Did Federal Censors Swing the 2020 Election?

By Jim Bovard | The Libertarian Institute | November 14, 2022
Did the Russiagate conspiracy entitle the federal government to censor Americans forever? Did federal shenanigans swing the 2020 election? A new report reveals how a new federal agency and federal grantees exploited a 2016 scam to launch the greatest covert censorship campaign in U.S. history.
In 2016, top FBI officials and the Obama administration fueled a conspiracy that the Trump presidential campaign was colluding with the Russian government. Numerous false FBI claims spurred a massive wiretapping operation approved by the Foreign Intelligence Surveillance Court. The allegations led to the appointment of Special Counsel Robert Mueller, who spent two years investigating before admitting that there was nothing to prosecute for his primary charge. But by that point, Trump had been irredeemably tainted and the Democrats had exploited the controversy to capture control of the U.S. House of Representatives in 2018.
Thanks to Russiagate, Congress created a new federal agency in 2018—the Cybersecurity Infrastructure Security Agency (CISA) in the Department of Homeland Security (DHS). CISA was purportedly intended to fight foreign threats to election security and U.S. infrastructure. But the agency quickly shifted its target to American citizens. As a report last week from the Foundation for Freedom Online (FFO) revealed, “Any U.S. citizen posting what DHS considered misinformation’ online was suddenly conducting a cyber attack against US critical infrastructure.”
CISA and DHS realized that they could not directly muzzle Americans so they colluded with a number of federal grantees who comprised the Election Integrity Project, a coalition formed in mid-2020. The result was “censorship by proxy,” as law professor Jonathan Turley observed, bludgeoning social media companies into submission. The DHS-spurred crackdown in 2020 resulted in the suppression of “22 million tweets labeled ‘misinformation’ on Twitter” and “hundreds of millions of individual Facebook posts, YouTube videos, TikToks, and tweets impacted” thanks to changes that would not have occurred without “‘huge regulatory pressure’ from government,” FFO reported.
Once the government claims a prerogative to censor “misinformation,” the definition of misinformation mushrooms to serve political purposes. The Election Integrity Partnership bragged about how social media posts were targeted that were merely purportedly guilty of offenses such as “exaggerate issue,” “misleading stats” and “out of context.” Many of those alleged factual infractions were piddling compared to the sweeping falsehoods continually uncorked by presidential candidates Trump and Biden.
Prior to the 2020 election, “the censorship focus was always and consistently foremost targeted at speech casting doubt on mail-in ballots,” FFO reported. Democrats exploited the COVID-19 pandemic to push through electoral changes that opened the floodgates to unverified mail-in ballots. Some states like Michigan sent absentee ballots to all voters, violating the Election Clause of the Constitution (which specifies that state legislatures make the rules for federal elections).
Election regimes that scrutinized mail-in ballots routinely had a high rejection rate. New York City relied on mail-in ballots for a June 2020 primary that the New York Daily News derided as a “dumpster fire.” Up to 20% of ballots “were declared invalid before even being opened, based on mistakes with their exterior envelopes,” The Washington Post noted, thanks largely to missing postmarks or signatures. Trump claimed that the shift to mail-in ballots could result in “the most corrupt vote in our nation’s history.”
But federal string-pulling minimized controversies. FFO noted, “Pre-censoring U.S. citizen debate about mail-in ballots five months before an election has the impact of devastating the ability of concerned citizens to pressure their state representatives to take legal action on changing voting procedures.” Rather than the traditional scrutiny for mail-in ballots, many locales defaulted to accepting practically any piece of paper with a mark. Mail-in ballots determined the outcome of the 2020 election. Trump received more votes on Election Day but 43,000 mail-in ballots in three states sealed Biden’s victory—a minuscule portion of the tens of millions of mail-in votes he received.
In a July 28, 2020 article for the American Institute for Economic Research, I warned that the controversies over mail-in ballots could lead to “the death of political legitimacy…Deep State federal agencies are a Godzilla that have established their prerogative to undermine if not overturn election results.”
Until I read the new FFO report, I did not realize that “the biggest category for [2020] censorship was ‘delegitimization’… defined to mean any speech that ‘casts doubt’ on any kind of election process, outcome or integrity issues [which] made all conservative and populist criticism of the administration of the election pre-banned at the narrative level, five months in advance of Election Day.” Damn, no wonder that article of mine got so little traction on Twitter and Facebook! “Delegitimization” resulted in “72% of its censorship tickets and targeted over 99% of the posts throttled by narrative during the 2020 election.”
The entire process looks like a Monty Python parody of democracy. As Mike Benz, the former State Department official who heads FFO, observed, “The same obscure DHS subagency tasked with election security also gained the power to censor any questions about election security.”
How much impact did federal censorship and suppression have on the most recent elections? The Election Integrity Project browbeat tech companies to accept “that social media posts about the 2022 elections be censorable under a low bar of simply ‘misleading,’” according to FFO. For the midterm elections, “the Election Integrity Project is tightly monitoring and working to censor ‘discussions surrounding the delays in counting ballots’ being ‘framed as fraud,’” FFO reported. Damned convenient considering the debacle in Arizona—which was foreseen if not foreordained. In a Washington speech just before the election, President Biden told listeners that “in some cases we won’t know the winner…until a few days after the election. It takes time to count all legitimate ballots in a legal and orderly manner.” Biden stressed that citizens must be “patient. That’s how this is supposed to work.”
But it never consistently worked that way before in American history. Arizona’s voting machines dismally failed on Election Day and Democrats are vehemently resisting a hand recount of all ballots.
