“In the current large population study of subjects, who were not vaccinated against SARS-CoV-2, we observed no increase in the incidence of myocarditis or pericarditis from day 10 after positive SARS-CoV-2.”
Remember when you were told to get vaccinated but you had concerns about myocarditis? Remember when the scientists, doctors and people we are meant to trust said not to worry because you were more likely to get myocarditis from Covid? Well, it wasn’t true.
A study published last month in the Journal of Clinical Medicine on MDPI took a look at the incidence of myocarditis and pericarditis in post COVID-19 unvaccinated patients. It was undertaken by the University of Jerusalem and Tel Aviv University and looked at 213,624 adult patients who had a documented positive COVID-19 test.
16,632 patients with a first vaccination received before COVID-19 infection were excluded, leaving 196,992 patients versus 590,976 in the control group, to study. The control group consisted of patients with one or more negative COVID-19 tests and no vaccination.
When the authors looked at the results of their study, they concluded that there was “no statistical difference in the incidence rate of both myocarditis and pericarditis… between the COVID-19 cohort and the control cohort” I.e. COVID-19 did not increase the risk of myocarditis and pericarditis when compared with those who did not get Covid.
These results tie in with a previous study in Nature, which I wrote about in April. This found a greater than 25% Increase in Cardiovascular events in under 40s during Vaccine rollout but NOT during Covid waves.
Numerous other studies have found that the vaccines increase the chances of myocarditis and pericarditis and this is openly acknowledged on government websites and vaccine reference material.
However, up until now, one of the excuses for continuing to give these vaccines was that you were more likely to get myocarditis or pericarditis with a Covid infection. This study shows this to be false.
Once again, a conspiracy theory has come true again.
From the very outset of this pandemic, the topic of natural infection has been a taboo. To suggest that anyone might have been better off risking infection and thereby gaining immunity from a respiratorial virus rather than hiding under the sofa for two years was seen as outrageous and irresponsible.
My theory is that the reason has always been political. And that’s tragic.
Generations have gone by that have understood it. A life strategy to flee all pathogens is deeply dangerous. The immune system, in order to be trained to protect against severe disease, needs exposure. Not to all things, of course, but to many pathogens that are not finally debilitating or fatal. We’ve evolved with pathogens in what Sunetra Gupta calls a “dangerous dance.” This dance is unavoidable, especially for fast-mutating viruses like SARS-CoV-2.
And yet from the beginning, this knowledge seemed to be lost. This is gravely embarrassing since it’s been known for 2,500 years. It was worse than just lost. As a person who wrote almost daily during the pandemic, I too was careful not to discuss this topic with too much bluntness. We all felt the political pressure to stay silent or at least cloud our prose with euphemisms.
The single most controversial sentence of the Great Barrington Declaration was this one: “The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk.”
That talk about building up immunity is what drove people bonkers, as if no one was somehow allowed to utter a settled scientific truth. And yet long before Fauci began to speak as if getting infected was the worst possible fate, he was more honest.
Even I knew (from what I learned in 9th grade and what my mother taught) that the pandemic would only end with endemicity naturally earned. That is precisely what is happening. The CDC’s publication MMWR printed a seroprevalence study showing that from December 2021 to February 2022 – that period during which it seemed like everyone in the country got covid – went from 33.5% to 57.7%. In children, it went from 44.2% to 75.2%. It’s higher in both groups now.That the study got no real attention to it shows that we are fast moving toward the end, and how? Not through vaccination, which protects against neither infection nor transmission. It ends with everyone meeting the virus. There is of course some threshold of herd immunity with this virus, though it keeps rising with each mutation, requiring ever more rounds of infection to achieve it. It is surely higher than 70% but probably less than 90% depending on population mobility and other factors.We can look at that data today and wonder. What if we had never locked down? What if we had gone on with life as normally while urging those in risk categories to wait it out a bit while we achieved endemicity? How long would it have taken to get there?
Might it have been over by the summer of 2020? It is possible. It’s hard to know such counterfactuals with precision, but it does seem highly likely that the lockdowns achieved nothing good, caused tremendous damage, and also unnecessarily prolonged the pandemic. In addition, they degraded everyone’s immune system: we didn’t just avoid covid but everything else too.
And the main reason was due to the unwillingness of public health authorities to talk about actual science. When Fauci was asked about natural immunity in September 2021, he said “I don’t have a really firm answer for you on that. That’s something that we’re going to have to discuss regarding the durability of the response…I think that is something that we need to sit down and discuss seriously.”
The WHO even changed its definition of herd immunity to exclude natural infection as a factor! The whole institution gave itself over to vaccine sales based on wild exaggerations of their effectiveness while all-but-denying robust and broad immunity through exposure.
A key political factor to natural immunity is that it does not call on government to assume totalitarian controls to stop a virus. It presumes the operations of a normal society. The government wanted all power and deployed it to stop the virus. Therefore, science was out of the question, replaced by political propaganda from start to finish.
It’s not well understood that the US policy from the very outset accepted and adopted a zero covid approach. That gradually unraveled over time as unworkable. Trump’s own advisors tricked him into believing that he could achieve that just like Xi Jinping did. He fell for it, and pushed the two weeks to flatten the curve under the belief that this would make the virus go away. His rhetoric that day set the stage for more than two years of utter nonsense.
And here we are all this time later and top headlines are finally admitting what should have been obvious from the beginning. For a virus this prevalent, it ends with widespread natural immunity. Here’s the Bloomberg headline:
The rest of the article is designed to walk back that core claim. We are still not ready to face the terrible realities that the lockdowns achieved nothing and that the vaccines did not end the pandemic. The taboo subject of meeting the virus is still today what it was 30 months ago, nearly unsayable.
My theory is that this is entirely for political reasons. They hatched a wild plan to control a virus that would come and go like all such viruses in history, and so therefore they had to pretend their efforts were essential to the great task. They never were. That’s the bitter reality.
Reflecting on this topic of exposure and immunity eventually leads a person to realize that we don’t need centralized control, coercion, and dictatorial power to manage a pandemic. Pandemics are unavoidable but they largely manage themselves while the best-possible outcomes rest with the intelligence of individuals informing choices based on their own risk assessment. (I feel like I’ve been writing some version of that sentence for 33 months.)
And this speaks to the big problem we have today. The people who did this to us have not admitted error and probably won’t. Despite all the failures, these same people are gearing up for another round of lockdowns based once again on the ideology that the worst-possible fate for anyone is to face a virus naturally and bravely.
Think about this: our lords and masters are saying that our only choice in the face of any prevalent pathogen is to hunker down, don’t hold parties, don’t send kids to school, don’t go to church, don’t go work, don’t travel, and instead just wait for them to make a fancy serum to inject in our arms, which we must accept whether we like it or not.
In short, a government that seeks to control all pathogenic spread is one with totalitarian powers that knows not human rights or freedoms.
Consortium News is being “reviewed” by NewsGuard, a U.S. government-linked organization that is trying to enforce a narrative on Ukraine while seeking to discredit dissenting views.
The organization has accused Consortium News, begun in 1995 by former Associated Press investigative reporter Robert Parry, of publishing “false content” on Ukraine.
It calls “false” essential facts about Ukraine that have been suppressed in mainstream media: 1) that there was a U.S.-backed coup in 2014 and 2) that neo-Nazism is a significant force in Ukraine. Reporting crucial information left out of corporate media is Consortium News‘ essential mission.
But NewsGuard considers these facts to be “myths” and is demanding Consortium News “correct” these “errors.”
Who is NewsGuard?
NewsGuard set itself up in 2018 as a judge of news organizations’ credibility. The front page of NewsGuard’s website shows that it is “partners” with the State Department and the Pentagon, as well as with several major corporations, such as Microsoft. The nature of these “partnerships” is not entirely clear.
NewsGuard is a private corporation that can shield itself from First Amendment obligations. But it has connections to formerly high-ranking U.S. government officials in addition to its “partnerships” with the State Dept. and the Pentagon.
Among those sitting on NewsGuard’s advisory board are Gen. Michael Hayden, the former Central Intelligence Agency and National Security Agency director; Tom Ridge, the first U.S. Homeland Security director and Anders Fogh Rasmussen, a former secretary general of NATO. NewGuard says its ”advisors provide advice and subject-matter expertise to NewsGuard. They play no role in the determinations of ratings or the Nutrition Label write ups of websites unless otherwise noted and have no role in the governance or management of the organization.”
The co-CEO, with former Wall Street Journal publisher Louis Gordon Crovitz, is Steven Brill, who in the 1990s published Brill’s Content, a magazine that was billed as a watchdog of the press, critiquing the role of the media to hold government to account. NewsGuard is a government-affiliated organization judging media like Consortium News that is totally independent of government or corporations.
NewsGuard has a rating process that results in a news organization receiving either a green or red label. Fox News and other major media, for example, have received green labels.
Getting a red label means that potentially millions of people that have the NewsGuard extension installed and operating on their browsers will see the green or red mark affixed to websites on social media and Google searches. (For individuals that do not already have it installed and operating on Microsoft’s browser, it costs $4.95 a month in the U.S., £4.95 in the U.K., or €4.95 in the EU to run the extension.)
According to NewsGuard, libraries in the U.S. and Britain have had it installed on their computers, and it is also being put on computers of U.S. active duty personnel. Slate reported in January 2019 that NewsGuard:
“struck a deal with Microsoft to incorporate those ratings into the tech giant’s Edge browser as an optional setting. That’s when the Guardian noticed that the Mail Online had been tagged by NewsGuard with a ‘red’ label, a reliability score of 3 out of 9, and the following warning: ‘Proceed with caution: This website generally fails to maintain basic standards of accuracy and accountability.’ For Microsoft Edge users with the ‘News Ratings’ feature turned on, that warning appeared alongside every link to the Mail Online—whether in Google search results, Facebook or Twitter feeds, or the Mail’s own homepage.”
Approach to Consortium News
Consortium News was contacted by NewsGuard analyst Zachary Fishman. In his request to speak to someone at Consortium News he said categorically that CN had published “false content” and that the interview would be on the record. “I’m hoping to talk with someone who could answer a few questions about its structure and editorial processes — including its ownership, its handling of corrections, and its publication of false content,” he wrote in an email.
As editor-in-chief, I informed him that our founder, editors and writers came from high levels of establishment journalism. I told him that in thousands of press interviews I’ve conducted over nearly half a century in journalism I had never known anyone accusing a prospective interviewee of misconduct upfront and then determining that the interview would be on the record, when the ground rules are usually set by the person being interviewed.
Fishman apologized and tried to say his mind wasn’t made up about Consortium News, when he had clearly stated that it was. “I do apologize that the wording of my email insinuated that I had come to a predetermined conclusion on whether your website has published false content, when I have not — be sure that I am interested in your responses to my questions,” he wrote in an email.
According to his LinkedIn profile, Fishman had one previous job in science and financial journalism that lasted 15 months for a company called Fastinform that is now defunct. Last month, all the links of his published pieces on LinkedIn went to a site that no longer exists. The links have now been removed.
Fishman has degrees in health, environment and science journalism and engineering physics. He has no experience in political reporting and especially of the politics of Eastern Europe and U.S.-Russia relations.
NewsGuard’s determination on Consortium News will be made by the analyst and, “At least one senior editor and NewsGuard’s co-CEOs review every Nutrition Label prior to publication to ensure that the rating is as fair and accurate as possible.”
Charge: There Was ‘No US-Backed Coup’
NewsGuard alleges that Consortium News has published “false content” by reporting that there was a U.S.-backed coup in Ukraine in 2014 and that neo-Nazis have significant influence in the country.
Fishman took issue with a:
“February 2022 article ‘Ukraine: Guides to Reflection,’ [which] asserted, ‘Hence, the inflation of Russian behavior in Ukraine (where Washington organized a coup against a democratically elected governmentbecause we disliked its political complexion) … .’
Fishman then wrote:
“The U.S. supported the Maidan revolution that ousted then-Ukraine President Viktor Yanikovych (sic) in 2014 — including a December 2013 visit by John McCain to Kyiv in support of protesters — but there is no evidence that the U.S. ‘organized’ a ‘coup.’ Instead, it has the markings of a popular uprising, precipitated by widely covered protests against Yanukovych’s decision to suspend preparations for the signing of an association and free-trade agreement with the European Union.”
