Throughout the invasion and 20-year occupation of Afghanistan, U.S. officials portrayed themselves as great saviors and benefactors of the Afghan people. Perhaps the best example of this phenomenon is the Pentagon’s application of the term “Operation Enduring Freedom” to its deadly and destructive operations in Afghanistan. There was also the supposed concern for “women’s rights” within the country.
It was always a lie. That was demonstrated by the fact that there was never an upward limit on the number of Afghan people who could be killed during the invasion and occupation. Why, early on, the Pentagon and the CIA even established a policy to not keep count of the number of Afghans they killed. It didn’t matter. Any number of deaths and injuries, no matter how high, was considered acceptable. The idea was that those people who survived the deadly and destructive U.S. violence would enjoy “enduring freedom” and “women’s rights.”
The truth is that U.S. officials never cared one whit for the well-being of the Afghan people, including all those people at Afghan wedding parties who were periodically bombed during the 20-year occupation.
Today, the U.S. government’s viciousness is, once again, on display, with two things: (1) The decision by President Biden and the Pentagon’s to enforce one of their patented systems of economic sanctions on the Afghan populace, and (2) Biden’s and the Pentagon’s decision to steal more than $7 billion from the Afghan government.
The sanctions are a pure display of viciousness. Why target the Afghan people with more death and suffering? The war is over. The Pentagon and the CIA lost. Get over it. Leave the Afghan people alone. Enough is enough. Can’t they be satisfied with the large number of deaths and the massive destruction they wreaked for the last 20 years on the Afghan people? Why kill and impoverish even more with a brutal system of economic sanctions?
The dark irony is that they’re enforcing the sanctions in the name of fighting “terrorism.” But isn’t the reason they condemn terrorism is that it targets innocent people as a means to achieve a political goal? Well, that is precisely what their evil system of sanctions does. It too targets innocent people with death, impoverishment, and suffering as a way to achieve a political goal — i.e., to make the Taliban regime look bad or even maybe — (hope springs eternal!) — brings regime change and another corrupt U.S. puppet regime into power.
Prior to the U.S. invasion of Afghanistan, the Taliban central bank had deposited more than $7 billion in the United States for safekeeping. That money rightly belongs to the Taliban central bank, which has demanded it back. It matters not that the Taliban defeated the Pentagon and the CIA and forced them to exit the country. The money still rightly belongs to the Afghan government.
President Biden and the Pentagon, however, have decided to steal it. They say that they are going to use half the money to compensate the victims of 9/11 and the other half for “humanitarian aid.” Oh, aren’t they such good, caring, and compassionate people? Who would have known?
But they are not. They are nothing more than common thieves. They have no moral or legal right to steal that money, no matter what they do with it. The money belongs to the Afghan government.
Moreover, the Taliban regime never had anything to do with the 9/11 attacks, and no one, including the victims of 9/11, has ever provided any evidence to the contrary. The only reason that the George W. Bush regime ordered the invasion of Afghanistan was because the Taliban refused his unconditional extradition demand for Osama bin Laden, which the Taliban had the legal right to do given that there was no extradition treaty between the two countries. The Bush regime never provided one iota of evidence indicating that the Taliban were complicit in the 9/11 attacks and neither have any of the 9/11 victims.
Moreover, the notion that Biden and the Pentagon are going to be “humanitarian” with the Taliban’s money is laughable. They couldn’t care less about humanitarian concerns among the Afghan people. Remember: There was never an upward limit on the number of Afghan people they were willing to kill, maim, and injure in the process of bringing “enduring freedom” and “women’s rights” to Afghanistan. Keep in mind also that 99 percent of the people they killed, maimed, and injured and whose homes and businesses were destroyed by U.S. bombs for 20 long years had nothing to do with the 9/11 attacks.
After wreaking so much death, suffering, and destruction on the people of Afghanistan, Biden and the Pentagon need to do the right thing. They need to lift those deadly and destructive sanctions and finally leave the Afghan people alone. They also need to return the Afghan government’s money to the Afghan government. Behaving like vicious common thieves seeking revenge and retribution for their defeat does not reflect well on the United States.
US Republican lawmakers have sent a letter pressing chief White House medical advisor Dr. Anthony Fauci for answers about his alleged silencing of concerns that the Covid-19 virus originally came from a Chinese lab.
The letter, sent on Monday by three US House members, cited emails suggesting that Fauci and Dr. Francis Collins, then director of the National Institutes of Health (NIH), tried in early 2020 to quash speculation among scientists that the virus may have originated in the Wuhan Institute of Virology. Instead of alerting national security officials to the pandemic’s potentially unnatural origin, Fauci and Collins sought to shut down the debate, the GOP lawmakers said.
The emails, which were obtained by media outlets under Freedom of Information Act requests, reportedly showed that some virology experts saw reason to believe that the virus was lab-created. Some of the messages made reference to a February 2020 conference call in which many scientists leaned toward the lab-leak theory. For instance, Tulane Medical School professor Robert Garry said he could see no “plausible natural scenario” for some aspects of Covid-19 otherwise.
“However, those same email communications, particularly when viewed in light of other publicly available information, demonstrate an apparent effort by you and Dr. Collins not only to cover up the concerns those virologists raised, but to suppress scientific debate about the origins of Covid-19,” the letter said.
Representatives Cathy McMorris Rodgers (R-Washington), Brett Guthrie (R-Kentucky) and Morgan Griffith (R-Virginia) signed the letter.
They demanded that Fauci provide details on how those conversations with scientists were initiated and who consulted him and Collins on Covid-19’s likely origins. The lawmakers also requested information on any communications by Fauci and Collins with Chinese scientists, as well as documents related to US funding of the research in Wuhan.
Even as scientists were speculating about Covid-19’s potentially manmade origins, Fauci told reporters in April 2020 that the sequencing of the virus was “totally consistent with a jump of a species from an animal to a human.” Earlier that same day, Collins sent him a message of concern about the lab leak theory, asking how NIH might “put down this very destructive conspiracy.”
Republican lawmakers have accused Fauci of directing taxpayer funding to gain-of-function research that could potentially make organisms more transmissible or lethal. In Monday’s letter, the House members claimed the efforts to quell the lab-leak theory may have stemmed at least partly from fears of those grants being exposed. “It appears you and Dr. Collins may have done so to protect China and avoid criticism about incredibly risky research that the National Institute of Allergy and Infectious Diseases was funding at the Wuhan lab,” the legislators said.
A May 2021 project report by the U.K. Ministry of Defense, created in partnership with the German Bundeswehr Office for Defense Planning, offers shocking highlights of the dystopian cybernetics future that global technocrats are pushing mankind toward.
The report, “Human Augmentation — The Dawn of a New Paradigm, a Strategic Implications Project,”1 reviews the scientific goals of the U.K. and German defense ministries, and they are precisely what the title suggests. Human augmentation is stressed as being a key area to focus on in order to win future wars.
But human augmentation will not be restricted to the military ranks. It’s really a way to further separate classes of humans, with the rich and powerful elite being augmented “super-humans.” It’s worth noting that anything released to the public is a decade or more behind current capabilities, so everything in this report can be considered dated news, even though it reads like pure science fiction.
“… the field of human augmentation has the potential to transform society, security and defense over the next 30 years,” the report states. “We must begin to understand the implications of these changes and shape them to our advantage now, before they are thrust upon us.
Technology in warfare has traditionally centered on increasingly sophisticated platforms that people move and fight from, or artefacts that they wear or wield to fight with. Advances in the life sciences and converging developments in related fields are, however, beginning to blur the line between technology and the human …
Many technologies that have the potential to deliver strategic advantage out to 2050 already exist and further advances will undoubtedly occur … Our potential adversaries will not be governed by the same ethical and legal considerations that we are, and they are already developing human augmentation capabilities.
Our key challenge will be establishing advantage in this field without compromising the values and freedoms that underpin our way of life …
When we think of human augmentation it is easy to imagine science fiction inspired suits or wonder drugs that produce super soldiers, but we are on the cusp of realizing the benefits in a range of roles now. Human augmentation will help to understand, optimize and enhance performance leading to incremental, as well as radical, improvements.”
Changing What It Means To Be Human
As noted in the report, “Human augmentation has the potential to … change the meaning of what it means to be a human.” This is precisely what Klaus Schwab, founder and executive chairman of the World Economic Forum (WEF), has stated is the goal of The Fourth Industrial Revolution.2
WEF has been at the center of global affairs for more than 40 years, and if you take the time to dive into WEF’s Fourth Industrial Revolution material, you realize that it’s all about transhumanism. It’s about the merger of man and machine. This is a dystopian future WEF and its global allies are actively trying to implement, whether humanity at large agrees with it or not.
Schwab dreams of a world in which humans are connected to the cloud, able to access the internet through their own brains. This, of course, also means that your brain would be accessible to people who might like to tinker with your thoughts, emotions, beliefs and behavior, be they the technocratic elite themselves or random hackers. As noted by history professor Yuval Noah Harari in late 2019, “humans are now hackable animals.”3 As noted in the featured report:4
“Human augmentation will become increasingly relevant, partly because it can directly enhance human capability and behavior and partly because it is the binding agent between people and machines.