The real goal is to control Americans’ minds—and not just on Election Day. Jen Easterly, the NSA honcho who Biden chose to run CISA, declared that “the most critical infrastructure is our cognitive infrastructure, so building that resilience to misinformation and disinformation… is incredibly important.” And the most important cognitive “fix” is to train Americans to never doubt Uncle Sam. In a March 2022 meeting with top Twitter executives, FBI official Laura Dehmlow “warned that the threat of subversive information on social media could undermine support for the U.S. government,” The Intercept recently reported. The FBI has 80 agents on a task force to curb “subversive data utilized to drive a wedge between the populace and the government.”
“Disinformation” is often simply the lag time between the pronouncement and the debunking of government falsehoods. If the feds can censor most if not almost all of their online critics, their cons become almost irrefutable. Perhaps that is the only way that many federal policies can retain any shard of legitimacy. As Mike Benz warns, “DHS is carrying out an official state policy that if public trust is not earned, it must be installed.” That is a recipe for the death of democracy.
Jim Bovard is the author of Public Policy Hooligan (2012), Attention Deficit Democracy (2006), Lost Rights: The Destruction of American Liberty (1994), and 7 other books. He is a member of the USA Today Board of Contributors and has also written for the New York Times, Wall Street Journal, Playboy, Washington Post, and other publications. His articles have been publicly denounced by the chief of the FBI, the Postmaster General, the Secretary of HUD, and the heads of the DEA, FEMA, and EEOC and numerous federal agencies.
US aid to Ukraine ‘invested’ in crypto FTX scheme

Free West Media | November 14, 2022
The sudden collapse of a crypto exchange linked to the Democratic Party in the US, has revealed that FTX presently suffers from $10-$50 billion in liabilities and virtually no assets. And among those liabilities, are “investments” made by Ukraine’s leadership clique.
The company FTX, in its bankruptcy filing appears to have held tens-of-billions in American “military aid” to Ukraine. Instead of using the alleged funds to fight Russia, the money was ‘invested’ in the FTX Ponzi scheme.
From the bankruptcy filing it is clear that this money has now disappeared.
“Instead of using US military aid to fight Russia, Ukraine ‘invested’ part or all of it, into FTX, and right now, it looks like all the money’s gone,” said Hal Turner, a well-known American radio host.
The crypto money from unsuspecting clients was also used to fund the Democratic Party in the United States. More evidence has surfaced suggesting that the funds may have been stolen.
The CEO of FTX, Sam Bankman-Fried, was one of the top donors to the Democrats, with only George Soros outperforming his largesse. Recently, he also shared a podium with inveterate globalists Tony Blair and Bill Clinton.
According to Turner, it seems that Ukraine was receiving money from the US, and then sent it to FTX, and FTX sent it to the same Democrats, who had originally voted to send it to Ukraine. “At this hour, it appears to some observers to be pure, criminal, money-laundering, and a criminal conspiracy to violate campaign finance laws,” said Turner.
Reuters exclusively reported that the founder and CEO FTX transferred $10 billion of customer funds from FTX to the trading company Alameda Research, which is run by his girlfriend Caroline Ellison.
Sam Bankman-Fried was born in 1992 on the campus of Stanford University into a family of academics. Born and raised to an upper-middle-class Jewish family in California, he is the son of Barbara Fried and Joseph Bankman, both professors at Stanford Law School. His aunt Linda P. Fried is the current dean of Columbia University Mailman School of Public Health. His brother, Gabe Bankman-Fried, is a former Wall Street trader and the director of the non-profit Guarding Against Pandemics.
He was the second-largest individual donor to Democratic causes in the 2021–2022 election cycle with total donations of $39,8 million, only behind Soros. Of this, $27 million was given to Protect our Future PAC, bankrolled by Bankman-Fried.
The US Securities and Exchange Commission and the Commodity Futures Trading Commission are currently looking into whether FTX.com mishandled customer funds. Bankman-Fried is also being investigated by the US Securities and Exchange Commission for potential violations of securities rules.
False and Misleading Efficacy Claims — What is the Motivation?
Dr. Rochelle Walensky Tweeting Counterfactuals with Intent
By Peter A. McCullough, MD, MPH | Courageous Discourse | November 10, 2022
CDC Director, Rochelle Walensky, MD, MPH, for the record, continues to make false claims about the COVID-19 vaccine boosters with the apparent motivation of getting more Americans “fully vaccinated.” This is in the backdrop of an 8.4% rate of Americans over age 5 taking one of them.[i]
No matter how hard the internal pressure is at the CDC to get a “needle in every arm,” what would be such a strong motivation for Walensky to blatantly deceive Americans with such obvious counterfactual information?
She states “COVID-19 vaccines may not prevent every infection (as apparent in her personal case), but they do provide us important protection against severe illness, hospitalization, and death…”

In order for that claim to be valid by US regulations, a COVID-19 vaccine would need to reduce the risk of adjudicated COVID-19 hospitalization and death as a primary endpoint in a prospective, double blind, randomized, placebo-controlled trial. The benefit would need to be meaningful, e.g., ~20% relative risk reduction, and statistically significant, e.g., p<0.05. The conclusive study should have no significant threats to validity such as loss to follow-up. There has been no pivotal randomized trial, and no one can claim COVID-19 vaccines reduce hospitalization and death. The shortest section on the FDA Pfizer Fact Sheet is the “Benefits” section! This is given with the consent form and makes no claims about severity, hospitalization, and death.[ii]

She goes on to promote a two-month period between the last injection (presumably legacy mRNA) and the new bivalent vaccine. This schedule has never been tested and demonstrated to be safe in human beings. Even more shocking, the bivalent boosters which failed in animal studies to stop Omicron, have never been tested for safety or efficacy in human RCTs with clinical outcomes. In academic medicine and the pharmaceutical regulatory community, the question is WHY does Walensky cross the line into making false claims, an illegal act for fully FDA approved and marketed drugs/vaccines? Only senate or congressional hearings with direct questions will get the truth out of her.
