New VAERS analysis reveals hundreds of serious adverse events that the CDC and FDA never told us about
Serious adverse events that are more elevated than myocarditis. New VAERS analysis by Albert Benavides blows the “safe and effective” narrative away.
By Steve Kirsch | November 9, 2021
The CDC and FDA have said the vaccines are “safe and effective.” They haven’t found any serious issues with the COVID vaccines. Zero. Zip. Nada. It was the DoD that found myocarditis.
The evidence in plain sight shows that they are either lying or incompetent. Or both. But of course, the medical community is never going to call them on this.
So that’s where our team of vaccine safety experts comes in; to reveal the truth about what is really going on.
In a brand new VAERS data analysis performed by our friend Albert Benavides (aka WelcomeTheEagle88), we found hundreds of serious adverse events that were completely missed by the CDC that should have been mentioned in the informed consent document that are given to patients. And we found over 200 symptoms that occur at a higher relative rate than myocarditis (relative to all previous vaccines over the last 5 years). All together, there were over 4,000 VAERS adverse event codes that were elevated by these vaccines by a factor of 10 or more over baseline that the CDC should have warned people about.
As of November 1, 2021, there have been more adverse events reported for the COVID vaccines than for all 70+ vaccines combined since they started tracking adverse events 30 years ago. That’s a stunning statistic, nobody can deny it, but nobody in the mainstream medical community (or mainstream media) seems to care much. It’s not even worth noting in passing. Wow.
Here’s what the evidence shows:
- The COVID vaccines are the most dangerous vaccines in human history. They are 800 times more deadly than the smallpox vaccine which was the previous record holder. The vaccines have killed over 150,000 Americans and permanently disabled even more. They don’t make sense for anyone of any age. The younger you are, the worse it gets. For kids, it is estimated that we kill 117 kids for every COVID death we prevent.
- The Pfizer 6 month trial showed the drug can save 1 life for every 22,000 people vaccinated. It also appeared from the trial that the drug killed more people than it saved (there were 20 deaths in the treatment group vs. 14 in placebo after unblinding). So we are “saving” fewer than 10,000 lives at the expense of over 150,000 deaths. In short, we kill 15 people to save 1. That’s incredibly stupid. But nobody in the Biden administration wants to meet with our team. They basically don’t want to hear the truth. Instead, they focus on deplatforming and censoring us which are techniques that are effective when the data doesn’t work out for you.
- Both the FDA and CDC have proven inept in spotting safety signals. They can’t even compute the VAERS URF which is a number that is required for any serious risk-benefit analysis. So the FDA and CDC outside committee members are all flying blind in approving the vaccines. Even after this deficiency is pointed out in the public comments by yours truly (and direct emails to the committee members), it makes no difference. We are ignored. The CDC safety monitoring is so bad that they even admitted at the last ACIP meeting that it was the DoD that spotted the myocarditis signal. So the FDA and CDC have basically been batting .000 in terms of spotting safety signals that have been sitting in plain sight the entire time.
- They can’t admit that they missed the signals now because that would be an admission they missed them before. So they will try to discredit this article with ad hominem attacks (this is a technique used to win an argument when you cannot win on the evidence).
- The serious events we highlight below are all consistent with the mechanism of action that Robert Malone and I first described in the Darkhorse podcast. Namely, that the spike protein that is produced in response to the delivery of the mRNA is cytotoxic and results in blood clots, inflammation and scarring throughout your body which then creates a wider range of severe adverse events than any vaccine in human history.
- The medical community is trained by the CDC to believe the vaccines are safe, so they interpret all the adverse events as not vaccine related. But if it wasn’t the vaccine that caused all these events, what was it? What’s worse is they tell their patients, “this is all in your head” or that “your baby died because you had a genetic defect.”
- In general, patients believe their doctors and never figure out where to get a cytokine panel to discover that they are vaccine injured (go to www.covidlonghaulers.com to get the cytokine panel and IncellDx to get the spike protein assay). So people never learn how to rid their body of the spike protein either (see my article on vaccine treatment for the drugs they use to do this) which is the first step in the road to recovery.
- The high adverse event rates aren’t “excess reporting.” It is due to excess events. For example, one neurologist had 0 cases of vaccine adverse events in her entire career, but this year, she has 2,000. Another physician I know has had 0 events in 29 years in his 700 patients. This year he needs to report 25 events. Physicians themselves have experienced stunningly higher incidence rates of reproductive, neurological, and cardiac events since the vaccines rolled in 2021. We couldn’t find a single cardiologist who actually had fewer cases of myocarditis after the vaccines rolled out as the members of the FDA and CDC claim.
- The serious events are primarily centered around menstruation, blood clots, inflammation and scarring, cardiovascular damage, and neurological damage, just as we predicted in the podcast in June of 2021.
- There are hundreds of serious adverse events that are caused by these vaccines. This of course is shocking to people since the CDC has repeatedly said you can’t ascribe causality to data in VAERS. Not true. The VAERS data analysis (temporal data, the dose dependency, and the elevated reporting rates compared to baseline) provide ample signal to enable us to show causality on all of these events using the five Bradford-Hill criteria applicable to vaccines.
- Nicki Minaj was right to complain about elevated rates of testicular swelling, impotence (erectile dysfunction), and orchitis. Every world authority who opined on the matter belittled her and said she was wrong, but all the symptoms she talked about are strongly elevated as you’ll see from the data below. None of these so-called experts of course ever looks at the data; it’s all based on arguing from their belief system rather than the scientific evidence. And even if those authorities disagreed with the VAERS data, it was irresponsible not to have pointed out the raw data to people and then explain why they totally ignored the elevated signal in the VAERS data. Today, we do science based on our belief system rather than the old-fashioned way of looking at what the data actually says. Our team is old-fashioned.
- There is a pretty good chance that the vaccines don’t really work at all and never did. We know the Pfizer Phase 3 trials were gamed in many ways. There is no doubt that the vaccines elevate antibodies, but it seems that it is quite possible that the immunity they confer is actually the result of killing off (or excluding as in the case of the trials) people with weaker immune systems. The people who are left are thus more resistant to the virus. Mathew Crawford will be coming out shortly with an analysis that makes a compelling case for this novel hypothesis. Subscribe to his substack here.