Viktor Yanukovych was democratically elected as president of Ukraine in 2010 in an election certified by the Organization for Security and Cooperation in Europe, a fact not mentioned in NewsGuard’s writings on the change of government in Ukraine. Even though Yanukovych agreed to an EU political settlement and early elections, violence forced him to flee from the capital on Feb. 21, 2014. Reporting that the neo-Nazi Right Sector was at the forefront of the violent overthrow, The New York Times (green check) wrote earlier that day:
“Dmytro Yarosh, the leader of Right Sector, a coalition of hard-line nationalist groups, reacted defiantly to news of the settlement, drawing more cheers from the crowd.
‘The agreements that were reached do not correspond to our aspirations,’ he said. ‘Right Sector will not lay down arms. Right Sector will not lift the blockade of a single administrative building until our main demand is met — the resignation of Yanukovych.’ He added that he and his supporters were ‘ready to take responsibility for the further development of the revolution.’ The crowd shouted: ‘Good! Good!’
A study on the violence used to overthrow the government, by Prof. Serhiy Kudelia, a political scientist at Baylor University, says the overthrow succeeded because of “the embeddedness of violent groups” in a non-violent protest. The violence began on Dec. 1, 2013 when these violent groups attacked police with “iron chains, flares, stones and petrol bombs” and tried to ram a bulldozer through police lines. The police viciously fought back that day.
As the International Business Times (IBT) (green check) wrote about these groups at the time:
“According to a member of anti-fascist Union Ukraine, a group that monitors and fights fascism in Ukraine, ‘There are lots of nationalists here [EuroMaidan] including Nazis. They came from all over Ukraine, and they make up about 30% of protesters.
Different groups [of anarchists] came together for a meeting on the Maidan. While they were meeting, a group of Nazis came in a larger group, they had axes and baseball bats and sticks, helmets, they said it was their territory. They called the anarchists things like Jews, blacks, communists. There weren’t even any communists, that was just an insult. The anarchists weren’t expecting this and they left. People with other political views can’t stay in certain places, they aren’t tolerated,’ a member of the group continued.”
The violence by far-right groups was evidently condoned by Sen. John McCain who expressed his support for the uprising by addressing the Maidan crowd later that month. Assistant Secretary of State Victoria Nuland and then U.S. ambassador Geoffrey Pyatt visited the square after the violence had broken out.
NewsGuard’s account of the events of Feb. 21, 2014 says that even though Yanukovych agreed to the early elections, “angry protestors demanded Yanukovych’s immediate resignation,” and he fled on that day after “hundreds of police guarding government buildings abandoned their posts.” NewsGuard then says “protestors took control of several government buildings the next day.”
Government Buildings Seized
But protestors had already seized government buildings as early as December 2013. On Jan. 24 protestors broke into the Agriculture Ministry building in Kiev and occupied it. On the same day barricades were set up near the presidential headquarters. Government buildings in the west of the country had also been occupied. The Guardian (green check) reported on Jan. 24:
“There were dramatic developments in the west of the country on Thursday as hundreds of people forced their way into the office of the regional governor in the city of Lviv, and forced him to sign a resignation letter. Oleh Salo, a Yanukovych appointee in a city where support for the president is in the low single digits, later said he signed the letter under duress and was rescinding his resignation.
Thousands also stormed regional administration headquarters in Rivne on Thursday, breaking down doors and demanding the release of people detained in the unrest there, Unian news agency reported. In the town of Cherkasy, 125 miles south of Kiev, about 1,000 protesters took over the first two floors of the main administration building and lit fires outside the building.
Similar action took place in Ternopil, Ivano-Frankivsk and Khmelnytsky in western and central Ukraine, as well as parts of the north-east, the Party of the Regions said.”
Protestors had begun occupying Kiev City Hall in December, with a portrait of Ukraine’s World War II fascist leader Stepan Bandera hanging from the rafters. On the night of Feb. 21, the leader of the Neo-fascist Right Sector, Andriy Parubiy, announced that the Verkhovna Rada (parliament), the Presidential Administration, the Cabinet of Ministers and the Ministry of Internal Affairs had all come under control of the protestors.
Therefore NewsGuard has published “false content” by reporting that government buildings were occupied the day after Yanukovych fled the capital. It should print a correction.
On the day after Yanukovych fled, the Rada voted without the presence of Yanukovych’s party — the largest in the country — to impeach him after the fact of his violent overthrow. NewsGuard omitted the key fact that the impeachment vote was tainted by the absence of Yanukovych’s party and that the impeachment became largely irrelevant after violence forced him to flee the capital.
Democratically-elected leaders are removed by electoral defeat, impeachment or votes of no confidence, not by violence. NewsGuard writes that “hundreds of police guarding government buildings abandoned their posts” on the day Yanukovych was forced out, but doesn’t say why. As Jacobin (NewsGuard green check) magazine reports:
“Whatever one thinks of the Maidan protests, the increasing violence of those involved was key to their ultimate victory. In response to a brutal police crackdown, protesters began fighting with chains, sticks, stones, petrol bombs, even a bulldozer — and, eventually, firearms, all culminating in what was effectively an armed battle in February, which left thirteen police officers and nearly fifty protesters dead. The police ‘could no longer defend themselves’ from protesters’ attacks,’ writes political scientist Sergiy Kudelia, causing them to retreat, and precipitating Yanukovych’s exit.”
NewsGuard calls the events a “revolution,” yet revolutions in history have typically been against monarchs or dictators, not against democratically-elected leaders. For instance, the 1776 American Revolution, the 1789 French Revolution, the 1917 Russian Revolution, the 1952 Egyptian Revolution, the 1979 Iranian Revolution and countless others were against monarchs. Coups have been against both elected and non-elected leaders.
By any measure, Yanukovych’s ouster was an unconstitutional change in government. His “impeachment” without his party present for the vote came after government buildings had been seized and after violence drove him from the capital.
Circumstantial Evidence
In its version of these events, NewsGuard only refers to circumstantial evidence of the coup, interpreting it as U.S. “support” for a “revolution” against a democratically-elected president.
NewsGuard fails to point out that McCain, Sen. Christopher Murphy (D-CT) as well as Nuland appeared on stage in the Maidan with Oleh Tyahnybok, leader of the Neo-fascist Svoboda Party, formerly known as the Social National Party.
NewsGuard does not consider how such events would be seen in the United States if a senior Russian foreign ministry official, two leading Russian lawmakers and Russia’s ambassador to the U.S. appeared on stage with a far-right American leader to address a crowd on the Washington Mall seeking to oust an elected U.S. president. If that president were overthrown violently, would Americans think it Russian-backed the coup?
NewsGuard discusses Nuland’s 2013 speech in which she revealed that since 1991 the U.S. had spent $5 billion to help bring about Ukraine’s “aspirations.” What it fails to point out is that U.S. aspirations were to turn Ukraine towards the West and away from Russia. And the U.S. had work to do.
NewsGuard does not mention that part of the $5 billion the U.S. spent was to help organize protests. There was genuine popular dissatisfaction with Yanukovych that the NED nurtured and trained. Jacobin reported of the 2014 events:
“US officials, unhappy with the scuttled EU deal, saw a similar chance in the Maidan protests. Just two months before they broke out, the NED’s then president, pointing to Yanukovych’s European outreach, wrote that “the opportunities are considerable, and there are important ways Washington could help.”
In practice, this meant funding groups like New Citizen, which the Financial Timesreported “played a big role in getting the protest up and running,” led by a pro-EU opposition figure. Journalist Mark Ames discovered the organization had received hundreds of thousands of dollars from US democracy promotion initiatives.”
The National Endowment for Democracy (NED), which funds NGOs in countries the U.S. targets for regime change, on Feb. 25, the day after the Russian invasion, deleted all projects in Ukraine it funded, which are archived here. The NED meddled in Ukrainian politics in 2004 in the so-called Orange Revolution. The Washington Post (green check) wrote in 1991 that what the C.I.A. once did in secret — destabilizing and overthrowing regimes — the NED was now doing openly.
C.I.A. or NED-led coups are never made up out of whole cloth. The U.S. works with genuine opposition movements within a country, sometimes popular uprisings, to finance, train and direct them. This U.S. has a long history of overthrowing foreign governments, the most infamous examples being Guatemala in 1952, Iran in 1953 and Chile in 1973.
The long-time NED head, Carl Gerhsman, said in 20——16 that the NED has been involved in Ukraine since the 1980’s and he praised the “overthrow of Yanukovych.”
Nuland-Pyatt Tape Omitted
Most significantly, NewsGuard’s attempt to refute U.S. involvement in the coup omits the 2014 intercepted and leaked telephone call between Nuland and Pyatt, the then U.S. ambassador to Ukraine, in which the two discuss who will make up the new government weeks before Yanukovych was overthrown.
On the leaked tape, Nuland and Pyatt talk about “midwifing” a new government; Vice President Joe Biden’s role, and setting up meetings with Ukrainian politicians to make it happen. Nuland says the prime minister should be Arseniy Yatsenyuk, and indeed he became prime minister after the coup.
At the time, the BBC (green check) wrote of the leak: “The US says that it is working with all sides in the crisis to reach a peaceful solution, noting that ‘ultimately it is up to the Ukrainian people to decide their future’. However this transcript suggests that the US has very clear ideas about what the outcome should be and is striving to achieve these goals.”
The U.S. State Department never denied the authenticity of the video, and even issued an apology to the European Union after Nuland is heard on the tape saying, “Fuck the EU.” Mainstream media at the time focused almost exclusively on that off-color remark as a distraction from the greater significance of U.S. interference in Ukraine’s internal affairs.
Why did Nuland say, “Fuck the EU”? At the time she said it, France, Germany and Poland were working for the EU on a political settlement with Russia to the Maidan crisis that would leave Yanukovych in power.
Indeed the E.U. brokered a deal with Yanukovych, who agreed to early elections by December, a restoration of the 2004 Constitution and an amnesty for all protestors, clearing the way for no one to be held responsible for the violent ouster. Yanukovych announced the agreement, with E.U. officials at his side in Kiev, on Feb. 21, 2014. Later that day he was violently driven from power.
Leaving the historic role of the NED and the essential Nuland-Pyatt conversation out of its reporting is an omission of evidence by NewsGuard, typical of corporate media. Omitting crucial elements of a story changes its meaning and in this case undermines NewsGuard’s account of the events of 2014.
This is an excellent example of why Parry started Consortium News: to report on crucial information that corporate media sometimes purposely and deceptively leave out to change the meaning of a story. NewsGuard should correct its story about the coup, not Consortium News. NewsGuard invites readers to request corrections by emailing them at corrections@newsguardtech.com.
Likely Reasons for the Coup
U.S. enabled Yeltsin’s 1996 reelection
Wall Street and Washington swept in after the fall of the Soviet Union in 1991 under a pliable Boris Yeltsin (who received direct U.S. help to win re-election in 1996) to asset-strip the formerly state-owned industries, enrich themselves and a new class of oligarchs and impoverish the former Soviet people.
The ascension of Vladimir Putin to power on New Year’s Eve 1999 gradually began to curb U.S. influence in post-Soviet Russia, especially after Putin’s 2007 Munich Security Conference speech, in which he blasted U.S. unilateral aggression, especially in Iraq.
Eventually Putin restored sovereignty over much of the Russian economy, turning Washington and Wall Street against him. (As President Joe Biden has now made clear on more than one occasion, the U.S. aim is to overthrow him.)
In his 1997 book,The Grand Chessboard: American Primacy and Its Geostrategic Imperatives, former U.S. national security adviser Zbigniew Brzezinski wrote:
“Ukraine, a new and important space on the Eurasian chessboard, is a geopolitical pivot because its very existence as an independent country helps to transform Russia. Without Ukraine, Russia ceases to be a Eurasian empire. Russia without Ukraine can still strive for imperial status, but it would then become a predominantly Asian imperial state.”
Thus U.S. “primacy,” or world dominance, which still drives Washington, is not possible without control of Eurasia, as Brzezinski argued, and that’s not possible without control of Ukraine by pushing Russia out (U.S. takeover of Ukraine in the 2014 coup) and dominating Moscow as it did when this was written in the 1990s.
