There follows a guest post by the Daily Sceptics’s in-house doctor, formerly a senior medic in the NHS. He’s run his eye over yesterday’s data release from NHS England that has given rise to some panicky headlines (“Frightening new Covid data shows Boris Johnson’s omicron gamble may be about to implode” – The Telegraph). Covid hospital admissions are indeed rising, but a third only have Covid incidentally, i.e. it’s not the reason they were admitted to hospital.
Yesterday afternoon the Primary Diagnosis update was released by the NHS. Readers of this site will be aware the spreadsheet contains information about which patients are being treated for Covid as the primary diagnosis (in other words symptoms sufficiently severe to put them in hospital for a while) and patients testing positive for Covid but being treated for something else.
The NHS concealed this information until they were forced by parliamentary pressure to publish in July 2021.
Graph One shows the overall situation in English Hospitals. Daily admissions in blue bars. 7 day moving average on the brown line. Readers will appreciate that the current seven day MA is the same as it was in mid-September and lower than mid-October. It can be seen on the right-hand side of the graph that on December 28th there was a sudden spike in cases. This may be recording artefact due to delay in logging cases over the bank holiday. There may also be some delay in discharging patients over the extended four-day weekend. Or it could be the beginning of a ‘nailed on tsunami of cases’. We will know more next week.
What we can’t tell from this graph is the turnover of patients in hospital. The NHS has this information but will not release it. It’s actually quite important because it gives a better impression of the severity of Omicron vs Delta. For clarity I should say that even if patients are less unwell, a large number of them can still stress the system, but as long as the inpatients can be managed through the hospital phase in an efficient manner and the numbers going out keep pace with the numbers coming in, the problem is manageable. The real difficulty with high turnover is the intensity of the workload on staff to keep up with the pace, and clearly there is also a problem with staff absence due to positive testing.
Graph Two is complicated but important. It shows the acute Covid cases on the blue bars, the incidental cases in the yellow bars and the ratio between the two on the gray line. Readers will see that the blue bars go up on the right-hand side, but the yellow bars go up a lot more. This means there are proportionately more ‘incidental’ cases than ‘real’ cases and the ratio (gray line) is dropping to 0.67. So, when the BBC report the number of Covid cases in hospital, only two thirds of that number are ill with Covid.
Again, for clarity, one should not assume that lots of patients with incidental Covid are not problematic. They do create a problem because of so called ‘cohorting’ – essentially positive patients need to be separated from negative patients and nursed separately. This creates difficulties in allocating specialist nurses and staffing rotas if the patients have to be located in different wards to where they otherwise would be. It also causes trouble for scheduling operations in respect of extra precautions being taken for positive patients and so on – so it generally increases organisation ‘friction’ and reduces efficiency.
Overall, the falling ratio of incidental to real cases reflects the transmissibility of the new variant. It seems to me that eventually everyone is going to get this virus one way or another. On the other hand, the symptoms it causes do genuinely seem to be mild in comparison to previous variants.
Experts in the media are commenting that the NHS is concerned about the risk of being overwhelmed by a surge of older people being admitted next week. The ZOE app data does show a rise in cases in the 55-75 age group in the last few days. Whether that translates into more severe admissions is difficult to say – the NHS do release information about age group admissions, but the next packet is not due until mid-January.
Finally Graph Three shows the data for London, the leading edge of the Omicron wave. Again, the blue line (acute admissions) is going up, but not as fast as the brown line. The doubling time of acute hospital cases is 28 days – this is quite clearly very much slower than the doubling time of positive community tests (about three days before Christmas).
The ratio between the lines is 0.67, the same as England as a whole. From the weekly hospital summary, also released yesterday, it is clear that not all London hospitals are equally affected. The East and South-East areas are proportionally worse off than the West and Central areas. This may reflect differences in community vaccination rates in parts of the capital.
In summary, this information is very revealing. It suggests that the real problem is not vast numbers of very sick people who are likely to die and use up large amounts of NHS resources. Rather there are large numbers of moderately ill people who do require some supportive care in hospital, but an increasing number of incidentally positive patients who create organisational friction as they have to be cared for separately from non-positive patients at a time when a lot of staff have also been sent home with positive tests or contacts.
Whether further social restrictions make a material difference to this situation is a moot point. Some of my colleagues think reimposing a societal lockdown will reduce the peak of the wave and allow hospital management to keep on top of the problem. Others think further lockdowns will serve no purpose and the wave will transmit through the population anyway regardless of euphemistic ‘non pharmaceutical interventions’.
Readers will remember that when societal restrictions were imposed in January of 2021 they were not lifted until July, and even then, there was substantial opposition from the NHS. Finally, in the intensifying clamour for lockdown from the usual quarters, I have not seen any balance in their argument in respect of the collateral damage to health and the obvious quantifiable damage to the economy, businesses and jobs. I wonder why that could be?
there is some really interesting data coming out of ontario on vaccine efficacy (VE) and vaccine evasion from omicron.
it also seems to be being widely misinterpreted/misread, so i want to put a paw in here and opine.
this is the key chart. (generated from the ontario gov’t website HERE)
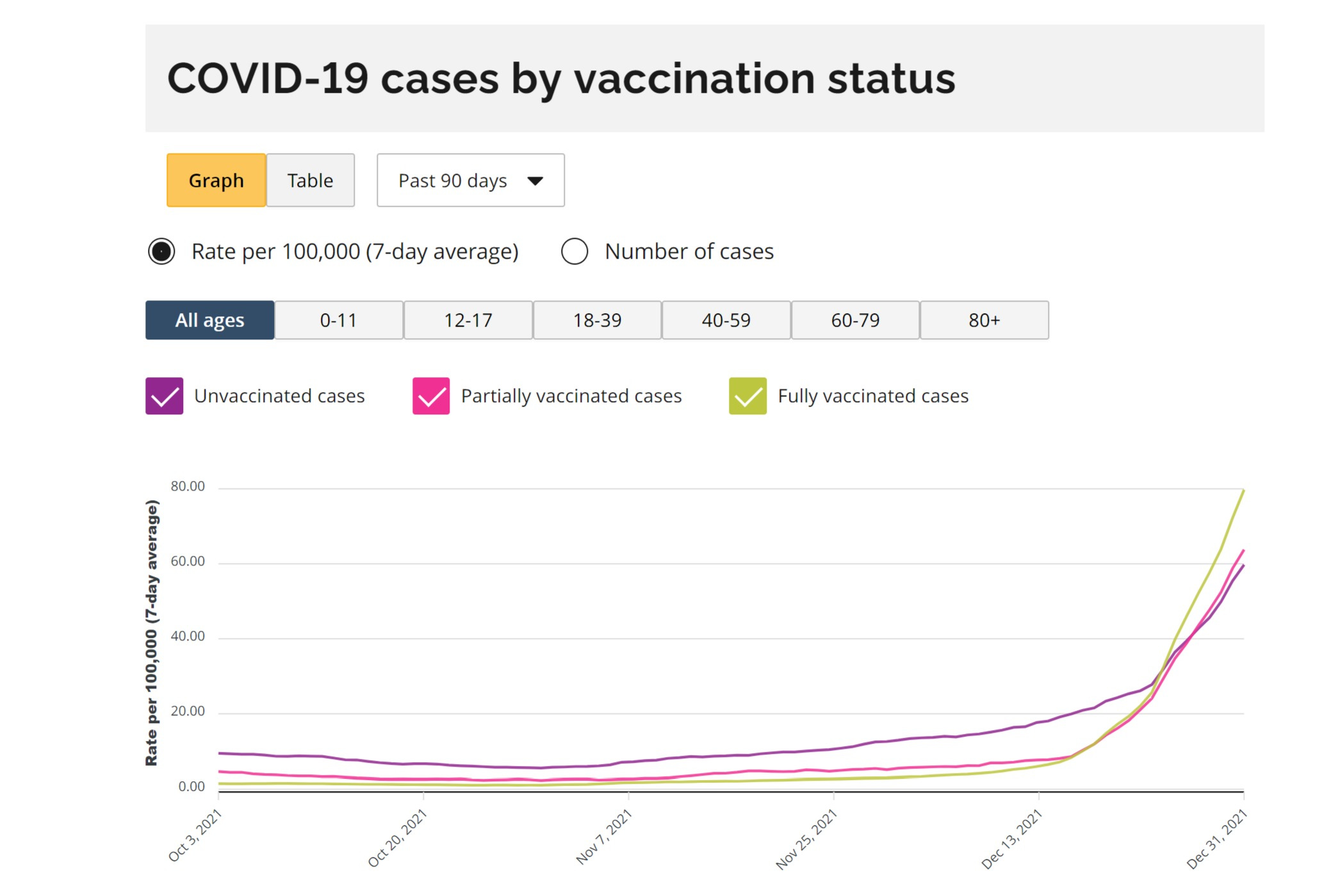
and it shows something incredibly interesting. it shows vaccines working to stop cases until mid december and then suddenly inverting. this is presumably due to omicron.