Here are some possibilities: 1) she is following orders from higher governmental authorities, 2) she knows the claims are false but truly believes the only way for vaccination to work is to keep everyone vaccinated on a continuous basis no matter what the costs, 3) she is in a form of a trance or psychological state driven by fear in herself and for humanity where COVID-19 vaccination has become like a talisman with special powers and cannot be challenged. Indeed, Walensky has never comprehensively discussed safety of COVID-19 vaccination, and she has not disclosed who should NOT take a COVID-19 vaccine. So, the next time someone in your circles claims you or your loved one should take a COVID-19 vaccine to be “safe” or “protected” from serious outcomes, ask them to take a look at the consent fact sheet and read the tiny benefit section.
[i] CDC COVID Tracker, Accessed November 9, 2022
[ii] VACCINE INFORMATION FACT SHEET FOR RECIPIENTS AND CAREGIVERS ABOUT COMIRNATY (COVID-19 VACCINE, mRNA), THE PFIZER-BIONTECH COVID-19 VACCINE, AND THE PFIZER-BIONTECH COVID-19 VACCINE, BIVALENT (ORIGINAL AND OMICRON BA.4/BA.5) TO PREVENT CORONAVIRUS DISEASE 2019 (COVID-19) FOR USE IN INDIVIDUALS 12 YEARS OF AGE AND OLDER, August 22, 2022
Feds Scramble To Hide Role Of Oath Keeper’s Informant In January 6th “Insurrection”
By Eric Striker | The Main Street Tribune | November 11, 2022
A bombshell New York Times report has revealed that Greg McWhirter, the Vice President of the Oath Keepers who helped lead the group’s presence on January 6th, is an FBI informant.
Federal officials worked hard to hide McWhirter’s status as a Confidential Human Source (CHS) in the seditious conspiracy trial of Oath Keeper’s leader Stewart Rhodes and his associates, presenting their asset in public filings as a mere “witness” instead.
In a furious November 8th filing, federal prosecutors accused defense attorneys of illegally disclosing confidential discovery about McWhirter to the press. It appears that the actual way McWhirter’s status was leaked was through a clerical error by DC court employees, who accidentally published the sealed document on the docket.
Federal officials have been suppressing information on the role their assets and agents played in inciting violence at the Capitol by having them testify as witnesses in cases related to January 6th.
McWhirter, a black Sheriff’s deputy in Montana, rose through the ranks of the Oath Keepers thanks in part to his existing contacts with law enforcement as well as his race. Rhodes regularly showcased McWhirter’s black heritage as evidence that he is not racist.
The infiltrator has also courted public controversy for other legally dubious stunts over the years. During the 2016 election, he called on members of his militia to patrol voting sites in order to discourage election fraud. In a more recent incident, he aided the FBI in attempting to manufacture an Oath Keeper’s conspiracy to kill members of Antifa in Portland as retaliation for the anarchist murder of Aaron Danielson.
Following the events of January 6th, McWhirter bought a gun shop and immediately began offering steep discounts on ammo and weapons to militia members, with implications that they had to prepare for civil war.
The defense for Rhodes, et al, was planning to call McWhirter as a witness in order to expose his role as an agitator. Yet, as the FBI informant boarded the plane to travel to his scheduled court appearance, he suffered heart trouble and could not testify. He is only 40-years-old.
On social media, many are speculating that federal agents either induced his emergency health issue with drugs or, more plausible, worked with him and his physician to fake the whole thing. In light of this curious coincidence, Rhodes’ defense was forced to rest its case without being able to cross examine the agent provocateur.
This is not the first irregular development in the trial. Witnesses Rhodes’ defense planned to call who were slated to tell the court that the defendants were innocent of plotting violence at the Capitol had FBI agents visit their homes right before they were scheduled to testify. The FBI agents told them that they would legally incriminate themselves and be prosecuted if they spoke in Rhodes’ defense. This intimidation tactic proved effective, leading to witnesses taking the fifth amendment when called, much to the shock and frustration of the defense.
McWhirter was not the only person working for the FBI inside the Oath Keepers. Another black member, Abdullah Rasheed, was also exposed in court for providing information on the group’s inner workings to federal agents in the run up to January 6th.
In addition to this, the FBI appears to be preparing to thwart expected Congressional inquiries into domestic counter-terrorism operations. Journalist Julie Kelly recently reported that Christopher Wray is rushing to replace the head of its Washington Field Office, Steven D’Antuono, who has led agents in using controversial tactics across the country to entrap persons with right-wing political beliefs of all types in fictitious terror plots. D’Antuono suddenly announced his retirement despite his recent lucrative and prestigious promotion, which will make it difficult for Congress to question him on his actions under the color of law in the last three years.
The Oath Keeper’s trial, which to date is the most serious and high profile prosecution of all January 6th cases, will soon be going to jury deliberation.
Pentagon exploits post 9/11 laws to wage ‘secret wars’ worldwide: Report
The Cradle | November 9, 2022
A report released last week by the New York University School of Law’s Brennan Center for Justice details how the US Department of Defense (DoD) has been allowed to covertly deploy troops and wage secret wars over the past two decades in dozens of countries across the globe.
Among the nations in West Asia affected by these so-called ‘security cooperation authorities’ are Lebanon, Iraq, Syria, and Yemen; however, they also include many African and Latin American nations.
Known as ‘security cooperation authorities,’ they were passed by the US Congress in the years following the 11 September attacks, and are a continuation of the 2001 Authorization for Use of Military Force (AUMF), a piece of legislation that has been stretched by four successive governments.
According to the report, the AUMF covers “a broad assortment of terrorist groups, the full list of which the executive branch long withheld from Congress and still withholds from the public.”
