New German Chancellor Says There Will Be “No Red Lines” As Regards COVID Restrictions
By Steve Watson | Summit News | December 15, 2021
Angela Merkel’s successor in Germany has declared that there is nothing he won’t do to battle COVID, a stark statement given previous pledges to make compulsory vaccinations legal.
Chancellor Olaf Scholz used his first address to the nation in Germany to push vaccinations, declaring that they are the only way Germany can overcome the pandemic.
Scholz added that there would be “no red lines” in the battle against the current wave of COVID, which he declared to be fueled by unvaccinated citizens.
“We will pull every possible lever,” he continued, adding “It will get better. Yes, we will win the fight against this pandemic with the biggest determination. And, yes, … we will overcome the crisis.”
He added that “our society is not divided,” and referring to people opposed to vaccinations proclaimed “We will not put up with a tiny minority of uninhibited extremists trying to impose their will on our entire society.”
While claiming “We are listening. We are looking for debate,” Scholz stated “There is in Germany today . . . denial of reality, absurd conspiracy stories, wilful disinformation and violent extremism.”
“We will counter this with the means of our democratic constitutional state. Our democracy is a democracy capable of defending itself,” the Chancellor further warned.
On Sunday, Scholz stated that he supports vaccine mandates across Germany, noting that he intends to “vote for compulsory vaccination, because it is legally permissible and morally right.”
Scholz previously said he wants to introduce mandatory coronavirus vaccination for all Germans as early as February, according to sources close to him.
Germany recently recorded its highest COVID death toll for 9 months, despite having mask mandates and stringent rules in many regions that banned the unvaccinated from numerous venues.
The country is preparing to follow the example of Austria by imposing new lockdown measures that will exclusively apply to the unvaccinated.
The Pandemicists Must Be Stopped
The Pandemicists at Work:

This strange and mildly disturbing illustration actually accompanies the article, one of many cases where the NYT betray the sinister undertones of their agenda via accompanying imagery.
eugyppius – December 14, 2021
Corona has vastly expanded the ranks of pandemic planners and public health botherers. Unless something is done, these people will destroy all of society in their radical pursuit of a few viruses.
Just a few words on “Omicron is a Dress Rehearsal for the Next Pandemic”, a New York Times article by Emily Anthes, a science journalist with ties to the World Economic Forum. It’s subtitled “America’s response to the variant highlights both how much progress we have made over the past two years — and how much work remains,” and it’s every inch as awful as you’d imagine.
In the piece, Anthes laments that the United States is “woefully unprepared for the challenges ahead, starting with the most fundamental of tasks: detecting the virus.” She quotes a microbiologist to complain that “We had a delay of one to two months before we were even able to identify the presence of [Omicron] … And by that time, it had already circulated widely between multiple states and from coast to coast.” She wastes many words on the necessity of “Testing, testing, testing”; here, apparently, America still needs vastly more capacity. She and her many scientist informants also want more gene sequencing to detect variants sooner. She’s sure that all of this is absolutely necessary, even though she doesn’t know why:
Scientists are finding more Omicron cases every day, and the variant could soon overtake Delta. What comes next — what we should aim for, even — is less clear. Should we spend the winter trying to stop every infection? Protecting the highest risk people from severe disease and death? Ensuring that hospitals are not overrun?
“One thing that we’ve lacked continuously through the pandemic is a goal,” said Emily Gurley, an epidemiologist at the Johns Hopkins Bloomberg School of Public Health. “We still don’t have that. Certainly, we don’t have that for Omicron.”
No realistic public health goal underpins this diagnostic mania, of course. People who test positive for Corona are sent home to suffer in untreated silence by themselves. Endlessly testing, tracing, sequencing, panicking and closing is, however, a goal in itself for people like Emily Gurley and all the other pandemicists Anthes gleefully quotes, from Eric Topol to Trevor Bedford to Ezekiel J. Emanuel. All of them want the Corona Circus to play on, and after it ends they hope for a sequel sometime soon. Never before have they enjoyed such personal and professional prominence.
Even if by some miracle all of this winds down tomorrow, this whole odious internationally networked enterprise of Virus Astrology, from virologers to sequencers to testers to planners to nudgers to vaccinators, won’t go away. They were a malign influence even before Corona, of course. In 2009, when we suffered under a small fraction of the Pandemicism that burdens us now, they succeeded in causing an international uproar over a mild strain of pandemic influenza. Now their ranks have been vastly expanded, and they are already hoping for the next opportunity to close our schools, lock us up at home and stick us full of needles.
The pandemicists are truly dangerous, and they will grind human civilisation into the dust unless we find some way of putting all of them out of work. They aren’t going to save anybody from the next pandemic; in the event it happens, they’ll just take advantage of the opportunity to expand their ranks still further and make all of our lives worse. And should novel viruses prove slow to materialise in the post-Corona era, they’ll get up to other tricks. Tricks like new and enhanced histrionics over every seasonal influenza outbreak. Tricks like the intentional release of more engineered viral pathogens to keep the grant funding flowing. Tricks like constant lunatic mass vaccination schemes against ever milder viruses. Still other tricks I haven’t considered. The pandemicists have to go.