vaccination just fell to a -33% VE for cases and this looks to be worsening rapidly, likely because of a rise in omicron prevalence.
this is consistent with not just vaccine escape, but vaccine driven acceleration.
the vaccinated are getting covid at higher rates than the unvaxxed and that rate looks to be increasing rapidly as omi gains viral share.
many are denying this and calling it a simpson’s paradox (SP) where each subgroup is actually showing strong VE but where the way they aggregate causes the net figure to invert and imply an erroneous relationship that does not actually pertain. such things have been common in covid data.
i think this claim is incorrect.
firstly, if this is an SP, then why did that not manifest before? why did the relationship for case reduction invert so suddenly? it was certainly not a massive, sudden change in who was vaccinated.
this confusion has been greatly amplified by the website itself. when you select for any given age cohort, it shows positive VE for cases. this seems to be an open and shut case for this being an SP.
but it’s not. such claims contain a severe error. can you spot it?
look closely at the dates. see where they end?
all the age cohorted data ends in october.
the same is true of the data in the table above. it’s full blown apples and oranges. there seems to be no post october age delineated data in this system at all.
but the change in vaccine efficacy pattern did not occur until mid decemeber. so, this is an irrelevant comparison to the current data and current situation. it actually agrees with the first chart.
whether this is just carelessness or sloth on the part the ontario health agencies or a subtle and cunning manipulation is anyone’s guess and i’m not going to wade into that. but i HAVE seen an awful lot of smart people miss this. (i missed it at first too) you simply do not expect to see the data truncate like that on the same graphing tool.
just one more cautionary tale on data handling…
ADDENDUM OF EXCELLENT GRAPHIC FROM GATOPAL™ ORWELL2024.
and an additional catch:
“The https://covid-19.ontario.ca/data says: “Due to technical difficulties, the case rate by vaccination status by age group is not available”.
We can lockdown the entire economy, but can’t fix a dashboard that would help showing what’s going on?”
this is what team work looks like and it’s how we make progress.
(END ADDENDUM)
but the conclusion here looks to be that this data (along with data from many other places) is consistent with omicron being not just a vaccine escaping variant, but one that is actually vaccine enabled.
if it was just escape, we’d see parity with the unvaxxed. having it go strongly negative is a sign that the vaccine is making it worse either though OAS/antigenic fixation or some other mechanism.
the good news is that omicron looks mild. the bad news is that it increasingly looks like the variant that original antigenic sin (OAS) begot and this means that the vaccinated may be wide open for it in a way they would not have been had these programs not been rolled out. worse, they may NEVER be able to generate sound immunity because that’s what OAS…
this leads me to predict that the curves will continue to separate in ontario as omicron becomes more prevalent and that we’ll start seeing VE’s that look more like denmark.
will keep an eye on it (and hope they keep reporting the data).
A major study from the University of Oxford into risks of myocarditis (heart inflammation) following Covid vaccination has found the risk in males under 40 to be significantly higher than the risk of the condition following Covid infection.
The researchers found that while there were seven additional myocarditis events per million in the 28 days following COVID-19 infection (95% Confidence Interval (CI): 2, 11), there were 14 following an AstraZeneca second dose (CI: 8,17), 12 following a Pfizer second dose (CI: 1,7), 101 following a Moderna second dose (CI: 95,104), and 13 following a Pfizer third dose (CI: 7,15). These findings are depicted above. Most of these figures represent a doubling of the risk compared with infection. However, the Moderna second dose figure is a massive 14.4 times greater. The Moderna vaccine uses a similar mRNA technology to the Pfizer vaccine, but delivers a dose three times as large, which may partly explain the difference.
For females and for males over 40 the study found greater risk of myocarditis following infection than following vaccination. However, some have criticised the study for under-counting Covid infections by using positive tests rather than antibody surveys, which means the risk following infection may be exaggerated. Another criticism was the use of only two age bands – above and below 40 years – which may conceal elevated risks for younger age groups.
The study, which is a pre-print, is an update to an earlier study published in Nature earlier in December which used data up to August 24th. The update brings us up to November 15th, extends the age range down to 13 years from 16 years, and also includes results split by both sex and age (rather than just by sex and age separately) – the original study was especially criticised for omitting this breakdown, leading to allegations of concealing important findings for political purposes.
The authors note: “These findings have important implications for public health and vaccination policy.”
Indeed they do. In particular, given the low risk of Covid to males under 40, the extreme elevated risk of myocarditis from the Moderna vaccine means it ought to be suspended for use in males under 40 with immediate effect.
Ontario’s former privacy commissioner Ann Cavoukian has warned that the government cannot be trusted with cellphone tracking amid the pandemic. The warning came after it was revealed last week that a federal agency has been using cellphone data to track the movements of Canadians since the beginning of the pandemic.
“It concerns me enormously that this would enable the government to collect more and more information,” Ann Cavoukian told The Epoch Times.
“I do not want to [see] a trend where the government is consistently doing this and starting now. You can’t trust the government.”
Last week, the Public Health Agency of Canada (PHAC) confirmed it has been using cellphone data to analyze movements for the purposes of pandemic policies. The agency plans to continue with the data analysis until 2026, expanding it to other health issues.
“In March 2020, [Prime Minister Justin] Trudeau said that tracking cell phone users was not being considered. Well, they did it, PHAC’s been doing it, and they want to do it even more,” Cavoukian said.
“[Officials] say ‘as soon as the emergency is over, we’re going to return to privacy.’ They don’t. The privacy invasive measures that are introduced during emergencies, pandemics, etc., often continue well after the emergency is over,” she added.
According to the former privacy commissioner, who served from 1997 to 2014, PHAC kept the data collection a secret because “they know people do not want their mobile devices tracked.”
Cavoukian was particularly concerned with the PHAC partnering with other unknown data providers, like the Communications Research Center (CRC).
“In partnership with CRC, PHAC has been producing report summaries to look at how movement trends of the Canadian population have changed over the course of the pandemic, including identifying new patterns to help direct public health messaging, planning and policy development,” PHAC said in a statement to The Epoch Times.
The agency insisted that it did not “receive or collect any individual mobility data” and that it has not stored or acquired individual level data.
