Stop ‘harmful’ mass testing of children now, demand MPs
TCW Defending Freedom – February 4, 2022
THE cross-party Pandemic Response and Recovery All-Party Parliamentary Group of MPs met this week to hear whether there is a case for the continued mass testing of healthy children by schools and nurseries.
The committee is co-chaired by Conservative MP Esther McVey and Labour MP Graham Stringer. The group examined the pros and cons of testing in schools, and growing concerns about the likely physical and mental health harms caused by constant testing. Their uncompromising conclusion was that the mass testing of healthy children is ‘harmful, invasive and unevidenced’.
Ms McVey told the group something few of the public outside parents are aware of, which is that children are still routinely being asked to take tests, even at primary school, regardless of whether they have symptoms.
Though the threat of school closures has been lifted and the requirement for children to wear masks rescinded, hundreds of thousands of children are still missing schooling, she said, owing to constant testing and the government requirement for healthy children to isolate.
She informed the group that the evidence presented by their experts found no benefits to mass testing and that the children are not drivers of transmission. They have been disrupted, harmed and distressed despite the absence of any robust randomised control trial evidence of the benefits of mass testing them: ‘The evidence we have heard is clear. Testing in schools must stop, especially in the absence of any sort of study on the impact it has on our children’s physical and mental health. Evidence sessions such as this one are so important, to allow us to get a full picture before we make a decision and put our case to the Government.’
Mr Stringer said: ‘We cannot continue to force such an invasive procedure and we have heard today of children as young as two being physically restrained by their parents, put in headlocks or vomiting after the tests. As I have said before, the evidence to impose these sorts of measures must be overwhelming and I’m not aware the evidence exists that testing healthy children is beneficial and will help stop the spread of SAR-CoV-2. Not to mention the eye-watering sums spent on testing which could have been so much better spent on redressing some of the damage already caused to child mental health. Surely the time has come to stop the mass testing of healthy children?’
The group heard from Dr Angela E Raffle, honorary senior lecturer, University of Bristol Medical School Department of Population Health Sciences, Dr Allyson Pollock, clinical professor of public health at the University of Newcastle, child and adolescent clinical psychologist Dr Zenobia Storah, Professor Ellen Townsend, professor of psychology at the University of Nottingham and Mark Ward, a parent who spoke about the traumatic experiences of testing his toddler.
They all argued against the mass testing of healthy children in schools, highlighting the insufficient scientific and clinical evidence and arguing that, far from being of any public health benefit, mass testing causes significant damage to children.
Dr Raffle said: ‘SARS-CoV-2 testing of healthy school children needs to stop. The World Health Organisation cautions against mass symptomless testing because of high costs, lack of evidence on impact, and risk of diverting resources from more important activities. There is no sound evidence that testing children leads to reduction in serious cases of Covid-19. The policy decision in England to introduce school testing appears to have been a political decision, to create the impression of safety, rather than investing in staffing and ventilation which would have made an impact. The tests being used have not been properly evaluated as self-tests or for use in children. Children are low transmitters compared with adults. The net effect of the school testing is harmful because of the trauma of repeated testing and the disruption to children’s lives through repeated exclusion and isolation. Testing is important when done under medical supervision in order to guide decisions about the best way to treat a child who is ill, but the indiscriminate use of tests in children who are well is unjustified.’
Professor Pollock said: ‘Many of the so-called public health measures applied over the last two years have been no more than blanket measures applied with no evidence but with serious consequences, such as mass testing healthy school children. The tests are inappropriate and in the UK we completely ignored the Wilson and Junger 1968 principles of screening. They are not tests of infectiousness so children were and are being isolated unnecessarily. We know from studies that infected children do not spread the virus to others readily, not other children, their families nor their teachers. Now with the milder Omicron variant, many of them will be asymptomatic, so constantly mass testing healthy children is not only a traumatic experience but an appalling waste of time and is something that should only be done if clinically necessary, such as if a child is ill enough to need medical attention.’
Dr Storah described mass testing of healthy children as ‘harmful, invasive and unevidenced’ and ‘nothing short of state-sponsored child abuse’. She said: ‘I have been working with young people throughout the last two years and have seen a steep rise in mental health conditions as a result of measures like testing. These obsessive infection control measures are causing worrying levels of highly anxious behaviour. They maintain and amplify the fear messaging, further exacerbated when children are surrounded by adults, their parents or teachers, also constantly testing. It is utterly extraordinary for a society to treat their young in such an abusive way, to throw decades of understanding about normal child development out of the window without having considered the risk factors. One in six young people now meets the diagnostic criteria for at least one mental health disorder but there is still time to lessen and even reverse the long-term psychological impact this is having on our children. Children and adolescents need to be prioritised and mass testing, like face coverings, must be consigned to the policy bin, once and for all. What is required immediately is a return to normality for all children and all school and extra-curricular environments.’
Professor of Psychology Ellen Townsend told the group: ‘It is unclear what mass testing healthy children is achieving from a Public Health perspective. No studies have been carried out to understand if there are any benefits and no evaluation has been done on the psychological impact of testing – this is a grave and unethical oversight. We must recognise that children are at minimal risk to others but the harms caused to children, the disruption of testing protocols in schools and the resulting absences, are completely disproportionate to the proclaimed benefits of indiscriminate mass testing. The president of the Royal College of Paediatrics and Child Health was quite correct when she said last year that testing in schools was causing unnecessary chaos.’
You can find information about the APPG and its membership here and here.
No question the vaccines increase your susceptibility to COVID. What else do they do?
By Meryl Nass, MD | February 3, 2022

