It’s time to end the mandates

By Steve Kirsch | January 24, 2022
Boris Johnson recently declared an end to the COVID restrictions in the UK. He said, “We will trust the judgment of the English people.”
Why can’t we do that in the US? Isn’t it time to trust the judgment of the American people?
Whether you ask a red or blue pill person, it’s clear that both sides have compelling rationales to end the mandates and the State of Emergency.
Interestingly, the rationale for each side is completely different, but the conclusion is the same. Here’s how they stack up.
Blue pill rationale
- We don’t need mandates for the vaccine or masks because we know they work. No need to sell us! Mandate or not, we will comply.
- We no longer fear those who are not compliant: we are all boosted up the wazoo using safe and effective vaccines with virtually no side effects AND we are wearing N95 or P100 masks at all times. And we always stay 6 feet from any other person. So there is basically no way to infect us.
- We have nothing to fear. Virtually none of us will be hospitalized, and none of us risk death. And the prevalence of Omicron makes our risk even lower.
- We think people who are not compliant are evil and deserve to die. Why force them to take life-saving medical interventions? We are better off as a society if these people are gone. Permanently.
- We trust our doctors to deliver quality medical advice. Our doctors always follow the CDC guidance which has been uniformly excellent. We all should be treated the same, no matter what our medical histories are. If the doctors follow the CDC guidelines, almost nobody dies. All the hospitals are filled with unvaccinated people.
- Just to be safe, we test ourselves every day using antigen tests for COVID. If we have a positive test result, we now have two new safe and effective drugs from the most trusted drug companies in the world so that in the rare chance that we get COVID, we can treat it with nearly 100% success.
Red pill rationale
- Mandates aren’t needed because we won’t comply with them anyway. They just create division and animosity in society. They divide us.
- We don’t fear the vaccinated.
- Cloth, surgical, and N95 masks don’t work so why should we wear them? P100 masks do work, but they are pretty cumbersome and not worth the trouble for a COVID variant that can’t hurt us.
- Social distancing is useless and doesn’t work. The 6 foot rule is not based on any science. Why isn’t it 5.2 feet? Nobody has seen the science justifying 6 feet so we aren’t going to comply with silly non-scientific rules.
- The current COVID vaccines are more likely to kill people than save them. In the Pfizer trial, 24% more people died in the group taking the vaccine! So it’s clear. If the vaccines don’t kill us, they will actually make the pandemic worse because they depress our immune system making us twice as likely to be infected with COVID as well as susceptible to other diseases (like reoccurrence of cancer). They also cause serious side effects. They are the most dangerous vaccines in human history. There is no way we will take them. Mandating them is just going to piss us off and hurt the economy. You will not get us to take them.
- Why would we take a drug that could kill us to prevent a variant that cannot? You’d have to be nuts. We will not comply so the mandates won’t make us.
- The primary variant is Omicron which if it happened today, we’d just ignore it since it is like getting a cold.
- If we get sick, we have very effective early treatment protocols using existing safe repurposed drugs like ivermectin, HCQ, aspirin, vitamin D, NAC, and Prozac. These protocols are 100% successful in preventing death from COVID when given early. We would never use Molnupiravir or Paxlovid; those drugs are both super dangerous.
- We use symptoms to determine if we have COVID. If we are unsure, we can use antigen tests. There is no need to test if we aren’t symptomatic because we know there is virtually zero asymptomatic spread and because the antigen tests almost never work reliably unless you are symptomatic so it’s a complete waste of money to test asymptomatic people. The testing companies don’t want anyone to know that, but we do.
- If we do get sick with COVID symptoms, we stay home and rest.
- Even if we had a truly safe vaccine, those of us who are recovered from COVID wouldn’t need it. A uniform mandate for everyone makes no sense.
- We believe doctors should be allowed to be doctors and that medical care should always be delivered by our healthcare professional we trust to use his professional judgement on our individual case. The CDC guidance is just awful.
13% of US hospitals critically understaffed, 22% anticipate shortages: Numbers by state
By Marissa Plescia and Kelly Gooch | Becker’s Hospital Review | January 24, 2022
Almost 13 percent — or 772 of 6,004 — of hospitals reporting staffing levels in the U.S. are experiencing critical staffing shortages, according to HHS data posted Jan. 23.
This is about 2 percentage points less than figures released Jan. 20.
A critical staffing shortage is based on a facility’s needs and internal policies for staffing ratios, according to HHS. Hospitals using temporary staff to meet staffing ratios are not counted among those experiencing a shortage.
Meanwhile, almost 22 percent — or 1,305 of 6,004 — of hospitals reporting staffing levels in the U.S. are anticipating shortages in the next week.
About 30 percent of hospitals did not report if they’re currently experiencing shortages, and about 21 percent did not report if they anticipate shortages.
Below are two lists showing current staffing shortages and anticipated shortages.
Percent of hospitals in each state and the District of Columbia experiencing critical staffing shortages, ranked in descending order:
1. Vermont: 58.82 percent
2. West Virginia: 47.62 percent
3. New Mexico: 47.27 percent
4. Wisconsin: 33.33 percent
5. North Dakota: 32.65 percent
6. Arizona: 29.52 percent
7. Michigan: 29.38 percent
8. Kentucky: 29.06 percent
9. South Carolina: 28.05 percent
10. Louisiana: 25.33 percent
11. Georgia: 24.71 percent
12. Indiana: 23.95 percent
13. Nebraska: 22.22 percent
14. Tennessee: 22.14 percent
15. Delaware: 20 percent
16. Pennsylvania: 19.03 percent
17. Minnesota: 17.14 percent
18. Montana: 16.92 percent
19. Washington: 16.5 percent
20. Virginia: 15.24 percent
21. Oklahoma: 13.1 percent
22. New Jersey: 12.5 percent
23. Hawaii: 12 percent
24. Missouri: 10.95 percent (tie)
24. Kansas: 10.95 percent (tie)
26. Wyoming: 9.68 percent
27. Oregon: 9.38 percent
28. Maryland: 9.09 percent
29. California: 8.71 percent
30. Colorado: 8.6 percent
31. North Carolina: 7.69 percent
32. Mississippi: 7.41 percent
33. New Hampshire: 6.67 percent (tie)
33. Rhode Island: 6.67 percent (tie)
35. Nevada: 6.56 percent
36. Arkansas: 5.61 percent
37. Maine: 5.41 percent
38. Alaska: 4.17 percent
39. Illinois: 3.96 percent
40. Idaho: 3.77 percent
41. Florida: 3.56 percent
42. Iowa: 3.17 percent
43. New York: 2.48 percent
44. Texas: 2.36 percent
45. Ohio: 0.86 percent
46. Alabama: 0 percent (tie)
46. District of Columbia: 0 percent (tie)
46. South Dakota: 0 percent (tie)
46. Utah: 0 percent (tie)
46. Connecticut: 0 percent (tie)
46. Massachusetts: 0 percent (tie)
Percent of hospitals in each state and the District of Columbia anticipating critical staffing shortages within the next week, ranked in descending order:
1. Vermont: 70.59 percent
2. Rhode Island: 53.33 percent
3. West Virginia: 52.38 percent
4. New Mexico: 47.27 percent
5. Kentucky: 41.03 percent
6. California: 40.3 percent
7. Alabama: 35.9 percent
8. Tennessee: 35.71 percent
9. Wyoming: 35.48 percent
10. Wisconsin: 35.33 percent
11. Michigan: 33.75 percent
12. Delaware: 33.33 percent
13. Missouri: 32.85 percent
14. North Dakota: 32.65 percent
15. Massachusetts: 32.35 percent
16. Nebraska: 32.32 percent
17. Arizona: 30.48 percent
18. Kansas: 29.93 percent
19. South Carolina: 29.27 percent
20. Oklahoma: 28.97 percent
21. Georgia: 28.82 percent
22. Indiana: 27.54 percent
23. Louisiana: 24.44 percent
24. Mississippi: 23.15 percent
25. Arkansas: 22.43 percent
26. Virginia: 21.9 percent
27. Pennsylvania: 21.68 percent
28. Washington: 20.39 percent
29. New Hampshire: 20 percent
30. Montana: 18.46 percent
31. Maryland: 18.18 percent
32. Minnesota: 17.14 percent
33. New Jersey: 16.67 percent (tie)
33. Alaska: 16.67 percent (tie)
35. Florida: 16.6 percent
36. Colorado: 13.98 percent
37. Idaho: 13.21 percent
38. Illinois: 12.87 percent
39. Hawaii: 12 percent
40. Oregon: 10.94 percent
41. North Carolina: 10.77 percent
42. South Dakota: 9.38 percent
43. Maine: 8.11 percent
44. Utah: 7.14 percent
45. Nevada: 6.56 percent
46. New York: 6.44 percent
47. Iowa: 4.76 percent
48. Texas: 3.54 percent
49. Connecticut: 2.56 percent
50. Ohio: 0.86 percent
51. District of Columbia: 0 percent
100s of Published Reports of Post-Vaccine Medical Distress (Part 1)
By Donna Laframboise | No Fracking Consensus | January 17, 2022
COVID-19 vaccines are harming people. This fact is now extensively documented in the peer-reviewed medical literature.