Following in this tradition, the ‘security cooperation authorities’ being abused by the Pentagon are Section 333 and Section 127e of Title 10 of the United States Code (USC).
Section 333 authorizes the US army to “train and equip foreign forces anywhere in the world,” while Section 127e authorizes the Pentagon to “provide support to foreign forces, paramilitaries, and private individuals who are in turn supporting US counterterrorism operations,” with a spending limit of $100,000,000 per fiscal year.
However, thanks to the vague definition of ‘support’ and ‘training’ in the text of these laws, both Section 333 and Section 127e programs have been abused to target “adversarial” groups under a strained interpretation of constitutional self-defense; they have also allowed the US army to develop and control proxy forces that fight on behalf of – and sometimes alongside – their own.
As a result of this, in dozens of countries, these programs have been used as a springboard for hostilities, with the Pentagon often declining to inform Congress or the US public about their secret operations under the reasoning that the incidents are “too minor to trigger statutory reporting requirements.”
“Researchers and reporters uncovered Section 127e programs not only in Afghanistan and Iraq, but also in Cameroon, Egypt, Kenya, Lebanon, Libya, Mali, Mauritania, Niger, Nigeria, Somalia, Syria, Tunisia, and Yemen,” the report highlights.
Researchers also point out that defense authorities “have given little indication of how [they] interpret Section 333 and 127e.”
Even more concerning, and ignoring the damage caused by these ‘anti-terror’ laws, the US Congress recently expanded the Pentagon’s security cooperation authorities, particularly with Section 1202 of the National Defense Authorization Act (NDAA).
Section 1202 allows the US army to allow “irregular warfare operations” against “rogue states” like Iran or North Korea, or “near-peers,” like Russia and China.
The report comes at a time when the US army and its proxy militias are accused of illegally occupying vast regions of Syria and Yemen, looting oil from the war-torn countries, just over a year after their brutal occupation of Afghanistan ended. Moreover, a former US official on Tuesday revealed that anti-Iran militias are being armed in the Iraqi Kurdistan Region (IKR), where both the CIA and the Mossad are known to operate.
Good News on Omicron Outcomes from Prison
Captive Environment Allows Real Look at Risk for Hospitalization and Death
By Peter A. McCullough, MD, MPH | Courageous Discourse | November 8, 2022
Prisoners and staff are a prototypical congregate group amenable to epidemiologic study and in the setting of the SARS-CoV-2 outbreak, ideal for study of the patterns of spread and risk for serious outcomes.
Throughout the pandemic, review and interpretation of peer-reviewed manuscripts in widely read journals has required careful review of data in supplementary tables. The conclusions by the authors in many papers must be ignored given the heavy bias for all journals to “promote” mass vaccination. For example, thus far, there has not been a single paper in the New England Journal of Medicine that has concluded COVID-19 vaccines are unsafe, or not indicated, or do not have a favorable risk to benefit ratio.
Prior to COVID-19 for any new therapy or surgery, there are always divergent views where some papers conclude an intervention is beneficial and others do not. Disagreement is normal in medicine. The pervasive heavy-handed government intelligence community and public health agency operations have biased the medical journals to publish a one-sided story on COVID-19 vaccination. The paper by Chin et al, in the New England Journal of Medicine is a perfect example.[i] They studied 59,794 residents and 16,572 staff, using data collected from December 24, 2021, through April 14, 2022. Buried in the supplemental tables are important data on the real risk of hospitalization and death with the Omicron variant in prisoners characterized by whether they had prior COVID-19 and how many doses of a vaccine they had received.
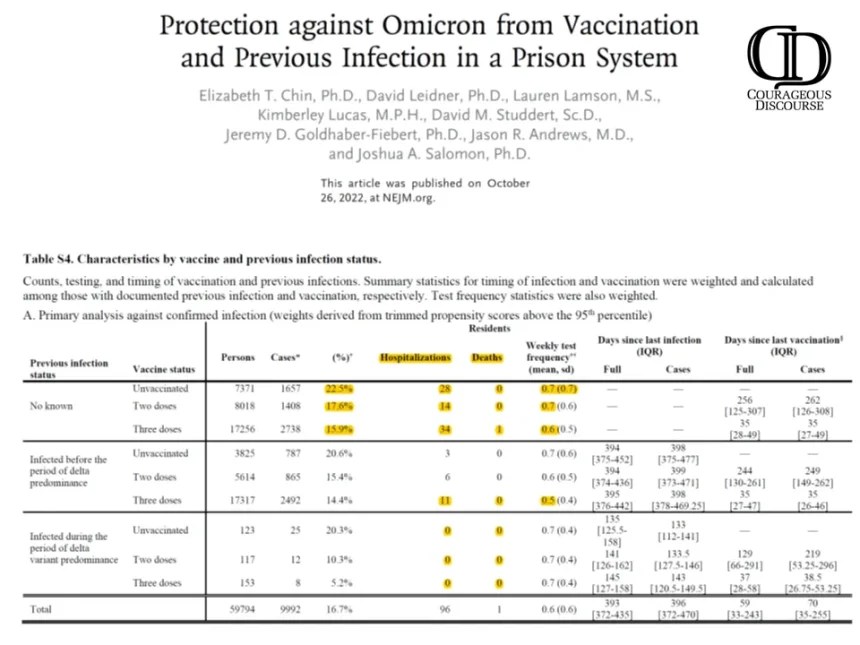
Chin ET, Leidner D, Lamson L, Lucas K, Studdert DM, Goldhaber-Fiebert JD, Andrews JR, Salomon JA. Protection against Omicron from Vaccination and Previous Infection in a Prison System. N Engl J Med. 2022 Oct 26. doi: 10.1056/NEJMoa2207082. Epub ahead of print. PMID: 36286260. Supplemental Tables.
