Google suppresses America’s Frontline Doctors in search results
By Didi Rankovic | Reclaim The Net | February 28, 2022
More evidence is emerging of Google manipulating algorithms powering its mammoth and highly influential search service to give certain results (much) more visibility than others.
And now, reports say, Google is not even trying to hide that this is the case, as America’s Frontline Doctors (AFLDS) has been informed its reach on the internet is being artificially limited.
This organization says it is dedicated to improving doctor-patient relationships that are jeopardized by what it calls politicized science and biased information. The AFLDS would also like to provide patients with access to “independent, evidence-based information” that will inform people’s decisions regarding their healthcare choices.
Well, meeting that goal might prove to be quite difficult since Google Search, on which a huge majority of US-based users rely for their internet queries, says it is deliberately deranking information coming from the AFLDS.
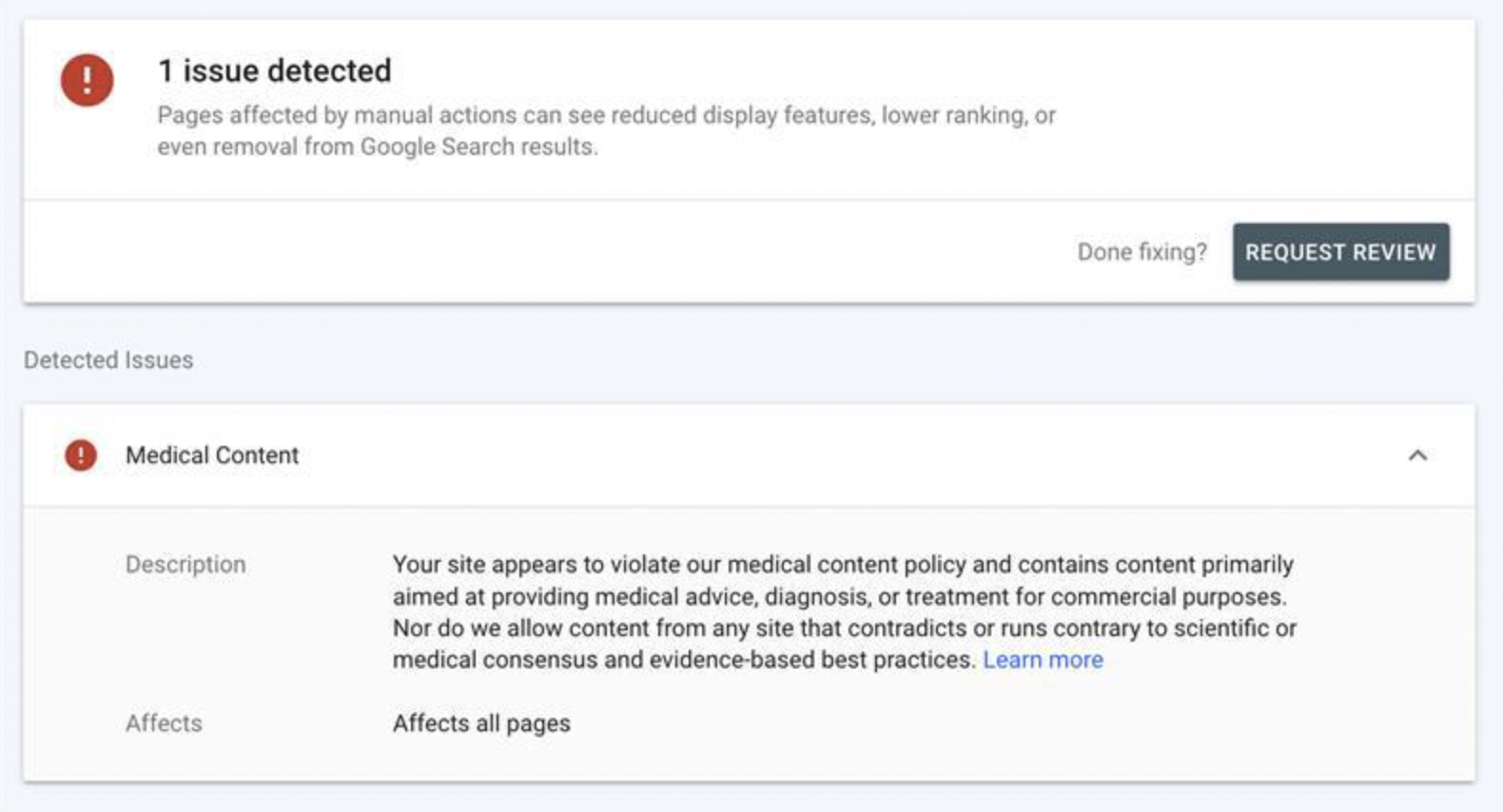
This transpires from alerts Google has been sending the organization, which state that an “issue” has been detected, which can be “fixed;” after that, the AFLDS can “request review.”
And when an “issue” has been detected, Google spells it out that “Pages affected by manual actions can see reduced display features, lower ranking or even removal from Google Search results.”
So what “issues” have been detected, you might ask next. Google’s “explanation” is the usual hodgepodge of vague language and qualifiers, in line with the giant’s now well-established censorship style.
The AFLDS is informed that its site “appears to violate” Google’s medical content policy, which is not allowed – and neither is content that “contradicts or runs contrary to scientific or medical consensus and evidence based best practices.”
That’s according to Google’s rules. What consensus, reached by who, and what best practices, determined by who, and at what time – none of this information is provided in the notices.
Google’s rigid, authoritarian style of promoting one-sided content and eliminating different arguments and positions would in this case work by first deranking (and eventually removing) AFLDS links – unless the group agrees to self-censor.
And that means deleting content from the site, and then clicking on “‘Request Review’ button which is prefaced with the question, ‘Done fixing?’,” the AFLDS explains.
The organization also takes issue with Google’s (deliberately) broad and ambiguous wording and lack of proper, or any definition of scientific and medical consensus and best practices – to ask why, “In a time when celebrities and computer programmers are allowed to express their views on virology, but actual doctors and scientists are censored, including the hundreds of doctors comprising AFLDS, such clarity is elusive.”
UK Gov’t to make some “Covid Laws” permanent
By Kit Knightly | OffGuardian | February 28, 2022
Some of the UK’s “temporary” measures intended to help “deal with the pandemic” are going to be added to future legislation and made permament laws by the spring of this year.
Of course, the truth is that many of the “temporary” Covid measures were already permanent.
As we detailed in fact check in the spring of 2020, although defenders claimed the Coronavirus Act was “temporary” and “only for two years”, this was completely untrue.
To quote ourselves…
Section 89 of the Coronavirus Act 2020 details just how many sections and sub-sections are not subject to the expiry clause. As well as all the “conditions” which, if met, would enable Ministers to waive the expiry clause on certain other sections and regulations.
The list is hugely long: Sections 1, 2, 5, 6, 11, 12, 13, 17, 19(11), 21(7), 59-70, 72-74, 75(1) and 76. As well as parts of Schedules 1, 4, 5, 7, 8 and 10 through 13.
These non-temporary measures included section 11, which guarantees legal indemnity for any public sector employee if they kill or injure a patient whilst attempting to treat Covid.
In total, over a quarter of the “temporary measures” were never actually temporary. And now, as Covid segues into war, the government are seeking to add a few more clauses to the non-temporary list.
It’s all detailed in the government’s “Living with Covid” planning document, released last week.
Among the double-think, back-pedalling and revisionism the document claims that the sections 30, 53, 54 and 55 of the Coronoavirus Act have “enabled revolutions in the delivery of public services” and should be made permanent.
They propose a sixth month extension now, while the sections are copied-and-pasted into legislation expected to pass later this year.
Section 30 gave coroners the right to have an inquest without a jury when Covid19 was a suspected cause of death, why they want this to be permanent I can’t see as yet. Except maybe to further erode the ideas behind the Jury system they’ve been attempting to undermine throughout the “pandemic”. Of course, it could also be amended to include any other disease they wish.
That is expected to be passed into law as part of the Judicial Review and Courts Bill.
Sections 53-55, though, empowered the justice system to hold trials over the internet, via audio or video link. Making this permanent has massive implications for human rights moving forward, not to mention leaving the system wide open for abuse and fakery (pre-recordings, deep fakes or other digital manipulation).
These will be added to the Police, Crime, Sentencing and Courts Bill
It was a terrible precedent to set, and now its here forever. We did warn you it wouldn’t be “just two years”.
The great debate: PolitiFact vs. “the world’s top misinformation spreaders”
The request from PolitiFact to remove the fact check recording
By Steve Kirsch | February 25, 2022
Recently, I got an email from PolitiFact’s Editor-in-Chief, Angie Holan, requesting I remove the recording of my conversation with their so-called “fact checker,” Gabrielle Settles who was doing a fact check on VAERS.
I refused her request.
Gabrielle asked if she could record the call and I consented, so that entitles all parties to record the call. PolitiFact did not deny that we both consented. She wrote,
I am not in the least embarrassed by how she conducted the interview. I’m asking that you remove the video as a professional courtesy because the reporter did not consent to be recorded.
First of all, she should be embarrassed by the interview. The interviewer was clearly focused on proving an agenda and showed no interest in exploring evidence that was counter her agenda. I gave her the story of the century if she would just follow up on what I suggested she do.
Secondly with respect to permission, by asking me if it was OK to record the call, she is giving implied consent for the call to be recorded since she is doing the asking. All parties on the call consented to being recorded meaning the conversation is no longer private and all parties can record the call.
The debate challenge
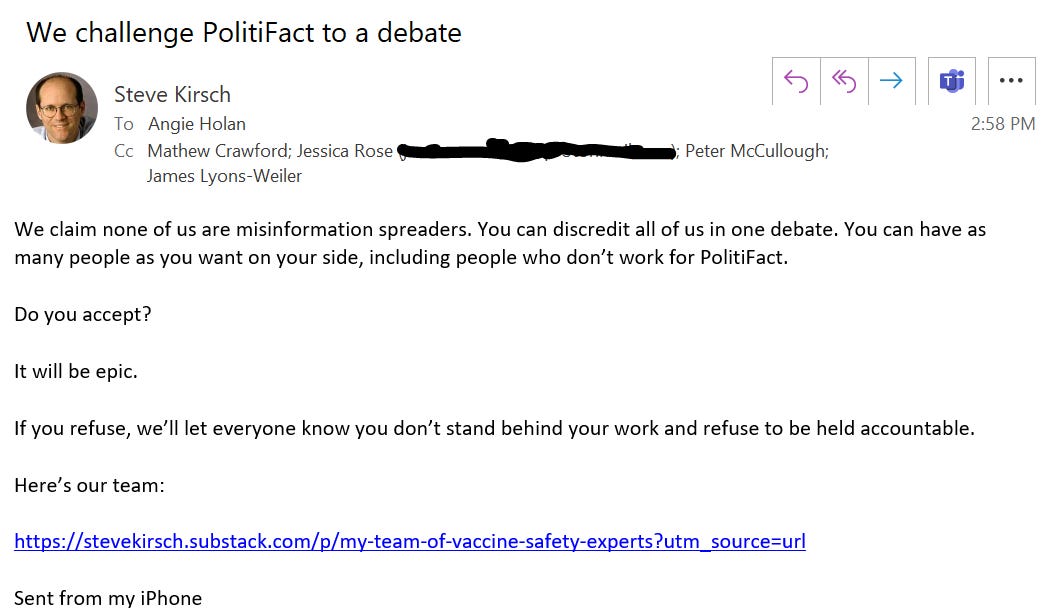
I then raised the stakes: I challenged PolitiFact to a debate to settle the matter once and for all in front of a live Internet audience as to who are the liars and who are the truth tellers. Here is the email I sent on Feb 25, 2022 at 2:58pm PST:
A good, old-fashioned debate.
They can have as many people as they want on their side, the more the better since it will remove all excuses when they lose.
We can use the debate rules suggested here, or anything else they are comfortable with.
The purpose is simple: to ascertain who is really spreading misinformation.
After all, the US Surgeon General has said how dangerous COVID-19 misinformation is. So has the California State Legislature: In House Resolution No. 74 of the 2021–22 Regular Session, the California State Assembly declared health misinformation to be a public health crisis, and urged the State of California to commit to appropriately combating health misinformation and curbing the spread of falsehoods that threaten the health and safety of Californians.
The fastest way to stop all COVID misinformation is to challenge the spreaders of the misinformation and discredit them in a debate
Of course, the problem with a debate is that usually one side wins. If it is the misinformation spreaders, the narrative is crushed. This is why nobody wants a debate: they can’t take the risk.
PolitiFact can’t win a fair debate. There is way too much information out now on how dangerous the vaccines are that is impossible for them to explain.
This is why I don’t think that there is a snowball’s chance in hell they will accept.
I sent the email to Angie earlier today and have not heard back. I will update this article if I do. Don’t hold your breath.
Watch the video that they don’t want you to see
The video they wanted me to remove exposes how the fact checker had absolutely no interest in exploring any of the evidence that proved that the VAERS data was correct.
In short, the video proves that these so-called fact checkers aren’t interested in the facts; they are interested in defending the false narrative.
Be sure to check out the original story (it’s point #5 in this article), and be sure to watch the video if you haven’t already. It shows just how biased these fact checkers are.
Be sure to check out the comments at Rumble on the video:
Other points about VAERS:
- The CDC warns in boldface lettering on its website, “[k]nowingly filing a false VAERS report is a violation of Federal law (18 U.S. Code Section 1001) punishable by fine and imprisonment.”
- Not only are there criminal penalties for filing false VAERS reports, but physicians or medical providers file a majority of them. Dr. McCullough says health care providers file 60 to 80% of VAERS reports. You can verify this by reading the reports.
- Whoever files the report has to have the lot number and batch number of the vaccine and it’s fairly time consuming process. McCullough says that the CDC has analysts call whoever entered the report in order to verify it. McCullough has received those calls.
- Doctors are of course not compensated for filing VAERS reports so they often don’t file them. Most are probably unaware that they are required to file VAERS reports. No one gives them training on filing VAERS reports. Hospital employees have said their hospitals don’t even know about the requirement to report VAERS injuries.
Read more about fact checkers
See this article.
In the meantime, California wants to ensure that no doctor can question whatever the government says
California just introduced a bill that would enable medical boards to take away the license of any doctor who spreads “COVID-19 misinformation.” This is a tacit admission that they can’t win on the facts, so they have to use threats and intimidation to keep the truth from emerging. Their only weapon is censorship.
Here’s the bill: AB-2098.
They define COVID-19 misinformation as anything going against the government narrative.
In short, they want to take away the free speech rights of doctors who would no longer be allowed to question anything the government says. After they do that, citizens will be next.
See this California Globe article, CA Lawmakers Propose Bill to Punish Doctors Who Speak Against COVID Treatment ‘Consensus’, for more info.
Florida is doing the opposite: Protecting the rights of doctors to speak freely
Meanwhile, Florida is doing the opposite by proposing a law that would protect the rights of doctors to speak the truth.
We live in interesting times.
Comments from my good friend Dr. Byram Bridle
Byram tried to debate the authorities in Canada, but they were a no show. He likes courts because the other party is forced to appear.
Here is what he wrote:
