
Former United Kingdom (UK) Prime Minister Tony Blair has called for global organizations such as the World Trade Organization (WTO) and World Economic Forum (WEF) to push national governments to introduce “digital infrastructure” that monitors who has been vaccinated and who hasn’t.
Blair pushed for this government-controlled digital vaccine database during an appearance at the World Economic Forum’s 2023 annual meeting — a yearly event where powerful business leaders, politicians, and other influential figures meet in Davos, Switzerland to discuss the agendas they want to advance.
The former Prime Minister emphasized the importance of “technology and digital infrastructure” and data collection for surveilling the status of the vaccinated and unvaccinated.
“You need the data,” Blair said. “You need to know who’s been vaccinated and who hasn’t been. Some of the vaccines that will come on down the line will be multiple, there’ll be multiple shots. So you’ve got to have, the reasons to do with the healthcare more generally, but certainly, for a pandemic or for…vaccines, you’ve got to have a proper digital infrastructure, and many countries don’t have that. In fact, most countries don’t have that.”
Blair continued by suggesting that his digital vaccination status surveillance dragnet should be pushed through by the WTO (an intergovernmental organization that regulates international trade), the WEF (an unelected global organization that seeks to “shape global, regional and industry agendas”), and intergovernmental forums such as the Group of Twenty (G20) and the Group of Seven (G7).
“Who are the people that can make this happen?” Blair said. “How do you get the right partnerships in place?…That should happen in the G20 particularly, I think, which is… G7 is an important forum, but the G20 is the broader forum… You’ve got to work out what is it that you want to achieve in order to make sure that any future pandemic is properly handled and what are the partnerships that you’re going to create in order to ensure that the answers you get are the right answers. And then you’re going to have the mechanisms of implementation. And those mechanisms will be partly through the formal institutions that you have, like the WTO, and they’ll also be through organizations like yours [the WEF] which… I think… have many advantages because they don’t get landed with the same bureaucracy and frankly small pea politics around them.”
Blair’s call is the latest of several that he and his nonprofit, The Tony Blair Institute for Global Change, have made for an expansion of mandatory digital surveillance infrastructure.
His institute has called for digital IDs and said increased surveillance is a “price worth paying.” Blair himself has also called for mandatory vaccine passports.
And two of the global groups that Blair wants to help push through this digital surveillance system, the WTO and the WEF, are also huge advocates of digital surveillance systems.
The WEF and the WTO have previously pushed “global digital identity of persons and objects.” And the WEF regularly advocates for digital ID programs around the world. This year’s WEF 2023 annual meeting subjected journalists to some of the surveillance technologies it advocates for including digital IDs and biometric scanning.
Not only do these surveillance systems reduce individual privacy but vaccine passports discriminate against citizens and restrict their access to businesses and services.
And the WEF wants to expand this surveillance and discrimination via digital ID. It has proposed a system that monitors online behavior, biometrics, purchases, and more to determine access to a wide range of services.
Related:
How Big Government and Big Tech used COVID to accelerate the adoption of digital ID
January 19, 2023
Posted by aletho |
Civil Liberties, Full Spectrum Dominance, Science and Pseudo-Science | COVID-19 Vaccine, Human rights, WEF, WTO |
Leave a comment

New Zealand’s Prime Minister Jacinda Ardern resigned last night after months of rumours. Ardern, whose popularity has plummeted during the last six months, told us she ‘had nothing left in the tank’.
The backstory to this resignation is a tale of woe. Ardern said she wants to be remembered as someone who tried to be kind. The subtext is: the country is in an unprecedented mess but don’t blame me. School attendance is running at just 67 per cent on any given day. Machete-wielding teenagers are ram-raiding liquor, tobacco and luxury stores daily in an unprecedented crime wave. The health system is overwhelmed. Ardern’s government promised to build 100,000 new homes over three years. It has delivered 1,500.
Our tourist, farming and hospitality industries have never recovered from lockdowns and border closures. It takes months to get a visa to visit NZ and the government says it only wants rich people to come. Ardern insisted on universal Covid vaccination mandates. There is a suspicion that our 90 per cent vaccination rate has left most people in a lethargic fog. Excess all-cause deaths are still running 15 per cent above the long-term trends, and it is not Covid.
History will judge Ardern harshly, but don’t blame her alone. This was a Parliament who woke up on all sides of the house to the weakness of our constitutional arrangements (there are none). The Bill of Rights was tossed aside and no one in Parliament cared.
The leader of the National opposition Chris Luxon said if he was in power, he would withdraw benefits from unvaccinated single mothers. David Seymour, leader of the ACT party, said those losing their jobs through vaccine mandates only had themselves to blame. Labour’s coalition partner, the Greens, led by example. They encouraged mothers in labour to ride to hospital on a bicycle.
Revelations this week (here and here) that Ardern personally overruled her scientific advisers who were expressing doubts about the safety of Covid vaccines for young people and the wisdom of mandates have circulated very widely and no doubt this further undermined confidence in the government.
Political insider and right-wing commentator Cameron Slater published an article ten days ago saying that out of all the politicians he has known (and he has known most since Muldoon in the 70s) Ardern is the only one he rates as truly evil.
