Jack Ruby: Israel’s Smoking Gun

BY LAURENT GUYÉNOT • UNZ REVIEW • NOVEMBER 13, 2021
By a strange paradox, most Kennedy researchers who believe that Oswald was “just a patsy” spend an awful lot of time exploring his biography. This is about as useful as investigating Osama bin Laden for solving 9/11. Any serious quest for the real assassins of JFK should start by investigating the man who shot Oswald at pointblank in the stomach at 11:21 a.m. on September 24, 1963 in the Dallas Police station, thereby sealing the possibility that a judicial inquiry would draw attention to the inconsistencies of the charge against him, and perhaps expose the real perpetrators. One would normally expect the Dallas strip-club owner Jack Ruby to be the most investigated character by Kennedy truthers. But that is not the case.
Of course, it is perfectly normal that Chief Justice Earl Warren, when Ruby told him on June 7, 1964, “I have been used for a purpose,” failed to ask him who had used him and for what purpose.[1] But what about independent investigators? Are only readers of the Forward (“News That Matters To American Jews”) worthy of being informed that “Lee Harvey Oswald’s Killer ‘Jack Ruby’ Came From Strong Jewish Background,” and that he told his rabbi Hillel Silverman that he “did it for the Jewish people”? Here is the relevant passage of Steve North’s 2013 article, relating Silverman’s reaction after hearing on the radio that a “Jack Rubenstein” had killed the assassin:
“I was shocked,” said Silverman. “I visited him the next day in jail, and I said, ‘Why, Jack, why?’ He said, ‘I did it for the American people.’” I interrupted Silverman, pointing out that other reports had Ruby saying he did it “to show that Jews had guts.” The rabbi sighed. “Yes, he mentioned that,” Silverman said. “But I don’t like to mention it. I think he said, ‘I did it for the Jewish people.’ But I’ve tried to wipe that statement from my mind.”[2]
Ruby’s defense lawyer William Kunstler also claims in his memoir that Ruby told him: “I did it for the Jews,” repeating on several occasions: “I did this that they wouldn’t implicate Jews.” During Kunstler’s last visit Ruby handed him a note in which he reiterated that his motive was to “protect American Jews from a pogrom that could occur because of anger over the assassination.”[3] There is only one possible interpretation of Ruby’s words: he must have known, and those who tasked him with killing Oswald must have known, that if Oswald was tried, the Jewish hand in JFK’s assassination would likely be made apparent.
Why is this crucial information not in any book on the Kennedy assassination, save in Michael Collins Piper’s (and now mine)? James Douglass, to take the most representative example, insists, without a shred of evidence, that Ruby, besides being a “Chicago mob functionary,” was “CIA-connected”.[4] Not once does Douglass mention Ruby’s Jewish background, and his real name can only be found in a single endnote quoting another author. Could Douglass’s strange omission have the same motive as Ruby’s murder of Oswald, namely to “protect American Jews from a pogrom that could occur because of anger over the assassination”?
Ruby is not the only person connected to Oswald whose confused words implicating “the Jews” are carefully concealed from the public. On March 29, 1977, George DeMohrenschildt, a Russian geologist who had befriended Oswald in Dallas in 1962 at the request of CIA agent J. Walton Moore, was found dead with a bullet through his head. His death was ruled a suicide, but the Sherriff’s report mentions that in his last months he complained that “the Jews” and “the Jewish mafia” were out to get him.[5] His wife confirmed to Jim Marrs, author of Crossfire: The Plot that Killed Kennedy (1989), that her husband thought that “the Jewish Mafia and the FBI” were out to get him.[6] Most people mildly interested in the JFK assassination know about DeMohrenschildt’s relationship with Oswald, but how many have ever heard this intriguing—even incriminating—detail?
After DeMohrenschildt moved away from Dallas in June 1963, Oswald was chaperoned by Ruth Paine, who found him a job at the Texas School Book Depository, where he started working on October 16.[7] It is repeated in every book that Ruth Paine looked after Oswald on behalf of the CIA, but no evidence is ever given. On the other hand, I was surprised to read in her testimony to the Warren Commission that in the 1950s, Ruth Paine had been “a leader in the Jewish community at Indianapolis,” working with Jewish immigrants who “spoke Yiddish in conducting their business meetings.”[8] Jack Ruby also made business deals in Yiddish, as we shall see. As a matter of fact, he sneaked into the Dallas Police Station under the pretense of translating for Yiddish reporters (what Yiddish reporters need a translator in the U.S.?).
This piece of information comes from the only useful book written about Ruby: Seth Kantor’s 1978 Who Was Jack Ruby? retitled The Ruby Cover-Up in 1980. Kantor was a reporter working for the Dallas Times Herald in 1963. He knew Ruby and was less than ten feet away from him when he shot Oswald. Kantor’s meticulous investigation is an important contribution to the search for the truth about Kennedy’s assassination. In the rest of this article, I will draw mostly from his book, as well as from Michael Collins Piper’s Final Judgment and a few other sources.

Jack Ruby in front of his Carousel strip club
Gangsters for Zion
In its final report, the Warren Commission declared that it could “not establish a significant link between Ruby and organized crime,” because “Ruby has disclaimed that he was associated with organized criminal activities, and law enforcement agencies have confirmed that denial.”[9] But there is plenty of evidence of Ruby’s association with organized crime. Robert Blakey, chief counsel for the House Select Committee on Assassinations from 1977 to 1979, said: “The most plausible explanation for the murder of Oswald by Jack Ruby was that Ruby had stalked him on behalf of organized crime, trying to reach him on at least three occasions in the forty-eight hours before he silenced him forever.”[10] Incriminating “organized crime” in the JFK assassination and the ensuing Oswald assassination was, of course, the most harmless conclusion that the HSCA could come up with, short of ridiculing itself by confirming the Warren Commission’s story of two lone nuts. And so the Washington Post could headline: “MOBSTERS LINKED TO JFK DEATH.”[11]
The missing word, here, is “Jewish”. Most Americans, learning that Jack Ruby was a mobster, must have thought he was Italian, like Hollywood gangsters. They were not told that his real name was Jacob Leon Rubenstein, that he was the son of Jewish Polish immigrants, that he went to the synagogue just before shooting Oswald, and that he later confessed to his rabbi that he “did it for the Jews.”
Jacob Rubenstein belonged to the Jewish mafia, also known as the Yiddish Connection. He had moved from Chicago to Dallas in 1947, on the trail of 15 other Chicago mobsters (3 Italians and 9 Jews) who had settled there to take over the prostitution business. That is when he changed his name from Rubenstein to Ruby. Ruby’s mentor and role model was Mickey Cohen, who operated in Chicago during the Prohibition but was then active in Hollywood. During his trial for shooting Oswald, Ruby’s legal team was fronted by Melvin Belli, a longtime friend and attorney of Cohen (Belli’s defense was that Ruby had suffered temporary insanity due to a bout of “psychomotor epilepsy”).[12] In 1947, Cohen had succeeded Benjamin Siegelbaum, aka Bugsy Siegel (romanticized by Hollywood in 1991) at the head of “Murder Incorporated”. Cohen and Siegelbaum were accountable to Meyer Lansky (born Suchowljansky), the most powerful Jewish mafia boss, who had built part of his fortune with his Havana casinos and brothels, of which he was dispossessed by Castro in 1959. Lansky’s biographer Hank Messick describes him as the head of the National Crime Syndicate. “Thanks largely to Lansky, organized crime has changed from an ugly growth on the body politic capable of being removed by surgery to a cancerous part of our economic and political systems.”[13]

Meyer Lansky in Israel, 1971
Mickey Cohen claims in his memoirs that, in the 1940s and 1950s, he was “engrossed with Israel”, and boasts about his financial and criminal contributions to the arms smuggling operations of the Haganah. Gary Wean, a detective sergeant for the Los Angeles Police Department, claims in his book There’s a Fish in the Courthouse (1987) that he saw Ruby twice in Hollywood in 1946 and 1947 in the presence of Cohen.[14] He also writes that Cohen had frequent contacts with Menachem Begin,[15] and that he was sharing his girlfriend, stripper Candy Barr, with Menachem Begin as well as Ruby.[16]
Cohen was not the only mobster working for Israel. A pact had been sealed between prominent Zionists and Jewish mafia bosses around 1945, when the Haganah organized a highly effective black market of weapons and explosives from the US to Palestine. The operation was orchestrated by a group of about 40 wealthy American Jews who pledged to help David Ben-Gurion when the latter visited New York in July 1945. Headed by Rudolf Sonneborn, the group acted under the legal cover of a charity, the Sonneborn Institute, whose story is told by Leonard Slater in The Pledge (Simon & Schuster, 1970).[17] The group operated separately from the Jewish Agency in order to shield it from direct involvement in unlawful activities. Among its active members was the future Jerusalem mayor (1965-93) Teddy Kollek, who also played a key role in forging the CIA-Mossad Alliance. Robert Rockaway has documented the contribution of the Jewish underworld to this operation, in his article “Gangsters for Zion: How Jewish mobsters helped Israel gain its independence”. He writes:
In 1945, the Jewish Agency, the pre-state Israeli government headed by David Ben-Gurion, created a vast clandestine arms-purchasing-and-smuggling network throughout the United States. The operation was placed under the aegis of the Haganah, the underground forerunner of the Israel Defense Forces, and involved hundreds of Americans from every walk of life. They included millionaires, rabbinical students, scrap-metal merchants, ex-GIs, college students, longshoremen, industrialists, chemists, engineers, Protestants and Catholics, as well as Jews. One group, who remained anonymous and rarely talked about, were men who were tough, streetwise, unafraid, and had access to ready cash: Jewish gangsters.
Sent by Ben-Gurion to the U.S. to purchase heavy armaments, Haganah operative Yehuda Arazi approached Meyer Lansky and met with members of Murder, Incorporated. Another Haganah emissary, Reuvin Dafni, who would become Israeli consul in Los Angeles and New York, also dealt with Jewish gangsters. “When I interviewed Dafni,” Rockaway writes, “he told me about his meetings with Jewish mobsters. His meetings were arranged by members of the local Jewish community. His first meeting was in Miami with Sam Kay, a leading Miami Jewish gangster.” Dafni also met with Bugsy Siegel.
As Dafni relates, “I told him my story, how the Haganah was raising money to buy weapons with which to fight. When I finished, Siegel asked, ‘You mean to tell me Jews are fighting?’ Yes, I replied. Then Siegel, who was sitting across the table, leaned forward till his nose was almost touching mine. ‘You mean fighting, as in killing?’ Yes, I answered. Siegel leaned back, looked at me for a moment and said, ‘OK, I’m with you.’” “From then on,” recalled Dafni, “Every week I got a phone call to go to the restaurant. And every week I received a suitcase filled with $5 and $10 bills. The payments continued till I left Los Angeles.” Dafni estimates that Siegel gave him a total of $50,000.[18]
Some of those “gangsters for Zion”, writes Rockaway, “did so out of ethnic loyalties,” or “saw themselves as defenders of the Jews, almost biblical-like fighters. It was part of their self-image.”[19]
Such was also the background and self-image of Jack Ruby. His activities in arms smuggling are well documented, although the fact that it was for the benefit of Israel is often blurred. In Coup d’État in America: The CIA and the Assassination of John F. Kennedy (1975), Allan Weberman refers to the arms-dealing activities of Ruby and other mobsters, but makes no mention of their Jewishness (unless saying that Ruby “was strongly anti-Nazi” counts as an euphemism for being Jewish), and claims that they were in fact arming Castro—while simultaneously participating in CIA plots to kill him.[20]
Ruby knew Lewis McWillie, the manager of the Lansky brothers’ Tropicana nightclub casino in Havana. After the overthrow of Batista by Castro in January 1959, Meyer Lansky relocated to Miami, but Jake Lansky was arrested and confined to a luxury prison, the Trescornia detention camp, together with another mafia figure, Santo Trafficante, Jr. Although not Jewish, Trafficante had sworn allegiance to the Lansky brothers, and controlled substantial portions of Havana’s gambling and prostitution rackets. While in prison, Jake Lansky and Trafficante were often visited by Lewis McWillie, who was negotiating their release by Castro. Ruby told the Warren Commission on June 7, 1964 about visiting Lewis McWillie in 1959 in Havana, and also spoke of knowing McWillie’s bosses, whom, from fear of pronouncing their name, he referred to as “the Fox brothers, the greatest that have been expelled from Cuba.”[21] (McWillie would later acknowledge to the HSCA that, “Jack Ruby could have been out there [Havana] one time with me.”) Ruby added to the Warren Commission that McWillie and one of the brothers later visited him in Dallas.[22]
Seth Kantor quotes from a classified message that was sent from CIA headquarters to National Security Advisor McGeorge Bundy, on November 28, 1963, confirming that, while Santo Trafficante was living “in relative luxury in a Cuban prison” in 1959, he was visited frequently by “an American gangster-type named Ruby.”[23]
In September 1962, Trafficante is reported to have said to José Alman, a prominent member of the Cuban exile community in Miami, that “President Kennedy would get what was coming to him.” Aleman disagreed and argued that Kennedy would be reelected. “No, José,” said Trafficante. “He is going to be hit.”[24] When Trafficante was asked by Richard Sprague of the HSCA, “did you ever discuss with any individuals plans to assassinate President Kennedy prior to his assassination?” Trafficante refused to answer.[25]
As Kantor shows in great detail, Jack Ruby had repeated contacts with members of the Jewish underworld in 1963. By June 8, “a large group of Chicago racketeers began to show up at Ruby’s Carousel and at two other nearby strip-show clubs, according to a confidential report to Dallas Police Chief Jesse E. Curry written by Lieutenant Robert L. May Jr., who had been head of the vice squad.”[26] Ruby’s underworld contact intensified during the 11 days leading up to President Kennedy’s assassination, “when Ruby abruptly signed a power of attorney, giving up certain rights to control his own money. He also suddenly bought and installed a safe for the first time in his 16 years as a Dallas nightclub operator, to store extra amounts of money.”[27] During this period, “Ruby was getting a series of phone calls at the Carousel from an unidentified man who never would leave a message when Ruby was out.”[28] On November 11, Ruby met in Dallas with Alexander Philip Gruber, who was known for his connections with Mickey Cohen. Gruber, who had not visited Ruby in years, told the FBI that he was in Joplin Missouri at that time, and had simply decided to drop in on Ruby “since Dallas, Texas, was about 100 miles from Joplin” (the distance is 360 miles).[29] In the afternoon of November 22, Ruby phoned Alex Gruber in Los Angeles. “Gruber subsequently told the FBI he didn’t really know why Ruby called.”[30] That is most probably when Ruby received an offer he couldn’t refuse.

Ruby was certainly informed about the precise moment when Oswald would be transferred from the Dallas Police Station to the County Jail. According to former British Intelligence Officer Colonel John Hughes-Wilson, it was Sam Bloom, the Jewish chairman of the “host committee” who had invited Kennedy to Dallas, who suggested to the Police “that they move the alleged assassin [Oswald] from the Dallas police station to the Dallas County Jail in order to give the newsmen a good story and pictures.” And “when the police later searched Ruby’s home, they found a slip of paper with Bloom’s name, address and telephone number on it.”[31]
In an apparent attempt to make it impossible for him to fulfill his contract, Ruby tried to warn the Dallas Police anonymously: Lieutenant Billy Grammer, a dispatcher for the Dallas Police Department, whose statement can be heard here, received an anonymous phone call at 3 a.m. on November 24 from a man who knew Grammer’s name. The caller told Grammer that he knew of the plan to move Oswald from the basement and that unless the plans for Oswald’s transfer were changed, “we are going to kill him.” After Oswald was shot, Grammer, who knew Ruby and had found the voice familiar at the time of the call, identified Ruby as the caller.[32]
Ruby and the Dallas Police
When Ruby shot Oswald on Sunday November 24, this was not the first time he had been allowed into the Dallas Police Station. He knew about every policeman in town, and was nearly as often hanging around in the Police station as the policemen were at his Carousel strip club. “I have always been very close to the police department, I don’t know why,” he told the Warren Commission. Most plausibly, being on friendly terms with the Dallas policemen was his special mob assignment, and certainly the reason why he was chosen for silencing Oswald: few people had as much ease in making their way into the Dallas Police station.
Ruby spent a lot of time there from Friday 22 to Sunday 23, making several attempt to enter room 317 on the third floor where Oswald was interrogated. Early evening on Friday, the day Kennedy was assassinated and Oswald arrested,
shortly after 7 p.m., John Rutledge, a veteran police reporter for The Dallas Morning News, saw Jack Ruby, whom he easily recognized by sight, step from a public elevator onto the third floor. / Ruby was between two men who wore lapel credentials identifying them as out-of-town reporters. The three walked rapidly past a police officer stationed at the elevators to keep out anyone not on official business. Ruby was hunched over, writing something on a piece of paper and then showing it to one of the reporters as they walked toward Room 317, where Oswald was being interrogated by Captain Fritz and others. … A guard was posted at the bureau door to keep reporters from getting in to use the phones, but Ruby had no trouble easing in. He knew the guard. Ruby walked in and shook hands with Eberhardt, who asked him what he was doing. Ruby had note paper in his hand and said he was acting as translator for the foreign press. Eberhardt figured Ruby was talking about the Israeli press or the Yiddish-speaking reporters Eberhardt guessed he heard in the bedlam of the corridor.[33]
Here are the exact words from Detective August M. Eberhardt’s deposition to the Warren Commission (online here):
Mr. EBERHARDT. He came in and said hello to me, shook hands with me. I asked him what he was doing. He told me he was a translator for the newspapers. Of course, I knew that he could speak Yiddish. Had a notebook in his hand…
Mr. GRIFFIN. Do you know if there were Israeli newspaper or Yiddish—
Mr. EBERHARDT. There was a bunch of them running around there talking that unknown tongue. I don’t know what they were saying.
What a shame these Yiddish-speaking reporters were not traced and identified. Victor R. Robertson Jr., a reporter for WFAA radio and TV in Dallas who knew Ruby, also testified seeing him in the Police Station, attempting to enter 317 while Oswald was in there. Despite those testimonies, the Commission denied that Ruby was ever on the third floor Friday evening.