A huge Israeli study shows natural Covid immunity is far superior to the vaccine-generated kind
By Alex Berenson | December 14, 2021
mRNA vaccine protection from Covid is far weaker than natural immunity and declines very fast, according to a new study of almost 6 million people in Israel.
During the summer Covid wave, more than 140,000 Israelis who had been vaccinated but not received a booster shot became infected with Covid. Put another way, in just two months, about 1 out of every 20 vaccinated Israelis became infected with Sars-Cov-2.
Natural immunity – the protection following infection and recovery – lasts much longer, the study shows.
In fact, people who had already had Covid once had better protection from the virus more than a year later than people who had been vaccinated only three months before.
The gap was even larger in cases of severe infection.
Vaccinated people were more than five times as likely to develop severe infections than people with natural immunity. Only 25 out of roughly 300,000 Israelis with natural immunity developed severe Covid infections in the summer wave – compared to almost 1,400 vaccinated Israelis.
The difference did not result from gaps in age between vaccinated and recovered people. People over 60 benefitted even more from natural immunity relative to vaccination than did younger people.
The study also showed that giving people who had natural immunity a vaccine dose did little to lower rates of infection for them, raising the question of why they should ever be vaccinated.
Finally, the study offered a disturbing signal that vaccination may ultimately interfere with the development of lasting immunity in people who are infected after being vaccinated.
A booster shot did lower the risk of infection about to the level of peak protection from natural immunity – but because the study ended in September, it is impossible to know how long that protection may last.
All these findings come out of a database of Covid infections among almost 6 million Israelis in August and September, at the peak of the fourth Covid wave in Israel. The database contains information on essentially every Israeli over age 16 who was fully vaccinated or had previously had a Covid infection.
The paper, “Protection and waning of natural and hybrid COVID-19 immunity,” is currently available as a preprint at:
https://www.medrxiv.org/content/10.1101/2021.12.04.21267114v1.full.pdf
Oddly, the paper’s title does not mention waning of vaccine immunity, although the figures it presents make the severity of the problem clear. Such shyness is common among researchers presenting bad news about Covid vaccines – they will offer the data, but not highlight it.

Israel has exclusively used the Pfizer mRNA vaccine, began mass vaccinations before almost any other country, and has an excellent health care database. As a result, it has among the best information on the effectiveness of the shots. It offers far more complete data than the United States.
The vaccine failure over the summer in Israel – following apparent success in the spring – has presaged a similar pattern across the United States and Europe, and a similar desperate campaign for boosters.
In this paper, the researchers examined infection rates among five different groups of Israelis – those with natural immunity, those who had received boosters, those who were vaccinated but had not received boosters, those with natural immunity who had also received a vaccine, and those who had become infected after being vaccinated.
The researchers specifically excluded unvaccinated Israelis without natural immunity from the comparison because Israel has very few of them and they are “unrepresentative of the overall population.”
In other words, the researchers explicitly denied the validity of the comparison that vaccine advocates make when they compare Covid rates among vaccinated and unvaccinated people in places with high vaccination rates (a point I have been trying to make for months).
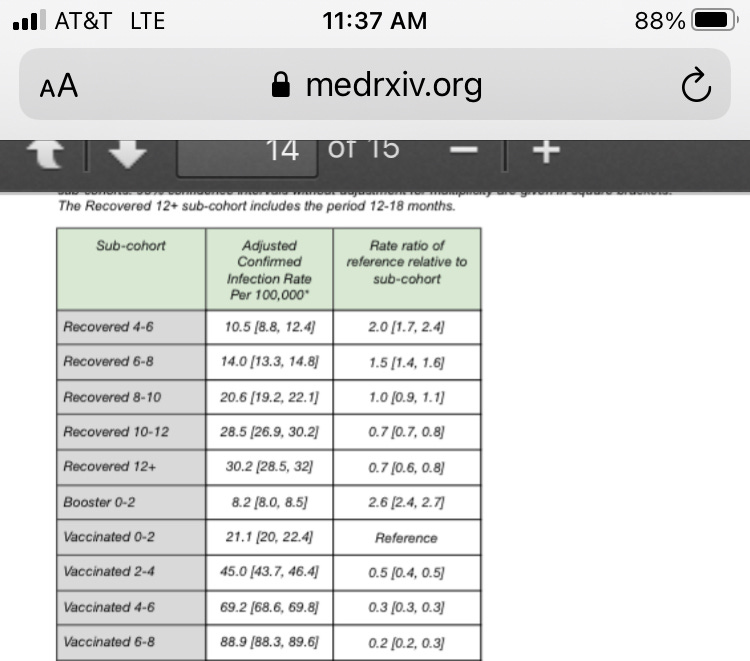
The researchers found that the highest rates of infection by far came in people who had been vaccinated at least six months before. They had a nearly 3 percent chance of being infected per month (the researchers present the figure as 89 per 100,000 “person-days.”)
Those people were four times as likely to be infected as newly vaccinated people. They were also seven times as likely to be infected as people who had natural immunity from an infection six to eight months before, and three times as likely as those who had natural immunity from an infection more than year before.
A single vaccination dose in people with natural immunity temporarily produced strong protection, the researchers found. But after six months, the advantage had faded to within the margin of statistical error. In other words, so-called hybrid immunity hardly appeared to exist after six months – natural immunity was once again providing the protection.
Nor did vaccination appear to stop severe disease.
