Danish Study Confirms That Natural Immunity Protects Better Against Infection Than the Vaccines
By Noah Carl | The Daily Sceptic | December 15, 2021
Last week, I wrote about a second major study finding that natural immunity protects better against infection than the Pfizer vaccine. Both this study and the earlier one were from Israel, and while there’s every reason to believe the results generalise to other populations, it’s always good to have data from multiple countries.
We now have those data in the form of a study published by the Statens Serum Institut in Denmark. I can’t say the report itself is worth reading in full, since it’s written in Danish. But I’ve posted the key figure below. It shows protection against infection for three different groups – adjusting for age, sex, comorbidities, and time of year.
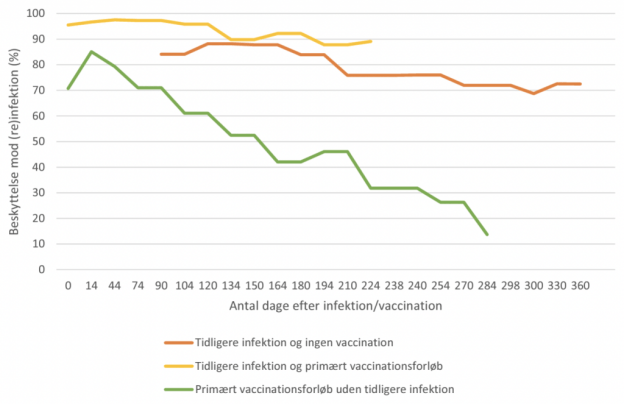
The orange line corresponds to people who’ve been previously infected but not vaccinated; the yellow line to those who’ve been previously infected and vaccinated; and the green line to those who’ve been vaccinated but not previously infected.
The y-axis gives the percentage reduction in the number of infections, compared to those who haven’t been vaccinated or previously infected. For example, a value of 90% means there would be only 10 infections for every 100 in the comparison group. The x-axis gives the number of days since the relevant event.
As you can see, vaccine-induced immunity wanes rapidly, beginning a few weeks after vaccination. And at the five month mark, protection is well below 50%. Natural immunity, by contrast, is robust: a full year after infection, protection is still above 70%.
Consistent with what the two Israeli studies found, hybrid immunity – conferred by the combination of vaccination and previous infection – is slightly better than natural immunity. However, the difference is small compared to that between natural and vaccine-induced immunity.
Evidence for the superiority of natural immunity is now robust. So while those who’ve already had Covid should be perfectly free to get vaccinated, there’s no obvious need for them to do so. The tricky part may be getting this message through to politicians.
32,649 Deaths 3,003,296 Injuries Following COVID Shots in European Database of Adverse Reactions
Young, Previously Healthy People Continue to Die

By Brian Shilhavy | Health Impact News | December 15, 2021
The European Union database of suspected drug reaction reports is EudraVigilance, and they are now reporting 32,649 fatalities, and 3,003,296 injuries, following COVID-19 injections.
A Health Impact News subscriber from Europe reminded us that this database maintained at EudraVigilance is only for countries in Europe who are part of the European Union (EU), which comprises 27 countries.
The total number of countries in Europe is much higher, almost twice as many, numbering around 50. (There are some differences of opinion as to which countries are technically part of Europe.)
So as high as these numbers are, they do NOT reflect all of Europe. The actual number in Europe who are reported dead or injured following COVID-19 shots would be much higher than what we are reporting here.
The EudraVigilance database reports that through December 4, 2021 there are 32,649 deaths and 3,003,296 injuries reported following injections of four experimental COVID-19 shots:
- COVID-19 MRNA VACCINE MODERNA (CX-024414)
- COVID-19 MRNA VACCINE PFIZER-BIONTECH
- COVID-19 VACCINE ASTRAZENECA (CHADOX1 NCOV-19)
- COVID-19 VACCINE JANSSEN (AD26.COV2.S)
From the total of injuries recorded, almost half of them (1,409,643) are serious injuries.
“Seriousness provides information on the suspected undesirable effect; it can be classified as ‘serious’ if it corresponds to a medical occurrence that results in death, is life-threatening, requires inpatient hospitalisation, results in another medically important condition, or prolongation of existing hospitalisation, results in persistent or significant disability or incapacity, or is a congenital anomaly/birth defect.”
A Health Impact News subscriber in Europe ran the reports for each of the four COVID-19 shots we are including here. It is a lot of work to tabulate each reaction with injuries and fatalities, since there is no place on the EudraVigilance system we have found that tabulates all the results.
Since we have started publishing this, others from Europe have also calculated the numbers and confirmed the totals.*
Here is the summary data through December 4, 2021.
Total reactions for the mRNA vaccineTozinameran (code BNT162b2,Comirnaty) from BioNTech/ Pfizer: 15,061 deaths and 1,399,513 injuries to 04/12/2021
- 38,170 Blood and lymphatic system disorders incl. 217 deaths
- 43,454 Cardiac disorders incl. 2,204 deaths
- 404 Congenital, familial and genetic disorders incl. 38 deaths
- 18,886 Ear and labyrinth disorders incl. 10 deaths
- 1,330 Endocrine disorders incl. 5 deaths
- 21,574 Eye disorders incl. 35 deaths
- 115,450 Gastrointestinal disorders incl. 602 deaths
- 354,635 General disorders and administration site conditions incl. 4,251 deaths
- 1,589 Hepatobiliary disorders incl. 78 deaths
- 15,371 Immune system disorders incl. 77 deaths
- 57,255 Infections and infestations incl. 1,605 deaths
- 22,928 Injury, poisoning and procedural complications incl. 261 deaths
- 34,691 Investigations incl. 464 deaths
- 9,568 Metabolism and nutrition disorders incl. 256 deaths
- 172,420 Musculoskeletal and connective tissue disorders incl. 187 deaths
- 1,254 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 122 deaths
- 236,435 Nervous system disorders incl. 1,609 deaths
- 2,000 Pregnancy, puerperium and perinatal conditions incl. 60 deaths
- 215 Product issues incl. 3 deaths
- 25,493 Psychiatric disorders incl. 182 deaths
- 4,981 Renal and urinary disorders incl. 236 deaths
- 49,076 Reproductive system and breast disorders incl. 5 deaths
- 60,177 Respiratory, thoracic and mediastinal disorders incl. 1,664 deaths
- 65,710 Skin and subcutaneous tissue disorders incl. 128 deaths
- 3,007 Social circumstances incl. 19 deaths
- 7,280 Surgical and medical procedures incl. 90 deaths
- 36,160 Vascular disorders incl. 653 deaths
Total reactions for the mRNA vaccine mRNA-1273(CX-024414) from Moderna: 9,084 deaths and 409,189 injuries to 04/12/2021
