Steve’s fact-based COVID-19 hub

By Steve Kirsch | February 2, 2022
Spotify made a press release about their new platform policies which prohibits any information which in their sole opinion may cause offline harm or poses a direct threat to public health. They refer people to their “fact-based” COVID-19 hub for accurate information.
I think their “fact-based” hub is filled with misinformation, so I decided to write my own simplified version that takes just a couple of minutes to read.
Here it is:
- Early treatments using repurposed drugs in a proven protocol are the best way to treat COVID. Treating as soon as symptoms appear is key. Fareed and Tyson have now treated over 10,000 people infected with COVID without any deaths as long as the people arrived early in the disease. The NIH and CDC ignore these treatments. I recommend you choose an early treatment protocol where there have been at least 10,000 COVID patients treated early without a single death (such as the Fareed-Tyson protocol), and start it as soon as you have symptoms.
- The evidence is clear that all of the current COVID vaccines available in the US today are both unsafe and ineffective. They are not suitable for anyone because they are more likely to kill you than to save you. If they don’t kill you, they may permanently damage your immune system or leave you permanently disabled. Avoid these at all costs. After 90 days, it appears that the vaccines have negative efficacy against Omicron, making you up to twice as likely to be infected. This is likely why case rates are so high in highly vaccinated countries. See Incriminating Evidence for details.
- Cloth and surgical masks do not work. There have been just two randomized trials with masks and COVID (Denmark and Bangladesh) and they proved that surgical and cloth masks have no effect. Similarly, N95 masks do not work in practice either. The FAA rules basically require you to wear these masks on planes, mandating a medical intervention that is much more likely to make you sick and has no chance to protect you. See Incriminating Evidence for details.
- If you require PPE that might protect you from COVID, consider a 3M respirator with a P100 filter. Even better is to use a PAPR with your respirator (with a P100 or P3 filter). See this article on masks and respirators for details. These products that protect you do not protect others. The FAA will not allow these devices on a plane.
- Social distancing is not the right way to think about risk reduction. Think instead the 4 D’s: draft, distance, density, duration. Putting yourself in an unventilated small room at close distance to a source for a long duration will maximize your exposure. The 6 foot rule for standing in line is nonsensical since as soon as you enter the airspace of the person in front of you, you will be breathing the virus from people who were standing in that spot hours (to days) ago (depending on the ventilation in the area). There is absolutely nothing magical about 6 feet.
- Mitigation strategies such as testing, masking, isolation, and vaccination are largely ineffective. See this article for a convincing example.
- The best way to treat COVID is to do the opposite of what the CDC and FDA advises. So when they tell you to mask up, get boosted, avoid all repurposed drugs and supplements (including ivermectin, HCQ, fluvoxamine, vitamin D, zinc, aspirin, budesonide, etc), take paxlovid, molnupiravir, and remdesivir, you know what to do.
- There is only significant spread if you have symptoms. For example, in a study in China, they looked at 1,174 close contacts of these asymptomatic individuals and could not find ONE CASE of a person getting COVID from the asymptomatic people. Therefore, testing asymptomatic people is unnecessary because it is a lot of effort for near 0 gain.
- Omicron is very mild compared to Delta. After you recover from an Omicron infection, data shows you will be protected from Delta as well.
- As of December 3, 2021, Omicron had spread to 38 countries, but the WHO couldn’t find anyone who died from Omicron. How is this a national emergency?
- People who get the virus and recover are always better off than a vaccinated patient. Unlike vaccinated people, if a naturally infected patient is ever re-infected, they cannot transmit the virus to others (as far as we know so far).
- Censorship of COVID advice by social media (in particular the hazards of the vaccines and the effectiveness of early treatment protocols) has cost hundreds of thousands of lives.
- None of the health authorities issuing mandates and directives are willing to participate in a recorded scientific discussion with the so-called “misinformation spreaders” such as Robert Malone, Peter McCullough, Robert Kennedy, … Our authorities are afraid of the truth.
- The CDC, FDA, and NIH are all corrupt agencies that have looked the other way at safety signals. There are over 1M adverse events in VAERS and these represent over 40M adverse events in the real world. This is unprecedented, yet the CDC isn’t able to find a safety signal other than a “slightly elevated” risk of myocarditis. Attempts to bring the VAERS data to their attention is futile. They won’t even do a proper calculation of the underreporting factor which is required to do a proper risk-benefit analysis. They ignore the DMED data entirely.
Compare my fact-based COVID-19 hub to Spotify’s and let me know which one you like better.
Former Pfizer VP Michael Yeadon demands apology from media over ‘lies’ asserting vaccine safety

Dr Michael Yeadon, former Pfizer vice president and co-founder of Doctors for COVID-19 Ethics
By Patrick Delaney | LifeSiteNews | February 2, 2022
After being excoriated by mainstream media outlets regarding his concern that COVID-19 gene-based vaccines could cause fertility issues in young women, Dr. Michael Yeadon is now requesting contrition on the part of media outlets as leaked data from the U.S. military indicates heavy spikes in these tragic outcomes.
“I’m not vindictive, but I want some humility and contrition from the BBC and all other media outlets that lied to their audiences,” said the former Pfizer vice president and Chief Scientist for allergy and respiratory.
Yeadon, who spent 32 years in the industry leading new medicines research and retired from the pharmaceutical giant with the most senior research position in his field, was an author of a submitted petition to the European Medicines Agency (EMA) in December 2020 that raised substantial concerns regarding a lack of sufficient testing of the experimental COVID-19 gene-based vaccines, prior to their emergency use authorizations.
