UK Government’s Case for Masks in Classrooms Accidentally Reveals They’re a Terrible Idea
By Will Jones | The Daily Sceptic | January 6, 2022
The Government on Wednesday published the evidence informing its recent controversial decision to recommend all secondary school pupils wear face masks in classrooms.
The new document from the Department for Education (DfE) explains that the decision “has been taken on the recommendation of UKHSA and is based on a range of evidence”. It says the Government has “balanced education and public health considerations, including the benefits in managing infection and transmission, against any educational and wider health and wellbeing impacts from the recommended use of face coverings”.
While conceding that the “direct COVID-19 health risks to children and young people are very low” – and rejecting SAGE’s advice to recommend masks in primary school classrooms (yes, really) – it claims that “the balance of risks for secondary classrooms has changed at this point in time, in accordance with the evolving evidence and the phase of the pandemic”.
The document summarises its evidence as follows:
Face coverings can be effective in contributing to reducing transmission of COVID-19 in public and community settings. This is informed by a range of research, including randomised control trials, contact tracing studies, and observational studies – assessed most recently by UKHSA, described in a review conducted in November 2021. The review’s conclusions were broadly in line with those of a previous Public Health England review; however, the addition of randomised control trials and substantially more individual-level observational studies increases the strength of the conclusions and strengthens the evidence for the effectiveness of face coverings in reducing the spread of COVID-19 in the community, through source control, wearer protection, and universal masking.
In fact, though, the UKHSA review from November 2021 found no high quality studies (except, it claims, the ONS study, which really isn’t high quality). Of the two randomised controlled trials (RCTs) that have been done and which were cited by the UKHSA, the one from Denmark found no statistically significant reduction in COVID-19 incidence from surgical masks (the study didn’t look at cloth masks) while the Bangladesh mask study found no benefit from cloth masks and the reported benefit from surgical masks was just 11%, with a 95% confidence interval that included zero. The UKHSA review also considered 23 observational studies, which it said had “mixed” results and many of which were of low quality and small.
This does not seem a strong basis to claim a large effect for mask wearing. A recent more comprehensive review (which included earlier evidence for other flu-like viruses) by Ian Liu, Vinay Prasad and Jonathan Darrow for the Cato Institute, entitled “Evidence for Community Cloth Face Masking to Limit the Spread of SARS‐CoV‑2: A Critical Review“, concluded that: “More than a century after the 1918 influenza pandemic, examination of the efficacy of masks has produced a large volume of mostly low- to moderate-quality evidence that has largely failed to demonstrate their value in most settings.”
That is a better summary of the evidence than the DfE managed.
Needless to say, the DfE gives the propaganda value of masking a nod: “It can be a visible outward signal of safety behaviour and a reminder of COVID-19 risks.”
Notably, there is no mention in this document of the potential harms of wearing a mask for an extended period, such as the impact on breathing, the heart, or the skin. Contamination gets a brief mention, though it’s quickly dismissed:
Face masks and coverings will become highly contaminated with upper respiratory tract and skin micro-organisms. Disposal of single-use face coverings could theoretically pose a risk of transmission for inappropriately discarded face coverings, but it is very likely that the reduction in transmission risk due to reduced droplet and aerosol emissions from wearing a face covering significantly outweighs any potential for enhanced risk of transmission through inadvertent contact with a contaminated face covering. This is likely to hold regardless of duration that the face covering is used.
The reference provided for these claims is a SAGE document from September 2020, “Duration of Wearing of Face Coverings.” This is an interesting document, but it can scarcely be said to support the claims the DfE is making. On harms from masks, for example, it says:
Neither surgical masks nor face coverings are designed for use for extended periods. Wearing a face covering for an extended period can maintain a higher moisture level around the face which can be uncomfortable for some people and may increase the likelihood of skin complaints. Masks will become highly contaminated with upper respiratory tract and skin micro-organisms. A review of the downsides of face masks and face coverings (by Bakhit et al) found 20 studies reporting irritation and discomfort from using masks. Participants in studies with surgical or cloth masks reported difficulty breathing (12%-34%), facial irritation and discomfort (11-35%). More serious symptoms of headache, acne, rashes were associated with use of N95 and goggles. A study among healthcare workers (by Han et al) associates acne with extended duration of wearing. …
In a clinical study of extended wearing (by Chughtai et al), 124/148 participants reported at least one problem associated with mask use including pressure on face, breathing difficulty, discomfort, trouble communicating with the patient and headache. …
Measurements of heart rate during activity (by Li et al) showed significantly lower rates with a surgical mask compared to N95. In a study (by Fikenzer et al) of healthy young male volunteers surgical masks and FFP2/N95 respirators, both had a significantly marked negative impact on pulmonary capacity (FEV, PEV and PEF) while wearing the mask (with a spirometry mask) during exercise.
The DfE document omits to mention any of these issues. It does, however, include some recognition of the negative impact on education. It mentions a survey conducted by the Department in March 2021 that found “80% of pupils reported that wearing a face covering made it difficult to communicate, and more than half felt wearing one made learning more difficult (55%)”. It also mentions a DfE survey from April 2021 that found “almost all secondary leaders and teachers (94%) thought that wearing face coverings has made communication between teachers and students more difficult, with 59% saying it has made it a lot more difficult”. It adds:
Research into the effect of mask wearing on communication has found that concealing a speaker’s lips led to lower performance, lower confidence scores, and increased perceived effort on the part of the listener. Moreover, meta-cognitive monitoring was worse when listening in these conditions compared with listening to an unmasked talker. A survey of impacts on communication with mask wearing in adults reported that face coverings negatively impact hearing, understanding, engagement, and feelings of connection with the speaker. People with hearing loss were impacted more than those without hearing loss. The inability to see facial expressions and to read lips have a major impact on speech understanding for those with hearing impairments. The worse the hearing, the greater the impact of the mask.
What about the evidence for the claims the document does make – that it is “very likely” that the transmission reduction from wearing a mask “significantly outweighs any potential for enhanced risk of transmission through inadvertent contact with a contaminated face covering” and that “this is likely to hold regardless of duration that the face covering is used”. This is what the cited SAGE document says:
There is a lack of good evidence relating to the wearing of face coverings, with very little data relating to duration of wearing. In particular we suggest that the following aspects would benefit from further research:
• Effectiveness of face coverings as a source control after longer duration wearing, including analysis of the influence of moisture on the performance of different types of face coverings.
• Analysis of the potential risk of transmission due to contaminated face coverings (during and after removal).
• Assessment of the prevalence of skin complaints associated with face coverings, including an understanding of the factors that contribute and potential mitigation.
• Analysis of user acceptability of face coverings for long duration use in different settings.
In other words, there was no good evidence on the things the DfE is claiming are “likely” or “very likely”, or on much else really.
The DfE also carried out its own analysis of the impact of masks in schools.
DfE has also undertaken initial observational analysis based on data reported by 123 secondary schools that implemented face coverings during a 2-3-week period in the autumn term 2021, compared to a sample of similar schools that did not. The preliminary findings demonstrate a potential positive effect in reducing pupil absence due to COVID-19.
What did it find? It found that COVID-19 absences fell by 0.6% more (absolute reduction) in secondary schools that used face masks compared to similar schools that did not over a 2-3-week period, which amounts to an 11% relative reduction.
In a weighted sample of secondary schools that did not use face masks, the average COVID-19 absence rate fell by 1.7 percentage points from 5.3% on October 1st 2021 to 3.6% in the third week of October. This is equivalent to a 32% decrease.
In secondary schools that did use face coverings (either face coverings only or a combination of face masks and additional communications e.g. providing more communications to parents but not introducing any further measures such as increased testing), the average COVID-19 absence rate fell by 2.3 percentage points from 5.3% on October 1st 2021 to 3.0% in the third week of October. This is equivalent to a 43% decrease.
At surface level, this suggests that COVID-19 absence fell by 0.6 percentage points more (an 11% relative difference) in secondary schools that used face masks compared to similar schools that did not over a 2-3-week period.
However, the study had numerous limitations, which made the finding a “non-statistical and unknown clinical significant” reduction, i.e., it may just be chance.
There is a level of statistical uncertainty around the result. The analysis is non-peer reviewed and with the current sample size, shows a non-statistical and unknown clinical significant reduction in infection in a short follow up period, including that a ‘false positive’ (i.e. finding that face coverings saw reduced absence when the finding is actually by chance) would emerge around 15% of the time; a 5% threshold is widely used to declare statistical significance in academic literature.
Therefore, further work should be done to extend the analysis in terms of scope: for example, looking at different statistical methodologies, capturing different and longer treatment time periods and controlling for a wider number of school and local area variables to ensure this is a consistent finding.
The statistical uncertainty around the result was such that the 95% confidence interval for the effect size included zero (note in the below the upper CI is positive).