As shown, there is a negligible risk of hospitalization and death with Omicron infection. Specifically, there were zero deaths in the unvaccinated. To demonstrate how far off-base authors and editors are on interpretation, take a look at the paper’s conclusions:
“Our findings in two high-risk populations suggest that mRNA vaccination and previous infection were effective against omicron infection, with lower estimates among those infected before the period of delta predominance. Three vaccine doses offered significantly more protection than two doses, including among previously infected persons.”
My conclusions are considering natural immunity status, COVID-19 vaccination provided no meaningful protection against hospitalization and death with Omicron. Based on these data, a rational prison physician or health administrator would conclude that bivalent boosters for Omicron are not clinically indicated nor medically necessary. So next time you see headlines regarding a journal article, look for a second opinion from “Courageous Discourse” or other reliable stacks and sources of analysis.
[i] Chin ET, Leidner D, Lamson L, Lucas K, Studdert DM, Goldhaber-Fiebert JD, Andrews JR, Salomon JA. Protection against Omicron from Vaccination and Previous Infection in a Prison System. N Engl J Med. 2022 Oct 26. doi: 10.1056/NEJMoa2207082. Epub ahead of print. PMID: 36286260.
STOP the Infanticide! 5,000% Increase in Fetal Deaths Following COVID-19 Vaccines!

The U.S. Government’s Vaccine Adverse Events Reporting System (VAERS) was updated today, and there are now 4,534 fetal deaths recorded in VAERS following COVID-19 vaccines given to pregnant and child-bearing women. (Source.)
And these recorded fetal deaths are but a fraction of the real number of unborn children who have died since the COVID-19 experimental vaccines were given emergency use authorization, as a previous report published for Department of Health and Human Services stated that fewer than 1% of all vaccine adverse events are actually reported to VAERS. (Source.)
Three of these fetal deaths have followed the new Bivalent COVID-19 booster shots from Pfizer and Moderna, including a 26-year-old woman from Arizona who developed breast cancer following the vaccine, and chose to have chemotherapy and terminate the life of her unborn child.
VAERS ID: 2447825: Began noting a breast lump 9/2021 Biopsied ER/PR + HER 2- breast cancer MRI 3/17/2022 with hepatic mets multiple small pulmonary mets also noted. Liver biopsy 4/1/22 consistent with metastatic breast cancer. Noted to be pregnant when she went for port-a-cath.
Choose to terminate pregnancy 3/31/22 to allow for complete chemo. ACT 4/5/22-7/23/22 . PET noted resolved axillary nodules and pulmonary nodules, Liver mets responding but still with activity. Sarted Lupron and anastrozole 8/10/22, Kisqoli addes 8/23/22.
I am not saying MRNA vaccines caused this but I have seen way more and way younger breast cancer in this remote population in than in a very long career.
We have had 18 new cancers since the vaccines only 1 was unvaccinated. This is the youngest ever. (Source.)
By way of contrast, for the 30 years prior to the emergency use authorization of the COVID-19 vaccines, there were 2,245 reported cases of fetal deaths following all FDA-approved vaccines, or about 75 fetal deaths per year. (Source.)
Taking the total fetal deaths following COVID-19 vaccines for the year 2021, 3,774 fetal deaths (source), that is an increase of 4,943% over the yearly average of fetal deaths following all FDA-approved vaccines for the previous 30 years.
Besides these government statistics from VAERS, medical professionals are corroborating this evidence of infanticide by COVID-19 vaccines based on the increase they are seeing in fetal deaths and stillborn babies following the roll outs of the COVID-19 vaccines.
An alleged leaked email from a “managing nurse” from a hospital in Fresno, California, states that there has been an increase in stillbirths following the COVID-19 vaccines, and that this trend is expected to continue according to Epoch Times.
This follows a report we recently published by Dr. John Campbell regarding the increase in neonatal deaths in Scotland.
And that follows another report we published last month (October, 2022) from Dr. James Thorp, a board certified OBGYN and Maternal Fetal Medicine Physician with over 43 years of obstetrical experience, who was interviewed by Dr. Drew Pensky and stated that in the past two years since the mRNA COVID vaccines were introduced, he has seen an “off-the-charts” rise in sudden fetal death and adverse pregnancy outcomes, such as fetal malformation and even fetal cardiac arrest, among his patients.
Pfizer to fast-track more vaccines for pregnant moms, despite mounting evidence rushed COVID shots harmed babies
The Defender | November 9, 2022
On Nov. 1, Pfizer issued a press release about an investigational vaccine for pregnant women the company said will protect babies from respiratory syncytial virus (RSV).
Not coincidentally, RSV is the latest viral bugaboo to hit the headlines, with frantic news accounts of “overwhelmed” hospitals sounding eerily reminiscent of the early coronavirus fear-mongering.
Buoyed by the successful global marketing of its COVID-19 jabs — an estimated 49% of pregnant women worldwide reportedly views the vaccines favorably and almost 1 in 4 pregnant women in the U.S. took them — Pfizer is hoping to hit another home run with the RSV vaccine.
The vaccine maker said it intends to seek U.S. Food and Drug Administration (FDA) approval by the end of the year.
The FDA, meanwhile, has been busy handing out “Breakthrough Therapy” designations to Pfizer as if they were papal dispensations, signaling a regulatory willingness to speed up approval not only for Pfizer’s RSV vaccine but also for a maternal Group B Streptococcus (GBS) vaccine the company is developing.
To this expedient end, the FDA allowed Pfizer to “stop the [RSV] study short,” halting enrollment at about 7,400 participants — though the trial was supposed to involve 10,000 pregnant women.
Researchers devoted to vaccine orthodoxy pay lip service to the need for an extra-high evidentiary bar for pregnancy vaccines — stating that such vaccines should not only prove they reduce illness, with minimal reactogenicity in the woman, the fetus and the neonate, but should also “demonstrate safety or lack of evidence of harm.”
