Omicron variant places vaccine efficacy in question – but evidence for enduring power of natural immunity remains strong
By Will Jones • The Daily Sceptic • December 1, 2021
Moderna boss Stephane Bancel has said he expects a “material drop” in the efficacy of his company’s vaccine against the new Omicron variant. He told the Financial Times:
I think it’s going to be a material drop. I just don’t know how much because we need to wait for the data. But all the scientists I’ve talked to … are like, ‘This is not going to be good.’ … There is no world, I think, where [the effectiveness] is the same level … we had with Delta
He also said it would take months for drugs companies to update the vaccines. This means any Omicron wave is likely to have arrived, peaked and receded before the shots can be manufactured and widely administered.
A more sanguine Boris Johnson claimed on Tuesday afternoon that there are good grounds for believing third vaccine doses will give “considerable protection” against the Omicron variant. This view was given support by Dr Ugur Sahin, co-founder of BioNTech and one of the scientists behind the Pfizer vaccine, who said he remains optimistic that the jab will continue to provide protection against severe disease (though, tellingly, did not mention protection against infection). “Our message is: Don’t freak out, the plan remains the same: Speed up the administration of a third booster shot,” he told the Wall Street Journal – though some might point out Dr Sahin may have other reasons for wanting to “speed up” the distribution of his product.
SAGE member Professor John Edmunds has warned that reported infections are rising rapidly in South Africa, where the new variant was first detected last week. While data from Gauteng province, where the new variant was discovered on November 24th, showed a slight decline on Sunday and Monday, this may be a weekend effect, and there has certainly been a sharp rise overall in the past eight days. It is worth keeping an eye on the region to see how it develops.

Daily new reported infections in Gauteng Province, South Africa
It has also transpired in the last couple of days that the variant was already in other countries including the Netherlands several days prior to its discovery in South Africa. Nonetheless, the WHO has said the earliest known specimen of the variant was collected on November 9th in southern Africa.
While vaccines may work less effectively against Omicron than against earlier variants such as Delta (efficacy against which, particularly after several months, is anyway disputed), natural immunity arising from previous infection is looking more robust.
Two new research papers, one in the NEJM and one in the Lancet, provide further compelling evidence of the protective power of natural immunity. In the NEJM paper, researchers from Qatar report on reinfections in the country during the back-to-back Alpha- and Beta-associated surges in the first half of 2021. Examining medical records from all 353,326 people who received a positive PCR test in the country between February 28th 2020 and April 28th 2021 (excluding 87,547 people who had received a vaccine), they found that the odds of severe disease on reinfection were 0.12 times those at first infection (95% confidence interval [CI]: 0.03-0.31), which translates to 88% protective efficacy. There were no cases of critical disease or death on reinfection versus 28 and seven respectively at first infection, giving 100% efficacy against these outcomes (though the small numbers here resulted in large confidence intervals). Putting the three outcomes of severe, critical, or fatal disease together, they found odds of 0.1 on reinfection compared to first infection (CI: 0.03-0.25), for an efficacy of 90%.
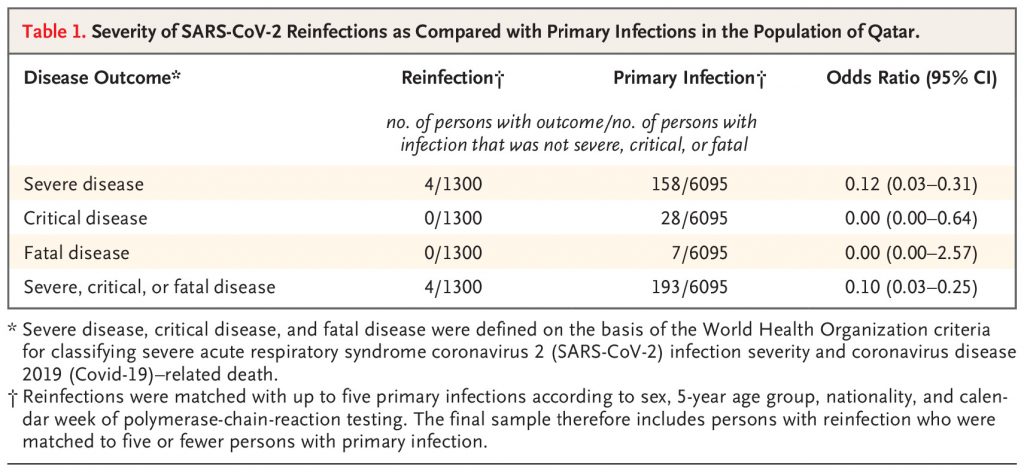
Four reinfections were severe enough to require hospitalisation, they say, but none led to ICU admission or ended in death. “Reinfections were rare and were generally mild, perhaps because of the primed immune system after primary infection,” they write.
They add that in earlier studies they had looked at the protective efficacy of natural infection against reinfection and estimated it at 85% or greater. Putting these figures together, this means prior infection has an efficacy of at least 98.5% against severe reinfection when compared to the immunologically naïve with no previous infection or vaccination. Does this mean that infection with SARS-CoV-2 will behave immunologically like the other ‘common cold’ coronaviruses and provide long-term immunity against severe illness, even if protection against mild reinfection fades, they ask? “If this were the case with SARS-CoV-2, the virus (or at least the variants studied to date) could adopt a more benign pattern of infection when it becomes endemic,” they suggest.
The Lancet paper supports these tentative conclusions. Reviewing all relevant papers on the online medical database PubMed, the authors Noah Kojima and Jeffrey D Klausner from the University of California find seven studies which show the risk of infection decreases by 80·5-100% for the previously infected compared to the immunologically naïve.
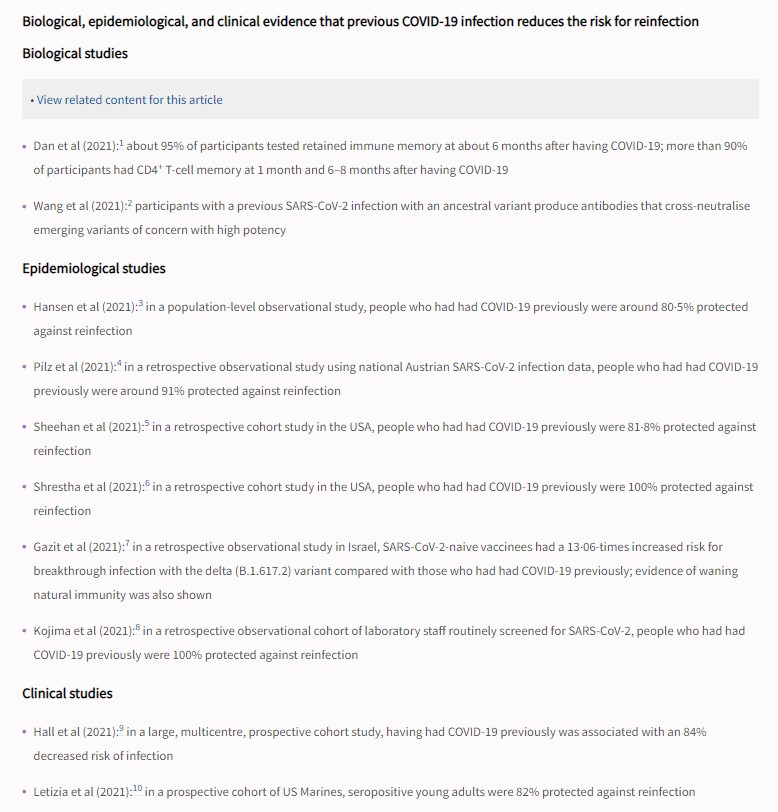
Kojima and Klausner make the case for the superiority of natural immunity versus vaccine immunity, including where variants are concerned.
It is known that SARS-CoV-2 infection induces specific and durable T-cell immunity, which has multiple SARS-CoV-2 spike protein targets (or epitopes) as well as other SARS-CoV-2 protein targets. The broad diversity of T-cell viral recognition serves to enhance protection to SARS-CoV-2 variants, with recognition of at least the Alpha (B.1.1.7), Beta (B.1.351), and Gamma (P.1) variants of SARS-CoV-2. Researchers have also found that people who recovered from SARS-CoV infection in 2002-03 continue to have memory T cells that are reactive to SARS-CoV proteins 17 years after that outbreak. Additionally, a memory B-cell response to SARS-CoV-2 evolves between 1·3 and 6·2 months after infection, which is consistent with longer-term protection.
Some people who have recovered from COVID-19 might not benefit from COVID-19 vaccination. In fact, one study found that previous COVID-19 was associated with increased adverse events following vaccination with the Comirnaty BNT162b2 mRNA vaccine (Pfizer-BioNTech). In addition, there are rare reports of serious adverse events following COVID-19 vaccination. In Switzerland, residents who can prove they have recovered from a SARS-CoV-2 infection through a positive PCR or other test in the past 12 months are considered equally protected as those who have been fully vaccinated.
Given this evidence, they argue, “policy makers should consider recovery from previous SARS-CoV-2 infection equal to immunity from vaccination for purposes related to entry to public events, businesses, and the workplace, or travel requirements”.
Based on the studies to date, natural immunity appears to convey 80-90% protection against reinfection and, on top of that, 90% protection against serious disease once reinfected, giving around 99% protection against serious reinfection. This protection doesn’t appear to have waned over time or against new variants in the way vaccine protection has done. Omicron may tax the vaccines, but on the evidence so far it seems unlikely to tax natural immunity in the same way.
The State of Emergency, Coercive Medicine, and Academia

By Maximilian C. Forte | Résistance Scolaire – Québec -Academic Resistance | December 1, 2021
“Two weeks to flatten the curve,” is what we heard across Canada1 just after March 11, 2020, when the World Health Organization unilaterally declared a global “pandemic” according to new criteria developed in 2009 that emphasized transmissibility over lethality.2 We are now approaching two years of a crisis that is routinely and deceptively blamed on “Covid”. Politicians, public health officials, and the mass media have made persistent pronouncements that tended towards the inflation of grim numbers and the exaggeration of threats.3
The State of Emergency and its Consequences
 Building on expanded threat perception, authorities have deliberately promoted fear, induced panic, and created stress.4 With the public suffering an epidemic of fear bordering on mass psychosis,5 states have multiplied and escalated the number and types of restrictions, few of which have the support of even a single published scientific study6: quarantining the healthy; school closures; shutting down small businesses; travel bans and internment of returning citizens; masking; social distancing; fines; curfews; vaccine passports7; and now, mandatory vaccination campaigns that threaten the livelihoods of hundreds of thousands across Canada, including students, support staff, and professors, and impeding non-vaccinated Canadians from leaving the country.8 In the case of Quebec, such measures have been advanced under a State of Emergency deployed in accordance with the Public Health Act,9 which has seen the “emergency” renewed every seven days. Since the “emergency” was first declared on March 13, 2020, it was renewed 84 times (to October 27, 2021), and continues being renewed without consultation and approval by the National Assembly.10 On each occasion, the Government of Quebec has failed to explain the nature or even the existence of a situation that merits classification as an “emergency”.11
Building on expanded threat perception, authorities have deliberately promoted fear, induced panic, and created stress.4 With the public suffering an epidemic of fear bordering on mass psychosis,5 states have multiplied and escalated the number and types of restrictions, few of which have the support of even a single published scientific study6: quarantining the healthy; school closures; shutting down small businesses; travel bans and internment of returning citizens; masking; social distancing; fines; curfews; vaccine passports7; and now, mandatory vaccination campaigns that threaten the livelihoods of hundreds of thousands across Canada, including students, support staff, and professors, and impeding non-vaccinated Canadians from leaving the country.8 In the case of Quebec, such measures have been advanced under a State of Emergency deployed in accordance with the Public Health Act,9 which has seen the “emergency” renewed every seven days. Since the “emergency” was first declared on March 13, 2020, it was renewed 84 times (to October 27, 2021), and continues being renewed without consultation and approval by the National Assembly.10 On each occasion, the Government of Quebec has failed to explain the nature or even the existence of a situation that merits classification as an “emergency”.11
By displacing the political onto the medical, in biologizing and thus naturalizing political acts, both governments and the media typically assign blame to “Covid,” the “pandemic,” or the “unvaccinated,” to justify authoritarian emergency measures and to rationalize the ensuing social upheaval. But the virus is just a virus. The virus is neither a politician, a legislator, an economic adviser, a public health official, a corporate CEO, nor is it a media executive. The virus has not been “managed”: it has been worked.
The social, economic, political, medical, psychological, and cultural damage wrought by emergency measures, though inadequately documented and tallied in Canada, appears to be both vast and ongoing. At least 36 studies explain why our unnecessarily extended period of lockdowns not only failed to control the virus or lower mortality, but may even have increased excess mortality.12 Quebec’s Minister of Health, Christian Dubé, publicly acknowledged the impacts of the emergency on delayed treatments and surgeries, often for illnesses far more severe than Covid.13 The health system’s lopsided emphasis on Covid, coupled with fear that kept many patients with severe illnesses away from hospitals and clinics, created such a backlog of surgeries and treatments that emergency rooms exploded far beyond capacity by the summer of 2021, as reported Covid infections plummeted. Quebec’s Ministry of Health estimated that up to 4,000 people have gone undiagnosed with cancer as a result of a sharp decline in mammograms, pap smears and colorectal cancer screenings.14 Across Canada, projected cancer cases are expected to surge in the thousands.15 During the lockdowns, deaths caused by opioid overdoses rose by 88% in 2020 when compared to 2019.16 Alcohol abuse, suicides, and even homicides in domestic settings all increased substantially. Statistics Canada reported that during this emergency period, deaths from “accidental poisonings” (substance abuse) reached a new high, while the numbers for deaths caused by alcohol abuse, and drug use all increased, particularly for younger Canadians.17 StatCan noted that “the economic, social, and psychological impacts” as well as “the public-health measures in place may have played a role in increasing alcohol use”.18 In North America, lockdowns had a disproportionate impact on minority youths in terms of education and employment.19 Families with children at home reported dramatic degrees of deteriorated mental health.20 The economic devastation wrought by the lockdowns further increased the social, psychological, and medical harms.21 In Montreal, the homeless population doubled in size just from March 2020 to October 2021.22 Canada’s federal debt increased by 66%; provinces and even most universities also posted vastly increased deficits; and, hundreds of thousands of retail businesses were expected to permanently close.23 Both the savings and the ability to save for working-class Canadians simply vanished, and personal debt levels skyrocketed; women and minorities were among those hit hardest.24
How is public health served by spreading fear, creating stress, inducing anxiety, and terminating the livelihoods of those who do not comply with arbitrary and indiscriminate measures? What kind of public health is it that assaults the dignity of those to be saved, creating divisions, escalating tensions and conflict? We have certainly come a long way from “two weeks to flatten the curve”. Today, federal employees, healthcare workers, and educators across Canada are being suspended and fired, sentenced to a form of social and economic internal exile, thus effectively rendered aliens in a country which also traps them within its borders. Citizens are now effectively criminalized based on their medical status.
Coercive Medicine
All of the devastation, displacement, and divisions have been to what end? What is it about the nature of this particular virus that makes it so spectacularly special that extreme measures are not only said to be warranted, but must also be continually multiplied and extended? Why are these “public health” measures so narrowly focused on only one specific solution—universal “vaccination”—when that “solution” has been shown to solve so little at the core of this crisis?
Encouraged by government and the media to conflate the two, most Canadians seem to have trouble remembering the difference between transmissibility (i.e., infectiousness) and lethality, such that any report of “cases” immediately sparks fears of impending and generalized death. The appearance of a “case” in an institution is called an “outbreak,” an alarmist term that inspires fear. Yet it is still true that official statistics reveal that this particular coronavirus, with its non-distinctive symptoms, is responsible for the deaths mostly of the very elderly, and even then those with advanced co-morbidities. In Canada as a whole, 63% of reported Covid deaths occurred among those aged 80 years or more; that number increases to 83% when we include those aged 60 years or more.25
This virus was never a lethal threat to the general population, but it has been governed as if it were. The global survival rate for Covid, for persons under the age of 70, is 99.83%; others report that it is as high as 99.95% (without “vaccination”), and for those under 45 years of age the infection fatality rate is almost zero.26 For the vast majority of the infected, 76.5%, Covid produces no symptoms at all, and for 86.1% no symptoms specific to Covid; for most of the rest, the symptoms are mild.27 The Norwegian government and the UK parliament have both recognized that Covid has fallen in lethality when compared with the seasonal flu.28 What then is the medical basis for instituting emergency measures, imposed on the total population? In early 2020, a few national leaders declared a “war on the virus”—but how do the facts of the virus justify use of tools of war, such as a state of emergency?
Throughout this crisis, premised on the generalization of the threat of death, we have nonetheless seen a differential and selective valuation of deaths.29 Death, rather than the possibilities for normal life, has been greatly emphasized. Regardless of co-morbidities, those who died with Covid were almost always reported as “Covid deaths,” even if Covid was not the cause of death. Yet, when persons have died after receiving injections, their deaths are usually attributed to co-morbidities, and they are not publicly reported by the media or state spokespersons as “vaccine deaths”. Some deaths, we discovered, matter more than others.
Having succeeded in spreading generalized fear of “Covid death,” the authorities have singled out that one “solution” of theirs: inoculation of the entire population, regardless of age, health, or natural immunity.30 They have denied effective early treatment of symptoms. They have obstinately ignored the fact that natural immunity has been proven to offer longer-lasting, broader and stronger protection than the current crop of novel gene therapies.31 We have been told, with absolute conviction, that these experimental gene therapies are “safe and effective”.32 Less assuring, however, has been the authorities’ refusal to share trial data with scientists.33 Doctors and scientists who question the “vaccine” dogma are censored, silenced, suspended, or fired, even as hundreds of thousands of doctors and healthcare workers worldwide34 have precisely detailed why these novel therapies are neither safe nor effective,35 with abundant empirical support and a growing number of published studies.36 Between the US and UK alone, nearly 20,000 persons have already died from the injectables, and more than two million people have suffered severe adverse reactions, according to officially published data.37 Yet the injectables themselves offer, at best, a 1.3% reduction in absolute risk of becoming ill from Covid. “Herd immunity” via “vaccination” is clearly impossible,38 particularly when the “vaccines” in question provide no sterilizing immunity, and when the virus has ample natural reservoirs in the wider animal population.