- 8,678 Blood and lymphatic system disorders incl. 102 deaths
- 13,650 Cardiac disorders incl. 953 deaths
- 166 Congenital, familial and genetic disorders incl. 7 deaths
- 4,940 Ear and labyrinth disorders incl. 4 deaths
- 373 Endocrine disorders incl. 4 deaths
- 5,992 Eye disorders incl. 31 deaths
- 33,407 Gastrointestinal disorders incl. 339 deaths
- 109,178 General disorders and administration site conditions incl. 3,117 deaths
- 673 Hepatobiliary disorders incl. 44 deaths
- 4,054 Immune system disorders incl. 16 deaths
- 15,636 Infections and infestations incl. 849 deaths
- 8,535 Injury, poisoning and procedural complications incl. 172 deaths
- 8,001 Investigations incl. 211 deaths
- 3,893 Metabolism and nutrition disorders incl. 220 deaths
- 49,233 Musculoskeletal and connective tissue disorders incl. 184 deaths
- 568 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 74 deaths
- 68,948 Nervous system disorders incl. 870 deaths
- 754 Pregnancy, puerperium and perinatal conditions incl. 6 deaths
- 82 Product issues incl. 2 deaths
- 7,472 Psychiatric disorders incl. 149 deaths
- 2,398 Renal and urinary disorders incl. 174 deaths
- 8,859 Reproductive system and breast disorders incl. 7 deaths
- 18,183 Respiratory, thoracic and mediastinal disorders incl. 975 deaths
- 21,946 Skin and subcutaneous tissue disorders incl. 82 deaths
- 1,872 Social circumstances incl. 39 deaths
- 1,642 Surgical and medical procedures incl. 115 deaths
- 10,056 Vascular disorders incl. 338 deaths
Total reactions for the vaccine AZD1222/VAXZEVRIA (CHADOX1 NCOV-19) from Oxford/ AstraZeneca: 6,515 deaths and 1,088,775 injuries to 04/12/2021
- 13,292 Blood and lymphatic system disorders incl. 254 deaths
- 19,523 Cardiac disorders incl. 720 deaths
- 203 Congenital familial and genetic disorders incl. 7 deaths
- 12,845 Ear and labyrinth disorders incl. 4 deaths
- 619 Endocrine disorders incl. 4 deaths
- 19,170 Eye disorders incl. 29 deaths
- 103,368 Gastrointestinal disorders incl. 340 deaths
- 286,356 General disorders and administration site conditions incl. 1,544 deaths
- 971 Hepatobiliary disorders incl. 62 deaths
- 4,99 Immune system disorders incl. 30 deaths
- 33,416 Infections and infestations incl. 441 deaths
- 12,583 Injury poisoning and procedural complications incl. 180 deaths
- 23,958 Investigations incl. 159 deaths
- 12,472 Metabolism and nutrition disorders incl. 96 deaths
- 161,308 Musculoskeletal and connective tissue disorders incl. 114 deaths
- 650 Neoplasms benign malignant and unspecified (incl cysts and polyps) incl. 25 deaths
- 223,680 Nervous system disorders incl. 1,007 deaths
- 533 Pregnancy puerperium and perinatal conditions incl. 14 deaths
- 191 Product issues incl. 1 death
- 20,150 Psychiatric disorders incl. 60 deaths
- 4,093 Renal and urinary disorders incl. 63 deaths
- 15,594 Reproductive system and breast disorders incl. 2 deaths
- 38,722 Respiratory thoracic and mediastinal disorders incl. 817 deaths
- 49,877 Skin and subcutaneous tissue disorders incl. 53 deaths
- 1,533 Social circumstances incl. 6 deaths
- 1,499 Surgical and medical procedures incl. 26 deaths
- 27,179 Vascular disorders incl. 457 deaths
Total reactions for the COVID-19 vaccine JANSSEN (AD26.COV2.S) from Johnson & Johnson: 1,989 deaths and 105,819 injuries to 04/12/2021
- 1,029 Blood and lymphatic system disorders incl. 41 deaths
- 1,952 Cardiac disorders incl. 169 deaths
- 36 Congenital, familial and genetic disorders
- 1,080 Ear and labyrinth disorders incl. 2 deaths
- 72 Endocrine disorders incl. 1 death
- 1,415 Eye disorders incl. 7 deaths
- 8,743 Gastrointestinal disorders incl. 80 deaths
- 27,925 General disorders and administration site conditions incl. 533 deaths
- 130 Hepatobiliary disorders incl. 11 deaths
- 473 Immune system disorders incl. 9 deaths
- 4,676 Infections and infestations incl. 157 deaths
- 974 Injury, poisoning and procedural complications incl. 20 deaths
- 4,927 Investigations incl. 111 deaths
- 664 Metabolism and nutrition disorders incl. 50 deaths
- 15,331 Musculoskeletal and connective tissue disorders incl. 45 deaths
- 59 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 4 deaths
- 20,725 Nervous system disorders incl. 219 deaths
- 43 Pregnancy, puerperium and perinatal conditions incl. 1 death
- 32 Product issues
- 1,479 Psychiatric disorders incl. 17 deaths
- 443 Renal and urinary disorders incl. 26 deaths
- 2,249 Reproductive system and breast disorders incl. 6 deaths
- 3,799 Respiratory, thoracic and mediastinal disorders incl. 259 deaths
- 3,241 Skin and subcutaneous tissue disorders incl. 8 deaths
- 337 Social circumstances incl. 4 deaths
- 718 Surgical and medical procedures incl. 58 deaths
- 3,267 Vascular disorders incl. 151 deaths

*These totals are estimates based on reports submitted to EudraVigilance. Totals may be much higher based on percentage of adverse reactions that are reported. Some of these reports may also be reported to the individual country’s adverse reaction databases, such as the U.S. VAERS database and the UK Yellow Card system. The fatalities are grouped by symptoms, and some fatalities may have resulted from multiple symptoms.
RFK Jr. as America’s #1 HIV/AIDS Denier and the Sounds of Media Silence
BY RON UNZ • UNZ REVIEW • DECEMBER 15, 2021
Robert F. Kennedy, Jr.’s book attacking Anthony Fauci and the medical establishment has become a publishing sensation, spending more than a full week as the #1 Amazon bestseller and racking up over 2,600 reviews, 94% of them five-star.
Now after nearly a month of stunned silence, the American media is finally taking belated notice. This morning the Associated Press released a 4,000 word hit-piece harshly attacking the most prominent public figure in America’s much-vilified anti-vaxxing movement.
- How a Kennedy Built an Anti-Vaccine Juggernaut Amid COVID-19
Michelle R. Smith • The Associated Press • December 15, 2021 • 4,000 Words
A great deal of effort had obviously been invested in this attack, and the byline of the named author was shared by five additional AP writers and researchers, underscoring the journalistic resources devoted to damaging the reputation of an individual who has obviously made such powerful enemies. But in reading the article, the phrase that came to my mind was “the Sounds of Silence” or perhaps the famous Sherlockian clue of “the Dog That Didn’t Bark.”