Deep Western involvement in Ukrainian politics and economy never ended from those early post-Soviet days. When Yanukovych acted legally (the Rada authorized it) to reject the European Union association agreement in favor of a Russian economic package on better terms, it threatened to curtail Western economic involvement. Yanukovych became a marked man.
Yanukovych had already made Russian an official language, he had rejected NATO membership, and reversed his pro-Western predecessor’s move to glorify Nazi collaborators. Yanukovych’s predecessor, President Viktor Yuschenko, had made Ukraine’s World War II-era fascist leader Stepan Bandera a “Hero of Ukraine.”
There was genuine popular dissatisfaction among mostly Western Ukrainians with Yanukovych, which intensified and became violent after he rejected the EU deal. Within months he was overthrown.
After the Coup
The U.S.-installed government in Kiev outlawed political parties, including the Communist Party, and stripped Russia as an official language. Yanukovych’s Party of the Regions was banned in several oblasts and eventually collapsed. An American citizen became finance minister and Vice President Joe Biden became Barack Obama’s virtual viceroy in Ukraine.
Videos have emerged of Biden giving instructions to the nominal president at the time, Petro Poroshenko. By his own admission, Biden forced the resignation of Viktor Shokin, Ukraine’s prosecutor general.
Shokin testified under oath that he was about to investigate Burisma Holdings, the company on which the vice president’s son was given a lucrative board membership just months after the U.S.-backed coup.
Biden, other U.S. officials, and the media at the time lied that Shokin was removed because he was corrupt. State Dept. memos released this year and published by Just the News (green-check) actually praise Shokin for his anti-corruption work. The question of whether the leader of a foreign nation has the right remove another country’s prosecutor was buried.
Eight days after nearly 50 anti-coup protestors in Odessa were burned to death on May 2, 2014 by far-right counter-protestors dominated by Right Sector, the coup-resisting provinces of Luhansk and Donetsk in the Donbass region declared independence from Ukraine. Russia began assisting them and, after a visit to Kiev by then C.I.A. Director John Brennan, Poroshenko launched a war against the separatists that lasted eight years, killing thousands of civilians, until Russia intervened in the civil conflict in February.
After the coup, NATO began arming, training and conducting exercises with the Ukrainian military, turning it into a de facto NATO member. These were not just the interests of part of Ukraine that were being served, but those of powerful foreign actors. It was akin to a 19th century-style colonial takeover of a country.
Charge: Nazi Influence ‘Exaggerated’
Torchlight parade behind portrait of Bandera on his birthday, Jan. 1, 2015. (Wikimedia Commons)
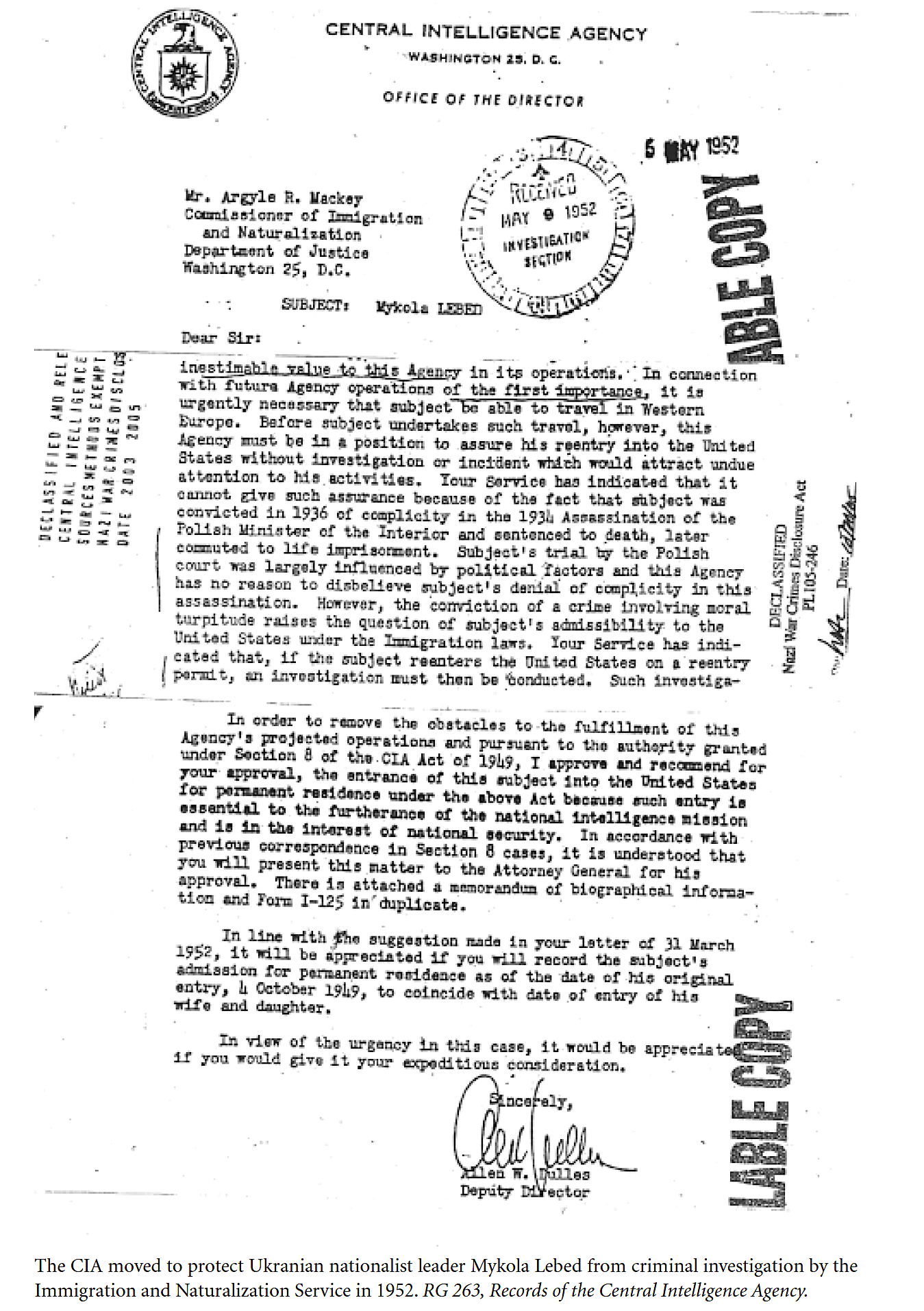
The U.S. relationship with Ukrainian fascists began after the Second World War. During the war, units of the Organization of Ukrainian Nationalists (OUN-B) took part in the Holocaust, killing at least 100,000 Jews and Poles. Mykola Lebed, a top aide to Stepan Bandera, the leader of the fascist OUN-B, was recruited by the C.I.A. after the war, according to a 2010 study by the U.S. National Archives.
The government study said, “Bandera’s wing (OUN/B) was a militant fascist organization.” Bandera’s closest deputy, Yaroslav Stetsko, said: “I… fully appreciate the undeniably harmful and hostile role of the Jews, who are helping Moscow to enslave Ukraine… I therefore support the destruction of the Jews and the expedience of bringing German methods of exterminating Jewry to Ukraine….”
The study says: “At a July 6, 1941, meeting in Lwów, Bandera loyalists determined that Jews ‘have to be treated harshly… We must finish them off… Regarding the Jews, we will adopt any methods that lead to their destruction.’”
Lebed himself proposed to “’cleanse the entire revolutionary territory of the Polish population,’ so that a resurgent Polish state would not claim the region as in 1918.” Lebed was the “foreign minister” of a Banderite government in exile, but he later broke with Bandera for acting as a dictator. The U.S. Army Counterintelligence Corps termed Bandera “extremely dangerous” yet said he was “looked upon as the spiritual and national hero of all Ukrainians…”
The C.I.A. was not interested in working with Bandera, pages 81-82 of the report say, but the British MI6 was. “MI6 argued, Bandera’s group was ‘the strongest Ukrainian organization abroad, is deemed competent to train party cadres, [and] build a morally and politically healthy organization…’” An early 1954 MI6 summary noted that, “the operational aspect of this [British] collaboration [with Bandera] was developing satisfactorily. Gradually a more complete control was obtained over infiltration operations … “
C.I.A.’s Allen Dulles asks U.S. Immigration to allow Lebed re-entry to U.S. despite murder conviction. (Click to enlarge.)
Britain ended its collaboration with Bandera in 1954. West German intelligence, under former Nazi intelligence chief Reinhard Gehlen, then worked with Bandera, who was eventually assassinated with cyanide dust by the KGB in Munich in 1959.
Instead of Bandera, the C.I.A. was interested in Lebed, despite his fascist background. They set him up in an office in New York City from which he directed sabotage and propaganda operations on the agency’s behalf inside Ukraine against the Soviet Union. The U.S. government study says:
“CIA operations with these Ukrainians began in 1948 under the cryptonym CARTEL, soon changed to AERODYNAMIC. … Lebed relocated to New York and acquired permanent resident status, then U.S. citizenship. It kept him safe from assassination, allowed him to speak to Ukrainian émigré groups, and permitted him to return to the United States after operational trips to Europe. Once in the United States, Lebed was the CIA’s chief contact for AERODYNAMIC. CIA handlers pointed to his ‘cunning character,’ his ‘relations with the Gestapo and … Gestapo training,’ and the fact that he was ‘a very ruthless operator.’”
The C.I.A. worked with Lebed on sabotage and pro-Ukrainian nationalist propaganda operations inside Ukraine until Ukraine’s independence in 1991. “Mykola Lebed’s relationship with the CIA lasted the entire length of the Cold War,” the study says. “While most CIA operations involving wartime perpetrators backfired, Lebed’s operations augmented the fundamental instability of the Soviet Union.”
Bandera Revival
The U.S. thus covertly kept Ukrainian fascist ideas alive inside Ukraine until at least Ukrainian independence was achieved. “Mykola Lebed, Bandera’s wartime chief in Ukraine, died in 1998. He is buried in New Jersey, and his papers are located at the Ukrainian Research Institute at Harvard University,” the U.S. National Archives study says.
The successor organization to the OUN-B in the United States did not die with him, however. It had been renamed the Ukrainian Congress Committee of America (UCCA), according to IBT.
“By the mid-1980s, the Reagan administration was honeycombed with UCCA members. Reagan personally welcomed [Yaroslav] Stetsko, the Banderist leader who oversaw the massacre of 7,000 Jews in Lviv, in the White House in 1983,” IBTreported. “Following the demise of Yanukovich’s regime, the UCCA helped organise rallies in cities across the US in support of the EuroMaidan protests,” it reported.
That is a direct link between Maidan and WWII-era Ukrainian fascism.
Despite the U.S. favoring the less extreme Lebed over Bandera, the latter has remained the more inspiring figure in Ukraine.
In 1991, the first year of Ukraine’s independence, the Neo-fascist Social National Party, later Svoboda Party, was formed, tracing its provenance directly to Bandera. It had a street named after Bandera in Liviv, and tried to name the city’s airport after him. (Svoboda won 10 percent of the Rada’s seats in 2012 before the coup and before McCain and Nuland appeared with its leader the following year.)
In 2010, pro-Western Ukrainian President Viktor Yushchenko declared Bandera a Hero of Ukraine, a status reversed by Yanukovych, who was overthrown.
More than 50 monuments, busts and museums commemorating Bandera have been erected in Ukraine, two-thirds of which have been built since 2005, the year the pro-American Yuschenko was elected. A Swiss academic study says:
“On January 13, 2011, the L’vivs’ka Oblast’ Council, meeting at an extraordinary session next to the Bandera monument in L’viv, reacted to the abrogation [skasuvannya] of Viktor Yushchenko’s order about naming Stepan Bandera a ‘Hero of Ukraine” by affirming that ‘for millions of Ukrainians Bandera was and remains a Ukrainian Hero notwithstanding pitiable and worthless decisions of the courts’ and declaring its intention to rename ‘Stepan Bandera Street’ as ‘Hero of Ukraine Stepan Bandera Street.’”
Torchlit parades behind Bandera’s portrait are common in Ukrainian cities, particularly on Jan. 1, his birthday, including this year.