- It is unlikely that anyone in the world will want to debate us publicly on any of the claims above (or on any of my articles or on any of Mathew’s articles), but if you are a prominent supporter of the false narrative and want a public debate, we are here for you. Our team would be thrilled to accept the challenge as we have no desire to spread misinformation. If we got it wrong, we are happy to correct our mistakes if you can explain to us clearly the mistake we made and the correction you suggest (e.g., the “right” answer). Yet even with multiple million dollar incentives (listed in this article), nobody seems to be interested in showing how we got it wrong. Everyone talks about how bad the vaccine misinformation problem is, but nobody is willing to do anything to show that we got it wrong. For example, I’ve asked any prominent scientist in America who disagrees with my analysis (showing eight different ways to validate that over 150,000 Americans have been killed by the vaccines) to let me see their “correct” analysis showing the “correct” number, but nobody will. They won’t even come on a recorded call to show us how we got it wrong. It’s baffling. They all want to do it in slow motion via documents because that way it’s easier to obfuscate the truth and they can avoid answering questions. The latter is key.
- It’s really easy to tell who is telling you the truth here. John Su is the CDC expert on VAERS. If he’s wrong, the entire narrative falls apart. I personally attacked Dr. Su in a widely read article accusing him of being corrupt. I offered to publish his response in the article. He said nothing. I offered to debate him. No dice. TrialSiteNews tried to interview him. He refused to reply. Seriously? If the CDC gave us 2 hours to ask John Su questions, we would destroy his credibility and the credibility of the CDC. That’s why he’s not talking and that’s why the CDC will never let him talk to anyone on our team. Because we don’t ask softball questions like what John gets at the ACIP meetings. We play hardball.
What we found in the VAERS analysis below can be verified by anyone because it is all publicly accessible. Albert spent only a few hours to produce the tables. So the CDC should have been able to do the same work Albert did.
You can easily verify any entry yourself via manual queries to any VAERS interface (my favorite is MedAlerts, but others such as openvaers and the HHS site give the same results).
Before we get to Albert’s analysis of the VAERS data, let’s do a little background.
The Darkhorse Podcast
On June 10, 2021, my friend Robert Malone and I appeared on Bret Weinstein’s Darkhorse Podcast to tell the world what we had learned about the COVID vaccines. You can watch the 3 hour version here or the condensed 1 hour version here if you haven’t already seen it. I highly recommend the whole thing; I know a lot of people who watched it multiple times and raved about it.
Basically, we said the COVID vaccines were super dangerous, they had killed a lot of people at the time, the Pfizer bio-distribution data that Dr. Byram Bridle obtained from the Japanese government using a FOIA request showed the lipid nanoparticles delivered a very substantial dose of mRNA to female ovaries, and that the spike protein that is subsequently produced causes blood clots, inflammation, and scarring leading to a large number of cardiovascular and neurological symptoms, a number of which would be irreversible. Robert in particular noted that we had no clue about the amount, dose, and duration of the spike protein that is produced (we still don’t) because this testing was never done in animals (they looked only at the distribution of the nanoparticles which is not the same thing). Bret referenced a very long article I had written on May 25, 2021 for TrialSiteNews entitled “Should you get vaccinated?”
For reference, here is the bio-distribution graph that Bret showed in that podcast:

See anything wrong? Note that we deliberately omitted areas of the body where the vaccine was expected to accumulate in order to highlight areas of the body where it wasn’t supposed to go. Naturally, those supporting the mainstream narrative that the vaccines are safe and effective went into overdrive to suppress the episode and discredit what we said. They said we were dishonest not to include everything in the chart. YouTube censored the video after nearly 1M views. Wikipedia accused both of us of spreading misinformation and then blocked me when I tried to point out that the scientific evidence supported what I said. Wikipedia relies on fact checks for science.
We were right about everything we said in the podcast, and now, thanks to the work Albert did, it’s now easier to see we were telling the truth: the top elevated events were neurological, cardiovascular, and related to the female reproductive system, just like we said. I was stunned at the sheer number of menstrual events that made it to the very top of the list. That was a surprise to me.
Openvaers has been highlighting the damaging effects on both male and female reproductive systems for months with a page dedicated to reproductive health, but the medical community, Congress, and mainstream press wasn’t paying any attention at all. These event counts are not normal, but nobody really seems to care. President Biden not only doesn’t care; he wants to force all our kids to be vaccinated with the most dangerous vaccine in human history.

With the new analysis, the counts are much easier to interpret because instead of being just raw counts, they are numbers relative to a baseline rate so we can instantly see what symptoms are “abnormal” meaning 10X or more higher than “expected.” The answer: over 4,000 adverse events.
The X factor analysis (November 7, 2021)
Before I give you the link to the spreadsheet of VAERS symptoms sorted by X factor, you need to know a few things to properly interpret the data.
First, let’s address the myth that is promoted by the FDA that the VAERS database is “over reported.” As we said above, there are more events this year than any previous year, so that’s why the events are up. But there still could be a component of overreporting as well, i.e., that people this year are more likely to make a report on an event compared to last year since everyone is so “highly aware” of the vaccines. Nice theory. No data to back it up. Nobody making that argument has ever included any data to back up their assertion. We call that a hand-waving argument. Doctor surveys we’ve done show that, if anything, they are less likely to report an adverse event this year for a variety of reasons (hospital frowns on it, no time, still too frustrating, too many events to report). The other way we can tell is to look at the rates of events that are not comorbidities or causal. We find that events like Musculoskeletal pain, Screaming, Head banging, Local reaction, Diet refusal, Croup infectious, Hepatitis A, Eyelid oedema, and more occur at pretty much the same rate this year as in previous years.