We’re told these events are rare. So what’s the magic number? How many reports of alarming medical outcomes are necessary before we admit the ‘cure’ might be worse than the disease?
Most people who contract COVID don’t develop serious medical issues. But the small percentage who do can overwhelm the health care system.
Most people who receive a COVID vaccine don’t develop serious medical issues. But the small percentage who do can also overwhelm the health care system. Everyone wants to talk about the first problem. No one wants to talk about the second.
Last week, an extensive list of articles from the peer-reviewed medical literature was posted on Reddit by someone known only as xxyiorgos. More than 400 articles are on that list (backup link here).
Here are the first 100. I’ve numbered, and verified them. In some cases, I’ve updated the hyperlink. This research is emerging from numerous countries including Belgium, Canada, Germany, Greece, Italy, Norway, Qatar, South Korea, Spain, the UK, and the US.
Comments in brackets added by me.
1. Cerebral venous thrombosis after COVID-19 vaccination in the UK: a multicentre cohort study [stroke, Lancet, Aug. 2021]
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)01608-1/
2. Vaccine-induced immune thrombotic thrombocytopenia with disseminated intravascular coagulation and death after ChAdOx1 nCoV-19 vaccination: [fatal blood clots, Journal of Stroke and Cerebrovascular Diseases, Sept. 2021]
https://www.strokejournal.org/article/S1052-3057(21)00341-4/fulltext
3. Fatal cerebral hemorrhage after COVID-19 vaccine: [fatal brain bleed, Journal of the Norwegian Medical Association, Apr. 2021]
https://tidsskriftet.no/2021/04/kort-kasuistikk/fatal-hjerneblodning-etter-covid-19-vaksine
4. “Myocarditis after mRNA vaccination against SARS-CoV-2, a case series:” [heart inflammation, American Heart Journal Plus: Cardiology Research & Practice, Aug. 2021]
https://www.sciencedirect.com/science/article/pii/S2666602221000409
5. Three cases of acute venous thromboembolism in women after vaccination against COVID-19: [blood clots, Journal of Vascular Surgery: Venous and Lymphatic Disorders, Jan. 2022]
https://www.jvsvenous.org/article/S2213-333X(21)00392-9/fulltext
6. Acute coronary tree thrombosis after vaccination against COVID-19: [blood clots, Journal of the American College of Cardiology: Cardiovascular Interventions, May 2021]
https://www.sciencedirect.com/science/article/pii/S1936879821003988
7. US case reports of cerebral venous sinus thrombosis with thrombocytopenia after Ad26.COV2.S vaccination, March 2 to April 21, 2020: [stroke, Journal of the American Medical Association, June 2021]
https://jamanetwork.com/journals/jama/fullarticle/2779731
8. Portal vein thrombosis associated with ChAdOx1 nCov-19 vaccine: [blood clots, Lancet, June 2021]
https://www.thelancet.com/journals/langas/article/PIIS2468-1253(21)00197-7/
9. Management of cerebral and splanchnic vein thrombosis associated with thrombocytopenia in subjects previously vaccinated with Vaxzevria (AstraZeneca): position statement of the Italian Society for the Study of Hemostasis and Thrombosis (SISET): [blood clots, Blood Transfusion, July-Aug. 201]
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC8297668/
10. Vaccine-induced immune immune thrombotic thrombocytopenia and cerebral venous sinus thrombosis after vaccination with COVID-19; a systematic review: [blood clots, Journal of the Neurological Sciences, Sept. 2021]
https://www.jns-journal.com/article/S0022-510X(21)00301-4/fulltext
11. Thrombosis with thrombocytopenia syndrome associated with COVID-19 vaccines: [blood clots, American Journal of Emergency Medicine, Nov. 2021]
https://www.sciencedirect.com/science/article/pii/S0735675721004381
12. Covid-19 vaccine-induced thrombosis and thrombocytopenia: a commentary on an important and practical clinical dilemma: [blood clots, Progress in Cardiovascular Diseases, July-Aug. 2021]
https://www.sciencedirect.com/science/article/abs/pii/S0033062021000505
13. Thrombosis with thrombocytopenia syndrome associated with COVID-19 viral vector vaccines: [blood clots, European Journal of Internal Medicine, July 2021]
https://www.sciencedirect.com/science/article/abs/pii/S0953620521001904
14. COVID-19 vaccine-induced immune thrombotic thrombocytopenia: an emerging cause of splanchnic vein thrombosis: [blood clots, Annals of Hepatology, July-Aug. 2021]
https://www.sciencedirect.com/science/article/pii/S1665268121000557
15. The roles of platelets in COVID-19-associated coagulopathy and vaccine-induced immune thrombotic immune thrombocytopenia (covid): [blood clots, Trends in Cardiovascular Medicine, Jan. 2022]
https://www.sciencedirect.com/science/article/pii/S1050173821000967
16. Roots of autoimmunity of thrombotic events after COVID-19 vaccination: [blood clots, Autoimmunity Reviews, Nov. 2021]
https://www.sciencedirect.com/science/article/abs/pii/S1568997221002160
17. Cerebral venous sinus thrombosis after vaccination: the United Kingdom experience: [brain blood clots, [stroke, Lancet, Sept. 2021]
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)01788-8/fulltext
18. Thrombotic immune thrombocytopenia induced by SARS-CoV-2 vaccine: [blood clots, New England Journal of Medicine, Apr. 2021]
https://www.nejm.org/doi/full/10.1056/nejme2106315
19. Myocarditis after immunization with COVID-19 mRNA vaccines in members of the US military: [heart inflammation, Journal of the American Medical Association, June 2021]
https://jamanetwork.com/journals/jamacardiology/fullarticle/2781601
20. Thrombosis and thrombocytopenia after vaccination with ChAdOx1 nCoV-19: [blood clots, New England Journal of Medicine, Apr. 2021]
https://www.nejm.org/doi/full/10.1056/NEJMoa2104882
21. Association of myocarditis with the BNT162b2 messenger RNA COVID-19 vaccine in a case series of children: [heart inflammation, Journal of the American Medical Association Cardiology, Aug. 2021]
https://jamanetwork.com/journals/jamacardiology/fullarticle/2783052
22. Thrombotic thrombocytopenia after vaccination with ChAdOx1 nCov-19: [blood clots, New England Journal of Medicine, June 2021]
https://www.nejm.org/doi/full/10.1056/NEJMoa2104840
23. Post-mortem findings in vaccine-induced thrombotic thrombocytopenia (covid-19): [fatal blood clots, Haematologica, Aug. 2021]
https://haematologica.org/article/view/haematol.2021.279075
24. Thrombocytopenia, including immune thrombocytopenia after receiving COVID-19 mRNA vaccines reported to the Vaccine Adverse Event Reporting System (VAERS): [blood clots, Vaccine, June 2021]
https://www.sciencedirect.com/science/article/pii/S0264410X21005247
25. Acute symptomatic myocarditis in seven adolescents after Pfizer-BioNTech COVID-19 vaccination: [heart inflammation, Pediatrics, Sept. 2021]
https://publications.aap.org/pediatrics/article/148/3/e2021052478/179728/Symptomatic-Acute-Myocarditis-in-7-Adolescents
26. Aphasia seven days after the second dose of an mRNA-based SARS-CoV-2 vaccine. [brain bleed, Brain Hemorrhages, Dec. 2021]
https://www.sciencedirect.com/science/article/pii/S2589238X21000292
27. Comparison of vaccine-induced thrombotic episodes between ChAdOx1 nCoV-19 and Ad26.COV.2.S vaccines: [blood clots, Journal of Autoimmunity, Aug. 2021]
https://www.sciencedirect.com/science/article/abs/pii/S0896841121000895
28. Hypothesis behind the very rare cases of thrombosis with thrombocytopenia syndrome after SARS-CoV-2 vaccination: [blood clots, Thrombosis Research, July 2021]
https://www.sciencedirect.com/science/article/abs/pii/S0049384821003315
29. Blood clots and bleeding episodes after BNT162b2 and ChAdOx1 nCoV-19 vaccination: analysis of European data: [blood clots, Journal of Autoimmunity, Aug. 2021]
https://www.sciencedirect.com/science/article/pii/S0896841121000937
