Another Israeli Spy Story: When Will It End?
By Philip Giraldi | Strategic Culture Foundation | July 29, 2021
It is perhaps not necessary to point out how the mainstream media in the United States as well as in Europe and Oceania persist in ignoring or otherwise covering up stories that make the Israelis look bad. Recent accounts of the slaughter of children and mostly civilians in Gaza by Israeli planes, missiles and artillery consistently try to depict the conflict as warfare between two comparable opponents, ignoring the enormous disparity in the military force available to the two sides. Israel has a modern army, air force and navy while Hamas has nothing but some small arms as well as improvised rockets and incendiary balloons.
The reluctance to criticize Israeli behavior is largely attributable to the power of the Zionist lobbies in the respective countries but it is also at least in part due to the complicity of Western governments in conniving at the Jewish state’s actions in its own region. The persistence in Israeli demands for war against Iran, preferable fought by the United States, was clear again this past week when the new government in Jerusalem declared that it would be increasing its military budget in anticipation of war with the Islamic Republic. Perhaps not surprisingly, the U.S. Congress also has several bills pending that would increase military assistance to Israel by a factor of three.
Aside from their overwhelming affection for the Jewish state, politicians and talking heads in Washington have always sought to have an enemy to explain why the foreign and national security policies have been such failures. Russia was so designated during the long years of the Cold War and more recently both the White House and Congress have begun to warn that it is China that is seeking to confront democratic norms and “export its authoritarian model.”
Given all of that, there must have been shock in a number of newsrooms when it turned out that the guilty party behind an explosive spy story that was revealed recently appears to be none other than America’s “closest ally and best friend.” It seems that a private Israeli surveillance plus security firm consisting of former cyberwarfare military and intelligence officers and having close ties to the Benjamin Netanyahu government has been selling advanced spyware to at least 45 governments. The sales are in theory restricted for use only in terrorism and criminal cases, but somehow the resource has instead been routinely used against journalists, political activists, business executives, and politicians. Saudi Arabia, for example, used the spyware to track dissident journal Jamal Khashoggi, who was murdered by Saudi agents in Istanbul in 2018.
And even though the software has been regularly used against U.S. government officials and journalists, it appears that the Biden Administration has been aware of its capabilities and has done nothing to stop it. In its own defense, the Israeli company NSO that developed the spyware has claimed, implausibly, that it can no longer be used to hack U.S. phones. That assertion was debunked by former NSA whistleblower Edward Snowden, who tweeted “NSO’s claim that it is ‘technologically impossible’ to spy on American phone numbers is a bald-faced lie: a exploit that works against Macron’s iPhone will work the same on Biden’s iPhone. Any code written to prohibit targeting a country can also be unwritten. It’s a fig leaf.”
The surprise revelation of the Israeli activity came not from a government counter-intelligence agency, but rather from a group of 17 international media organizations that formed a consortium to investigate a data leak relating to hacked telephones. The group included major news outlets that had apparently been targeted using the Pegasus hacking spyware developed by the NSO Group, which was primarily designed to penetrate the security features of smartphones. One former cybersecurity engineer from the U.S. intelligence community described Pegasus as an “eloquently nasty” tool that could be used to “spy on almost the entire world population.” The spyware “can be installed remotely on a targeted person’s smartphone without requiring them to take any action such as clicking on a link or answering a call. Once installed, it allows clients to take complete control of the device, including accessing messages from encrypted messaging apps like WhatsApp and Signal, and turning on the microphone and camera.” It can also reveal the phone’s location.
The software was designed with a backdoor which allowed NSO to monitor the surveillances and it is presumed that the information was also shared with Israeli intelligence. By one estimate 50,000 smartphones were accessed worldwide, including 10 prime ministers, three presidents including Emmanuel Macron of France, a king, foreign ministers and assorted journalists and government officials both in the U.S. and elsewhere.
A more cautious estimate from the Washington Post, which participated in the investigation, states only that “1,000 people spread across 50 different countries were identified as having numbers on the list, among them are ‘several Arab royal family members, at least 65 business executives, 85 human rights activists, 189 journalists, and more than 600 politicians and government officials.’ This includes Robert Malley, the Biden administration’s lead Iran negotiator, and journalists for CNN, the Associated Press, the Wall Street Journal, and the New York Times.” Other news agencies that were hacked by Pegasus include Agence France-Presse, Al Jazeera, France 24, Radio Free Europe, Mediapart, El País, the Associated Press, Le Monde, Bloomberg, the Economist, Reuters and Voice of America.
Some are inevitably wondering why the Biden White House has been silent about NSO. It has not identified the Israeli firm as a threat to national security and made demands to the Israeli government that it intercede with NSO and shut down the use of Pegasus until some international regulation of the use of hacking software can be developed. Part of the explanation for the reluctance might be that Biden’s senior adviser Anita Dunn’s consulting firm SKDKickerbocker was hired by NSO in 2019 to provide “public relations” advice to improve the company’s image.
The reluctance, of course, also derives from the fact that Israel is involved, but those with longer memories of the Jewish state’s record in stealing American secrets should not be surprised by this latest venture. Israeli-recruited U.S. Navy analyst Jonathan Pollard was, for example, the most damaging spy in U.S. history. And Israel has, in fact, a long history of stealing U.S. technology and military secrets to include sharing them with countries that Washington has regarded as enemies, including China and Russia.
Israel always features prominently in the annual FBI report called Foreign Economic Collection and Industrial Espionage. The 2005 report states: “Israel has an active program to gather proprietary information within the United States, these collection activities are primarily directed at obtaining information on military systems and advanced computing applications that can be used in Israel’s sizeable armaments industry.” It adds that: “Israel recruits spies, uses electronic methods, and carries out computer intrusion to gain the information.” A 1996 Defense Investigative Service report noted that: “Israel has great success stealing technology by exploiting the numerous co-production projects that it has with the Pentagon.” It says: “Placing Israeli nationals in key industries is a technique utilized with great success.” A General Accounting Office (GAO) examination of espionage directed against American defense and security industries described how: “Israeli citizens residing in the U.S. had stolen sensitive technology to manufacture artillery gun tubes, obtain classified plans for reconnaissance systems, and pass sensitive aerospace designs to unauthorized users.” The GAO concluded that: “Israel conducts,” and this is a quote, “conducts the most aggressive espionage operation against the United States of any U.S. ally.” More recently, FBI counterintelligence officer John Cole has reported how many cases of Israeli espionage are dropped under orders from the Justice Department. He has provided a conservative estimate of 125 viable investigations into Israeli espionage — involving both American citizens and Israelis — that were stopped due to political pressure.
So Israel gets yet another pass on its spying against the United States. Indeed, the Biden Administration has yet to definitively comment on the latest impropriety. One wonders when the penny will drop and the American people will rise up and say “enough is enough.”
How a Psychic Healer Blog Convinced the Government to Fund “Long Covid” Research
By Phillip W. Magness | AIER | July 27, 2021
The National Institutes for Health (NIH) is exceptionally keen on the study of “Long Covid.” The federal agency recently allocated over $1 billion in funding for this purpose, and NIH Director Francis Collins has made the claimed ailment a recurring subject of his press commentary over the last year. The Department of Health and Human Services similarly signaled that it intends to classify “Long Covid” as a recognized disability for government funding and classification purposes.
So what is Long Covid, and why is it drawing so much attention and funding out of the federal government? As with any respiratory illness, Covid-19 does appear to have long-term sufferers who do not follow the normal recovery pattern and continue to demonstrate symptoms for weeks or months after an infection. At the same time however, the push to make “Long Covid” a distinctive medical classification unto itself appears to be a political phenomenon, wrapped up in clear signs of pseudoscience and linked back to a fringe “alternative wellness” blog that originally coined the term in March 2020.
