Magnesium Is a Cornerstone Mineral for Health
This article was previously published April 1, 2019, and has been updated with new information.
By Dr. Joseph Mercola
Magnesium is the fourth most abundant element in your body,1 and one of the seven essential minerals we can’t live without.2 It’s necessary for the healthy functioning of most cells, but especially your heart, kidneys and muscles. Low levels of magnesium impede cellular metabolic function and deteriorate mitochondrial function.
As it is also required for the activation of vitamin D, deficiency may hamper your ability to convert vitamin D from sun exposure and/or oral supplementation. Unfortunately, deficiency is common and research shows even subclinical deficiencies may jeopardize your health.
If you’ve recently had a blood panel drawn, you may assume it would reveal a magnesium deficiency. However, only 1% of magnesium is distributed in your blood, which means a blood test is not useful to determine whether you are deficient at the cellular level.3 Recent research confirms optimal levels of magnesium are necessary for your heart4 and kidney health.5
Magnesium Deficiency Affects the Vast Majority
Statistics show that at least 50% of Americans are deficient in magnesium, with some estimations going as high as 75% overall, and as many as 84% of postmenopausal women being deficient in it.6,7,8 Other scientists believe the deficiency affects the vast majority of individuals based on current dietary habits, saying:9
“[B]ecause of chronic diseases, medications, decreases in food crop magnesium contents and the availability of refined and processed foods, the vast majority of people in modern societies are at risk for magnesium deficiency.”
The recommended daily allowances (RDA) for magnesium are based on age, gender and pregnancy status.10 Although it may be difficult to pinpoint the exact percentage of individuals who suffer from magnesium deficiency, data do demonstrate subclinical levels of magnesium contribute to a number of widespread health problems.
The number who suffer from deficiency increases with an aging population as the elderly tend to consume less and don’t efficiently absorb magnesium from what is eaten.11
Digestive disorders, such as Crohn’s disease and celiac, may also affect magnesium absorption.12 Individuals who suffer from Type 2 diabetes13 or use diuretics may lose more magnesium through their urine.14
As the number of people suffering Type 2 diabetes is growing, and the age at which the condition arises is getting younger,15 the number who are also at risk for magnesium deficiency is also rising. Type 2 diabetes is associated with a number of health conditions also linked to magnesium deficiency, including heart disease and kidney disease.
Magnesium Integral to Arterial Health
Magnesium is required for energy production and is a cofactor in more than 300 enzyme systems that regulate biochemical reactions, including muscle and nerve function, and blood pressure regulation.16 Magnesium also helps regulate your blood vessels and helps prevent calcification known as coronary artery calcification (CAC).
CAC is an indicator of advanced atherosclerosis, a common predictor of cardiovascular disease and chronic kidney disease.17 In 1948, researchers undertook a nearly 70-year-long heart study under the direction of the National Heart Institute.
The Framingham Heart Study18 became a joint project of the National Heart, Lung and Blood Institute and Boston University with the objective to identify factors contributing to cardiovascular disease.
Magnesium Is Necessary for Optimal Heart and Kidney Health
Researchers19 recently examined data of magnesium intake in those free of cardiovascular disease at the beginning of the Framingham Heart Study and followed them over a period of 11 years.
They found a strong association between higher self-reported magnesium intake and lower calcification in the coronary arteries, which translates to lower risk of atherosclerosis and cardiovascular disease.
The researchers believe this may play a role in magnesium’s protective association in stroke and fatal coronary artery disease. The data also revealed a lower risk of abdominal aortic calcification,20 also associated with cardiovascular disease.21 A second study22 analyzed the associated risk of hypomagnesemia with diabetes and hypertension, which can contribute to a decline in kidney function.
The hypothesis was that subclinical levels contributed to a decline in glomerular filtration rate. Researchers engaged over 2,000 participants from the Dallas Heart Study. During a median follow-up of seven years, researchers evaluated glomerular filtration rate, biochemical parameters, C-reactive proteins and the prevalence of hypertension and diabetes.
The results led the researchers to conclude subclinical levels of magnesium were independently associated with decline in glomerular filtration rates indicating declining kidney function.23
Magnesium is a natural calcium antagonist and has several effects on vasodilation, regulation and changes in metabolism enhancing atherosclerotic changes in arterial stiffness, likely in part contributing to heart and kidney disease.24
Magnesium for Your Bone and Muscle Health
Magnesium contributes to the structural development of bone, and adult bone contains nearly 60% of the total magnesium in your body.25 As it is involved in bone formation, subclinical levels may contribute to the development of osteoporosis.
Research26 has found women with osteoporosis have lower serum magnesium levels than those without osteoporosis or osteopenia. Magnesium is also fundamental for physical performance.27 Just as it contributes to heart muscle contraction, skeletal muscles also require magnesium to relax muscle cramping and it is a cornerstone for circulatory health.
Magnesium is also important in energy regulation and plays a role in oxygen delivery and uptake in muscle. The relationship between magnesium and circulation also affects your brain. Dr. Maiken Nedergaard, co-director of the University of Rochester Center for Translational Neuromedicine, commented on the energy supply needed by the brain:28
“Our brains require a tremendous amount of energy and in order to meet this demand the flow of blood must be precisely choreographed to ensure that oxygen is being delivered where it is needed and when it is needed. This study demonstrates that microvessels in the brain play a key role in reacting to spikes in demand and accelerating the flow of blood to respond to neuronal activity.”
Magnesium Deficiency Affects Migraines, Anxiety, Depression
Although the brain is just 2% of your body weight, it uses nearly 20% of your oxygen supply in metabolic processes,29 remaining remarkably constant despite changes in mental and motor activities. Magnesium facilitates processing in the neural networks and is used to keep the blood-brain barrier healthy.30
Magnesium has proven to be essential for learning, concentration and memory and enables the brain’s plasticity, or its ability to adapt to challenges.31 Additionally, maintaining optimal levels of magnesium has proven effective in reducing the number of attacks and the number of days per month you may experience a migraine.32
In a comparison against valproate sodium, a medication used to help prevent migraine headache attacks, a randomized, controlled, double-blind study indicated 500 milligrams (mgs) of magnesium per day was an effective prophylaxis, similar to the effectiveness experienced by those taking valproate sodium, without side effects.
Anxiety disorders affect up to 13% of the population in the U.S.33 The condition may be debilitating, and like other mental disorders, it exists on a spectrum. Low levels of magnesium have been associated with increasing levels of noradrenaline, leading to a higher heart rate and blood pressure.
Conversely, optimal levels of magnesium may decrease the release of adrenocorticotropic hormone (ACTH), responsible for the controlled release of cortisol. Essentially, this means the release of fewer stress hormones and the modulation of the ones released.34
Optimal levels of dietary intake are also inversely associated with anxiety and depression.35 In an outpatient clinic treating 126 adults with mild to moderate symptoms, researcher found supplementation with magnesium chloride for six weeks resulted in clinically significant improvements in depression and anxiety without side effects.36
Higher Magnesium Intake Lowers Risk of Vitamin D Deficiency
Vitamin D levels below 20 nanograms per milliliter (ng/mL) or 50 nanomoles per liter (nmol/L) have repeatedly been shown to raise your risk of a number of health conditions, including depression and Type 2 diabetes. According to the most recent research, a vitamin D level between 60 and 80 ng/mL (150 and 200 nmol/L) appears to offer the greatest protection against cancer and other chronic diseases.37
Adequate vitamin D levels may also help prevent or treat dry eye syndrome,38 macular degeneration,39 neurological diseases,40 fractures41 and obesity.42 Adequate levels of vitamin D also lower your mortality risk associated with heart disease,43 and may lower your risk of mortality from all causes.44
However, without adequate levels of magnesium, any vitamin D supplementation may be ineffective,45 as magnesium is required for the activation of vitamin D, and vitamin D may trigger vascular calcification if magnesium and vitamin K2 levels are not optimal.46 Higher levels of magnesium may actually lower your risk of vitamin D deficiency by allowing for the activation of more vitamin D.47
Magnesium — Supplementation and Natural Sources
One of the biggest culprits behind deficiencies is processed foods, which unfortunately has become a staple in the American diet. Some of the magnesium rich foods you may add to your diet include:48,49
- Spinach
- Swiss chard
- Avocado
- Papaya
- Bok Choy
- Beet greens
- Turnip greens
- Seeds and nuts, such as pumpkin seeds, sesame seeds, cashews and raw almonds
- Fatty fishes like wild-caught Alaskan salmon
- Dried seaweed or agar
- Brussels sprouts
An interesting number of factors may affect your ability to absorb magnesium from your foods. Herbicides like glyphosate act as agricultural chelators, effectively obstructing the uptake of minerals from the soil in many foods grown today. As a result, it may be quite difficult to find truly magnesium-rich foods. Cooking and processing further depletes magnesium.
Meanwhile, certain foods may actually influence your body’s absorption of magnesium. High levels of sugar intake may trigger excretion of magnesium through your kidneys, “resulting in a net loss,” according to Dr. Danine Fruge, associate medical director at the Pritikin Longevity Center in Florida.50
When it comes to oral supplementation, my personal preference is magnesium threonate, as it appears to be the most efficient at penetrating cell membranes, including your mitochondria and blood-brain barrier. Other effective ways to boost your magnesium level include:
•Taking Epsom salt (magnesium sulfate) baths, as the magnesium will effectively absorb through your skin.
•Using a topical solution — I prepare a supersaturated solution of Epsom salt by dissolving 7 tablespoons of the salt into 6 ounces of water and heating it until all the salt has dissolved. I pour it into a dropper bottle and then apply it to my skin and rub fresh aloe leaves over it to dissolve it.
This is an easy and inexpensive way to increase your magnesium and will allow you to get higher dosages into your body without having to deal with its laxative effects.
Magnesium can be taken with or without food. If you’re also taking calcium, take them together. If you exercise regularly, consider taking your calcium and magnesium in a ratio of one part calcium to two parts magnesium with your pre-workout meal.
While the ideal ratio of magnesium to calcium is thought to be 1-to-1, most people get far more calcium than magnesium from their diet, so your need for supplemental magnesium may be two to three times greater than calcium.
Sources and References
- 1 Austin Journal of Nutrition and Food Sciences, March 31, 2015
- 2 Michigan Medicine, University of Michigan, March 28, 2018
- 3, 9 Open Heart, 2018;5(1):e000668
- 4, 32 Acta Neurologica Belgica 2019; doi: 10.1007/s13760-019-01101-x [Epub ahead of print]
- 5, 22, 23 Journal of Investigative Medicine, 2019; doi: 10.1136/jim-2018-000966
- 6 Nutrition Today, May/June 2016
- 7 American Family Physician, July 15, 2009
- 8 BMJ Open Heart, 2018
- 10, 16, 25 National Institutes of Health, Magnesium
- 11 Geriatric Nephrology and Urology, 1994;4:101
- 12 Crohn’s Colitis Foundation, Diet, Nutrition and Inflammatory Bowel Disease
- 13 World Journal of Diabetes, 2015;6(10):1152
- 14 Drugs 1984 Oct;28 Suppl 1:167-81
- 15 American Diabetes Association, Statistics About Diabetes
- 17 National Heart, Lung and Blood Institute, Atherosclerosis
- 18 Framingham Heart Study, History of the Framingham Heart Study
- 19, 20 JACC Cardiovascular Imaging, 2014;7(1):59
- 21 Korean Journal of Family Medicine, 2013;34(3):213
- 24 International Journal of Molecular Sciences, 2018; 19(6):1724
- 26 Journal of International Medical Research, 2007;35(5):692
- 27 Strength and Conditioning Journal, 2010;32(1)
- 28 University of Rochester Medical Center, August 8, 2016
- 29 PNAS, 2002;99(16):10237
- 30 Molecular Neurobiology, 2018;55(9):7118
- 31 Magnesium Research, 2006;19(3):199
- 33 Pharmacy and Therapeutics, 2013;38(1):30
- 34 Magnesium in the Central Nervous System, Cuciureanu, M., Vink, R.
- 35 Australian and New Zealand Journal of Psychiatry, 2009;43(1):45
- 36 PLOS|One 2017;12(6): e0180067
- 37 European Journal of Cancer 2005 May;41(8):1164-9
- 38 Endocrinology Advisor August 24, 2015
- 39 JAMA Ophthalmology August 27, 2015;133(10):1171-1179
- 40 The Journals of Gerontology 2012 Nov;67(11):1205-11
- 41 American Journal of Clinical Nutrition July 2006: 84(1); 18-28
- 42 Clinical Nutrition 2012 doi.org/10.1016/j.clnu.2012.08.014
- 43 J Clin Endocrinol Metab 2013;98:2160-2167
- 44 American Journal of Public Health, 2014;104(8):e43
- 45 Science Daily. Low Magnesium Levels Make Vitamin D Ineffective. February 26, 2018
- 46 Eurekalert February 27, 2018
- 47 BMC Medicine 2013; 11: 187
- 48 Medical News Today, July 26, 2017
- 49 Cleveland Clinic, Magnesium Rich Food
- 50 CNN, December 31, 2014
July 16, 2022 Posted by aletho | Science and Pseudo-Science, Timeless or most popular | Leave a comment
A ‘Vaccine-Palooza’ Is Underway, Thanks to COVID — But Will Public Accept Endless Jabs?