Given that the “fully vaccinated” can still be infected and transmit the virus among themselves, the stated logic for the domestic “vaccine passport” system has been nullified39—yet the mandate remains in place. Even with such mandates in place on US college campuses, with almost all students, staff and faculty injected, “outbreaks” have occurred.40 It should now be obvious that the “vaccine passport” is not a public health measure designed to “protect” people and “save lives”. Instead, it is a political measure designed to maximize control and foment divisions among the wider population, deflecting blame away from the state and toward the new dangerous Other, the “unvaccinated”.41
Questions for Academia
Universities in Quebec and across Canada have internalized the “vaccine passport” system, notwithstanding public knowledge of the facts as shown above. They have done so even when aware of the differential impact on religious and ethnic minorities.42 Institutions that have adopted principles of “equity, diversity, and inclusion,” have failed the first real test of their policies. In Canada, as in the US, Black and Indigenous communities are among the most “vaccine hesitant” or “vaccine resistant” of all ethnic groups.43 However, given that the “war on the virus” has become a de facto war on the people, a larger segment of the national population has been created as a new minority suffering discrimination, one that has been as stigmatized as it has been caricatured.44 Where do academics stand here?
If “vaccination” was intended as a means of exiting the WHO’s declared pandemic, that has clearly not happened. Is it in fact intended as an exit, or as a gateway to something else? This is just one of many questions that academics should have been addressing, instead of cowering in fear before Covid, deferring to political authority, and clamouring for still more draconian restrictions.
As academics who have committed ourselves to ethics, integrity, and honesty, do we not see anything problematic in what is happening before our very eyes? Are we not disturbed by what is being committed in our name, for this alleged “common good” which none of us were ever called upon to define? What “common good” is it that thrives on coercion, exclusion, and works towards the monopolistic profits of Pfizer, which has an established criminal history,45 and Moderna, which has never before produced a vaccine?
Whether one is “adequately vaccinated” or not—according to the shifting standards and definitions of the moment—is not the core issue that should concern us. What should concern us is that the legal rights of all citizens are being transformed into temporary privileges; that coercion trumps democratic participation; that key institutions—including academic ones—are being rapidly conscripted for political purposes, and their basic missions are being undermined and distorted.
While many believe and assert that a “public health emergency” must limit basic human freedoms, it is precisely when faced by a real or alleged emergency that we need to be most careful and protective of human rights. Basic human rights are inalienable, and cannot be “suspended” because of any war, disaster, or other emergency.46 Bodily autonomy,47 informed consent, and by extension not being subjected to invasive testing or genetic treatment, are among the key rights which have been suspended or violated.48 Rights of conscience, as guided by religious and spiritual beliefs, along with the right to political beliefs and freedom of expression, must also be protected.49
Did we as scholars anticipate living in a country where our universities would purge tenured professors, fire support staff, and expel registered students (even escorting them off campus in front of other students), because of their health status, their innate biological characteristics, and their desire to preserve their privacy and bodily autonomy free from discrimination? When did we become comfortable with violating the right to an education and the right to work? How did we come to accept this discrimination, this deliberate segregation of a category of persons from the rest of society? Did we predict that one day we would see a demarcated group of Canadians being targeted not just for segregation, discrimination, and demonization, but that they would also be denied their livelihoods? Did we imagine that leaders, from the Prime Minister to the Premier, would verbally assault this same group and use the most threatening and dehumanizing language against it? This is happening, right now, all around us, right in front of us. Now that history has found us, how do we meet history? Do we even stop to take notice? When are we going to stand up and speak out?
In Canadian universities, many if not most scholars and students are not living up to goals of offering critical and independent perspectives on a crisis of momentous proportions. Ethics, freedom of choice, privacy, and democracy, have not been defended by our universities. Instead what has risen is a culture of silence, with some willingly reinforcing an instant orthodoxy that could only have been produced by widespread fear and unconditional trust in the authorities. Is this what we expect from our universities? Should students and professional scholars not be dedicated to developing independent, critical analytical abilities? Should they be trusting the authorities to the point of silently acquiescing with or even staunchly upholding their edicts and decrees? By not defending basic ethical principles of bodily autonomy, informed consent, and freedom of choice, and by even going as far as denying these rights, universities are actively engaged in violating human rights that are protected by the Charter of Rights and Freedoms and by international human rights law. By not challenging mandatory “vaccination” and “vaccine passports,” we allow a ready-made canon, furnished by the state and media, to supplant our own investigation and knowledge production. Worse yet, by directly engaging in censoring and silencing scientists, and by allowing intimidation and mobbing, universities in Canada appear to be engaging in intellectual, moral, and ethical suicide. What kind of university will emerge from this process? Can we even properly speak of a “university” in such a context?
In our universities, we have looked on silently as the media, backed by powerful private interests and our own bureaucrats, actively censor fellow scientists’ research and stifle critical questioning, to the benefit of transnational corporations such as Pfizer.50 We have watched tenure being invalidated, rendered null and void according to the whims of the state, as the terms and conditions of our employment are radically altered to depend—in clear violation of the Privacy Act—on disclosure of our medical status.51 Professors have been involuntarily deputized as auxiliary police forces, made to enforce mask mandates in their classrooms. Simply questioning the logic of such measures, and asking to see the scientific evidence that supports them, risks censure for “spreading misinformation”. Faculty unions have turned against faculty who resist the mandates, while most faculty either remain silent, or loudly support harsh restrictions.52 Academic freedom is in greater peril in Canada today than it ever has been.53 We have witnessed science succumb to the dictates of politics. As one concerned epidemiologist observed, with obvious restraint: “there will be lasting consequences from mingling political partisanship and science during the management of a public-health crisis”.54
In both medicine and international human rights law, the principle of voluntary and prior informed consent is fundamental and inviolable. Yet without adequate information, consent cannot be informed. The denial of informed consent is a grave violation of human rights, as established under multiple instruments of international human rights law. Coercion is also a denial of informed consent. Penalties, punishments, and threats offer the same kind of “choice” that is offered during the psychological torture of detainees under abusive interrogation. It is strange medicine that restricts family members from gatherings, worshippers from communing, workers from working—that creates unemployment and targets dissenting persons’ ability to clothe, house, and feed their families. “Vaccine hesitant” adults are treated as children, with medicine forced down their throats by a paternalistic state. Even if we had been dealing with actual children, in Canada we were supposed to have moved past our history of such abusive treatment. Mandates and restrictions have been overbearing, indiscriminate, redundant, authoritarian, arrogant, and punitive. Our strange medicine is the outcome of the politics of dispossession, which has reached such an extreme that it would have people sign off the rights to their immune system to a giant pharmaceutical corporation with a criminal record.
In such an environment, “vaccine refusal” is treated as tantamount to treason, an expression of “selfishness,” and a “threat to the community”. Yet a more sober and considered view would highlight the realization that, “mandatory vaccination amounts to discrimination against healthy, innate biological characteristics, which goes against the established ethical norms and is also defeasible a priori”.55
Independent, rational, critical analysis that seeks truth has been supplanted by deference to authority and its alternative “science”: the science of politicians, technocrats, the media, and lawyers. This alternative science has us thinking what was previously unimaginable, and doing what was previously unacceptable: never do you quarantine the healthy; never do you vaccinate the immune; never do you inject new treatments into children who do not need them;56 never do you vaccinate during a pandemic; and, never do you try new drugs on pregnant women.57 As we think the unthinkable, collaborate with the unimaginable, and support the unsupportable, we as academics are conspiring with those who demand we assert the unquestionable.
This has to change, and it has to change now.
1 “Here’s what each Canadian province is doing to ‘flatten the curve’ of the novel coronavirus,” Toronto Star, March 15, 2020; “Our window to flatten the COVID-19 curve is narrow, says Dr. Theresa Tam,” The Canadian Press, March 15, 2020.
2 The WHO’s original definition of a pandemic specified simultaneous epidemics worldwide that were marked by “enormous numbers of deaths and illnesses”; this definition was changed just prior to the declaration of the 2009 swine flu “pandemic,” by deleting the criteria of severity and high mortality. See: Ron Law, “[Response] WHO and the pandemic flu ‘conspiracies’,” British Medical Journal, June 4, 2010, p. 340; Peter Doshi, “The Elusive Definition of Pandemic Influenza,” Bulletin of the World Health Organization, 89, pp. 532–538.
3 ON PCR TESTS AND THE PRODUCTION OF “CASES”:
One of the means by which numbers were inflated lies in the use of inappropriate testing procedures and their interpretation. Positive results using reverse-transcription polymerase chain reaction (RT-PCR, or just “PCR tests”) were reported as “cases,” a term that denotes a patient receiving medical attention, when in most cases persons did not even show symptoms. Numerous scientists criticized the use of PCR tests, beginning with Dr. Kary Mullis who won the 1993 Nobel Prize for inventing the PCR testing process now in wide use to diagnose coronavirus infection. Dr. Mullis is on record for challenging the utility of PCR tests: “it’s just a process that’s used to make a whole lot of something out of something. That’s what it is. It doesn’t tell you that you’re sick and it doesn’t tell you that the thing you ended up with really was going to hurt you or anything like that”—see: Patrick Howley, “Inventor of PCR Test Said Fauci ‘Doesn’t Know Anything’ and is Willing to Lie on Television,” National File, March 15, 2021. The World Health Organization advised caution in using PCR testing, warning of the potential for increased false positives and recommending that PCR testing be used only as “an aid for diagnosis”—see: “WHO Information Notice for Users 2020/05: Nucleic acid testing (NAT) technologies that use polymerase chain reaction (PCR) for detection of SARS-CoV-2,” World Health Organization, January 20, 2021.
The original publication which advocated using PCR testing for SARS-CoV-2 (the “Corman-Drosten paper”) came in for severe criticism from 22 scientists who identified 10 fatal flaws with the paper, including its rush to publication after a single day of peer review. The Corman-Drosten paper, which influenced policy worldwide, originally recommended using 45 cycles of thermal amplification of swab samples for SARS-CoV-2—yet a published study reported that even at 35 cycles of amplification, up to 97% of the positive results using RT-PCR tests would be false (see: Rita Jaafar, Sarah Aherfi, Nathalie Wurtz, et al. “Correlation Between 3790 Quantitative Polymerase Chain Reaction–Positives Samples and Positive Cell Cultures, Including 1941 Severe Acute Respiratory Syndrome Coronavirus 2 Isolates,” Clinical Infectious Diseases, 72(11), 2021). The Corman-Drosten article has since been subjected to three stages of correction. See: Victor M. Corman, Christian Drosten, et al., “Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR,” Eurosurveillance, 25(3), 2020. For the critical review of the Corman-Drosten paper, see: Pieter Borger, Bobby Rajesh Malhotra, Michael Yeadon, et al., “External peer review of the RTPCR test to detect SARS-CoV-2 reveals 10 major scientific flaws at the molecular and methodological level: consequences for false positive results,” Corman-Drosten Review Report, January 2021; also see: Peter Andrews, “A global team of experts has found 10 Fatal Flaws in the main test for Covid and is demanding it’s urgently axed. As they should,” RT, December 1, 2020, and, Peter Andrews, “Flawed paper behind Covid-19 testing faces being retracted, after scientists expose its ten fatal problems,” RT, December 9, 2020.
The practical utility of using PCR testing to gauge infectiousness was also called into question by various public health agencies. The US Centers for Disease Control and Prevention (CDC) cautioned that, “detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms” (“CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel,” CDC, July 7, 2021, p. 38). The Department of Health of the Government of Australia cautioned, “that PCR tests cannot distinguish between ‘live’ virus and noninfective RNA” (“Novel coronavirus (COVID-19): Information for Clinicians,” March 2020, p. 2). This was echoed by Ireland’s specialist agency for the surveillance of communicable diseases, which stated: “PCR does not distinguish between viable virus and non-infectious RNA,” and warned of the dangers of false positives—see page 10: “Guidance on the management of weak positive (high Ct value) PCR results in the setting of testing individuals for SARS-CoV-2,” HSE Health Protection Surveillance Centre (HPSC), July 7, 2021. “RT-PCR detects RNA, not infectious virus”: this is stated at the outset of a published study supported by the Public Health Agency of Canada and its National Microbiology Laboratory—see: Jared Bullard, Kerry Dust, Duane Funk, James E Strong, et al., “Predicting Infectious Severe Acute Respiratory Syndrome Coronavirus 2 From Diagnostic Samples,” Clinical Infectious Diseases, 71(10), November 15, 2020, pp. 2663–2666. For similar cautions, see: “Interpreting the results of Nucleic Acid Amplification testing (NAT; or PCR tests) for COVID-19 in the Respiratory Tract,” BC Centre for Disease Control/BC Ministry of Health, April 30, 2020.
In November of 2020 in Portugal, a verdict from the Lisbon Appeal Court ruled that a positive PCR test result could not definitively prove that someone was infected with SARS-CoV-2. In addition, the court cited published research that reported that, at the high cycle thresholds that were commonly used, the rate of false positives could be as high as 97%. See: Proc. 1783/20.7T8PDL.L1, Tribunal da Relação de Lisboa, November 11, 2020, and Peter Andrews, “Landmark legal ruling finds that Covid tests are not fit for purpose. So what do the MSM do? They ignore it,” RT, November 27, 2020.
In 2007, in an article in The New York Times titled, “Faith in Quick Test Leads to Epidemic That Wasn’t,” what was believed to be an epidemic of whooping cough in New Hampshire turned out just to be a common cold—what is instructive is how health officials came to make this mistake which created what the paper called a “pseudo-epidemic”. At the centre of this pseudo-epidemic was reliance on PCR testing; experts quoted in the paper called them unreliable, and stated that they should not be used. PCR testing was applied to a sickness that had non-distinctive symptoms. This mistake led to further mistakes, that were not seen as mistakes: “Yet, epidemiologists say, one of the most troubling aspects of the pseudo-epidemic is that all the decisions seemed so sensible at the time”. Doctors tested anyone with a cough or runny nose, and the PCR tests returned false positive results for whooping cough. See: Gina Kolata, “Faith in Quick Test Leads to Epidemic That Wasn’t,” The New York Times, January 22, 2007.
In July of 2021 the CDC announced that, “after December 31, 2021, CDC will withdraw the request to the U.S. Food and Drug Administration (FDA) for Emergency Use Authorization (EUA) of the CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel, the assay first introduced in February 2020 for detection of SARS-CoV-2 only,” in part because of the test’s inability to distinguish between SARS-CoV-2 and seasonal flu (“Lab Alert: Changes to CDC RT-PCR for SARS-CoV-2 Testing,” CDC, July 21, 2021).
ON COVID DEATH STATISTICS AND EXAGGERATION OF THREATS:
Official reports on the numbers of deaths ascribed to Covid, have also been revealed to be highly controversial. In most countries, “Covid deaths” included both those who died with Covid, and those who specifically died from Covid, thus producing the largest possible number. On April 20, 2020, the World Health Organization published its “International Guidelines for Certification and Classification (Coding) of Covid-19 as Cause of Death”. The WHO advised public health authorities that when Covid-19 is the “suspected”, “probable,” or even just the “assumed” cause of death, then it must always be recorded in death certificates as the “underlying cause of death” (see pps. 3-7). This was to be done even if a decedent suffered from serious chronic illnesses. Indeed, comorbidities such as diabetes, heart disease, cancer, or chronic non-Covid respiratory infections, should only be indicated as a “contributing cause” lower down in a death certificate. The WHO added: “Always apply these instructions, whether they can be considered medically correct or not” (p. 8).
In Quebec, both the Premier, François Legault, and the Director of Public Health, Horacio Arruda, publicly admitted that Quebec’s Covid ceath numbers were higher than Ontario’s, because in Quebec—regardless of the actual cause of death—once one had tested positive for Covid, the death was attributed to Covid. As Dr. Arruda explained, “Anytime, in Quebec, someone dies from cancer or another disease, if they have COVID-19 it will be counted as COVID-19”: Kelly Greig & Selena Ross, “Legault asks if Ontario’s under-counting COVID-19 deaths, drawing scientist’s ire,” CTV News, October 29, 2020.
Such practices, as recommended by the WHO and widely followed internationally, were subject to a successful legal challenge in Portugal. On May 15, 2021, a ruling from the Tribunal Administrativo de Círculo de Lisboa found that verified deaths from SARS-CoV-2 amounted to just 0.9% of all reported Covid deaths—that is, 152 deaths rather than the 17,000 plus Covid deaths reported by the state. See: Mordechai Sones, “Lisbon court rules only 0.9% of ‘verified cases’ died of COVID, numbering 152, not 17,000 claimed,” America’s Frontline Doctors, June 23, 2021; the ruling can be accessed here. In Italy there were also questions stemming from data published by the government’s national institute of health—Istituto superiore di Sanità—regarding the alleged Covid mortality rate; according to one interpretation, only 2.9% of registered Covid deaths from the end of February 2020 were due to Covid as such, thus of the 130,468 official Covid deaths, only 3,783 can be attributed to Covid alone—see: Franco Bechis, “Gran pasticcio nel rapporto sui decessi. Per l’Iss gran parte dei morti non li ha causati il Covid,” Il Tempo, October 21, 2021.
One exceptionally detailed empirical analysis of public health pronouncements and media reports in Canada found a consistent pattern of misdirection. The pattern was one that generalized from the situation of the deaths of very elderly persons with comorbidities (whose average age exceeded the national average for life expectancy), and who were primarily confined to long-term care homes, to the rest of the population. As of April, 2021, nearly 91% of all Covid deaths recorded in Canada occurred in long-term care homes for the elderly. By imposing a “one size fits all” approach, Canadians were thus increasingly taught to fear for the safety of their children. Canada had only one seriously deadly wave, and that was the first wave in March-May of 2020—the majority of those deaths took place inside of tightly controlled institutional settings which in many cases were publicly-administered. Long-term care and retirement homes, added to hospitals, and prisons, together accounted for 98.6% of all Covid deaths; thus if 13,611 Covid deaths occurred inside such tightly-controlled institutional settings, only 178 deaths occurred in the wider community. Yet what was an institutional crisis was then inflated into a population-wide health crisis. There was a massive failure that occurred on governments’ side of the institutional barrier, with attention subsequently and deliberately redirected to the rest of the population—healthy people had to be locked in their homes presumably to save the lives of those in nursing homes. For this, and much more, see: Julius Ruechel, “The Lies Exposed by the Numbers: Fear, Misdirection, & Institutional Deaths (An Investigative Report),” May 28, 2021.
Another study found that there was “no extraordinary surge in yearly or seasonal mortality in Canada, which can be ascribed to a Covid-19 pandemic” and that “several prominent features” in all-cause mortality per week during the Covid-19 period, “exhibit anomalous province-to-province heterogeneity,” one that is “irreconcilable with the known behaviour of epidemics of viral respiratory diseases”. The authors of the study stated: “We conclude that a pandemic did not occur”. See: Denis G. Rancourt, Marine Baudin, Jérémie Mercier, “Analysis of all-cause mortality by week in Canada 2010-2021, by province, age and sex: There was no COVID-19 pandemic, and there is strong evidence of response-caused deaths in the most elderly and in young males,” August 6, 2021.