What’s more, the control group of 1,192 schools that didn’t use masks were very different to the 123 treatment schools which did, so that the above findings only emerged after significant weighting was added to the control group schools using a process the document calls “entropy balancing”.
Exploration of the data showed that the control and treatment group had differing characteristics, so weights for the control group schools were calculated using entropy balancing.
Prior to this weighting, the non-mask schools actually had lower average absence rates throughout the study period – though the treatment schools reduced more from their higher starting point.
Prior to weighting, the mean absence rate of the control group increases across the treatment period, whereas the mean absence rate of the treatment group decreases. However, the absence rates in the control group remain lower overall than those in the treatment group.

All-in-all, not exactly robust, compelling evidence of the benefits of masking, particularly given all the well-documented harms, which the document itself either sets out or cites other documents which do.
The document at one point hints at what I suspect is the real reason masks were brought back into classrooms: “In a Unison survey of support staff, 71% said face coverings in secondary school classrooms are an important safety measure.” Conservative MP Jonathan Gullis wrote in the Times this week that: “Face masks have been a central demand of teaching unions.” Sounds vey much like politics rather than science to me. (See this recent Daily Sceptic article by Ben Irvine on the role the teaching unions played in forcing the Government to lockdown in March 2020.)
When are we going to stop harming our young people with pointless interventions to deal with a virus that poses no threat to them and let them live normal lives again?
Stop Press: Oxford Professor of Evidence Based Medicine Carl Heneghan tells Julia Hartley-Brewer he is unimpressed by the Government’s “evidence” for masking in classrooms.
Do We Trust Paxlovid? Pfizer’s New COVID Treatment Medicine
By Joel S. Hirschhorn | Principia Scientific International | January 5, 2022
The pro-drug industry mainstream media are insanely positive over the newly FDA approved Pfizer antiviral COVID treatment pills.
The drug, Paxlovid, received an emergency use authorization by FDA for use in patients 12 years old and up who have tested positive for COVID-19 and are at high risk.
Now is the time to speak calmly and accurately about Paxlovid. First, everyone should appreciate that there was very little testing of the short- and long-term safety of this product, exactly what happened with COVID vaccines.
Really good testing of a new drug should take many months or even years.
All you get is positive news for this new drug – actually a combination of drugs.
Here are brief summary statements about this new product:
It was approved by the FDA without any external meetings, serious reviews of test data or opportunity for public input. Pretty much all the regulatory work was done behind closed doors.
Terrific for Pfizer. Bad for the public.
Of importance, note that in the trials only 21 percent of people had a comorbidity, while in reality 94 percent of COVID deaths have at least one comorbidity, and the average number of underlying medical conditions is four.
As to antiviral science, protease enzymes must be present for the virus to successfully infect by completing the cycle before taking the cell over. Paxlovid or any drug classified as a ‘Protease Inhibitor’ will inhibit or decrease the protease enzyme interfering with the virus.
Paxlovid blocks the 3CLPro protease from chopping up the long protein into pieces. The virus can’t separate out which pieces to cut out and assemble. It can’t make copies of itself. The covid infection quickly stops.
Contrary to what the government says, Ivermectin is the most successful and proven protease inhibitor in use worldwide. Just as with Paxlovid, ivermectin decreases the protease enzyme but… there are benefits of ivermectin in covid treatment that are not present in Paxlovid.
Additional actions of ivermectin include anti-coagulant action and anti-inflammatory actions, both observed in covid infections. And IVM has been safely used for decades and there have been many medical studies as well as clinical results showing its antiviral and anti-inflammatory effectiveness.
Paxlovid requires combination with an HIV/AIDS drug, Ritonavir, preventing the breakdown of the Paxlovid so it may inhibit or decrease the enzyme interrupting the viral life cycle. Ritonavir acts as a booster for Paxlovid, keeping it active inside a person’s body. Ritonavir also has its own black box warning and side effects include life-threatening liver, pancreas and heart issues.
Does the public really want to take an HIV/AIDS drug?
A course of the treatment is 20 Paxlovid pills and 10 ritonavir pills taken over five days. Taking 6 pills daily can pose challenges for many elderly people in particular.
According to Pfizer’s press release, for people with proven COVID infection, Paxlovid reduces hospitalization/death by 89 percent when taken within three days of symptom onset. So in the treatment group there were 5 of 697 hospitalized with no deaths compared to 44/682 hospitalized with 9 subsequent deaths.
Think about that statement of taking this drug combo within three days of symptom onset. Here are critical problems facing ordinary people:
- How can you accurately identify COVID symptoms from similar symptoms from the flu or a bad cold;
- How can you get a fast test; how can you get in touch with your doctor within just a day or two and decide whether you really have COVID (don’t have drug interactions) and if so get a prescription; how can you get the prescription filled quickly?
- None of these are easy to address and overcome. All this makes this new combo medicine unrealistic and impractical for nearly everyone.
Also reported was an approximate 10-fold decrease in viral load at day 5, relative to placebo, indicating robust activity against SARS-CoV-2 and representing (supposedly) the strongest viral load reduction reported to date for a COVID-19 oral antiviral agent.
How interesting it would have been to test the Pfizer drug against an ivermectin protocol.
For example, how does the Pfizer drug compare with the Dr. George Fareed and Dr. Brian Tyson protocol? Well, Fareed and Tyson had many more patients (about 7,000) taking the drug combo and yet they had fewer hospitalizations (4) and the same number of deaths (0).
So, you’re way better off with the Fareed and Tyson protocol. And the safety protocol of IVM after billions of uses globally is far better proven than for the Pfizer product.
For a good discussion on how IVM compares to Paxlovid see this article. Especially on scientific evidence of ivermectin’s ability to block 3CL protease.
In terms of safety, the most common side effects reported during treatment and up to 34 days after the last dose of Paxlovid were dysgeusia (taste disturbance), diarrhea and vomiting. But what more serious side effects may turn up months or years later?
Paxlovid must not be used with certain other medicines, either because due to its action it may lead to harmful increases in their blood levels, or because conversely some medicines may reduce the activity of Paxlovid itself. The list of medicines that must not be used with Paxlovid is included in the proposed conditions for use.
That list includes a very large number of drugs and supplements used by many millions of people, including, for example, Lipitor and St. John’s Wort. Paxlovid must also not be used in patients with severely reduced kidney or liver function.
Paxlovid is not recommended during pregnancy and in people who can become pregnant and who are not using contraception. Breastfeeding should be interrupted during treatment. These recommendations are because laboratory studies in animals suggest that high doses of Paxlovid may impact the growth of the fetus.
As to availability, Pfizer CEO Bourla recently said the company can manufacture 80 million courses in 2022, with 30 million available in the first half of the year. That is not enough to serve many millions of Americans coming down with symptoms and a positive test result.
This too was said, tens of thousands of the pills will ship in the US before the end of 2021 and hundreds of thousands more are expected at the beginning of 2022, a Pfizer spokesperson told the Wall Street Journal. The US government is paying Pfizer $5.3 billion for 10 million treatment courses that will be delivered by the end of next year, according to the paper. Will medical insurance cover $530 per course?
Always follow the money. A month ago, SVB Leerink analyst Geoffrey Porges projected the drug will generate $24.2 billion in 2022 sales. Together with the company’s megablockbuster COVID-19 vaccine, Pfizer could be looking at $50 billion in peak pandemic vaccine and drug sales, Cantor Fitzgerald analyst Louise Chen wrote earlier this month.
No surprise that some top Pfizer executives have become billionaires.
Do you want to do what is right for you, or terrific for Pfizer?
They Said They Would Slow the Spread
BY JEFFREY A. TUCKER | BROWNSTONE INSTITUTE | JANUARY 3, 2022
It’s been the most astonishing two weeks for American public life, with so many prescient changes, from new censorships, admissions, backtracks, experts speaking out, public outrage, and what strikes me as a progressive unraveling of every orthodoxy imposed nearly two years ago.
Not even the influential and powerful are in a position to defend what has happened to us. They seem to be gradually pulling away from public life, unable to say things that connect to what everyone knows.
Above all else, what’s remarkable right now is the undeniable arrival of Covid to a degree to which hardly anyone could have imagined all that time ago, when so many experts set out to deploy their fabulous new system for stopping the spread of a disease.
There was a goal (stop cases). There was a method (state compulsion). And there was a test (cases were supposed to go down and go away). There would be a war on a virus and the state would win! And now we look around and see the evidence of failure so pronounced, so impossible to deny, that we must face that which so many have worked so hard to deny for so long.
The best way I can describe this is by observation. In the Northeast of the US, and in many other parts of the country, everywhere you go, right now, you see sick people milling around. They don’t admit it and they don’t talk about it with strangers simply because there is such shame attached to having Covid. They complain of a cold, of a flu, or just suffer in silence. But there it is.
After nearly two years of work to control the spread, after brutal shutdowns of the whole country – shutdowns that happened two years too early, as judged by actual case trends (but of course lockdowns never should have been considered in the first place) – Covid is here. Not just here. It is everywhere. The case counts are beyond anything anyone on the planet could have imagined a year or two ago. The spikes make everything that came before look like child’s play.
Here is the global chart.