The Defender | July 12, 2022
Two-and-a-half years ago, the Grand Poobahs of global vaccinology admitted — in behind-closed-door confessions caught on camera at the World Health Organization (WHO) — that public and professional confidence in vaccines was “wobbly,” and deservedly so.
As the gathered experts conceded, the glaring inadequacies of vaccine safety science and the dysfunctional safety monitoring systems that permit routine “obfuscation” of serious adverse events were understandable reasons for public distrust.
At the time, it seemed as though such momentous disclosures would presage a death knell for vaccine “business as usual” — but then along came COVID-19, and with it, the instant memory-holing of the WHO’s stunning admissions.
Rather than finally address the self-confessed vaccine disaster, public health officials and global leaders — ranging from presidents to private-sector employers to top military brass to central bankers — used COVID-19 as an opportunity to double down in the opposite direction, forcibly stuffing the “vaccine hesitancy” genie back in the bottle with ethically untenable vaccine mandates.
After 18 months of force-feeding the COVID-19 jabs, however, manufacturers are now discarding tens of millions of doses “amid sagging demand.”
In some respects, this could be construed as evidence of policy failure, but the fact is that the COVID-19 shots accomplished a significant goal for the parties that pushed them, launching a renewed vaccine gold rush that — with growing emphasis on voguish, biotech-reliant biopharmaceuticals — seems likely to extend well beyond the COVID-19 era.
As the head of Bayer’s pharmaceuticals division observed in late 2021, mRNA vaccine technology and other forms of cell and gene therapy — for all of their by now well-documented and even species-threatening dangers — have crossed over both the regulatory and public palatability threshold.
Pfizer, Johnson & Johnson (J&J), AstraZeneca, Sanofi and Eli Lilly — some of major players in the biopharma space — are actively prioritizing “strategic alliances” and “collaborations to expand their [biopharmaceutical] product portfolios.”
Meanwhile, the U.S. Food and Drug Administration (FDA) and Centers for Disease Control and Prevention (CDC) are poised to roll out, at breakneck speed, approvals and recommendations for whatever new childhood and adult vaccines are sent their way.
In short, using technologies both “conventional” and new, a multipronged effort is afoot to jump-start and ensure a frenzied vaccine-palooza.
The mRNA pipeline
Having succeeded in foisting COVID-19 mRNA injections on an initially unsuspecting public, manufacturers and government agencies like the National Institutes of Health (NIH) are now salivating at the prospect of an endless series of mRNA vaccines.
It is no coincidence that the mRNA jabs in the works target some of the very conditions being reported as COVID-19 vaccine adverse events, a neat “create-a-problem, develop-a-drug-to-manage-the problem” trick that accounts for many other drugs already on the market.
In the pipeline are mRNA vaccines for the following:
- Cancer: Researchers are conducting dozens of clinical trials to test “mRNA treatment vaccines in people with various types of cancers.” Dr. Ryan Cole, a pathologist, described the dramatic surge in endometrial and other cancers following the rollout of COVID-19 shots.
- Shingles: Cole and others also noted the uptick of shingles in COVID-19 vaccine recipients. Moderna in March announced its development of an mRNA shingles vaccine, as well as mRNA vaccines for herpes and cancer.
- Other forms of immune suppression: With numerous indications that COVID-19 shots are reprogramming the immune response, officials and manufacturers are dusting off HIV as the supposed bogeyman. Moderna and NIH are partnering in mRNA vaccine clinical trials for HIV. This would represent a particular coup for Dr. Anthony Fauci, who over four decades has found development of an HIV vaccine to be “a daunting scientific challenge.”
- Heart attacks: Cardiac problems are among the few COVID-19-vaccine-related adverse events grudgingly acknowledged by manufacturers and the FDA. In the U.K., researchers are investigating the use of “exactly the same technology as the Pfizer and Moderna vaccines to inject micro RNAs to the heart,” claiming they can get whatever heart cells survive after a heart attack to proliferate.
- COVID and influenza: Manufacturers also are gearing up for a new generation of mRNA-based flu shots and mRNA combination vaccines which, they promise, will “protect against several different infections at the same time, such as influenza, COVID-19 and other respiratory infections.”In the meantime, CDC just recommended that seniors (aged 65 years or older) receive “enhanced” flu shots — either high-dose, adjuvanted or recombinant — in lieu of “standard-dose unadjuvanted, inactivated vaccines.” Adjuvanted influenza vaccines feature a new generation of “smart” vaccine adjuvants designed to ensure even the most mediocre vaccine sends recipients’ immune systems into overdrive.
For babies — something old, something new
In June, the FDA reaffirmed its long-standing allegiance to an agenda of guaranteed harm when it authorized emergency use COVID-19 shots for infants as young as 6 months old.
After the conflict-of-interest-riddled FDA advisors’ 21-0 vote, Rep. Louie Gohmert (R-Texas) commented, “[I]n balancing the risk to rewards here, all the risks are to the innocent children and all of the billion-dollar rewards go to the government-protected pharmaceuticals.”
Seizures and psychosis are already being reported as adverse events in the under-5 age group.
In decrying FDA’s decision to give COVID-19 shots to tots, some dissenters waxed nostalgic about the perceived “rigor” of the pre-COVID-19 vaccine approval process, seemingly amnesiac about the FDA’s lengthy history of regulatory capture and business-friendly shortcuts.
As a reminder, at least two-thirds of the vaccines approved by the FDA from 2006 through late 2020 benefited from “flexibility in the evidence required for approval,” resulting in accelerated approvals.
This “turn-a-blind-eye” pattern also held sway in the FDA’s and CDC’s recent decisions to pile on two more options to the childhood schedule, options that will do nothing to improve the safety of measles-mumps-rubella (MMR) and pneumococcal conjugate vaccines (PCV) that have been injuring children for decades.
First, on June 3, the FDA approved GlaxoSmithKline’s (GSK’s) Priorix, an MMR vaccine initially launched in Europe in the late 1990s.
GSK developed Priorix using the MRC-5 cell line (derived from the lung tissue of a male fetus aborted at 14 weeks).
A 2020 analysis by the Italian association CORVELVA of a version of Priorix that also contains a varicella component found that the amount of DNA in the vaccine was “well above the allowed threshold,” and that continuous use of the cell line over time resulted in “vaccines containing progressively more and more modified human genetic material, that is dangerous for the health of the vaccinees themselves.”
The FDA’s go-ahead for Priorix shatters Merck’s position as the sole U.S. purveyor of MMR vaccines. Previously, FDA showed no sign of being troubled by Merck’s monopoly, despite the pharmaceutical behemoth being dogged by “a slew of controversies” that included whistleblower allegations of MMR-related fraud and undeniable evidence of a link with autism.
Moreover, as Children’s Health Defense Chairman Robert F. Kennedy, Jr. pointed out in late 2019, when the FDA belatedly began to “tee up” Priorix as a replacement for Merck’s scandal-ridden MMR-II, rather than use an inert placebo to test Priorix, the FDA allowed GSK to use MMR-II as the comparator!
Even these sham clinical trials, Kennedy noted, had “horrifying” results. Within 42 days, nearly 50% of recipients of both manufacturers’ formulations experienced adverse events, with over 10% ending up in the emergency room. By six months, almost 4% of recipients had been diagnosed with a “new onset chronic disease.”
To date, the European Medicines Agency (EMA) has received more than 37,000 adverse event reports for Priorix and another 11,000-plus for the varicella-containing version — with 58% and 79% of adverse events, respectively, occurring in the under-two age group that will now receive the jabs in the U.S.
Following the nominal slap on the wrist for Merck’s MMR-II, the FDA and CDC also offered Merck some good news, approving on June 17 and then recommending — for routine use in infants and children 6 weeks to 2 years of age — the company’s 15-valent PCV15 (brand name “Vaxneuvance”) as an interchangeable alternative to Pfizer’s Prevnar 13 (PCV13).
The CDC stopped short of issuing a “preferential recommendation” for PCV15, however. Admitting to “certain uncertainties, including concerns related to potentially higher reactogenicity” — with “reactogenicity” defined as the “state of being able to produce adverse reactions” — the CDC leaves it up to the hapless infants who receive Vaxneuvance to discover the shots’ “higher reactogenicity” for themselves.
Even without the addition of Vaxneuvance to the schedule, pneumococcal conjugate vaccines — with ingredients like aluminum and polysorbate 80 — have shown themselves plenty capable of wreaking havoc on the health of the infants expected to get four doses by the time they are 12 to 15 months old.
Eager to add even more injections to the childhood vaccine schedule, the industry is also eyeing as a potential cash cow a pediatric (and adult) mRNA vaccine against respiratory syncytial virus (RSV).
In 2019, 30 candidate RSV vaccines were in the pipeline, and in 2021, the FDA fast-tracked an mRNA-based RSV vaccine developed by Moderna.
HPV downsizing — getting HPV shots into young people by any means necessary
The competition between Merck and GSK is also fierce where human papillomavirus (HPV) vaccines are concerned.
In the U.S., Merck’s Gardasil (and later, Gardasil 9) handily beat out GSK’s Cervarix, which is no longer available to American youth — but with 100 or more countries having added HPV jabs to their national vaccination schedules, much more than the U.S. market is in play.
Data suggest HPV vaccine coverage in the U.S. starts out relatively high, with an estimated 66% of 13- to 17-year-olds getting a first dose, but the percentage completing the series (an additional one to two doses) drops off to 49%.
Worldwide, acceptance of HPV vaccines is even lower — for girls, global coverage is estimated at about 15% of those in the target age range.
Undoubtedly, one of the reasons for the global public’s lukewarm stance on HPV vaccination is the occurrence of serious adverse autoimmune reactions that have left many recipients, both female and male, disabled for life.
Merck is mired in lawsuits (with attorneys, including Kennedy) alleging it knowingly concealed Gardasil-associated adverse events.
Rather than re-evaluate — as some researchers have strongly urged — the adverse event profile that, until COVID-19 shots, made HPV vaccines some of the most dangerous on the market, agencies like the National Cancer Institute (NCI) are instead beginning to argue in favor of single-dose HPV vaccination (either Cervarix or Gardasil 9).
Punting to a one-dose regimen would, NCI officials disingenuously say, “simplify the logistics of vaccination, which could allow more girls [and boys] worldwide to be vaccinated.”
Monkeypox profiteering
As Rob Verkerk, Ph.D., reported last month, the suspected case definition of monkeypox is broad enough to include anyone with a common cold — or with post-COVID-19-vaccine immune suppression — who has a shingles rash.
Verkerk’s counsel is to worry about “what the WHO and collaborating institutions, governments and corporations are up to,” rather than succumb to fear-mongering about monkeypox itself.
In the U.S., what the government is “up to” is ordering more than 4 million doses of monkeypox vaccine — a whitewashed smallpox vaccine linked to heart inflammation — and formulating a “national monkeypox vaccine strategy,” including a protocol aimed at the vaccine’s use in children.
In other words, with a “COVID-19 corporatocracy playbook” that, in Verkerk’s words, “is now well and truly oiled,” corporate and government leaders of ill intent appear to believe they can continue to play the vaccine game indefinitely, using “fear and manipulated science to engender support for the global control of health.”
It is up to us to prove them wrong.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
July 15, 2022 Posted by aletho | Science and Pseudo-Science, Timeless or most popular | CDC, COVID-19 Vaccine, FDA, United States | Leave a comment
There’s something wrong with Joe
Paul Joseph Watson | July 14, 2022
Democrats are starting to panic.
INTRO MUSIC: Sagittarius V – Lucidator: http://sagittariusvmusic.bandcamp.com
July 15, 2022 Posted by aletho | Timeless or most popular | Joe Biden, United States | Leave a comment
How Jewish Is the War Against Russia? Let’s be honest about who is promoting it
BY PHILIP GIRALDI • UNZ REVIEW • JULY 12, 2022
Five years ago, I wrote an article entitled “America’s Jews Are Driving America’s wars.” It turned out to be the most popular piece that I have ever written and I was rewarded for it by immediately being fired by the so-called American Conservative magazine, where I had been a regular and highly popular contributor for fourteen years. I opened the article with a brief description of an encounter with a supporter whom I had met shortly before at an antiwar conference. The elderly gentleman asked “Why doesn’t anyone ever speak honestly about the six-hundred-pound gorilla in the room? Nobody has mentioned Israel in this conference and we all know it’s American Jews with all their money and power who are supporting every war in the Middle East for Netanyahu? Shouldn’t we start calling them out and not letting them get away with it?”