Later that same day, after a short visit to the synagogue, Ruby bought a dozen corned beef sandwiches and “telephoned homicide detective Richard M. Sims and offered to deliver the free food right to the office. Sims thanked him but said the day’s work was about over and they wouldn’t need anything to eat. Ruby found another reason to go anyway and, at about 11:30 p.m., he stepped off the elevator on the third floor again.”[34] At midnight, Ruby made his way to the press conference in the basement police assembly room, when Oswald was put on display. The Warren Report admits Ruby’s presence there, but portrays him as a casual bystander. “Nowhere in its 888-page report to the public did the Commission include Ruby’s admission to the FBI, a month after the crime, that he was carrying a loaded, sub-nosed revolver in his right-hand pocket during the Oswald press session in the assembly room.” Ruby couldn’t approach Oswald close enough to shoot him, as the room was packed with reporters and photographers.[35]
On Saturday 23, Ruby brought sandwiches to reporters in the Police press room; “reliable outside witnesses reported seeing Ruby or talking with him at intervals during Saturday afternoon—witnesses such as Jeremiah A. O’Leary Jr. of The Washington Star and Thayer Waldo, a reporter to The Fort Worth Star-Telegram.” Yet, Kantor notes,
the Warren Commission said it could reach “no firm conclusion as to whether or not Ruby visited the Dallas police department on Saturday” because “no police officer has reported Ruby’s presence on that day” and because “Ruby has not mentioned such a visit.” / In other words, the Warren Commission decided there had been no conspiracy between Dallas police officers and Jack Ruby because none of them reported it at the time.[36]
On Sunday morning, arrangements were made for the transfer of Oswald to the County Jail. A little after 10:30, Kantor hypothesizes, “a call was placed to the unlisted phone in Ruby’s apartment; Ruby was told where to enter the station and that the transfer van was en route.”[37] Ruby first went to the Western Union office in the next block, and arrived just in time to see Oswald being transferred. This narrow timing has been used as evidence that there was no premeditation and therefore no conspiracy. But Kantor theorizes that Ruby’s entrance into the Police station using the public stairway to the basement jail office area “could have triggered the go-ahead signal for Oswald to be brought down”, and he produces plausible evidence that it did.[38] The way Ruby entered the station is still unclear, but the House committee voted in 1979 that “it was less likely that Ruby entered the police station without assistance.”[39]

Jack Ruby after his pre-trial hearing in February 1964
The Johnson-Ruby connection
Besides Ruby, we know of one person who took steps to make sure that Oswald was silenced forever. Because Ruby could only shoot one bullet to Oswald—he said he had planned to shoot three—, Oswald was still alive when he arrived at Dallas Parkland Hospital. Dr. Charles Crenshaw recalls in his book JFK, Conspiracy of Silence (1992) that, while operating on Oswald with other surgeons, he noticed that an unknown man looking like Oliver Hardy with a pistol hanging from his back pocket had entered the operation room. Minutes later, he was told about an urgent call for him and left the operating room to take it. The call was from the new sworn president Lyndon Johnson who first asked “Dr. Crenshaw, how is the accused assassin?” Crenshaw answered: “Mr. President, he’s holding his own at the moment.” Then Johnson said firmly: “Dr. Crenshaw, I want a deathbed confession from the accused assassin. There’s a man in the operating room who will take the statement. I will expect full cooperation in this matter.” Dr. Crenshaw answered “Yes, sir,” and hung up. Thirty years later, he comments: “As I stood there in a state of disbelief, my mind was racing. First, ‘deathbed confession’ implies that someone is going to die. If Oswald doesn’t die on the table, is ‘Oliver Hardy’ or someone else going to kill him?” Since Dr. Crenshaw had just told Johnson that Oswald was “holding his own,” the expression “deathbed confession” did sound like an implicit order that Oswald should not leave the operating room alive. It really sounded as if Johnson wanted Ruby’s job finished. Moments after Dr. Crenshaw went back to the operating room, Oswald’s heart beat stopped: “Oliver Hardy” disappeared, never to be seen again. “The incident,” wrote Crenshaw, “confounded logic. Why the President of the United States would get personally involved in the investigation of the assassination, or why he would take the inquest out of the hands of the Texas authorities was perplexing.”[40]
There is plenty of evidence of Johnson’s central role in Kennedy’s assassination. And it happens that Jack Ruby directly pointed to him as the mastermind. At the end of a short filmed news conference in the Dallas County Jail in March 1965, Ruby said, “When I mentioned about Adlai Stevenson, if he was Vice-President there would never have been an assassination of our beloved President Kennedy.” Asked to explain what he meant, Ruby continued, “Well the answer is the man in office now.”[41]
How could Ruby know of Johnson’s guilt? Former Nixon operative Roger Stone claims that, in his presence, Nixon recognized Ruby as one of “Johnson’s boys.”[42] I doubt that story; Stone could have made it up to counter another rumor about Ruby’s connection to Nixon, sparked by a forged 1947 FBI memo stating that “one Jack Rubenstein of Chicago […] is performing information functions for the staff of Congressman Richard Nixon.”[43] But there is one more thing linking Ruby to Johnson.
In his testimony to Chief Justice Earl Warren and other Commission members on June 7, 1964, Ruby pleaded to be given a chance to talk directly to Johnson, otherwise “you will see the most tragic thing that will ever happen,” adding that “maybe something can be saved … if our President, Lyndon Johnson, knew the truth from me.”[44] This can be interpreted as a veiled threat addressed to Johnson. Ruby, who by this time had been sentenced to death, may have been trying to remind Johnson that his contract included a presidential pardon (he had shot Oswald out of love for the Kennedys, hadn’t he?). Even more curiously, Ruby hinted that Israel’s reputation could suffer if he spoke: “There will be a certain tragic occurrence happening if you don’t take my testimony and somehow vindicate me so my people don’t suffer because of what I have done.” He feared, he said, that his act would be used “to create some falsehood about some of the Jewish faith.” Ruby also declared to Warren, “I have been used for a purpose,” but no one in the Commission bothered to ask him who had used him and for what purpose.[45] All Ruby got out of his confused testimony was a second pointless Warren Commission interview one month later (July 18, 1964), this time by none other than Arlen “Magic Bullet” Specter (transcript here). His frustration would explain why in March 1965, he finally accused Johnson. Shortly thereafter, he wrote a letter of sixteen pages that he managed to get smuggled out of jail, blaming Johnson for Kennedy’s murder and calling the former “a Nazi of the worst order.”[46] By doing so, he probably hastened his own death, on January 3, 1967.
The case against Johnson
One commenter to my previous Kennedy article argued that the thesis of Israel’s motive is unconvincing because the Israeli Deep State had other options than killing Kennedy in order to go on with its Dimona project. I responded that a murderer’s motive is rarely that he has no other choice than to kill, but that he finds a crucial advantage in the killing. I also remarked that, whoever the assassins were, their purpose was obviously not just to get rid of Kennedy, but to put Johnson in charge. And that had to be done quickly, because the Kennedys were busy destroying Johnson’s reputation and would soon be announcing a change in the vice-presidency. According to Horace Busby, longtime LBJ aide and author of The Thirty-First of March (2005), Johnson had found out that, in early November 1963, Robert Kennedy had sent a team of national reporters to Texas to utterly destroy him. “We’re here to do a job on Lyndon Johnson,” said one the newsmen to an attorney whom he mistakenly believed to be a Johnson enemy. “When we get through with the sonofabitch, Kennedy won’t be able to touch him with a ten-foot pole in 1964”[47] (quoted from this article by Robert Morrow, who wrote more informative articles on Johnson and his “murderous psychopathy”). Richard Nixon, who happened to be in Dallas the day before Kennedy, leaked the rumor to the Dallas Morning News, who reported it on November 22nd under the headline “Nixon Predicts JFK May Drop Johnson.” Instead, Johnson became president that very day (and Nixon knew that Johnson was behind it).[48]

So, since the assassination of Kennedy was a coup to put Johnson in power—what else can it be?—there was no time to waste: it had to be done before the new campaign started and news of a change of vice-presidential ticket was published (Nixon’s prediction was the first and the last). If we now want to know the motive of the coup, we only have to ask: What major change occurred in US policy under Johnson? The change was not visible to the American public then, but they are now well-known, at least to readers of the Jewish and Israeli press. “Lyndon Johnson: Israel Has Had No Better Friend,” headlined Haaretz on May 9, 2018.
“Historians generally regard Johnson as the president most uniformly friendly to Israel,” we are told by the Jewish Telegraphic Agency.
Johnson was the first president to invite an Israeli prime minister, Levi Eshkol, on a state visit. They got along so well — both men were farmers — that Johnson paid Eshkol the rare compliment of inviting him to his ranch.
LBJ soon abandoned pressure on Israel to come clean about the Dimona reactor. He increased arms sales to Israel and in 1968, after Israel’s primary supplier, France, imposed an embargo as a means of cultivating ties in the Arab world, the United States became Israel’s main supplier of weapons, notably launching the talks that would lead to the sale of Phantom fighter jets to Israel.
Johnson wanted to commit more forcefully to Israel’s cause in the lead-up to the 1967 Six-Day War, but he felt constrained from a dramatic show of military might because of the failures of the war in Vietnam then dogging his presidency. Nonetheless, during the war, he ordered warships to within 50 miles of Syria’s coast as a warning to the Soviets not to interfere.
In a speech in the war’s immediate aftermath, Johnson effectively nipped in the bud any speculation that the United States would pressure Israel to unilaterally give up the lands it had captured. He laid down not only the “land for peace” formula that would inform subsequent U.N. Security Council resolutions, but made it clear that any formula had to ensure Jewish access to Jerusalem’s Old City.
It is a good thing that Johnson is being praised by the Israeli press as the US president who “firmly pointed American policy in a pro-Israel direction”, because, on the other hand, his crucial role in the Dallas coup is also getting mainstream attention, as illustrated by the December 2, 2019 issue of the National Enquirer. Anybody who can add one plus one can also make the logical inference.

Watch Laurent Guyénot’s film “Israel and the Assassinations of the Kennedy Brothers” and share it:
https://www.youtube.com/watch?v=a_kh5tb7PtA
Notes
[1] Seth Kantor, The Ruby Cover-Up, Zebra Books , 1980, p. 49.
[2] Steve North, “Lee Harvey Oswald’s Killer ‘Jack Ruby’ Came From Strong Jewish Background,” The Forward, November 17, 2013, on forward.com
[3] William Kunstler, My Life as a Radical Lawyer, Carol Publishing, 1994, p. 158.
[4] James Douglass, JFK and the Unspeakable: Why He Died and Why It Matters, Touchstone, 2008, p. 357.
[5] Douglass, JFK and the Unspeakable, p. 47; Sheriff’s Office report on mcadams.posc.mu.edu/death2.txt
[6] Jim Marrs, Crossfire: The Plot that Killed Kennedy, Carroll and Graf, 1989, p. 285.
[7] Douglass, JFK and the Unspeakable, pp. 169-171.
[8] On https://mcadams.posc.mu.edu/russ/testimony/paine_r3.htm
[9] Kantor, The Ruby Cover-Up, p. 48.
[10] https://en.wikipedia.org/wiki/Jack_Ruby#Ruby’s_motive
[11] Gaeton Fonzi, The Last Investigation: A Former Federal Investigator Reveals the Man Behind the Conspiracy to Kill JFK, 1993, Skyhorse, 2013, k. 405–76.
[12] Michael Collins Piper, Final Judgment: The Missing Link in the JFK Assassination Conspiracy, American Free Press, 6th ed., 2005, p. 239.
[13] Hank Messick, Lansky, Putnam’s Sons, 1971, p. 9.
[14] Michael Collins Piper, Final Judgment, p. 222.
[15] Gary Wean, There’s a Fish in the Courthouse, Casitas Books, 1987, p. 681, quoted by Piper, Final Judgment, op. cit., p. 219-27, 232-7.
[16] Michael Collins Piper, Final Judgment, p. 224.
[17] Read Ricky-Dale Calhoun, “Arming David: The Haganah’s illegal arms procurement network in the United States 1945-1949,” Journal of Palestine Studies Vol. XXXVI, No. 4 (Summer 2007), pp. 22–32, online here.
[18] Robert Rockaway, “Gangsters for Zion. Yom Ha’atzmaut: How Jewish mobsters helped Israel gain its independence”, April 19, 2018, on tabletmag.com
[19] Robert Rockaway, “Gangsters for Zion,” on tabletmag.com
[20] Alan J. Weberman and Michael Canfield, Coup d’État in America: The CIA and the Assassination of John F. Kennedy, Quick American Archives, 1975, pp. 151-180 (p. 178). Michael Piper mentions (Final Judgment, p. 232) that JFK researcher Alan J. Weberman has revealed the little-known fact that Ruby traveled to Israel in 1955, but the link to Weberman’s website is now dead, and I hold Weberman as a very unreliable source
[21] Bernard Fensterwald, in Coincidence or Conspiracy (quoted by Piper, Final Judgment, pp. 228-229).
[22] Richard Gildbride, Matrix for Assassination: the JFK Conspiracy, Trafford, 2009.
[23] Kantor, The Ruby Cover-Up, pp. 255-256.
[24] Kantor, The Ruby Cover-Up, pp. 259-264.
[25] Kantor, The Ruby Cover-Up, p. 402.
[26] Kantor, The Ruby Cover-Up, p. 53.
[27] Kantor, The Ruby Cover-Up, p. 48.
[28] Kantor, The Ruby Cover-Up, p. 104.
[29] Kantor, The Ruby Cover-Up, pp. 56-59.
[30] Kantor, The Ruby Cover-Up, p. 91.
[31] John Hughes-Wilson, JFK-An American Coup d’État: The Truth Behind the Kennedy Assassination, John Blake, 2014.
[32] Mentionned in this comment.
[33] Kantor, The Ruby Cover-Up, pp. 96-97.
[34] Kantor, The Ruby Cover-Up, p. 98.
[35] Kantor, The Ruby Cover-Up, pp. 100-101.
[36] Kantor, The Ruby Cover-Up, p. 116.
[37] Kantor, The Ruby Cover-Up, p. 132.
[38] Kantor, The Ruby Cover-Up, p. 141.
[39] Kantor, The Ruby Cover-Up, p. 409.
[40] Charles A. Crenshaw, JFK, Conspiracy of Silence, Signet, 1992, pp. 185-189, 5, and
[41] This sequence can be seen in the 1988 documentary “The day the dream died” at 38:20; for more information on Ruby’s declarations about Johnson and about Jews, check this webpage.)
[42] Patrick Howley, “Why Jack Ruby was probably part of the Kennedy conspiracy,” The Daily Caller, March 14, 2014, on dailycaller.com
[43] Copy at www.jfkmurdersolved.com/nixonruby.htm. The forgery is proven by several inconsistencies: first, Nixon was a freshman in the role as junior counsel in 1947, and only started prosecuting Alger Hiss (the only likely context for this memo) the following year. Second, it refers to “Jack Rubenstein” living in Chicago in November of 1947, when Ruby had in fact already changed his name and moved to Dallas by that time. Finally , the document carries a zip code, when they did not exist at the time.
[44] Read Ruby’s deposition here.
[45] Seth Kantor, The Ruby Cover-Up, p. 49.
[46] Phillip Nelson, LBJ: The Mastermind of JFK’s Assassination, pp. 604-607.
[47] Horace Busby, The Thirty-First of March: An intimate portrait of Lyndon Johnson’s final days in office, Farrar, Straus and Giroux, 2005, pp. 129-130.
Prominent Scientists Go Public: ‘Fauci Fooled America’
By Jeremy Loffredo | The Defender | November 2, 2021
In an op-ed, “Fauci Fooled America,” published Monday in Newsweek, two scientists accused Dr. Anthony Fauci of bungling the government’s response to COVID by getting “major epidemiology and public health questions wrong.”
Martin Kulldorff, Ph.D., an epidemiologist at Harvard Medical School, and Jay Bhattacharya, M.D., Ph.D., professor of Health Policy at Stanford University School of Medicine wrote: “Reality and scientific studies have now caught up with him.”
Kulldorff and Bhattacharya, both senior scholars at the Brownstone Institute and signers of the Great Barrington Declaration, had this message for Newsweek readers:
“The evidence is in. Governors, journalists, scientists, university presidents, hospital administrators and business leaders can continue to follow Dr. Anthony Fauci or open their eyes. After 700,000-plus COVID deaths and the devastating effects of lockdowns, it is time to return to basic principles of public health.”
The authors ticked off a list of “key issues” Fauci got wrong, including failure to recognize natural immunity, protecting the elderly, school closures, masks and contact tracing.
“By pushing vaccine mandates, Dr. Fauci ignores naturally acquired immunity among the COVID-recovered, of which there are more than 45 million in the United States,” the authors wrote. “Mounting evidence indicates that natural immunity is stronger and longer lasting than vaccine-induced immunity.”
Kulldorff and Bhattacharya cited a study from Israel, which concluded the vaccinated were 27 times more likely to get symptomatic COVID than the unvaccinated who had recovered from a prior infection.
They pointed out that the scientific community has known about natural immunity from disease “at least since the Athenian Plague in 430 BC.”
On Fauci’s dictates to mandate the vaccine for healthcare workers, the two argued: “Under Fauci’s mandates, hospitals are firing heroic nurses who recovered from COVID they contracted while caring for patients. With their superior immunity, they can safely care for the oldest and frailest patients with even lower transmission risk than the vaccinated.”
On school closures they wrote: “Considering the devastating effects of school closures on children, Dr. Fauci’s advocacy for school closures may be the single biggest mistake of his career … While children do get infected, their risk for COVID death is minuscule, lower than their already low risk of dying from the flu.”
Kulldorff and Bhattacharya pointed to Sweden, noting that during the 2020 spring wave of COVID, the country kept daycare and schools open for all 1.8 million children ages 1 to 15, with no masks, testing or social distancing.
According to the authors, Sweden’s strategy resulted in “zero COVID deaths among children and a COVID risk to teachers lower than the average of other professions.”
The authors argued contact tracing “was a hopeless waste of valuable public health resources that did not stop the disease,” and that Fauci failed at protecting the vulnerable.
“After more than 700,000 reported COVID deaths in America, we now know that lockdowns failed to protect high-risk older people,” they said.
On collateral public health damage, they argued that a “fundamental public health principle is that health is multidimensional; the control of a single infectious disease is not synonymous with health.”