30. Cerebral venous thrombosis after BNT162b2 mRNA SARS-CoV-2 vaccine: [stroke, Journal of Stroke and Cerebrovascular Diseases, Aug. 2021]
https://www.sciencedirect.com/science/article/abs/pii/S1052305721003098
31. Primary adrenal insufficiency associated with thrombotic immune thrombocytopenia induced by the Oxford-AstraZeneca ChAdOx1 nCoV-19 vaccine (VITT): [blood clots, European Journal of Internal Medicine, Sept. 2021]
https://www.sciencedirect.com/science/article/pii/S0953620521002363
32. Myocarditis and pericarditis after vaccination with COVID-19 mRNA: practical considerations for care providers: [heart inflammation, Canadian Journal of Cardiology, Oct. 2021]
https://www.sciencedirect.com/science/article/pii/S0828282X21006243
33. “Portal vein thrombosis occurring after the first dose of SARS-CoV-2 mRNA vaccine in a patient with antiphospholipid syndrome”: [blood clots, Thrombosis Update, Dec. 2021]
https://www.sciencedirect.com/science/article/pii/S2666572721000389
34. Early results of bivalirudin treatment for thrombotic thrombocytopenia and cerebral venous sinus thrombosis after vaccination with Ad26.COV2.S: [blood clots, Annals of Emergency Medicine, Oct. 2021]
https://www.sciencedirect.com/science/article/pii/S0196064421003425
35. Myocarditis, pericarditis and cardiomyopathy after COVID-19 vaccination: [heart inflammation, Heart, Lung and Circulation, Oct. 2021]
https://www.sciencedirect.com/science/article/pii/S1443950621011562
36. Mechanisms of immunothrombosis in vaccine-induced thrombotic thrombocytopenia (VITT) compared to natural SARS-CoV-2 infection: [blood clots, Journal of Autoimmunity, July 2021]
https://www.sciencedirect.com/science/article/abs/pii/S0896841121000706
37. Prothrombotic immune thrombocytopenia after COVID-19 vaccination: [blood clots, Blood, July 2021]
https://www.sciencedirect.com/science/article/pii/S0006497121009411
38. Vaccine-induced thrombotic thrombocytopenia: the dark chapter of a success story: [blood clots, Metabolism Open, Sept. 2021]
https://www.sciencedirect.com/science/article/pii/S2589936821000256
39. Anti-PF4 antibody negative cerebral venous sinus thrombosis without thrombocytopenia following immunization with COVID-19 vaccine in an elderly non-comorbid Indian male, managed with conventional heparin-warfarin based anticoagulation: [stroke, Diabetes & Metabolic Syndrome: Clinical Research & Reviews, July-Aug. 2021]
https://www.sciencedirect.com/science/article/pii/S1871402121002046
40. Thrombosis after COVID-19 vaccination: possible link to ACE pathways: [blood clots, Thrombosis Research, Oct. 2021]
https://www.sciencedirect.com/science/article/pii/S0049384821004369
41. Cerebral venous sinus thrombosis in the U.S. population after SARS-CoV-2 vaccination with adenovirus and after COVID-19: [stroke, Journal of the American College of Cardiology, July 2021]
https://www.sciencedirect.com/science/article/pii/S0735109721051949
42. Middle-age Asian male with cerebral venous thrombosis after COVID-19 AstraZeneca vaccination: [stroke, American Journal of Emergency Medicine, Jan. 2022]
https://www.sciencedirect.com/science/article/pii/S0735675721005714
43. Cerebral venous sinus thrombosis and thrombocytopenia after COVID-19 vaccination: report of two cases in the United Kingdom: [stroke, Brain, Behavior, and Immunity, July 2021]
https://www.sciencedirect.com/science/article/abs/pii/S088915912100163X
44. Immune thrombocytopenic purpura after vaccination with COVID-19 vaccine (ChAdOx1 nCov-19): [blood clots, Blood, Sept. 2021]
https://www.sciencedirect.com/science/article/abs/pii/S0006497121013963
45. Antiphospholipid antibodies and risk of thrombophilia after COVID-19 vaccination: the straw that breaks the camel’s back?: [blood clots, Cytokine & Growth Factor Reviews, Aug. 2021]
https://www.sciencedirect.com/science/article/pii/S1359610121000423
46. Vaccine-induced thrombotic thrombocytopenia, a rare but severe case of friendly fire in the battle against the COVID-19 pandemic: What pathogenesis? [blood clots, European Journal of Internal Medicine, Sept. 2021]
https://www.sciencedirect.com/science/article/pii/S0953620521002314
47. Diagnostic-therapeutic recommendations of the ad-hoc FACME expert working group on the management of cerebral venous thrombosis related to COVID-19 vaccination: [stroke, Neurología, Spanish Neurology Society, July-Aug. 2021]
https://www.sciencedirect.com/science/article/pii/S2173580821000754
48. Thrombocytopenia and intracranial venous sinus thrombosis after exposure to the “AstraZeneca COVID-19 vaccine Astrazeneca” exposure: [stroke, Journal of Clinical Medicine, Apr. 2021]
https://www.mdpi.com/2077-0383/10/8/1599/htm
49. Thrombocytopenia following Pfizer and Moderna SARS-CoV-2 vaccination: [blood clots, American Journal of Hematology, Feb. 2021]
https://onlinelibrary.wiley.com/doi/10.1002/ajh.26132
50. Severe and refractory immune thrombocytopenia occurring after SARS-CoV-2 vaccination: [blood clots, Journal of Blood Medicine, Feb. 2021]
https://www.dovepress.com/severe-refractory-immune-thrombocytopenia-occurring-after-sars-cov-2-v-peer-reviewed-fulltext-article-JBM
51. Purpuric rash and thrombocytopenia after mRNA-1273 (Modern) COVID-19 vaccine: [blood clots, Cureus, Mar. 2021]
https://www.cureus.com/articles/54984-purpuric-rash-and-thrombocytopenia-after-the-mrna-1273-moderna-covid-19-vaccine
52. COVID-19 vaccination: information on the occurrence of arterial and venous thrombosis using data from VigiBase: [stroke, European Respiratory Journal, July 2021]
https://erj.ersjournals.com/content/58/1/2100956
53. Cerebral venous thrombosis associated with the covid-19 vaccine in Germany: [stroke, Annals of Neurology, July 2021]
https://onlinelibrary.wiley.com/doi/10.1002/ana.26172
54. Cerebral venous thrombosis following BNT162b2 mRNA vaccination of BNT162b2 against SARS-CoV-2: a black swan event: [stroke, American Journal of Hematology, June 2021]
https://onlinelibrary.wiley.com/doi/10.1002/ajh.26272
55. The importance of recognizing cerebral venous thrombosis following anti-COVID-19 vaccination: [stroke, European Journal of Internal Medicine, May 2021]
https://pubmed.ncbi.nlm.nih.gov/34001390/
56. Thrombosis with thrombocytopenia after messenger RNA vaccine -1273: [blood clots, Annals of Internal Medicine, Oct. 2021]
https://www.acpjournals.org/doi/10.7326/L21-0244
57. Blood clots and bleeding after BNT162b2 and ChAdOx1 nCoV-19 vaccination: an analysis of European data: [blood clots, Journal of Autoimmunity, Aug. 2021]
https://www.sciencedirect.com/science/article/pii/S0896841121000937
58. First dose of ChAdOx1 and BNT162b2 COVID-19 vaccines and thrombocytopenic, thromboembolic, and hemorrhagic events in Scotland: [blood clots, Nature Medicine, June 2021]
https://www.nature.com/articles/s41591-021-01408-4
59. Exacerbation of immune thrombocytopenia after COVID-19 vaccination: [blood clots, British Journal of Haematology, June 2021]
https://onlinelibrary.wiley.com/doi/10.1111/bjh.17645
60. First report of a de novo iTTP episode associated with a COVID-19 mRNA-based anti-COVID-19 vaccine: [blood clots, Journal of Thrombosis and Haemostasis, June 2021]
https://onlinelibrary.wiley.com/doi/10.1111/jth.15418
61. PF4 immunoassays in vaccine-induced thrombotic thrombocytopenia: [blood clots, New England Journal of Medicine, July 2021]
https://www.nejm.org/doi/full/10.1056/NEJMc2106383
62. Antibody epitopes in vaccine-induced immune immune thrombotic thrombocytopenia: [blood clots, Nature, July 2021]
https://www.nature.com/articles/s41586-021-03744-4
63. Myocarditis with COVID-19 mRNA vaccines: [heart inflammation, Circulation, July 2021]
https://www.ahajournals.org/doi/full/10.1161/CIRCULATIONAHA.121.056135
64. Myocarditis and pericarditis after COVID-19 vaccination: [heart inflammation, Journal of the American Medical Association, Aug. 2021]
https://jamanetwork.com/journals/jama/fullarticle/2782900