In Quebec, the public is familiar with how during the “first wave” a massive number of deaths occurred in long-term care and retirement homes: 73% of all deaths occurred in such institutions (CHSLDs). About 92% of people who died between February 25 and July 11, 2020, were 70 and older, according to the Institut national de santé publique du Québec (INSPQ). This was the high point of claimed Covid deaths; there has been no repetition of the mortality level we saw in that period. However, even here there is reason to doubt official numbers. Given the conditions in the homes, as reported by nurses, physicians, and by the Canadian military, an unspecified number of residents died due to starvation, dehydration, neglect, and even the deliberate administration of morphine to accelerate death—while all of these deaths were tallied as “Covid deaths”. In the UK there were similar reports of the administration of Midazolam which has been “been associated with respiratory depression and respiratory arrest, especially when used for sedation” according to published warnings. For more on these reports, see: Levon Sevunts, “Military report on conditions in Quebec nursing homes details several flaws,” Radio Canada International, May 27, 2020; Brig-Gen. F.G. Carpentier, “Observations sur les Centres D’hébergement de Soins Longues Durées de Montréal,” 2nd Canadian Division and Joint Task Force (East), May 18, 2020; The Canadian Press, “‘Systemic ageism’ to blame for CHSLD deaths during pandemic’s first wave, says expert,” CTV News, November 1, 2021; The Canadian Press, “Officials blamed COVID-19 for Herron deaths, when some were due to hunger, thirst: witness,” CTV News, September 14, 2021; The Canadian Press, “Health officials, Herron staff clashed as situation got worse, Quebec coroner hears,” CTV News, September 16, 2021; The Canadian Press, “Doctors concerned about rise in dangerous medications in long-term care homes during pandemic,” CTV News, December 3, 2020; Tu Thanh Ha, “Quebec nursing home often gave morphine rather than treat COVID-19 patients, inquest told,” The Globe and Mail, June 16, 2021; Emily Mangiaracina, “‘I had never seen deaths happen so quickly’: Quebec nursing home gave COVID patients morphine instead of virus treatments,” LifeSite News, July 22, 2021; and, despite the deceptive headline which adopts the perspective of an official responsible for instituting the use of morphine in Quebec nursing homes, see The Canadian Press, “No ‘euthanasia’ in Quebec care homes during COVID-19, expert tells coroner’s inquest,” CTV News, November 2, 2021.
Similar reports of inappropriate or questionable administration of sedatives such as Midazolam, that accelerated death among nursing and retirement home residents, were also registered internationally—see for example: Stephen Adams & Holly Bancroft, “Did care homes use powerful sedatives to speed Covid deaths? Number of prescriptions for the drug midazolam doubled during height of the pandemic,” The Mail on Sunday, July 11, 2020.
4 The Canadian Joint Operations Command used the WHO-declared “pandemic” as an opportunity to test new propaganda techniques on unsuspecting Canadians, using techniques similar to those used for counterinsurgency in Afghanistan; the Canadian Forces also invested in training public affairs officers on “behaviour modification” techniques: David Pugliese, “Military leaders saw pandemic as unique opportunity to test propaganda on Canadians: report,” National Post, September 27, 2021. Also see: Susan Delacourt, “‘The nudge unit’: Ottawa’s behavioural-science team investigates how Canadians feel about vaccines, public health and who to trust,” Toronto Star, February 21, 2021. The behavioural science sub-group (SPI-B) of the UK government’s Scientific Advisory Group for Emergencies (SAGE) prepared a document in May of 2020 advising on measures to be taken to increase public adherence to social distancing measures. The promotion of fear was explicitly advocated: “The perceived level of personal threat needs to be increased among those who are complacent, using hard-hitting emotional messaging. To be effective this must also empower people by making clear the actions they can take to reduce the threat” (emphasis in the original)—see: SPI-B, “Options for increasing adherence to social distancing measures,” SAGE, March 22, 2020; also see, “How SAGE and the UK media created fear in the British public,” Evidence Not Fear, June 27, 2020. On the “doom loop” created by the UK government’s behaviour modification techniques—which dangerously spread fear when it is known to weaken immune systems—and which used the UK public for psychological experimentation, see Gordon Rayner, “State of fear: how ministers ‘used covert tactics’ to keep scared public at home,” The Telegraph, April 2, 2021, and Gary Sidley, “A year of fear,” The Critic, March 23, 2021. Sidely describes how the UK Government’s Behavioural Insights Team (BIT) developed strategies that would create “‘low cost, low pain ways of ‘nudging’ citizens…into new ways of acting by going with the grain of how we think and act’. Several interventions of this type have been woven into the Covid-19 messaging campaign, including fear (inflating perceived threat levels), shame (conflating compliance with virtue) and peer pressure (portraying non-compliers as a deviant minority)”. See also Laura Dodsworth, “Winter is coming, and so are the nudges,” October 4, 2021.
5 Knowing that “a frightened population is a compliant one” (Sidley, fn. 4), state officials and the media promote fear, and thus justify ever accumulating and restrictions on civil liberties and negation of key human rights. The demonstrable result of the prolonged and coordinated promotion of fear is an emergent mass psychosis, one that inoculates those suffering from psychosis from rational questioning and normal scepticism. For some psychiatrists, the real public health crisis of this period has been the wide extent of mass delusional psychosis, an indicator of the harm done to mental health in the name of “controlling Covid”. What a psychosis fueled by a sustained sense of everpresent danger has spawned, is a culture of control, or authoritarian risk management that redirects blame away from the virus (and the fact that the state cannot control its spread) and directes blame toward the behaviour of “unruly” others, thus also fomenting divisions and inter-personal and inter-group hostility. In the US, such divisions have been enlisted in the service of heightened partisanship. In such a context, truth has been replaced by authority: people looking up to the authorities for guidance, rather than seeking out knowledge individually, independently, and critically. While stressing “scientific evidence,” the tendency in this culture of mass control is to steer away actual evidence, with fear-driven mandates persisting. For more on these points, see: Philipp Bagus, José Antonio Peña-Ramos, & Antonio Sánchez-Bayón, “COVID-19 and the Political Economy of Mass Hysteria,” International Journal of Environmental Research and Public Health, 18(1376), 2021; S.G. Cheah, “Psychiatrist: Americans Are Suffering From ‘Mass Delusional Psychosis’ because of Covid-19,” Evie, December 22, 2020; “Are We Experiencing a Mass Psychosis?” The Pulse, August 17, 2021; and, Emma Green, “The Liberals Who Can’t Quit Lockdown,” The Atlantic, May 4, 2021.
Fear appeals have also been very effective in North America and Europe in promoting “vaccine” uptake (even if fear can also undermine the effectiveness of injected treatments). Psychologists have found that, “Moderation analyses based on prominent fear appeal theories showed that the effectiveness of fear appeals increased when the message included efficacy statements, depicted high susceptibility and severity, recommended one-time only (vs. repeated) behaviors, and targeted audiences that included a larger percentage of female message recipients. Overall, we conclude that (a) fear appeals are effective at positively influencing attitude, intentions, and behaviors, (b) there are very few circumstances under which they are not effective, and (c) there are no identified circumstances under which they backfire and lead to undesirable outcomes”: Melanie B. Tannenbaum, Justin Hepler, & Rick S. Zimmerman, et al., “Appealing to fear: A Meta-Analysis of Fear Appeal Effectiveness and Theories,” Psychological Bulletin, 141(6), 2015, pp. 1178–1204. Scientists writing in the bulletin of the WHO warned in 2011 about the creation of “pandemics of fear” and a “culture of fear” caused by health-scares about viruses, leading to worst-case thinking and disproportionate responses that cause harm. Looking at prior “pandemics of fear,” they noted: “the exaggerated claims of a severe public health threat stemmed primarily from disease advocacy by influenza experts. In the highly competitive market of health governance, the struggle for attention, budgets and grants is fierce. The pharmaceutical industry and the media only reacted to this welcome boon. We therefore need fewer, not more ‘pandemic preparedness’ plans or definitions. Vertical influenza planning in the face of speculative catastrophes is a recipe for repeated waste of resources and health scares, induced by influenza experts with vested interests in exaggeration. There is no reason for expecting any upcoming pandemic to be worse than the mild ones of 1957 or 1968, no reason for striking pre-emptively, no reason for believing that a proportional and balanced response would risk lives”—see: Luc Bonneux & Wim Van Damme, “Health is more than influenza,” Bulletin of the World Health Organization, 89, 2011, pp.539–540.
Furthermore, fear can also produce negative immunological effects. Excessive and prolonged fear, suffered by large parts of the population during the past 19 months, can do both serious damage to persons’ physical health, and it can damage their brains—see: Baycrest Centre for Geriatric Care, “Chronic Stress, Anxiety can Damage the Brain, Increase Risk of Major Psychiatric Disorders,” ScienceDaily, January 21, 2016, and Debra Fulghum Bruce, “How Worrying Affects the Body,” WebMD, September, 2020. A published study from a team of researchers at the University of Nottingham stated: “It is well known that when negative mood states persist over time they result in the dysregulation of physiological systems involved in the regulation of the immune system. Thus, there exists significant potential for the psychological harm inflicted by the pandemic to translate into physical harm. This could include an increased susceptibility to the virus, worse outcomes if infected, or indeed poorer responses to vaccinations in the future”—see: Ru Jia, Kieran Ayling, & Trudie Chalder, et al., “Mental health in the UK during the COVID-19 pandemic: cross-sectional analyses from a community cohort study,” BMJ Open, 10(9); Rosa Silverman, “What a year of lockdown has done to our immunity – and how to strengthen it,” The Telegraph, February 24, 2021; Shaoni Bhattacharya, “Brain study links negative emotions and lowered immunity,” New Scientist, September 2, 2003; APA, “Stress Weakens the Immune System,” American Pyschological Association, February 23, 2006; and, Suzanne C. Segerstrom & Gregory E. Miller, “Psychological Stress and the Human Immune System: A Meta-Analytic Study of 30 Years of Inquiry,” Psychological Bulletin, 130(4), 2004, pp. 601–630.
For more conceptual and philosophical understandings of fear in the contemporary context, the following is recommended: Giorgio Agamben, “What is Fear?” Old News, October 26, 2020, and Gustavo Esteva, “Uses of Fear,” D. Alan Dean, March 28, 2020.
6 ON LOCKDOWNS:
Published scientific research has found little if any evidence to support the notion that lockdowns reduced mortality. Instead, deaths rates tended to be determined more by the greater proportion of elderly citizens, the environment, and the prevalence of metabolic diseases—see: Quentin De Larochelambert & Andy Marc, et al., “Covid-19 Mortality: A Matter of Vulnerability Among Nations Facing Limited Margins of Adaptation,” Frontiers in Public Health, 8, 2020. Another study concluded, “it has become clear that a hard lockdown does not protect old and frail people living in care homes—a population the lockdown was designed to protect. Neither does it decrease mortality from COVID-19, which is evident when comparing the UK’s experience with that of other European countries”—see: Johan Giesecke, “The Invisible Pandemic,” The Lancet, 395(10238), 2020. One cross-national study reported that an “examination of lockdown intensity and the number of cumulative deaths attributed to Covid-19 across jurisdictions shows no obvious relationship,” adding that, “an examination of over 100 Covid-19 studies reveals that many relied on false assumptions that over-estimated the benefits and under-estimated the costs of lockdown,” and it reaffirmed that, “the unconditional cumulative Covid-19 deaths per million is not negatively correlated with the stringency of lockdown across countries”—see: Douglas W. Allen, “Covid-19 Lockdown Cost/Benefits: A Critical Assessment of the Literature,” International Journal of the Economics of Business, 2021. Another study that measured and compared weekly mortality rates from 24 European countries, found no clear association between lockdown policies and mortality rates: Christian Bjørnskov, “Did Lockdown Work? An Economist’s Cross-Country Comparison,” Social Science Research Network (SSRN), August 2, 2020. A medical study concluded that, “rapid border closures, full lockdowns, and wide-spread testing were not associated with COVID-19 mortality per million people,” and that “obesity, advanced age and higher per capita GDP are associated with increased national case load and mortality”—see: Rabail Chaudhry & George Dranitsaris, et al., “A country level analysis measuring the impact of government actions, country preparedness and socioeconomic factors on COVID-19 mortality and related health outcomes,” EclinicialMedicine, 25(100464), 2020. In the critical case of Italy, published research found that tiered restrictions not only failed to reduce the spread of infection, such measures might have even been counterproductive for limiting the reproduction of the virus: Maurizio Rainisio, “The tiered restrictions enforced in November 2020 did not impact the epidemiology of the second wave of COVID-19 in Italy,” medRxiv, September 13, 2021.
ON MASKS:
Masking and mandates governing mask-wearing are likely among the very last to go. Yet, from the outset, there was no conclusive scientific evidence to support the notion that masks could ever reduce transmission or infection by any significant measure, and public health officials who supported masking had in previous weeks denied their utility. States have taken the reversal and turned it into decrees, with fines imposed for not wearing a mask; in some countries, arrest is possible. Masking also publicly spreads fear of infection and intensifies calls for increased risk management. There is also some scientific evidence that shows the different harms caused by prolonged masking. In Quebec, millions of masks had to be recalled due to their incorporation of known carcinogens and other toxic substances. See: Kai Kisielinski, Paul Giboni, &Andreas Prescher, et al., “Is a Mask That Covers the Mouth and Nose Free from Undesirable Side Effects in Everyday Use and Free of Potential Hazards?” International Journal of Environmental Research and Public Health, 18(8), 4344, 2021; LifeSiteNews Staff, “47 studies confirm ineffectiveness of masks for COVID and 32 more confirm their negative health effects,” LifeSite News, July 23, 2021; Shane Neilson, “The Surgical Mask is a Bad Fit for Risk Reduction,” Canadian Medical Association Journal (CMAJ), 188(8), 2016, pp. 606–607; Antonio I. Lazzarino, et al., “Face masks for the public during the covid-19 crisis,” BMJ, 369(1435), 2020; Jingyi Xiao, Eunice Y. C. Shiu, & Huizhi Gao, et al., “Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings—Personal Protective and Environmental Measures,” Emerging Infectious Diseases, 26(5), 2020; Michael Klompas, Charles A. Morris, & Julia Sinclair, et al., “Universal Masking in Hospitals in the Covid-19 Era,” New England Journal of Medicine, 382, 2020; Anna Balazy, Mika Toivola, & Atin Adhikari, et al., “Do N95 respirators provide 95% protection level against airborne viruses, and how adequate are surgical masks?” American Journal of Infection Control (AJIC), 34(2), 2006, pp. 51–57; Youlin Long, Tengyue Hu, & Liqin Liu, et al., “Effectiveness of N95 respirators versus surgical masks against influenza: A systematic review and meta-analysis,” Journal of Evidence-Based Medicine, 13(2), 2020, pp. 93–101; Angel N. Desai & Preeti Mehrotra, “Medical Masks,” Journal of the American Medical Association (JAMA), 323(15), 2020, pp. 1517–1518; ECDC, “Using face masks in the community: Effectiveness in reducing transmission of COVID-19,” European Centre for Disease Prevention and Control, February 15, 2021; Heow Pueh Lee & De Yun Wang, “Objective Assessment of Increase in Breathing Resistance of N95 Respirators on Human Subjects,” The Annals of Occupational Hygiene, 55(8), 2011, pp. 917–921; Cong Liu, Guojian Li, & Yuhang He, et al., “Effects of wearing masks on human health and comfort during the COVID-19 pandemic,” Earth and Environmental Science, 531, 2020; Richard Besser & Baruch Fischhoff, “Rapid Expert Consultation on the Effectiveness of Fabric Masks for the COVID-19 Pandemic,” The National Academies of Science, Engineering, Medicine, April 8, 2020; Robert C.Hughes, Sunil S.Bhopal, & MarkTomlinson, “Making pre-school children wear masks is bad public health,” Public Health in Practice, 2, 2021; Tom Jefferson, Chris B Del Mar, & Liz Dooley, et al., “Physical interventions to interrupt or reduce the spread of respiratory viruses,” Cochrane Library, November 20, 2020; WCH, “Face masks – the risks vs benefits for children,” World Council for Health, October 2, 2021; Damian D. Guerra & Daniel J. Guerra, “Mask mandate and use efficacy in state-level COVID-19 containment,” International Research Journal of Public Health, 5, 2021; Arjun Walia, “Masks Do ‘More Damage to the Children’ than COVID: Belgian Academy For Medicine,” The Pulse, October 11, 2021; Tom Jefferson & Carl Heneghan, “Masking lack of evidence with politics,” The Centre for Evidence-Based Medicine, July 23, 2020; SPR, “Are Face Masks Effective? The Evidence,” Swiss Policy Research, October 2021; Henning Bundgaard & Johan Skov Bundgaard, et al., “Effectiveness of Adding a Mask Recommendation to Other Public Health Measures to Prevent SARS-CoV-2 Infection in Danish Mask Wearers,” Annals of Internal Medicine, 174(3), 2021, pp. 335–343; Kiva A. Fisher, Mark W. Tenforde, & Leora R. Feldstein, et al. “Community and Close Contact Exposures Associated with COVID-19 Among Symptomatic Adults ≥18 Years in 11 Outpatient Health Care Facilities — United States, July 2020,” Morbidity and Mortality Weekly Report, 69(36), 2020, pp. 1258–1264; Lillian Roy, “After recalling graphene-coated masks out of safety concerns, Health Canada says some models can come back on the market,” CTV News, July 14, 2021; Gabrielle Fahmy & Selena Ross, “Montreal transit workers the latest to learn they’ve been wearing potentially toxic masks,” CTV News, March 29, 2021; The Canadian Press, “Quebec’s education union wants to close down establishments where recalled masks were distributed,” CTV News, March 28, 2021; Selena Ross, “‘I just now feel a bit betrayed’: Quebec teachers and parents respond after potentially toxic masks pulled,” CTV News, March 26, 2021. For a philosopher’s understanding of masking, see Giorgio Agamben, “The Face and the Mask,” Old News, October 11, 2020.