In my article I named many of the individual Jews and Jewish groups that had been leading the charge to invade Iraq and also deal with Iran along the way. They used fake intelligence and out-and-out lies to make their case and never addressed the central issue of how those two countries actually threatened the United States or its vital interests. And when they succeeded in committing the US to the fiasco in Iraq, as far as I can determine only one honest Jew who had participated in the process, Philip Zelikow, in a moment of candor, admitted that the Iraq War, in his opinion, was fought for Israel.
There was considerable collusion between the Israeli government and the Jews in the Pentagon, White House, National Security Council and State Department in the wake of 9/11. Under President George W. Bush, Israeli Embassy staff uniquely had free access to the Pentagon office of Deputy Secretary of Defense Paul Wolfowitz, not being required to sign in or submit any security measures. It was a powerful indication of the special status that Israel enjoyed with top Jews in the Bush Administration. It should also be recalled that Doug Feith’s Office of Special Plans was the source of the false WMD information used by the Administration to justify invading Iraq, while that information was also funneled directly to Vice President Dick Cheney without any submission to possibly critical analysts by his chief of Staff “Scooter” Libby. Wolfowitz, Feith and Libby were of course Jewish as were many on their staffs and Feith’s relationship with Israel was so close that he actually partnered in a law firm that had a branch in Jerusalem. Feith also served on the board of the Jewish Institute for National Security Affairs (JINSA), which is dedicated to nurturing the relationship between the US and Israel.
Currently, the top three State Department officials (Tony Blinken, Wendy Sherman and Victoria Nuland) are all Zionist Jews. The head of the Department of Homeland Security, which is hot on the trail of domestic “terrorist” dissidents, is also Jewish as is the Attorney General and the president’s chief of staff. They and their boss Joe Biden do not seem concerned that their client Ukraine is no democracy. The nation’s current government came into power after the 2014 coup engineered by President Barack Obama’s State Department at an estimated cost of $5 billion. The regime change carried out under Barack Obama was driven by State Department Russophobe Victoria Nuland with a little help from international globalist George Soros. It removed the democratically elected President Viktor Yanukovych who was, unfortunately for him, a friend of Russia.
Ukraine is reputedly both the poorest and most corrupt country in Europe, witness the Hunter Biden saga. The current President Volodymyr Zelensky, who is Jewish and claims to have holocaust victims in his family tree, is a former comedian who won election in 2019. He replaced another Jewish president Petro Poroshenko, after being heavily funded and promoted by yet another fellow Jew and Ukraine’s richest oligarch Ihor Kolomoyskyi, who is also an Israeli citizen and now lives in Israel.
It all sounds like deja vu all over again, particularly as many of the perpetrators are still around, like Nuland, priming the pump to go to war yet again for no reason. And they are joined by journalists like Bret Stephens at the New York Times, Wolf Blitzer and Jake Tapper at CNN, and also Max Boot at the Washington Post, all of whom are Jewish and can be counted on to write regular pieces both damning and demonizing Russia and its head of state Vladimir Putin, which means it is not only about the Middle East anymore. It is also about weakening and even bringing about regime change in nuclear armed Russia while also drawing some lines in the sand for likewise nuclear armed China. And I might add that playing power games with Russia is a hell of a lot more dangerous that kicking Iraq around.
To put it bluntly, many US government and media Jews hate Russia and even though they benefited substantially as a group by virtue of their preeminent role in the looting of the former Soviet Union under Boris Yeltsin and continue to be among the most prominent Russian oligarchs. Many of the oligarch billionaires, like Boris Berezovsky, self-exiled when Vladimir Putin obtained power and began to crack down on their tax avoidance and other illegal activity. Many moved to Western Europe where some bought up football teams while others went south and obtained Israeli citizenship. Their current grievances somewhat reflect their tribe’s demand for perpetual victimhood and the deference plus forgiveness of all sins that it conveys, with the self-promoted tales of persecution going back to the days of the Tsars, full of allegations about pogroms and Cossacks arriving in the night, stories that rival many of the holocaust fabrications in terms of their lack of credibility.
Many Jews, particularly younger Jews, are finding it difficult to support apartheid Israel and the constant wars being initiated and fought for no particularly credible reason by both Democratic and Republican parties when in power, which is a good thing. But Jewish power in Washington and across the US is difficult to ignore and it is precisely those Jewish groups and individuals who have been empowered through their wealth and connections who have been the most vocal leading warmongers when it has come to the Middle East and to Russia.
Interestingly, however, some pushback is developing. The Jewish peace group Tikkun has recently published a devastating article by Jeffrey Sachs on the Jews who have been agitating for war. It is entitled “Ukraine Is the Latest Neocon Disaster” and describes how “The war in Ukraine is the culmination of a 30-year project of the American neoconservative movement. The Biden Administration is packed with the same neocons who championed the US wars of choice in Serbia (1999), Afghanistan (2001), Iraq (2003), Syria (2011), Libya (2011), and who did so much to provoke Russia’s invasion of Ukraine. The neocon track record is one of unmitigated disaster, yet Biden has staffed his team with neocons. As a result, Biden is steering Ukraine, the US, and the European Union towards yet another geopolitical debacle…”
Tikkun explains how “The neocon movement emerged in the 1970s around a group of public intellectuals, several of whom were influenced by University of Chicago political scientist Leo Strauss and Yale University classicist Donald Kagan. Neocon leaders included Norman Podhoretz, Irving Kristol, Paul Wolfowitz, Robert Kagan (son of Donald), Frederick Kagan (son of Donald), Victoria Nuland (wife of Robert), Elliott Abrams, and Kimberley Allen Kagan (wife of Frederick).” It might be added that Kimberley Kagan heads the Institute for the Study of War, which is often cited in media coverage and even in Congress to explain why we must fight Russia.
It has long been recognized by many that a particular antipathy directed against Russia permeates the so-called neoconservative world view. The neocons are hugely overrepresented at the top levels of government and, as noted above, a number of them are running the State Department while also holding high level positions elsewhere in the Biden Administration as well as in the foreign policy think tanks, including Richard Haass at the influential Council on Foreign Relations. Likewise, the intensely Russophobic US and Western media, foundations and social networking sites are disproportionately Jewish in their ownership and staffing.
And beyond that, Ukraine is to a certain extent a very Jewish-identified place. The Jewish media in the US and elsewhere has been showering Zelensky with praise, referring to him as a genuine “Jewish hero,” a modern Maccabee resisting oppression, a David versus Goliath. T-shirts bearing his image are being sold that read “Resisting tyrants since Pharaoh” while the largely Orthodox Jewish community in New York City has already been raising millions of dollars for Ukrainian aid.
The Jewish Telegraphic Agency reports that a “2020 demographic survey estimated that besides a ‘core’ population of 43,000 Jews, around 200,000 Ukrainians are technically eligible for Israeli citizenship, meaning that they have identifiable Jewish ancestry. The European Jewish Congress says that number could be as high as 400,000.” If that is true, it is one of the largest Jewish communities in the world and it includes at least 8,000 Israelis, many of whom have returned to Israel.
As US-Russian negotiations leading up the current fighting were clearly designed to fail by the Biden Administration, one therefore has to wonder if this war against Russia is largely a product of a long enduring ethno-religious hatred coupled with a belief in the necessity for a strong American military applied as needed to dominate the world and thereby protect Israel. The neocons are most visible, but equally toxic are the Jews who would prefer to describe themselves as neoliberals or liberal interventionists, that is liberals who promote a strong, assertive American leadership role to support the basically phony catchwords “democracy” and “freedom.” Both neocons and neoliberals inevitably support the same policies so they have both ends of the political spectrum covered, particularly concerning the Middle East and against Russia. They currently dominate the foreign policy thinking of both major political parties as well as exercising control over media and entertainment industry coverage of the issues that concern them, largely leaving the American public with only their viewpoint to consider.
There is plenty of other evidence that prominent Jews both inside and outside the Administration have been stirring things up against Russia with considerable success as President Biden has now declared insanely that his Administration is engaged in “a great battle for freedom. A battle between democracy and autocracy. Between liberty and repression.” He has confirmed that the US is in Ukraine’s war against Russia until we “win.” How else does one explain the ridiculous trip by Attorney General Merrick Garland to Kiev in late June to help set up a war crimes investigation directed against Russia?
As Garland is supposed to be the US Attorney General, it might first be useful to investigate crimes relating to the United States. He might start with American war crimes in Iraq and Afghanistan or Israeli war crimes using Washington provided weapons in Lebanon and Syria, not to mention the human rights violations using those same weapons that occur on a daily basis directed against the Palestinians. Some conservatives are also wondering why the Attorney General spends his time pursuing “white supremacists” and has failed to investigate the rioting, looting and killing that rocked the nation in the BLM Summer of 2020.
Nevertheless, an undeterred and fearless Garland announced while in Kiev that Eli Rosenbaum, Jewish of course, and a 36-year veteran of the Justice Department who previously served as the director of the Office of Special Investigations, which was primarily responsible for identifying, denaturalizing and deporting Nazi war criminals, will lead a War Crimes Accountability team made up of DOJ experts in investigating Russian human-rights abuses. After the obligatory photo op sucking up to Zelensky, the diminutive but steely eyed Attorney General declared that “There is no hiding place for war criminals. The US Justice Department will pursue every avenue of accountability for those who commit war crimes and other atrocities in Ukraine. Working alongside our domestic and international partners, the Justice Department will be relentless in our efforts to hold accountable every person complicit in the commission of war crimes, torture and other grave violations during the unprovoked conflict in Ukraine.” And if any further evidence is required to demonstrate the Jewishness of that week in Kiev, actor Ben Stiller, also a Jew, visited Zelensky and gave him a big hug.
If Eli Rosenbaum is still seriously interested in finding Nazis he will find many more of them in Ukraine than within the Russian Army. So, one has to ask “Whose war is it and who is making it happen?” Can you please explain Joe Biden? Or, given your perpetual blank look, should I ask Merrick Garland or Tony Blinken or maybe even Victoria Nuland?
Philip M. Giraldi, Ph.D., is Executive Director of the Council for the National Interest, a 501(c)3 tax deductible educational foundation (Federal ID Number #52-1739023) that seeks a more interests-based U.S. foreign policy in the Middle East. Website is councilforthenationalinterest.org, address is P.O. Box 2157, Purcellville VA 20134 and its email is inform@cnionline.org.
July 12, 2022 Posted by aletho | Timeless or most popular, Wars for Israel | Israel, Middle East, Palestine, Ukraine, United States, Zionism | Leave a comment
Don’t vaccinate your children with covid-vaccines! Ever!
Tomaris
In a video message, Dr. Geert Vanden Bossche begs parents not to have their children vaccinated against COVID under any circumstances. “If you do, it could mean their death sentence.”
Full transcript:
“My name is Geert Vanden Bossche. I am a vaccinologist. I have worked in the vaccine industry for many, many years. I am trained as a virologist, having worked for many years not only in the vaccine industry but also with Gavi and the Bill & Melinda Gates Foundation.
Today I want to talk about your children.
I beg you, I really beg you, do not vaccinate your children against COVID.
I will do my best to explain as best I can why this would be dramatic.
I’m not even going to talk about the fact that there’s no need to vaccinate children against COVID. And that there are too many and too dangerous side effects.
I’m going to talk about how these vaccines affect children’s immune systems. I am not exaggerating when I say that these vaccines could be a death sentence for your child.
Innate Antibodies
Let me explain how these vaccines will damage your child’s innate immune system.
First, and these are facts and data that you can check, we have never, really ever used a viral vaccine other than live attenuated vaccine. During childhood, we never use any vaccine other than live attenuated vaccine. And there’s a good reason for that.
This has everything to do with the innate or innate antibodies in the child. A child is equipped with a special kind of antibodies, innate antibodies. And those antibodies are only present for a limited time during childhood, then they disappear.
Kick-off immune system
These innate antibodies have an extremely important function. They help the child to kick-off his own immune system. The only way it can do this properly is thanks to its innate antibodies. What do these antibodies do?
First, the innate antibodies can neutralize the virus. And not just COVID but all kinds of viruses. Viruses are everywhere and people are continuously exposed to them.
But more importantly, by binding to the live virus, the innate antibodies learn to give proper instructions to the immune system to recognize not only the viruses it faces, but many other viruses as well. And that is important because the innate antibodies will disappear over time. So the immune system has to be trained to recognize viruses later in life, when the innate antibodies are no longer there.
But that’s not all. By binding to viruses, the innate antibodies will prevent your innate immune system from recognizing self-components. These are components of the child’s own body that should not be recognized.
What Happens When You Vaccinate Your Child?
What Happens When You Vaccinate Your Child? Then the vaccine creates antibodies, which will bind strongly to the virus and they will displace the innate antibodies. The innate antibodies are then no longer able to bind to the virus.
Source: https://rumble.com/v1az8uc-dont-vaccinate-your-children-with-covid-vaccines-ev
July 11, 2022 Posted by aletho | Timeless or most popular, Video | COVID-19 Vaccine | Leave a comment
The Work of Factions and the Pandemic’s Political Collapse
By Maximilian C. Forte | Zero Anthropology | July 10, 2022
We are now facing a regime that is losing, is aware that it is losing, and wants at all costs to survive even if it means damning everyone else. That is the picture that we get, in bold strokes. In practice, there may be considerable divisions and emergent factionalism within the pandemicist regime. By pandemicism I mean the intersection of catastrophism and authoritarianism. This article is written from within the Canadian and sometimes the Quebec contexts.