On December 16, the PHAC posted a Research for Proposal for a contractor that could “provide it with a steady flow de-identified cell phone data,” reported The Epoch Times.
In a statement, the agency said it “requires access to cell-tower/operator location data that is secure, processed, and timely in addition to being adequately vetted for security, legal, privacy and transparency considerations to assist in the response to the COVID-19 pandemic.”
According to Cavoukian the language in the RFP “reflects an intention to collect this data and retain it.”
She is concerned that the de-identification of data could be done so poorly that it could easily be re-identified.
“At the very least, the Privacy Commissioner’s Office should be all over this, and saying we need to examine exactly what measures you introduced to do this and how you’re going to protect privacy and de-identify data such that it cannot be re-identified,” she said.
“Examine this from end to end. Look under the hood.”
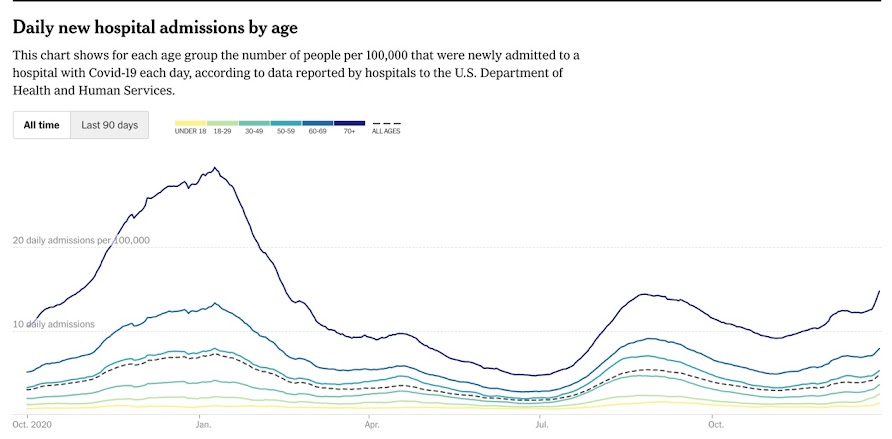
The yellow line represents pediatric hospitalizations over the past 15 months, per the NY Times. Yes, they did increase a bit, just like hospitalizations in every other age group, and the increase was proportional to that of the other age groups.
Cases rose much more dramatically.
Why are the media hollering? Because 80% of parents have been too smart to fall for the vaccinations for their 5-11 year olds. Peer pressure did not work as well on this age group, so parents have to be scared.
Please protect your children from this horribly damaging scam. See Robert Malone about how the benefits are marginal, while the risks are major for children.
CLIMATE change and coronavirus lockdown policies have diametrically opposite approaches to valuing life in the present and the future, yet they are both enthusiastically endorsed by state bureaucracies around the world, not least in the United Kingdom. Have they something in common in spite of their apparent differences?
Vaccines to protect against Covid-19 have not apparently excused the Prime Minister from his perceived obligation to put most of the population under what is little better than house arrest at the appearance of any variant of the present virus, and it seems inevitable that the British government, acting as a Committee of Public Safety, will immediately resort to this policy in the case of future pandemics. Many of us are struggling to understand how this extraordinarily oppressive state of affairs has come about, and so quickly, and with so little real resistance. Comparison with another risk management policy, climate change mitigation, sheds a little, not very reassuring, light on the matter. Superficially different in character, these two contrasted policies share a common answer to the ever-relevant question, Cui bono? But let us start with the differences.
Climate change policy applies little or no discount to the interests of the infinite future, and so as a consequence gives the interests of the present little or no weight. Those currently alive are asked to make unlimited sacrifices to save an infinitely distant future generation.
Lockdown policy applies a zero discount to a small selection of present interests and thus attempts to prevent death, with only scant regard for the long-term societal damage incurred. The interests of the future are heavily discounted and thus sacrificed to preserve a subsection of the present whose interests are ostensibly given overwhelming privilege.
Neither of these policies is consistent with the way that human beings in actual behavioural fact value their own lives and the lives of others in the present and in the future. This is puzzling since it is not particularly difficult to determine what human beings are maximising through their varied behaviour.
Banal though it may seem, we have no evidence that humans are anything more than straightforward reproductive organisms that value their own lives insofar as they gather resources and secure their reproduction. They do not maximise their individual longevity or their individual hedonic experience, both of which are proxies and not ultimate ends. The only final goal that we can infer from evident human behaviour is the securing of reproduction, bearing in mind that this is achieved through the extended family as well as immediate offspring. This behavioural purpose is so far from transcendent that it will seem to many hardly worthy of the name, but observation has so far indicated no other human goal.
Of course, human behaviour is characterised by balanced self-sacrifice in the interests of offspring, but climate and lockdown policies require unbalanced sacrifices of a kind that men and women do not as a matter of behavioural record spontaneously offer. The policies run against the psychological grain.
Consider the details. The coronavirus lockdown is intended to save human life. But the virus does not, apparently, threaten the young, only the very old who are post-reproductive and in most cases contributing little or perhaps nothing to the wellbeing of their nevertheless much-loved children and grandchildren.
The sacrifice is predominantly required of the young and the active who are still gathering resources to produce and rear families. But lockdowns do indeed harm the life’s work of the old by putting their continued personal existence before the interests of their offspring and extended families, a preference that the old themselves would never express.
Thus, coronavirus lockdown policy frustrates the bedrock of altruism underlying the family, and also burdens the old, against their will, with a terrible responsibility.
Climate policy tends in a different direction. The interests of the infinite future are put before those of everyone or nearly everyone at present living. Great sacrifices must be made in the short run to reduce emissions and protect populations as yet unborn. This is, once again, a decision that actual men and women would never spontaneously make, for if the interests of the present are not sufficiently well served there can be no future generations. Climate preachers urge their congregations to ‘think of the kids’ and not themselves, but the advice is both absurd and redundant. Parents care for their families but must first care for themselves. The pelican certainly tears its breast to feed its young, but it does not start by cutting its own throat.
The rhetoric of climate policy describes present generations as selfish hedonic maximisers who must be compelled to relegate their own experiential hunger to protect the interests of future generations. But, as we have seen, this is false and needless; living generations are already engaged in a balancing of interests to produce and secure the existence of future individuals, far into the future, and they need no pressure from climate policy to think in this selfless way. Indeed, extreme climate policy, and at present we have no other for Net Zero comes in only one flavour, is harmful to the interests of future generations as well as those living because it frustrates precisely those current interests that must be satisfied if there is to be a future generation of human beings.
Both lockdown and climate policies, therefore, suffer from an ostensibly uncompromising and absolutist morality which demands that equal value is put on all human lives regardless of their position in the reproductive trajectory. As a matter of real-world fact, this runs counter to the interests of all parties involved, and, unsurprisingly, is not how men and women behave in practice. Parents must satisfy enough of their own requirements to reproduce and care for their families, but they will not absolutely sacrifice the interests of their descendants to preserve their own lives. The pelican, we have noted, will not cut its own throat, yet, mythically speaking, it most certainly does tear its own breast curtailing its hedonic satisfactions and shortening its life in order to rear its young.
Nonetheless, and contrary to observation, lockdown policy must presume that mature human beings would wish to preserve their individual lives at the cost of sacrificing the future of their offspring, which in fact they do not and would never do.
Climate policy, on the other hand, claims that the living will not willingly sacrifice themselves for a future generation, which as a matter of routine fact they do, though in a necessarily pragmatic way which is incompatible with the extreme action required by the currently predominant low-carbon policies.