However, those turn out to be empty words.
In fact, the influenza and Tdap (tetanus-diphtheria-acellular pertussis) vaccines that public health agencies have long recommended for pregnant women never underwent any clinical trial safety testing in that population, and the FDA never licensed those vaccines specifically for pregnant women.
Moreover, flu shots and Tdap shots have never even resulted in any statistically significant reduction in the outcomes they are supposed to address.
With the advent of Emergency Use Authorization COVID-19 vaccines, the FDA, Pfizer and other manufacturers barely made any pretense of assessing maternal safety, and likely “colluded together to conceal damaging data” about high rates of fetal death.
Other researchers, however — and even vaccine insiders — began to speak out in 2021.
For example, Canadian researchers writing in late 2021 worried that many of the systemic reactions commonly reported after COVID-19 vaccination might be “sufficient to affect fetal/neonatal development.”
Those authors included vaccinologist Byram Bridle, Ph.D., who earlier in 2021 characterized the COVID-19 vaccines’ disturbing biodistribution and accumulation in vital organs as “a big mistake,” and neurology professor Dr. Steven Pelech, who expressed repeated concerns about myocarditis and the vaccines’ risks to young people.
Now, as horrified pregnant women who took the COVID-19 jabs experience skyrocketing miscarriages, stillbirths and fetal malformations, they are wondering why regulators issued no warnings.
But as Pfizer’s exuberant RSV press release and the FDA’s complacent endorsement of clinical trial shortcuts suggest, vaccine makers and regulators not only intend to ignore or bulldoze even the most outsized safety signals but are clearly positioning themselves to go after pregnant women in an even bigger way.
‘Quibbles’ and questions
The details provided — or omitted — about Pfizer’s RSV clinical trial exemplify manufacturers’ and regulators’ cavalier approach toward pregnant women.
Commenting on Pfizer’s announcement, family physician Dr. Buzz Hollander — who clarified that he is predisposed to celebrate the new RSV vaccine offering — nonetheless noted a number of serious criticisms:
- Pfizer released “just a press release” but no data, making it “impossible to pick [the vaccine’s declared efficacy] apart.”
- Pfizer offered no explanation as to how it defined “severe” disease, its primary endpoint.
- A year into the trial, Pfizer fishily altered an important endpoint, defying a fundamental clinical trial design principle that “involves setting out in advance the endpoints that will be assessed.”
- In Hollander’s words, Pfizer “switched their secondary (critical!) endpoint of RSV hospitalizations to 360 days from 180 days… and then inspired my suspicion by not reporting any hospitalization data, interim or otherwise, in their breathless press release.”
- Researchers have published only one small safety study for the RSV shot, about which Hollander said: “I quibble with studies finding >40% of placebo participants reporting systemic symptoms; when queried enticingly enough, half of us might recall a headache or some fatigue the day after our placebo shot, and that can bury a difference in real adverse reactions compared to the vaccine group.”
- Curtailing study enrollment was unwise, Hollander said, because “bigger is better when it comes to … finding safety signals.”
- Earlier this year, GlaxoSmithKline (GSK) “stopped cold” a three-times-bigger trial of a similar RSV vaccine for pregnant women after detecting a safety signal, yet there has been no discussion as to why Pfizer’s maternal RSV vaccine is “fine” while GSK’s was deemed “untouchable.”
Hollander’s modest conclusion: “We should have all learned by now that even the appearance of cutting corners in the vaccine approval process will carry its own unknown costs.”
Readers reacting to Hollander’s post were less circumspect. One acerbically remarked, “The problem here is Pfizer. They’ve paid billions in fines for shady practices and data manipulation. And that was before the Covid vaccines (for which they’re indemnified).”
Another reader expressed his reservations even more succinctly: “Trust Pfizer numbers? You must be joking.”
Adverse pregnancy outcomes after COVID vaccination — no joke
As Pfizer, with the FDA’s help, tees itself up to “dominat[e] the maternal RSV vaccine market,” OB-GYNs on the front lines of maternal care are stepping forth to sound the alarm about the COVID-19 shots’ infanticidal fallout.
Dr. Kimberly Biss recently tweeted, “Since the vaccine rollout started, we have seen in our practice a decrease in new OB numbers, which would be infertility, by about 50%; we’ve also seen an increase in miscarriage rate by about 50%, and … probably about a 25% increase in abnormal pap smears as well as cervical malignancies.”
Similarly, Dr. James Thorp, in multiple interviews, described an “off-the-charts” rise in sudden fetal death and other adverse outcomes, including fetal malformation and fetal cardiac arrest.
Asked to comment on information recently leaked from a California hospital, Thorp characterized the uptick in fetal deaths — from under 6 per 1,000 in 2020 to more than 29 per 1,000 following the rollout of COVID-19 injections — as being “way way beyond” what the Centers for Disease Control and Prevention ordinarily would consider a safety signal.
Thorp published a preprint in September (along with co-authors who include Children’s Health Defense’s Megan Redshaw) describing “significantly more frequent” pregnancy-related adverse events reported to the Vaccine Adverse Event Reporting System, or VAERS, after COVID-19 shots than in the aftermath of flu shots — which themselves are far from benign.
Cataloging significant increases in “miscarriage, fetal chromosomal abnormalities, fetal malformation, fetal cystic hygroma, fetal cardiac disorders, fetal arrhythmia, fetal cardiac arrest, fetal vascular mal-perfusion, fetal growth abnormalities, fetal abnormal surveillance, fetal placental thrombosis, low amniotic fluid, and fetal death/stillbirth” and also menstrual abnormalities, Thorp and co-authors called for a “worldwide moratorium on the use of COVID-19 vaccines in pregnancy.”