Three Factions: Fugitives, Perpetual Promoters, and Vandals
Fugitives: Typically led by provincial government leaders, some local politicians, the federal Conservative Party, and a small number of doctors, academics, and journalists who have broken away. At the provincial level these are politicians who have lifted all mandates and restrictions, even as the federal Liberals wanted them to be permanent, and augmented (national compulsory “vaccination,” for example). They have resisted reimposing any of the previous measures—yet they also state that what they have done is merely to “suspend” such measures.
An unflattering description, by those who have suffered their harms, would go like this: this faction consists of those who, like unwilling accomplices fleeing the scene of a crime, seek refuge in a web of alibis, disclaimers, disavowals, and caveats.
They may wish to recant, but do not want to admit guilt publicly—instead, they revoke, recall, and “relax the public health measures”. This faction seeks to avoid further damage to the economy, society, and health and welfare of citizens, by cutting losses and trying to withdraw under the pretext that success has either been achieved, or the costs are too high to continue. At least there is recognition in this group that the imposed restrictions did far more harm than good (as they should have known, since not even the WHO recommended such policies, and pre-existing preparedness plans in Canada were simply discarded—see Dr. Schabas here). This faction realizes that its members have served as an instrument for causing massive damage—politically, economically, and socially—and at most can only indirectly admit to that fact by now pursuing a different course. The fugitive faction would like to see us exit this trauma without any hard feelings, with little if any accountability, cheered by the promise that “we won’t do it again”. They would prefer to declare that “it is all subsiding” as we “learn to live with the virus”.
The existence of a faction of fugitives may also explain why suddenly there is more room in some media outlets for views that, until moments ago, were banished and censored as “misinformation” and “fake news”. We see such examples appearing in Newsweek (on multiple occasions), the Wall Street Journal (also here), the Toronto Sun (numerous times in fact—also here) and even the Globe & Mail (more than once), among others. While in Canada regime media speak of “anti-mandate” figures as if they were a rogue species of criminals, even a hard-line publication like The Economist can paint a grim picture of the harms of lockdowns for children. That these media publish the views of members of this faction is just a reaffirmation of the simple fact that it is easier for former insiders to be heard, than it is for outsiders who were never let in to begin with.
Fugitives, having developed doubts, misgivings, or even regrets, are joined by a large portion of the population that simply does not want to hear anything ever again about Covid, lockdowns, “masks,” “the pandemic,” and so on. Typically, these are people who have had two doses of the non-vaccines, and will not have a third—and will also resist having their children injected (more on this later).
In the Canadian context, in terms of size and influence, this is the largest of the factions. Its size and influence has grown particularly as 2022 has progressed. At the leadership level particularly, this faction contains those who have drifted away from the other two factions. Elements of this faction existed very early in 2020, before folding themselves into the pandemicist lockdown regime. Early expressions of doubt from political leaders, messages that contradicted the lockdown dogma that was imposed at lightning speed, and reopening policies that alarmed the media, were some of the indications of the existence of this prospective faction. A large percentage of the population that was coerced into getting “jabbed” forms the popular base of this faction. Otherwise, it is quite distinct from the resistance that has been fighting “vaccine” mandates, lockdowns, and other restrictions from the start—and who do not constitute a splinter of a regime to which they never belonged.
Internationally, the already existing global mass movement against mandates and restrictions is being joined by other disaffected quarters that have been harshly affected by economic transformation, ushered in by the same lockdown regimes, in what appears to be a rising global rebellion.
Perpetual Promoters: Unperturbed enthusiasts of eternal lockdowns, this middling class of stay-at-home professionals cherishes the pandemic as a lifestyle choice. This faction seeks straightforward continuity—maintain or reintroduce “measures,” encourage further “vaccination,” maintain or bring back “masking,” and so on. A Zoom-based social segment, this preachy faction consists of regime media and regime academia, whose specialties as advocates is to manipulate symbols and re-engineer values in order to normalize the state of exception. These exponents of the emergency lifestyle strive to maintain a permanent pandemic by sustaining a high level of propaganda and fear-mongering. They are constantly on alert. They are champions of “vigilance”. Behaving like overzealous hall monitors and pompous snitches, they are pious apostles of authoritarianism. In terms of its reality-denial capacity, it is the most psychotic of the factions—that is not an insult, but more of a clinical diagnosis.
This faction now invites ridicule from former believers (citizens qua parishioners), because this faction’s members fail to recognize the depth of indifference or anger that has sprouted in the society, especially post-Omicron, with the evident failure of the non-vaccines and the resulting rupture of the contract that believers were promised. Members of this faction also seem entirely numb to the consequences of their choices.
Unbridled enthusiasts of every wrong decision and the worst of choices, they continue cheerleading even when the game is over. They are idealists, true believers, who will cheerfully offer one booster after another until immune systems completely collapse, just in time for the complete collapse of the social system. This faction can sometimes be difficult to distinguish from the following, far more sinister cluster of interests, because to a significant extent it is, in functional terms, the “useful idiot” of what follows.
Initially extremely influential, and well remunerated from the Canadian federal government, this faction has seen its influence decline dramatically, especially in 2022.
Vandals: The third faction, that of the progressivist wreckers proclaiming a new order, is the one that is most worrying. This faction, consisting of champions of demolition, is the one that is capable of considering one final all-out assault that is so massive that it can only end in total destruction and provoke generalized violence in the form of civil unrest. This is the faction that seeks to crash the economy, by aggravating inflation, maximizing fuel shortages, damaging agricultural production, all under the pretext of “greening” the economy and ushering in a “transition” to “renewables” while fighting to preserve the phony “liberal world order” against the Russian bogeyman. Failed tools, like “vaccines” and sanctions, have been their favourites thus far, but they are capable of worse forms of collective punishment against recalcitrants. This third faction actively aims to escalate tensions and create further divisions in the society. This faction desires censorship to be institutionalized, legalized, and normalized. It wants pure dictatorship (in the name of “saving our democracy,” that is, the democracy that allows space only for them alone). The model some admire is China’s dictatorship, because that totalitarian system has served their interests very well. Key actors in this faction include the Bill & Melinda Gates Foundation, GAVI, Big Pharma, the World Health Organization, numerous Harvard graduates, NATO, the European Commission, the Atlantic Council, and so on. The third faction is also the one serviced by political functionaries such as Justin Trudeau, Mark Rutte, Emanuel Macron, and Joe Biden. Members of this faction may call themselves “liberals,” but they are in fact ex-liberals, illiberals, or post-liberals. They detest individual freedoms, civil liberties, and human rights. They embrace “social justice” only when it is cost-free, benefits (microscopic) minorities, and helps to create social divisions. (Note: according to the most recent census, Canada’s “trans” and “non-binary” population amounts to a whopping 0.003% of the total population—and even that is more than twice as large as the number of officially proclaimed “Covid deaths”.) They want a New World Order ruled by absolutist technocrats, unaccountable and non-elected “experts,” and they are willing to tempt the apocalypse to get to their destination.
If the experts, elites, and functionaries in power, who belong to this third faction, come to the realization that they cannot rule any longer, then they are going to make sure that there is nothing left to rule, or nothing left that is worth ruling. They are that suicidal and nihilistic. Bringing forth the full violence that is latent in progressivist ideology, they will opt for a scorched earth policy if they are not defeated first.
This third faction is the one that is least popular in the society, but it retains most of the levers of power—in particular, a monopoly over the means of violence, a tight grip on the country’s finances, and almost total sway over the courts and the media. It is by far the most dangerous faction and is located at the top of the regime’s pyramid of power.
The main difference between the second and third factions is that the latter is far more extreme, while the former is in denial about the extremism of the latter. The second faction is largely dependent on the third, but not vice versa.
What is common about all three factions is that they are dominated by actors who are neither willing nor capable of admitting mistakes. This is a problem, especially because they have been wrong on just about every major issue and significant problem for the past two decades, who can boast only of an uninterrupted litany of failures. In “The Insufferable Arrogance of the Constantly Wrong,” Clayton Fox listed just some of these epic failures of reason, analysis, or basic credibility among these discredited and defeated “experts” and technocrats.
What is to be hoped is that the first faction will break off completely, and form something like a mass movement comprising a cross-section of all classes, occupations, and regions of the country. Within the current regime of interlocking interests and partnerships between governments, the media, universities, the courts, the police and armed forces, and private corporations and foundations, the first faction is the one creating the most friction where the advancement of the plans of the other two are concerned. One hopes that friction will evolve into open resistance.
Outside of this arrangement of factions are those that resisted, criticized, and protested the lockdowns, “masking,” mandates, and the “vaccines” themselves. In Canada they numbered about 10% of the adult population (far less than many nations in Europe, and most in Africa and the Caribbean). However, their influence is growing. Much like the power structure they oppose, they consist of a complete cross-section of the national society: members of all ethnic groups and classes; representatives of every professional occupation; residents in every part of Canada; the complete range of educational achievement; supporters of every political party and ideology; and even politicians at all levels of government. Totally non-existent within the outsider group, however, is the presence of Big Banks, Big Tech, or Big Pharma.
The Stakes: Capital and Power
Much is at stake for the regime, beyond its reputation. The political economy of pandemicism is at stake—the ability to extract capital from the people, and accumulate it in the pockets of the super-rich and their corporations. “Vaccine uptake,” even after the repeated, demonstrated failures of the non-vaccines to achieve even the most minimal of the promised goals (while evidence of damage accumulates), remains a key goal. “Vaccine uptake” is about sustaining demand, that is, of sustaining the profit margins for commercial pharmaceutical interests. The maintenance of fear is thus essential to sustaining demand. In addition to extracting capital, there is the very basic question of power: the unrestrained ability to dominate the masses, without question, triumphing against resistance. The “vaccine” gravy train coming to its last stop threatens all of this, as do a number of other challenges: Ukraine, inflation, and the recession, and the immense unpopularity of those in power.
Like the “war on drugs,” then the “war on terror,” this horrific “war on the virus” (which is in fact a war on the people) is one more grand failure (except, perhaps, as an intentional crime). A regime can withstand only so many monumental failures, or commit so many crimes, before it can stand no more.
Regarding sustaining demand, there is now a gradation of forms of “vaccine resistance,” as reported in data from Public Health Canada:
- 15% of the population has had no dose;
- The 82% of the population that took two doses, dropped to 49% of who took a third—even as the federal government declared those with two doses “not up to date” and removed the term “fully vaccinated” (following Fauci);
- Less than 10% have had a fourth dose;
- 56% of children (5 to 11 years of age) have had one dose, which drops to 42% having the “primary series” (two doses).
As things stand now in Canada, 64% of the population is defined as “not up to date,” that is, not in compliance. In the US there is growing public criticism about the rush to “vaccinate” toddlers, including from esteemed persons who previously formed part of the mainstream second faction, the promoters, such as Dr. Paul Offit.
To an extent, the growing extremism of the second and third factions is apparently impelling the formation of the first faction listed at the outset, driving away even some stalwarts.
In an ongoing effort to “study up,” which includes reading and analyzing the scripts produced by regime media, what follows is just about a week’s worth of snapshots that illustrate some of the main points above. Before proceeding, I want to explore the “regime media” concept a little further.
Regime Media, Part 2
Regime media are a fusion of a police force and a public relations firm. Whether they are privately owned, yet receive government payouts, or they are publicly owned and prey to corporate advertisers, in Canada all of the media of domination (CBC, CTV, Global News, The Toronto Star, The Globe & Mail, etc.) are aligned with and actively support the pandemicist regime and indulge its elitist virtue signalling about select, preferred minorities that are elevated for special recognition and rewards. Gesticulating toward celebrity-approved “social justice” issues, and fanning all of the latest moral panics that occupy the minds of the dependent urban middle class, regime media have thus been able to dull suspicions from the left. The self-identified left has largely fallen in line with regime media and extend the regime’s core messages through various “alternative” media—which are no alternatives at all (they are simply less resourced). It is not surprising then to find some of the most extreme advocacy for Zero Covid policies emanating from the left, much of which is also pro-China, the industrial engine of contemporary globalization and the first country to set the pattern for the lockdowns that followed around the world.
Regime media may call themselves “news media,” but there is next to no actual journalism involved in their work. In that spirit, students at contemporary Canadian schools of “journalism” are in fact being trained in the methods of policing restive subjects with “unacceptable views”. Embracing “advocacy,” they have degenerated into mere practitioners of propaganda whose ultimate aim is the reproduction of the ideas of the ruling faction of the regime.
