17 reasons why it is irrational to trust the medical community regarding the covid vaccines
Public health policies over the past two years have failed to curb covid at all but wrought unmitigated societal devastation. What exactly have they done right?
Ashmedai | February 3, 2022
One of the most intractable impediments to convincing people of straightforward facts relating to the covid vaccines is their instinctive and unshakeable trust of the mainstream medical community, and especially their personal doctor/s.
To that end, here a series of arguments or reasons why it is not just imprudent but irrational to have faith in the mainstream medical community and everyone who relies on them as a primary source of covid vaccine information.
Another objective is to empower people to articulate their clear and reliable intuition that the medical community lacks institutional credibility and objectivity rather than doubt their own intellectual ability.
It is necessary to preface that when I refer to the medical community or establishment, I am not referring to any of the heroic doctors and other professionals who do think and act independently of the mainstream medical community. In fact, you can pretty much apply to them the inverse of all the arguments enumerated below.
Another critical point to keep in mind is that even though most of the arguments below only directly apply to part – or even a select few individuals – of the mainstream medical community, they are nevertheless an indictment of the entire medical community. It is a tightly interwoven, interconnected and insular group that shares information widely through a variety of channels and feedback mechanisms. Information deriving from a corrupted source anywhere in the medical community thus infects the entire medical community. Its insular nature regarding what they consider to be acceptable sources for scientific or medical information means that they largely lack a mechanism for allowing correction of faulty information from an external source.
For the most part, I restricted the arguments presented to those that can be made from premises that are objectively true regardless of where one falls regarding the covid vaccines.
One final point is that the contention that it is irrational to trust the medical community regarding the vaccines is derived from the totality of the evidence. In other words, when there are a dozen major red flags, it is prudent to assume that there is something systematically rotten about the whole system; in this case it that means it would be irrational to regard them as a reliable source of information for anything to do with the covid vaccines.
For the following reasons, the medical establishment is unequivocally untrustworthy regarding the vaccines:
- The mother of all biases: The medical community bet every ounce of credibility and authority they had on the vaccines being safe and effective, so they cannot afford to ever admit they were wrong should the vaccines ultimately turn out to have real safety issues
- The politicization of the medical community
- The insistence on a “One Size Fits All” contrary to fundamental medical practice
- The lack of consistent evidentiary standards
- Few medical professionals including those involved in making policy or opining on the vaccines have any idea how the vaccines work
- They got pretty much everything about covid wrong before the vaccines
- The failure to treat covid
- The lack of critical or independent thinking by anyone in the mainstream medical community
- The medical community failed to convey basic risk stratification
- Public health officials used wrong information and spurious data to construct pandemic policies
- The medical community never admitted that they made serious mistakes
- The denial of natural immunity
- Censorship and Fraud
- They don’t denounce useless and harmful practices derived from their policies and statements
- The medical establishment is riddled with massive financial conflicts of interest
- Every specific claim made regarding the vaccines so far has ultimately proven to be false
- A significant % of the medical community are genuinely evil people
1. The mother of all biases: The medical community bet every ounce of credibility and authority they had on the vaccines being safe and effective, so they cannot afford to ever admit they were wrong should the vaccines ultimately turn out to have real safety issues
Never in recent memory has there been such a powerful bias afflicting the medical community or public health officials. They have loudly and daily proclaimed in the most definitive ways imaginable that the covid vaccines are absolutely safe and effective, to the point of advocating that people be compelled by various means to get vaccinated. Billions of people followed their advice, and billions more succumbed to their pressure.
If the truth is that these vaccines are not quite as safe as they say, that would mean that potentially millions people died, and perhaps tens or even hundreds of millions suffered all sorts of horrible injuries because of them, or contracted covid despite vaccination because they were lulled into a false sense of security that the vaccines are essentially impervious and subsequently contracted severe covid disease or even died.
Their credibility would be absolutely blown to pieces. After all, they were as definitive as possible. And they attacked with unrestrained zealotry anyone who dared to even voice a little skepticism. They have publicly humiliated, attacked, defamed, castigated, chastised, mocked and scorned those who refused to accept their proclamations of functionally impervious vaccine safety.
The inherent human impulse to preserve one’s sense of integrity, morality, and righteousness is severely threatened by the prospect of conning the world into a hastily rushed intervention that proved to be the deadliest therapeutic ever released and foisted upon the public.
Another powerful innate human impulse is to preserve oneself from facing accountability for enormously consequential rank negligence – if the vaccines are anywhere near as dangerous and lethal as a growing mountain of data and studies now indicate, “rank negligence” doesn’t even begin to describe the depth of culpability here.
And let’s not forget that not only is their expertise is on the line, but so is the essence of their professional identity. If the medical community got this wrong and people figure it out, the medical community will become a pejorative to many if not most people, an institution completely denuded of credibility and thought of as a modern cult.
This is true as much for the small community doctors as it is for Fauci, for they too are complicit in convincing people that the vaccines were “safe and effective”, albeit on a smaller scale.
In Short: It is not rational to expect that the medical community can be remotely objective about the issues pertaining to the covid vaccines, let alone be willing to admit that the vaccines are not safe, when they are so heavily and intractably invested in the vaccines being as safe as they promised they would be. This is especially true now that they took a significant hit on the efficacy claims as Omicron publicly humiliated them when it shredded any notion that the vaccines could stop transmission, a critical and prominent early claim of vaccine proponents.
2. Politicization of the Medical Community
The medical community has become extremely politicized. Consider the following:
- JAMA sacked their President because he had the temerity to defend doctors as not intrinsically racist
- the AMA declared that racism is a not only a public health crisis, but is the #1 PH crisis (!)
- the inclusion of race in itself as a “risk factor” used for triaging scarce covid treatments
- the sudden and radical switch from “a 10-person outdoor funeral was too unsafe to allow” to “27 million people mass protesting George Floyd was somehow not only safe but necessary to address the aforementioned “public health crisis” of systemic racism”
- The CDC’s prior advocacy for gun control, calling gun ownership a public health crisis
These are but a few of the numerous and ubiquitous instances of clear political entanglement with what are supposed to be non-partisan medical institutions, showing that political considerations clearly supersede scientific considerations in the most high-profile and impactful sorts of decisions and policies.
And this corruption of scientific standards extends into published literature. Consider the study Glaciers, gender, and science: A feminist glaciology framework for global environmental change research, where we are duly informed in the abstract:
Just what the devil are “human-ice interactions”?? This sounds more like pseudo-religious mysticism than anything remotely scientific.
And their conclusion opens with the following declaration:
“Ice is not just ice. The dominant way Western societies understand it through the science of glaciology is not a neutral representation of nature.”
Scientifically, ice is indeed just ice. Apparently, however, scientists understanding a topic solely via the scientific method is “not a neutral representation of nature”.
This used to be my cardinal example of politics conquering the scientific journals, but that was before I came across the study On Having Whiteness:
Ask yourself: just how rotten does the culture in academia have to be for an actual journal to publish the rabid deranged rantings of an unhinged lunatic? (Just imagine if someone tried to publish this sort of vile screed about “Jewishness” or “Blackness”…)
And lest you think that this paper is somehow a one-off exception, here are many more.
To cap it off, here is an example specifically related to the covid pandemic response: Approaching the COVID-19 Pandemic Response With a Health Equity Lens: A Framework for Academic Health Systems. Title says it all.
In Short: The medical establishment is openly and blatantly political, and has a history of acting against science for political reasons; this means that they are willing to put politics over science.
3. The insistence on a “One Size Fits All” contrary to fundamental medical practice that patients are unique individuals with unique health profiles
One of the cardinal rules of medicine is that every patient is a unique individual with unique medical characteristics that therefore requires individualized treatment. There is certainly no such thing as a treatment that is magically the optimal choice for every one of the hundreds of millions of people in the country.
As the few intrepid inquisitive people who bother to actually read granular scientific literature about the vaccines know, there is considerable variation between types of individuals regarding the vaccine and how best to administer it.
It is axiomatic that different people have different risks from different medical interventions. Or at least it used to be. The myopically focused hyper-aggressive campaign that quite literally every adult and child, man and woman, get vaccinated is contraindicated by all of medical history, and suggests that the medical community literally sees the vaccine as some sort of magical unicorn, something that would be seen in a cult but out of place in the practice of medicine.
The manic obsession to vaccinate even those with so-called “natural immunity” – ie immunity from having been infected with the covid virus – stands as ironclad proof of the morally unhinged and the firmly anti-science character of the medical community’s agenda to vaccinate every living human on the planet.
In Short: The aggressive, unrelenting insistence on the biggest one-size-fits-all in history that everyone get vaccinated is contrary to all prior medical standards and practice; this means that they are at minimum acting and thinking more like cult members than doctors. This also means that they are not treating patients as unique individuals in the same way they used to.
4. The lack of consistent evidentiary standards
It goes without saying that objective, unchanging standards for evaluating evidence is the very definition of scientific research and inquiry.
The utter lack of any standards used for anything Covid related stands as a starkly visible sign of the decidedly unscientific character of the medical community throughout Covid.
Lockdowns were implemented on the basis of a fringe lunatic’s crackpot model. I say “fringe lunatic” because he has a long history of delusional epidemiological predictions of viruses becoming mass-casualty pandemics where the magnitude that he was off by was itself considerably larger than the total actual deaths from the prognosticated pandemic super-killer:
[Imperial College epidemiologist Neil] Ferguson was behind the disputed research that sparked the mass culling of eleven million sheep and cattle during the 2001 outbreak of foot-and-mouth disease. (Sheep genocide!!) He also predicted that up to 150,000 people could die. There were fewer than 200 deaths.
In 2002, Ferguson predicted that up to 50,000 people would likely die from exposure to BSE (mad cow disease) in beef. In the U.K., there were only 177 deaths from BSE.
In 2005, Ferguson predicted that up to 150 million people could be killed from bird flu. (And then he said maybe 200,000,000!) In the end, only 282 people died worldwide from the disease between 2003 and 2009.
In 2009, a government estimate, based on Ferguson’s advice, said a “reasonable worst-case scenario” was that the swine flu would lead to 65,000 British deaths. In the end, swine flu killed 457 people in the U.K.
And Ferguson is still going strong:

Mask usage and mandates were adopted suddenly and unexpectedly without any sort of scientific rationale whatsoever, at least that was documented in any scientific literature.
Remdesivir was given its EUA on the basis of one trial conducted by its manufacturer, and whose primary endpoint was changed midway (which is something that typically constitutes scientific fraud) when the preselected primary endpoint failed to show that Remdesivir had any efficacy, namely that there was no reduction in mortality or hospitalization. The same story repeated itself for every pharma drug granted approval for a covid indication.
On the other hand, HCQ was demonized despite having hundreds of trials showing very convincingly that it was effective as a prophylaxis and early treatment.
Ivermectin was similarly demonized despite having dozens of RCT’s showing a clear and consistent benefit in all stages of covid.
The same goes for most of the other drugs/treatments used by thousands of doctors worldwide, such as those found in the FLCCC’s protocols – numerous studies showing a clear and consistent significant benefit, and all ignored by the medical establishment and government agencies.
The vaccine trials that provided the “robust” data for the FDA’s approval were a colossal joke. This article is long enough so I’ll avoid going through the details here, but suffice it to say that the Pfizer kids trial simply lied about paralyzing one of the kids in the trial – Maddie de Garay (along with an inhuman ordeal of excruciating agony and mental/emotional trauma). All of the treatment options on the FLCCC protocols have far more robust evidence than any of the vaccines hurriedly rushed out on the skimpiest data imaginable.
In Short: The medical establishment simply cast aside all evidentiary standards (in favor of a particular political agenda); this means that the medical establishment’s culture is against objectivity in science, and lacks the necessary mechanisms or guardrails critical to conducting objective scientific inquiry.
5. Few medical professionals including those involved in making policy or opining on the vaccines have any idea how the vaccines work
Doctors, surgeons, GP’s, infectious disease specialists, OBGYN’s, etc, etc, etc haven’t the foggiest idea of how the covid vaccines work. If you don’t believe me, go ahead and ask your local [fill in the blank] specialist/doctor to explain codon optimization, the proline swaps in the vaccine’s spike protein, self-assembling lipids, the chemical alterations to switch the positive charge of cationic lipids to neutral in a neutral PH, spike biodistribution, lipid biodistribution, and so on.