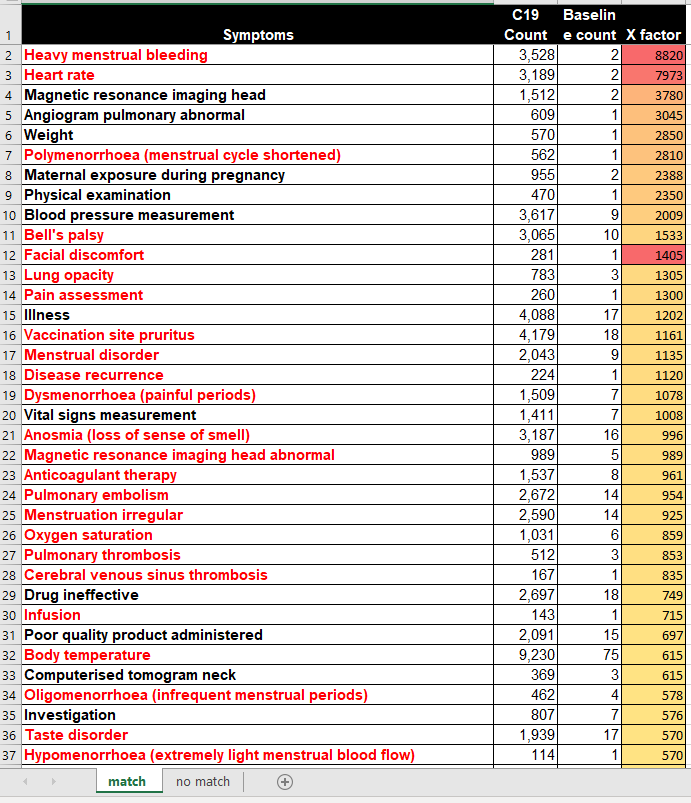
Now let’s tackle the columns:
Symptom
This is the VAERS symptom name. These are coded by HHS upon receipt of the report based on the contents of the report. Some of these symptoms are tests that are ordered. An elevation of a test is a good signal something is amiss. Other symptoms are not causal, but are comorbidities. For example, it might be that diabetes is there more often not because it makes diabetes worse, but because diabetic people are more likely to report symptoms. So for these symptoms, we have to be careful about the analysis. But for many of these symptoms such as cancer, herpes zoster (shingles), diabetes and more, these are all exacerbated by the vaccine as we know from talking directly to doctors. Finally, some symptoms like “rib fracture” or “suicide” are elevated because they are caused by the vaccine. For example, the vaccine can make you lose consciousness and fall and fracture your hip. The vaccine can give you tinnitus which is so bad that you want to kill yourself. So we have to be extremely careful to examine each one of these symptoms carefully because in most cases, we’ll find that they are indeed caused by the vaccine. I’ve coded a bunch of symptoms red that I thought were serious/interesting. I’m not done yet, so the redness coding was only methodically done on the first 100 symptoms and sporadically after that. When I get more time, I’ll go through them and update the file. Note that myocarditis is located on row 274, i.e., way way down.
Also, when looking at deaths, we never look at a “symptom” of death since death is coded in a separate field. So the event count for the “death” symptom (6,487) is lower than the over 8,000 domestic deaths.
Guillain-Barre syndrome is only elevated by a factor of 6 from baseline, likely because other vaccines also elevate GBS; this vaccine elevates it even more.
C19 count
This is the raw number of VAERS events in 2020 and 2021 due to the COVID vaccines for that symptom. The key here is that this count should be multiplied by 41 (known as the underreporting factor or URF to estimate the absolute number of events that occurred). See this article for how that is computed.
Baseline count
The baseline rate is the # of incidents occurring in a 5 year period from 2015-2019 for all vaccines given in that time period.
X-factor
The X-factor is the (C19 count*5/Baseline count). This is because the baseline is 5 years so we compare the COVID counts in a year vs. the average count in a typical year. So an X-factor of 10 or more would mean that the symptom is very likely to be caused by the vaccine since it is highly elevated from the “normal” rate.
Now let’s tackle the tabs. There are two tabs:
match tab
On the match tab are symptoms where the baseline count !=0
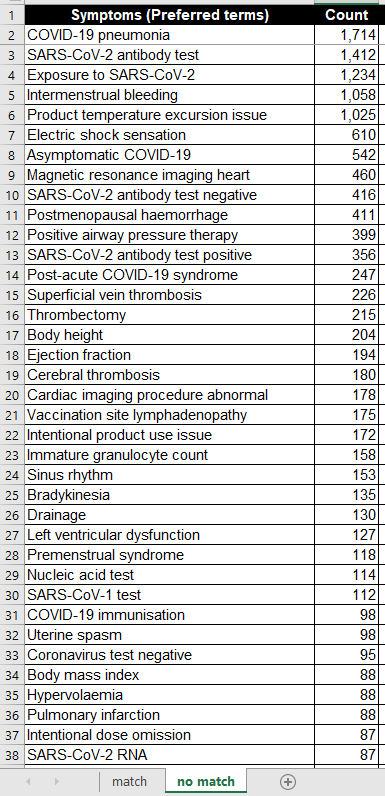
no match tab
On the “no match” tab are symptoms where the baseline count=0. So these are quite extraordinary since these symptoms are not typically seen even once in 5 years. So here, even a small value in the “count” field is very significant, e.g., 2 or more would be comparable to a 10X or more on the “match tab.”
Now here are some screenshots of the first page of the two tabs:
And the no match tab:
What the data tells us
Here are a few quick observations from the complete data set (see next section for downloading):
- Female reproductive issues top the list. These are strongly elevated by these vaccines. Many of the top symptoms are all related to the menstrual process.
- There are an enormous number of cardiovascular and neurological events that are strongly elevated, many of them serious.
- Fibrin D dimer increased is #53 on the list, elevated by a factor of over 400x above baseline. Charles Hoffe discovered D-dimer was elevated in over 60% of the patients he measured. This is very serious as D-dimer is a lagging indicator of blood clots.
- Troponin increased was #130, elevated by a factor of 205. Troponin indicates heart damage and it is elevated to extreme levels (10X heart attack levels or more) and can stay elevated for months at a time (with a heart attack, the levels start returning back to normal immediately after the incident)
- Death as a symptom (which is pretty unusual coding since it isn’t a symptom), is #433 and elevated by 96X. Hardly a “safe” vaccine.
- Brain herniation at #405 is elevated by a factor of 100X over baseline. However, this is not considered a big deal at the CDC (perhaps because many people there don’t use their brain).
- Cardiac arrest at #450 is elevated by 93X. This is when your heart stops. This is a relatively serious condition since you don’t last for too long after that. It’s a bit surprising that the CDC missed that one. Perhaps because they don’t have a heart?
- Pulmonary embolism #24 is elevated by 954 times normal. How the CDC can miss that one is simply astonishing! This was the cause of death of 2 of the 14 kids that the CDC looked at in their death analysis. Mainstream press will never ask them that question as to why the CDC would not find causality here. They wrote: “CDC reviewed 14 reports of death after vaccination. Among the decedents, four were aged 12–15 years and 10 were aged 16–17 years. All death reports were reviewed by CDC physicians; impressions regarding cause of death were pulmonary embolism (two), …” 954 times normal is hard to explain, isn’t it? So no causality? That’s hard to explain, so they didn’t. They just moved on as if there is nothing to see.
- Intracranial haemorrhage (their spelling) is at #604 and is elevated by 79X. Two of the 14 kids from the CDC analysis died from that. How could that not be causal? They never explained that.
- Tinnitus at #362 is elevated by 105X. This can be so bad that people can kill themselves from this alone. One of the people who work at Vaccine Safety Research Foundation (VSRF) had to talk a friend out of suicide.
- There are many many more issues to be concerned with, but I wanted to get the list out quickly so there can be more eyes on this.
- For months, I’ve offered to discuss our data and analyses to both the FDA and CDC outside committees as well as the CDC and FDA themselves, but nobody wanted to see it. Most hit delete on my emails. A few told me to wait for the public comment period and submit it then (which I’ve done). Nobody followed up.