Future wars will be won, not by those with the most advanced technology, but by those who can most effectively integrate the unique capabilities of both people and machines. The importance of human-machine teaming is widely acknowledged but it has been viewed from a techno-centric perspective.
Human augmentation is the missing part of this puzzle. Thinking of the person as a platform and understanding our people at an individual level is fundamental to successful human augmentation.”
Key words I’d like to draw your attention to is the affirmation that human augmentation can “directly enhance behavior.” Now, if you can enhance behavior, that means you can change someone’s behavior. And if you can change a person’s behavior in a positive way, you can also control it to the person’s own detriment.
Theoretically, absolutely anyone, any random civilian with a brain-to-cloud connection and the needed biological augmentation (such as strength or speed) could be given wireless instructions to carry out an assassination, for example, and pull it off flawlessly, even without prior training.
Alternatively, their physical body could temporarily be taken over by a remote operator with the prerequisite skills. Proof of concept already exists, and is reviewed by Dr. Charles Morgan, professor in the department of national security at the University of New Haven, in the lecture below. Using the internet and brain implants, thoughts can be transferred from one person to another. The sender can also directly influence the physical movements of the receiver.
The Human Platform
On page 12 of the report, the concept of the human body as a platform is described, and how various parts of the human platform can be augmented. For example:
Physical performance such as strength, dexterity, speed and endurance can be enhanced, as well as physical senses. One example given is gene editing for enhanced sight
Psychological performance such as cognition, emotion and motivation can be influenced to activate and direct desired behavior. Examples of cognitive augmentation include improving memory, attention, alertness, creativity, understanding, decision-making, intelligence and vigilance
Social performance — “the ability to perceive oneself as part of a group and the readiness to act as part of the team” — can be influenced. Communication skills, collaboration and trust are also included here
They list several different ways to influence the physical, psychological and social performance of the “human platform,” including genetics (germ line and somatic modification), the gut microbiome, synthetic biology, invasive (internal) and noninvasive (external) brain interfaces, passive and powered exoskeletons, herbs, drugs and nano technology, neurostimulation, augmented reality technologies such as external holograms or glasses with built-in artificial intelligence, and sensory augmentation technologies such as external sensors or implants. As noted in the report:
“The senses can be extended by translating frequencies beyond the normal human range into frequencies that can been seen, heard or otherwise detected. This could allow the user to ‘see’ through walls, sense vibrations and detect airborne chemicals and changes to magnetic fields.
More invasive options to enhance existing senses have also been demonstrated, for example, coating retinal cells with nanoparticles to enable vision in the infrared spectrum.”
They also point out that, from a defense perspective, methods to de-augment an augmented opponent will be needed. Can you even imagine the battlefield of the future, where soldiers are barraged from both sides with conflicting inputs?
As for ethics, the paper stresses that “we cannot wait for the ethics of human augmentation to be decided for us.” There may even be “moral obligations” to augment people, they say, such as when it would “promote well-being” or protect a population from a “novel threat.”
Interestingly, the paper notes that “It could be argued that treatments involving novel vaccination processes and gene and cell therapies are examples of human augmentation already in the pipeline.” This appears to be a direct reference to mRNA and vector DNA COVID jabs. If so, it’s an open admission that they are a human augmentation strategy in progress.
The Challenge of Unintended Consequences
Of course, there can be any number of side effects and unintended outcomes when you start augmenting an aspect of the human body or mind. As explained in the featured report:
“The relationship between augmentation inputs and outputs is not as simple as it might appear. An augmentation might be used to enhance a person’s endurance but could unintentionally harm their ability to think clearly and decisively in a timely fashion.
In a warfighting context, an augmentation could make a commander more intelligent, but less able to lead due to their reduced ability to socially interact or because they increasingly make unethical decisions. Even a relatively uncontentious enhancement such as an exoskeleton may improve physical performance for specific tasks, but inadvertently result in a loss of balance or reduced coordination when not being worn.
The notion of enhancement is clouded further by the intricacies of the human nervous system where a modifier in one area could have an unintended effect elsewhere. Variation between people makes designing enhancements even more challenging.”
Still, none of that is cause to reconsider or slow down the march toward transhumanism, according to the authors. We just need to understand the human body better, and for that, we need to collect and analyze more data on human performance, behavior, genetics and epigenetics. As noted by the authors:
“Devices that track movement, heart rate, oxygenation levels and location are already commonplace and will become increasingly accurate and sophisticated, making it possible to gather an increasingly wide array of performance data in real time. We can also analyze data in ways that were impossible even five years ago.
Artificial intelligence can analyze massive sets of information almost instantaneously and turn it into products that can inform decision-making. This marriage of data collection and analytics is the foundation of future human augmentation.”
Lab-Grown Designer Babies
As mentioned, by the time a technological advancement is admitted publicly, the research is already a decade or more down the road. Consider, then, the February 1, 2022, article in Futurism,5 which announced that Chinese scientists have developed an artificial intelligence nanny robot to care for fetuses grown inside an artificial womb. According to Futurism :6
“The system could theoretically allow parents to grow a baby in a lab, thereby eliminating the need for a human to carry a child. The researchers go so far as to say that this system would be safer than traditional childbearing.”
As of now, the AI robot is only in charge of lab-raised animal embryos, as “experimentation on human embryos is still forbidden under international law.” However, that could change at any time. In May 2021, the International Society for Stem Cell Research went ahead and relaxed the rules7 on human embryonic experimentation.8
Up until then, the rule had been that no human embryo could be grown in a lab environment beyond 14 days. Human embryos may now be grown beyond 14 days if certain conditions are met. In some countries, laws would still need to be changed to go beyond 14 days, but regardless, there’s no doubt that as transhumanism gets underway in earnest, ethical considerations about growing babies in laboratories will be tossed out.
Combine the announcement of an AI robot nanny to care for lab-grown embryos with the 2018 announcement that Chinese scientists were creating CRISPR gene-edited babies. As reported by Technology Review, November 25, 2018,9 “A daring effort is underway to create the first children whose DNA has been tailored using gene editing.”
The embryos were genetically edited to disable a gene called CCR5, to make the babies “resistant to HIV, smallpox and cholera.” The embryos were then implanted into a human mother using in vitro fertilization. At the time, the lead scientist refused to answer whether the undertaking had resulted in a live birth, but shortly thereafter it was confirmed that one trial participant had indeed given birth to gene-edited twins in November 2018.10
In June 2019, Nature magazine published an article11 questioning whether the CRISPR babies might inadvertently have been given a shorter life span, as research had recently discovered that people with two disabled copies of the CCR5 gene were 21% more likely to die before the age of 76 than those with one functioning copy of that gene. The babies might also be more susceptible to influenza and autoimmune conditions, thanks to this genetic tinkering.
Should We Breed Chimeras to Satisfy Need for Organs?
Ethical considerations about animal-human hybrids (chimeras) will probably also fall by the wayside once transhumanism becomes normalized. Already, human-monkey hybrid embryos have been grown by a team of Chinese and American scientists.12
The hybrid embryos are part of an effort to find new ways to produce organs for transplant patients. The idea is to raise monkeys with human-compatible organs that can then be harvested as needed. Here, the embryos were grown in test tubes for as long as 20 days — and this was done before the ISSCR officially agreed to relaxing the 14-day rule.
The question is, if this kind of research ends up being successful, and the creation of animals with human organs is actually feasible, at what point does the chimera become a human?
How do we know that what looks like a monkey doesn’t have a human brain, with the intelligence that goes with it? Taking it a step further, even, what’s to prevent scientists from growing human organ donors? Human clones, even? It’s a slippery slope, for sure.
Privacy in the Age of Transhumanism
Perhaps one of the greatest concerns I (and many others) have is that not only are we moving toward a merger of man and machine, but at the same time we’re also increasingly outsourcing human morality to machines. I cannot imagine the end result being anything but devastating. How did that happen? Timandra Harkness, a BBC Radio presenter and author of “Big Data: Does Size Matter?” writes:13
“As the recent pandemic years have shown, the desire to be free from scrutiny unless there’s a good reason to be scrutinized is widely seen as, at best, eccentric and, at worst, automatic grounds for suspicion.
We simply can’t articulate why a private life is valuable. We have no sense of ourselves as autonomous beings, persons who need a space in which to reflect, to share thoughts with a few others, before venturing into public space with words and actions that we feel ready to defend …
Part of the appeal of technologies like AI is the fantasy that a machine can take the role of wise parent, immune to the emotion and unpredictability of mere humans. But this tells us less about the real capabilities of AI, and more about our disillusionment with ourselves.
The urge to fix COVID, or other social problems, with technology springs from this lack of trust in other people. So does the cavalier disregard for privacy as an expression of moral autonomy.