Ardern introduced ‘rule by regulation’. Adopting the enabling model favoured by fascists in the 1930s, her government has empowered authorities to tell us all what to do, when to stay at home, and where not to go. The courts, the Human Rights Commission and the broadcast regulators have all followed the government line meticulously which has had a devastating effect on business, families, communities and professions. To cement her policies, Ardern introduced massive government funding of our media and broadcasters.
Ardern’s government, in an absurd overreach, funded a nationwide effort to discredit critics of policy, labelling them terrorists. This has divided a formerly egalitarian society, instituting a Stasi-like snitch culture that encourages us to report a neighbour. Government Disinformation Project employees appeared on funded films aired on television labelling knitting, blond hair, braids, vaccine hesitancy, love of natural foods, yoga and motherhood as signs of terrorism that should be reported to the intelligence services (view it here if you can stand watching this nasty piece of propaganda and hate).
Why did Ardern suddenly change overnight in August 2021 from being a kindly figure saying she would never mandate vaccines, to being one of the world’s most draconian proponents? We can only speculate. NZ is a member of the Five Eyes intelligence network. Given the Pentagon’s recently revealed massive involvement in US Covid policy and gain of function research funding, was she fed information that a bioweapon was in play?
For a couple of weeks now government announcements and advertisements encouraging vaccination and boosters have been conspicuously absent. Has the penny finally dropped? We doubt it. It will take an honest, intelligent politician (are there any?) to roll back Ardern’s dictatorial powers and kickstart New Zealand. Why would any aspiring newby give up that much power? The prospect will be too intoxicating.
Ardern was a protege of Tony Blair and Klaus Schwab of WEF. They must bear some blame too. What fantasies of global power did they offer to a young person who was given to idealistic dreaming that segued into fanaticism?
Our final verdict: It is not Ardern but the whole NZ Parliament elected in 2020 that will be judged as the worst in our short history as an independent island nation, formerly famous for championing the underdog and offering opportunity to all. Ardern’s resignation has lit the bonfire of modern democracy.
January 19, 2023
Posted by aletho |
Civil Liberties, Full Spectrum Dominance, Timeless or most popular, Video, War Crimes | Covid-19, COVID-19 Vaccine, Human rights, New Zealand |
Leave a comment
What is Davos? The World Economic Forum’s (WEF) annual meeting happens each year in the alpine Swiss ski resort town. Each year global leaders, elected and unelected, gather to collude on policy initiatives and hot button topics concerning humanity overwhelmingly without the consent of the people.
Intel coming out of this year’s meeting has had a more pressing, alarmist nature from the self-proclaimed global elite minders. Don’t worry, the meeting was still filled with the annual hypocrisy we are used to. Squadrons of ‘unsustainable,’ carbon-emitting private jets still flew in at will. Fleets of non-electric cars openly chauffeured the climate alarmist around while they preached about the end of gas vehicles and individual car ownership… for the planet of course. But lets turn to moves by the medical–industrial complex.
Coming off the back of a rushed Covid shot that failed to stop transmission and whose harms and shortcomings are still unraveling in the public conversation, the ‘global leaders’ of Davos used the forum to do what they always do in the uncomfortable spotlight – double down on agendas.
After some of the biggest, concerted global protests in a century against lockdowns and the digital Covid vaccine passports used by governments to enforce them, a call was made to expand such tools of restriction.
Former UK PM Tony Blair of Iraq war criminal fame apparently received his new marching orders speaking passionately at Davos for the implementation of a ‘national digital infrastructure.’
For ‘the vaccines coming down the line [that] will be multiple shots,’ for ‘vaccines [in general]’ and for ‘a pandemic’ Blair stated you need a proper digital infrastructure to know ‘who’s been vaccinated and who hasn’t.’
Founded in Davos by the Gates Foundation, the UK-based Wellcome Trust, the WEF and other governments, the Coalition for Epidemic Preparedness Innovations or CEPI was a central player in global Covid vaccine development efforts.
They now have a new ‘100 day goal’ which has been embraced by the G7 and G20 nations according to a Davos speech attended by Pfizer’s CEO Bourla, Blair and others.
To ‘accelerate vaccine development over and above what was achieved in 2020’ and to be able to deliver vaccines for new threats within 100 days.
So the idea again would be to sidestep proper safety testing to put massive mutation pressure on a new circulating virus or pathogen by vaccinating in a middle of an ongoing pandemic – something Dr. Geert Vanden Bossche has continually warned against.
CEPI’s goal to take Covid’s fast tracking vaccine development precedent and fast track it further has been aided, intentionally or unintentionally, by the newly enacted FDA Modernization Act 2.0 which allows drug and vaccine developers to rely upon computer modeling and testing with virtual patients in their safety assessments of new products to convince regulators they’ve been ‘de-risked.’
While the Davos crowd, along with many others in the public, like Neil DeGrasse Tyson, still believe the official narrative that the rushed Covid shot was a wild, safe and effective success, a growing critical mass continues to expose the truth.