https://www.publichealthscotland.scot/media/11404/22-02-02-covid19-winter_publication_report.pdf
If you live in Scotland, a small country, the government, with its NHS, is like Santa: it knows if you’ve been bad or good. Scotland has 5.5 million residents. Over 5 million of them are listed in Scotland’s report of cases, above. The rest are kids too young for the vaccine. Sadly for Scots, 80% went along with the jab. It didn’t help them. And you can’t dispute these numbers: look at the narrow confidence intervals.
So now we know the jabbed get more COVID. What we suspect is that they also get more heart attacks, strokes, blood clots, autoimmune diseases and myocarditis. Will Scotland release those data, ever?
Am I immune to Omicron if I have already become infected with the Delta variant?
Q&A #12 with Geert Vanden Bossche | February 3, 2022
Question
“Those who became infected with the Delta variant are therefore not immune to the Omicron,” says Frank Vandenbroucke, Minister of Public Health Belgium. Is this correct? Will my T cells then not recognize the coronavirus? Or will my antibodies not protect me? Or maybe I will be infected asymptomatically and thus not get sick and then this is equivalent to “after vaccination”?
Answer
When you get infected with another variant there is always a chance that you will get sick. However, if you are in good health, the chance that SARS-CoV-2 will make you seriously ill is negligible. We owe this to our innate immunity which – especially in young people – is the first line of defense to clean up and eliminate large amounts of the virus (vacuum cleaner!). Young people, but even all healthy people who are in excellent health (e.g. no excess weight and regular exercise / sport), will often not even get sick or at best develop some vague, mild symptoms. If the first line of defense is broken, then our acquired immune system rushes to the rescue whereby our T cells ensure that the sick, virus-infected cells are eliminated. This allows us to recover from illness.
But whenever our innate immune system is exposed and eliminates the virus (with or without the help of the acquired immune system) it also immediately learns to recognize the virus better in the future. While it continues to recognize all SARS-CoV-2 variants (and even all CoVs), it now does so with more efficiency/affinity. This phenomenon is called “training” of the innate immune system. It is a form of adaptive immunity caused by epigenetic changes that effect a reprogramming of immune cells that secrete innate antibodies. That is, with subsequent exposure to the virus, there is an increasing chance that that person will develop an asymptomatic infection and actually not get sick at all, even if the virus undergoes antigenic drift (antigenic drift). If the virus undergoes an antigenic shift (i.e., severe change due to multiple mutations as in the case of Omicron), then the innate immunity will have to train again for a while before being able to withstand an infection with such a variant without giving rise to illness.
A pandemic is of course an excellent opportunity to train the innate immune system against SARS-CoV-2. However, it also means that if a variant with an antigenic shift (e.g. Omicron) dominates, more people may become ill anyway and within a short period of time the virus will be under pressure due to the induced natural antibodies, which are not able to suppress the virus at high infection pressure. Reducing the infection pressure is possible via (one-time) antiviral chemoprophylaxis. On the contrary, continued vaccination will increase the immune pressure and ensure that the vicious circle of the pandemic is maintained.
Thus, trained innate immunity to SARS-CoV-2 is not equivalent to COVID-19 vaccination but is superior because
- It is effective against all variants
- It has a sterilizing effect in contrast to vaccine antibodies
- Because of its non-varying character it does not lead to the selection of more infectious or resistant variants.
In other words, it benefits both individual and public health. It is the only way to acquire group immunity (independent of the circulating SARS-CoV-2 variant) and thus to move the pandemic into the endemic phase.
These 5 Studies Reveal a Disturbing Trend — Researchers Presenting Conclusions That Don’t Match the Data
By Josh Mitteldorf, Ph.D. and Madhava Setty, M.D. | The Defender | February 2, 2022
It was January 2020, the very beginning of COVID, when news articles began appearing that connected the genetics of the virus with gain-of-function research on bat coronaviruses at the Wuhan Institute of Virology.
These speculations were put to rest by an authoritative statement in the prestigious journal Nature Medicine, echoed by a summary in Science and an unusual affidavit in the Lancet signed by an impressive list of prominent scientists.
The message in the Nature Medicine article was dispositive: “Our analyses clearly show that SARS-CoV-2 is not a laboratory construct or a purposefully manipulated virus.”
But where was the support for this confident conclusion in the article itself?
The 2,200-word article in Nature Medicine (Anderson, et al) contained a lot of natural history and sociological speculation, but only one tepid argument against laboratory origin: that the virus’s spike protein was not a perfect fit to the human ACE-2 receptor.
The authors expressed confidence that any genetic engineers would certainly have computer-optimized the virus in this regard, and since the virus was not so optimized, it could not have come from a laboratory. That was the full content of their argument.
Most readers, even most scientists, take in the executive summary of an article and do not wade through the technical details. But for careful readers of the article, there was a stark disconnect between the Cliff Notes and the novel, between the article’s succinct (and specious) conclusion and its detailed scientific content.
This was the beginning of a new practice in the write-up of medical research. Recent revelations in the Fauci/Collins emails shed light on the origins of this tactic and the motives behind it.
In the past, if a company wanted, for example, to make a drug look more effective than it really was, it would choose a statistical technique that masked its downside, or it would tamper with the data.
What companies would not do, in the past, was describe the results of a statistical analysis that proves X is false, then publish it with an Abstract that claims X is true.
But this strange practice has become more common in the last two years. Academic papers are being published in which the abstract, the discussion section and even the title flatly contradict the content within.
Why is this happening? There are at least three possibilities:
- The authors cannot understand their own data.
- The authors are being impelled by the editorial staff to arrive at conclusions that match the ascendant narrative.
- The authors and editors realize the only way to get their results into publication is to avoid a censorship net that gets activated by any statement critical of vaccination efficacy or safety.
Before reaching any conclusions, let’s take a closer look at some examples of this troubling phenomenon arising in what should be the foundation of what is known: published scientific data.
In this article, we present five different published studies. Each to varying degrees exemplifies a disconnect between the data and the conclusions.
Example 1: ‘Phase I Study of High-Dose L-Methylfolate in updates Combination with Temozolomide and Bevacizumab in Recurrent IDH Wild-Type High-Grade Glioma’
This example is unrelated to the pandemic, but it typifies a common practice in the pharma-dominated world of medical research. If a remedy is cheap and out of patent, there is no one motivated to study its efficacy.
But research practice has gone well beyond neglect. In fact, investigators are skewing statistics to make cheap, effective treatments look ineffective if they are in competition with expensive pharma products.
This is ridiculously easy to do — all it requires is incompetence. Using the wrong statistical test, using a weak test when a stronger one applies — or just about any mistake in parsing the data — is far more likely to make compelling data appear random than the opposite.
Is it always incompetence? Or is it more often a well-thought-out deception that uses seemingly erudite analysis to lead the undiscerning reader into believing the wrong conclusion?
In the case of this article, a simple B vitamin (L-Methylfolate) was shown to double the life expectancy of 6 out of 14 brain cancer patients who received it, while showing no benefit (and no harm) to the other half of the patients.