And it’s not only the vaccines themselves that are ridiculously intricate and complicated. The immune system itself is massive, twisted maze of different types of cells, molecules, pathways, and chemistry that involves the entire human anatomy. Even an experienced immunologist could not possibly predict in advance how the different and truly novel vaccine products would interact with the various human anatomical biomes.
Expert opinion is considered the lowest form of “evidence,” because when it comes to predictions, experts are almost always wrong. Were scientists’ inability to conceive of a plausible mechanism for speculative harms a viable standard to adjudicate safety concerns, the FDA could be largely retired, what with little need for the robust testing regiment all novel therapies and biological agents are subjected to in the face of staunch expert claims of lack of plausibility for unexpected adverse effects to occur. Regrettably, experts seldom recognize the limits of their expertise, and vis-à-vis covid seem unaware that any exist altogether.
In Short: The bottom line is that none of the “experts” and none of the ‘local doctors’ who are telling people the vaccines are safe and effective have any idea of the actual technical underlying science. This means that they cannot possibly provide any scientific insight, credibility, or authority regarding the vaccines.
6. They got pretty much everything about covid wrong before the vaccines
If a particular methodology consistently yields wrong answers, than it can be reasonably assumed that it will continue to do so. It is irrational to trust the same people who got masks, lockdowns, distancing, asymptomatic spread, risk stratification, seasonality, children’s risks from and spreading covid, testing, case data, hospitalization data, mortality rate, etc., etc., etc. dead wrong to suddenly know what they’re talking about when it comes to the vaccines.
And as we will get to later, pretty much every specific statement made about the vaccine that we can test against real-world results has been proven to be dead wrong.
In Short: They were wrong about everything else before the vaccines, and there is no compelling reason to think that they will do better regarding the vaccines.
7. The failure to treat covid
The failure to treat what was allegedly the worst plague in modern times is possibly the greatest medical failure of modern times. This is without considering the war they waged on effective cheap repurposed FDA-approved drugs – simply their failure to ever really treat covid is itself astounding. Quite literally the whole point of doctors is to treat medical maladies and diseases. Never in human history have doctors systematically decided not to even try and treat something, never mind the most pressing existential medical crisis in a century.
Contrast the failure of the medical establishment to treat covid with the amazing success of the thousands of heroic doctors and nurses around the world in treating covid. All that this small minority of doctors did was to simply practice the art of medicine using the tools available to them. In the words of Dr. Brian Tyson, one of the most prolific doctors who treats covid:
If you see inflammation, use anti-inflammatories
If you see blood clots, treat blood clots
If you see pneumonia, treat pneumonia
If you see hypoxemia, treat hypoxemia
If you know it’s viral, use antivirals
If you do nothing, quit practicing!!!
This isn’t complicated. The failure to treat covid is a failure to treat covid.
In Short: The medical community has failed – by choice – to treat covid, allegedly the worst plague in a hundred years; this means that something has replaced their Hippocratic culture and healer mindset as their guiding principle/s.
8. The lack of critical or independent thinking by anyone in the mainstream medical community
Consulting an expert is only meaningful if the expert will apply his or her expertise and judgement to analyze the issue presented. On the flip side, experts who uncritically go along with whatever those atop the medical community’s hierarchy promulgate not only cannot be considered as “expert opinion”, but also indicate that the free-flowing debate that is the lifeblood of scientific inquiry has clotted as though it was invaded by hordes of marauding spike proteins.
One of the more glaringly obvious characteristics of the pandemic is the shocking, Borg-like unanimity among the medical establishment. Pretty much every mainstream doctor on the establishment side is in 100% agreement with 100% of what the establishment says or does 100% of the time.
Exhibit A: Covid treatment. After two years of covid, how many prestigious hospital systems or universities have developed their own covid treatment protocol? Outpatient treatment? Prophylaxis regiment? The answer – again quite shockingly – is ZERO. Every major hospital and academic center has simply just went along with the NIH panel’s recommendations.
And no, that isn’t because they tried and just couldn’t come up with anything. How many medical conferences have been held where frontline doctors got together to share notes and compare clinical experiences, or where the world’s preeminent researchers and protocol designers swapped theoretical possibilities to study? Zero. Is there even an official online platform or portal in either the government or in academia where doctors and clinicians can network in the aforementioned manner? Nope.
So they never bothered to even take the most basic and rudimentary steps to try and develop any treatment protocols for covid.
We’ll get to the censorship and crusading against any dissenters later, but let’s state for now that the medical community literally censoring dissent within their own ranks is also indicative of a lack of independent or critical thinking by the establishment medical community.
In Short: The medical establishment’s members do not think critically or independently of the medical organizations and government agencies; this means that firstly the doctors/medical professionals not in positions of significant authority are not exercising any personal judgement, and second, that the few people in charge of the medical community are not engaging in the sort of rigorous debate that is the basic diligence for scientific analysis as they simply never face any dissenting views when making decisions.
9. The medical community failed to convey basic risk stratification
One of the most basic if not the most foundational axioms in Public Health is to figure out who, and to what degree, is at risk.
So first off, the med community failed to notice the severe age and comorbidity stratification of covid risk. This was obvious immediately as covid set in from the earliest analysis of covid deaths in Italy and from the Diamond Princess cruise ship, to pick 2 prominent examples.
They subsequently compounded this indefensible negligence by failing to communicate this to the public when the medical literature, and more importantly worldwide clinical experience, decisively proved this to be the case.
In order for an individual to make personal health decisions regarding covid, they obviously need to know what the risks and benefits are for them specifically from covid. The failure of the medical community to communicate the most basic risk breakdowns is flat-out dishonest manipulation with the aim to deceive the people into believing that they were at substantially higher risk than they actually were (and they largely succeeded too, as polling showed that in the US for instance on average respondents thought that already midway through 2020 9% of the US population had died from covid, and younger people perceived their personal risk from covid as 1000x (or more) than what it was in reality). That their intent was (allegedly) to prevent covid transmission is not a justification whatsoever; indeed, such arguments are ubiquitous amongst aspiring dictators looking for a superficial façade to grant themselves unlimited emergency powers.
The medical community has even admitted outright to lying to the public. The media (eventually) asked Fauci to explain his original stance advising against public masking in light of his current position that facemasks were the single most important and impactful public health measure in reducing covid transmission. That the media even asked such a question is a testament to the profoundly troubling and seemingly impossible contradiction between his flip-flopping from an unequivocal no on masks to masks being the most powerful policy tool in the arsenal. Completely nonplussed by what should have been a humbling recognition of the very real limits of human expertise, Fauci comfortably explained that he had lied in order to protect what were at that time scarce supplies of PPE for healthcare workers.
Fauci would subsequently go on to admit to moving the goalposts on what percentage of the population needed to be vaccinated in order to reach the critical threshold that would end the pandemic spread of covid based on his sense of the mood and sensibilities of the public.
The failure of the medical community to communicate even elementary risk stratification is also at its core base authoritarian paternalism, devoid of compassion or regard for people as individuals.
In Short: Public health officials and doctors are supposed to keep people apprised of the reality of what is going on so that they can make informed and rational personal health decisions, and also to prevent masses of people from seeking medical information from crackpots which inevitably occurs when the medical establishment is clearly not acting in good faith or honestly. That they deliberately failed to do so means that the medical establishment routinely lies to the public, and that it also has an unmistakably elitist & paternalistic culture that looks down derisively upon the ‘peasants’.
10. Public health officials used wrong information and spurious data to construct pandemic policies
The medical community literally used the wrong metrics, information, and data. Imagine if Fauci said that we’re locking down because of the astrological alignment of the North Star relative to the position of Saturn – the position of the North Star in the sky relative to Saturn has nothing whatsoever to do with the pandemic. Same idea here – the medical establishment relied on similarly irrelevant data or information to decide pandemic policy.
And the examples are legion. From models to death data, it was all garbage. Models, especially models written by known fraudulent quacks like Mr. Ferguson, do not provide any sort of reliable information; what they do provide is many ways to imagine a worst-case scenario playing out without a shred of evidence to back it up.
Then there are the various covid metrics. From cases to deaths and everything inbetween, all the metrics were defined so ineptly (and corruptly) that they were rendered meaningless (and numerous radical and novel assumptions were made without any evidence and contrary to all previous conventional medical wisdom and data). Covid deaths due to gunshots and alcohol poisoning. Covid hospitalizations from physical trauma. Covid cases of bits of viral debris or bits of random nucleotide junk amplified by asinine PCR parameters. Test positivity %’s that didn’t account for covid-recovering individual testing multiple times to test out of quarantine. Case counts that didn’t account for increased testing. And so on.
The flip side of this coin is the failure of any government or academic agency/institution – especially the CDC, whose primary raison d’etre is to conduct research on contagious diseases – to even attempt to curate high-quality and granular data on covid.
For instance, the CDC has still two years into the pandemic failed to conduct even once a random antibody seroprevalence sampling for the US. How can you hope to deal with a pandemic virus if you don’t know how many people were infected is a mystery to everyone (at least those of us who aren’t not in public health). This suggests that the CDC and the public health establishment have ulterior motives leading them to prefer ignorance over rigorous data (that might prove highly embarrassing to the medical community…).
(The CDC has also failed to perform even a single autopsy for any reported deaths tied to the vaccines, which suggests that the CDC similarly thinks that ignorance is indeed bliss regarding vaccine injuries and deaths.)
The failure to curate rigorously defined proper metrics was the wholesale rejection of science. Scientific inquiry and analysis requires accuracy and precision. The blasé nonchalant dismissal of proper metrics is a searing indictment that the medical establishment does not practice science as defined by the scientific method.
In Short: The medical community knowingly curated and used corrupted and irrelevant metrics and data to characterize the epidemiology of covid; this means that they ignored the scientific method.
11. The medical community never admitted that they made serious mistakes
The medical establishment, despite their innumerable ‘errors’ that were incredibly destructive to literally hundreds of millions of people across the world, has never admitted that they were wrong to have done what they did about anything. The only exception to this is that once their mistakes and missteps started becoming so obvious that it was impossible to deny them anymore, the medical establishments go-to explanation has been that “science is always evolving and we did the best we could do with the limited data we had”.
The notion that the medical community couldn’t or shouldn’t have done better than they did is sheer lunacy. And their failure to be able to admit that they have even the slightest degree of culpability in the societal devastation wreaked by their policies (more on that later) is, frankly, despicable.
In Short: The medical community refuses to admit that they made any substantial mistakes at any point; this means that they are at minimum detached from reality and unable to learn from past mistakes, ie that they will continue to make the same “mistakes” going forward, including regarding the vaccines. This also is indicative of a powerful “us-vs-them” mentality of the medical community, where they emotionally cannot tolerate the cognitive dissonance of admitting that they (“us”) were wrong and the ‘conspiracy theorists’ (“them”) were right.
12. The denial of natural immunity
The denial that natural immunity provides robust protection against not just reinfection but even from severe disease stands as one of the most blatant and illiterate contentions of the entire pandemic. Immunity following recovery from an infection or disease is as basic and standard Bio101 as it gets. It’s called the immune system.
Now, it is possible to have exceptions. But it is completely illogical and unprecedented to just assert the most radical hypothesis and adopt it as the default without any evidence whatsoever. Furthermore, as the pandemic wore on, the glaring lack of documented reinfection phenomena – anywhere in the world – surely proved the inadequacy of this nonsensical theory. If natural immunity didn’t work, then where were the second waves in nursing homes? They are the most vulnerable to covid, and have the weakest immune systems generally, so surely at least some nursing homes should have experienced subsequent outbreaks of reinfected residents?
Even more indicting, there was clinical evidence that immune specific cells were still circulating in individuals from the 1918 Spanish Flu. And there was also documented clinical evidence of robust SARS-CoV-1 immunity documented 17 years later. So why should SARS-CoV-2 be different with >80% shared genome with SARS1? What exactly was so “novel” about SARS-CoV-2 that the immune system was suddenly and obviously inadequate??
Furthermore, there were a number of studies that documented this thing called “cross-reactive immunity”, whereby immune specific cells acquired from infections mostly with other coronaviruses (that are responsible now for common colds) were able to help out with SARS-CoV-2. So let’s try a basic syllogism:
- Immunity from other coronaviruses demonstrated significant neutralizing activity against the other coronaviruses and even against covid.
- The immune system produces immune-specific cells against infection by SARS-CoV-2.
- The logical conclusion: Immune specific cells generated against covid are effective at neutralizing covid, consistent with historical observation and the fundamental tenets of immunology.
- The conclusion of the medical community: Immune specific cells generated against covid don’t work because they are inferior than less-specific immunity from other somewhat related coronaviruses.