And we are talking really sick. Not so much death. Not even out-of-control hospitalization. We are talking about being sick in bed or walking around with misery. The nasty bug lasts maybe two days, maybe two weeks, maybe longer but it is vexing and wicked, not like a cold or flu but something more electric and strange.
Which variant? Two weeks ago, the CDC wanted to blame it all on Omicron. That is no longer possible. Perhaps that constitutes 20%; we just do not know for sure because tracking is so weak. Most of it is evidently Delta, meaning very sick but with no serious loss of taste and smell. Most everyone eventually gets well, and that’s what happens here.
We get to endemicity perhaps in a month or so and life will move on, my experts tell me, at least in some areas of the country. What’s striking and truly shocking is that all of the efforts, all of the propaganda, all of the astonishing spending and compulsion – the shutdowns, masking, size limits, travel restrictions, vaccination requirements, the track and trace, the endless testing, the enforcement, the intimidations, the censorship – and what do we have to show for it?
Lockdown architect Carter Mecher promised us as follows: “If you got everyone and locked each of them in their own room and didn’t let them talk to anyone, you would not have any disease.” They attempted a version of that, experimenting on the human population in ways without precedent. And let’s say that is true (it probably isn’t). That is not life. That is not society. That is not freedom. That is something else unimaginably horrific.
It was unsustainable. They pushed their theory without regard to the history of public health or, really, the whole of human experience. And now, the true pandemic finally arrived. And what is it? There are a ton of sick people. People are calling in sick because they cannot come to work. Institutions are having to shut down, not because government closed them but because people are too sick to come to work. This is the normal course of events – exactly what one would expect in a pandemic.
And it’s not just Covid. The head of an Indiana life insurance company reports that deaths among people aged 18-64 are up 40%, an astonishing increase. It’s suicide, drug overdoses, and every other manner of horror. And that’s just death. Many others are just sick from other things.
I personally know dozens and they each know many dozens of more people in the Northeast right now who are down for the count, miserable and pathetic, but still testing negative for Covid. Why would this be? It’s because immune systems have decayed over two years. The lack of vitamin D, the lack of exposure to normal germs in life, the isolation and depression, the overconsumption of liquor and drugs – it’s all been a terrible drain on health.
Meanwhile, the actual pandemic of Covid has certainly arrived. And it is far worse than the data indicated. Look at Massachusetts, New York, Pennsylvania, Rhode Island, Connecticut, any of these states, and including some Southern and Midwestern states, and what you find is increases of 500-1,000% in cases. And keep in mind that these are just cases as discovered by official testing spots.
Go to any CVS or Walgreens and you find long lines of people buying testing kits. If they are available. If they are not, the wait is weeks. They are $23 a kit and people are buying as many as possible. Why? Partially it’s because employers and schools are demanding negative tests, but it is also just curiosity. People are sick as dogs and want to confirm their illnesses.
People are estimating that real cases are 50x to 100x what the official data say.
But let’s talk now about a real scandal. When you are sick, you need treatment. Every competent medical professional I know is pretty darn sure that the best hope for dealing with Covid is a combination of Zinc, Vitamin D, and (sorry to mention the dreaded name) Ivermectin. This is not ideological. This is what experienced doctors are saying right now. I’m on many email lists with serious medical professionals and they are all saying the same thing. We can add HCQ to the list if you catch it early enough.
But here’s the kicker – and let me be clear that I’m NOT giving ANY medical advice here, merely just reporting the sense of the community out there. What’s remarkable is that people are having a very difficult time getting these basic therapeutics. Vaccines are everywhere but things to make you well once the virus penetrates the vaccine? Those are hard to come by.
There is a problem getting a prescription because state medical boards are actually barring people and preventing them from serving patients if they prescribe HCQ or Ivermectin, as incredible as that sounds. But once you get the prescription – if you have a doctor brave enough to risk it – finding a pharmacy to fill it is another challenge.
Most people in the UK today are getting their therapeutics from India. Americans get them from Mexico. And some are shipping to the US and they are being distributed via gray markets for anyone who is lucky enough to have a contact. It’s a speakeasy nation but this time for distributing basic therapies.
I feel like I’ve seen horrible things for almost two years now, and you feel the same way. But of all the scandals, and there are so many, this one seems to top the list, namely that once the real pandemic has arrived, there are no effective medicines that are widely available. Doctors are actually being blocked from doing their jobs.
Beyond belief. But you know this. I’m sure you have your own stories. I suspect that many of our readers have encountered this virus for the first time in the last two weeks and have dealt with the horrors of just getting basic medicines to get through this.
The NIH has funded almost no serious trials of these generic drugs. It is not in the interest of pharmaceutical companies to fund them either. As a result, we are truly at a loss – nearly two years into a pandemic at a time when people need meds more than ever.
Meanwhile, the FTC is spending its time cracking down on pharmacies that advertise that they have therapeutics available for people. They are sending cease and desist letters all over the country as a way of intimidating providers. I’ve seen these letters. They have invited me to post them but I’ve declined in the interest of keeping people out of trouble.
One merciful upside to all of this is that there is no more talk of lockdowns. At last, even the experts are saying that society must function. Lockdowns are not even being considered. The whole country is fed up with the phony baloney enterprise of virus control. It did not and cannot work.
Nearly two years ago, they deployed a new experiment in stopping a pathogen. It was a plan that was 15 years in the making, hatched by fanatics who imagined that state policy could outwit a virus.
The wreckage was astonishing, and yet what was the payoff? Here we are today with a wave of sickness that defies every prediction, and with collateral damage beyond even the worst predictions (including my own). And the truth of this is all over the data that anyone can see and the stories that anyone can hear.
The country is right now sicker than it has ever been in our lifetimes.
What a stunning repudiation of state policy – the worst failing of public health and public policy perhaps in the history of the US if not the entire world. We are right now living in its last days. Remember these days, my friends. They are legion and mark what is likely the end of the great fiasco.
And yet it is not really the end. There will be decades of hell to pay for what has happened to us.
Jeffrey A. Tucker is Founder and President of the Brownstone Institute and the author of many thousands of articles in the scholarly and popular press and ten books in 5 languages, most recently Liberty or Lockdown.
The Shadowy CIA Data Firms Behind the Creation of Digital Vaccine Passport IDs
Daily Veracity | December 17, 2021
In January 2021, tech giants such as Microsoft, Oracle, and MITRE Corporation announced their launch of the Vaccination Credential Initiative (VCI) in partnership with healthcare companies.
On their website, the VCI describes itself as an alliance of private and public organizations dedicated to the development of the ‘issuance of verifiable health credentials’ bound to an individual digital identity.
The VCI idea depends upon a common platform from which digital wallets can be created, and on the VCI website they call for “participating organizations to commit to implementing, testing, and refining the SMART Health Cards Framework within their sphere of influence.”
According to VCI, their ‘SMART Health Cards’ are meant to “work across organizational and jurisdictional boundaries.”
SMART health cards as of now include a person’s name, gender, birth date, phone number, and email address, as well as vaccination status. Developers hope, however, that these cards will eventually become all-encompassing universal digital identities that reside within a universal digital wallet.
Josh Mandel, one of the main developers behind VCI’s SMART health cards system, said once that a complete universal digital identity is ‘essential’ to the effort of creating digital vaccination passes.
On their website, the group uses the term ‘digital wallet’ often and notes that SMART Health Cards could soon be used as digital IDs for all activities, including travel and every purchase an individual makes during commercial activity.
According to the ‘about’ section on their website, the group’s members section includes corporations like Amazon, Microsoft, Google, Apple, and the MITRE Corporation.
Along with the MITRE Corporation, one of the groups listed in the governance section on the website is the Commons Project Foundation, which is the main backer of the VCI and also hosts the VCI website.
The Commons Project Foundation also describes itself as a ‘private and public alliance.’
Listed on the leadership board of the Commons Project Foundation is the President of the Rockefeller Foundation, the Global Head of Performance at BlackRock, the senior managing director at the Blackstone Group, and Julie Gerberding, the former director of the CDC. Gerberding once wrote an op-ed in Time Magazine calling for an ‘International Pandemic Surveillance Network.’
There are many other heads of multilateral development banks (MDBs), former Goldman Sachs partners, UN advisers, and other multinational corporations listed on their assembly.