Mainstream on Neo-Nazis
From the start of the 2013-2014 events in Ukraine, Consortium News founder Robert Parry and other writers began providing the evidence NewsGuard says doesn’t exist, reporting extensively on the coup and the influential role of Ukraine’s neo-Nazis. At the time, corporate media also reported on the essential part neo-Nazis played in the coup.
As The New York Timesreported, the neo-nazi group, Right Sector, had the key role in the violent ouster of Yanukovych. The role of Neo-fascist groups in the uprising and its influence on Ukrainian society was well reported by mainstream media outlets at the time.
The BBC, the NYT, the Daily Telegraph and CNN all reported on Right Sector, C14 and other extremists’ role in the overthrow of Yanukovych. The BBC ran this report a week after his ouster:
And this one in July 2015:
After the coup a number of ministers in the new government came from Neo-fascist parties. NBC News (green check) reported in March 2014: “Svoboda, which means ‘Freedom,’ was given almost a quarter of the Cabinet positions in the interim government formed after the ouster of President Viktor Yanukovych in February.”
Svoboda’s leader, Tyahnybok, whom McCain and Nuland stood on stage with, once called for the liberation of Ukraine from the “Muscovite-Jewish mafia.” The International Business Times (green check) reported:
“In 2005 Tyahnybok signed an open letter to then Ukrainain president Viktor Yushchenko urging him to ban all Jewish organisations, including the Anti-Defamation League, which he claimed carried out ‘criminal activities [of] organised Jewry’, ultimately aimed at the genocide of the Ukrainian people.”
Before McCain and Nuland embraced Tyahnybok and his social national party, it was condemned by the European Parliament, which said in 2012:
“[Parliament] recalls that racist, anti-Semitic and xenophobic views go against the EU’s fundamental values and principles and therefore appeals to pro-democratic parties in the Verkhovna Rada [Ukraine’s legislature] not to associate with, endorse, or form coalitions with this party.”
Such mainstream reports on Banderism have stopped as the Neo-fascist role in Ukraine was suppressed in Western media once Putin made “de-nazification” a goal of the invasion.
The Azov Battalion, which arose during the coup, became a significant force in the war against the Russian-speaking people of the Donbass, who resisted the coup. Its commander, Andriy Biletsky, infamously said Ukraine’s mission is to “lead the White Races of the world in a final crusade for their survival … against the Semite-led Untermenschen.”
In 2014 the now Azov Regiment was officially incorporated into Ukraine’s National Guard under the control of the Ministry of Internal Affairs. It is further integrated into the state by working closely with the SBU intelligence service. Azov is the only known Neo-fascist component in a nation’s military anywhere in the world.
As part of the Ukraine military, Azov members have still sported yellow arm bands with the Wolfsangel once worn by German SS troops in World War II. Including the atrocities it has continued to commit, Azov shows the world that integration into the state has not denazified them. On the contrary, it may have increased its influence on the state.
The U.S. and NATO have also trained and armed Azov since Barack Obama had denied lethal aid to Ukraine. One reason Obama declined sending arms to Ukraine was because he was afraid they may fall into these right-wing extremists’ hands. According to the green-checked New York Times,
“Mr. Obama continues to pose questions indicating his doubts. ‘O.K., what happens if we send in equipment — do we have to send in trainers?’ said one person paraphrasing the discussion on the condition of anonymity. ‘What if it ends up in the hands of thugs? What if Putin escalates?”
NewsGuard’s Objections
Collage of Neo-fascist leader Oleh Tyahnybok. meeting with McCain, Biden and Nuland. (Facebook image by Red, White and You of clip from film Ukraine on Fire)
NewsGuard’s argument against the major influence of neo-Nazi groups in Ukraine rests on Neo-fascist political parties faring poorly at the polls. This ignores the stark fact that these groups engage instead in extra-parliamentary extremism.
In its charge against Consortium News for publishing “false content” about Neo-fascism in Ukraine, NewsGuard’s Fishman wrote:
“There isn’t evidence that Nazism has a substantial influence in Ukraine. Radical far-right groups in Ukraine do represent a ‘threat to the democratic development of Ukraine,’ according to 2018 Freedom House report. But it also stated that far-right extremists have poor political representation in Ukraine and no plausible path to power — for example, in the 2019 parliamentary elections, the far-right nationalist party Svoboda won 2.2 percent of the vote, while the Svoboda candidate, Ruslan Koshulynskyy, won just 1.6 percent of the vote in the presidential election.”
But this argument of focusing on elections results has been dismissed by a number of mainstream sources, not least of which is the Atlantic Council, probably the most anti-Russian think tank in the world. In a 2019 article, a writer for the Atlantic Council said:
“To be clear, far-right parties like Svoboda perform poorly in Ukraine’s polls and elections, and Ukrainians evince no desire to be ruled by them. But this argument is a bit of ‘red herring.’ It’s not extremists’ electoral prospects that should concern Ukraine’s friends, but rather the state’s unwillingness or inability to confront violent groups and end their impunity. Whether this is due to a continuing sense of indebtedness to some of these groups for fighting the Russians or fear they might turn on the state itself, it’s a real problem and we do no service to Ukraine by sweeping it under the rug.” [Emphasis added.]
“Fear that they might turn on the state itself,” acknowledges the powerful leverage these groups have over the government. The Atlantic Council piece then underscores how influential these groups are:
“It sounds like the stuff of Kremlin propaganda, but it’s not. Last week Hromadske Radio revealed that Ukraine’s Ministry of Youth and Sports is funding the neo-Nazi group C14 to promote ‘national patriotic education projects’ in the country. On June 8, the Ministry announced that it will award C14 a little less than $17,000 for a children’s camp. It also awarded funds to Holosiyiv Hideout and Educational Assembly, both of which have links to the far-right. The revelation represents a dangerous example of law enforcement tacitly accepting or even encouraging the increasing lawlessness of far-right groups willing to use violence against those they don’t like.
Since the beginning of 2018, C14 and other far-right groups such as the Azov-affiliated National Militia, Right Sector, Karpatska Sich, and others have attacked Roma groups several times, as well as anti-fascist demonstrations, city council meetings, an event hosted by Amnesty International, art exhibitions, LGBT events, and environmental activists. On March 8, violent groups launched attacks against International Women’s Day marchers in cities across Ukraine. In only a few of these cases did police do anything to prevent the attacks, and in some they even arrested peaceful demonstrators rather than the actual perpetrators.”
The Atlantic Council is not the only anti-Russian outfit that recognizes the dangerous power of the Neo-fascist groups in Ukraine. Bellingcatpublished an alarming 2018 article headlined, “Ukrainian Far-Right Fighters, White Supremacists Trained by Major European Security Firm.”
NATO has also trained the Azov Regiment, directly linking the U.S. with far-right Ukrainian extremists.
The Hill reported in 2017 in an article headlined, “The reality of neo-Nazis in Ukraine is far from Kremlin propaganda,” that:
“Some Western observers claim that there are no neo-Nazi elements in Ukraine, chalking the assertion up to propaganda from Moscow. Unfortunately, they are sadly mistaken.
There are indeed neo-Nazi formations in Ukraine. This has been overwhelmingly confirmed by nearly every major Western outlet. The fact that analysts are able to dismiss it as propaganda disseminated by Moscow is profoundly disturbing.
Azov’s logo is composed of two emblems — the wolfsangel and the Sonnenrad — identified as neo-Nazi symbols by the Anti-Defamation League. The wolfsangel is used by the U.S. hate group Aryan Nations, while the Sonnenrad was among the neo-Nazi symbols at this summer’s deadly march in Charlottesville.
Neo-facism has infected Ukrainian popular culture as well. A half-dozen neo-Nazi music groups held a concert in 2019 commemorating the day Nazi Germany invaded the Soviet Union.
Amnesty International in 2019 warned that “Ukraine is sinking into a chaos of uncontrolled violence posed by radical groups and their total impunity. Practically no one in the country can feel safe under these conditions.”
Zelensky & Neo-Nazis
One of Ukraine’s most powerful oligarchs from the early 1990s, Ihor Kolomoisky, was an early financial backer of the Neo-Nazi Azov Battalion. According to a 2015 Reuters (green-checked) report:
“Many of these paramilitary groups are accused of abusing the citizens they are charged with protecting. Amnesty International has reported that the Aidar battalion — also partially funded by Kolomoisky — committed war crimes, including illegal abductions, unlawful detention, robbery, extortion and even possible executions.
Other pro-Kiev private battalions have starved civilians as a form of warfare, preventing aid convoys from reaching separatist-controlled areas of eastern Ukraine, according to the Amnesty report.
Some of Ukraine’s private battalions have blackened the country’s international reputation with their extremist views. The Azov battalion, partially funded by Taruta and Kolomoisky, uses the Nazi Wolfsangel symbol as its logo, and many of its members openly espouse neo-Nazi, anti-Semitic views. The battalion members have spoken about “bringing the war to Kiev,” and said that Ukraine needs “a strong dictator to come to power who could shed plenty of blood but unite the nation in the process.”
In April 2019, the F.B.I. began investigating Kolomoisky for alleged financial crimes in connection with his steel holdings in West Virginia and northern Ohio. In August 2020 the U.S. Department of Justice filed civil forfeiture complaints against him and a partner:
“The complaints allege that Ihor Kolomoisky and Gennadiy Boholiubov, who owned PrivatBank, one of the largest banks in Ukraine, embezzled and defrauded the bank of billions of dollars. The two obtained fraudulent loans and lines of credit from approximately 2008 through 2016, when the scheme was uncovered, and the bank was nationalized by the National Bank of Ukraine. The complaints allege that they laundered a portion of the criminal proceeds using an array of shell companies’ bank accounts, primarily at PrivatBank’s Cyprus branch, before they transferred the funds to the United States. As alleged in the complaint, the loans were rarely repaid except with more fraudulently obtained loan proceeds.”
Meanwhile, the Azov backer’s television channel had by this time aired the hit TV show Servant of the People (2015-2019), which catapulted Volodymyr Zelensky to fame and ultimately into the presidency under the new Servant of the People Party. The former actor and comedian’s presidential campaign was bankrolled by Kolomoisky, according to multiple reports, including this one by Radio Free Europe (not rated).
During the presidential campaign, Politico reported:
“Kolomoisky’s media outlet also provides security and logistical backup for the comedian’s campaign, and it has recently emerged that Zelenskiy’s legal counsel, Andrii Bohdan, was the oligarch’s personal lawyer. Investigative journalists have also reported that Zelenskiy traveled 14 times in the past two years to Geneva and Tel Aviv, where Kolomoisky is based in exile.”
Before their run-off election, Petro Poroshenko called Zelensky “Kolomoisky’s puppet.” According to the Pandora Papers, Zelensky stashed funds he received from Kolomoisky off shore.
During the campaign Zelensky was asked about Bandera. He said it was “cool” that many Ukrainians consider Bandera a hero.
Zelensky was elected president on the promise of ending the Donbass war. About seven months into his term he traveled to the front line in Donbass to tell Ukrainian troops, where Azov is well-represented, to lay down their arms. Instead he was sent packing. The Kyiv Post (green check) reported:
“When one veteran, Denys Yantar, said they had no arms and wanted instead to discuss protests against the planned disengagement that had taken place across Ukraine, Zelensky became furious.
‘Listen, Denys, I’m the president of this country. I’m 41 years old. I’m not a loser. I came to you and told you: remove the weapons. Don’t shift the conversation to some protests,’ Zelensky said, videos of the exchange show. As he said this, Zelensky aggressively approached Yantar, who heads the National Corps, a political offshoot of the far-right Azov volunteer battalion, in Mykolaiv city.
‘But we’ve discussed that,’ Yantar said.
‘I wanted to see understanding in your eyes. But, instead, I saw a guy who’s decided that this is some loser standing in front of him,’ Zelensky said.”
It was a demonstration of the power of the military, including the Azov Regiment, over the civilian president.
After the Russian invasion, Zelensky was asked in April by Fox News about Azov, which were later defeated in Mariupol. “They are what they are,” he responded. “They were defending our country.” He then tries to say because they are part of the military they are somehow no longer Neo-Nazis, though they still wear Nazi insignia (until Tuesday). (Fox’s YouTube post removed that question from the interview, but it is preserved here:)
Outrages Greek Officials
Also in April, Zelensky infuriated two former Greek prime ministers and other officials by inviting a member of the Azov Regiment to address the Greek Parliament. Alexis Tsipras, a former premier and leader of the main opposition party, SYRIZA-Progressive Alliance, blasted the appearance of the Azov fighters before parliament.