The purple jagged line extending out to the right represents 40% of patients who lived dramatically longer when treated with L-Methylfolate (LMF).
The abstract reports that “LMF-treated patients had median overall survival of 9.5 months [95% confidence interval (CI), 9.1–35.4] comparable with bevacizumab historical control 8.6 months (95% CI, 6.8–10.8).”
The increase in median survival time is just a few months and not statistically significant. But the average survival time of the folate-treated group was more than double, and the difference was statistically significant (by my calculation, not in the article).
But the average is what is more commonly reported, and most readers don’t understand the difference between average and median.
The longest surviving patient on the B vitamin was still alive at the end of the study (3.5 years) when every one of the patients treated only with traditional chemo was dead before 1.5 years.
There were three different dosages in the study, (30, 60, 90 mg) and it was not reported whether the longest-living patients were receiving the highest dosages.
This is, in fact, a hugely promising pilot study about treating a common, fatal cancer with a simple vitamin. If it were an expensive chemotherapy drug instead of a cheap vitamin, you can be sure it would have been hailed as a breakthrough.
But this study will not create much excitement, and few oncologists will even know to prescribe methylfolate for their glioma patients.
Example 2: ‘Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons’
Earlier this year, MacLeod et al used data from a prominent Centers for Disease Control and Prevention (CDC) study to calculate that for women in their first trimester, the rate of miscarriage following administration of an mRNA COVID vaccine was an alarming 82%.
On Jan. 7, the CDC released a report designed to dispel our misgivings about vaccinating pregnant women. Its conclusions were unequivocal:
“These data support the safety of COVID-19 vaccination during pregnancy. CDC recommends COVID-19 vaccination for women who are pregnant, recently pregnant, who are trying to become pregnant now, or who might become pregnant in the future.”
The Defender reported on the numerous flaws in this study. The most egregious deficiency was the dearth of pregnant women in the study who were vaccinated early in their pregnancy (less than 2%).
The authors admit their study could not quantify the risk of vaccine exposure in the first trimester: “First trimester vaccinations are not included in analyses stratified by trimester because few exposures occurred…”
How then can they recommend COVID vaccination for women who are “recently pregnant” if their analyses excluded women in their first trimester?
This report serves a purpose. People who read it superficially will find the reported results reassuring — including front-line doctors who don’t have time to evaluate the research critically.
The CDC chose to paint over troubling safety concerns with reassuring words that are unsupported by clear science.
Example 3: ‘Public Health Scotland COVID-19 & Winter Statistical Report’
There is a section of this report comparing vaccinated and unvaccinated rates of disease, preceded by a warning to the reader not to take the data at face value.
“PLEASE READ BEFORE REVIEWING THE FOLLOWING TABLES AND FIGURES There is a large risk of misinterpretation of the data presented in this section due to the complexities of vaccination data …”
The data the authors don’t want us to misinterpret say that people who have been vaccinated with one shot or three shots are 50% more likely to contract COVID-19 compared to people who are unvaccinated.
People who receive two shots are more than twice as likely to contract COVID-19. This is according to the authors’ own method of calculating age-standardized disease rates.

The authors emphasize it’s not about case numbers — it’s about severe outcomes, hospitalizations and deaths:
“Evidence suggests the COVID-19 vaccines are 90% effective at preventing a severe outcome of COVID-19. COVID-19 hospitalizations and deaths are strongly driven by older age, with most deaths occurring in those over 70 years old and having multiple other illnesses. But overall, you are less likely to be hospitalized if you are vaccinated with a booster.”
What data are they talking about? Here are results from their own data table:
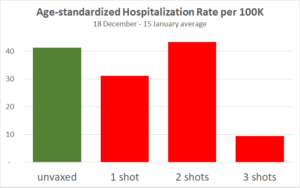
The only substantial reduction is from people who received the third shot, which has only recently been available in Scotland. But for the three-shot cohort only, vaccination effectiveness is declining over the four weeks.
This adds to previous evidence that protection from the vaccine is short-lived, and each injection provides a shorter window of protection than the previous one. Also, note the hospitalization statistics may have been gamed.
Since the publication of this article, England but not Scotland has backed off requirements for vaccination IDs.
Example 4: ‘Clinically Suspected Myocarditis Temporally Related to COVID-19 Vaccination in Adolescents and Young Adults’
Myocarditis, or inflammation of the heart, is a severe and life-shortening disease. It is virtually unknown in young people, but it is a recognized side effect of the COVID vaccines, especially in boys and young men.
This article summarizes the experience of 139 young patients (ages 12 to 20) who were hospitalized for myocarditis following vaccination.
19% of them were taken into intensive care.
Two required infusions of pressors and inotropes (potent intravenous drugs used to raise critically low blood pressure).
Every patient had an elevated Troponin I level. Troponin is an enzyme specific to cardiac myocytes. Levels above 0.4 ng/ml are strongly suggestive of heart damage. These young patients had a median Troponin I level of 8.12 ng/ml — over 20 times greater than the levels found in people suffering heart attacks.
“Conclusions: Most cases of suspected COVID-19 vaccine myocarditis occurring in persons <21 years have a mild clinical course with rapid resolution of symptoms.”
“Mild clinical course” — We suppose this refers to the 81% who did not go to the ICU or the fact that none died or required ECMO (Extracorporeal Membrane Oxygenation, a desperate means to keep the body oxygenated when a patient’s heart or lungs have completely failed).
In any case, every single person in this study was hospitalized. When does a “mild clinical course” require hospitalization for a two-day median length of stay?
“Rapid resolution of symptoms” — How would anyone know this? Myocarditis in older patients doubles the probability of death for the long term.
We don’t know what it will do to young boys in the long term, especially since every patient had some damage to their heart as evidenced by significantly abnormal troponin levels. And we don’t fully understand the mechanism by which the vaccines cause myocarditis.
Example 5: ‘Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States’
This is the title of a paper by two statisticians from the Harvard School of Public Health, published on Sept. 30, 2021, in the European Journal of Epidemiology.
The title makes the important claim that there is no public health benefit from vaccination. COVID-19 is spreading at the same rate in different populations, unrelated to whether the population is mostly vaccinated or mostly unvaccinated.
It’s a powerful counterpoint to the ubiquitous demand that more people should undergo vaccination for the sake of their community.
The paper completely undermines the requirement of vaccination to attend meetings, concerts, theater and other public gatherings. It says there is no legitimacy to the creeping government vaccine mandates for travel.

But the data in the paper don’t show that vaccination and spread of COVID-19 are “unrelated.” In fact, there is a paradoxical relationship, an insidious relationship: The more vaccinated countries had more new COVID-19 cases (during the week when the survey was conducted). The correlation is significant (p=0.04).
Still, the authors conclude by explicitly recommending propagandizing of the unvaccinated: “In summary, even as efforts should be made to encourage populations to get vaccinated it should be done so with humility and respect.”
It may sometimes be wrong to promote flawed health policy, but apparently, it’s a good thing, so long as it is done with humility and respect.
Why would these researchers take the trouble to publish data that is so damning to the vaccine narrative, and then pull punches in the title and in the conclusions?
Are we to assume that these authors who have assiduously extracted data from 68 different countries and nearly 3,000 U.S. counties were unable to notice their meticulous scatter plot unequivocally demonstrates high vaccination uptake is associated with higher (NOT lower) prevalence of COVID-19?
This seems to be a different case from the first example, where shills for the pharmaceutical industry set out to create a deceptive narrative. We think it’s probable that in this case, soft-pedaling the implications of these glaring data may not have been the authors’ choice, but rather a decision by the journal’s editors.
We know from personal experience how difficult it is to get an article through peer review at most “reputable” medical journals when the results are out of sync with the COVID narrative.
It may well be that these authors fought hard to get their subversive message into print, and in order to get past peer review, they softened the language, especially, the title.
Conclusions
The church was once the most trusted institution in Europe. Then the bishops started selling indulgences — a kind of get-out-of-hell-free pass for rich sinners.
Today the most trusted institution is science.