With the help of the World Economic Forum and the Rockefeller Foundation, the Commons Project Foundation runs the Common Trust Network. Like the Vaccination Credential Initiative and the Commons Project Foundation, the Commons Trust Network describes itself as a ‘private and public alliance.’
The World Economic Forum’s website lists the CEO and CMO of the Commons Project Foundation as Paul Meyer and Bradley Perkins respectively. Following his career at the US Center for Disease Control, Perkins was on the advisory board for the RAND Corporation, and his Partner Paul Meyer wrote President Clinton’s speeches while attending Yale.
In partnership with the World Economic Forum and the Rockefeller Foundation — as well as an almost endless list of corporations and government agencies — the Commons Project Foundation created the CommonPass.
According to the World Economic Forum’s website, just like the VCI, the Commons Project Foundation seeks to “develop and launch a standard global model to enable people to securely document and present their COVID-19 status to facilitate international travel and border crossing.”
The site states that their ‘CommonPass‘ is powered by their “CommonTrust Network™ Registry and VCI™ Directory.” and will allow individuals to document their “COVID-19 status to satisfy country or state entry requirements,” and “access lab results and vaccination records when you need it.”
Why RFK, Jr.’s Latest Book Didn’t Hit No. 1 on New York Times Best Sellers List
By Tony Lyons | The Defender | January 4, 2022
The New York Times reportedly bases a book’s position on its bestseller list on what they call a proprietary algorithm. Whatever their method, they favor specific books, ignore others, and rankings are often disconnected from how many copies of a book were actually sold to consumers.
You probably thought the New York Times Best Sellers list reflected book sales, but it doesn’t. It’s an engine of censorship, corruption and misinformation.
How do we know this? Follow the numbers.
Can a book outsell every other book in the U.S. and not be the #1 New York Times Bestseller? Sure. Is that perhaps a form of censorship? Yup.
Robert F. Kennedy, Jr.’s latest book, “The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health,” was published Nov. 16, 2021, by Skyhorse Publishing, Inc.
The New York Times reportedly bases a book’s position on its bestseller list on what it calls a proprietary algorithm. Whatever the method, the Times favor specific books, ignore others, and rankings are often bizarrely disconnected from how many copies of a book were actually sold to consumers.
As every publisher in America knows, you can’t make the Times’ list without selling a substantial number of books through Barnes & Noble, as well as “the independents.”
But what if Barnes & Noble decides to buy very few copies of a book based on its subject matter? And what if some independents exhibit similar bias by boycotting the book, refusing to carry it and telling customers that they won’t even special order the book?
That’s what happened in the case of Kennedy’s “The Real Anthony Fauci”: Barnes & Noble purchased an unusually small quantity, and they kept the book invisible in most of their stores.
Independent booksellers, such as the San Francisco-based City Lights, don’t list the book on their website, tell customers they “don’t carry the book” and refuse to order it, even upon request. These decisions have nothing to do with customer demand or interest in the book.
Perhaps because of the trend toward politicization by bookstores that report sales to the Times, Amazon now accounts for an increasingly large percentage of book sales in the U.S.
On the one hand, the Times’ list is inaccurate because it applies an outdated, and increasingly irrelevant, view of how books are sold. On the other hand, it appears the Times’ bestseller list intentionally misrepresents actual consumer sales and demand.
Let’s see that in action by using “The Real Anthony Fauci” as a case study. The book boldly challenges mainstream narratives. It’s a serious work that makes legitimate, meticulously researched arguments.
With more than 2,000 citations and references, the book asks readers to engage in dialog and debate. At the end of each chapter, there’s a QR code that links to a website containing updates, critiques and new information.
“The Real Anthony Fauci” was carefully vetted by doctors, scientists and lawyers. It has received substantial support from leading scientists, including at least one Nobel Prize-winning scientist.
This type of book cannot possibly be what any reasonable person has in mind when they seek to protect the public from “misinformation.”
Kennedy’s tour de force resonates so strongly with the American public that, despite epic censorship, “The Real Anthony Fauci” is one of the bestselling books in America.
It has achieved this status despite a total media blackout. There hasn’t been a single review in a major newspaper, online platforms have rejected advertising — some calling it “misinformation” before anyone could actually have read it — and bookstores are boycotting it.
In the past, people perused the New York Times Best Sellers list because they believed it represented an honest account of what people across the country were reading.
Today, alas, the New York Times Best Sellers list represents a political point of view and has become a way to encourage Times readers to buy and read books that the newspaper owners approve of — and to avoid books they don’t approve of.
The playbook from major newspapers and other media outlets is transparent: Attack the author, ignore the book.
In Kennedy’s case, the hit pieces have come from Town & Country, The New York Post, Vanity Fair, The Associated Press and others. (The Times hasn’t reviewed the book, of course, but describes it as a new book by an “anti-vaxxer.”)
Again, despite the epic censorship, there has been enormous grassroots demand for this book, and it’s burst through the blockade to hold the #1 spot on Amazon Charts and also become the #1 USA Today, #1 Publishers Weekly, and #1 Wall Street Journal bestseller.
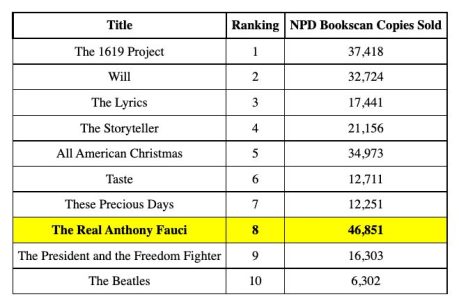
The New York Times, however, listed it at #7 in the first week and #8 in the second. That must mean the book sold fewer copies than the books with higher rankings on the list, right? Wrong.
Few people ever see the actual numbers of books sold, so let’s break that tradition and share it all: The week Kennedy’s book was ranked #7 by the Times, it sold more than 92,000 hardcover copies.
That’s four-and-a-half times as many copies as two of the books ranked ahead of “The Real Anthony Fauci,” and more than double the average of all the books ranked ahead of it.
The fact is no book anywhere on the list sold more copies than “The Real Anthony Fauci.” (The book that earned the coveted #1 slot was the Times’ own “1619 Project,” which sold thousands fewer copies than Kennedy’s book.)
New York Times Best Sellers List
Nov. 21, 2021 (Reported Dec. 5)