With regard to the possibility of the shots endangering the fertility of women, Yeadon and his colleague, Dr. Wolfgang Wodarg, wrote, “There is no indication whether antibodies against spike proteins of SARS viruses would also act like anti-Syncytin-1 antibodies. However, if this were to be the case this would then also prevent the formation of a placenta which would result in vaccinated women essentially becoming infertile.”
Such a possibility would need to be ruled out through standard experimentation prior to imposing such substances onto the entire population, according to the doctors.
“It’s important to note that none of these gene-based agents had completed what’s called ‘reproductive toxicology,’” Yeadon wrote in his recent statement. “Over a year later, this battery of tests in animals still has not been done. So there was and still is no data package supporting safety in pregnancy or prior to conception.”
Media response to valid concerns: attacks, smears, vilifications
“As a society, we’ve practiced the precautionary principle most assiduously in relation to conception and pregnancy ever since the tragedy of thalidomide, over 60 years ago. So we had hoped that some at least in the media would take this [concern] with the seriousness it deserved,” he wrote.
“Did that happen? No. Instead, we were attacked, smeared and vilified in every medium, from Twitter to the BBC,” the British national wrote. “[M]ajor broadcasters actively lied to the public, explicitly stating that these agents were completely safe in pregnancy.”
Indeed, Reuters excoriated the doctors for making their inquiry “without providing evidence, that the vaccines could cause infertility in women,” shifting the burden of proof onto the petitioners from the regulators whose job it is to ensure proper safety trials are completed before the release of such drugs.
The article quoted an anonymous spokesman for Britain’s Department of Health & Social Care, saying, “These claims are false, dangerous and deeply irresponsible.”
Reuters later attempted to “fact-check” Yeadon as well over several concerns including the danger to fertility, to which he simply reiterated common ethical principles with regard to human experimentation: “No one in their right mind thinks giving experimental treatments to pregnant women is other than reckless. Especially when reproductive toxicity testing is incomplete.”
Of special note for Yeadon was BBC Radio talk show hostess Emma Barnett, who “directly attacked me by name on air in the most unpleasant terms,” which also led to his charging the program with slander. In response, after a bit of investigation, the program editor conceded, apologized to Yeadon, and cut their false representation of the former Pfizer scientist from their recorded podcast.
“[Barnett] also had her guest, who was from the Royal College of Obstetrics and Gynecology, repeat the lies that it was perfectly safe for young women to be injected,” Yeadon called out in his statement.
Preprint paper reveals placental-damaging antibodies increased 2.5 fold after shots
Also of note for the former executive was a preprint study published last May that appeared to attempt a rebuttal of his concern that anti-Syncytin-1 antibodies could be developed due to the shots, but instead reinforced them showing a 2.5 fold increase of the placental-damaging antibodies in days 1 to 4 after COVID-19 gene-therapy injections.
The paper, which claimed a conflict of interest in being funded by Johnson & Johnson, went on to explain that though they had observed this major increase, they did not examine its “clinical significance,” thus admitting they didn’t know if these higher levels of the antibody flagged an actual safety problem with regards to fertility and miscarriage.
At the same time, the study’s authors acknowledged data showing “spontaneous miscarriage as the most common obstetric outcome after COVID-19 mRNA vaccination.”
Based on the outcome of this study alone, Yeadon said “all of these experimental products as a class should have been completely contraindicated in women younger than menopause.”
Pfizer & Moderna ‘definitely knew’ these mRNA products would ‘accumulate in the ovaries’
An additional source of concern regarding fertility was that “the mRNA products (Pfizer and Moderna) would accumulate in ovaries,” the British national explained.
“An FOI request to the Japanese Medicines Agency revealed that product accumulation in ovaries occurred in experiments in rodents. I searched the literature based on these specific concerns and found a 2012 review [here], explicitly drawing attention to the evidence that the lipid nanoparticle formulations as a class do, in fact, accumulate in ovaries and may represent an unappreciated reproductive risk to humans. This was ‘a well-known problem’ to experts in that field,” Yeadon explained.
“I’ll say that again. The pharmaceutical industry definitely knew, in 2012, that formulating these agents in lipid nanoparticles would lead them to accumulate in the ovaries of women to whom these were given.
“No one in the industry or in leading media could claim ‘they didn’t know about these risks to successful pregnancy,’” he emphasized.
Results from the U.S. military leak confirm damage done to unborn children and fertility
“So it’s with tremendous anger and sorrow that I heard of military physicians blowing the whistle about the evidence of harms in pregnancy that their proprietary safety monitoring database had thrown out,” Yeadon said, referring to last week’s revelations during a U.S. Senate panel discussion.
“In the intervening months since journalists (including but definitely not limited to Emma Barnett) chose to downplay or downright lie about our concerns, we learned that women in the U.S. military were experiencing 3X normal rates of miscarriage,” he explained.
In fact, these data leaks, given by three “decorated high-ranking soldiers who are doctors and public health officials,” in sworn declarations under penalty of perjury, show several increases in negative impacts upon fertility, including spontaneous abortion, among this military population where enforcement of an experimental COVID gene-vaccine mandate is strictly observed.
As presented by these soldiers, the following 2021 increases only include the first 10 months of the year (January through October) and are compared with the full five-year average of figures taken from 2016 through 2020.