Here they are followed by professors and students in a variety of disciplines which these days are busy churning out one predictable thesis after another that essentially involves policing : using the Internet to engage in surveillance of troublesome “fringe minorities” with “extremist views” that threaten to “incite hatred”—and they do this without any sense of irony. Their work is one-dimensional, simplistic, conspiratorial, and their “data” is cherry-picked. Rather than full and richly textured biographies, they produce caricatures dressed up in the theoretical jargon that is currently in fashion in their disciplines. Master compilers of shitlists, they squat for long days in social media on the lookout for anyone deviating from their preferred narrative, so they can then pounce and declare deviants to be violent extremists. Nobody is permitted to be “wrong” on the Internet. The aim of the students and professors is to make these “minorities” legible to the authorities, while reaffirming their own sense of superiority as specially endowed super-citizens with a natural right to manage inferior others, “for their own good”. Regime academia, like regime media, consists of a non-elected political class mesmerized by its belief in its own inherent goodness, and its right to rule. The writing of this class reads more like pseudo-legislation than scholarly analysis, and their “theories” are little more than ideological wishful thinking mixed in with complaints. They see the world as a collection of “problems” that require their management. An inanely partisan document produced by the UNESCO research chair in Quebec exemplifies many of these traits—see “Le mouvement conspirationniste au québec : leaders, discours et adhésion” (“The Conspiracy Movement in Quebec: Leaders, Discourse and Membership”). The art of these “scholars” consists of punching down while sucking up.
Regime media’s main functions are: surveillance, censorship, and prosecution. Stories are written with a tensely vigilant, accusatory tone, meant to put readers on guard, or on notice. Critical-minded questions, if they are even mentioned, are instantly dismissed out of hand or simply associated with mental illness or amorphous “extremism”. They do not try to keep their “finger on the pulse” of society—they instead aim to determine the pulse rate itself.
Regime media’s public scripts involve a regression to some of the most outmoded forms of propaganda seen since World War I. Their work involves a classically crude command structure: they tell people what to think, plain and simple. Then they tell people what to think about, and here the agenda-setting is particularly exclusive. One will never read stories of the “vaccine injured,” or see or hear interviews with anti-mandate protesters, dissident doctors, and so forth. Theirs is a regimist record, cleansed of all opposition and inconvenient facts. It reads almost like a colonial archive, only with greater gaps and silences.
What the regime media tell people to think is hatred, especially hatred for the non-compliant Other. Inciting hatred against marginalized categories of Canadians over the past two plus years has already been abundantly documented—this is not a theoretical statement, it is now merely an observation.
What the regime media tell people to think about is emergency and safety. Also well documented, any perusal of the pages of the print and Web regime media will quickly confirm this.
Inversion and projection are key tools of regime media: their work consists of broadcasting disinformation, propaganda, conspiracy theories, false allegations, hyperbole, fear-mongering and character assassination, while producing “news stories” that are entirely and exclusively one-sided and indistinguishable from straightforward editorials.
In 2022, such regime media turned their attention to explicitly attacking freedom. Openly praising sheep, an article in the Globe & Mail advocated that humanity follow the example of sheep. In the same paper, another article cautioned that freedom “is not absolute,” and it does not mean we have the right to do anything we want—in other words, the author fully tilted against a complete straw man (absolutely none of the anti-mandate protesters ever advocated any such thing… they just wanted their jobs back). The CBC laboured to turn “freedom” into a dirty word that it conflated with the politics of “far-right” extremism. Canadians though they may be, they publicly worry about flying the Canadian flag, because it has been sullied by those fighting for freedom. Perennially perturbed by “nationalism,” they have no such qualms when painting their social media profiles with the Ukrainian flag, or claiming to support First Nations.
Perpetual Promoters: “Do Not Allow the People to Rest Even for a Moment”
Here I will continue my commentary on the work of the second faction, and simply illustrate it with snapshots taken over the course of a week (if that much). The significance of the week in question is that it featured the proclamation of a “seventh wave” in Quebec. This time—given the degree of popular contempt for restrictions that are proven failures, and mindful of a provincial election in October—the government of Quebec is acting like a member of the Fugitive faction. Members of the Perpetual Promoters’ faction are turning on the government, trying to school it back into authoritarian “measures”.
As an anthropologist, I have been trained to view the narratives of authorities with considerable skepticism, knowing that such narratives tend to push for a desired reality more than they accurately describe an actually existing reality, and that such narratives reflect the vested interests of powerful actors. Reality in the papers and reality on the ground are thus often very different. As an anthropologist with ethnographic experience, I tend to privilege reality on the ground—and on the ground, there is no “seventh wave”. People are carrying on as normal, meaning a pre-2020 normal. They seem to be enjoying their summer as best as they can, at least in the rural region where I live: swimming in lakes; boating; barbecuing; setting off fireworks every weekend; gathering with friends around backyard fires; neighbourhoods alive with the sounds of children playing; shopping and dining occurring without “masks” or any apparent concern for “social distancing,” and so on. Nobody is panicking. The Perpetual Promoters just hate that.
One example of a common injunction against any relaxation from anxiety, is an article like this one from the Montreal Gazette: “It’s too soon for Montrealers to bet on a COVID-free summer: experts”. No summer for the masses—the “experts” have sealed this: “Few masks, plentiful travel and a highly contagious sub-variant mean we need to remain cautious”. The fear-mongering was thus also intended to boost the social capital of “experts” while draining the people of any sense of hope: “As COVID-19 case counts fall and hospitalizations slowly drop, Quebecers are wondering if they’ll be able to enjoy another relatively COVID-free summer this year. The short answer is probably not…”. The experts warn, and lament: “only 52 per cent of Quebecers have gotten a third vaccination, leaving half the population vulnerable as the immunity from their vaccinations or infections wane”. They added: “And for sure get your third dose. This is not a virus that anyone wants to get”. The stress is on an imputed “vulnerability” which then becomes a sales pitch for Big Pharma’s experimental gene therapies which have done nothing to prevent spread. The experts also imagine a severe virus, one that nobody wants to get, but everyone got anyway (and without a massive die off). Be cautious, feel vulnerable—even knowing all of the damage done by sustained fear and anxiety for people’s mental health, in a desperate bid to remain relevant the perpetual promoters throw any real care for public health to the wind.
They are immune—so now it is time to scare them to death. This time courtesy of Global News, we have another lesson in how sophistry works. To be clear, absolutely nothing in the article proves that those infected by Omicron will likely get sick from a subsequent infection with an Omicron variant. The purpose of the article is simply to make people feel insecure, and then rush for the nearest shot of precious mRNA. The way the author of the article tries to smuggle through the fear messaging, is first by lumping together both those who were mRNA injected and got Covid, and those who kept their systems clear of the experimental gene therapies to begin with (with no increased incidence of myocarditis or pericarditis, which is not the case for the injected). By conflating the two groups, the author does not need to talk about immune imprinting, and the fact that those with three doses now have significantly negative immunity. Across Canada, in British Columbia, Ontario, and Quebec, government data show that those with three doses or more account for the majority of hospitalizations and deaths, despite numbering no more than 50% of the population. However, it is standard fare for regime media to generalize all risks, which justify one-size-fits-all (i.e., totalitarian) “solutions”.
What Global News does is to take the analogy of the glass half full to an extreme: “… one in every eight people who contract the virus do not develop antibodies in their blood from their illness”. “So forget going to some kind of ‘COVID party,’” said Dr. Catherine Hankins, a professor at McGill University in the Faculty of Medicine and co-chair of Canada’s COVID-19 Immunity Task Force: “Infection is not a viable strategy to achieve or maintain immunity”. Why forget the Covid party? Did the article not just state that 7/8 people develop immunity? Therefore, if we take their data at face value—with zero scrutiny or debate—that means that 87.5% of persons have immunity. That sounds like a pretty viable strategy. At this point one might only hear the din of preparations resuming for Covid parties (not that it would even be necessary to have these anymore).
The article also quietly conflates infection with actual sickness. So you might test positive again for Covid (assuming you even care to be tested). And so what? The Perpetual Promoters continue to instill shame in infection, as if infection were proof of some sin. Colleagues and students of mine have “admitted” to getting Covid: “I know!” one exclaimed apologetically.
Prof. Hankins, the party pooper at McGill, also added: “We do have one in eight people that don’t show any antibodies in their blood, so they’re not responding to the vaccine. And if they get infected, we’re not seeing evidence of it… So we don’t quite know what’s going on”. Indeed.
Later in the same article Global News’ “experts” admit that one reason why there are lower levels of antibodies among the Omicron-infected, is because “it’s a milder infection”. However, as if forgetting themselves and losing the train of their own thought, moments later they repeat the mantra: “there is strong scientific evidence showing the vaccine does prevent severe illness and death”. But if Omicron itself does not cause severe illness and death—which they admitted—then how do they credit the non-vaccines with saving people?
The real purpose of the article is clearly revealed at the end. It uses fear as a sales pitch: “I think it’s important that people understand that if you’ve had it before, you are still a sitting duck… you don’t have the immunity that you had closer to when you got your vaccine… So it’s really important to get that booster”.
Yet another editorial appeared in The Montreal Gazette moaning about breathing barriers not being forced onto everyone’s faces, immediately. It has been only a couple of weeks since “mask” mandates have been lifted in Quebec, for all settings except medical ones. We are only half way through the summer, but regime media cannot wait until the fall—restrictions need to come right back now. Remember: no summer for you, the party is over. This is the second such editorial in a week. The editorial board is complaining that Quebec’s plans looks like “everyone for themselves”—and while they speak of “everyone,” what they are really doing is using “the immunocompromised” as rhetorical and political shields. Adept as hostage-takers (humanitarian abduction), regime media will hold any minority they can find at ransom, until everyone else is forced to bend.
To further add to a record of deception, deflection, and sophistry, the editorial board argues: “It is hard to imagine that the dropping of just about all masking requirements has not also contributed to the upswing in cases. Relatively few people seem to be wearing masks these days”. There is not even a pretense of “science” anymore; now it is just a matter of “imagining”. For some reason they are unable to recollect, even a few short weeks later, that 50% of Canadians got Omicron over the past few months, when we were still at the height of mandates and restrictions. “Masks” did nothing to “protect” people. Indeed, virtually nobody needed “protection”. Most visitors to the Gazette’s website now know that.
But the Montreal Gazette, with its increasing desperation on display, is starting to play its hand too visibly. From “science” we have gone to “imagination”. From “protecting health,” we have gone to the Gazette’s real target: that “segment of the population being courted by the Quebec Conservative Party, whose star seems to be rising”. Here they allude to Eric Duhaime, the popular leader of the Quebec Conservative Party, only you would not know how popular he has become thanks to the blackout in Anglophone Quebec media. His weekly meetings and call-in programs with tens of thousands of Quebecers during “the pandemic,” have helped to build a powerful grassroots anti-mandate, anti-emergency movement that, in Quebec, likely helped to shape the first faction mentioned at the outset of this article.
Regime academia, promoted by regime media. Regime academia is keen to gin up fear of the “seventh wave,” but is clearly anxious about not being able to exploit it. McGill’s Donald Vinh “says the province should reimplement public health measures. And refusing to do so because it may seem like taking a step backward after removing them, he added, is a ‘failing mentality that could get us in trouble’”. Dr. Nathalie Grandvaux outright proclaims a permanent pandemic, and urges everyone to follow her hysterical signalling: “The virus is constantly here, she said, and there’s no reason to believe the province will somehow be shielded from future variants, either”. “Speaking about waves is a bit like telling people there’s nothing to be concerned about between them,” Grandvaux said. “But that’s not the case — the virus is always there”.
They do not deny reality on the ground, that is, how people (fail to) respond to their fear-mongering. Instead they attack reality on the ground. We see a glimpse of this in, “Montreal businesses, customers have no plans to return to COVID-19 restrictions”. Here are some of the opinions that were expressed:
“I think at this point, we all have to make it part of our life. I think we have to start moving on and moving forward, because the number of small businesses that closed and didn’t get to reopen, it can’t happen again because too many people will suffer.”
“I think that the media likes to play on people’s fears and make it worse. We just have to deal with it.”
“I think we should be talking more about what it means to live with a virus period, rather than this virus, because there are going to be many viruses and it’s going to happen again. I think the world is a little more prepared for a heavy-duty virus. I’m not particularly worried about it.”
“Maybe we should stop talking about waves and start talking about a new normal.”
“I think the customers feel super safe here. Those who don’t feel comfortable just don’t come. It feels like normal times again.”
“I think it’s just another virus we will have to live with, like the flu.”
As minimal and polite as such remarks are, they are the surface evidence that people have turned against the narrative of the failed elites and the discredited expert class. They have joined all the other fugitives. Pandemicism eventually has to meet resistance, and it can and will be defeated. And not even a reich proclaimed for a thousand years lasted more than 12. Tick-tock.
July 10, 2022 Posted by aletho | Civil Liberties, Mainstream Media, Warmongering, Malthusian Ideology, Phony Scarcity, Supremacism, Social Darwinism, Timeless or most popular | Canada, Covid-19, COVID-19 Vaccine, Human rights, Quebec | Leave a comment
From Wild-Type SARS-2 to Omicron: Towards a Theory of Corona Evolution
With additional thoughts on why mass containment probably made everything worse, by playing to the most central strategy of the virus
eugyppius | July 10, 2022
Scientific discourse on Corona remains focused on microbiological minutiae, while ignoring the broader evolutionary and behavioural patterns of SARS-2. This is especially frustrating, because our mass containment policies were at base attempts to change the behaviour of the virus, and their failure has prompted no introspection about the limits of our understanding.