Technology ethics can’t save us, any more than technology can. Even during a pandemic, how we regard one another is the fundamental question at the root of ethics. So we do need to treat technology as just a tool, after all. Otherwise we risk being made its instruments in a world without morals.”
An 1871 dataset of sea temperatures across the Great Barrier Reef in Australia has been compared to recent measurements logged at the same reef areas. No differences in temperature were found by Dr. Bill Johnson, leading him to conclude: “Alarming claims that the East Australian Current has warmed due to global warming are therefore without foundation.”
The 1871 temperatures were taken by the SS Governor Blackall steamship on a voyage around the Australian east coast to observe a total eclipse of the sun in the north of the continent. Hourly measurements were made between 6am and 6pm every day in the voyage from Port Stanley, north of Sydney, to Cape York and repeated on the journey back. Dr. Johnson, a former research scientist at the New South Wales Department of Natural Resources, allowed for the considerable seasonal variations in temperature across the reef but concluded that nothing much had changed. He said there was no evidence that the system regulating temperature had broken down “or is likely to break down in the future”.
Needless to say, such stories do not tend to appear in the media, most of which is firmly wedded to the notion that human-caused global warming is destroying the coral reefs around the world. In October 2020, the BBC reported that the Great Barrier Reef had lost half of its coral since 1995, citing a report that said it was due to “warmer seas driven by climate change”. But Professor Peter Ridd, who has spent 40 years observing the reef, noted recently that it was in robust good health. Coral growth rates have if anything “increased over the last 100 years”. The graph below, compiled by Ridd from Australian Institute of Marine Science records, illustrates recent growth.
Agence France-Presse‘s award-winning reporter Marlow Hood recently quoted a University of Leeds paper that said coral reefs anchoring a quarter of marine wildlife will “most likely” be wiped out, even if the rise in global warming from pre-industrial times is capped at 1.5°C – which amounts to future warming of just 0.4°C, as 1.1°C has already occurred since 1820. Mr. Hood describes himself on his twitter feed as the “Herald of the Anthropocene” and was recently given €100,000 by the Spanish bank BBVA , which is heavily involved in Net Zero finance. In his commendation, Mr Hood was praised for his ability to “synthesize complex scientific models and studies and explain them in simple terms”. Certainly, Mr Hood went to the heart of the Leeds paper by further reporting that with an increase of 2°C, reef mortality “would be 100%”. This finding is said to have come from a “new generation of climate models”.
Corals have long occupied an exalted place in the climate tablets of doom. Their demise is commonly projected from the natural bleaching that occurs when they expel symbiotic algae, suggested to occur in reaction to sudden changes in water temperature. However, most bleaching – which also appears to have an important evolutionary function – occurs around weather oscillations, such as the El Niño event. These happen on a regular basis and once localised conditions have been stabilised, the coral usually recovers. Tropical coral thrives in temperatures between about 24°C and 32°C and sometimes grows quicker in warmer waters. Any change in long term global temperatures is unlikely to be a threat and certainly not one as small as 0.4°C. In any case, according to Dr. Johnson’s discoveries, there hasn’t been any change in such conditions on the Great Barrier Reef for at least 150 years.
A more practical threat to coral reefs is the less discussed practice of blowing them up and using them for building materials, jewellery, calcium health supplements and marine aquarium decorations. According to Big Blue Ocean Cleanup, an environmental non-profit organisation, this trade is worth $375 billion a year. This is an astonishing sum. Across the Pacific, Blue Ocean identifies two techniques of destruction. The first is small-scale mining using crowbars and sledgehammers to break off the coral branches. The second involves the use of dynamite.
Needless to say, this has an enormous impact on the surrounding eco-system, killing marine life and leaving a barren ocean behind. Indiscriminate destruction also causes sand erosion and removes coastal protection. Ironically, much of the coral has been used to build airports and resorts in places like the Maldives to house tourists who come to marvel at the reefs.
Coral reefs need protecting. It is not a good idea to drench them in untreated sewage, douse them with toxic chemicals, smash up their habitat with reckless fishing or rearrange the ocean floor with high explosives. But this is relatively mundane environmental housekeeping work. It is a world away from using unproven science statements and climate models to spout ‘save the planet’ rhetoric and push for an unrealistic control-and-distribute Net Zero project.
In the run up to COP26, one of Prince William’s £1 million “Earthshot” gifts was handed to a small Bahamian company called Coral Vita that says it grows coral to replant in the ocean. Writing in the Spectator Australia, the biologist Jennifer Marohasy noted that the Australian government permitted the mining every year of 200 tonnes of coral from the Great Barrier Reef. At the same time, $1 billion Australian dollars was provided to save the ‘dying’ reef. Some of this money, she noted, will be used to replant corals.
She added: “[T]here will be jobs for scuba divers, and it will be filmed by underwater videographers, marine scientists will collect data around the programme and boats will be chartered. There will be money for almost everyone who wants to participate – if they are vaccinated, believe in human-caused climate change and believe the Great Barrier Reef is dying.”
Last year, cartoons began to appear depicting an endless cycle of variants and government responses. They call to mind the definition of insanity (misattributed to Einstein) as “doing the same thing over and over again and expecting different results.” Or perhaps the less well known line from a 1990s Stephen King miniseries “Hell is repetition.”
The direction of public health policy over the past two years has been difficult to understand. It may be a fool’s errand to use logic and reason for something that by design makes no sense. But coming at it as I do with no prior education in medicine or epidemiology, crude tools such as logic and common sense may still be useful: The basic principles of reality are true for all endeavors. For a plan to work, it must work within a finite time; for every on ramp, there must be an exit.
We started out with “Two weeks to flatten the curve.” If nothing else can be said in favor of this plan, credit must be given for how well it was explained. Pictures like this were clear enough. With my university-level education in math and physics, I understood that the area under the curve was expected to remain equal under both alternatives: the one with and the other without “precautions” (as the label in the diagram euphemistically refers to life under communism). The peak of the curve would be lower, at the cost of the epidemic being extended in duration.
While the plan might or might not work, it is possible to state the premise without contradicting laws of logic or common sense. The flattening plan does accept that nearly everyone will eventually be exposed and the contagion will exhaust itself. If the plan enables some people to delay their exposure, up to a point, that could buy doctors some time to better learn how to treat them. Or perhaps a miraculous vaccine will be introduced that would create sterilizing immunity and halt the outbreak in its tracks enabling those who had delayed to avoid infection entirely.
While the plan was clear, it was not guaranteed to work. Subtle effects could undermine the simple story told by the picture. Perhaps everyone staying at home will not help because people will get infected at home. Or perhaps too many people must leave home because essential critical infrastructure workers such as marijuana dispensaries must remain open to keep society running.
Some suggested then a policy that postpones population immunity would give the virus more time to mutate. Given enough time, people who were infected and have developed natural immunity to an earlier variant would face a virus sufficiently different that they might become infected again. Along these lines, biotech executive Vivek Ramaswamy and medical professor Dr Apoorva Ramaswamy MD, writing in the Wall Street Journal, question whether we should even try to slow the spread when “Speeding It May Be Safer.” Cognitive scientist Mark Changzi suggests “slowing the spread among the healthy not-at-risk, which just raises the frail’s chances of getting infected.” “Dr. Robert Malone and Dr. Geert Vanden Bossche, who have been asserting that you can’t vaccinate your way out of a pandemic for months” believe that vaccination during an outbreak accelerates the evolution of the virus away from the version targeted by the vaccine.
Quite likely the “precautions” did nothing to make the curve flatter. With the benefit of hindsight we can observe that outbreaks of the virus in proximate US states (or neighboring nations that are similar in size and demographics in other regions of the world) rise and fall side by side in cyclical surges, regardless of when or if efforts to slow the spread were made. There is no impact on the variability of any public health metric based on when a “precaution” was undertaken.
After the hospitalizations peaked and then declined to near zero in the spring of 2020, I naively expected that we had done what we could, and it was over. Whether we had flattened the curve, or, the virus did what it would have done anyway, was at that point irrelevant. Instead of ending the precautions, there was an unstated shift from the original strategy to a new one. Unlike the original, the new policy was not clearly explained. I suspect the reason is that it could not have been explained without it becoming obvious that it did not make any sense.
“Flatten the curve” assumes contagions come to an end – either through immunity or viruses burn themselves out for reasons we do not fully understand. All things come to an end. Even the plague of the Black Death ran out of gas before it wiped out the entire human race. If an outbreak ends when most of us have been exposed (and either died or developed immunity), how can slowing it down be said to save lives? Is it not the best we can hope for that some people are exposed and suffer the consequences later rather than sooner?
Evidence of the new reality appeared to me one day when I was stuck in a traffic jam, on a trip I (and many of my neighbors) made in violation of my locality’s “shelter in place” order. As I puzzled over this new reality, I noticed overhead digital signage (paid for by my governor’s massive ad spend on Covid propaganda), stating: “Stay at home: save lives.” This was the initial wave of a propaganda tsunami imploring us to “slow the spread.”