The Excel file with the full results
I’m trying to increase the number of paying subscribers I have as this supports the substack community. All proceeds will go to paying the salaries of people working for the Vaccine Safety Research Foundation (vacsafety.org) as well as buying ads so we can get the message out.
You can find the full Excel file and Albert’s analysis in this article.
YouTube suspends senator over Covid-19 vaccine video
RT | November 13, 2021
Wisconsin Senator Ron Johnson was temporarily suspended from YouTube for allegedly spreading “harmful misinformation” after he published a video discussing injuries related to Covid-19 vaccination.
Johnson accused YouTube of “censoring the truth” on Friday evening after his roundtable discussion video, which featured “stories from doctors, scientists and the vaccine injured,” was taken off the platform and led to his temporary suspension.
In the video, the Republican senator listed statistics relating to alleged vaccine side-effect victims, while his guests made comments questioning the effectiveness of Covid-19 vaccines in preventing death.
“Why won’t they let the vaccine injured tell their stories and medical experts give a second opinion?” Johnson questioned in a statement. “Why can’t we discuss the harmful effects of mandates?
“Apparently, the Biden administration and federal health agencies must not be questioned,” he said.
In its own statement, YouTube cited policies on reducing “the risk of real-world harm” and “preventing the spread of harmful misinformation” as the reason behind Johnson’s suspension.
It is the second time that the senator has been suspended by the platform, and his account could be permanently removed if he receives further sanctions within the next 90 days.
Since May 2020, YouTube has enforced a lengthy ‘Covid-19 medical misinformation policy’, which prohibits users from questioning the effectiveness of vaccines or claiming that they can “cause death, infertility, miscarriage, autism, or contraction of other infectious diseases.”
In August, YouTube temporarily suspended Kentucky Senator Rand Paul for questioning the effectiveness of face masks, while in the same month, Sky News Australia was suspended for allegedly violating Covid-19 rules.
In January, YouTube even suspended the sitting president of the United States after it accused Donald Trump of violating policies which prohibit the incitement of violence.
Biden’s vaccine mandate fails ‘reality & common sense’ check, judge rules

FILE PHOTO. © Reuters / Evelyn Hockstein
RT | November 13, 2021
A US federal appeals court has again ruled against President Joe Biden’s national vaccine mandate for companies with 100 or more workers, shredding the policy as “staggeringly overbroad” and an abuse of “extraordinary power.”
The Fifth Circuit Court of Appeals issued a stark rebuke to Biden’s vaccine requirement for larger American companies in a ruling on Friday, stating that the Occupational Safety and Health Administration (OSHA) – the federal agency tapped to enforce the mandate – was not created to “make sweeping pronouncements on matters of public health affecting every member of society in the profoundest of ways.”
“The Mandate is staggeringly overbroad,” Judge Kurt Engelhardt said, noting that it does not take into account the diversity of workplaces across the country, nor the fact that Covid-19 “is more dangerous to some employees than to other employees.” As an example, he compared a hypothetical 28-year-old truck driver who works in isolation to a “62-year-old prison janitor” employed in more cramped conditions.
“One constant remains – the Mandate fails almost completely to address, or even respond to, much of this reality and common sense.”
The Biden administration initially announced the requirement in September, with OSHA following up earlier this month with an emergency order to enforce the mandate. The agency will require all workers at firms with more than 100 employees to be fully vaccinated against Covid-19 by early next year, or else test for the virus regularly and wear masks at all times while working.
The appeals court issued its first stay on November 6 after a litany of plaintiffs – including a number of companies and several US states – challenged the move, conducting an expedited judicial review. Friday’s ruling reaffirmed the pause, telling OSHA to “take no steps to implement or enforce the Mandate until further court order.” Despite the first stay, the White House has continued to urge businesses to follow the vaccine dictate and effectively ignore the ruling, potentially setting up a battle in the Supreme Court.
While OSHA does have the power to issue what’s known as an “emergency temporary standard,” or ETS, the judge observed that only a single standard has survived legal scrutiny since the agency was founded in the 1970s.
“The reason for the rarity of this form of emergency action is simple,” Engelhardt went on, adding that courts and OSHA itself have agreed “for generations” that such orders constitute “extraordinary power” which must be “delicately exercised, and only in those emergency situations which require it.”
“The Mandate at issue here is anything but a ‘delicate exercise’ of this ‘extraordinary power.’”
VAERS COVID Vaccine Data Show Surge in Reports of Serious Injuries, as 5-Year-Olds Start Getting Shots
By Megan Redshaw | The Defender | November 12, 2021
The Centers for Disease Control and Prevention (CDC) released new data today showing a total of 875,653 adverse events following COVID vaccines were reported between Dec. 14, 2020, and Nov. 5, 2021, to the Vaccine Adverse Event Reporting System (VAERS). VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S.
The data included a total of 18,461 reports of deaths — an increase of 383 over the previous week, and 135,400 reports of serious injuries, including deaths, during the same time period — up 7,943 compared with the previous week.
Excluding “foreign reports” to VAERS, 643,957 adverse events, including 8,456 deaths and 53,780 serious injuries, were reported in the U.S. between Dec. 14, 2020, and Nov. 5, 2021.
Foreign reports are reports received by U.S. manufacturers from their foreign subsidiaries. Under U.S. Food and Drug Administration (FDA) regulations, if a manufacturer is notified of a foreign case report that describes an event that is both serious and does not appear on the product’s labeling, the manufacturer is required to submit the report to VAERS.
Of the 8,456 U.S. deaths reported as of Nov. 5, 10% occurred within 24 hours of vaccination, 15% occurred within 48 hours of vaccination and 26% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 427.6 million COVID vaccine doses had been administered as of Nov. 5. This includes: 250 million doses of Pfizer, 162 million doses of Moderna and 16 million doses of Johnson & Johnson (J&J).

Every Friday, VAERS publicizes vaccine injury reports received as of a specified date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed. Historically, VAERS has been shown to report only 1% of actual vaccine adverse events.
Numbers this week do not yet include reports from the authorization of Pfizer’s pediatric COVID vaccine for the 5 to 11 age group. Reports currently in VAERS for children under 12 are due to ”product administered to patient of inappropriate age.”
During a meeting on Oct. 26, by the U.S. Food and Drug Administration’s vaccine panel, Dr. Jessica Rose, a viral immunologist and biologist, said tens of thousands of reports have been submitted to the Vaccine Adverse Event Reporting System for children ages 0 to 18, and that 60 children have died — 23 of them were under 2 years old.
“It is disturbing to note that “product administered to patients of inappropriate age was filed 5,510 times in this age group,” Rose said. Two children were inappropriately injected, presumably by a trained medical professional, and subsequently died. This is malfeasance.”