A recent study published in the Lancet-owned journal EClinicalMedicine purported to document over 200 symptoms of Long Covid, ranging from fairly common Covid-19 ailments such as fatigue, cough, or long-term loss of smell to an eclectic assortment of problems such as hallucination, brain fog, tearfulness, insomnia, and mood anxiety. Media reports breathlessly repeated these findings to press the urgency of funding for Long Covid research, while also hyping the syndrome as a further justification for alarmism in justifying lockdowns and similar measures. After all, if Long Covid afflicts a sizable subset of Covid patients – as some claim – and can strike young people who are at a much lower mortality risk from the virus itself, then perhaps more restrictive measures are warranted on the general population – or so the argument goes.
Many lockdown advocates have seized onto the Long Covid narrative, incorporating it into their defenses of the draconian non-pharmaceutical interventions they have advocated over the last year and a half. The CovidFAQ website – a UK-based project set up by “neoliberal” activist Sam Bowman and British MP Neil O’Brien – invokes the threat of Long Covid in its attacks the Great Barrington Declaration (GBD), arguing that the hypothesized syndrome undermines evidence that the virus is substantially less-severe among younger demographics. Several pro-lockdown scientists and epidemiologists issued coordinated statements attacking the GBD in October 2020 for “ignor[ing] the emerging burdens of long COVID.” These statements are usually offered as declarative assessments, treating Long Covid as an established medical fact.
With billion-dollar budgets and the prospect of additional sweeping policy measures at stake, it only makes sense to ask if the science behind Long Covid is sound. There is no doubt that some Covid-19 victims have symptoms that linger for weeks or months beyond the typical recovery, although that is true of many diseases. Whether it has 200 plus symptoms is another story – and a closer look reveals an alarming amount of outright quackery is currently shaping the scientific and media discourse around Long Covid.
The problem arises from the amorphous definition of the phrase “Long Covid” itself. Far from a careful clinical diagnosis, Long Covid has become a catch-all term for any extended medical ailment, real or imagined, attributed to the effects of the Covid-19 virus. An alarming amount of alleged data about the phenomenon traces back to a single source called the “Body Politic Wellness Collective” – an alternative medicine blog with dubious scientific credentials. To quote one recent study of the term’s origins, “the emergence and recognition of Long COVID as a potentially major public health problem is largely due to advocacy groups such as the Body Politic COVID-19 Support Group, and Patient Led Research For COVID-19” – the latter an affiliated survey administrator that, according to its own website, was “born out of the Body Politic Slack support group.”
The same Body Politic group frequently appears in an already large and growing literature on “Long Covid” in other scientific journals. In September 2020, NIH Director Collins devoted his personal column on the agency’s website to touting the group. He later credited their work when launching the aforementioned $1 billion research initiative. In July 2021, Body Politic reappeared at the center of the aforementioned EClinicalMedicine study along with a spinoff organization called the Patient-Led Research Collaborative. The two groups administered the survey behind the claim that Long Covid carries over 200 symptoms.
Before we get into the survey itself, it’s useful to take a closer look at the Body Politic group. TheWall Street Journal recently ran a lengthy expose of the organization by Jeremy Devine, an Ontario-based psychiatrist. Devine found that the group’s initiatives sprang to life at the outset of the pandemic in March 2020. They first coined the Long Covid moniker around this time, promoting it in a flurry of media appearances. In early April, the New York Times ran an op-Ed by Body Politic’s co-founder calling attention to the syndrome and recounting her own experience as a “long hauler” (which, at the time, consisted of experiencing symptoms for about three weeks after testing positive).
As Devine documented in the WSJ, the Body Politic group’s approach to scientific survey design appeared highly unorthodox. It frequently relied on self-reported descriptions of Long Covid symptoms, instead of independent medical verification. It also had a habit of diagnosing people with Long Covid even after they tested negative for Covid-19 itself. A March 2021 report by Adam Gaffney for StatNews called attention to similar problems with Body Politic’s research design. “[A]t least some people who identify themselves as having long Covid appear never to have been infected with the SARS-CoV-2 virus,” Gaffney noted. They were nonetheless touted by the media as case studies in the alleged syndrome.
A closer look at the Body Politic group itself raises several red flags about their scientific qualifications. The group’s executive board boasts few, if any, actual medical practitioners or scientific experts. Instead we find an eclectic assortment of political activists, musicians, poets, and journalists, many of whom share common interests in “alternative medicine.” Body Politic’s Treasurer and principle support group organizer describes herself as a “practicing Spiritual Medium” who specializes in detecting “invisible illness.” The website’s Vice President is a “social & racial justice activist,” and its Secretary is an “aspiring sex coach.” Other affiliates include a self-described “socialist poet,” multiple “social justice activists,” and people who describe their careers as operating at the intersection between art and natural wellness. The group’s website and social media accounts frequently invoke political terminology from the critical theory literature. They describe themselves as “a queer feminist wellness collective and a space for inclusivity, accessibility, and crucial discussions about the very real connection between wellness, politics, and personal identity.” Their values statement espouses “patient-led” research to “democratize” medicine – descriptions that appear to forgo traditional scientific methods of testing and verification in favor of placing heavier reliance on patient testimonials and personal experience.
While the group’s activism alone does not disqualify their commentary, the unconventional qualifications of its leadership should raise suspicion about their claimed expertise on Long Covid. When NIH Director Collins personally promotes Body Politic’s work, he is creating a false sense of scientific credibility around their work. Few who read Collins’s statements are aware that the group he praises as “citizen scientists” might be better characterized as an odd assortment of psychic healers, magic crystal gurus, and alternative medicine activists. As a leading public health official, Collins’s many endorsements of this quackery border on irresponsible.
Turning to Body Politic’s survey projects, we quickly find that skepticism of their credibility is warranted. The group’s survey design specifically eschews requiring a positive Covid-19 test or antibody test to confirm that their respondents actually had the disease. “[W]e do not believe people’s experiences with COVID-19 symptoms should be discounted because they did not receive a positive test result,” states one justification for this unconventional data collection procedure. To qualify as a sufferer of Long Covid, it seems, a person needs only to claim that he or she suffers from Long Covid. Lived experience of the disease trumps any requirement of scientific verification.
The prevalence of unverified and untested Covid claimants being classified nonetheless as Long Covid sufferers is stunning. In the WSJ, Devine reports the numbers from the group’s first survey, administered through their website in 2020: “Nearly half (47.8%)” of Body Politic’s survey respondents “never had testing and 27.5% tested negative for Covid-19. Body Politic publicized the results of a larger, second survey in December 2020. Of the 3,762 respondents, a mere 600, or 15.9%, had tested positive for the virus at any time.” As Gaffney notes in StatNews, this practice raises the distinct possibility that survey respondents are misattributing other chronic symptoms to the virus.
Their new study in the Lancet’s journal EClinical Medicine does not offer much hope that Body Politic has improved its survey design. Its authors state that “We analyzed responses from 3762 participants with confirmed (diagnostic/antibody positive; 1020) or suspected (diagnostic/antibody negative or untested; 2742) COVID-19, from 56 countries.” Unconfirmed Covid patients with self-reported Long Covid symptoms outnumber confirmed Covid patients by almost 2.7 to 1. To their credit, the group discloses the lack of PCR or antibody testing confirmation among the majority of their respondents. The extremely high rates of unconfirmed cases, however, are more than sufficient to cast doubt upon their claims to have identified over 200 separate Long Covid symptoms.
The survey’s design also appears to self-select for people who are inclined to claim Long Covid symptoms, whether valid or not. According to the paper, the survey consisted of 257 questions, took almost 70 minutes on average to complete, allowed participants to revisit their answers for up to 30 days, and was primarily marketed to readers of the Body Politic group’s various blogs and Slack channels. This design practically ensures that the majority of the people who received and completed the survey were drawn from a readership that already gravitates towards the group’s political messaging and medical eccentricities.