Climate mitigation and lockdown policies are not only inconsistent with human wishes and actual behaviour, but they are clearly inconsistent with one another; lockdown policy insisting on the absolute value of some present lives, and climate policy insisting on the absolute value of all future lives. In addition, climate policy suffers from an internal flaw: it threatens future lives by leaving the present unable to raise a viable generation with a secure societal future.
These policies are obviously errors, but are they pure errors, random walks in possibility space that have strayed quite accidentally from the path of practicality? One has to allow that this is a possibility; delusions and mistakes do occur even in minds of the finest quality, and it is possible that both these faulty policies arise from a very widely distributed popular misconception or from an honest administrative error.
But a population-wide delusion does not seem likely. Humans are extremely good at perceiving and acting on their own interest, and they rarely go down the wrong path for long. To err is certainly human; but so is learning from error. A population-wide mistake that endures for long periods has never been observed. Some peoples have been said to try every other available course before doing the right thing, but the joke has its laugh because they do eventually find their way back to the path. Populations may indeed be destroyed by the weight of circumstances, but not by their errors; they do the best they can in the most miserable and constrained of conditions. One thinks of the desperate jeopardy of the Melians.
Pure errors, then, are quickly corrected, but climate policy, at least, has been with us in its present form for some 20 years, and in spite of manifest failures and vast costs appears to be insusceptible to criticism, even when extremely well aimed. It is therefore unlikely to be a pure population-wide error. Some other force accounts for its survival. We cannot be certain if this is also true of lockdown policies, since these are not even two years old, but they are already showing signs of extreme resilience in the face of informed opposition and public resistance. Lockdown may not be a pure populational error either. Perhaps this very ill wind blows good to someone.
If these policies are not pseudoxia epidemica, perhaps they are administrative errors, arising from a deeply rooted governmental misconception? That is not unlikely; civil servants are people and people make mistakes; but unlike people outside the chalk circle of the state apparatus, civil servants are very slow to learn from their mistakes because they are insulated from the consequences of failure. But if this were the case for climate and lockdown policies one might expect them both to possess or to flow from similar logical structures, a departmental or cross-departmental ‘view’ on societal emergencies for example. But as been argued above this does not appear to be true. Indeed, these policies approach discounting in diametrically opposing and contradictory ways, one privileging the present and the other privileging the future. They possess different logical foundations.
It would appear, then, that these policies are not based on pure errors. In which case they must be impure, and instead serve some more or less concealed interest. But whose interest? The ultimate beneficiaries are hardly likely to raise their hands when asked, and they may not even be aware of their involvement. As a little candid introspection will begin to dimly perceive, we all hold some of our vested self-interest in blind and frequently offshore trusts.
But the situation is not hopeless. We can confidently identify the way harm is distributed, and in doing so we will arrive at a common feature in the policies that points us in the direction of those who probably benefit.
Both lockdown and climate policies are to the disadvantage of people who are vigorous, active and present. In the case of lockdown policies, they directly harm anyone not old. Furthermore, they even harm the interests of the old indirectly by compromising the future wellbeing of their offspring and extended families. Climate policies harm anyone alive, with benefits being imagined for the abstract, absent, unborn.
In other words, both policies appear to harm people living, while pretending to act on behalf of a weak and voiceless population, the very old and the as yet unborn.
Thus, at a gross level these policies appear to be universally harmful. But a moment’s reflection will show that the net effect is different. Both sets of policies frustrate the free wishes of a population that seeks to secure its own reproduction through balanced self-sacrifice, and the frustration of such firmly held wishes requires coercive regulation and enforcement, activities that can be delivered only with the sanction of state violence and through the offices of secure and securely remunerated positions within the state and its associated clients. The ultimate net beneficiaries of both lockdown policies and climate policies are state employees and state contractors.
Government policies with contradictory approaches to present and future can occur simultaneously because their ultimate end, the reason that they are preferred over other policies, is to provide plausible justification for coercive intrusion into the lives of the vigorous population. The policies efficiently disarm criticism by claiming to act on behalf of parties that are practically unable to disown and reject the ‘help’ offered to them; the old because they are infirm, and the unborn because they are absent. Because these parties lie at opposite ends of the life-cycle, in the process of justification those responsible for state policy have been compelled to adopt two incompatible discounting models in their rhetoric. The future is seen in different ways because the beating of different dogs calls for different varieties of stick.
But it is the hand wielding those sticks that interests us. The historical record provides ample evidence, quite apart from our own recent experience, to suggest that the administrative opportunities of large societies will create a clerisy which comes to have strong interests that can be in deep and considerable conflict with the wishes of the population it claims to serve. This divergence is on occasion betrayed by the character of the altruism, the public interest, called for by policies such as the public health measures addressing the coronavirus or the emissions reduction strategy employed to mitigate climate change.
This suggests a political litmus test. If any public interest policy is inconsistent with the balanced self-sacrifice of parents, then it is almost certainly exploiting the population to serve the administration and its clients. History suggests that this will not be a stable situation. All normative discounting models, such as those employed explicitly by Lord Stern in his notorious climate review, and implicitly in the current lockdown policies, should be firmly rejected as politically dangerous. Naturalistic models derived from the observed behaviour of the population are to be preferred on all occasions.
And better still, let us dispense with discounting models altogether except as academic descriptive and predictive tools. A free society can confidently rely on the spontaneous judgment of men and women correctly to value the future and the present, themselves and each other, as their intuitions direct them in the expression of familial love and friendship. The outcome will be qualified self-sacrifice and a prosperous society with as long a future as fate permits.
As we come to the end of the second year in Covidia, I reflect on just how much the instigators of the entire scam have managed to reshape reality in an amazingly short timeframe, such that what was considered normal 12 months ago is now considered abnormal, and what was considered abnormal 12 months ago is now seen as normal.
For instance, had one predicted 12 months ago that after “vaccinating” the elderly and those considered vulnerable, which was the “route back to freedom”, the Johnson Regime and countless others around the world would:
Proceed to push the injection onto all adults
Move on to getting it into children
Make thousands jobless who do not wish to partake in the experiment
Begin the introduction of Vaccine Passports
Announce that the allegedly 95% effective products wane so quickly they’ll need to be taken every few months
Start talking about the possibility of mandatory jabs
Reintroduce the restrictions that these injections were supposed to do away with
… why such a person would have been called a Conspiracy Nut. Yet a year later the same person is called a Conspiracy Nut for opposing these very things they got called a Conspiracy Nut for predicting, but which are now reality.
There is something horribly ironic, and also deeply chilling about this. For it shows not only how easily manipulated so many people are, but also just how easy it has been for the Covidian Regimes to reshape reality such that millions have come to accept as normal the very things they would have dismissed just months earlier as the product of deranged minds.
The last two years has felt like people are living in parallel universes, so much so that it’s almost tempting to wonder whether Zuckerberg’s hideous Metaverse is already a thing, with millions having unwittingly entered it in early 2020 without noticing.
In the Metaverse, SARS-CoV-2 is a new Black Death that kills indiscriminately no matter what age. In the real world, it is a virus that has a 99.9% Survivability Rate, and there are effective early treatments available to the 0.1% for whom it might potentially be lethal.
In the Metaverse, Lockdowns of healthy people are how we’ve always dealt with outbreaks of transmissible illnesses. In the real world, other than a hastily ended five-day trial in Mexico during the 2009 Swine Flu outbreak, the quarantining of the healthy has never been done before the Chinese Communist Party implemented it in early 2020, to be copied all over the world by Governments ignoring their own long existing pandemic preparedness plans.
In the Metaverse, masks are about loving your neighbour because wearing them stops you passing on the virus you don’t have to others. In the real world, masks do not and cannot stop viral transmission, and thus they are a not a health aid, but a political and psychological tool of subjugation and dehumanisation, designed to humiliate and perpetuate fear.