This week’s U.S. data for 12- to 17-year-olds show:
- 22,782 total adverse events, including 1,400 rated as serious and 29 reported deaths. Two of the 29 deaths were suicides.
The most recent death includes a 17-year-old female from Washington (VAERS ID 1828901) who reportedly died Oct. 29 from a heart condition after receiving her second dose of Pfizer. According to the VAERS report, the girl had COVID in August and fully recovered. She received her first dose of Pfizer on Sept. 3 and her second dose on Sept 15.
On Oct. 23, she presented to the ER with chest pain and elevated troponin. She had an abnormal echocardiogram, abnormal EKG and became increasingly tachycardic. She then suffered cardiac arrest.
“Unfortunately she was not able to be resuscitated and died,” the report states. “Cause of death possible acute myocarditis.”
Other deaths include a 12-year-old girl from South Carolina (VAERS I.D. 1784945) who hemorrhaged 22 days after receiving Pfizer’s COVID vaccine, a 13-year-old girl from Maryland (VAERS I.D. 1815096) who died from a heart condition 15 days after receiving her first dose of Pfizer’s vaccine and a 17-year-old female from Texas (VAERS I.D. 1815295 who experienced an acute hyperglycemic crisis 33 days after being vaccinated.
- 59 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment or resulted in death — with 96% of cases
attributed to Pfizer’s vaccine. - 552 reports of myocarditis and pericarditis (heart inflammation) with 542 cases attributed to Pfizer’s vaccine.
- 131 reports of blood clotting disorders, with all cases attributed to Pfizer.
This week’s U.S. VAERS data, from Dec. 14, 2020, to Nov. 5, 2021, for all age groups combined, show:
- 19% of deaths were related to cardiac disorders.
- 54% of those who died were male, 42% were female and the remaining death reports did not include gender of the deceased.
- The average age of death was 72.7.
- As of Nov. 5, 4,260 pregnant women reported adverse events related to COVID vaccines, including 1,337 reports of miscarriage or premature birth.
- Of the 3,123 cases of Bell’s Palsy reported, 51% were attributed to Pfizer vaccinations, 41% to Moderna and 8% to J&J.
- 723 reports of Guillain-Barré syndrome (GBS), with 41% of cases attributed to Pfizer, 30% to Moderna and 28% to J&J.
- 2,093 reports of anaphylaxis where the reaction was life-threatening, required treatment or resulted in death.
- 10,857 reports of blood clotting disorders. Of those, 4,790 reports were attributed to Pfizer, 3,864 reports to Moderna and 2,149 reports to J&J.
- 3,071 cases of myocarditis and pericarditis with 1,922 cases attributed to Pfizer, 1,016 cases to Moderna and 123 cases to J&J’s COVID vaccine.
Teen diagnosed with Guillain-Barré syndrome After COVID Vaccine
A 17-year-old girl was hospitalized for Guillain-Barré syndrome (GBS) — a rare disorder in which the body’s immune system attacks its nerves — after receiving a COVID vaccine. Shelby Allen said she’s thankful she isn’t paralyzed and didn’t die.
Allen started experiencing back pain and tingling in her arms after getting vaccinated. Symptoms progressed until she found herself unable to feel her arms and legs while bowling with her school’s team. Allen’s parents took her to the doctor in Jackson, Tennessee, where she was diagnosed with GBS and admitted to the ICU.
Allen’s doctor “knew right off the bat” her reaction was caused by a COVID vaccine, but still recommended people get vaccinated. Allen is hoping she’ll be able to walk by March for her high school graduation.
Taiwan temporarily halts second dose of Pfizer over myocarditis concerns
The Central Epidemic Command Center (CECC) said on Wednesday a panel of experts is suspending second doses of Pfizer-BioNTech’s COVID vaccine for children 12 to 17 years old amid concerns it may increase the risk of myocarditis.
Cases of myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the outer lining of the heart) have been reported in children between 12 and 17 years old who received Pfizer’s vaccine.
CECC cited U.S. statistics which show the risk of experiencing heart inflammation after receiving a second dose is 10 times higher than after the first dose.
Chen Shih-chung, who heads up the CECC, said the Ministry of Health and Welfare’s Advisory Committee for Immunization Practices halted second doses of Pfizer for two weeks, during which time experts and CDC physicians will assess 16 cases of myocarditis among adolescents after Pfizer vaccination before making a decision on whether to go ahead with the second dose.
Hong Kong gives only a single dose to teens 12 to 17, while the UK recommends only one shot for children between ages 12 and 18.
More countries restrict Moderna vaccine over reports of myocarditis
France’s public health authority recommended people under 30 receive Pfizer’s COVID vaccine instead of Moderna, due to higher risks of heart problems in young adults, Reuters reported.
The Haute Autorite de Sante (HAS), an independent advisor to the French health sector, cited “very rare” risks linked to myocarditis, confirmed by a French study published Monday.
“Within the population aged under 30, this risk appears to be around five times lesser with Pfizer’s Comirnaty jab compared to Moderna’s Spikevax jab,” HAS said.
Germany’s advisory committee, known as STIKO, said on Wednesday people under age 30 should receive only Pfizer’s vaccine, as it causes fewer cases of heart inflammation in younger people. STIKO also recommended pregnant women receive only the Pfizer vaccine, regardless of their age.
The recommendations were based on new safety data from the Paul Ehrlich Institute — Germany’s authority in charge of vaccines, and new data.
The decision came after several other countries restricted the use of Moderna to older populations, including Canada, Finland, Denmark and Sweden. France’s medical regulator on Oct. 15 recommended using only Pfizer’s vaccine for booster shots, despite the European Union’s drug regulator last month approving Moderna’s booster for all age groups over 18.
Pfizer asks FDA to authorize third booster dose for all people 18 and older
As The Defender reported Nov. 10, Pfizer and BioNTech on Tuesday asked the FDA to authorize a third dose of their COVID vaccine for all people 18 and older, even though advisory panels to the FDA and CDC in September overwhelmingly rejected a similar request.
The companies said their new request is based on the results of a study, conducted by Pfizer and BioNTech, which has not been published or peer-reviewed. The companies said the study of more than 10,000 volunteers showed vaccine efficacy against symptomatic infection of 95% or greater for people receiving the booster.
Pfizer did not disclose how many participants experienced asymptomatic infection, or whether the clinical trial — as did Pfizer’s clinical trial for 5 to 11 years olds — included individuals with natural immunity acquired from previous SARS-CoV-2 infection.
Children’s Health Defense asks anyone who has experienced an adverse reaction, to any vaccine, to file a report following these three steps.