7 David Cayley, “The Case against Vaccine Passports,” First Things, September 16, 2021; Giorgio Agamben, “Bare Life and the Vaccine,” D. Alan Dean, April 16, 2020; Lisa Bildy, “Trudeau’s vaccine passports are an affront to liberty,” Justice Centre for Constitutional Freedoms, August 15, 2021; Douglas Farrow, “An Open Letter on Coercive Mandates and Vaccine Passports,” Crisis Magazine, August 30, 2021; Claus Rinner, Laurent Leduc, & Jan Vrbik, et al., “No, COVID-19 vaccine passports and mandatory vaccination do not ‘protect the health and safety of Canadians’,” Toronto Sun, August 24, 2021; Aaron Rock, “25 reasons to ban vaccine passports,” LifeSite News, August 31, 2021; Anthony Furey, “Why vaccine passports make things worse,” National Post, September 7, 2021; Jon Miltimore, “Harvard Epidemiologist Says the Case for COVID Vaccine Passports Was Just Demolished,” FEE Stories, August 30, 2021; Ann Cavoukian, “Vaccine passports to create ‘appalling’ level of surveillance tracking: Former Ontario privacy watchdog,” BNN Bloomberg; Isaac Teo, “Vaccine Passports Will Create a ‘Global Digital Infrastructure of Surveillance’: Former Ontario Privacy Commissioner,” The Epoch Times, October 20, 2021; OPCC, “Privacy and COVID-19 Vaccine Passports: Joint Statement by Federal, Provincial and Territorial Privacy Commissioners,” Office of the Privacy Commissioner of Canada, May 19, 2021; Jeremy Loffredo & Max Blumenthal, “Public health or private wealth? How digital vaccine passports pave way for unprecedented surveillance capitalism,” The GrayZone, October 19, 2021; The Canadian Press, “Debate on vaccine passports would expose Quebecers to conspiracy theories: Legault,” CTV News, August 12, 2021; Daniel J. Rowe, “‘We have to confront our clients’: Quebec bars and restaurants struggling with COVID-19 vaccine passport rollout,” CTV News, September 24, 2021.
8 In almost all provinces of Canada, tenured and tenure-track plus part-time faculty, students, and staff, face expulsion and loss of employment for refusal to comply with the demand that they disclose their private and personal medical status; others have explicitly refused mandatory vaccination, while others still have rejected discriminatory testing in order to keep their jobs. See: Dr. Byram Bridle, “An Open Letter to the President of the University of Guelph,” September 17, 2021; Dr. Michael Palmer, et al., “Open letter to UW officials: Repeal the COVID vaccination and testing mandates,” August 26, 2021, see also “Requests to Repeal UW’s Mandatory Vaccination and Testing Policy”; CCCA, “Ethics professor threatened with dismissal for refusing vaccine,” Canadian Covid Care Alliance, also Arjun Walia, “Canadian Ethics Professor Dismissed For Refusing COVID Vaccine: A Powerful Message,” The Pulse, September 8, 2021; Justice Centre for Constitutional Freedoms, “University Fires Surgeon Who Voiced Safety Concerns About COVID Vaccines for Kids,” The Defender, June 23, 2021. Many faculty unions have not only failed to stand by colleagues who faced termination over an abrupt change in the terms and conditions of their employment, the unions themselves have pushed for mandates. On the domestic travel ban that blocks non-vaccinated Canadians from accessing means of travel within the country, and that blocks them from leaving the country by normal means, see: Justin Trudeau, “Prime Minister announces mandatory vaccination for the federal workforce and federally regulated transportation sectors,” Prime Minister of Canada, October 6, 2021.
9 See in particular, “Division III: Public Health Emergency” (articles 118–130) of the Public Health Act (Bill 36, 2001, chapter 60), Second Session of the 36th Legislature, National Assembly of Quebec, 2001.
10 For the complete list of Quebec’s emergency measures, see: Measures adopted by Orders in Council and Ministerial Orders in the context of the COVID-19 pandemic (Orders in Council and Ministerial Orders related to COVID-19), Gouvernement du Québec,
11 Indeed, the Government of Quebec has gone as far as to admit publicly that the state of emergency is not being used because of a “public health emergency,” but as a political tool that permits interference in collective bargaining. Quebec Premier François Legault said on Thursday, November 18: “Right now we’re paying an additional $4 an hour (for staff) because there’s a shortage of people working in health establishments. To do that, which is something not included in the collective agreement, we’re obliged to use the state of emergency. We need the state of emergency to pay bonuses and we still need those bonuses to get more people working in health establishments” (emphases added). Reporters also noted that, “Legault made no reference to the province’s opposition parties, which have for weeks called for the state of emergency to be lifted in order to debate government decisions in a democratic manner. He was also silent concerning legal and rights experts who are questioning why emergency measures remain in effect”. These observations record the fact that the Quebec government has failed to explain or demonstrate the need for any continued state of emergency—see: The Canadian Press, “Quebec’s state of emergency will remain in effect until start of 2022,” Montreal Gazette, November 19, 2021. On the concept of rule by “state of emergency” (or state of exception), and the consequences of such rule in Canada, see the following: David Cayley, “Pandemic Revelations,” December 4, 2020; “Coronavirus and philosophers: M. Foucault, G. Agamben, S. Benvenuto,” European Journal of Psychoanalysis; Giorgio Agamben, “The State of Exception Provoked by an Unmotivated Emergency,” Praxis, February 26, 2020; Giorgio Agamben, “The Coronavirus and the State of Exception,” Autonomies, March 3, 2020; Giorgio Agamben, “Contagion,” Write.as, March 11, 2020; Giorgio Agamben, “Reflections on the Plague,” Enough 14, April 7, 2020; Giorgio Agamben, “Social Distancing,” Ill Will, April 9, 2020; Giorgio Agamben, “A Question,” An und für sich, April 15, 2020; Giorgio Agamben, “New Reflections,” D. Alan Dean, April 22, 2020; Giorgio Agamben, “Medicine as Religion,” An und für sich, May 2, 2020; Giorgio Agamben, “Biosecurity and Politics,” D. Alan Dean, May 11, 2020; Giorgio Agamben, “State of Exception and State of Emergency,” Old News, July 30, 2020; Giorgio Agamben, “When the House Burns,” Architects for Social Housing, October 15, 2020; Giorgio Agamben, “Some Data,” Old News, November 2, 2020; Giorgio Agamben, “War and Peace,” Ill Will, February 24, 2021.
12 Virat Agrawal, Jonathan H. Cantor, Neeraj Sood, & Christopher M. Whaley, “The Impact of the Covid-19 Pandemic and Policy Responses on Excess Mortality,” National Bureau of Economic Research, Working Paper 28930, June, 2021; AIER Staff, “Lockdowns Do Not Control the Coronavirus: The Evidence,” American Institute for Economic Research, December 19, 2020; Greg Ip, “New Thinking on Covid Lockdowns: They’re Overly Blunt and Costly,” Wall Street Journal, August 24, 2020.
13 The Canadian Press, “‘We’ll be living with overflow for a few months,’ says minister Dube regarding Quebec emergency rooms,” CTV News, July 5, 2021; Adam Kovac, “Many Quebec ERs stretched to capacity even as COVID numbers shrink,” CTV News, June 16, 2021. The explosive growth in ER visits for non-Covid sickness, as a result of delayed treatments, is also occurring in the US: “Except for initial hot spots like New York City, many ERs across the U.S. were often eerily empty in the spring of 2020. Terrified of contracting COVID-19, people who were sick with other things did their best to stay away from hospitals. Visits to emergency departments dropped to half their normal levels, according to the Epic Health Research Network, and didn’t fully rebound until the summer of 2021. But now, they’re too full. Even in parts of the country where COVID-19 isn’t overwhelming the health system, patients are showing up to the ER sicker than they were before the pandemic, their diseases more advanced and in need of more complicated care”—see: Kate Wells, “ERs are now swamped with seriously ill patients — but many don’t even have COVID,” NPR, October 26, 2021.
14 The Executive Director of the Quebec Cancer Coalition was reported as saying, “Where this gets us is another pandemic”; Dr. Neil Fleshner, Chair of Urology at the University of Toronto: “I do believe that patients with cancer in Canada…are being rendered fatal, terminal or incurable, as a result of what’s happened”—see: Tom Blackwell, “Pandemic-related cuts in cancer screening, surgery have doctors worried more people will die,” National Post, April 13, 2021.
15 StatCan, “Disruptions to cancer screening may lead to increases in cancer rates and deaths,” Statistics Canada, March 11, 2021.
16 Stephane Giroux & Luca Caruso-Moro, “Montreal records increase in opioid deaths in pandemic year as national fatalities skyrocket,” CTV News, June 25, 2021; Health Canada, “Opioid- and Stimulant-related Harms in Canada,” Government of Canada, September, 2021.
17 Becky Robertson, “Way more young people in Ontario died from effects of lockdown than of Covid itself,” BlogTO, July, 2021; Nadine Yousif, “‘Very, very concerning’: Pandemic taking heavy toll on children’s mental health, Sick Kids study shows,” Toronto Star, July 8, 2021; and, Denette Wilford, “More young Canadians died from ‘unintentional side effects’ of the pandemic, not COVID,” Toronto Sun, July 13, 2021.
18 “Provisional death counts and excess mortality, January 2020 to April 2021,” Statistics Canada, July 12, 2021.
19 Simran Kalkat, Julie Yixia Cai, & Shawn Fremstad, “Over 3.8 Million Young Adults Found Not Working or in School in Early 2021,” Center for Economic and Policy Research (CEPR), June 23, 2021.
20 Anne C. Gadermann, Kimberly C. Thomson, Chris G. Richardson, et al., “Examining the Impacts of the COVID-19 Pandemic on Family Mental Health in Canada: Findings from a National Cross-Sectional Study,” BMJ Open, 2021.
21 Professor Douglas Allen, economist at Simon Fraser University, concluded that the lockdowns were possibly Canada’s greatest peacetime policy failure, one that also increased excess deaths—see: Douglas W. Allen, “Covid Lockdown Cost/Benefits: A Critical Assessment of the Literature”; HillNotes, “Impacts of COVID-19 on Employment in Canada by Sector,” Library of Parliament, June 25, 2020.
22 Matt Gilmour, “Number of homeless Montrealers doubled in pandemic; Plante floats new approach on campaign trail,” CTV News, October 11, 2021.
23 Tristin Hopper, “What 16 months of COVID lockdowns have cost us,” National Post, July 28, 2021; Nicole Gibillini, “Up to 225,000 Canadian firms could close because of COVID: CFIB CEO,” BNN Bloomberg, November 11, 2020; The Canadian Press, “Canada has slipped into recession due to COVID-19, C.D. Howe council says,” Global News, May 1, 2020.
24 Zara Liaqat, “Why COVID-19 is an inequality virus,” Policy Options Politiques, April 30, 2021. We note that “the virus” has no power to breed inequalities; this crisis bears only the imprints of the heavy hands of the state and large transnational corporations.
25 Government of Canada: Covid-19 daily epidemiology update.
26 Cathrine Axfors & John P.A. Ioannidis, “Infection fatality rate of COVID-19 in community-dwelling populations with emphasis on the elderly: An overview,” medRxiv, July 13, 2021; John P.A. Ioannidis, “Infection fatality rate of COVID-19 inferred from seroprevalence data,” Bulletin of the World Health Organization, October 14, 2020; Andrew T. Levin, William P. Hanage, & Nana Owusu-Boaitey, et al., “Assessing the Age Specificity of Infection Fatality Rates for COVID-19: Systematic Review, Meta-Analysis, and Public Policy Implications,” European Journal of Epidemiology, 35, 2020, pp. 1123–1138; Dr. Jay Bhattacharya, MD, PhD, from the Stanford University School of Medicine, appearing on a JAMA (The Journal of the American Medical Association) Network conversation alongside Mark Lipsitch, DPhil and Dr. Howard Bauchner; Dominick Mastrangelo, “Stanford doctor: Coronavirus fatality rate for people under 45 ‘almost 0%’,” Washington Examiner, July 2, 2020.
27 UCL, “Symptoms of Covid-19 are a poor marker of infection,” UCL News, October 8, 2020, and Irene Petersen & Andrew Phillips, “Three Quarters of People with SARS-CoV-2 Infection are Asymptomatic: Analysis of English Household Survey Data,” Clinical Epidemiology, 12, 2020, pp. 1039‒1043.
28 The Norwegian Directorate of Health and the National Institute of Public Health (NIPH) via: Office of the Prime Minister, “Norge går over til en normal hverdag med økt beredskap,” Regjeringen, September 24, 2021; in the UK, Jo Churchill, then Parliamentary Under Secretary of State at the Department of Health and Social Care, stated that, “as of 15 July [2021], Public Health England’s modelling group, with the MRC Biostats Unit, estimated that overall infection mortality rate is approximately 0.096%”: “Coronavirus: Death—Question for Department of Health and Social Care,” UK Parliament, July 12, 2021; the last point is relevant to the fact that, by some estimates, Covid is less fatal than the annual flu—see Simon Thornley, “The covid-19 elimination debate needs correct data,” BMJ, 371(3883), November 8, 2020.
29 Responding to news that a woman died from blood clotting caused by the AstraZeneca injectable (AstraZeneca has since been pulled from the market in Canada), Quebec Premier François Legault stated the following: “I’m very sad to know that a 54-year-old woman in good shape….died because she was vaccinated. Unfortunately these cases happen….I think people will still continue getting vaccinated. It’s very unfortunate and we’re sad about it, but unfortunately, that’s the price of vaccination” (emphases added): Amy Lift & Luca Caruso-Moro, “Experts worry AstraZeneca death will deter others from getting vaccinated,” CTV News, April 27, 2021. Death by “vaccination” was accepted as “the price to pay,” while even one death from the virus was condemned as “one death too many”—see: Franca Mignacca, “Quebec children can enjoy Halloween this year — but with some conditions,” CBC News, October 15, 2020, Kalina Laframboise, “Quebec mulls stricter COVID-19 measures but decision will be made next week, Legault says,” CTV News, December 11, 2020.
30 See this study which, “demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity”: Sivan Gazit, Roei Shlezinger, & Galit Perez, et al., “Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections,” medRxiv, August 25, 2021; plus, Jennifer Block, “Vaccinating people who have had covid-19: why doesn’t natural immunity count in the US?” BMJ, 374(2101), 2021. For a study conducted in Vancouver, that showed that, “more than 90% of uninfected adults showed antibody reactivity against the spike protein, receptor-binding domain (RBD), N-terminal domain (NTD), or the nucleocapsid (N) protein from SARS-CoV-2”: Abdelilah Majdoubi, Christina Michalski, & Sarah E. O’Connell, et al., “A majority of uninfected adults show preexisting antibody reactivity against SARS-CoV-2,” JCI Insight, 6(8), 2021. This research echoes what was published in the summer of 2020 by Sweden’s prestigious Karolinska Institute which showed that, “many people with mild or asymptomatic COVID-19 demonstrate so-called T-cell-mediated immunity to the new coronavirus, even if they have not tested positively for antibodies….this means that public immunity is probably higher than antibody tests suggest”: “Immunity to COVID-19 is probably higher than tests have shown,” Karolinska Institutet, August 18, 2020; see also, Takuya Sekine, André Perez-Potti, & Olga Rivera-Ballesteros, et al., “Robust T Cell Immunity in Convalescent Individuals with Asymptomatic or Mild COVID-19,” Cell, 183(1), 2020, pp. 158–168.
31 Jeremy Loffredo, “We’re Not in a ‘Pandemic of the Unvaccinated,’ Peter Doshi Explains During COVID Panel,” The Defender, November 5, 2021. Just as Peter Doshi critiqued the redefinition of the term “vaccine” to include treatments, the descriptive phrase “novel gene therapy,” is one that came from its developers—see: Grant A. Brown, “Can We Really Inject Our Way Out of This Pandemic? Part Two of a Special Series,” C2C Journal, September 22, 2021. This point was reinforced by Stefan Oelrich, president of Bayer’s Pharmaceuticals Division, who explained that cell and gene therapies have been marketed as “vaccines” to the public, to make them more palatable: Jack Bingham, “Bayer executive: mRNA shots are ‘gene therapy’ marketed as ‘vaccines’ to gain public trust,” LifeSite News, November 10, 2021.
32 On the advertised safety of the Pfizer product, see the whistle blower’s damning account of the nature of the actual safety trials: Paul D. Thacker, “Covid-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial,” BMJ, 375(2635), November 2, 2021. See also, Peter Doshi, “Does the FDA think these data justify the first full approval of a covid-19 vaccine?” BMJ, August 23, 2021, and, Alex Berenson, “More people died in the key clinical trial for Pfizer’s Covid vaccine than the company publicly reported,” Unreported Truths, November 16, 2021.
33 Aaron Siri, “FDA Asks Federal Judge to Grant it Until the Year 2076 to Fully Release Pfizer’s COVID-19 Vaccine Data,” Injecting Freedom, November 17, 2021.
34 See the Great Barrington Declaration; Declaration of the International Alliance of Physicians and Medical Scientists; the Canadian Covid Care Alliance COVID-19 Declaration; Canadian Frontline Nurses; World Council for Health; World Doctors’ Alliance; Doctors for Covid Ethics; Children’s Health Defense.
35 Several prominent Canadian scientists, doctors, and academics wrote in an open letter to Ontario Premier Doug Ford regarding recommendations by the Science Advisory Table (SAT). The SAT’s claims were: 1.That COVID-19 vaccines are safe; 2. That COVID-19 vaccines are effective; 3. That general infection prevention and control to reduce the spread of COVID-19 is imperfect whereas vaccines provide safe and effective protection; and, 4. That efforts to counter ‘vaccine hesitancy’ among the most vulnerable, e.g., racialized workers, through ‘education’ and ‘personalized outreach’, will lead to trust building and will avoid losing ‘valuable members of the workforce’”. The authors of the open letter summarized their response as follows (backed by published scientific research): “None of these claims are based on scientific evidence”. See: Claudia Chauffan, Stephen Pelech, & Deanna McLeod, et al., “Response: COVID-19 vaccine mandates for Ontario’s hospital workers,” United Healthcare Workers of Ontario (UHCWO), October 28, 2021. See also, Arjun Walia, “UBC Immunologist Cautions People On COVID Vaccine Safety & Efficacy,” The Pulse, November 16, 2021.