- Miscarriages — increase of 279%
- Female infertility – increase of 471%
- Male infertility — increase of 344%
- Congenital malformations (birth defects) – increase of 156%
And considering most children conceived after these injections had not been born before November 2021, the final figure of birth defects is likely to significantly increase as well.
Journalists, regulators and manufacturers: ‘You are way out over thin ice and deep water’
After Yeadon’s request for contrition from the BBC and other media outlets, he went on to implore readers, “please do not get injected with these inherently dangerous and ineffective experimental products. Warn anyone you know about the risks to pregnancy, now confirmed by whistleblowers from physicians in the U.S. military.
“Please also tell them there are likely to be other reproductive health consequences, even in young girls, because of accumulation [of lipid nanoparticles] in their ovaries.“
Having originally alerted the EMA of several other possible toxic outcomes due to the injections, Yeadon highlighted that he and Dr. Wodarg were sadly also right about their warning of “allergic, potentially fatal reactions to the vaccination,” citing examples from the UK of emergency interventions and tragic deaths.
“Having had two of two serious harms we warned about, prior to regulatory authorisations, come to pass,” he said. “I humbly recommend that governments and journalists everywhere recognise what you’ve done and lobby for or directly decide to immediately and completely withdraw all these experimental products from the market, before some of the other specified concerns (or issues we didn’t think of) show up in the safety monitoring systems.”
“Journalists, regulators, healthcare professionals and politicians, as well [as], of course, the manufacturers, you are way out over thin ice and deep water. I don’t know how you’re planning to get out from under this before the wider public more fully appreciates what you’ve done,” Yeadon wrote.
“One possibility is that you won’t be able to hide your complicity in the massed harms you’ve done to millions of people. In this case, I look forward to giving evidence against you in a court of law,” he concluded.
Dr. Yeadon’s full statement can be accessed here.
These 5 Studies Reveal a Disturbing Trend — Researchers Presenting Conclusions That Don’t Match the Data
By Josh Mitteldorf, Ph.D. and Madhava Setty, M.D. | The Defender | February 2, 2022
It was January 2020, the very beginning of COVID, when news articles began appearing that connected the genetics of the virus with gain-of-function research on bat coronaviruses at the Wuhan Institute of Virology.
These speculations were put to rest by an authoritative statement in the prestigious journal Nature Medicine, echoed by a summary in Science and an unusual affidavit in the Lancet signed by an impressive list of prominent scientists.
The message in the Nature Medicine article was dispositive: “Our analyses clearly show that SARS-CoV-2 is not a laboratory construct or a purposefully manipulated virus.”
But where was the support for this confident conclusion in the article itself?
The 2,200-word article in Nature Medicine (Anderson, et al) contained a lot of natural history and sociological speculation, but only one tepid argument against laboratory origin: that the virus’s spike protein was not a perfect fit to the human ACE-2 receptor.
The authors expressed confidence that any genetic engineers would certainly have computer-optimized the virus in this regard, and since the virus was not so optimized, it could not have come from a laboratory. That was the full content of their argument.
Most readers, even most scientists, take in the executive summary of an article and do not wade through the technical details. But for careful readers of the article, there was a stark disconnect between the Cliff Notes and the novel, between the article’s succinct (and specious) conclusion and its detailed scientific content.
This was the beginning of a new practice in the write-up of medical research. Recent revelations in the Fauci/Collins emails shed light on the origins of this tactic and the motives behind it.
In the past, if a company wanted, for example, to make a drug look more effective than it really was, it would choose a statistical technique that masked its downside, or it would tamper with the data.
What companies would not do, in the past, was describe the results of a statistical analysis that proves X is false, then publish it with an Abstract that claims X is true.
But this strange practice has become more common in the last two years. Academic papers are being published in which the abstract, the discussion section and even the title flatly contradict the content within.
Why is this happening? There are at least three possibilities:
- The authors cannot understand their own data.
- The authors are being impelled by the editorial staff to arrive at conclusions that match the ascendant narrative.
- The authors and editors realize the only way to get their results into publication is to avoid a censorship net that gets activated by any statement critical of vaccination efficacy or safety.
Before reaching any conclusions, let’s take a closer look at some examples of this troubling phenomenon arising in what should be the foundation of what is known: published scientific data.
In this article, we present five different published studies. Each to varying degrees exemplifies a disconnect between the data and the conclusions.
Example 1: ‘Phase I Study of High-Dose L-Methylfolate in updates Combination with Temozolomide and Bevacizumab in Recurrent IDH Wild-Type High-Grade Glioma’
This example is unrelated to the pandemic, but it typifies a common practice in the pharma-dominated world of medical research. If a remedy is cheap and out of patent, there is no one motivated to study its efficacy.
But research practice has gone well beyond neglect. In fact, investigators are skewing statistics to make cheap, effective treatments look ineffective if they are in competition with expensive pharma products.
This is ridiculously easy to do — all it requires is incompetence. Using the wrong statistical test, using a weak test when a stronger one applies — or just about any mistake in parsing the data — is far more likely to make compelling data appear random than the opposite.
Is it always incompetence? Or is it more often a well-thought-out deception that uses seemingly erudite analysis to lead the undiscerning reader into believing the wrong conclusion?
In the case of this article, a simple B vitamin (L-Methylfolate) was shown to double the life expectancy of 6 out of 14 brain cancer patients who received it, while showing no benefit (and no harm) to the other half of the patients.

The purple jagged line extending out to the right represents 40% of patients who lived dramatically longer when treated with L-Methylfolate (LMF).