In the Metaverse, a public health crisis caused by a virus has zero medical advice given out to people, but just a relentless barrage of talk about cases, hospitalisations and deaths, with all knowledge of effective early treatments ruthlessly suppressed. In the real world, a public health crisis caused by a virus would see Governments, health officials, and doctors recommending cheap and effective ways of boosting one’s immune system, such as Vitamin C and D, Zinc, Quercetin, sunshine and plenty of exercise and fresh air.
In the Metaverse, people who aren’t ill can spread the illness they don’t have, and so must take a test which cannot diagnose illness and which gives huge numbers of false positives, after which they must stay in their house for a prolonged period to stop the virus they don’t have from spreading. In the real world, if you’re well, you go about your daily life; if you have what are called “symptoms”, you stay home and rest.
In the Metaverse, the injection of billions of lipid nanoparticles containing mRNA, which has never been injected into people before, which tricks the cells into allowing it to enter, which then causes billions of cytotoxins to be produced in cells throughout every organ, and for which the manufacturers have indemnity but no proper safety data, is hailed as a saviour. In the real world, this is the most dangerous, reckless medical experiment ever performed on masses of people without their knowledge of what they are being given, and the long-term consequences could be unimaginably disastrous, as Professor Sucharit Bhakdi explains in this horrifying warning.
In the Metaverse, a product which doesn’t prevent infection, doesn’t provide immunity, and which requires top-ups every three months, is a vaccine, even if it needs the dictionary definition of what a vaccine is to be changed to accommodate it. In the real world, the Groucho Marx rule about ducks applies — if it looks, walks, and quacks like a duck then it probably is a duck. Thus if it doesn’t stop infection, doesn’t provide immunity, and wanes after 10 weeks, then it probably isn’t a vaccine.
In the Metaverse, willfully going along with abnormal, illegitimate and authoritarian rules & behaviours is the way back to normality and freedom. In the real world, willfully going along with abnormal, illegitimate and authoritarian rules & behaviours is about conditioning us to accept abnormality, the end of a law based society, and the long term loss of freedom.
In the Metaverse, bringing in Vaccine Passports for nightclubs and other large venues is about keeping people safe, and of course won’t be extended to other venues. In the real world, Vaccine Passports are a Trojan Horse, firstly to be extended into other venues of much smaller size (as has been the case in many European countries), but ultimately to facilitate the creation of a Digital ID Social Credit Hellhole where your every move and transaction can be tracked, you have credits not money, and freedom as we knew it is a thing of the past.
In the Metaverse, people who refuse to submit to the mass medical experiment only have themselves to blame if they find themselves excluded by law from entering certain venues, doing certain jobs, buying certain goods, and even being able to avail themselves of the basic necessities of life. In the real world, this unscientific, unholy, sinister apartheid system shows that we are edging eerily close to repeating the ugliness and depravity of certain 20th century regimes that we smugly told ourselves we were not capable of repeating, due to our apparent goodness.
It is baffling that people can view what’s going on so differently, but I would point out that all the views in the real world are derived from facts, data, reason, logic and historical examples, whereas all the views in the Metaverse are taken from Government and media propaganda.
One of the exasperating things in dealing with this is that whilst there are an endless potential number of lies that can be told, there is only one truth. And what the Government and media are very skillful at doing is layering lies upon lies upon lies, such that whilst the critical thinkers and data analysts are busy trying to debunk lie number one, lies number two, three, four and following are already being laid on that foundation so that by the time the original lie has been shown to be false, things have moved on and hardly anyone can remember, let alone care about the original claim.
However, the good news is that this is also the Achilles Heel of the Globalist’s narrative. Firstly, the more lies that are told, the harder it is to sustain the story because it can only be kept going by more lies, each of which tends to become increasingly blatant and absurd, such that even those who have been slumbering for two years begin to stir. For instance, if you try to assure the huge numbers of people that have had adverse events from the injection, or who know others that have suffered, that they must get the next one and it’s perfectly safe, clearly you are going to have your work cut out as stark reality highlights the lie in what is being told.
But the other part of this Achilles Heel is this: The Truth will win because The Truth must win. It is The Truth. It cannot not win. Attempting to suppress it is like trying to hold a cork under water. It will always be wanting to get to the surface, and as soon as you tire of holding it and release your grip, that’s what it will do. And so although these lies will continue, and although they will appear to prevail for some time to come, there is coming a time when they will be defeated because The Truth, not lies, is the ultimate reality:
“Truthful lips endure forever, but a lying tongue is but for a moment.” (Proverbs 12:19)
As we look forward to 2022, although we do not know the details of what is to come, because it is very clear that the goal of the Covidian Regimes is to get everybody injected with their mRNA witches’ brew over and over again by carrot or by stick, by hook or by crook, we can be absolutely sure there will be many more lies, many more difficulties, and much more wickedness. Yet we can also be equally sure that these lies will ultimately be defeated, because he who is The Truth (John 14:6) is guaranteed the victory (Revelation 17:14), and he will suffer their lies only so far, until such time as he destroys their unholy, totalitarian, anti-human agenda. There will be a Reckoning. Just make sure that you are on the right side when it comes.
Researchers working at Belgium’s Princess Elisabeth Polar Station in Antarctica have contracted Covid-19, even though all personnel have been inoculated and any new arrival has to follow rigorous safety protocols.
Two-thirds of the station’s staff of 25 have been infected with the coronavirus, Belgium’s polar secretariat confirmed to local media earlier this week. But how the virus could have reached the remote station, located some 220km (137 miles) from the Antarctic coast, remains a mystery.
“All those present have received two doses of vaccine, and one person has even received a booster shot,” said Alain Hubert, the facility’s executive operator and head of security measures. All staff members also have to undergo a series of PCR tests on their long journey to the station.
Those en route there take one PCR test in Belgium before leaving for South Africa and another five days after their arrival. They self-isolate for 10 days in Cape Town, then undergo two further tests: one before leaving for Antarctica and another five days after arriving at the station.
Nonetheless, even such strict control measures were apparently not stringent enough, as the first Covid-19 case was reported at the station in mid-December among a group of new arrivals. The person in question was immediately placed in isolation, but two others were soon revealed to have contracted the coronavirus as well.
All three infected researchers were evacuated on December 23, but this measure did not stop the virus from spreading further. A virologist contacted by the polar secretariat said the variant that has infected personnel at the station might be Omicron – the highly transmissible strain recently discovered in South Africa.
There are two emergency doctors and all the necessary equipment at the station to treat anyone who falls ill, according to the media. In the meantime, the polar secretariat has placed all personnel under quarantine and put a halt to any new arrivals until the Covid-19 cluster there dissipates. Explorers venturing on two new expeditions had been expected on January 12, but their arrival has now been delayed.