Meanwhile, the FDA still doesn’t have ‘robust’ data from Pfizer or Moderna on their mRNA Covid shot product’s ability to cause potentially deadly heart inflammation.
A 2021 letter by the FDA to Pfizer gave the company until October 2025 to turn in their study looking at that piece which public health leaders and agencies will take, at face value, as the final word on the subject. Despite the foot-dragging by regulators, members of the public and medical community have filled the vacuum with actual data and warnings.
Top UK cardiologist Dr. Aseem Malhotra made history becoming one of the BBC’s most watched segments of the last two years [27.1M view on Twitter] warning about the myocarditis risk live on-air along with its role in the soaring number of excess deaths – the highest in 50 years according to the BBC.
Will the public accept digital restrictions on their life again in the form of vaccine passports?
Will the public accept new, multi-dose vaccines unpinned by even less safety testing and transparency than the mRNA Covid shots?
January 19, 2023
Posted by aletho |
Civil Liberties, Full Spectrum Dominance, Science and Pseudo-Science | COVID-19 Vaccine, Human rights, WEF |
Leave a comment
▪︎ Dr. James Lyons-Weiler, USA, research scientist and CEO of the Institute for Pure and Applied Knowledge:
▫️The smoking gun in the genes: Traces of toxic “medicines” used in the course of past “epidemics”.
January 19, 2023
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular, Video, War Crimes | Covid-19, COVID-19 Vaccine |
Leave a comment
A new Covid-19 variant has appeared: XBB.1.5 (or ‘Kraken’, for the fear factor). This could explain why deaths are surging again, with Japan recording about 400 daily, and Australia (despite being in the height of summer) in the dozens. But are people really dying from the latest strain of coronavirus?
Excess mortality is highest in countries with the highest rates of Covid-19 vaccination. Correlation is not causation, but only the wilfully blind are describing this human toll as ‘baffling’. Ordinary people do not need scientific expertise to join the dots. At the very least, the authorities should be investigating this unprecedented rise in mortality as a possible iatrogenic disaster (ie caused by medical treatment, like thalidomide).
While there is growing public awareness of the lethality of the mRNA injections, the scientific orthodoxy is continuing to suppress the truth. In reports showing an increased incidence of cardiovascular disease after vaccination, researchers always moderate the message by stating that the benefits overwhelmingly outweigh the risks. However, many publications do not even consider the vaccines as a cause of illness or death.
Our editor alerted us to the article Covid Leading Cause of Death Among Law Enforcement for Third Year in Medscape. The data for this study of police officers across the US were taken from an annual report issued by the National Law Enforcement Officers Memorial Fund, titled 2022 End-Of-Year Preliminary Law Enforcement Officers Fatalities Report.
The report claims that in the past year 70 officers died in the line of duty of causes related to Covid-19. The good news is that this is ‘down dramatically from 2021, when 405 officer deaths were attributed to Covid’, but this was still a significant loss of front-line personnel, surpassing the number of deaths from firearms-related incidents.
The authors of the original report attribute the decline in deaths to ‘reduced infection rates and the broad availability and use of vaccinations’. However, this putative triumph of the Covid-19 vaccine needs more scrutiny than afforded by Medscape writer Lisa O’Mary.
In the original report we were keen to know how many law enforcement officers had died of other deadly infections. We anticipated influenza, meningitis, gastroenteritis and septicaemia among other potential killers, but none of these are mentioned in the report despite exposure on duty. We also wondered what the ‘background noise’ was in terms of how many law enforcement officers had died in total during the preceding years whether in the line of duty or not. Sadly, this figure was not reported either.
Covid-19, uniquely amongst infectious diseases, is being recorded as a cause of death in the line of duty but it is not clear why. We do not have any doubts about the bona fides of the National Law Enforcement Officers Memorial Fund and we do not, at face value, question their use of the numbers with which they have been provided. What is clear is that, like most of the public sector in the US (and the UK) they have fallen for the Covid-19 narrative and been willing participants in the ‘fear porn’ that has gripped so many otherwise well-meaning organisations.
We see several problems with the researchers’ claim that low Covid-19 mortality in officers was due to the vaccine. The first problem is the distinction between the definition of deaths ‘with’ as opposed to ‘of’ Covid-19 and the possible attenuation of the Covid-19 virus over time. Then, we are not informed in the report, and data seem unavailable, about the extent to which Covid-19 testing was or is still being carried out. If there was a significant reduction in Covid-19 testing between 2021 and 2022 that would be a significant confounding factor.
A bold claim about the success of the vaccine rollout would need, at least, to show how many law enforcement officers were vaccinated. Even then the outcome would not provide much insight into cause (vaccination) and effect (death from Covid-19).
It is not clear how many US law enforcement officers are vaccinated. There were indications that compulsory vaccination was going to be introduced for law enforcement officers. But there was also evidence that the law enforcement unions ‘pushed back’ against the idea. In fact, uptake of Covid-19 vaccines was so low amongst law enforcement officers that hundreds were reported to be dying and that, according to the Washington Post, they were a danger to the public. Therefore, it seems incongruous that, on the one hand, law enforcement officers are a public hazard due to their low Covid-19 vaccination status, and on the other hand have their own lives saved ‘dramatically’ as a result of the Covid-19 vaccines.