The abstract reports that “LMF-treated patients had median overall survival of 9.5 months [95% confidence interval (CI), 9.1–35.4] comparable with bevacizumab historical control 8.6 months (95% CI, 6.8–10.8).”
The increase in median survival time is just a few months and not statistically significant. But the average survival time of the folate-treated group was more than double, and the difference was statistically significant (by my calculation, not in the article).
But the average is what is more commonly reported, and most readers don’t understand the difference between average and median.
The longest surviving patient on the B vitamin was still alive at the end of the study (3.5 years) when every one of the patients treated only with traditional chemo was dead before 1.5 years.
There were three different dosages in the study, (30, 60, 90 mg) and it was not reported whether the longest-living patients were receiving the highest dosages.
This is, in fact, a hugely promising pilot study about treating a common, fatal cancer with a simple vitamin. If it were an expensive chemotherapy drug instead of a cheap vitamin, you can be sure it would have been hailed as a breakthrough.
But this study will not create much excitement, and few oncologists will even know to prescribe methylfolate for their glioma patients.
Example 2: ‘Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons’
Earlier this year, MacLeod et al used data from a prominent Centers for Disease Control and Prevention (CDC) study to calculate that for women in their first trimester, the rate of miscarriage following administration of an mRNA COVID vaccine was an alarming 82%.
On Jan. 7, the CDC released a report designed to dispel our misgivings about vaccinating pregnant women. Its conclusions were unequivocal:
“These data support the safety of COVID-19 vaccination during pregnancy. CDC recommends COVID-19 vaccination for women who are pregnant, recently pregnant, who are trying to become pregnant now, or who might become pregnant in the future.”
The Defender reported on the numerous flaws in this study. The most egregious deficiency was the dearth of pregnant women in the study who were vaccinated early in their pregnancy (less than 2%).
The authors admit their study could not quantify the risk of vaccine exposure in the first trimester: “First trimester vaccinations are not included in analyses stratified by trimester because few exposures occurred…”
How then can they recommend COVID vaccination for women who are “recently pregnant” if their analyses excluded women in their first trimester?
This report serves a purpose. People who read it superficially will find the reported results reassuring — including front-line doctors who don’t have time to evaluate the research critically.
The CDC chose to paint over troubling safety concerns with reassuring words that are unsupported by clear science.
Example 3: ‘Public Health Scotland COVID-19 & Winter Statistical Report’
There is a section of this report comparing vaccinated and unvaccinated rates of disease, preceded by a warning to the reader not to take the data at face value.
“PLEASE READ BEFORE REVIEWING THE FOLLOWING TABLES AND FIGURES There is a large risk of misinterpretation of the data presented in this section due to the complexities of vaccination data …”
The data the authors don’t want us to misinterpret say that people who have been vaccinated with one shot or three shots are 50% more likely to contract COVID-19 compared to people who are unvaccinated.
People who receive two shots are more than twice as likely to contract COVID-19. This is according to the authors’ own method of calculating age-standardized disease rates.

The authors emphasize it’s not about case numbers — it’s about severe outcomes, hospitalizations and deaths:
“Evidence suggests the COVID-19 vaccines are 90% effective at preventing a severe outcome of COVID-19. COVID-19 hospitalizations and deaths are strongly driven by older age, with most deaths occurring in those over 70 years old and having multiple other illnesses. But overall, you are less likely to be hospitalized if you are vaccinated with a booster.”
What data are they talking about? Here are results from their own data table:
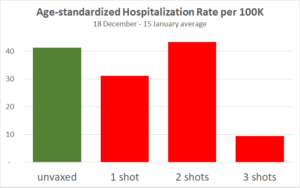
The only substantial reduction is from people who received the third shot, which has only recently been available in Scotland. But for the three-shot cohort only, vaccination effectiveness is declining over the four weeks.
This adds to previous evidence that protection from the vaccine is short-lived, and each injection provides a shorter window of protection than the previous one. Also, note the hospitalization statistics may have been gamed.
Since the publication of this article, England but not Scotland has backed off requirements for vaccination IDs.
Example 4: ‘Clinically Suspected Myocarditis Temporally Related to COVID-19 Vaccination in Adolescents and Young Adults’
Myocarditis, or inflammation of the heart, is a severe and life-shortening disease. It is virtually unknown in young people, but it is a recognized side effect of the COVID vaccines, especially in boys and young men.
This article summarizes the experience of 139 young patients (ages 12 to 20) who were hospitalized for myocarditis following vaccination.
19% of them were taken into intensive care.
Two required infusions of pressors and inotropes (potent intravenous drugs used to raise critically low blood pressure).
Every patient had an elevated Troponin I level. Troponin is an enzyme specific to cardiac myocytes. Levels above 0.4 ng/ml are strongly suggestive of heart damage. These young patients had a median Troponin I level of 8.12 ng/ml — over 20 times greater than the levels found in people suffering heart attacks.
“Conclusions: Most cases of suspected COVID-19 vaccine myocarditis occurring in persons <21 years have a mild clinical course with rapid resolution of symptoms.”
“Mild clinical course” — We suppose this refers to the 81% who did not go to the ICU or the fact that none died or required ECMO (Extracorporeal Membrane Oxygenation, a desperate means to keep the body oxygenated when a patient’s heart or lungs have completely failed).
In any case, every single person in this study was hospitalized. When does a “mild clinical course” require hospitalization for a two-day median length of stay?