Megan Redshaw is a freelance reporter for The Defender. She has a background in political science, a law degree and extensive training in natural health.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Indonesia cut Covid by 98% with Ivermectin while Australia grew cases 500% with Lock-n-Vax
JoNova | October 22, 2021
When we last looked at Indonesia their massive wave in Covid cases had just peaked after ivermectin was approved again on July 15th. Since then the cases have dropped from 50,000 a day to about 900. On a per capita basis today Indonesia is managing Covid about ten times better than Australia. Think about that.
Remember the reason for the Indonesian surge. In June, they had a controlled rolling caseload of 5,000 a day. It was not rising thanks to a philanthropist called Haryoseno who had been arranging for ivermectin supplies at low cost to help people. But in a fit of modern-medicine, in line with the deadly WHO recommendations, the Indonesian government banned ivermectin on June 12th. Cases took off. Mayhem ensued. And about 90,000 people died in the following surge.
By early July the anti-parasitic drug ivermectin was hot property in Indonesia, even if it was banned. A number of high-ranking politicians championed it, and people were flocking to buy it.
“Indonesians have ignored health warnings to stock up on a “miracle cure” for COVID-19 backed by leading politicians and social media influencers, as an out-of-control virus surge sweeps the country.”
By July 15th the Indonesian government relented, and BPOM approved Ivermectin as Covid-19 Therapeutic Drug. By July 18th new daily cases peaked across Indonesia and now they are lower than they were before. During the surge, at least two million Indonesians were infected.
Perhaps Governments shouldn’t run around banning a wonder drug so safe that researchers in Australia feed it to small children to kill head lice.

All bell curves look the same, but some are bigger than others. Timing is everything. OWID
Google Trends show Indonesians were searching for ivermectin in early July. The average Indonesian apparently knows more about treating Covid than our Minister of Health. More even than our Chief Medical Officer.

There was one popular search in Indonesia as cases rocketed.
Greg Hunt could have managed the Covid debacle so much better if he’d just phoned up a pharmacist in Bali.
Compare the Rich-mans Vax plan
Australia, on the other hand, decided to vaccinate 15 million people or 70% of the entire population and still has twice as many cases as Indonesia does — even though Indonesia has ten times as many people and only on third of the government revenue.
The Australian TGA committee banned ivermectin on Sept 11th, by the way, possibly to make sure we didn’t accidentally eliminate Covid, or Pfizer’s third quarter profits. Who can tell?
That lockdown-and-vax plan and the roadmap to freedom doesn’t seem to be working too well. In Australia billions of dollars were burnt at the stake, not to mention the health risks of using experimental prophylactics, while Indonesia reduced Covid cases by 98% for about point-one percent of the cost and the main side effects were the deaths of worms, lice and bed bugs.
If Gladys had just dished out the Ivermectin — Uttar Pradesh style — on July 5th, the outbreak would have been over in a few weeks.

Australia vaccinated 70% of the population and locked down its two largest states to control Covid and still hasn’t succeeded. Source: OWID
Since July 18th when Indonesia cases peaked, Australian cases have grown from 31,000 to 150,000.
The only thing more scary than the Ministry of Health’s incompetence is that politicians and philanthropists in the third world have more freedom than Australian ones do. The Indonesian media is more worth watching than the Australian ABC.
At this point people are still dying who could be saved.
As David Archibald says “It means that Australia could end its covid problem anytime it wanted to at hardly any expense at all. Our government would be aware of what the Indonesians have achieved. It also means that any covid deaths from here on are state-sanctioned murder. “
___________________________________________________________
The wonder drug that disappeared
My summary of Ivermectin
If you only email friends one link — make it this story. It’s the biggest medical scandal since 1850— Why is a cheap safe drug being ignored? Could it be that there would be no medical emergency and no need to rush out other riskier new treatments which are still classed as “experimental” if there was a safe alternative? There are billions of reasons to ask this question but newspapers wouldn’t publish the story. In desperation, some Americans are going to court to get rulings to order doctors to use Ivermectin on their loved ones. Even if they win, sometimes hospitals still refuse to use it on patients with few options left. One family hired a helicopter to take their mother away from intensive care in a hospital that refused to give Ivermectin (and had a happy ending). The debate is so suppressed, there are rumours the US President was treated with it in secret last year.
For peer reviewed studies read: The BIG Ivermectin Review: It may prevent 86% of Covid cases.
Ivermectin has also been used, with apparent success in India, Peru and Mexico (and so many other places). Covid cases fell in the states of India that approved Ivermectin use but rose in Tamil Nadu where it wasn’t permitted. Despite the success, India’s Health dept suddenly stopped Ivermectin use again and people in India are suing the WHO in disgust. In Peru, Ivermectin cut covid deaths by 75% in 6 weeks.
The FDA and others will say there is little evidence of success so far, but that’s a scandal in itself. Why are there no large trials? And why are other drugs like Remdesivir approved with only one trial? Ivermectin is so safe some 3.7 billion doses have already been used around the world. The inventors won a Nobel Prize for its discovery in 2015. We’ve known it might be useful since April last year, when an Australian group searched through many cheap safe drugs looking for any that might help against Covid. The news then was “Another possible cure for coronavirus, found in sheep dip: Ivermectin”. This was just a lab study, and it suggested doses would need to be too high. Even so, successes keep turning up in the real world? By July last year there were already signs Ivermectin could save as many as 50%. Why were large trials not started then? The UK trial is hobbled from the start.
LinkedIn censors interview with British cardiologist who criticized Pfizer vaccine data coverup
By Didi Rankovic | Reclaim The Net | November 11, 2021
LinkedIn has decided that a video about the efficacy of Covid vaccines, originally posted on YouTube and featuring Dr. Aseem Malhotra was violating its “professional community policies.”
Interviewer Maajid Nawaz posted a screenshot of the message he received from LinkedIn on Facebook, informing him of the removal and that only he can now see the post.