65. Myocarditis temporally associated with COVID-19 vaccination: [heart inflammation, Circulation, June 2021]
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.121.055891
66. COVID-19 Vaccination Associated with Myocarditis in Adolescents: [heart inflammation, Pediatrics, Nov. 2021]
https://publications.aap.org/pediatrics/article/148/5/e2021053427/181357/COVID-19-Vaccination-Associated-Myocarditis-in
67. Acute myocarditis after administration of BNT162b2 vaccine against COVID-19: [heart inflammation, Revista Española de Cardiología, Spanish Society of Cardiology, Sept. 2021]
https://www.sciencedirect.com/science/article/pii/S188558572100133X
68. Temporal association between COVID-19 vaccine Ad26.COV2.S and acute myocarditis: case report and review of the literature: [heart inflammation, Cardiovascular Revascularization Medicine, Aug. 2021]
https://www.sciencedirect.com/science/article/pii/S1553838921005789
69. COVID-19 vaccine-induced myocarditis: a case report with review of the literature: [heart inflammation, Diabetes & Metabolic Syndrome: Clinical Research & Reviews, Sept.-Oct. 2021]
https://www.sciencedirect.com/science/article/pii/S1871402121002253
70. Potential association between COVID-19 vaccine and myocarditis: clinical and CMR findings: [heart inflammation, Journal of the American College of Cardiology: Cardiovascular Imaging, Sept. 2021]
https://www.sciencedirect.com/science/article/pii/S1936878X2100485X
71. Recurrence of acute myocarditis temporally associated with receipt of coronavirus mRNA disease vaccine 2019 (COVID-19) in a male adolescent: [heart inflammation, Journal of Pediatrics, Nov. 2021]
https://www.sciencedirect.com/science/article/pii/S002234762100617X
72. Fulminant myocarditis and systemic hyper inflammation temporally associated with BNT162b2 COVID-19 mRNA vaccination in two patients: [heart inflammation, International Journal of Cardiology, Oct. 2021]
https://www.sciencedirect.com/science/article/pii/S0167527321012286
73. Acute myocarditis after administration of BNT162b2 vaccine: [heart inflammation, Infectious Disease Cases, 2021]
https://www.sciencedirect.com/science/article/pii/S2214250921001530
74. Lymphohistocytic myocarditis after vaccination with COVID-19 Ad26.COV2.S viral vector: [heart inflammation, International Journal of Cardiology: Heart & Vasculature, Oct. 2021]
https://www.sciencedirect.com/science/article/pii/S2352906721001573
75. Myocarditis following vaccination with BNT162b2 in a healthy male: [heart inflammation, American Journal of Emergency Medicine, Dec. 2021]
https://www.sciencedirect.com/science/article/pii/S0735675721005362
76. Acute myocarditis after Comirnaty (Pfizer) vaccination in a healthy male with previous SARS-CoV-2 infection: [heart inflammation, Radiology Case Reports, Nov. 2021]
https://www.sciencedirect.com/science/article/pii/S1930043321005549
77. Myopericarditis after Pfizer mRNA COVID-19 vaccination in adolescents: [heart inflammation, Journal of Pediatrics, Nov. 2021]
https://www.sciencedirect.com/science/article/pii/S002234762100665X
78. Pericarditis after administration of BNT162b2 mRNA COVID-19 mRNA vaccine: [heart inflammation, Revista Española de Cardiología, Spanish Society of Cardiology, Dec. 2021]
https://www.sciencedirect.com/science/article/pii/S1885585721002218
79. Acute myocarditis after vaccination with SARS-CoV-2 mRNA-1273 mRNA: [heart inflammation, Canadian Journal of Cardiology: Open, Nov. 2021]
https://www.sciencedirect.com/science/article/pii/S2589790X21001931
80. Temporal relationship between the second dose of BNT162b2 mRNA Covid-19 vaccine and cardiac involvement in a patient with previous SARS-COV-2 infection: [heart problems, International Journal of Cardiology: Heart & Vasculature, June 2021]
https://www.sciencedirect.com/science/article/pii/S2352906721000622
81. Myopericarditis after vaccination with COVID-19 mRNA in adolescents 12 to 18 years of age: [heart inflammation, Journal of Pediatrics, Nov. 2021]
https://www.sciencedirect.com/science/article/pii/S0022347621007368
82. Acute myocarditis after SARS-CoV-2 vaccination in a 24-year-old man: [heart inflammation, Portuguese Journal of Cardiology, July 2021]
https://www.sciencedirect.com/science/article/pii/S0870255121003243
83. Important information on myopericarditis after vaccination with Pfizer COVID-19 mRNA in adolescents: [heart inflammation, Journal of Pediatrics, Nov. 2021]
https://www.jpeds.com/article/S0022-3476(21)00749-6/fulltext
84. A series of patients with myocarditis after vaccination against SARS-CoV-2 with mRNA-1279 and BNT162b2: [heart inflammation, Journal of the American College of Cardiology: Cardiovascular Imaging, Sept. 2021]
https://www.sciencedirect.com/science/article/pii/S1936878X21004861
85. Takotsubo cardiomyopathy after vaccination with mRNA COVID-19: [heart problems, Heart, Lung and Circulation, Dec. 2021]
https://www.sciencedirect.com/science/article/pii/S1443950621011331
86. COVID-19 mRNA vaccination and myocarditis: [heart inflammation, European Journal of Case Reports in Internal Medicine, June 2021]
https://www.ejcrim.com/index.php/EJCRIM/article/view/2681/2723
87. COVID-19 vaccine and myocarditis: [heart inflammation, American Journal of Cardiology, July 2021]
https://www.ajconline.org/article/S0002-9149(21)00639-1/fulltext
88. Allergic reactions after COVID-19 vaccination: putting the risk in perspective: [allergic reactions, JAMA Network Open, Aug. 2021]
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2783633
89. Anaphylactic reactions to COVID-19 mRNA vaccines: a call for further studies: [allergic reactions, Vaccine, May 2021]
https://www.sciencedirect.com/science/article/pii/S0264410X21003777
90. Risk of severe allergic reactions to COVID-19 vaccines among patients with allergic skin disease: practical recommendations. An ETFAD position statement with external experts: [allergic reactions, Journal of the European Academy of Dermatology and Venereology, June 2021]
https://onlinelibrary.wiley.com/doi/10.1111/jdv.17237
91. COVID-19 vaccine and death: causality algorithm according to the WHO eligibility diagnosis: [fatal blood clots, Diagnostics, May 2021]
https://www.mdpi.com/2075-4418/11/6/955
92. Fatal brain hemorrhage after COVID-19 vaccine: [fatal brain bleed, Journal of the Norwegian Medical Association, April 2021]
https://tidsskriftet.no/en/2021/04/kort-kasuistikk/fatal-cerebral-haemorrhage-after-covid-19-vaccine
93. A case series of skin reactions to COVID-19 vaccine in the Department of Dermatology at Loma Linda University: [skin problems, Journal of the American Academy of Dermatology: Case Reports, Aug. 2021]
https://www.jaadcasereports.org/article/S2352-5126(21)00540-3/fulltext
94. Skin reactions reported after Moderna and Pfizer’s COVID-19 vaccination: a study based on a registry of 414 cases: [skin problems, Journal of the American Academy of Dermatology, Apr. 2021]
https://www.jaad.org/article/S0190-9622(21)00658-7/fulltext
95. Clinical and pathologic correlates of skin reactions to COVID-19 vaccine, including V-REPP: a registry-based study: [skin problems, Journal of the American Academy of Dermatology, Sept. 2021]
https://www.jaad.org/article/S0190-9622(21)02442-7/fulltext
96. Skin reactions after vaccination against SARS-COV-2: a nationwide Spanish cross-sectional study of 405 cases: [skin problems, British Journal of Dermatology, July 2021]
https://onlinelibrary.wiley.com/doi/10.1111/bjd.20639
97. Varicella zoster virus and herpes simplex virus reactivation after vaccination with COVID-19: review of 40 cases in an international dermatologic registry: [herpes, Journal of the European Academy of Dermatology and Venereology, Sept. 2021]
https://onlinelibrary.wiley.com/doi/10.1111/jdv.17646