Equally neglected is the evolutionary trajectory of Corona. Aside from simplistic, one-dimensional concerns about things like escape variants, almost nobody in mainstream scientific circles has tried to account for observed evolution or describe the various selection pressures SARS-2 faces.
Among the few people to have given serious thought to the evolution of viral pathogens is Paul Ewald, author of the book Evolution of Infectious Disease, as well as numerous articles explaining the evolutionary pressures on the virulence and transmissibility of viruses.
As he explains in this piece from 2011:
Much of the variation in the harmfulness of acute infections is associated with the dependence of transmission on host mobility. When transmission occurs by direct contact, infected hosts generally need to be mobile to facilitate contact with susceptibles. When transmission of pathogens does not depend on the mobility of infected hosts, evolutionary considerations predict that natural selection should favor high degrees of host exploitation and hence high degrees of virulence.
Basically, the virus wants to make as many copies of itself as possible. But, very roughly speaking, the more aggressively the virus copies itself, the sicker its hosts become. This places an upper limit on the virulence of viruses that depend on person-to-person contact, and it explains why widely transmitted respiratory viruses all fall within the same narrow range of pathogenicity and cause the same kinds of symptoms. The pandemicists raise money by wargaming pandemic viruses with 10% fatality rates, but in the real world, the truly deadly viruses never get very far. They’re all like SARS-1 – they put people in the hospital too soon.
But what about smallpox? And cholera, and yellow fever and dengue fever? Are these not deadly viruses?
They are, but they don’t spread via direct contact. Smallpox falls into what Ewald calls a “sit-and-wait” category of transmission. These are viruses that have remarkable durability, remaining viable in the external environment for months or (in the case of Variola) even years. They can thus disable their hosts while still having hope of new victims. Yellow fever and dengue, meanwhile, are “vector-borne.” They depend on mosquitoes to hop from host to host, and they’re free to make their victims as sick as they want. “Waterborne” pathogens like cholera are similarly advantaged.
More importantly for our purposes, Ewald defines a fourth category of what we might call mediated transmission facilitating higher virulence. This is “attendant-borne” transmission, which occurs primarily in hospitals, where staff unwittingly circulate viruses among patients. Attendant-borne viruses, like their vector-borne and waterborne colleagues, are free to develop remarkably high virulence. Ewald believes that the 1918 influenza outbreak achieved its unusually high mortality via attend-borne transmission related to troop transports at the end of the First World War.
SARS-1, although never properly adapted to human hosts, also depended on attendant-borne transmission, and MERS is a more straightforward case of this phenomenon. But the clearest example of all is surely pre-Omicron SARS-2, which caused elevated mortality near the top of what we would expect for pandemic influenza; and which flourished nowhere as effectively as in healthcare institutions, including hospitals and especially nursing homes.
Remember that SARS-2 arrived in Europe no later than November 2019, and in America no later than December 2019. The West saw multiple months of community Corona transmission, in other words, without anybody noticing that anything was amiss. Hospitals remained as empty or as full as ever. As soon as we imposed lockdowns and started testing everybody, though, mortality spiked. These containment procedures involved nothing so much as identifying Corona patients and putting as many of them as possible in environments favouring attendant-borne transmission – from Corona testing centres to hospitals. And as the mass containment regime continued through 2021, SARS-2 began evolving towards greater virulence, as nosocomial and nursing home infections came to dominate the case statistics almost everywhere.
Omicron, whatever its origins, broke this dynamic. Unlike prior SARS-2 lineages, this is a classic direct-contact respiratory pathogen. With the advent of Omicron, Corona no longer spreads preferentially in healthcare institutions, and behaves much more like a mild flu or the common cold, with an emphasis on keeping its hosts healthy and mobile.
The worst thing we could do, from an evolutionary perspective, is continue the mass containment regime. We want to keep SARS-2 circulating via direct contact in the community. All such respiratory viruses, despite their stark differences, have been subject to the same convergent evolution, with remarkably similar effects on their human hosts. We must stop intervening in matters we don’t understand, or we’ll just continue our recent history, of always making everything worse.
July 10, 2022 Posted by aletho | Science and Pseudo-Science, Timeless or most popular | Covid-19 | Leave a comment
Infertility: A Diabolical Agenda
https://www.bitchute.com/video/aJDAjtkBchfw
ChildrensHealthDefense
Dr. Joseph Mercola | July 9, 2022
“Infertility: A Diabolical Agenda,” is the fourth vaccine-related documentary by Dr. Andrew Wakefield. It tells the story of an intentional infertility vaccine program conducted on African women, without their knowledge or consent.
While it’s been brushed off as a loony conspiracy theory for years, there’s compelling evidence showing it did, in fact, happen, and there’s nothing to prevent it from happening again.
The Backstory
As explained in the film, the World Health Organization began working on an anti-fertility vaccine, led by Dr. G.P. Talwar in New Delhi, India, in the 1970s, “in response to perceived overpopulation.” For 20 years, the WHO’s Task Force on Vaccines for Fertility Regulation worked with population control in mind.
In 1993, the WHO finally announced a birth-control vaccine had successfully been created to help with “family planning.”1 The paper trail reveals that by 1976, WHO researchers had successfully conjugated, meaning combined or attached, human chorionic gonadotropin (hCG) onto tetanus toxoid, used in the tetanus vaccine. As a result, when given to a woman, she develops antibodies against both tetanus and hCG.
HCG is a hormone produced by cells surrounding the growing embryo. These hormone-producing cells protect and support embryonic growth and eventually form the placenta.
As explained in the film, hCG is the first signal that tells the woman’s body she’s pregnant. In response to this signal, her ovaries then produce a second hormone, progesterone, which maintains the pregnancy to term.
By combining hCG with tetanus toxoid, it causes this crucial pregnancy hormone to be attacked and destroyed by your immune system, as it’s now misperceived as an invading pathogen. Since hCG is destroyed, progesterone is never produced and, hence, the pregnancy cannot be maintained.
So, if you’re already pregnant when taking this witches’ brew, it will likely result in a spontaneous abortion, and if you’re not already pregnant, you won’t be able to get pregnant, as this crucial pregnancy hormone is under constant attack by your immune system. Repeated doses prolong these effects, effectively rendering you sterile.
The WHO Has Been in the Depopulation Business for Decades
As detailed in a Scientific Research paper published in 2017,2 “WHO publications show a long-range purpose to reduce population growth in unstable ‘less developed countries.’”
In other words, the WHO’s longstanding policy has been to support depopulation in third world countries, and they’ve studied depopulation strategies in India, Bangladesh, Pakistan, Nigeria, Mexico, Indonesia, Brazil, The Philippines, Thailand, Egypt, Turkey, Ethiopia and Colombia for decades.3
While creating an anti-fertility vaccine for those who really don’t want children is one thing, using deception to lure girls and young women into taking it is another entirely. As it turns out, the WHO is not above using deception and trickery to shut down fertility in populations they deem unworthy of reproduction.
The Great Deception
The central figures of the film are two Kenyan gynecologists, Drs. Wahome Ngare, and the late Stephen K. Karanja. Both state in the film that infertility is now the biggest gynecological problem in Africa. In recent years, there’s been a significant increase in women losing their pregnancies and couples who cannot conceive.
“I have seen the tears. They lose their identity. You die inside,” Antoninah Mutinda says. She knows, because she’s one of the African women whose fertility has been mysteriously impacted. After her third miscarriage, she was tested and found to have extremely high anti-hCG antibodies. She now suspects the tetanus vaccine she was given may be the culprit.
The anti-fertility vaccine was rolled out in the mid-‘90s, but despite support from the Kenyan leadership and “elite groups,” it was not popular among Kenyan women, who were concerned about the potential for abuse. They worried it might be disguised as a regular tetanus vaccine program.
Their concerns were valid because, as it turns out, this had already happened. In 1995, the Catholic Women’s League of the Philippines won a court order halting a UNICEF tetanus program that was using tetanus vaccine laced with hCG. Three million women between the ages of 12 and 45 had by that time already been vaccinated. Anti-hCG-laced vaccines had also been found in at least four other countries.
Undeterred by bad press, that same year, 1995, the Kenyan government launched a WHO tetanus campaign under the guise of eradicating neonatal tetanus. There were telltale signs that something was wrong, however, because it was already standard practice to vaccinate pregnant women against tetanus. Now, the WHO insisted women who weren’t pregnant needed the shot as well, in case they were to become pregnant.
Karanja learned of the deceptive anti-fertility campaigns in other countries during a medical conference in 1995, and became immediately suspicious of the tetanus campaign in his own country. Karanja convinced leaders of the Catholic church — one of the largest health care providers in Kenya — to test the tetanus vaccine being given, to make sure there was no foul play.
Without explanation, the WHO suddenly abandoned the campaign. Alas, 19 years later, in 2013, they were back. All girls and women, 15 to 49 years of age, were instructed to get vaccinated with a series of five injections, six months apart. This, it turns out, is the exact schedule required for the anti-fertility vaccine to produce sterility. Regular tetanus prevention requires only one injection every five to 10 years, and under no circumstance would you need five of them.
Vaccines Test Positive for Anti-hCG
The Catholic Church decided to test the vaccines, and collected three sample vials directly from clinics during the 2014 campaign. The samples were then sent to three independent laboratories for testing. As feared, they found hCG in them. Another six vials were then collected, and tested by six independent labs. This time, half were found to contain hCG.
At this point, the Catholic Church went public, urging girls and women to not comply with the vaccination campaign. In an effort to settle the dispute, an investigative committee was formed, consisting of three representatives selected by the Catholic bishops, and three government officials.
It was agreed that the nine vials already collected would be retested, along with 52 samples from a distributor who sells tetanus vaccine to the Kenyan government. This time, a more precise type of test, high performance liquid chromatography (HPLC), was chosen.
Dr. Nicholas Muraguri, director of medical services for the Kenyan government, contracted agriQ Quest to perform this testing. However, he urged them to test samples provided directly by him rather than the vials previously agreed upon. AgriQ Quest decided to analyze both batches.
The vials that tested positive for hCG using enzyme-linked immunosorbent assay (ELISA), still tested positive using HPLC, but none of the samples provided by Muraguri tested positive.
A Decades’ Long Cover-Up
Shockingly, the government then demanded agriQ Quest “alter their report to indicate that they were safe to be administered.” When agriQ Quest refused, the government, the WHO and UNICEF responded by launching a public attack, accusing the Catholic Church of “peddling misinformation.”
And, since the only samples found to contain hCG were those provided by the Church, the government accused them of tampering with the vials in an effort to undermine confidence in the vaccine.
An added twist here is that the vials that tested positive had the same batch numbers as vials that tested negative. Only later did agriQ Quest discover that these negative vials had fake labels on them. They were not, in fact, from the same lots as those that tested positive. They weren’t even made by the same manufacturer.
AgriQ Quest also claims they can prove the positive samples were not tampered with, because they did not test positive for hCG in general. The test clearly shows the hCG was conjugated with tetanus toxoid, and this cannot occur by simply adding hCG to a vial of tetanus vaccine.
The conjugation — the chemical linking or bonding — of hCG to the tetanus toxoid can only occur during the manufacturing process. This is the smoking gun that proves the neonatal tetanus vaccine campaign was a cover for a population control campaign.
Muraguri also lied when he claimed the Kenyan government had only one supplier of tetanus vaccine. As it turns out, there were two. Biological E. Limited provided a regular tetanus vaccine, while the hCG-positive batches came from Serum Institute of India — the same country where most of the WHO’s anti-fertility research had been conducted.
Both Ngare and Karanja paid a steep price for their vigilance. The medical board called them for disciplinary action. Karanja was issued a gag order, and since 2014 was not allowed to speak publicly about vaccines in Kenya. He broke that gag order for this film. April 29, 2021, Karanja died, allegedly from COVID infection.
A Truly Diabolical Agenda
Speaking for millions of women just like her, Mutinda, who has now struggled with infertility for years, says:
“To imagine there’s a system somewhere, that some people somewhere are behind my inability to carry pregnancy to term, that is a diabolical agenda!”
Before his untimely death, Karanja shared a message with the world, through the makers of this film:
“When they are through with Africa, they’re coming for you.”
Sources and References
July 10, 2022 Posted by aletho | Deception, Malthusian Ideology, Phony Scarcity, Timeless or most popular, Video | Africa, Human rights, WHO | Leave a comment
Taiwan: Birth Rate CRATERED -27.66% in June 2022!!!
By Igor Chudov | July 9, 2022
A couple of weeks ago, I wrote an article based on the shocking news that Taiwan’s birth rate in May 2022 fell by 23.34% compared to May 2021.
