Pfizer Is Calling The Shots To Jab Kids
Dr. Joseph Mercola | November 1, 2021
In late February 2021, The Bureau of Investigative Journalism reported1 that Pfizer was demanding countries put up sovereign assets as collateral for expected vaccine injury lawsuits resulting from its COVID-19 inoculation.
While at least two countries, Argentina and Brazil, initially rejected the demands, calling them abusive, many others accepted Pfizer’s terms from the start.
Public Citizen has now reviewed and published the secret contracts2,3 between Pfizer and Albania, Brazil, Colombia, Chile, Dominican Republic, the European Commission, Peru, the U.S. and the U.K. These contracts reveal nations have handed over unprecedented power to Pfizer. In virtually all scenarios, Pfizer’s interests come first.
Pfizer Is Calling The Shots
Public Citizen points out six ways in which nations are allowing Pfizer to call the shots. For example, Albania, Brazil and Colombia have handed over unilateral authority to the company for the delivery schedule and other key decisions. As reported by Public Citizen:4
“As a condition to entering into the agreement, the Colombian government is required to ‘demonstrate, in a manner satisfactory to Suppliers, that Suppliers and their affiliates will have adequate protection, as determined in Suppliers’ sole discretion’ … from liability claims.
Colombia is required to certify to Pfizer the value of the contingent obligations (i.e., potential future liability), and to start appropriating funds to cover the contingent obligations, according to a contribution program.”
Pfizer also maintains tight control over vaccine supplies, and dictates who can buy their vaccine, when, and who can give and receive vaccine donations. If there are shortages, Pfizer decides which countries get priority.
Bypassing Pfizer can be costly. For example, if Brazil were to accept vaccine donations from another country without Pfizer’s approval, the company can terminate the contract and force Brazil to pay the full prize for all remaining contracted doses. Meanwhile, Pfizer incurs no penalty if its delivery is late, even if it’s so late that the shots are no longer needed.
Some countries, including Brazil, Chile, Colombia, the Dominican Republic and Peru, also ended up agreeing to Pfizer’s demand to put up sovereign assets as collateral for vaccine injury lawsuits, including bank reserves, military bases and embassy buildings.
In short, theses governments are guaranteeing Pfizer will be compensated for any expenses resulting from injury lawsuits against it, so the company won’t lose a dime if its COVID shot injures people — even if those injuries are the result of negligent company practices, fraud or malice!
At the same time, government purchasers must acknowledge that the effectiveness and safety of the shots are completely unknown. This is the ultimate corporate maleficence, using their leverage to force the kill shot down these countries’ throats and avoiding any personal responsibility for damages.
Secret Arbitration
The contracts also dictate how contractual disputes will be settled. As reported by Public Citizen:5
“What happens if the United Kingdom cannot resolve a contractual dispute with Pfizer? A secret panel of three private arbitrators — not a U.K court — is empowered under the contract to make the final decision. The arbitration is conducted under the Rules of Arbitration of the International Chamber of Commerce (ICC). Both parties are required to keep everything secret:
‘The Parties agree to keep confidential the existence of the arbitration, the arbitral proceedings, the submissions made by the Parties and the decisions made by the arbitral tribunal, including its awards, except as required by Law and to the extent not already in the public domain.’
The Albania draft contract and Brazil, Chile, Colombia, Dominican Republic, and Peru agreements require the governments to go further, with contractual disputes subject to ICC arbitration applying New York law. While ICC arbitration involving states is not uncommon, disputes involving high-income countries and/or pharmaceuticals appear to be relatively rare
Private arbitration reflects an imbalance of power. It allows pharmaceutical corporations like Pfizer to bypass domestic legal processes. This consolidates corporate power and undermines the rule of law.”
Pfizer Secured Intellectual Property Rights
Amazingly, the contracts not only secure Pfizer’s intellectual property rights, but should Pfizer be found guilty of stealing the intellectual property rights of others, some of the contracts shift the responsibility away from Pfizer onto the government purchasers! What this means is that Pfizer can steal the intellectual property of others without consequence in at least four countries.
“For example, if another vaccine maker sued Pfizer for patent infringement in Colombia, the contract requires the Colombian government to foot the bill,” Public Citizen writes.6 “Pfizer also explicitly says that it does not guarantee that its product does not violate third-party IP, or that it needs additional licenses.
Pfizer takes no responsibility in these contracts for its potential infringement of intellectual property. In a sense, Pfizer has secured an IP waiver for itself. But internationally, Pfizer is fighting similar efforts to waive IP barriers for all manufacturers.”
Pfizer Given Right To Silence Governments
Perhaps most egregious of all, some of the contracts give Pfizer the right to muzzle government. In Brazil, government officials are prohibited from making “any public announcement concerning the existence, subject matter or terms of [the] Agreement” without the written consent of the company.
The gag order also includes commenting on the government’s relationship with Pfizer in general. Similar nondisclosure provisions are included in the contracts with the European Commission and the U.S. government. The only difference, Public Citizen notes, is that the nondisclosure rules apply to both parties.
Pfizer Can Prevent Use Of Other Remedies
Equally shocking, though, is that countries are forced to follow through on their vaccine orders even if other drugs or treatments emerge that can prevent, treat or cure COVID-19.7 Is it any wonder, then, that governments around the world have suppressed the use of drugs like hydroxychloroquine and ivermectin?
If these drugs were allowed to be used and could be proven to work, the COVID injections would be completely unnecessary, yet governments are on the hook for hundreds of millions of doses. While COVID-19 vaccines are “free” to receive in the U.S., they’re being paid for by taxpayer dollars at a rate of $19.50 per dose. In Albania, the cost of each dose is $12, and in the EU, $14.70.
In the case of the price disparity between the U.S. and the EU, Pfizer is said to have given a price break to the EU because it financially supported the development of their COVID-19 vaccine.
As noted Public Citizen, Pfizer is being allowed to profit from this self-inflicted global disaster in unprecedented ways. In many instances, a nation’s laws will not apply to Pfizer.
These secret contracts grant Pfizer total control over its product and ensures full payment, regardless of whether the shots are needed or usable, while simultaneously eliminating all liability. In short, Pfizer wins, no matter what the outcome of the vaccination campaign might be.
At the same time, Pfizer is also controlling media through its advertising dollars. As you’ve probably realized by now, media companies in most instances will not report on anything that might jeopardize the profits of its advertisers.
As illustrated in the short video above, it couldn’t be more obvious that Pfizer is bankrolling the media, which in turn will refuse to bite the hand that feeds it. You can see the wide spectrum of media programming being sponsored by Pfizer, including “Nightline,” “Making a Difference,” “CNN Tonight,” “Early Start,” “Erin Burnett Out Front,” “This Week with George Stephanopoulos,” “CBS Sports,” “Meet the Press,” “CBS This Morning” and “60 Minutes.”
The terms of these contracts are all the more disturbing when you consider how dangerous the Pfizer shot is turning out to be. No wonder the company refused to accept any liability.
According to Pfizer’s own data, one COVID death per 20,000 fully vaccinated individuals is prevented. That means 10,000 lives are saved if 200 million are fully vaccinated.
But how many lives are lost from the shots? This is the other side of the equation that simply demands to be analyzed before any governmental authority can make a decision as to whether the mass vaccination campaign is of benefit or not.
Here, we find that Pfizer’s data10 show the shots are actually killing more than they save. To look at this information yourself, click on “Supplementary Material” on the right-hand side of the paper, then, beside Supplementary Appendix, click on supplements/261159 and scroll down to page 12, Table S4.
In the vaccine group, 15 died; in the placebo group 14 died. Two people died from COVID-19 in the placebo group, while only one died from COVID pneumonia in the vaccine group. That’s how you get a net false positive impact — one life is spared from COVID. However, the all-cause mortality was actually higher in the vaccine group (15, compared to 14).
So, while the shots saved one person from dying from COVID, they also killed one extra person. So, the net effect is nil. There’s no mortality benefit at all. Other investigations using different data strongly suggest the net effect is profoundly negative, and the shots are doing FAR more harm than good.
We Face Looming Vaccine-Induced Public Health Catastrophe
For this, Kirsch cites a paper11 by Dr. Bart Classen, published in the August 2021 issue of the journal Trends in Internal Medicine. Classen points out that Pfizer, Moderna and Janssen are all using a “dangerously misleading” clinical trial design. The problem is that they’re all using a surrogate endpoint for health, namely “severe infections with COVID-19.”
Disease specific primary endpoints are no longer used in many fields of medicine, for the fact that it can hide problems. If a person dies from the treatment or is severely injured by it, even if the treatment helped block the progression of the disease they’re being treated for, the end result is still a negative one.
For this reason, the appropriate endpoint that should be used is all-cause mortality and morbidity. When Classen reexamined the clinical trial data from all three manufacturers using all-cause severe morbidity as the endpoint, a disturbing picture emerged.