There is a more serious question that the researchers failed to ask themselves. Is it possible that some of the 70 officers dying in 2022, and some of the 405 in the year of the initial vaccine rollout, were victims of the Covid-19 vaccine? Consider, for example, an officer who is hospitalised for breathlessness, and is discovered to have dangerous blood clots. On admission he tests positively on a PCR test, which is notoriously prone to false positives. If this officer were to die, he would be added to the Covid-19 mortality figures. This is not fantasy, but the reality of how the pandemic has been perpetuated over the last three years – with the collusion of the scientific community.
January 18, 2023
Posted by aletho |
Science and Pseudo-Science | Covid-19, COVID-19 Vaccine, United States |
Leave a comment
From population bomb to false prophet, Ehrlich, and his protege John Holdren’s, book Ecoscience has a concerning passage about a bioweapon as a “solution” to overpopulation. Meanwhile, history shows Holdren lifted the moratorium on gain-of-function research less than two weeks before Trump’s inauguration in 2017. Another data point to a troubling, ongoing investigation.
When it comes to the COVID-19 vaccine, world-renowned doctors and scientists are jumping ship. Many of those same experts, however, are pivoting sharply, insisting the same skepticism should not be applied to ‘safe and effective’ childhood vaccines. The HighWire host, Del Bigtree, whose 7-year investigation into Vaccine Safety and Policy in America inspired the launch of ICAN (icandecide.org) and The HighWire, explains why ‘it ain’t Just the Covid Vax’ that you should be worried about.
January 18, 2023
Posted by aletho |
Malthusian Ideology, Phony Scarcity, Timeless or most popular, Video, War Crimes | COVID-19 Vaccine, Human rights, United States |
Leave a comment
On 20 October 2022, the CDC published a grant opportunity to develop a public health tool to predict the virality of vaccine misinformation narratives. The application closed a few days ago.
The purpose of the $1,000,000 grant is “to conduct research to develop and pilot a predictive model and tool to aid…in identifying emerging vaccine misinformation about recommended vaccines, including COVID-19 vaccines, that is likely to spread and have a high potential for impacting vaccine confidence”. It will enable public health agencies to identify misinformation before it spreads or impacts people’s health decisions.
According to the proposal, evidence for the negative impact of misinformation continues to grow. Therefore, this proposal has the potential to impact the Healthy People 2030 scheme by ensuring people get vaccinated. Healthy People 2030 sounds and looks suspiciously like something from Agenda 2030 but equally this might just be someone jumping on the bandwagon. However, one of the developmental objectives is to “increase the proportion of immunization information systems that track adult immunizations across their lifespan” which sounds a lot like vaccine passports. Maybe not but unfortunately these things need keeping an eye on these days.
The CDC estimates that “COVID-19 misinformation and disinformation caused $50-$300 million per day in additional medical costs, monetized lives lost and morbidity, and economic costs”. Therefore, they want this new tool to increase vaccination rates and disseminate accurate scientific messages.
There are 3 phases to successfully complete the proposal:
- Phase 1 – Develop a predictive model that identifies misinformation. To do this they will look at old data to find topics (such as vaccine safety and fertility), the types of people sharing this information and the relationship to societal concerns (e.g. personal liberty);
- Phase 2 – Develop a tool that can be used to prioritise the response to misinformation.
- Phase 3 – Pilot and evaluate the tool (that can be used at federal, state, local, tribal and territorial public health agency levels)
Now, I’m all for getting rid of misinformation. In an ideal world I just want to be reading facts, more facts with a few more facts sprinkled on top. However, this isn’t an ideal world and unfortunately, over the last few years, much of the misinformation has come from the CDC itself.
So a ‘Minority Report’ style system that will identify vaccine misinformation pre-crime and eliminate it before it can get out will only add to public distrust.
A Soviet-style public health propaganda set-up is not going to increase vaccine take-up. The only way to do that is to provide transparent data and allow hypotheses to formulate. These can quite easily be shut-down with accurate and open data.
What does increase vaccine hesitancy, is not having a truly independent body to analyse pharmaceutical data and then trying to bury that data for 75 years. Misinforming the public that they are going to die without a vaccine was the most harmful thing they could have done to trust in public health. Along with the suppression of adverse event signals, harms and deaths. However rare they may or may not be, by hiding just one of these causes the public to question what else is being hidden.
So I would like to claim the $1,000,000 to reduce vaccine misinformation with the following steps:
- Firstly produce a product that actually does what it is supposed to do;
- Conduct proper trials that look at short, medium and long term risks;
- Create a truly independent body that not only analyses the data it’s provided with but tests the products themselves;
- Remove propaganda such as ‘95% effective’ or ‘safe and effective’;
- Don’t conduct studies on how to manipulate the population into taking vaccines;
- Don’t force anybody to take a vaccine (by use of the psychological techniques above or through vaccine passports);
- Don’t use fear to convince people they are going to die without being vaccinated;
- Don’t supress safety-signals;
- Don’t gaslight the vaccine injured or families with members killed by vaccines;
- Remove the product from the market as soon as any safety signals, injuries or deaths occur. Explain clearly and openly what has been found and why the product has been removed;
- Don’t label anybody concerned about big pharma corruption or vaccine safety a conspiracy theorist or worse.