36 For more on each of these points, see the following: Piero Olliaro, Els Torreele, & Michel Vaillant, “COVID-19 vaccine efficacy and effectiveness—the elephant (not) in the room,” The Lancet, 2(7), E279-E280, 2021; Paul Elias Alexander, “22 Studies and Reports that Raise Profound Doubts about Vaccine Efficacy for the General Population,” Brownstone Institute, October 28, 2021; Harald Walach, Rainer J. Klement, & Wouter Aukema, “The Safety of COVID-19 Vaccinations—Should We Rethink the Policy?” Science, Public Health Policy, and the Law, 3, 2021, pp. 87‒99; Barbara A. Cohn, Piera M. Cirillo, & Caitlin C. Murphy, et al., “SARS-CoV-2 vaccine protection and deaths among US veterans during 2021,” Science, November 4, 2021; Berkeley Lovelace Jr., “Israel says Pfizer Covid vaccine is just 39% effective as delta spreads, but still prevents severe illness,” CNBC, July 23, 2021; “UK study finds vaccinated people easily transmit Delta variant in households,” Reuters, October 28, 2021; Michelle Roberts, “Covid: Double vaccinated can still spread virus at home,” BBC News, October 28, 2021; Anika Singanayagam, Seran Hakki, Jake Dunning, “Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: a prospective, longitudinal, cohort study,” The Lancet, October 29, 2021; HART, “Compulsory vaccination for NHS staff back on the agenda?” Health Advisory & Recovery Team, June 3, 2021; Paul Elias Alexander, “96 Research Studies Affirm Naturally Acquired Immunity to Covid-19: Documented, Linked, and Quoted,” Brownstone Institute, October 17, 2021; Carolina Lucas, Chantal B.F. Vogels, & Inci Yildirim, et al. “Impact of circulating SARS-CoV-2 variants on mRNA vaccine-induced immunity,” Nature, October 11, 2021; Gaëlle Breton, Pilar Mendoza, & Thomas Hagglof, et al., “Persistent Cellular Immunity to SARS-CoV-2 Infection,” bioRxiv, December 9, 2020; Jennifer M. Dan, Jose Mateus, & Yu Kato, et al., “Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection,” Science, 371(6529), 2021; Victoria Jane Hall, Sarah Foulkes, & Andre Charlett, “SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: a large, multicentre, prospective cohort study (SIREN),” The Lancet, 397(10283), 2021, pp. 1459–1469; Jackson S. Turner, Wooseob Kim, & Elizaveta Kalaidina, et al., “SARS-CoV-2 infection induces long-lived bone marrow plasma cells in humans,” Nature, 595, 2021, pp. 421–425; Ronald B. Brown, “Outcome Reporting Bias in COVID-19 mRNA Vaccine Clinical Trials,” Medicina, 57(199), 2021; Peter Doshi, “Pfizer and Moderna’s ‘95% effective’ vaccines—let’s be cautious and first see the full data,” BMJ, November 26, 2020; and, note that even when giving full approval to Pfizer, the FDA in a letter to the company listed numerous safety studies yet to be undertaken by Pfizer, and in some cases the completion dates for these studies are in 2025—the list of 13 safety studies to be undertaken begins on page 5.
37 See: VigiAccess, produced by the WHO Collaborating Centre for International Drug Monitoring with the Uppsala Monitoring centre, reported a total of 2,528,564 adverse events reported for Covid-19 vaccines; “From the 11/5/2021 release of VAERS data: Found 18,461 cases where Vaccine is COVID19 and Patient Died,” National Vaccine Information Center; MHRA, “Coronavirus vaccine – weekly summary of Yellow Card reporting,” Medicines & Healthcare products Regulatory Agency; “29,934 Deaths 2,804,900 Injuries Following COVID Shots in European Database of Adverse Reactions,” Vaccine Impact; and, Megan Redshaw, “Reports of Injuries, Deaths After COVID Vaccines Climb Steadily, as FDA, CDC Sign Off on Third Shot for Immunocompromised,” The Defender, August 16, 2021.
38 “Even if vaccination were universal, the coronavirus would probably continue to spread”: Melissa Healy, “CDC shifts pandemic goals away from reaching herd immunity,” Los Angeles Times, November 12, 2021.
39 See: Paul Elias Alexander, “28 Studies on Vaccine Efficacy that Raise Doubts on Vaccine Mandates,” Brownstone Institute, October 28, 2021; Catherine M Brown, Johanna Vostok, & Hillary Johnson, et al., “Outbreak of SARS-CoV-2 Infections, Including COVID-19 Vaccine Breakthrough Infections, Associated with Large Public Gatherings – Barnstable County, Massachusetts, July 2021,” Morbidity and Mortality Weekly Report, 70(31), 2021, pp. 10591062; Laurel Wamsley, “Vaccinated People With Breakthrough Infections Can Spread The Delta Variant, CDC Says,” NPR, July 30, 2021; S.V. Subramanian & Akhil Kumar, et al. “Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States,” European Journal of Epidemiology, September 30, 2021; Günter Kampf, “The epidemiological relevance of the COVID-19-vaccinated population is increasing,” The Lancet Regional Health – Europe, 11, December, 2021; Pnina Shitrit, Neta S Zuckerman, & Orna Mor, et al., “Nosocomial outbreak caused by the SARS-CoV-2 Delta variant in a highly vaccinated population, Israel, July 2021,” Eurosurveillance, 26(39), 2021; Kasen K. Riemersma, Brittany E. Grogan, & Amanda Kita-Yarbro, et al., “Shedding of Infectious SARS-CoV-2 Despite Vaccination,” medRxiv, October 15, 2021; Venice Servellita, Alicia Sotomayor-Gonzalez, & Amelia S. Gliwa, et al., “Predominance of antibody-resistant SARS-CoV-2 variants in vaccine breakthrough cases from the San Francisco Bay Area, California,” medRxiv, October 8, 2021; Charlotte B. Acharya, John Schrom, & Anthea M. Mitchell, et al., “No Significant Difference in Viral Load Between Vaccinated and Unvaccinated, Asymptomatic and Symptomatic Groups When Infected with SARS-CoV-2 Delta Variant,” medRxiv, October 5, 2021; Nguyen Van Vinh Chau & Nghiem My Ngoc, et al., “Transmission of SARS-CoV-2 Delta Variant Among Vaccinated Healthcare Workers, Vietnam,” The Lancet, October 11, 2021; “Pandemic of the Vaccinated – Worldwide data on 188 countries proves the highest Covid-19 case rates are in the most vaccinated countries,” The Exposé, November 2, 2021; and, Will Jones, “Vaccine Passports Make No Sense as the Vaccinated Are More Likely to Be Infected, Scientists Tell MPs,” The Daily Sceptic, November 22, 2021.
40 Elizabeth Redden, “Hundreds of Positive COVID Tests at Mostly Vaccinated Duke,” Inside Higher Ed, August 31, 2021; Kate Murphy, “Duke sets new campus restrictions after rise in COVID cases among vaccinated students,” The News & Observer, August 31, 2021; Joseph Silverstein, “Despite 95% vaccination rate, Cornell today has five times more COVID cases than it did this time last year,” The College Fix, September 4, 2021.
41 Eva Bartlett, “‘It’s absolutely appalling’: Unvaccinated Canadians become social outcasts and the new persecuted minority,” RT, October 21, 2021.
42 Even as the administration proclaimed its support for the vaccine passport system, and adopted it for all “non-essential” campus services (which include eating and fitness), the public relations unit of Concordia University proudly directed attention to new research involving Concordia that confirmed the large presence of “traditionally underrepresented groups” among the “vaccine hesitant”—see: Patrick Lejtenyi, “New data from a Montreal-led global study helps explain vaccination rates and vaccine hesitancy,” Concordia University News, August 31, 2021. See also, Kennedy Hall, “‘Absolutely forbidden’ to give COVID shots to kids, young men and women, Jewish court rules,” LifeSite News, November 2, 2021.
43 Statistics Canada reported that, “Among people designated as a visible minority, 74.8% reported being very or somewhat willing to receive the COVID-19 vaccine. Some differences exist for willingness among particular visible minority groups. Compared to non-visible minorities (77.7%), a much lower proportion of the Black population (56.4%) reported being somewhat or very willing to receive a COVID-19 vaccine….A lower rate of vaccine willingness was also seen among the Latin American population (65.6%)”: StatCan, “COVID-19 vaccine willingness among Canadian population groups,” Statistics Canada, March 26, 2021; see also Cosmin Dzsurdzsa, “Trudeau ignores impact of mandatory vaccines on First Nations, black Canadians,” True North, August 9, 2021; Michèle Newton, “Vaccine hesitancy a problem for us all,” Toronto Star, August 26, 2021; and, Selena Ross, “Vaccine refusal very high in Nunavik for ‘religious’ reasons or fears; cases escalating,” CTV News, November 8, 2021. However, note the dismissive and disbelieving CTV News headline in the latter reference, putting religious reasons inside quotation marks, as if such reasons were false or not worthy of respect—this, while Canadians preach about the dangers of “systemic racism”. Similar impacts on minorities from mandates are felt in the US—see: Joseph Goldstein & Matthew Sedacca, “Why Only 28 Percent of Young Black New Yorkers Are Vaccinated,” The New York Times, August 12, 2021; Kevin Jenkins & Joshua Coleman, “Thanks to Vaccine Mandates, Segregation Is Making a Comeback. Once Again, Black Americans Will Suffer Most,” The Defender, August 13, 2021; “Voter ID is racist but this isn’t? Fury over New York City vaccine pass that ACTUALLY discriminates against black Americans,” RT, August 3, 2021.
44 For studies and reports that paint a more realistic portrait of the “unvaccinated,” see: Bruce Anderson, “Typical ‘vaccine hesitant’ person is a 42-year-old Ontario woman who votes Liberal: Abacus polling,” Maclean’s, August 11, 2021; also, Amy Judd, “Polling the unvaccinated: Why Canadians say they won’t get a COVID vaccine,” Global News, November 3, 2021. On educational levels see UnHerd, “The most vaccine-hesitant group of all? PhDs,” The Post, August 11, 2021 and in particular this survey which found that, “The association between hesitancy and education level followed a U-shaped curve with the lowest hesitancy among those with a master’s degree (RR=0.75 [95% CI 0.72-0.78] and the highest hesitancy among those with a PhD (RR=2.16 [95%CI 2.05-2.28]) or ≤high school education(RR=1.88 [95%CI 1.83-1.93]) versus a bachelor’s degree”: Wendy C. King & Alex Reinhart, et al., “Time trends and factors related to COVID-19 vaccine hesitancy from January-May 2021 among US adults: Findings from a large-scale national survey,” medRxiv, July 23, 2021.
45 Robert G. Evans, “Tough on Crime? Pfizer and the CIHR,” Healthcare Policy, 5(4), 2010, pp. 16–25; DoJ, “Justice Department Announces Largest Health Care Fraud Settlement in Its History,” The United States Department of Justice, September 2, 2009; FBI, “The Case Against Pfizer,” The Federal Bureau of Investigation, September 2, 2009; Drew Griffin & Andy Segal, “Feds found Pfizer too big to nail,” CNN, August 2, 2010; Pratap Chatterjee, “Pfizer Admits Bribery in Eight Countries,” CorpWatch, August 8, 2012; Richard Gale & Gary Null, “Pfizer’s History of Crimes and Misdemeanors,” Progressive Radio Network, March 10, 2021.
46 Gail Davidson, “The Right to Say No to COVID-19 Vaccines: International Human Rights Law Guarantees Rights and Prohibits Unlawful Restrictions,” Canadian Covid Care Alliance (CCCA), October 28, 2021.
47 Michael Kowalik, “Ethics of vaccine refusal,” Journal of Medical Ethics, February 26, 2021.
48 “The specific and significant COVID-19 risk of ADE [antibody-dependent enhancement] should have been and should be prominently and independently disclosed to research subjects currently in vaccine trials, as well as those being recruited for the trials and future patients after vaccine approval, in order to meet the medical ethics standard of patient comprehension for informed consent”: Timothy Cardozo & Ronald Veazey, “Informed consent disclosure to vaccine trial subjects of risk of COVID-19 vaccines worsening clinical disease,” The International Journal of Clinical Practice, 75(3), 2021.
49 See: Title II, Chapter I, Art. 7 of Quebec’s Act Respecting Health Services and Social Services.
50 Arjun Walia, “Rockefeller Foundation Pledges $13.5 Million To Censor Health ‘Misinformation’,” The Pulse, July 19, 2021.
51 Janice Flamengo, “How Covid-19 Killed Academic Tenure,” The Pipeline, October 14, 2021.
52 Janice Flamengo, “The Silence of the Professors,” Truth USA, August 31, 2021.
53 See the Special Issue on Covid Policies and Universities in Canada, published by the Society for Academic Freedom and Scholarship, and edited by Janice Flamengo.
54 Joseph A. Ladapo & Harvey A. Risch, “Are Covid Vaccines Riskier Than Advertised?” Wall Street Journal, June 22, 2021.
55 Michael Kowalik, “Ethics of Vaccine Refusal,” Journal of Medical Ethics, February 26, 2021. See also Lisa Boothe, “Why I’m Not Vaccinated,” Newsweek, November 15, 2021; and, Raelle Kaia, “What’s To Be Done about the Vaccine Hesitant?” November 11, 2021.
56 Ronald N. Kostoff, Daniela Calina, & Darja Kanduc, et al., “Why are we vaccinating children against COVID-19?” Toxicology Reports, 8, 2021, pp. 1665–1684; Heidi Ledford, “Deaths from COVID ‘incredibly rare’ among children,” Nature, 595, July 15, 2021; and, Larry Kwak, Steven T. Rosen, & Idit Shachar, “Applying brakes on ‘Warp Speed’ COVID-19 vaccinations for children: The long-term side effects are unknown,” The Washington Times, October 28, 2021; Elia Abi-Jaoude, Peter Doshi, & Claudina Michal-Teitelbaum, “Covid-19 vaccines for children: hypothetical benefits to adults do not outweigh risks to children,” BMJ, July 13, 2021; Jonas F. Ludvigsson, Lars Engerström, Charlotta Nordenhäll, Emma Larsson, “Open Schools, Covid-19, and Child and Teacher Morbidity in Sweden,” New England Journal of Medicine, 384, 2021, pp. 669‒671.
57 Zachary Stieber, “Researchers Call for Halt on COVID-19 Vaccines for Pregnant Women After Re-analysis of CDC Study,” The Epoch Times, November 2, 2021; Aleisha R. Brock & Simon Thornley, “Spontaneous Abortions and Policies on COVID-19 mRNA Vaccine Use During Pregnancy,” Science, Public Health Policy, and the Law, 4, 2021, pp. 130–143; Colleen Huber, “COVID vaccines may rival or exceed ‘the morning-after pill’ in abortion efficacy,” The Defeat of Covid, August 6, 2021.
Résistance Scolaire – Québec -Academic Resistance (RSQAR) is a collective of Quebec professors and teachers at all levels of the education system who have joined with students and support staff in fighting against the state of emergency and coercive medical practices.
Police question Doctor who wrote letters to MP outlining Covid-19 Vaccine concerns
The Exposé • November 29, 2021
An Australian doctor says that he was questioned by police after sending his local MP emails expressing concerns about the Covid-19 vaccines.
The incident took place at the home of Dr Bruce Paix in Adelaide, South Australia. Although police originally said they had come to his house for a firearms check, an officer who was caught on video later admitted that he was there due to emails that Dr Paix had sent to his local MP, Josh Teague of South Australia.
Dr Paix has 32 years of experience and is a former military physician. He has served as a senior doctor in South Australia’s government system, a rescue doctor and also as an anesthesiologist. During his time as a senior military doctor in the Middle East during the MERS outbreak, he managed many health threats.
After educating himself over a long period of time on coronavirus, he concluded that “nothing about the world’s COVID response template makes sense (including in my own state of South Australia) and indeed is likely harmful.”
Dr Paix is particularly concerned about the way that the mainstream media has been censoring reports of adverse reactions caused by the Covid-19 vaccines. He wrote: “The vaccines, in particular, have numerous valid safety risks, and knowledge of these is being systematically suppressed by governments, professional bodies, and media.”
Additionally, the doctor took issue with the ban on alternative treatments against the virus, such as Ivermectin, which is often denied to patients despite a wealth of evidence showing it can be effective in fighting Covid-19.
“Valuable therapeutic options (Vit D, Ivermectin) are being outlawed in favour of a ‘jab or nothing’ strategy,” he lamented.
Dr Paix said that he contacted the MP’s office multiple times to voice his concerns. However, his requests to meet with Teague were denied, and eventually, he says, the MP’s response was to send the police to threaten him.
The doctor pressed the police officer as to why he was there, pointing out that the firearms check was not random and was instead being done in the context of the letters he had sent his MP. In response, the officer told him that he was not aware that the emails contained any criminal offences and that his aim was just to let the doctor know that the police were aware of the emails.
Dr. Paix is not the only physician who has come under fire in the country because of his opinions on the virus. The clinic of Australian physician Dr. Mark Hobart was raided by health officers just a few days before the incident; they confiscated his appointment book and confidential patient files.
Both of the doctors had been giving patients vaccine and mask exemptions, and Dr. Paix had also been instructing patients on how they can obtain Ivermectin for protection against the virus.
3 bad cat facts
el gato malo – bad cattitude – December 1, 2021
1. it is not nor will it ever be possible to be “fully vaccinated” with these vaccines.

2. almost none of this has ever worked and only serves to drive hysteria.
all we need to do to have our lives and livelihoods back is to stop pretending we ever needed to give them up.

3. continuing to play cards with an opponent who smiles at you while dealing off the bottom of the deck is the literal height of stupidity and has been since i first posted this meme over a year ago…

bonus fact:
you cannot obey your way out of tyranny or an appease an oppressor until they stop.
complying so that it will end simply ensures that it will NEVER end.
going along to get along is the interminable, grinding road to subjugation.
disobey.

Putin Takes 2 Doses in 2 Days, Fumbles the Story, and NOBODY Has Any Questions

By Edward Slavsquat | November 29, 2021
Your humble Moscow correspondent recently reported on Vladimir Putin’s mystifying tale about receiving an intranasal COVID vaccine as part of a clinical trial. As you might recall, Russia’s president claimed he inhaled some kind of virus-murdering powder via a syringe. But the drug he allegedly took is actually a liquid nasal spray. No powder was involved. We thought it was funny that Putin said something so insane and made jokes alluding to illicit drug usage.
It’s still funny; but after thinking more about it, and not just typing cocaine jokes, we came to the conclusion that this is a Real Story and if the lamestream media (including Russia’s completely castrated “opposition” press) weren’t such pathetic vax-peddling Big Pharma boot-lickers, it would probably be frontpage news everywhere. It would probably be called Powdergate and it would probably have its own Wikipedia page.
Please, allow us to explain our thought process. If you think we are overreacting, tell us in the Comments Section.
Hardcore double-dose makes Putin QUADRUPLE-VAXXED!
Putin’s nose-dose was allegedly administered just one day after he was injected with a Sputnik Light booster shot. The Russian prez was already fully vaxxed (he received his second dose in April, although at the time the Kremlin was mum on which vaccine was used), which means Putin has been given four doses of Sputnik in less than a year. FOUR! That’s a lot. Putin is almost as gigavaxxed as Vladimir Zhirinovsky, who claims he injected himself with six COVID serums.