The week after that, the Times again placed the “1619 Project” in the #1 position, as if it had sold the most books, even though it undersold Kennedy’s book by more than 20%.
And they moved “The Real Anthony Fauci” down to the #8 position — even though it outsold every other book on the list. It sold nearly three times as many copies as the book the Times listed as #3.
New York Times Best Sellers List
Nov. 28, 2021 (Reported Dec. 12)
The Times obviously doesn’t want its readers to know how well Kennedy’s book is selling, likely hoping that’ll stymie demand.
But Americans are smarter than the New York Times gives them credit for — in less than four weeks, “The Real Anthony Fauci” sold more than 400,000 copies in all formats.
Americans clearly don’t like to be told what to think or what to read — or what not to read. Buying “The Real Anthony Fauci” has become a vote, sort of like a straw poll, against the increasingly insidious censorship in America.
Tony Lyons, president and publisher at Skyhorse publishing, and an attorney, was publisher at The Lyons Press between 1997 and 2004. He founded Skyhorse Publishing in 2006 and has been involved with every aspect of the book publishing process.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
BUY TODAY: Robert F. Kennedy, Jr.’s New Book — ‘The Real Anthony Fauci’
Reports of COVID Vaccine Injuries Pass 1 Million Mark, FDA Signs Off on Pfizer Booster for Kids 12 and Up
By Megan Redshaw | The Defender | January 3, 2022
The Centers for Disease Control and Prevention on Dec. 31, 2021, released new data showing a total of 1,000,229 reports of adverse events following COVID vaccines were submitted between Dec. 14, 2020, and Dec. 24, 2021, to the Vaccine Adverse Event Reporting System (VAERS). VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S.
The data included a total of 21,002 reports of deaths and 162,506 reports of serious injuries. Excluding “foreign reports” to VAERS, 709,084 adverse events, including 9,623 deaths and 62,069 serious injuries, were reported in the U.S. between Dec. 14, 2020, and Dec. 24, 2021.
Foreign reports are reports received by U.S. manufacturers from their foreign subsidiaries. Under U.S. Food and Drug Administration (FDA) regulations, if a manufacturer is notified of a foreign case report that describes an event that is both serious and does not appear on the product’s labeling, the manufacturer is required to submit the report to VAERS.
Of the 9,623 U.S. deaths reported as of Dec. 24, 20% occurred within 24 hours of vaccination, 25% occurred within 48 hours of vaccination and 61% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 499.7 million COVID vaccine doses had been administered as of Dec. 23. This includes 291 million doses of Pfizer, 190 million doses of Moderna and 18 million doses of Johnson & Johnson (J&J).