A story about a superspreader who went to a party and infected multiple people who subsequently died attributed the deaths to the careless person who probably did not wear a mask. Was there some alternate version of reality in which the dead partygoers lived out the rest of their natural life never being exposed to a virus to which they were vulnerable? Should the superspreader be held responsible for their exposure, or was it only a matter of time until the virus found them, one way or another?
Sanctimonious lockdowners heaped scorn and ridicule on countries that did not slow the spread. A small industry of curve-fitting explanations were offered to explain the “success stories:” they locked down, they wore face masks, they tested, they quarantined, they contact-traced, they social distanced. They did as they were told. They obeyed authority. And we should do likewise.
According to Dr. Anthony Fauci MD, it was the time for us ornery Americans to do as we were told. In retrospect every one of the virtuous nations had its own spike or two, or three, often after getting fully vaccinated, taking a victory lap, and dislocating both of their shoulders by patting themselves on the back overly vigorously.
Consider testing. Some virtuous nations tested. Based on the long lines of cars to get into the popup centers, the United States tested a lot too. When former president Donald Trump suggested that – perhaps – we were overtesting, he was subjected to enormous ridicule. Yet how could testing help slow the spread of a virus? By itself testing does nothing other than identify sick people.
Can a test do a better job at identifying sick people than they can do on their own simply by noticing whether they have symptoms? If testing once a week does not help, does testing twice a week? And if so, then why do we care about a test result, if asymptomatic people are not contagious? In reality testing produced too many false positives to be useful.
Testing could in theory help if combined with contact tracing and quarantines to isolate the infected people. Contact tracing was another ritual of the success stories – yet contact tracing could not possibly work if someone could be infected by coming within six feet of a sick person or walking down the same side of the street because the second-order contacts of contacts would rapidly explode to include everyone in an entire city or region. This was another instance of Yogi Berra’s observation that “In theory there is no difference between theory and practice. In practice there is.”
I wondered what the goals of the new policy of “slow the spread” could be. Was it zero-covid? Zero-covid was the objective of a small cultof fanatics that never gained much traction in the US. A serious go at it would require a country to permanently ban inbound international travel. This was done in a small and tightly controlled nation where a friend of mine lives. According to my friend, they had very low levels of infection; however, the nation’s economy was tourism-based and the continued success of the policy requires that travelers not enter the country. The operation was a success, the patient died.
We were not flattening the curve, nor did it look like a strategy of total eradication. We were in a strange middle ground. At best we were pushing the pain into the future but with no plan to ever deal with it. The goals and exit conditions of the plan were not clearly explained. I did at one point find a statement by Dr. Fauci that preventive measures could drive the disease down to a very low level. Was it assumed to remain low forever? If not, then from that low base, outbreaks could be somehow contained?
So when people heard in Summer 2020 that Biden aimed to “get covid under control,” some people imagined an optimistic state of affairs whereby, once we all got vaccinated or wore masks for just 100 days (link), covid might be suppressed to such a permanently low level that most of us could forget about it, just as we forget about polio. Such people imagined a one-time, short-term effort to “get covid under control,” like unlocking a door.
If we are to believe that a worldwide pandemic grew from an outbreak of twelve people in Wuhan, China to infect nearly the entire world (even indigenous tribes in the Amazon jungle who are by definition quarantined) why would it not do the same when we emerged from our underground fallout shelters? What if through assiduously standing in small circles painted on the floor in grocery stores and wearing underwear on our faces, we succeeded in driving the number of Covid infections down to a very small number? To pick a number, for example, twelve people. Why would the contagion not, in the absence of broader acquired immunity, spread again from that new base of twelve, until eventually reaching all of those remaining uninfected?
It took me some time to give it a name. I settled on “suppression.” The fundamental reason that suppression is not a policy is that it has no exit. For a thing to work it must work within a limited time. If the measures to slow the spread succeeded in slowing it, then what? The nature of the off ramp is the answer to the question, “What happens when we stop doing it?” If the answer is, “It would go right back to what it was doing before,” then there is no exit.
During 2020 I had people tell me that we could not end the lockdown because the epidemic would pick up right where it left off and millions would die AND (sometimes the same people ) that if we keep up the restrictive measures for a while then we could stop because the virus would not come back. A bit of logic rules out the possibility that the virus could both come back and not come back.
Do we then spend the rest of our lives acting out Covid theater? Dr. Fauci said that he would never shake hands again. Blue check marks fret about quarantining their children. Jenin Younes reflected on a survey in which hypochondriac epidemiologists who are afraid to open their mail explain that they now consider a normal life to be dangerously reckless. Substack author Eugyppius writes about a medical journal editor who “can’t work out what we’re even doing here, but he wants us to keep doing it.”
Dr Prasad explained the difference between finite and infinite strategies:
Even if most of Biden’s voters agreed with his campaign promise to “get covid under control” in the abstract, this slogan does not specify whether the state of being “under control” involves a one-time effort, or a sustained effort over time. If you unlock a door, you do it once and you can forget it; if you lift an overhead hatch, maybe you have to keep holding it up so that it doesn’t fall back down again.
Slowing the spread – if such a thing is even possible – means we get to the same place later rather than sooner. Flat or not, it is over when you reach the right tail of the curve. The strange middle ground of slowing the spread with no exit condition, would, if tried, ruin our lives forever. Are you willing to live under covid restrictions for the rest of your life? And your children for the rest of their lives and all subsequent generations? For some measures that slow the spread of disease, such as indoor plumbing, garbage removal and better diet, the answer is yes. But if our forebears during the plague of the Black Death had adopted a covid-like attempt at suppression, no one would have gone outdoors since the 15th century.
During this time of insanity, some of us went about our lives as best we could and ignored the restrictions. The rest of the world is now coming to terms with the understanding that the “precautions” don’t do much. At best what is going to happen anyway, happens. If there is no off ramp then the change is either permanent or it will go on until failure is evident and people stop caring. Then they will go back to normal one by one.
Robert Blumen is a software engineer and podcast host who writes occasionally about political and economic issues.
OTTAWA – The Justice Centre for Constitutional Freedoms today filed a lawsuit in Federal Court seeking to strike down the federal government’s mandatory Covid-19 vaccine requirements for air travellers. The court action is on behalf of several Canadians from across Canada whose Charter rights and freedoms have been infringed.
On October 30, 2021, the federal government announced that anyone travelling by air, train, or ship, must be fully vaccinated. The travel vaccination mandate has prevented approximately 6 million unvaccinated Canadians (15% of Canada’s population) from travel within Canada and prevents them from flying out of Canada. Some of the Canadians involved in the lawsuit cannot travel to help sick loved ones, get to work, visit family and friends, take international vacations, and live ordinary lives.
The main applicant in the case is former Newfoundland Premier, The Honourable A. Brian Peckford. Mr. Peckford, pictured, is the only surviving drafter and signatory 40 years after the 1982 Constitution and the Charter of Rights and Freedoms was enacted.
“It is becoming more obvious that being vaccinated does not stop people from getting Covid and does not stop them from spreading it”, says the former Premier. “The government has not shown that the policy makes flying safer—it simply discriminates”, he notes. “When I heard Prime Minister Trudeau call the unvaccinated ‘racists,’ ‘misogynists, ‘anti-science’ and ‘extremist’ and his musing ‘do we tolerate these people?’ it became clear he is sowing divisions and advancing his vendetta against a specific group of Canadians—this is completely against the democratic and Canadian values I love about this country”, adds Mr. Peckford.
“The federal travel ban has segregated me from other Canadians. It’s discriminatory, violates my Charter rights and that’s why I am fighting the travel ban,” explains Mr. Peckford.
The Justice Centre’s legal challenge cites violations of Charter rights including mobility, life, liberty and security of the person, privacy, and discrimination. The lawsuit also challenges whether the Minister of Transportation has the jurisdiction to use aviation safety powers to enforce public health measures.
In discussing effective border control measures at the start of the Covid-19 outbreak, Canada’s chief medical officer, Dr. Tam, said: “As you move further away from that epicentre, any other border measures are much less effective. Data on public health has shown that many of these are actually not effective at all… WHO advises against any kind of travel and trade restrictions, saying that they are inappropriate and could actually cause more harm than good in terms of our global effort to contain.” (Canada House of Commons, Standing Committee on Health Meeting, February 5, 2020)
The World Health Organization (“WHO”) continues to maintain that position and on January 19, 2022, urged all countries to: “Lift or ease international traffic bans as they do not provide added value and continue to contribute to the economic and social stress experienced by States Parties. The failure of travel restrictions introduced after the detection and reporting of Omicron variant to limit international spread of Omicron demonstrates the ineffectiveness of such measures over time.” The WHO repeated that countries should: “not require proof of vaccination against COVID-19 for international travel.” (World Health Organization, Statement on the tenth meeting of the International Health Regulations (2005) Emergency Committee regarding the coronavirus disease (COVID-19) pandemic, January 19, 2022.)