Zhirinovsky is a bumbling lunatic—nobody would care if six COVID shots caused him to grow another arm. But Vladimir Putin is literally the president of the Russian Federation. He’s kind of a big deal! Why are Russian scientists using the most consequential person in Russia as a guinea pig? Even if you firmly believe Sputnik V is “safe and effective,” surely it is unwise to repeatedly inject your president with new doses of an experimental drug? It’s a very weird thing to do. Maybe this is part of Russia’s “hybrid warfare” doctrine?
Please remember, despite RT.com trying to convince you otherwise: there is zero long-term safety data for Sputnik V (unless you count “six months” as long-term?). Expedited Phase III trials for normal, two-dose Sputnik V haven’t even finished yet. Think about what that means.

Putin can’t wait for the science to catch up
But here’s Vladimir Putin, with four doses of Sputnik now running through his veins. Do people understand the issue here?
Isn’t this a bit… irresponsible? There are many incendiary adjectives we could use to describe Putin’s purported vaccination status, actually.
Why would you even need a fourth dose? Does the booster shot suck that bad?
Sputnik Light is the first component of Sputnik V. The nasal spray is the second component. Typically, you’re supposed to wait 21 days (minimum) between reloading on Sputnik V.
Putin went on a serious vax binge, guzzling down two doses in two days! Someone take away his car keys.
Powdergate: revisited
Do people fully appreciate how hilarious Putin’s “powder” story really is? It was so bizarre and nonsensical that RBC—quite a serious, straight-laced Russian news outlet—suggested Putin had not even been given the nasal spray, but rather a VIP mystery powder administered in the “same way” as the liquid drug he was supposed to be testing.
“Putin received the vaccine in the form of a powder… so far this drug is not widely used… The President explained that the preparation in powder form is taken in the same way as a nasal spray,” RBC reported on November 24, after Putin said the drug was a powder, while emphasizing it had not been administered in a liquid form.
A few hours later, RBC reported the clarification from Kremlin spokesman Dmitry Peskov:
“The President meant that we are talking about a liquid. This is a nasal vaccine in which he took part in the trials,” said Peskov.
Can anyone make sense of this madness? How did Putin screw up the basic facts here so badly?
This is a Joe Biden-level brain malfunction. Which brings us to our next point…
Imagine if Joe Biden had been “corrected” after blabbering about magic vax powder
Thought experiment: replace Putin with Biden, Peskov with Psaki. This story would have been everywhere. It would have completely broken Twitter. The hashtags and memes alone would have been history-making.
95% of “indy media” would have basically imploded, shouting about how this was proof of a massive vax hoax. FactCheck.org would be working overtime telling everyone how racist they were for suggesting there was anything fishy about Biden getting a fourth vaccine dose and referring to it as a powder.
Guys, just think about it. Let’s be honest here.
Total impunity for the Kremlin vax clowns?
We’re not claiming anything, by the way! We’re just making observations. The problem is that almost nobody is making observations.
The Kremlin could probably announce Putin undergoes daily Sputnik intravenous therapy (Sputnik IV, get it? ha-ha), and every single media outlet on earth would nod and clap. Only an apostate would dare to question whether it made any sense at all.
The vax is sacred. You do not question the vax or anyone who takes it or promotes it. The vax is life. The vax is love.
Israel Shamir touched on this very weird phenomenon in an article from July:
The Mandatory Vaxx Regime brings new conspirators (like Alexei Navalny, the Russian Guaido presently in jail for swindling) and old school Kremlin propagandists into a rare (and suspicious) agreement. Now they all excrete New York mainstream media.
No one is willing to ask even the most basic questions. It’s a total orgy of non-stop lying in Russia right now (just like it is everywhere else), and not a single media outlet is willing to step up to the plate and say: “just one moment, does any of this make sense?”
We can’t even rely on Russia’s so-called “Kremlin-hating, corruption fighting” western-funded “liberal” press. Meduza published a one-sentence bullet point about Powdergate, while the Moscow Times seemed entirely satisfied with Peskov’s non-explanation explanation. These people are truly pathetic. They are just horrible!

Shame! Shame! Shame!
So what’s the takeaway?
If you hope to survive the next few years—which will feature daily Powdergates, sometimes thousands of Powdergates, back to back, over the course of several hours—you will have to adopt a transcendental Zen-like state, like this monkey who has made peace with the world:
Omicron Variant Sends Pharma Stocks Soaring, as VAERS Data Show 913,000 Reported Adverse Events
By Megan Redshaw | The Defender | November 30, 2021
The Centers for Disease Control and Prevention released new data late Monday showing a total of 913,268 adverse events following COVID vaccines were reported between Dec. 14, 2020, and Nov. 19, 2021, to the Vaccine Adverse Event Reporting System (VAERS). VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S.
The data included a total of 19,249 reports of deaths — an increase of 396 over the previous week — and 143,395 reports of serious injuries, including deaths, during the same time period — up 4,269 compared with the previous week.
Excluding “foreign reports” to VAERS, 664,745 adverse events, including 8,898 deaths and 56,297 serious injuries, were reported in the U.S. between Dec. 14, 2020, and Nov. 19, 2021.
Foreign reports are reports received by U.S. manufacturers from their foreign subsidiaries. Under U.S. Food and Drug Administration regulations, if a manufacturer is notified of a foreign case report that describes an event that is both serious and does not appear on the product’s labeling, the manufacturer is required to submit the report to VAERS.
Of the 8,898 U.S. deaths reported as of Nov. 19, 20% occurred within 24 hours of vaccination, 26% occurred within 48 hours of vaccination and 56% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 447.7 million COVID vaccine doses had been administered as of Nov. 19. This includes: 260 million doses of Pfizer, 171 million doses of Moderna and 16 million doses of Johnson & Johnson (J&J).
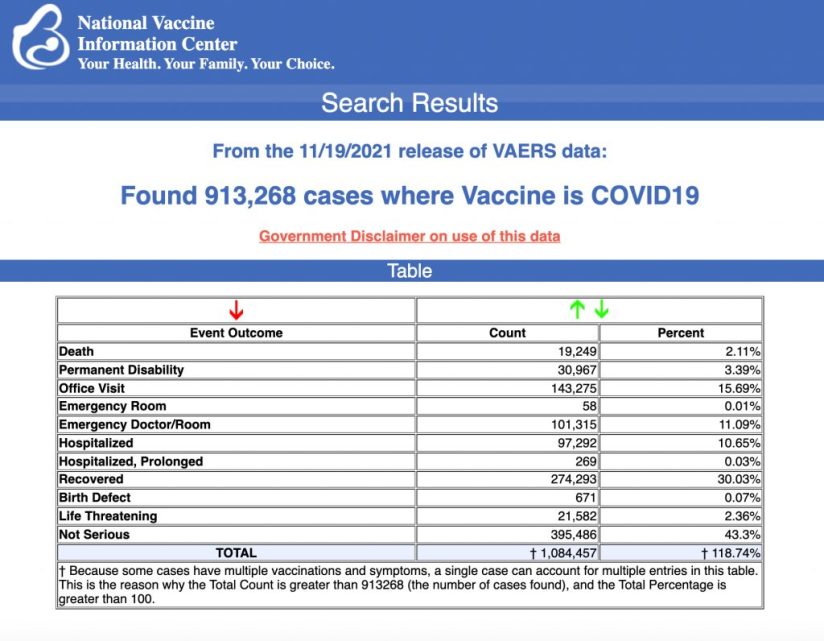
Every Friday, VAERS publishes vaccine injury reports received as of a specified date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed. Historically, VAERS has been shown to report only 1% of actual vaccine adverse events.
U.S. VAERS data from Dec. 14, 2020, to Nov. 19, 2021 for 5- to 11-year-olds show:
- 2,093 total adverse events, including 22 rated as serious and 1 reported death that occurred in an 11-year-old girl from Georgia vaccinated Sept. 14, prior to the authorization of Pfizer’s COVID vaccine in the 5 to 11 age group.
- 1,103 adverse events have been reported in the 5 to 11 age group since Nov. 1.
- The rest of the reports in VAERS for children in the 5 to 11 age group occurred prior to the authorization of Pfizer’s COVID vaccine, and are due to ”product administered to patient of inappropriate age.”
U.S. VAERS data from Dec. 14, 2020, to Nov. 19, 2021 for 12- to 17-year-olds show:
- 23,484 total adverse events, including 1,439 rated as serious and 31 reported deaths.
The most recent death involves a 16-year-old girl from Georgia (VAERS I.D. 1865389) who died reportedly from a heart condition and multi-organ failure two days after receiving Pfizer’s COVID vaccine.
Other recent deaths include a 16-year-old girl from Missouri (VAERS I.D. 1823671) who died after receiving her second dose of Pfizer, and a 17-year-old female from Washington (VAERS I.D. 1828901) who died Oct. 29 reportedly from a heart condition after receiving her second dose of Pfizer.
- 59 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment or resulted in death — with 96% of cases
attributed to Pfizer’s vaccine. - 560 reports of myocarditis and pericarditis (heart inflammation) with 549 cases attributed to Pfizer’s vaccine.
- 139 reports of blood clotting disorders, with all cases attributed to Pfizer.
U.S. VAERS data from Dec. 14, 2020, to Nov. 12, 2021, for all age groups combined, show:
- 19% of deaths were related to cardiac disorders.
- 54% of those who died were male, 42% were female and the remaining death reports did not include gender of the deceased.
- The average age of death was 72.7.
- As of Nov. 19, 4,424 pregnant women reported adverse events related to COVID vaccines, including 1,390 reports of miscarriage or premature birth.
- Of the 3,197 cases of Bell’s Palsy reported, 51% were attributed to Pfizer vaccinations, 41% to Moderna and 8% to J&J.
- 760 reports of Guillain-Barré syndrome (GBS), with 41% of cases attributed to Pfizer, 30% to Moderna and 28% to J&J.
- 2,149 reports of anaphylaxis where the reaction was life-threatening, required treatment or resulted in death.
- 11,209 reports of blood clotting disorders. Of those, 4,960 reports were attributed to Pfizer, 4,000 reports to Moderna and 2,195 reports to J&J.
- 3,209 cases of myocarditis and pericarditis with 1,999 cases attributed to Pfizer, 1,067 cases to Moderna and 133 cases to J&J’s COVID vaccine.
Man with natural immunity forced to get vaccinated against COVID to remain on lung transplant list, dies after second dose of Moderna
Bobby Bolin, a 49-year-old Texas man who previously had COVID, was told he would have to get vaccinated against COVID in order to be eligible for a double-lung transplant, even though he had already recovered from the virus.
After his second Moderna shot, received on April 17, Bolin developed a pulmonary embolism and atrial fibrillation — a heart condition characterized by an irregular heartbeat, shortness of breath, chest pain and extreme fatigue. His health rapidly deteriorated and he passed away Aug. 20, before receiving new lungs.
In an exclusive interview with The Defender, his wife, Amy Bolin, said there was no reason her husband should have been forced to get the vaccine in order to receive new lungs, but unfortunately, he was desperate and very sick.
Amy said she didn’t know what timeline her husband had with his organs, but she saw a complete change in him over four months’ time and doesn’t want others to face the same things they experienced.
Pfizer, Moderna vaccines ‘dramatically increase’ heart attack risk
In an analysis presented during a meeting of the American Heart Association, Dr. Steven Gundry, a pioneer in infant heart transplant surgery, said mRNA COVID vaccines put many patients at higher risk of a new acute coronary syndrome, such as a heart attack.
The analysis concluded in part that mRNA vaccines “dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy and other vascular events following vaccination.”
Thousands of heart-related injuries have been reported following COVID mRNA vaccines, and scientists have established a myriad of heart- and blood-related effects in some patients, including young people.
Among the adverse events linked to the vaccines are thrombosis blood clots and heart inflammation known as myocarditis and pericarditis.
COVID vaccine stocks surge amid fears of new omicron variant
Shares of major COVID vaccine makers surged amid the latest pandemic fears surrounding the new Omicron variant, CNN Business reported.
Moderna climbed more than 20% during Black Friday’s short trading session on Wall Street and increased by an additional 10% on Monday.
Shares of BioNTech, which partners with Pfizer to produce COVID vaccines, soared 14% on Friday and were up 3% Monday, as Pfizer gained 6% Friday.
Investors are hoping the vaccine makers will be able to quickly update their COVID vaccines to offer protection for the Omicron variant.
Moderna said Friday it “will rapidly advance an Omicron-specific booster candidate” while Pfizer said it hoped to have an update of its vaccine ready in 100 days if Omicron shows resistance to its current vaccine.
Moderna CEO predicts reduction in COVID vaccine effectiveness against Omicron variant
Stéphane Bancel, CEO of Moderna, said in an interview Tuesday current COVID vaccines will likely be much less effective against the new Omicron variant, compared with previous variants, The Washington Post reported.
“I just don’t know how much, because we need to wait for the data,” Bancel said. “But all the scientists I’ve talked to … are, like, ‘This is not going to be good.’”
Bancel said scientists did not expect such a highly mutative variant to emerge for another year or two, noting 32 of the 50 mutations in Omicron involve the spike protein — the area targeted by existing COVID vaccines.
In early March, Dr. Geert Vanden Bossche, a vaccinologist who worked with GSK Biologicals, Novartis Vaccines, Solvay Biologicals, Bill & Melinda Gates Foundation’s Global Health Discovery team in Seattle and Global Alliance for Vaccines and Immunization in Geneva, broke down the dangers of mass vaccination for COVID compared to natural infection and concluded:
“There can be no doubt that continued mass vaccination campaigns will enable new, more infectious viral variants to become increasingly dominant and ultimately result in a dramatic incline in new cases despite enhanced vaccine coverage rates. There can be no doubt either that this situation will soon lead to complete resistance of circulating variants to the current vaccines.”
As The Defender reported March 26, a combination of lockdowns and extreme selection pressure on the virus induced by the intense global mass vaccination program, might diminish the number of cases, hospitalizations and deaths in the short-term, but will ultimately induce the creation of more mutants of concern.
This is the result of what Vanden Bossche called “immune escape,” which will in turn trigger vaccine companies to further refine vaccines that will add to, not reduce, the selection pressure, producing ever more transmissible and potentially deadly variants.
Vanden Bossche argued the selection pressure would cause greater convergence in SARS-CoV-2 mutations affecting the spike protein of the virus responsible for breaking through the mucosal surfaces of our airways — the route used by the virus to enter the human body — effectively outsmarting the highly specific antigen-based vaccines that are being used and tweaked, dependent on the circulating variants.
Children’s Health Defense asks anyone who has experienced an adverse reaction, to any vaccine, to file a report following these three steps.
Megan Redshaw is a freelance reporter for The Defender. She has a background in political science, a law degree and extensive training in natural health.
BUY TODAY: Robert F. Kennedy, Jr.’s New Book — ‘The Real Anthony Fauci’
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Northern New England Defies Brandon
el gato malo – bad cattitude – november 30, 2021
the essence of science and scientific credibility is generating a hypothesis, making forward predictions about outcomes, and then testing them to see if you got it right.
it’s really little more than that, but it’s also certainly nothing less.
so let’s take a look at this set of hypotheses and predictions made by the president on august 3rd 2021.
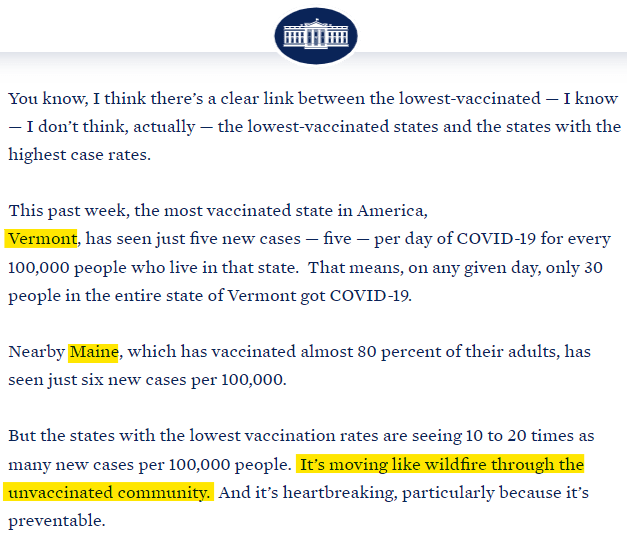
attribution was crystal clear.
so, let’s see how he did on this claim:
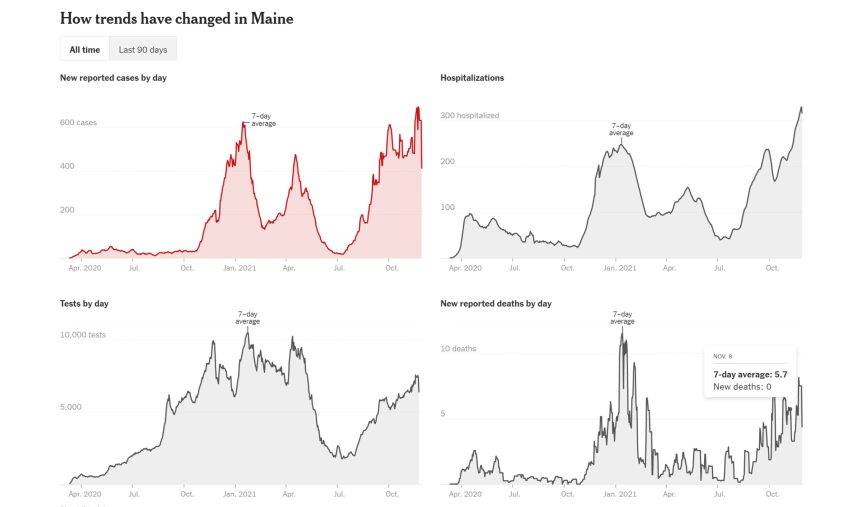
maine is 90% 12 and up vaxxed and more than 99% of the over 65’s . yet it has seen has seen record cases, record hospitalizations and near record deaths despite being nowhere near wheat is usually peak season. that won’t be for 4-6 weeks.
compared to this date last year, hospitalizations are 85% higher.
the lion’s share of hospitalizations are in 70+ with many of the rest in 60-69. this is a 99%+ vaccinated demographic.