Sources: Gallup, Gallup, Gallup, Pew
This is true despite the fact that scientists are human, subject to error and to corruption.
Medical journals have become financially dependent on their advertisers, which are almost exclusively the pharmaceutical giants.
For several decades now, the “Church of Science” has been selling indulgences. With enough money, you could buy a scientific study that says what you want it to say.
Darell Huff’s book, “How to Lie with Statistics,” first published in 1954, remains the all-time best-seller in its field.
Recently, Gerald Posner documented the way in which the pharmaceutical industry has used its profits to affect science at every level, from medical researchers to journal editors to government regulatory agencies to the journalists who interpret science for the public.
Pressure is being placed on independent researchers by the journal editors and peer reviewers, many of whom have ties to Big Pharma. Valid studies, honestly reported, can be rejected for publication if they send a message that threatens corporate profits.
In the age of COVID, we see three reasons that an article’s conclusions might become detached from its statistical findings:
- Scientists have suddenly abandoned basic logic and reason. This is an implausible explanation because, as has been demonstrated above, these examples demonstrate diligence in gathering data. There is no reason why they would abandon diligence in arriving at reasonable conclusions.
- Shortcuts by pharmaceutical companies and their shills in academia. Rigging clinical trials the old-fashioned way is expensive and time-consuming. It’s also uncertain. Sometimes the truth rears its head even if a study is designed to conceal it. Even a study that is designed to fail might succeed when the inconvenient truths are sufficiently stubborn. How much easier it is to report the results and then tack on an abstract and a discussion section that say what you want to say, regardless of the data tables in the body of the article!
- Scientist authors are well aware of the pernicious censorship in scientific publication that has emerged in recent days. This is perhaps the most intriguing possibility. If researchers behind the study have some prestige and some influence, they still may find they have to soften their rhetoric in order to pass peer review. However, what we are witnessing today is more than a tendency to be “diplomatic” in their choice of words. What does it mean when their conclusions do not match the findings? Are they trying to tell us that they are gagged? Are they silently screaming at us to look at the data and not their interpretation of them?
The Nature Medicine article on the origins of the SARS-CoV-2 virus (reviewed first) seems to be an example of researcher corruption.
The article in the European Journal of Epidemiology (Example 5), which relates vaccination rates to COVID prevalence, is more likely an example of corruption by journal editors and peer reviewers.
In this instance, the data and conclusions are so disparate that it begs us to reconsider the cynical position that all scientists have been corrupted. Is there a better way for conscientious scientists to signal their community that they are being censored than by compiling solid data that tell a compelling story and then arriving at a nonsensical conclusion? Are they imploring us to read between the lines?
For the other four articles reviewed above, we leave it to your judgment — how do you think the conclusions came to be so disconnected from the statistical findings in these same articles?
Obviously, this blatant distortion of scientific write-ups is not a long-range strategy, but the world is moving fast, and people who count on their ability to shape scientific conclusions to their financial interests will be successful for long enough to do a great deal of mischief.
What will be the damage to the credibility of science when the dust clears?
Josh Mitteldorf, Ph.D., has a background in theoretical physics. Since the 1990s, he is best known for his contributions to the biology of aging, including many articles and two books.
Madhava Setty, M.D. is senior science editor for The Defender.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
How Many Pregnant Women Have Actually Died of COVID-19?
The Daily Sceptic | February 3, 2022
There follows a guest post by a Daily Sceptic reader, who wishes to remain anonymous, who, being pregnant, was following closely the advice and studies concerning pregnant women. However, her own analysis of the reports on the deaths of pregnant women with COVID-19 suggested that the alarming statistics about Covid in pregnancy she was being provided with did not stack up.
As a pregnant woman, I have been following advice and studies that concern this group closely. Unfortunately, it is becoming increasingly difficult to find any balanced information amongst the blatant propaganda. I am so sick of being told at every turn that ICU is full of unvaccinated pregnant women. Below is an example of the stuff that gets shared online by my local maternity team.

So I thought I would look at what stats MBRRACE had released lately. They have two reports that caught my eye in particular: one on maternal Covid deaths March-May 2020 (10 women) and another covering the period June 2020-March 2021 (17 women).
Despite being such a small group of people, I feel that each case is a fascinating story that paints a dramatically different picture to that portrayed by the media and the NHS. Here are some points that stood out to me from each report
March-May 2020 (10 deaths)
- None of the women who died received any actual treatment, just support.
- Three of the ten women died because they were too scared to go to hospital.
- Four women died of suicide and not being able to access help was a factor (I don’t think they were included in the ten deaths, but the insinuation is that Covid restrictions contributed to their deaths).
- Two women were murdered by their partners, with health services already knowing they were at risk (again, I don’t think they were included in the ten, but the insinuation about restrictions is there again).
- The quote “pregnancy [sic] and postpartum women do not appear to be at higher risk of severe COVID-19 than non-pregnant women” seems telling.
- Only two women were classified as having received “good care”.
June 2020-March 2021 (17 deaths)
- Three women did not even have Covid but died as a result of the side effects of restrictions.
- Four women tested positive but died of unrelated causes – two of these women received poor care because of their Covid status.
- 60% of the women who actually died from Covid were obese and a further 20% were overweight.
- 50% had pre-existing mental health conditions (personally I believe that this both prevents women from being able to speak up for themselves and creates a stigma that they are ‘difficult patients’).
- One woman died at home of a urinary tract infection because no translator was available for her telephone appointment.
- Four women died because they were too scared to go to hospital – one of these women sought no antenatal care at all and died after giving birth at home.
- One woman died after being given painkillers for backache – she was only seen remotely by a GP so he or she couldn’t see she was both heavily pregnant and had sepsis.
- Another woman died of sepsis from a miscarriage because doctors assumed she just had (asymptomatic) Covid.
- A woman died of obvious kidney/liver problems shortly after birth because again, doctors bizarrely assumed she was actually suffering from Covid following a positive routine test.
- 90% of the women who died had “care” that was not managed by the RCOG guidelines.
- One woman was not given treatment despite poor clinical indications, as she did not “look sick”.
- Three women who were very poorly and were considered for ECMO were denied this despite not having any contraindications.
- One woman died from a pulmonary embolism at home after her GP’s online triage system did not recognise either her Covid status or recent pregnancy as risk factors and didn’t give her an urgent appointment.
- Only 10% of the women received “good care”, and in 70% improvements in care may have meant they survived.
The reports are heartbreaking and I do not wish to diminish the pain that these women’s families must be suffering, but it is abundantly clear that very few of these women died from actual Covid – many appear to be victims of the restrictions and fear – and the handful that did had significant confounding factors.
Omicron did not “slam labor markets.” Covid policy did. And it was entirely avoidable.
el gato malo – bad cattitude – february 2, 2022
CNBC would appear to wish to have us believe that the drop in jobs was caused by “the variant” as though this was some act of nature instead of an act of government.
it is not. this is a deeply misleading framing intended to obscure causality rather than reveal it.

it’s way past the point where even these people could possibly be this ignorant of baseline reality.
this is, instead, a clear bet that you are.
this drop in jobs was not “unexpected” at least not by anyone paying attention. this is the direct, proximate effect of imposing vaccine mandates as a precondition to work. the OSHA mandate fell, but the federal mandate for contractors did not. thousands of mandates for health care workers imposed by states and hospital systems did not. requirements for many truckers and teachers and hospitality workers did not. many employers went ahead and imposed these anyway. they waited until after the holidays, but here we are.

