Higher Infection Rates in Vaccinated Not an Artefact of Wrong Population Data, New Analysis Shows
By Will Jones • The Daily Sceptic • November 26, 2021
Back in October, when the critics rounded on the UKHSA for publishing vaccine data that didn’t fit the narrative, front and centre of their complaints was the claim that they were using poor estimates of the size of the unvaccinated population, and thus underestimating the infection rate in the unvaccinated. Cambridge’s Professor David Speigelhalter didn’t hold back, writing on Twitter that it was “completely unacceptable” for the agency to “put out absurd statistics showing case-rates higher in vaxxed than non-vaxxed” when it is “just an artefact of using hopelessly biased NIMS population estimates”.
To the UKHSA’s credit, while it conceded other points, it never gave in on this one, sticking to its view that the National Immunisation Management System (NIMS) was the “gold standard” for these estimates. It pointed out that ONS population estimates have problems of their own, not least that for some age groups the ONS supposes there to be fewer people in the population than the Government counts as being vaccinated.
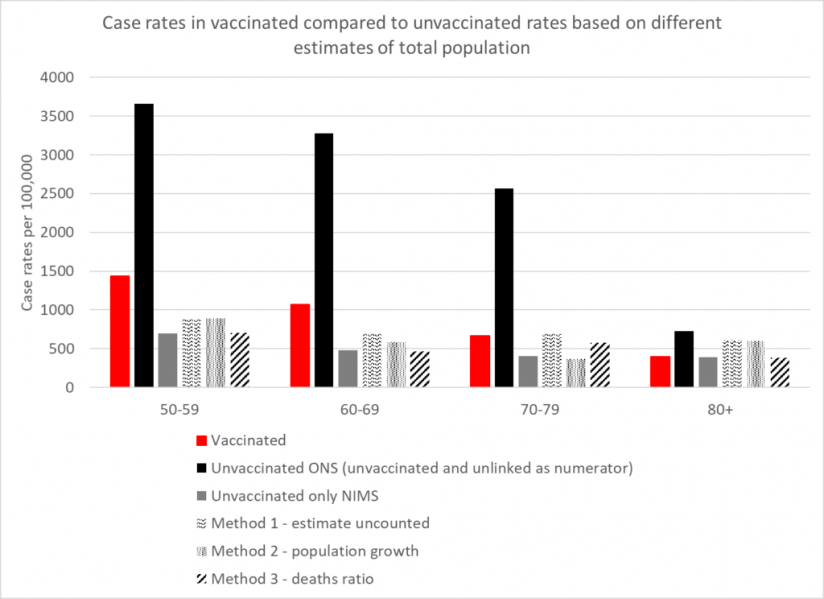
How can we know which estimates are more accurate? A group of experts has applied analytical techniques in order to estimate the size of the unvaccinated population independently of ONS and NIMS figures. Using three different methods, experts from HART found that estimates from all three methods were in broad agreement with the NIMS estimates, whereas the ONS estimate was a much lower outlier.
The first method involves recognising that people not within the NHS database system still catch Covid and still get tested. Assuming these people have the same infection rates per 100,000 people as the unvaccinated, you can calculate how many people there are outside of the database system and add these to the NIMS totals.
The second method involves looking at the rate of growth of people with an NHS number, which has been remarkably steady at around 2.9% per year. If you assume that people who are not yet registered in the NHS will sometimes become sick enough to seek healthcare, and thus a record will be created for them, applying this growth rate to the 2011 ONS population estimates give another figure for the total population.
The third method involves assuming that, in low-Covid weeks, deaths within an age bracket should occur at a similar rate in vaccinated and unvaccinated, allowing the size of the total population to be inferred from the percentage of deaths in the unvaccinated.
The results in terms of reported infection rates according to the five different estimates are depicted in the chart above. They show that the ONS is a clear outlier, its estimates sitting far too low, and NIMS is likely to be much more accurate. The ONS puts the unvaccinated population at around 4.59 million whereas NIMS puts it at 9.92 million, a difference of 5.33 million. That’s a lot of people not to be included in estimates, and suggests, among other things, that the ONS has not adequately estimated the magnitude of illegal immigration into the country.
As well as vindicating the UKHSA in its decision to stick with NIMS over ONS, HART’s analysis also indicates that, contrary to the assertions of Prof Spiegelhalter, the UKHSA data showing infection rates higher in the vaccinated compared to the unvaccinated is not a mere artefact of using the wrong population estimates. There may be other biases in it, but this is not one of them.
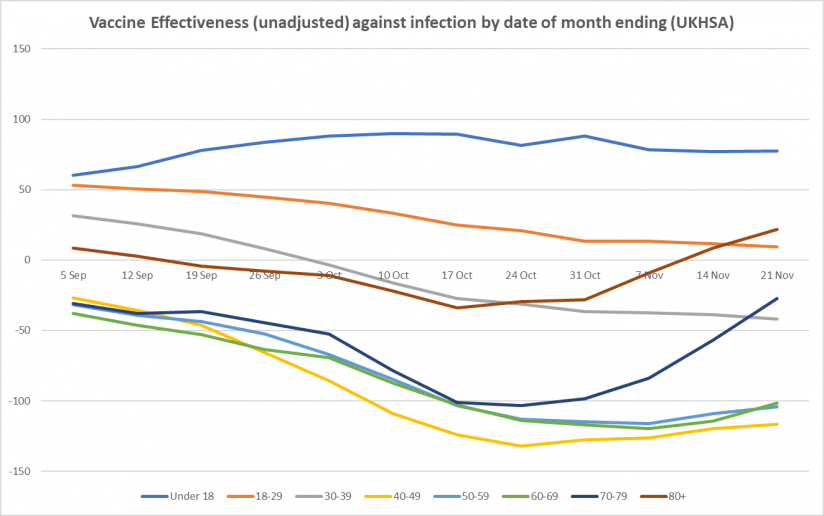
Here is the weekly update on unadjusted vaccine effectiveness based on the raw data in the UKHSA Vaccine Surveillance report. The unadjusted vaccine effectiveness estimates against infection have remained low in all adult age brackets this week, particularly in those aged 40-70, though there is little sign of further decline; in the older age groups (over 40), the recent vaccine effectiveness revival continues, possibly as a result of the third doses. There is also a sign of a rise in vaccine effectiveness against hospitalisation in the over-70s.