There you go. You don’t need any fancy and expensive systems to get people vaccinated. Just follow the steps above. But unfortunately, if your product isn’t up to scratch, you won’t make any money. You can send my $1,000,000 cheque in the post. Thanks.
Did I miss any points? And is it too late anyway? Has the amount of public health misinformation eroded away all trust, never to be regained again?
January 16, 2023
Posted by aletho |
Deception, Full Spectrum Dominance, Science and Pseudo-Science, War Crimes | COVID-19 Vaccine, Human rights |
Leave a comment
The Public Good Projects (PGP), a nonprofit that has developed several projects to fight so-called Covid “misinformation,” received $1,275,000 from the Pfizer and Moderna lobbying group, Biotechnology Innovation Organization (BIO), to create a content moderation campaign that influenced Twitter’s Covid misinformation rules. As part of this campaign, PGP sent Twitter lobbyists and content moderators weekly emails containing lists of tweets to censor.
Journalist Lee Fang published one of the weekly emails that Twitter received from PGP as part of the latest release of the Twitter Files — collections of internal Twitter communications that have exposed the censorship relationships Twitter had with government agencies and other powerful groups before Elon Musk took over.
The email shows Todd O’Boyle, a senior manager on Twitter’s Public Policy team, sharing “this week’s misinfo report” from PGP. The February 24, 2022 email included a list of top trends the PGP had seen during the week and two attached lists. According to Fang, one of the lists contained tweets the PGP wanted Twitter to take down and the other list contained tweets that it wanted Twitter to verify.
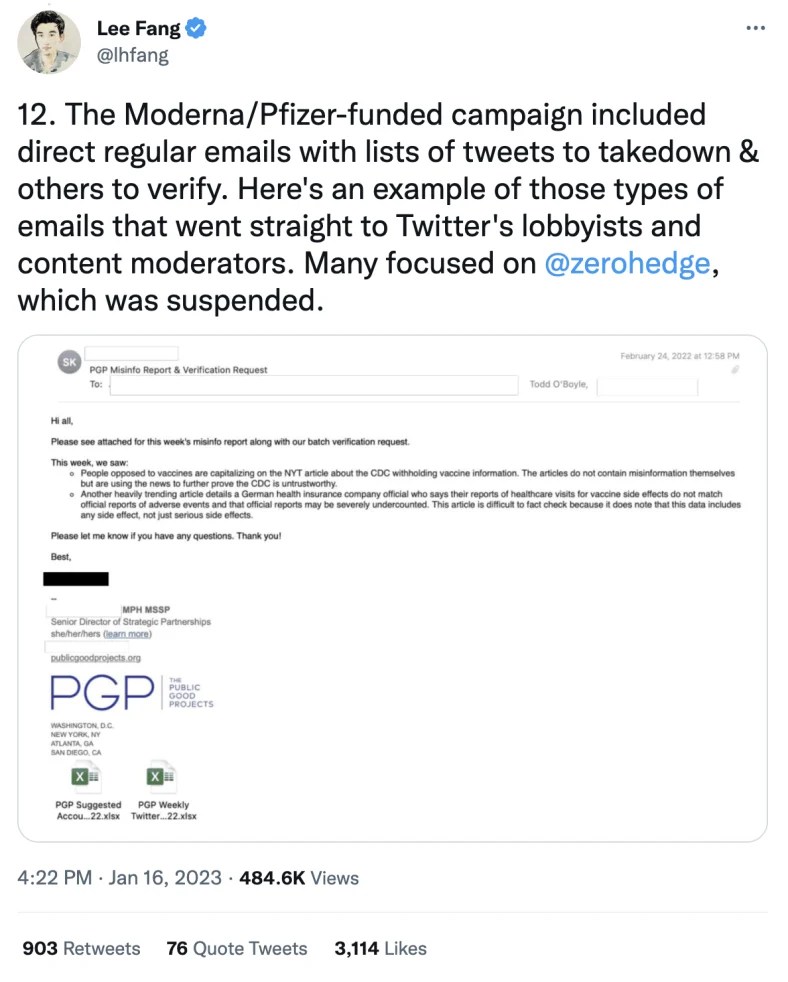
Despite flagging two trends in this weekly misinfo report, the PGP admitted that articles related to the first trend “do not contain misinformation themselves but are using the news to further prove the CDC is untrustworthy.”
The PGP also acknowledged that the second trending article it flagged, which described a German health insurance company official suggesting that reports of healthcare visits for vaccine side effects may be severely undercounted, “is difficult to fact check because it does note that this data includes any side effect, not just serious side effects.”
Fang said many of the PGP’s emails to Twitter focused on independent news outlet ZeroHedge which was banned from Twitter in January 2020 and reinstated in June 2020.