“Rapid resolution of symptoms” — How would anyone know this? Myocarditis in older patients doubles the probability of death for the long term.
We don’t know what it will do to young boys in the long term, especially since every patient had some damage to their heart as evidenced by significantly abnormal troponin levels. And we don’t fully understand the mechanism by which the vaccines cause myocarditis.
Example 5: ‘Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States’
This is the title of a paper by two statisticians from the Harvard School of Public Health, published on Sept. 30, 2021, in the European Journal of Epidemiology.
The title makes the important claim that there is no public health benefit from vaccination. COVID-19 is spreading at the same rate in different populations, unrelated to whether the population is mostly vaccinated or mostly unvaccinated.
It’s a powerful counterpoint to the ubiquitous demand that more people should undergo vaccination for the sake of their community.
The paper completely undermines the requirement of vaccination to attend meetings, concerts, theater and other public gatherings. It says there is no legitimacy to the creeping government vaccine mandates for travel.

But the data in the paper don’t show that vaccination and spread of COVID-19 are “unrelated.” In fact, there is a paradoxical relationship, an insidious relationship: The more vaccinated countries had more new COVID-19 cases (during the week when the survey was conducted). The correlation is significant (p=0.04).
Still, the authors conclude by explicitly recommending propagandizing of the unvaccinated: “In summary, even as efforts should be made to encourage populations to get vaccinated it should be done so with humility and respect.”
It may sometimes be wrong to promote flawed health policy, but apparently, it’s a good thing, so long as it is done with humility and respect.
Why would these researchers take the trouble to publish data that is so damning to the vaccine narrative, and then pull punches in the title and in the conclusions?
Are we to assume that these authors who have assiduously extracted data from 68 different countries and nearly 3,000 U.S. counties were unable to notice their meticulous scatter plot unequivocally demonstrates high vaccination uptake is associated with higher (NOT lower) prevalence of COVID-19?
This seems to be a different case from the first example, where shills for the pharmaceutical industry set out to create a deceptive narrative. We think it’s probable that in this case, soft-pedaling the implications of these glaring data may not have been the authors’ choice, but rather a decision by the journal’s editors.
We know from personal experience how difficult it is to get an article through peer review at most “reputable” medical journals when the results are out of sync with the COVID narrative.
It may well be that these authors fought hard to get their subversive message into print, and in order to get past peer review, they softened the language, especially, the title.
Conclusions
The church was once the most trusted institution in Europe. Then the bishops started selling indulgences — a kind of get-out-of-hell-free pass for rich sinners.
Today the most trusted institution is science.

Sources: Gallup, Gallup, Gallup, Pew
This is true despite the fact that scientists are human, subject to error and to corruption.
Medical journals have become financially dependent on their advertisers, which are almost exclusively the pharmaceutical giants.
For several decades now, the “Church of Science” has been selling indulgences. With enough money, you could buy a scientific study that says what you want it to say.
Darell Huff’s book, “How to Lie with Statistics,” first published in 1954, remains the all-time best-seller in its field.
Recently, Gerald Posner documented the way in which the pharmaceutical industry has used its profits to affect science at every level, from medical researchers to journal editors to government regulatory agencies to the journalists who interpret science for the public.
Pressure is being placed on independent researchers by the journal editors and peer reviewers, many of whom have ties to Big Pharma. Valid studies, honestly reported, can be rejected for publication if they send a message that threatens corporate profits.
In the age of COVID, we see three reasons that an article’s conclusions might become detached from its statistical findings:
- Scientists have suddenly abandoned basic logic and reason. This is an implausible explanation because, as has been demonstrated above, these examples demonstrate diligence in gathering data. There is no reason why they would abandon diligence in arriving at reasonable conclusions.
- Shortcuts by pharmaceutical companies and their shills in academia. Rigging clinical trials the old-fashioned way is expensive and time-consuming. It’s also uncertain. Sometimes the truth rears its head even if a study is designed to conceal it. Even a study that is designed to fail might succeed when the inconvenient truths are sufficiently stubborn. How much easier it is to report the results and then tack on an abstract and a discussion section that say what you want to say, regardless of the data tables in the body of the article!
- Scientist authors are well aware of the pernicious censorship in scientific publication that has emerged in recent days. This is perhaps the most intriguing possibility. If researchers behind the study have some prestige and some influence, they still may find they have to soften their rhetoric in order to pass peer review. However, what we are witnessing today is more than a tendency to be “diplomatic” in their choice of words. What does it mean when their conclusions do not match the findings? Are they trying to tell us that they are gagged? Are they silently screaming at us to look at the data and not their interpretation of them?
The Nature Medicine article on the origins of the SARS-CoV-2 virus (reviewed first) seems to be an example of researcher corruption.
The article in the European Journal of Epidemiology (Example 5), which relates vaccination rates to COVID prevalence, is more likely an example of corruption by journal editors and peer reviewers.
In this instance, the data and conclusions are so disparate that it begs us to reconsider the cynical position that all scientists have been corrupted. Is there a better way for conscientious scientists to signal their community that they are being censored than by compiling solid data that tell a compelling story and then arriving at a nonsensical conclusion? Are they imploring us to read between the lines?
For the other four articles reviewed above, we leave it to your judgment — how do you think the conclusions came to be so disconnected from the statistical findings in these same articles?
Obviously, this blatant distortion of scientific write-ups is not a long-range strategy, but the world is moving fast, and people who count on their ability to shape scientific conclusions to their financial interests will be successful for long enough to do a great deal of mischief.