we also cut off the flow of travel and of patronage. we closed businesses (again). we limited capacity. we mandated vaccination as a pre-requisite for going out to eat or staying in hotels. and like clockwork, it choked off the flow of tourists and local patrons alike because people HATE this and hate playing officious games and pretending that the made up “covid physics” of “wear your mask to the table then take it off when you sit” make any sense at all. they hate having some hostess demand “their papers.” maybe not everyone does, but enough people do that it has savaged businesses.
we’re living though needless damage to no useful effect at all.
this is NOT the virus.
it’s the predictable and unavoidable output of deeply stupid public health policy.
the damage since this began has been acute and severe. “2 weeks to flatten the curve” was, as many of us were screaming right from the beginning, the commencement of the nastiest economic hit to jobs and small business per unit time in US history and probably in global history.
in the US, we dropped 20 million jobs in 2 months. that is so far outside any precedent it’s staggering.
the entire 2008 recession and financial crisis led to a job reduction of 8 million over 24 months…
and we have NOT recovered to previous levels. current job levels are about the same as jan 2018.
they are 4 million jobs below the level from early 2020.
they are 9 million below where we would be had job growth continued as before. (added in red)
might job growth have slowed anyway? yes, perhaps, but this gives us a set of fairly reasonable bookends to assess the scope of what this has cost in terms of private nonfarm employment.
we’re 4-9 million jobs short of where we would likely have been without this public health response and claims that the US jobs market looks strong are pretty iffy.
(keep in mind that the unemployment rate drops when people drop out of the labor force/stop looking for work. it does not mean they found jobs.)

“but it was the virus! most of this would have happened anyway!”
this is a predictable claim, but seems out of step with reality. fortunately, we have a control group.
compare this damage to a place like sweden who did not lock down and freak out.
sweden’s payrolls figure is much more seasonally variable than the US, but looking through this seeming cardiac rhythm the overall difference in outcome is unavoidably obvious.
the dip was extremely minor in comparison. it was extremely short in comparison. and, despite the effects of many neighbors locking down, tourism and travel dropping, and global supply chain issues, their jobs figures currently look indistinguishable from 2019 and pre pandemic 2020.
employment today is higher than dec 2019 or jan 2020.
the US is nowhere close.

it’s really very simple: places that locked down harder got no better outcomes on covid. but they got much, much worse outcomes on economic and societal damage.
this was all known and knowable.
the base prior for pandemics was to never, never do this.
it’s what the guidelines said.
i did a ton of work on this back in the twitter days. it was obvious right from the start that drops in google mobility data (measuring actual human behavior from cell phone tracking) had zero effect on bending any epidemiological curve. it was clearly doing nothing at all. this was already glaring. and so was the harm.
i pulled this data from BLS way back in 2020:
it was more than a little apparent that it was predominantly politics and policy, not covid putting people out of work.
the no lockdown states were back at baseline by the fall.

the relationship was not subtle:

at this stage of the game and with this much clear data at one’s disposal, it’s pretty absurd to still be trying to blame upon a virus that which’s fault lies with public health response.
to do so is neither economically or epidemiologically accurate.
these are choices, not happenstance.
and it’s long past time to be making different ones.
Major Study Says Lockdowns Did More Harm Than Good – Well D’uh!