They wrote that Fauci: “ … failed to properly consider and weigh the disastrous effects lockdowns would have on cancer detection and treatment, cardiovascular disease outcomes, diabetes care, childhood vaccination rates, mental health and opioid overdoses, to name a few. Americans will live with — and die from — this collateral damage for many years to come.”
In private conversations, Kulldorff and Bhattacharya said, most of their scientific colleagues agree with them on these points but few have spoken up out of fear of “financial censorship.”
“Many are afraid of losing positions or research grants, aware that Dr. Fauci sits on top of the largest pile of infectious disease research money in the world,” they wrote.
In his forthcoming book, “The Real Anthony Fauci,” Robert F. Kennedy, Jr. includes a comprehensive discussion of Fauci’s influence and power over the scientific community, revealing how Fauci uses the “financial clout at his disposal to wield extraordinary influence over hospitals, universities, journals and thousands of influential doctors and scientists — whose careers and institutions he has the power to ruin, advance or reward.” Kennedy’s book is due out Nov. 16.
Jeremy Loffredo is a freelance reporter for The Defender. His investigative reporting has been featured in The Grayzone and Unlimited Hangout. Jeremy formerly produced news programs at RT America.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Polio Vaccine ‘Hero’ Was Into Eugenics And Depopulation
https://www.bitchute.com/video/FnEUFYG0w7uY/
Amazing Polly | October 23, 2021
Researcher Jay Dyer goes through Jonas Salk’s book “Survival of the Wisest.” Salk was the ‘father of mass vaccination’ and a big inspiration for Bill Gates.
He also happens to want depopulation and genetic manipulation of human beings. Salk and his friends, of course, are among the ‘Wisest’ and they will rule the rest of us. Are his fantasies coming true with the COVID shots?

See the video and discussion here.
To support Amazing Polly’s work please go here: https://amazingpolly.net/contact-support.php
Crossword clues and bullying – the influence of Australia’s pro-Israel lobby unveiled
Michael West Media | October 3, 2021
The intimidating power of Australia’s pro-Israel lobby limits what mainstream media outlets dare publish about Israel and forces self-censorship on editors and journalists alike, writes John Lyons in his latest book Dateline Jerusalem: Journalism’s toughest assignment. Kim Wingerei reports.
In 2019, Fairfax Media’s Sydney and Melbourne mastheads made an error. In the daily crossword section, the answer to the clue “Holy land” turned out not to be six letters starting with an I, as some would expect, but nine letters: Palestine. So affronted was the Australia/Israel and Jewish Affairs Council (AIJAC) that they demanded an investigation.
Fairfax acceded, blamed the error on an external contractor and apologised to Colin Rubenstein, executive director of the AIJAC.
This is just one of many examples which John Lyons uses to illustrate the power of a lobby group so influential it can force changes to Government policy, hound journalists out of their jobs and pressure the ABC board to justify the appointment of foreign correspondents.
… there are only three people who can tell the editors of The Australian what they can or can’t use: Rupert Murdoch, Lachlan Murdoch and Colin Rubenstein. – John Lyons
 John Lyons is an experienced journalist. Currently the head of investigative journalism at the ABC, his 40 years in the media include being editor of the Sydney Morning Herald, Middle East correspondent for The Australian and winning one of his three Walkley Awards for “Stone Cold Justice”, a Four Corner’s episode which exposed the human rights abuses in Israel military courts.
John Lyons is an experienced journalist. Currently the head of investigative journalism at the ABC, his 40 years in the media include being editor of the Sydney Morning Herald, Middle East correspondent for The Australian and winning one of his three Walkley Awards for “Stone Cold Justice”, a Four Corner’s episode which exposed the human rights abuses in Israel military courts.
His earlier book Balcony over Jerusalem covered his six years of witnessing the tragedies and contradictions of a region which has suffered more armed conflict than any other since World War II.
In his latest book released this weekend (at 85 pages, it’s closer to essay size), Lyons focuses entirely on the Israel-Palestine conflict and specifically how pro-Israel lobbyists seek to control the narrative for the Australian audience.
He makes the point several times that the press in Israel is far more overtly critical of the policies of Israel’s Government than is the media in Australia, including how the regular flare-ups in the West Bank are covered.
To the AIJAC it’s a war of words. It is a battle to control how and what is said.
For example, Colin Rubenstein and his fellow lobbyists are particularly sensitive about using the word “occupation” in reference to Israel’s occupation of Palestinian Territories. But as the lieutenant colonel responsible for Israel’s army operations in the occupied territories quips:
If this is not occupied then the media has missed one of the biggest stories of our time, (Israel’s) withdrawal from the West Bank! – LC Eliezer Toledano, Israel Army
The pro-Israel lobby has even developed a special dictionary. The Global Language Dictionary was funded by The Israel Project to “guide politicians and journalists on the language to use to win support for settlement expansion.”
Merely using the word Palestine can land a journalist in trouble. Jennine Khalik, a Palestinian Australian and former journalist at The Australian recounts in the book how she was yelled at by a sub-editor for referring to a refugee and singer as coming from Palestine:
PALESTINE DOES NOT EXIST … Palestine is NOT a place … What kind of journalist are you, using the word Palestine?
For Jennine Khalik this was the last straw, she left the paper shortly after, following what had been a concerted campaign by the pro-Israel lobby, including diplomats from the Israel embassy questioning her editors about the appointment of “a Palestinian activist”.
In another example of the tactics used to control the narrative, Lyons refers to a story told by former The Age editor, Andrew Holden, where Colin Rubenstein and Mark Leibler – lawyer and well known leader of the Jewish business community – marched into his office and complained loudly about the paper’s coverage of the 2014 Gaza war.
Anyone who thinks that such a display by an esteemed member of the Australian community doesn’t have a chilling effect is kidding themselves. I have seen its effect in the years since in hesitancy on the part of editors and trepidation about any story which may show Israel in a negative light. – John Lyons
Lyons himself has also been subjected to threats and intimidation over the years for his reporting on Israel and Palestine. Like many who have dared to criticise the Israeli Government, he has been called an anti-semite, but also a “Goebbels” and “a Hamas smelly used tampon”.
It is a tactic he says is used persistently by those in Australia agitating for positive coverage of Israeli government actions.
I think the aim is to make journalists and editors decide that, even if they have a legitimate story that may criticise Israel it is simply not worth running, as it will cause more trouble than it’s worth. – John Lyons
As a result, most Australians don’t know much about the plight of the Palestinian people. They don’t know about the 101 permits that Palestinians need to obtain from Israel to be able to work and live in what they believe is their own land. They don’t know that Palestinians don’t enjoy free speech, freedom of movement or equality before the law.
In April 2021, Human Rights Watch (HRW) released its landmark report “A Threshold Crossed: Israel Authorities and the Crimes of Apartheid and Persecution”. It was largely ignored by mainstream media in Australia. “Including by my own organisation, the ABC,” says Lyons.
Abusive Israeli policies constitute crimes of apartheid, persecution
The pro-Israel lobby is so effective it has achieved the ultimate aim of information suppression – self-censorship.
John Lyons: Dateline Jerusalem: Journalism’s Toughest Assignment – now available from Monash University Publishing
Kim Wingerei is a businessman turned writer and commentator. He is passionate about free speech, human rights, democracy and the politics of change. Originally from Norway, Kim has lived in Australia for 30 years. Author of ‘Why Democracy is Broken – A Blueprint for Change’.
Winter is coming, and so are the nudges.
The UK government’s Winter Plan is rife with nudges
By Laura Dodsworth | October 4, 2021
There’s a chill in the air. Not from the changing seasons, it’s still beautifully balmy, but because the behavioural scientists’ fingertips have traced a hoar frost of psychocratic nudge on the government’s “Autumn and Winter Plan”.
The UK government’s Winter Plan plan contained some welcome news. The most draconian schedules of the Coronavirus Act will be revoked, including the powers to close schools, allow potentially infectious people to be detained, and restrictions on gatherings and events. The language around the plan’s launch was thankfully more cool-headed. The times are “challenging” but it is no longer claimed that Covid is the “biggest threat this country has faced in peacetime history”.
But the plan is also rife with “nudges” – sneaky ways to prime, prepare and prod you into the desired mindset and course of action.
The contents are freighted with the sunk cost fallacy; we’ve come so far, we mustn’t allow our good work to be undone. This also taps into people’s innate sensitivity to loss.
The trigger from Plan A to Plan B will be “unsustainable pressure” on the NHS rather than deaths. It’s under serious pressure every winter so consider yourselves to be put on notice.
There are other indications of the inevitability of Plan B. I spoke to behavioural scientist Patrick Fagan, who observed that:
“the Plan A / Plan B approach is a classic example of the foot-in-the-door technique. Firstly it makes us accept Plan A because, compared to Plan B, it looks more reasonable; then, once we have accepted and acclimatised to Plan A, we are more likely to then accept Plan B, because it is just one extra step on top of the commitment we’ve already made. The announcement of Plan B may also be an example of the mere exposure effect: simply by talking about the measures (even if, ironically, saying they won’t be implemented), the government makes them more familiar and therefore more psychologically acceptable.”
Bizarrely, after 18 months we’re trapped in a Groundhog Day of modelling and worst case scenarios. Almost a year ago, on the 21st September, Chris Whitty and Patrick Vallance warned of infections hitting 50,000 per day by mid-October in their “Shock and Awe” presentation. When the day arrived, the moving average was 16,228.
According to the doom-mongers at SAGE, up to 7,000 people could be hospitalised per day within the month. And this September the modellers were wrong once again – hospitalisations peaked at about a 1,000 a day and are now falling.
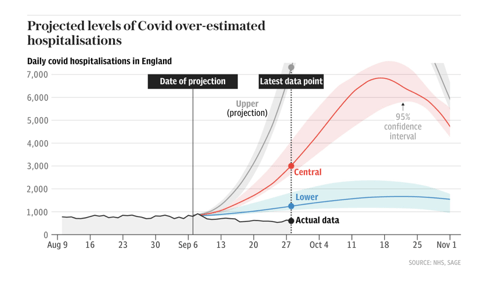
Source: The Telegraph
The big numbers both fuel the policies and justify them. It doesn’t matter that there are more optimistic scenarios, or that the modelling has limitations, because the first supine headline sticks in the brain. The behavioural psychology principle of “salience” draws your attention to what is novel and risky.
Dr Alex De Figueiredo, who conducts mathematical and statistical analyses for the Vaccine Confidence Project, told me that:
“Since the beginning of the pandemic it seems many modelling assumptions, such as the infection fatality rate, have been quite pessimistic. I think this has been why many of the predictions — such as hospitalisations and deaths — have been overstated. It also appears there has been little effort to validate forecasts out-of-sample, such as applying the models to Sweden or Florida, who have had far fewer restrictions.”
There are no quantifiable measures for what justifies each step from Plan A to Plan B. The parameters are fluid, unspecified. This creates confusion and stress, which infantilises people and makes them look to the government for direction. Essentially, confusion increases compliance.
The threat of lockdown hangs like a Sword of Damocles. Will we, or won’t we? It seems unlikely that the public and businesses could be persuaded again. Regardless, the threat of lockdown might be leveraged to justify the introduction of Covid Passports, in what is known as a “reciprocation nudge” – we appear to be given a concession in return for reduced resistance to another option.
Covid Passports have been vigorously opposed by MPs and civil liberties groups, and there hasn’t been a vote in Parliament yet. Despite this, they squat in Plan B as a fait accompli, in the denouement of the “door in the face” technique. This is when a huge request is made, then refused, to be followed by a second smaller request, in this case relegation to Plan B and for limited venues only. Boris Johnson said that it’s “not sensible to rule out this kind of option now when it might still make the difference between keeping businesses open or not.” But why would it be sensible when the Public Administration and Constitutional Affairs Committee produced a damning report against them and found the government could make no scientific case in their favour?
Covid Passports appear to be a behavioural science tool, used to increase vaccine uptake. This may backfire. ‘A Cross-Sectional Study in the UK and Israel on Willingness to Get Vaccinated against COVID-19’ found that vaccine passports deter a significant minority of people who want autonomy over their bodies. This also chimes with the research conducted by De Figueiredo and colleagues at The Vaccine Confidence Project. The bullying and resultant mistrust may impact Covid-19 vaccine uptake as well as other public health initiatives.
When my book A State of Fear: how the UK government weaponised fear during the Covid-19 pandemic was published some people believed, quite quaintly, that public health measures and messaging were unrelated to behavioural science. I think that the book and the writings of other academics and journalists have moved the dial. Once nudge is seen it can’t be unseen. The public increasingly see the nudge. If the behavioural scientists have been dazzling people with card tricks they have over-played their hand.
As such, there is more honesty about the purpose Covid Passports serve. Nicola Sturgeon, Scotland’s First Minister, said that the passport scheme
“will not eradicate transmission completely but it will help reduce it in some higher risk settings, and it will maximise protection against serious illness. And we believe – as we have seen already in some other countries – it will help encourage take-up of the vaccine.”
Similarly, Linda Bauld, Professor of Public Health and Interim Social Policy Adviser to the Scottish Government, also admitted that Covid Passports are “to increase uptake in vaccination” and the “rationale” is that it particularly boosts vaccination in 18 to 29 year olds.
While Covid Passports are in Plan B, Ministers say different things about them each day. Within the space of a week, Sajid Javid scrapped them but also didn’t rule them out for pubs. Javid admitted there’s “no evidence” for them but Boris Johnson called them “sensible”. Does the left hand not know what the right hand is doing? Or maybe a big behavioural science brain lurks in between. The epidemic management is reminiscent of the uncertainty created by Vladislav Surkov in the Soviet Union to deliberately turn politics into a performance of confusion – you don’t know what’s real anymore.
There are never-ending question marks over travel, although double-vaccinated travellers will no longer need expensive and inconvenient PCR tests. The double-jabbed will delight in the news, and it sounds sensible on the surface. However, this is not about “following the science”, since the previously infected do not benefit from the exemption. This is an incentive, a classic nudge, to encourage jabs. The vaccinated are rewarded and the unvaccinated are punished. Bearing in mind that negative tests and prior infection could suffice, this decision reeks of disdain for personal autonomy.
Vaccines for 12 to 15 year olds have been authorised. Politicians have stirred up debate amongst all corners regarding whether children should be jabbed with their parents’ consent or not. This utilises what Patrick Fagan calls “the leapfrog effect”. He says,
“it leapfrogs one stage of the debate and in doing so, sets the baseline assumptions which become accepted implicitly. Specifically, by having people debate whether or not parents’ consent should be sought, they are establishing the unspoken assumption that children should receive the jab in the first place. Those who think they are debating the government, arguing that parents’ consent is needed, are actually accepting its true goal, to jab kids.”
The government might be more in control of the narrative than many people like to believe. (Of course, chaos and confusion are alternatives…)
Worryingly, can teens truly provide informed consent? Throughout 2020 they were exhorted not to “kill granny”, which would provoke fear, shame and stress. Ads on Tiktok tell youngsters that the way to get back to normal is to take the vaccine. The vaccine will be rolled out in schools which will create peer pressure, in a particularly egregious use of “norms”. Finally, if the JCVI found the decision difficult, how is a 12 year old supposed to weigh up the evidence? (Nudging teens is the subject matter of my next article.)
Since the Cabinet reshuffle, Michael Gove has been informally dubbed the ‘Minister for Christmas’. Boris Johnson joked that he “didn’t want to have to cancel Christmas again”. Did you know Christmas might be cancelled and needs saving? You do now, the idea has been “seeded”.
Although it is ostensibly supply chains which threaten Christmas, the joke draws a comparison with last year’s Covid reasons. Again, you are put on notice. The nudges are still focussed on increasing vaccination, for now, but the threat to Christmas might hint at the beginning of a behavioural science approach to meet green targets.
We must be good boys and girls if we want Santa to come. And be aware, the nudgers are drafting our collective New Year’s Resolutions.
BBC submarine drama is anti-Russian propaganda machine in action
By Johanna Ross | September 25, 2021
The scene: a British nuclear submarine. A detective has been sent to investigate the death of a sailor. When she asks the Naval Commander why there needs to be so much secrecy, as Britain is not at war, he responds ‘That is an illusion. We have always been at war’.
The series, entitled ‘Vigil’ is the BBC’s most watched drama of the year, and has been well publicised, attracting an audience of 10.2 million over its first week. It depicts a fight with an illusive, ruthless adversary that successfully manages to infiltrate a UK submarine to ‘knock out Britain’s nuclear deterrent’, killing British citizens in the process. The murder weapon of choice is a nerve agent; can you guess who the enemy is yet?
Of course it’s Russia. Nuclear submarines, nerve agent, a treacherous opponent; from the opening sequence with video footage of Vladimir Putin and Dmitry Medvedev projected onto a submarine, the audience is under no illusion as to who this adversary is. Nowadays, the British public almost expects it to be Russia.
For years now the UK population has been schooled on ‘evil Russia’ across all media platforms – from the news to TV dramas to films – with the line between fiction and reality becoming increasingly blurred. One of the most Googled questions about the ‘Vigil’ drama series is ‘is it real?’ This is hardly surprising given the sheer volume of anti-Russian content, with cinema often dramatising real life events and vice versa.
Take the Skripal case, for instance. The apparent poisoning with ‘Novichok’ of the former spy Sergei Skripal and his daughter took place just a few months after a British/American TV series ‘Strike Back’ was released, in which a ‘rogue Russian biochemist‘ was working on a substance of the very same name. That was probably the first time that western audiences had ever heard the word ‘Novichok’, and yet, by extraordinary coincidence, it was to appear on our TV screens just a few months later, in the news. The finger of blame was immediately pointed at Moscow, just as preparations were being made for Russia to host the 2018 world cup. The timing could not have been worse for the Kremlin, and yet it helped Britain considerably in its bid to discredit Russia in its hosting of the sporting event.
TV and cinema being used by governments as instruments to sway and foster public opinion is nothing new. In the book ‘Propaganda and empire: the manipulation of British public opinion, 1880-1960’ John M MacKenzie explores the plethora of ways the British government promoted imperialism throughout the empire’s existence, not only through cinema, but using everything from cigarette cards to school textbooks. During the war, the British Ministry of Information also pumped out films with instructive government messaging under the direction of Humphrey Jennings. These documentaries were more about what to do and what not to do, promoting slogans such as ‘grow your own’ and ‘make do and mend’ to aid the war effort on the home front.