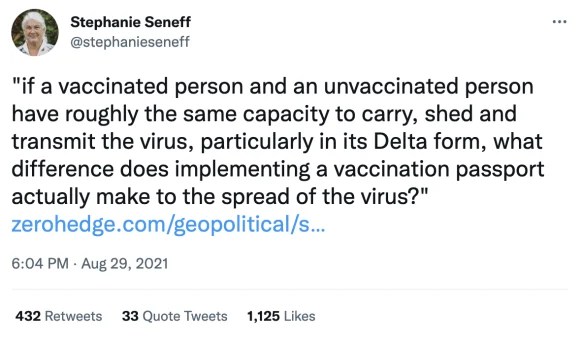
Fang also noted that this campaign flagged a tweet from senior Massachusetts Institute of Technology (MIT) scientist Stephanie Seneff that questioned vaccine passports on the basis that vaccinated and unvaccinated people have “roughly the same capacity to carry, shed and transmit the virus.”
Additionally, Fang shared a screenshot of a BIO tax form that revealed part of the funding ($883,000) it provided to PGP for this campaign.
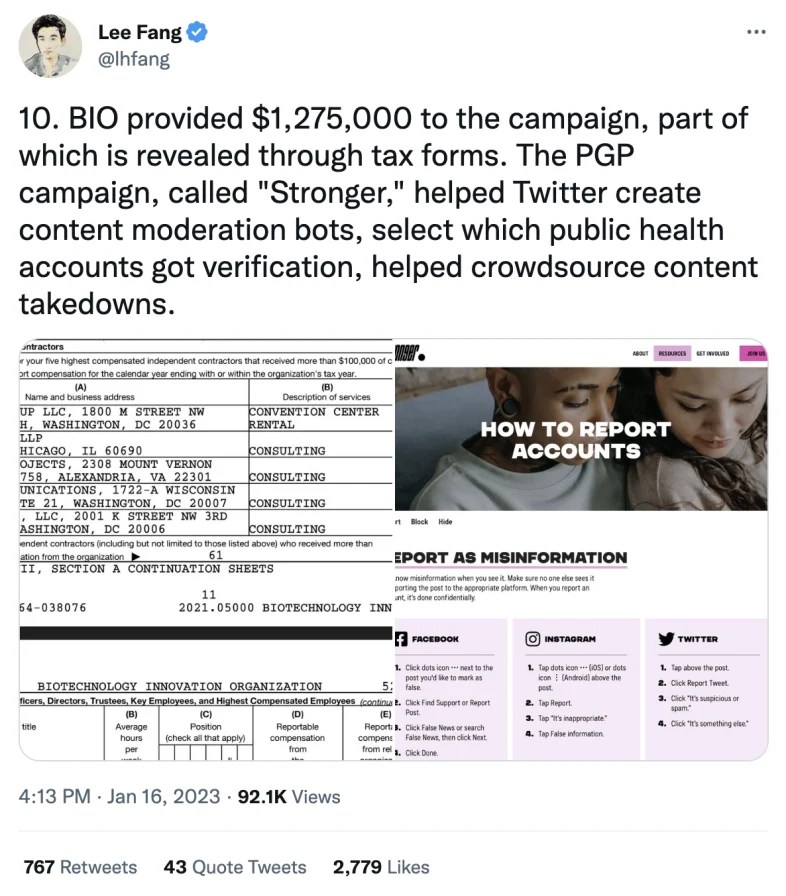
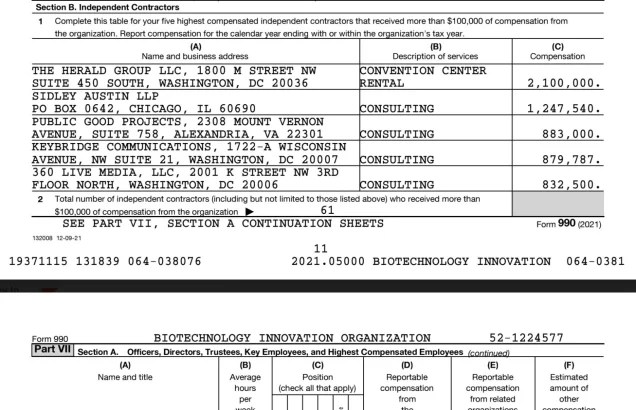
The PGP campaign is called “Stronger” and, according to Fang, it worked with Twitter to craft the platform’s content moderation rules around Covid misinformation, helped Twitter create content moderation bots, and helped Twitter select which public health accounts got verification.
Stronger says its goal is to “stop the spread of misinformation” and its website contains a page that encourages people to flag misinformation to Twitter and other platforms.
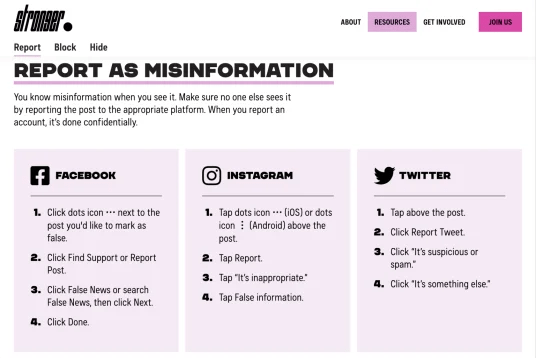
This page also contains a form for users to submit alleged misinformation to Stronger.