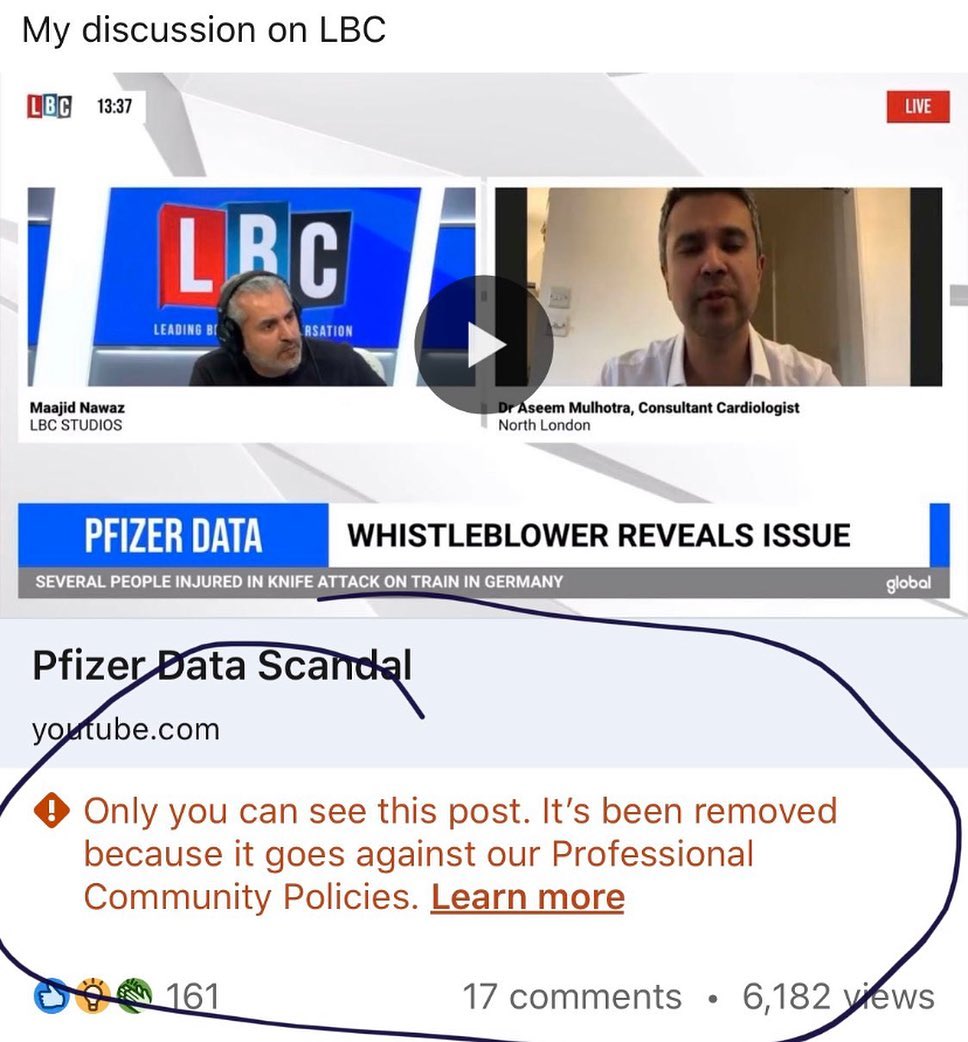
No other details for the censorship were given, other than a link presumably leading to LinkedIn’s policy page which requires users to be “safe, civil and respectful,” trustworthy by using their real identity and sharing “real and authentic” information, as well as make sure the content users posts is professionally relevant.
The video, which is still available on YouTube as of this writing, features Dr. Malhotra interviewed on the LBC talk radio station, posted under the headline, “Pfizer data scandal.”
Dr. Malhotra’s conversation with LBC’s Maajid Nawaz shown in the video focused on vaccine mandates, which he believes to be unethical, and the cardiologist’s belief that the healthcare crisis is the result of what he called “the corporate capture of public health.”
Dr. Malhotra also does not think that getting the jab has proved to significantly reduce transmission of the virus, he revealed during the interview, accusing Big Food and Big Pharma industries of chasing profits rather than looking for ways to improve health, and as more willing to pay billions in fines over the years, than changing their way of doing business.
He also commented on a whistleblower revealing that a Pfizer contractor was falsifying Covid vaccine trials data, which would mean that the effectiveness of the vaccine might have been overstated.
Speaking more broadly about the problem in the pharmaceutical industry and in the healthcare system, Malhotra said that clinical decisions are made on what he said were incomplete, biased, “and in many cases potentially corrupted data.”
The doctor also revealed that he was vaccinated with both doses earlier in the year believing he was protecting his patients from getting infected by him – but that he now thinks this belief was false.
“What’s now very very clear, as this data’s evolving,” Malhotra said, “is that there’s no significant reduction in transmission from taking the vaccine.”
However, he also noted that he thinks there is valid data showing the vaccine does prevent serious illness and death – but that healthy and young individuals likely don’t benefit from it.
welcome to the hospital california
you can check in any time you like, but there might not be any doctors…
el gato malo | bad cattitude | November 11, 2021
president brandon and his merry band of miscreants have been busy mandating covid vaccines for health care workers. many states have done so as well.
this is going to create severe staffing crunches.
18% of front line HCW’s are not planning to vaccinate.
this rises to 24% in nursing homes.
this winter when hospitals are having “weather disruptions” like american and southwest airlines because the winds of “i do not wish to be vaccinated against my will” among health workers are reaching gale force, just remember:
this is not covid.
this is bad policy.
this is literally an attempt by health officials to:
“make hospitals and assisted living facilities safe by preventing doctors and nurses from making healthcare choices.”
no sane public health official would do this.

this has NOTHING to do with a virus. if it did, you’d trust acquired immunity and the medical judgement of doctors.
these people are wreckers.
they WANT these systems to break. they want a hospital crisis because that will create “an emergency” that allows them to step in and regulate or grab control or nationalize.
do NOT fall for this. this is a game of chicken and the doctors who want to have their own bodies be their own choice are in the right.
support health workers as they strike and stand up for themselves.
they were there for us. be there for them.
not only is this the morally correct thing to do, but it’s also in your own self-interest if you ever again want to be able to have your own medical choices be between you and your chosen physician.
can you seriously believe that a system that will not allow doctors to make THEIR OWN healthcare choices can be trusted to let them help you make YOURS?
this is not about your health, it’s about their power. their regulatory edifice seeks to subsume all of healthcare and to do it, they’re seeking to BREAK all healthcare.
this will not be market failure.
this will be market sabotage.
be sure you blame the right people.
and be sure you repay wreckers with being wrecked in return.
Top NIH Unvaxxed Scientist Willing to Lose Job and License, Will Argue Against Vaccine Mandates in Livestreamed Ethics Review
By Megan Redshaw | The Defender | November 9, 2021
A senior bioethicist who heads a research team at the National Institute of Allergy and Infectious Diseases (NIAID) is taking the lead at the National Institutes of Health (NIH) in the debate over the ethics of COVID vaccine mandates.
Dr. Matthew Memoli, director of the Laboratory of Infectious Diseases at NIH, will argue against vaccine mandates during a Dec. 1 livestreamed roundtable session, which will be open to the public.
“There’s a lot of debate within the NIH about whether [a vaccine mandate] is appropriate,” David Wendler, a senior NIH bioethicist in charge of planning the session, told the WSJ. “It’s an important, hot topic.”
Memoli opposes mandates for the COVID vaccines authorized for emergency use in the U.S., and has chosen not to be vaccinated.