more early takes on omicron variant
reports from SA indicate that the virus is VERY mild
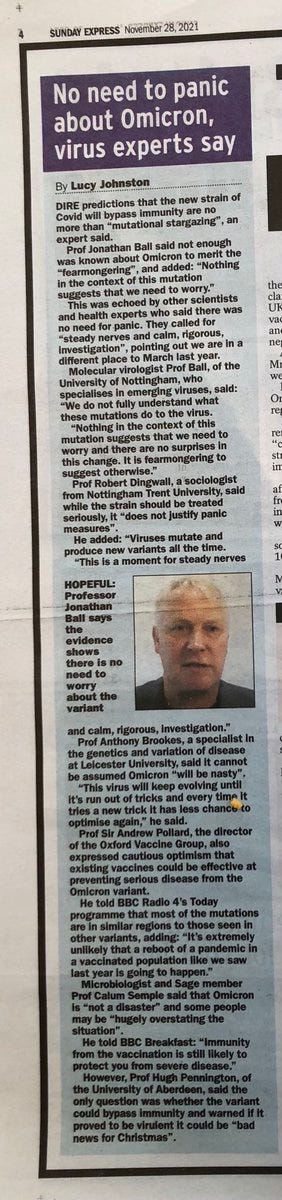
el gato malo | bad cattitude | november 28, 2021
aside from all the breathless reporting about “MOAR SPIKE MUTATIONS!!” i have yet to see a single report with any actual clinical evidence that the newly branded omicron variant is anything other than less dangerous than delta was.
it’s just, to steal a wonderful quote “mutational stargazing.”

this makes sense. not only are we continuing to evolve AWAY from an what looks near certain to be a lab engineered virulence optimum, but this is the natural path of viral evolution.
delta was a deeply attenuated version of prior versions. it’s original CFR was around 0.1%. this rose sharply over the summer as vaccine fade hit and this rise affected the vaccinated and the unvaccinated alike, so it appears to be a property of the virus, not of the vaccines. it was also mirrored by all cause mortality and so appears to be a real rise in fatality, not a definitional artifact.
i will still bet dollars to doughnuts that it was the vaccines themselves that, by being leaky but semi-protective, drove this inverted gradient to hotter strains.
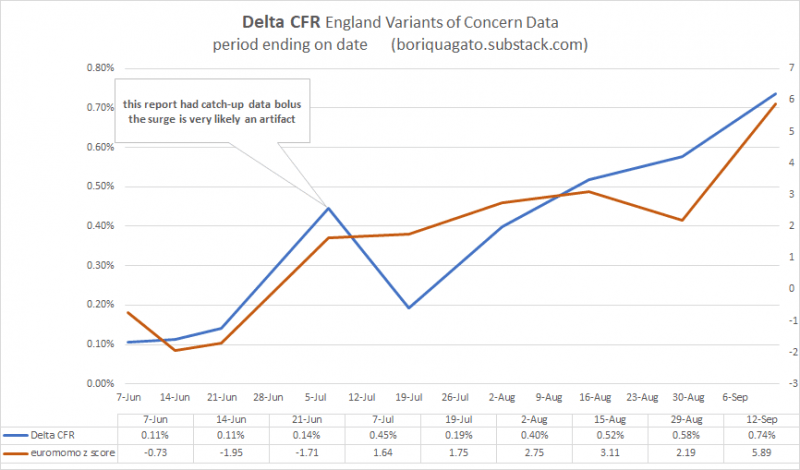
full discussion and data HERE.
a virus “wants” one thing: to spread. make a copy of me and pass it on. that’s the whole ballgame. harming the host and incapacitating them is maladaptive to this goal. mild viruses spread better. asymptomatic viruses spread best of all.
and that looks more and more like the case here. omicron looks milder than delta, especially than the souped up delta strains that emerged over the summer.