Hi Steve, I can’t get any of the narrative-pushers in Canada to debate the science. It would be great if you could have some success with this in the US. But, I agree with you; they almost certainly won’t. Those who don’t stand on the science will never engage in a conversation. People who love the narrative need to start asking their ‘champions’ why they keep refusing to step into the arena with the dissidents. At some point they are going to have to admit that their ‘champions’ are cowards and do nothing more than ‘talk the talk’ from behind their keyboards. A lack of scientific expertise becomes quite apparent when one has to respond off-the-cuff to another scientist in real-time. One place that the ‘experts’ for the narrative cannot hide is in court. So far, I have been seeing them crushed in this venue. This is why many court decisions are being made on technicalities; to avoid ruling on the evidence, the weight of which is not in favor of the narrative.
They are censoring doctors in the UK
From the comments:
GPs have been warned that criticising the Covid vaccine or other pandemic measures via social media could leave them ‘vulnerable’ to GMC* investigation.’1
*GMC = General Medical Council. This is the body that can strike doctors from the medical register so they cannot work as a doctor.
‘Vulnerable to GMC investigation’. What a deliciously creepy phrase that is, dripping with unspoken menace, whilst pretending to be helpful. It sounds like something the Mafia would come up with.
‘I would keep quiet about this, if I were you.’ Baseball bat tapping gently on the floor. ‘No, this is not a threat, think of it as advice from a friend. We don’t like to see anybody making themselves, or their family, vulnerable, and getting seriously injured now, would we?’
It seems that, unless you prostrate yourself before the mighty vaccine, and intone ‘Our vaccine, which art in heaven, hallowed be thy name…’ and suchlike, you will be attacked from all sides … simultaneously. Indeed, to suggest that vaccines are not perfect in every way is the twenty first century’s equivalent of blasphemy.”
See: https://drmalcolmkendrick.org/2022/02/23/a-few-thoughts-on-covid19-vaccination/
They are censoring doctors in Australia
Elizabeth Hart in the comments notes that muzzling doctors from questioning the Covid jabs is the same in Australia.
AHPRA, the regulator of ‘health practitioners’ here, issued a Position Statement dated 9 March 2021, which states: “Vaccination is a crucial part of the public health response to the COVID-19 pandemic. Many registered health practitioners will have a vital role in COVID-19 vaccination programs and in educating the public about the importance and safety of COVID-19 vaccines to ensure high participation rates.”
Health practitioners are also warned: “Any promotion of anti-vaccination statements or health advice which contradicts the best available scientific evidence or seeks to actively undermine the national immunisation campaign (including via social media) is not supported by National Boards and may be in breach of the codes of conduct and subject to investigation and possible regulatory action.” (Search for AHPRA position statement 9 March 2021 to download PDF.)
Who defines what is “the best available scientific advice”? We know what a disastrous quagmire of conflicts of interest is “the best available scientific advice”…
In regards to ‘anti-vaccination’, in practice, any questioning of Covid jabs in Australia is regarded as ‘anti-vaccination’, as tennis star Novak Djokovic discovered when he tried to come here recently to participate in the Australian Open. The Immigration Minister banished Djokovic from Australia because he “has previously stated that he ‘wouldn’t want to be forced by someone to take a vaccine’ to travel or compete in tournaments”. For being an individual wanting to retain his bodily autonomy, Immigration Minister Alex Hawke considered the presence of Djokovic “may be a risk to the health of the Australian community”, presumably as Djokovic might inspire Australians to make their own informed decision about the Covid-19 jabs, counter to government diktats. (See the court judgement here: https://www.judgments.fedcourt.gov.au/judgments/Judgments/fca/full/2022/2022fcafc0003 )
What does the antagonism against Novak Djokovic mean for critical thinking Australians who have similarly made their own informed decision to refuse to consent to Covid jabs that don’t prevent infection nor transmission, injections which purportedly provide questionable ‘protection’ of very limited duration, against a disease it was known from the beginning wasn’t a serious threat to most people?
Now we have a dire situation in Australia where millions of people have been coerced to be jabbed to maintain their livelihoods under state government and business/employer mandates, this directly flouts the obligation for valid voluntary consent to be given before vaccination.
I’ve complained about this matter to medical organisations in Australia, see my email to the Medical Board of Australia, AHPRA, RACGP, RACP, AMA, 8 June 2021: https://vaccinationispolitical.files.wordpress.com/2021/06/coercive-covid-19-injections-in-australia-medical-board-of-australia-ahpra-racgp-racp-ama.pdf
After perseverance, I finally received a response from AHPRA, which confirms: “Practitioners have an obligation to obtain informed consent for treatment, including vaccination. Informed consent is a person’s voluntary decision about health care that is made with knowledge and understanding of the benefits and risks involved.” See: https://vaccinationispolitical.files.wordpress.com/2021/10/response-from-ahpra-re-informed-consent.pdf
But this isn’t happening! With so many people being coerced and manipulated into submitting to the jabs under state government and business/employer mandates, this isn’t authentic voluntary consent. The situation is really bad in Australia, which I suspect is possibly the most mandated jab country in the world.
Summary
We want to make sure people know the truth about PolitiFact. I literally handed Gabrielle Settles the story of the century and she had no interest at all in pursuing any of it.
Everyone should watch the video of how they operate.
If PolitiFact and others want to end misinformation, all they have to do is debate us. Instead, governments are passing laws to censor doctors since they don’t have the facts on their side.
All over the world, governments do not want the people to hear the fully story.
Vaccination – silencing doctors in the UK
By Dr. Malcolm Kendrick | February 27, 2022
My last blog discussed the possibility that mRNA COVID19 vaccines significantly increase the risk of myocarditis. Following this, a fellow doctor reached out to tell me about what has happened to them. They too, had questioned some aspects of the safety and efficacy of the vaccines.
As a result, they have been sent two threatening letters, which are both of the ‘iron fist in a velvet glove’ variety. I asked their permission to reproduce them here. One is from the General Medical Council (GMC). The other from their responsible officer – I shall explain what this title means a bit further on.
Below is the letter from the GMC:
Dear Dr….
The GMC have received several complaints regarding your recent social media posts.
All doctors have a right to express their personal opinion regarding the Covid-19 vaccine, and while the GMC in no way supports this opinion, we don’t consider your comments are sufficiently strong to open a fitness to practice investigation at this stage.
However, we are referring this matter to your Responsible Office for your reflection through the appraisal process.
We ask that you consider what implications this complaint might have for your practise when you are discussing this with your appraiser. We would also like to remind you of GMC guidance, in particular ‘Doctors’ use of social media, and of the requirement of doctors to act with honesty and integrity to justify the public’s trust in them
What we will do now
We will share the complaint with your responsible officer for them to consider in the wider context of your practice and revalidation.
‘The wider context of your practice and revalidation.’ Which means what, exactly? I sometimes wonder if there a special training scheme where you learn to write creepy and threatening phrases that can later be denied as being creepy and threatening? ‘I was only trying to be nice. They just took it the wrong way.’
‘Your children look charming. However, you may want to consider their continued existence on the planet in the wider context of your practice.’
The GMC, as mentioned before, have the powers to investigate complaints made against doctors in the UK, and impose various punishments (they call them sanctions, which sounds far prettier). Ranging from nothing very much to permanent erasure from the medical performers list.
The latter means that you cannot work as a doctor ever again. Anywhere in the world. The GMC will communicate your erasure to other national statutory bodies, upon request. They do it gladly… and speedily.
On the face of it, in this case, the GMC have decided to do nothing. ‘We don’t consider your comments are sufficiently strong to open a fitness to practice investigation at this stage.’
Jolly good.Nothing to see here, move along. Although they add the rider … ‘at this stage.’ Well, what other stages are left, after deciding to take no action? The … I have changed my mind and I am going to have you guillotined, stage?
However, in reality they have not done nothing – have they dear reader? The GMC have decided to refer the complaint to this doctor’s responsible officer. A responsible officer is a doctor who is ‘responsible’ for ensuring that other doctors working in their area have met the necessary requirement for revalidation.
Revalidation is a five-year cycle whereby a doctor has to meet various requirements. A few hundred hours of medical education, keeping up do date with mandatory training. Carrying out an audit, and a patient satisfaction questionnaire, getting sufficient colleague feedback, and suchlike.
There is also a need to have a yearly appraisal. Which is a meeting with an allocated appraiser, to discuss how things have gone. A look through any complaints about you, work you have done, audits that have been completed, actions to take in the next year to improve your practice – a personal development plan. Release of thumbscrews – or a tightening.
If all this is done successfully, over a five-year period, the responsible officer ‘signs you off’ and you are now able to continue work. If not, you are removed from the performers list, and you cannot work as a doctor until you are successfully re-validated. No-one has ever explained to me how you actually do get revalidated. In fact, there is no system in place for this to happen.
If you manage to fulfil the re-validation cycle, and attend appraisals, in theory there can be no grounds for removal. You cannot actually ‘fail’ an appraisal. You simply have to turn up, and ‘reflect’ on your practice. I have never heard of a responsible officer stepping in to remove a doctor from the performers list any time they so wish.
Bearing all that in mind, here is the follow up letter from the responsible officer.
Dear Dr….
I have today received a communication from the GMC regarding an ‘incident that occurred on social media.’ The GMC have advised that they have reviewed the complaint and that it does not meet the threshold for investigation.
However, I understand that you have been asked to consider what implications this complaint may have for your practise and there is a requirement for you to reflect on this matter at your next appraisal meeting.
As your Responsible Officer I have a statutory duty to ensure that any concern or complaint about your practise is responded to and dealt with appropriately.
I would be grateful if you could let me have your views on this issue, by completing the attached form and returning it as a matter of urgency.
Can you also complete the attached Monitoring of Clinical Practise for your file, please.
Your co-operation with this process is vital in order for us to come to an acceptable resolution as soon as possible, minimising impact to your practice and cost in time and money.
If you have any questions regarding this process, please to contact me to discuss further.
Kind regards
Dr X
Responsible Officer for X region.
I love the ‘Kind regards’ sign off. For this is a letter dripping with unspoken menace. Just to highlight one phrase ‘An incident that occurred on social media…’ An ‘incident’. You mean, someone wrote something that someone didn’t like, they then complained about it. This was not an incident, in the sense that anyone would normally choose to use this word.