Almost half of the entire book under attack—around 200 pages—is devoted to the presenting and promoting the astonishing claim that everything we have been told about HIV/AIDS for more than 35 years probably amounts to a hoax. As I wrote last week:
Yet according to the information provided in Kennedy’s #1 Amazon bestseller, this well-known and solidly-established picture, which I had never seriously questioned, is almost entirely false and fraudulent, essentially amounting to a medical media hoax. Instead of being responsible for AIDS, the HIV virus is probably harmless and had nothing to do with the disease. But when individuals were found to be infected with HIV, they were subjected to the early, extremely lucrative AIDS drugs, which were actually lethal and often killed them. The earliest AIDS cases had mostly been caused by very heavy use of particular illegal drugs, and the HIV virus had been misdiagnosed as being responsible. But since Fauci and the profit-hungry drug companies soon built enormous empires upon that misdiagnosis, for more than 35 years they have fought very hard to maintain and protect it, exerting all their influence to suppress the truth in the media while destroying the careers of any honest researchers who challenged that fraud. Meanwhile, AIDS in Africa was something entirely different, probably caused mostly by malnutrition or other local conditions.
I found Kennedy’s account as shocking as anything I have ever encountered.
By any reasonable standard, Robert F. Kennedy, Jr. has now established himself as America’s #1 “HIV/AIDS Denier,” and prior to the Covid outbreak, AIDS had probably spent almost four decades as the world’s highest-profile disease, reportedly absorbing some two trillion dollars in research and treatment costs. So for someone to essentially claim that the disease doesn’t actually exist would seem the height of utter lunacy, on a par with Flat Earthism. Yet not a single word of this astonishing situation appears in the long AP article, that attacks Kennedy on almost all other possible grounds, fair or unfair. Did all six of the AP writers and researchers somehow skip over those 200 pages in Kennedy’s bestseller?
That large team of AP journalists seems to have spent at least ten days working on their lengthy article, mining Kennedy’s record for almost everything controversial they could possibly find, even highlighting a photograph that merely shows him standing next to Trump allies Roger Stone and Michael Flynn.

Surely these reporters consulted numerous leading figures in the medical establishment on the HIV/AIDS issue, yet not a single word on that incendiary topic was included in their 4,000 word denunciation.
Although ferocious attacks against Kennedy’s HIV/AIDS claims might naturally have been expected, perhaps certain aspects of the book caused the senior editors of the Associated Press to draw back and decide that discretion on this matter was the better part of valor. As I had explained:
However, the first endorsement on the back cover is from Prof. Luc Montagnier, the medical researcher who won a Nobel Prize for discovering the HIV virus in 1984, and he writes: “Tragically for humanity, there are many, many untruths emanating from Fauci and his minions. RFK Jr. exposes the decades of lies.” Moreover, we are told that as far back as the San Francisco International AIDS Conference of June 1990, Montagnier had publicly declared “the HIV virus is harmless and passive, a benign virus.”
Perhaps this Nobel Laureate endorsed the book for other reasons and perhaps the meaning of his striking 1990 statement has been misconstrued. But surely the opinion of the researcher who won a Nobel Prize for discovering the HIV virus should not be totally ignored in assessing its possible role.
I went on to note:
And he was hardly alone. Kennedy explains that the following year, a top Harvard microbiologist organized a group containing some of the world’s most distinguished virologists and immunologists and they issued a public statement, endorsed by three additional science Nobel Laureates, that raised the same questions:
It is widely believed by the general public that a retrovirus called HIV causes a group of diseases called AIDS. Many biomedical scientists now question this hypothesis. We propose a thorough reappraisal of the existing evidence for and against this hypothesis, to be conducted by a suitable independent group. We further propose that the critical epidemiological studies be designed and undertaken.
As Kennedy tells the story, by that point AIDS researchers and the mainstream media were completely in thrall to the ocean of government funding and pharmaceutical advertising controlled by Fauci and his corporate allies, so these calls by eminent scientists were almost entirely ignored and unreported. According to one journalist, some two trillion dollars has been spent on HIV/AIDS research and treatment over the decades, and with so many research careers and personal livelihoods dependent upon what amounts to an “HIV/AIDS industrial-complex,” few have been willing to critically examine the basic foundations of that empire.
Until a couple of weeks ago, I had never given any thought to questioning AIDS orthodoxy. But discovering the longstanding scientific skepticism of so many knowledgeable experts, including four Nobel Laureates, one of them the actual discoverer of the HIV virus, has completely shifted my perspective. I cannot easily ignore or dismiss the theories Kennedy presents… And in basic fairness to the author, he himself also repeatedly emphasizes that he can “take no position on the relationship between HIV and AIDS” but is simply disturbed that Fauci has successfully used his government funding and media clout to suppress an ongoing and perfectly legitimate scientific debate. According to Kennedy, his book is intended “to give air and daylight to dissenting voices.”
So the total silence of the article does certainly raise certain obvious suspicions. As I previously wrote:
Robert F. Kennedy, Jr. is a top figure in America’s much-vilified anti-vaxx movement and his book is becoming a major element of that cause. His strident attacks against pharmaceutical companies, medical orthodoxy, and Fauci have earned him numerous, powerful enemies. If his AIDS claims were really as ridiculous as they might seem, would they not have already become a lightning rod for attacks against him? Suppose that his anti-vaxx tome had devoted 200 pages to arguing that our world was secretly controlled by invisible 12-foot-tall Reptilians from another dimension. Surely Kennedy’s enemies would have unleashed a huge storm of media ridicule against him for that lunacy, thereby discrediting his critique of vaccination campaigns. Yet instead complete silence has greeted his AIDS claims, raising questions in my mind of whether the medical establishment suspects that it has a great deal to hide and that many of Kennedy’s accusations might be correct.
As an outside observer with no special expertise in these areas of medicine, I was impressed by much of the material that Kennedy marshaled in support of his unorthodox views on vaccines and Covid treatments, but found that the evidence he provided on HIV and AIDS was vastly more comprehensive and persuasive, while being backed by far more authoritative experts. But if as he argues, the truth about HIV and AIDS has been successfully suppressed for decades by the entire medical industry, we must necessarily become very suspicious about other medical claims, including those regarding Covid and vaccinations.
Unless the medical and media establishments swiftly and forthrightly challenges Robert F. Kennedy, Jr. on the issue of HIV/AIDS, any fair-minded observers must necessarily conclude they recognize that he is substantially correct. And if he is correct about AIDS, any shreds of remaining credibility in our public health authorities will surely be destroyed, while the longstanding theories of Berkeley Prof. Peter Duesberg will have been vindicated:
- The chemical bases of the various AIDS epidemics: recreational drugs, anti-viral chemotherapy and malnutrition
Peter Duesberg, Claus Koehnlein, and David Rasnick • Journal of Bioscience • June 2003 • 24,000 Words
So as some have suggested, HIV/AIDS might very well become the Achilles’ Heel of our corrupt and incompetent medical establishment.
Forget China, was it CEPI’s bio-spooks who locked down the West?
By Paula Jardine | TCW Defending Freedom | December 15, 2021
IT is nearly two years since the world turned upside down and a sequence of unprecedented lockdowns and quarantines in the name of public health and safety were imposed across the West.
The narrative of the still unfolding story of Covid-19 is familiar to all of us, with China the chief bogeyman of the tale. But is that right?
In this drama has something really important been overlooked? Namely, the role of a powerful, self-appointed supranational organisation, set up 2017, called the Coalition for Epidemic Preparedness Innovations (CEPI).