I have no idea how the logic works according to the esteemed experts over at the CDC and NIH. I’m pretty sure that they don’t either.
At any rate, this anti-science flat-Earth “immunity-denier” stance by the medical community became even more egregious when the vaccines were rolled out. Now, they had to get us to believe that vaccines would induce reliable and robust immunity after they had spent months explaining how actually getting infected with covid did not.
So let’s go back to our syllogism test:
- Immune system exposure to the pathogen that causes covid does not result in the immune system developing strong and effective immune cells against the virus.
- Vaccines – which by design are mimicking infection so as to provoke the immune system to respond in a similar manner – will provoke an immune response as if an infection was happening.
- The logical conclusion: Assuming premise #1 is true, then the vaccines would be expected to not elicit robust or reliable immunity.
- The conclusion of the medical community: The immune response to the vaccine will be robust and reliable, even though the immune response to infection with the real thing is not, and even though there has never been a vaccine that elicited superior immunity to a pathogen than infection.
The only consistency in the logic of the medical community regarding immunity is that if we don’t make it, it’s bad, but if we make it, it’s amazing.
They had no way of knowing that vaccines would produce superior immunity, and certainly had no indication from prior science or from real clinical evidence (and in fact all of the available evidence had and has soundly and unambiguously contradicted them). All they had was this bizarre theory that we’re just going to assume that the immune response to the natural pathogen was of course going to be inadequate, and our designer vaccines will be better because they are producing antibodies to the spike protein which is of course superior, although we have no actual evidence for such a proposition.
There is actually much, much more to say regarding how insane and anti-science the natural immunity denialism by the medical establishment was (and still is), but this should suffice to illustrate the delusional quackery of this position.
In Short: The medical community denied the obvious reality of natural immunity from the beginning without any basis despite this being one of the most radical and wacky theories ever conjured up in the history of the scientific method; and then they did a partial about-face when it came to the vaccines, despite the inescapable contradiction between the two positions; this means that the medical community has been so conditioned to follow anything that is said by the medical “authorities” that they resemble a religious cult more than scientists. It also means that there is no limit to what they will be willing to cast aside of science that was previously held as a foundational truth.
13. Censorship and Fraud
Censorship is a weapon employed by authoritarians to hold onto their power – a mafioso intellectual thuggery that remains the last refuge of charlatans cornered by the truth.
I’m putting censorship and fraud together because censorship in science is by definition fraud — the process of scientific inquiry is to debate different hypotheses and test various options; if some are censored, then the scientific inquiry is being conducted fraudulently.
So… who remembers the original letter to Nature that became the justification to portray the “lab leak hypothesis” as a lunatic conspiracy theory? And let’s not forget the Great HCQ Fraud Paper (What is… Surgisphere?) that got published in The Lancet, which was the catalyst for government agencies and medical organizations around the world to suspend HCQ even from ongoing active trials. The paper whose data was entirely fabricated out of thin air. And it was far from the only corrupt fraudulent paper published.
Then there is the newest fad in academic medicine: Retractions. Papers threatening the establishment narrative or “facts” that somehow elide the censors and pass peer review are suddenly without any warning yanked by journals, something that is unprecedented in modern academia. Daniel Horowitz wrote a great article documenting this phenomenon: Retraction serves as the new academic censorship.
And lets not forget the now-infamous Ouchy-Fauci emails that were openly plotting in plain English to “takedown” the Great Barrington Declaration & the universally acclaimed preeminent epidemiologists who authored it. If trying to depict world-renowned expert epidemiologists as fringe in order to disabuse the public of their considered expert opinion isn’t censorship, I don’t know what is.
And then there is the entire regime of threatening to yank the license, and even possibly investigate criminally, any medical professional who is judged to be guilty of spreading “covid disinformation”. Literally straight out of the Soviet playbook.
So although Big Tech seems to get all the attention as censors, the medical community seem to be far better at it in some respects. After all, if the big medical journals keep out “unapproved” opinions, how will the majority of the medical community – the front-line doctors, nurses, etc who don’t do their own research but rely on their weekly emails from various medical societies or journals of that week’s “notable” developments – be able to stay abreast of actual developments and research? It is no wonder that the vast, vast majority of doctors are so illiterate and ignorant.
In Short: The medical community has engaged in a wholesale, all-out censorship regime in order to eliminate any dissenting facts, data, and expert opinions that challenge their preferred narrative; censorship always and everywhere is the attempt to hide the truth from public view.
14. They didn’t denounce useless and harmful practices derived from their policies and statements
If someone distorts your opinion egregiously in a way that makes it look insane, you would protest, especially regarding a national policy that affects >330 million people. In addition to making you look like a fool, such distortions will deter people from accepting your policies.
Yet, we were treated to all manner of theater of the absurd, such as wearing masks when alone in your car or outside, and even when taking a shower. My parents were recently on a packed flight whereupon the plane landing, the stewardess kindly reminded the passengers to please be mindful to socially distance while getting off the plane. Umm, what now??? Good luck with that.
Then there were the insane policies, like Governor Whitmer in Michigan banning people already in a store from purchasing “non-essential” items. She irrationally banned gardening at one point of Michigan’s lockdown, the scientific justification of which still remains unclear.
In some states, even driving by yourself was prohibited. So people who were literally going mad cooped up all day in their house who desperately needed to get out for a bit so they didn’t become one of the >25% of people who considered suicide by June 2020 were forbidden to do so. What could possibly justify such a draconian nonsense measure? This list is endless. (If you really want to get a sense of how crazy this all was, just look at the evolution of headlines over at The Babylon Bee from the lockdown months.)
Special emphasis is reserved for restaurant policies: wear your mask into the restaurant but take it off when you sit down only to put it back on when you walk to the bathroom??
To be fair, often enough, it wasn’t the people misinterpreting the scientific catechisms of the elite public health demigods — their policies or statements were frequently objectively incoherent.
Warning: you are entering the Twilight Zone
The initial “15 days to flatten the curve” underwent numerous evolutions to finally reach the status of indefinite emergency without any defined objective or stopping conditions; it has given rise to a host of devastating memes capturing the sheer lunacy, mendacity, hypocrisy and tyranny of the rapidly changing policies.
Masks were initially (and accurately) explained to be not only useless for reducing the community transmission of covid, but likely to be counterproductive as well in the hands of untrained laypeople who would handle them very unsanitarily. But the science made a radical turnabout after a few months, when we were then informed that masks were the single most critical measure in reducing covid transmission. This kabuki theater reached a climax with then-CDC director Robert Redfield picking up his mask, putting it down, holding it up, and then declaring that it provides more protection than a vaccine would (!?!) – all of this during a nationally televised hearing in front of a senate committee. This stood as the most illiterate statement of any prominent public health official over the course of the pandemic until the covid vaccine rollout. Mask mandates were reimposed in numerous jurisdictions following the obvious failure of the vaccines to mitigate covid transmission from the vaccinated. So in hindsight, Dr. Redfield was not really that off base.
The IHME models routinely failed to accurately predict the covid metrics for the day the model was released. These divorced-from-reality IHME models also predicted the imminent overwhelming of hospital capacity in numerous states, which was the catalyst that convinced governors in a few states to infamously compel nursing homes to accept positive covid patients back from hospitals – in order to clear space for the expected tsunami of critically ill covid patients. Besides the obvious stupidity of starting cascades of nursing home outbreaks that would produce many extra and unnecessary severe covid cases that would require hospitalization, why would anyone listen to the doomsday predictions of an algorithm so inept that it couldn’t even accurately capture the metrics that already existed, let alone predict future numbers? This is the equivalent of watching the local weather forecaster saying that there is a thunder storm right now and tomorrow there will be a hurricane as you’re relaxing on the beach under an umbrella to protect you from the sun.
Where did 6 feet come from? Nobody knows really, but the one place it definitely didn’t come from was a scientific publication or study. What difference does it make if we’re standing 6 feet apart or 1 foot apart in an indoor room, and the aerosols carrying the live covid virions could hang in the air for literally days and sometimes weeks? Also unclear, but distancing definitely made people feel better.
What was the minimum age that wearing a mask is safe? That depended on which agency you consulted. The CDC was by far the most optimistic, declaring that masking 2-year-old kids was perfectly ok. The WHO took a far more cautious approach, asserting that masks should categorically not be worn by anyone under the age of 5, and that children under the age of 12 should only wear masks if absolutely necessary and under the supervision of a competent adult. Various European countries fell all over the map in between, in a haphazard manner that resembled a Wonder-8 ball more than science. Although science itself had by then become virtually indistinguishable from shaking a Wonder-8 ball.
Speaking of competent adults, I am fairly confident that no one except perhaps for the teachers union representatives would consider the average public school teacher in Chicago or NYC to be “competent” in the way the WHO’s guidance had in mind.
And for anyone who was wondering what the actual efficacy of masks was, that mostly depended on who was interviewing Fauci that day. To be honest though, Fauci had a tendency not to provide numbers all that much, which left a confused and vexed population to parse the adjectives Fauci used to try and decipher the degree of efficacy of mask wearing for any particular day. For instance, “confers a high degree of protection” meant more efficacy than “it’s better than nothing”. Precisely where “it is undeniable that wearing a mask helps” fell on this scale was left to the individual cable news viewers to figure out for themselves.
Some policies even confounded justices on the Supreme Court, some of whom struggled to grasp for instance why casinos were not a significant covid risk operating at 50% capacity but churches were virtually guaranteed super-spreaders even at a mere 10%.
And who can forget the profound mysteries of viral kinetics that confounded the best and brightest scientists, who were never quite able to explain the precise scientific rationale by which 10-person outdoor funerals were unacceptably risky but 27 million screaming protesters were perfectly safe.
Did anyone once ever hear Fauci call out these excesses? And not just Fauci, but anyone and everyone who was prominent or influential. It’s almost as though they wanted the most draconian, incoherent measures. As every good tyrant and cult leader knows, forced irrationality conditions people to blind, unquestioning obedience.
In Short: The medical community never called out any of the innumerable excesses that were the result of authorities and individuals misinterpreting their policies and statements. This means that they were not perturbed by the obvious unwarranted and false conclusions being assumed by many local policymakers or regular people evident from their own policies, statements or actions.
15. The medical establishment is riddled with massive financial conflicts of interest
The financial conflicts are everywhere. The vast majority of the establishment gets significant money from either the government, a hospital institution, a billionaire-funded non-profit, or Pharma – all of whom will stop the flow of finance the instant the recipient steps out of line. There is an incestuous merry-go-round of high-profile FDA regulators joining Pharma board members. Etc.
In Short: There is an otherworldly degree of financial inducements and pressures on the vast majority of medical professionals and anyone else caught up in the orbit of the mainstream medical institutions to toe the official narrative, or else; this means that they are compromised – and certainly not trustworthy – to think independently, much less to openly defy the establishment.
16. Every specific claim made regarding the vaccines so far has ultimately proven to be false
Here are just a few of the many specific claims made about the vaccines by the medical community that have since been resoundingly debunked:
- The injected serum of the vaccine will stay in the area of the injection site
- The spike proteins will remain tethered to the cell membrane and won’t escape into circulation
- The spike protein is not biologically active
- The spike protein has no significant toxicities
- No corners were cut in the development or trials of the vaccines
- There were no life-altering SAE’s in the Pfizer kids trial
- The lipid nanoparticles are safe and won’t circulate all over the anatomy
- The vaccines confer superior immunity to natural infection
- The vaccines prevent infection & transmission
- There are no serious side effects associated with the vaccines
- there is no plausible mechanism or basis by which the vaccines can affect fertility
- reports of menstrual irregularities are exaggerated and fake
- VAERS reports are mostly submitted by random people who are simply assuming without any basis that a random adverse event that happened after vaccination is related to the vaccine
- The CDC investigated all of the VAERS reports of death and determined that none were attributable to the vaccine
- There is no need for long term observation to determine that there are no serious long term effects
- 99% of the hospitalizations for covid are unvaccinated patients
- There is no basis for a causal link between myocarditis and the vaccines
- Myocarditis is an exceedingly rare complication from the vaccines, and everyone is more likely to get myocarditis from covid than from the vaccines
In Short: Every specific thing they said about the vaccines that can be adjudicated so far has turned out to be demonstrably false. Why would anyone trust someone on a topic where everything they say is wrong?
17. A significant % of the medical community are genuinely evil people
In numerous cases around the country, hospitals have refused giving deathly ill covid patients Ivermectin, preferring to see them die rather than recover.