[I also note that the GMC spells practice, practice. The responsible officer spells it practise – maybe they need to reflect on their spelling between them].
If you look up the word ‘incident’ on the Cambridge Dictionary it gives an example of its use:
‘A youth was seriously injured in a shooting incident on Saturday night.’1
It does not say. ‘Someone wrote a blog post that upset someone, somewhere, for a bit. But it’s alright now, they are looking at pictures of kittens to recover.’
Words. Words, words, words. They can be used in so many different ways. Their true meaning hidden behind layers of sophistry. But we all know what the word ‘incident’ means in this case. Someone was badly damaged by your actions on that day – do not attempt to deny it, comrade.
Then we move on to the real threat. The responsible officer wants to ensure an acceptable resolution, thus … ‘minimising impact to your practise and cost in time and money.’
What the responsible officer here is saying is that I have the powers to stop you practising medicine in the UK. If I find that your answer to this complaint – which was not strong enough to open a fitness to practice investigation by the GMC – does not satisfy me. Indeed (subtext), I do not actually care what answer you give, I may remove you anyway. This will certainly maximise the impact on this doctor’s ‘practise and cost in time and money’.
If you think this is not what is being threatened. Then ask yourself what else it could mean? There is nothing that needs to be ‘resolved’. A complaint has been made, but the GMC didn’t think it was serious enough to take forward. No patient was harmed, no laws broken … no wrecks and nobody drowned, in fact nothing to laugh at, at all. (small prize for who knows where that came from).
At this point you may have begun to allow the thought to enter your mind that the GMC have quite deliberately handed this complaint down to the responsible officer to carry out the required sentence and execution. Whatever the accused doctor says, the responsible officer can simply respond. ‘Sorry, not satisfied with your answer. I am now going to stop you working – for as long as I wish.’ No hearing, no possibility of review, no accountability. Bosh.
In truth I have always known that responsible officers possess this amazing and unrestrained power. I tried, and failed, to stop this happening years ago – when I was on various British Medical Association (BMA) committees. I found it incredible that the legislation in this area was going to hand over, to one individual, the ability to destroy someone’s career, with no regard to anyone else, or anything else.
Yes, we live in a democracy that has created a form of local tyranny.
Tyranny (noun) def: government by a ruler or small group of people who have unlimited power of the people in their country or state and use it unfairly, and cruelly.
You could say that this situation suits the GMC very well … Very well indeed. Because, you see, the GMC has tried to remove other doctors from the medical register for criticising vaccination. [The medical register is not quite the same thing as the performer’s list, but you need to be on both of them to work as a doctor in the UK].
These punishments were quashed in the High Court. Here from a legal firm that works in this area:
‘On Friday, the High Court handed down a judgment quashing the GMC interim order of conditions previously imposed on a GP, Dr Samuel White, as a result of his actions arising from the pandemic. Dr White came to the GMC’s attention as a result of “spreading misinformation and inaccurate details about the Coronavirus and how it is diagnosed and treated”. His comments have included assertions that the COVID-19 vaccine “inserts a code”, masks do “absolutely nothing” and hydroxychloroquine, budesonide inhalers and ivermectin are “safe and proven treatments”.
The interesting point arising from Dr White’s High Court appeal is the technical point on which he won. The High Court found that the Medical Practitioners Tribunal Service (MPTS – the adjudication wing of the GMC) panel made an error of law in not properly considering the test required by section 12(3) of the Human Rights Act 1998 when deciding whether to impose an interim order.’2
As this company also says:
As time goes on, we’re seeing more fitness to practise cases arising from COVID-19-related activities. We’ve previously posted about the Irish GP interim suspended after describing COVID-19 as a hoax and the first UK nurse struck off by the Nursing and Midwifery Council (NMC) as a result of COVID-19 denial activities.
‘COVID denial activities’ – what a deliciously Soviet phrase.
I have to say that I very much enjoyed the lawyers’ assertion that the GMC interim order was quashed on a ‘technical point’. Namely that the GMC had failed to consider the small matter of the Human Rights Act 1998. Riding roughshod over someone’s human rights is now a technical point of law. How quaint.
However, undeterred, the GMC have not been deterred from their vital work in punishing COVID-19 vaccine deniers – to ensure that they can never work again. They have just found another, simpler, far cheaper, and far quicker route to obliterate a doctor’s career. Call the responsible officer. No-one expects the responsible officer.
Who needs time consuming and costly hearings, where you might have to bear in mind the Human Rights act 1998 – and other such woolly liberal nonsense? When you can alert the local ‘tyrant’ to a doctor’s non-comradely Soviet ‘denial’ activities. Sorry, COVID19 ‘denial’ activities.
They will know precisely what to do, and they have the powers to do it. Why on earth did the GMC not think of this of this before? I could have told them about the ridiculous, frightening, and untrammelled powers of a responsible officer, but they never asked me.
Of course, you could argue the following. If the local responsible officer does obliterate someone’s medical career and does this without paying any heed to such things as well, the law, for example, then their actions will be over-turned in court. Well, I certainly hope so, in fact I would expect so. This may act as a deterrent … maybe.
However, during the months, or years, that it takes to get such a case to court, the doctor will be out of work and unable to earn. They will almost certainly end up bankrupt, and their reputation (have been struck off the performers’ list) will lie shattered in the gutter.
As for the responsible officer. Their punishment ‘please don’t do it again,’ would just about cover it. This is very much asymmetric warfare. I can punish you, terribly, but you can do absolutely nothing to me in return.
In the financial world they call this moral hazard. A banker can bankrupt you, and your family, and half the country, making stupid and risky decisions – that will earn them huge short-term bonuses. If, as a result, their bank goes bust, the Government simply bails them out and they keep their job, and their bonus. All gain, no pain.
As a sign off, the responsible officer (washing his hands of any personal responsibility of course) wrote this ‘I have a statutory duty to ensure that any concern or complaint about your practise is responded to and dealt with appropriately.’ Kind regards … Pontius.
However, one thing that has not happened, so far, is to actually take the time and effort to forward a copy of the complaints to the doctor concerned. Still, they must be guilty of something or other. So, it is clearly critical that they respond to these unknown complaints, of some sort or another, in some-way or other. ‘Here is a bottle of whisky, and a revolver…. You know what you must do.’
What a world this has become. I had hoped I would not live to see such a time in this country, but I have.
1: https://dictionary.cambridge.org/dictionary/english/incident
The CDC Discovers Actual Public Health, Just in Time
BY JEFFREY A. TUCKER | BROWNSTONE INSTITUTE | FEBRUARY 26, 2022
One day I’m reading an internal memo commissioned by the Democratic Party to provide advice to dealing with Covid policy. The next day I’m reading headlines about how the CDC has drastically altered its advice on how to deal with Covid.
Is there a relationship? At this point, only the hopelessly naive would think otherwise.
Let’s look at the memo produced by Impact Research. Some excerpts:
- Democrats have a tremendous opportunity to claim an incredible, historic success – they vaccinated hundreds of millions of people, prevented the economy from going into freefall, kept small businesses from going under, and got people back to work safely. Because of President Biden and Democrats, we CAN safely return to life feeling much more normal – and they should claim that proudly.
- Six in ten Americans describe themselves as “worn out” by the pandemic. The more we talk about the threat of COVID and onerously restrict people’s lives because of it, the more we turn them against us and show them we’re out of touch with their daily realities.
- [I]t means recognizing that the threat of COVID is no longer what it was even a year ago and therefore should not be treated as such – shutdowns, masks, and lockdowns were meant to save lives when there was not yet a vaccine that could do that. Voters know we now have the tools in the toolkit to be responsible in combatting and living with COVID – vaccines and boosters to minimize illness, and masks and social distancing around vulnerable groups.
- They think the virus is here to stay, and 83% say the pandemic will be over when it’s a mild illness like the flu rather than COVID being completely gone, and 55% prefer that COVID should be treated as an endemic disease. And that’s what most Americans are dealing with—a disease with fatality rates like the flu—because most of us took the personal responsibility to protect ourselves and our families by getting vaccinated.
- Stop talking about restrictions and the unknown future ahead. If we focus on how bad things still are and how much worse they could get, we set Democrats up as failures unable to navigate us through this. When 99% of Americans can get vaccinated, we cause more harm than we prevent with voters by going into our third year talking about restrictions. And, if Democrats continue to hold a posture that prioritizes COVID precautions over learning how to live in a world where COVID exists, but does not dominate, they risk paying dearly for it in November.
A few points.
This memo is not epidemiology but politics, most strongly illustrated by the idea that polling should make the difference as to whether a pathogen is pandemic or endemic. The constant incantation of “vaccines” here has nothing to do with the known data: they have nowhere stopped infection or spread, a point which the memo obscures with the line about how they “minimize illness.” They minimize serious outcomes for some strains so long as they last.
From a policy point of view, there are two main features that stand out: Covid is here to stay and “most people in the US will eventually get COVID-19” (thereby hinting at the reality that vaccines are not effective in the way that Biden/Fauci/Walensky promised) and therefore the focus should be on protecting the vulnerable.
There is nothing new about this. It was always true! You can shout “Omicron” all day but it was also true with Alpha and Delta as well. The virus should have been treated rationally the entire time and policies that have wrecked public health should have been off the table from 2020. The memo writers did not cite the Great Barrington Declaration but they might as well have.
As for how the Democrats somehow prevented an economic freefall, the worst economic outcomes are very clearly in Democratic-controlled states that retained restrictions for nearly two years in some places, including keeping schools closed. There is a reason for the mass migration that this has inspired.
If we are looking for thriving economies, look to the states that never closed up or opened earliest: South Dakota, Florida, Texas, Georgia, and so on. So none of this is remotely true but, hey, this is politics, right?, so it doesn’t have to be true.
The real problem that the Democrats need to solve is revealed in this chart:

Now, let us consider the dramatic turnaround at the CDC that came out the very next day. The full PDF is embedded below.
Here are the talking points handed to the director. It’s not just about masking, which is being relaxed. The CDC says there needs to be a dramatic shift away from endless monitoring of cases that are overwhelmingly mild and instead focus only on actual sickness that lands people in the hospital and threatens life. We need to stop obsessing about cases and start looking mainly at “medically significant disease.” The focus should be on “protecting the most vulnerable.”
This makes all of us want to say, shout, scream: THANK YOU!
In order to justify this change, the CDC posts four sets of charts on Covid prevalence during episodes of the pandemic. The last chart illustrates the point that an exclusive focus on controlling the spread is utterly preposterous at this point. Under the old protocols, the whole country should be back in lockdown. It’s unimaginable what attempting this now would cause.

To be sure, all of this is enormously frustrating for those of us engaged in this battle for two years. Instead of focusing on getting sick people well, the CDC experimented with wild guidelines that imagined some kind of society-wide solution that seemed designed to crush the virus while vast amounts of social and economic activity were shut down by law. This necessitated a crushing of freedoms, including of travel, association, commerce, religion, and, eventually even speech.
The CDC nowhere admits this much less apologizes for it. Two years in, the CDC seems to have rediscovered the traditional practice of public health, and has justified this new wisdom based on changed conditions, while never even bothering to claim that its previous measures and guidelines achieved anything along the way.
We’ve seen a massive collapse in public health, economic vitality, and essential rights, while closing schools and wrecking education and so much more, all in the name of virus control, even as the evidence is now overwhelming that the entire enterprise was not only a distraction from what should have happened (therapeutics and protecting the vulnerable) but also an astonishing failure.
Why the change? It had to happen at some point. The entire machinery of lockdowns and mandates were destined to fail. As to the timing of the reversal, it’s hard to resist the speculation that it is entirely political. See the memo above.
Still, there is a worrisome aspect to the CDC’s announcement. They reserve the right to do it all over again. “We want to give people a break from things like mask-wearing, when these metrics are better, and then have the ability to reach for them again should things worsen,” she said.
No one should be satisfied with a politically motivated change in the messaging. We need fundamental regime change to make sure that nothing like this can ever happen again.
Jeffrey A. Tucker is Founder and President of the Brownstone Institute and the author of many thousands of articles in the scholarly and popular press and ten books in 5 languages, most recently Liberty or Lockdown.
WHO planning new “pandemic treaty” for 2024
By Kit Knightly | OffGuardian | February 26, 2022
In December of last year, the World Health Organization (WHO) announced plans for an “international treaty on pandemic prevention and preparedness”.
According to the Council of Europe’s website, an “intergovernmental negotiating body” has been formed, and will be holding its first meeting next week, on March 1st.
The aim is to “deliver a progress report to the 76th World Health Assembly in 2023” and then have the proposed instrument ready for legal implementation by 2024.
None of this should come as much of a surprise, the signs have all been there. If you’ve been paying attention you could probably predict almost everything that will be in this new legislation.
A paper titled “Multilateralism in times of global pandemic: Lessons learned and the way forward” was published by the G20 in Decemeber 2020.
It details all the problems faced by international multilateral organizations during the “pandemic” [emphasis added]:
Individual states cannot effectively manage global public threats such as the COVID-19 pandemic on their own […] overcoming the current health crisis and rebuilding livelihoods can only be achieved through multilateral action on both the economic and social fronts […] The COVID-19 pandemic and its economic consequences have revealed the weakness of the current arrangements for multilateral cooperation. International organizations with the mandate to play leading roles in dealing with international crises have not functioned effectively.
And goes on to propose several solutions, including…
The G20 should reinforce the capacity of the World Health Organization. A stronger and more responsive WHO can help the international community manage pandemics and other health challenges more effectively. It can provide early warning systems and coordinate rapid global responses to health emergencies.
In January of 2021 the EU thinktank Foundation for European Progressive Studies published a 268-page document titled “Reforming Multilateralism in Post Covid Times”, which called for a “more legitimate and binding United Nations”, suggested the EU join the UN Security Council, and asked:
Is national sovereignty compatible with multilateralism?”
A few months later the United Nations Foundation published its own variation on this theme: “Reimagining multilateralism for a post-Covid future”
Then, in May 2021, the International Panel on Pandemic Preparedness released its report on how the world handled Covid, which echoes the G20 paper almost word-for-word in places. We did a detailed breakdown of it here.
Former New Zealand Prime Minister Helen Clark, chair of the panel, told the Guardian…
[The pandemic was] compounded by a lack of global leadership and coordination of geopolitical tensions and nationalism weakening the multilateral system, which should act to keep the world safe.”
Earlier this month, the UN Commission for Social Development met for the first time in 2022, with an emphasis on “Strengthening multilateralism”.
Then, on February 17th, the European Council on Foreign Relation’s Robert Dworkin published this article, Health of nations: How Europe can fight future pandemics, which also expresses concern over “the failures of international cooperation during the pandemic” and proposes :
The EU should combine a push for reform of and increased funding for the WHO with support for a new fund for health emergencies, overseen by a representative group of countries.
It goes on and on and on… the messaging is more than clear.
Even just last week, speaking on a panel at the Munich Security Conference, Sweden’s Foreign Minister Anne Linde warned that Covid has “exposed holes” in the international order, and that the UN, WHO and EU were not empowered enough to take appropriate action.
The signs are all there, and they’ve been flashing like neon lights for months: New international legislation to “deal with future pandemics”.
We all knew it was coming eventually. Now we have a timeline, and it starts on March 1st.
Isn’t it amazing what you can almost miss when you’re distracted by a war?
Speaking of the war, the attitude the WHO takes to Russia during this process will be a very interesting barometer. Whether Russia denounces the proposed treaty, or is excluded from negotions, will tell us a lot about how real the conflict in Ukraine truly is, and what direction the Great Reset will take next.
Indeed, if the war itself is used to further argue we need “stronger multilateral institutions” or “important reforms in the security council”, it may go some way to revealing the grander agenda.
The Glorious Flop of New Zealand Virus Control
BY IAN MILLER | BROWNSTONE INSTITUTE | FEBRUARY 26, 2022
An infuriatingly consistent aspect of the mainstream media’s COVID coverage was their determination to prematurely credit a country with a wildly successful set of policy interventions.
While there has been no track record of universally accurate predictions or expectations, the desire to claim victory as far back as spring 2020 has led to subsequent embarrassments as trends change.
Naturally, New Zealand is no stranger to such untimely praise, with the BBC in July 2020 doing an in-depth look at how New Zealand became “COVID free.”
Of course, it was because New Zealand “… locked down early and aimed for elimination” and achieved “effective communication and public compliance.”
This is really the whole problem in a nutshell, isn’t it?
Assuming that elimination was possible through effective communication, compliance and early lockdowns ignores the inevitably that COVID will eventually spread throughout the population, whenever you “open up.”
Elimination of COVID throughout the world is and always was impossible, and therefore Fauci’s assertion that COVID could be “eliminated in certain countries” was inane and virtually impossible.
So how successful has New Zealand been in eliminating COVID in the long term through effective communication, public compliance and early lockdowns?
Well. The numbers speak for themselves.