By Richie Allen | February 3, 2022
Lockdowns did far more harm than good. A new study published by Johns Hopkins University, in the US, Lund University, in Sweden and Denmark’s Centre for Political Studies found that lockdowns prevented just 0.2 per cent of deaths compared to letting people get on with their lives.
According to The Telegraph :
Researchers from Johns Hopkins University, in the US, Lund University, in Sweden and the Centre for Political Studies, in Denmark, said the costs to society far outweighed the benefits and called for lockdown to be “rejected out of hand” as a future pandemic policy.
The team even found that some lockdown measures may have increased deaths by stopping access to outdoor space, “pushing people to meet at less safe places” while isolating infected people indoors, where they could pass the virus on to family members and housemates.
“We do find some evidence that limiting gatherings was counterproductive and increased Covid-19 mortality,” the authors concluded. “Often, lockdowns have limited people’s access to safe outdoor places such as beaches, parks, and zoos, or included outdoor mask mandates or strict outdoor gathering restrictions, pushing people to meet at less safe indoor places.”
This isn’t earth-shattering. In March 2020, when the first lockdown was implemented, many doctors and healthcare workers warned that locking down would be ineffective against an airborne virus and that the measure would be devastating for public health.
They weren’t just ignored, they were banned by the mainstream media. I featured many of them on The Richie Allen Show.
Look, the government and its scientific advisers knew that lockdowns would be ineffective and dangerous. The policy wasn’t pursued in the interest of public health, rather it was implemented in the interest of public coercion.
The events of the last 22 months have nothing to do with a virus and all to do with mRNA drugs. They grossly exaggerated the threat of covid-19 and forced the world into lockdown after lockdown, to push their experimental jabs.
The major new study on the ineffectiveness and danger of lockdowns concludes thus:
“Lockdowns during the initial phase of the Covid-19 pandemic have had devastating effects. They have contributed to reducing economic activity, raising unemployment, reducing schooling, causing political unrest, contributing to domestic violence and undermining liberal democracy.
These costs to society must be compared to the benefits of lockdowns, which our meta-analysis has shown are marginal at best. Such a standard benefit-cost calculation leads to a strong conclusion: lockdowns should be rejected out of hand as a pandemic policy instrument.”
Costa Rica Anti-Vaccine group enters hospital by force
The Tico Times | January 27, 2022
In a chaotic, and at times violent confrontation, a group of anti-vaccine advocates forcibly entered a hospital in Heredia as part of their protest and to remove a child with Covid-19. Six protestors were arrested at the scene. Police later arrested another person after he posted threatening comments online against government officials enforcing Covid-19 health restrictions.
The confrontation arose from a situation where, reportedly, a six year old unvaccinated patient was admitted for one issue and then was discovered to have tested positive for Covid-19.
Hospital officials were reluctant to release the child back into the community while infectious, at the same time the patient’s parents, both anti-vaccine advocates, claimed their child was being held “hostage” as hospital officials waited for guidance from the Ministry of Health.
A small, but hardline group organized online, reportedly initially to go to the hospital to physically remove the child themselves. Included in the group was a member of the National Assembly by the name of Diaz.
Security personnel and hospital employees confronted the protestors and scuffles ensued until police arrived and the “rescue mission” became a sit in. Hospital officials denounced the participants for putting patients at a crucial medical facility at risk for what they described as a political stunt. Prosecutors promised to take a hard line against any violent protestors that may have broken the law.
The Race Is On for an Omicron Jab
By Dr. Joseph Mercola | February 1, 2022
At this stage in the game, it’s apparent that the COVID jab no longer works. Many health officials and world leaders are even openly acknowledging that the COVID shots cannot end the pandemic and that we must learn to live with the virus.
A major driver for this U-turn in the pandemic narrative is the emergence of the Omicron variant which, by mid-January 2022, accounted for 99.5% of all COVID cases in the U.S.1
The infection, which is far milder than previous ones, is ripping through populations, leaving natural herd immunity in its wake. Despite that, vaccine makers are still hard at work to produce an Omicron-specific injection.2 Pfizer has promised to have one ready by March 2022.3
The question is why, seeing how by the time the shot is released, just about everybody will have been exposed. If natural herd immunity is already maxed out, what good could a “vaccine” possibly do?
‘Everyone’ Will Have Natural Immunity
As Dr. William Moss, executive director of the International Vaccine Access Center at the Johns Hopkins Bloomberg School of Public Health told CNBC,4 “An omicron-targeted vaccine was needed in December [2021]. It still could be valuable but I do think in many ways, it’s too late.”
Dr. Shaun Truelove, an infectious disease epidemiologist at Johns Hopkins Bloomberg School of Public Health and a member of a team of researchers who make COVID projections, agreed, saying, “Given how quickly this [variant] is happening, [the targeted vaccine] may not matter because everybody’s going to be infected.”5 Pfizer CEO Albert Bourla even admits he doesn’t know “whether or not the new vaccine is needed or how it could be used,” CNBC reports.
January 25, 2022, Pfizer and Moderna announced they’ve started enrolling adults, 18 to 55, for trials on an Omicron-specific jab in the U.S. and South Africa.6 Pfizer will evaluate safety, tolerability and immune response in 1,420 volunteers,7 some of whom will have received two doses while others will have received three already. A third cohort will be unvaccinated (although one wonders where they’ll get those from).
Moderna has also joined the pointless race to produce an Omicron booster,8 although it’s doubtful they’ll be able to produce one any faster than Pfizer.
Moderna CEO Stéphane Bancel told CNBC that a fourth COVID jab also may be on the horizon, “as the efficacy of boosters will likely decline over time.”9 It’s unclear what strain that fourth shot would target.
Israel Proves Failure of COVID Boosters
For a preview of what’s in store after third and fourth booster shots, all we have to do is look at Israel, where more than 250,000 fourth doses had already been given by early January 2022. According to CNBC:10
“Early data from Israel shows that a fourth dose does increase antibody levels, says Dr. David Hirschwerk, infectious disease specialist and medical director at Northwell Health’s North Shore University Hospital.”
What CNBC neglects to note is that, after the rollout of a fourth dose, Israel now has the highest COVID case rate per capita of any country in the world since the beginning of the pandemic.
Looking at a Reuters graph11 of Israel’s seven-day average case rate, something absolutely abnormal appears to have happened in mid-January 2022, as the line shoots straight upward, hitting an all-time high of 75,603 new infections per day on January 24, 2022.
This, despite 74% of the population having received at least one dose, 67% having received two doses, and 56% having received at least one booster, as of January 25, 2022.12
What Does It Mean To Be ‘Fully Vaxxed’?
While the pandemic narrative has recently shifted, and rather dramatically, with some leaders openly speaking out against boosters without getting canceled or censored, it seems clear that we’re not out of the woods yet when it comes to COVID shots.
Vaccine makers clearly aim to make the COVID shot, at bare minimum, an annual injection.13 In the meantime, the definition of what it means to be “fully vaccinated” against COVID keeps shifting. At the beginning of 2021, many people undoubtedly got their primary series (two shots of Pfizer or Moderna, or a single jab in the case of AstraZeneca and Janssen) thinking life would be easier that way.
Being “fully vaccinated,” they wouldn’t be inconvenienced by vaccine passport restrictions and mandates. Well, that fantasy only lasted a few months. Now, those who got the first required series find themselves in the unwelcome position of being among the “unvaccinated” again unless they submit to a third jab.
As explained by U.S. Centers for Disease Control and Prevention director Dr. Rochelle Walensky during a recent press briefing:14
“What we’re really working to do is pivot the language to make sure everyone is up to date with their COVID-19 vaccines as they personally could be, should be, based on when they got their last vaccine. If you’ve recently gotten your second dose but you’re not eligible for a booster, you’re up-to-date. If you’re eligible for a booster and you haven’t gotten it, you’re not up-to-date and you need to get your booster.”
It’s only a matter of time before those with three jabs will be “unvaccinated” unless they submit to a fourth, and so on, ad nauseum. An as-yet unanswered question is how many mRNA injections can a person survive?
Considering the injection causes your body to produce toxic spike protein in uncontrolled amounts, it seems reasonable to assume there’s a tolerance limit, although that limit may vary from person to person. There’s really no telling how many people are one shot away from a crippling side effect or sudden death.
Each Shot Degrades Your Immune System
As reported by The Exposé,15 January 22, 2022, government data from around the world suggest people who have received at least two shots are now showing signs of serious immune system degradation.
According to that report, data from Australia, the U.S., Canada, Scotland and England clearly show “that their vaccinated populations immune system capability has been decimated when compared to the not-vaccinated population.” For starters, Omicron cases are rising far more rapidly and readily among the fully jabbed and boosted than among the unvaxxed.
In Australia, the fully jabbed are 2.2 times more likely to catch COVID than the unvaccinated. “So, the vaccine passports holders are 2.2x more likely to spread COVID than the unvaxxed who are denied vaccine passports and locked up in detention centers,” The Exposé dryly notes.
Several studies have also shown the effectiveness of the jab wanes incredibly rapidly. And, disturbingly, it doesn’t peter out at zero. Immunity goes negative, meaning the fully vaxxed and boosted rapidly become MORE prone to COVID infection than they ever were before.
Negative Effectiveness Rates Found in Many Countries
In the U.S., a study16 on 780,225 U.S. veterans found the effectiveness of the jab dropped precipitously over six months:
- Janssen dropped from 86.4% effectiveness at the outset to 13.1% in the sixth month
- Moderna dropped from 89.2% to 58%
- Pfizer dropped from 86.9% to 43.3%
A Canadian study17 found vaccine effectiveness started declining sharply within as little as the second week after the second jab. By the sixth month after the second jab, the blood of 70% of nursing home residents had “very poor ability to neutralize the coronavirus infection in laboratory experiments.”
In the U.K., government data “show a clear linear fall-off in vaccine efficiency at an average rate of 4.8% per week for the over 18s,” The Exposé reports,18 and by the time you get past Week 9 after jab No. 2, effectiveness starts going negative.
“Doubly vaxxed (unboosted) people in the U.K. have now (as of January 2022) run right out of immune system efficiency against both Delta and Omicron when compared to unvaccinated people,” The Exposé writes. The question is whether or not there might be a point at which the immune system stops deteriorating. As of now, we don’t know.
Using data from five UK HSA COVID-19 Vaccine Surveillance Reports, The Exposé created the following graph, illustrating “the overall immune system performance among all age groups in England over the past five months.”