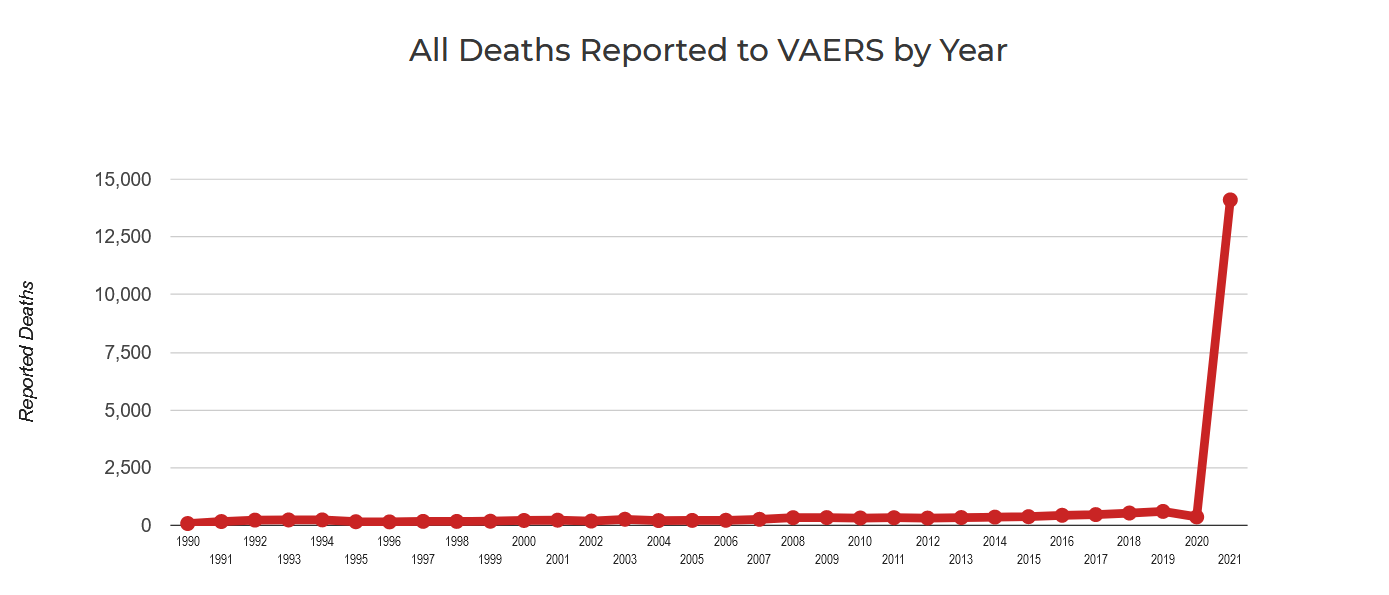
**Displays number of deaths and disabilities associated with each batch/lot number = indication of relative toxicity of one batch/lot compared to another
**No one currently knows the reason why some batches/lots are associated with excessive deaths, disabilities and adverse reactions (up to 50 x). Until we do know, it is best to be cautious
**[“Batch-code” = “Lot Number” = the number they write on your vaccination card.]
All data is sourced from VAERS, a public database of over 700,000 adverse reaction reports for Moderna, Pfizer and Janssen Covid 19 vaccines in the USA.
Our intention is to present the VAERS data in an accessible and unadulterated form, that can be easily verified using the links below
I haven’t written about this because some people who I rely on for advice believe that there are too many unknowns to make a determination as to whether increased adverse event reports are due to a bad “batch” or a bad “vial” or something else.
The unknowns include:
were certain sites just reporting more reliably so any vials sent there would appear more dangerous?
how many vials are in a particular lot?
where did all the vials of a given lot go?
could there have a been a problem in transit?
could there have been a problem with storage?
if a vial is not kept at the proper temperature, could it become dangerous?
…
The inability for anyone to analyze these vials as well as the lack of transparency about each batch makes finding the answer to these questions very difficult.
In this talk delivered in Fresno, California, Dr. McCullough delivers one of his best lectures to date, discussing Covid-19, vaccines, SARS-CoV-2, spike proteins, Covid-19 home treatments, censorship, and Prof. Mattias Desmet’s theories about mass formation psychosis, among many other topics.
Dr. McCullough summarizes the lecture as follows:
* COVID pandemic is a global disaster
* Pathophysiology is complex—not amenable to single-drug treatment
* The prehospital phase is the therapeutic opportunity
* Early ambulatory therapy with a sequenced, multi-drug regimen is supported by available sources of evidence and has a positive benefit-to-risk profile
* Reduces the risk for hospitalization and death
* More safely temporize to close the crisis with herd immunity
* COVID-19 genetic vaccines
* Unfavorable safety profile
* Protection not sufficiently complete or durable
* Censorship and reprisal are working to crush freedom of speech, scientific discourse and medical progress
(no, this has nothing to do with the american koch brothers. it’s a common name and this is a quasi-government health agency.)
data such as this is easy to misinterpret and nearly everyone is doing it incorrectly, so i’d like to walk through why, counter to what many are claiming, this data actually shows that boosters have negative VE (vaccine efficacy).
caveat: this is a small and likely incomplete societal dataset. the sample size is possibly large enough to give us a sense of outcomes, but as with all societal data, it’s difficult to know what bias may be injected by self selection for testing and for vaccination. error bars are likely meaningful.
but we work with what we have, not what we would prefer, so let’s take a look:
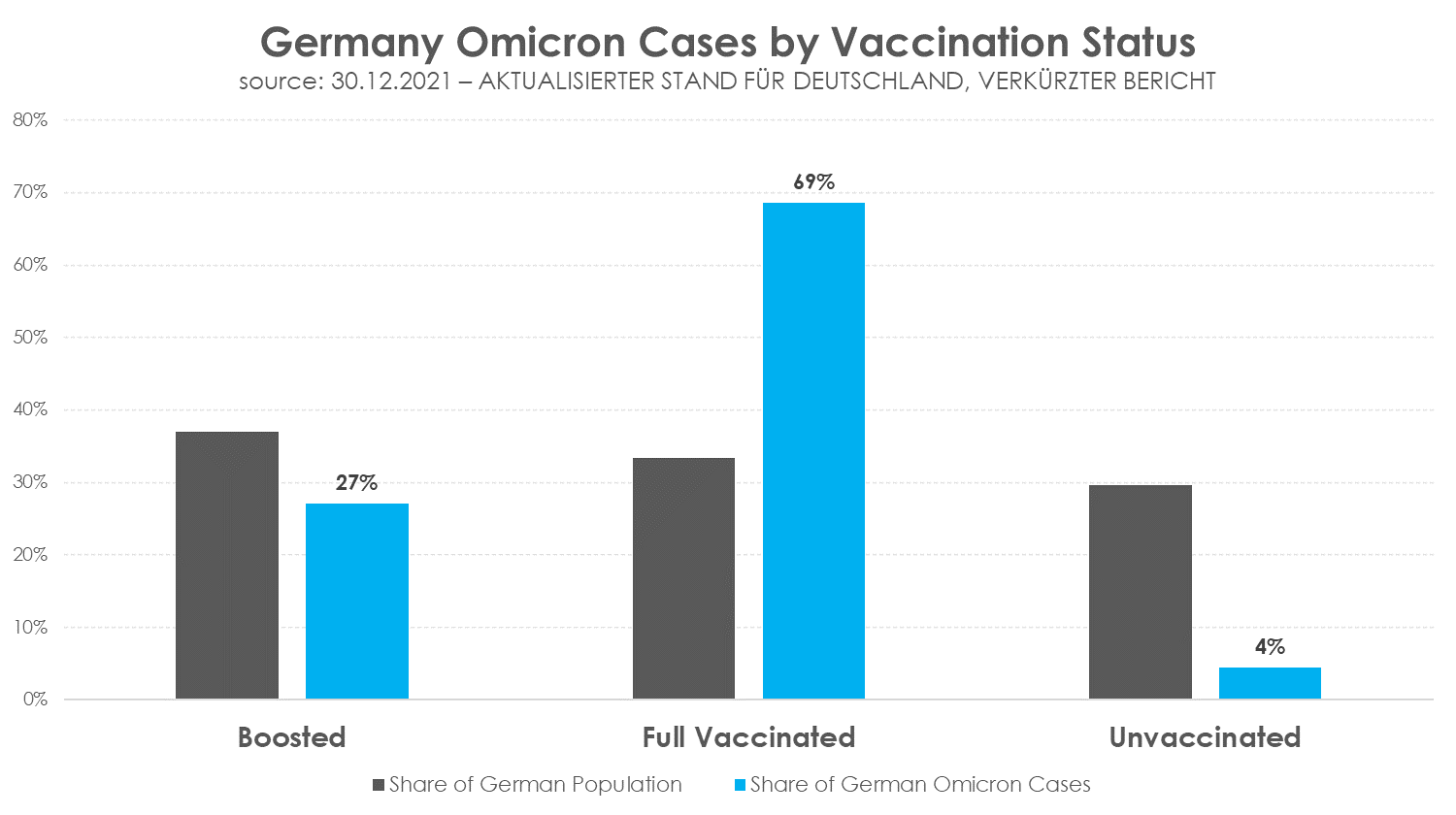
– 4020, ergo 95,58 % vollständig Geimpfte (1137 davon geboostert) – 186 Ungeimpfte (4,42 %)
4020 cases with 2 or more doses of vaccine, 1137 of them with boosters.