98. Immune thrombosis and thrombocytopenia (VITT) associated with the COVID-19 vaccine: diagnostic and therapeutic recommendations for a new syndrome: [blood clots, European Journal of Haematology, May 2021]
https://onlinelibrary.wiley.com/doi/10.1111/ejh.13665
99. Laboratory testing for suspicion of COVID-19 vaccine-induced thrombotic (immune) thrombocytopenia: [blood clots, International Journal of Laboratory Hematology, June 2021]
https://onlinelibrary.wiley.com/doi/10.1111/ijlh.13629
100. Intracerebral hemorrhage due to thrombosis with thrombocytopenia syndrome after COVID-19 vaccination: the first fatal case in Korea: [brain bleed, Journal of Korean Medical Science, Aug. 2021]
https://jkms.org/DOIx.php?id=10.3346/jkms.2021.36.e223
Maori Science Beats Woke Myths

By Jennifer Marohasay | January 21, 2022
Every community has those who are designated wise — sometimes able to anticipate imminent catastrophe. For example, back in the 1500s, some in rural England and France would suspend dead birds — specifically kingfishers — from silken threads that purportedly acted as natural weathercocks. It was thought that the dead kingfisher was able to anticipate approaching storms and turn its breast into the wind. This is an unfortunate example, though, because Thomas Browne showed it to be nonsense. He suspended two dead kingfishers, side by side, and they pointed in different directions, thus demolishing the myth. I can’t imagine that all the wise ones took their dead birds down immediately, but Browne’s book Pseudodoxia Epidemica of 1646 championed a new kind of evidence-based science that relied on simple experiment.
For a period of some few hundred years, science came to replace superstition and key zoological texts including, for example, Origin of Species by Charles Darwin, were penned by the curious who tried hard to sort fact from fiction through observation. Browne and Darwin’s works followed Nicolaus Copernicus’ book On the Revolution of the Heavenly Spheres, published in 1543, that explained humankind was not at the centre of the universe.
Before evidence-based science, natural historians and even astronomers, relied on the work of Aristotle who thought mankind was at the centre of the universe. In the twelfth century, Aristotle was a major source of information for the medieval encyclopaedias of animals, known as Bestiaries, with moral biblical lessons added.
We have somehow returned to this practice where natural history is once again interwoven with moralising. Worse, many of those designated as wise are full of hubris and carry on as though humankind can affect the weather and climate. This extends to projects at universities, where, even in zoology departments the ‘research’ must lament the trace gas carbon dioxide and its perceived impact on the distribution and abundance of species.
Even in The Spectator Australia, James Allan in ‘Decline and Fall of New Zealand’ (11 December) remonstrates about how woke our universities have become but then lauds the superiority of Western science relative to Maori mythology. But is woke science superior to Maori myths? Arguably the most significant climate event since satellites began measuring global temperatures in 1979, was the very strong El Niño of 2015/16. It caused global temperatures to spike in February 2016, corals to bleach, and so on. This hottest period – according to the UAH satellite record – was forecast some years earlier by long range weather forecaster Ken Ring relying on Maori mythology. It was not forecast by Western meteorological bureaus that run simulation models on super computers.
In 1974, Ring, then a high school mathematics teacher ‘dropped out’ to home school his children. He moved his family to the remote East Coast of the North Island of New Zealand and over a period of six years befriended local Maori fishermen. He returned to ‘civilization’ six years later with what he has described as ‘the rudiments of a weather prediction system’ based on traditional Maori knowledge. Sometime later he began publishing weather almanacs for Australia, New Zealand and Ireland with rain, frost and snow maps including fishing calendars and gardening guides.
I’ve no doubt that the forecasts in those almanacs could be vastly improved, including through the mining of historical weather data using artificial neural networks, a form of machine learning that uses artificial intelligence. John Abbot and I showed its application to monthly rainfall forecasting in a series of research papers published from 2012 to 2017, including in the Chinese Academy of Sciences’ Advances in Atmospheric Sciences (Abbot J. & Marohasy J., 2012. Vol. 29, No. 4, Pgs. 717-730).
What has made Ken Ring’s long-range forecasts often more accurate than those from our bureaus of meteorology is their reliance on lunar cycles, uncorrupted by simulation modelling that misguidedly insists atmospheric concentrations of carbon dioxide are relevant to weather and climate forecasting.
It is possible to forecast El Niño and other key weather events years in advance because the passage of the Moon overhead is regular and cyclical. A 2019 technical paper by Jialin Lin and Taotao Qian entitled ‘Switch Between El Niño and La Niña is Caused by Subsurface Ocean Waves Likely Driven by Lunar Tidal Forcing’ explains the underlying physical mechanisms in terms of Newtonian physics.
In fact, observations of the Moon’s changing trajectory were a main test of the theories detailed in Isaac Newton’s The Principia, published in 1687 and recognised as a highlight of the Scientific Revolution in the 17th century.
If we open our eyes to the evidence – as Thomas Browne implored a few hundred years ago – we would notice that the very hot year globally of 2016 immediately followed a year of minimum lunar declination, as did the super El Niño exactly 18 years earlier, in 1998, that also caused mass coral bleaching. It is now well understood, beyond Maori mythology, that there is an 18.6-year lunar declination cycle. But this is wilfully ignored by mainstream meteorologists lest such extra-terrestrial influences on weather and climate detract from the moralising about humankind’s influence.
More than ever, Westerners who claim to respect science —could benefit from a return to simple observation as practiced by Maori fishermen who see the weather patterns created by the passage of the Moon and its changing declination. Browne’s contemporary, John Ray wrote, ‘Let us not suffice to be book-learned, to read what others have written and to take on trust more falsehood than truth, but let us ourselves examine things as we have the opportunity, and converse with Nature as well as with books …’
In meteorological bureaus, simulation modelling has replaced observation and Heads of state are urged to sign international treaties absurdly pledging to stop climate change. The true nature of this woke western climate forecasting would be better appreciated if it was evaluated against other methods. Forecasts from different systems could be placed next to each other, in much the same way that Thomas Browne strung up dead kingfishers – side by side.
This article was first published in The Spectator Australia magazine.

Since the article was published, I’ve received a note from Ken Ring with the following comment:
I’ve since learned that the Tuhoe fishermen of the East Coast were descended from Celtic peoples. They weren’t Maori at all, but originally pale skinned and red hair. There’s a whole political argument going on re-Treaty funds. Money seems to guide and hide our true prehistory …
Truth is, the Maori Fishing Calendar (which I published each year in the 2000s) was exactly the same as the Canadian Rockies Hunting Calendar, and Hindu writings, and harkened back to a time when the lunar laws were universal knowledge …
There are remnants of stone circles in New Zealand, but they are almost certainly pre- Maori.