Nearly every case of severe disease in the database – almost 1,400 of the roughly 1,600 cases – came in vaccinated but unboosted people. Boosters did appear to reduce severe disease significantly. Again, though, the study covered less than two months after the booster program began, when boosters should be at peak effectiveness.
Finally, the study showed that people who had been vaccinated and then been infected and recovered were actually more likely to be infected again six months later than those who had only “pure” natural immunity.
That finding, though based on a small number of cases, adds to worrying data that mRNA vaccination may actually wrong-foot our immune systems in the long run and make it harder to build lifelong protection against Covid.
Is Vaccine Effectiveness Against Death Mostly a Statistical Illusion?

By Will Jones | The Daily Sceptic | December 12, 2021
One of the big challenges in analysing the data on Covid has been definitions. What is a Covid death, what is a Covid case or infection? What the data appears to say can change radically depending on the definitions adopted.
This has been a particular issue with vaccination, as vaccination status is subject to a variety of conflicting definitions. In particular, when does someone count as vaccinated? Is it as soon as they have the needle in their arm, or do they remain ‘unvaccinated’ after that for a period of time, say seven, 14 or 21 days?
For instance, the recent ICNARC report stated the number of ICU admissions by vaccination status. But it also clarified that ‘unvaccinated’ includes those who received a jab less than 14 days prior to testing positive. This means that some (an unknown number) who were counted as unvaccinated had in fact received a dose.
This may be more than just a minor problem. For one thing, there is now a lot of evidence that people are more vulnerable to infection in the days following their jab, likely due to temporary immune suppression. This means a significant proportion of the vaccinated who are susceptible to infection with the current dominant variant are infected in the immediate post-jab period when in many studies and reports they don’t count as vaccinated. This creates a ‘survivorship bias‘ in the remaining vaccinated group that exaggerates vaccine efficacy. For instance, in a study of the U.S. nursing home population published in NEJM, once the post-jab period was included – when the vaccinated experienced higher incidence than the unvaccinated – the overall proportion of vaccinated and unvaccinated groups testing positive was the same at 6.8%. This makes it essential that all the data is presented, including for past-jab periods, and definitions are clear.
A similar problem occurs with the classification of deaths as vaccinated and unvaccinated. New analysis led by Norman Fenton, Professor in Risk Information Management, and Martin Neil, Professor in Computer Science and Statistics, both at Queen Mary, University of London, has highlighted a strange anomaly in the ONS deaths data that may be indicative of a deeper problem. They noticed that if non-Covid deaths in the unvaccinated were plotted against time over the course of the vaccine rollout then a strange spike appeared during the rollout in which the mortality rate among the unvaccinated shot up to well above the background level. The same thing happened with the non-Covid mortality rate in the single-dosed as second doses were rolled out, and the phenomenon was repeated in each age group as vaccines were administered.

Since there is no obvious reason that vaccination should impact on non-Covid mortality in this way, Prof Fenton, Prof Neil and team argue that this is evidence of a problem in the way the data is recorded or defined. In particular, if it is assumed that the unvaccinated in fact continue to die of non-Covid causes at the background rate and that the additional non-Covid deaths above that are deaths that are actually in the vaccinated but have been misclassified (owing, say, to not counting those who die within 14 days of their jab) then, they argue, a more realistic pattern emerges (see below).
In each age group there is now a spike in non-Covid deaths in the vaccinated right at the start of the rollout, which the team argue makes sense as vaccination was prioritised for the most vulnerable who are more likely to die of any cause. Indeed, it was confusing in the original data that this initial spike was absent and the vaccinated died of non-Covid causes at a lower rate than the unvaccinated despite the most vulnerable being prioritised for vaccination.
The team discovered a different problem when they looked at Covid deaths by vaccination status. Here, the vaccines appear to be highly efficacious, but there is an anomaly that may again be indicative of deeper problems in the data.