As explained by Classen in his paper, “US COVID-19 Vaccines Proven to Cause More Harm than Good Based on Pivotal Clinical Trial Data Analyzed Using the Proper Scientific Endpoint, ‘All Cause Severe Morbidity’”:12
“‘All-cause severe morbidity’ in the treatment group and control group was calculated by adding all severe events reported in the clinical trials. Severe events included both severe infections with COVID-19 and all other severe adverse events in the treatment arm and control arm respectively.
This analysis gives reduction in severe COVID-19 infections the same weight as adverse events of equivalent severity. Results prove that none of the vaccines provide a health benefit and all pivotal trials show a statistically significant increase in ‘all-cause severe morbidity’ in the vaccinated group compared to the placebo group.
The Moderna immunized group suffered 3,042 more severe events than the control group. The Pfizer data was grossly incomplete but data provided showed the vaccination group suffered 90 more severe events than the control group, when only including ‘unsolicited’ adverse events.
The Janssen immunized group suffered 264 more severe events than the control group. These findings contrast the manufacturers’ inappropriate surrogate endpoints:
Janssen claims that their vaccine prevents 6 cases of severe COVID-19 requiring medical attention out of 19,630 immunized; Pfizer claims their vaccine prevents 8 cases of severe COVID-19 out of 21,720 immunized; Moderna claims its vaccine prevents 30 cases of severe COVID-19 out of 15,210 immunized.
Based on this data it is all but a certainty that mass COVID-19 immunization is hurting the health of the population in general. Scientific principles dictate that the mass immunization with COVID-19 vaccines must be halted immediately because we face a looming vaccine induced public health catastrophe.”
To make the above numbers more clear and obvious, here are the prevention stats in percentages:
- Pfizer 0.00036 percent
- Moderna 0.00125 percent
- Janssen 0.00030 percent
CDC Claims COVID Shots Lower All-Cause Mortality
Despite all of that, the U.S. Centers for Disease Control and Prevention now claims Americans “vaccinated” against COVID-19 have lower all-cause mortality rates.13 As reported by Forbes:14
“Partially and fully vaccinated people died from non-coronavirus causes at a lower rate than their unvaccinated peers, according to the study,15 which looked at millions of patients at seven U.S. health organizations from December to July.
All three vaccines approved by U.S. regulators were tied to lower non-COVID death rates, though the difference in mortality among people who took Johnson & Johnson’s vaccine was slightly smaller than for recipients of Pfizer or Moderna’s vaccines …
This result suggests the vaccines don’t increase a patient’s risk of death, which ‘reinforces the safety profile of currently approved COVID-19 vaccines,’ the study said.”
October 26, 2021, the FDA unanimously voted to grant emergency use approval of the COVID shots for children between the ages of 5 and 11.16 This despite acknowledging they have no idea what the long-term risk to children might be. As noted by one voting member, “We’re never going to learn about how safe the vaccine is until we start giving it.”17
All we have at present is two Pfizer trials, one in which 5- to 11-year-olds were followed for two months and another with just six weeks of follow-up. Both were too small to detect potential risks such as myocarditis. That won’t be studied until AFTER the shot is authorized for children. As reported by The Defender :18
“Experts raised concerns over the lack of safety and efficacy data presented by Pfizer for use of its COVID vaccine in younger children, and they pointed to increasing safety signals based on reports to the Vaccine Adverse Event Reporting System (VAERS). They also questioned the need to vaccinate children — whose risk of dying from COVID is “almost nil” — at all.
According to Dr. Meryl Nass, member of the Children’s Health Defense Scientific Advisory Panel, Pfizer once again did not use all of the children who participated in the trial in their safety study.
‘Three thousand children received Pfizer’s COVID vaccine, but only 750 children were selectively included in the company’s safety analysis,’ Nass said.
‘Studies in the 5-11 age group are essentially the same as the 12-15 group — in other words, equally brief and unsatisfying, with inadequate safety data and efficacy data, with no strong support for why this type of immuno-bridging analysis is sufficient … All serious adverse events were considered unrelated to the vaccine’
Dr. Jessica Rose, viral immunologist and biologist, told the panel EUA of biological agents requires the existence of an emergency and the nonexistence of alternate treatment. ‘There is no emergency and COVID-19 is exceedingly treatable,’ Rose said.
In a peer-reviewed study19 co-authored by Rose, myocarditis rates were significantly higher in people 13 to 23 years old within eight weeks of the COVID vaccine rollout. In 12- to15-year-olds, Rose said, reported cases of myocarditis were 19 times higher than background rates …
Rose said tens of thousands of reports have been submitted to VAERS for children ages 0 to 18. Rose explained: ‘In this age group, 60 children have died — 23 of them were less than 2 years old. It is disturbing to note that ‘product administered to patient of inappropriate age’ was filed 5,510 times in this age group. Two children were inappropriately injected, presumably by a trained medical professional, and subsequently died.’”
During the meeting, Dr. Cody Meissner noted we don’t know whether the shot is safe for this age group, and the risk of COVID is extremely low. If the shot is authorized, mandates will likely follow, which would be “bad.”
Brownstone Institute is also objecting to the authorization. In an October 20, 2021, article,20 Paul Elias Alexander, Ph.D., a former assistant professor of evidence-based medicine and research methods, called the plan to vaccinate young children “absolutely reckless” and “dangerous based on lack of safety data and poor research methodology.”
Meanwhile, data show not a single child has died from COVID-19 who did not have a serious underlying health condition. Alexander reviews a lot of that data in his article.
Staggering Conflicts Of Interest
When you look at the roster of the FDA’s committee members21 who reviewed and voted to authorize the Pfizer shot for children as young as 5, the unanimous “yes” vote becomes less of a mystery. As reported by National File,22 they have staggering conflicts of interest. Members include:
- Gregg Sylvester — A former vice president of Pfizer Vaccines
- Arnold S. Monto — A paid Pfizer consultant
- Archana Chatterjee — A recent Pfizer research grant recipient
- Myron Levine — Mentor to Raphael Simon, senior director of vaccine research and development at Pfizer
- James Hidreth — President of Meharry Medical College, which administers Pfizer vaccines
- Geeta Swamy — Chair of the Independent Data Monitoring Committee for the Pfizer Group B Streptococcus Vaccine Program
- Steven Pergam — Proudly photographed taking a Pfizer vaccine
- Several people who are already on the record supporting coronavirus vaccines for children, including Ofer Levy, Jay Portnoy and Melinda Wharton
In addition to that, former FDA commissioner Scott Gottlieb is currently on Pfizer’s board of directors.
FDA Buries Data On Seriously Injured Children
With these shots now being pushed on young children, it’s more imperative than ever to understand how data are being massaged and manipulated to support the ongoing lunacy. Of particular concern is evidence that the U.S. Food and Drug Administration is burying data on children who were seriously injured in the vaccine trials. As reported by Aaron Siri on Substack:23
“Pfizer’s clinical trial for children aged 12-15 included only 1,131 children who were vaccinated and at least one of those children suffered a devastating, life-altering injury which, despite incontrovertible proof and the cries of both the victim and her parents, has not been appropriately acknowledged by Pfizer or the FDA.
Putting aside that one serious injury in a small trial should alone raise blaring alarm bells, one must ask: what other serious adverse events have been hidden and ignored by regulators?”
Siri tells the story of 12-year-old Maddie de Garay, who along with her two brothers were enrolled by her parents in Pfizer’s clinical trial. That decision has changed the lives of the entire family, possibly forever. Within 24 hours of her second dose, Maddie suffered crippling pain and systemic injuries.
Maddie is now wheelchair-bound and requires a feeding tube. Pfizer’s principal investigator initially claimed Maddie’s injuries were unrelated to the shot and treated her as a mental patient. Eventually, her injury was listed as “functional abdominal pain” in Pfizer’s report to the FDA.
“For a virus that rarely harms children, the need to assure safety of the Covid-19 vaccine is high. A study with only 1,131 children is underpowered. It will not pick up anything but the most common adverse events.
If what Maddie suffered will occur in 1/1,000 children, that would result in 75,000 children in this country suffering this serious injury. If it happens 1/10,000 children, that is 7,500 suffering this serious injury.
“It could be that the cure is worse than the disease. But that will only be known if there is a properly powered (a.k.a., sized) clinical trial with children,” Siri writes, adding that:
“International scientists have declared that ‘inadequately powered studies should themselves be considered a breach of ethical standards.’24 Without a clinical trial of sufficient size that reviews all potential adverse events, such as that experienced by Maddie, for a sufficient duration, this potentially catastrophic result will not be identified prior to authorization or licensure …
The real lesson is not that pharmaceutical companies, or the FDA should act better or do a better job. That just won’t always be the case. The real lesson is that civil and individual rights should never be contingent upon a medical procedure. Never.