Every Friday, VAERS publishes vaccine injury reports received as of a specified date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed. Historically, VAERS has been shown to report only 1% of actual vaccine adverse events.
U.S. VAERS data from Dec. 14, 2020, to Dec. 24, 2021, for 5- to 11-year-olds show:
- 5,706 adverse events, including 114 rated as serious and 2 reported deaths.
- 11 reports of myocarditis and pericarditis (heart inflammation).
- 14 reports of blood clotting disorders.
U.S. VAERS data from Dec. 14, 2020, to Dec. 24, 2021, for 12- to 17-year-olds show:
- 25,802 adverse events, including 1,506 rated as serious and 34 reported deaths.
The most recent death involves a previously healthy 15-year-old girl from Wisconsin (VAERS I.D. 1963633), who experienced a cerebral and intraventricular hemorrhage secondary to a ruptured aneurysm. She also tested positive for SARS-CoV-2 despite having been fully vaccinated.
- 61 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment or resulted in death — with 96% of cases
attributed to Pfizer’s vaccine. - 579 reports of myocarditis and pericarditis with 568 cases attributed to Pfizer’s vaccine.
- 146 reports of blood clotting disorders, with all cases attributed to Pfizer.
U.S. VAERS data from Dec. 14, 2020, to Dec. 10, 2021, for all age groups combined, show:
- 19% of deaths were related to cardiac disorders.
- 54% of those who died were male, 41% were female and the remaining death reports did not include the gender of the deceased.
- The average age of death was 72.3.
- As of Dec. 24, 4,692 pregnant women reported adverse events related to COVID vaccines, including 1,487 reports of miscarriage or premature birth.
- Of the 3,358 cases of Bell’s Palsy reported, 51% were attributed to Pfizer vaccinations, 41% to Moderna and 8% to J&J.
- 815 reports of Guillain-Barré syndrome (GBS), with 41% of cases attributed to Pfizer, 29% to Moderna and 28% to J&J.
- 2,241 reports of anaphylaxis where the reaction was life-threatening, required treatment or resulted in death.
- 12,070 reports of blood clotting disorders in the U.S. Of those, 5,341 reports were attributed to Pfizer, 4,302 reports to Moderna and 2,275 reports to J&J.
- 3,405 cases of myocarditis and pericarditis with 2,379 cases attributed to Pfizer, 1,197 cases to Moderna and 152 cases to J&J’s COVID vaccine.
FDA clears Pfizer boosters for 12- to 15-year-olds, bypasses experts
The FDA today amended Emergency Use Authorization (EUA) for Pfizer’s COVID vaccine expanding eligibility for boosters to children 12 through 15 years of age.
The agency did not consult its expert panel of vaccine advisors, who in September, overwhelmingly rejected boosters for healthy people 16 and older.
The FDA also shortened the time for both adolescents and adults to receive a booster from six months to five months after receiving a second dose and authorized a third shot for immunocompromised children aged 5 to 11.
Dr. Peter Marks, director of the Center for Biologics Evaluation and Research at the FDA, said in a statement the agency made its decision because a third dose “may help provide better protection against both the Delta and Omicron variants.”
The FDA said it reviewed real-world data from Israel of more than 6,300 individuals 12- to 15-years-old who received a booster at least five months after their second Pfizer dose and found no serious safety concerns.
Likewise, additional data showed no problems giving anyone eligible for a Pfizer booster an extra dose at five months instead of six, the Associated Press reported.
The FDA said it will continue to review the information and communicate with the public if data emerges suggesting booster doses are needed for the younger pediatric population.
Pediatrician weighs in on FDA decision: children aren’t ‘mini-adults’
Dr. Michelle Perro, pediatrician and co-author of “What’s Making Our Children Sick,” disagreed with the FDA’s decision, pointing out that “children are not mini-adults.” In an email to The Defender, Perro said children’s rapid growth, quick cellular turnover and less efficient detoxification pathways are factors that must be considered whenever any new therapeutics are being introduced.
Perro said:
“This newest immunomodulating therapy, the mRNA inoculation, has already been shown to have produced multisystem negative health outcomes in children garnered from the CDC’s own database.”
Perro outlined five reasons she believes this “experimental therapy” must be immediately withdrawn:
- Gene-edited injectables have not been adequately studied in children as per Pfizer’s own data, where they meshed childrens’ and adults’ data together.
- The injection utilizes nanotechnology which is now part of the emerging technology in vaccinology research. These nanoparticles are so small in size they can cross the blood-brain barrier which can adversely affect our already fragile population of children.
- The mRNA itself is unstable and is thus encapsulated in a lipid biosphere comprised of a polyethylene glycol shell which in itself is toxic.
- The number of children suffering from already documented irreparable side effects from the inoculations, such as those occurring in their hearts (myocarditis), is not only unacceptable but immoral.
- Children’s healthcare providers are neither educated or proactive in diagnosing and treating the effects from this experimental therapy.
Perro questioned the FDA’s motives, given that children suffer nearly zero morbidity and mortality from COVID infections.
She also said the FDA is “veering from” its own historical stance.
“When previous true vaccines were introduced historically (rotavirus vaccine), after just a few cases of adversity, they were immediately withdrawn,” Perro told The Defender. “The FDA must adhere to its own historical position regarding their assigned task of the protection and oversight of our country’s greatest asset: our children.”
Fauci says hospitalization numbers for kids with COVID are overcounted
Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, in an interview on MSNBC, said statistics for hospitalizations among children with COVID are overcounted, making clear the distinction between children hospitalized with COVID and children hospitalized “because of COVID.”
Speaking to MSNBC’s Ayman Mohyeldin, who was filling in for Rachel Maddow on Dec. 29, about the rise in hospitalizations among children amid the Omicron variant, Fauci said the surge is due to two contributing factors — more children getting infected and the way COVID cases are counted.
“And what we mean by that — if a child goes in the hospital, they automatically get tested for COVID. And they get counted as a COVID-hospitalized individual,” Fauci said. “When in fact, they may go in for a broken leg or appendicitis or something like that. So it’s overcounting the number of children who are, quote, ‘hospitalized with COVID,’ as opposed to because of COVID.”
UK plans to test EVERY school child TWICE this week
… so what happens when you run 7 million lateral flow tests in five days? And are you ready for the “new wave” of “cases” it will likely produce?
OffGuardian | January 3, 2022
New plans, announced before Christmas, will require every secondary school pupil in the UK to take an on-site Covid test when school resumes after the Christmas break.
The government plans, allegedly to “monitor” Covid infection in students, go on to suggest that every child should receive a follow-up test 3-4 days later.
The tests being used are lateral flow tests, which have repeatedly been shown to be completely unreliable, and can test positive using apple juice or coca-cola.
There are roughly 3.5 million school pupils aged 11-16 in the UK and they plan to test them all twice.
If just 2% of them test positive just once, the media will scream about 140,000 new “cases” of Covid in children.
Further, the “recommendations” suggest children should then continue to be tested twice a week, every week, or “more frequently if asked to do so”:
Secondary, college and university students and education staff and early years staff should then continue to test themselves twice a week, and more frequently if they are specifically asked to do so, such as in the event of an outbreak.
At least 7 million lateral flow tests per week, every week.
It’s not hard to see where it goes from there, with the headlines blaring that lack of social distancing over the holidays gave rise to a “fourth wave” (or would it be fifth? I’ve lost count).
I would start preparing for a new lockdown, if I were you.
Lukashenko Told You It Was a Psychosis TWO YEARS Ago

Anti-Empire | January 3, 2022
The entire interwebs are ablaze with the term “mass formation psychosis”. Since a smart Ph.D. visited Joe Rogan everyone and their grandmother are now reading up on it, and emitting into the ether how the COVID panic (hysteria) is nothing but a mass psychosis. That is great. Except that it is January freaking 2022.

It has been a psychosis for nearly TWO YEARS now. It has been evident it is nothing but brain rot in the heads of excitable idiots this whole time. Aleksandr Lukashenko, a Belarusian potato farmer, and a much less educated man than Dr. Robert Malone, diagnosed it as a “psychosis” and an “info-demic” way back in March 2020.
“Despite some criticism on my part, I call this coronavirus nothing other than a psychosis, and I will never deny that, because I’ve gone through many situations of psychosis together with you, and we know what the results were.
“Coronavirus is yet another psychosis, which will benefit some people and will harm others.”
Doesn’t it seem to you that the powerful forces of the world would like to remake the world, without a ‘war’(Emmanuel Macron has already called it a war), through this so-called ‘corona-psychosis’, or ‘info-demic’? Many people are asking: ‘what will happen after the pandemic?’”
Some need the permission of a PhD to start thinking, preferably a PhD they saw on a massive media outlet like Rogan.* Others, like Lukashenko have their common sense.