“Despite the confirmed science that the vaccine does not stop people from getting or spreading the virus and the repeated warnings from the WHO, it’s clear the federal government is out of step and arbitrarily restricting Canadians fundamental rights and freedoms,” says Keith Wilson, Q.C., lead counsel for the legal challenge. “It is profoundly disturbing that a marginalized group in Canada—the unvaccinated—are essentially prohibited from leaving the country,” he adds.
“Canadians have been losing hope in the Charter and our courts. We are going to put the best arguments and evidence forward so that the court can clarify where governments overstep,” concludes Mr. Wilson.
The court will be asked to hear the case on an expedited basis given the serious infringement on Canadians’ mobility and other rights. Canada is the only country in the developed world that has banned Covid vaccine-free travellers from air travel.
The ongoing Truckers for Freedom convoy in Ottawa has triggered a shockwave that is reaching all around the world. Even as our authoritarian federal regime continues to double down on measures and threatens to use brute force tactics against peaceful protesters, many provinces are nervously beginning to lay out a timeline for ending mandates.
But there is something important missing from the conversation surrounding the end of mandates. If the mandates are simply dropped today without calling out the underlying legal and ethical fallacy that was used to justify them, government overreach will have become normalized. We will be left without the legal protections to stop them from doing this to us again after the truckers go home. All it will take to put us back in a cage is for the government to point at the next wave, the next virus variant, or the next non-Covid emergency. We will have normalized that our rights, our freedoms, our bodily autonomy, and even access to our lives are conditional privileges, subject to opinion polls and technocratic impulses, and that they can be withdrawn again at any time, “for our safety.”
Quebec Health Minister Christian Dubé admits that vaccine passports and mandatory masks have no end in sight, and will remain “tools” to ensure a return to “normal life” when another wave hits. pic.twitter.com/TXJnN4xJ8x
In March of 2020, in violation of the principles embedded in our constitutions, governments around the world convinced citizens to give their leaders and public institutions the authority to overrule individual rights in order to “flatten the curve.” That impulse went unchallenged under the false assumption that human rights violations could be justified as long as the benefits to the majority outweighed the costs to the minority. By accepting this excuse for overriding unconditional rights, we transformed ourselves into an authoritarian police state where “might makes right”. That is the moment when all the checks and balances in our scientific and democratic institutions stopped functioning.
Liberal democracy was built around the principle that individual rights must be unconditional. In other words, they are meant to supersede the authority of government. Consequently, individual rights (such as bodily autonomy) were meant to serve as checks and balances on government power. They were meant to provide a hard limit to what our government can do to us without our individual consent.
If the government cannot override your rights to bend you to its will, then it will be forced to try to convince you by talking with you. That forces government to be transparent and to engage in meaningful debate with critics. Your ability to say NO, and to have your choice respected, is the difference between a functioning liberal democracy and an authoritarian regime.
The natural instinct of fearful people is to control those around them. Unconditional rights force people to negotiate voluntary participation in collective solutions. Thus, unconditional rights prevent the formation of echo chambers and provide an important counter-weight to rein in uncontrolled panic. When no-one has the option to use the brute force of State power to force others to submit to what they think is “the right thing to do”, then the only path forward is to keep talking to everyone, including to “fringe minorities” with “unacceptable views”. When we allow rights to become conditional, it is virtually a certainty that during a crisis, panicked citizens and opportunistic politicians will give in to their worst impulses and trample those who disagree with them.
Unconditional individual rights prevent governments from taking unwilling citizens on crusades. They prevent scientific institutions from transforming themselves into unchallengeable “Ministries of Truth” that can double down on their mistakes to avoid accountability. They ensure that the checks and balances that make science and democracy work do not break down in the chaos of a crisis. In the heat of an emergency when policy decisions are often made on the fly, unconditional rights are often the only safeguards to protect minorities from panicked mobs and self-anointed kings.
If we allow our leaders to normalize the idea that rights can be switched off during emergencies or when political leaders decide that “the science is settled”, then we are giving the government terrifying and unlimited power over us. It gives those who control the levers of power the authority to turn off access to your life. That turns the competition for power into a zero-sum game: the winners become masters, the losers become serfs. It means you can no longer afford to allow the other side to win an election, at any cost, nor agree to a peaceful transfer of power, because if you lose the winning team becomes the master of your destiny. And so, a zero-sum game of brutal power politics is set in motion. Unconditional individual rights are the antidote to civil war. Liberal democracy collapses without them.
Withdrawing mandates because “the Omicron variant is mild” or because “the costs of continuing the measures outweigh the benefits” does not undo what has been normalized and legitimized. If the legitimacy of mandates is not overturned, you will not be going back to your normal life. It may superficially look similar to your life before Covid, but in reality you will be living in a Brave New World where governments temporarily grant privileges to those who conform with the government’s vision of how we should live. You will no longer be celebrating your differences, cultivating your individuality, or making your own free choices. Only conformity will enable you to exist. You will be living under a regime in which any new “crisis” can serve as justification to impose restrictions on those who don’t “get with the program” as long as mobs and technocrats think the restrictions are “reasonable”. You will no longer be the master of your own life. A golden cage is still a cage if someone else controls the lock on the door.
Politicians and public health authorities MUST be forced to acknowledge that mandates are a violation of civil liberties. The public MUST be confronted by the fact that liberal democracy ceases to exist without the unconditional (inalienable) safeguards of individual rights and freedoms. The public MUST recognize that science ceases to function when mandates can be used to cut off scientific debates. Our governments and our fellow citizens MUST be made to understand that unconditional rights are especially important during a crisis.
If the legal and ethical fallacies that were used to justify mandates are not called out as inexcusable violations of our constitutional rights, we will have inadvertently normalized the illiberal idea that, as long as someone in a lab coat says it’s okay, this can be done to us again, at any time, whether to fight the next wave of Covid, to take away freedoms to fight “climate change”, to seize assets to solve a government debt crisis, or simply to socially engineer outcomes according to whatever our leaders define as a “fairer and more equitable world”.
How we navigate the end of mandates determines whether we win our freedom or whether we allow our leaders to normalize a Brave New World with conditional rights that can be turned off again during the next “emergency”.
Lawyers working for Hillary Clinton’s 2016 presidential campaign paid an IT firm to “infiltrate” servers at Trump Tower and the White House in order to establish a “narrative” that would link Donald Trump to Russia, an explosive new legal filing alleges.
The legal motion, filed in a District of Columbia court on Friday by a Justice Department (DOJ) prosecutor investigating the origins of the FBI’s ‘Russiagate’ probe, relates to potential conflicts of interest by former Clinton campaign lawyer Michael Sussmann. Sussmann has previously pleaded not guilty to a one-count charge of lying to federal agents.
Two months before the 2016 election, Sussmann, a partner at Perkins Coie, the law firm that represented the Democrats and Clinton’s campaign, allegedly told the FBI he was not working on behalf of Clinton when he presented the agency with supposedly incriminating documents.
In the filing, Special Counsel John Durham alleges that Sussmann was working on behalf of the Clinton campaign and an unnamed “technology executive” at a US tech firm when he submitted “purported data” and “white papers” to then-FBI General Counsel James Baker in September 2016. They apparently pointed to a “covert communications channel” between the Trump Organization and Russia-based Alfa Bank (identified as “Russian Bank-1”).
Highlighting Sussmann’s “billing records,” Durham alleges that he had “repeatedly billed the Clinton Campaign for his work on the Russian Bank-1 allegations.” This involved an unnamed lawyer working with the campaign, the tech executive (identified as “Tech Executive-1”), an investigative firm, several cyber-researchers, and employees at “multiple internet companies,” the motion states.
It alleges that the executive “exploited his access to non-public and/or proprietary Internet data” and tasked researchers at an unnamed US university to “mine Internet data” so as to create “an inference” and “narrative” linking Trump to Russia. The executive claimed to be working “to please certain VIPs.”
While many US media outlets pointed to the Alfa Bank claims as proof of Trump’s “collusion” with the Kremlin, the FBI found that the email server in question was run by an advertising agency that sent out promotional emails for Trump’s hotels, among other things.
Among the internet data exploited was “domain name system (DNS) Internet traffic” from Trump Tower, Trump’s apartment building in New York City, and the White House, the filing states. It alleged that Tech Executive-1’s employer (identified as “Internet Company-1”) provided DNS resolution services to the White House – and accused the executive and his associates of exploiting this arrangement to mine data for “derogatory information” about Trump.
Then, in 2017, Sussmann apparently used this information to compile “an updated set of allegations” about Trump’s supposed Russian ties – noting “suspicious DNS lookups” and “Russian-made wireless phones” – to another US government agency, the motion states. Durham said he found “no support for these allegations” and added that some of the lookups occurred as early as 2014 during the Obama administration.
Demanding “reparations” be paid, Trump said in a statement on Saturday that the filing provided “indisputable evidence” that his campaign and presidency were “spied on by operatives paid by the Hillary Clinton Campaign” to “develop a completely fabricated connection to Russia.”
“This is a scandal far greater in scope and magnitude than Watergate and those who were involved in and knew about this spying operation should be subject to criminal prosecution,” he added, noting that there was a time when the alleged crime “would have been punishable by death.”