When the BBC wrote the article explaining New Zealand’s remarkable success in eliminating the virus, they were averaging 1.5 cases each day. It’s now 2,918 cases each day.
That’s an increase of nearly 195,000%.
Elimination is a pipe dream.
No matter what policy interventions they’ve added, no matter how many early lockdowns they’ve tried, COVID has not been eliminated.
Remember how New Zealand’s amazing tracking and tracing system allowed them to identify transmission that could have only occurred via aerosols? And recall how all of the pre-pandemic guidance on masking suggested that masks could not stop aerosols? Did that stop New Zealand from using mask mandates to try and continue their elimination goals?
Of course not!
The following are the currently enforced rules on face masks in New Zealand:
- As a general rule, you should wear a face mask whenever you are indoors. The exceptions are at your home or your place of work if it is not public facing. Your employer may encourage you to wear a face mask even if your job is not public facing.
- When it is hard to physically distance from people you do not know, we encourage you to wear a face mask.
- Everyone must wear a mask that is attached to the face by loops around the ears or head. This means people can no longer use scarves, bandannas or t-shirts as face coverings.
We know New Zealanders are complying because the BBC assured us that their success was due to population compliance, but the survey data backs that up as well:

Mask wearing has been consistently high since the mandate came into effect in August, yet cases have exploded anyway.
None of it has mattered.
And this isn’t an insignificant increase. New Zealand’s now reporting more new cases adjusted for population than the United States, and identical numbers to the United Kingdom:

Working perfectly!
Elimination Through Vaccination
In the previously referenced interview, Fauci said that the most successful way to “eliminate” COVID was to reach extraordinary levels of vaccination uptake in the population.
While the Our World in Data download hasn’t been updated in the past week, over 88% of the population had received at least one vaccination dose in New Zealand by February 15th.
The numbers are even more impressive when considering only those over 12 years of age. 95% of everyone over in that demographic has been at least partially vaccinated or booked their appointment. 94% are fully vaccinated:

Nearly 2.3 million people over 12 have been given boosters, roughly 53% of that entire population.
Clearly those incredible rates of uptake must have been enough to maintain the “blanket of herd immunity” that Fauci claimed would be achievable with 75-85% of the population vaccinated.

Not exactly!
Whenever you reference the dramatic failure of Australia or New Zealand to maintain “zero COVID” lockdowns and “elimination” strategies, adherents to the cult of inaccurate expertise will respond by claiming their goal was only to eliminate cases until widespread vaccination.
By allowing for vaccines to blunt the impact of cases, these countries would prevent surges in hospitalizations. We already saw that this was wildly off in Australia:

But what about New Zealand? Maybe they’ve been able to successfully stave off any surge in severe cases due to their exceptional vaccination rate:

Well. Not exactly.
Hospitalizations have risen dramatically since January and continue to rise significantly each day.
News reports from New Zealand sound like those from any generic location in the US where local doctors report concerns of hospitals being overwhelmed:
Authorities anticipate Omicron will become the predominant Covid-19 variant in New Zealand within just two to four weeks of it being introduced into the community – and hospitals are bracing to be “swamped”.
Dr John Bonning, a frontline emergency department doctor and immediate past president of the Australasian College for Emergency Medicine, said EDs were already under “enormous duress”.
So their elimination strategy did not prevent a dramatic increase in cases, nor a concerning, overwhelming surge of hospitalizations.
And deaths, while thankfully still low, have increased in recent months as well:

New Zealand’s supposed “elimination” through their zero COVID policy has completely collapsed.
Mask mandates, as their own research indicated, have not prevented surges. Elimination until vaccination has not prevented surges. Zero COVID has been an unmitigated failure, as any rational person would have known and suggested as far back as summer 2020.
They’ve maintained an unearned sense of superiority, exemplified in this quote from the BBC’s story:
He says it is “a bit of a puzzle for us at a distance to understand why” with the UK’s extensive scientific expertise and health care, “you haven’t looked at the evidence and worked out a pattern like New Zealand’s”.
The UK government has previously defended its coronavirus strategy, saying its approach was “being guided by the science.”
That undeserved attitude can no longer be maintained.
The policies that never had the slightest possibility of long term success, the policies that Fauci claimed could be successful in “certain countries,” have turned into yet another example of the delusions of hubris.
While many areas are lifting mandates, they’re doing so without acknowledging the underlying flaws in their strategy. Iceland’s health ministry summed up the inescapable reality of COVID while announcing an end to all restrictions:
“Widespread societal resistance to COVID-19 is the main route out of the epidemic,” the ministry said in a statement, citing infectious disease authorities.
“To achieve this, as many people as possible need to be infected with the virus as the vaccines are not enough, even though they provide good protection against serious illness,” it added.
Until they understand and accept those sentiments, there will always be excuses for politicians and public health officials to bring back their prized, ineffectual interventions.
New Zealand is the latest in a long list of countries to be hailed as showing the world the “right” way to prevent surges; to keep COVID under control.
But as with masks, vaccine passports and “early” lockdowns, zero COVID never had a chance of working — despite the endless media and expert praise.
As always, Eric Feigl-Ding had absolutely no idea what he was talking about:

Public health needs restrictions
It is time for a taste of its own medicine
By Vinay Prasad MD MPH | February 26, 2022
Just yesterday, I read that NYC public schools will remove the OUTDOOR mask mandate starting Monday. How Brave!
Let’s reflect on this for a moment. NYC school district has been requiring children wear masks OUTSIDE all this time. Years after we knew the virus almost never spreads outside. During recess when kids play, forced to wear a mask while exerting themselves. Wow!
Whoever made the policy is an idiot. No way around it. They are not fit for policymaking. They abused the power of government to coerce children (at incredibly low risk of bad outcomes) to wear a mask in a setting where the virus simply does not spread. In other words, they participated in something done in the name of public health, which actually made human beings worse off. Worse, they used coercive force to do it.
Post-COVID we need to seriously talk about setting restrictions. But not on people. We need to place restrictions on public health and things done in the name of public health. We cannot allow individuals who are poor at weighing risk and benefit and uncertainty to coerce human beings, disproportionately the young and powerless (waiters/ servers) to participate in interventions that have no data supporting them, for years on end.
Public health be the subject of restrictions; a taste of its own medicine. Some of those restrictions should be placed on governments, but others on private actors who are appealing to public health. Here is what that might look like:
- In an emergency situation, if governments mandate or advise individual level behavioral interventions (e.g. masking), those entities should have to generate robust data in 3 months (cluster RCTs) to demonstrate efficacy, or the intervention is automatically revoked. Some may argue 3 months is too short, but if it is truly a crisis warranting emergency proclamations, then you should see a signal in 3 months, and governments can expand sample size to ensure prompt results.
- If a trial is positive that does not mean the policy continues forever, but must be debated (net benefit/ net harms/ tradeoffs) by the body politic.
- Private entities should be prohibited from mandating emergency drug products. Check out this tweet by my conversation partner— VPZD PODCAST— Zubin Daminia:
Cal Academy is a museum in Golden Gate Park. Do they have any business nor ability to mandate boosters in adolescents? No, it is absurd. Two senior officials with the FDA— Gruber and Krause- resigned over this decision. Paul Offit and Luciano Boro and others have been publicly critical of boosters for young people, and Cal Academy mandates it? Cal Academy is not qualified to make this decision.
- The same is true for daycares and private schools that have already mandated kids vax 5 to 11. Should random private individuals be permitted to coerce vaccination under Emergency Use Authorization (EUA)? I believe restrictions must be put in place to prevent them from doing such a thing. Perhaps it should be explicit that it is illegal to coerce any medical product under EUA status. This would stop Cal Academy and private schools.
- The same is true for boosters. Colleges should be prohibited from mandating medical products under the auspices of EUA. What is going on right now on college campuses is astonishing foolishness.
- Hospital patients deserve a bill of rights. Prohibitions on visitation, particularly of children or older people; especially near the end of life were cruel and disgusting. Even long after PPE was adequate— into 2022— these rules continued. Patients need a bill of rights, and hospitals should face severe restrictions on their ability to banning visitors. To my knowledge the US has not— like Hong Kong— Separated a baby from her parents, but our rules are unjust.
- Do people have the right to return to the their home country? Read this excellent article about Australians trapped in India. This is an important issue.
- Who decides if schools should close? Schools are too important to permit local decision makers to close them for years on end. In the USA, this happened along partisan lines, with the most progressive cities punishing children the most. There has to be some bill of rights for kids to prevent this from happening. Schools might need to close in rare circumstances in the future, but this should be done only in extraordinary times, and no one can justify closing schools only in Democratic cities. Kids need a real champion, and it is not the AAP.
These are just a few examples of where governments or institutions have overreached in the name of public health, but there are many more. Post COVID, the group that needs to face the strongest restrictions is public health itself. We must careful remove the power we have granted public health, which has often been misused.
Vinay Prasad MD MPH is a hematologist-oncologist and Associate Professor in the Department of Epidemiology and Biostatistics at the University of California San Francisco. He runs the VKPrasad lab at UCSF, which studies cancer drugs, health policy, clinical trials and better decision making. He is author of over 300 academic articles, and the books Ending Medical Reversal (2015), and Malignant (2020).
How seasonality affects the spread of a new virus
Professor Sunetra Gupta explains the concept of herd immunity threshold and how seasonality affects the way a virus spreads.
Collateral Global | February 16, 2022
Transcript
Many viruses are better able to spread at particular times of the year. How does this seasonality in transmission affect the way that a new virus will spread through the population?
In order to answer this question, we need to first understand the concept of a herd immunity threshold.
Herd immunity refers to the accumulation of immune individuals in a population.
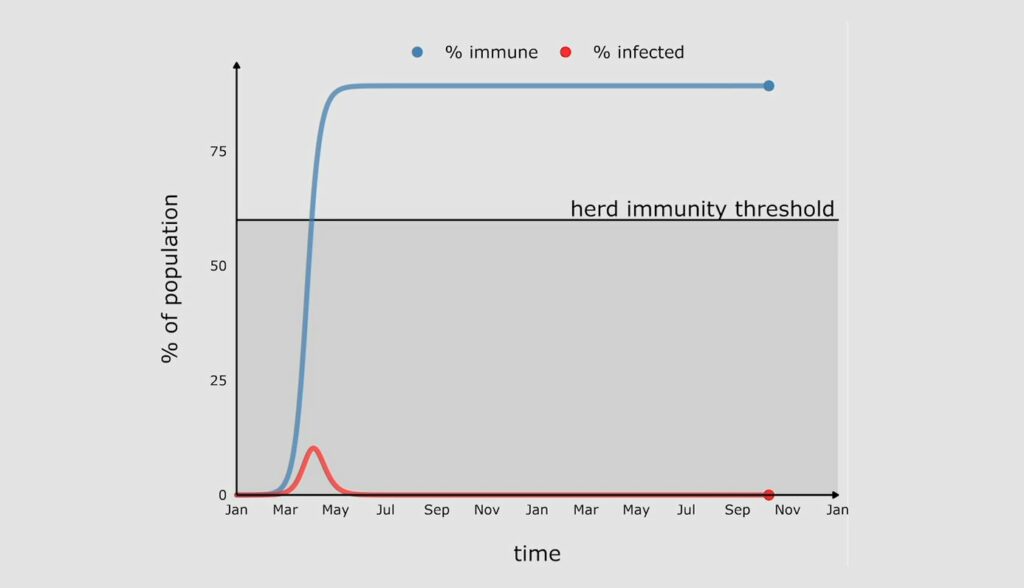
When a new virus enters a population, it muddles along for a while, and then it really starts to take off, as you can see here in this red line, which is tracking the proportion of the population infected by this new virus. And as you can see, after a while, this peaks, and the proportion infected starts to come down again.