*Who is on record as saying that without lockdowns you would have had more COVID deaths.
Covid Hospital Admissions Rising, but a Third Admitted For Something Else
By Toby Young | The Daily Sceptic | January 1, 2022
There follows a guest post by the Daily Sceptics’s in-house doctor, formerly a senior medic in the NHS. He’s run his eye over yesterday’s data release from NHS England that has given rise to some panicky headlines (“Frightening new Covid data shows Boris Johnson’s omicron gamble may be about to implode” – The Telegraph). Covid hospital admissions are indeed rising, but a third only have Covid incidentally, i.e. it’s not the reason they were admitted to hospital.
Yesterday afternoon the Primary Diagnosis update was released by the NHS. Readers of this site will be aware the spreadsheet contains information about which patients are being treated for Covid as the primary diagnosis (in other words symptoms sufficiently severe to put them in hospital for a while) and patients testing positive for Covid but being treated for something else.
The NHS concealed this information until they were forced by parliamentary pressure to publish in July 2021.
Graph One shows the overall situation in English Hospitals. Daily admissions in blue bars. 7 day moving average on the brown line. Readers will appreciate that the current seven day MA is the same as it was in mid-September and lower than mid-October. It can be seen on the right-hand side of the graph that on December 28th there was a sudden spike in cases. This may be recording artefact due to delay in logging cases over the bank holiday. There may also be some delay in discharging patients over the extended four-day weekend. Or it could be the beginning of a ‘nailed on tsunami of cases’. We will know more next week.

What we can’t tell from this graph is the turnover of patients in hospital. The NHS has this information but will not release it. It’s actually quite important because it gives a better impression of the severity of Omicron vs Delta. For clarity I should say that even if patients are less unwell, a large number of them can still stress the system, but as long as the inpatients can be managed through the hospital phase in an efficient manner and the numbers going out keep pace with the numbers coming in, the problem is manageable. The real difficulty with high turnover is the intensity of the workload on staff to keep up with the pace, and clearly there is also a problem with staff absence due to positive testing.
Graph Two is complicated but important. It shows the acute Covid cases on the blue bars, the incidental cases in the yellow bars and the ratio between the two on the gray line. Readers will see that the blue bars go up on the right-hand side, but the yellow bars go up a lot more. This means there are proportionately more ‘incidental’ cases than ‘real’ cases and the ratio (gray line) is dropping to 0.67. So, when the BBC report the number of Covid cases in hospital, only two thirds of that number are ill with Covid.
Again, for clarity, one should not assume that lots of patients with incidental Covid are not problematic. They do create a problem because of so called ‘cohorting’ – essentially positive patients need to be separated from negative patients and nursed separately. This creates difficulties in allocating specialist nurses and staffing rotas if the patients have to be located in different wards to where they otherwise would be. It also causes trouble for scheduling operations in respect of extra precautions being taken for positive patients and so on – so it generally increases organisation ‘friction’ and reduces efficiency.

Overall, the falling ratio of incidental to real cases reflects the transmissibility of the new variant. It seems to me that eventually everyone is going to get this virus one way or another. On the other hand, the symptoms it causes do genuinely seem to be mild in comparison to previous variants.
Experts in the media are commenting that the NHS is concerned about the risk of being overwhelmed by a surge of older people being admitted next week. The ZOE app data does show a rise in cases in the 55-75 age group in the last few days. Whether that translates into more severe admissions is difficult to say – the NHS do release information about age group admissions, but the next packet is not due until mid-January.
Finally Graph Three shows the data for London, the leading edge of the Omicron wave. Again, the blue line (acute admissions) is going up, but not as fast as the brown line. The doubling time of acute hospital cases is 28 days – this is quite clearly very much slower than the doubling time of positive community tests (about three days before Christmas).
The ratio between the lines is 0.67, the same as England as a whole. From the weekly hospital summary, also released yesterday, it is clear that not all London hospitals are equally affected. The East and South-East areas are proportionally worse off than the West and Central areas. This may reflect differences in community vaccination rates in parts of the capital.

In summary, this information is very revealing. It suggests that the real problem is not vast numbers of very sick people who are likely to die and use up large amounts of NHS resources. Rather there are large numbers of moderately ill people who do require some supportive care in hospital, but an increasing number of incidentally positive patients who create organisational friction as they have to be cared for separately from non-positive patients at a time when a lot of staff have also been sent home with positive tests or contacts.
Whether further social restrictions make a material difference to this situation is a moot point. Some of my colleagues think reimposing a societal lockdown will reduce the peak of the wave and allow hospital management to keep on top of the problem. Others think further lockdowns will serve no purpose and the wave will transmit through the population anyway regardless of euphemistic ‘non pharmaceutical interventions’.
Readers will remember that when societal restrictions were imposed in January of 2021 they were not lifted until July, and even then, there was substantial opposition from the NHS. Finally, in the intensifying clamour for lockdown from the usual quarters, I have not seen any balance in their argument in respect of the collateral damage to health and the obvious quantifiable damage to the economy, businesses and jobs. I wonder why that could be?
Happy New Year everyone.
Vaccine evasion and an Original Antigenic Sin signal in Ontario
el gato malo – bad cattitude – january 2, 2022
there is some really interesting data coming out of ontario on vaccine efficacy (VE) and vaccine evasion from omicron.
it also seems to be being widely misinterpreted/misread, so i want to put a paw in here and opine.
this is the key chart. (generated from the ontario gov’t website HERE)
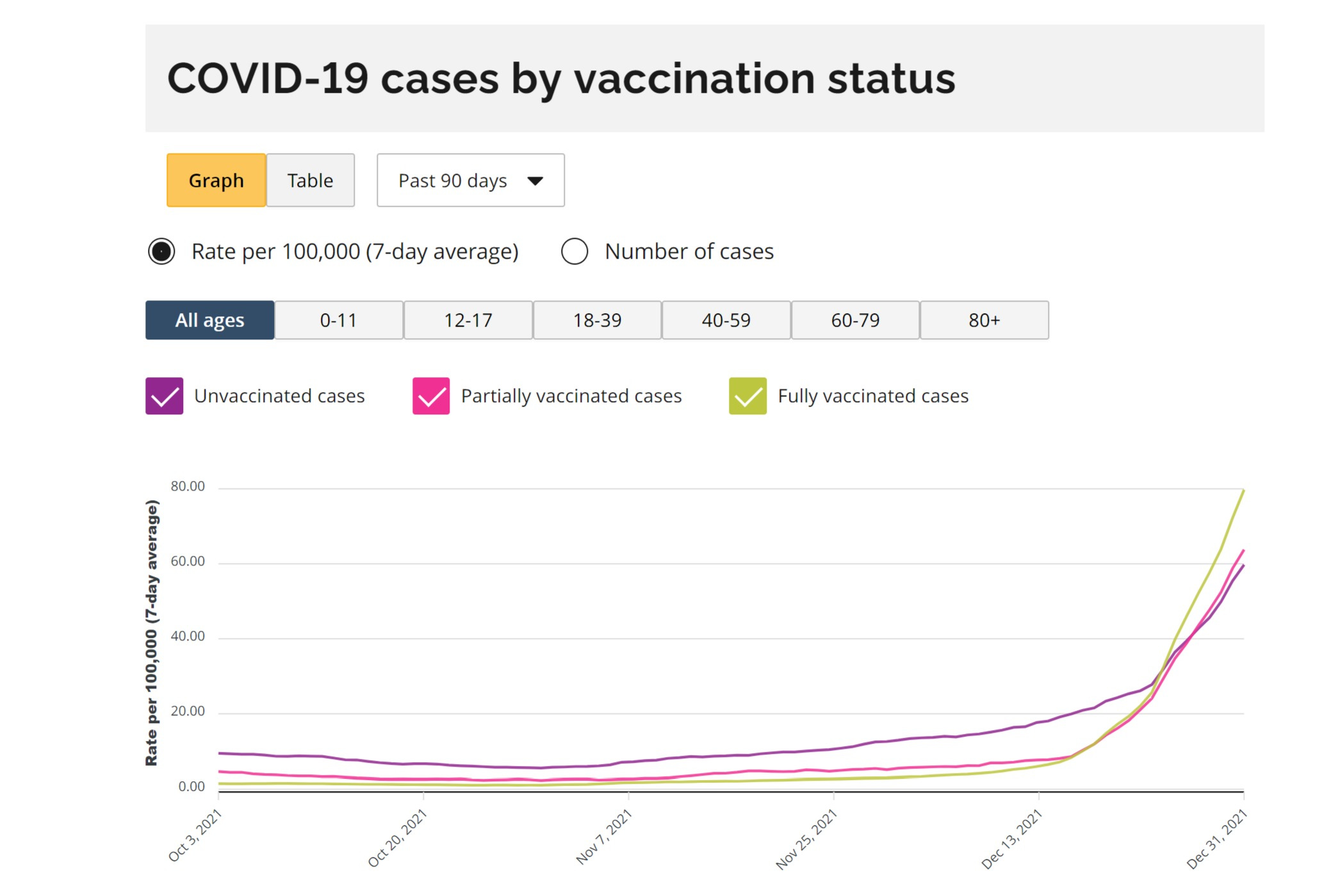
and it shows something incredibly interesting. it shows vaccines working to stop cases until mid december and then suddenly inverting. this is presumably due to omicron.
vaccination just fell to a -33% VE for cases and this looks to be worsening rapidly, likely because of a rise in omicron prevalence.
this is consistent with not just vaccine escape, but vaccine driven acceleration.
the vaccinated are getting covid at higher rates than the unvaxxed and that rate looks to be increasing rapidly as omi gains viral share.