Imagine if a survey on diet products collected its sample entirely from the mailing list of Gwyneth Paltrow’s “Goop” store. And imagine if the CDC decided to use that survey as a basis for a billion dollar program to revise its food nutrition guidelines, claiming that it is a representative study of the average American’s diet. Because that’s essentially what NIH Director Francis Collins has done with Body Politic’s surveys when justifying his current research initiative into Long Covid before the public.
With most Long Covid research at the moment, self-diagnosis by amateur groups appears to have supplanted scientific rigor in driving the NIH’s research priorities. Even minimal scrutiny should cast doubt upon the Body Politic group’s deficit of scientific credentials and surplus of outright “alternative medicine” quackery. Yet in January 2021 the New York Times heavily leaned on testimonials from Body Politic’s resident psychics and alternative wellness healers in a feature story on so-called Long Covid, aiming to demonstrate the scientific validity of the diagnosis.
So did an August 2020 piece in the Atlantic that is widely credited with popularizing the concept. Indeed, the New York Times has turned its opinion page over to Body Politic writers on multiple occasions over the last year, giving them free rein to promote unscientific claims about the concept. Simply scanning over mainstream media coverage of “Long Covid” in the last year reveals that Body Politic-affiliated activists with dubious scientific credentials have become go-to “experts” on the subject. Here they are being interviewed in Vox, in the Guardian, in the Washington Post, on NPR, in Buzzfeed, and on MSNBC.
In calling attention to Body Politic’s influence over shaping the Long Covid narrative, I do not question the possibility that some of the organization’s activists may exhibit genuine long-term Covid-related symptoms, even if they are not a distinct classification unto itself. But scientific assessment of their claims remains woefully inadequate relative to the authority that the media has bestowed upon them. In this sense, much of the Long Covid literature bears striking resemblance to other claimed chronic illnesses that have less-than-robust scientific grounding (for example, consider the difference between Celiac disease – a rare but severe dietary illness involving gluten – and the mid-2010s “gluten sensitivity” craze, which mixed together real and imagined but also self-diagnosed symptoms, fad dietary practices, and dubious scientific attestation)
Despite their scientific shortcomings, Body Politic’s own surveys have found a welcome audience among many academics who should know better. Even leading medical journals now regularly tout Body Politic’s dubious survey results as if they are scientific fact.
Last fall, the BMJ published an article on “Long Covid” from a team of scientists led by Oxford’s Trisha Greenhalgh, an outspoken pro-lockdown regular on the BBC and other UK media circuits. Greenhalgh’s team estimated that perhaps as many as 10% of people infected with Covid develop “Long Covid” symptoms – a number that has since become a standard estimate for Long Covid risks.
Their empirical “evidence” for Greenhalgh’s claim, in turn, derives primarily from Body Politic’s “patient-led survey” of alleged Long Covid sufferers – the same survey where half or more of respondents never even had a confirmed Covid diagnosis. This was no accidental reliance on a substandard source, deriving from insufficient scrutiny of the survey’s methods. Greenhalgh credited the Body Politic group by name on Twitter for inspiring their paper, endorsing the “lived experience” of their “patient-led research.” Echoing the Body Politic survey, Greenhalgh and her co-authors further embrace the proposition “that a positive test for covid-19 is not a prerequisite for diagnosis” for Long Covid. It’s apparently sufficient to simply believe that you had a prior bout with Covid, and attribute your claimed long-term symptoms to the same.
Not surprisingly, Long Covid has become a favored fallback argument among lockdowner epidemiologists to argue for prolonged restrictions. Duke University’s Gavin Yamey has made a name for himself by credulously circulating conspiracy theories about the Great Barrington Declaration by blogger Nafeez Ahmed. Sure enough, he’s also a Long Covid activist, promoting Greenhalgh’s study as well as an assortment of news articles that blur the lines between legitimate reporting of long-term symptoms and quackery.
Although Body Politic is far from the only group advocating for Long Covid research funding, their high-profile promotion by the NIH, by leading news outlets, and by medical journals suggests a similar phenomenon to the pattern seen among other lockdown advocates in allegedly-mainstream epidemiology. We’re witnessing a full-scale breakdown of the screening mechanisms that normally steer scientific discourse away from fringe and conspiracist viewpoints – provided that those viewpoints may be used to advance the alarmist ideologies that have emerged around Covid policy over the last year. The doors have, sadly, been thrown wide open to psychic healing and alternative wellness gibberish. Lockdowner scientists have, in turn, given these suspect claims and defective survey designs a welcome home in the most prestigious institutions of journalism, government, and the ivory tower.
Phillip W. Magness is a Senior Research Fellow at the American Institute for Economic Research. He holds a PhD and MPP from George Mason University’s School of Public Policy, and a BA from the University of St. Thomas (Houston).
Prior to joining AIER, Dr. Magness spent over a decade teaching public policy, economics, and international trade at institutions including American University, George Mason University, and Berry College.
Photoshopping, fraud and circular logic in research

By Mike Hearn | Daily Sceptic | July 22, 2021
It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgement of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of the New England Journal of Medicine.
Check out this image from a peer reviewed research paper that supposedly shows skin lesions being treated by a laser:

Left: before treatment for keratoses. Right: after they were airbrushed out. (image diff is available here)
On being challenged the authors said:
The photograph was taken in the same room with a similar environment; unfortunately the patient wore the same shirt.
The journal found this explanation acceptable and forwarded the response to the complainants.
It’s becoming clear that science has major difficulties with not only a flood of incorrect and intellectually fraudulent claims, but also literally faked, entirely made up papers with random data, imaginary experiments and photoshopped images in them. Some of these papers are sold by organised gangs to Chinese doctors who need them to get promoted. But others come from really sketchy outfits like (sigh) the National Health Service, to whom we owe the masterpiece seen above.
The British Government hasn’t noticed that its doctors are massaging medical evidence. Instead this example comes from Elizabeth Bik, who runs a blog where she and a few other volunteers try to spot clusters of fraudulent papers. She embarrassed the journal in public here, and the paper was finally retracted. But she’s just a volunteer who raises money on Patreon for her work. Here’s her assessment of what’s going on:
Science has a huge problem: 100s (1000s?) of science papers with obvious photoshops that have been reported, but that are all swept under the proverbial rug, with no action or only an author-friendly correction… There are dozens of examples where journals rather accept a clean (better photoshopped?) figure redo than asking the authors for a thorough explanation.
As the only people trying to spot these fake papers are bloggers, we can safely assume that far larger numbers of papers are fake than the “thousands” they have already found and reported. For example,
0.04% of papers are retracted. At least 1.9% of papers have duplicate images “suggestive of deliberate manipulation”. About 2.5% of scientists admit to fraud, and they estimate that 10% of other scientists have committed fraud.