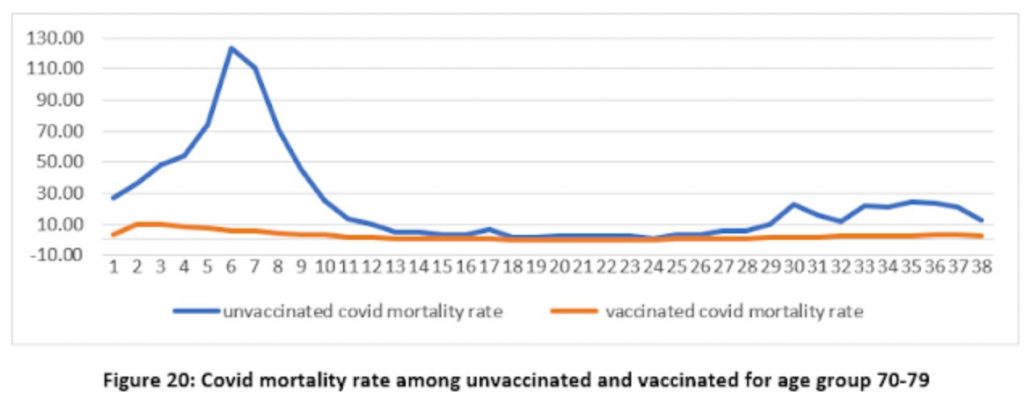
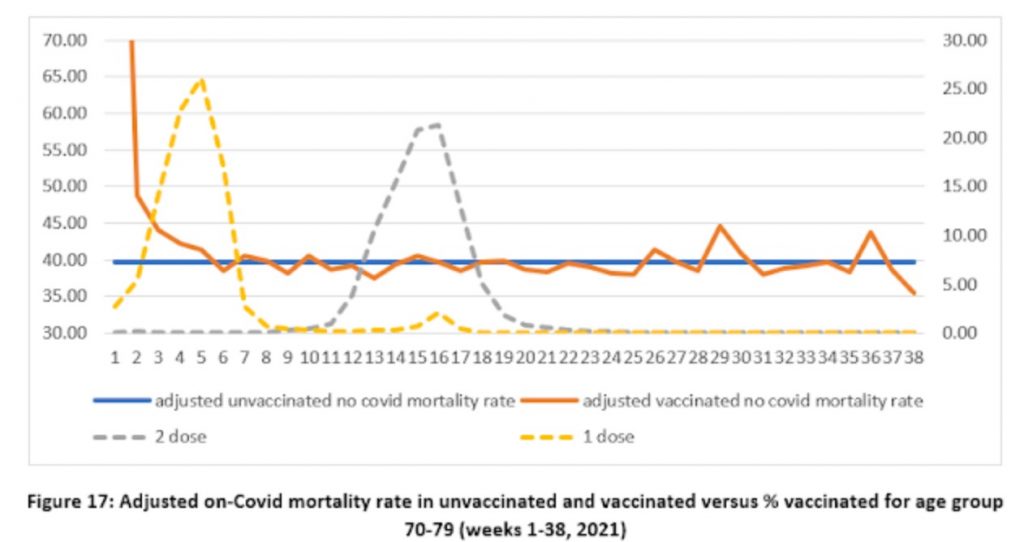
Again a spike appears in the unvaccinated mortality rate where there is none in the vaccinated. Fair enough, you might think, as the vaccines are protecting the vaccinated. However, it’s important to remember that the vaccines are not expected to work until 21 days after the first jab, yet here we have a spike in unvaccinated Covid mortality in the middle of the rollout before most of the vaccines should take effect – referring to figure 17 above we can see that the vaccine rollout in the age group peaked in week five, around the same time as the mortality rate in the unvaccinated peaked (week six), which all seems much too early.
Prof Fenton, Prof Neil and team suggest that the problem here may be in the denominator, that is to say, in how many people are supposed to be in the vaccinated and unvaccinated populations when calculating the mortality rate each week. It’s important to realise that the populations here are changing fast as tens of thousands of people get vaccinated each week. Using the right figure for the right week therefore makes a big difference to the mortality rate reported. Could this anomalous spike in unvaccinated Covid deaths be an artefact of this kind of problem?
Professor Fenton thinks so. He and his team suggest that the problem may be that the relevant denominator or number of people vaccinated for each week is not how many are vaccinated in the week a person dies but in the week they were infected, which is around three weeks earlier on average. What happens if the denominators are shifted by three weeks to allow for this? (Prof Fenton demonstrates the effect of shifting denominators in a short video of a hypothetical example here.)
The effect is remarkable, as shown below (note the change of scale on the y-axis).
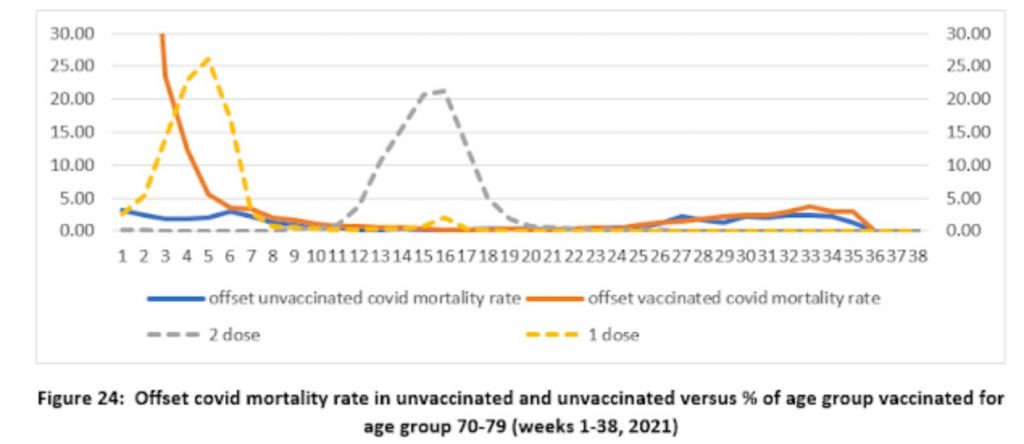
Shifting the population denominator estimates by three weeks means that the number of vaccinated for calculating the vaccinated mortality rate becomes much smaller, making the mortality rate much higher, while the denominator for the unvaccinated becomes much larger, making the mortality rate much lower. This massively reduces the mortality rate in the unvaccinated to low levels – to under five deaths per 100,000 people throughout the period, rather than as many as 125 per 100,000 in week six previously. Instead, a mortality spike appears in the vaccinated at the start of the vaccine rollout (though note that the scale is smaller so it only reaches 30 per 100,000 people), which makes some sense as the vulnerable were prioritised for vaccination and at this point the population of vaccinated was small, so contained a high proportion of vulnerable people. Prof Fenton and team remark that it also tallies with what we know of the increased vulnerability of the recently-vaccinated to infection, as noted above.