“Solidarity with the Ukrainian people is a given. But nazis cannot be allowed to speak in parliament,” Tsipras said on social media. “The speech was a provocation.” He said Greek Prime Minister Kyriakos Mitsotakis “bears full responsibility. … He talked about a historic day but it is a historical shame.”
Former Greek Prime Minister Antonis Samaras called the Azov video being played in parliament a “big mistake.” Former Foreign Affairs Minister Nikos Kotzias said: “The Greek government irresponsibly undermined the struggle of the Ukrainian people, by giving the floor to a Nazi. The responsibilities are heavy. The government should publish a detailed report of preparation and contacts for the event.”
Former Finance Minister Yanis Varoufakis’ MeRA25 party said Zelenky’s appearance turned into a “Nazi fiesta.”
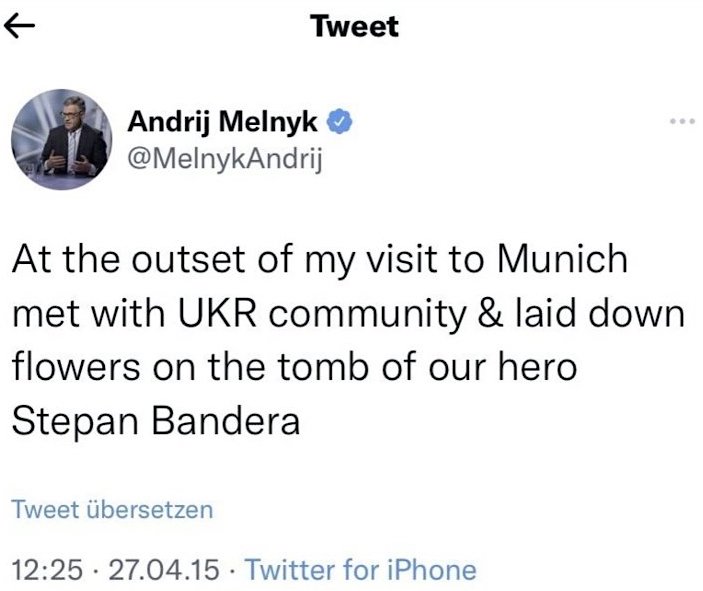
Zelensky has also not rebuked his ambassador to Germany, Andrij Melnyk, for visiting Bandera’s grave in Munich, which provoked this reaction from a German MP: “Anyone like Melnik who describes the Nazi collaborator Bandera as ‘our hero’ and makes a pilgrimage to his grave or defends the right-wing Azov Battalion as ‘brave’ is actually still benevolently described as a ‘Nazi sympathizer.’”
Zelensky has closed media outlets and outlawed 11 political parties, including the largest one, Eurosceptic Opposition Platform for Life (OPZZh) and arrested its leader. None of the 11 shut down are far-right parties.
Donald Trump was rightly castigated for remarks he made about white supremecists in Charlottesville. But Zelensky, whose oligarch backer funded Azov, and who brought a Neo-Nazi to address a European Parliament, is given a pass by a Democratic administration and the U.S. media though he condones the far worse problem of Neo-fascism in Ukraine.
‘Infested’
NewsGuard’s Fishman took issue with similar phrases that appear in Consortium News articles by columnist Patrick Lawrence, and by legendary journalist John Pilger. Lawrence refers to the Ukrainian government as a “Nazi-infested regime” and Pilger to the “the coup regime, infested with neo-Nazis.” NewsGuard objects to this characterization because the political wings of violent neo-Nazi groups fare poorly in Ukrainian elections.
Fishman wrote:
“The March 2022 article ‘PATRICK LAWRENCE: Imperial Infantilism’ stated: ‘Now the names we have for Putin roll around among like pinballs. ‘Hitler’ has fallen somewhat out of fashion, the hyperbole having proven too silly, or maybe because NATO is now arming a Nazi-infested regime,’ which was a reference to the Ukrainian government.
The February 2022 article “John Pilger: War in Europe & the Rise of Raw Propaganda” stated: “Vladimir Putin refers to the ‘genocide’ in the eastern Donbass region of Ukraine. Following the coup in Ukraine in 2014 – orchestrated by former U.S. President Barack Obama’s ‘point person’ in Kyiev, Victoria Nuland – the coup regime, infested with neo-Nazis,launched a campaign of terror against Russian-speaking Donbass, which accounts for a third of Ukraine’s population.” This article makes the claims similar to the ones highlighted in the previous … articles, and are seemingly false for the same reasons.”
One can quibble over whether “infested” is the best choice of words, but it is clear that the Ukrainian state has long protected influential Neo-Nazism. Consortium News gives a wide latitude to columnists and commentators like Lawrence and Pilger, both vastly experienced journalists, to express themselves. There is no doubt about the outsized influence of Neo-fascism in Ukrainian society and government, especially since the events of 2014.
NewsGuard’s dismissal of the influence of Neo-fascism by looking only at election results completely misses the point. Fishman has demanded CN correct its reporting on neo-Nazism in Ukraine. But Fishman’s statement that “There isn’t evidence that Nazism has a substantial influence in Ukraine” should instead be corrected by NewsGuard.
The ‘G’ Word
Fishman also took exception to the use of the word “genocide” in two Consortium News articles published about Ukraine.
“I also found some instances where Consortium News appeared to publish false or misleading claims, and I’d like to get your comments on them. I’ve listed some examples and provided brief explanations on why they seem to be false:
The March 2022 article ‘A Proposed Solution to the Ukraine War’ stated: ‘The government of Ukraine has denied human rights and political self-determination to the peoples of the Donbass. Some 13,000 people have died during the eight years since the 2014 coup, according to the United Nations. The Ukrainian government has overtly genocidal policies toward Russian minorities.’
The February 2022 article “John Pilger: War in Europe & the Rise of Raw Propaganda” stated: ‘Vladimir Putin refers to the “genocide” in the eastern Donbass region of Ukraine. Following the coup in Ukraine in 2014 … the coup regime … launched a campaign of terror against Russian-speaking Donbass, which accounts for a third of Ukraine’s population.”
Fishman went on:
“The International Criminal Court, the Office of the U.N. High Commissioner for Human Rights, and the Organization for Security and Co-operation in Europe (OSCE) have all said they have found no evidence of a genocide in Donbas. For example, A 2016 report by the International Criminal Court found that the acts of violence allegedly committed by the Ukrainian authorities in 2013 and 2014 could constitute an ‘attack directed against a civilian population,’ but it also said that’“the information available did not provide a reasonable basis to believe that the attack was systematic or widespread.’
And the U.S. Mission to OSCE stated in a February 2022 Twitter post, ‘The SMM [Special Monitoring Mission] has complete access to the government controlled areas of Ukraine and HAS NEVER reported anything remotely resembling Russia’s claims [of genocide in Ukraine].’”
Genocide is defined in the 1948 Convention on the Prevention and Punishment of the Crime of Genocide, ratified by 153 nations. The convention says:
“In the present Convention, genocide means any of the following acts committed with intent to destroy, in whole or in part, a national, ethnical, racial or religious group, as such:
(a) Killing members of the group;
(b) Causing serious bodily or mental harm to members of the group;
(c) Deliberately inflicting on the group conditions of life calculated to bring about its physical destruction in whole or in part;
(d) Imposing measures intended to prevent births within the group; (e) Forcibly transferring children of the group to another group.”
The Convention adds:
“The following acts shall be punishable:
(a) Genocide;
(b) Conspiracy to commit genocide;
(c) Direct and public incitement to commit genocide;
(d) Attempt to commit genocide;
(e) Complicity in genocide.”
Based on the convention, an argument for and against genocide in Donbass could be made. The Ukraine military and extreme right militias have undoubtedly carried out attacks on civilians who, by reason of their language and religion, constitute a separate ethnic group. Points (a) and (b) of the definition are certainly true, (c) and (d) are questionable. The question of “intent” is crucial. Have the Ukrainian authorities had the “intent to destroy, in whole or in part, a national, ethnical, racial or religious group”?
The charge of “genocide” is thrown about by political opponents with less than due care to its actual definition. For instance, Biden and Zelensky have both accused Russia of “genocide” in its ongoing military operation. There is no defined number of civilian deaths that constitute an intent to destroy a people “in part.” Three months after the Russian invasion, the OSCE reports around 4,000 civilians killed. Both sides are shooting and killing civilians.
It is a judgement call whether genocide has taken place. The ICC report, referred to by Fishman, says Ukraine’s military action against Donbass could “constitute” an “attack directed against a civilian population,” but the ICC’s judgement about genocide was not definitive as it was based on “the information available.”
His second reference does not come from the OSCE itself, but from the U.S. mission to the OSCE, undercutting its objectivity since it is a narrow, national view from a country with a distinct political interest in events in Ukraine.
Consortium News has not taken a position that genocide was committed in Donbass. These are the only references made to genocide in Donbass and both CN articles are clearly labeled as commentaries with the disclaimer: “The views expressed are solely those of the author and may or may not reflect those of Consortium News.“
Pilger only says that Putin “refers to genocide,” while Pilger himself calls it “a campaign of terror against Russian-speaking Donbass.”
Consortium News did not endorse the judgment of these two commentators as it often publishes material with which it does not share editorial positions. Genocide in the context of Donbass is an arguable point, and therefore CN published these commentaries.
Financing and Other Questions
NewsGuard has also demanded detailed information about Consortium News‘ financing. Consortium News is funded almost entirely by small contributions from its readers raised during three public fund raisers per year.
IRS rules require donors who contribute more than $5,000 in a year be told to the tax agency. But their names do not have to be revealed to the public to protect the donors’ privacy. CN has made public its two major donors from its last tax returns. Roger Waters, the rock musician of Pink Floyd fame, donated $25,000 in both 2020 and 2021. The other major donor is the New York-based Cloud Mountain Foundation, which has donated $25,000 in each of the past three years.
Consortium News has never taken a penny from any government, corporation or advertiser. To prove this, CN is hiring an independent auditor to attest to this fact. It will publish on this website the independent audit statement as soon as it is prepared to once and for all end any smears or suspicions about the sources of CN‘s funding.
Fishman also mistakenly wants to know why authors’ bios don’t appear below CN articles, when they clearly do. NewsGuard wants to know what CN‘s corrections policy is. It is as follows: typos are corrected without a notice, factual errors are corrected with a CORRECTION notice at the bottom of the article.
A History of Dissent
The United States was founded by dissenters. The Declaration of Independence is one of history’s most significant dissenting documents, inspiring people seeking freedom around the world, from the French revolutionists to Ho Chi Minh, who based Vietnam’s declaration of independence from France on the American declaration.
But over the centuries a corrupt centralization of American power seeking to maintain and expand its authority has at times sought to crush the very principle of dissent which was written into the United States Constitution.
Freedom to dissent was first threatened by the second president. Just eight years after the adoption of the Bill of Rights, press freedom had become a threat to John Adams, whose Federalist Party pushed through Congress the Alien and Sedition Laws. They criminalized criticism of the federal government.
The Union then shut down newspapers during the U.S. Civil War.
Woodrow Wilson came within one vote in the Senate of creating official government censorship in the 1917 Espionage Act. The 1918 Alien and Sedition Act that followed jailed hundreds of people for speech until it was repealed in 1921.
Since the 1950s, McCarthyism has become the byword for one of the worst periods of repression of dissent in U.S. history.
The closest we’ve come to Wilson’s troubling dream is the Biden administration’s Disinformation Governance Board under the Department of Homeland Security, now on hold.
The roots are in the earliest English settlers in North America, described in The Scarlet Letter and applied to McCarthyism in Arthur Miller’s The Crucible. Though its industrial and scientific achievements are most lauded, America’s tradition of dissent is probably the greatest thing in U.S. history and it is once again under threat.
The Current Climate
NewsGuard’s accusations against Consortium News that could potentially limit its readership and financial support must be seen in the context of the West’s war mania over Ukraine, about which dissenting voices are being suppressed. Three CN writers have been kicked off Twitter.