Members of CEPI’s board and scientific advisory committee have been, and still are, key actors in global and national responses to the Covid-19 virus. Its mission? To ‘create a world in which epidemics are no longer a threat to humanity’.
At the start of 2020, all eyes were glued on China. The communist government had dutifully notified the World Health Organisation (WHO) on New Year’s Eve 2019 of its concerns over a small cluster of cases of ‘pneumonia of unknown origin’.
Three weeks later, when the death toll stood at 17, the CCP was sufficiently alarmed to order the home confinement of nearly 12 million mostly healthy people who were unfortunate enough to reside in the outbreak city, Wuhan.
Having fingered as the culprit a relative of the SARS virus that claimed 774 victims in 2003, the Chinese determination to contain the self-evidently nastier 2019 co-variant at all costs was made plain to the world.
The scenes broadcast out of China nightly on the TV news were surreal, but strangely familiar to anyone with a passing familiarity with vintage sci-fi. A nightmare amalgamation of The Andromeda Strain and The Hamburg Syndrome was unfolding in real life, right before our eyes.
Here, a man falling down dead in the street. There, men in white hazmat suits walking through empty Chinese thoroughfares equipped with Ghostbuster-esque backpacks blowing smoke in a desperate attempt to fumigate the invisible peril out of existence.
Knowing that the Queen’s own men at the Porton Down chemical and biological defence establishment long ago discovered that fresh air and sunlight, two commodities already in short supply in Chinese cities, are the most potent of disinfectants, it seemed a strangely futile spectacle. What on Earth were they trying to do? Death apparently lurked around every corner.
As the Wuhan lockdown was being imposed on January 23, 2020, the global elite were busy congregating at their annual networking fest, the World Economic Forum, in Davos, Switzerland (where CEPI had been founded three years earlier by the governments of Norway and India, the Bill & Melinda Gates Foundation, the Wellcome Trust global charity organisation, and the World Economic Forum).
Next day, a little-noticed press conference was convened in Davos to discuss the SARS-like, closely-related, but definitely novel, SARS Wuhan coronavirus.
Appearing in front of about 30 reporters were Sir Jeremy Farrar, Director of the Wellcome Trust and board member of CEPI; Richard Hatchett, chief executive of CEPI, and Stephane Bancel, chief executive of Moderna, one of three companies being funded to develop a coronavirus vaccine. A Chinese reporter asked the panel if there was any historical precedent for the lockdown.
Hatchett said: ‘One thing that is important to understand, is that when you don’t have treatments and you don’t have vaccines, non-pharmaceutical interventions are literally the only thing that you have, and it’s a combination of isolation, containment, infection prevention and control and then these social distancing interventions.
‘There is historical precedent for their use. We looked intensively and did an historical analysis of the use of non-pharmaceutical interventions in US cities in 1918 and what we found was that cities that introduced multiple interventions, early in an epidemic, had much better outcomes.
‘The challenge of course is that it is very difficult to sustain these interventions, as they impose enormous cost and they also can produce enormous anxiety among the affected population.’
The ‘we’ Hatchett was referring to was the US Department of Homeland Security where, as an official, he had helped develop the US pandemic preparedness plan in 2005 and 2006 during the H5N1 avian influenza outbreak, which Farrar had discovered in Vietnam.
Hatchett continued: ‘At that time, we looked at how could you have those interventions implemented in a way that maximised their benefit and minimised the cost and we developed an approach that we called “community mitigation” interventions and CDC (the US Centres for Disease Control and Prevention) published guidance on this several years ago.
‘There is a literature which I would certainly encourage Chinese authorities to review and certainly I would be happy to talk to them about that, although that’s not my current job.’
There was no need to encourage the Chinese authorities to review the literature. CEPI already had a man in Beijing, Dr George Gao, the director of China’s Centre for Disease Control, but also member of the CEPI scientific advisory panel. The community mitigation approach the Chinese adopted in Wuhan was straight out of the 2006 US Homeland Security pandemic playbook.
Gao, like Farrar, completed his PhD at Oxford University before conducting post-doctoral work under Sir John Bell, the controversial Regius Professor of Medicine at Oxford, holder of several extranumerary positions and multiple interests, not least as chair of the global health scientific advisory board of the Bill & Melinda Gates Foundation.
An expert on coronaviruses, Gao served on CEPI’s first scientific advisory committee in 2016 and was a player in Event 201, the pandemic simulation hosted in October 2019 by the World Economic Forum, Bill & Melinda Gates Foundation and the Johns Hopkins Bloomberg School of Health – discussed here by Robert F Kennedy Jr.
In all probability, Gao is the old friend Farrar was referring to when he said on Desert Island Discs that he had had a phone call on December 31, 2019 – the day the Chinese authorities reported the Wuhan pneumonia outbreak to the WHO – to alert him that China would release the genome of the new virus on January 10. As things stood on New Year’s Eve, the virus had yet to cause any deaths, although it was making a few people very ill.
By January 17, another CEPI scientific adviser, Dr Christian Drosten, had conveniently developed a PCR test from the genetic sequence posted online by the Chinese, which the WHO advised laboratories could be used as a diagnostic test for Covid-19.
This was almost two months before the WHO declared the novel coronavirus a pandemic on March 11, 2020. Following a visit to Wuhan by the WHO in February 2020, led by its assistant director-general Dr Bruce Aylward, the world was being encouraged to adopt what were now being called Chinese measures.
‘China didn’t approach this new virus with an old strategy for one disease or another disease,’ said Aylward. ‘It developed its own approach to a new disease and extraordinarily has turned around this disease with strategies most of the world didn’t think would work.’
The Chinese government, with its own Big Brother infrastructure, had its own reasons for going along with that. But the response plan is in reality far more complex, and has a much darker background in the West.
The Yellow Brick Road that passes through CEPI and Beijing leads right back to the US Department of Homeland Security, and its 1998 Pentagon strategy paper.
The response plan is in reality an American scheme, with its origins more than decade and a half earlier and against a backdrop of bioterrorism concerns. Uncle Sam is the wizard behind the curtain, not acting in the West’s interests at all.
FDA Colludes with US Postal Service to Destroy Ivermectin Shipments
InfoWars | December 15, 2021
The US Food and Drug Administration is colluding with the US Postal Service to intercept inbound international shipments of Covid wonder drug ivermectin, reports circulating on social media claim.
According to letters from the FDA being shared online, the federal regulatory agency blocked shipments of ivermectin from reaching their intended recipients as they came through ports of entry.
“A shipment addressed to you from a foreign country is being held by the post office at the request of the US Food and Drug Administration,” reads one letter shared by attorney Aaron Siri.
According to the letter, the package containing 200 tablets of “Iverheal ivermectin tablets” was intercepted at the JFK Airport Port of Entry on November 9, 2021.
In another letter, the FDA intercepted 300 tablets of “Iverpac12” back in August, which they said were “subject to refusal of admission into the United States and are subject to administrative destruction.”
News of the FDA’s collusion with the US Postal Service comes as more people seek the effective drug and other preventative early treatments to remedy Covid-19 symptoms.