Now why does that happen? This is because once people recover from infection, they become immune, and this means that the virus starts to run out of susceptible people to infect. The blue line here is showing you how the proportion immune is growing at the same time.
There comes a point when the proportion of the population immune is high enough that the rate of growth of infection become negative, and that’s when the virus hits peak and the infections start to decline. This occurs when the proportion of the population immune has crossed a threshold, which is known as the herd immunity threshold. That herd immunity threshold is determined by the fundamental transmissibility of the pathogen itself.
If there’s no loss of immunity, the proportion immune, this blue line, will stay above the herd immunity threshold, which means that no new epidemics can occur and the virus will die out.
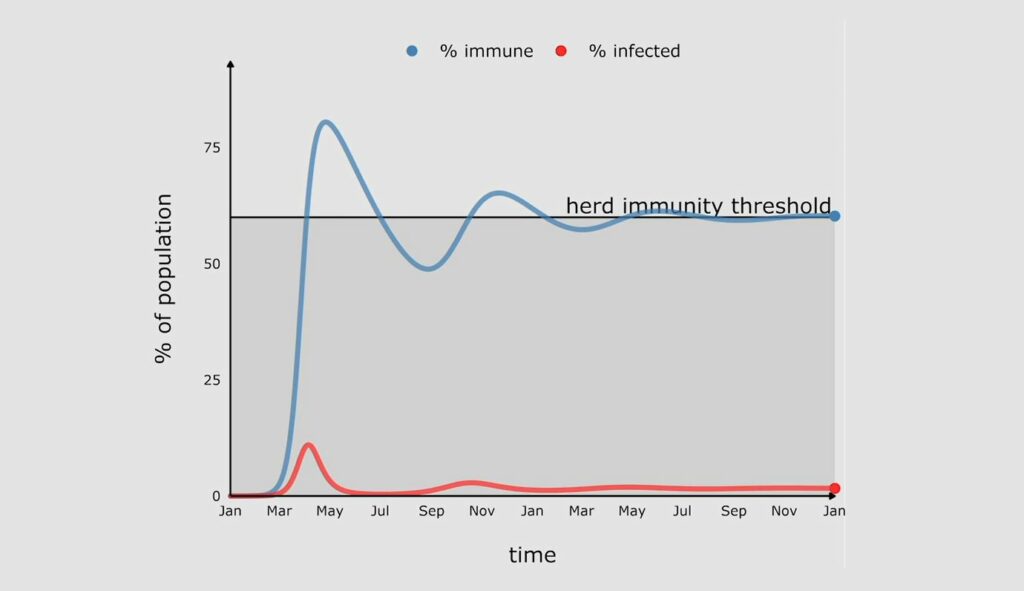
In reality the proportion immune will decline with time. For viruses like measles which give you lifelong immunity against infection, this will happen at a very slow pace. For many other viruses, like the coronaviruses, immunity against infection declines on a much shorter timescale. And as soon as it dips below the herd immunity threshold, infections will start to climb again, and we will see a second wave.

The second wave is smaller than the first wave because this time the gap between the proportion immune and the herd immunity threshold is much smaller and therefore more quickly closed.
The other thing to note about the second wave is that many infections are actually reinfections, so people who’ve lost immunity are becoming infected again. What this means is that the rates of severe disease and death are likely much lower, because people will retain the ability to resist disease even though they have lost their ability to resist infection.
Further waves will occur when the proportion immune falls below the herd immunity threshold again, but the gaps will get smaller and smaller and the waves will get smaller and smaller until they sort of flatten out at an endemic equilibrium.
Now let’s go back to our original question. What happens if there is seasonality in transmission?
As I’ve just explained, the herd immunity threshold is strongly dependent on the transmissibility of the virus, so as the transmissibility goes up and down with seasons, so will the herd immunity threshold. And that’s what’s show here by the gradated area.

So now you see a more complex picture emerging which is the result of an interaction between waning immunity and the changes in the herd immunity threshold.
After the first peak, immunity wanes, but because the herd immunity threshold is also declining it takes longer for the blue line to dip below the herd immunity threshold. And so the next peak is delayed. Eventually this settles into a pattern which is characteristic of the seasonal respiratory viruses which we live with at endemic equilibrium.
Without seasonality it doesn’t make much of a difference at what time of the year the virus arrives. But when you have seasonality in transmission, it makes a really big difference.
A virus that arrives just before peak season will have a very big first wave, because the proportion immune will have to reach a very high herd immunity threshold before we see a decline in infections.

But if the virus arrives in a low season, the first wave could be quite small because the proportion immune only has to reach that lower herd immunity threshold before a turning point occurs.

However, as the herd immunity threshold starts to climb again, we will get a second wave in order to catch up with the new higher herd immunity threshold. And in some instances this could actually be larger than the first wave.
Of course the virus could arrive at different times of the year in different regions of the same country. What that means is lumping all these patterns together can be quite misleading.
Eventually all viruses will reach a state of endemic equilibrium, but their journey to that state from the point of introduction depends crucially on the rate at which infection blocking immunity decays for that particular virus as well as seasonality in transmission.