PayPal’s cancellation of Consortium News‘ account is an evident attempt to defund it for what is almost certainly the company’s view that CN violated its restrictions on “providing false or misleading information.” It cannot be known with 100 percent certainty because PayPal is hiding behind its reasons, but CN trades in information and nothing else.
CN supports no side in the Ukraine war but seeks to examine the causes of the conflict within its recent historical context, all of which are being whitewashed from mainstream Western media.
Those causes are: NATO’s expansion eastward despite its promise not to; the coup and 8-year war on Donbass against coup resisters; the lack of implementation of the Minsk Accords to end that conflict; and the outright rejection of treaty proposals by Moscow to create a new security architecture in Europe taking Russia’s security concerns into account.
Historians who point out the onerous Versailles conditions imposed on Germany after World War I as a cause of Nazism and World War II are neither excusing Nazi Germany nor are they smeared as its defenders.
Consortium News can be wrong at times, but never as wrong as mainstream media was on WMD in Iraq or Russiagate. CN got both those consequential stories right while they were happening, and contends it is correct in its analysis of the Ukraine crisis. In any case, it is entitled to its analysis. On Iraq, Russiagate and Ukraine, Consortium News has clashed with the conventional wisdom forged by powerful forces and its corporate media allies. In response CN has been repeatedly smeared as agents of Iraq and Russia.
An overly self-confident Western establishment cannot appear to understand how experienced Western journalists could exercise their own agency and editorial judgment to critique U.S. foreign policy in real time, without them being agents of a foreign power. Consortium News sued the Canadian television network Global News for publishing such a smear.
It is evidently not enough for powerful forces to simply disagree and respect CN‘s constitutional right to free speech.
Justice Oliver Wendell Holmes in Abrams v. United States wrote: “[T]hat the ultimate good desired is better reached by free trade in ideas—that the best test of truth is the power of the thought to get itself accepted in the competition of the market… That at any rate is the theory of our Constitution.” Justice Louis Brandeis added in Whitney v. California that the remedy for ill-conceived speech is more speech, not enforced silence.
NewsGuard’s review of Consortium News and other independent media is a test case: Can the U.S. establishment tolerate dissent or is it joining the tradition of Adams and Wilson to crush it?
Joe Lauria is editor-in-chief of Consortium News and a former U.N. correspondent for The Wall Street Journal, Boston Globe, and numerous other newspapers, including The Montreal Gazette and The Star of Johannesburg. He was an investigative reporter for the Sunday Times of London, a financial reporter for Bloomberg News and began his professional work as a 19-year old stringer for The New York Times. He can be reached at joelauria@consortiumnews.com and followed on Twitter @unjoe
Over Extending and Unbalancing Russia (OEAUR) is a freely accessible 2019 Rand Corporation policy paper that posits how the United States and her satellites can most efficiently destroy Russia mainly, as it happens, through militarizing Ukraine and escalating sanctions. Rand’s objective is to strangle Russia by throttling her at her choke points, a vulnerability Russia’s own policy advisors have long been aware of, just as they have been aware of Rand’s well entrenched Russophobia.
Because Rand knows they have been rumbled, OEAUR now begins that readers should first visit their two related sites which explain how Rand defends truth and combats Russia’s Firehouse of Falsehood. Alas for the truth seekers, those two further pages are, like OEAUR itself, repetitive swill, roughly equivalent to a very bad first year university essay. This can be seen in the bibliographies’ over reliance on Michael Weiss, a rabidly pro Israeli member of the far right Henry Jackson Society who was long located in Beirut, from where he shilled ceaselessly for Syria’s CIA sectarian rebels and for the destruction of the Syrian people.
Though OEAUR might very well fail as a first year essay, OEAUR was not geared at university tutors but at NATO policy makers, weapons’ procurers and the media and think thank parasites like Michael Weiss who feed off them and, in that, OEAUR did as good a job as their paymasters needed.
In those respects, Rand positing Russia as “the firehose of falsehood” because of her apparently “high numbers of channels and messages and a shameless willingness to disseminate partial truths or outright fictions” seem to be Rand externalizing NATO’s internal, where we see, time and again, each and every one of its affiliated media and think tank outlets hammering home the same message of Moscuam dēlenda est, Moscow must be destroyed.
Because OEAUR has long ago made no secret of NATO’s desire to emasculate Russia by fair means or foul, by escalating or depressing global prices as needed, look no further than the Pentagon to round up the usual suspects who are behind the Putin Price Hike and the terrible events unfolding in Sri Lanka, Nigeria and elsewhere.
The Brookings Institution is another key think tank for hire, with significant links to the CIA and the Pentagon. It includes such notorious war hawks as Robert Kagan, who repackaged himself for Hillary Clinton as an Orwellian named “liberal interventionist”. Kagan is married to Victoria Fuck the EU Nuland, another Clinton favorite and the chief architect of the Ukrainian war.
The 2009 Brookings Institution paper The Path to Persia: Options for a New American Strategy toward Iran spelled out America’s plans to destroy the Middle East in sufficient clarity and detail any war crimes court worth its salt would accept. In detailing every under handed and duplicitous means from economic sanctions and U.S.-backed political upheaval, to the use of terrorism and proxy wars to undermining and destroying Iranian and Syrian sociopolitical stability and eventually the Syrian and Iranian states themselves, that seminal paper became the blueprint not only for all the CIA and NATO driven carnage and associated mass murders that followed but also for Rand’s pathetic OEAUR opus as well.
Given OEAUR’s two Russian focused caveats, it is also noteworthy that this subversive Brookings document also detailed the need to manipulate, corral and emasculate public opinion so that Iran and Syria could follow Iraq and Libya into the abyss. It stressed the use of false and duplicitous negotiations with Iran to make them an offer they could neither refuse nor accept over nuclear weapons and to use Iran’s apparent refusal to capitulate to what the West’s embedded media would paint as a reasonable American offer as an excuse to wage a full scale war of sectarian extermination on Iran, much like that currently being played out in Yemen. Under this scenario, the American President could paint himself as a reluctant mass murderer, not unlike what Obama managed to do with his Drone assassination campaigns in Yemen, in Syria and in other countries on the CIA’s hit list.
Studying Rand, Brookings and similar think tanks for hire is far from an academic exercise. These groups help NATO develop, hone and implement their war plans and they also bestow an underserved sheen of academic respectability to them. Brookings, Rand, their employees, apologists and collaborators are very much a part of the Ukrainian, Yemeni, Syrian and related problems and they should answer in a war crimes’ court for it.
Gillian Dymond is determined to find out what the Medicines and Healthcare products Regulatory Agency (MHRA) is doing to investigate the enormous number of adverse reactions to the Covid vaccines that have been reported under the Yellow Card scheme and what risk/benefit analysis was carried out to justify rolling out the experimental gene therapy to under-18s.
We published her letters to MHRA chief executive officer Dame June Raine, first sent in November last year, here and here.
At the end of April, after an unsatisfactory response from the MHRA’s Chief Safety Officer Dr Alison Cave, Gillian returned to the fray, to ask Dame June for a copy of the risk assessment carried out by the MHRA before it decided to approve experimental Covid medications for use on children. After 20 working days, having still received no reply, she emailed her the following:
Dear Dame June,
Open letter: Your failure to produce a risk assessment justifying the approval of injections against SARS-CoV-2 for people under 18 years of age
On April 28 I wrote to you requesting a copy of the risk assessment which I assumed you must certainly have carried out prior to approving the incompletely tested medications against SARS-CoV-2 for children as young as five years of age.
I asked you to send this information within 20 working days. That period has now elapsed without a response to my request or an acknowledgement of my email.
It seems that you are either unable or unwilling to provide me with a copy of the document requested.
We parents and grandparents must therefore conclude that:
1. You have approved an experimental treatment for our young families without carrying out and recording a thorough risk/benefit analysis for the age group in question; or
2. You did carry out such an analysis, but are reluctant to make it public because its conclusions do not support approval of the medications in question.
Where you have remained silent, however, others have stepped in to fill the gap. Doctors for Covid Ethics have now produced a risk/benefit analysis for the Pfizer and Moderna vaccines, in relation to children and adolescents: exactly the kind of analysis that we had every right to expect from your own organisation.
This analysis concludes that the medications under investigation are neither necessary, nor effective, nor safe for prescription to the age group in question. It also ‘addresses the risk of genotoxicity of the mRNA vaccines, which according to recent experimental evidence of their integration into host cell genomes must be considered urgent’.
I note from your public meeting in February this year that the MHRA, in its headlong rush to become a ‘world-class regulatory agency’, is planning to build on the ‘success’ of the Covid injection roll-out by fast-tracking a succession of ‘100-day vaccines’ tweaked into being on computers, shortening the time necessary for approval by using the public as ‘real-time’ guinea pigs. Any checks on medium to long-term safety, it seems, are to be thrown to the winds.
The steadily accumulating numbers of serious adverse reactions to the present experimental treatments argue against these foolhardy proposals.
As the numbers of deaths and injuries following injection grow, it is becoming clear that the genuine successes against Covid have come not from pharmaceutical innovations or top-down diktats by centralised bureaucracies kow-towing to the World Health Organisation, but from the cross-border co-operation of dedicated doctors all over the world who have faced censorship, smears, and even loss of their livelihoods, as they relied on tried and trusted medicines and years of solid experience to devise the early-treatment protocols which have saved so many lives and which, but for the intervention of those charged with assuring our safety, might have saved so many more.
The facts could not be clearer. In future, the MHRA should respect the precautionary principle. Meanwhile, you should lose no time in withdrawing approval for the injection of our children with unnecessary, ineffective and unsafe experimental substances whose long-term effects on young people with their lives before them will for many years remain unknown.
Ukrainian President Volodymyr Zelensky has announced he will submit a draft bill to parliament giving special status to Poles in Ukraine. It mirrors and reciprocates a similar bill recently endorsed by Poland. The unprecedented bill grants Ukrainians almost the same rights as Polish citizens, regarding social benefits, education, residence, and so on. Zelensky’s announcement was made during the Polish President Andrzej Duda’s visit to the Ukrainian Parliament on May 22.
In his speech, Zelensky also announced plans for bilateral agreements pertaining to joint border and customs control. Interestingly, he had this to say about Poland: “Our nations are also brothers (…) and there should be no borders or barriers between us.” He added: “The unity of our nations must last forever”. Given the complex Warsaw-Kiev history, these dramatic statements have certainly raised eyebrows. Andrzej Duda in turn said in his own speech that “the Polish–Ukrainian border should unite, not divide.” On May 3, Duda had already stated that he hopes one day “there will be no border” between the two countries.
Considering these statements and previous Russian intelligence reports, it is no wonder Maria Zakharova, official representative of the Russian Ministry of Foreign Affairs, has described Zelensky’s plan as “legalizing the Polish takeover of Ukraine.”
Since the beginning of the Russian military operation in Ukraine in February, Polish authorities in Warsaw have been providing Kiev with support and there has been a lot of cooperation. The Russian-Ukrainian conflict has projected Poland – NATO’s largest state member in Eastern Europe – as a strategic player in the region, as it is no stranger to great-power confrontations.
It is thus not far-fetched at all to interpret the initiatives discussed and the rhetoric employed by the two leaders as a kind of first step towards a future Ukrainian-Polish confederation. Such a “merging” scenario, in a very creative way, could thereby “hack” the long process of bringing Kiev into the EU and the Western bloc, a goal which the West clearly pursues by whatever means necessary – as has been indicated by Macron’s recent proposal to create a new and more inclusive European political organization, for instance.
Interestingly, this possible future development would accomplish the same thing a military “annexation” would – and even so might also pave the way for a future Polish peace mission. On April 28, the Russian Foreign Intelligence Service’s director claimed Poland was secretly planning to employ its troops to partly take over Western Ukraine, with American support. The justification for that would be “to defend” the neighboring country from “Russian aggression”. According to Russian intelligence, in late April, this so-called peace mission was being discussed with Biden’s officials and was still under preliminary agreements.
Moreover, Polish officials were supposedly negotiating with members of the Ukrainian elite to change Kiev’s policies by making them more “democratic” and pro-Warsaw, so as to counterbalance its nationalist elements. These data have been reported by the Russian press and such coverage has often been labeled as Russian “propaganda” and “disinformation” by Western media. The Russian intelligence also worried that such a development, if it came to fruition, would actually pave the way for a kind of future “reunification”.