Meanwhile, the FDA has continued it’s fear-mongering campaign advising Americans not to consume the “horse dewormer” drug to treat Covid, as it has not been formally approved [for COVID use].
Medical Tyranny the New Abnormal

By Stephen Lendman | December 15, 2021
State-sponsored/MSM supported medical tyranny is the new abnormal throughout the US/West and elsewhere worldwide.
I’m greatly indebted to numerous truth-telling medical and scientific experts for teaching me what I’ve learned about all things flu/covid — a medical education I never imagined getting pre-2020 but got since then on this most cutting edge of all issues.
To my great dismay, intelligent people I know are oblivious to reality on what’s crucial to know — believing rubbish fed them daily from official, MSM, and other disreputable sources instead of what’s scientifically indisputable.
Protecting and preserving public health and freedom depend on enough committed people rising up against what’s going on — slaying it before it slays us.
Relief won’t come judicially or legislatively.
On all issues mattering most, positive change never comes top down, only bottom up by committed people demanding no less.
The anti-public health/anti-freedom scheme was planned well before its rollout early last year.
As explained time and again, it’s all about wanting maximum numbers of unwanted people eliminated worldwide, along with transforming free and open societies into ruler/serf ones for survivors.
It’s a draconian new world order fit only for privileged interests at the expense or all others.
It’s what no one anywhere should tolerate, a tyrannical world that’s unsafe and unfit to live for the vast majority worldwide — the worst of all possible worlds.
Things don’t have to be this way.
Ordinary people have power to rise up against injustice, defy unjustifiable rules, disrupt best laid plans of dark forces and achieve positive change by their actions.
History proves it. Years of anti-war activism helped end a decade of US aggression in Southeast Asia — a pyrrhic victory as things turned out because anti-war activism waned.
The same applies to moving from chattel to wage slavery, from Jim Crow to its modern-day version, from freedom to mass incarceration, from healthcare as it should be to toxic mass-jabbing with unparalleled genocide in mind.
Governance of, by and for entrenched interests in the US/West and elsewhere is too debauched to fix.
The same goes for MSM guardians of wealth, power and privilege.
Scattered reforms won’t work. Transformational change is needed.
The only solution is popular revolution. Anything less assures no change of unacceptable same old, same old.
Wealth, power and privileged interests are enemies of ordinary people everywhere.
Collective defiance is needed to turn things from what’s destructive of the general welfare to what’s beneficial.
Former Pfizer vice president, its chief scientist for allergy and infectious diseases, co-founder of Doctors for (flu/covid) Ethics, Dr. Michael Yeadon, is on the right side of history for this most crucial of all issues.
Commenting on what’s gone on since early last year, he said the diabolical scheme has nothing to do with protecting us, everything to do with establishing “totalitarian control.”
Fundamental freedoms are being abolished incrementally.
Things began by denying refuseniks free access to restaurants and other places where large numbers gather.
Widespread use of freedom-destroying health passports may follow as a requirement to stay free from societal isolation altogether.
Yeadon compared the above to “dropping a cancerous cell into your body (that) grows and metastasizes and then it kills you.”
“(T)hat’s what” health passports are all about if instituted.
“So don’t tolerate them anywhere,” Yeadon stressed.
Once instituted, metastasizing will “regulate access to essential services like food, money, fuel, trains and things like that.”
“You’ll never get rid of (them). We’ve got to stop (what’s going on) beforehand.”
Otherwise we’ll “lose the ability to decide where to be at any time.”
Health passports will “regulate entry and exit from almost any controlled space, possibly even including your own home.”
“You’ll be required to keep your passport up to date by being fully jabbed” — meaning forever-jabbed one or more time annually.
The more toxic jabs gotten, the sooner your end time will arrive, most likely very unpleasantly from painful and/or debilitating disease(s).
Getting informed from reliable independent sources, getting motivated and enraged enough to no longer tolerate what’s going on is the only way to halt it once and for all.
“(I)t’s us” on our own against the diabolical scheme. We alone can and must stop it.
The alternative is deeply entrenched tyranny, a permanent new abnormal, dystopia no one should tolerate.
Jabs are vehicles of mass-extermination.
Pharma profiteers and Big Government backers “are the most ruthless of all corporate entities,” Dr. Vernon Coleman stressed, adding:
It’s been known since last year that mass-jabbing “cause(s) heart trouble, strokes, neurological problems,” and other serious health issues.
Coleman believes that most jabbed individuals will be “lucky to last five years.”
Individuals taking them “should be considered suicidal or certified insane.”
“Life expectation is going to fall dramatically – and not just because the quality of health care is deteriorating daily.”
“I honestly find it difficult to believe that there are people around who are so brainwashed and so terrified by the lies they’ve heard that they will accept as many jabs as they are offered.”
The power of repetition, especially on propaganda TV, gets most people — including intelligent ones — to believe almost anything no matter how scientifically or otherwise untrue.
With minimal effort, anyone connected online can learn enough about what’s going on from reliable, independent sources to know we’re being scammed by US/Western and other governments, Pharma and their MSM press agents.
Getting mad as hell, rising up and refusing to take it any more is the only way to beat the diabolical scheme.
Nothing else can work.
The Pandemicists Must Be Stopped
The Pandemicists at Work:

This strange and mildly disturbing illustration actually accompanies the article, one of many cases where the NYT betray the sinister undertones of their agenda via accompanying imagery.
eugyppius – December 14, 2021
Corona has vastly expanded the ranks of pandemic planners and public health botherers. Unless something is done, these people will destroy all of society in their radical pursuit of a few viruses.
Just a few words on “Omicron is a Dress Rehearsal for the Next Pandemic”, a New York Times article by Emily Anthes, a science journalist with ties to the World Economic Forum. It’s subtitled “America’s response to the variant highlights both how much progress we have made over the past two years — and how much work remains,” and it’s every inch as awful as you’d imagine.
In the piece, Anthes laments that the United States is “woefully unprepared for the challenges ahead, starting with the most fundamental of tasks: detecting the virus.” She quotes a microbiologist to complain that “We had a delay of one to two months before we were even able to identify the presence of [Omicron] … And by that time, it had already circulated widely between multiple states and from coast to coast.” She wastes many words on the necessity of “Testing, testing, testing”; here, apparently, America still needs vastly more capacity. She and her many scientist informants also want more gene sequencing to detect variants sooner. She’s sure that all of this is absolutely necessary, even though she doesn’t know why:
Scientists are finding more Omicron cases every day, and the variant could soon overtake Delta. What comes next — what we should aim for, even — is less clear. Should we spend the winter trying to stop every infection? Protecting the highest risk people from severe disease and death? Ensuring that hospitals are not overrun?
“One thing that we’ve lacked continuously through the pandemic is a goal,” said Emily Gurley, an epidemiologist at the Johns Hopkins Bloomberg School of Public Health. “We still don’t have that. Certainly, we don’t have that for Omicron.”