“Paste the link to a post, account, or website below, and the Stronger team will report it to the appropriate platform,” the form states.

Previous campaigns from the Public Good Project have involved recruiting pro-vaccine keyboard warriors to mass report anti-vaccine social media posts.
Fang’s revelations are the latest of several examples of those affiliated with Pfizer pushing for the censorship of content that questions or criticizes Covid vaccines.
Pfizer board member Scott Gottlieb complained to Twitter in August 2021 that it was promoting an article from journalist Alex Berenson. A few days after this complaint, Berenson was banned from Twitter. Twitter also censored another tweet after it was flagged by Gottlieb in August 2021.
Meanwhile, Pfizer’s CEO has branded those who share what he deems to be misinformation about vaccines as “criminals.”
January 16, 2023
Posted by aletho |
Civil Liberties, Full Spectrum Dominance, Science and Pseudo-Science | COVID-19 Vaccine, Human rights |
Leave a comment
In summary:
- On 6 May 2021 The Lancet published a blatantly flawed study of the effectiveness of the Pfizer covid vaccine on the population of Israel, claiming it was 95% effective.
- On 17 May 2021 we submitted a rapid response 250 word letter explaining why the study was flawed.
- After an initial response saying they would ask the authors for a response to our letter we heard nothing until 20 months later.
- On 8 January 2023 we got an email out of the blue from The Lancet Senior Editor Josefine Gibson apologising for never having got back to us about the letter, saying that they had asked the lead author Dr Sharon Alroy-Preis (SA-P) to respond to our letter but, because she did not provide any formal response, they have decided not to publish our letter.
- We tweeted The Lancet’s response and within 24 hours it got over one million impressions. We also published a substack article highlighting the fact we were now aware of additional problems with the paper relating to SA-P’s relationship with Pfizer.
- On 10 January 2023 we got an unsolicited email from Josefine Gibson (which we can only assume was a result of the reputation hit they got from our tweet) saying “Thank you for bringing your letter from May 2021 back to our attention. We are looking into next steps and will get back to you as soon as we can.”
- On 11 January 2023 (at 10:58) we sent an email to The Lancet’s Editor-in-Chief Richard Horton directing him to our substack article (which highlighted these new problems relating to SA-P’s relationship with Pfizer) stating that The Lancet was clearly taking a credibility hit surrounding the publication of the Israel-Pfizer study and its response to criticisms of it.
- On 11 January 2023 (at 11:21) we got an email from Josefine Gibson apologising for the ‘sub standard experience’ we had with The Lancet. She said that, after discussing it with Horton, they were now inviting us to publish the original letter or an update to it, suggesting the update ‘reflect more current experience with the vaccine’.
- On 12 January 2023 we submitted our updated letter (of an agreed 350 words).
- On 13 January 2023 we got a response from Josefine Gibson saying they had decided against publishing the letter.
Here is the full narrative and January 2023 correspondence in date order (personal details redacted)… continue
January 15, 2023
Posted by aletho |
Corruption, Deception, Science and Pseudo-Science | COVID-19 Vaccine, The Lancet |
Leave a comment
It was beaten down in DC but that did not stop these criminals
I have the documents showing that kids in Philadelphia, San Francisco and Kings County, WA were given COVID vaccines without parental permission. I have been told this happened elsewhere. So the perps are doing what makes sense for them: trying to legalize the process so they can’t be penalized for this crime.
Why are their efforts so focused on HS and college kids? To give kids access? ‘Access’ my A—-ss.
The age of ‘self-consent’ was lowered to 11 from 12 by Philadelphia’s health authorities. Presumably CDC came up with this brilliant idea.
Now, In order to give itself cover regarding the fig leaf that children can in fact provide a legal informed consent without a parent or guardian, the Health Commissioner of Philadelphia, PA claimed that handing a totally inadequate EUA “Fact Sheet” to an 11 year old at the time of vaccination would substitute for informed consent.
However, we know that the Fact Sheets that were used in lieu of a package insert omitted known information on health risks of the vaccine and incorrectly stated the benefits of the vaccine. So how could there be informed consent?