For children who survive, Thorp suggested they may suffer from lifelong “vaccine-induced acquired immune deficiency syndrome.”
In Scotland, meanwhile, the government ordered an investigation into the “spike in newborn baby deaths” in 2021 and 2022, an increase “larger than expected from chance alone.”
Even in a gerrymandered study clearly designed to exonerate the COVID-19 shots during pregnancy — focusing on immediate reactions after a first or second dose and hampered by “limited perinatal outcome assessment” — researchers found that 4.4-7.5% of pregnant women reported obstetrical symptoms.
Careless and worse
As Substack writer Etana Hecht wrote last May, “The topic of pregnant and nursing moms getting vaccinated under encouragement and coercion is painful,” particularly once one becomes aware of “how carelessly the most precious among us are being treated.”
That carelessness is evident as we witness some of the same players involved in the COVID-19 vaccine fiasco now circling back around to help build the case for Pfizer’s RSV vaccine.
That includes figures such as Dr. Robert Frenck, the Pfizer-beholden principal investigator of the Cincinnati Children’s Hospital clinical trial that tested the company’s COVID-19 shot in children. Frenck reported 12-year-old Maddie de Garay’s serious vaccine injuries to the FDA as a mere “stomachache.”
Graphs clearly show that none of the vaccines pushed on pregnant women are safe for babies or moms — but given that from one-fourth to one-half of pregnant women acquiesce to getting them, those who know the truth need to work even harder to get the word out.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Effects on mother and child that bear out Mike Yeadon’s warnings
By Neville Hodgkinson | TCW Defending Freedom | November 7, 2022
A British scientist with 32 years of experience in the pharmaceutical industry warned right at the start of the Covid vaccine rollout that under no circumstances should the gene-based, mRNA jab be given to women of child-bearing age without studies to confirm it was safe.
Dr Mike Yeadon, former vice president for research at Pfizer, one of the manufacturers of the experimental mRNA products, filed a petition with the European Medicines Agency on December, 1, 2020, urging that even testing the jab on human volunteers was unethical without significant safety concerns being taken into account.
One of these was a similarity between virus proteins targeted by the proposed vaccinations and a protein (syncitin) essential for forming the placenta in pregnancy. If antibodies produced by the jab also acted against those proteins, the petition said, ‘it would result in vaccinated women essentially becoming infertile’.
Co-signed by Dr Wolfgang Wodarg, a leading German physician, the document also warned that the vaccine trials were much too short to flag up late adverse effects. It added that the design was such that the trials could not show whether the product worked either in stopping a person from becoming infected, or from infecting others.
Subsequently, Yeadon became one of the first scientists to highlight evidence from a previously confidential Pfizer study showing that the vaccine products do not stay at the injection site but become widely distributed throughout the body, including the ovaries.
In view of the toxic nature of the ‘spike’ protein that the jab manufactures (summarised here), Yeadon warned in August, 2021: ‘My assumption at the moment is that these vaccines are concentrating in the ovaries of every female who has been given them. We don’t know what that will do, but it cannot be benign and it could be seriously harmful.’
It is now widely acknowledged that the jab neither protects against infection nor transmission, as Yeadon and Wodarg spelled out in their petition. If their knowledge had been sought at the outset of the Covid crisis the UK alone could have been spared the £500billion lockdown bill, with enormous associated social damage.
But what about the fertility warnings? Despite his years of experience at the top of his field, Yeadon has been vilified for speaking out. Is he really no more than ‘a hero of Covid conspiracy theorists’, as the Times described him?
Birth rates have fallen significantly in many countries, including the UK, in the wake of the vaccine rollouts. Various reasons for the fall have been suggested – usually excluding the jab.
Yet Dr James Thorp, a 68-year-old American physician who has practised obstetrics for more than 42 years and sees thousands of high-risk pregnant patients each year, has observed many complications attributable to the jabs, including foetal death and miscarriage. ‘What I’ve seen in the last two years is unprecedented,’ he says.
With help from several colleagues, he compared rates of adverse events following the Covid jabs with those reported post-flu vaccination in women of reproductive age. The focus was on events related to pregnancy and menstruation, using data from the US Vaccine Adverse Event Reporting System (VAERS).
A preprint of their findings published on September 28 shows a thousand-fold increase in menstrual abnormalities after the Covid jab, and significant increases in miscarriage, foetal malformation, growth abnormalities, cardiac disorders, foetal death and stillbirth.
Thorp has also highlighted risks to newborn babies taking milk from their vaccinated mothers. One study found mRNA from the jab in five out of 11 lactating women who had received the vaccination within six months of their delivery.
Last month, in a wide-ranging review in the US-based Epoch Times of these and other findings, US microbiologist and biomedical scientist Dr Sean Lin revealed that Thorp ‘has seen at least three newborns, completely healthy at the time of their birth, who passed away after being breastfed by their recently vaccinated mothers’. This suggested the vaccine components can not only accumulate in the ovaries but can also be passed on to infants via breastfeeding, he wrote.
He added that details of animal experiments performed before the jabs were authorised, recently obtained under freedom of information legislation, showed that mRNA and spike protein can travel through all barriers in a mother rat to enter its foetus. The rats themselves experienced toxicity during gestation, with some becoming infertile and losing the use of their hind legs.
Calling for an end to all Covid shots for pregnant women until long-term safety data become available, Lin writes: ‘The medical field and health agencies should still adhere to the fundamental ethical principle of ‘Do No Harms’.’
A hospital memo leaked to the Epoch Times by a nurse in Fresno, California, revealed how the hospital is experiencing a dramatic rise in the number of stillbirth cases, now upwards of 22 a month compared with an average of one to two every three months previously. This massive increase seems to align with similar evidence from across the country showing a potential rise in problems with fertility, miscarriages and foetal development, the newspaper reported.