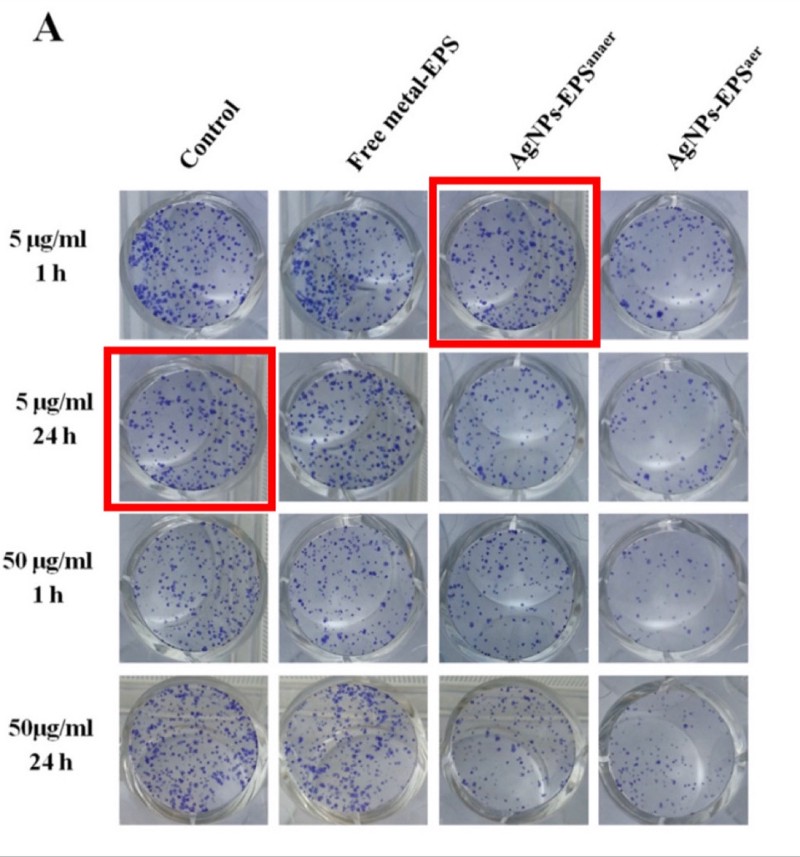
Photos of supposedly different samples in which two images are identical. From “Anticancer activity of biogenerated silver nanoparticles: an integrated proteomic investigation”. The journal investigated and concluded that this is fine.
It’s been known for years that a lot of claims made by scientists can’t be replicated. In some fields, the majority of all claims appear to not replicate due to a large mix of issues like overly lax thresholds for claiming statistical significance, poor study design and other somewhat subtle errors. But how much research is deliberate falsehood?
The sad truth is the size of the fraud problem is entirely unknown because the institutions of science have absolutely no mechanisms to detect bad behaviour whatsoever. Academia is dominated by (and largely originated) the same ideology calling for the total defunding of the police, so no surprise that they just assume everyone has absolute integrity all the time: research claims are constantly accepted at face value even when obviously nonsensical or fake. Deceptive research sails through peer review, gets published, cited and then incorporated into decision making. There are no rules and it’d be pointless to make any because there’s nobody to enforce them: universities are notorious for solidly defending fraudulent professors.
So let’s turn over the rock and see what crawls out. We’ll start with China and then turn our attention back to more western types of deception.
Chinese fraud studios
In 2018, the U.S. National Science Foundation announced that: “For the first time, China has overtaken the United States in terms of the total number of science publications.” Should the USA worry about this? Perhaps not. After some bloggers exposed an industrial research-faking operation that had generated at least 600 papers about experiments that never happened, a Chinese doctor reached out to beg for mercy:
Hello teacher, yesterday you disclosed that there were some doctors having fraudulent pictures in their papers. This has raised attention. As one of these doctors, I kindly ask you to please leave us alone as soon as possible… Without papers, you don’t get promotion; without a promotion, you can hardly feed your family… You expose us but there are thousands of other people doing the same. As long as the system remains the same and the rules of the game remain the same, similar acts of faking data are for sure to go on. This time you exposed us, probably costing us our job. For the sake of Chinese doctors as a whole, especially for us young doctors, please be considerate. We really have no choice, please!
Note the belief that “thousands of other people” are doing the same, and that these doctors need more than one paper to keep being promoted, so the 600 found so far is surely the tip of an iceberg given China’s size. There are about 3.8 million doctors in China implying that there are quite possibly tens of thousands, maybe hundreds of thousands of these things in circulation.
The fake papers are remarkable:
- They are so good they are undetectable in isolation. The NHS photo is an aberration – normally these papers get spotted by noticing re-used technical images across papers that claim to be different experiments by different people. The fake papers are probably produced by real scientists with access to real lab equipment. The use of spammy-looking Gmail accounts is also a signal because Gmail is banned in China (e.g.
BrendaWillingham12192@gmail.com,RosettajKirkland3814@gmail.com,CaseyPeiffer8311@gmail.com). The reliance on bot-generated Gmail accounts implies enormous scale. - They are peer reviewed and published in western journals. For instance, the Journal of Cellular Biochemistry by Wiley or Biomedicine & Pharmacotherapy by Elsevier. They claim to be doing advanced micro-biology on serious diseases: a typical title is something like “MicroRNA-125b promotes neurons cell apoptosis and Tau phosphorylation in Alzheimer’s disease”. Journals have no way to detect these papers and aren’t trying to develop any.
- Some of them present traditional Chinese medicine as scientific. TCM is more or less the Chinese equivalent of homeopathy with lots of herbal remedies, eating body parts of exotic animals to cure erectile dysfunction, and so on. But the Chinese Government is obsessed with it and thinks it’s the same as normal medicine. From the top down, Chinese scientists are expected to produce papers claiming that TCM works, and they do! Mostly this stuff stays in Chinese but the ever increasing reliance of western universities on Chinese funding means it’s now finding its way into the English language literature as well, e.g. “Probing the Qi of traditional Chinese herbal medicines by the biological synthesis of nano-Au” was published by the Royal Society of Chemistry.

Advert by a research faking operation. Credit to “Smut Clyde” and “TigerBB8”.
Most western scientists are too clever to buy a completely fake paper (or so we hope). But their promotion incentives are identical, and there are other techniques that let you publish as many fake papers as you want. Let’s turn our attention to…
Impossible numbers in western science
The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue.
Richard Horton, editor of the Lancet
How many scientists just make up their data? A well known recent case of this was the Surgisphere scandal, in which a paper appeared in The Lancet that claimed to be based on a proprietary dataset of nearly 100,000 COVID-19 patients across over 670 U.S. hospitals. This figure was larger than the official case counts of some entire continents at the time, and there was no reason for hospitals to share tightly controlled medical data with a random company nobody had heard of, so the claim was implausible on its face. Sure enough, when challenged it turned out none of the authors had ever actually seen the data, just summaries of it provided by one guy, who on investigation had a long track record of dishonesty. The Lancet probably accepted this paper because it made Trump look bad and the editor (Horton, quoted above) appears to hate Trump more than he hates bad science.
There are some other cases like this that came to light over the years, like the story of Brian Wansink, or that of Paolo Macchiarini, who left a trail of dead patients in his wake. But while anecdotes about individual cases are interesting, can we be more rigorous?
One clue comes from automated tools that scan research papers looking for mathematically impossible numbers, which can sometimes be detected even in the absence of the raw original data. In recent years a few such tools have been developed and deployed, mostly against psychology and food science.
- The statcheck program showed that “half of all published psychology papers… contained at least one p-value that was inconsistent with its test”.
- The GRIM program showed that of the papers it could verify, around half contained averages that weren’t possible given the sample sizes, and more than 20% contained multiple such inconsistencies.
- The SPRITE program detected various experiments on food that would have required subjects to eat implausible quantities (e.g. a child needing to eat 60 carrots in a single sitting, or 3/4 kilogram of crisps).
Being flagged by a stats checker doesn’t guarantee the data is made up: GRIM can detect simple mistakes like typos and SPRITE requires common sense to detect that something is wrong (i.e., no child will eat a plate of 60 carrots). But when there are multiple such problems in a single paper, things start to look more suspicious. The fact that half of all papers had incorrect data in them is concerning, especially because it seems to match Richard Horton’s intuitive guess at how much science is simply untrue. And the GRIM paper revealed a deeper problem: more than half of the scientists refused to provide the raw data for further checking, even though they had agreed to share it as a condition of being published. This is rather suspicious.