186 cases in the unvaccinated.
(unfortunately, there is no breakout for 1 dose only, so i’m presuming that group has been included in “unvaccinated”)
germany is 70.5% “full vaccinated.” (per OWID) thus, by the definitions this report uses, it is 29.5% unvaccinated.
it is 38.2% boosted as of 12/30/21. it’s not clear to me if this study is using that figure or only counting as boosted those who got their booster more than 14 days ago (as many seem to count it). if this is so, the number drops to 29.3%. i will look at it both ways to try to create some bookends for the range. (if anyone can clarify, i’d be grateful)
to see what is happening more granularly, we first need to regroup the terms:
from this one can see that the 3 groups are actually fairly similar in size, but quite divergent in outcomes.
many seem to presume that because cases in the boosted are a lower percentage of overall cases than the boosted are of the overall population that this shows vaccine efficacy.
this is not, however, correct as can be readily seen once we adjust this data to a per capita level.
that data looks like this (using 83.2mm for german population)
and this makes the issue obvious.
to calculate VE, we need to compare the vaccinated cohorts to the unvaccinated. that’s the control group. there are probably some pretty significant error bars here, but this outcome is STARK. the risk ratios for all vaccinated groups are far, far higher than control.
boosting does seem to lead to a 2/3 risk reduction vs just being double vaxxed but still leaves one at 4.7X the risk of the unvaccinated.
this risk ratio leads to VE figures that are, frankly, so bad that i suspect there must be some sort of bias here. this looks too extreme to be entirely plausible and far exceeds all other data i have seen.
one possible source of this issue is definitional. if the german study is using “boosted +14 days” as its definition, then the numbers change quite a bit as the size of the boosted group shrinks and the size of double vaxxed rises causing their risk rates to converge somewhat.
another possible source of contamination is the actual act of running a booster campaign during an outbreak.
the tendency toward transitory immune suppression created by mRNA vaccine administration is well documented.
the danes found it to be on the order of 40-100% increase in the likelihood of infection in the 2 weeks following administration (with 100% likely being a better proxy for genpop as they resemble HCW’s more than NH residents). this study was during a period of relatively low prevalence and with a less contagious variant than omicron. this needle could have moved quite a lot by now.
and all this piles up, so if you are doubling the risk of a group already showing increased risk due to vaccine escape/antigenic fixation/OAS the issue may become multiplicative. […]
Fully referenced facts about covid-19, provided by experts in the field, to help our readers make a realistic risk assessment.
“The only means to fight the plague is honesty.” (Albert Camus, 1947)
Overview
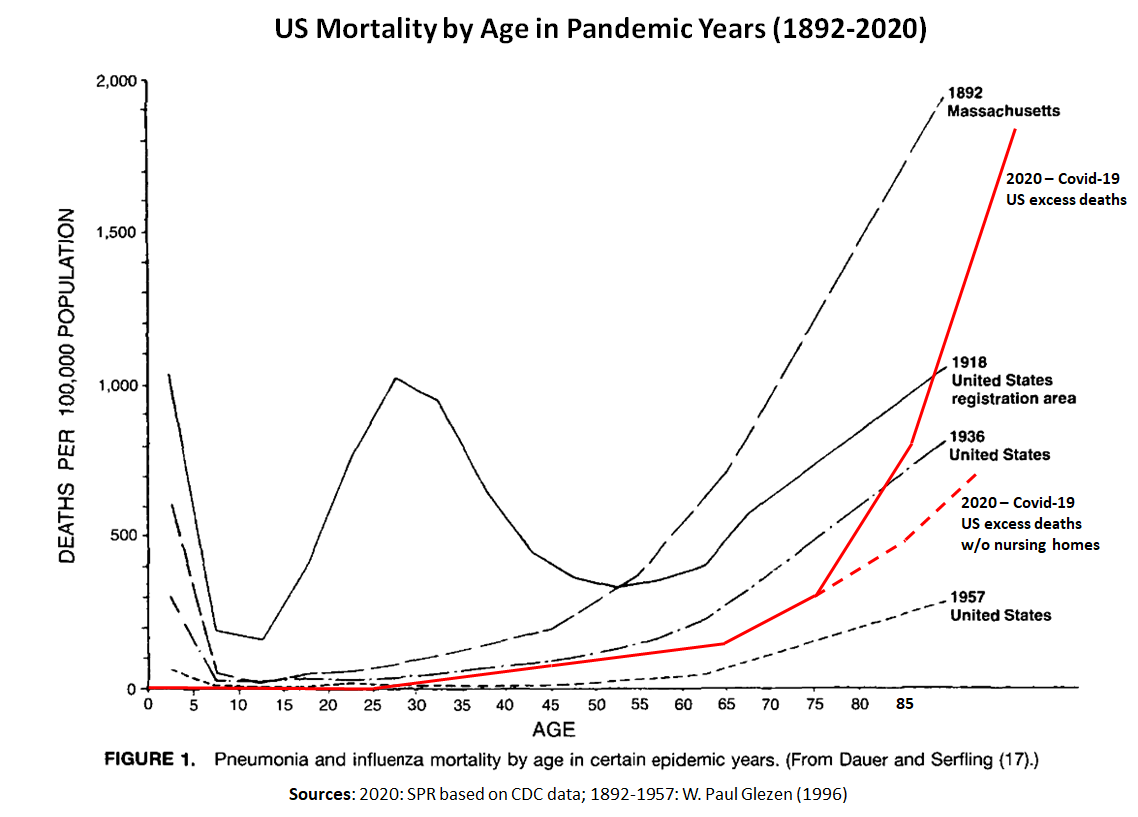
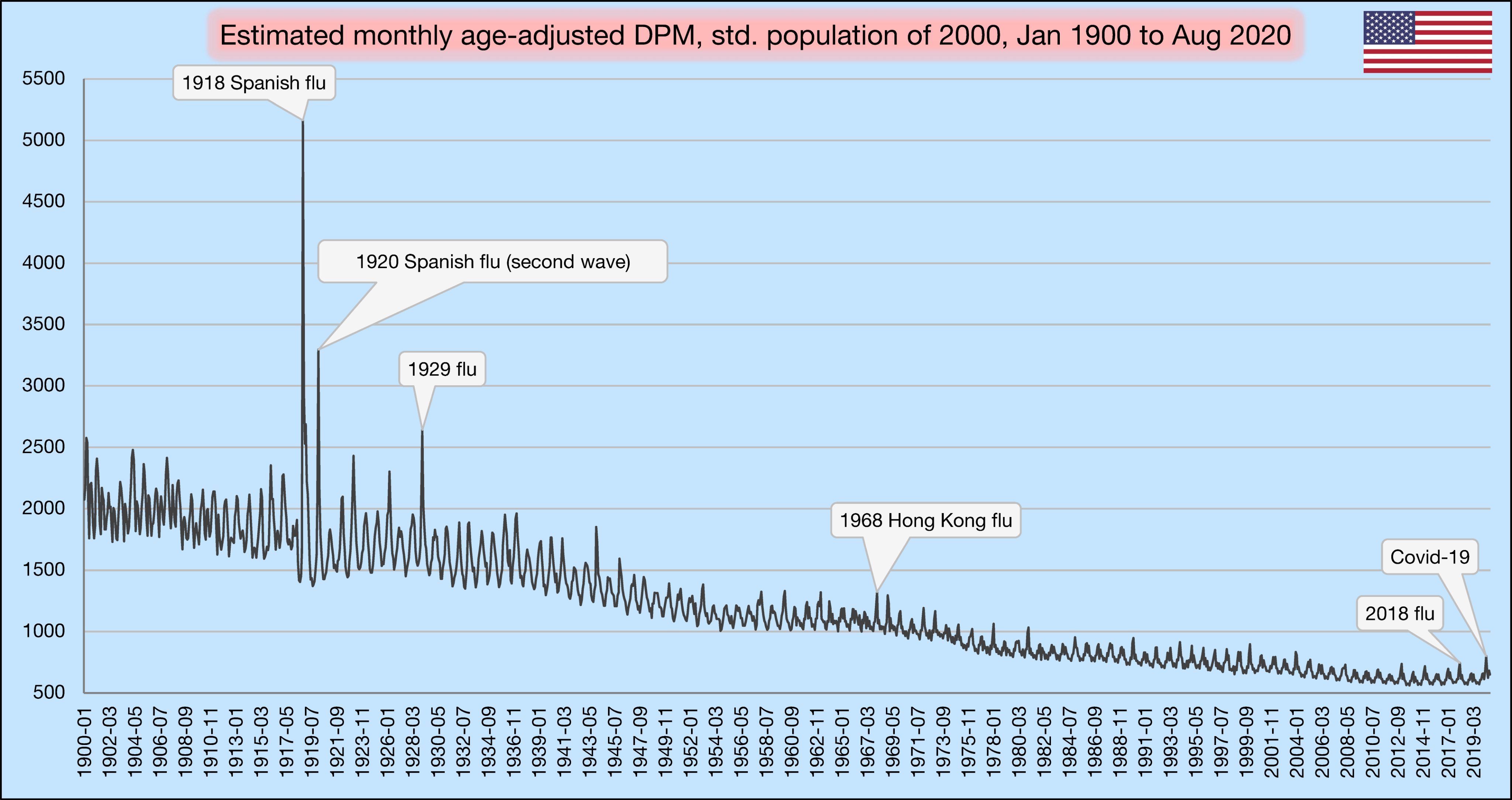
Lethality: According to the latest immunological studies, the overall infection fatality rate (IFR) of covid in the general population is about 0.1% to 0.5% in most countries, which is most closely comparable to the medium influenza pandemics of 1936, 1957 and 1968.
Vaccines: Real-world studies have shown a very high, but rapidly declining covid vaccine effectiveness against severe disease. Vaccination cannot prevent infection and transmission. Various severe and fatal vaccine adverse events have been reported, including in young people. A prior infection generally confers superior immunity compared to vaccination.
Treatment: For people at high risk or high exposure, early or prophylactic treatment is essential to prevent progression of the disease. According to numerous international studies, early outpatient treatment of covid may significantly reduce hospitalizations and deaths.
Age profile: The median age of covid deaths is over 80 years in most Western countries (78 in the US) and about 5% of the deceased had no serious preconditions. The age and risk profile of covid mortality is therefore comparable to normal mortality, but increases it proportionally.
Nursing homes: In many Western countries, about 50% of all covid deaths have occurred in nursing homes, which require targeted and humane protection. In some cases, care home residents died not from the coronavirus, but from weeks of stress and isolation.