What will be the damage to the credibility of science when the dust clears?
Josh Mitteldorf, Ph.D., has a background in theoretical physics. Since the 1990s, he is best known for his contributions to the biology of aging, including many articles and two books.
Madhava Setty, M.D. is senior science editor for The Defender.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
The Race Is On for an Omicron Jab
By Dr. Joseph Mercola | February 1, 2022
At this stage in the game, it’s apparent that the COVID jab no longer works. Many health officials and world leaders are even openly acknowledging that the COVID shots cannot end the pandemic and that we must learn to live with the virus.
A major driver for this U-turn in the pandemic narrative is the emergence of the Omicron variant which, by mid-January 2022, accounted for 99.5% of all COVID cases in the U.S.1
The infection, which is far milder than previous ones, is ripping through populations, leaving natural herd immunity in its wake. Despite that, vaccine makers are still hard at work to produce an Omicron-specific injection.2 Pfizer has promised to have one ready by March 2022.3
The question is why, seeing how by the time the shot is released, just about everybody will have been exposed. If natural herd immunity is already maxed out, what good could a “vaccine” possibly do?
‘Everyone’ Will Have Natural Immunity
As Dr. William Moss, executive director of the International Vaccine Access Center at the Johns Hopkins Bloomberg School of Public Health told CNBC,4 “An omicron-targeted vaccine was needed in December [2021]. It still could be valuable but I do think in many ways, it’s too late.”
Dr. Shaun Truelove, an infectious disease epidemiologist at Johns Hopkins Bloomberg School of Public Health and a member of a team of researchers who make COVID projections, agreed, saying, “Given how quickly this [variant] is happening, [the targeted vaccine] may not matter because everybody’s going to be infected.”5 Pfizer CEO Albert Bourla even admits he doesn’t know “whether or not the new vaccine is needed or how it could be used,” CNBC reports.
January 25, 2022, Pfizer and Moderna announced they’ve started enrolling adults, 18 to 55, for trials on an Omicron-specific jab in the U.S. and South Africa.6 Pfizer will evaluate safety, tolerability and immune response in 1,420 volunteers,7 some of whom will have received two doses while others will have received three already. A third cohort will be unvaccinated (although one wonders where they’ll get those from).
Moderna has also joined the pointless race to produce an Omicron booster,8 although it’s doubtful they’ll be able to produce one any faster than Pfizer.
Moderna CEO Stéphane Bancel told CNBC that a fourth COVID jab also may be on the horizon, “as the efficacy of boosters will likely decline over time.”9 It’s unclear what strain that fourth shot would target.
Israel Proves Failure of COVID Boosters
For a preview of what’s in store after third and fourth booster shots, all we have to do is look at Israel, where more than 250,000 fourth doses had already been given by early January 2022. According to CNBC:10
“Early data from Israel shows that a fourth dose does increase antibody levels, says Dr. David Hirschwerk, infectious disease specialist and medical director at Northwell Health’s North Shore University Hospital.”
What CNBC neglects to note is that, after the rollout of a fourth dose, Israel now has the highest COVID case rate per capita of any country in the world since the beginning of the pandemic.
Looking at a Reuters graph11 of Israel’s seven-day average case rate, something absolutely abnormal appears to have happened in mid-January 2022, as the line shoots straight upward, hitting an all-time high of 75,603 new infections per day on January 24, 2022.
This, despite 74% of the population having received at least one dose, 67% having received two doses, and 56% having received at least one booster, as of January 25, 2022.12
What Does It Mean To Be ‘Fully Vaxxed’?
While the pandemic narrative has recently shifted, and rather dramatically, with some leaders openly speaking out against boosters without getting canceled or censored, it seems clear that we’re not out of the woods yet when it comes to COVID shots.
Vaccine makers clearly aim to make the COVID shot, at bare minimum, an annual injection.13 In the meantime, the definition of what it means to be “fully vaccinated” against COVID keeps shifting. At the beginning of 2021, many people undoubtedly got their primary series (two shots of Pfizer or Moderna, or a single jab in the case of AstraZeneca and Janssen) thinking life would be easier that way.
Being “fully vaccinated,” they wouldn’t be inconvenienced by vaccine passport restrictions and mandates. Well, that fantasy only lasted a few months. Now, those who got the first required series find themselves in the unwelcome position of being among the “unvaccinated” again unless they submit to a third jab.
As explained by U.S. Centers for Disease Control and Prevention director Dr. Rochelle Walensky during a recent press briefing:14
“What we’re really working to do is pivot the language to make sure everyone is up to date with their COVID-19 vaccines as they personally could be, should be, based on when they got their last vaccine. If you’ve recently gotten your second dose but you’re not eligible for a booster, you’re up-to-date. If you’re eligible for a booster and you haven’t gotten it, you’re not up-to-date and you need to get your booster.”
It’s only a matter of time before those with three jabs will be “unvaccinated” unless they submit to a fourth, and so on, ad nauseum. An as-yet unanswered question is how many mRNA injections can a person survive?
Considering the injection causes your body to produce toxic spike protein in uncontrolled amounts, it seems reasonable to assume there’s a tolerance limit, although that limit may vary from person to person. There’s really no telling how many people are one shot away from a crippling side effect or sudden death.
Each Shot Degrades Your Immune System
As reported by The Exposé,15 January 22, 2022, government data from around the world suggest people who have received at least two shots are now showing signs of serious immune system degradation.