The ‘Vigil’ drama obviously had a considerable budget. And its political function is twofold; it highlights the ‘threat’ from Russia, and the question of the Trident’s future in an independent Scotland. By playing up the idea of a real, imminent danger from Russia, it persuades the viewer of the importance of retaining Britain’s nuclear deterrent. As tensions grow between East and West, and Boris Johnson pursues his ‘Global Britain’ strategy, we will no doubt see more programmes emphasising Britain’s military strength countering Russia and let’s not forget, China. Sadly, such manipulation of the population doesn’t encourage understanding between peoples and instead, fosters division and discrimination. At best it is Britain using Russia as a scapegoat to bolster its sense of national pride; at worse, it is laying the groundwork for a future conflict with Russia.
Johanna Ross is a journalist based in Edinburgh, Scotland.
US Officials Demand Ban on Dr. Mercola’s Book
By Dr. Joseph Mercola | September 20, 2021
Since the publication of my book, “The Truth About COVID-19: Exposing The Great Reset, Lockdowns, Vaccine Passports, and the New Normal,” which became an instant best seller on Amazon.com, there’s been a significant increase in censorship and ruthless attacks.
Sadly, many of these attacks have been levied by the very people elected to safeguard democracy and our Constitutional rights. Most recently, U.S. Sen. Elizabeth Warren, D-Mass., sent a letter1 to Andy Jassy, chief executive officer of Amazon.com, demanding an “immediate review” of Amazon’s algorithms to weed out books peddling “COVID misinformation.”2,3,4
Warren specifically singled out “The Truth About COVID-19” as a prime example of “highly-ranked and favorably-tagged books based on falsehoods about COVID-19 vaccines and cures” that she wants to see banned from sale.
“Dr. Mercola has been described as ‘the most influential spreader of coronavirus misinformation online,” Warren writes,5 adding: “Not only was this book the top result when searching either ‘COVID-19’ or ‘vaccine’ in the categories of ‘All Departments’ and ‘Books’; it was tagged as a ‘Best Seller’ by Amazon and the ‘#1 Best Seller’ in the ‘Political Freedom’ category.
The book perpetuates dangerous conspiracies about COVID-19 and false and misleading information about vaccines. It asserts that vitamin C, vitamin D and quercetin … can prevent COVID-19 infection … And the book contends that vaccines cannot be trusted, when study after study has demonstrated the overwhelming effectiveness and safety of COVID-19 vaccines.
It should come as no surprise that the book is rife with misinformation. One of the authors, Dr. Mercola, is one of the ‘Disinformation Dozen,’ a group responsible for 65% of anti-vaccine content on Facebook and Twitter …”
Two days later, September 9, 2021, U.S. Rep. Adam Schiff, D-Calif., followed in Warren’s footsteps, sending letters6 to Facebook and Amazon, calling for more prolific censorship of vaccine information.7
Modern-Day Book Burning
Essentially, what Warren is calling for is modern-day book burning. “The Truth About COVID-19” exposes the hidden agenda behind the pandemic, showing the countermeasures have nothing to do with public health and everything to do with ushering in a new social and economic system based on totalitarian technocracy-led control. So, it’s not misinformation they fear. It’s the truth they want to prevent from spreading.
To make her case, Warren leans on a discredited report by the Center for Countering Digital Hate (CCDH). In that report, “The Disinformation Dozen,”8 the CCDH founder Imran Ahmed claims to have identified the top most influential “anti-vaxxers” in the U.S. The problem is Ahmed made that up.
CCDH ‘Manufactured Narrative Without Evidence’ Facebook Says
August 18, 2021 — nearly three weeks before Warren sent that letter to Amazon — Facebook actually called out the CCDH for having manufactured a faulty narrative without evidence against the 12 individuals targeted in its reports.9 Monika Bickert, vice president of Facebook content policy, set the record straight, stating:10
“In recent weeks, there has been a debate about whether the global problem of COVID-19 vaccine misinformation can be solved simply by removing 12 people from social media platforms. People who have advanced this narrative contend that these 12 people are responsible for 73% of online vaccine misinformation on Facebook. There isn’t any evidence to support this claim …
That said, any amount of COVID-19 vaccine misinformation that violates our policies is too much by our standards — and we have removed over three dozen Pages, groups and Facebook or Instagram accounts linked to these 12 people, including at least one linked to each of the 12 people, for violating our policies.
We have also imposed penalties on nearly two dozen additional Pages, groups or accounts linked to these 12 people, like moving their posts lower in News Feed so fewer people see them or not recommending them to others. We’ve applied penalties to some of their website domains as well so any posts including their website content are moved lower in News Feed.
The remaining accounts associated with these individuals are not posting content that breaks our rules, have only posted a small amount of violating content, which we’ve removed, or are simply inactive.
In fact, these 12 people are responsible for about just 0.05% of all views of vaccine-related content on Facebook. This includes all vaccine-related posts they’ve shared, whether true or false, as well as URLs associated with these people.
The report11 upon which the faulty narrative is based analyzed only a narrow set of 483 pieces of content over six weeks from only 30 groups, some of which are as small as 2,500 users. They are in no way representative of the hundreds of millions of posts that people have shared about COVID-19 vaccines in the past months on Facebook.
Further, there is no explanation for how the organization behind the report identified the content they describe as ‘anti-vax’ or how they chose the 30 groups they included in their analysis. There is no justification for their claim that their data constitute a ‘representative sample’ of the content shared across our apps.”
‘Disinfo Dozen’ Barely Register on the Social Media Radar
In its report, the CCDH claims 12 people, including me, are responsible for 65% of anti-vaccine content on social media. I’m not sure where Bickert got the 73% figure from. Either way, we’re not responsible for anywhere near either 65% or 73%.
According to Facebook’s own investigation, we account for a minuscule 0.05% of vaccine-related content — 1,460 times lower than the CCDH’s outrageous claim. Still, Warren and myriad other government officials are using the CCDH as some sort of ultimate authority.
U.S. Surgeon General Dr. Vivek Murthy, White House press secretary Jen Psaki and President Biden have all used the CCDH as the sole source for their wild assertions. Now, Warren wants to use the CCDH’s fraudulent report to ban the sale of certain books, and she does so even after Facebook itself has refuted the CCDH report as being baseless!
In an email, Kara Fredrick, a research fellow in technology policy at the Heritage Foundation, told Fox News that:12
“Warren’s push for more censorship is yet another example of the growing symbiosis between Big Tech and big government,” and is indicative of a “broader trend: That of the Biden Administration and other progressive officials attempting to circumvent the Constitution by pressuring private tech companies to restrict freedom of expression under a broad definition of misinformation.”
Fredrick further stressed that “A healthy body politic depends on the genuine interrogation of ideas,” and that “Big Tech companies’ eagerness to suppress specific points of view is already corroding our free society.”
Freedom Is Corroding Before Our Eyes
Indeed, in early August 2021, I decided to remove the entire article archive from my website — articles I’ve made available for free for the last 24 years — and only make new articles readable for 48 hours. I did this in an effort to appease the power players who have an arsenal of overwhelming tools at their disposal, and are actively using them against us.
Cyberwarfare and authoritarian forces are beyond our abilities to withstand, and these changes were deemed necessary to keep us moving forward, even if hobbled. Still, Warren is not satisfied. She wants me silenced entirely. She doesn’t even want people willing to pay for the information to have access to it.
Clearly, she’s panicked about something. Reading her letter, I see before me the giant Goliath, yelling and screaming for help, demanding an army of fighters because the pea-sized David with his makeshift slingshot is in the neighborhood.
What is she really afraid of? Why pick on a person whose social media reach is a fraction of 0.05%? Could it be because the ‘Disinfo Dozen’ are actually telling the truth, and the truth has a tendency to win against all odds?
Goal Posts Set in Shifting Quicksand
According to U.S. Centers for Disease Control and Prevention data, Biden met his 70% vaccination rate at the beginning of August 2021.13 For months, we were told that all would be well and good if only we would meet the goal of 70%.
Yet as soon as it was met, we were told 70% “should be seen as a floor, rather than a ceiling” and Biden went on the news saying his patience with the vaccine hesitant is “wearing thin.” Because a small minority — if we are to believe CDC data — refuses to take the shot despite myriad bribes, Biden is now calling on businesses with more than 100 employees to mandate the COVID shots or face fines.
It’s beyond irrational, and to many seems highly irrational, unjustified and unconstitutional. This is especially egregious as ALL illness and injury expenses will be paid by the patient, even though they were forced to take the injection as the companies have zero liability.
However, as noted by Dr. Peter Breggin in yesterday’s interview, these actions are completely logical once you realize we are at war, and there are evil people out there who are intentionally trying to hurt us under the banner of providing protection. It’s no different than being in an abusive relationship where the abuser says he or she is beating you and locking you in the basement “to make you a better person.”
The Web of Elite Extremists Behind the Censorship
I’ve written many articles over the years about attempts by various groups and organizations to smear my credibility and label this site as a fake news hub. In March 2021, it was The Bureau of Investigative Journalism (TBIJ) that accused me of spreading misinformation about vaccines and COVID-19.14
Not surprisingly, TBIJ is funded by Bill Gates,15,16 a leading force within the technocratic takeover movement who doles out money to anything and anyone that will help further the globalist agenda, including media.17
In November 2019, as if blessed with some particular foresight, the Bill & Melinda Gates Foundation gave TBIJ a $1,068,169 grant from its “Global Health and Development Public Awareness and Analysis” advocacy program.18
Other TBIJ sponsors include19 the Google News Initiative,20 George Soros’ Open Society Foundation and the Wellcome Trust.21 All of these — Gates, Google, Soros and Wellcome — are easily identified as parts of the technocratic globalist network that is reaping unprecedented financial rewards from the pandemic.
Whose Interests Does CCDH Protect and Promote?
While the financial supporters of the CCDH are far more opaque, it seems clear this group is yet another front for the technocratic power structure. It’s founded by a British national and unregistered foreign agent named Imran Ahmed, who is also a member of the Steering Committee on Countering Extremism Pilot Task Force under the British government’s Commission for Countering Extremism.
When you think about it, isn’t it rather curious that American government officials are targeting and violating the Constitutional rights of citizens based on the opinions of an unregistered foreign agent funded by dark money?22 As noted in a July 20, 2021, Drill Down article:23
“When a report goes viral in the news cycle, it only makes sense to question where it came from — especially if that report has influence all the way up to the Oval Office, affecting public health policy, while also having dangerous implications for free speech.
The Center for Countering Digital Hate … released a bombshell report earlier this week. It was picked up everywhere and had the following revelation: The majority of COVID misinformation came from just 12 people … But could this be a wily gambit by outside interests to justify the Biden administration’s censorship partner-up with Big Tech? …
According to its website, the left-wing Center for Countering Digital Hate prides itself on ‘researching, exposing, and then shutting down users and news sites it deems unacceptable in the digital sphere.’
Users and news sites it deems unacceptable? That seems potentially dangerous, considering we know very little about the CCDH. Senator Josh Hawley (R-MO) expressed his concerns on Twitter with the following post:
‘Who is funding this overseas dark money group — Big Tech? Billionaire activists? Foreign governments? We have no idea. Americans deserve to know what foreign interests are attempting to influence American democracy’ …
No one knows who funds them. No one knows who is driving their research. But their findings are being used in censorship efforts under the guise of controlling misinformation?”
Violating Bioethical Principles Puts Lives at Risk
The sad irony is that government officials are really the ones contributing to most of the unnecessary death and suffering by not adhering to bioethical principles that are enshrined in law. These laws exist for a good reason. They protect people from unnecessary harm and unwanted medical risks.
As an experimental trial participant, which is what everyone is at the moment who accepts a COVID shot, you have the right to receive full disclosure of any adverse event risks. Based on that disclosure, you then have the right to decide whether you want to participate.
Adverse event risk disclosure should be provided at the level of detail disclosed in any drug package insert. Not only do vaccinees not get any such disclosure documents, the censorship also prevents them from getting any balancing information regarding their risk-reward ratio, along with risk of death and permanent disability, from other sources, be it through Google searches, social media or mainstream news.
When given just one side of the story, informed consent simply isn’t possible, and as such, violates several different national and international laws, including the U.S. Code of Federal Regulations 45 CFR 46 (subpart A, the Belmont report),24 the International Covenant on Civil and Political Rights treaty,25 the Declaration of Helsinki26 and the Nuremberg Code.27 U.S. Supreme Court rulings have also clarified that Americans have the right to choose their own health care in general.28,29
As just one example of many, Marie Follmer, in an interview with Robert F. Kennedy Jr.,30 said no one ever warned her there was a risk of myocarditis. Her athletic son, Greyson, took the shot and is now unable to do much of anything and she fears he might die.
She admits not doing any of her own research, blindly trusting what she was told. Now, she distrusts the whole process, including doctors, as all have refused to acknowledge that there might be a link to the shot, and no one knows how to treat him.
Most importantly, the acceptance of an experimental product must be fully voluntary and uncoerced. Enticement is forbidden. It’s downright impossible to argue that incentives ranging from free junk food to million-dollar lotteries and threats of losing your job, refusal of an education, travel and shopping restrictions and more do not constitute coercion.
At the end of the day, if you decide you want to participate in a medical experiment, whatever it might be, that’s up to you. But everyone else also has that same right to choose.
Sen. Warren Threatens Amazon to Ban ‘The Truth About COVID-19’
Since the publication of my latest book, “The Truth About COVID-19” there’s been a significant increase in calls for censorship and ruthless attacks against me.
Most recently, so-called “progressive” U.S. Sen. Elizabeth Warren, D-Mass., in an outrageous, slanderous and basically unconstitutional attempt to suppress free speech, sent a letter to Amazon, demanding an “immediate review” of their algorithms to weed out books peddling “COVID misinformation.”
Warren specifically singled out “The Truth About COVID-19” as a prime example of “highly ranked and favorably tagged books based on falsehoods about COVID-19 vaccines and cures” that she wants to see banned from sale.
Two days later, U.S. Rep. Adam Schiff, D-Calif., followed in Warren’s footsteps, sending letters to Facebook and Amazon, calling for more prolific censorship of vaccine information. Even President Joe Biden has recently used a debunked report as his sole source to call for my censorship.
Sadly, these attacks are being levied by the very people elected to safeguard democracy and our Constitutional rights. Essentially, what they are calling for is modern-day book burning. This is a democracy, not a monarchy.
Sources and References
- 1, 5 Warren’s letter to Andy Jassy September 7, 2021
- 2 National Interest September 12, 2021
- 3 The Guardian September 13, 2021
- 4 New York Times September 8, 2021
- 6 Twitter Adam Schiff September 9, 2021
- 7 The Hill September 9, 2021
- 8, 11 CCDH, The Disinformation Dozen
- 9, 10 Facebook August 18, 2021
- 12 Fox News September 13, 2021
- 13 CNBC August 2, 2021
- 14 TBIJ February 28, 2021
- 15, 19 TBIJ Sponsors and Supporters
- 16, 18 Bill & Melinda Gates Foundation Grant to TBIJ November 2019
- 17 Columbia Journalism Review August 21, 2020
- 20 Thebureauinvestigates.com Bureau Fellowship
- 21 Wellcome Trust
- 22 The Federalist July 20, 2021
- 23 The Drill Down July 20, 2021
- 24 HHS.gov The Belmont Report
- 25 UN International Covenant on Civil and Political Rights
- 26 WMA Declaration of Helsinki
- 27 British Medical Journal December 7, 1996; 7070(313): 1448 (PDF)
- 28 Justia Rochin v. California
- 29 Justia Griswold v. Connecticut
- 30 Podbean The Defender, Child Casualty in Ohio
APOE-4: The Clue to Why Low Fat Diet and Statins may Cause Alzheimer’s
By Dr. Stephanie Seneff | December 15, 2009
Abstract
Alzheimer’s is a devastating disease whose incidence is clearly on the rise in America. Fortunately, a significant number of research dollars are currently being spent to try to understand what causes Alzheimer’s. ApoE-4, a particular allele of the apolipoprotein apoE, is a known risk factor. Since apoE plays a critical role in the transport of cholesterol and fats to the brain, it can be hypothesized that insufficient fat and cholesterol in the brain play a critical role in the disease process. In a remarkable recent study, it was found that Alzheimer’s patients have only 1/6 of the concentration of free fatty acids in the cerebrospinal fluid compared to individuals without Alzheimer’s. In parallel, it is becoming very clear that cholesterol is pervasive in the brain, and that it plays a critical role both in nerve transport in the synapse and in maintaining the health of the myelin sheath coating nerve fibers. An extremely high-fat (ketogenic) diet has been found to improve cognitive ability in Alzheimer’s patients. These and other observations described below lead me to conclude that both a low-fat diet and statin drug treatment increase susceptibility to Alzheimer’s.
1. Introduction
Alzheimer’s is a devastating disease that takes away the mind bit by bit over a period of decades. It begins as odd memory gaps but then steadily erodes your life to the point where around-the-clock care is the only option. With severe Alzheimer’s, you can easily wander off and get lost, and may not even recognize your own daughter. Alzheimer’s was a little known disease before 1960, but today it threatens to completely derail the health system in the United States.
Currently, over 5 million people in America have Alzheimer’s. On average, a person over 65 with Alzheimer’s costs three times as much for health care as one without Alzheimer’s. More alarmingly, the incidence of Alzheimer’s is on the rise. Dr. Murray Waldman has studied epidemiological data comparing Alzheimer’s with femur fractures, looking back over the last fifty years [52]. Alarmingly, he has found that, while the incidence of femur fractures (another condition which typically increases with age) has gone up only at a linear rate, the increase in the incidence of Alzheimer’s has gone up exponentially, between 1960 and 2010 Alzheimer’s Epidemic [15]. Just between 2000 and 2006, US Alzheimer’s deaths rose by 47%, while, by comparison, deaths from heart disease, breast cancer, prostate cancer, and stroke combined decreased by 11%. This increase goes far beyond people living longer: for people 85 and older, the percentage who died from Alzheimer’s rose by 30% between 2000 and 2005 [2]. Finally, it’s likely these are under-estimates, as many people suffering with Alzheimer’s ultimately die of something else. You likely have a close friend or relative who is suffering from Alzheimer’s.