A very simple question: What possible reason could hospitals have to go to court to fight patients they themselves had already given up on, and for whom they had no more treatment options, in order to prevent even outside doctors from prescribing a medication that is safer than Tylenol? And even if you can somehow come up with some sort of justification for the first time, once there were a few of these cases on record, surely there is no rational moral basis for not trying Ivermectin on every patient, let alone fighting in court to ensure that the precious few patients whose families have the temerity to demand Ivermectin should be denied lifesaving treatment??
Whistleblowers have revealed cruel treatment of patients in Covid wards – negligent treatment, letting patients starve to death, putting patients on ventilators unnecessarily and without critical safeguards in place resulting in numerous “covid” deaths, denying patients their vitamins and doctor prescribed medicines, etc.
Society trusted medical professionals due to its ethos of prizing saving life above all else. This is most certainly no longer the case regarding the medical community writ large. At a minimum, a medical community whose culture breeds such contempt for the value of a patient’s life that hospitals will fight in court to deny potentially lifesaving treatment that is essentially cost-free and without any legal liability is a medical profession that has lost all credibility that their overriding concern is saving lives and the welfare of their patients.
Within this context, let us turn to the war on covid treatments more generally.
As practically anyone reading this is undoubtedly aware, at the height of the HCQ political controversy, The Lancet – arguably the world’s top medical journal – published what was initially presented as the coup de grâce to kill HCQ’s viability: the aforementioned Surgisphere study. This study purported to have data from more than 90,000 patients from hospitals on all six inhabited continents showing not only that HCQ had no efficacy against covid, but additionally was toxic and raised the mortality of hospitalized covid patients.
To make a long story short, the entire study was quickly debunked as a massive fraud – literally the entire dataset they had was fabricated out of thin air. And it was obvious to anyone who was even a little bit familiar with the details of how such studies are conducted.
Which all begs the question: Why would the editors and scientists at The Lancet be willing to publish a colossal fraud??
The only rational conclusion from this affair is that they had an overwhelming desire to kill HCQ and debunk it, that was powerful enough to get the editors at the world’s most prestigious medical journal to forever tarnish their reputation by publishing an obvious and wholesale fraud on the most controversial political issue at the time — there wasn’t even a snowball’s chance in a volcano that the fraud wouldn’t be easily spotted and debunked.
Why would they oppose a cheap, safe and widely available drug that could significantly mitigate covid disease??
Why would they quash a potentially effective drug that might save millions of lives if deployed widely, but might result in millions of deaths if denied??
And the medical community has continued to prosecute an organized and systematic war on every cheap and effective covid treatment that is being successfully used by thousands of heroic doctors around the US and around the world.
The FDA even went so far as to publicly tweet out that Ivermectin – pound for pound the most effective covid treatment widely available – was a “horse-dewormer” and potentially very dangerous. This was despite the fact that the discovery of Ivermectin won a Nobel prize in 2015 and is one of the safest drugs ever made, having been dispensed over 4 Billion times over the past few decades without any known toxicities.
There’s one more dimension to point out regarding the genuine evil within a large segment of the medical community: the absolute devastation caused by the covid policies.
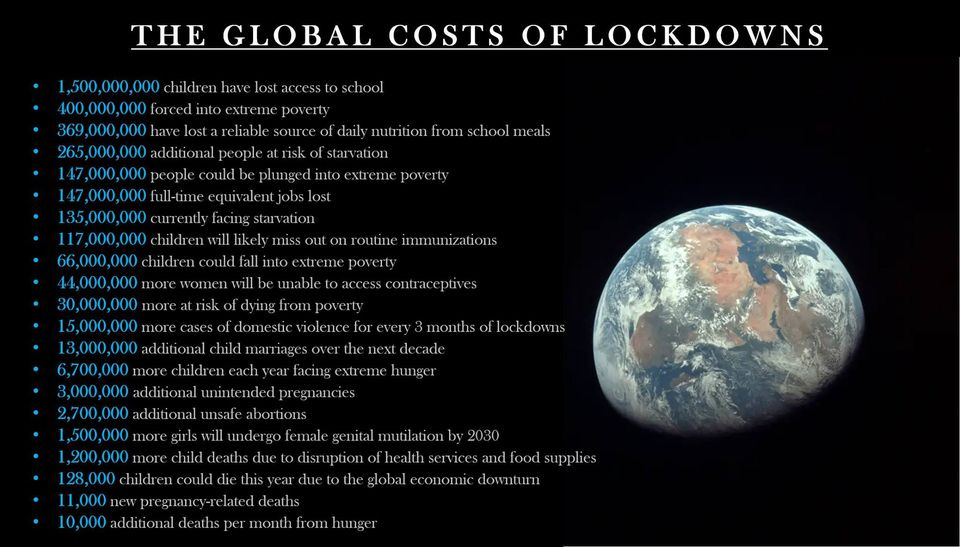
Rational Ground has a partial list of lockdown harms (with supporting documentation) that is simply way too long to reproduce here, but it conveys a sense of the scope and destruction inflicted by public health officials worldwide.
Very disturbingly, children bore the brunt of the societally calamitous covid policies. Perhaps the most enduring symbol of the pandemic will ultimately be the useless and abusive masking of children. The institutionalization of child abuse through forced masking in schools, lockdowns, quarantines, the inhuman deprivation of sociality — these are unforgivable sins. And these are all policies that were suggested and implemented by the medical community, who were the driving force behind this unequivocal abomination.
Realize that prior to covid, if a teacher would have disciplined an impossibly unruly and disruptive student by forcing the student to wear a surgical facemask, the teacher would quickly find him/herself under criminal indictment for child abuse. Somehow, though, masking children as young as two (!?!) has become the norm.
For some perspective: Sweden never closed their schools, had no mask policies, and didn’t have a test-and-quarantine regiment. Not one child died from covid and teachers in Sweden tested positive for covid at a slightly lower rate than the occupational average for jobs with a similar covid risk profile.
In Short: A significant portion of the medical community are genuinely evil people responsible for the deaths and suffering of hundreds of millions. The culture of the medical community is sufficiently rotten to the core to not only allow for the ascendance of such evil people to positions of influence and authority, but also celebrate them. Such evil should not be tolerated, nor regarded as an authoritative source for any matter.
Conclusion
There is so much more to say on every issue raised here, but the need for brevity restrains how much can be included.
In summation, with the advent of the covid vaccines we were assured – promised, really – that the mRNA vaccines were truly a once-in-a-generation medical miracle akin to the discovery of penicillin or hand hygiene by physicians.
We were promised. But that’s all we ever had: the guarantee of the medical community. They still won’t let us have meaningful access to the real data or science behind the vaccines. We still don’t have:
- the raw data from any of the vaccine trials
- any reports from government agencies tasked with vaccine safety monitoring providing details of how they have so far adjudicated the existing pharmacovigilance data such as VAERS
- any reports from government agencies tasked with vaccine safety monitoring providing details of the manufacturing and production infrastructure and how it has fared so far
- the methodology by which the CDC/FDA/NIH (allegedly) adjudicates potential causality of reported vaccine injuries
- access to internal FDA communications regarding their adjudication of the trial data for any of the approved vaccines
- access to the military data – probably the dataset that most readily can establish causality per the Bradford-Hill criteria and per common sense – but we have a few whistleblowers alleging that the data has been corruptly altered to expunge reports of vaccine injuries
- access to the internal developmental animal studies/experiments conducted by the vaccine companies that are not subject to disclosure requirements by the FDA, but that are typically used by the Pharma manufacturers to characterize their own products for themselves so that they understand exactly how they work and what might happen in real life so that they can figure out in advance how to design trials, depict the product/drug in media, and so on.
- access to any reports regarding the manufacturing processes used to create billions of vaccine doses, especially in so short a window – manufacturing capacity was scaled up from zero to billions practically overnight by industry standards, without the typical extensive development of manufacturing capacity that includes myriad levels of reviews and testing to ensure that the manufacturing process is consistent and free of any impurities
- access to the copious data filed with the FDA by the vaccine manufacturers that the FDA used to adjudicate awarding the EUA’s, and which the FDA is now lying – yes, openly lying – in court to avoid surrendering the data to a FOIA request. This after the FDA’s initial request for a release timeline that would require 75 years for the full release of the requested documents was rebuffed by the judge in a glimmer of judicial sanity.
All we have to rely on is their word.
After all that has transpired, can it be at all rational to trust them?
Germany prepares to extend the legal basis for containment indefinitely
Long Lauterbach

Health minister Karl Lauterbach caught maskless on a train
eugyppius | March 5, 2022
On 20 March, in just fifteen days, Germany’s Infection Protection Act expires. If nobody does anything, the whole legislative basis of containment will simply disappear. That is how easy a freedom day could be in Germany, and with the entire attention of the press on Ukraine, you’d think nothing could be simpler than letting that happen. Alas, Karl Lauterbach is our health minister, and we have the worst government since the war. On 16 February, we learned that the plan was to replace the Infection Protection Act and its “more intrusive protections” with “simple, basic protection measures to contain infections and protect at-risk groups.”
Today, in a very bad interview with the Westdeutsche Allgemeine Zeitung, Lauterbach finally explains what he hopes that these “simple, basic protection measures” will amount to. They are anything but simple or basic:
German states must have the capacity to react early to future waves. This includes mask mandates and contact restrictions. It should be possible to set limits on the size of private meetings and public events, as well as access rules for restaurants, for example [vaccination and testing requirements.]
To this end, we must still have the capacity to implement testing requirements for businesses and public spaces. All these instruments should only be used if they are actually necessary. The state parliaments would then have to determine this.
All of this will remain necessary for a very long time. Lauterbach counts on a summer wave, and a fall wave after that. In fact, he envisions just wave after wave, forever:
Corona will occupy us for a long time, a decade or more. HIV appeared 40 years ago, and it’s still there. We’ll always have to deal with Corona variants, perhaps also dangerous variants. There will also always be outbreaks. That’s what you call the endemic phase. And there will always be a group of people, who are not adequately vaccinated, whose vaccine protection is waning, and for whom the vaccine protection is insufficient, because of weak immune systems.
Always new little problems for the new little Lauterbachs of our government to solve.
This new law will be pushed through parliament with as little discussion as possible. Olaf Scholz’s coalition is supposed to present draft legislation to a parliamentary subcommittee by 16 March. A full vote is then planned for the 18th, preceded by a mere 70 minutes of debate. Two years ago, when the law was first passed, things went much the same way; it was all so urgent, you see. Now the reasons are of course much different. The last thing any member of parliament wants to be, is on the record supporting these indefensible rules and the continued destruction of German society. So the most minute aspects of our everyday will continue to be regulated in relative silence, by unreasonable people, for unattainable ends.
As attention wanders from Corona and the virus becomes less dangerous, other countries have found it convenient to end restrictions. Germany, thanks to Lauterbach, will choose a different path. He’s an unbalanced man of limited mental capacity, who ended up in the cabinet because nobody else wanted to touch the health minister position. For him, a spotlight on Ukraine is an opportunity not to fold up the tables and go away, but to pour more poison into the law. Corona will never end in Germany as long as this man is health minister, because the virus is a very large part of who he is. Before March 2020, Lauterbach was a nobody, but ceaseless freaking out about SARS-2 has turned him into one of Germany’s most prominent politicians.
As long as Lauterbach is allowed to preserve the legal basis for containment, pressure will build on state governments to impose closures every time there is a new Corona headline. Every new variant, every infection spike, every rise in hospitalisations or deaths, will see renewed calls to bring out more masks, more vaccines, more tests, more capacity limits, and more closures. These measures don’t even have to be implemented to do their damage; the mere possibility disrupts business models and future plans. The longer these restrictions hang over us, the more deeply they change every aspect of our social and political existence, from music concerts to Oktoberfest to restaurants to schooling to public transit.
Almost as enraging as the continuation of the containment regime, are the near-total absence of good arguments for it. Future variants won’t matter as much as Lauterbach pretends, because almost all Germans have antibodies of one kind or another. A wealth of respiratory viruses, including many varieties of influenza, surge seasonally every year. Many of them are no more dangerous than SARS-2 is right now, and none of them ever inspired any restrictions. The regulatory regime that Lauterbach hopes to continue has become a bizarre superstition, something approaching a collection of religious observances. They are increasingly removed from any stated goals, from any basis in evidence at all, and even from the expectation that they might do anything. It’s just a habit now, stuff we have to do whenever cases rise, because rising cases mean we have to do this stuff.