The shift in population estimates also greatly reduces the implied effectiveness of the vaccines in the autumn wave, where the lines are now much closer to one another, which is in line with findings from Sweden and elsewhere as vaccine efficacy wanes. Prof Fenton and team suggest that once you take into account the initial spike in the vaccinated, then this new analysis suggests there is “no reliable evidence that the vaccines reduce all-cause mortality”.
So is this what’s going on? There are certainly anomalies that need to be explained, and the analysis by Professor Fenton, Professor Neil and team makes a lot of sense. It deserves to be taken seriously by the ONS and UKHSA.
Stop Press: Watch Prof Fenton discussing his team’s findings with Maajid Nawaz on LBC radio.
The most detailed evidence yet of the devastating damage Covid vaccines can do
By Neville Hodgkinson | TCW Defending Freedom | December 13, 2021
INJECTING millions of people with countless copies of a gene that instructs the body to produce a toxic protein might not seem very sensible. But it was hoped that this approach, the basis of the Covid vaccine, would help minimise damage caused by the protein – the ‘spike’ that the genetically engineered SARS-CoV-2 uses to invade our body cells – when we meet the actual virus.
Last month we reported an American heart specialist’s finding that most of his patients showed biochemical changes signalling increased cardiovascular risk in the weeks following their Covid mRNA jab. Markers for inflammation, cell death and an immune response to coronary artery injury all increased compared with results from a few months previously. The overall results indicated a ‘dramatic’ rise, from 11 per cent to 25 per cent, in the likelihood of a heart attack or similar event occurring some time over the next five years should those changes persist.
The report was presented as an abstract to a meeting of the American Heart Association (AHA), and subsequently published in Circulation, the AHA’s journal. After being made public, an ‘expression of concern’ was added to the abstract, saying there are ‘potential errors’ and it may not be reliable.
There is however every reason to take it seriously – apart from UK researchers reportedly having found similar results, which they are not prepared to publish for fear of losing research money.
Last Friday the most detailed evidence yet of the damage the vaccine can do was presented at an online symposium on Covid science organised by Doctors for Covid Ethics. This is an international group that has long opposed the mass rollout of the Covid jab, arguing in particular that the immune system may attack our own tissues when it detects the presence of the spike protein.
Thousands of deaths have been reported in the wake of the jab, but regulators claim most of these are coincidental, and have neglected detailed investigation of whether or not the vaccine was responsible.
Exactly that kind of investigation was carried out by German pathologist Professor Dr Arne Burkhardt, who has 40 years of experience in the field. He examined the tissues and organs of 15 patients where a post-mortem had been performed, an exceptional opportunity that came about because the bodies were in institutes of legal medicine and institutes of pathology.
There were seven men and eight women aged between 28 and 95. They died between seven days and six months post-injection.
In essence, Burkhardt found internal damage in most of the deceased, caused by a self-destruct process in which immune cells – lymphocytes – had invaded different parts of the body.
In five of the 15 cases, it was concluded that the correlation with the vaccination was very probable; in seven, it was probable; and in two cases it was not clear, but possible. ‘In one case we did not find any of these changes of any significance,’ Burkhardt said.
He presented slides showing how the lymphocytes infiltrated heart muscle in particular, causing inflammation. Resulting lesions were small and easily overlooked, ‘but the destruction of just a few muscle cells may have a devastating effect’, he said. ‘If the inflammatory infiltration is found where the impulse for the contraction of the heart is given, this may lead to heart failure.’
Another finding, also easily missed, was lung damage caused by the lymphocyte invasion, seen in nearly half the cases. Liver, kidney, uterus, brain, thyroid and skin also showed signs of autoimmune damage.
Summarising Burkhardt’s presentation, Canadian microbiologist Professor Dr Michael Palmer said: ‘Anybody with a medical training will see just how devastating the effect of these vaccines can be, at least in those who die after the vaccination . . . we also now know why the authorities were very hesitant to have autopsies performed on such victims.’
Elsewhere, Palmer has argued that even though deaths after vaccination are few compared with the numbers who have received the jab, ‘the total lifetime dose of these messenger RNA vaccines that you can tolerate before you die is limited. We don’t know the exact amount because there is simply not enough experimental data. That’s one of the great scandals of these vaccines, that no proper toxicity studies have been carried out.’
Animal studies have shown clearly that the jab does not just stay at the site of the injection. It circulates widely, such that the spike protein can combine with receptors in many parts of the body, and especially cells that line our blood vessels, causing both clotting and excessive bleeding. Many sudden clusters of deaths (see here and here) have been reported in the immediate wake of the vaccine drives, also observed in athletes.
Burkhardt’s findings, highlighting immune cell infiltration of tissues where the vaccine-induced spike protein has manifested, come in the wake of many warnings of such a mechanism and are supported by various studies suggesting long-term risks. These include:
· US physician Dr Patrick Whelan warned the US Food and Drug Administration a year ago, before the vaccine rollouts, that jabs based on the spike protein may themselves trigger symptoms of severe Covid, including blood clots, brain inflammation and damage to the heart, liver and kidneys. Whelan, a paediatric specialist caring for children with multisystem inflammatory syndrome, urged particular caution over giving the vaccine to children and young adults, as they normally fight off the infection in its early stages. Before any of the vaccines were approved for widespread use in humans, he said, there should be an assessment of the effects on the heart.