The Exposé explains:19
“What we can see from the above is that the immune system performance for adults aged between 18 and 59 has deteriorated to the worst levels yet since they were given the COVID-19 vaccine.
Whilst the immune system performance of everyone over the age of 60 has deteriorated dramatically following receipt of the booster shot, but not yet to the level seen between week 37 and week 40. The over 70’s have however seen the most dramatic fall in immune system performance between month 4 and month 5 alongside 18-29-year-olds.
The 55% boost to the immune systems of the over 80’s given by the boosters between month 3 and month 4 has all but deteriorated between month 4 and month 5. Their immune system is performing 1% better than it was in month 3 but still 54% worse than their unvaccinated counterparts.
The 73% boost to the immune systems of the 70-79-year-olds given by the boosters between month 3 and month 4 has also all but deteriorated between month 4 and month 5. Their immune system is performing 10% better than it was in month 3 but still 63% worse than their unvaccinated counterparts.
The minor boost however, given to the immune systems of everyone between the age of 30 and 59 by the boosters between month 3 and 4 has been completely decimated by the following month, whilst 18-29-year-olds have seen a 60% decline in their immune system performance between months 4 and 5.”
Are Double- and Triple-Jabbed People at Risk for VAIDS?
By now you may be wondering whether this negative effectiveness could be indicative of something far worse than just being more prone to Omicron infection. The Exposé20 believes the double- and triple-jabbed may actually have vaccine-acquired immunodeficiency syndrome or VAIDS, similar to AIDS.
While I think it’s still too early to come to a definitive conclusion, former Pfizer vice president Michael Yeadon has made a similar statement.21 In a December 6, 2021, article on americasfrontlinedoctors.org, Yeadon is quoted saying:22
“If immune erosion occurs after two doses and just a few months, how can we exclude the possibility that effects of an untested ‘booster’ will not erode more rapidly and to a greater extent?”
The article goes on to cite a Lancet preprint23 that compared outcomes among “vaccinated” and unvaccinated Swedes over the course of nine months. As in other studies, they found that protection against symptomatic COVID rapidly declined, and by six months’ post-jab, “some of the more vulnerable vaccinated groups were at greater risk than their unvaccinated peers.”
“Doctors are calling this phenomena in the repeatedly vaccinated ‘immune erosion’ or ‘acquired immune deficiency,’ accounting for elevated incidence of myocarditis and other post-vaccine illnesses that either affect them more rapidly, resulting in death, or more slowly, resulting in chronic illness,” the Frontline Doctors explain.24
The article also cites an August 2021 report from Scotland,25 which found those who had received the jab were 3.3 times more likely to die from COVID infection than the unvaccinated — a finding that certainly blows a huge hole in the claim that the jab prevents serious illness and death even if you do get symptomatic infection.
ICU Admissions Spike Among Vaxxed Immunocompromised Brits
The Daily Mail at the end of November 2021 also reported that weekly ICU admissions of “most vulnerable patients” had risen by 50% in the two preceding months, and that 1 in 28 ICU patients had conditions affecting their immune system. Blood cancer patients and organ transplant patients made up a bulk of this group.26
While the Daily Mail blamed the unusually high rate of admissions of immunocompromised patients on the government’s failure to roll out booster shots fast enough to counteract waning immunity, this is incredibly short-sighted. As noted by America’s Frontline Doctors, the shots are creating “vaccine addicts,” in the sense that their immune system won’t be able to ward off COVID without them. However, it’s still a losing venture, as each shot only worsens the immune erosion.
In the final analysis, it looks as though many may indeed end up being just one shot away from VAIDS as they continue to chase protection from an ever-mutating coronavirus.
The Daily Mail article tells the story of a transplant patient who was desperate to get his booster, knowing he was at high risk for COVID complications. It took three weeks, but he finally got his third shot. The very next day — THE NEXT DAY — he developed “a blinding headache, nausea and dizziness. A lateral flow test was positive and a follow-up PCR test confirmed that he had caught COVID.”
But rather than realizing he’s a victim of that third shot, the man is irrationally convinced that had he just gotten the third dose sooner, he wouldn’t have gotten COVID at all. Sadly, people like these will likely die from their “COVID jab addiction.” In closing, The Exposé writes:27
“Acquired immunodeficiency syndrome is a condition that leads to the loss of immune cells and leaves individuals susceptible to other infections and the development of certain types of cancers. In other words, it completely decimates the immune system.
Therefore, could we be seeing some new form of COVID-19 vaccine induced acquired immunodeficiency syndrome? Only time will tell, but judging by the current figures it looks like we will only need to wait a matter of weeks to find out.”
Sources and References
- 1 CDC COVID Data Tracker Data for 1/9/2022-1/15/2022
- 2, 4, 5, 9, 10 CNBC January 10, 2022
- 3 New York Post January 25, 2022
- 6 ZeroHedge January 25, 2022
- 7 CNN January 25, 2022
- 8 CNBC November 28, 2021
- 11 Reuters COVID tracker Israel as of January 24, 2022 (Archived)
- 12 New York Times COVID Vaccination Tracker, Israeli data as of January 25, 2022 (Archived)
- 13 Reuters January 22, 2022
- 14 Axios January 24, 2022
- 15, 18, 19, 20, 27 The Expose January 22, 2022
- 16 Science November 4, 2021; 375(6578): 331-336
- 17 Medical Express September 2, 2021
- 21, 22, 24 Americas Frontline Doctors December 6, 2021
- 23 Lancet Preprint October 25, 2021
- 25 Public Health Scotland August 2, 2021
- 26 Daily Mail November 20, 2021
“Medical boards get pushback as they try to punish doctors for Covid misinformation”/ Politico
Meryl Nass, MD | February 1, 2022
The medical boards are getting in trouble for swallowing the malarky from the Federation of State Medical Boards and other bloated medical nonprofits. These organizations somehow worked in concert during the second half of 2021 to terrorize doctors who failed to hew to the current medical narrative. Presumably they got paid to do so. Presumably those trying to cement control over Americans felt it necessary to act extrajudicially to use threats to enforce only ‘approved’ medical speech.
The clueless Medical Licensing Board members, a mix of medical professionals and citizens, rely on attorneys on their staff to get the legal details right. Instead, the attorneys never told the Board members that none of them them had any authority to legislate new crimes, that misinformation is not a crime under US law, that Freedom of Speech is a foundational principle of law that may not be abrogated, ever, especially not by any state or state agency.
A few Medical Boards, including my own, got too far out over their skis, and now it is starting to sink in what they have done. Their legislators are saying, “Whoa, Nellie! You guys were supposed to protect the citizens from drunkards, druggies and rapists. We never asked you to trash the 1st and 14th Amendments.”
From Politico,
… the responses from some medical boards and state officials have been stymied by political backlash. States like Tennessee and North Dakota, for example, have restricted state medical boards’ powers. And now legislators in 10 other states — including Florida and South Carolina — have introduced similar measures.
Some state boards also lack the legal tools to discipline doctors for sharing unreliable information via social media. They believe the precedents in their states for unprofessional or unethical behavior more narrowly apply to actions or speech made directly to patients under their care…
Meantime, my license remains suspended while the Maine Medical Licensing Board hopes against hope that if they keep fishing, they might someday be able to find a crime with which to charge me. It’s your taxpayer dollars they are spending to destroy my career and silence my voice. They think it is free money. What do you think?
Justice For the Hyde Park One