I explained that in terms of statistics, the change in Taiwan is an unthinkable 26-sigma event of enormous magnitude.
Like most people would, I was hoping, despite evidence from other countries, that this is a data fluke.
Well, it is not, and the data for June was just released in Taiwan. I am very upset.
June Birth Rate Cratered by 27.66%!
Compared to June 2021, birth rate in Jun 2022 is down by -27.66%. This is far worse than the previous month (May) drop of -23.34% and indicates a worsening birth rate trend.

Here’s the updated chart:
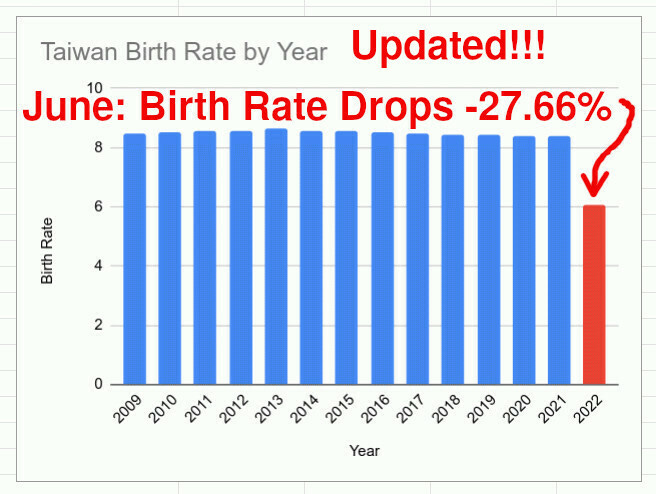
Mind you, last August of 2021, when June 2022 babies were conceived in Taiwan, the people of Taiwan were mostly unaware of what was going to happen, and kept their family making plans intact. They probably did not notice a 27.66% decrease in pregnancies, or an increase in stillbirths. If someone told them, the young people of Taiwan probably thought that it was antivax propaganda that they should dutifully ignore, like their government and TV told them.
Young people were being happily vaccinated.
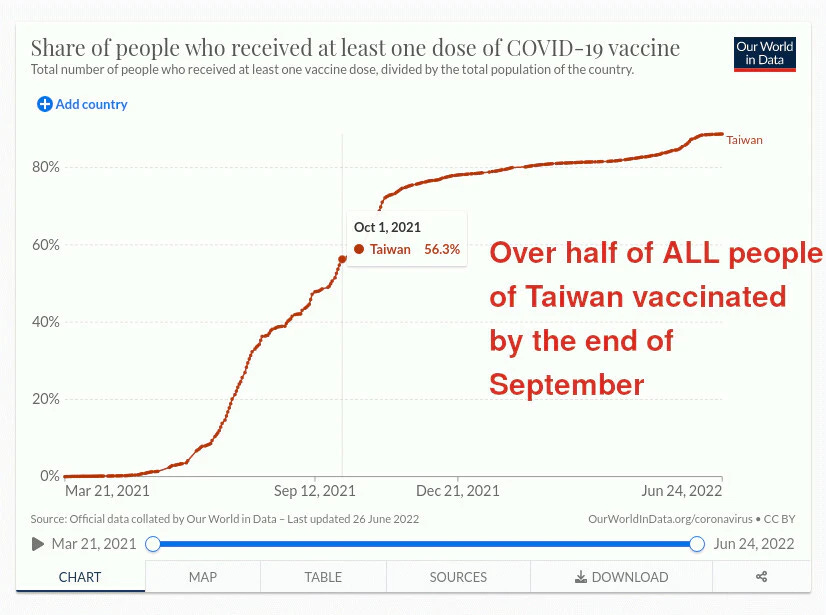
The result? An “impossible” birth rate drop of -27.66% is basically a slow death sentence for the population of Taiwan, if it continues, especially combined with a 26% increase in deaths.
Media Coverage
The mainstream media is beginning to cover drops in birth rates:

Further Reading
Concerned?
Check out my “depopulation series”:
July 9, 2022 Posted by aletho | Timeless or most popular, War Crimes | COVID-19 Vaccine, Taiwan | Leave a comment
The self-inflicted genocide of late capitalism
By Toby Rogers | July 8, 2022
At some point over the last 50 years, the bourgeoisie (in the U.S. and throughout the developed world) embarked on the first self-inflicted genocide in human history.
While the roots may go way back, the self-inflicted genocide became systematized and legalized with the 1986 National Childhood Vaccine Injury Act.
By 2001 with the publication of Autism: a novel form of mercury poisoning by Bernard, Enayati, Redwood, Roger, and Binstock it was clear that vaccines were largely responsible for the explosion in autism cases.
Faced with this news, the mainstream went all in to cover up the genocide and accelerate the pace of the destruction.
Thomas Verstraeten at the CDC took a job from GlaxoSmithKline in Belgium rather than tell the truth about the genocide.
William Thompson took a promotion from CDC rather than call a press conference to stop the genocide.
Julie Gerberding, Frank DeStefano, and Coleen Boyle at CDC aggressively covered up widespread harms to children like eager S.S. officers at Auschwitz.
Once everyone knew that methyl mercury was neurotoxic, Pharma with the blessing of FDA and CDC took most of the mercury out of vaccines and replaced it with even more aluminum — which leads to more autism cases but less severe symptoms. The genocide marched on.
A new generation of fixers including Tom Shimabukuro, John Su, and Matthew Oster at CDC as well as Nicola Klein at Kaiser Permanente dedicate their careers to hiding vaccine injury.
And now with rushed experimental Covid-19 shots, the genocide has accelerated and expanded to include adults throughout the developed world.
Responsible Parties
Harms are driven by the pharmaceutical industry. It’s gigantic — $1 trillion a year in revenue even before Covid-19. Toxic Covid-19 shots, useless treatments including Paxlovid and Remdesivir, and medicines to treat vaccine injury (including a sharp increase in myocarditis cases) will generate hundreds of billions of dollars of additional profits for Pharma. Pharmaceutical industry executives are avaricious, predatory, and they absolutely do not care who they hurt and kill. Many are also likely eugenicists who want to shrink the size of the global population.
Grifter billionaire psychopaths — including Bill Gates, Klaus Schwab, and Alain Mérieux — gravitate towards vaccines because they see the opportunity to vastly increase their wealth while inflicting pain. Their billions of dollars buy them talent — the best management consultants, the best PR firms, and the best private Psy-Ops firms. They also purchased the global public health system, the political system, and the regulatory state. They clearly want to take over the world and enslave (via chronic illness and twice yearly injections of gene modifying substances) anyone who is not a billionaire.
But the genocide also relies on the participation of bourgeois civil society. As we have seen over the last two years, bougiecrats are gleeful about participating in their own self-destruction.
Yes, Pharma propaganda, marketing, and psy-ops are very good. Over the last forty years, the average person just did not know about the dangers of vaccines. But at this point, there is more than enough information in the public square about the dangers of these products (just look around for gawdsakes!) for the bourgeoisie to opt out of shots. And yet they drive themselves to their own demise.
Self-preservation is the most fundamental of all human instincts, more primal even than sex. Yet the most educated class in human history has lost its ability to feel the urgent necessity to protect one’s own life and protect their kids from those who are harming them.
All of our elite institutions failed over the last two years. The fact that Harvard, Princeton, Yale, and Columbia require staff and students to be vaccinated with useless toxic Covid-19 shots shows that almost no one at these institutions is capable of understanding basic statistics nor risk benefit analysis. Why do these institutions even exist at this point?
I think there is a common factor that explains the participation of the bourgeoisie in their own self-destruction and the failure of all of our institutions to respond appropriately to a virus that could have been handled with existing off the shelf medicines.
We are in the midst of a mass-poisoning-event.
As I explained above, the children born after 1986 are massively over-vaccinated. But wide-scale vaccine programs began in the 1960s with polio and measles so anyone who lived through those eras may be affected as well (albeit to a lesser degree). 2,021 nuclear weapons tests during the Cold War likely made matters worse.
A strong case can be made that the societal chaos we are experiencing — from a lack of fundamental self-preservation instincts to the inability to think critically — is evidence of society-wide neurological injury. People are not experiencing ennui, they are experiencing too much aluminum (and other toxic chemicals) in their brains. There is likely a dose response relationship as well — the more shots, the more crazy things become. And with globalization and concentrated wealth, neurologically injured psychopathic billionaires can inflict unprecedented harm around the world and turn global politics into their own live action version of Orwell’s 1984.
So the task before us is this:
1. We must opt out of the crazy and say no to their toxic drugs;
2. Detox from the toxic chemicals that already exist in our bodies; and
3. Build the better sane world out of the ashes of the collapse of mainstream society.
July 8, 2022 Posted by aletho | Science and Pseudo-Science, Timeless or most popular | COVID-19 Vaccine | Leave a comment
John Deere Engineers Really Aiming To Build Battery-Powered Harvesters?
By P Gosselin – No Tricks Zone – 8. July 2022
It’s hard to believe that an internationally renowned company like John Deere would be led down such a dubious technical route: electric powered heavy agricultural equipment.
Consider that a battery for a typical electric car weights half a ton. Imagine what it would need to weigh for a machine that weighs over 25 tons.

With diesel, harvesters can run day and night. Image: John Deere Company
Perhaps it’s just lip service to placate idiot politicians and activist groups. I wonder if Caterpillar is thinking along the same lines: powering its massive excavators with batteries?
Here’s a post I found at Facebook from Will F. Leeman and that I’m having a hard time to believe it’s true:
For those of you that think electric vehicles are the answer- this is a true story from a farmer in the Midwest- and I’m reposting it-
A close friend farms over 10,000 acres of corn in the midwest. The property is spread out over 3 counties. His operation is a “partnership farm” with John Deere. They use the larger farm operations as demonstration projects for the promotion and development of new equipment. He recently received a phone call from his John Deere representative, and they want the farm to go to electric tractors and combines in 2023. He currently has 5 diesel combines that cost $900,000 each that are traded in every 3 years. Also, over 10 really BIG tractors.
JD wants him to go all-electric soon.
He said: “Ok, I have some questions. How do I charge these combines when they are 3 counties away from the shop in the middle of a cornfield, in the middle of nowhere?”
“How do I run them 24 hours a day for 10 or 12 days straight when the harvest is ready, and the weather is coming in?”
“How do I get a 50,000+ lb. combine that takes up the width of an entire road back to the shop 20 miles away when the battery goes dead?”
There was dead silence on the other end of the phone.
When the corn is ready to harvest, it has to have the proper sugar and moisture content. If it is too wet, it has to be put in giant dryers that burn natural or propane gas, and lots of it. Harvest time is critical because if it degrades in sugar content or quality, it can drop the value of his crop by half a million dollars or more.
It is analyzed at the time of sale.
It is standard procedure to run these machines 10 to 12 days straight, 24 hours a day at peak harvest time.
When they need fuel, a tanker truck delivers it, and the machines keep going. John Deere’s only answer is “we’re working on it.”
They are being pushed by the lefty Dems in the government to force these electric machines on the farmer.
These people are out of control.
They are messing with the production of food crops that feed people and livestock… all in the name of their “green dream.”
Look for the cost of your box of cornflakes to triple in the next 24 months…”
As mentioned above, a harvester weighs some 50,000 lbs, which means the battery would have to weigh in the neighborhood of 25,000 pounds (staying proportional to an e-car battery). Note that an e-car’s energy is used mostly for moving the vehicle on a hard even surface. For a harvester, energy is not only needed for moving it on high rolling resistance surfaces, but also for driving all the mechanical equipment onboard needed for cutting, conveying and chopping up the crop. Consequently an even bigger and heavier battery would be needed.
One problem today with modern tractors and harvesters is weight. Farmers are concerned about excessive weight because they don’t want their equipment excessively compacting the soil. Adding 15 tons or more of weight just for batteries for being able to power the machinery for just a couple of hours would be horribly inefficient.
Of course batteries for small garden equipment might make some sense, but for heavy machinery that needs to operate non-stop for hours and hours seems technically very impractical.
But with today’s green energy cult movement, where common sense has been thrown overboard to make room for ideology, it should not surprise us if the story really is true.
July 8, 2022 Posted by aletho | Malthusian Ideology, Phony Scarcity, Timeless or most popular | Leave a comment
Is a Colonoscopy Worth the Risk?
By Dr. Joseph Mercola | October 16, 2019
Knowing your potential risk for developing cancer can help you weigh the risks against the benefits of different tests for your situation. According to the American Cancer Society,1 more than 16.9 million people in the U.S. have a history of cancer. At least 1.9 million new cases will be diagnosed in 2022, which does not include a diagnosis of carcinoma in situ (noninvasive cancer).
The society estimates 609,360 people will die from cancer in 2022, which is about 1,670 deaths per day. The four most common types include lung, breast, prostate and colorectal cancer. One of the screening tests commonly prescribed to rule out colorectal cancer is a colonoscopy.