WHEREAS, on April 21, 2021, the Health Commissioner issued an Emergency Order
Concerning COVID-19 Vaccine Information Statements, which clarified that an FDA-issued COVID-19 Fact Sheet for Recipients and Caregivers is an appropriate substitute for a VIS for purposes of Section 4 of the Board of Health’s Regulations Governing the Immunization and Treatment of Newborns, Children, and Adolescents; and
WHEREAS, on May 10, 2021, the FDA authorized a COVID vaccine for use in people twelve years of age or older pursuant to an EUA; and
WHEREAS, the Board of Health hereby reaffirms, consistent with Section 4 of its Regulations Governing the Immunization and Treatment of Newborns, Children, and Adolescents, that minors eleven (11) years of age and older are typically capable of providing informed consent on their own behalf to be vaccinated for a reportable disease, subject to a vaccine provider’s individual determination that the minor is able to and does provide such informed consent, and the Board hereby clarifies that an FDA-issued COVID-19 Fact Sheet for Recipients and
Caregivers is an appropriate substitute for a VIS; and
NOW, THEREFORE, the Board of Health hereby adopts the following emergency regulation, effective upon delivery to the Department of Records, while the remaining procedures and formalities of Section 8-407 are followed to promulgate this as a formal regulation:
Section 1. Temporary Emergency Supplement to Board of Health Regulations
Governing the Immunization and Treatment of Newborns, Children, and
Adolescents
With respect to a minor eleven (11) years of age or older, the Emergency Use
Authorization Fact Sheet for Recipients and Caregivers for a COVID-19 vaccine authorized by the U.S. Food and Drug Administration for use in persons of the age of the vaccine recipient, if and when such an authorization exists, may be provided for the purposes of Section 4 of the Board of Health’s Regulations Governing the Immunization and Treatment of Newborns, Children, and Adolescents, when a Vaccine Information Statement does not exist for the COVID-19 vaccine being administered…
https://vax.phila.gov/wp-content/uploads/2021/05/BOH-reg-VIS-substitution-1-2.pdf
January 15, 2023
Posted by aletho |
Deception, Timeless or most popular, War Crimes | COVID-19 Vaccine, United States |
Leave a comment
The time to proclaim pfraud throw the vaxx companies under the bus approaches
you gotta hand it to the project veritas gang, their investigative journos get the goods.
back in 2021 they managed this interview.
meet chris croce, pfizer “senior associate scientist” and doubtless “recipient of some serious stink eye around the watercooler” blabbermouth.
according to señor chris:
- myocarditis is a concern from the vaxx, especially for younger people
- and they “are looking into” why
- they just sent 3000 patients’ samples for testing for elevated troponin levels (a marker associated with heart attacks)
- has no idea “what it looks like” as they do not have data back yet
- hopefully, it’s good because if it’s bad, that might “pull something from the market”
goodness!
has anyone ever seen this data?
because i certainly have not.
odd.
but then … continue
January 15, 2023
Posted by aletho |
Deception, Science and Pseudo-Science, Timeless or most popular, Video, War Crimes | COVID-19 Vaccine, United States |
Leave a comment
Sudden Cardiac Death Leads all Fatal Diagnoses
Almost everyday in the news is another reported case of sudden, unexpected cardiac death. The vaccination status is carefully concealed in the report and any mention of past SARS-CoV-2 immunization appears to be scrubbed from the internet. Families maintain an airtight silence on a simple medical query — did they take a COVID-19 vaccine? Yes or No? Prior to COVID-19 vaccination, the usual causes of death were almost always known antemortem, and were roughly 40% cardiovascular, 40% cancer, and 20% other causes. Chaves and colleagues have shown these proportions have been dramatically shifted to sudden cardiac death.

Chaves JJ, Bonilla JC, Chaves-Cabezas V, Castro A, Polo JF, Mendoza O, Correa-Rodríguez J, Piedrahita AC, Romero-Fandiño IA, Caro MV, González AC, Sánchez LK, Murcia F, Márquez G, Benavides A, Quiroga MDP, López J, Parra-Medina R. A postmortem study of patients vaccinated for SARS-CoV-2 in Colombia. Rev Esp Patol. 2023 Jan-Mar;56(1):4-9. doi: 10.1016/j.patol.2022.09.003. Epub 2022 Oct 31. PMID: 36599599; PMCID: PMC9618417.
In a series of 121 deaths primarily after the whole virus CoronaVac (Sinovac) injection, 57% were classified as sudden cardiac death and the pathologies included myocardial infarction, aortic dissection, and in few cases with no cardiac pathology assumed primary arrhythmic death. Pulmonary embolism, another accepted complication comprised 21% of the cases. Despite the authors claim of “no association,” its my interpretation of the data that 78% of the deaths could be directly attributed to a known mechanism of COVID-19 vaccination. This is very consistent with the recent report from Schwab et al from Germany whose data revealed 71% of deaths within 20 days of vaccination occurred in the context of acute problems known to be caused by the vaccines.
When autopsies done by separate teams in different countries arrive at similar findings, we have external consistency. This is one of many criteria that are used in determining scientific validity. The assertion that COVID-19 vaccines are causing death is increasingly supported in the peer-reviewed literature.
Peter A. McCullough, MD, MPH, Found Dead at Home after COVID-19 Vaccination Autopsy Series Finds an Array of Fatal Vaccine Syndromes
Chaves JJ, Bonilla JC, Chaves-Cabezas V, Castro A, Polo JF, Mendoza O, Correa-Rodríguez J, Piedrahita AC, Romero-Fandiño IA, Caro MV, González AC, Sánchez LK, Murcia F, Márquez G, Benavides A, Quiroga MDP, López J, Parra-Medina R. A postmortem study of patients vaccinated for SARS-CoV-2 in Colombia. Rev Esp Patol. 2023 Jan-Mar;56(1):4-9. doi: 10.1016/j.patol.2022.09.003. Epub 2022 Oct 31. PMID: 36599599; PMCID: PMC9618417.
January 14, 2023
Posted by aletho |
Aletho News | COVID-19 Vaccine |
Leave a comment