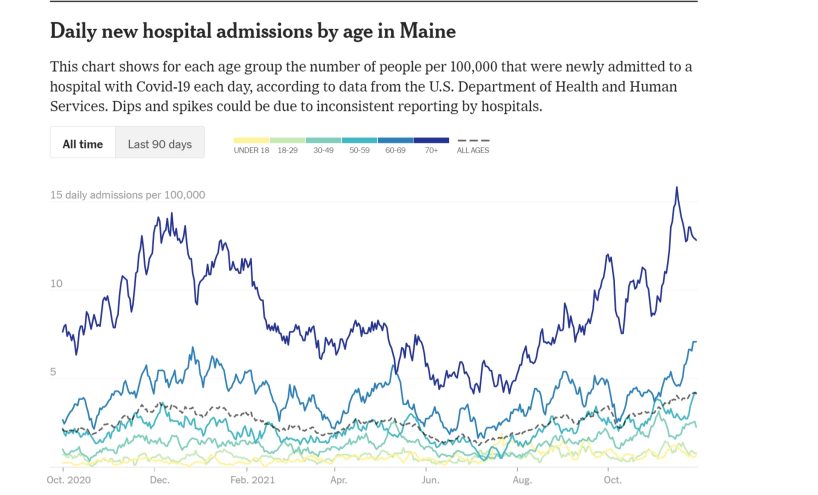
this is NOT a pandemic of the unvaxxed. 70+ already set new highs at 99% vaxxed vs last year’s peak when 0% were DESPITE more natural immunity as well.
new hampshire looks the same. and it’s similarly 4-6 weeks from peak season. 98% of 12 and over vaxxed. 99%+ of over 65’s.
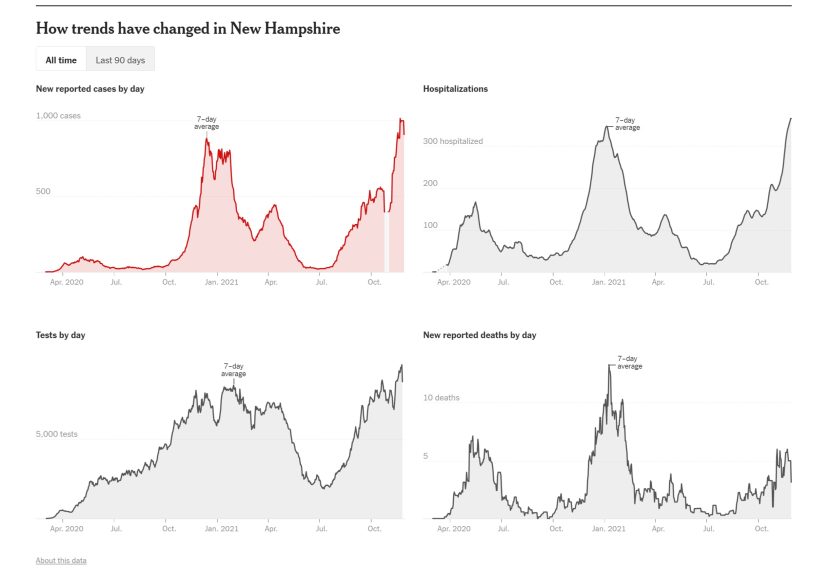
compared to this date last year, hospitalizations are 133% higher.

maybe vermont is better? nope. 94% of over 12’s vaxxed, 99%+ of over 65’s.
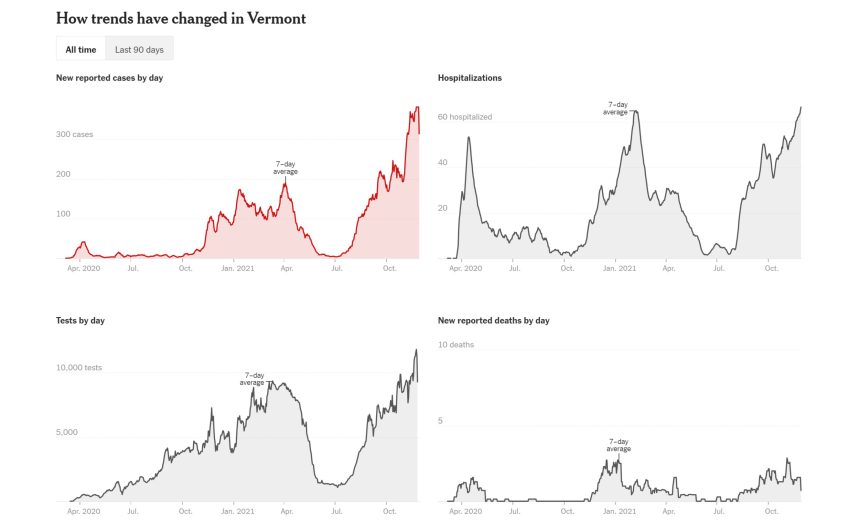
compared to this date last year, hospitalizations are 214% higher.
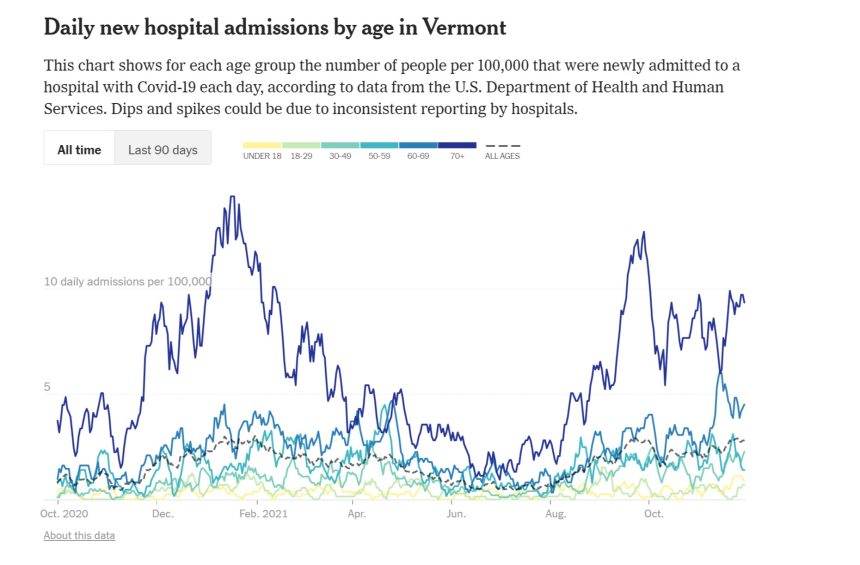
they have all exploded since biden’s claims (made right at about seasonal nadir) and all have vastly exceeded last year at this time. on cases and hospitalization, all have already exceeded last year’s PEAKS (though cases may be affected by testing rates and i have not run the math).
all are 4-6 weeks from what is usually the seasonal peak and just coming into what was the steep ramp last year.
clearly, brandon was trying to pass off seasonality as vaccine efficacy.
this prediction of a “clear link” between vaccines and lower rates and lower severity looks to have failed utterly.
there is simply no other way to put it.
it was just a cross correlation of vaccine rates and latitude.
seasons shifted, and so did covid expression. and vaccines seem to have done little or nothing to stop it.
just like certain internet felines hypothesized.
meanwhile, covid has dropped to the lowest rates since data collection began in the southern states biden and others were so anxious to pillory.
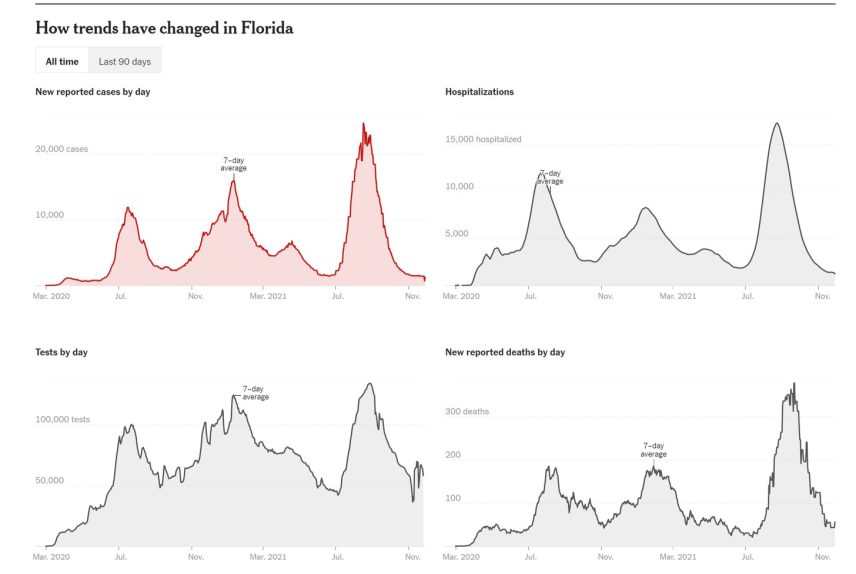
this has been an utter shambles of misinformation and misleading claims coming from DC. the fact that the white house is still getting this astonishingly wrong when the data is so clear that even internet DOGS much less cats are nailing it is inexcusable.
this is either such rank incompetence or such towering mendacity as to disqualify those promulgating it from any future epidemiological utterances, much less determinations on what constitutes disinformation.
The English data on vaccines and mortality, revisited
By Alex Berenson | November 28, 2021
Last Saturday morning I posted a short post with a very simple chart – two lines in all.
One line tracked the number of weekly deaths per 100,000 vaccinated people aged 10-59 in England. The other tracked the number of deaths per 100,000 unvaccinated people in England. The chart showed that vaccinated people in this age group were dying overall at a higher rate than unvaccinated people.
I’m never exactly sure which posts will “land” – gain traction and go viral. This chart landed. Hard. Someone wrote me that it broke the Internet. It didn’t break the Internet, only Kim Kardashian’s ass can break the Internet, but it has rocketed around ever since. It has been seen over 800,000 times on this page alone and many millions more in screenshots and Twitter posts elsewhere.
Clearly, the reason the chart has gained so much attention is that it quickly and simply provides a way for people who are concerned about the vaccines to provide apparent visual proof that they are increasing all-cause mortality – overall death rates.
The chart has also engendered a fierce backlash from the usual fact-checkers and vaccine fanatics who say it is – wait for it – “misinformation.” (To be clear, I didn’t actually create the chart, but I checked the underlying British government report to make sure it accurately represents the report’s figures. It does, as everyone agrees.)
The “fact-checkers” have two primary complaints about the chart.
The first is that the vaccinated and unvaccinated groups are not exactly the same. A smaller percentage of teenagers than fifty-somethings are vaccinated, so the unvaccinated group overall skews somewhat younger than the older group. Since death rates rise with age, that difference may be enough to explain the gap between the two groups.
The second is that overall death rates in people over 60 (who are not covered in the chart) are much higher than those in the 10-59 range and appear to be lower in the vaccinated over the unvaccinated.
Another way to look at the objections: the first is that the chart doesn’t say what it seems to say, because of a hidden flaw in the data. The second is that it would be basically meaningless even if it did, because other more robust datasets contradict it.
—
Part of being on Team Reality is acknowledging reality, and acknowledging when your critics have a factually correct objection. So I want to acknowledge that, like the chart itself, these objections BOTH are valid and factually accurate, viewed individually.
What the fact-checkers and vaccine fanatics appear incapable of understanding is that the two objections effectively cancel each other out – and do nothing to address concerns over the long-term failure of Covid vaccines or their impact on all-cause mortality.
These folks think they are sophisticated thinkers who have blown up apparent evidence that the vaccines are dangerous. In fact, just as they have for the last several months, they are telling themselves what they want to hear instead of listening to what the data are saying – and, increasingly, shouting.
—
They have identified and latched on to ONE complication of using population-level data to judge vaccine effectiveness – the fact that differing rates of uptake by age may make the Covid vaccines seem less effective than they are.
But they – deliberately or out of ignorance – are ignoring another one, one that makes the vaccines seem MORE effective than they are.
The second problem is not a secret to epidemiologists.
It has been quietly discussed for flu vaccines for more than a decade, and I have written about it repeatedly in the last year. The problem is this: the popular belief that sick people are more likely to be vaccinated than healthy people is entirely wrong.
People who receive vaccines are healthier overall than those who do not. They care more about avoiding sickness, and they have the time and energy and money to find their way to a vaccination site. They are not healthier because they get vaccines; they get vaccines because they are healthier.
Older people who receive flu vaccines die – of both the flu and all causes – at much lower rates than unvaccinated people after they receive flu shots. But they also die at much lower rates BEFORE they receive the vaccines. The seminal study demonstrating this relationship is now more than 15 years old; it was published in the International Journal of Epidemiology in April 2006.
“The reductions in risk before influenza season indicate preferential receipt of vaccine by relatively healthy seniors,” the authors wrote.
This paradox helps explain why a huge study of flu vaccines in the United Kingdom showed that increasing vaccination levels in older people did not reduce the number of hospitalizations or deaths from the flu.
The researchers took advantage of the fact that Britain prioritizes people 65 and older for vaccinations and that people are much more likely to get a shot when they are 65 or 66 than 64 or 63. Vaccination levels rose sharply as people turned 65, but the health of the people who received the shots did not improve.

(SOURCE: https://www.acpjournals.org/doi/10.7326/M19-3075?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed)
The same pattern is visible in the United States, where a massive increase in the number of flu vaccines in the last generation has made no apparent difference in the number of flu deaths. In fact, in 2005, researchers noted that although vaccinations had risen from 20 percent of elderly people in 1980 to 65 percent in 2001, “unexpectedly, estimates of influenza-related mortality in this age group also increased [emphasis added] during this period.”
In other words, influenza vaccines only seem to work. Any observational estimate that compares death rates in people who have gotten shots to those who have not will be inherently untrustworthy, no matter how hard researchers try to correct for the healthy recipient bias.
—
What is true for flu vaccines appears to be even more true for Covid vaccines.
The relentless vaccination push means that in many countries, more than 90 percent of elderly people are vaccinated. The split is even more stark in countries like England, where 2.44 million people 80 and over have been fully vaccinated, compared to 69,000 who are unvaccinated (and 24,000 who have received the first dose but not the second).
Look at those numbers again.
2,440,000 people in England 80 and over vaccinated. Almost 97 percent of the total number of elderly people.
69,000 80 and over unvaccinated. Less than 3 percent.
These two groups cannot remotely be compared.
How do they differ? I can’t find any hard data, but we know that at least a fraction of the elderly unvaccinated are too ill to be vaccinated. Some are in hospice care. Norway recommended against giving people in hospice the Covid vaccine in January following deaths in terminally ill patients.

A paper published online in March in the Journal of Pain and Symptom Management noted that “communication from hospice organizations has primarily emphasized the vaccination of hospice staff without the same priority mention for patients” and called for hospices to do more to offer vaccines to patients.
The paper’s title was even starker:
A Shot at Inclusion: Reconsidering Categorical Exclusion of Hospice Patients from COVID Vaccine Allocation.
How many Covid deaths in unvaccinated elderly people are actually “with Covid” deaths in people dying in hospice? Again, we don’t know. But what we know is that even a small number of those deaths will hopelessly bias the relative risk ratio for unvaccinated to vaccinated Covid deaths, because the overall number of unvaccinated people is so small.
As of September, about 30 to 35 unvaccinated English people 80 and over died of or with Covid each week, compared to about 250 fully vaccinated people a week.
So trying to measure vaccine effectiveness by looking at the relative risks of the vaccinated and unvaccinated elderly is impossible. But that is exactly what the health authorities and their servants in the media do when they put out figures that seem to show the risk of death from Covid is much lower in elderly people who have been vaccinated.
They are lying with truthful data, and they (some of them, anyway, though probably not the reporters who are writing the stories) are smart enough to know exactly what they’re doing.
—
Meanwhile, they are ignoring a much more important indicator – trends in both Covid and all-cause mortality are very much going the wrong way in the vaccinated elderly population.
In the last four weeks for which British data are available, roughly coinciding with September, about 1,000 vaccinated English people 80 and over died from Covid and 16,000 from all causes.
Compare those numbers to four weeks in May, when fewer than 70 vaccinated English people 80 and over died from Covid and 13,000 from all causes.
Put another way, overall deaths rose more than 20 percent in the vaccinated elderly from May to September, and Covid deaths 15-fold. And this was not because many more people were vaccinated. The number of vaccinated elderly people rose only about 4 percent from May to September.
Compare that to the mortality trends in unvaccinated English people 80 and over.
About 800 died of all causes in four weeks in May (at the time, there were about 77,000 unvaccinated elderly people, compared to 69,000 in September). Fewer than 20 of those died of Covid.
In September, about 140 unvaccinated elderly people died of Covid – a eight-fold increase compared to the 15-fold increase in the vaccinated.
(All data from the British government:
See tables 3 and 4 in downloaded file.)
But that difference isn’t the striking part.
The striking part is that only 700 unvaccinated elderly English people died OF ALL CAUSES in those four weeks in September – FEWER than back in May. (The trend roughly tracked the overall drop in the elderly unvaccinated population. It appears that about 1 percent of those folks die a month, at least in warmer months.)
This trend is stunning for two reasons.
First, the fact that 100 more unvaccinated elderly people (supposedly) died of Covid in September yet 100 fewer of them died overall strongly suggests that many of those reported deaths are actually with and not from Covid.
Second, per capita all-cause mortality – not just Covid mortality, all-cause mortality – rose close to 20 percent in the very large group of the vaccinated elderly. Some of those extra deaths came from Covid. But most did not.
And though death rates are still somewhat higher in the unvaccinated – as they should be, given the fact that vaccine recipients are healthier – but that fact is far less relevant than the notable rise in the vaccinated.
What’s behind the rise in those deaths in the vaccinated elderly? We don’t know. But we’d better find out. Especially since we are now stuffing boosters into their arms.
—
All of this is somewhat complicated, I’ll admit. The data has lots of confounders and continues to evolve. And trying to explain relative changes in all-cause mortality in the context of healthy vaccine recipient bias using papers about flu vaccine – well, it’s not a soundbite.
Which comes back to the chart from last week.
The chart IS a soundbite.
It is a simple and factually accurate way to say:
Something is wrong. The promises that the health authorities have made over the last 12 months about the vaccines are not coming true. Despite near-complete levels of adult vaccination in Europe, many countries are seeing skyrocketing Covid cases and deaths. And worst of all, all-cause non-Covid mortality is running well above normal in country after country.
Not everyone is going to wade through this article. But everyone can read that chart from last week. It’s not perfect, but it uses real data to raise a crucial issue.
That’s why it landed. And that’s why the vaccine fanatics hate it so much.
What’s the Truth About Covid Vaccines and Heart Attacks?
By Will Jones • The Daily Sceptic • November 27, 2021
A further three football players collapsed during play this week, bringing new interest to the question of what might be the connection between this unusually high number of on-field medical emergencies and the Covid vaccines. Football pundit Trevor Sinclair got into hot water for raising the question on-air, while scientists argued that the disturbing trend is more likely to be a consequence of Covid itself than the vaccines.