I agree with the school of thought that says Aborigines were in New Zealand 40,000 years ago, based on rock drawings, and were only one of 100 or so cultures living peacefully side by side. At our closest point, we are only 900 nautical miles from Australia, and it is daft to think that for 60,000 years we were unknown to them. The ancient Chinese, too, settled on the east coast of Australia, and established a greenstone industry in New Zealand, but all this is completely shunned by historians. It means that indeed there may have been towns of 1000 people in Australia, but they were probably Asian, not Aboriginal.
You may be interested in this documentary, Skeletons in the Cupboard part 1 and Skeletons in our Cupboard part 2
I would like to thank Barry Goldman for the link to the article by Ben Finney et al. entitled ‘Wait for the West Wind’ that explains something of the complexity of navigating the South Pacific and the importance of understanding wind direction and its seasonality. It concludes with comment that:
Without the ability to sail over long distances, to find islands strewn over many thousands of miles of open sea, and to carry enough people, tools, plants and animals to found viable colonies on the islands discovered, there would have been no Polynesian culture, no vast triangular section of ocean occupied by closely related neolithic peoples. That the large, stable, and seaworthy double-canoe was the critical artefact of this cultural development and expansion is generally accepted, just as the ability to make one’s way across the ocean and find distant islands by reading the stars, the winds, the swells, the flight of birds, and other clues provided by nature is often cited as the skill most crucial to this process. To the double-canoes, and ways of navigating them without instruments, we would add a third main element of this oceanic adaptation that made the colonisation of so many far-flung islands possible: knowledge of the winds of the sea and the skill to exploit spells of westerly winds to sail far to the east.
While the more intermittent character of the westerlies in the tropical south-eastern Pacific may have slowed the momentum of eastward expansion across the Pacific, the ethnographic and experimental evidence suggests that early Polynesian voyagers were able to adapt to this wind regime and to use periodic episodes of westerly winds to find and settle all the oceanic islands to the east of their mid-Pacific homeland. The evidence further suggests that they would have been able to make the multiple landfalls throughout central East Polynesia, and that, once settled on the various islands and archipelagos, they and their descendants would have been capable of exploiting the alternating rhythm of monsoonal and subtropical westerlies with easterly trade winds to maintain some communication ties within the central East Polynesia region, and also to some extent between East and West Polynesia. The actual history of East Polynesia colonisation may, therefore, turn out to be much more complex than suggested by broad arrows commonly drawn on maps to indicate migration paths.
Instead of searching for a single island or archipelago as the sole site of first settlement in East Polynesia, and of assuming one-way population dispersal from there to all the other eastern archipelagos, perhaps we should think of early East Polynesian colonisation in terms of a large multi-archipelago, intercommunicating region with some two-way links back and forth between there and West Polynesia. Although the camp-sites and settlements made by the first people to reach the islands of East Polynesia may be sparse and difficult to find, and evidence of interisland communication even harder to discern, the archaeologists should keep looking for evidence of early colonies and their interrelations throughout the islands and archipelagos lying to the east of the Polynesian homeland.
The feature image was taken at dawn at Lake Wanaka under the Milky Way and a rising Full Moon.
The Political Economy of Autism
By Toby Rogers | September 14, 2021
Autism is an epidemic and a pandemic by any reasonable definition of those words. J.B. Handley in, How to End the Autism Epidemic, produced the best chart showing the growth in autism prevalence in the U.S. over the last 50 years:
Increase in Autism Prevalence in the U.S. 1970 to 2017
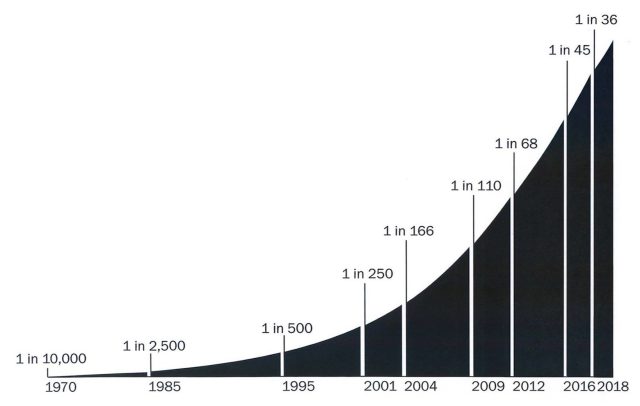
Source: Handley (2018).
Darold Treffert at Winnebago State Hospital in Wisconsin was one of the first people to attempt to measure autism in the general population. His study, published in Archives of General Psychiatry in 1970, showed an autism rate of less than 1 in 10,000 children.
Then, sometime around 1987, the autism rate in the United States began to skyrocket. By 2017, the autism rate in the U.S. was 1 in 36 kids (Zablotsky et al., 2017). So the U.S. has experienced a 277-fold increase in autism prevalence in the last 50 years.
In some places and populations the rates are even higher: in Tom’s River, NJ, the state’s largest suburban school district, 1 in 14 eight-year-olds is on the autism spectrum; in Newark, NJ, 1 in 10 Black boys is on the spectrum (forthcoming).
The United States is in the midst of a genocide.
Genetic theories of autism never made much sense because “there is no such thing as a genetic epidemic” — the human genome just does not change that fast. An early twin study by Susan Folstein and Michael Rutter at the Institute of Psychiatry in London in 1977 suggested a strong genetic component to autism. More recent scholarship shows that this was likely overstated; the study only had 21 twin pairs and did not effectively control for environmental factors (twins usually grow up in the same family and are thus likely exposed to the same toxicants).
As the autism rate exploded throughout the U.S., the state of California hired eleven of the best geneticists in the country to examine the role of genes in autism. They concluded that genetics explains at most 38% of autism cases and in two places they explained that this was likely an overestimate (Hallmayer et al., 2011). Whatever is driving the surge in autism prevalence, it is not primarily genetics.
Well perhaps the increase in autism prevalence is just the result of better awareness (and what’s called “diagnostic expansion and substitution”)? That theory of the case does not check out either. The state of California funded two multimillion dollar studies to examine sharply rising prevalence in the state and whether it was the result of social factors. The first study was led by pediatric epidemiologist Robert S. Byrd at UC Davis who directed a team of investigators at UC Davis and UCLA. The investigators concluded that, “The observed increase in autism cases cannot be explained by a loosening in the criteria used to make the diagnosis” and “children served by the State’s Regional Centers are largely native born and there has been no major migration of children into California that would explain the increase in autism” (Byrd et al., 2002).
The state of California revisited this question in 2009 with a study led by the top environmental epidemiologist in the state — Irva Hertz-Picciotto at the UC Davis Mind Institute. This study concluded that changes in diagnostic criteria, the inclusion of milder cases, and earlier age at diagnosis explain about a quarter to a third of the total increase in autism (Hertz-Picciotto & Delwiche, 2009). In a subsequent interview with Scientific American, Hertz-Picciotto explained that these three factors “don’t get us close” to explaining the sharp rise in autism over that time period and she urged the scientific community to take a closer look at environmental factors (Cone, 2009).
There are now seven good ‘societal cost of autism’ studies (Jarbrink and Knapp, 2001; Ganz, 2007; Knapp et al., 2009; Buescher et al., 2014; Leigh & Du, 2015; Cakir et al., 2020; Blaxill, Rogers, & Nevison, 2021). They all show that the U.S. and much of the developed world is heading for economic and social collapse as a result of surging autism costs.
Autism increases poverty and inequality. Lifetime care costs for autism range from $1.4 to $2.4 million. Mothers of kids with autism earn 35% less than mothers of kids with other health limitations and 56% less than mothers of kids with no health limitations (Buescher et al., 2014).
In 2015, autism cost the U.S. an estimated $268 billion a year in direct costs & lost productivity; given current rates of increase, autism costs will reach $1 trillion a year (3.6% of GDP) by 2025 (Leigh & Du, 2015). As a point of comparison, the U.S. Defense Department budget is “just” 3.1% of GDP.
All of the more recent studies show autism costs surpassing $1 trillion a year in the near future. There is no plan by any level of government to raise revenue to meet these costs or prevent autism to mitigate these costs. Elected officials are frozen like a deer in the headlights.
In the last decade, three groups of top epidemiologists have published consensus statements declaring that neurodevelopmental disabilities including autism are caused by toxicants in the environment (The Collaborative on Health and the Environment, 2008; Mount Sinai Hospital, 2010; Project TENDR, 2016).