Historically, Western Ukraine was ruled by Poland a number of times, including after the 1921 Riga peace treaty, and anti-Polish feelings are part of Ukrainian nationalism today. While Warsaw has been supporting Kiev in key strategic issues since the 2014 Maidan revolution, the very way both countries perceive and politicize 20th century history has hampered their bilateral relations. During World War II, the Ukrainian Insurgent Army (UPA) cooperated with the Nazi Waffen-SS and several war crimes were commited against Poles. Today’s post-Maidan Ukraine glorifies UPA leader Stepan Bandera and this fact is not well received in Poland.
Here, some older history is relevant. A large part of today’s Ukraine was once dominated by the then Polish-Lithuanian Commonwealth. After 1349, then Ruthenia, which largely corresponds to today’s Western Ukraine, was subjected to foreign domination. By 1569, most of it became Polish territory. The pressures for Polonization, which included converting to Roman Catholicism, the ongoing enserfment of the peasantry by Poland, and the persecution of the Orthodox Church alienated peasants and Cossacks. In 1648, the Cossack leader Bohdan Khmelnytsky led an uprising against the Polish King, founded the Cossack Hetmanate, and was hailed a liberator of the people. In 1654, with the Pereyaslav agreement, this new Cossack state pledged its loyalty to the Russian Tsar. To this day, Khmelnytsky is hailed by some as a Ukrainian national hero and a precursor of nationalism because of his fight against Polish domination – even though some criticize him for his alliance with the Tsar.
Dmytro Yarosh, adviser to the Commander-in-Chief of the Armed Forces of Ukraine Valerii Zaluzhny, stated in an interview on May 27, 2019 that Zelensky would “lose his life” and “hang on a tree on Khreshchatyk” if he “betrayed” Ukrainian nationalists by negotiating an end to the civil war in Donbass. Yarosh is a co-founder of the Right Sector and former commander of the far-right Ukrainian Volunteer Army. Therefore, considering Kiev’s persistent problem with extremist violence and the blatant neo-Nazism of its key Azov battalion, not to mention the complicated Polish-Ukrainian relations historically, one can conclude that Zelensky and Duda’s plans will face some challenges, and could escalate internal tensions dramatically.
To understand the war in Ukraine, you have understand the events that led up to it. And no preceding event is more important than the toppling of Viktor Yanukovych’s government in February of 2014.
Officially known as the ‘Revolution of Dignity’, it was denounced by Vladimir Putin as an “unconstitutional coup”. And while most Western media stick to the official nomenclature, some prominent voices dissent. John Mearsheimer has referred to “the illegal overthrow of Ukraine’s democratically elected and pro-Russian president”, while George Friedman has described what happened as “the most blatant coup in history”.
A recap of the basic facts is in order.
In November of 2013, Yanukovych’s government suspended plans for signing an Association Agreement with the EU, and decided to renew talks with Russia. This decision sparked protests in Ukraine’s capital city, Kiev. By December, the number of protestors had reached the tens of thousands, and a permanent encampment had been established on Maidan square. Although most of the protesters were ordinary Ukrainians, far-right groups were also present.
Beginning in December, there were violent clashes between protesters and the police. On 23rd January, protestors succeeded in occupying various buildings around Maidan square. The situation came to a head on 18–20th February when protestors were fired upon by snipers, leaving scores dead and hundreds wounded. A dozen police offers were also killed in the clashes. From November 2013 to February 2014, 112 protestors and 18 police officers lost their lives; though most of the killings happened on 20th February.
On 21st February, Yanukovych signed an agreement with the parliamentary opposition calling for reforms and new elections. But the next day, he was impeached by the Ukrainian parliament. This impeachment process was in several respects unconstitutional, and Yanukovych declared he was still “the legitimate head of the Ukrainian state elected in a free vote by Ukrainian citizens”. However, he subsequently fled to Russia and a new government was formed.
The ‘Revolution of Dignity’ led immediately to Russia’s annexation of Crimea, and the outbreak of civil war in Donbas – so its geopolitical importance can hardly be overstated. Yet despite huge international attention, one question remains shrouded in mystery: who ordered snipers to fire at protestors on 18–20th February?
The ‘official’ narrative is that the snipers were from the Berkut – a special police unit loyal to Yanukovych. On the other hand, Russia has long maintained they were deployed by the Ukrainian far-right as part of a false flag operation to bring down Yanukovych’s government.
What is true is that more than eight years after the massacre – which took place amid a giant demonstration at the centre of Ukraine’s capital in front of dozens of television cameras – not a single person has been convicted. The perpetrators of one of the deadliest mass shootings in European history remain at large.
Why don’t we have an answer? Well, perhaps we do.
Away from the limelight, one Canadian academic has been poring over the evidence for the last eight years. And he’s convinced the ‘official’ narrative is wrong. Ivan Katchanovski (a political scientist at the University of Ottawa) believes the Maidan massacre was a false flag operation carried out by the Ukrainian far-right.
Professor Katchanovski cannot be dismissed as some fringe commenter or stooge of the Kremlin. He has published his arguments in scholarly books and journals, and has presented them at academic conferences. His latest article, which can be accessed for free, reviews all the evidence he’s collected to date – including witness testimonies, weapon ballistics and medical forensics. It’s based on hundreds of hours of footage of the Maidan massacre trials, as well as synchronised video segments of the massacre itself.
As Katchanovski explains, the ‘false flag theory’ first gained credence in March of 2014, when a phone call between two European officials was leaked online. During the call, the Estonian Foreign Minister Urmas Paet tells the EU’s Catherine Ashton about a conversation he’d had with someone called Olga:
What was quite disturbing, the same Olga told, all the evidence shows that people who were killed by snipers from both sides among policemen and then people from the streets – that they were the same snipers, killing people from both sides. She also showed me some photos. She said that as medical doctor, she can, you know, say that it is the same handwriting, same type of bullets. And it’s really disturbing that now the new coalition, that they don’t want to investigate what exactly happened. So that there is now stronger and stronger understanding that behind snipers it was not Yanukovych but it was somebody from the new coalition.
‘Olga’ was later identified as Olga Bohomolets, a doctor who had treated wounded protestors on Maidan square. When quizzed by the press, she said she had not told Paet that somebody from the new coalition was behind the snipers. Likewise, the Estonian Foreign Ministry said, “We reject the claim that Paet was giving an assessment of the opposition’s involvement in the violence” (though they acknowledged the recording was authentic). It is still unclear why Paet would divulge such shocking revelations if he did not believe they had some basis in fact.
Aside from TV recordings and media reports, much of Katchanovski’s evidence comes from the trials of five Berkut police officers, who were charged with the murder of protestors on 20th February, 2014. Various other state actors, including Yanukovych himself, were also charged, but they were not brought to trial as they had already fled the country. (Recall that none of those put on trial were convicted.)
What, then, is Katchanovski’s evidence?
The majority of wounded protestors who testified at the trail said they were shot by snipers from Maidan-controlled buildings. Remarkably, even many witnesses for the prosecution said this. Their testimony is consistent with video footage of journalists and protestors pointing to snipers in buildings like the Hotel Ukraine, which were under Maidan control at the time.
Police snipers testified that they had been ordered to locate and neutralise snipers firing from Maidan-controlled buildings. And Yanukovych himself, who appeared at the trial via video-link, testified that he had received reports of snipers firing from those buildings.
Several Georgian ex-military personnel who testified at the trail actually confessed they were among the snipers, and had been given orders by specific Maidan leaders to fire upon the protestors. They also testified that they had witnessed other snipers shooting from Maidan-controlled buildings. By contrast, no police officers or other state actors confessed to having fired upon protestors.
In the majority of cases where wounded protestors testified that they had been shot by snipers from police-controlled areas, other evidence contradicted their testimony. For example, synchronized video segments showed the exact times they were hit did not coincide with the exact times police officers were discharging their weapons. Other videos showed that several protesters were killed before police officers had even taken up their positions.
Forensic examinations by government experts revealed that the majority of protestors were shot from the side or back, and from top to bottom, strongly suggesting they had been hit by snipers from Maidan-controlled buildings. Only one protestor had a horizontal entry wound. Experts also determined that several protestors were killed by bullets that did not match those used by the police.
An American architecture company created a 3D model of the killing of three protestors, which was used as evidence that those protestors were in fact killed by the police. (This 3D model was covered in a 2018 New York Timesarticle.) However, the wound locations in the model did not match the wound locations from forensic medical examinations.
A screenshot from the video appendix to Katchanovski’s latest paper.
Aside from what Katchanovski calls “overwhelming evidence” that protestors were shot from Maidan-controlled buildings, he believes there was a cover-up by the post-Maidan authorities.
On 21st February, the Ukrainian parliament passed an amnesty law granting blanket immunity to Maidan protestors for serious crimes that had taken place during the protests. This law also prohibited investigation of the protestors for such crimes, and ordered that existing evidence be destroyed.
Two of the Berkut police officers who had been charged with murdering protestors were released by trial judges due to lack of evidence, suggesting the charges against them were trumped up. And all remaining defendants were released in a prisoner exchange within several months of the expected verdict.
Public statements made by various Maidan participants concerning the far-right’s involvement in the massacre were never investigated. One politician said she saw Maidan leaders bringing snipers into a building and then saw snipers firing from that building. Several activists said they witnessed snipers being evacuated by Maidan leaders. And another politician said that Maidan leaders had “arranged” the massacre.
There were unexplained reversals of testimony on the part of wounded Maidan protestors. Key pieces of evidence went missing or were destroyed. Several trees with bullet holes in them were cut down; all helmets and shields used by those who were shot disappeared, as did security camera footage from Maidan-controlled buildings.
Finally, two far-right politicians stated in separate interviews that a Western government official told them killings of a few protestors would not be enough for Western governments to stop recognising Yanukovych, and for that to happen the number of victims would need to be 100. The protesters who lost their lives subsequently became known as the “Heavenly Hundred”, even though some of those ‘hundred’ were not killed in the massacre itself (and in fact simply died of illness.)
On the basis of all the evidence he’s gathered, Katchanovski concludes that the Maidan massacre was “a false flag operation” which involved “elements of the Maidan leadership”.
If true, the implications are immense. It would mean the event that marked the turning point of Euromaidan – that set in motion Yanukovych’s removal from power – was in fact orchestrated by his political opponents. And aside from implicating those individuals in a brutal act of mass murder, it would remove any doubt that the that the ‘Revolution of Dignity’ was illegitimate.
Is it true?
I have been unable to track down any serious criticism of Katchanovski’s work, and when I reached out to him, he told me “there is no other scholarly study” that disputes his findings. What’s more, the political scientist Gordon Hahn reached similar conclusions in his bookUkraine Over the Edge: Russia, the West and the “New Cold War”.
So why haven’t Western governments shown more interest in investigating the massacre? I put this question to Katchanovski. He said that such an investigation would be “politically inconvenient” because it would “upend the narrative that the Western backed overthrow of the Ukrainian government in 2014 by the pro-Western Maidan opposition was peaceful and democratic”. He added that a definitive answer could be obtained by consulting relevant documents once they are declassified.
As I mentioned above, Katchanovski has published his arguments concerning the ‘false flag theory’ in scholarly books and journals, and has presented them at academic conferences. All the germane papers are available for free online. You might therefore expect for his work to have received significant media attention – particularly in the last few months.
Yet with the exception of a few ‘non-mainstream’ outlets, it hasn’t. Major Western media have ignored his studies “for political reasons”, he told me. This is despite the fact that Katchanovski’s other work on Ukraine (unrelated to the massacre) has received ample media attention, including from the Associated Press, Reuters and the Washington Post.
Katchanovski knows that certain media outlets are aware of his work because he’s brought it to their attention. Following the New York Timesarticle on the 3D model of killings at Maidan, he sent a letter to the editor pointing out they had “misrepresented the wound locations”. But his letter wasn’t published. In another case, “Open Democracy accepted a popular version of my Maidan massacre study, but then did not publish it.” Katchanovski said he gave “long interviews concerning the Maidan massacre to several major TV and Radio networks” but “none of them were broadcast”. In every single case “there was no reason given”.