There has been no official response from Clinton as yet.
Last year, Sussmann’s attorneys said their client had “committed no crime,” calling charges against him “baseless [and] unprecedented.” Meanwhile, a lawyer for the person who fed Sussmann the Alfa Bank claims said that his client did not know his law firm had a relationship with the Clinton campaign “and was simply doing the right thing.”
Sussmann represented the Democratic National Committee (DNC) during proceedings related to the alleged 2016 hack of its computers. Both Clinton and the DNC had blamed Russia, but could not back up their accusations.
The original Russia probe ballooned into a two-year investigation led by then-Special Counsel Robert Mueller, who failed to produce evidence of collusion between Trump’s campaign and Russia.
in the age of government sponsored science driven by grants, sinecure, and sponsorship, scientists face a difficult set of choices.
they must, if they wish to continue receiving the largess of the gold-givers toe the party line of state or commercially sponsored science. he who has paid the piper demands to call the tune and producing work that does not suit “the narrative” is career suicide. your funding will dry up. so may your position, your prospects for advancement, and even your tenure. you will not be asked to join committees, interviewed for articles, citied, or supported. you may be outright attacked. i discuss this in more depth HERE.
but scientists also face another constraint: they need to be accurate. they need to run good experiments, collect good data, and relay it faithfully. if they do not, they will get called out and revealed as incompetents or frauds. this too will end one’s career as it means that not only are you doing no useful work (apart from to propogandists) but will reveal that you have sold out integrity for lucre and that is the end of peers taking you seriously. you play for team lysenko now.
the need to thread this needle and appease and please both demands has led to an odd practice:
many times, the claims made in the abstract or in the conclusions are not supported by the actual data.
i know this sounds a little bizarre, but as someone who reads perhaps 1000 such papers a year, allow me to assure you, it is stunningly common in any politically loaded sphere. (and you would be amazed how many are politically loaded. it need not be government pushing it. watching geneticists tie their conclusions in knots to claim that you can breed horses for speed and endurance or dogs for intelligence but that of course there is no such thing as eugenics in humans because that would be unspeakable despite your having just proved that there is in fact, eugenics in humans is really quite something. they go to astounding lengths in the introductions of their books to disavow what they are about to prove.)
this odd compromise sort of works, but mostly, it doesn’t.
it gives those who fund studies and the journals who curate them for ideological purity their bone. the abstract says “X means Y.” this is what they want for the press releases and for waving around.
it also puts the actual data out into the world. this is what researchers, both those who did the work and those who will read it in detail, actually need. they can see the facts and will not be gulled in by the claims in the conclusion as they are adept at drawing their own conclusions.
this leads to the weird outcome of the public and the politicians frequently having one idea about what a study says and the experts in the field having more or less the opposite take.
the “experts” all know what the data means and why they are not allowed to say it. it works a bit like the foils used by renaissance dialogue writers to ape at being fools while presenting the actual case being made while the “authorities” presented the “narrative” and were made fools of by those able to read between the lines.
in the age of the internet, this sets up a bizarre and deeply frustrating conflict: those who can and do really read studies are constantly having to pick them apart and explain to the “google and spam” crowd who just selectively confirm their biases and skim the lead paragraph of a study why the study they just cited does not, in fact, say what they are claiming it does.
and, of course, trying to convince someone that the authors deliberately misstated the facts in the summary is like trying to teach a new trick to the very oldest of dogs. they are just not having it.
this has created a rancorous and dangerously stupid level of debate and an impossible burden for any one individual to carry. it takes 10 seconds to search, skim, and spam with a study you never read and start yelling “peer review!” over and over as if that means something.
it can take hours to pick the study apart and see if it really does support the conclusions stated in the summary and then hours more to convince someone who has not even read it (and probably does not know how). that’s unwinnable. it’s like sisyphus getting and additional rock to push back up the hill every time he reaches the top. pretty soon it’s 20 boulders and nothing is going anywhere.
fortunately, the internet age has produced a large group of folks interested in picking these studies apart and publishing their takes. and we form communities and help one another. so no one has to do ALL the work when the CDC publishes yet more self refuting “wave around” data.
this is, in fact, what real peer review is. it’s supposed to be hostile and to pick holes.
the upshot here is that you should be very careful taking studies you have not actually read at face value.
you need to read them. thoroughly. waving them around as if you did when you have not is a recipe for being wrong.
this article is being used to push boosters. this is because the authors said this:
i have not spoken to them. perhaps they believe this, perhaps they do not but felt they had to say it or be pariahs. i have no special insight there. but i can read data.
so we have some ingrained bayesian issues with our cohorts that may inject serious bias toward making vaccines look effective.
the data itself was rendered quite challenging to read. (heavy text, few graphics)
it was also truncated in a somewhat misleading fashion.
if you read it closely, you’ll see that even the longest follow ups on infection data were lumped after 210 days, several were 180 (before it really gets bad) others were 120.
this is just typical bayesian datacrime and presentation bias as we’ve seen so many times before. and it does not really speak to the interesting issue of “are the vaccines preventing severity?”
this is, in fact, omitted from the study. but they did collect the data, they just made it REALLY difficult to find. you need to go HERE to the supplemental materials page. you then need to download the actual PDF as the data is not on the webpage. then you need to go to the very last page of that supplement.
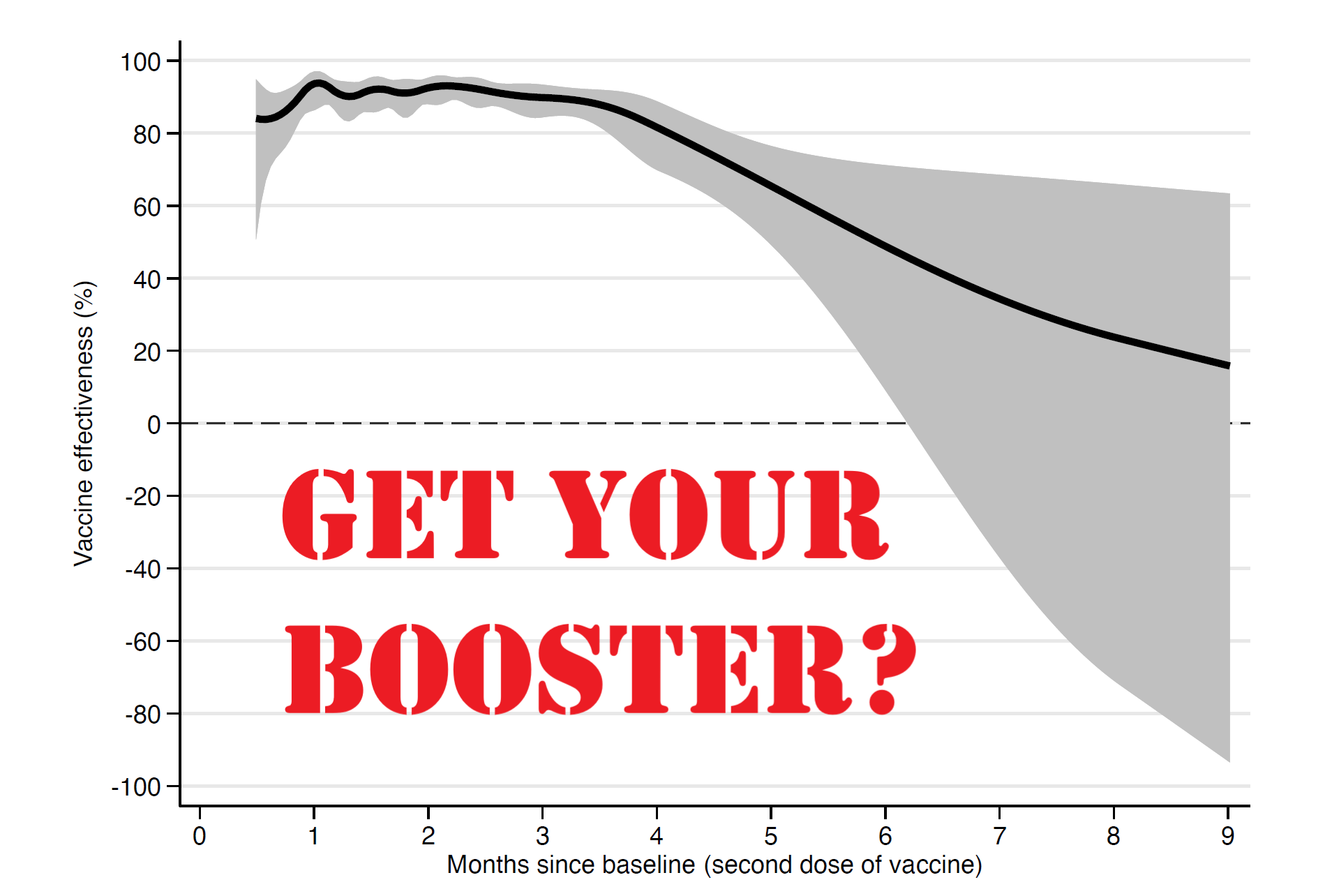
those who do so (and i’m guessing we’re down to a very few folks by then) will be rewarded with this graph:
and this one has profound and powerful implications.