Colorectal cancer can start in the colon or in the rectum but the two types are grouped together since they have many of the same characteristics.2 The society estimates that in 2022 there will be 106,180 new cases of colon cancer diagnosed and 44,850 new cases of rectal cancer. Although it remains the third leading cause of cancer-related deaths in men and women, the rate has been dropping for several decades.3
According to the Colorectal Cancer Alliance,4 the five-year survival rate has been rising and there are more than 1 million colorectal cancer survivors alive in the U.S. Knowing your risk factors and making lifestyle changes to prevent the development of colorectal cancer are the basis of the most recently published Rapid Recommendation of The BMJ initiative.5
In Many Cases Routine Colonoscopies Are Unnecessary
The 2019 practice guidelines published in The BMJ 6 recommend physicians use a tool to estimate an individual’s potential risk for developing colorectal cancer in the next 15 years. The team recommends that only those who have a risk of 3% or greater should undergo screening tests.
Current guidelines recommend screening for everyone over the age of 50, without regard to their individual risk. At the age of 50, this is typically less than 3%.7 The international panel reviewed scientific evidence and research data to evaluate the risks versus the benefits of colonoscopies.
They found their recommendations could accurately be applied to healthy people from 50 to 79 years who expected to live another 15 years. The Centers for Disease Control and Prevention recommends colorectal cancer screening for those over 50.8
Using data from across the U.S., they found the number who were up to date with their screening went up 1.4% from 2016 to 2018, representing an additional 3.5 million people.
In addition to asking if screening made a difference in health outcomes, The BMJ initiative team also attempted to differentiate the type of testing best used to screen for colorectal cancer.9 They recommended that those with a 3% risk or greater over the following 15 years could choose from one of four screening options.
The first was a fecal immunochemical test (FIT) done every year, or every two years depending upon their risk factors. Patients may also choose a single sigmoidoscopy or, the weakest recommendation from the team, a single colonoscopy.
Possibility of Cancer Compared to Screening Hazards
From their examination of the evidence, the team believed a yearly FIT, sigmoidoscopy or colonoscopy could reduce the incidence of cancer while a FIT every two years may not have an effect on incidence over 15 years. They wrote:
“Based on benefits, harms, and burdens of screening, the panel inferred that most informed individuals with a 15-year risk of colorectal cancer of 3% or higher are likely to choose screening, and most individuals with a risk of below 3% are likely to decline screening. Given varying values and preferences, optimal care will require shared decision making.”
The team determined that the risks associated with colorectal cancer screening outweighed the benefits in many cases. For instance, the risk of death from a colonoscopy from one source was 1 in 16,318 procedures evaluated.10 In the same analysis, the researchers also found 82 suffered serious complications.
Colonoscopies Are Not Risk Free
Although a colonoscopy is supposed to help find early tumor growth, one study reported a 17% rate of missed diagnosis.11 Other risks associated with a colonoscopy include worsening stool patterns and contributing to the growth of colorectal polyps or tumors.
Perforation of the colon during the exam has an incidence of 0.2% to 5% and is widely recognized as a serious complication associated with a high morbidity and mortality rate.12 The risk of perforation rises with the age of the patient and the presence of two or more other health conditions. One study showed 51.9 people per 1,000 whose colons were perforated died within the first 14 days.13
Dysbiosis may occur after using harsh laxatives to prepare for a colonoscopy. A study published in Cell14 suggested even a short-term course of laxative use could trigger an immune response. Research on an animal model15 found treatment eliminated one family of beneficial gut bacteria and allowed another to flourish. Even two weeks after completing the laxatives the bacteria showed reduced diversity.
Many experts agree you should opt for the lightest level of sedation possible, or none at all, as full anesthesia increases risks. Those who have sleep apnea, are obese, have high blood pressure or diabetes are at increased risk from the anesthesia.16 Across the U.S. 34.4% of those undergoing a colonoscopy used anesthesia.17
The use of anesthesia was associated with a 13% increased risk of experiencing complications within 30 days of the procedure and specifically associated with an increased risk of perforations of the colon and/or a stroke. The risk of complications varied by area, with those in the Northeast reporting an increase of any complication of 12%, but among those performed in the West this increased to 60%.
Researchers who conducted one study found an increased risk of aspiration pneumonia.18 Another19 sought to determine if the procedure could be successfully completed without any sedation. Patients were given the option of undergoing a colonoscopy without premedication and then evaluated immediately following the procedure, two and five days later.
The researchers asked about the severity of pain and willingness to consider the procedure again without sedation. When questioned, only 5% experienced no pain; 41% had mild pain; 34% reported moderate pain and 20% said they experienced severe pain. However, despite the level of pain experienced, 73% were willing to repeat it without sedation and only 18% said they would request sedation the next time.
Equipment Contamination Another Risk of Colonoscopies
A real risk of undergoing an endoscopy of any nature is chance of improper sterilization of the flexible scope. David Lewis, Ph.D., and I discuss this in the short video above. One issue is the inability to thoroughly clean the inside of the scope.
Lewis describes a problem that he states is commonly experienced by physicians. During the examination the physician may be unable to see through the scope and is unsuccessful in the attempt to flush it using the air/water channel as it is clogged with human tissue from a past exam.20 The scope must be retracted and another one used.
Since endoscopes have sensitive equipment attached, they cannot be heat sterilized. Unfortunately, manufacturers have not been made to produce a scope with the ability to be heat sterilized. As Lewis points out:21 “We can put a Rover on Mars, surely we can build a flexible endoscope that we can put in an autoclave.”
These expensive tools are not disposable but require sterilization between each patient. Lewis reports that up to 80% of hospitals are sterilizing the flexible endoscopes with glutaraldehyde (Cidex). On testing, he finds this has complicated the process as it does not dissolve tissue in the endoscope but rather preserves it.
When sharp biopsy tools are run through the tube, patient material from past testing is scraped off and potentially carried into your body. This is why it’s important to find a clinic or hospital that uses peracetic acid to thoroughly sterilize the equipment by dissolving proteins found in the flexible endoscopes. Before scheduling any endoscopic examination call to ask how the equipment is sterilized between patients.
Tailor Lifestyle Choices to Reduce the Risk of Colon Cancer
Like many other types of cancer, colorectal cancer is often preventable. Research suggests only 5% to 10% of all cancer cases are due to genetic defects, while the rest are linked to environmental and lifestyle factors.22 The Mayo Clinic writes that one-third of the most diagnosed cancers in the U.S. could be prevented through diet and nutrition alone, i.e., with plenty of fresh fruits and vegetables.23
The extent that diet contributes to cancer death varies by the type of cancer, which researchers find is associated by as much as 70% in the case of colorectal cancer.24 For example, long-term exposure to chlorinated drinking water can increase the risk of leukemia, colorectal cancer and bladder cancer.
There are several strategies you can use to lower your risk of developing this potentially deadly disease as it is impacted by your diet, vitamin D levels, exercise and alcohol intake.
Sources and References
- 1 American Cancer Society Cancer Facts and Figures 2022
- 2 American Cancer Society, What Is Colorectal Cancer
- 3 American Cancer Society, Key Statistics For Colorectal Cancer
- 4 Colorectal Cancer Alliance, Determine Your Risk and Practice Prevention
- 5, 6 The BMJ, 2019;367: l5515
- 7 MedicalXpress, October 2, 2019
- 8 Centers for Disease Control and Prevention
- 9 The BMJ, 2019;367: l5515 Abstract
- 10 Annals of Internal Medicine 2006 Dec 19;145(12):880
- 11 Annals of Gastroenterology, 2015;28(1):94
- 12 World of Gastroenterology, 2010;16(4):425 Introduction
- 13 Journal of the National Cancer Institute, 2003;95(3):230
- 14 Cell, 2018;173(7):p1742
- 15 Nature, June 19, 2018
- 16 Medical News Today, January 5, 2018
- 17 Gastroenterology, 2015;doi.org/10.1053/j.gastro.2015.12.018
- 18 JAMA, 2013;173(7):551
- 19 Journal of Clinical Gastroenterology, 1998;26(4):279
- 20, 21 Bitchute
- 22, 24 Pharmaceutical Research, 2008;25(9):2097
- 23 Mayo Clinic
July 8, 2022 Posted by aletho | Science and Pseudo-Science, Timeless or most popular | Leave a comment
Featured Video

Israel furious at Trump over Turkey, Syria to invade Lebanon
or go to
Aletho News Archives – Video-Images
From the Archives
Bum Rap for the Rapa Nui
By Thomas Riggins | Dissident Voice | February 5, 2014
A new report in Science News Magazine (1-25-2014) by Bruce Bower details a reevaluation of the view that the Rapa Nuians, the native inhabitants of Easter Island (Rapa Nui), were responsible for the collapse of their population and society due to over exploitation of natural resources and the destruction of the rain forest on their island, a view recently popularized by Jared Diamond in his book Collapse (2005).
As Bower reports, the anthropologist Maria Mulrooney has published the results of her studies of the Rapa Nui culture (Journal of Archeological Science, December 2013) based on new radiocarbon dates from archeological sites on the island. She has concluded that after the clear cutting of the forest in the 1500s, to make room for agricultural production, the population of Rapa Nui remained sufficiently vibrant to carry on food production and continue their cultural development.
Exactly when the Rapa Nui arrived on Easter Island is unknown but it was on or before 1200 A.D. or so. Mulrooney maintains they had a thriving culture which was still going strong even after their “discovery” by the Dutch explorer Jacob Roggeveen on Easter Sunday 1722. This would indicate that they had not suffered “collapse” as a result of forest clearance. … continue
Blog Roll
-
Join 2,449 other subscribers
Visits Since December 2009
- 7,568,270 hits
Looking for something?
Archives
Calendar
Categories
Aletho News Civil Liberties Corruption Deception Economics Environmentalism Ethnic Cleansing, Racism, Zionism Fake News False Flag Terrorism Full Spectrum Dominance Illegal Occupation Mainstream Media, Warmongering Malthusian Ideology, Phony Scarcity Militarism Progressive Hypocrite Russophobia Science and Pseudo-Science Solidarity and Activism Subjugation - Torture Supremacism, Social Darwinism Timeless or most popular Video War Crimes Wars for IsraelTags
Afghanistan Africa AIPAC al-Qaeda Australia BBC Benjamin Netanyahu Brazil Canada CDC Central Intelligence Agency China CIA CNN Covid-19 COVID-19 Vaccine Donald Trump Egypt European Union Facebook FBI FDA France Gaza Germany Google Hamas Hebron Hezbollah Hillary Clinton Human rights Hungary India Iran Iraq ISIS Israel Israeli settlement Japan Jerusalem Joe Biden Korea Latin America Lebanon Libya Middle East National Security Agency NATO New York Times North Korea NSA Obama Pakistan Palestine Poland Qatar Russia Sanctions against Iran Saudi Arabia Syria The Guardian Turkey Twitter UAE UK Ukraine United Nations United States USA Venezuela Washington Post West Bank WHO Yemen Zionism
 Aletho News
Aletho News- US-backed deal with Israel has ‘no legitimacy’, top Lebanese cleric warns
- Israeli occupation forces advance in southern Lebanese towns after truce deal with Beirut
- Abelardo De la Espriella’s Victory Renews Pressure on Venezuela
- Israel furious at Trump over Turkey, Syria to invade Lebanon – w/ Col. Macgregor
- IRGC says it struck US military positions, warns of broader response
- Russia stops record number of Ukrainian drones overnight – MOD
- Denmark admits ‘no evidence’ for Russian drone hysteria
- Washington agreement ‘will not pass’: MP Fadlallah
- Iran mocks US for ‘solving’ domestic hunger problem, lecturing others on issue
- Germany, Israel hold joint naval drill off Haifa amid Gaza genocide
- If Americans Knew
- Israel kills Gaza’s public servants again – this time it’s police – Daily Update
- Four Reasons the Netanyahu-Backed Plan to ‘End’ U.S. Military Aid to Israel Is a Scam
- Archbishop of Canterbury vows to help Palestinians achieve ‘freedom you deserve,’ calls for end to Israeli occupation
- The scars left behind by Israel’s white phosphorus in Lebanon
- Drones and decomposing babies: What’s in UN report on Israel’s genocide of Palestinian children
- Crimson Thread: The new Israeli separation wall that cuts through the ‘breadbasket of Palestine’
- Gaza ceasefire talks back to square one as Israel changes the rules – Daily Update
- The NDAA Proposed Merger of the U.S. and Israeli Military is Strategically Unwise and Inherently Unconstitutional
- Victories by Pro-Palestinian Democrats Show the Party’s Shift on Israel
- Massie moves to strike $3.3B in Israel military aid from the budget
- No Tricks Zone
- Lousy Station Siting: Swirling Controversy Surrorunds Germany’s Latest “New Alltime Record High” Temperature
- 2025 Study: Cloud Effects Reduce Downwelling Longwave Radiation, Overriding The CO2 Impact
- 3 New Studies Find Increasing Trends In Solar Radiation Since The 1980s – Easily Explaining Warming
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
Contact:
atheonews (at) gmail.com
Disclaimer
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.