If we can’t end this now, we may not be able to end it for years or even decades. That seems at least as great a threat, as events in Ukraine.
Most Kids Are Already Naturally Immune to COVID. So Why Are We Vaccinating Them?
The Defender | March 1, 2022
The “majority” of children in the U.S. have already been infected with COVID-19, The Washington Post today reported, after reviewing data from the Centers for Disease Control and Prevention (CDC).
The Post’s report begs the question: If so many kids have natural immunity to the virus, and, as reported Monday, the vaccines aren’t very effective in children 5 to 11 years old, why are public health officials, schools, businesses and others pushing to vaccinate kids?

Source: Centers for Disease Control and Prevention
During a security conference in Munich on Feb. 18, Bill Gates said:
“Sadly, the virus itself, particularly the variant called Omicron, is [a] type of vaccine — that is, it creates both B cell and T cell immunity — and it’s done a better job of getting out to the world population than we have with vaccines.”
Did Gates actually admit natural immunity to Omicron is succeeding where vaccines have failed — and that he’s “sad” about that?
Gates isn’t the only one talking about natural immunity these days.
Eric Topol, executive vice president of Scripps Research last month argued for including an option of natural immunity in the definition of “fully vaccinated.”
Even vaccine advocate Dr. Paul Offit, director of the Vaccine Education Center and member of the U.S. Food and Drug Administration’s vaccine advisory committee, is going to bat for recognizing natural immunity to COVID.
During a Jan. 25 interview, Offit described a meeting with Dr. Francis Collins, then-director of the National Institutes of Health, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, Dr. Rochelle Walensky, director of the Centers for Disease Control and Prevention (CDC) and U.S. Surgeon General Dr. Vivek Murthy where Offit was asked, along with three others, whether he thought natural immunity should count as a vaccine.
Offit and one other person said yes, natural immunity should count. But they were out-voted, leading U.S. health officials to decide natural immunity should not be recognized in the U.S, as an alternative to a vaccine mandate.
To this day, the CDC maintains this position in its official guidance for the public — despite the agency’s own studies showing natural immunity against COVID is superior to the immunity provided by COVID vaccines.
Some U.S. lawmakers think the CDC is wrong, as evidenced by the introduction of two the Natural Immunity Is Real Act in the Senate (S.2846) and the House (H.R. 5590).
The bills would require “all federal agencies to acknowledge and consider natural immunity to COVID-19 when promulgating any regulation related to the COVID-19 public health emergency.
But for now, in the U.S. at least, those states, businesses and schools requiring “proof of COVID vaccination” make no exceptions for people — including kids — who recovered from COVID, and therefore have natural immunity.
UK data show most unvaccinated kids already have natural immunity
Unfortunately, the CDC doesn’t provide up-to-date seroprevalence data for children in the U.S., but UK data may shed light on children and natural immunity.
The UK Office of National Statistics (ONS) early last month reported these data based on population sampling:
“In the week beginning 10 January 2022, the percentage who would have tested positive for antibodies against SARS-CoV-2 ranged from 90.2% to 93.3% for children aged 12 to 15 years and from 63.3% to 72.7% for those aged 8 to 11 years across the UK. Estimates show the percentage of children testing positive for antibodies against SARS-CoV-2 at or above 42 ng/ml.”
In the UK, vaccines have not yet been made available for the under 12 age group (except those who are at very high risk). The 63.3 to 72.7% is thus overwhelmingly due to natural immunity and not vaccination.
Also, as noted by the ONS, individuals testing below the threshold level may also have natural immunity, presumably in the form of T cells and B cells, where the antibodies have waned. Thus these data may be underestimates of the true population-level immunity.
The UK government had previously reported:
“It is estimated that over 85% of all children aged 5 to 11 will have had prior SARS-CoV-2 infection by the end of January 2022 with roughly half of these infections due to the Omicron variant. Natural immunity arising from prior infection will contribute towards protection against future infection and severe disease.”
The UK’s Joint Committee on Vaccination and Immunisation (JCVI) on Dec. 22, 2021, authorized the vaccine only for high-risk children ages 5 to 11.
Yet despite the encouraging data on natural immunity in this age group, the JCVI on Feb. 16, in updated guidance, expanded its recommendations to include a “non-urgent offer” of the vaccine to children who are not in a clinical risk group.
To be clear, the UK government authorized an mRNA vaccine for the original SARS-CoV-2 strain, to be made available in April, to a group of 5 million young healthy children — 85% or more of whom are expected to have natural immunity.
As John Campbell, Ph.D., said, if and when a future COVID wave ever comes, any possible beneficial effect from these shots will likely have waned.
Studies may explain why children are protected from SARS-COV2
A study in 2020 reported that cross cellular immunity and immunomodulation from previous existing childhood vaccines may provide protection against COVID infections.
A more recent study of children as young as 3 years old measured spike-specific T cell responses and found they were twice as high as those in adults. The authors suggested this is in part due to pre-existing cross-reactive responses to seasonal coronaviruses.
A January 2022 study demonstrated a protective effect from high levels of pre-existing immune cells generated by other coronaviruses like the common cold, which attack the proteins within the virus (nucleocapsid), rather than the spike protein on the virus.
According to the senior author of the study:
“The spike protein is under intense immune pressure from vaccine-induced antibodies which drives evolution of vaccine escape mutants. In contrast, the internal proteins targeted by the protective T cells we identified mutate much less.
“Consequently, they are highly conserved between the various SARS-CoV-2 variants, including omicron. This suggests that the existing cross-reactive T cells may provide better protection than an mRNA vaccine that focuses only on the original variant spike protein.”
Despite these studies, the latest data on how many children likely have immunity because they’ve recovered from COVID and the well-established scientific theory that natural immunity to a pathogen is superior to vaccine-induced immunity, places like New York City continue to demand proof of vaccination for all children age 5 and over in order for them to participate in extracurricular school activities, visit museums, zoos, theaters, gyms, and restaurants.
For the most comprehensive list of 150 research articles on natural immunity visit the Brownstone Institute.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Russia Prevents Washington from Unleashing Biological Warfare

By Vladimir Platov – New Eastern Outlook – 03.03.2022
In view of the unrest that US intelligence services have been actively initiating lately, whether in Central Asia, Transcaucasia or other areas bordering Russia and China, the risk of a biological disaster from multiple secret military biological laboratories deployed by the US in potentially politically and socially unstable regions is objectively increasing. In this regard, the issue of the US preparing a biological time bomb in Kazakhstan has been raised many times before. The growing risk of the Pentagon initiating biological warfare using over 400 US biological laboratories located overseas around the world and the need for a clear response to the risk of worldwide biological disaster from such secret US overseas facilities has been repeatedly pointed out. After all, these biological laboratories employ some 13,000 “employees” who are busy creating strains of killer pathogens (microbes and viruses) that are resistant to vaccines.
It is no secret nowadays that the US has set up such biological laboratories in 25 countries around the world: in the Middle East, Africa, South-East Asia. Only within the former Soviet Union there are US military biological laboratories in Ukraine, Azerbaijan, Armenia, Georgia, Kazakhstan, Kyrgyzstan, Moldova and Uzbekistan.
The Americans try to deny the military nature of the studies conducted in such laboratories. However, the secrecy that surrounds them is only comparable to that of the most important military facilities. There is no accountability to the local and global public about the “work” being done there. Moreover, no scientific “achievements” have been publicly demonstrated by American biologists over the many years of the existence of such foreign secret laboratories, and the results of their research are not published anywhere in the public domain.
Meanwhile, laboratories are actively collecting information on the gene pool of the populations of countries where such laboratories operate. All this indicates that the Pentagon is undoubtedly preparing to wage a biological war using biological weapons, which the US is building in such biological laboratories. It is well known that the US has already spent over $100bn in recent years developing biological warfare weapons. The US is the only country that still blocks the establishment of a verification mechanism under the 1972 Convention on the Prohibition of the Development, Production and Stockpiling of Bacteriological (Biological) and Toxin Weapons and on their Destruction.
However, like Russia’s demands to the West for a clear agreement on universal security measures and on the non-proliferation of NATO to the east, warnings about US readiness to unleash a global biological war have never been heeded in Washington and Western capitals.
With this in mind, one can hardly deny that Russia, like any other country, does not wish to have such weapons near its borders, thus jeopardizing the security of all.
Therefore, in Moscow’s military operation to denazify and demilitarize Ukraine in recent days, getting rid of the numerous US military biological laboratories on the territory of that country is an important point.
On February 24, the British conservative publication THE EXPOSÉ published an article entitled “Is there more to the Ukraine/Russia conflict than meets the eye?” It recognizes that Russia should have conducted the current military operation on the basis of its security interests and confirms that there has long been a very serious threat to the lives and health of the Russian Federation population from the territory of Ukraine. It refers to at least 16 US military biological laboratories located in Odessa, Vinnitsa, Uzhgorod, Lviv (three), Kharkiv, Kiev (also three), Kherson, Ternopil, Dnepropetrovsk, as well as near Luhansk and the border with Crimea. Such “cooperation” between the Pentagon and the Ukrainian Ministry of Health dates back to 2005. Opposition parties managed to push through the Verkhovna Rada in 2013 to end this “cooperation”, but the US-led coup d’état in Kiev in February 2014 prevented the implementation of this decision, resulting in this “cooperation” not only continuing but also actively developing at the initiative of Washington.
Many of the Pentagon’s and White House’s official secrets about US clandestine biological laboratories overseas have been revealed by Francis Boyle, professor of international law at the University of Illinois at Champaign (USA) and author of the Biological Weapons Anti-Terrorism Act of 1989 (BWATA). As this American scientist points out, “We now have an Offensive Biological Weapons industry in this country that violates the Biological Weapons Convention and my Biological Weapons Anti-Terrorism Act of 1989”. According to Boyle, “American universities have a long history of willingly permitting their research agenda …. to be co-opted, corrupted, and perverted by the the Pentagon and the C.I.A. into death science”. He cites as an example the group of Dr. Yoshihiro Kawaoka of the University of Wisconsin, which managed to increase the toxicity of the flu virus by a factor of 200. According to Boyle, the Pentagon and the CIA are “ready, willing and able to launch biowarfare when it suits their interests… They have a stockpile of that super-weapons-grade anthrax that they already used against us in October 2001”.
The threat to people living even at a distance from such laboratories is evidenced by an investigation conducted by USA Today newspaper, which showed that from 2006 to 2013 alone, more than 1,500 accidents and safety violations occurred in 200 military biological laboratories on the territory of the US. So what about possible similar incidents in biological laboratories in Ukraine or other former Soviet republics?
In the summer of 2019, “America’s main biological warfare lab has been ordered to stop all research into the deadliest viruses and pathogens over fears contaminated waste could leak out of the facility,” reported Britain’s The Independent. The Centers for Disease Control and Prevention (CDC), the public health authority in the US, has revoked the military bioresearch center at Fort Detrick’s license to handle Ebola, smallpox and anthrax after CDC inspectors found “problems with the procedures used to decontaminate wastewater” at Fort Detrick. In this regard, it is notable that the possibility of “deadly viruses and pathogens” leaking into Fort Detrick’s wastewater was detected shortly before the COVID-19 outbreak, which the Americans were quick to blame on China. It is also noteworthy that the Pentagon has significantly stepped up the activities of its overseas biological laboratories since 2019, clearly shifting the “work” on particularly dangerous strains and biological weapons development there.
In these circumstances, the task of terminating the activities of the US secret biological laboratories as part of the demilitarization of that country is justified in the program of Moscow’s military operation in Ukraine.
Against this background, it is noteworthy that the US embassy in Ukraine removed all documents about the biological laboratories in Kiev and Odessa from its official website after Moscow launched its military operation. This further confirms that in addition to the nuclear threat from Zelensky, Russia was also being prepared for bio-extinction behind the ocean. Under these circumstances, the announcement by the US Defense Threat Reduction Agency (DTRA) on the US government procurement website last October of an addendum on “combating highly dangerous pathogens” is understandable. This document concerned the $3.6mln finishing work to launch two biological laboratories in Ukraine – in Kiev and Odessa, where machinery, equipment and personnel were already being prepared for the United States to unleash a biological war under the cover of Ukraine.
Public Health Erred on the Side of Catastrophe
In a coercive mass experiment, governments opened a Pandora’s box of harms
By Brian McGlinchey | February 21, 2022
Throughout the Covid-19 pandemic, proponents of lockdowns, shelter-in-place orders, mask mandates and other coercive government interventions have characterized these measures as benevolently “erring on the side of caution.”