This is good news because it means that autism is likely preventable. The bad news is that the leading mainstream toxicologists do not want to lose their jobs so they generally avoid mentioning pharmaceutical products (even though these products appear to have an outsized impact). Parents groups have made up for the cowardice of mainstream toxicology by funding their own research.
We have fairly good data that five classes of toxicants increase autism risk:
- Mercury from coal fired power plants and diesel trucks;
- Plastics;
- Pesticides & herbicides;
- EMF/RFR; and
- Pharmaceuticals (Tylenol, SSRIs, & vaccines).
Taking each toxicant in turn…
For every 1,000 pounds of environmentally released mercury, there was a 61% increase in the rate of autism (Palmer, 2006). For every 10 miles closer a family lives to a coal fired power plant the autism risk increases by 1.4% (Palmer, 2009).
Plastics: Children with autism had significantly increased levels of 3 endocrine disruptors (two phthalates — MEHP & DEHP, & BPA) in blood samples as compared with healthy controls (Kardas, 2016).
Pesticides & herbicides: Increased use of RoundUp is strongly correlated (r = 0.989) with the rising prevalence of autism (Swanson, 2014). Organophosphates increase autism risk 60 – 100%; chlorpyrifos increase risk 78% – 163%; pyrethroids increase risk 78% (Shelton et al., 2014).
9 studies show an association between acetaminophen (Tylenol) use & adverse neurodevelopmental outcomes (Bauer et al., 2018). Avella-Garcia (2016) & Liew et al. (2016) found that males exposed to Tylenol in utero have significantly elevated risk of autism.
8 studies show a statistically significant association between selective serotonin reuptake inhibitor (SSRI) use in pregnant women and subsequent autism in their children (see meta-analysis in Kaplan et al., 2016). Doctors who prescribe SSRIs to pregnant women are committing malpractice.
Unfortunately, in the debate over toxicants that increase autism risk, all roads lead back to vaccines. At least 5 studies show a statistically significant association between vaccines & autism (Gallagher & Goodman, 2008 & 2010; Thomas & Margulis, 2016; Mawson et al., 2017a & 2017b).
Dr. Paul Thomas is the most successful doctor in the world at preventing autism. Data from his practice show:
If zero vaccines, autism rate = 1 in 715;
If alternative vaccine schedule, autism rate = 1 in 440;
If CDC vaccine schedule, autism rate = 1 in 36.
That study had large sample size (3,344 children), access to medical files, and good researchers working on it. But look closely. His alternative vaccine schedule reduces autism risk by more than 1200%. However even an alternative vaccine schedule increases autism risk by 160% versus no vaccines at all.
And all of those other toxicants that I described above that have been shown to increase autism risk? Those are the 1 in the 715 cases when the parent does not vaccinate at all. Autism appears mostly be a story of iatrogenic injury from vaccines.
This is not a surprise. Thousands of parents have been telling us for years that their children regressed into autism following vaccinations. Ethylmercury is a known neurotoxin and is still in 7 different vaccines (Thomas & Margulis, 2016, p. 14).
Aluminum is a known neurotoxin (Grandjean & Landrigan, 2014) and is used in a majority of vaccines. “The dose makes the poison” paradigm has collapsed in recent years and now we know that many toxicants have no safe dose.
In a sane world, all of this would be seen as good news. In a sane world the CDC, EPA, NIH and every major newspaper would rush out to Portland, Oregon to examine whether the data from Dr. Paul’s practice (and other studies) are correct. But we live in an insane world…
To date, the CDC, EPA, NIH, the federal government, and all state governments have ignored Dr. Paul’s work. None of the top 10 major newspapers in the U.S. have reviewed his book, The Vaccine Friendly, plan even though it is a bestseller on Amazon. In fact the Oregon Medical Board was so incensed by Dr. Paul’s success in preventing autism that they pulled his medical license briefly in 2021 (he has since been reinstated).
All of this information is public and available to anyone with an internet connection and a library card. By 1999 it was clear that vaccines that contained mercury were a problem (see Kirby, 2005). By the early 2000s it was clear that the problems with vaccines went well beyond mercury. Government had a choice to make: come clean or double down. And starting with senior scientist Thomas Verstraeten and then William Thompson the CDC decided to just flat out lie, manipulate findings, and destroy data.
The pharmaceutical industry also had a choice to make: improve their products or utilize their extensive capture of media and government to protect their existing toxic products. As everyone now knows, they chose to protect their existing toxic products. But the pharmaceutical industry has an enormous problem on their hands. We know some vaccines (hepatitis B, HPV, flu, DTaP…) cause catastrophic harms. And pockets of unvaccinated people across the country — who are healthier than vaccinated children — are the control group that provides evidence of Pharma’s crimes.
So starting in 2015, with the introduction of SB277 in California, the pharmaceutical industry began a systematic effort to eliminate the unvaccinated control group in all 50 states. They start by removing religious or personal belief exemptions to vaccination. In subsequent years they introduce bills to eliminate all medical exemptions to vaccination (SB 277 in CA in 2019) to get to 100% vaccination rates (even though all scientists will tell you that there are some children who should not be vaccinated because of underlying health conditions). In the Pharma legislative blitzkrieg no one is spared so that there will be no evidence left of the harms from these products. If 100% of children are treated, then there is no background rate of illness and all vaccine injuries just appear “normal”.
These mandatory vaccine bills are racketeering and crimes against humanity. With the introduction of coronavirus vaccines in late 2020, the situation has gotten much worse. Pharma now aims to vaccinate 100% of adults as well as 100% of kids and the results thus far have been catastrophic.
So here’s where things stand. The vaccine paradigm has collapsed (and no, mRNA, DNA, and adenovirus vector vaccines are not going to save it). Pharma has piles of cash and extensive capture of the media, academia, and government. So they have the ability to do just about whatever they want. Fearing prosecution and seeking immense profits, Pharma has abandoned any pretense of science, consent, or health and pushed all in to set up a totalitarian state that will serve their interests.
But Pharma has harmed so many people — first with the childhood schedule and now with coronavirus vaccines — that there are now millions of people who have seen vaccine injury first-hand and are now fighting back with everything they’ve got. Variously referred to as the medical freedom movement, the health choice movement, and/or the personal sovereignty movement, these brave citizens are taking on the most powerful industry in the world and fighting to save our country from Pharma fascism. The fighting is so fierce because the stakes are enormous. We are fighting to preserve human life as we know it from the most predatory and corrupt industry in the world.
To learn more about the toxicants associated with autism, read The Political Economy of Autism. To learn more about the battle to save our country and the world from Pharma totalitarianism, please subscribe to my Substack.
Guardian: ANTI-VAXXERS ARE JOINING RACIST MILITIAS
OffGuardian | January 23, 2022
This Week in the New Normal is our weekly chart of the progress of autocracy, authoritarianism and economic restructuring around the world.
1. “ANTI-VAXXERS ARE JOINING RACIST MILITIAS”
We’ve covered the increasing demonisation of the “anti-vaxxers” regularly for over a year now. Ever since Joe Biden announced his new “domestic terrorism bill”, it was obvious that “Anti-vaxxers” were going to be re-branded as some kind of violent threat to democracy (and they were).
Now it’s happening in the UK too, with a story being published warning that “anti-vaxxers” are becoming more militant and there are fears they will “evolve towards US-style militias”, according to the Guardian.
The article references nameless “counter terrorism” officials and anonymous “Whitehall sources”, who warn that…
Latest intelligence assessments describe the anti-vaxxer movement as ostensibly a conveyor belt, delivering fresh recruits to extremist groups, including racially and ethnically motivated violent extremist organisations.
So there you have it, being anti-Covid “vaccines” is a gateway protest. Before you know it you’ll be shaving your head and sieg hieling all over the place.
Absolutely pathetic propaganda, and hopefully not an early warning sign of legislation to come.
2. “WHAT IF DEMOCRACY AND CLIMATE MITIGATION ARE INCOMPATIBLE?”
OK, this is from two weeks ago, but it’s too important to skip. The title says it all, Foreign Policy is genuinely wondering if climate change is too much of a threat to let democracy stand in the way of fighting it.