Preserving those rights to choose whether to get a medical product, without any government coercion, is the final and ultimate safeguard.
Removing that right results in dangerous authoritarianism because just as the FDA will not admit to Maddie’s serious injury after having promoted this vaccine, politicians that mandate the vaccine will not want to later admit a mistake by repealing the mandate.”
FDA Sued To Access COVID Jab Trial Data
We’re now in a position where it’s near-impossible for many to refuse the COVID jab, and if injured, they cannot sue anyone for damages. Adding insult to injury, we don’t even have access to all the data governments are supposedly relying on to mandate these hazardous products.
To address this last point, an organization called Public Health and Medical Professionals for Transparency (PHMPT) is now suing25 the FDA after the agency refused to release the data on which it based its decision to approve Comirnaty.26
The FDA denied the PHMPT request for expedited processing of its Freedom of Information Act (FOIA) request on the basis that no “imminent threat to the life or physical safety of an individual” existed. Per the complaint:27
“… in an effort to ensure that the FDA acts in furtherance of its commitment to transparency, PHMPT seeks to obtain the data and information relied upon by the FDA to license the Pfizer Vaccine.
The importance of releasing to the public this information is also recognized under federal law which provides that: ‘After a license has been issued, the following data and information in the biological product file are immediately available for public disclosure unless extraordinary circumstances are shown: (1) All safety and effectiveness data and information. (2) A protocol for a test or study …’”
‘Just Say No’ To The COVID Shot
While U.S. authorities are doing their best to hide incriminating data and manipulating the rest to show some sort of benefit, common sense, medical facts and available data all point in the opposite direction. It’s crystal clear to me that children do not need the COVID shot, as their risk of serious COVID-19 infection and death is virtually nonexistent.
On the other hand, children are quite likely to be seriously injured by these injections. The reason you’re not getting the truth from the media is explained by Dr. Peter McCullough in the video above. In short, it’s a planned propaganda campaign — “the promotion of false information by the people in charge.”
According to McCullough, anyone under the age of 50 has a less than 1 percent chance of a bad outcome if they come down with COVID-19. “Why would you take the vaccine?” he asks. “My advice,” he says, “is just say no to this [shot], especially young people who are not at risk.”
Sources and References
- 1 The Bureau of Investigative Journalism February 23, 2021
- 2, 4, 5, 6 Public Citizen October 19, 2021
- 3 Twitter Zain Rizvi October 19, 2021
- 7 COVID19up.org August 17, 2021
- 8 SKirsch.io/vaccine-resources
- 9, 10 MedRxiv July 28, 2021
- 11, 12 Trends in Internal Medicine 2021; 1(1): 1-6 (PDF)
- 13, 15 CDC Morbidity and Mortality Weekly Report October 22, 2021: 70
- 14 Forbes October 22, 2021
- 16 ZeroHedge October 26, 2021
- 17 Twitter Techno Fog October 26, 2021
- 18 The Defender October 26, 2021
- 19 Curr. Probl. Cardiol. September 30, 2021; 101011
- 20 Brownstone Institute October 20, 2021
- 21 FDA Members Office of Vaccine Research and Review Meeting Roster
- 22 National File October 26, 2021
- 23 Aaronsiri.substack.com October 22, 2021
- 24 PLOS Medicine August 2008; 5(8): e172
- 25, 27 US District Court Northern District of Texas Case 4:21-cv-01058-P
- 26 Aaronsiri.substack.com October 11, 2021
Dodgy Climate Models Should be Discarded
By Chris Morrison • The Daily Sceptic • November 3, 2021
A devastating indictment of the accuracy of climate models is contained in a paper just published by the highly credentialed Physicist Nicola Scafetta from the University of Naples. Professor Scafetta analysed 38 of the main models and found that most had over-estimated global warming over the last 40 years and many of them should be “dismissed and not used by policymakers”.
But the majority still are. In the absence of conclusive proof that humans are causing all or most global warming, the science is deemed to be settled almost entirely on the basis of forecasts from models that have never been correct. And of course this lies at the heart of a drive to so-called net zero and the removal from human use of the one cheap and efficient fuel we all rely on to sustain a comfortable, healthy, modern lifestyle – namely, fossil fuel.
At the heart of the climate model problem is determining the equilibrium climate sensitivity (ECS). This is defined in climate science as the increase in the global mean surface temperature that follows a doubling of atmospheric CO2. Nobody knows what this figure is – the science for this crucial piece of the jigsaw is missing, unsettled you may say. So guesses are made and they usually range from 1C to as high as 6C. Models that use a higher figure invariably run hot and Professor Scafetta has proved them to be the least accurate in their forecasts.
Scafetta demonstrates this clearly in the graph (below). The thick green line is the actual average global temperature and all the other lines are the models’ projections. The red lines show the models that put the temperature at 6C. Interestingly, the models started to go haywire at a time when global warming was gaining political traction and debate on the science started to be discouraged. Perish the thought, of course, that the two are in any way related. Scafetta also goes into great detail about the performance of models in all latitudes and concludes “significant model data discrepancies are still observed over extended world regions for all models”.

Many scientists are highly sceptical about climate models. The reason the hypothesis that humans cause all or most global warming is unproven is that the atmosphere is too chaotic a place to pin the blame for warming (and cooling) on our meagre contribution to CO2 emissions, which accounts for about 3% of the total each year. Professor Scafetta points to the influence of the sun and other scientists look at the role of orbits, the moon, ocean currents, naturally occurring weather oscillations, volcanoes – the list is almost endless. We have little idea about the role of other greenhouse gases such as water vapour, which accounts for 6% of the atmosphere, and the way they all react with each other to increase, or decrease, their ability to trap heat.
More detailed research into this by Professor William Happer at Princeton has led him to conclude that a very low ECS, suggesting gentle if any warming, occurs when CO2 rises above the current atmospheric level of 420 parts per million. Far from being harmful, the extra CO2 is highly beneficial for plant growth and food. Slightly warmer temperatures can also be desirable. Homo Sapiens started in the tropics and only ventured out when the ice age started to lift – we like being warm and far more people die of the cold than the heat.
Failing to discuss the science behind climate change and simply blaming it all on humans is not science, it is anti-science, leading to faith-based green ideology. A plea for a more scientific approach was made two years ago by Professor Scaffeta along with a group of over 70 Italian scientists, including many distinguished academics, in a direct plea to Italian politicians. They stated that the human responsibility for climate change observed in the last century was “unjustifiably exaggerated and catastrophic predictions are not realistic”. Signatories of the letter included Antonino Zichichi, Professor emeritus of Physics and the discoverer of nuclear antimatter, and Renato Angelo Ricci, also an emeritus Professor of Physics and former President of the Italian Society of Physics. In total it was signed by 48 science professors. Needless to say it went unreported in the mainstream media at the time
The scientists said that climate models do not reproduce the observed natural variability of the climate of the past, notably the Medieval warm period and the hot Roman period, noted to be warmer than the present “despite the CO2 concentrations being lower than the current”. Of course, models are not alone in downplaying the balmy climate in medieval times. The IPCC produced its infamous hockey stick in 2001 to emphasise recent warming, but it disappeared quickly when the Climategate emails were published eight years later.
The Italian scientists were also of the opinion that the ECS is “considerably lower” than that estimated by the IPCC models. “The advanced alarmist forecasts, therefore, are not credible since they are based on models whose results contradict the experimental data,” they wrote. Natural variability, they said, “explains a substantial part of global warming observed since 1850″. Catastrophic predictions “are not realistic”.
And finally they have a swipe at the so-called 97% ‘settled’ consensus, a mad-up figure recently inflated to 99%. “In fact there is a remarkable variability of opinions among specialists – climatologists, meteorologists, geologists, geophysicists, astrophysicists – many of whom recognise an important natural contribution to global warming observed from the pre-industrial period and even from the post-war period to today.”
One minute to midnight to save the world, proclaimed Boris Johnson at COP26. Perhaps he forgot to put his clocks back last weekend.
Prominent Scientists Go Public: ‘Fauci Fooled America’
By Jeremy Loffredo | The Defender | November 2, 2021
In an op-ed, “Fauci Fooled America,” published Monday in Newsweek, two scientists accused Dr. Anthony Fauci of bungling the government’s response to COVID by getting “major epidemiology and public health questions wrong.”
Martin Kulldorff, Ph.D., an epidemiologist at Harvard Medical School, and Jay Bhattacharya, M.D., Ph.D., professor of Health Policy at Stanford University School of Medicine wrote: “Reality and scientific studies have now caught up with him.”
Kulldorff and Bhattacharya, both senior scholars at the Brownstone Institute and signers of the Great Barrington Declaration, had this message for Newsweek readers:
“The evidence is in. Governors, journalists, scientists, university presidents, hospital administrators and business leaders can continue to follow Dr. Anthony Fauci or open their eyes. After 700,000-plus COVID deaths and the devastating effects of lockdowns, it is time to return to basic principles of public health.”