According to that report, data from Australia, the U.S., Canada, Scotland and England clearly show “that their vaccinated populations immune system capability has been decimated when compared to the not-vaccinated population.” For starters, Omicron cases are rising far more rapidly and readily among the fully jabbed and boosted than among the unvaxxed.
In Australia, the fully jabbed are 2.2 times more likely to catch COVID than the unvaccinated. “So, the vaccine passports holders are 2.2x more likely to spread COVID than the unvaxxed who are denied vaccine passports and locked up in detention centers,” The Exposé dryly notes.
Several studies have also shown the effectiveness of the jab wanes incredibly rapidly. And, disturbingly, it doesn’t peter out at zero. Immunity goes negative, meaning the fully vaxxed and boosted rapidly become MORE prone to COVID infection than they ever were before.
Negative Effectiveness Rates Found in Many Countries
In the U.S., a study16 on 780,225 U.S. veterans found the effectiveness of the jab dropped precipitously over six months:
- Janssen dropped from 86.4% effectiveness at the outset to 13.1% in the sixth month
- Moderna dropped from 89.2% to 58%
- Pfizer dropped from 86.9% to 43.3%
A Canadian study17 found vaccine effectiveness started declining sharply within as little as the second week after the second jab. By the sixth month after the second jab, the blood of 70% of nursing home residents had “very poor ability to neutralize the coronavirus infection in laboratory experiments.”
In the U.K., government data “show a clear linear fall-off in vaccine efficiency at an average rate of 4.8% per week for the over 18s,” The Exposé reports,18 and by the time you get past Week 9 after jab No. 2, effectiveness starts going negative.
“Doubly vaxxed (unboosted) people in the U.K. have now (as of January 2022) run right out of immune system efficiency against both Delta and Omicron when compared to unvaccinated people,” The Exposé writes. The question is whether or not there might be a point at which the immune system stops deteriorating. As of now, we don’t know.
Using data from five UK HSA COVID-19 Vaccine Surveillance Reports, The Exposé created the following graph, illustrating “the overall immune system performance among all age groups in England over the past five months.”

The Exposé explains:19
“What we can see from the above is that the immune system performance for adults aged between 18 and 59 has deteriorated to the worst levels yet since they were given the COVID-19 vaccine.
Whilst the immune system performance of everyone over the age of 60 has deteriorated dramatically following receipt of the booster shot, but not yet to the level seen between week 37 and week 40. The over 70’s have however seen the most dramatic fall in immune system performance between month 4 and month 5 alongside 18-29-year-olds.
The 55% boost to the immune systems of the over 80’s given by the boosters between month 3 and month 4 has all but deteriorated between month 4 and month 5. Their immune system is performing 1% better than it was in month 3 but still 54% worse than their unvaccinated counterparts.
The 73% boost to the immune systems of the 70-79-year-olds given by the boosters between month 3 and month 4 has also all but deteriorated between month 4 and month 5. Their immune system is performing 10% better than it was in month 3 but still 63% worse than their unvaccinated counterparts.
The minor boost however, given to the immune systems of everyone between the age of 30 and 59 by the boosters between month 3 and 4 has been completely decimated by the following month, whilst 18-29-year-olds have seen a 60% decline in their immune system performance between months 4 and 5.”
Are Double- and Triple-Jabbed People at Risk for VAIDS?
By now you may be wondering whether this negative effectiveness could be indicative of something far worse than just being more prone to Omicron infection. The Exposé20 believes the double- and triple-jabbed may actually have vaccine-acquired immunodeficiency syndrome or VAIDS, similar to AIDS.
While I think it’s still too early to come to a definitive conclusion, former Pfizer vice president Michael Yeadon has made a similar statement.21 In a December 6, 2021, article on americasfrontlinedoctors.org, Yeadon is quoted saying:22
“If immune erosion occurs after two doses and just a few months, how can we exclude the possibility that effects of an untested ‘booster’ will not erode more rapidly and to a greater extent?”
The article goes on to cite a Lancet preprint23 that compared outcomes among “vaccinated” and unvaccinated Swedes over the course of nine months. As in other studies, they found that protection against symptomatic COVID rapidly declined, and by six months’ post-jab, “some of the more vulnerable vaccinated groups were at greater risk than their unvaccinated peers.”
“Doctors are calling this phenomena in the repeatedly vaccinated ‘immune erosion’ or ‘acquired immune deficiency,’ accounting for elevated incidence of myocarditis and other post-vaccine illnesses that either affect them more rapidly, resulting in death, or more slowly, resulting in chronic illness,” the Frontline Doctors explain.24
The article also cites an August 2021 report from Scotland,25 which found those who had received the jab were 3.3 times more likely to die from COVID infection than the unvaccinated — a finding that certainly blows a huge hole in the claim that the jab prevents serious illness and death even if you do get symptomatic infection.
ICU Admissions Spike Among Vaxxed Immunocompromised Brits
The Daily Mail at the end of November 2021 also reported that weekly ICU admissions of “most vulnerable patients” had risen by 50% in the two preceding months, and that 1 in 28 ICU patients had conditions affecting their immune system. Blood cancer patients and organ transplant patients made up a bulk of this group.26
While the Daily Mail blamed the unusually high rate of admissions of immunocompromised patients on the government’s failure to roll out booster shots fast enough to counteract waning immunity, this is incredibly short-sighted. As noted by America’s Frontline Doctors, the shots are creating “vaccine addicts,” in the sense that their immune system won’t be able to ward off COVID without them. However, it’s still a losing venture, as each shot only worsens the immune erosion.