Could the vaccine have contributed to a ‘very unusual’ spike in deaths among newborn babies now being investigated in Scotland?
In the UK, one and a half million Yellow Card reports of suspected adverse reactions to the vaccines include 821 miscarriages and 58,171 reproductive/breast disorders.
With tens of millions of doses administered, those numbers have still not persuaded regulators that there is a problem, although real-world adverse effects can be at least ten times higher than those reported. ‘Our advice remains that the Covid-19 vaccines are safe and effective during pregnancy and breastfeeding,’ the Medicines and Health products Regulatory Agency (MHRA) reaffirmed in September.
A review last month in the journal Vaccine declared that based on studies published so far ‘there is no scientific proof’ of any association between the jabs and impaired fertility in either men or women.
It depends on what is meant by ‘scientific proof’. If scientists do not ask the right questions, they can avoid receiving unwelcome answers. Those who drove the vaccine rollout are choosing not to see the thousands of reported disorders as related to the jabs, despite the record numbers, and clearly demonstrated mechanisms of harm.
It took a mathematician/businessman, for example, to point out evidence of a dose-response relationship between the jabs and infant deaths, with significantly more deaths reported when the higher-dose Moderna jab is used during pregnancy than with the Pfizer product.
Igor Chudov, who highlighted this phenomenon using US Centers for Disease Control (CDC) figures, says the Moderna product is associated with nearly twice as many neonatal deaths as the Pfizer vaccine, and 42 per cent more miscarriages.
In the light of these data, he asks: ‘How can Covid vaccine given during pregnancy be safe, and NOT affect infant deaths? How come nobody at the CDC asked this question? How come our media is silent on this?’
It is as though there are parallel universes: one occupied by those who can see no harm, and the other by doctors and scientists who insist a grave situation is staring us in the face.
The latter include three American medical whistle-blowers who found a 2021 rise of nearly 300 per cent in miscarriages among women serving in the US Army compared with the previous five years. There was no increase in 2020, when Covid arrived.
Doctors calling for a halt to Covid vaccination for pregnant women often meet abuse and censorship.
In October 2021, obstetrician and gynaecologist Dr Christiane Northrup told the Epoch Times: ‘Women are having bleedings. The doctors in our area are doing hysterectomies in young women, like 30-somethings. They said “Oh, it’s not unusual”. Let me tell you, as a board-certified gynaecologist, that’s very unusual. Women’s periods are messed up all over the place . . . I’ve had a huge Facebook group of thousands of women talking about this situation that was removed.’
What of Yeadon’s worry that an immune reaction to the spike protein might block pregnancy?
A small study from Singapore, in 15 women, reported that none had developed anti-syncitin antibodies after the jab, but Yeadon says the actual data showed a clear increase, arbitrarily ruled as insignificant by the researchers.
‘It looked like someone had tried to dismiss our concerns by testing for evidence of the particular problem we’d warned about. Unfortunately, all they did is to reinforce our concerns.
‘We’d envisioned the risk that, in responding to the synthetic piece of virus spike protein, women’s immune systems would also make an immune response to their own placental protein. That’s exactly what was reported in the pre-print paper.
‘Based on this concern alone, all these experimental products as a class should have been completely contraindicated in women younger than menopause.’
He insists that a series of toxicology issues meant ‘adverse impacts on conception and ability to sustain a pregnancy were foreseeable from the start . . . There was and still is no data package supporting safety in pregnancy, or prior to conception.’
Featured Video

Fear Is the Mind Killer
or go to
Aletho News Archives – Video-Images
From the Archives
Infertility: A Diabolical Agenda
Dr. Joseph Mercola | July 9, 2022
“Infertility: A Diabolical Agenda,” is the fourth vaccine-related documentary by Dr. Andrew Wakefield. It tells the story of an intentional infertility vaccine program conducted on African women, without their knowledge or consent.
While it’s been brushed off as a loony conspiracy theory for years, there’s compelling evidence showing it did, in fact, happen, and there’s nothing to prevent it from happening again. … continue
Blog Roll
 Aletho News
Aletho News- Fear Is the Mind Killer
- Israeli strikes kill 10 in southern Lebanon, including 3 rescue workers
- Israeli military ‘failed on all fronts’: Poll
- US at a crossroads: Iran’s firm positions leave Trump no option but to capitulate
- Iran signals decisive response to end US maritime bullying, piracy
- Trump eager for off-ramp in war on Iran, but Netanyahu has him trapped: Former official
- Trump’s ‘Golden Dome’ offers ‘limited’ shield against ballistic missiles: Defense official
- Ukraine Seeks to Provoke a Nuclear Conflict: Zakharova
- US squares up to China over Panama Canal
- Monroe Doctrine 2.0: ‘Great Reset’ for US Imperialism?
- If Americans Knew
- How Tony Dokoupil Became the Face of ‘Zionist Fanatic’ Bari Weiss’s CBS
- Far Right Israeli Settler Movement Enters Syria in a Push for “Greater Israel”
- ‘People Have the Right to Be Buried’: In Gaza, Thousands of Palestinians Remain Trapped Under Rubble
- Born during Israel’s genocide: Gaza’s child survivors bear the scars of war
- Who are the women and girls behind Gaza war’s horrific casualty toll?
- Beloved Gaza doctor detained “indefinitely” without charge – Daily Update
- By Week’s End, Trump’s War Will Be Plainly Illegal
- CBS News Reportedly Ousts London Bureau Chief Over Differences With Bari Weiss Over Gaza Coverage
- State Department Says US Is in Conflict With Iran ‘At the Request’ of Israel
- What ceasefire? Israel won’t stop killing in Gaza, Lebanon – Daily Update
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