The authors ticked off a list of “key issues” Fauci got wrong, including failure to recognize natural immunity, protecting the elderly, school closures, masks and contact tracing.
“By pushing vaccine mandates, Dr. Fauci ignores naturally acquired immunity among the COVID-recovered, of which there are more than 45 million in the United States,” the authors wrote. “Mounting evidence indicates that natural immunity is stronger and longer lasting than vaccine-induced immunity.”
Kulldorff and Bhattacharya cited a study from Israel, which concluded the vaccinated were 27 times more likely to get symptomatic COVID than the unvaccinated who had recovered from a prior infection.
They pointed out that the scientific community has known about natural immunity from disease “at least since the Athenian Plague in 430 BC.”
On Fauci’s dictates to mandate the vaccine for healthcare workers, the two argued: “Under Fauci’s mandates, hospitals are firing heroic nurses who recovered from COVID they contracted while caring for patients. With their superior immunity, they can safely care for the oldest and frailest patients with even lower transmission risk than the vaccinated.”
On school closures they wrote: “Considering the devastating effects of school closures on children, Dr. Fauci’s advocacy for school closures may be the single biggest mistake of his career … While children do get infected, their risk for COVID death is minuscule, lower than their already low risk of dying from the flu.”
Kulldorff and Bhattacharya pointed to Sweden, noting that during the 2020 spring wave of COVID, the country kept daycare and schools open for all 1.8 million children ages 1 to 15, with no masks, testing or social distancing.
According to the authors, Sweden’s strategy resulted in “zero COVID deaths among children and a COVID risk to teachers lower than the average of other professions.”
The authors argued contact tracing “was a hopeless waste of valuable public health resources that did not stop the disease,” and that Fauci failed at protecting the vulnerable.
“After more than 700,000 reported COVID deaths in America, we now know that lockdowns failed to protect high-risk older people,” they said.
On collateral public health damage, they argued that a “fundamental public health principle is that health is multidimensional; the control of a single infectious disease is not synonymous with health.”
They wrote that Fauci: “ … failed to properly consider and weigh the disastrous effects lockdowns would have on cancer detection and treatment, cardiovascular disease outcomes, diabetes care, childhood vaccination rates, mental health and opioid overdoses, to name a few. Americans will live with — and die from — this collateral damage for many years to come.”
In private conversations, Kulldorff and Bhattacharya said, most of their scientific colleagues agree with them on these points but few have spoken up out of fear of “financial censorship.”
“Many are afraid of losing positions or research grants, aware that Dr. Fauci sits on top of the largest pile of infectious disease research money in the world,” they wrote.
In his forthcoming book, “The Real Anthony Fauci,” Robert F. Kennedy, Jr. includes a comprehensive discussion of Fauci’s influence and power over the scientific community, revealing how Fauci uses the “financial clout at his disposal to wield extraordinary influence over hospitals, universities, journals and thousands of influential doctors and scientists — whose careers and institutions he has the power to ruin, advance or reward.” Kennedy’s book is due out Nov. 16.
Jeremy Loffredo is a freelance reporter for The Defender. His investigative reporting has been featured in The Grayzone and Unlimited Hangout. Jeremy formerly produced news programs at RT America.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
CDC Advisors Unanimously Endorse Pfizer’s COVID Vaccine for Kids 5-11 Despite Expert Concerns Over Clinical Data
By Megan Redshaw | The Defender | November 2, 2021
The Centers for Disease Control and Prevention’s (CDC) vaccine advisory panel today unanimously recommended Pfizer’s COVID vaccine for children 5 to 11, despite concerns raised during the meeting about Pfizer’s clinical data, the fact that children who previously acquired natural immunity to COVID were included in clinical trials and evidence showing COVID poses little risk to children.
If Dr. Rochelle Walensky, the CDC’s director signs off on the decision, children ages 5 through 11 could start receiving COVID vaccines as early as tonight.
The younger age group will receive one-third of the dose authorized for those 12 and older in two shots at least three weeks apart. The doses will be delivered by smaller needles and stored in smaller vials to avoid a mix-up with adult doses.
The CDC’s guidelines for the vaccine’s use are not legally binding, but heavily influence the medical community’s practice.
Prior to today’s decision by the CDC’s Advisory Committee on Immunization Practices (ACIP) the Biden administration enlisted more than 20,000 pediatricians, family doctors and pharmacies to administer the vaccines — with 15 million doses already packed with dry ice, loaded into small specialized containers and shipped via airplanes and trucks to vaccination sites across the country, federal officials said on Monday.
Walensky sent a clear signal during the ACIP meeting about where she stands, CNN reported. “We have been asking when we will be able to expand this protection to our younger children,” Walensky said in opening comments to the committee.
“As you review the data today, it will be key to keep in mind the specific risks to children from this virus and the pandemic, and to put that risk into context of other vaccine-preventable diseases,” Walensky said.
Walensky noted that children are routinely vaccinated against diseases like chickenpox — which results in far fewer hospitalizations and deaths in children compared to COVID.
During today’s meeting, ACIP members reviewed and discussed the science behind the U.S. Food and Drug Administration’s (FDA) authorization last week of Pfizer’s COVID vaccine in all children 5-11 years old.
That authorization was based mostly on a Pfizer-BioNTech study of 4,600 children worldwide, of whom approximately 3,100 got the low-dose vaccine and about 1,500 got a placebo.
These studies showed the vaccine is about 91% effective against COVID. The immune system response to the vaccine, as measured by antibodies, was comparable to the response seen in 16- to 25-year-olds, NPR reported.
During the meeting, the CDC said 745 children under 18 have died of COVID since the beginning of the pandemic — although the COVID-19 team admitted 79% were confirmed to be hospitalized for COVID, while the rest were hospital admissions for other causes.
“The chance that a child will have severe COVID, require hospitalization or develop a long-term complication like MIS-C [multisystem inflammatory syndrome] remains low, but still the risk is too high and too devastating to our children, and far higher than for many other diseases for which we vaccinate children,” Walensky said.
Efficacy of Pfizer’s COVID vaccine in children
The CDC said Pfizer’s COVID vaccine was 90.9% effective against symptomatic COVID and none of the adverse events experienced during clinical trials were assessed by “the investigator” as related to the vaccine.
To determine the efficacy of the Pfizer-BioNTech COVID vaccine, Pfizer measured the blood of 264 children for antibodies.
“There were 3,000 vaccinated children in the trial. Why isn’t blood from the other 2,700-plus being measured for antibodies?” asked Dr. Meryl Nass, a member of the Children’s Health Defense Scientific Advisory Panel.
“Pfizer never explains why, when they have an important clinical trial in which over 3,000 children were injected in this age group, only a subset of less than 10% were used to assess efficacy,” Nass said.
Nass explained:
“Pfizer claims three cases of COVID in the vaccinated group versus 16 in the placebo group show efficacy of the vaccine. But the FDA did not accept this claim. Note that all cases were mild, none hospitalized or died. So are they planning to vaccinate 28 million kids to prevent colds?”
Nass noted Pfizer also enrolled kids who had prior evidence of having had COVID in the clinical trial, “which should never have been allowed.”
“Of the kids who were already immune at the start of the trials, none developed COVID,” Nass said. “About 150 kids in the placebo group were recovered and none got COVID.”
Nass said kids with preceding COVID infection did not have their antibody levels checked after the first dose, as Pfizer stated they did not collect the data because they “tried to minimize blood draws in children.”
“The real reason they did not want to collect data is because it might support the fact that kids who already had COVID might only need one vaccine dose, or none at all,” Nass said.
During the brief public comment session, Patricia Neuenschwander, a registered nurse noted there was no prevention of hospitalization, death or multisystem inflammatory syndrome in children — a condition being used to justify vaccinating younger children against COVID, despite numerous cases of MIS-C having been reported after receipt of a COVID vaccine.
Neuenschwander reminded the ACIP that vaccinations do not prevent infection or transmission. It is a mild illness in the vast majority of children, she said, and prior immunity is being ignored — the expansion group was only followed for 17 days.
David Wiseman, a research scientist with a background in pharmacy, pharmacology and experimental pathology, asked the CDC panel why the efficacy study was not validated by the FDA, and why Pfizer changed the buffer [see page 14] in the vaccine but did not test it in animals or kids — planning to use an untested version of the vaccine in 5 to 11-year-olds.
Wiseman said the FDA abandoned its responsibility, and he asked if the ACIP would do the same.
Myocarditis and COVID in 5- to 11-year-olds
One side effect that generated considerable discussion at today’s meeting was myocarditis — a form of heart inflammation.
The CDC said 1,640 cases of myocarditis have been reported to the CDC’s Vaccine Adverse Event Reporting System in people under age 30 after having received a COVID vaccine, but only 877 met the CDC’s case definition.