Memoli sought a religious exemption from the mandatory vaccine requirements imposed by health authorities in the District of Columbia, where he is licensed to practice medicine.
Memoli said he is willing to risk his job and his license for the right not to receive a COVID vaccine. During the scheduled roundtable early next month, he will make the case against mandates.
“I think the way we are using the vaccines is wrong,” Memoli said in a July 30 email to Dr. Anthony Fauci, director of the NIAID, and two of his lieutenants. Memoli called mandated vaccination “extraordinarily problematic.”
Memoli told the WSJ one of Fauci’s colleagues thanked him for his email. Memoli said he supports COVID vaccines for high-risk populations including the elderly and obese, but said, “blanket vaccination of people at low risk of severe illness could hamper the development of more-robust immunity gained across a population from infection.”
Memoli, a 16-year veteran at the NIH was selected this month for a 2021 NIH director’s award — a top recognition from the head of the agency, for his supervision of a national study into undiagnosed COVID cases early in the pandemic.
Memoli said his children have received their childhood vaccines, and he will support the results of the ethics discussion regardless of the outcome.
“I do vaccine trials. I, in fact, help create vaccines,” Memoli told the WSJ. “Part of my career is to share my expert opinions, right or wrong … I mean, if they all end up saying I’m wrong, that’s fine. I want to have the discussion.”
Christine Grady, head of NIH’s Clinical Center bioethics department and Fauci’s wife, approved the Dec. 1 seminar — a session called “Grand Rounds.”
Grady said in an email she believes there is interest in the topic across the agency.
“Our hope is that the December Grand Rounds will be relevant to the debates that are going on around the country regarding vaccine mandates,” an agency spokeswoman said on Grady’s behalf.
Federal appeals court temporarily halts Biden’s COVID vaccine mandate for private employers
A federal appeals court on Saturday issued a stay temporarily halting the Biden administration’s private-employer COVID vaccine mandate, citing, “grave statutory and constitutional” issues with the requirement.
“Because the petitions give cause to believe there are grave statutory and constitutional issues with the mandate, the mandate is hereby stayed pending further action by this court,” the U.S. Court of Appeals for the Fifth Circuit said in the order.
The case was brought by multiple businesses and several states, including Texas, Utah, Louisiana, South Carolina and Mississippi. They argued the requirements exceed the authority of the Occupational Safety and Health Administration (OSHA), which will enforce the mandates, and amount to an unconstitutional delegation of power to the executive branch by Congress.
The Biden administration on Monday asked the federal court to lift the order blocking the mandate for large private employers. The administration said the petitioners were not claiming a “major prospect of harm” from the rule, so the court should allow the mandate to proceed while the case makes its way through the system.
“Accordingly, there is no need to address petitioners’ stay motions now, and the court should lift its administrative stay and allow this matter to proceed under the process that Congress set forth for judicial review of OSHA standards,” lawyers for the administration argued.
The White House on Monday said businesses should move forward with Biden’s vaccine mandate for private businesses, despite a federal court order temporarily halting the rules, CNBC reported.
“People should not wait,” White House Deputy Press Sec. Karine Jean-Pierre told reporters during a press briefing. “They should continue to move forward and make sure they’re getting their workplace vaccinated.”
The OSHA regulation applies to employers with at least 100 workers, creating an emergency temporary rule that will require employers to mandate workers be vaccinated against COVID or submit to regular testing. A deadline for companies to comply with the regulation was set for Jan. 4.
Petitioners said the mandate, publicized as an emergency temporary standard by OSHA, should be struck down because it exceeds OSHA’s authority under the Occupational Safety and Health Act.
More than two dozen states have filed lawsuits against the Biden administration over the vaccine mandate for large private employers in the 5th, 6th, 7th, 8th, 11th and D.C. Circuits. Federal law dictates cases be consolidated and heard by one federal appeals court chosen by a lottery.
According to the U.S. Department of Justice, the lottery could take place on or around Nov. 16, and the case could make its way to the Supreme Court.
Megan Redshaw is a freelance reporter for The Defender. She has a background in political science, a law degree and extensive training in natural health.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Featured Video

“Trump’s presidency is at risk of being destroyed” Col Douglas Macgregor
or go to
Aletho News Archives – Video-Images
From the Archives
Mutually Assured Delusion (MAD)
By Judith Curry | Climate Etc. | November 5, 2013
Groupthink: A pattern of thought charaterized by self-deception, forced manufacture of consent, and conformity to group values and ethics.
Groupthink: Collective Delusions in Organizations and Markets, by Roland Benabou, published in the Review of Economic Studies. Benabou also has a talk (ppt slides) on this subject.
First, a definition of groupthink (from the ppt slides):
Janis (1972)’s eight symptoms [of groupthink]:
- illusion of invulnerability
- collective rationalization
- belief in inherent morality
- stereotyped views of out-groups
- direct pressure on dissenters
- self-censorship
- illusion of unanimity
- self-appointed mind guards
Sound like any groups that we know? … continue
Blog Roll
 Aletho News
Aletho News- “Trump’s presidency is at risk of being destroyed” Col Douglas Macgregor
- Iran has legal right to act in Hormuz, holds US responsible for disruptions: UN mission
- Sudan’s RSF leaders build Dubai property empire with UAE backing: Investigative group
- West losing leadership position to Global South: Russia’s president
- How Cognitive Science Explains Our Looming Nuclear Crisis
- Have the US and Israel killed non-proliferation?
- Moscow, Tehran to support each other amid US aggression: Russia’s defense minister
- Iran says EU’s insistence on sanctions hastens its ‘embarrassing descent into irrelevance’
- Argentina’s Javier Milei sells out his country for Israel
- Putting Nukes in Finland Won’t Make Country Safer, Finnish Politician Cautions
- If Americans Knew
- By Week’s End, Trump’s War Will Be Plainly Illegal
- CBS News Reportedly Ousts London Bureau Chief Over Differences With Bari Weiss Over Gaza Coverage
- State Department Says US Is in Conflict With Iran ‘At the Request’ of Israel
- What ceasefire? Israel won’t stop killing in Gaza, Lebanon – Daily Update
- Palestinians in Gaza Want to Rebuild Food Systems. Israel Isn’t Letting Them.
- Under Trump, Green Card Seekers Face New Scrutiny for Views on Israel
- Sheep Theft Sent Shockwaves Through a Palestinian Village. Then, a 12-year-old Boy Was Shot Dead
- Trump alum helps Israel mount AI influence campaign
- Dispatches From Catastrophe
- Despite Denials, AIPAC Is Now Funding Campaign of Ala Stanford In Philadelphia
- No Tricks Zone
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