In the final analysis, it looks as though many may indeed end up being just one shot away from VAIDS as they continue to chase protection from an ever-mutating coronavirus.
The Daily Mail article tells the story of a transplant patient who was desperate to get his booster, knowing he was at high risk for COVID complications. It took three weeks, but he finally got his third shot. The very next day — THE NEXT DAY — he developed “a blinding headache, nausea and dizziness. A lateral flow test was positive and a follow-up PCR test confirmed that he had caught COVID.”
But rather than realizing he’s a victim of that third shot, the man is irrationally convinced that had he just gotten the third dose sooner, he wouldn’t have gotten COVID at all. Sadly, people like these will likely die from their “COVID jab addiction.” In closing, The Exposé writes:27
“Acquired immunodeficiency syndrome is a condition that leads to the loss of immune cells and leaves individuals susceptible to other infections and the development of certain types of cancers. In other words, it completely decimates the immune system.
Therefore, could we be seeing some new form of COVID-19 vaccine induced acquired immunodeficiency syndrome? Only time will tell, but judging by the current figures it looks like we will only need to wait a matter of weeks to find out.”
Sources and References
- 1 CDC COVID Data Tracker Data for 1/9/2022-1/15/2022
- 2, 4, 5, 9, 10 CNBC January 10, 2022
- 3 New York Post January 25, 2022
- 6 ZeroHedge January 25, 2022
- 7 CNN January 25, 2022
- 8 CNBC November 28, 2021
- 11 Reuters COVID tracker Israel as of January 24, 2022 (Archived)
- 12 New York Times COVID Vaccination Tracker, Israeli data as of January 25, 2022 (Archived)
- 13 Reuters January 22, 2022
- 14 Axios January 24, 2022
- 15, 18, 19, 20, 27 The Expose January 22, 2022
- 16 Science November 4, 2021; 375(6578): 331-336
- 17 Medical Express September 2, 2021
- 21, 22, 24 Americas Frontline Doctors December 6, 2021
- 23 Lancet Preprint October 25, 2021
- 25 Public Health Scotland August 2, 2021
- 26 Daily Mail November 20, 2021
Featured Video
MIT Professsor Ted Postol: Patriot Missile Capabilties
or go to
Aletho News Archives – Video-Images
From the Archives
Neocons confess: “We did 9/11-anthrax”
By Kevin Barrett | Press TV | September 6, 2014
As the 13th anniversary of the crimes of September, 2001 approaches, the neoconservatives are shrieking from the rooftops – and effectively confessing that they were the real perpetrators of the 9/11-Anthrax false flag operation. (The neocons, you may recall, openly called for a “new Pearl Harbor” in September, 2000 – and got one exactly one year later.)
Every year at this time, the neocons orchestrate and hype a series of public relations stunts designed to magnify fears of “radical Islam” and reinforce their crumbling 9/11-Anthrax cover story. But this year’s propaganda campaign is so extreme that it represents a tacit confession: The neocons know that the truth about the 9/11-Anthrax operation is slowly closing in on them; so they are over-reacting by desperately trying to stoke the dying embers of the so-called War on Terror, in order to maintain the myth that Muslims (rather than neoconservative Zionists) attacked America in the autumn of 2001.
When a hysterical person exhibits guilty demeanor by trying too hard to blame a crime on someone else, that person is almost certainly the real perpetrator. As the neocons try much too hard to blame Islam for 9/11 and “terrorism” in general, their hysteria inadvertently reveals their own culpability. Like Shakespeare’s Lady MacBeth, the neoconservative movement has blood on its hands and “doth protest too much.” … continue
Blog Roll
 Aletho News
Aletho News- MIT Professsor Ted Postol: Patriot Missile Capabilties
- Israel Brings The War Rhetoric Towards Türkiye
- The Swiss summit of imperial humiliation
- Iran to continue IAEA cooperation under existing framework, SNSC decision: Baghaei
- Report highlights US munitions crisis: Missiles cannot be replenished quickly even with al the money in the world
- Iran’s Oil Spigot Could Open Soon But Hurdles Remain
- Trump’s Attempt to End the Iran War Infuriates the Uniparty
- First round of Swiss-hosted Iran-US talks ends with 5 key agreements
- What Is Hay Fever?
- IRAN WALKS OUT ON PEACE DEAL DUE TO TRUMP’S THREATS – w/ Prof. Seyed Mohammad Marandi
- If Americans Knew
- The Republican & Democratic Politicians Trying to Scuttle Iran Agreement
- Israel’s continued targeting of civilians in Lebanon renders ceasefire meaningless
- U.S. intelligence warns Israel is likely to undermine Iran peace deal, officials say
- In Gaza, Fathers Can’t Promise Their Children Food, Safety, or Even Survival
- This baby joins thousands of Gazans in need of medical evacuation
- Israel Kills Al Jazeera Journalist & Beloved Ecologist: 2 Articles
- Promoters of Israel: Leo Terrell, Ghana, Floyd Mayweather, Van Jones
- Gaza Soccer Player Who Dreamed of Competing in World Cup Can Now Barely Watch It
- Gaza baby loses mom and a leg; Palestinian prisoner tortured to death – Daily Update
- JNS Policy Summit to kick off in Israel
- No Tricks Zone
- 3 New Studies Find Increasing Trends In Solar Radiation Since The 1980s – Easily Explaining Warming
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