Something in our current lifestyle is increasing the likelihood that we will succumb to Alzheimer’s. My belief is that two major contributors are our current obsession with low-fat diet, combined with the ever expanding use of statin drugs. I have argued elsewhere that low-fat diet may be a major factor in the alarming increase in autism and adhd in children. I have also argued that the obesity epidemic and the associated metabolic syndrome can be traced to excessive low-fat diet. Statins are likely contributing to an increase in many serious health issues besides Alzheimer’s, such as sepsis, heart failure, fetal damage, and cancer, as I have argued here. I believe the trends will only get worse in the future, unless we substantially alter our current view of “healthy living.”
The ideas developed in this essay are the result of extensive on-line research I conducted to try to understand the process by which Alzheimer’s develops. Fortunately, a great deal of research money is currently being spent on Alzheimer’s, but a clearly articulated cause is still elusive. However, many exciting leads are fresh off the press, and the puzzle pieces are beginning to assemble themselves into a coherent story. Researchers are only recently discovering that both fat and cholesterol are severly deficient in the Alzheimer’s brain. It turns out that fat and cholesterol are both vital nutrients in the brain. The brain contains only 2% of the body’s mass, but 25% of the total cholesterol. Cholesterol is essential both in transmitting nerve signals and in fighting off infections.
A crucial piece of the puzzle is a genetic marker that predisposes people to Alzheimer’s, termed “apoE-4.” ApoE plays a central role in the transport of fats and cholesterol. There are currently five known distinct variants of apoE (properly termed “alleles”), with the ones labelled “2”, “3” and “4” being the most prevalent. ApoE-2 has been shown to afford some protection against Alzheimer’s; apoE-3 is the most common “default” allele, and apoE-4, present in 13-15% of the population, is the allele that is associated with increased risk to Alzheimer’s. A person with apoE-4 allele inherited from both their mother and their father has up to a twenty-fold increased likelihood of developing Alzheimer’s disease. However, only about 5% of the people with Alzheimer’s actually have the apoE-4 allele, so clearly there is something else going on for the rest of them. Nonetheless, understanding apoE’s many roles in the body was a key step leading to my proposed low fat/statin theory.
2. Background: Brain Biology 101
Although I have tried to write this essay in a way that is accessible to the non-expert, it will still be helpful to first familiarize you with basic knowledge of the structure of the brain and the roles played by different cell types within the brain.
At the simplest level, the brain can be characterized as consisting of two major components: the gray matter and the white matter. The gray matter comprises the bodies of the neurons, including the cell nucleus, and the white matter contains the myriad of “wires” that connect each neuron to every other neuron it communicates with. The wires are known as “axons” and they can be quite long, connecting, for example, neurons in the frontal cortex (above the eyes) with other neurons deep in the interior of the brain concerned with memory and movement. The axons will figure prominently in the discussions below, because they are coated with a fatty substance called the myelin sheath, and this insulating layer is known to be defective in Alzheimer’s. Neurons pick up signals transmitted through the axons at junctures known as synapses. Here the message needs to be transmitted from one neuron to another one, and various neurotransmitters such as dopamine and GABA exert excitatory or inhibitory influences on signal strength. In adidtion to a single axon, neurons typically have several much shorter nerve fibers called dendrites, whose job is to receive incoming signals from diverse sources. At a given point in time, signals received from multiple sources are integrated in the cell body and a decision is made as to whether the accumulated signal strength is above threshold, in which case the neuron responds by firing a sequence of electrical pulses, which are then transmitted through the axon to a possibly distant destination.
In addition to the neurons, the brain also contains a large number of “helper” cells called glial cells, which are concerned with the care and feeding of neurons. Three principle types of glial cells will play a role in our later discussion: the microglia, the astrocytes, and the oligodendrocytes. Microglia are the equivalent of white blood cells in the rest of the body. They are concerned with fighting off infective agents such as bacteria and viruses, and they also monitor neuron health, making life-and-death decisions: programming a particular neuron for apoptosis (intentional self-destruction) if it appears to be malfunctioning beyond hope of recovery, or is infected with an organism that is too dangerous to let flourish.
The astrocytes figure very prominently in our story below. They nestle up against the neurons and are responsible for assuring an adequate supply of nutrients. Studies on neuron cultures from rodent central nervous systems have shown that neurons depend upon astrocytes for their supply of cholesterol [40]. Neurons critically need cholesterol, both in the synapse [50] and in the myelin sheath [45], in order to successfully transmit their signals, and also as a first line of defense against invasive microbes. Cholesterol is so important to the brain that astrocytes are able to synthesize it from basic ingredients, a skill not found in most cell types. They also supply the neurons with fatty acids, and they are able to take in short chain fatty acids and combine them to form the longer-chain types of fatty acids that are especially prominent in the brain [7][24][36], and then deliver them to neighboring neurons and to the cerebrospinal fluid.
The third type of glial cell is the oligodendrocyte. These cells specialize in making sure the myelin sheath is healthy. Oligodentrocytes synthesize a special sulfur-containing fatty acid, known as sulfatide, from other fatty acids supplied to them by the cerebrospinal fluid [9]. Sulfatide has been shown to be essential for the maintenance of the myelin sheath. Children born with a defect in the ability to metabolize sulfatide suffer from progressive demyelination, and rapid loss of motor and cognitive functions, resulting in an early death before the age of 5 [29]. Depletion in sulfatide is a well-known characterization of Alzheimer’s, even in early stages before it has been manifested as cognitive decline [18]. And ApoE has been shown to play a crucial role in the maintenance of sulfatide [19]. Throughout a person’s life, the myelin sheath has to be constantly maintained and repaired. This is something that researchers are only beginning to appreciate, but two related properties of Alzheimer’s are poor quality myelin sheath alongside a drastically reduced concentration of fatty acids and cholesterol in the cerebrospinal fluid [38].
3. Cholesterol and Lipid Management
In addition to some knowledge about the brain, you will also need to know something about the processes that deliver fats and cholesterol to all the tissues of the body, with a special focus on the brain. Most cell types can use either fats or glucose (a simple sugar derived from carbohydrates) as a fuel source to satisfy their energy needs. However, the brain is the one huge exception to this rule. All cells in the brain, both the neurons and the glial cells, are unable to utilize fats for fuel. This is likely because fats are too precious to the brain. The myelin sheath requires a constant supply of high quality fat to insulate and protect the enclosed axons. Since the brain needs its fats to survive long-term, it is paramount to protect them from oxidation (by exposure to oxygen) and from attack by invasive microbes.
Fats come in all kinds of shapes and sizes. One dimension is the degree of saturation, which concerns how many double bonds they possess, with saturated fats possessing none, monounsaturated fats having only one, and polyunsaturated fats having two or more. Oxygen breaks the double bond and leaves the fat oxidized, which is problematic for the brain. Polyunsaturated fats are thus the most vulnerable to oxygen exposure, because of multiple double bonds.
Fats are digested in the intestine and released into the blood stream in the form of a relatively large ball with a protective protein coat, called a chylomicron. The chylomicron can directly provide fuel to many cell types, but it may also be sent to the liver where the contained fats are sorted out and redistributed into much smaller particles, which also contain substantial amounts of cholesterol. These particles are called “lipoproteins,” (henceforth, LPP’s) because they contain protein in the spherical shell and lipids (fats) in the interior. If you’ve had your cholesterol measured, you’ve probably heard of LDL (low density LPP) and HDL (high density LPP). If you think these are two different kinds of cholesterol, you would be mistaken. They are just two different kinds of containers for cholesterol and fats that serve different roles in the body. There are actually several other LPP’s, for example, VLDL (very-low) and IDL (intermediate), as shown in the accompanying diagram.  In this essay I will refer to these collectively as the XDL’s. As if this weren’t confusing enough, there is also another unique XDL that is found only in the cerebrospinal fluid, that supplies the nutritional needs of the brain and nervous system. This one doesn’t seem to have a name yet, but I will call it “B-HDL,” because it is like HDL in terms of its size, and “B” is for “brain [13]”
In this essay I will refer to these collectively as the XDL’s. As if this weren’t confusing enough, there is also another unique XDL that is found only in the cerebrospinal fluid, that supplies the nutritional needs of the brain and nervous system. This one doesn’t seem to have a name yet, but I will call it “B-HDL,” because it is like HDL in terms of its size, and “B” is for “brain [13]”
An important point about all the XDL’s is that they contain distinctly different compositions, and each is targeted (programmed) for specific tissues. A set of proteins called “apolipoproteins” or, equivalently, “apoproteins” (“apo’s” for short) figure strongly in controlling who gets what. As you can see from the schematic of the chylomicron shown at the right, it contains a rainbow of different apo’s for every conceivable application. But the XDL’s are far more specific, with HDL containing “A,” LDL containing “B,” VLDL containing “B” and “C,” and IDL containing only “E.” The apo’s have special binding properties that allow the lipid contents to be transported across cell membranes so that the cell can gain access to the fats and choleseterol contained inside.
gets what. As you can see from the schematic of the chylomicron shown at the right, it contains a rainbow of different apo’s for every conceivable application. But the XDL’s are far more specific, with HDL containing “A,” LDL containing “B,” VLDL containing “B” and “C,” and IDL containing only “E.” The apo’s have special binding properties that allow the lipid contents to be transported across cell membranes so that the cell can gain access to the fats and choleseterol contained inside.
The only apo that is of concern to us in the context of this essay is apoE. ApoE is very important to our story because of its known link with Alzheimer’s disease. ApoE is a protein, i.e., sequence of amino acids, and its specific composition is dictated by a corresponding DNA sequence on a protein-coding gene. Certain alterations in the DNA code lead to defects in the ability of the transcribed protein to perform its biological roles. ApoE-4, the allele associated with increased risk to Alzheimer’s, is presumably unable to perform its tasks as efficiently as the other alleles. By understanding what apoE does, we can better infer how the consequences of doing it poorly might impact the brain, and then observe experimentally whether the features of the Alzheimer’s brain are consistent with the roles played by apoE.
A strong clue about apoE’s roles can be deduced from where it is found. As I mentioned above, it is the only apo in both B-HDL in the cerebrospinal fluid and IDL in the blood serum. Only selected cell types can synthesize it, the two most significant of which for our purposes are the liver and the astrocytes in the brain. Thus the astrocytes provide the linkage between the blood and the cerebrospinal fluid. They can usher lipids and cholesterol across the blood-brain barrier, via the special key which is apoE.
It turns out that, although apoE is not found in LDL, it does bind to LDL, and this means that astrocytes can unlock the key to LDL in the same way that they can gain access to IDL, and hence the cholesterol and fatty acid contents of LDL are accessible to astrocytes as well, as long as apoE is functioning properly. The astrocytes reshape and repackage the lipids and release them into the cerebospinal fluid, both as B-HDL and simply as free fatty acids, available for uptake by all parts of the brain and nervous system [13].
One of the critical reshaping steps is to convert the fats into types that are more attractive to the brain. To understand this process you need to know about another dimension of fats besides their degree of saturation, which is their total length. Fats have a chain of linked carbon atoms as their spine, and the total number of carbons in a particular fat characterizes it as short, medium length, or long. The brain works best when the constituent fats are long, and, indeed, the astrocytes are able to take in short chain fats and reorganize them to make longer chain fats [24].
A final dimension of fats that plays a role is where the first double bond is located in a polyunsaturated fat, which distinguishes omega-3 from omega-6 fats (position 3; position 6). Omega-3 fats are very common in the brain. Certain ones of the omega-3 and omega-6 fats are essential fatty acids, in that the human body is unable to synthesize them, and therefore depends upon their supply from the diet. This is why it is claimed that fish “makes you smart”: because cold water fish is the best source of essential omega-3 fats.
Now I want to return to the subject of the XDL’s. It is a dangerous journey from the liver to the brain, as both oxygen and microbes are found in abundance in the blood stream. The XDL’s protective shell contains both LPP’s andunesterified cholesterol, as well as the signature apo that controls which cells can receive the contents, as shown in the accompanying schematic.  The internal contents are esterified cholesterol and fatty acids, along with certain antioxidants that are conveniently being transported to the cells packaged in the same cargo ship. Esterification is a technique to render the fats and cholesterol inert, which helps protect them from oxidation [51]. Having the antioxidants (such as vitamin E and Coenzyme Q10) along for the ride is also convenient, as they too protect against oxidation. The cholesterol contained in the shell, however, is intentionally not esterified, which means that it is active. One of its roles there is to guard against invasive bacteria and viruses [55]. Cholesterol is the first line of defense against these microbes, as it will alert the white blood cells to attack whenever it encounters dangerous pathogens. It has also been proposed that the cholesterol in the XDL’s shell itself acts as an antioxidant [48].
The internal contents are esterified cholesterol and fatty acids, along with certain antioxidants that are conveniently being transported to the cells packaged in the same cargo ship. Esterification is a technique to render the fats and cholesterol inert, which helps protect them from oxidation [51]. Having the antioxidants (such as vitamin E and Coenzyme Q10) along for the ride is also convenient, as they too protect against oxidation. The cholesterol contained in the shell, however, is intentionally not esterified, which means that it is active. One of its roles there is to guard against invasive bacteria and viruses [55]. Cholesterol is the first line of defense against these microbes, as it will alert the white blood cells to attack whenever it encounters dangerous pathogens. It has also been proposed that the cholesterol in the XDL’s shell itself acts as an antioxidant [48].
HDL’s are mostly depleted of the lipid and cholesterol content, and they are tasked with returning the empty shell back to the liver. Once there, cholesterol will be recommissioned to enter the digestive system as part of the bile, which is produced by the gall bladder to help digest ingested fats. But the body is very careful to conserve cholesterol, so that 90% of it will be recycled from the gut back into the blood stream, contained in the chylomicron that began our story about fats.
In summary, the management of the distribution of fats and cholesterol to the cells of the body is a complex process, carefully orchestrated to assure that they will have a safe journey to their destination. Dangers lurk in the blood stream, mostly in the form of oxygen and invasive microbes. The body considers cholesterol to be precious cargo, and it is very careful to conserve it, by recycling it from the gut back to the liver, to be appropriately distributed among the XDL’s that will deliver both cholesterol and fats to the tissues that depend upon them, most especially the brain and nervous system.
4. The Relationship between Cholesterol and Alzheimer’s
Through retrospective studies, the statin industry has been very successful at the game of pretending that benefits derived from high cholesterol are actually due to statins, as I have described at length in an essay on the relationship between statins and fetal damage, sepsis, cancer, and heart failure. In the case of Alzheimer’s, they are playing this game in reverse: they are blaming cholesterol for a very serious problem that I believe is actually caused by statins.
The statin industry has looked long and hard for evidence that high cholesterol might be a risk factor for Alzheimer’s. They examined cholesterol levels for men and women of all ages between 50 and 100, looking back 30 or more years if necesssary, to see if there was ever a correlation between high cholesterol and Alzheimer’s. They found only one statistically significant relationship: men who had had high cholesterol in their 50’s had an increased susceptibility to Alzheimer’s much later in life [3].
The statin industry has jumped on this opportunity to imply that high cholesterol might cause Alzheimer’s, and, indeed, they have been very fortunate in that reporters have taken the bait and are promoting the idea that, if high cholesterol many years ago is linked to Alzheimer’s, then statins might protect from Alzheimer’s. Fortunately, there exist lengthy web pages (Cholesterol Doesn’t Cause Alzheimer’s) that have documented the long list of reasons why this idea is absurd.
Men who have high cholesterol in their 50’s are the poster child for statin treatment: all of the studies that have shown a benefit for statins in terms of reducing the number of minor heart attacks involved men in their 50’s. High cholesterol is positively correlated with longevity in people over 85 years old [54], and has been shown to be associated with better memory function [53] and reduced dementia [35]. The converse is also true: a correlation between falling cholesterol levels and Alzheimer’s [39]. As will be discussed further later, people with Alzheimer’s also have reduced levels of B-HDL, as well as sharply reduced levels of fatty acids, in the cerbrospinal fluid, i.e, impoverished supply of cholesterol and fats to the myelin sheath [38]. As we saw earlier, fatty acid supply is essential as building blocks for the sulfatide that is synthesized by oligodendrocytes to keep the myelin sheath healthy [29].
The obvious study that needs to be done is to bin the men who had high cholesterol in their 50’s into three groups: those who never took statins, those who took smaller doses for shorter times, and those who took larger doses for longer times. Such a study would not be hard to do; in fact, I suspect something like it has already been done. But you’ll never hear about it because the statin industry has buried the results.
In a very long term retrospective cohort study of members of the Permanente Medical Care Program in northern California, researchers looked at cholesterol data that were obtained between 1964 and 1973 [46]. They studied nearly ten thousand people who had remained members of that health plan in 1994, upon the release of computerized outpatient diagnoses of dementia (both Alzheimer’s and vascular dementia). The subjects were between 40 and 45 years old when the cholesterol data were collected.
The researchers found a barely statistically significant result that people who were diagnosed with Alzheimer’s had higher cholesterol in their 50’s than the control group. The mean value for the Alzheimer’s patients was 228.5, as against 224.1 for the controls.
The question that everybody ought to be asking is: for the Alzheimer’s group, how did the people who later took statins stack up against the people who didn’t? In extreme understatement, the authors offhandedly remark in the middle of a paragraph: “Information on lipid-lowering treatments, which have been suggested to decrease dementia risk [31], was not available for this study.” You can be sure that, if there was any inkling that the statins might have helped, these researchers would have been allowed access to those data.
The article they refer to for support, reference [19] in [46] (which is reference [44] here) was very weak. The abstract for that article is repeated in full here in the Appendix. But the concluding sentence sums it up well: “A more than a modest role for statins in preventing AD [Alzheimer’s Disease] seems unlikely.” This is the best they can come up with to defend the position that statins might protect from Alzheimer’s.
An intuitive explanation for why high cholesterol at an early age might be correlated with Alzheimer’s risk has to do with apoE-4. People with that allele are known to have high cholesterol early in life [39], and I believe this is a protective strategy on the part of the body. The apoE-4 allele is likely defective in the task of importing cholesterol into the astrocytes, and therefore an increase in the bioavailability of cholesterol in blood serum would help to offset this deficit. Taking a statin would be the last thing a person in that situation would want to do.