The CDC said there were nine reported deaths in people with myocarditis, but then the agency reduced the number to three, with two cases pending evaluation and one case without adequate information.
“I have to say that it is beyond belief that CDC could whittle down 877 cases reported in young people to three actual cases. Where did the rest go?” Nass asked.
“According to the CDC’s Vaccine Safety Datalink, 7 of 16 12- to 17-year-olds with myocarditis were still on exercise restriction three months after diagnosis — that is 44% could not exercise three months later,” Nass said. “This is huge.”
Nass further noted 25% of 250 myocarditis cases were still symptomatic at three months, and only 74% of cases were designated by cardiologists as definitely resolved at 3 months.
As it pertains to safety, some who testified during a public comment period, as well as other commentators, questioned whether the study used by the FDA to grant Emergency Use Authorization is large enough to assure parents that the vaccine is safe in young children.
“The bottom line is getting COVID, I think, is much riskier to the heart than getting this vaccine,” said Dr. Matthew Oster, a pediatric cardiologist at Children’s Hospital of Atlanta.
Dr. Tom Shimabukuro covered vaccine safety monitoring from the CDC’s surveillance system in children. Shimabukuro said COVID is getting the “most intensive vaccine monitoring program in history,” yet he did not go into detail on surveillance data.
Acknowledging that some parents are hesitant about vaccinating their children right away, Dr. Matthew Daley, a member of the ACIP said, “we hear you loud and clear and of course you only want what’s best for your child. I encourage you to talk to your family physician or pediatrician, they can walk through this with you.”
Megan Redshaw is a freelance reporter for The Defender. She has a background in political science, a law degree and extensive training in natural health.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
The News is being Nudged
A joint report from Sky and the UK government’s Nudge Unit reveals a startling collaboration
By Laura Dodsworth | November 2, 2021
propaganda, n
The systematic dissemination of information, esp. in a biased or misleading way, in order to promote a political cause or point of view.
– Oxford English Dictionary
Is the news still news when it is being nudged by the UK government’s behavioural scientists?
Sky announced this week that behaviour change on climate can be driven by TV. It released a video which opened with the lines, “We cannot understate the urgency. But faced with issues of such enormity, what role can we play?”
It’s not actually a question, they have already decided their role. Sky announced that it was collaborating with the “independent Behavioural Insights Team”. That sounds more palatable than collaborating with the government doesn’t it? But the Behavioural Insights Team (BIT) is one third owned by the Cabinet Office and appears to be on permanent tenure at Downing Street. Can a company which is one third owned by the government be fairly described as “independent”?
BIT’s report The Power of TV: Nudging Viewers to Decarbonise their Lifestyles makes a number of startling admissions.
“Behaviour change via broadcasting and traditional media has historically been aimed at improving public health, boosting gender equality, and reducing violence. Imagine the potential for emissions reductions if the same methods were used to encourage sustainable behaviours!”
The key word is “historical”. If you have ever suspected that social and political issues were being confected somewhat artificially in TV programming, you were right. This is an admission of social engineering.
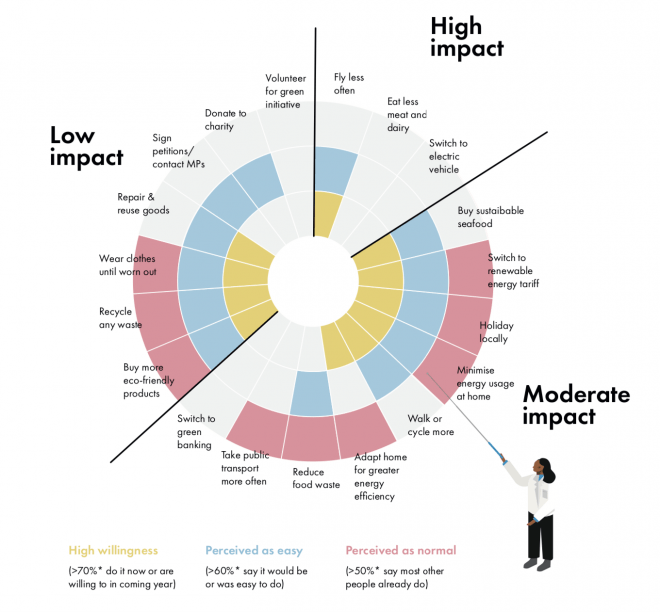
According to a joint survey by Sky and BIT, 70% of people across Europe are willing to change their behaviour to address the climate crisis and 80% support TV broadcasters ‘nudging’ viewers to think about the environment, whether that’s through documentaries, advertising or increasing the coverage of environmental issues in the news.
Climate policy is a tricky nut to crack – persuading us to have under-performing and expensive boilers, asking us to switch insects for meat, stop taking foreign holidays and drive our cars less is going to be a hard sell. So the nudgers are going to use the telly box to persuade the recalcitrant masses.
The survey itself uses ‘social conformity’. Ah, you are supposed to think, if 80% of people think TV programming should be used to ‘nudge’ us, then that’s what I think too. Notoriously, however, there is a gap between what people say they want in surveys and what they actually want. The ultimate proof will be in behaviour and ratings.
The report states that broadcasters and content creators have a “unique opportunity to make a difference for the planet”. (I wonder what difference it would make if Sky’s CEO stopped commuting transatlantically by private jet?)
According to the report, the British public are unwilling to take supposedly “high impact” actions, such as eating less meat and dairy, switching to electric vehicles, using public transport, and switching to green pensions.
The Power of TV: Nudging Viewers to Decarbonise their Lifestyles
The report is audaciously bossy about how broadcasters and content creators should change the British public’s behaviour.
Advice such as “Frequency of exposure to green themes could be enhanced by building ecological beliefs and traits into core characters within a show so that green issues can fluently be raised time and time again,” sounds potentially tedious.
You will see fewer characters “carelessly drinking from a plastic bottle”. But you will see more kids programming centre on green issues to influence you as well as the kids to promote “intergenerational spillover”.
Suggestions continue with “a family could discuss reducing their waste” in a comedy show. Making that funny is quite the gauntlet throw. News segments could “explore barriers to acting green and share stories for overcoming them,” which doesn’t sound particularly newsworthy. An episode of a drama could include references to buying an electric vehicle and, of course, characters should order vegetarian options in restaurants.
Plump the cushions, grab a cuppa and get ready for the green themes in your favourite psyopera, I mean soap opera. During COP26, storylines are converging on the environment. Soap ratings have diminished over the years and is it any wonder? People don’t want to be preached to. Creativity cannot be programmed and storytelling is an art. It is naïve arrogance to believe this sort of technocratic tinkering will engage viewers. We gravitate to good stories.
Mercifully, BIT suggests that broadcasters “avoid a negative tone” and warns that “fear-mongering, guilt-tripping, blaming, or preaching can be counter-productive.” (I wonder if a certain book had an impact?)
In addition to Sky, another eleven major UK media brands, including the BBC, ITV, Channel 4, RTE, Britbox and Discovery, have pledged to increase the amount and “quality” of their climate coverage. So expect the airwaves to be flooded with the techniques suggested in the BIT report. At the same time, expect very little media scrutiny of this astonishing collaboration between nudgers and newscasters. And in print and online, the BBC, The Guardian, The Times and the Financial Times have added specific climate sections to their news.
A few months after the publication of A State of Fear, a government advisor told me that the behavioural scientists are “very pleased with themselves” and “Britain is seen as leading the way in how to manipulate people. There is skipping in Whitehall corridors. The public have been proved to be incredibly sheepish, so there’s more nudge coming.” And so there is.
My book concluded that the UK government’s use of behavioural science during the Covid epidemic lacked transparency and was anti-democratic. BIT’s report might appear to rebut both accusations. Don’t be fooled. It rests upon a survey which says people want to be nudged through the media. But research conducted by biased and vested parties is not a substitute for a democratic mandate. The British public never voted for or consented to the creation of a Nudge Unit to subliminally influence them and then set the news agenda. Furthermore, when behavioural scientists – and by extension the government – influence the news, it risks the inquiry, debate and balance that the media owes the public.
Whatever you believe about climate, or Covid-19, or any other agenda, can any mental contortions justify the news being nudged? We would criticise such blatant propaganda if it happened in any other country and we should not tolerate here. We should switch it off.
What is the Number Needed to Vaccinate to prevent a single COVID fatality in kids 5 to 11 based on Pfizer’s EUA application?
And what are the risks that go along with injecting that many kids?
By Toby Rogers | October 31, 2021
Number Needed to Vaccinate (NNTV), the standard policy tool that Pharma, the FDA, & CDC no longer want to talk about
A funny thing happened this afternoon. Not funny as in “haha”. More like funny as in, “ohhhhh that’s how the FDA rigs the process.”