No realistic public health goal underpins this diagnostic mania, of course. People who test positive for Corona are sent home to suffer in untreated silence by themselves. Endlessly testing, tracing, sequencing, panicking and closing is, however, a goal in itself for people like Emily Gurley and all the other pandemicists Anthes gleefully quotes, from Eric Topol to Trevor Bedford to Ezekiel J. Emanuel. All of them want the Corona Circus to play on, and after it ends they hope for a sequel sometime soon. Never before have they enjoyed such personal and professional prominence.
Even if by some miracle all of this winds down tomorrow, this whole odious internationally networked enterprise of Virus Astrology, from virologers to sequencers to testers to planners to nudgers to vaccinators, won’t go away. They were a malign influence even before Corona, of course. In 2009, when we suffered under a small fraction of the Pandemicism that burdens us now, they succeeded in causing an international uproar over a mild strain of pandemic influenza. Now their ranks have been vastly expanded, and they are already hoping for the next opportunity to close our schools, lock us up at home and stick us full of needles.
The pandemicists are truly dangerous, and they will grind human civilisation into the dust unless we find some way of putting all of them out of work. They aren’t going to save anybody from the next pandemic; in the event it happens, they’ll just take advantage of the opportunity to expand their ranks still further and make all of our lives worse. And should novel viruses prove slow to materialise in the post-Corona era, they’ll get up to other tricks. Tricks like new and enhanced histrionics over every seasonal influenza outbreak. Tricks like the intentional release of more engineered viral pathogens to keep the grant funding flowing. Tricks like constant lunatic mass vaccination schemes against ever milder viruses. Still other tricks I haven’t considered. The pandemicists have to go.
A huge Israeli study shows natural Covid immunity is far superior to the vaccine-generated kind
By Alex Berenson | December 14, 2021
mRNA vaccine protection from Covid is far weaker than natural immunity and declines very fast, according to a new study of almost 6 million people in Israel.
During the summer Covid wave, more than 140,000 Israelis who had been vaccinated but not received a booster shot became infected with Covid. Put another way, in just two months, about 1 out of every 20 vaccinated Israelis became infected with Sars-Cov-2.
Natural immunity – the protection following infection and recovery – lasts much longer, the study shows.
In fact, people who had already had Covid once had better protection from the virus more than a year later than people who had been vaccinated only three months before.
The gap was even larger in cases of severe infection.
Vaccinated people were more than five times as likely to develop severe infections than people with natural immunity. Only 25 out of roughly 300,000 Israelis with natural immunity developed severe Covid infections in the summer wave – compared to almost 1,400 vaccinated Israelis.
The difference did not result from gaps in age between vaccinated and recovered people. People over 60 benefitted even more from natural immunity relative to vaccination than did younger people.
The study also showed that giving people who had natural immunity a vaccine dose did little to lower rates of infection for them, raising the question of why they should ever be vaccinated.
Finally, the study offered a disturbing signal that vaccination may ultimately interfere with the development of lasting immunity in people who are infected after being vaccinated.
A booster shot did lower the risk of infection about to the level of peak protection from natural immunity – but because the study ended in September, it is impossible to know how long that protection may last.
All these findings come out of a database of Covid infections among almost 6 million Israelis in August and September, at the peak of the fourth Covid wave in Israel. The database contains information on essentially every Israeli over age 16 who was fully vaccinated or had previously had a Covid infection.
The paper, “Protection and waning of natural and hybrid COVID-19 immunity,” is currently available as a preprint at:
https://www.medrxiv.org/content/10.1101/2021.12.04.21267114v1.full.pdf
Oddly, the paper’s title does not mention waning of vaccine immunity, although the figures it presents make the severity of the problem clear. Such shyness is common among researchers presenting bad news about Covid vaccines – they will offer the data, but not highlight it.

Israel has exclusively used the Pfizer mRNA vaccine, began mass vaccinations before almost any other country, and has an excellent health care database. As a result, it has among the best information on the effectiveness of the shots. It offers far more complete data than the United States.
The vaccine failure over the summer in Israel – following apparent success in the spring – has presaged a similar pattern across the United States and Europe, and a similar desperate campaign for boosters.
In this paper, the researchers examined infection rates among five different groups of Israelis – those with natural immunity, those who had received boosters, those who were vaccinated but had not received boosters, those with natural immunity who had also received a vaccine, and those who had become infected after being vaccinated.
The researchers specifically excluded unvaccinated Israelis without natural immunity from the comparison because Israel has very few of them and they are “unrepresentative of the overall population.”
In other words, the researchers explicitly denied the validity of the comparison that vaccine advocates make when they compare Covid rates among vaccinated and unvaccinated people in places with high vaccination rates (a point I have been trying to make for months).
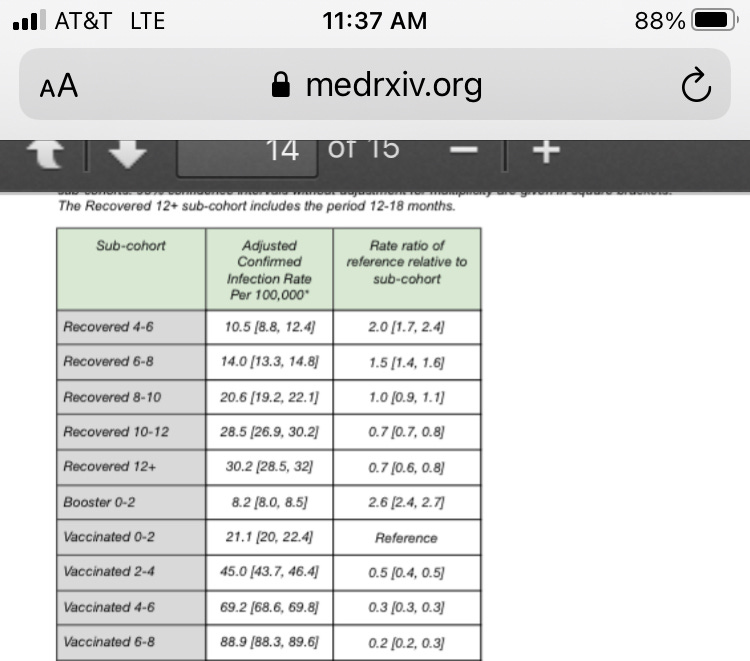
The researchers found that the highest rates of infection by far came in people who had been vaccinated at least six months before. They had a nearly 3 percent chance of being infected per month (the researchers present the figure as 89 per 100,000 “person-days.”)
Those people were four times as likely to be infected as newly vaccinated people. They were also seven times as likely to be infected as people who had natural immunity from an infection six to eight months before, and three times as likely as those who had natural immunity from an infection more than year before.
A single vaccination dose in people with natural immunity temporarily produced strong protection, the researchers found. But after six months, the advantage had faded to within the margin of statistical error. In other words, so-called hybrid immunity hardly appeared to exist after six months – natural immunity was once again providing the protection.
Nor did vaccination appear to stop severe disease.
Nearly every case of severe disease in the database – almost 1,400 of the roughly 1,600 cases – came in vaccinated but unboosted people. Boosters did appear to reduce severe disease significantly. Again, though, the study covered less than two months after the booster program began, when boosters should be at peak effectiveness.