One of the difficulties with detecting scientific fraud is that the line between dishonesty and simple absurdity can get quite blurry. Sometimes scientists “calculate” data that is clearly wrong, but don’t actually try to hide or it may even admit to it in the paper, knowing full well that nobody cares and nonsensical data won’t actually matter. Here’s an example from a COVID modelling paper:
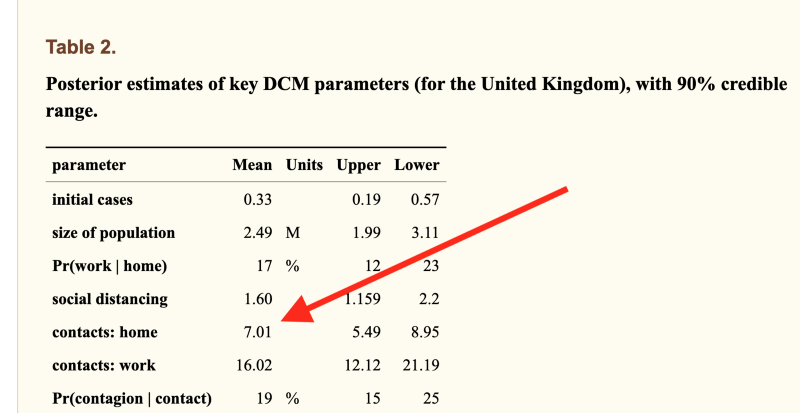
The model was allowed to calculate that the average Brit must live with 7 other people, because it couldn’t obtain data fit otherwise (actual number=2.4). This one comes from University College London, is written by 12 neuroscientists, passed peer review and has 37 citations. The peer reviewer noticed that the incorrect number was in the paper but signed off on it anyway.
For decades psychiatrists published research into the “gene for depression” 5-HTTLPR. They created an entire literature not only linking the gene to depression but explaining how it worked, linking it to parenting styles, developing treatments based up on it. Over 450 papers were published on the topic. Eventually a geneticist discovered what they were doing and used DNA databanks to point out that none of those papers could possibly be true.
Sometimes numbers aren’t “wrong” but are instead logically vacuous. The Flaxman et al paper from Imperial College that tried to prove lockdowns work had the usual problem of statistically implausible numbers, but more importantly was built on circular logic: their model assumed only government interventions could end epidemics. This is obviously nonsense and they breezily admitted it in the paper, where they said their work was “illustrative only” and that “in reality even in the absence of government interventions we would expect Rt to decrease”. No problem: this fictional illustration got published in Nature and the authors presented the model’s outputs as scientific proof of their own assumption to the media. The paper is vacuous mathematical obfuscation, but scientists either can’t tell or don’t care: it has racked up over 1,300 citations and the number is still growing rapidly. To put that number in perspective, in physics the top 1% of all researchers have around 2,000 citations over their entire career.
Time to assume that health research is fraudulent until proven otherwise?
Earlier this month, the BMJ published an astounding blog post with the same title as this section. There’s no need to add anything because simply quoting it is sufficient:
The anaesthetist John Carlisle analysed 526 trials submitted to Anaesthesia and found that… when he was able to examine individual patient data in 153 studies, 67 (44%) had untrustworthy data and 40 (26%) were zombie trials… [Ben] Mol’s best guess is that about 20% of trials are false. Very few of these papers are retracted.
We have now reached a point where those doing systematic reviews must start by assuming that a study is fraudulent until they can have some evidence to the contrary.
Richard Smith
Richard Smith is a former editor of the BMJ, cofounder of the Committee on Medical Ethics (COPE), for many years the chair of the Cochrane Library Oversight Committee, and a member of the board of the U.K. Research Integrity Office.
Or put another way, an overseer of the Research Integrity Office believes research has no integrity.
What can be done?
600 fraudulent papers here, 450 over there, 1300+ citations of just one bad paper… pretty quickly it starts adding up.
We’re often told science is self-correcting. Is that true? Probably not. “The Science Reform Brain Drain” is perhaps the bleakest essay I’ve read this year. Reformers like the men who developed SPRITE and GRIM have been giving up and leaving science entirely. Pointing out in public that your colleagues are dishonest is never a great career move, and the work was often futile. One scientist who quit and went into industry summed up his fraud detection work like this:
The clearest consequence of my actions has been that Zhang has gotten better at publishing. Every time I reported an irregularity with his data, his next article would not feature that irregularity.
Even when a bull enters the China shop and gets a few papers retracted, it doesn’t actually matter because it has little effect: retracted papers keep getting cited for years afterwards and actually may be cited more than non-retracted papers, because one of the effects of retraction is that the article becomes free to download.
In the past year most talk of bad science has been about models with bad assumptions. This is an issue but has been hiding problems that are far worse: scientists are buying fake papers, Photoshopping evidence, refusing to upload their data, knowingly publishing numbers that cannot be correct, citing papers that were retracted for being fraudulent and (of course) presenting mathematical obfuscations of what they want to be true as if it were science. Journals usually ignore fraud reports entirely, or when put under pressure let scientists submit “corrected” versions of their papers. And worst of all, the journal editors that are responsible for scientific gatekeeping know all this is happening, but aren’t doing anything about it.
In fact, very little can be done because above all, universities rely on reputation and don’t want anyone to find out about bad behaviour, so they fight tooth and nail to protect academics no matter how badly they are behaving. There are no rules. Any rules that are alleged to exist turn out when tested to be illusions.
Claims made by scientists are automatically trusted by the majority of people. Maybe they shouldn’t be?
Mike Hearn is a former Google software engineer. You can read his blog at Plan 99.
British journalists could face jail for publishing leak stories that embarrass the government
Chilling new proposals
By Dan Frieth | Reclaim the Net | July 20, 2021
As if there needed to be yet another threat to free speech in the UK, British journalists could face 14-year prison sentences for publishing stories embarrassing the government, under proposed reforms to the Official Secrets Act. According to the government, the new proposals will crack down on foreign spies but many fear it could even be used domestically.
The UK government, through the Home Office, has proposed reforms to the 1989 Official Secrets Act, to account for changes technology and the internet has enabled in the sharing of leaked data.
But critics have noted that with the proposed changes local journalists are not protected if charged under the new laws.
Critics further noted that if the new proposals were currently law, the journalists who revealed that former Health Secretary Matt Hancock broke his own COVID rules while having an affair with his aide would have been charged. The leak was newsworthy and the story broke through leaked CCTV footage.
Last week, the Information Commissioner’s Office came under fire when it emerged that it searched two homes while investigating how the CCTV footage leaked to The Sun, the news outlet that first broke Matt Hancock’s affair story.
Among the groups criticizing the new proposals is the National Union of Journalists (NUJ), which noted that the new law would treat whistleblowers and those who publish leaked content the same way foreign spies are treated.
A spokesperson for the organization said:
“Existing legislation distinguishes provisions and penalties between those who leak or whistleblow, those who receive leaked information, and foreign spies.
“The government proposes to eliminate or blur these distinctions. The government also wants to increase the maximum penalties that journalists might suffer for receiving leaked material from two to 14 years…
“The NUJ has long argued that where whistleblowers believe that they have acted in the public interest, they should be able to make this case in court, and if a jury agrees with them, be protected.”
But according to the Home Office:
“Since the passage of the Act in 1989, there have been unprecedented developments in communications technology (including data storage and rapid data transfer tools) which in our view, means that unauthorized disclosures are now capable of causing far more serious damage than would have been possible previously.
“As a result, we do not consider that there is necessarily a distinction in severity between espionage and the most serious unauthorized disclosures, in the same way that there was in 1989.
“Although there are differences in the mechanics of and motivations behind espionage and unauthorized disclosure offenses, there are cases where an unauthorized disclosure may be as or more serious, in terms of intent and/or damage.
“For example, documents made available online can now be accessed and utilized by a wide range of hostile actors simultaneously, whereas espionage will often only be to the benefit of a single state or actor.
“In severe cases, the unauthorized disclosure of the identities of agents working for the UK intelligence community, for example, could directly lead to imminent and serious threat to life.”
The Law Commission and the human rights organizations that helped draft the new proposals insist there should be a “public interest defense” in the amendment to protect journalists who receive leaked content.