I was reading the CDC’s “Guidance for Health Economics Studies Presented to the Advisory Committee on Immunization Practices (ACIP), 2019 Update” and I realized that the FDA’s woeful risk-benefit analysis in connection with Pfizer’s EUA application to jab children ages 5 to 11 violates many of the principles of the CDC’s Guidance document. The CDC “Guidance” document describes 21 things that every health economics study in connection with vaccines must do and the FDA risk-benefit analysis violated at least half of them.
Today I want to focus on a single factor: the Number Needed to Vaccinate (NNTV). In four separate places the CDC Guidance document mentions the importance of coming up with a Number Needed to Vaccinate (NNTV). I did not recall seeing an NNTV in the FDA risk-benefit document. So I checked the FDA’s risk-benefit analysis again and sure enough, there was no mention of an NNTV.
Because the FDA failed to provide an NNTV, I will attempt to provide it here.
First a little background. The Number Needed to Treat (NNT) in order to prevent a single case, hospitalization, ICU admission, or death, is a standard way to measure the effectiveness of any drug. It’s an important tool because it enables policymakers to evaluate tradeoffs between a new drug, a different existing drug, or doing nothing. In vaccine research the equivalent term is Number Needed to Vaccinate (NNTV, sometimes also written as NNV) in order to prevent a single case, hospitalization, ICU admission, or death (those are 4 different NNTVs that one could calculate).
Pharma HATES talking about NNTV and they hate talking about NNTV even more when it comes to COVID-19 vaccines because the NNTV is so ridiculously high that this vaccine could not pass any honest risk-benefit analysis.
Indeed about a year ago I innocently asked on Twitter what the NNTV is for coronavirus vaccines.
Pharma sent a swarm of trolls in to attack me and Pharma goons published hit pieces on me outside of Twitter to punish me for even asking the question. Of course none of the Pharma trolls provided an estimate of the NNTV for COVID-19 shots. That tells us that we are exactly over the target.
Various health economists have calculated a NNTV for COVID-19 vaccines.
- Ronald Brown, a health economist in Canada, estimated that the NNTV to prevent a single case of coronavirus is from 88 to 142.
- Others have calculated the NNTV to prevent a single case at 256.
- German and Dutch researchers, using a large (500k) data set from a field study in Israel calculated an NNTV between 200 and 700 to prevent one case of COVID-19 for the mRNA shot marketed by Pfizer. They went further and figured out that the “NNTV to prevent one death is between 9,000 and 100,000 (95% confidence interval), with 16,000 as a point estimate.”
You can see why Pharma hates this number so much (I can picture Pharma’s various PR firms sending out an “All hands on deck!” message right now to tell their trolls to attack this article). One would have to inject a lot of people to see any benefit and the more people who are injected the more the potential benefits are offset by the considerable side-effects from the shots.
Furthermore, the NNTV to prevent a single case is not a very meaningful measure because most people, particularly children, recover on their own (or even more quickly with ivermectin if treated early). The numbers that health policy makers should really want to know are the NNTV to prevent a single hospitalization, ICU admission, or death. But with the NNTV to prevent a single case already so high, and with significant adverse events from coronavirus vaccines averaging about 15% nationwide, Pharma and the FDA dare not calculate an NNTV for hospitalizations, ICU, and deaths, because then no one would ever take this product (bye bye $93 billion in annual revenue).
Increased all cause mortality in the Pfizer clinical trial of adults
As Bobby Kennedy noted in personal correspondence with me, Pfizer’s clinical trial in adults showed alarming increases in all cause mortality in the vaccinated :
In Pfizer’s 6 month clinical trial in adults — there was 1 covid death our of 22,000 in the vaccine (“treatment”) group and 2 Covid deaths out of 22,000 in the placebo group (see Table s4). So NNTV = 22,000. The catch is there were 5 heart attack deaths in the vaccine group and only 1 in placebo group. So for every 1 life saved from Covid, the Pfizer vaccine kills 4 from heart attacks. All cause mortality in the 6 month study was 20 in vaccine group and 14 in placebo group. So a 42% all cause mortality increase among the vaccinated. The vaccine loses practically all efficacy after 6 months so they had to curtail the study. They unblinded and offered the vaccine to the placebo group. At that point the rising harm line had long ago intersected the sinking efficacy line.
Former NY Times investigative reporter Alex Berenson also wrote about the bad outcomes for the vaccinated in the Pfizer clinical trial in adults (here). Berenson received a lifetime ban from Twitter for posting Pfizer’s own clinical trial data.
Pfizer learned their lesson with the adult trial and so when they conducted a trial of their mRNA vaccine in children ages 5 to 11 they intentionally made it too small (only 2,300 participants) and too short (only followed up for 2 months) in order to hide harms.
Estimating an NNTV in children ages 5 to 11 using Pfizer’s own clinical trial data
All of the NNTV estimates above are based on data from adults. In kids the NNTV will be even higher (the lower the risk, the higher the NNTV to prevent a single bad outcome). Children ages 5 to 11 are at extremely low risk of death from coronavirus. In a meta-analysis combining data from 5 studies, Stanford researchers Cathrine Axfors and John Ioannidis found a median infection fatality rate (IFR) of 0.0027% in children ages 0-19. In children ages 5 to 11 the IFR is even lower. Depending on the study one looks at, COVID-19 is slightly less dangerous or roughly equivalent to the flu in children.
So how many children would need to be injected with Pharma’s mRNA shot in order to prevent a single hospitalization, ICU admission, or death?
Let’s examine Pfizer’s EUA application and the FDA’s risk-benefit analysis. By Pfizer’s own admission, there were zero hospitalization, ICU admissions, or deaths, in the treatment or control group in their study of 2,300 children ages 5 to 11.
So the Number Needed to Vaccinate in order to prevent a single hospitalization, ICU admission, or death, according to Pfizer’s own data, is infinity. ∞. Not the good kind of infinity as in God or love or time or the universe. This is the bad kind of infinity as in you could vaccinate every child age 5 to 11 in the U.S. and not prevent a single hospitalization, ICU admission, or death from coronavirus according to Pfizer’s own clinical trial data as submitted to the FDA. Of course Pfizer likes this kind of infinity because it means infinite profits. [Technically speaking the result is “undefined” because mathematically one cannot divide by zero, but you get my point.]
Estimating an NNTV and risk-benefit model in children ages 5 to 11 using the limited data that are available
Everyone knows that Pfizer was not even trying to conduct a responsible clinical trial of their mRNA shot in kids ages 5 to 11. Pfizer could have submitted to the FDA a paper napkin with the words “Iz Gud!” written in crayon and the VRBPAC would have approved the shot. They are all in the cartel together and they are all looking forward to their massive payoff/payday.
But let’s not be like Pharma. Instead, let’s attempt to come up with a best guess estimate based on real world data. Over time, others will develop a much more sophisticated estimate (for example, Walach, Klement, & Aukema, 2021 estimated an NNTV for 3 different populations based on “days post dose”). But for our purposes here I think there is a much easier way to come up with a ballpark NNTV estimate for children ages 5 to 11.
Here’s the benefits model:
- As of October 30, 2021, the CDC stated that 170 children ages 5 to 11 have died of COVID-19-related illness since the start of the pandemic. (That represents less than 0.1% of all coronavirus-related deaths nationwide even though children that age make up 8.7% of the U.S. population).
- The Pfizer mRNA shot only “works” for about 6 months (it increases risk in the first month, provides moderate protection in months 2 through 4 and then effectiveness begins to wane, which is why all of the FDA modeling only used a 6 month time-frame). So any modeling would have to be based on vaccine effectiveness in connection with the 57 (170/3) children who might otherwise have died of COVID-related illness during a 6-month period.
- At best, the Pfizer mRNA shot might be 80% effective against hospitalizations and death. That number comes directly from the FDA modeling (p. 32). I am bending over backwards to give Pfizer the benefit of considerable doubt because again, the Pfizer clinical trial showed NO reduction in hospitalizations or death in this age group. So injecting all 28,384,878 children ages 5 to 11 with two doses of Pfizer (which is what the Biden administration wants to do) would save, at most, 45 lives (0.8 effectiveness x 57 fatalities that otherwise would have occurred during that time period = 45).
- So then the NNTV to prevent a single fatality in this age group is 630,775 (28,384,878 / 45). But it’s a two dose regimen so if one wants to calculate the NNTV per injection the number doubles to 1,261,550. It’s literally the worst NNTV in the history of vaccination.
If you inject that many children, you certainly will have lots and lots of serious side effects including disability and death. So let’s look at the risk side of the equation.
Here’s the risk model:
- Because the Pfizer clinical trial has no useable data, I have to immuno-bridge from the nearest age group.
- 31,761,099 people (so just about 10% more people than in the 5 to 11 age bracket) ages 12 to 24 have gotten at least one coronavirus shot.