Excess mortality: Overall, the pandemic has increased mortality by 5% to 25% in most Western countries. In some countries, up to 30% of additional deaths have been caused not by covid, but by indirect effects of the pandemic and lockdowns (including drug overdose deaths).
Antibodies: By the end of 2020, between 10% and 30% of the population in most Western countries had coronavirus antibodies. In India and some Latin American countries, coronavirus infection prevalence reached up to 75% by the summer of 2021.
Symptoms: About 30% of all infected persons show no symptoms. Overall, about 95% of all people develop at most mild or moderate symptoms and do not require hospitalization. Early outpatient treatment may significantly reduce hospitalizations.
Long covid: Up to 10% of symptomatic people experience post-acute or long covid, i.e. covid-related symptoms that last several weeks or months. Long covid may also affect younger and previously healthy people whose initial course of disease was rather mild.
Transmission: Indoor aerosols appear to be the main route of transmission of the coronavirus, while outdoor aerosols, droplets, as well as most object surfaces appear to play a minor role. The coronavirus season in the northern hemisphere usually lasts from November to April.
Masks: There is still little to no scientific evidence for the effectiveness of face masks in the general population, and the introduction of mandatory masks couldn’t contain or slow the epidemic in most countries. If used improperly, masks may increase the risk of infection.
Children and schools: In contrast to influenza, the risk of disease and transmission in children is rather low in the case of covid. There was and is therefore no medical reason for the closure of elementary schools or other measures specifically aimed at children.
Contact tracing: A WHO study of 2019 on measures against influenza pandemics concluded that from a medical perspective, contact tracing is “not recommended in any circumstances”. Contact tracing apps on cell phones have also proven ineffective in most countries.
Virus mutations: Similar to influenza viruses, mutations occur frequently in coronaviruses. Most of these mutations are insignificant, but some of them may increase the transmissibility, virulence or immune evasion of the virus to some extent.
Sweden: In Sweden, covid mortality without lockdown has been comparable to a strong influenza season and somewhat below the EU average. About 50% of Swedish deaths occurred in nursing homes and the median age of Swedish covid deaths was about 84 years.
Virus origin: The origin of the new coronavirus remains unknown, but the best evidence currently points to a covid-like pneumonia incident in a Chinese mine in 2012, whose virus samples were collected, stored and researched by the Wuhan Institute of Virology (WIV). Due to cooperations, some US labs may also have had access to these viruses.
Surveillance: NSA whistleblower Edward Snowden warned that the coronavirus pandemic may be used to expand global surveillance. Many governments have restricted fundamental rights of their citizens and announced plans to introduce digital biometric vaccine passports.
If you regard the United States as perhaps flawed but overall a force for good in the world . . .
If you scoff at the notion that the US, a republic founded on principles of freedom and democracy, has morphed into a world empire, perpetrating assassinations, coups d’état, acts of terror and illegal warfare . . .
If you want to promote peace but haven’t yet explored deceptive events that precipitate US warmongering . . .
. . . here is a volume that will clear the air and paint an honest picture of the significant, not-so-rosy impact US foreign policy and actions have had in the world around us.
USA: The Ruthless Empire, by Swiss historian and peace researcher Daniele Ganser, is the newly published English language translation of his book Imperium USA, originally written in German and published in 2020. Here is a summary of key points — including some lesser-known ones — along with remedies for a more peaceful future, that are covered in the book. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.





















 If you regard the United States as perhaps flawed but overall a force for good in the world . . .
If you regard the United States as perhaps flawed but overall a force for good in the world . . .