However, the Home Office argues that such a provision would “undermine our efforts to prevent damaging unauthorized disclosures, which would not be in the public interest.”
A Home Office spokesman said:
“Freedom of press is an integral part of the UK’s democratic processes and the government is committed to protecting the rights and values that we hold so dear.
“It is wrong to claim the proposals will put journalists at risk of being treated like spies and they will, rightly, remain free to hold the government to account.
“We will introduce new legislation so security services and law enforcement agencies can tackle evolving state threats and protect sensitive data.
“However, this will be balanced to protect press freedom and the ability for whistleblowers to hold organizations to account when there are serious allegations of wrongdoing.”
Do drug trials underestimate side effects?

By Dr Sebastian Rushworth | July 19, 2021
One commonly used trick in drug trials is to exclude any group that might make the drug look worse, such as those that are more likely to experience side effects. A good recent example of this is the covid vaccine trials, which largely excluded people with auto-immune diseases (more likely to develop an auto-immune disease after vaccination), people with allergies (more likely to have an allergic reaction to the vaccine), and, of course, the elderly (less likely to develop immunity after getting the vaccine, and more likely to become seriously sick from it).
These three groups are all frequently excluded from trials, and the exclusion is particularly galling when it comes to the elderly, because they are a big segment of the population, and they are also usually the most likely to end up actually using the drugs being tested.
When drug companies have gotten a drug approved, and move on to market the drug, they will studiously avoid mentioning the fact that large segments of the population were excluded from the trials. When drug reps show their flashy powerpoints to gatherings of doctors, say for a new drug to lower blood pressure, they will always present impressive looking graphs of benefit, and they will of course point out how safe their drug was shown to be in the trials. Not once will they mention that the groups of patients the doctors will primarily be prescribing the drug to weren’t even included in the trials.
The doctors will then happily go off and prescribe the drug to multi-morbid 90 year olds, which might explain why prescription drugs are now the third leading cause of death in the western world.
The manipulation of who is included in trials is probably one of the main reasons why findings of side effects always end up being much higher in reality than in clinical trials. It might explain, for example, why muscle pain is a massively common side effect of statins in the real world, while being vanishingly rare in the statin trials (as Dr. Malcolm Kendrick has written about in detail).
A study recently published in the Lancet Healthy Longevity sought to estimate the extent to which drug trials underestimate side effects. It was funded by the UK Medical Research Council and the Wellcome Trust. The study chose as its particular focus people being treated for high blood pressure with a certain class of blood pressure lowering drugs known as RAAS blockers (which includes all drugs with names ending in -pril and all drugs with names ending in -sartan). The advantage with looking at this particular class of drugs is that there are a ton of trials. Every major pharmaceutical company has its own RAAS-blocker. It should therefore be possible to draw relatively broad conclusions about the results – whatever they show, they apply to the entire pharmaceutical industry, not just to a few specific companies. It’s also reasonable to think that the results apply to other classes of drugs too – there’s no reason to think trials of RAAS-blockers have been done differently than trials of other drug classes.
What the study sought to do more specifically was compare the rate of serious adverse events in clinical trials of RAAS-blockers with the rate observed in the real world. A serious adverse event is any event that is potentially life threatening or that results in death, hospitalization or lasting disability. If a trial has been designed in such a way that it is representative of reality, then the rate of serious adverse events in the trial should largely mirror that seen in the real world.
110 trials of RAAS-blockers were identified by the researchers. Of these, 11 were specifically designed to look at older people (i.e. didn’t recruit anyone under the age of 60). The data on serious adverse events from these 110 trials was extracted and compared to real world data on deaths and hospitalizations taken from a UK government funded database of 55,000 people living in Wales, who were being treated with RAAS-blockers. Deaths and hospitalizations are not exactly the same thing as serious adverse events (which as mentioned above also include “life threatening events”, and could for example include someone who is treated in an emergency department after a fall but not admitted to the hospital), but they’re close enough to allow a reasonable comparison.
So, what were the results?
Let’s begin with comparing the trials of older people with the “standard” trials. The relative rate of serious adverse events in the trials of older people was 76% higher than the rate in the standard trials. This shows the importance of including elderly people in drug trials – they are much more likely to experience adverse events of all kinds (including those actually caused by the drug being tested), and excluding them will therefore likely underestimate side effects.
Considering that many of the drugs in common use show marginal benefits at best (statins have, for example, only been shown to prolong life by a few days on average), this is important information. Why? Because a drug that is beneficial, on balance, to a fifty year old, who has a fully functioning kidney and liver, and is therefore unlikely to suffer side effects, could easily be harmful, on balance, to an 80 year old.
That’s why drug studies done on younger people should not be used to guide treatment of older people. No shock there. Everyone already knows that we shouldn’t be extrapolating results from one group to another (even though it happens all the time, as we’ve seen most recently with the covid vaccine trials).
Next we come to the more important, and perhaps more shocking finding.
The real world patients were between 300% and 400% more likely to experience a serious event than the participants in the trials! That is in spite of the fact that the trials, as mentioned above, were using a broader definition of what constituted a serious event. If the trials were representative of reality, then they should have a higher rate of events than is seen in the real world data. Instead they have a rate that is several times lower!
Interestingly, the trials of older people were just as far from the real world results as the trials of younger people. Clearly, doing trials on the elderly is not enough on its own to produce trials that are representative of reality. What’s happening here exactly?
There are three possible explanations, as far as I can see. The first explanation is that the trials are representative of reality, but that the Welsh die and are hospitalized at a rate that is several times higher than people in the countries where the studies were conducted. Many of the trials were conducted in the US, not in Wales. But Wales has a higher life expectancy than the United States, so that seems unlikely. I think we can discount that explanation.
The second explanation is that the trials are unrepresentative in so many different ways that just correcting the age issue doesn’t make a noticeable difference. That’s probably part of the explanation. The average age even in the trials of “older people” was 73, which isn’t very old from my perspective. And those 73 year olds included in the trials were probably at the healthier end of the spectrum.
The third, more sinister explanation, is that the pharmaceutical companies are hiding serious adverse events… But wait a minute, the trials are randomized and blinded, so the people running the drug trials have no way of knowing if someone experiencing a possible side effect is in the treatment group or the placebo group, right?
Yes, that’s right, so the easiest solution, if you want to avoid finding nasty side effects, is to not report them, regardless of which treatment group the participant is in. That will cut down on total adverse events in both groups, which will make any difference between the groups that does exist smaller in absolute terms, and also less likely to reach the level of statistical significance. Voila – the treatment group and the placebo group end up having similar rates of side effects, and the drug company can conclude that the drug is completely safe.
Is that what’s happened here? Are the pharmaceutical companies hiding adverse events? Well, it’s very strange that the real world data shows a rate of serious adverse events that is several times higher than is found in the trials. It’s hard to see how that massive difference could be explained in any other way.
So, how big a problem is this?
Big. Very big. It should shake the very foundations of evidence based medicine. If the drug trials and the real world data show such wildly different rates of adverse events, then it really begs the question how much we can trust the trials at all. It would be perfectly reasonable in this situation to say that all “evidence” produced by pharmaceutical companies is so suspect that it should be dismissed out of hand, and that only independently funded trials should be used as a basis for medical treatment decisions.
The problem with that is that it would mean saying goodbye to most of the trials that form the basis of modern medical treatment, and there is not much to replace them with. This issue could be solved over the longer term through large tax payer funded investments in new independent trials. But there’s no quick fix.
The problem is most acute when it comes to the many drugs in common use that only show marginal benefits, such as statins. If the rate of side effects is actually 300% to 400% higher than seen in the trials, then the harms of these drugs could easily outweigh the benefits. In other words, the cost-benefit calculation could shift entirely for many of the most commonly used drugs.
Ok, let’s wrap this up. What can we conclude?
Drug trials do no accurately represent rates of adverse events. It is likely that the true rate of side effects is often many times higher than that seen in drug trials.