5. Do Statins Cause Alzheimer’s?
There is a clear reason why statins would promote Alzheimer’s. They cripple the liver’s ability to synthesize cholesterol, and as a consequence the level of LDL in the blood plummets. Cholesterol plays a crucial role in the brain, both in terms of enabling signal transport across the synapse [50] and in terms of encouraging the growth of neurons through healthy development of the myelin sheath [45]. Nonetheless, the statin industry proudly boasts that statins are effective at interfering with cholesterol production in the brain [31][47] as well as in the liver.
Yeon-Kyun Shin is an expert on the physical mechanism of cholesterol in the synapse to promote transmission of neural messages, and one of the authors of [50] referenced earlier. In an interview by a Science Daily reporter, Shin said: “If you deprive cholesterol from the brain, then you directly affect the machinery that triggers the release of neurotransmitters. Neurotransmitters affect the data-processing and memory functions. In other words — how smart you are and how well you remember things.”
A recent review of two large population-based double-blind placebo-controlled studies of statin medications in individuals at risk for dementia and Alzheimer disease showed that statins are not protective against Alzheimer’s [34]. The lead author of the study, Bernadette McGuinness, was quoted by a reporter from Science Daily as saying, “From these trials, which contained very large numbers and were the gold standard — it appears that statins given in late life to individuals at risk of vascular disease do not prevent against dementia.” A researcher at UCLA, Beatrice Golomb, when asked to comment on the results, was even more negative, saying, “Regarding statins as preventive medicines, there are a number of individual cases in case reports and case series where cognition is clearly and reproducibly adversely affected by statins.” In the interview, Golomb remarked that various randomized trials have shown that statins were either adverse or neutral towards cognition, but none have shown a favorable response.
A common side effect of statins is memory dysfunction. Dr. Duane Graveline, fondly known as “spacedoc” because he served as a doctor to the astronauts, has been a strong advocate against statins and is collecting evidence of statin side effects directly from statin users around the world. He was led to this assault on statins as a consequence of his own personal experience of transient global amnesia, a frightening episode of total memory loss which he is convinced was caused by the statin drugs he was taking at the time. He has now completed three books describing a diverse collection of damning side effects of statins, the most famous of which is Lipitor: Thief of Memory [17].
A second way (besides their direct impact on cholesterol) in which statins likely impact Alzheimer’s is in their indirect negative effect on the supply of fatty acids and antioxidants to the brain. It is a given that statins drastically reduce the level of LDL in the blood serum. This is their claim to fame. It is interesting, however, that they succeed in reducing not just the amount of cholesterol contained in the LDL particles, but rather the actual number of LDL particles altogether. This means that, in addition to depleting cholesterol, they reduce the available supply to the brain of both fatty acids and antixodiants, which are also carried in the LDL particles. As we’ve seen, all three of these substances are essential to proper brain functioning.
I conjecture that the reasons for this indirect effect are two-fold: (1) there is inadequate cholesterol in the bile to metabolize dietary fats, and (2) the rate-limiting effect on the production of LDL is the ability to provide adequate cholesterol in the shell to assure survival of the contents during transport in the blood stream; i.e., to protect the contents from oxidation and marauding bacteria and viruses. People who take the highest 80 mg/dl dosage of statins often end up with LDL levels as low as 40mg/dl, well below even the lowest numbers observed naturally. I shudder to think of the probable long-term consequences of such severe depletion in fats, cholesterol, and antioxidants.
A third way in which statins may promote Alzheimer’s is by crippling the ability for cells to synthesize coenzyme Q10. Coenzyme Q10 has the misfortune of sharing the same metabolic pathway as cholesterol. Statins interfere with a crucial intermediate step on the pathway to the synthesis of both cholesterol and coenzyme Q10. Coenzyme Q10 is also known as “ubiquinone” because it seems to show up everywhere in cell metabolism. It is found both in the mitochondria and in the lysosomes, and its critical role in both places is as an antioxidant. The inert esters of both cholesterol and fatty acids are hydrolyzed and activated in the lysosomes [8], and then released into the cytoplasm. Coenzyme Q10 consumes excess oxygen to keep it from doing oxidative damage [30], while also generating energy in the form of ATP (adenosine triphosphate, the universal energy currency in biology).
The final way in which statins should increase Alzheimer’s risk is through their indirect effect on vitamin D.  Vitamin D is synthesized from cholesterol in the skin, upon exposure to UV rays from the sun. In fact, the chemical formula of vitamin D is almost indistinguishable from that of cholesterol, as shown in the two attached figures (cholesterol on the left, vitamin D on the right). If LDL levels are
Vitamin D is synthesized from cholesterol in the skin, upon exposure to UV rays from the sun. In fact, the chemical formula of vitamin D is almost indistinguishable from that of cholesterol, as shown in the two attached figures (cholesterol on the left, vitamin D on the right). If LDL levels are  kept artificially low, then the body will be unable to resupply adequate amounts of cholesterol to replenish the stores in the skin once they have been depleted. This would lead to vitamin D deficiency, which is a widespread problem in America.
kept artificially low, then the body will be unable to resupply adequate amounts of cholesterol to replenish the stores in the skin once they have been depleted. This would lead to vitamin D deficiency, which is a widespread problem in America.
It is well known that vitamin D fights infection. To quote from [25], “Patients with severe infections as in sepsis have a high prevalence of vitamin D deficiency and high mortality rates.” As will be elaborated on later, a large number of infective agents have been shown to be present in abnormally high amounts in the brains of Alzheimers patients [27][26].
Dr. Grant has recently argued [16] that there are many lines of evidence pointing to the idea that dementia is associated with vitamin D deficiency. An indirect argument is that vitamin D deficiency is associated with many conditions that in turn carry increased risk for dementia, such as diabetes, depression, osteoporosis, and cardiovascular disease. Vitamin D receptors are widespread in the brain, and it is likely that they play a role there in fighting off infection. Vitamin D surely plays other vital roles in the brain as well, as powerfully suggested by this quote taken from the abstract of [32]: “We conclude there is ample biological evidence to suggest an important role for vitamin D in brain development and function.”
6. Astrocytes, Glucose Metabolism, and Oxygen
Alzheimer’s is clearly correlated with a deficiency in the supply of fat and cholesterol to the brain. IDL, when functioning properly, is actually incredibly efficient in cholesterol and fat throughput from the blood across cell membranes, compared to LDL [8]. It gives up its contents much more readily than the other apo’s. And it achieves this as a direct consequence of apoE. IDL (as well as LDL) in the blood delivers fats and cholesterol to the astrocytes in the brain, and the astrocytes can thus use this external source instead of having to produce these nutrients themselves. I suspect, in fact, that astrocytes only produce a private supply when the external supply is insufficient, and they do so reluctantly.
Why would it be disadvantageous for an astrocyte to synthesize its own fats and cholesterol? In my opinion, the answer has to do with oxygen. An astrocyte needs a significant energy source to synthesize fats and cholesterol, and this energy is usually supplied by glucose from the blood stream. Furthermore, the end-product of glucose metabolism is acetyl-Coenzyme A, the precursor to both fatty acids and cholesterol. Glucose can be consumed very efficiently in the mitochondria, internal structures within the cell cytoplasm, via aerobic processes that require oxygen. The glucose is broken down to produce acetyl-Coenzyme A as an end-product, as well as ATP, the source of energy in all cells.
However, oxygen is toxic to lipids (fats), because it oxidizes them and makes them rancid. Lipids are fragile if not encased in a protective shell like IDL, HDL, or LDL. Once they are rancid they are susceptible to infection by invasive agents like bacteria and viruses. So an astrocyte trying to synthesize a lipid has to be very careful to keep oxygen out, yet oxygen is needed for efficient metabolism of glucose, which will provide both the fuel (ATP) and the raw materials (acetyl-Coenzyme A) for fat and cholesterol synthesis.
What to do? Well, it turns out that there is an alternative, although much less efficient, solution: to metabolize glucose anaerobically directly in the cytoplasm. This process does not depend on oxygen (a great advantage) but it also yields substantially less ATP (only 6 ATP as contrasted with 30 if glucose is metabolized aerobically in the mitochondria). The end product of this anaerobic step is a substance called pyruvate, which could be further broken down to yield a lot more energy, but this process is not accessible to all cells, and it turns out that the astrocytes need help for this to happen, which is where amyloid-beta comes in.
7. The Crucial Role of Amyloid-Beta
Amyloid-beta (also known as “abeta”) is the substance that forms the famous plaque that accumulates in the brains of Alzheimer’s patients. It has been believed by many (but not all) in the research community that amyloid-beta is the principal cause of Alzheimer’s, and as a consequence, researchers are actively seeking drugs that might destroy it. However, amyloid-beta has the unique capability of stimulating the production of an enzyme, lactate dehydrogenase, which promotes the breakdown of pyruvate (the product of anaerobic glucose metabolism) into lactate, through an anaerobic fermentation process, with the further production of a substantial amount of ATP.
The lactate, in turn, can be utilized itself as an energy source by some cells, and it has been established that neurons are on the short list of cell types that can metabolize lactate. So I conjecture that the lactate is transported from the astrocyte to a neighboring neuron to enhance its energy supply, thus reducing its dependence on glucose. It is also known that apoE can signal the production of amyloid-beta, but only under certain poorly understood environmental conditions. I suggest those environmental triggers have to do with the internal manufacture of fats and cholesterol as opposed to the extraction of these nutrients from the blood supply. I.e., amyloid-beta is produced as a consequence of environmental oxidative stress due to an inadequate supply of fats and cholesterol from the blood.
In addition to being utilized as an energy source by being broken down to lactate, pyruvate can also be used as a basic building block for synthesizing fatty acids. So anaerobic glucose metabolism, which yields pyruvate, is a win-win-win situation: (1) it significantly reduces the risk of exposure of fatty acids to oxygen, (2) it provides a source of fuel for neighboring neurons in the form of lactate, and (3) it provides a basic building block for fatty acid synthesis. But it depends upon amyloid-beta to work.
Thus, in my view (and in the view of others [28] [20] Amyloid-Beta and Alzheimer’s), amyloid-beta is not a cause of Alzheimer’s, but rather a protective device against it. The abstract of reference [28] arguing this point of view is reproduced in full in the Appendix. Several variants of a genetic defect associated with amyloid precursor protein (APP), the protein from which amyloid-beta is derived, have now been identified. A defect in this protein, which is associated with an increased risk of early onset Alzheimer’s, would likely lead to a reduced ability to synthesize amyloid-beta, which would then leave the brain with a big problem, since both the fuel and the basic building blocks for fatty acid synthesis would be in short supply, while oxygen trekking through the cell to the mitochondria would be exposing whatever fats were being synthesized to oxidation. The cell would likely be unable to keep up with need, and this would lead to a reduction in the number of fatty acids in the Alzheimer’s cerebrospinal fluid, a well-established characteristic of Alzheimer’s [38].
8. Cholesterol’s Role in the Brain
The brain comprises only 2% of the body’s total weight, yet it contains nearly 25% of the total cholesterol in the body. It has been determined that the limiting factor allowing the growth of synapses is the availability of cholesterol, supplied by the astrocytes. Cholesterol plays an incredibly important role in the synapse, by shaping the two cell membranes into a snug fit so that the signal can easily jump across the synapse [50]. So inadequate cholesterol in the synapse will weaken the signal at the outset, and inadequate fat coating the myelin sheath will further weaken it and slow it down during transport. A neuron that can’t send its messages is a useless neuron, and it only makes sense to prune it away and scavenge its contents.
The neurons that are damaged in Alzheimer’s are located in specific regions of the brain associated with memory and high level planning. These neurons need to transmit signals long distances between the frontal and prefrontal cortex and the hippocampus, housed in the midbrain. The transport of these signals depends on a strong and tight connection in the synapse, where the signal is transferred from one neuron to another, and a secure transmission across the long nerve fiber, a part of the white matter. The myelin sheath which coats the nerve fiber consists mainly of fatty acids, along with a substantial concentration of cholesterol. If it is not well insulated, the signal transmission rate will slow down and the signal strength will be severely reduced. Cholesterol is crucial for the myelin as well as for the synapse, as demonstrated dramatically through experiments conducted on genetically defective mice by Gesine Saher et al. [45]. These mutant mice lacked the ability to synthesize cholesterol in myelin-forming oligodendrocytes. They had severly disturbed myelin in their brains, and exhibited ataxia (uncoordinated muscle movements) and tremor. In the abstract, the authors wrote unequivocally, “This shows that cholesterol is an indispensable component of myelin membranes.”
In a post-mortem study comparing Alzheimer’s patients with a control group without Alzheimer’s, it was found that the Alzheimer’s patients had significantly reduced amounts of cholesterol, phospholipids (e.g, B-HDL), and free fatty acids in the cerebrospinal fluid than did the controls [38]. This was true irrespective of whether the Alzheimer’s patients were typed as apoE-4. In other words, reductions in these critical nutrients in the spinal fluid are associated with Alzheimer’s regardless of whether the reduction is due to defective apoE. The reductions in fatty acids were alarming: 4.5 micromol/L in the Alzheimer’s patients, compared with 28.0 micromol/L in the control group. This is a reduction by more than a factor of 6 in the amount of fatty acid available to repair the myelin sheath!
People with the apoE-4 allele tend to have high serum cholesterol. The question of whether this high cholesterol level might be an attempt on the part of the body to adjust for a poor rate of cholesterol uptake in the brain was addressed by a team of researchers in 1998 [39]. They studied 444 men between 70 and 89 years old at the time, for whom there existed extensive records of cholesterol levels dating back to several decades ago. Most significantly, cholesterol levels fell for the men who developed Alzheimer’s prior to their showing Alzheimer’s symptoms. The authors suggested that their high cholesterol might have been a protective mechanism against Alzheimer’s.
One might wonder why their cholesterol levels fell. There was no mention of statin drugs in the article, but statins would certainly be an effective way to reduce cholesterol levels. The statin industry would like people to believe that high cholesterol is a risk factor for Alzheimer’s, and they are quite thrilled that high cholesterol early in life is correlated with Alzheimer’s much later. But these results suggest quite the opposite: that blood cholesterol levels are kept high intentionally by the body regulatory mechanisms in an attempt to compensate for the defect. A high concentration will lead to an increase in the rate of delivery to the brain, where it is critically needed to keep the myelin sheath healthy and to promote neuron signaling in the synapses.
Using MRI technology, researchers at UCLA were able to measure the degree of breakdown of myelin in specific regions of the brain [6]. They conducted their studies on over 100 people between 55 and 75 years old, for whom they also determined the associated apoE allele (2, 3, or 4). They found a consistent trend in that apoE-2 had the least amount of degradation, and apoE-4 had the most, in the frontal lobe region of the brain. All of the people in the study were thus far healthy with respect to Alzheimer’s. These results show that premature breakdown of myelin sheath (likely due to an insufficient supply of fats and cholesterol to repair it) is associated with apoE-4.
To summarize, I hypothesize that, for the apoE-4 Alzheimer’s patients, defective apoE has led to an impaired ability to transport fats and cholesterol from the blood stream, via the astrocytes, into the cerebrospinal fluid. The associated high blood serum cholesterol is an attempt to partially correct for this defect. For the rest of the Alzheimer’s patients (the ones without the apoE-4 allele but who also have severely depleted fatty acids in their cerebrospinal fluid), we have to look for another reason why their fatty acid supply chain might be broken.
9. Infections and Inflammation
To summarize what I have said so far, Alzheimer’s appears to be a consequence of an inability of neurons to function properly, due to a deficiency in fats and cholesterol. A compounding problem is that the fats over time will become rancid if they cannot be adequately replenished. Rancid fats are vulnerable to attack by microorganisms such as bacteria and viruses. Amyloid-beta is part of the solution because it allows the astrocytes to be much more effective in utilizing glucose anaerobically, which protects the internally synthesized fats and cholesterol from toxic oxygen exposure, while at the same time providing the energy needed both by the astrocyte for the synthesis process and by neighboring neurons to fuel their signal firings.
Besides the astrocytes, the microglia in the brain are also implicated in Alzheimer’s. Microglia promote neuron growth when all is well, but trigger neuron programmed cell death in the presence of toxic substances secreted by bacteria such as polysaccharides [56]. Microglia will defensively secrete cytokines (communication signals that promote an immune response) when exposed to infective agents, and these in turn will lead to inflammation, another well-known feature associated with Alzheimer’s [1]. The microglia are able to control whether neurons should live or die, and they surely base this decision on factors related to how well the neuron functions and whether it is infected. Once enough neurons have been programmed for cell death, the disease will manifest itself as cognitive decline.
10. Evidence that Infection is Associated with Alzheimer’s
There is substantial evidence that Alzheimer’s is related to an increased likelihood of infective agents appearing in the brain. Some researchers believe that infective agents are the principle cause of Alzheimer’s. There are a number of bacteria that reside in the human digestive system and can co-exist with our own cells without any harm. However, H. pylori, one that is quite common, has been recently shown to be responsible for stomach ulcers. It has been suspected that H. Pylori might be implicated in Alzheimer’s, and, indeed, a recent study showed that Alzheimer’s patients had a significantly higher concentration of an antibody against H. Pylori in both their cerebrospinal fluid and their blood than non-Alzheimer’s controls [26]. H. pylori was detected in 88% of the Alzheimer’s patients but only 47% of the controls. In an effort to treat the Alzheimer’s patients, the researchers administered a potent combination of antibiotics, and assessed the degree of mental decline over the next two years [27]. For 85% of the patients, the infection was successfully routed, and for those patients, cognitive improvement was also detected after two years had elapsed. So this was a nice example of the possibility of treating Alzheimer’s through antibiotics.
C. pneumoniae is a very common bacterium, estimated to infect 40-70% of adults. But there’s a big difference between a bacterium being in the blood stream and making its way into the inner sanctum of the brain. A study of post-mortem samples from various regions of the brains of Alzheimer’s patients and non-Alzheimer’s controls revealed a remarkably different statistic: 17 out of 19 Alzheimer’s brains tested positive for the bacterium, whereas only 1 out of 19 brains from the control group tested positive [5].