The only time Katchanovski’s work on the massacre has been put under the spotlight was in Oliver Stone’s 2019 documentary Revealing Ukraine. This film is available on Rumble, and the relevant segment begins at 20:00.
What about everything that’s happened since? In our email exchange, Katchanovski clarified that the Maidan massacre “does not justify the Russian invasion and other actions in Ukraine”. Equally, however, Russia’s invasion does not justify ignoring – in his words – “overwhelming and undeniable evidence” of Maidan snipers.
If others believe that Katchanovski is mistaken, they must come forward and present their arguments. In the meantime, I would strongly recommend reading his papers: they make a compelling case that what’s been labelled a “conspiracy theory” is, in fact, true.
Billionaire Bill Gates says there’s a 50 per cent chance the next pandemic will be caused by man-made climate change or be deliberately released by a bio-terrorist.
The Microsoft founder made the comments during an interview with Spanish news outlet El Diario.
Asserting that the next major pandemic is likely to occur within 20 years, Gates said, “It could be a virus made by man, by a bioterrorist who designed it and intentionally circulated it. That is a very scary scenario because they could try to spread it in different places at once.”
“Or it could be something that makes the leap from the natural world. The human population is growing and we are invading more and more ecosystems. That is why I calculate that there is a 50% chance that we will have a pandemic of natural origin in the next 20 years, as a consequence of climate change,” he added.
The prediction that climate change will cause a virus which will then require another global vaccine rollout is somewhat convenient for Gates given that he is heavily invested in both areas.
Gates reiterated the call made in his recent book to pump billions of dollars into researching future pathogens by creating a 3,000-strong team of specialists under the control of the World Health Organization, which would require a 25% budgetary increase.
Commenting on the recent outbreak of monkeypox, Gates said “there is very little chance” it will have an impact anything like coronavirus, although he cautioned that it could mutate into something significantly nastier.
Gates infamously warned of a coming super-virus five years before the emergence of COVID-19 during a 2015 TED talk.
As we highlighted earlier this month, Gates warned that COVID was not over and that there is likely to be an “even more fatal” variant of the virus coming.
During an event at the Munich Security Conference back in February, Gates said that “sadly” Omicron is a “type of vaccine” and has “done a better job getting out to the world population than we have with vaccines” by providing natural immunity.
Israel’s Supreme Court has decided that the Palestinian region of Masafer Yatta in the southern hills of Hebron is to be appropriated entirely by the Israeli military and that the local population of more than 1,000 Palestinians is to be expelled. The court’s decision on 4 May was hardly surprising. Israel’s military occupation is not only enforced by soldiers with guns, but also elaborate political, military, economic and legal structures, all of which are dedicated to the expansion of illegal Jewish settlements and the slow — and sometimes not-so-slow — expulsion of the Palestinians.
When Palestinians say that the Nakba (“Catastrophe”), which led to the ethnic cleansing of Palestine in 1948 and the establishment of the state of Israel on its ruins, is an ongoing unfinished project, they mean exactly that. The ethnic cleansing of Palestinians from East Jerusalem and the endless torment of Palestinian Bedouins in the Naqab, and now in Masafer Yatta, are all testament to this reality.
However, Masafer Yatta is particularly unique. In the case of occupied East Jerusalem, for example, Israel has made a fallacious, ahistorical claim that the city is the eternal and undivided capital of the Jewish people. It combined its unsubstantiated narrative with military action on the ground, followed by a systematic process to increase the Jewish population and eject the native inhabitants of the city. Such notions as ‘Greater Jerusalem‘ and legal and political structures, like that of the Jerusalem Master Plan 2000, have all contributed towards turning the once absolute Palestinian majority in Jerusalem into a constantly shrinking minority.
In the Naqab, Israel’s objectives were put into motion as early as 1948, and again in 1951. The process of ethnically cleansing the natives remains in effect to this day.
Although Masafer Yatta is part of the same colonial scheme, its uniqueness stems from the fact that it is situated in Area C of the occupied West Bank. In July 2020, Israel purportedly decided to postpone its plan to annex nearly 40 per cent of the West Bank, perhaps fearing a Palestinian rebellion and unwanted international condemnation. However, the plan went ahead in all but name.
The wholesale annexation of large swathes of the West Bank would mean that Israel would become responsible for the welfare of entire Palestinian communities living therein. As a settler-colonial state, though, Israel wants the land, but not the people. In Tel Aviv’s calculation, annexation without the expulsion of the population could lead to a demographic nightmare, hence Israel’s need to reinvent its annexation plan. De jure annexation may have been “postponed”, but it has continued in de facto terms, which has attracted very little international political and media attention.
The Israeli court’s decision regarding Masafer Yatta, which is already being carried out with the expulsion of the Najjar family on 11 May, is an important step towards the annexation of Area C. If Israel can evict the Palestinian residents of twelve villages, more than 1,000 people, unhindered, more such expulsions can be expected, not only south of Hebron, but across the occupied Palestinian territories.
The Palestinian villagers of Masafer Yatta and their legal representation know very well that no real “justice” can be obtained from the Israeli court system. Nevertheless, they continue to fight the legal war in the hope that a combination of factors, including solidarity in Palestine and pressure from outside, can ultimately succeed in compelling Israel to delay its planned destruction and Judaisation of the whole region.
However, it seems that Palestinian efforts, which have been underway since 1997, are failing. The Israeli Supreme Court decision is predicated on the erroneous and utterly bizarre notion that the Palestinians of that area could not demonstrate that they belonged there prior to 1980, when the Israeli government decided to turn the area into “Firing Zone 918”.
Sadly, the Palestinian defence was based partly on documents from the Jordanian era and official UN records that reported on Israeli attacks on several Masafer Yatta villages in 1966. The Jordanian government, which administered the West Bank until 1967, compensated some of the residents for the loss of their “stone houses” — not tents — animals and other properties that were destroyed by the Israeli military. Palestinians tried to use this evidence to show that they have existed, not as nomadic people but as rooted communities. This was unconvincing to the Israeli court, which favoured the occupation army’s argument over the rights of the native population.
Israeli firing zones occupy nearly 18 per cent of the total area of the West Bank. It is one of several ploys used by the Israeli government to lay a pseudo-legal claim on Palestinian land and, eventually, to claim legal ownership as well. Many of these firing zones exist in Area C, and are one way that Israel appropriates Palestinian land officially with the support of the courts.
Now that the Israeli military has managed to acquire Masafer Yatta — a region covering 32 to 56km2 — based on completely flimsy excuses, it will become much easier to ensure the ethnic cleansing of many similar communities in various parts of occupied Palestine.
While discussions and media coverage of Israel’s annexation scheme in the West Bank and the Jordan Valley have largely subsided, the settler-colonial state is now preparing for gradual annexation. Instead of taking 40 per cent of the West Bank all at once, Israel is now annexing smaller tracts of land and regions, like Masafer Yatta, separately. Tel Aviv will eventually connect all these annexed areas through Jewish settler-only bypass roads to larger Jewish settlement infrastructures in the West Bank.
Not only does this alternative strategy allow Israel to avoid international criticism, but it will also permit the settler-colonial state to annex Palestinian land while incrementally expelling Palestinians. Thus, demographic imbalances will be prevented before they can even occur.
What is happening in Masafer Yatta is not only the largest ethnic cleansing scheme to be carried out by Israel since 1967, but the move should also be considered as the first step in a much larger scheme of illegal land misappropriation, ethnic cleansing and official mass annexation.
Israel must not be allowed to succeed in Masafer Yatta. If it does, its original, mass annexation scheme will become a reality in no time at all.
Israel’s bombardment of the biggest agrochemical warehouse in the besieged Gaza Strip by incendiary artillery shells last year amounts to chemical warfare, a rights group report finds.
On May 15, 2021, the Israeli military launched an artillery attack on the Khudair Pharmaceuticals and Agricultural Tools Company, considered as the largest agrochemical warehouse in the north of the blockaded enclave, setting fire to tons of pesticides, fertilizers, plastics and nylons.
The shelling attack occurred in the midst of the 11-day Israeli war against Gaza Strip, after weeks of violence against Palestinians in Al-Quds and a brutal crackdown on worshipers at the al-Aqsa Mosque, as well as attempts to steal their land in the Sheikh Jarrah neighborhood.
The results of a new investigation in the attack and its consequences by the West Bank-based Palestinian human rights NGO Al-Haq showed that Israel deliberately employed highly flammable munitions in the targeted attack, which burned tons of dangerous pesticides and set off an unfolding environmental disaster.
The FAI Unit built a 3D model of the warehouse after interviewing the locals, consulting international experts and analyzing data obtained from dozens of videos, including CCTV and drone footage, in a bid to establish the circumstances of the blaze, and determine the effects of the release of toxic chemicals.
“Our findings reveal that Israeli forces illegally employed highly flammable munitions in a targeted attack on the warehouse, whose location and contents are known to Israel, setting on fire over 50 tons of hazardous chemicals stored on the site,” said al-Haq.
The report is the first publication by Al-Haq’s newly-established Forensic Architecture Investigation Unit (FAI Unit), a first-of-its-kind collaboration in the Middle East with Forensic Architecture, a research agency based at Goldsmiths, University of London, which conducts spatial and media analysis for NGOs and in international human rights cases.
The shelling created a toxic plume, which engulfed an area of nearly six sq km, leaving local residents struggling with health problems.
“Within the first hour, the toxic plume had affected an area of approximately 5.7 square kilometers — spanning Beit Lahiya and its agricultural zones, as well as the densely populated Jabaliya refugee camp — placing approximately 3,000 homes in its shadow,” the report said, adding that the six-hour-long fire at the warehouse destroyed most of the facility and consuming the majority of its contents.
Al-Haq said that a toxic plume produced by the attack is tantamount to the indirect deploying of chemical weapons.
“Israeli occupation forces’ shelling of the Khudair Agrochemical Warehouse, with knowledge of the presence of toxic chemicals stored therein, is tantamount to chemical weapons through indirect means. Such acts are clearly prohibited… and prosecutable under the Rome Statute of the International Criminal Court,” the group said in a legal report based on the findings of the investigation.
The probe determined that the Israeli military used several M150 Smoke HC 155mm shells in its attack against the warehouse.
“The dimensions and the smoke tail match the M150 Smoke HC 155mm ammunition developed by the Israeli weapons manufacturer Elbit Systems: an ‘advanced smoke projectile’ and a new type of shell designed to splinter into five separate canisters, all of which emit high-density smoke,” the report said.
It also stressed that the attack on the Khudair agrochemical warehouse was the first in an apparent string of similar attacks by the Tel Aviv regime, intentionally hitting civilian economic infrastructure and the industrial sector.
“On 17 May, two days after the Khudair Warehouse was destroyed, the Fomco Sponge Factory near Jabaliya camp was attacked in a similar manner, causing a large-scale fire. On the same day, over half a dozen other factories and warehouses, located in the industrial zone east of Gaza’s Shejaiyyeh neighborhood, were also bombed,” it stated.
In the latest bombardment campaign of Gaza by Israel in May last year, at least 260 Palestinians, including over 60 children, were killed in a time span of 11 days that began on May 10. The Gaza-based resistance movements retaliated.
The regime was eventually forced to announce a ceasefire, brokered by Egypt, which came into force in the early hours of May 21.
The Gaza Strip, home to some two million people, has been under a blockade imposed by Israel since June 2007.
Millions of people suffer and die from the effects of radiation exposure from decades of nuclear weapons testing. Their experience should give serious pause to those who continue to embrace the viability of a nuclear deterrent.
A dust storm originating in the Sahara Desert swept across parts of Spain, France, the UK, and Ireland last month. In addition to bringing a red tinge to the sky, the dust caused a slight, yet noticeable, spike in radiation in the areas it reached. This radiation spike was caused by the presence of cesium-137, a radioactive isotope produced through the nuclear fission of uranium-235 in nuclear weapons. A legacy of French nuclear weapons testing that occurred in Algeria during the 1960s, the cesium-137 contamination is a reminder that while the testing of nuclear weapons may have been halted for the time being, the consequences of these tests live on through the poisoning of the planet mankind calls home.
The Saharan radioactive dust cloud is but the most recent visible phenomenon of a plague that has infected much of the world. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.