Bill Gates’s stranglehold on the MSM: Part 2 – Britain

By Karen Harradine | The Conservative Woman | July 16, 2021
WITH an estimated fortune of $128.9billion, Bill Gates is the fourth richest man in the world, after Amazon’s Jeff Bezos, Bernard Arnault and Elon Musk, according to Forbes.
He’s stepped back from the day-to-day running of Microsoft, the company he founded in 1975, and focuses on his so-called philanthropy through the Bill & Melinda Gates Foundation (GF), and is best known for his worldwide vaccination and anti-malaria programmes.
Less widely known is that he has spent hundreds of millions bankrolling news outlets, in the process turning the GF into one of journalism’s main gatekeepers. According to Tim Schwab of Columbia Journalism Review, by last June more than $250million had gone to news operations including the BBC, NBC, Al Jazeera, ProPublica, National Journal, the Guardian, the Financial Times, Univision, Medium, the Atlantic, the Texas Tribune, Gannett, Washington Monthly, Le Monde, and the Center for Investigative Reporting; and to charitable organisations affiliated with news outlets, like the BBC’s Media Action and the New York Times’s Neediest Cases Fund.
As I reported in Part One of this investigation, most of this funding comes under the fine sounding GF heading of Global Policy and Advocacy, of which the BBC is a major beneficiary. Little wonder that there is little that is dispassionate about its reporting on Covid-19 vaccination or climate change.
It’s not just the BBC that the GF manipulates through these means. Between 2016 and 2020, the Financial Times received $2.3million from the GF, including $1.3million to fund ‘global health awareness’. The Guardian is another recipient of Mr Gates’s largesse. Like the BBC, it sports a ‘Global Development’ site, the common root being GF funding. Its claimed editorial independence is contradicted by its stated sole campaigning purpose to provide special focus on the Millennium Development Goals, eight targets set in 2000 by the United Nations Millennium Declaration. The Guardian has bought into this to the extent that it operates mainly as a deferential PR channel for both the UN and the GF.
The collaboration with the GF to ‘help focus the world’s attention on global development’ goes back 11 years. This is a sophisticated propaganda exercise to convince the public of the beneficial nature of Gates’s investments in a multitude of global development projects including vaccines and solutions for climate change. It helps ensure that any alternative narrative or critique is unlikely to see the light of day in any of the outlets to which he extends his munificence.
Since August 2011, the GF has given the Guardian $12.2million towards this, the latest grant being almost $2million last September. The Guardian has not only busily promoted the Millennium Development Goals, but also its spawn, the UN 2030 Agenda for Sustainable Development, yet another dishonest scheme to take guilt money from Western taxpayers and give it to the world’s despots and dictators, all in the name of climate change.
Yet, as I have previously set out: ‘Very little information is available on exactly how the money is invested and who benefits from it. No information is offered to indicate if it has been cost-effective and beneficial to the economies and welfare of the 193 countries signed up to it.’
The British public have been drip-fed this propaganda for years through various GF-funded MSM mouthpieces such as the BBC. Yet it’s the economically fragile West which pays for the 2030 Agenda and its climate change ‘remedies’, draining it of even more of its resources while authoritarian regimes like China benefit financially and increase their dominance over the UN. The MSM barely protests.
The worry is that the GF has not only captured the Left-wing media in Britain: it has also made inroads into the so-called Centre and Right. The Telegraph accepted $3.4million from the GF in November 2017 to ‘raise awareness’ of global health issues. The London Evening Standard was awarded money in the same year too, receiving $20,000 to spread the GF propaganda on the ‘global health crisis’.
The growing financial dependence of the MSM on a combination of Government advertising and GF largesse has already put its impartiality in jeopardy. This is threatened further by the GF’s funding of a global network of young ‘journalists’. This project, called the International Centre of Journalists, has been given $20.4million to promote ‘public awareness’ around global health. Based in the US, the organisation finances activists to promote ‘better governments’ and make ‘communities safer and healthier’, amongst other woke ideals. Their 2020 annual review predictably emphasises the need to highlight racial injustice and climate change, and combat ‘disinformation’ about Covid-19.
As Robert Kennedy Junior says, Gates’s press bribes have paid off. ‘During the pandemic, bought and brain-dead news outlets have treated Bill Gates as a public health expert despite his lack of medical training or regulatory experience.’
Gates also funds an army of independent fact checkers including the Poynter Institute and Gannett which, Kennedy points out, use their platforms to silence detractors and to debunk as ‘false conspiracy theories’ and ‘misinformation’ charges that Gates has championed and invested in sinister endeavours like biometric chips, vaccine passports and satellite systems.
Yet all the evidence is available at a click of a mouse button. Last March, Gates began his vaccine passport campaign. The GF-funded Guardian and the BBC have unquestionably cheered on this digital slavery. In 2018, Gates gave a satellite start-up $1billion to build a system which broadcasts real-time videos globally. What better way to ensure that the little people are behaving themselves than by funding a satellite system to monitor us all? Despite the vehement denials of the GF funded ‘fact checkers’, Gates has built his Covid-19 vaccine factories, and seemingly now seeks a return on his investments.
Many lament the decline of journalistic standards in our New Dark Age. Of those responsible for turning a once-brilliant British media into an uncritical disseminator of propaganda, the GF must be placed centre stage. Now the MSM, like the Government, are often nothing more than useful idiots for the GF and its destructive policies, mindlessly chanting the GF narrative on development, climate change and Covid-19; and whose ‘solutions’ to these are destroying the free and prosperous West.
Don’t expect our MSM journalists to protest: they have long since been bought, paid for and brainwashed.
Israel exploits case of Mexico official wanted for torture, murder for diplomatic gain
MEMO | July 15, 2021
The notorious case of former top Mexican official wanted in connection with the torture, abduction and murder of 43 students, and for embezzling $50 million of state funds, has become mired in a diplomatic tussle between Israel and Mexico over the occupation state’s treatment of Palestinians.
Tomás Zerón de Lucio, the former director of Mexico’s equivalent of the FBI, fled to Israel following the opening of an investigation into his role in the 2014 Iguala mass kidnapping, which continues to cause a storm in Mexico to this day. Zeron headed the criminal investigation, but his report was discredited after it was discovered that crucial testimony was obtained under torture, evidence was mishandled and promising leads ignored.
Zeron has dismissed the charges and has been seeking political asylum in Israel, where he has lived for nearly two years. Mexican officials say that Zeron has connections to powerful Israeli companies that helped him flee Mexico.
Allegations against the former official also include the embezzlement of $50 million worth of state funds. While in office, Zeron is said to have authorised the purchase of tens of millions of dollars in surveillance systems from private Israeli intelligence firms including the notorious Pegasus software developed by Israel’s NSO Group. The software has been used to target journalists, lawyers and activists in several countries around the globe. It’s claimed that in some cases the intelligence gear purchased by Zeron were never delivered.
Mexico has demanded the extradition of Zeron. Israel however has not acted on either the extradition request or the asylum claims and is said to be looking for ways to squeeze diplomatic concessions out of the highly sensitive case.
Senior Israeli officials were cited in the New York Times saying that Zeron’s extradition case was being slow-walked as “tit-for-tat diplomacy” against Mexico, which has supported United Nations inquiries into allegations of Israeli war crimes against Palestinians. “Why would we help Mexico?” the official said, speaking on condition of anonymity to offer a candid view of a diplomatic dispute.
The senior Israeli official said that the current Mexican government has repeatedly supported resolutions criticising Israel at the UN Human Rights Council in Geneva, including decisions to investigate Israel’s killing of Palestinian protesters in Gaza in 2018 and the killing of civilians in the besieged enclave during the occupation state’s latest onslaught.