- The COVID-19 vaccine program has only existed for 10 months and younger people have only had access more recently (children 12 to 15 have had access for five months; since May 10) — so we’re looking at roughly the same observational time period as modeled above.
- During that time, there are 128 reports of fatal side effects following coronavirus mRNA injections in people 12 to 24. (That’s through October 22, 2021. There is a reporting lag though so the actual number of reports that have been filed is surely higher).
- Kirsch, Rose, and Crawford (2021) estimate that VAERS undercounts fatal reactions by a factor of 41 which would put the total fatal side effects in this age-range at 5,248. (Kirsch et al. represents a conservative estimate because others have put the underreporting factor at 100.)
- With potentially deadly side effects including myo- and pericarditis disproportionately impacting youth it is reasonable to think that over time the rate of fatal side effects from mRNA shots in children ages 5 to 11 might be similar to those in ages 12 to 24.
So, to put it simply, the Biden administration plan would kill 5,248 children via Pfizer mRNA shots in order to save 45 children from dying of coronavirus.
For every one child saved by the shot, another 117 would be killed by the shot.
The Pfizer mRNA shot fails any honest risk-benefit analysis in children ages 5 to 11.
Even under the best circumstances, estimating NNTV and modeling risk vs. benefits is fraught. In the current situation, with a new and novel bioengineered virus, where Pfizer’s data are intentionally underpowered to hide harms, and the FDA, CDC, & Biden Administration are doing everything in their power to push dangerous drugs on kids, making good policy decisions is even more difficult.
If the FDA or CDC want to calculate a different NNTV (and explain how they arrived at that number) I’m all ears. But we all know that the FDA refused to calculate an NNTV not because they forgot, but because they knew the number was so high that it would destroy the case for mRNA vaccines in children this age. Your move CDC — your own Guidance document states that you must provide this number.
The Vaccines Cannot Do What Is Asked of Them
eugyppius | November 1, 2021
Increasingly, politicians and medical bureaucrats are entranced by a bizarre pandemic ideology. Like most ideologies, it remains oblivious to evidence and argument, holding that the risk of severe outcomes from Corona infection is far more evenly distributed across the population than it is; and allowing only universal solutions, such as quarantining and vaccinating entire populations. These obtuse views, which just won’t go away, are at the root of our failed and destructive policies. For 20 months now, this pandemic ideology has blinded everyone in charge to the possibility of shielding the vulnerable, leveraging seasonal patterns in infection, and leaving the kids alone. The stratified nature of Corona risk is the key to unravelling the pandemic, and it’s the one thing nobody will recognise.
Success in the pandemic has come to be defined by a series of vague, poorly differentiated statistics, including above all Corona infections, hospitalisations and deaths, and now vaccination rates. In their exclusive focus on these numbers, the press propagate constantly the myth that this is all there is to know about Corona. This impoverished discussion drives bureaucrats and politicians to seek solutions for one vague meaningless metric (Corona ICU admissions) in another vague meaningless metric (vaccination rates). In this way their policies are constructed in a rhetorical world that has very little to do with what is actually happening.
Every day our understanding of what the vaccines can do becomes clearer. It’s not nothing, but it’s much less than we were promised.
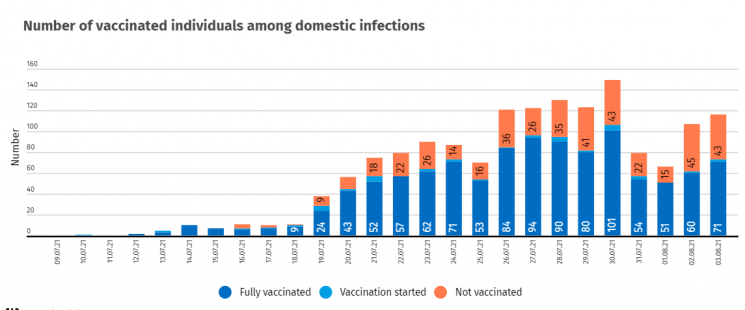
Some of our best evidence so far comes from this Swedish retrospective cohort study, which tracks outcomes in 1,684,958 individuals (matched vaccinated and unvaccinated pairs) from 12 January to 4 October 2021. It has been around the block, with an especially good analysis by El Gato Malo, so there’s no point in anything more than a brief review here.
Above all, they find that the vaccines provide temporary protection against infection:
![]()
Unfortunately, this protection likely falls below zero – into the zone of negative efficacy – after 7 to 9 months. This is one of multiple lines of evidence confirming that the vaccinated, sooner or later, achieve higher rates of infection than the unvaccinated. According to me, even early vaccine efficacy is likely overstated in studies like these. Probably the vaccinated are always highly vulnerable to infection, but they’re not tested as rigorously and at first their symptoms are so mild as to be nearly unnoticeable. SARS-2 nevertheless lurks among them, mostly undetected, until vaccine protection against overt disease dissipates.
This would explain what happened in Iceland over the summer: A bunch of freshly vaccinated Icelanders went on holiday in the UK, where they promptly picked up SARS-2 and brought the latest Delta update back home with them. In the following weeks, energetic Icelandic testing uncovered rates of infection almost as high in the vaccinated as in the unvaccinated – and this well before we would’ve expected the vaccines to have faded.
The Swedish study finds that efficacy against severe disease last longer, but also decays substantially in much the same way:
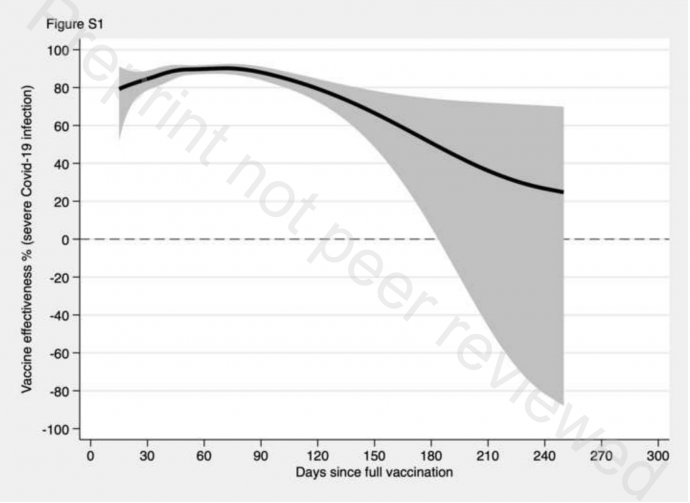
After the 240-day mark, protection against severe outcome is not even at 30%. The decay is most rapid among men, the old and frail, and those with comorbidities – precisely those subpopulations already at greatest risk of severe disease.
So those are the benefits, but as in everything there are also costs – and here they turn out to be substantial.
We’ve already touched on one: The vaccines appear to induce negative efficacy against infection. This probably arises from a combination of minimally symptomatic super-spreading among the vaccinated, the selective pressure that vaccine-elicited antibodies place upon the virus, and the narrow immunity against an obsolete arrangement of the spike protein that the vaccines confer. For a period of several weeks after dose 1 (and likely dose 3), they also make the vaccinated more susceptible to infection, and mass vaccination campaigns have induced case spikes across many countries.
By now it is also clear that the vaccines cause a range of adverse reactions. The best documented is myocarditis in young men, a side effect observed most frequently after dose 2 of the mRNA vaccines. We probably won’t know the true rate of vaccine-induced myocarditis for many years. From excess mortality in younger cohorts and many anecdotal media reports, we can surmise that it is much more common than anybody will admit.
It does not take a Ph.D. in public health to extract a sensible vaccination policy from all this:
1. There is just no question that vaccinating low-risk cohorts (including the recovered) is not only pointless, but also dangerous. These aren’t the people who end up in the hospital dying of Corona anyway. And because the vaccinated sooner or later end up driving transmission, there is only downside and no upside here.
2. All the vaccines are good for, is reducing the likelihood of severe disease among the old and the vulnerable. It follows that only the old and the vulnerable should be vaccinated.
3. In these groups, carefully timed annual vaccinations, like flu shots, might well provide good protection at the height of the winter coronavirus season and limit mortality. Even here, though, you’d have to proceed carefully, to avoid causing case spikes in the newly vaccinated during that brief period where their vulnerability to infection is heightened.
Of course, this is the opposite of what our pandemic ideology permits. Instead, almost all of our governments deploy the vaccines in the most reckless and counterproductive ways possible.
The southern districts of Bavaria are quickly becoming the regions of highest infection in Germany, and Markus Söder, our governor, is demanding a renewed “vaccine push,” including a campaign for booster doses “independently of age,” even obliquely threatening lockdown if we can’t ensure the “safety and stability” of hospitals.
These are exactly the kinds of crackpot universalist solutions that have failed for the past twenty months, and that will do nothing to unburden our healthcare facilities, and very likely end up swamping them with unnecessary patients.