· The vaccine includes a modification in the RNA code aimed at synthesising abundant copies of the spike protein – running into trillions of molecules, according to this visual display produced by Dr Charles Hoffe, a Canadian doctor. He says the majority of people who receive the Covid shot ‘are getting blood clots that they have no idea they’re even having.’ The modification, along with a device that protects the RNA mechanism against immediate destruction by the body, may enable the jabs to present a bigger risk in some recipients than natural infection, since this is usually dealt with successfully by a healthy immune system. No one knows exactly how much of the protein is produced by the jab, nor how long it lasts in the body.
· Dr Robert Malone, inventor of the mRNA technology, says ‘multiple peer-reviewed references’ demonstrate that the virus’s spike protein poisons body cells (see for example here), but the vaccine developers have not demonstrated the safety of their version of the protein. Proper evaluation of the risks is still not being carried out, he says.
· Another German pathologist found from autopsies conducted on 40 people who died in the wake of the jab that 30-40 per cent were vaccine-related. Professor Peter Schirmacher believes many such deaths are missed, with doctors attributing them to natural causes.
· American cardiologist and journal editor Dr Peter McCullough has warned that the vaccine can damage heart tissue in ways that go unnoticed at first, but which create scar tissue liable to cause permanent cardiac dysfunction later in life. ‘This will go down as the most dangerous biological medicinal product rollout in human history,’ he says. McCullough has also highlighted an increase in deaths among children in the UK since the NHS began vaccinating teenagers aged 12 and over against Covid.
· An analysis of UK ‘Yellow Card’ adverse reaction data by Dr Tess Lawrie’s Evidence-Based Medicine Consultancy found thousands of reports of blood clotting after the Covid jabs. Almost every vein and artery was affected, and every organ including parts of the brain, lungs, heart, spleen, kidneys, ovaries and liver, ‘with life-threatening and life-changing consequences’. Lawrie urged the UK regulators as long ago as last June to declare the vaccine unsafe for use in humans because of the deaths and adverse reactions being reported.
· A ‘chilling’ acknowledgement of the specific risks of mycocarditis (inflammation of the heart muscle) and pericarditis (swelling in tissue surrounding the heart) following Covid vaccination was issued this month by the UK Health Security Agency. The agency still insists such cases are rare and that most patients recover fully, but evidence such as Burkhardt’s suggests many deaths may go unrecognised as vaccine-related.
It’s a terrible mess, and there is a desperate need for a review of the entire Covid vaccine strategy. UK pathologists, please come to the rescue!
Since Biden’s Injection Order the Rate of Covid Deaths in the US Military Has Quadrupled
Anti-Empire | December 12, 2021
On August 25th Biden ordered that every member of the US military (active, reserve and national guard) must perform a fundamental sacrament of the mind virus cult known as “vaccination”.
A week before the order US military Covid deaths stood at 34.
Presently they stand at 79.
In other words, in the 4 months since the injection order as many US servicemen were deemed to have died with/from Covid as in the entire 17 months before the order was given.
In the entire vaccine-free 2020 fewer than 20 US servicemen died with/from Covid. (24 by March.)
The unvaccinated military of 2020 experienced three times fewer Covid deaths than the heavily injected military of 2021.
Even so at 2 million strong and 79 deaths, a Covid death is still rarer than a lottery win.
The Pentagon says the dead were overwhelmingly “not fully vaccinated,” but the Pentagon also doesn’t consider troops “fully vaccinated” until 14 days after the 2nd dose — that is to say until the initial period of negative vaccine efficiency has ended.
Comirnaty, liability, and how the HHS lies, cheats and steals
By Meryl Nass, MD | December 12, 2021
I checked the Federal Register and there has been no notice that Comirnaty has been added to the National Childhood Vaccine injury Program (NVICP). I confirmed this by checking whether Comirnaty had been added to the childhood schedule, and according to the HRSA, which manages both compensation programs, it has not.
So, if you receive the licensed Comirnaty vaccine, correctly labeled as the brand-name product and not the vaccine being fobbed off as licensed product, and you are injured, you are free to sue the manufacturer for your injury. Could this be why Pfizer wrote, “Pfizer does not plan to produce any product with these new [Comirnaty National Drug Codes] and labels over the next few months while EUA authorized product is still available and being made available for U.S. distribution.”
If, however, you receive the Pfizer-BioNTech vaccine under Emergency Use Authorization, or the Moderna or J and J vaccine, you can’t sue anyone. You have the right to beg HRSA for compensation of lost wages and unpaid medical bills, period. So far, HRSA and the Countermeasures Injury Compensation Program it administers have not paid out one dime for the approximately one million injuries and 20,000 deaths reported to VAERS for any COVID vaccine.
In other words, the federal government (DHHS) has not admitted a single injury was caused by a COVID vaccine. CDC says it has not linked a single death to a COVID vaccine–not even when the patient walked into the vaccination center but got carried out to the morgue. FDA doesn’t know much about myocarditis, Bell’s Palsy, thrombosis, thrombocytopenia, pulmonary emboli, etc. There are no black box warnings on any of the COVID vaccines.