It’s a long read, soaked to the bone in double-talk and built on some very shaky assumptions, but there’s some good material on there…
Democracy works by compromise, but climate change is precisely the type of problem that seems not to allow for it. As the clock on those climate timelines continues to tick, this structural mismatch is becoming increasingly exposed. And as a result, those concerned by climate change—some already with political power, others grasping for it—are now searching for, and finding, new ways of closing the gap between politics and science, by any means necessary.
It warns in the opening section, before concluding…
… democracy, in its current form, is not necessarily the path to a solution. It might, instead, be part of the problem.
It’s not hard to see where this is going. We warned, several times, that we would be moving on from Covid to climate, and that “climate lockdowns” were a very real possibility. This kind of talk is setting the groundwork for that movement.
3. ‘MORE PEOPLE IS THE LAST THING THIS PLANET NEEDS’
Another from the Guardian, this time interviewing all the hip and happening young men who are “getting vasectomies to save the world”
It’s about the climate. Again.
Apparently, there are already too many people (that’s not true, but whatever), and so young men are getting the snip. Bravely preventing placing the burden of climate catastrophe onto the next generation… by making sure there isn’t one.
One of the (anonymous, and therefore potentially made-up) interviewees went right out cut his balls off the week Donald Trump was elected. That’ll show ’em.
But wait… It’s not just about climate, it’s also about feminism.
Specifically, it’s about correcting the “gender imbalance” traditionally associated with birth control:
Vasectomies address the gender imbalance that still accompanies the choice and practice of birth control. They come with less risk than more invasive and less reliable methods of female contraception, including sterilisation and the coil.
They are genuinely arguing that making yourself sterile forever is less risky and less invasive than having a completely 100% reversible IUD inserted.
Then they start bemoaning that vasectomies can be “hard to come by, especially for younger, childless men“. NHS GPs are apparently reticent to simply sterilise perfectly healthy young men for no good reason:
While there are no laws on the age at which men in the UK can get a vasectomy, the NHS advises that they may be more likely to be accepted if they are older than 30 and have children. “Your GP can refuse to carry out the procedure … if they don’t believe it’s in your best interests,”
Not only that, but the NHS has cut funding to for vasectomies, and perhaps as a result of this, vasectomy numbers are down nationwide. The Guardian want us to think this is a bad thing, but considering the UK’s birth rate has been falling for decades, it might not be.
Nevertheless, there is hope that “world vasectomy day”, and its links to the fight against climate change, will help “burnish” the vasectomy’s progressive image.
The story ends with inspiring words from one of the voluntarily snipped…
“A lot of people are happy to point and say: ‘That’s wrong,’ or film it on their phone… I look at the world and say: ‘That’s not right; I’m going to try to do something about it.’”
A wonderful attitude. I hope he can pass that wisdom on to his children and his children’s children.
… oh, wait.
BONUS: (NEW) HELLHOLE OF THE WEEK
Not Australia this time, well done guys.
This time it’s New Zealand, where Prime Minister Jacinda Ardern has just put in place strict new rules to “combat” the spread of Omicron.
Starting today, the whole of the country will move into the red on New Zealand’s “traffic light” system, meaning mandatory masks, lockdowns for the unvaccinated and an increased self-isolation period of 24 days.
How many cases prompted this decision? Nine.
Nine Covid cases in Motueka are confirmed to have the Omicron variant, prompting the decision, Ardern said.
Australia has been pretty aggressive in the game of “anything you can do, I can do worse” they have going with both New Zealand and Canada, so expect a move from them sometime this week.
IT’S NOT ALL BAD…
Yesterday marked 2022’s first “Worldwide Freedom Rally”, with marches taking place all over the world, from London to Bern, to Vancouver to Warsaw to Liverpool to Genoa.
Bilbao, Graz, Brisbane. The list goes on and on and on.
Huge crowds turned out in Toronto… Stockholm… and Sydney.
In London NHS staff threw down their uniforms in front of Downing Street.
These are the people who they want to classify as domestic terrorists and militias.
Also, someone also sent us this sign, which is our new favourite:
All told a pretty hectic week for the new normal crowd, and we didn’t even mention that the world’s ten richest men have doubled their fortunes during the pandemic or the Fed’s report on a digital dollar.
News the BBC couldn’t ignore as top doctors demand jab mandates are ditched
By Will Jones | TCW Defending Freedom | January 23, 2022
THE NHS vaccine mandate should be cancelled to prevent staff shortages, the Royal College of GPs has said, as thousands took to the streets across England to protest against the policy. The BBC reported:
‘NHS workers who oppose the Government’s mandatory vaccination policy have staged a protest in central London.
‘Demonstrations were also held in other cities across England including Manchester, Birmingham and Leeds.
‘Martin Marshall, Chairman of the Royal College of GPs, said compulsory vaccination for health professionals in England was “not the right way forward”.
He said the vast majority of staff were vaccinated but some 70,000 to 80,000 were not and they accounted for 10 per cent of staff at some hospital or GP surgeries.
If unvaccinated staff were taken out of frontline roles by April 1st there would be “massive consequences” for the NHS, he told BBC Radio 4’s Today programme.
‘He said a delay would allow time for booster jabs and a “sensible conversation” about whether vaccines should be mandatory at all.
‘Danny Mortimer, deputy chief executive of the NHS Confederation, said some frontline staff would have to leave their roles if they choose not to be vaccinated.
‘He said: “This will reduce frontline NHS staff numbers even further and lead to more gaps in capacity at a time of intense pressure and patient demand.”
‘In London, demonstrators marched from Regents Park to the BBC headquarters in Portland Place in a peaceful protest against mandating vaccines for health workers.’
Update:
The Telegraph and Daily Mail report that mandatory vaccines for NHS staff could now be pushed back by six months, following these nationwide protests over the requirement and amid demands by Tory backbenchers to drop the rule entirely.
Featured Video
Israel and the Palestinians — It’s about Mind Over Matter
or go to
Aletho News Archives – Video-Images
Book Review
The Greatest Threat to World Peace? A Review of Daniele Ganser’s ‘USA: The Ruthless Empire’
Review by Marilyn Langlois | November 10, 2023
 If you regard the United States as perhaps flawed but overall a force for good in the world . . .
If you regard the United States as perhaps flawed but overall a force for good in the world . . .
If you scoff at the notion that the US, a republic founded on principles of freedom and democracy, has morphed into a world empire, perpetrating assassinations, coups d’état, acts of terror and illegal warfare . . .
If you want to promote peace but haven’t yet explored deceptive events that precipitate US warmongering . . .
. . . here is a volume that will clear the air and paint an honest picture of the significant, not-so-rosy impact US foreign policy and actions have had in the world around us.
USA: The Ruthless Empire, by Swiss historian and peace researcher Daniele Ganser, is the newly published English language translation of his book Imperium USA, originally written in German and published in 2020. Here is a summary of key points — including some lesser-known ones — along with remedies for a more peaceful future, that are covered in the book. … continue
Blog Roll
 Aletho News
Aletho News- Villains of Judea: Douglas Feith
- US pension fund invests hundreds of millions in weapons firms supplying Israel
- US bill to grant Americans serving in Israeli army same rights as US troops
- What a president, a movie star, a congressman, and a cell phone all dared to say
- ‘An entire nation is being humiliated by the Iranian leadership’: Merz
- Pakistan Throws Open Its Gates for Iran’s Transit Trade to Third Countries
- Iran to charge ships passing Strait of Hormuz in rial: Lawmaker
- Talks would resume if US accepts 3-phase framework Iran put forward
- Israeli forces raid Syria’s Dara’a, Quneitra countryside, set up checkpoints
- IRGC says to reverse engineer 15 undetonated US missiles uncovered in southern Iran
- If Americans Knew
- Israel escalates in Gaza: killing, torture, hunger – Daily Update
- Six Months into Gaza Ceasefire, Setting the Record Straight About Aid
- ‘Silent suffering’: Why children in Gaza are losing their ability to speak
- In Gaza, 17,000 infections linked to rodents and external parasites – Daily Update
- Lobby group taking journalists on propaganda tours of Israel
- The Shattered Figure of Jesus Is Not an Exception. It’s a Pattern
- Israel’s idea of ceasefire includes killing 21 in one day – Daily Update
- Christians in Israel and Palestine, past and present
- Israel eager to restart Iran war, Gaza genocide – Daily Update
- Meet the Top “Content” Producers Linked to Canary Mission
- No Tricks Zone
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