Finally, the study showed that people who had been vaccinated and then been infected and recovered were actually more likely to be infected again six months later than those who had only “pure” natural immunity.
That finding, though based on a small number of cases, adds to worrying data that mRNA vaccination may actually wrong-foot our immune systems in the long run and make it harder to build lifelong protection against Covid.
Since Biden’s Injection Order the Rate of Covid Deaths in the US Military Has Quadrupled
Anti-Empire | December 12, 2021
On August 25th Biden ordered that every member of the US military (active, reserve and national guard) must perform a fundamental sacrament of the mind virus cult known as “vaccination”.
A week before the order US military Covid deaths stood at 34.
Presently they stand at 79.
In other words, in the 4 months since the injection order as many US servicemen were deemed to have died with/from Covid as in the entire 17 months before the order was given.
In the entire vaccine-free 2020 fewer than 20 US servicemen died with/from Covid. (24 by March.)
The unvaccinated military of 2020 experienced three times fewer Covid deaths than the heavily injected military of 2021.
Even so at 2 million strong and 79 deaths, a Covid death is still rarer than a lottery win.
The Pentagon says the dead were overwhelmingly “not fully vaccinated,” but the Pentagon also doesn’t consider troops “fully vaccinated” until 14 days after the 2nd dose — that is to say until the initial period of negative vaccine efficiency has ended.
Comirnaty, liability, and how the HHS lies, cheats and steals
By Meryl Nass, MD | December 12, 2021
I checked the Federal Register and there has been no notice that Comirnaty has been added to the National Childhood Vaccine injury Program (NVICP). I confirmed this by checking whether Comirnaty had been added to the childhood schedule, and according to the HRSA, which manages both compensation programs, it has not.
So, if you receive the licensed Comirnaty vaccine, correctly labeled as the brand-name product and not the vaccine being fobbed off as licensed product, and you are injured, you are free to sue the manufacturer for your injury. Could this be why Pfizer wrote, “Pfizer does not plan to produce any product with these new [Comirnaty National Drug Codes] and labels over the next few months while EUA authorized product is still available and being made available for U.S. distribution.”
If, however, you receive the Pfizer-BioNTech vaccine under Emergency Use Authorization, or the Moderna or J and J vaccine, you can’t sue anyone. You have the right to beg HRSA for compensation of lost wages and unpaid medical bills, period. So far, HRSA and the Countermeasures Injury Compensation Program it administers have not paid out one dime for the approximately one million injuries and 20,000 deaths reported to VAERS for any COVID vaccine.
In other words, the federal government (DHHS) has not admitted a single injury was caused by a COVID vaccine. CDC says it has not linked a single death to a COVID vaccine–not even when the patient walked into the vaccination center but got carried out to the morgue. FDA doesn’t know much about myocarditis, Bell’s Palsy, thrombosis, thrombocytopenia, pulmonary emboli, etc. There are no black box warnings on any of the COVID vaccines.
HRSA, FDA, CDC and NIH are all agencies within the federal Department of Health and Human Services. They have all gotten their stories straight. They know nothing and they are just following orders. Heil HHS!
They can’t find a doggone problem in the 20 or so databases they are spending many $millions of your money to “study.”
Want to know the biggest conspiracy in the US right now? It is the HHS.
FDA has access to a bunch of electronic databases it has termed the “BEST” Initiative, and it published a plan to use them to study heart attacks, pulmonary embolism, thrombocytopenia, etc. back in July. Where are the results, FDA? What are you waiting for? (According to CDC, “More than 459 million doses of COVID-19 vaccines were administered in the United States from December 14, 2020, through November 29, 2021.”). It seems clear that we aren’t supposed to be informed of FDA’s findings until everyone possible has been vaccinated, at which point the results will be irrelevant.
In October 2020, FDA’s Steve Anderson told us there were even more databases that would be studied.
On August 23, 2021, FDA announced its databases were inadequate to assess myocarditis, so BioNTech would have to do it for them. Here is what FDA wrote about its inability to use VAERS and its many other databases:
- As noted above, the FDA acknowledges that “We have determined that an analysis of spontaneous postmarketing adverse events reported under section 505(k)(1) of the FDCA [in other words, VAERS–Nass] will not be sufficient to assess known serious risks of myocarditis and pericarditis and identify an unexpected serious risk of subclinical myocarditis.
- Furthermore, the pharmacovigilance system that FDA is required to maintain under section 505(k)(3) of the FDCA [in other words, FDA’s many other databases that cost the taxpayer zillions–Nass] is not sufficient to assess these serious risks.”
NOT SUFFICIENT???
Unsaid, but implied, is that if FDA is incapable of studying thousands of reported cases of myocarditis, it probably cannot study the other serious adverse events that have been reported in conjunction with COVID vaccines.
VAERS has operated for 30 years, collecting reports of vaccine adverse events. It averaged under 100 cases of myocarditis reported yearly until this year. Through November, CDC reports it received 1949 reports of myocarditis and pericarditis, in those under 30. CDC didn’t say what the total number of reports for all ages was.
Somehow, these HHS don’t seem all that concerned that the admitted reporting rate of myocarditis is over 20 times the average during the past 30 years. Why?