HRSA, FDA, CDC and NIH are all agencies within the federal Department of Health and Human Services. They have all gotten their stories straight. They know nothing and they are just following orders. Heil HHS!
They can’t find a doggone problem in the 20 or so databases they are spending many $millions of your money to “study.”
Want to know the biggest conspiracy in the US right now? It is the HHS.
FDA has access to a bunch of electronic databases it has termed the “BEST” Initiative, and it published a plan to use them to study heart attacks, pulmonary embolism, thrombocytopenia, etc. back in July. Where are the results, FDA? What are you waiting for? (According to CDC, “More than 459 million doses of COVID-19 vaccines were administered in the United States from December 14, 2020, through November 29, 2021.”). It seems clear that we aren’t supposed to be informed of FDA’s findings until everyone possible has been vaccinated, at which point the results will be irrelevant.
In October 2020, FDA’s Steve Anderson told us there were even more databases that would be studied.
On August 23, 2021, FDA announced its databases were inadequate to assess myocarditis, so BioNTech would have to do it for them. Here is what FDA wrote about its inability to use VAERS and its many other databases:
- As noted above, the FDA acknowledges that “We have determined that an analysis of spontaneous postmarketing adverse events reported under section 505(k)(1) of the FDCA [in other words, VAERS–Nass] will not be sufficient to assess known serious risks of myocarditis and pericarditis and identify an unexpected serious risk of subclinical myocarditis.
- Furthermore, the pharmacovigilance system that FDA is required to maintain under section 505(k)(3) of the FDCA [in other words, FDA’s many other databases that cost the taxpayer zillions–Nass] is not sufficient to assess these serious risks.”
NOT SUFFICIENT???
Unsaid, but implied, is that if FDA is incapable of studying thousands of reported cases of myocarditis, it probably cannot study the other serious adverse events that have been reported in conjunction with COVID vaccines.
VAERS has operated for 30 years, collecting reports of vaccine adverse events. It averaged under 100 cases of myocarditis reported yearly until this year. Through November, CDC reports it received 1949 reports of myocarditis and pericarditis, in those under 30. CDC didn’t say what the total number of reports for all ages was.
Somehow, these HHS don’t seem all that concerned that the admitted reporting rate of myocarditis is over 20 times the average during the past 30 years. Why?
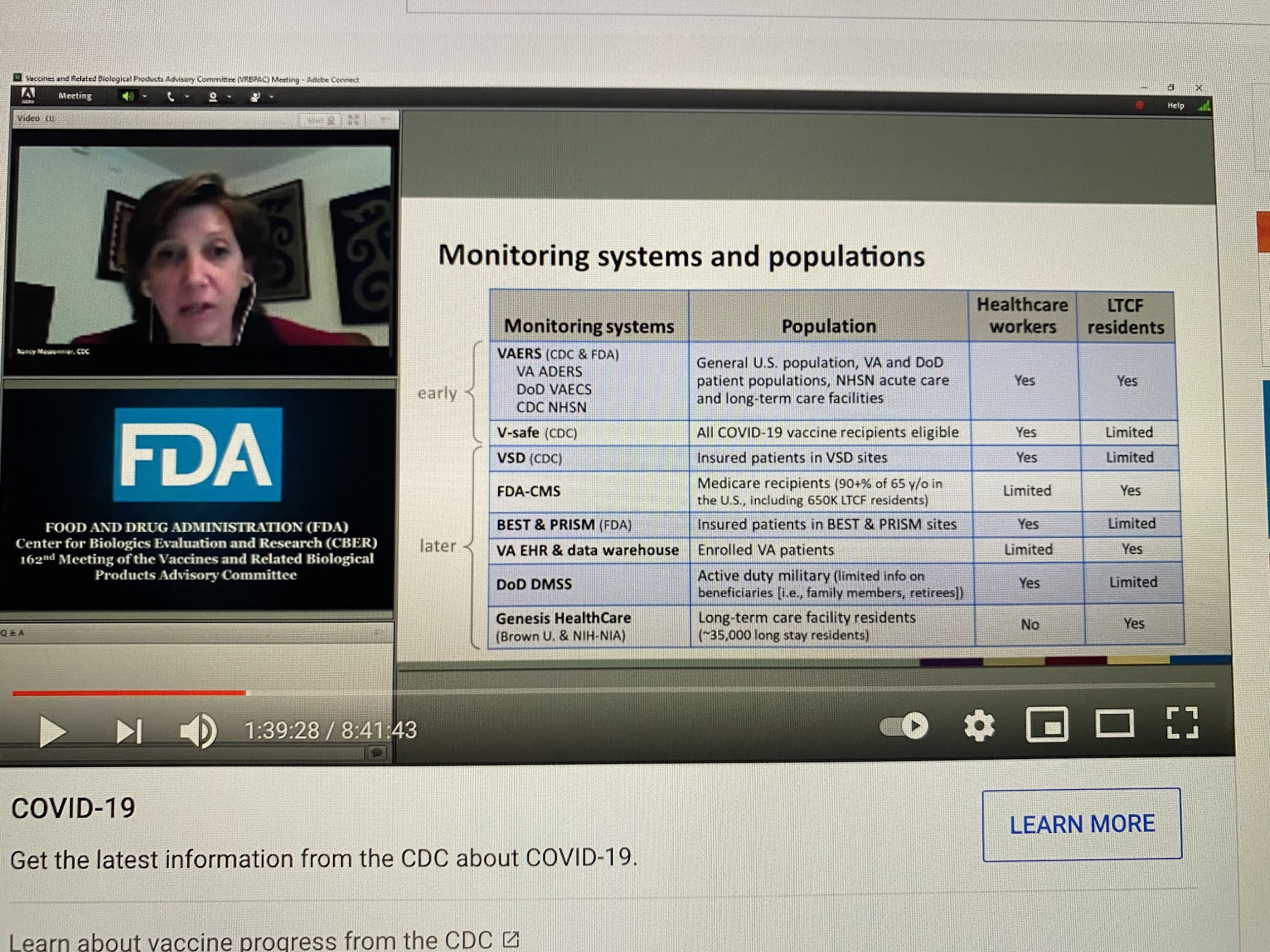
CDC has been even more shady in its analyses of safety as FDA, if that is even possible. Below, Nancy Messonier, then head of Immunizations and Respiratory Diseases at CDC, presented this list of databases that CDC would be using in the evaluation of COVID vaccine safety, on December 10, 2020. Apart from the V-safe (which they stopped talking about last January), VSD (which somehow can’t find any problems, not even myocarditis) and VAERS, all these other databases have been MIA.