Sunetra Gupta is Professor of Theoretical Epidemiology in the Department of Zoology, University of Oxford and a member of Collateral Global’s Scientific Advisory Board.
A short history of laboratory leaks and gain-of-function studies
By Professor Paul R. Goddard | GM Watch | February 19, 2022
Two myths have hindered investigations into the origins of the SARS-CoV-2 virus: one, that viruses seldom escape from laboratories; and two, that most pandemics are zoonotic, caused by a natural spillover of a virus from animals to humans.
Promoters of the first myth include the World Health Organization (WHO). At a press conference in Wuhan, China, in February 2021, Peter Ben Embarek, the head of the WHO inspection team tasked with looking into the origins of the virus, said it was “extremely unlikely” that it had leaked from a lab and as a result the lab escape hypothesis would no longer form part of the WHO’s continuing investigations.[1]
Dr Peter Daszak, president of the EcoHealth Alliance, has promoted both myths. As long ago as 2012, Dr Daszak co-authored a paper in The Lancet claiming that “Most pandemics – e.g. HIV/AIDS, severe acute respiratory syndrome, pandemic influenza – originate in animals”.[2] Since the start of the pandemic, he has claimed that “lab accidents are extremely rare”, and that they “have never led to large scale [disease] outbreaks”. He also said that suggestions that SARS-CoV-2 might have come out of a lab are “preposterous”, “baseless”, “crackpot”, “conspiracy theories”, and “pure baloney”.[3]
In September 2020 Dr Anthony Fauci, director of the US National Institutes of Health’s (NIH) National Institute of Allergy and Infectious Diseases (NIAID), and his co-author wrote in a paper about COVID’s origins, “Infectious diseases prevalent in humans and animals are caused by pathogens that once emerged from other animal hosts.”[4] Fauci has tried to quash the notion that SARS-CoV-2 could have come from a lab. In May 2020 he said that the virus “could not have been artificially or deliberately manipulated” and in October 2020 that year that the lab leak theory was “molecularly impossible”.[5]
But emails uncovered this year by a Freedom of Information request in the US reveal a wide gap between what Fauci was being told by experts about the virus’s origins and what he was saying publicly. In January 2020, a group of four virologists led by Kristian G. Andersen of the Scripps Research Institute told Fauci that they all “find the genome inconsistent with expectations from evolutionary theory”[6] – in other words, it likely didn’t come from nature and could have come from a lab.
Fauci hastily convened a teleconference with the virologists on 1 February 2020.[7] As the New York Post reported, “Something remarkable happened at the conference, because within three days, Andersen was singing a different tune. In a Feb. 4, 2020, email, he derided ideas about a lab leak as ‘crackpot theories’ that ‘relate to this virus being somehow engineered with intent and that is demonstrably not the case’.”[8]
Andersen and his colleagues then published an article on 17 March 2020 in the journal Nature Medicine that declared, “Our analyses clearly show that SARS-CoV-2 is not a laboratory construct or a purposefully manipulated virus.”[9] The article was highly influential in persuading the mainstream press not to investigate lab leak theories.[10]
While the emails do not prove a conspiracy to mislead the public, they certainly make it more plausible. Just one day after the teleconference at which his experts explained why they thought the virus seemed manipulated, Francis Collins, then-director of the NIH, complained about the damage such an idea might cause.
“The voices of conspiracy will quickly dominate, doing great potential harm to science and international harmony,” he wrote on 2 February 2020, according to the emails.[11]
But there is another reason why Fauci and Collins might not want the lab leak idea to take hold. Dr Daszak’s EcoHealth Alliance had channelled funding from the NIH’s NIAID to the Wuhan Institute of Virology (WIV) in China, for dangerous gain-of-function (GoF) research on bat coronaviruses. So money from organisations headed by Fauci, Collins, and Daszak funded research that could have led to the lab leak that some believe caused the pandemic.[12]
While it should have been clear from the beginning that Drs Fauci and Daszak have strong vested interests in denying the lab leak theory, until recently their assertions were taken as objective fact by most science writers and media.
But a brief look at the history of lab leaks and the origins of pandemics confirms that their claims are highly misleading. Research shows that the escape of viruses from laboratories and supposedly contained experiments, such as vaccine research and programmes, is a common occurrence. In addition, many pandemics have arisen from lab escapes and almost all have not been directly zoonotic. Even when viruses do ultimately originate in animals and make the jump into humans, they mostly fester in a separated community of human beings for many years – centuries or millennia – before spreading during abnormal movements of people due to wars and famines.
What is GoF research?
In its broadest definition, GoF research provides a virus or other microbe with a new function, such as making it more virulent or transmissible, or widening its host range (the types of hosts that the organism can infect).[13] Through GoF, researchers can create new diseases in the laboratory.
GoF can be achieved by any selection process that results in changes in the genes of the organism and as a result, its characteristics. One example of such a process is passing a virus through different animal cells, which can result in a loss of function (weakening it) or a gain of function (making it more able to replicate in a new host species). The researcher can then select the altered organism, depending on the purpose of the research.
In the last decade, GoF researchers have used genetic engineering to directly intervene in the genome of viruses to enhance a desired function.
But long before GoF studies involving deliberate genetic alteration, researchers had started to experiment with widening the host range of certain viruses, in order to develop vaccines. Often these experiments had unintended outcomes, including causing outbreaks of the disease being targeted.
Smallpox
An example is the development of the smallpox vaccine. Most of us are aware of how Edward Jenner in 1796 put cowpox to work in a new way, to infect humans. This led to the successful vaccination programme that eventually eliminated smallpox from the world.
But what many people do not know is that the experiments of 1796 were not his first attempts at using an animal pox in humans. His first subject was his baby son, who had been born in 1789. He inoculated the lad with swinepox and later tested the inoculation’s effectiveness with smallpox. As Greer Williams pointed out in the book Virus Hunters, “The best we can say for this experiment is that it muddied the water… whether the experimental infections had anything to do with [the son’s] mental retardation it is impossible to say.”[14]
Vaccination does not give immunity from smallpox for life: A booster is required every few years. The last person to die from smallpox was Janet Parker, a photographer who worked on the floor above a lab in Birmingham, UK, where research on the virus was being conducted. She had been vaccinated against smallpox in 1966 but contracted the disease in 1978 when the virus escaped from the lab by an unknown route. She died some days later (see Table 1).
Introducing a virus or other microbe to a new host has historically been associated with problems. Before Jenner, inoculation with variola minor (smallpox from a sufferer with minor disease), had been used as a preventive measure in China as early as the tenth century.[15] Variolation, as it was termed, was introduced to the UK in 1717, but is reported to have killed 1 in 25. So Jenner’s experiments have to be viewed in the light of the contemporary practice, which was killing 4% of those inoculated.
What is more, as Greer Williams noted, variolation was an “excellent way of spreading the disease and starting new epidemics”.[16]
Yellow fever
In 1900 the French had given up on building the Panama Canal due to yellow fever decimating the workers. Eventually the disease was conquered in the region by a mosquito eradication programme based on the experiments of the US Army surgeon Major Walter Reed.[17] This success was crucial to the completion of the project in 1914.
But what is often forgotten is that a series of doctors and laboratory workers died trying to combat yellow fever. In 1900 Dr Jesse W. Lazear was the first researcher to die from yellow fever after he apparently allowed himself to be bitten by an infected mosquito as part of his experiments.[18] Between 1927 and 1930, yellow fever caused 32 laboratory infections, killing five people.[19]
As the research into viruses continued, so did the infection rate amongst the researchers and the death toll of researchers and those inoculated against diseases rose. I do not doubt that the final outcome was to the good of mankind, but occasionally a “vaccine” would go spectacularly wrong.
Polio
In the 1930s, 40s and 50s the infection that seemed to most frighten Western society was poliomyelitis. Perhaps it was because unlike with most infectious diseases, cleanliness did not seem to be a protection and exercising could be positively harmful. In fact polio struck those who were healthy and wealthy and was worse if the person was fit and active. Much effort was put into finding a vaccine and among the first to succeed was Dr Jonas Salk. There had been abortive attempts in the 1930s but the 1935 vaccination programme had actually killed people.
Salk was a meticulous researcher and his technique was excellent. Unfortunately this was not the case with all of the laboratories that prepared the vaccine for public use. In particular, the Cutter Laboratories failed to kill the virus and poliomyelitis was spread by their version of the Salk vaccine, paralysing and killing the recipients. Eventually the proper controls permitted the successful rollout of the killed vaccine. It was later replaced by an attenuated polio virus vaccine, which has nearly eliminated polio from the world. It will not, however, succeed in completely eliminating the disease, as the attenuated virus can revert to a wild form. Thus the final push may require the use, once again, of the killed virus polio vaccine.
The infection of laboratory workers with the microbes they were working on was so common that steps were introduced in the 1940s to prevent escape of the organisms. According to Wikipedia, the first prototype Class III (maximum containment) biosafety cabinet was fashioned in 1943 by Hubert Kaempf Jr., then a US Army soldier.[20] The regulations were enhanced and the escape of dangerous organisms decreased, but has never disappeared. This is clearly demonstrated in Table 1, which lists some, but by no means all, of the known lab leaks since the 1960s.
Escapes from bioweapons facilities
Whilst all of the incidents in the table are of interest, some are more worrying than others. In 1971 and 1979 there were outbreaks of smallpox and anthrax in the Soviet Union, caused by escapes of weaponised smallpox and weaponised anthrax from their own bioweapons facilities. In 1977 it is believed that a laboratory somewhere on the border of China and Russia put the H1N1 virus back together and it escaped and caused at least two pandemics. SARS1, which erupted first in 2003, later escaped from laboratories six times, four of which were in China, plus Singapore and Taiwan.[21]
The more you look at the table, the more you wonder if there is any virus that has not at some time escaped from a laboratory. Laboratory workers have told me that it is common for technicians to become infected with the organisms they are working with and their usual response in the past has been to take multivitamins and hydroxychloroquine.