If booster doses are a good idea for anyone – and it’s far from clear they are – it’s frail nursing home residents, most of whose vaccinations are now well past their expiration date, and who are once again beginning to die of SARS-2 just as they did last fall. Vaccinating children and triple vaccinating low-risk adults won’t prevent nursing home deaths, and it will do very little to keep our hospitals “safe,” because the vaccines don’t reduce spread and these people rarely end up in hospital. What is worse, ever newer pushes to vaccinate all hospital personnel and nursing home staff threaten to introduce vaccinated super-spreaders into these sensitive environments. Söder will continue to pound the table demanding ever harsher restrictions for the unvaccinated and more vaccine doses for the already-vaccinated, all while deaths and hospitalisations continue to climb.
Ultimately, the great problem with our vaccine policies, as with our lockdowns, arises from the fact that they don’t work. Because lockdowns and vaccination campaigns are powerless to remove the conditions that brought them about, you can never stop locking down, and you can never stop vaccinating – even as your policies turn out to do worse than nothing.
Blood Clots Associated with Johnson & Johnson COVID Shot
By Dr. Joseph Mercola | November 2, 2021
Researchers at Mayo Clinic have published a study in JAMA showing that there is a 3.5 times higher risk of getting brain blood clots if you take the Astra Zeneca or Johnson & Johnson COVID-19 shots.
Reported incidents of cerebral venous sinus thrombosis (CVST) after the jabs were what instigated a temporary pause in their rollout in April 2021. The researchers used data from the CDC’s Vaccine Adverse Event Reporting System (VAERS) to compare to data compiled in a Minnesota county from 2001 to 2015.
Study authors said women appeared to be more affected than men, although they couldn’t ascertain why. “Most CVST events occurred within 15 days after vaccination, which is likely the highest at-risk period,” they added. ‘The postvaccination CVST rate among females was higher than the prepandemic rate among females. The highest risk was among women aged 30 to 49 years.”
Is it Really True, as Climate Change Activists Claim, That 97% of Scientists Agree With Them?
By Luke Perry • The Daily Sceptic • October 27, 2021
Our Government is imposing draconian limitations on our lifestyles, our economy and our finances in order to achieve net zero carbon emissions to supposedly save the planet from catastrophic anthropogenic global warming (CAGW), now renamed as climate change. Probably one of the most repeated arguments you’ll hear, over and over again, in support of the need to achieve net zero is that “97% of scientists agree CAGW is happening”.
Former President Barack Obama is just one of many who have made this claim: “97% percent of scientists agree: climate change is real, man-made and dangerous.”
So did President Joe Biden’s Special Presidential Envoy for Climate, John Kerry, when he warned of the “crippling consequences” of climate change and that: “97% percent of the world’s scientists tell us this is urgent.”
This claim is widely accepted. Yet, in spite of the damaging effects reaching net zero will have on Western economies, not a single politician or journalist seems to have made the effort to find out where this ‘97%’ figure came from and how accurate it actually is.
Statistical smoke and mirrors?
The main author of the paper which came up with the famous 97% figure was an Australian former web programmer and blogger who later gained a PhD in Philosophy at the School of Psychology, University of Western Australia and then founded what could be seen as a climate alarmist website.
He assembled a group of volunteers as part of a ‘citizen science’ project and tasked them with”‘examining 11,944 climate abstracts from 1991-2011 matching the topics ‘global climate change’ or ‘global warming’”. Note that the volunteers didn’t read the actual scientific papers, they just looked at the abstracts – a summary paragraph or two describing what was in the papers. The volunteers then classed the abstracts into one of seven categories according to their opinions of Anthropogenic Global Warming (AGW):
1. Explicit endorsement of AGW with quantification
2. Explicit endorsement of AGW without quantification
3. Implicit endorsement of AGW
4. No position or Uncertain
5. Implicit rejection of AGW
6. Explicit rejection of AGW without quantification
7. Explicit rejection of AGW with quantification
The reviewers then ‘simplified’ results into four main categories as follows:
Endorse AGW 3,896 32.6% of abstracts
No AGW position 7,930 66.4% of abstracts
Reject AGW 78 0.7% of abstracts
Uncertain on AGW 40 0.3% of abstracts
So, this gave only 32.6% who, the reviewers concluded, endorsed AGW. This was clearly not quite the stunning super-majority of 97% which the study claimed to have identified. Now comes the clever bit. Instead of admitting that just 32.6% of papers (actually just abstracts of papers) endorsed AGW, the group decided to remove all the 7,930 abstracts which didn’t take a position on AGW. Then, hey presto, magic happened. That left just 4,014 abstracts of which 3,896 (97%) supposedly ‘endorsed’ AGW.
But that’s not the end of the magic employed to reach that wondrous 97%. The reviewers decided to lump together three categories of abstracts – Explicit endorsement with quantification; Explicit endorsement without quantification and Implicit Endorsement. But in the paper claiming 97% support for AGW, the reviewers don’t tell us how many papers fitted into each of these three categories. An independent researcher managed to get hold of the original data file and claimed to have found that in 3,896 abstracts which supposedly ‘endorsed’ AGW, just 64 were in the Explicit endorsement with quantification category; 922 were in the Explicit endorsement without quantification; and the vast majority – 2,910 (out of 3,896) – were in the Implicit endorsement of AGW category. Deciding from an abstract of a scientific article that the article ‘implicitly’ supports AGW is a bit like walking down a high street and deciding you know how people will vote based purely on looking at the kind of clothes they wear. To propose this as a serious survey is beyond ludicrous.
Thus, if this independent researcher’s figures are accurate, when you dig down into how the ‘97% of scientists’ figure was actually conjured up, you find that only 986 of 11,944 – that’s just 8.2% – of abstracts actually explicitly said they agreed with the theory of man-made global warming. And that’s clearly not the kind of figure the apocalypse-threatening climate catastrophists would really want to publicise too widely.
So, this ‘97% of scientists’ claim is based on about 11 to 12 volunteers, whose scientific credentials have not (as far as I know) been released and all of whom were probably firm AGW believers, each having to look at around 1,000, often quite obtuse, scientific abstracts. During this review, they decided whether they thought the scientific papers (which they hadn’t read as they had only looked at the abstracts) explicitly or implicitly supported the AGW theory. To claim such an approach is statistically valid is beyond farcical. Given the damage reaching net zero will do to our economies and our lives, it is beyond incredible that not a single politician, mainstream-media journalist or editor seems to have had either the ability or the inclination to expose the more than dubious origins of the almost ubiquitous ‘97% of scientists endorse AGW’ claim.
Featured Video

“Trump’s presidency is at risk of being destroyed” Col Douglas Macgregor
or go to
Aletho News Archives – Video-Images
From the Archives
Infertility: A Diabolical Agenda
Dr. Joseph Mercola | July 9, 2022
“Infertility: A Diabolical Agenda,” is the fourth vaccine-related documentary by Dr. Andrew Wakefield. It tells the story of an intentional infertility vaccine program conducted on African women, without their knowledge or consent.
While it’s been brushed off as a loony conspiracy theory for years, there’s compelling evidence showing it did, in fact, happen, and there’s nothing to prevent it from happening again. … continue
Blog Roll
 Aletho News
Aletho News- Continued US maritime piracy will face ‘practical, unprecedented’ response from Iran
- China discovers 225 large, medium-sized crude oil, natural gas fields from 2021 to 2025: Ministry of Natural Resources
- No More Bombs for Iran, Economic War Instead?
- “Trump’s presidency is at risk of being destroyed” Col Douglas Macgregor
- Iran has legal right to act in Hormuz, holds US responsible for disruptions: UN mission
- Sudan’s RSF leaders build Dubai property empire with UAE backing: Investigative group
- West losing leadership position to Global South: Russia’s president
- How Cognitive Science Explains Our Looming Nuclear Crisis
- Have the US and Israel killed non-proliferation?
- Moscow, Tehran to support each other amid US aggression: Russia’s defense minister
- If Americans Knew
- By Week’s End, Trump’s War Will Be Plainly Illegal
- CBS News Reportedly Ousts London Bureau Chief Over Differences With Bari Weiss Over Gaza Coverage
- State Department Says US Is in Conflict With Iran ‘At the Request’ of Israel
- What ceasefire? Israel won’t stop killing in Gaza, Lebanon – Daily Update
- Palestinians in Gaza Want to Rebuild Food Systems. Israel Isn’t Letting Them.
- Under Trump, Green Card Seekers Face New Scrutiny for Views on Israel
- Sheep Theft Sent Shockwaves Through a Palestinian Village. Then, a 12-year-old Boy Was Shot Dead
- Trump alum helps Israel mount AI influence campaign
- Dispatches From Catastrophe
- Despite Denials, AIPAC Is Now Funding Campaign of Ala Stanford In Philadelphia
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