Now, as the grim toll of those public health measures comes into ever-sharper focus, it’s increasingly clear those characterizations were terribly wrong.
What’s less readily apparent, however, is how the very use of the “erring on the side of caution” framing was injurious in itself—by thwarting reasoned debate of public health policies, diverting attention from unintended consequences, and buffering the Covid regime’s architects from accountability.
To understand how the misuse of “erring on the side of caution” performed a sort of mass hypnosis that coaxed populations into two years of submission to disastrous, overreaching policies, consider how the expression is typically used.
In everyday life, one might err on the side of caution by:
- Leaving for the airport an extra 30 minutes early
- Carrying an umbrella when there’s a 25% chance of rain
- Opting for a less-challenging ski slope
- Going back into the house to make sure the iron is unplugged
- Getting a second medical opinion
Generally speaking, “erring on the side of caution” in everyday life means lowering risk with a precaution that has a negligible cost.
When mandate proponents portrayed their edicts as “erring on the side of caution,” it had the effect of tacitly assuring the public—and themselves—that there’d be little or no harm associated with extreme measures like:
- Shutting down businesses for months at a time
- Knowingly forcing millions of people into unemployment
- Halting in-person attendance at schools and colleges
- Ordering people of all ages and risk profiles to wear masks
- Denying people opportunities to socialize, recreate and enjoy living
That implicit low-downside assurance not only fostered unthinking support for draconian measures among citizens and experts alike, it also cultivated an atmosphere of intolerance toward those who questioned the wisdom of these interventions and predicted the great many harms that have resulted.
“Overconfident, unnuanced messaging conditioned us to assume that all dissenting opinions are misinformation rather than reflections of good faith disagreement or differing priorities,” write Rutgers professors Jacob Hale Russell and Dennis Patterson in their essay, The Mask Debacle. “In doing so, elites drove out scientific research that might have separated valuable interventions from the less valuable.”
Of course, in addition to its implicit assurance that a risk-reduction measure comes at little cost, “erring on the side of caution” conveys an assumption that the precaution will actually be effective.
That hasn’t been the case with Covid mandates. Though many continue embracing the illusion of government control over Covid, the contrary studies and real-world observations are stacking far too high to be denied any longer by the intellectually honest among us.
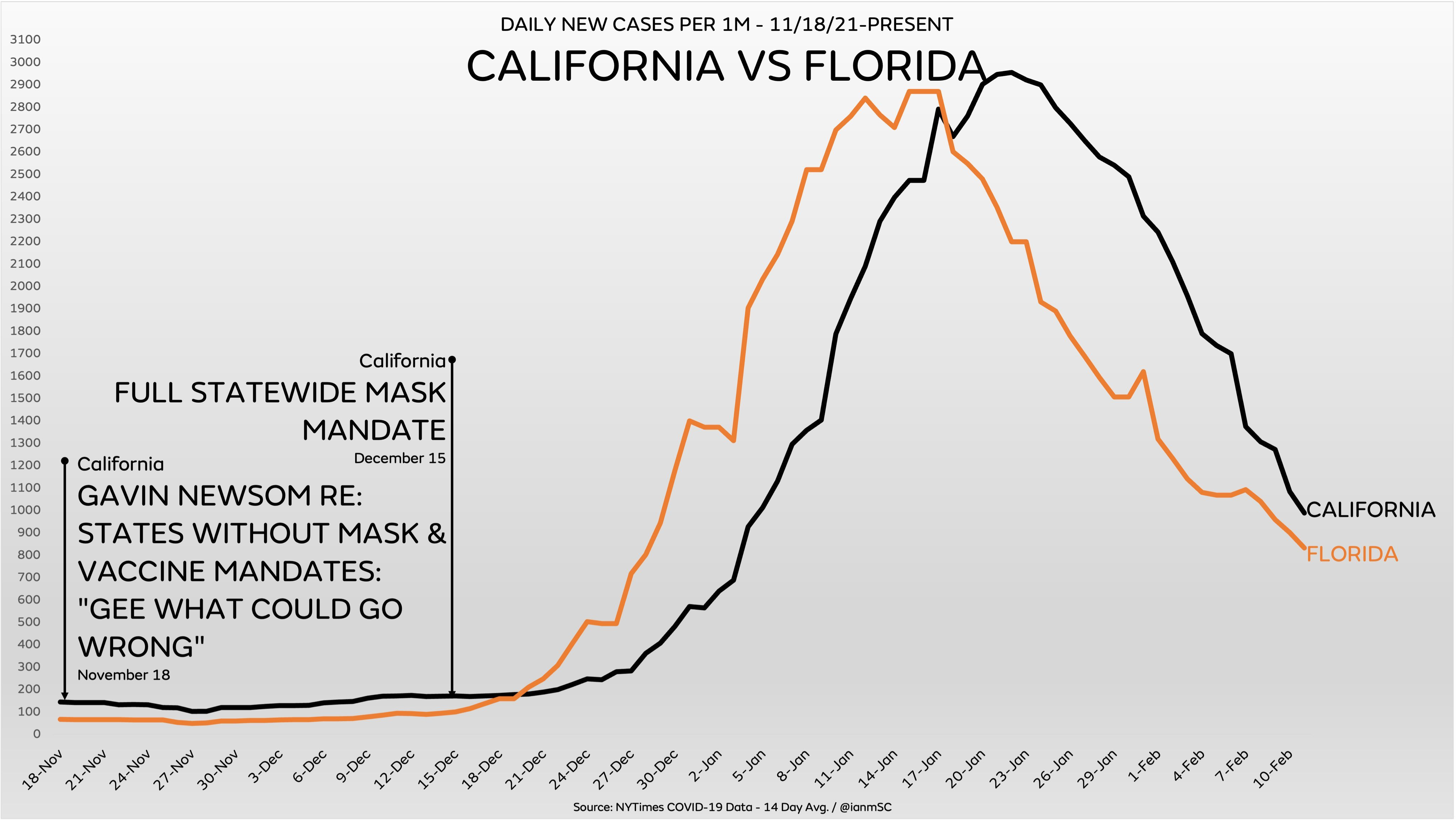
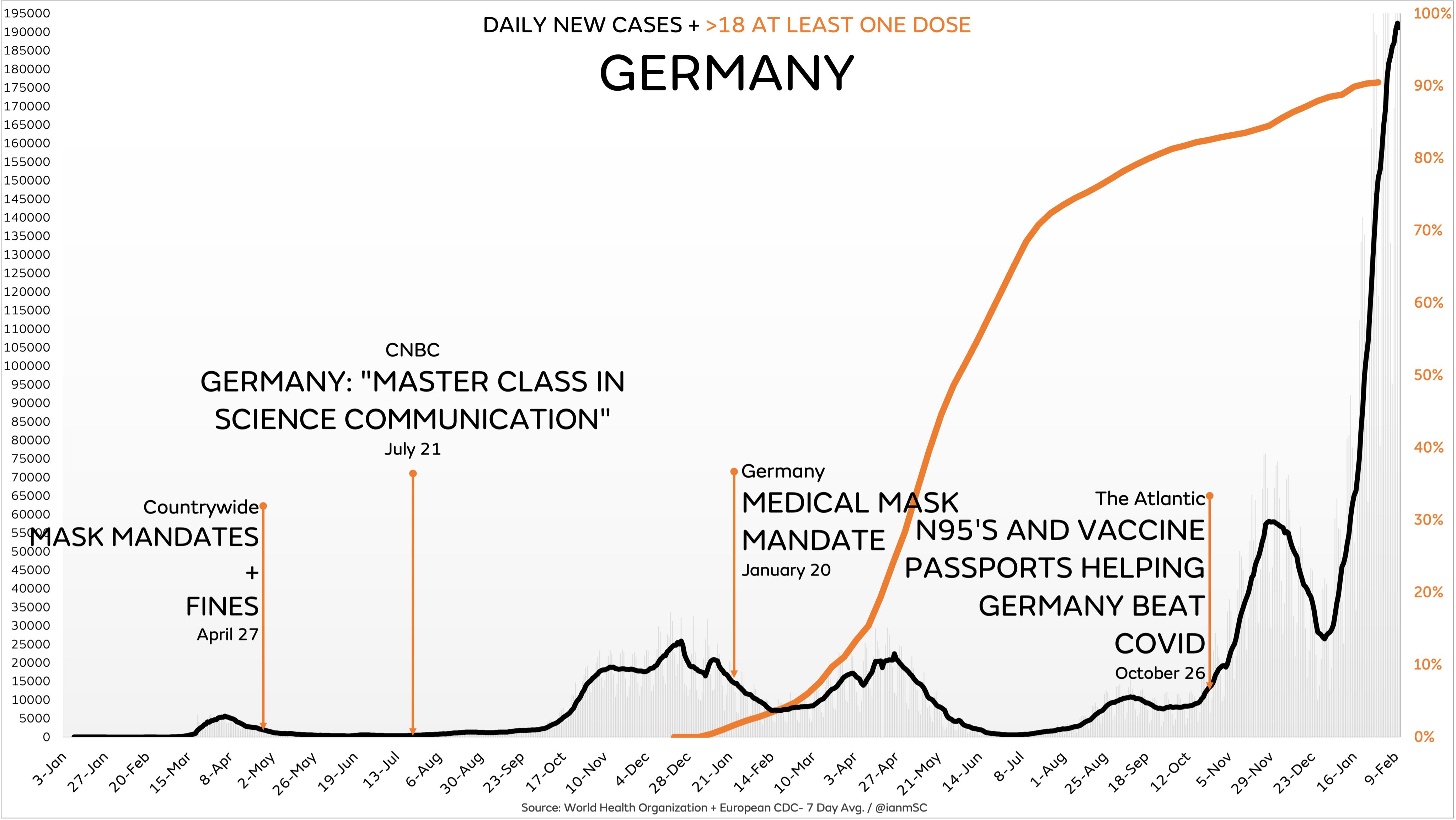
Charts via Ian Miller at Unmasked
Public Health Threw Out the Playbook and Threw Pandora’s Box Wide Open
The masses who’ve chanted “I trust science,” as they praise each government intervention and idolize those who impose them, are likely unaware that, before Covid-19, the well-considered scientific consensus was against lockdowns, broad quarantines and masking outside of hospital settings—particularly for a virus like Covid-19 that has a 99% survival rate for most age groups.
For example, a 2006 paper published by the Center for Biosecurity of the University of Pittsburgh Medical Center—focusing on mitigation measures against another contagious respiratory illness, pandemic influenza—reads like a warning label against many of the policies inflicted on humanity in the face of Covid-19:
- “There is no basis for recommending quarantine either of groups or individuals. The problems in implementing such measures are formidable, and secondary effects of absenteeism and community disruption as well as possible adverse consequences… are likely to be considerable.”
- “Widespread closures [of schools, restaurants, churches, recreations centers, etc] would almost certainly have serious adverse social and economic effects.”
- “The ordinary surgical mask does little to prevent inhalation of small droplets bearing influenza virus… There are few data available to support the efficacy of N95 or surgical masks outside a healthcare setting. N95 masks need to be fit-tested to be efficacious.”
The point of that and other pre-2020 research into pandemic mitigation was to be prepared, in times of crisis, with policies that reflected a well-reasoned and dispassionate weighing of costs and benefits.
However, when the pandemic arrived, panicking public health officials and academics threw out the playbook and took their policy inspiration from the government that was first to confront the virus. Sadly for the world, that was communist China.
The breadth of the resulting harms from the ensuing plunge into public health authoritarianism is staggering. Far from erring on the side of caution…
Public health erred on the side of a mental health crisis. Anxiety and depression have surged, particularly among adolescents and young adults, where symptoms have doubled during the pandemic.
“I have never been as busy in my life and I’ve never seen my colleagues as busy,” New York psychiatrist Valentine Raiteri told CNBC. “I can’t refer people to other people because everybody is full.”
Public health erred on the side of juvenile suicide attempts. In the summer of 2020, emergency room visits for potential suicides by children leapt over 22% compared to the summer of 2019.
Public health erred on the side of drug overdoses. According to the National Institute on Drug Abuse, overdose deaths surged 30% in 2020 to a record-high of more than 93,000. Among the factors cited: social isolation, people using drugs alone, and decreased access to treatment.