Many other infective agents, both viruses and bacteria, have been found to be associated with Alzheimer’s, including herpes simplex virus, picornavirus, Borna disease virus, and spirochete [23]. One proposal was that a particularbacteriophage — a virus that infects the bacterium C. pneumoniae — might be responsible for Alzheimer’s [14]. The authors argued that the phages might make their way into the mitochondria of the host cell and subsequently initiate Alzheimer’s.
11. Ketogenic Diet as Treatment for Alzheimer’s
One of the promising new treatment paradigms for Alzheimer’s is to have the patient switch to an extremely high fat, low carb diet, a so-called “ketogenic” diet. The name comes from the fact that the metabolism of dietary fats produces “ketone bodies” as a by-product, which are a very useful resource for metabolism in the brain. It is becoming increasingly clear that defective glucose metabolism in the brain (so-called “type-3 diabetes”) is an early characteristic of Alzheimer’s. Ketone bodies, whether they enter the astrocyte directly or are produced in the astrocyte itself by breaking down fats, can be delivered to adjacent neurons, as shown in the accompanying figure. These neurons can utilize the ketone bodies both as an energy source (replacing and therefore relieving glucose) and as a precursor to GABA, a critical neurotransmitter that is widespread in the brain.
These neurons can utilize the ketone bodies both as an energy source (replacing and therefore relieving glucose) and as a precursor to GABA, a critical neurotransmitter that is widespread in the brain.
Evidence that a ketogenic diet might help Alzheimer’s was first found through research conducted on mice who had been bred to be prone to Alzheimer’s disease [21]. Researchers found that the mice’s cognition improved when they were treated with a high-fat low-carb diet, and also that the amount of amyloid-beta in their brain was reduced. The latter effect would be anticipated based on the premise that amyloid-beta promotes full utilization of glucose anaerobically, as I discussed previously. By having ketone bodies as an additional source of fuel, the dependence on glucose is reduced. But another effect that may be more important than this is the availability of high-quality fats to improve the condition of the myelin sheath.
This idea is supported by other experiments done on human Alzheimer’s patients [11] [42]. A placebo-controlled 2004 study [42] of the effect of dietary fat enrichment on Alzheimer’s is especially informative, because it uncovered a significant difference in effectiveness for the fat-enrichment for subjects who did not have the apoE-4 allele as compared with those who did. The experimental test group were given a supplemental drink containing emulsified medium chain triglycerides, found in high concentration in coconut oil. The subjects without the apoE-4 allele showed a significant improvement in score on a standard test for Alzheimer’s, whereas those with the apoE-4 allele did not. This is a strong indicator that the benefit may have to do with an increase in uptake by the astrocyte of these high-quality fats, something that the subjects with the apoE-4 allele are unable to accomplish due to the defective IDL and LDL transport mechanisms.
12. NADH Treatment: the Crucial Role of Antioxidants
One of the very few promising treatments for Alzheimer’s is the coenzyme, NADH (nicotinamide adenine dinucleotide) [12]. In a placebo-controlled study, Alzheimer’s subjects given NADH for six months exhibited significantly better performances on verbal fluency, visual constructional ability and abstract verbal reasoning than the control subjects given a placebo.
Why would NADH be effective? In the process of converting pyruvate to lactate, lactate dehydrogenase consumes oxygen by oxidizing NADH to NAD+, as illustrated in the accompanying figure. So, if the bioavailability of NADH is increased, it stands to reason that the astrocyte would have an enhanced ability to convert pyruvate to lactate, the critical step in the anaerobic metabolic pathway that is enhanced by amyloid-beta. The process, by absorbing the toxic oxygen, would reduce the damage to the lipids due to oxygen exposure, and would also provide lactate as a source of energy for the neurons.
13. Excessive Oxygen Exposure and Cognitive Decline
It has been observed that some elderly people suffer temporary and sometimes permanent cognitive decline following a lengthy operation. Researchers at the University of South Florida and Vanderbilt University suspected that this might be due to excessive exposure to oxygen [4]. Typically, during an operation, people are often administered high doses of oxygen, even as much as 100% oxygen. The researchers conducted an experiment on young adult mice, which had been engineered to be predisposed towards Alzheimer’s but had not yet suffered cognitive decline. They did however already have amyloid-beta deposits in their brains. The re-engineered mice, as well as a control group that did not have the Alzheimer’s susceptibility gene, were exposed to 100-percent oxygen for a period of three hours, three times over the course of several months, simulating repeated operations. They found that the Alzheimer’s pre-disposed mice suffered significant cognitive decline following the oxygen exposure, by contrast with the control mice.
This is a strong indication that the excessive oxygen exposure during operations is causing oxidative damage in the Alzheimer’s brain. Given the arguments I have presented above, this result makes good sense. The brain, by converting to anaerobic metabolism for generating energy (with help from amyloid-beta) is trying its best to avoid exposing the fatty acids and cholesterol to oxidative damage. But an extremely high concentration of oxygen in the blood makes it very difficult to protect the fats and cholesterol during transport through the blood, and also probably causes an unavoidable increase in oxygen uptake and therefore exposure within the brain itself.
14. Fats are a Healthy Choice!
You would practically have to be as isolated as an Australian Aborigine not to have absorbed the message that dietary fats, particularly saturated fats, are unhealthy. I am extremely confident that this message is false, but it is nearly impossible to turn the opinion tide due to its pervasive presence. Most people don’t question why fats are bad; they assume that researchers must have done their homework, and they trust the result.
To say that the current situation with regard to dietary fats is confusing would be an understatement. We are repeatedly told to keep our total fat intake down to, ideally, 20% of our total calories. This is difficult to achieve, and I believe it is misguided advice. In direct contradiction to this “low-fat” goal, we are encouraged to consume as much as possible of the “good” kinds of fats. Fortunately, the message is finally becoming widely embraced that omega-3 fats are healthy and that trans fats are extremely unhealthy. DHA (docosahexaenoic acid) is an omega-3 fat that is found in large quantities in the healthy brain. In the diet, it is available mainly from cold water fish, but eggs and dairy are also good sources. Trans fats are generated by a high-heat process that hydrolyzes polyunsaturated fats into a more stable configuration, which increases their shelf life but makes them so unnatural they almost can no longer be called a food. Trans fats are extremely damaging both to heart and brain health. A high consumption of trans fats has recently been shown to increase the risk of Alzheimer’s [41]. Trans fats are especially prevalent in highly processed foods — particularly when fats are converted to a powdered form.
We are told to avoid saturated fats, mainly because they have appeared, from empirical evidence, to be more likely to raise LDL levels than unsaturated fats. Yet these fats are less susceptible to oxidation, and this may be why they show up in LDL — because they are of higher quality and therefore should preferentially be delivered to the tissues for functional roles rather than as fuel (i.e., free fatty acids). Coconut oil, a saturated fat, has been shown to benefit Alzheimer’s patients [42]. And high-fat dairy (also highly saturated) has been shown to be beneficial both to fertility among women [10] and, remarkably, to heart disease [37][22].
Despite the widespread belief that fats (particularly saturated fats) are unhealthy, an article that appeared in the American Journal of Clinical Nutrition in 2004 [37] claims that, for a group of post-menopausal women, a high-fat, high-saturated-fat diet affords better protection from coronary artery disease than a low-fat (25% of calories from fats) diet. The subjects in the study were obese women with coronary artery disease. Most of them had high blood pressure, and many had diabetes. They fit the profile for metabolic syndrome that I have previously argued is a direct consequence of a prolonged low-fat high-carb diet. I am gratified to see that my hypothesis that an increase in fat intake would decrease their risk of heart disease has been verified by a carefully controlled study.
Another investigation where fats were shown to afford protection against heart disease has just been completed. It involved a long-term study of a large number of Swedish men [22]. The authors looked at low- vs high-fat dairy, as well as consumption of fruits and vegetables, meats, grains, etc. The only statistically significant result that afforded protection from heart disease was a combination of high-fat dairy and lots of fruits and vegetables. Fruits and vegetables with low-fat dairy afforded no protection.
I suspect one of the critical nutrients the fruits and vegetables provide is antioxidants that help prolong the life of the fats. Other excellent sources of antioxidants include richly colored fruits like berries and tomatoes, coffee, green tea, and dark chocolate, and several spices, most especially cinnamon and turmeric (a major ingredient of curry). These should be consumed in abundance along with fats for optimal results.
Polyunsaturated fats such as corn oil and canola oil are unhealthy for the brain precisely because they are unsaturated. There are two major problems: (1) they have a low melting point, which means that, if they are used for frying they will be converted to trans fats, which are extremely unhealthy, and (2) they are much more susceptible to becoming rancid (oxidized) at room temperature than saturated fats, i.e., they have a shorter shelf life.
Researchers in Germany recently conducted an ingenious experiment designed to determine how the degree of freshness of polyunsaturated fats affects the metabolism of those fats in female lactating rats [43]. They divided female rats into two groups, and the only difference between the test group and the controls was that the test group was given fats that had been left in a relatively warm place for 25 days, which caused considerable oxidative damage, whereas the controls were fed fresh fats instead. The rats’ unusual diet was begun on the day that they gave birth to a litter. The researchers examined the mammary glands and the milk produced by the two groups for apparent differences. They found that the test group’s milk was markedly reduced in the amount of fat it contained, and their mammary glands correspondingly took up less fat from the blood supply. One might surmise that the rats’ metabolic mechanisms were able to detect oxidative damage to the fats, and therefore rejected them, prefering to do without rather than to risk the consequences of feeding their pups oxidized fats. Consequently, the pups of the test group gained significantly less weight than the control group’s pups.
Boxed items like cookies and crackers that contain processed polyunsaturated fats are doctored with antioxidants and even antibiotics to protect them from spoiling. Once they’re consumed, however, they still have to be protected from going rancid. Biochemical laws work the same way whether inside or outside the body. There are plenty of bacteria throughout the body that would be eager to take up house-keeping in rancid fats. The body has devised all kinds of strategies for protecting fats from oxidation (becoming rancid) and from attack by bacteria. But its task is rendered much easier for saturated rather than unsaturated fats, and for fresh rather than stale fats.
If we stop trying to get by on as few fats as possible in the diet, then we don’t have to become so preoccupied with getting the “right” kinds of fats. If the body is supplied with an overabundance of fats, it can pick and choose to find the perfect fat to match each particular need; excess or defective fats can just be used as fuel, where it’s not very important which fat it is, as long as it can be broken down to release energy.
15. Summary and Conclusion
This is an exciting time for Alzheimer’s research, as new and surprising discoveries are coming out at a rapid pace, and evidence is mounting to support the notion that Alzheimer’s is a nutritional deficiency disease. It is an indication of how much progress has been made in recent years to note that 42% of the references in this essay were published in 2008 or 2009. A popular new theory is that Alzheimer’s may grow out of an impaired ability to metabolize glucose in the brain. The term “type-3 diabetes” has been coined to describe this defect, which often appears long before any symptoms of Alzheimer’s [49]. A shift from aerobic towards anaerobic glucose metabolism in the brain seems to be a harbinger of Alzheimer’s later in life, but I argue that the reason for this shift is both to provide a basic ingredient (pyruvate) from which to synthesize fatty acids, while simultaneously protecting them from potentially damaging oxidation. The ApoE-4 allele, which is associated with increased risk to Alzheimer’s, clearly implicates defects in fat and cholesterol transport, and the remarkable 6-fold reduction in the amount of fatty acids present in the cerebrospinal fluid of Alzheimer’s patients [38] speaks loudly the message that fat insufficiency is a key part of the picture. The observation that the myelin is degraded in the frontal lobes of the brains of people possessing the apoE-4 allele further substantiates the theory that the myelin repair mechanism is defective.
Cholesterol obviously plays a vital role in brain function. A whopping 25% of the total cholesterol in the body is found in the brain, and it is present in abundance both in the synapses and in the myelin sheath. The cholesterol in both of these places has been shown to play an absolutely essential role in signal transport and in growth and repair.
Given the strong positive role played by cholesterol, it can only be assumed that statin drugs would increase the risk of developing Alzheimer’s. However, the statin industry has been remarkably successful thus far in hiding this painful fact. They have managed to make much of the observation that high cholesterol much earlier in life is associated with an increased risk to Alzheimer’s thirty years later. Yet they offer not a single study, not even a retrospective study, to substantiate any claim that actively reducing cholesterol through statin therapy would improve the situation for these people. In fact, most damningly, the statin usage evidence that would answer the question was “unavailable” to the researchers who conducted the seminal study.
Beatrice Golomb is an M.D. Ph.D. who heads up the UCSD Statin Study group, a research team who are actively investigating the risk-benefit balance of statin drugs. She is increasingly becoming convinced that statin drugs should not be recommended for the elderly: that in their case the risks clearly outweigh the benefits. She makes a strong case for this position in an on-line article available here [15]. The section on Alzheimer’s is particularly compelling, and it points out the pitfalls in relying on previous studies done by the statin industry, where often those who have memory problems as side-effects of the statin drugs are excluded from the study, so that the results end up inappropriately biased in favor of statins. In summary, she wrote: “It must be emphasized that the randomized trial evidence has, to date, uniformly failed to show cognitive benefits by statins and has supported no effect or frank and significant harm to cognitive function.”
In addition to refusing to take statin therapy, another way in which an individual can improve their odds against Alzheimer’s is to consume plenty of dietary fats. It seems odd to suddenly switch from a “healthy” low-fat diet to an extremely high fat ketogenic diet, once a diagnosis of Alzheimer’s is made. A ketogenic diet consists, ideally, of 88% fat, 10% protein, and 2% carbohydrate [11]. That is to say, it is absurdly high in fat content. It seems much more reasonable to aim for something like 50% fat, 30% protein, and 20% carbohydrate, so as to pro-actively defend against Alzheimer’s.
I highly recommend a recent book written by the pediatric brain surgeon, Larry McCleary, M.D., called The Brain Trust Program [33]. This book gives a wealth of fascinating information about the brain, as well as specific recommendations for ways to improve cognitive function and avert later Alzheimer’s. Most significantly, he recommends a diet that is high in cholesterol and animal fats, including an abundance of fish, seafood, meat, and eggs. He also recommends coconuts, almonds, avocados and cheese, all foods that contain a significant amount of fat, while encouraging the avoidance of “empty carbs.” His knowledge on this subject grew out of his interest in helping his young patients heal more rapidly after brain trauma.
Our nation is currently bracing itself for an onslaught of Alzheimer’s, at a time when baby boomers are approaching retirement, and our health care system is already in a crisis of escalating costs and shrinking funds. We can not afford the high cost of caring for the swelling population of Alzheimer’s patients that our current practices of low-fat diet and ever expanding statin usage are promoting.
Appendix In this appendix, I include the full abstract of two papers that are relevant to the theory presented here. The first is the abstract of reference [19] in [46], which is reference [44] here [see the section on statin drugs above for context]:
Abstract, “Epidemiological and clinical trials evidence about a preventive role for statins in Alzheimer’s disease:”
“This paper reviews epidemiological and clinical trials data about whether statin use reduces the risk of Alzheimer’s disease (AD). The available information has come in three waves. The initial, mostly cross-sectional observational reports suggested that statins might prevent dementia. Next, two large clinical trials with cognitive add-on studies showed no benefit and neither did the third wave, again with observational studies. The latter were mostly longitudinal, and were critical of the first studies for not adequately addressing confounding by indication (i.e. that patients with dementia would be denied statins). Most recently, new data from the Canadian Study of Health and Aging have produced a mixed result. While methodological considerations are clearly important in understanding why the reports are so variable, there might also be merit in differentiating between statins, based on their presumed – and variable – mechanisms of action in dementia prevention, before concluding that the initial reports are entirely artefactual. Still, the first reports appear to have overestimated the extent of protection, so that unless there are important effects achievable with specific statins, a more than a modest role for statins in preventing AD seems unlikely.” The second abstract is taken from reference [28], on the “alternative hypothesis” that amyloid-beta is protective rather than detrimental to Alzheimer’s, i.e., that it is a “protective response to neuronal insult:”
Abstract, “Amyloid-beta in Alzheimer disease: the null versus the alternate hypotheses:”
“For nearly 20 years, the primary focus for researchers studying Alzheimer disease has been centered on amyloid-beta, such that the amyloid cascade hypothesis has become the “null hypothesis.” Indeed, amyloid-beta is, by the current definition of the disease, an obligate player in pathophysiology, is toxic to neurons in vitro, and, perhaps most compelling, is increased by all of the human genetic influences on the disease. Therefore, targeting amyloid-beta is the focus of considerable basic and therapeutic interest. However, an increasingly vocal group of investigators are arriving at an “alternate hypothesis” stating that amyloid-beta, while certainly involved in the disease, is not an initiating event but rather is secondary to other pathogenic events. Furthermore and perhaps most contrary to current thinking, the alternate hypothesis proposes that the role of amyloid-beta is not as a harbinger of death but rather a protective response to neuronal insult. To determine which hypothesis relates best to Alzheimer disease requires a broader view of disease pathogenesis and is discussed herein.”
Contact: seneff@csail.mit.edu
References
[1] H. Akiyama, S. Barger, S. Barnum, B. Bradt, J.Bauer, G.M. Cole, N.R. Cooper, P. Eikelenboom, M. Emmerling, B.L. Fiebich, C.E. Finch, S. Frautschy, W.S. Griffin, H. Hampel, M. Hull, G. Landreth, L. Lue, R. Mrak, I.R. Mackenzie, P.L. McGeer, M.K. O’Banion, J. Pachter, G. Pasinetti, C. Plata-Salaman, J. Rogers, R.Rydel, Y. Shen, W. Streit, R. Strohmeyer, I. Tooyoma, F.L. Van Muiswinkel, R. Veerhuis, D. Walker, S. Webster, B. Wegrzyniak, G. Wenk, and T. Wyss-Coray, “Inflammation and Alzheimer’s disease.” Neurobiol Aging (2000) May-Jun;21(3):383-421,
[2] Alzheimer’s Association, “Alzheimer’s Disease Facts and Figures,” Alzheimer’s and Dementia (2009) Vol. 5, Issue 3.
[3] K.J. Anstey, D.M. Lipnicki and L.F. Low, “Cholesterol as a risk factor for dementia and cognitive decline: a systematic review of prospective studies with meta-analysis.” Am J Geriatr Psychiatry (2008) May, Vol. 16, No. 5, pp. 343-54.