NIH, whose job has never been to issue treatment guidelines, but instead to do and fund research, suddenly took over the treatment guidelines for COVID early in 2020. It formed a committee of internal and eternal “experts” to make up the guidelines. How were they chosen? That is not clear, but what is clear is that 16 of these so-called experts had current or recent financial entanglements with Gilead, the maker of remdesivir. NIH and the US Army also owned pieces of remdesivir. A number of other had financial conflicts with Merck. While NIH is the biggest single funder of medical research in the world, I cannot recall seeing a single study it funded on the safety of COVID vaccines. But somehow vaccines are its number one recommendation.
But it is not even clear that the committee is functional. The NIH has been sued to learn whether a vote was even taken by the committee regarding its ivermectin guidelines, which fly in the face of the evidence on ivermectin. How was NIH somehow authorized to issue guidelines in the first place?
Here is what has obviously occurred. All these agencies were told they had to keep quiet on vaccine problems (and perhaps problems of other COVID treatments), and they had to fiddle with their data or their analytic methods, or both, to get the required results. And there was to be NO BAD NEWS, no matter what. And no good news regarding generic treatments.
As we have seen, the so-called scientists and physicians working as bureaucrats in these agencies all caved, sucked it up, did the dirty work, kept their jobs, and betrayed their oaths and the trust of the people of the USA and the world.
Featured Video

Argentina’s Javier Milei sells out his country for Israel
or go to
Aletho News Archives – Video-Images
From the Archives
Mutually Assured Delusion (MAD)
By Judith Curry | Climate Etc. | November 5, 2013
Groupthink: A pattern of thought charaterized by self-deception, forced manufacture of consent, and conformity to group values and ethics.
Groupthink: Collective Delusions in Organizations and Markets, by Roland Benabou, published in the Review of Economic Studies. Benabou also has a talk (ppt slides) on this subject.
First, a definition of groupthink (from the ppt slides):
Janis (1972)’s eight symptoms [of groupthink]:
- illusion of invulnerability
- collective rationalization
- belief in inherent morality
- stereotyped views of out-groups
- direct pressure on dissenters
- self-censorship
- illusion of unanimity
- self-appointed mind guards
Sound like any groups that we know? … continue
Blog Roll
 Aletho News
Aletho News- How Cognitive Science Explains Our Looming Nuclear Crisis
- Have the US and Israel killed non-proliferation?
- Moscow, Tehran to support each other amid US aggression: Russia’s defense minister
- Iran says EU’s insistence on sanctions hastens its ‘embarrassing descent into irrelevance’
- Argentina’s Javier Milei sells out his country for Israel
- Putting Nukes in Finland Won’t Make Country Safer, Finnish Politician Cautions
- Ukrainian drone strike kills worker at Europe’s largest nuclear power plant
- What the West Hides About Soviet Role in De-Colonization
- Villains of Judea: Douglas Feith
- US pension fund invests hundreds of millions in weapons firms supplying Israel
- If Americans Knew
- Palestinians in Gaza Want to Rebuild Food Systems. Israel Isn’t Letting Them.
- Under Trump, Green Card Seekers Face New Scrutiny for Views on Israel
- Sheep Theft Sent Shockwaves Through a Palestinian Village. Then, a 12-year-old Boy Was Shot Dead
- Trump alum helps Israel mount AI influence campaign
- Dispatches From Catastrophe
- Despite Denials, AIPAC Is Now Funding Campaign of Ala Stanford In Philadelphia
- Israel’s neighbors are irate about its treatment of religious sites
- Israel escalates in Gaza: killing, torture, hunger – Daily Update
- Six Months into Gaza Ceasefire, Setting the Record Straight About Aid
- ‘Silent suffering’: Why children in Gaza are losing their ability to speak
- No Tricks Zone
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