Public health erred on the side of auto fatalities. Traffic deaths had been on a general downtrend since the 60s, reaching a near-record low in 2019. However, even with shutdown-lightened traffic, deaths jumped 17.5% in the summer of 2020 compared to 2019, and kept rising into 2021.
Blame increased drug and alcohol use, along with psychological fallout from people being denied life’s fundamental pleasures. University of Texas cognitive scientist Art Markman told The New York Times that anger and aggression behind the wheel in part reflects “two years of having to stop ourselves from doing things that we’d like to do.”
Public health erred on the side of domestic violence. A review of 32 studies found an increase in domestic violence around the world, with the increases most intense during the first week of lockdowns. “The home confinement led to constant contact between perpetrators and victims, resulting in increased violence and decreased reports,” the researchers found.
Public health erred on the side of riots, arson and looting. It’s my own conviction that 2020’s eruption of summer violence following a Minneapolis police officer’s callous homicide of George Floyd was greatly magnified by the period of forced mass confinement that preceded it.
Floyd’s death was a match dropped into a tinderbox of humanity confined to veritable house arrest. People blocked from restaurants and bars were suddenly granted a societal waiver to venture out into enormous crowds, where they found excitement, socialization and, far too often, a senselessly destructive means of venting months of pent-up energy, anxiety and frustration. It stands as the costliest civil unrest episode in American history.
Public health erred on the side of confining people where the virus is transmitted most. Lockdowns ordered people away from workplaces, schools, restaurants and bars and into their homes, where New York contract tracers found 74% of Covid spread was happening, compared to just 1.4% in bars and restaurants and even less in schools and workplaces.
Public health erred on the side of obesity. According to the CDC, “the risk of severe COVID-19 illness increases sharply with higher BMI [Body Mass Index].” So what happens when public health “experts” shut down schools, workplaces and recreation options and told people to stay home to stay “safe”?
The CDC found that, in 2020, the rate by which BMI increased among 2- to 19-year olds doubled. Another study found that 48% of adults gained weight during the pandemic, with those who were already overweight most likely to add even more. Among other factors, the study pointed to psychological distress and having schoolchildren at home.
Public health erred against fresh air, exercise and Vitamin D. Governments raced to shut down playgrounds, basketball courts and other outdoor recreation facilities. In a move that’s profoundly emblematic of heavy-handed, counterproductive authoritarianism in the age of Covid, the city of San Clemente, California filled a skate park with 37 tons of sand.
Public health erred on the side of impaired child development. “We find that children born during the pandemic have significantly reduced verbal, motor, and overall cognitive performance compared to children born pre-pandemic,” say the authors of a study from Paediatric Emergency Research in the UK and Ireland (PERUKI).
“Results highlight that even in the absence of direct SARS-CoV-2 infection and COVID-19 illness, the environmental changes associated [with the] COVID-19 pandemic [are] significantly and negatively affecting infant and child development.”
Public health erred on the side of learning loss. Children are less vulnerable to Covid-19 than they are to the flu, and rarely transmit it to teachers. Unfortunately, American public health officials and teacher unions prevailed in halting in-person instruction (and socialization) in favor of “remote learning.”
It was a poor substitute that fell hardest on the youngest learners. For example, according to curriculum and assessment provider Amplify, the percentage of first-graders scoring at or above the goals for their grade in mid-school-year dropped from 58% before the pandemic to just 44% this year.
Public health erred on the side of pointlessly masking schoolchildren. When schools did open, mask mandates abounded—despite children’s relative invulnerability to the virus and the documented rarity of in-school transmission. A Spanish study showed no discernible difference in transmission among 5-year-olds—who aren’t required to mask—and 6 year olds, who are.
“Masking is a psychological stressor for children and disrupts learning. Covering the lower half of the face of both teacher and pupil reduces the ability to communicate,” wrote Neeraj Sood, director of the Covid Initiative at USC, and Jay Bhattacharya, professor of medicine at Stanford. “Positive emotions such as laughing and smiling become less recognizable, and negative emotions get amplified. Bonding between teachers and students takes a hit.”
“Most of the masks worn by most kids for most of the pandemic have likely done nothing to change the velocity or trajectory of the virus,” writes University of California associate professor of epidemiology and biostatistics Vinay Prasad. “The loss to children remains difficult to capture in hard data, but will likely become clear in the years to come.”
Public health erred on the side of giving masked people a false sense of security. As I wrote in August, “Covid-19 particles are astoundingly small. Hard as it is to imagine, the imperceptible gaps in surgical masks can be 1,000 times the size of a viral particle. Gaps in cloth masks are well larger.” That’s to say nothing of the respirated air that simply goes around the mask’s edges.
Earlier in the pandemic, questioning cloth masks triggered outrage and swift social media censorship. Now, even mandate-happy CNN medical analyst Leanna Wen has declared they’re “little more than facial decorations.” Mask skepticism is sprouting elsewhere in mainstream media; the Washington Post and Bloomberg even published an essay titled “Mask Mandates Didn’t Make Much of a Difference Anyway.”
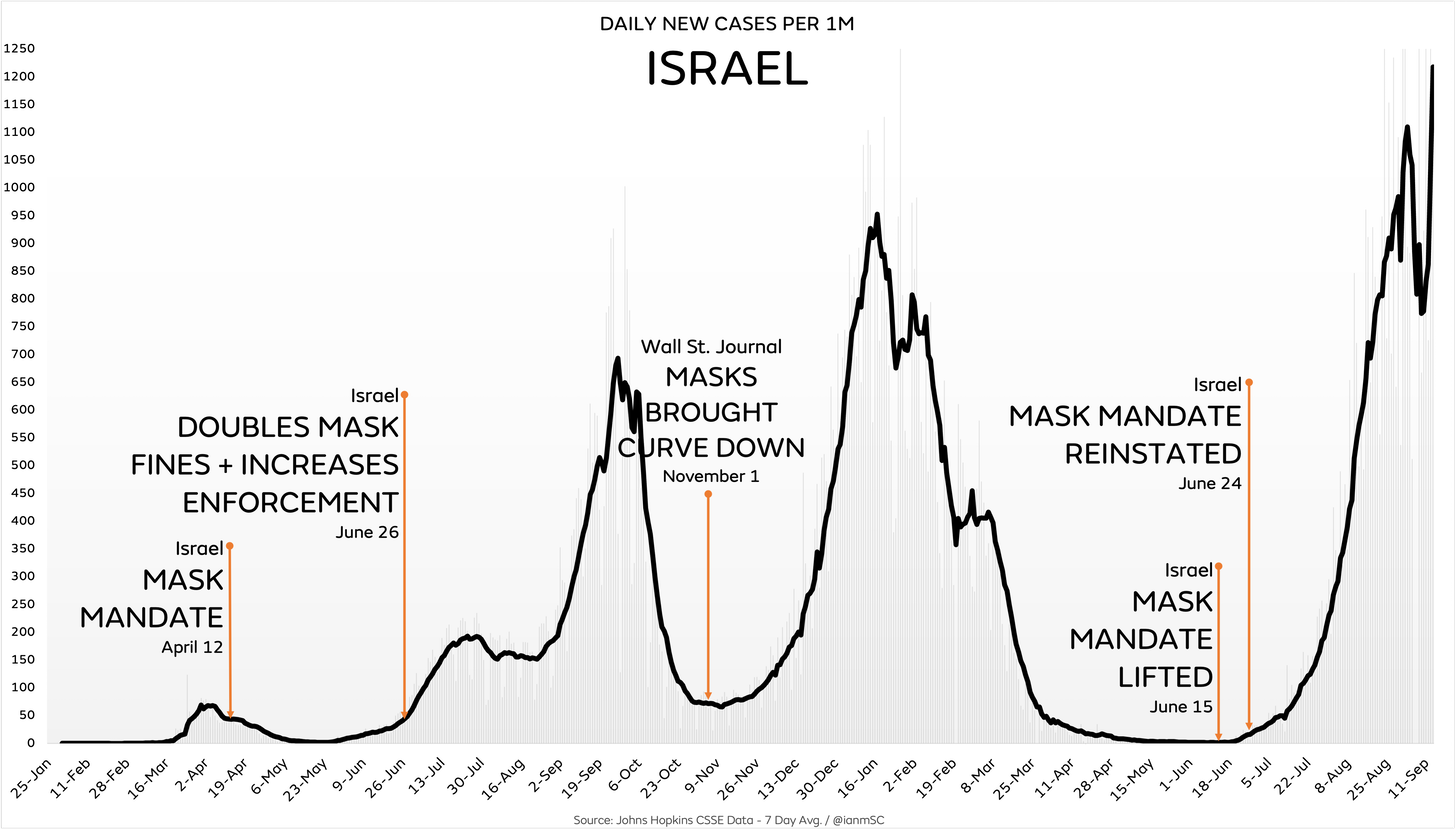
Chart via Ian Miller at Unmasked
When public health officials exaggerated the power of masks, they did more than promote pointless discomfort and a dystopian way of life. “Naively fooled to think that masks would protect them, some older high-risk people did not socially distance properly, and some died from Covid-19 because of it,” said epidemiologist, biostatistician and former Harvard Medical School professor Martin Kulldorff.
Public health erred on the side of killing small businesses. Thanks in large part to government’s targeting of so-called “non-essential businesses,” the first year of the pandemic brought an additional 200,000 business closures over prior levels.
Public health erred on the side of harming women’s careers. Women comprise a greater proportion of the sectors hid hardest by lockdowns, and the closing of schools and child care centers prompted many more women than men to put their careers on hold.
Public health erred on the side of inflation. To offset the massive economic destruction inflicted by public health shutdowns, the federal government plunged into an astounding spending spree, handing out cash to individuals, businesses and city and state governments.
It was money the government didn’t have, so the Federal Reserve essentially created it out of thin air. Pushing all that new fiat money into circulation debases the currency, fueling today’s surging price inflation—which is a stealth tax with no maximum rate, which hits poor people hardest.
Note: Lockdowns and other mandates weren’t the exclusive driver of many of the various harms I’ve described; general fear of the virus also contributed to some of them. However, it should also be noted that public health officials—and media that overwhelmingly emphasized negative stories—whipped up a level of fear that led people to overstate the level of danger actually posed by the virus.
There’s one more way in which characterizing lockdowns and other mandates as “erring on the side of caution” plays a psychological trick: Since the phrase is embedded with the notion of good intentions, it conditions citizens to be forgiving of the bureaucrats and politicians who imposed them.
Note, however, that in most everyday usage of “erring on the side of caution,” the choice to “err” is made voluntarily by individuals who bear the consequences of their own decisions—or by others, like an airplane pilot or a surgeon, to whom we’ve voluntarily and unmistakably granted control of our well-being.
The grim impacts of lockdowns and other mandates, however, were coercively imposed on society, to say nothing of the fact that so many of the edicts represented gross usurpations of power and violations of human rights.
On top of all that, the edicts were reinforced by Orwellian censorship and ostracism leveled at those who dared raise questions that have now proven valid.
So make no mistake: Overreaching public health officials and politicians—and the journalists-in-name-only who served as their mindless, unquestioning megaphones—have fully earned our withering condemnation. Indeed, holding them accountable is essential to sparing ourselves and future generations from repeating this dystopian chapter of human history.
Papua New Guinea’s pandemic leadership is an inspiration to us all
Harry Dougherty Blog | February 24, 2022
When I find myself arguing with pro mandate Australians in social media comment sections (tragic, I know) I get the impression that they desperately want the last couple of years they’ve squandered to have been worthwhile.
Australia’s official Covid19 death rate happens to be low by international standards, which makes it easier for the Dan Andrews fanboys to delude themselves that the sick cruelty they inflicted on their fellow citizens was justified.
For a recap, this cruelty includes but is not limited to:
- Prolonged mass house arrest
- Vaccine Passports
- Vaccine injuries and deaths in individuals (often young and not at serious risk from Covid) who were coerced into getting it.
- The four newborn babies in South Australia who died after domestic Covid19 travel restrictions prevented them from being transferred for specialist life-saving emergency treatment in Victoria.
- In Western Australia, the prevention of unvaccinated parents from visiting their sick children in hospital.
If I was Australian Prime Minister Scott Morrison, (that snivelling, gaslighting, modern-day Pontius Pilate), I would not want to admit that pointlessly I stole two years of quality life from my citizens and presided over state policies that killed people,
“Australians have made many sacrifices during this pandemic,… together we have achieved one of the lowest death rates in the world,” he says.