Presumably something lies behind the recent rise, which according to some analysts has involved 21 sudden deaths (most heart-related) of FIFA players so far in 2021, compared to around 4.2 in an average year (with a standard deviation of 2.0). Assuming this isn’t a reporting phenomenon, this is an extraordinary spike and highly statistically significant.
The two major unusual factors this year are the presence of SARS-CoV-2 and the Covid vaccination programme. However, only two such deaths were reported in 2020, when Covid was also around, which would seem to lend weight to a vaccine explanation.
The vaccines are known to affect the heart and cardiovascular system in some cases, which is why blood clots and heart inflammation (e.g. myocarditis) are among the side-effects listed and why a number of countries have ceased using some of the vaccines in younger age groups. This means the idea that there could be a link between an unusual spate of heart-related emergencies and the vaccines shouldn’t be dismissed out of hand.
On the other hand, some studies have shown that the risk of developing myocarditis is substantially higher following SARS-CoV-2 infection than vaccination.
A number of scientists have pointed out that insofar as cardiovascular problems arise from the effect of the SARS-CoV-2 spike protein (and there seems to be some agreement that the spike protein is a large part of the causal story here) a bout of SARS-CoV-2 exposes the body to at least as much spike protein as a course of vaccination. Against that, those who suspect that the vaccines are playing a key role say that in fact most SARS-CoV-2 infections are not systemic but remain localised to the respiratory system, so have little impact on the cardiovascular system, whereas vaccination always allows the spike protein to have a systemic impact by gaining easy access to the bloodstream.
This matter would seem to merit much closer and more urgent attention than it appears to be receiving from regulators. It should be straightforward for those with access to the relevant data (most of which unfortunately is not publicly available) to analyse cardiovascular deaths according to vaccination status and prior infection status to see if there are patterns that may be a signal of concern.
An abstract appeared in the leading journal Circulation earlier this month which concluded: “The mRNA vaccines dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy, and other vascular events following vaccination.” There was no study to accompany the abstract, however, and it has been heavily criticised by some specialists. Nonetheless, leading NHS Consultant Cardiologist Dr Aseem Malhotra stuck his neck out this week on GB News to reveal that a cardiology researcher colleague found similar results, but was not prepared to publish for fear of the repercussions for his or her career: “They aren’t going to publish their findings, they are concerned about losing research money.”
What are the wider trends in deaths?
Since July, ONS data shows there have been 20,823 excess deaths in England and Wales, with 11,531 involving Covid, leaving 9,292 excess deaths from other causes (if we make the conservative assumption that all Covid deaths are excess deaths).
Analysis of cause of death data for England shows that between July 4th and November 5th 2021 there have been 3,095 excess deaths involving heart failure, of which 854 could be put down to COVID-19, leaving 2,241 from other causes; 4,460 excess deaths involving ischaemic heart diseases, of which 1,413 could be Covid, leaving 3,047 from other causes; 1,307 excess deaths involving cerebrovascular diseases, of which 489 could be Covid, leaving 818 from other causes; and 8,109 excess deaths involving ‘other circulatory diseases’, of which 3,357 could be Covid, leaving 4,752 from other causes. These categories can overlap – a death certificate can mention more than one of them – so the figures can’t simply be added to get a grand total, and the underlying cause could be recorded as something different. Nonetheless, we are talking about thousands of additional cardiovascular deaths since the summer.
Despite this, ONS data shows that deaths where the underlying cause was cardiovascular have been below average in this period. At the same time, deaths where Covid is recorded as the underlying cause account for only a fraction of cardiovascular deaths in the period. So what was the underlying cause of all these excess deaths involving cardiovascular conditions that weren’t Covid either? A query to the ONS came back suggesting that it was down to the significant excess in deaths where the underlying cause was recorded as “symptoms, signs and ill-defined conditions”. In other words, we don’t really know. So according to official data, there have been thousands of excess deaths involving cardiovascular conditions in the past four months, but the underlying cause of many of those deaths is unknown. This would seem to warrant further investigation, and since the vaccines may be implicated, without delay.
31,014 Deaths 2,890,600 Injuries Following COVID Shots in European Database of Adverse Reactions
Young, Previously Healthy People Continue to Die
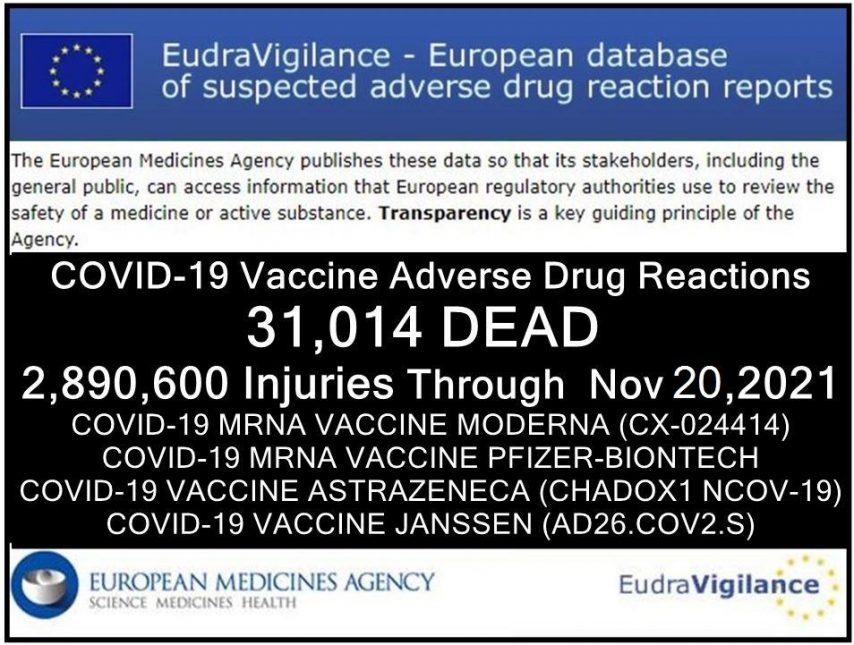
By Brian Shilhavy | Health Impact News | November 28, 2021
The European Union database of suspected drug reaction reports is EudraVigilance, and they are now reporting 31,014 fatalities, and 2,890,600 injuries, following COVID-19 injections.
A Health Impact News subscriber from Europe reminded us that this database maintained at EudraVigilance is only for countries in Europe who are part of the European Union (EU), which comprises 27 countries.
The total number of countries in Europe is much higher, almost twice as many, numbering around 50. (There are some differences of opinion as to which countries are technically part of Europe.)
So as high as these numbers are, they do NOT reflect all of Europe. The actual number in Europe who are reported dead or injured following COVID-19 shots would be much higher than what we are reporting here.
The EudraVigilance database reports that through November 20, 2021 there are 31,014 deaths and 2,890,600 injuries reported following injections of four experimental COVID-19 shots:
- COVID-19 MRNA VACCINE MODERNA (CX-024414)
- COVID-19 MRNA VACCINE PFIZER-BIONTECH
- COVID-19 VACCINE ASTRAZENECA (CHADOX1 NCOV-19)
- COVID-19 VACCINE JANSSEN (AD26.COV2.S)
From the total of injuries recorded, almost half of them (1,355,192) are serious injuries.
“Seriousness provides information on the suspected undesirable effect; it can be classified as ‘serious’ if it corresponds to a medical occurrence that results in death, is life-threatening, requires inpatient hospitalisation, results in another medically important condition, or prolongation of existing hospitalisation, results in persistent or significant disability or incapacity, or is a congenital anomaly/birth defect.”
A Health Impact News subscriber in Europe ran the reports for each of the four COVID-19 shots we are including here. It is a lot of work to tabulate each reaction with injuries and fatalities, since there is no place on the EudraVigilance system we have found that tabulates all the results.
Since we have started publishing this, others from Europe have also calculated the numbers and confirmed the totals.*
Here is the summary data through November 20, 2021.
Total reactions for the mRNA vaccine Tozinameran (code BNT162b2, Comirnaty) from BioNTech/ Pfizer: 14,526 deaths and 1,323,370 injuries to 20/11/2021
- 35,826 Blood and lymphatic system disorders incl. 207 deaths
- 40,230 Cardiac disorders incl. 2,128 deaths
- 376 Congenital, familial and genetic disorders incl. 33 deaths
- 17,995 Ear and labyrinth disorders incl. 10 deaths
- 1,217 Endocrine disorders incl. 5 deaths
- 20,443 Eye disorders incl. 32 deaths
- 110,658 Gastrointestinal disorders incl. 585 deaths
- 337,450 General disorders and administration site conditions incl. 4,118 deaths
- 1,502 Hepatobiliary disorders incl. 75 deaths
- 14,528 Immune system disorders incl. 76 deaths
- 53,108 Infections and infestations incl. 1561 deaths
- 20,222 Injury, poisoning and procedural complications incl. 240 deaths
- 33,067 Investigations incl. 451 deaths
- 9,103 Metabolism and nutrition disorders incl. 249 deaths
- 164,885 Musculoskeletal and connective tissue disorders incl. 179 deaths
- 1,163 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 114 deaths
- 225,032 Nervous system disorders incl. 1,556 deaths
- 1,851 Pregnancy, puerperium and perinatal conditions incl. 55 deaths
- 206 Product issues incl. 2 deaths
- 24,225 Psychiatric disorders incl. 174 deaths
- 4,667 Renal and urinary disorders incl. 224 deaths
- 43,949 Reproductive system and breast disorders incl. 5 deaths
- 57,013 Respiratory, thoracic and mediastinal disorders incl. 1,617 deaths
- 62,414 Skin and subcutaneous tissue disorders incl. 125 deaths
- 2,765 Social circumstances incl. 19 deaths
- 4,797 Surgical and medical procedures incl. 60 deaths
- 34,678 Vascular disorders incl. 626 deaths
Total reactions for the mRNA vaccine mRNA-1273 (CX-024414) from Moderna: 8,518 deaths and 390,163 injuries to 20/11/2021
- 8,227 Blood and lymphatic system disorders incl. 94 deaths
- 12,657 Cardiac disorders incl. 915 deaths
- 156 Congenital, familial and genetic disorders incl. 6 deaths
- 4,698 Ear and labyrinth disorders incl. 2 deaths
- 348 Endocrine disorders incl. 3 deaths
- 5,731 Eye disorders incl. 29 deaths
- 32,091 Gastrointestinal disorders incl. 326 deaths
- 104,720 General disorders and administration site conditions incl. 2,986 deaths
- 644 Hepatobiliary disorders incl. 40 deaths
- 3,820 Immune system disorders incl. 16 deaths
- 14,668 Infections and infestations incl. 782 deaths
- 8,158 Injury, poisoning and procedural complications incl. 162 deaths
- 7,117 Investigations incl. 143 deaths
- 3,703 Metabolism and nutrition disorders incl. 206 deaths
- 47,355 Musculoskeletal and connective tissue disorders incl. 174 deaths
- 531 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 67 deaths
- 66,320 Nervous system disorders incl. 823 deaths
- 722 Pregnancy, puerperium and perinatal conditions incl. 6 deaths
- 78 Product issues incl. 2 deaths
- 7,100 Psychiatric disorders incl. 142 deaths
- 2,277 Renal and urinary disorders incl. 164 deaths
- 8,061 Reproductive system and breast disorders incl. 7 deaths
- 17,235 Respiratory, thoracic and mediastinal disorders incl. 914 deaths
- 20,963 Skin and subcutaneous tissue disorders incl. 76 deaths
- 1,769 Social circumstances incl. 36 deaths
- 1,374 Surgical and medical procedures incl. 78 deaths
- 9,640 Vascular disorders incl. 319 deaths
Total reactions for the vaccine AZD1222/VAXZEVRIA (CHADOX1 NCOV-19) from Oxford/AstraZeneca: 6,145 deaths and 1,075,335 injuries to 20/11/2021
- 13,124 Blood and lymphatic system disorders incl. 248 deaths
- 19,128 Cardiac disorders incl. 696 deaths
- 195 Congenital familial and genetic disorders incl. 8 deaths
- 12,669 Ear and labyrinth disorders incl. 3 deaths
- 597 Endocrine disorders incl. 4 deaths
- 18,919 Eye disorders incl. 29 deaths
- 102,402 Gastrointestinal disorders incl. 312 deaths
- 283,288 General disorders and administration site conditions incl. 1,469 deaths
- 950 Hepatobiliary disorders incl. 60 deaths
- 4,834 Immune system disorders incl. 29 deaths
- 32,441 Infections and infestations incl. 413 deaths
- 12,358 Injury poisoning and procedural complications incl. 177 deaths
- 23,611 Investigations incl. 150 deaths
- 12,369 Metabolism and nutrition disorders incl. 91 deaths
- 159,668 Musculoskeletal and connective tissue disorders incl. 94 deaths
- 624 Neoplasms benign malignant and unspecified (incl cysts and polyps) incl. 22 deaths
- 221,536 Nervous system disorders incl. 958 deaths
- 521 Pregnancy puerperium and perinatal conditions incl. 12 deaths
- 188 Product issues incl. 1 death
- 19,933 Psychiatric disorders incl. 58 deaths
- 4,031 Renal and urinary disorders incl. 58 deaths
- 15,124 Reproductive system and breast disorders incl. 2 deaths
- 37,980 Respiratory thoracic and mediastinal disorders incl. 735 deaths
- 49,247 Skin and subcutaneous tissue disorders incl. 48 deaths
- 1,498 Social circumstances incl. 6 deaths
- 1,404 Surgical and medical procedures incl. 25 deaths
- 26,696 Vascular disorders incl. 437 deaths
Total reactions for the COVID-19 vaccine JANSSEN (AD26.COV2.S) from Johnson & Johnson: 1,825 deaths and 101,732 injuries to 20/11/2021
- 986 Blood and lymphatic system disorders incl. 40 deaths
- 1,837 Cardiac disorders incl. 155 deaths
- 35 Congenital, familial and genetic disorders
- 1,033 Ear and labyrinth disorders incl. 2 deaths
- 69 Endocrine disorders incl. 1 death
- 1,351 Eye disorders incl. 7 deaths
- 8,500 Gastrointestinal disorders incl. 75 deaths
- 26,871 General disorders and administration site conditions incl. 488 deaths
- 121 Hepatobiliary disorders incl. 11 deaths
- 445 Immune system disorders incl. 9 deaths
- 4,315 Infections and infestations incl. 143 deaths
- 920 Injury, poisoning and procedural complications incl. 18 deaths
- 4,766 Investigations incl. 103 deaths
- 625 Metabolism and nutrition disorders incl. 45 deaths
- 14,897 Musculoskeletal and connective tissue disorders incl. 43 deaths
- 54 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 3 deaths
- 20,097 Nervous system disorders incl. 197 deaths
- 41 Pregnancy, puerperium and perinatal conditions incl. 1 death
- 26 Product issues
- 1,407 Psychiatric disorders incl. 16 deaths
- 417 Renal and urinary disorders incl. 22 deaths
- 2,059 Reproductive system and breast disorders incl. 6 deaths
- 3,617 Respiratory, thoracic and mediastinal disorders incl. 234 deaths
- 3,094 Skin and subcutaneous tissue disorders incl. 8 deaths
- 319 Social circumstances incl. 4 deaths
- 690 Surgical and medical procedures incl. 54 deaths
- 3,140 Vascular disorders incl. 140 deaths
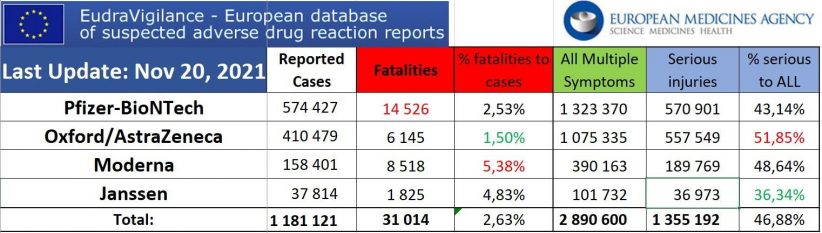
*These totals are estimates based on reports submitted to EudraVigilance. Totals may be much higher based on percentage of adverse reactions that are reported. Some of these reports may also be reported to the individual country’s adverse reaction databases, such as the U.S. VAERS database and the UK Yellow Card system. The fatalities are grouped by symptoms, and some fatalities may have resulted from multiple symptoms.
Featured Video

“Trump’s presidency is at risk of being destroyed” Col Douglas Macgregor
or go to
Aletho News Archives – Video-Images
From the Archives
Infertility: A Diabolical Agenda
Dr. Joseph Mercola | July 9, 2022
“Infertility: A Diabolical Agenda,” is the fourth vaccine-related documentary by Dr. Andrew Wakefield. It tells the story of an intentional infertility vaccine program conducted on African women, without their knowledge or consent.
While it’s been brushed off as a loony conspiracy theory for years, there’s compelling evidence showing it did, in fact, happen, and there’s nothing to prevent it from happening again. … continue
Blog Roll
 Aletho News
Aletho News- Israeli strikes kill 10 in southern Lebanon, including 3 rescue workers
- Israeli military ‘failed on all fronts’: Poll
- US at a crossroads: Iran’s firm positions leave Trump no option but to capitulate
- Iran signals decisive response to end US maritime bullying, piracy
- Trump eager for off-ramp in war on Iran, but Netanyahu has him trapped: Former official
- Trump’s ‘Golden Dome’ offers ‘limited’ shield against ballistic missiles: Defense official
- Ukraine Seeks to Provoke a Nuclear Conflict: Zakharova
- US squares up to China over Panama Canal
- Monroe Doctrine 2.0: ‘Great Reset’ for US Imperialism?
- Nuclear Apartheid: Iran’s Rise Exposes the NPT Fraud and the West’s Israel Exception
- If Americans Knew
- How Tony Dokoupil Became the Face of ‘Zionist Fanatic’ Bari Weiss’s CBS
- Far Right Israeli Settler Movement Enters Syria in a Push for “Greater Israel”
- ‘People Have the Right to Be Buried’: In Gaza, Thousands of Palestinians Remain Trapped Under Rubble
- Born during Israel’s genocide: Gaza’s child survivors bear the scars of war
- Who are the women and girls behind Gaza war’s horrific casualty toll?
- Beloved Gaza doctor detained “indefinitely” without charge – Daily Update
- By Week’s End, Trump’s War Will Be Plainly Illegal
- CBS News Reportedly Ousts London Bureau Chief Over Differences With Bari Weiss Over Gaza Coverage
- State Department Says US Is in Conflict With Iran ‘At the Request’ of Israel
- What ceasefire? Israel won’t stop killing in Gaza, Lebanon – Daily Update
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