it shows that efficacy against severe outcomes like hospitalization and death also wanes very rapidly
it shows that this efficacy keeps waning over time
it shows that it could easily be strongly negative based on the huge downside bias to the error range (gray shaded area)
and it shows that this data is of very low quality in terms of error magnitude.
at 9 months, midline expectation is ~15% reduction. (i’m eyeballing) but look at the confidence interval: it runs from (ballpark) +63% to -90%. that is not a useful range upon which to base anything. it implies that there is a very strong chance that vaccination is associated with greatly increased risk of severe outcomes for a great many people.
this pattern implies that boosters are likely, at best, a treadmill that will need constant refreshing, likely 3X a year or so, if you want to sustain efficacy. vaccine fade after 4 months degrades rapidly. (and frankly, the first 4 could well be an illusory halo generated by the dose 2 +14 vaccinated definition as linked above)
given the adverse events profile and the lack of severity of omicron this seems a truly odious proposition that looks likely to fail for most people on any sort or risk/benefit analysis. it is telling that the researchers here did not even attempt to take risk reward into account before claiming:
“The results strengthen the evidence-based rationale for administration of a third vaccine dose as a booster.”
what is also telling is the other part of the data required to make this claim:
do boosters work? do they refresh clinical immunity and mitigate severity? could they ever have done so and is this data even relevant with the emergence of omicron that seems to be at least an escape variant and far more likely a full blown hoskins effect/OAS variant that is enhanced, not mitigated by the vaccines.
note that all this data is from before oct 4th 2021, so it has no omicron impact whatsoever in it. claiming it bolsters the case for boosters without presenting evidence of booster efficacy on this new variant makes their claim feel like a rote bolt on, placed there to mollify and placate patrons and authorities.
there is absolutely no data here to validate that point.
the study does not even speak to the data that would be needed to make such a claim.
“efficacy wanes, so boost” is not a valid argument unless we know that boosters work, yet any evidence that boosters actually do anything to help is absent and all past data shows such rapid fade on efficacy vs severity as to make boosters a poor appearing proposition.
there is no data whatsoever on the new variant.
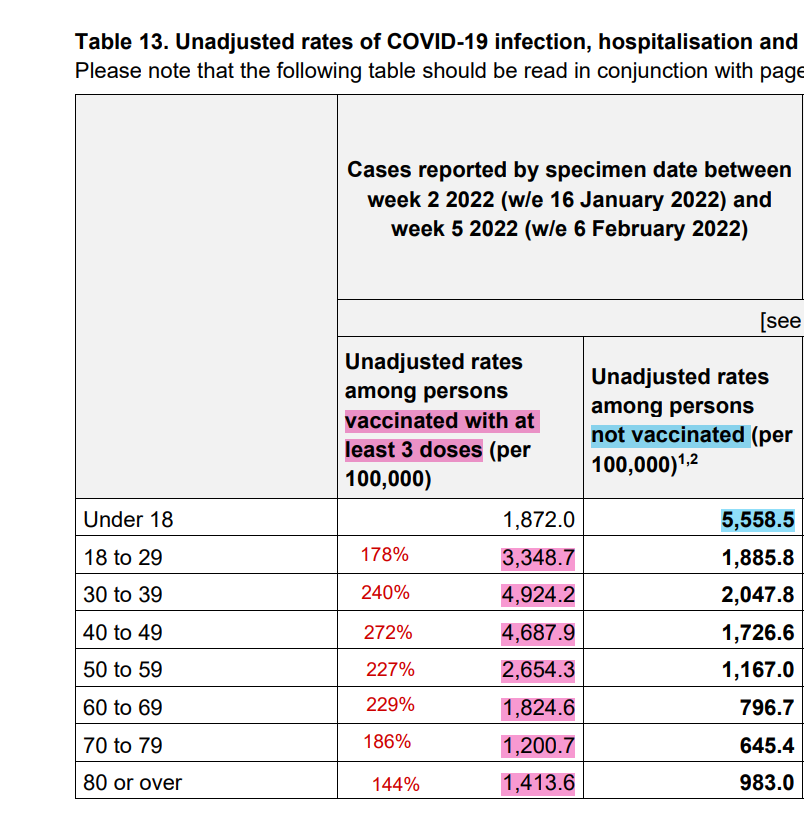
and boosters are sure not seeming to help in the UK. omi is driving rates of infection in the boosted at roughly double the rate of the unvaxxed.
the swedish study uses possibly irrelevant data and not only fails to prove out the ostensible interpretation, but winds up far more consistent with the conclusion that boosters are a waste of time and will provide ephemeral, at best, protection.
having seen this, go back and read the “interpretation” again.
now do you see my point about “the abstract says one thing while the data says another?”
i mean, they literally buried the lede at the very end of a hard to find supplement. it’s like putting the actual object of a video game inside of an easter egg.
most vexing, this easter egg also shows that vaccines may be making immunity to severe covid outcomes significantly worse.
call me mister suspicious, but i have a hunch that’s WHY they put it there.
let’s explore that a bit further:
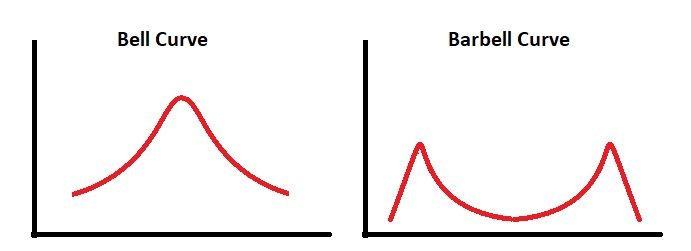
what would be REALLY interesting is to see how this population distribution looks.
if it barbells then we likely have a serious confound going on. we really have no idea what the prior incidence of covid was in those who got vaccinated. one could expect it to be quite meaningful.
if vaccines look like they are working well in some and are strongly negative in others with not much in the middle (this is suggested but not proven by the skew in the confidence interval) then i would posit that the most likely explanation is that what looks like VE is actually naturally acquired immunity.
but if you got vaxxed without having had covid, it could be acting as an immunosuppressant or driving hoskins effect/OAS antigenic fixation that makes you more vulnerable.
this, along with all cause deaths in vaxxed vs unvaxxed measured from the moment you got your first jab is some data i’d really like to see.
it’s continuing non-availability certainly frustrating and likely telling. this data absolutely exists.
why we are not getting to see it is fast becoming a question too big to ignore.
As with so many things that are happening at the moment, the attack on free speech is happening in multiple countries at the same time.
Firstly in the UK.
A draft Online Safety Bill was first presented to Parliament in May 2021 but has been strengthened in the last few weeks. Originally the draft Bill focussed on large web companies but the government has recently announced that more changes would be made and new criminal offences added.
One of these new offences would be spreading Covid-19 disinformation under a crime of sending a false communication. This offence would be committed if a person sends a communication they know to be false with the intention to cause non-trivial emotional, psychological or physical harm. The maximum sentence is 51 weeks.
The average person might think it is reasonable to imprison somebody for communicating something they know to be false with the intention to cause harm. However, what is “false” and what is “harm”? The last few years have shown us that these are now very subjective topics. Information that was true in 2019 became false in 2020 and is starting to be true again in 2022. A truth that is communicated to somebody who believes it to be false may cause them emotional or psychological harm. Intention is necessary for the crime to take place but if something is deemed to be false and deemed to cause harm then it could be argued that if the person who communicated the information, knew the information was on the “harmful list” then intention was there.
And who is deciding what information is false? The government? That almost sounds like a punchline to a joke. We’ll just end up with news articles such as the one below – Sponsored by the UK Government (see the text in blue).
The Bill was already censorial enough, making online companies remove content which was deemed to be harmful but not illegal. As we have seen in recent times, corporations’ misinformation policies have been arbitrary enough, which will only worsen with governments deciding what is true and what is false. Now, in a step one-removed from pre-crime, these companies will be made to proactively “prevent people being exposed in the first place”.
The government press release on the strengthening of this bill says that “to proactively tackle the priority offences, firms will need to make sure the features, functionalities and algorithms of their services are designed to prevent their users encountering them and minimise the length of time this content is available. This could be achieved by automated or human content moderation, banning illegal search terms, spotting suspicious users and having effective systems in place to prevent banned users opening new accounts”.
In almost Orwellian double-speak the press release says the Bill “will better protect people’s right to free expression online”. What this means is, it will better protect people’s free expression of government approved material. It continues by saying “it will have to be proven in court that a defendant sent a communication without any reasonable excuse and did so intending to cause serious distress or worse, with exemptions for communication which contributes to a matter of public interest”. So the government says something is a matter of public interest (e.g. vaccines) and suddenly intention doesn’t have to be proven.
Please sign this online petition to remove requirements that specifically target lawful speech from the Bill.