Achieved? Everywhere in the Oceania region has a low death rate by global standards. When will Papua New Guinea’s PM be praised for his inspirational leadership? Don’t hold your breath, but PNG is Australia’s immediate neighbour, (and the only other country on Earth with kangaroos), yet has a lower Covid19 death rate than does oz.
Could that be because of the success of PNG’s vaccination rollout? Did they her the sheep through the gate, so to speak?
Vaccination rate for Australia (at least one dose): 85%
Vaccination rate for PNG (at least one dose): 3.4%
Since we are only allowed to compare Sweden with its neighbours, it’s only fair that the same rules must apply to everyone. I assume vaccine passports aren’t really a thing in PNG. But they seem to be coping without them.
Covid19 deaths per million for Australia: 193/1M
Covid19 deaths per million for PNG: 69/1M
Most countries in Europe have relatively high death rates, though the few nations that had extremely low death rates (Norway and Finland) did not have the strictest measures. Lockdown rejecting Sweden’s death rate is firmly in Europe’s lower half.
At present, the UK is the least restricted country in Europe, possibly in the developed world and has been since July 2021, yet our (questionably recorded) Covid19 death rate is only the 22nd highest in Europe, currently slightly lower than that of Italy, which has vaccine passports and vaccine mandates, and surgical masks remain compulsory.
What would Australia’s death rate be were it somehow squeezed into the North Atlantic or continental Europe? We cannot know.
The Nudge: Ethically Dubious and Ineffective
BY GARY SIDLEY | BROWNSTONE INSTITUTE | MARCH 1, 2022
More and more people in the US will be wising up to their government’s use of behavioural science – or ‘nudging’ – as a means of increasing compliance with Covid-19 restrictions. These psychological techniques exploit the fact that human beings are almost always on ‘automatic pilot,’ habitually making moment-by-moment decisions without rational thought or conscious reflection.
The use of behavioural science in this way represents a radical departure from the traditional methods – legislation, information provision, rational argument – used by governments to influence the behaviour of their citizens. But why expend all that time and energy when, by contrast, many of the ‘nudges’ delivered are – to various degrees – acting upon the public automatically, below the level of conscious thought and reason?
By going with the grain of how we think and act, the state-employed ‘nudgers’ can covertly shape our behaviour in a direction deemed desirable by the regime of the day – an appealing prospect for any government. The ubiquitous deployment of these behavioural strategies – which frequently rely on inflating emotional distress to change behaviour – raises profound moral questions.
The UK has been an innovator in these methods, but they are now raising widespread disquiet here. In fact serious concerns about our Government’s use of behavioural science were previously raised in relation to other spheres of government activity. In 2019, a Parliamentary report found that the distress evoked in people targeted by behavioural insights in relation to tax collection may, in some instances, have led to victims taking their own lives.
In the Covid-19 era, it appears the behavioural scientists have been given free reign. As a retired consultant clinical psychologist, I – and 39 professionals from the psychology/therapy/mental health sphere – have become so concerned we are calling on the UK Parliament to formally investigate the government’s use of behavioural science. People across the world can glean from the UK experience what may also have been done to them, and what may be next.
The Behavioural Insights Team
The appetite for using covert psychological strategies as a means of changing people’s behaviour was boosted by the emergence of the ‘Behavioural Insights Team’ (BIT) in 2010 as ‘the world’s first government institution dedicated to the application of behavioural science to policy.’ The membership of BIT rapidly expanded from a seven-person unit embedded in the UK Government to a ‘social purpose company’ operating in many countries across the world. A comprehensive account of the psychological techniques recommended by the BIT is provided in the document, MINDSPACE: Influencing behaviour through public policy, where the authors claim that their strategies can achieve ‘low cost, low pain ways of nudging citizens … into new ways of acting by going with the grain of how we think and act.’
Since its inception in 2010, the BIT has been led by Professor David Halpern who is currently the team’s chief executive. Professor Halpern and two other members of the BIT also currently sit on the Scientific Pandemic Insights Group on Behaviours (SPI-B), which advises the Government on its Covid-19 communications strategy. Most of the other members of the SPI-B are prominent UK psychologists who have expertise in the deployment of behavioural-science ‘nudge’ techniques.
‘Nudges’ of concern: fear inflation, shaming, peer pressure
The BIT and the SPI-B have encouraged the deployment of many techniques from behavioural science within the UK Government’s Covid-19 communications. However, there are three ‘nudges’ which have evoked most alarm: the exploitation of fear (inflating perceived threat levels), shame (conflating compliance with virtue) and peer pressure (portraying non-compliers as a deviant minority) – or “affect,” “ego” and “norms,” to use the language of the MINDSPACE document.
Affect and Fear
Aware that a frightened population is a compliant one, a strategic decision was made to inflate the fear levels of all the UK people. The minutes of the SPI-B meeting dated the 22nd of March 2020 stated, ‘The perceived level of personal threat needs to be increased among those who are complacent’ by ‘using hard-hitting emotional messaging.’ Subsequently, in tandem with the UK’s subservient mainstream media, the collective efforts of the BIT and the SPI-B have inflicted a prolonged and concerted scare campaign upon the UK public. The methods used have included:
– Daily statistics displayed without context: the macabre mono focus on showing the number of Covid-19 deaths without mention of mortality from other causes or the fact that, under normal circumstances, around 1,600 people die each day in the UK.
– Recurrent footage of dying patients: images of the acutely unwell in Intensive Care Units.
– Scary slogans: for example, ‘IF YOU GO OUT YOU CAN SPREAD IT, PEOPLE WILL DIE,’ typically accompanied by frightening images of emergency personnel in masks and visors.
Ego and Shame
We all strive to maintain a positive view of ourselves. Utilising this human tendency, behavioural scientists have recommended messaging that equates virtue with adherence to the Covid-19 restrictions and subsequent vaccination campaign. Consequently, following the rules preserves the integrity of our egos while any deviation evokes shame. Examples of these nudges in action include:
– Slogans that shame the non-compliant: for example, ‘STAY HOME, PROTECT THE NHS, SAVE LIVES.’
– TV advertisements: actors tell us, ‘I wear a face covering to protect my mates’ and ‘I make space to protect you.’
– Clap for Careers: the pre-orchestrated weekly ritual, purportedly to show appreciation for NHS staff.
– Ministers telling students not to ‘kill your gran.’
– Shame-evoking adverts: close-up images of acutely unwell hospital patients with the voice-over, ‘Can you look them in the eyes and tell them you’re doing all you can to stop the spread of coronavirus?’
Norms and Peer Pressure
Awareness of the prevalent views and behaviour of our fellow citizens can pressurise us to conform, and knowledge of being in a deviant minority is a source of discomfort. The UK Government repeatedly encouraged peer pressure throughout the Covid-19 crisis to gain the public’s compliance with their escalating restrictions, an approach that – at higher levels of intensity – can morph into scapegoating.
The most straightforward example is how, during interviews with the media, Government ministers often resorted to telling us that the vast majority of people were ‘obeying the rules’ or that almost all of us were conforming.
However, in order to enhance and sustain normative pressure, people need to be able to instantly distinguish the rule breakers from the rule followers; the visibility of face coverings provides this immediate differentiation. The switch to the mandating of masks in community settings in summer 2020, without the emergence of new and robust evidence that they reduce viral transmission, strongly suggests that the mask requirement was introduced primarily as a compliance device to harness normative pressure.
Ethical questions
Compared to a government’s typical tools of persuasion, the covert psychological strategies outlined above differ in both their nature and subconscious mode of action. Consequently, there are three main areas of ethical concern associated with their use: problems with the methods per se; problems with the lack of consent; and problems with the goals to which they are applied.
First, it is highly questionable whether a civilised society should knowingly increase the emotional discomfort of its citizens as a means of gaining their compliance. Government scientists deploying fear, shame, and scapegoating to change minds is an ethically dubious practice that in some respects resembles the tactics used by totalitarian regimes such as China, where the state inflicts pain on a subset of its population in an attempt to eliminate beliefs and behavior they perceive to be deviant.
Another ethical issue associated with these covert psychological techniques relates to their unintended consequences. Shaming and scapegoating have emboldened some people to harass those unable or unwilling to wear a face covering. More disturbingly, the inflated fear levels will have significantly contributed to the many thousands of excess non-Covid deaths that have occurred in people’s homes, the strategically-increased anxieties discouraging many from seeking help for other illnesses.
Furthermore, a lot of older people, rendered housebound by fear, may have died prematurely from loneliness. Those already suffering with obsessive-compulsive problems about contamination, and patients with severe health anxieties, will have had their anguish exacerbated by the campaign of fear. Even now, after all the vulnerable groups in the UK have been offered vaccination, many of our citizens remain tormented by ‘COVID-19 Anxiety Syndrome’), characterised by a disabling combination of fear and maladaptive coping strategies.
Second, a recipient’s consent prior to the delivery of a medical or psychological intervention is a fundamental requirement of a civilised society. Professor David Halpern explicitly recognised the significant ethical dilemmas arising from the use of influencing strategies that impact subconsciously on the country’s citizens. The MINDSPACE document – of which Professor Halpern is a co-author – states that, ‘Policymakers wishing to use these tools … need the approval of the public to do so’ (p74).
More recently, in Professor Halpern’s book, Inside the Nudge Unit, he is even more emphatic about the importance of consent: ‘If Governments … wish to use behavioural insights, they must seek and maintain the permission of the public. Ultimately, you – the public, the citizen – need to decide what the objectives, and limits, of nudging and empirical testing should be’ (p375).
As far as we are aware, no attempt has ever been made to obtain the UK public’s permission to use covert psychological strategies.
Third, the perceived legitimacy of using subconscious ‘nudges’ to influence people may also depend upon the behavioural goals that are being pursued. It may be that a higher proportion of the general public would be comfortable with the government resorting to subconscious nudges to reduce violent crime as compared to the purpose of imposing unprecedented and non-evidenced public-health restrictions. Would UK citizens have agreed to the furtive deployment of fear, shame and peer pressure as a way of levering compliance with lockdowns, mask mandates and vaccination? Maybe they should be asked before the government considers any future imposition of these techniques.
A truly independent and comprehensive evaluation of the ethics of deploying psychological ‘nudges’ – during public health campaigns and in other areas of government – is now urgently required, not only in Britain, but in all countries where these interventions have been used.
Dr Gary Sidley is a retired consultant clinical psychologist who worked in the UK’s National Health Service for over 30 years, a member of HART Group and a founder member of the Smile Free campaign against forced masking.
Featured Video
Deep Dive Intel Briefing 6/20/2026 Lt Col Daniel Davis
or go to
Aletho News Archives – Video-Images
From the Archives
As Hillary Clinton kisses up to Henry Kissinger, RT looks at 4 of his most heinous acts
RT | September 3, 2016
… While Clinton retains the ultimate warmongering seal, RT examines some of Kissinger’s most memorable acts… Read full article
Blog Roll
 Aletho News
Aletho News- Terms of US capitulation to Iran presage new era for the region
- Strategic Oil Reserve Nears Collapse… US Must Choose: Guns or Butter
- The Story the Media — and the Government — Don’t Want You to Hear
- Deep Dive Intel Briefing 6/20/2026 Lt Col Daniel Davis
- The Targeted Assassination of Studies Showing Vaccines Cause Injury
- BMJ Probe Into Excess Mortality Study Drags On for Two Years With No Resolution
- Securing Peace with Iran Compels Trump to Divorce Israel
- Old Iraq war architects rise up to wag finger at Trump’s Iran deal
- Strait of Hormuz closed over Israeli aggression on Lebanon
- Keir Starmer arson mysteries multiply
- If Americans Knew
- ‘Reproductive genocide’ in Gaza; death toll in Lebanon tops 4,000 (during a ceasefire) – Daily Update
- Israelis Invaded Lebanon And Then Cried Victim When Their Soldiers Got Killed
- FARA Docs: Israel is Spying On Millions Of Christian Americans In Their Churches
- Why US presidents from both parties end up cursing Benjamin Netanyahu
- Israel Asked Facebook to Censor Iran War Content, Internal Documents Show
- Deaths in Gaza undercounted, possibly by 100s of thousands; “Psychopath” Ben-Gvir talks trash – Daily Update
- UNICEF: “Trauma is woven into the very fabric of childhood in Gaza”
- 15 articles a day: The extent of the Israeli army’s media interference
- Greek Orthodox Patriarchate denounces Israeli seizure of church land in Jerusalem
- How Hillel International uses antisemitism training and ‘campus climate’ concerns to attack Palestine solidarity
- No Tricks Zone
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