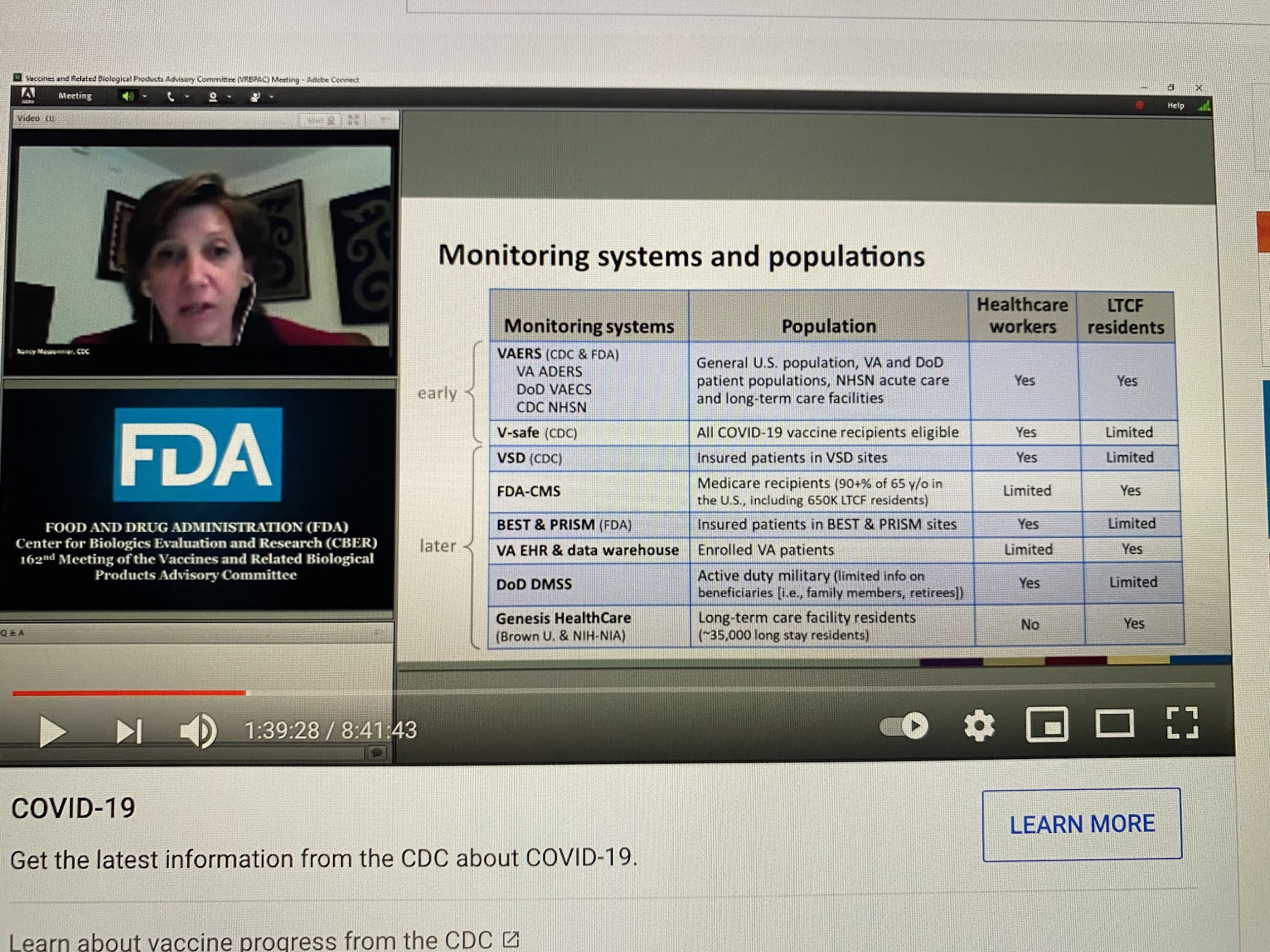
CDC has been even more shady in its analyses of safety as FDA, if that is even possible. Below, Nancy Messonier, then head of Immunizations and Respiratory Diseases at CDC, presented this list of databases that CDC would be using in the evaluation of COVID vaccine safety, on December 10, 2020. Apart from the V-safe (which they stopped talking about last January), VSD (which somehow can’t find any problems, not even myocarditis) and VAERS, all these other databases have been MIA.
NIH, whose job has never been to issue treatment guidelines, but instead to do and fund research, suddenly took over the treatment guidelines for COVID early in 2020. It formed a committee of internal and eternal “experts” to make up the guidelines. How were they chosen? That is not clear, but what is clear is that 16 of these so-called experts had current or recent financial entanglements with Gilead, the maker of remdesivir. NIH and the US Army also owned pieces of remdesivir. A number of other had financial conflicts with Merck. While NIH is the biggest single funder of medical research in the world, I cannot recall seeing a single study it funded on the safety of COVID vaccines. But somehow vaccines are its number one recommendation.
But it is not even clear that the committee is functional. The NIH has been sued to learn whether a vote was even taken by the committee regarding its ivermectin guidelines, which fly in the face of the evidence on ivermectin. How was NIH somehow authorized to issue guidelines in the first place?
Here is what has obviously occurred. All these agencies were told they had to keep quiet on vaccine problems (and perhaps problems of other COVID treatments), and they had to fiddle with their data or their analytic methods, or both, to get the required results. And there was to be NO BAD NEWS, no matter what. And no good news regarding generic treatments.
As we have seen, the so-called scientists and physicians working as bureaucrats in these agencies all caved, sucked it up, did the dirty work, kept their jobs, and betrayed their oaths and the trust of the people of the USA and the world.
Featured Video

Iran Walks Out On Peace Deal Due To Trump’s Threats
or go to
Aletho News Archives – Video-Images
From the Archives
Neocons confess: “We did 9/11-anthrax”
By Kevin Barrett | Press TV | September 6, 2014
As the 13th anniversary of the crimes of September, 2001 approaches, the neoconservatives are shrieking from the rooftops – and effectively confessing that they were the real perpetrators of the 9/11-Anthrax false flag operation. (The neocons, you may recall, openly called for a “new Pearl Harbor” in September, 2000 – and got one exactly one year later.)
Every year at this time, the neocons orchestrate and hype a series of public relations stunts designed to magnify fears of “radical Islam” and reinforce their crumbling 9/11-Anthrax cover story. But this year’s propaganda campaign is so extreme that it represents a tacit confession: The neocons know that the truth about the 9/11-Anthrax operation is slowly closing in on them; so they are over-reacting by desperately trying to stoke the dying embers of the so-called War on Terror, in order to maintain the myth that Muslims (rather than neoconservative Zionists) attacked America in the autumn of 2001.
When a hysterical person exhibits guilty demeanor by trying too hard to blame a crime on someone else, that person is almost certainly the real perpetrator. As the neocons try much too hard to blame Islam for 9/11 and “terrorism” in general, their hysteria inadvertently reveals their own culpability. Like Shakespeare’s Lady MacBeth, the neoconservative movement has blood on its hands and “doth protest too much.” … continue
Blog Roll
 Aletho News
Aletho News- Iran’s Oil Spigot Could Open Soon But Hurdles Remain
- Trump’s Attempt to End the Iran War Infuriates the Uniparty
- First round of Swiss-hosted Iran-US talks ends with 5 key agreements
- What Is Hay Fever?
- IRAN WALKS OUT ON PEACE DEAL DUE TO TRUMP’S THREATS – w/ Prof. Seyed Mohammad Marandi
- Moderna’s mRNA Flu Vaccine Gets Unanimous Thumbs-Up Despite Risks, Low Efficacy
- UK Speech Regulator’s Telegram Questions Point Toward Private Chats
- Cuban FM blasts Rubio for ‘chronically lying’ about US fuel blockade
- Al-Jazeera demands punishment for Israeli officials following latest assassination of cameraman
- Iran opens hundreds of legal cases over US, Israeli aggression: Prosecutor general
- If Americans Knew
- Gaza Soccer Player Who Dreamed of Competing in World Cup Can Now Barely Watch It
- Gaza baby loses mom and a leg; Palestinian prisoner tortured to death – Daily Update
- JNS Policy Summit to kick off in Israel
- Fatalities From Israel’s Vast Gaza Genocide Deliberately Undercounted
- ‘Reproductive genocide’ in Gaza; death toll in Lebanon tops 4,000 (during a ceasefire) – Daily Update
- Israelis Invaded Lebanon And Then Cried Victim When Their Soldiers Got Killed
- FARA Docs: Israel is Spying On Millions Of Christian Americans In Their Churches
- Why US presidents from both parties end up cursing Benjamin Netanyahu
- Israel Asked Facebook to Censor Iran War Content, Internal Documents Show
- Deaths in Gaza undercounted, possibly by 100s of thousands; “Psychopath” Ben-Gvir talks trash – Daily Update
- No Tricks Zone
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