Table 1: Some serious leaks of viruses from laboratories[22]k
The recent history of gain-of-function studies
Since 2010, GoF studies have increasingly focused on finding out whether non-pathogenic strains of viruses could be made infective and harmful to human beings.[23] This was supposedly in order to know whether or not the microbe was likely to be hazardous to human beings and then, if it was, devise vaccines and drugs against it.
In my opinion, such work simply increases the sum total of different pathogens that can affect human beings. When medical doctors are made aware of this type of research, they are usually speechless at the stupidity that anybody would contemplate doing such work. I now call such studies Make Another Disease (MAD) research.
This type of MAD research dramatically increased in laboratories in the USA between 2012 and 2014. The resulting accidents in which small outbreaks of novel viral diseases occurred led to three hundred scientists writing to the Obama administration asking for GoF to be stopped. The US Government responded by announcing a pause on the research in 2014 because of the inherent dangers.[24]
In the same year Dr Fauci, whose recorded belief was that the studies were worth the risk,[25] gave money from the NIH to Dr Daszak of Ecohealth Alliance to continue GoF research on coronaviruses.[26] This was carried out at the Wuhan Institute of Virology using genetically engineered humanized mice, culminating in reports in 2017 and 2018 that the researchers had successfully made harmless coronaviruses pathogenic to humans.[27]
In the autumn of 2019 the Covid-19 pandemic of SARS-2 started in Wuhan and, to date, over five million people across the world have died from the virus.
Are pandemics ever zoonotic?
In addition to stating erroneously that viruses only rarely escape from laboratories and/or that SARS-Cov-2 was unlikely to have done so, Drs Daszak and Fauci hold that most pandemics are zoonotic in origin. They say that pandemics start from a disease spreading from an animal but they do not state the time period involved. I would suggest that pandemics never occur from the immediate spread from an animal. In order for a pandemic to occur, a reservoir of the infection, adapted to human beings, must develop. This usually takes many years. Moreover the spread usually occurs due to the unnaturally large movement of people that occurs due to wars and famines.
I will give just a couple of well known examples.
When the Europeans invaded the Americas, 90% or more of the indigenous people of America died from the introduced diseases, which included measles, smallpox and mumps. In return, syphilis spread to Europe. Yes, the diseases had all arisen from animals initially, but the adaptation to make them pathogenic enough to cause a pandemic must have occurred over a period of the several thousand years during which the populations of Europe and America were separated.
AIDS was discovered in the early 1980s and it was soon clear that the Human Immunodeficiency Virus had arisen from the Simian Immunodeficiency Virus. However, studies have concluded that the first transmission of SIV to HIV in humans took place around 1920 in Kinshasa in the Democratic Republic of Congo (DR Congo),[28] so that it had at least 40–50 years of sporadic infection of human beings before it started to spread round the world as a pandemic. During that time there were many local wars in Africa and, of course, the 2nd World War.
In my book PANDEMIC, I document the world’s worst pandemics and conclude that it is only malaria that seems to be indifferent to wars, killing people whether or not there are hostilities. All other historical pandemics have at least some connection with war and occur when isolated groups with an endemic disease meet another group without the disease.
Conclusion
Thus historically we come to an impasse with SARS-CoV-2. This arose in a city many miles away from an animal population that might have harboured a similar virus, at a time when the supposed original host was dormant (late autumn), near a laboratory known to be working on the viruses. It then spread from person to person at an alarming rate and was seen to be totally adapted to human beings, to the extent that it was unable to even infect the bat it was supposed to have arisen from.
As a person who has studied the history of pandemics and lab leaks, imagine my surprise when authorities, not only in China but also in the USA and UK, stated categorically that the virus was obviously zoonotic and we were conspiracy theorists if we proposed the opposite. I had to conclude that they were misguided or purposely lying.
References
1. Matthews J (2021). WHO investigation descends into farce in rush to rule out a lab leak. GMWatch. 10 Feb. https://www.gmwatch.org/en/news/archive/2021-articles2/19691
2. Morse SS et al (2012). Prediction and prevention of the next pandemic zoonosis. The Lancet 1-7 Dec; 380(9857):1956–1965. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3712877/
3. Matthews J (2020). Why are the lab escape denialists telling such brazen lies? GMWatch. 17 Jun. https://gmwatch.org/en/news/archive/2020-articles/19437
4. Morens DM, Fauci AS (2020). Emerging pandemic diseases: How we got to COVID-19. Cell 182. 3 Dec. https://www.cell.com/cell/pdf/S0092-8674(20)31012-6.pdf
5. Chaffetz J (2022). Fauci, Feds tried to quash COVID lab leak origin theory – protecting Chinese interests over American lives. Fox News. 27 Jan. https://www.foxnews.com/opinion/fauci-covid-lab-leak-origin-theory-china-jason-chaffetz
6. Wade N (2022). Emails reveal scientists suspected COVID leaked from Wuhan lab – then quickly censored themselves. New York Post. 17 Feb. https://nypost.com/2022/01/24/emails-reveal-suspected-covid-leaked-from-a-wuhan-lab-then-censored-themselves/
7. Carlson J, Mahncke H (2021). Behind the scenes of the natural origin narrative. Epoch Times. 30 Sep. https://www.theepochtimes.com/behind-the-scenes-of-the-natural-origin-narrative_4023181.html
8. Wade N (2022). As above.
9. Andersen KG et al (2020). The proximal origin of SARS-CoV-2. Nature Medicine 26:450–452. 17 Mar. https://www.nature.com/articles/s41591-020-0820-9
10. Wade N (2022). As above.
11. Wade N (2022). As above.
12. Lerner S, Hvistendahl M, Hibbett M (2021). NIH documents provide new evidence US funded gain-of-function research in Wuhan. The Intercept. 10 Sep. https://theintercept.com/2021/09/09/covid-origins-gain-of-function-research/
13. Board on Life Sciences et al (2015). Gain-of-function research: Background and alternatives. In: Potential Risks and Benefits of Gain-of-Function Research: Summary of a Workshop. National Academies Press (US). Apr 13. https://www.ncbi.nlm.nih.gov/books/NBK285579/
14. Williams G (1959). Virus Hunters. Knopf.
15. Goddard PR (2020). PANDEMIC: Plagues, Pestilence and War: A Personalised History. Clinical Press. https://www.amazon.co.uk/PANDEMIC-Paul-Goddard-MD-FRCR/dp/1854570994
16. Williams G (1959). Virus Hunters. As above.
17. Feng P (undated). Yellow fever. National Museum of the United States Army. https://armyhistory.org/major-walter-reed-and-the-eradication-of-yellow-fever/
18. College of Physicians of Philadelphia (undated). Jesse Lazear. https://www.historyofvaccines.org/content/jesse-lazear
19. Berry GP and Kitchen SF (1931). Yellow fever accidentally contracted in the laboratory: A study of seven cases. The American Journal of Tropical Medicine and Hygiene s1–11(6):365–434. https://www.ajtmh.org/view/journals/tpmd/s1-11/6/article-p365.xml
20. Wikipedia (undated). Biosafety level. https://en.wikipedia.org/wiki/Biosafety_level#:~:text=The%20first%20prototype%20Class%20III,Laboratories%2C%20Camp%20Detrick%2C%20Maryland.
21. Mihm S (2021). The history of lab leaks has lots of entries. Bloomberg. 27 May. https://www.bloomberg.com/opinion/articles/2021-05-27/covid-19-and-lab-leak-history-smallpox-h1n1-sars
22. Sources:
* 1967 https://www.who.int/news-room/fact-sheets/detail/marburg-virus-disease
* 1966 and 1978 https://en.wikipedia.org/wiki/1978_smallpox_outbreak_in_the_United_Kingdom
* 1971 Aral smallpox incident: https://en.wikipedia.org/wiki/1971_Aral_smallpox_incident; 1973 https://api.parliament.uk/historic-hansard/written-answers/1973/apr/12/smallpox
* 1977, 1979 The history of lab leaks has lots of entries: https://www.bloomberg.com/opinion/articles/2021-05-27/covid-19-and-lab-leak-history-smallpox-h1n1-sars
* 2003-2017 Breaches of safety regulations are probable cause of recent SARS outbreak, WHO says BMJ. 2004 May 22; 328(7450): 1222 and The Origin of the Virus (Clinical Press, Bristol) 2021;
* 2007 https://en.wikipedia.org/wiki/2007_United_Kingdom_foot-and-mouth_outbreak
* 2015 US military accidentally ships live anthrax to labs. https://doi.org/10.1038/nature.2015.17653
23. Herfst S et al (2012). Airborne transmission of influenza A/H5N1 virus between ferrets. Science 336(6088):1534-41. https://pubmed.ncbi.nlm.nih.gov/22723413/
24. The White House (2014). Doing diligence to assess the risks and benefits of life sciences gain-of-function research. 17 Oct. https://obamawhitehouse.archives.gov/blog/2014/10/17/doing-diligence-assess-risks-and-benefits-life-sciences-gain-function-research
25. Fonrouge G (2021). Fauci once argued for risky viral experiments – even if they can lead to pandemic. New York Post. 28 May. https://nypost.com/2021/05/28/fauci-once-argued-viral-experiments-worth-the-risk-of-pandemic/ ; Barnard P, Quay S, Dalgleish A (2021). The Origin of the Virus. Clinical Press.
26. NIH (2014). Understanding the Risk of Bat Coronavirus Emergence. Project Number 1R01AI110964-01. https://reporter.nih.gov/search/-bvPCvB7zkyvb1AjAgW5Yg/project-details/8674931
27. Barnard P, Quay S, Dalgleish A (2021). The Origin of the Virus. Clinical Press.
28. Avert (2019). Origin of HIV and AIDS. https://www.avert.org/professionals/history-hiv-aids/origin
About the author: Professor Paul R Goddard BSc, MBBS, MD, DMRD, FRCR, FBIR, FHEA is Emeritus Professor, University of the West of England, Bristol; retired consultant radiologist; and former president of the Radiology Section of the Royal Society of Medicine. He is the author of PANDEMIC, A Personalised History of Plagues, Pestilence and War, Clinical Press Ltd, August 2020, and PANDEMIC, 2nd Edition 2021, Clinical Press, Bristol, available from Gazelle Book Services Ltd and good bookshops, ISBN 978-1-85-457105-2. On a similar theme, see The Origin of the Virus, Clinical Press 2021.
The above article is adapted from material that was first presented as the Long Fox lecture to The Bristol Medico-Chirurgical Society and Bristol University (2017) and to the British Society for the History of Medicine Biennial Congress (September 2021).
Featured Video
Deep Dive Intel Briefing 6/20/2026 Lt Col Daniel Davis
or go to
Aletho News Archives – Video-Images
From the Archives
As Hillary Clinton kisses up to Henry Kissinger, RT looks at 4 of his most heinous acts
RT | September 3, 2016
… While Clinton retains the ultimate warmongering seal, RT examines some of Kissinger’s most memorable acts… Read full article
Blog Roll
 Aletho News
Aletho News- Terms of US capitulation to Iran presage new era for the region
- Strategic Oil Reserve Nears Collapse… US Must Choose: Guns or Butter
- The Story the Media — and the Government — Don’t Want You to Hear
- Deep Dive Intel Briefing 6/20/2026 Lt Col Daniel Davis
- The Targeted Assassination of Studies Showing Vaccines Cause Injury
- BMJ Probe Into Excess Mortality Study Drags On for Two Years With No Resolution
- Securing Peace with Iran Compels Trump to Divorce Israel
- Old Iraq war architects rise up to wag finger at Trump’s Iran deal
- Strait of Hormuz closed over Israeli aggression on Lebanon
- Keir Starmer arson mysteries multiply
- If Americans Knew
- ‘Reproductive genocide’ in Gaza; death toll in Lebanon tops 4,000 (during a ceasefire) – Daily Update
- Israelis Invaded Lebanon And Then Cried Victim When Their Soldiers Got Killed
- FARA Docs: Israel is Spying On Millions Of Christian Americans In Their Churches
- Why US presidents from both parties end up cursing Benjamin Netanyahu
- Israel Asked Facebook to Censor Iran War Content, Internal Documents Show
- Deaths in Gaza undercounted, possibly by 100s of thousands; “Psychopath” Ben-Gvir talks trash – Daily Update
- UNICEF: “Trauma is woven into the very fabric of childhood in Gaza”
- 15 articles a day: The extent of the Israeli army’s media interference
- Greek Orthodox Patriarchate denounces Israeli seizure of church land in Jerusalem
- How Hillel International uses antisemitism training and ‘campus climate’ concerns to attack Palestine solidarity
- No Tricks Zone
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