By Andrew Rootsey | The Daily Sceptic | February 1, 2022
As you may recall, we secured Debbie’s acquittal at Cheltenham Magistrates Court on the December 20th 2021 for offences relating to organising/being involved in organising a gathering of more than 30 people during a period of national lockdown or alternatively for participating in the gathering.
The relevant gathering was a protest held in Stratford Park in Stroud in November 2020 against the restrictions imposed on the British public under the Coronavirus Regulations. The protest was called the ‘Freedom Rally’ and was attended by more than 50 people.
The Stroud ‘Freedom Rally’ was held two days into the second national lockdown and therefore at the time it was illegal to organise a gathering of more than 30 people or to meet in groups of more than two people. A conviction would have left her liable for a £10,000 fine.
Ms. Hicks was acquitted of both offences after the court accepted our argument that her arrest and prosecution was a disproportionate interference with her human rights – namely the rights to freedom of expression and freedom of assembly, given that she was engaging in a legitimate protest.
The court found that Ms. Hicks had organised the ‘Freedom Rally’ and had breached the Coronavirus Regulations in force at the time by doing so. However, she had a reasonable excuse because she was attending a legitimate, peaceful and well-organised protest. The officers on the ground at the protest had been labouring under a misapprehension of the law – that protesting was not lawful under the Regulations – and were essentially imposing a blanket ban on protesting. Therefore, their actions in arresting her were not rational or proportionate.
In complete contrast – and a perfect example of how this contentious piece of legislation is flawed and open to misinterpretation – on the November 16th 2021 the City of London Magistrates Court convicted Debbie of breaching similar coronavirus regulations by protesting in Hyde Park against the imposition of lockdown restrictions during the pandemic. The District Judge in this case found that Debbie did not have a ‘reasonable excuse’ for protesting and found that the interference with her Human Rights was proportionate. Debbie was convicted and sentenced to a financial penalty.
The case raises important issues on freedom of expression and assembly, as well as the chilling of the right to protest. We wish to appeal this case to the High Court in order for the High Court to settle the important questions of law raised.
A fundamental consideration for the High Court is the ambiguity of the right to protest during the Coronavirus pandemic during periods of national lockdown and the operation of the ‘reasonable excuse’ jurisdiction in this regard.
The Government has made it clear, as have the courts, including in Debbie’s case before the Cheltenham Magistrates Court, that protesting during the Coronavirus pandemic was never illegal. Yet that was not always clear from the Coronavirus regulations nor was it the understanding of most police officers. How the reasonable excuse defence is to operate in these circumstances requires clarity and we are confident that the High Court will settle the issue in our favour and set a precedent for future cases and those seeking to appeal against their own convictions.
Debbie Hicks is probably best known for filming within the Gloucester Royal Hospital in December 2020 during Tier 3 restrictions. Debbie did so, exercising her freedom of expression, in order to highlight that Government restrictions were having a devastating effect upon access to healthcare across the board and to investigate mainstream media reports that hospitals were overflowing with patients.
Despite her efforts to avoid confrontation, she was challenged at the hospital by two employees. During the exchange, which lasted less than a minute, Debbie did not film the staff members. She explained the purpose of her visit and her views as to the provision of NHS services during lockdown. Staff members took offence at her comments and subsequently made a complaint to the police. Debbie immediately left the hospital voluntarily and was subsequently arrested at her home in front of her family and charged with using abusive, threatening or disorderly words or behaviour.
Debbie was not at the hospital deliberately seeking an encounter with staff. She has in the past been a vociferous supporter of the NHS and has supported NHS staff in respect of vaccine mandates.
In connection with this episode, Debbie stood trial for an offence under Section 5 of Public Order Act on January 6th 2022 and having adjourned the case in order to hand down his judgement the District Judge convicted Debbie of a S5 Public Order Act offence on January 19th 2022 at Cirencester Magistrates Court.
We wish to appeal this conviction as well and ask that the High Court settle this case on the basis that the District Judge was wrong in law to convict Debbie of this offence. We are firmly of the view that the Prosecution case simply did not cross the threshold of what constitutes abusive, threatening or disorderly words or behaviour. The District Judge’s analysis was flawed and did not properly interpret Supreme Court authorities nor give appropriate weight to Debbie’s rights of freedom of expression and assembly as enshrined in the European Convention for Human Rights, nor give appropriate weight to the political nature of Debbie’s views when the case law makes clear political freedom of expression should be given special protection.
Debbie is trying to raise £10,000 to take both cases to the High Court. She hopes that those who continue to believe in freedom of speech and the the right to protest will continue to support her. Our hope is that if we can get these convictions overturned, it will set a legal precedent for those convicted of similar offences and who may face prosecution in the future.
Debbie needs to raise funds in order to pay her legal costs and any help is hugely appreciated. Her fundraiser can be found here.
Andrew Rootsey is a solicitor at Murray Hughman.
Featured Video
Deep Dive Intel Briefing 6/20/2026 Lt Col Daniel Davis
or go to
Aletho News Archives – Video-Images
From the Archives
As Hillary Clinton kisses up to Henry Kissinger, RT looks at 4 of his most heinous acts
RT | September 3, 2016
… While Clinton retains the ultimate warmongering seal, RT examines some of Kissinger’s most memorable acts… Read full article
Blog Roll
 Aletho News
Aletho News- Moderna’s mRNA Flu Vaccine Gets Unanimous Thumbs-Up Despite Risks, Low Efficacy
- UK Speech Regulator’s Telegram Questions Point Toward Private Chats
- Cuban FM blasts Rubio for ‘chronically lying’ about US fuel blockade
- Al-Jazeera demands punishment for Israeli officials following latest assassination of cameraman
- Iran opens hundreds of legal cases over US, Israeli aggression: Prosecutor general
- Iran delegation protests Trump’s threat at Switzerland talks, weighs ‘proper’ response: Source
- Terms of US capitulation to Iran presage new era for the region
- Strategic Oil Reserve Nears Collapse… US Must Choose: Guns or Butter
- The Story the Media — and the Government — Don’t Want You to Hear
- Deep Dive Intel Briefing 6/20/2026 Lt Col Daniel Davis
- If Americans Knew
- JNS Policy Summit to kick off in Israel
- Fatalities From Israel’s Vast Gaza Genocide Deliberately Undercounted
- ‘Reproductive genocide’ in Gaza; death toll in Lebanon tops 4,000 (during a ceasefire) – Daily Update
- Israelis Invaded Lebanon And Then Cried Victim When Their Soldiers Got Killed
- FARA Docs: Israel is Spying On Millions Of Christian Americans In Their Churches
- Why US presidents from both parties end up cursing Benjamin Netanyahu
- Israel Asked Facebook to Censor Iran War Content, Internal Documents Show
- Deaths in Gaza undercounted, possibly by 100s of thousands; “Psychopath” Ben-Gvir talks trash – Daily Update
- UNICEF: “Trauma is woven into the very fabric of childhood in Gaza”
- 15 articles a day: The extent of the Israeli army’s media interference
- No Tricks Zone
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