[4] G. Arendash, A. Cox, T. Mori, J. Cracchiolo, K. Hensley, J. Roberts 2nd, “Oxygen treatment triggers cognitive impairment in Alzheimer’s transgenic mice,” Neuroreport. (2009) Jun 18.
[5] B.J. Balin, C.S. Little, C.J. Hammond, D.M. Appelt, J.A. Whittum-Hudson, H.C. Gerard, A.P. Hudson, “Chlamydophila pneumoniae and the etiology of late-onset Alzheimer’s disease.” J. Alz. Dis. (2008) Vol. 13, pp. 371-380.
[6] G. Bartzokis, MD; P.H. Lu, Psy, D.H. Geschwind, MD, N.Edwards, MA, J. Mintz, PhD, and J.L. Cummings, MD, “Apolipoprotein E Genotype and Age-Related Myelin Breakdown in Healthy Individuals: Implications for Cognitive Decline and Dementia,” Arch Gen Psychiatry (2006) Vol. 63, pp. 63-72.
[7] N. Bernoud, L. Fenart, C. Bénistant, J. F. Pageaux, M. P. Dehouck, P. Molière, M. Lagarde, R. Cecchelli,d, and J. Lecerf, “Astrocytes are mainly responsible for the polyunsaturated fatty acid enrichment in blood-brain barrier endothelial cells in vitro” Journal of Lipid Research (1998) Sept., Vol. 39, pp. 1816-1824.
[8] M. S. Brown and J. L. Goldstein, “A Receptor-Mediated Pathway for Cholesterol Homeostasis,” Nobel Lecture, December 9, 1985.
[9] N. Cartier, C. Sevin, A. Benraiss, P. DeDeyn, D. Bonnin, M-T Vanier, M. Philippe, V. Gieselmann and P. Aubourg, “AAV5-Mediated Delivery of Human Aryl Sulfatase A (hARSA) Prevents Sufatide Storage and Neuropathological Phenotype in Metachromatic Leukodystrophy (MLD) Mice,” Molecular Therapy (2005) 11, S166-S167; doi: 10.1016/j.ymthe.2005.06.431
[10] J. Chavarro, W.C. Willett, and P.J. Skerrett, The Fertility Diet, (2008) McGraw Hill.
[11] L.C. Costantini, L.J. Barr, J.L. Vogel and S.T. Henderson, “Hypometabolism as a therapeutic target in Alzheimer’s disease” BMC Neurosci (2008) Vol. 9, Suppl. 2, S16. doi: 10.1186/1471-2202-9-S2-S16.
[12] V. Demarin, S.S. Podobnik, D. Storga-Tomic and G. Kay, “Treatment of Alzheimer’s disease with stabilized oral nicotinamide adenine dinucleotide: A randomized, double-blind study” Drugs Exp Clin Res. (2004) Vol. 30, No. 1, pp. 27-33.
[13] R.B. DeMattos, R.P. Brendza, J.E. Heuser, M.Kierson, J.R. Cirrito, J. Fryer, P.M. Sullivan, A.M. Fagan, X. Han and D.M. Holtzman, “Purification and characterization of astrocyte-secreted apolipoprotein E and J-containing lipoproteins from wild-type and human apoE transgenic mice,” Neurochem Int. (2001) Nov-Dec;39(5-6):415-25. doi:10.1016/S0197-0186(01)00049-3.
[14] M. Dezfulian, M.A. ShokrgozarA, S. Sardari, K. Parivar and G. Javadi, “Can phages cause Alzheimer’s disease?” Med Hypotheses (2008) Nov;71(5):651-6.
[15] B.A. Golomb, M.D., Ph.D., “Statin Adverse Effects: Implications for the Elderly,” Geriatric Times (2004) May/June, Vol. V, Issue 3
[16] W.R. Grant, Ph.D., “Does Vitamin D Reduce the Risk of Dementia?” Journal of Alzheimer’s Disease (2009) May, Vol. 17, No. 1., pp. 151-9.
[17] Dr. Duane Graveline, Lipitor: Thief of Memory, Statin Drugs and the Misguided War on Cholesterol, (2004) http://www.buybooksontheweb.com.
[18] X. Han, “Potential mechanisms contributing to sulfatide depletion at the earliest clinically recognizable stage of Alzheimer’s disease: a tale of shotgun lipidomics,” J Neurochem (2007) November, Vol. 103, Suppl. 1. pp. 171-179. doi: 10.1111/j.1471-4159.2007.04708.x.
[19] X. Han, H. Cheng, J.D. Fryer, A.M. Fagan and D.M. Holtzman, “Novel Role for Apolipoprotein E in the Central Nervous System: Modulation of Sulfatide Content” Journal of Biological Chemistry, March 7, 2003, Vol. 278, pp. 8043-8051, DOI 10.1074/jbc.M212340200.
[20] K. Heininger, “A unifying hypothesis of Alzheimer’s disease. IV. Causation and sequence of events,” Rev Neurosci. (2000) Vol. 11, Spec No, pp.213-328.
[21] S.T. Henderson, “Ketone Bodies as a Therapeutic for Alzheimer’s Disease,” NeuroTherapeutics,, (2008) Jul;5(3):470-80, doi:10.1016/j.nurt.2008.05.004
[22] S. Holmberg, A. Thelin and E.-L. StiernstrNvm, “Food Choices and Coronary Heart Disease: A Population Based Cohort Study of Rural Swedish Men with 12 Years of Follow-up,” Int. J. Environ. Res. Public Health (2009) Vol. 6, pp. 2626-2638;
[23] K. Honjo, R. van Reekum, and N.P. Verhoeff, “Alzheimer’s disease and infection: do infectious agents contribute to progression of Alzheimer’s disease?” Alzheimers Dement. (2009) Jul;5(4):348-60.
[24] S.M. Innis and R.A. Dyer, “Brain astrocyte synthesis of docosahexaenoic acid from n-3 fatty acids is limited at the elongation of docosapentaenoic acid,” (2002) Sept. Journal of Lipid Research, Vol. 43, pp. 1529-1536.
[25] L. Jeng, A.V. Yamshchikov, S.E. Judd, H.M. Blumberg, G.S. Martin, T.R. Ziegler and V. Tangpricha, “Alterations in Vitamin D Status and Anti-microbial Peptide Levels in Patients in the Intensive Care Unit with Sepsis,” Journal of translational Medicine,” (2009) Vol. 7, No. 28.
[26] J. Kountouras, M. Boziki, E. Gavalas, C. Zavos, G. Deretzi, N. Grigoriadis, M. Tsolaki, D. Chatzopoulos, P. Katsinelos, D. Tzilves, A. Zabouri, I. Michailidou, “Increased cerebrospinal fluid Helicobacter pylori antibody in Alzheimer’s disease,” Int J Neurosci. (2009) 119(6):765-77.
[27] J. Kountouras, M. Boziki, E. Gavalas, C. Zavos, N. Grigoriadis, G. Deretzi, D. Tzilves, P. Katsinelos, M. Tsolaki, D. Chatzopoulos, and I. Venizelos, “Eradication of Helicobacter pylori may be beneficial in the management of Alzheimer’s disease,” J Neurol. (2009) May;256(5):758-67. Epub 2009 Feb 25.
[28] H.G. Lee, X. Zhu, R.J. Castellani, A. Nunomura, G. Perry, and M.A. Smith, “Amyloid-beta in Alzheimer disease: the null versus the alternate hypotheses,” J Pharmacol Exp Ther. (2007) June, Vol. 321 No. 3, pp. 823-9. doi:10.3390/ijerph6102626.
[29] J. Marcus, S. Honigbaum, S. Shroff, K. Honke, J. Rosenbluth and J.L. Dupree, “Sulfatide is essential for the maintenance of CNS myelin and axon structure,” Glia (2006), Vol. 53, pp. 372-381.
[30] R.T. Matthews, L. Yang, S. Browne, M. Baik and M.F. Beal, “Coenzyme Q10 administration increases brain mitochondrial concentrations and exerts neuroprotective effects,” Proc Natl Acad Sci U S A. (1998) Jul 21, Vol. 95, No. 15, pp.8892-7.
[31] D. Lutjohann and K. von Bergmann, “24S-hydroxycholesterol: a marker of brain cholesterol metabolism”Pharmacopsychiatry (2003) January 10, Vol. 36 Suppl 2, pp. S102-6, DOI: 10.1055/s-2003-43053.
[32] J. C. McCann and B.N. Ames, “Is there convincing biological or behavioral evidence linking vitamin D deficiency to brain dysfunction?”, (2008) FASEB J. Vol. 22, pp. 982-1001. doi: 10.1096/fj.07-9326rev.
[33] Larry McCleary, M.D., The Brain Trust Program (2007) September, The Penguin Group, New York, New York.
[34] B. McGuinness et al., “Statins for the prevention of dementia,” Cochrane Database of Systematic Reviews,(2009) No. 2.
[35] M.M. Mielke, P.P. Zandi, M. Sjogren, et al. “High total cholesterol levels in late life associated with a reduced risk of dementia,” Neurology (2005) Vol. 64, pp. 1689-1695.
[36] S.A. Moore, “Polyunsaturated Fatty Acid Synthesis and Release by Brain-Derived Cells in Vitro,” Journal of Molecular Neuroscience (2001), Vol. 16, pp. 195ff.
[37] D. Mozaffarian, E.B. Rimm, D.M. Herrington, “Dietary fats, carbohydrate, and progression of coronary atherosclerosis in postmenopausal women,” Am J Clin Nutr (2004) Vol. 80, pp. 1175-84.
[38] M. Mulder, R. Ravid, D.F. Swaab, E.R. de Kloet, E.D. Haasdijk, J. Julk, J.J. van der Boom and L.M. Havekes, “Reduced levels of cholesterol, phospholipids, and fatty acids in cerebrospinal fluid of Alzheimer disease patients are not related to apolipoprotein E4,” Alzheimer Dis Assoc Disord. (1998) Sep, Vol. 12, No. 3, pp. 198-203.
[39] I.L. Notkola, R. Sulkava, J. Pekkanen, T. Erkinjuntti, C. Ehnholm, P. Kivinen, J. Tuomilehto, and A. Nissinen, “Serum total cholesterol, apolipoprotein E epsilon 4 allele, and Alzheimer’s disease,” Neuroepidemiology (1998) Vol. 17, No. 1, pp. 14-20.
[40] F.W. Pfrieger, “Outsourcing in the brain: Do neurons depend on cholesterol delivery by astrocytes?”, BioEssays(2003) Vol. 25 Issue 1, pp.72-78.
[41] A. Phivilay, C. Julien, C. Tremblay, L. Berthiaume, P. Julien, Y. Giguère and F. Calon, “High dietary consumption of trans fatty acids decreases brain docosahexaenoic acid but does not alter amyloid-beta and tau pathologies in the 3xTg-AD model of Alzheimer’s disease.” Neuroscience (2009) Mar 3, Vol. 159, No. 1, pp. 296-307. Epub 2008 Dec 14.
[42] M.A. Reger, S. T. Henderson, C. Hale, B. Cholerton, L.D. Baker, G.S. Watson, K. Hyde, D. Chapman and S. Craft, “Effects of Beta-hydroxybutyrate on cognition in memory-impaired adults,” Neurobiology of Aging (2004) Vol. 25, No. 3, March, pp. 311-314,
[43] R. Ringseis, C. Dathe, A. Muschick, C. Brandsch and K. Eder, “Nutrient Physiology, Metabolism, and Nutrient-Nutrient Interactions Oxidized Fat Reduces Milk Triacylglycerol Concentrations by Inhibiting Gene Expression of Lipoprotein Lipase and Fatty Acid Transporters in the Mammary Gland of Rats,” American Society for Nutrition J. Nutr. (2007) Sept., Vol. 137, pp. 2056-2061.
[44] K. Rockwood, “Epidemiological and clinical trials evidence about a preventive role for statins in Alzheimer’s disease.” Acta Neurol Scand Suppl. (2006) Vol. 185, pp. 71-7.
[45] G. Saher, B. Brugger, C. Lappe-Siefke, W. Mobius, R. Tozawa, M.C. Wehr, F. Wieland, S. Ishibashi, and K.A. Nave, “High cholesterol level is essential for myelin membrane growth.” Nat Neurosci (2005) Apr, Vol. 8, No. 4, pp. 468-75. Epub 2005 Mar 27.
[46] A. Solomon, M. Kivipelto, B. Wolozin, J. Zhou, and R.A. Whitmer, “Midlife Serum Cholesterol and Increased Risk of Alzheimer’s and Vascular Dementia Three Decades Later,” Dementia and Geriatric Cognitive Disorders (2009) Vol. 28, pp. 75-80, DOI: 10:1159/000231980.
[47] M. Simons, MD, P. Keller, PhD, J. Dichgans, MD and J.B. Schulz, MD, “Cholesterol and Alzheimer’s disease: Is there a link?” Neurology (2001) Vol. 57, pp. 1089-1093.
[48] L.L. Smith, “Another cholesterol hypothesis: cholesterol as antioxidant,” Free Radic Biol Med. (1991) Vol. 11, No. 1, pp. 47-61.
[49] E. Steen, B.M. Terry, E.J. Rivera, J.L. Cannon, T.R. Neely, R. Tavares, X.J. Xu, J.R. Wands, and S.M. de la Monte “Impaired insulin and insulin-like growth factor expression and signaling mechanisms in Alzheimer’s disease – is this type 3 diabetes?” Journal of Alzheiner’s Disease (2005) Vol. 7, Number 1, pp. 63-80.
[50] J. Tong, P.P. Borbat, J.H. Freed and Y-K Shin, “A scissors mechanism for stimulation of SNARE-mediated lipid mixing by cholesterol,” PNAS (2009) March 31 Vol. 106, No. 13, pp. 5141-5146.
[51] M-C Vohl, T. A.-M. Neville, R. Kumarathasan, S. Braschi, and D.L. Sparks, “A Novel Lecithin-Cholesterol Acyltransferase Antioxidant Activity Prevents the Formation of Oxidized Lipids during Lipoprotein Oxidation,”Biochemistry (1999) Vol. 38 No. 19, pp. 5976-5981. DOI: 10.1021/bi982258w.
[52] M. Waldman, MD,, 9th International Conference on Alzheimer’s and Parkinson’s Diseases (2009) Abstract 90, Presented March 12-13.
[53] R. West, M.A., M. Schnaider Beeri, Ph.D., J. Schmeidler, Ph.D., C. M. Hannigan, B.S., G. Angelo, M.S., H.T. Grossman, M.D., C. Rosendorff, M.D., Ph.D., and J.M. Silverman, Ph.D., “Better memory functioning associated with higher total and LDL cholesterol levels in very elderly subjects without the APOE4 allele,” Am J Geriatr Psychiatry(2008) September; Vol. 16, No. 9, pp. 781-785. doi: 10.1097/JGP.0b013e3181812790.
[54] A.W.E. Weverling-Rijnsburger, G.J. Blauw, A.M. Lagaay, D.L. Knook, A.E. Meinders, and R.G.J. Westendorp, “Total cholesterol and risk of mortality in the oldest old,” The Lancet, (1997) Vol. 350, No. 9085, pp. 1119-1123,
[55] R.F. Wilson, J.F. Barletta and J.G. Tyburski, “Hypocholesterolemia in Sepsis and Critically Ill or Injured Patients”Critical Care (2003), Vol. 7, pp. 413-414.
[56] S.-C. Zhang and S. Fedoroff, “Neuron-microglia Interactions in Vitro,” Acta Neuropathol (1996) Vol. 91, pp. 385-395.
Featured Video

Seyed Marandi: Trump lost the Iran war – Must sell it as victory
or go to
Aletho News Archives – Video-Images
From the Archives
UK Researchers: Tax Food to Reduce Climate Change

I doubt these professors have anything to fear from a food tax
By Eric Worrall | Watts Up With That? | November 19, 2016
A group of researchers in Oxford University, England have suggested that imposing a massive tax on carbon intensive foods – specifically protein rich foods like meat and dairy – could help combat climate change. […]
This proposal, from a group of people who have probably never missed a meal in their lives, is totally obscene. High income countries often have a lot of poor people who would be hard hit by increases in the price of food.
Needlessly exacerbating the risk poor people don’t get enough to eat, especially children and pregnant mothers, who are especially vulnerable to adverse health impacts from lack of protein in their diet – if this ghastly proposal is ever implemented, future generations will look upon it as a crime against humanity. – Read full article
Blog Roll
 Aletho News
Aletho News- Seyed M. Marandi: Trump Lost the Iran War – Must Sell It as a Victory
- Iran, Saudi FMs hold phone talks as Persian Gulf states rethink US ties
- The Illusions of Western Virtue: Ursula von der Leyen and Europe’s Moral Bankruptcy
- AIPAC-backed candidates lose New York primaries as voters reject pro-genocide lobby
- The West’s Post-Soviet ‘Democracy’ Playbook
- UK suppressed intel on Sudan genocide to protect UAE ties: Report
- Starmer’s exit exposes dirty secret: UK can’t afford Ukraine War
- Putin Warns the West: Russia Is Ready
- BEN-GVIR: “ALL OF LEBANON MUST BURN” — w/ Mouin Rabbani
- There Are No Budget Constraints In New York City: “Coastal Resiliency” Edition
- If Americans Knew
- Israel’s Attacks on Gaza’s Children (Photos)
- ‘His only crime is that he is a Palestinian doctor’
- ‘Killed pursuing her dream’: Gaza girl on her way to school dies in Israeli drone strike
- Unbelievable pressure on Gaza from Israel, “Board of Peace” – Daily Update
- UN: Israel Continues to Commit Genocide and Other Atrocity Crimes by Deliberately Targeting Palestinian Children
- Bari Weiss, Free-Speech Fraud & Zionism Promoter, Would Rather Deport Than Debate
- ‘Doctor of the Poor’: Israeli Occupation Arrests Prominent Palestinian Physician
- Search for Your Church (and see if it has been targeted by the Israeli gov’t)
- Mark Levin Flying to Israel as Netanyahu Reportedly Seeks to ‘Leverage’ Levin to Trash Trump’s Iran Deal
- Watch: Zionist Brags about Israel’s Power to Get the World to Do What Israel Wants
- No Tricks Zone
- 3 New Studies Find Increasing Trends In Solar Radiation Since The 1980s – Easily Explaining Warming
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