this is good news, not a reason for terror. the ideal outcome would be a virus with no symptoms and infinite spread that would immediately inoculate everyone.
primary symptoms appear to be lethargy. loss of taste and smell is largely absent.
as this virus looks to outcompete delta, but with lower risk, the idea that we want to keep it out seems exactly wrong. this is the variant you want. more spread, considerably less risk, mostly asymptomatic, but will generate the real, sterilizing immunity that the vaccines do not.
this is how pandemics end, not how panics should begin.
watching the west once more lose its collective mind is just pathetic.
based on the early looks, this is not even a chipmunk in the road to swerve around, it’s the shadow of a chimpunk and it’s a less dangerous strain that the one we currently have and another even lower risk bite at the immunity apple.
whether it will follow delta in terms of vaccine mediated evolution toward hotter future strains is anyone’s guess (and certainly possible) but if it is, indeed, destined to do so, then that’s all the more reason to let it spread now.
“we should panic in case it turns out we need to panic” is simply not a basis for public health.
pandemics can and do end themselves and it’s become manifestly obvious that the vaccines developed here and pushed endlessly as panacea are of little to no help in that regard and quite a strong case to be made that they have made it, overall, worse for everyone, including the vaccinated.
boosters, lockdowns, and travel bans are not the way out. the generation of low risk natural herd immunity is.
it is long past time we stopped playing these stupid games.
the prizes we stand to win are not going to get any less stupid this time…
We are mandating a vaccine where there is no scientific evidence that it has ever saved a single life
BMJ notes we will NEVER have the evidence, vaccine makers structured the trials to avoid proving an all-cause mortality benefit since they know it’s negative
By Steve Kirsch | November 27, 2021
If you are are still in doubt as to whether we are being hoodwinked on the safety and efficacy of the COVID vaccines, this Editorial in the BMJ today should remove all doubt. We are being hoodwinked. And it’s not going to get better. Ever. So we are stuck with a vaccine that is being mandated where most people have no fu*&($#ing clue as to whether it works or not.
Why? It’s simple. They know full well from the VAERS data that the vaccine kills far more people than it saves (regardless of age) and they want to make sure you will never find out.
Get it?
Those of us who know how to interpret the safety data from VAERS and other similar systems know full well what is going on, but when we try to warn people, we are being marginalized as spreaders of misinformation. Who’s lying? Well, suffice it to say that no self-proclaimed VAERS expert will agree to a debate.
Note: For those of you upset about the headline, sure, they can argue that the COVID vaccines saved people from dying from COVID. I concede that. But the all-cause mortality (ACM) rate (which nobody is looking at), has always been far greater than the COVID lives saved.
And that my friends is the inconvenient truth.