many are denying this and calling it a simpson’s paradox (SP) where each subgroup is actually showing strong VE but where the way they aggregate causes the net figure to invert and imply an erroneous relationship that does not actually pertain. such things have been common in covid data.
i think this claim is incorrect.
firstly, if this is an SP, then why did that not manifest before? why did the relationship for case reduction invert so suddenly? it was certainly not a massive, sudden change in who was vaccinated.
this confusion has been greatly amplified by the website itself. when you select for any given age cohort, it shows positive VE for cases. this seems to be an open and shut case for this being an SP.
but it’s not. such claims contain a severe error. can you spot it?

look closely at the dates. see where they end?
all the age cohorted data ends in october.
the same is true of the data in the table above. it’s full blown apples and oranges. there seems to be no post october age delineated data in this system at all.
but the change in vaccine efficacy pattern did not occur until mid decemeber. so, this is an irrelevant comparison to the current data and current situation. it actually agrees with the first chart.
whether this is just carelessness or sloth on the part the ontario health agencies or a subtle and cunning manipulation is anyone’s guess and i’m not going to wade into that. but i HAVE seen an awful lot of smart people miss this. (i missed it at first too) you simply do not expect to see the data truncate like that on the same graphing tool.
just one more cautionary tale on data handling…
ADDENDUM OF EXCELLENT GRAPHIC FROM GATOPAL™ ORWELL2024.

and an additional catch:
“The https://covid-19.ontario.ca/data says: “Due to technical difficulties, the case rate by vaccination status by age group is not available”.
We can lockdown the entire economy, but can’t fix a dashboard that would help showing what’s going on?”
https://twitter.com/orwell2022/status/1477636960348946436?s=20
this is what team work looks like and it’s how we make progress.
(END ADDENDUM)
but the conclusion here looks to be that this data (along with data from many other places) is consistent with omicron being not just a vaccine escaping variant, but one that is actually vaccine enabled.
if it was just escape, we’d see parity with the unvaxxed. having it go strongly negative is a sign that the vaccine is making it worse either though OAS/antigenic fixation or some other mechanism.
See:
Is original antigenic sin starting to dominate covid?
the good news is that omicron looks mild. the bad news is that it increasingly looks like the variant that original antigenic sin (OAS) begot and this means that the vaccinated may be wide open for it in a way they would not have been had these programs not been rolled out. worse, they may NEVER be able to generate sound immunity because that’s what OAS…
and this data starts to get STARK when you isolate the omi variant alone.
this leads me to predict that the curves will continue to separate in ontario as omicron becomes more prevalent and that we’ll start seeing VE’s that look more like denmark.
will keep an eye on it (and hope they keep reporting the data).
Featured Video

Argentina’s Javier Milei sells out his country for Israel
or go to
Aletho News Archives – Video-Images
From the Archives
Mutually Assured Delusion (MAD)
By Judith Curry | Climate Etc. | November 5, 2013
Groupthink: A pattern of thought charaterized by self-deception, forced manufacture of consent, and conformity to group values and ethics.
Groupthink: Collective Delusions in Organizations and Markets, by Roland Benabou, published in the Review of Economic Studies. Benabou also has a talk (ppt slides) on this subject.
First, a definition of groupthink (from the ppt slides):
Janis (1972)’s eight symptoms [of groupthink]:
- illusion of invulnerability
- collective rationalization
- belief in inherent morality
- stereotyped views of out-groups
- direct pressure on dissenters
- self-censorship
- illusion of unanimity
- self-appointed mind guards
Sound like any groups that we know? … continue
Blog Roll
 Aletho News
Aletho News- Iran says EU’s insistence on sanctions hastens its ‘embarrassing descent into irrelevance’
- Argentina’s Javier Milei sells out his country for Israel
- Putting Nukes in Finland Won’t Make Country Safer, Finnish Politician Cautions
- Ukrainian drone strike kills worker at Europe’s largest nuclear power plant
- What the West Hides About Soviet Role in De-Colonization
- Villains of Judea: Douglas Feith
- US pension fund invests hundreds of millions in weapons firms supplying Israel
- US bill to grant Americans serving in Israeli army same rights as US troops
- What a president, a movie star, a congressman, and a cell phone all dared to say
- ‘An entire nation is being humiliated by the Iranian leadership’: Merz
- If Americans Knew
- Palestinians in Gaza Want to Rebuild Food Systems. Israel Isn’t Letting Them.
- Under Trump, Green Card Seekers Face New Scrutiny for Views on Israel
- Sheep Theft Sent Shockwaves Through a Palestinian Village. Then, a 12-year-old Boy Was Shot Dead
- Trump alum helps Israel mount AI influence campaign
- Dispatches From Catastrophe
- Despite Denials, AIPAC Is Now Funding Campaign of Ala Stanford In Philadelphia
- Israel’s neighbors are irate about its treatment of religious sites
- Israel escalates in Gaza: killing, torture, hunger – Daily Update
- Six Months into Gaza Ceasefire, Setting the Record Straight About Aid
- ‘Silent suffering’: Why children in Gaza are losing their ability to speak
- No Tricks Zone
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