Video producer Matt Orfalea censored again for calling out YouTube censorship
By Tom Parker | Reclaim the Net | July 13, 2021
After he published a video discussing YouTube’s censorship last month, video producer Matt Orfalea was censored and had his channel demonetized. Now, YouTube has targeted Orfalea once again and removed another video where he and his guest, independent journalist Alison Morrow, called out the tech giant’s censorship.
In the video, which is titled “YouTube BANS Reporter Exposing YouTube HYPOCRISY,” Orfalea and Morrow recapped the escalating YouTube censorship they have both faced.
This censorship began in June when Orfalea’s YouTube channel was suspended for uploading what he described as “unpublished rough cuts” of a video highlighting YouTube’s censorship of ivermectin.
Orfalea was then demonetized in July after YouTube flagged a seven year old, 13 second parody video for allegedly violating its “violent criminal organizations” policy. After facing backlash, YouTube admitted “error” but did not re-monetize his videos.
A few days after Orfalea was demonetized, he was a guest on Morrow’s channel in a video where she highlighted how mainstream media outlets are allowed to violate YouTube’s “medical misinformation” policy without facing sanctions. This video was censored and then reinstated after YouTube faced pushback for taking it down.
In the “YouTube BANS Reporter Exposing YouTube HYPOCRISY” video, Morrow suggested that her video may have been removed because of Orfalea’s guest appearance and speculated that YouTube’s artificial intelligence (AI) could be flagging people that have previously been sanctioned by YouTube and then censoring videos from other creators that associate with those that have been flagged.
“This is just a perfect example of what’s happening now,” Orfalea added. “Where we have this caste system, this blatant double standard… so clearly, as you’ve described, this is not about protecting viewers from misinformation, this is about allowing, you know, some privileged class of journalists… corporate media and allow them to say things without being challenged.”
Shortly after Orfalea posted this video where he and Morrow criticized YouTube for its censorship, YouTube took it down for allegedly violating the platform’s “medical misinformation” rules.
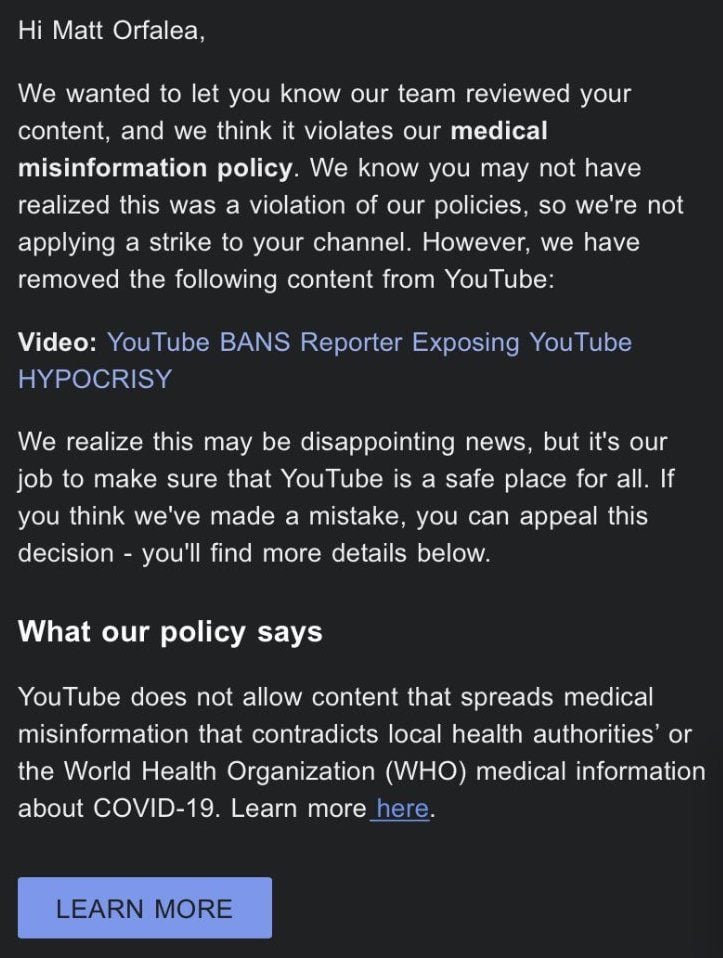
Orfalea appealed but YouTube rejected the appeal and told him: “We reviewed your content carefully, and have confirmed that it violates our medical misinformation policy.”
“I’ve been dealing with this insanity for almost a full month now,” Orfalea said after YouTube rejected his appeal. “YT reinstated Alison’s video. So they should reinstate my video, referencing hers, too!”
YouTube’s consistent targeting of Orfalea is reflective of the double standard on YouTube between independent creators and mainstream media outlets that he called out in this now-censored video.
Independent creators are 20x less likely to top coronavirus search results, 14x less likely to be recommended on election related content, and 10x less likely to top search results for some other newsworthy events.
YouTube’s CEO Susan Wojcicki has also admitted that the platform’s recommendation algorithm was changed in response to the media’s radicalization theory and said the platform won’t recommend YouTubers for breaking news.
Related: 🛡 Big Tech’s double standard on “conspiracy theories” when they come from mainstream media
Featured Video

BEN-GVIR: “ALL OF LEBANON MUST BURN” — w/ Mouin Rabbani
or go to
Aletho News Archives – Video-Images
From the Archives
Jewish Guilt is the Discourse of The Goyim
By Gilad Atzmon | April 24, 2018
For quite some time the British have accepted that British Jewish organizations have hijacked the political discourse. As has happened in other Western countries, the British political establishment has engaged is a relentless rant against antisemitsm. Sometime the focus drifts for a day or two. An alleged ‘Russian nerve gas attack’ provided a 48 hour pause. Occasionally we bomb Arabs in the name of ‘human intervention’ only to realize a day or two later that we have, once again, followed a premeditated foreign agenda. But, somehow, we always return to the antisemitism debate, as if our media and politicians are a herd of flies gravitating to a pile of poop. … continue
Blog Roll
 Aletho News
Aletho News- BEN-GVIR: “ALL OF LEBANON MUST BURN” — w/ Mouin Rabbani
- There Are No Budget Constraints In New York City: “Coastal Resiliency” Edition
- The UN’s plan to levy taxes on global trade is a sinister power grab
- Is there a future for the U.S. strategy in the Arctic?
- UN inquiry finds Israel ‘intentionally’ targeting Palestinian children in Gaza, occupied West Bank
- Citizens Around the World Demand Israel’s Expulsion From the United Nations
- ‘Israel not party to US-Iran talks, will continue full operations in Lebanon,’ Israeli far-right minister says
- Two killed in brazen Israeli ceasefire violation in southern Lebanon
- Which Country Is the Big Loser from the Ramadan War?
- Israeli Intel Whistleblower: Israel Ended Clinton Iran Deal With Epstein Blackmail
- If Americans Knew
- UN: Israel Continues to Commit Genocide and Other Atrocity Crimes by Deliberately Targeting Palestinian Children
- Bari Weiss, Free-Speech Fraud & Zionism Promoter, Would Rather Deport Than Debate
- ‘Doctor of the Poor’: Israeli Occupation Arrests Prominent Palestinian Physician
- Search for Your Church (and see if it has been targeted by the Israeli gov’t)
- Mark Levin Flying to Israel as Netanyahu Reportedly Seeks to ‘Leverage’ Levin to Trash Trump’s Iran Deal
- Watch: Zionist Brags about Israel’s Power to Get the World to Do What Israel Wants
- In Gaza, another senseless death on what should have been a joyous day – Daily Update
- The Republican & Democratic Politicians Trying to Scuttle Iran Agreement
- Israel’s continued targeting of civilians in Lebanon renders ceasefire meaningless
- U.S. intelligence warns Israel is likely to undermine Iran peace deal, officials say
- No Tricks Zone
- 3 New Studies Find Increasing Trends In Solar Radiation Since The 1980s – Easily Explaining Warming
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
