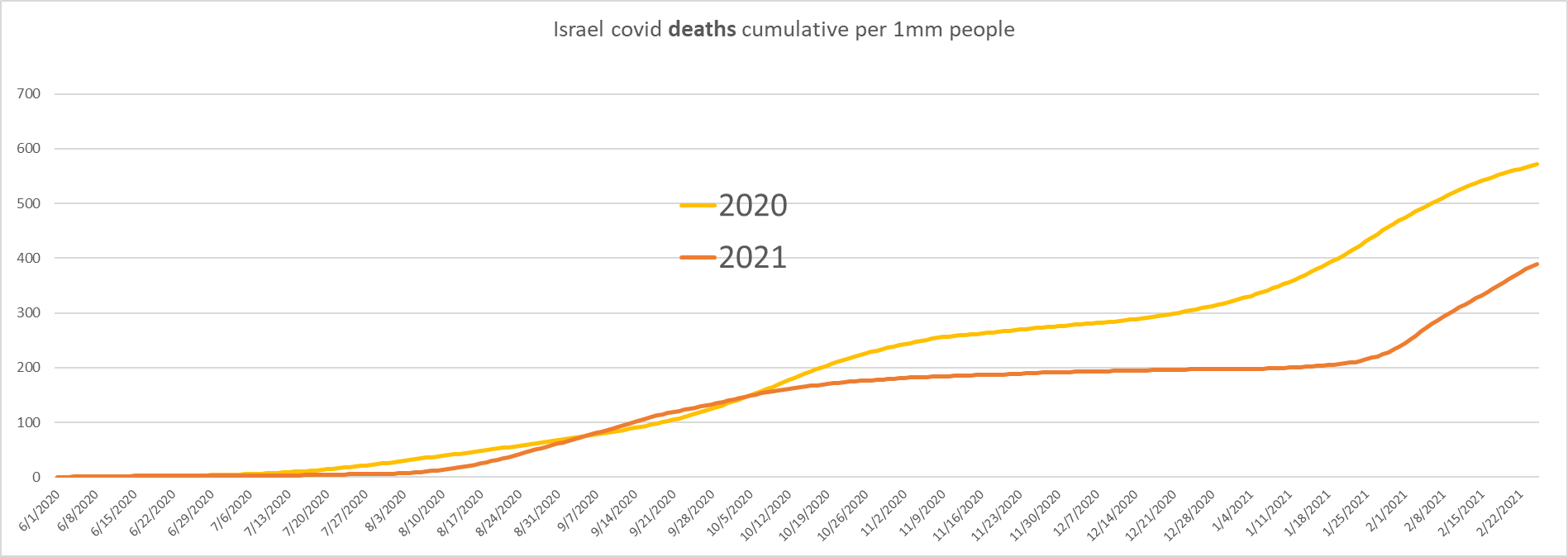
taken as a whole, this is pretty damning of the booster programs.
israel saw a big spike in deaths that was not present in the palestine control group.
it saw a massive jump in cases, a big jump in hospitalizations, and is rapidly converging on deaths (which will lag the others by ~3-4 weeks).
there is just no way to spin this as a win. it looks like an own goal.
this was the known and knowable outcome of widespread inoculation with a leaky vaccine. it is, in fact, WHY we do not use leaky vaccines.
they will rapidly and inevitably select for escape or vaccine enhanced variants. and now it makes you worse and worst of all, locks you into a suboptimal antigenic response pattern that may keep you from EVER generating real sterilizing immunity. the truly nasty part of this may take years to really see.
omicron was not “bad luck” it was invoked consequence of ill conceived intervention. even assuming they ever worked as claimed (dubious) these vaccines were always going to fail because that’s what leaky vaccines do.
this was known and knowable. the drug companies that made them knew it. the regulatory agencies that approved them knew it. and many, many doctors, researchers and public health officials all over the world knew it. they were silenced, threatened, and attacked for it. and this is the bitter fruit of that harvest.
in the US, the data has been manipulated and misused so badly as to render it outright fraud. it becomes obvious when one compares the US data (which calls all “unknown or undetermined” patients “unvaxxed” and used the fact that the EPIC system is awful to create a false sense of VE) with a system that keeps good records as longtime gatopal™ HOLD2, newly on substack, has done here.
like so much of the rest of the covid response, we knew better than to do this, but it was done anyway.
and now, the US is lying about it while others are, at least, coming clean.
but this truth will be too vast to hide much longer, even behind these big lies.
and american health and regulatory agencies are going to have a great deal to answer for.
dr atlas (with whom many at rational ground, including even notorious internet felines, had the pleasure to collaborate) is correct in everything he says here except in his use of the world “almost.”
Featured Video
Israel and the Palestinians — It’s about Mind Over Matter
or go to
Aletho News Archives – Video-Images
Book Review
The Greatest Threat to World Peace? A Review of Daniele Ganser’s ‘USA: The Ruthless Empire’
Review by Marilyn Langlois | November 10, 2023
 If you regard the United States as perhaps flawed but overall a force for good in the world . . .
If you regard the United States as perhaps flawed but overall a force for good in the world . . .
If you scoff at the notion that the US, a republic founded on principles of freedom and democracy, has morphed into a world empire, perpetrating assassinations, coups d’état, acts of terror and illegal warfare . . .
If you want to promote peace but haven’t yet explored deceptive events that precipitate US warmongering . . .
. . . here is a volume that will clear the air and paint an honest picture of the significant, not-so-rosy impact US foreign policy and actions have had in the world around us.
USA: The Ruthless Empire, by Swiss historian and peace researcher Daniele Ganser, is the newly published English language translation of his book Imperium USA, originally written in German and published in 2020. Here is a summary of key points — including some lesser-known ones — along with remedies for a more peaceful future, that are covered in the book. … continue
Blog Roll
 Aletho News
Aletho News- Putting Nukes in Finland Won’t Make Country Safer, Finnish Politician Cautions
- Ukrainian drone strike kills worker at Europe’s largest nuclear power plant
- What the West Hides About Soviet Role in De-Colonization
- Villains of Judea: Douglas Feith
- US pension fund invests hundreds of millions in weapons firms supplying Israel
- US bill to grant Americans serving in Israeli army same rights as US troops
- What a president, a movie star, a congressman, and a cell phone all dared to say
- ‘An entire nation is being humiliated by the Iranian leadership’: Merz
- Pakistan Throws Open Its Gates for Iran’s Transit Trade to Third Countries
- Iran to charge ships passing Strait of Hormuz in rial: Lawmaker
- If Americans Knew
- Israel escalates in Gaza: killing, torture, hunger – Daily Update
- Six Months into Gaza Ceasefire, Setting the Record Straight About Aid
- ‘Silent suffering’: Why children in Gaza are losing their ability to speak
- In Gaza, 17,000 infections linked to rodents and external parasites – Daily Update
- Lobby group taking journalists on propaganda tours of Israel
- The Shattered Figure of Jesus Is Not an Exception. It’s a Pattern
- Israel’s idea of ceasefire includes killing 21 in one day – Daily Update
- Christians in Israel and Palestine, past and present
- Israel eager to restart Iran war, Gaza genocide – Daily Update
- Meet the Top “Content” Producers Linked to Canary Mission
- No Tricks Zone
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s

{kind=link}