Next to the US.
At almost the same time, the US sent out a bulletin “Summary of Terrorism Threat to the U.S. Homeland”.
This states that “the United States remains in a heightened threat environment fueled by several factors, including an online environment filled with false or misleading narratives and conspiracy theories, and other forms of mis- dis- and mal-information (MDM) introduced and/or amplified by foreign and domestic threat actors. These threat actors seek to exacerbate societal friction to sow discord and undermine public trust in government institutions to encourage unrest, which could potentially inspire acts of violence”.
According to the bulletin, “the proliferation of false or misleading narratives, which sow discord or undermine public trust in U.S. government institutions” has “increased the volatility, unpredictability, and complexity of the threat environment”.
Key factors contributing to the current heightened threat environment include “widespread online proliferation of false or misleading narratives regarding unsubstantiated widespread election fraud and COVID-19”.
Furthermore, “as COVID-19 restrictions continue to decrease nationwide, increased access to commercial and government facilities and the rising number of mass gatherings could provide increased opportunities for individuals looking to commit acts of violence to do so, often with little or no warning. Meanwhile, COVID-19 mitigation measures—particularly COVID-19 vaccine and mask mandates—have been used by domestic violent extremists to justify violence since 2020 and could continue to inspire these extremists to target government, healthcare, and academic institutions that they associate with those measures”.
So in a step up from the UK’s response, the US is labelling individuals who produce any MDM as terrorists. Obviously, any language that incites violence is unacceptable but to confuse people encouraging unrest with those discussing whether Ivermectin could help save lives is completely unacceptable.
And finally in Canada.
Again, as if in lockstep, Justin Trudeau is trying to revive his controversial Internet legislation bill. Once known as Bill C-10, to fool those unintelligent Covid deniers, it has been changed to Bill C-11.
There are concerns that the legislation could be used to censor social media. The government have denied this but experts hold the opposite view. Who to believe, hmmm? The Toronto Sun reports that Trudeau is using the current national tensions as a smokescreen to let them slip in unpopular pieces of legislation. Never let a good crisis go to waste!
When we remove freedom of speech and censorship of controversial topics becomes common place, we turn into a dangerous society. Not only can authors be imprisoned for airing their views but, just as importantly, debate becomes restricted resulting in truths being hidden and novel and radical ideas supressed.
But if they can’t censor you, maybe they’ll just give you a morality pill so you don’t produce the stuff in the first place!
A Professor of Surgery at John Hopkins, Dr. Marty Makary, said that a research letter he helped author was censored by LinkedIn for violating the platform’s “Professional Community Policies.” The post was reinstated later “after a friend complained to the CEO.”
The censored post contained a link to a research letter published in the Journal of the American Medical Association (JAMA). The letter is a study Makary conducted about the “prevalence and Durability of SARS-CoV-2 Antibodies Among Unvaccinated US Adults.”
According to the screenshots Makary shared on Twitter, LinkedIn removed the letter “because it goes against Professional Community Policies.”
The policies prohibit users from sharing “false or misleading content.”
They also forbid users, including researchers and scientists, from posting “content that directly contradicts guidance from leading global health organizations and public health authorities.”
It is not clear how the study Makary posted violated any of LinkedIn policies.
All these tragedies have been due to failures of testing or failures in manufacturing processes. Most occurred before vaccine manufacturers were given virtually complete protection from liability in 1987. With the duration of patent exclusivity determining how much new products earn, products are rushed to market as quickly as possible, most using a shortened path for FDA review. Recalls and market removals of approved products are much more common than they used to be. We can only expect more of these disasters in the future, especially if the products are mandated for everyone.
1955: (Improperly inactivated) live polio vaccine caused polio in 40,000 children
The Cutter (now part of Bayer) Incident of 1955: This early US Salk polio vaccine contained live polio virus, which had not been inactivated. It caused 40,000 cases of polio; 200 of these recipients became paralyzed; and ten died. Other companies also had problems with viral inactivation. The NIH director lost his job in the aftermath, since NIH scientist Bernice Eddy had earlier warned this lot of vaccine paralyzed monkeys, but her findings were suppressed in the rush to vaccinate.
1970s-1985: Factor 8 Concentrate a pooled blood product used to prevent bleeding in hemophiliacs, was contaminated with HIV and Hepatitis C, but was sold worldwide even after manufacturers became aware of the contamination
Its manufacturers knew it was contaminated with HIV (and Hepatitis C), which spread through the injectable blood products used by hemophiliacs. About 8,000 US hemophiliacs at the time developed HIV infections this way, and an estimated 150,000 developed Hepatitis C, which frequently results in chronic liver disease, cirrhosis or death. The practice of distributing contaminated blood was widespread internationally, with many companies involved, and continued even after the problem was identified. It led to suits against pharmaceutical companies in a number of countries. It led to thousands of deaths. Doctors went to jail.
Cutter/ Bayer knowingly sold HIV-contaminated products in the US and overseas, seemingly having learned nothing from its polio-contaminated vaccine disaster 25 years earlier.
1976-1977: Swine flu vaccine given to 45 million Americans for a non-existent disease, causing hundreds of cases of paralysis
A new flu virus was discovered in a soldier who died at Fort Dix, NJ. Concern that the virus might cause a 1918-like influenza pandemic led to a huge federally-instigated program to develop a vaccine and vaccinate every American against the virus. But the epidemic never occurred. And the affected soldier, despite having an acute infection, had been on a rigorous march before he died. No one knew if the flu had killed him. US vaccine manufacturers agreed to produce vaccine on a short timeline, but only if they received a waiver of liability for possible vaccine injuries. The decision to use the vaccine was strongly influenced by political considerations, according to a National Academy of Sciences investigation of the program, commissioned by HEW Secretary Joe Califano. The report gives a bird’s eye view of how personal and political agendas came together to supercede considerations of the public health.
45 million Americans received the new vaccine, of whom 400 people developed autoimmune paralysis (Guillain-Barre syndrome) at a rate 6-8 times expected during the six weeks post-inoculation, and about 30 died.
This oral Rotashield vaccine was designed to prevent a mild form of gastroenteritis. However, it caused 1-2 cases per 10,000 recipients of intussusception of the bowel, and many affected babies required surgery to repair “telescoping” of the gut. Several died. Months after being licensed, the vaccine was taken off the market.
2009-10 Pandemrixswine flu vaccine caused over 1300 cases of narcolepsy in Europe
Children aged 5-19 were about 15 times more likely to develop narcolepsy if they received the GSK Pandemrix brand of swine flu vaccine, which was not sold in the US. Other age groups were also at an increased risk of narcolepsy, but to a lesser degree. Narcolepsy is caused by autoimmune destruction of cells in the brain’s Locus Ceruleus, and is newly recognized as a vaccine adverse reaction. The narcolepsy cases were severe, often preventing children from attending school.
** The adverse effect profile of drugs and vaccines is generally not well known until millions of people have received the drug or vaccine. New federal legislation (21st Century Cures Act of 2016 etc.) that speeds up licensing of vaccines, and removes liability from the manufacturers for all vaccines placed on the childhood schedule, all vaccines recommended by CDC for pregnant women, and new, potentially unlicensed products used during declared emergency situations — increases the potential risk of vaccines. http://www.fda.gov/RegulatoryInformation/Guidances/ucm125127.htm#categories
As the 13th anniversary of the crimes of September, 2001 approaches, the neoconservatives are shrieking from the rooftops – and effectively confessing that they were the real perpetrators of the 9/11-Anthrax false flag operation. (The neocons, you may recall, openly called for a “new Pearl Harbor” in September, 2000 – and got one exactly one year later.)
Every year at this time, the neocons orchestrate and hype a series of public relations stunts designed to magnify fears of “radical Islam” and reinforce their crumbling 9/11-Anthrax cover story. But this year’s propaganda campaign is so extreme that it represents a tacit confession: The neocons know that the truth about the 9/11-Anthrax operation is slowly closing in on them; so they are over-reacting by desperately trying to stoke the dying embers of the so-called War on Terror, in order to maintain the myth that Muslims (rather than neoconservative Zionists) attacked America in the autumn of 2001.
When a hysterical person exhibits guilty demeanor by trying too hard to blame a crime on someone else, that person is almost certainly the real perpetrator. As the neocons try much too hard to blame Islam for 9/11 and “terrorism” in general, their hysteria inadvertently reveals their own culpability. Like Shakespeare’s Lady MacBeth, the neoconservative movement has blood on its hands and “doth protest too much.” … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.

 The main applicant in the case is former Newfoundland Premier, The Honourable A. Brian Peckford. Mr. Peckford, pictured, is the only surviving drafter and signatory 40 years after the 1982 Constitution and the Charter of Rights and Freedoms was enacted.
The main applicant in the case is former Newfoundland Premier, The Honourable A. Brian Peckford. Mr. Peckford, pictured, is the only surviving drafter and signatory 40 years after the 1982 Constitution and the Charter of Rights and Freedoms was enacted.