Canadian landlord says tenants need to show a vaccine passport to live in building
By Christina Maas | Reclaim The Net | November 27, 2021
Strategic Group, a major rental housing provider in Alberta, Canada, announced that all new tenants need to show a vaccine passport to live in its properties. Critics claim the renter’s vaccine mandate sets a dangerous precedent.
“Vaccination of everyone in our community is the only way we are going to get through this pandemic and back to a sense of normalcy,” said Riaz Mamdani, founder and CEO of Strategic Group, in an October 28 press release.
“The safety of our team and our residents is a top priority, so ensuring full vaccination across the board is the least we can do.”
The press release said that “all employees, residents, and prospective residents” have to be vaccinated. Existing tenants will have to show proof of vaccination. Anyone “unable to be vaccinated (i.e., children under the age of 12) is exempt until able to receive the vaccine.”
“These rules apply to all of Strategic Group’s residential communities in Alberta.”
The renter owns more than 100 1 and 2-bedroom units in Edmonton and Calgary.
The Canadian Press reported that the Strategic Group COO Tracey Steman said that the company was “very proud” of the mandatory vaccination policy.
“And we’d like to see other landlords implement the same policy… It will help to end this pandemic,” Steman continued. “We’ve had really good feedback from our tenants.”
According to the company’s CEO, residents inspired the new policy as they were saying that “they value knowing that all their neighbors are vaccinated – they feel even safer in their own homes.”
Eva Chipiuk of the Justice Center for Constitutional Freedoms (JCCF) told LifeSiteNews that Strategic Group’s vaccine mandate for tenants “sets a dangerous precedent in Alberta and in Canada.”
“According to this renter’s policy, you do not deserve a roof over your head unless you have taken an experimental injection,” said Chipiuk.
“Such a policy, utterly unthinkable two years ago, is now frighteningly announced with pride,” she added.
“Under what authority is this policy being made?”
Chipiuk noted that the laws banning smoking indoors were discussed in “government housing.”
“This is not the same. These rental companies are taking the law into their own hands. If we allow this to happen, what will be next and who will find themselves without a place to live?” the lawyer asked.
In an article on The Lawyers Daily, landlord-tenant lawyer Caryma Sa’d explained why it is illegal for landlords to enforce vaccine passport mandates for tenants. Sa’d noted that refusing a potential client because of their vaccination status is discrimination.
Also, “landlords cannot simply make unilateral changes to the terms of the agreement, which would include imposing proof of vaccination as a condition of the tenancy.”
“This would prevent a landlord from attempting to evict a tenant based on vaccination status, unless it can be established that the tenant is substantially interfering with the reasonable enjoyment of others within the unit or otherwise causing serious problems at the residential complex because of their vaccination status,” the lawyer continued.
The president of the Canadian Federation of Apartment Associations John Dickie told the Canadian Press that it was “possible” for some landlords to follow Strategic Group’s lead and implement a vaccine passport mandate, but that was not likely to be “very widespread.”
“We’re not the health police,” said Dickie.
“Rental housing providers realize people need housing. We’re not in the habit of inquiring into people’s political views.”
PROOF: COVID vaccines cause prion diseases
By Steve Kirsch | November 26, 2021
Twitter suspended my account (likely forever since there is no appeal) due to one post on prion diseases. Here’s the information they wanted to make sure you NEVER find out.
Summary
There is no doubt the mRNA vaccines are causing prion diseases. People didn’t have these diseases before the shot and suddenly they develop them after the shot. There is no other explanation for this. None of the “fact checkers” can explain the cause of the excess rates. Prion diseases are incurable and always fatal. You can die as soon as 6 weeks after COVID vaccination (see within 6 weeks and within 6 months examples).
However, Twitter believes this is not true, but they refuse to tell anyone why they think that. Other fact checkers who have checked this out never did a VAERS query and are unable to explain away the “excess” number of reports other than doing a blanket dismissal that everything in VAERS is fraudulent without providing any evidence of that claim (other than one report out of 1.6M reports).
None of the fact checkers will debate on this to set the record straight.
On November 24, 2021 I posted the following message on Twitter:

Twitter suspended my account hours later. There is no appeal available. All content over the last 12 years was removed. All my 75K followers were zeroed. My messages were removed. There was no opportunity to download my content.
The only thing left: that my Twitter ID was @stkirsch.
Twitter refuses to tell us what I said that was misleading?
Twitter won’t tell me that!!! They are deliberately withholding their definitive analysis on this extremely important scientific issue. Why???
I really want to know. Obviously, Twitter fact-checkers (all of whom I presume must have PhD degrees or MD degrees to be able to assess my claims) were able to quickly read all the medical literature and determine without a doubt I made an error and should be terminated for making a mistake. But they won’t tell me the mistake!!
If they want to fight misinformation, why aren’t they posting a link to their research proving me wrong when they terminate the account. They obviously invested hours of time in the research before they terminated me. Why not provide a link to that research so everyone can learn from it including me??
Here’s the evidence for my claim
Back in May 2021 when Professor Byram Bridle was disclosing the FOIA request on the Pfizer vaccine bio-distribution data he mentioned that the spike protein was associated with Lewy body formation which is linked to prion diseases. He expressed concern that the vaccines could cause prion diseases like dementia, Alzheimer’s, and Creutzfeldt-Jakob disease (CJD).
What do you know. He was right. Now we have proof.
Check out these VAERS query results. These searches are over all 30 years of VAERS and all 70+ vaccines. See anything unusual? Yeah, for less than 1 year of the COVID vaccines, the results are off the charts.

And for CJD which is extremely rare:

Remember, these are 30 year searches for all vaccines. Clearly there are excess reports. And we know VAERS isn’t being “over-reported” this year which I’ve shown many times before (events not caused by the vaccine are reported at rates comparable to other vaccines).
If it wasn’t the COVID vaccines causing this, what was the cause?
Nobody can answer that question, not even the Twitter fact checkers!
For further reading, check out these articles:
- Jessica Rose’s article on COVID vaccines and prion diseases
- Stephanie Seneff’s paper on prion disease and the COVID vaccines
- Bart Classen’s paper linking the vaccines and prion diseases
- SARS-CoV-2 causes brain inflammation and induces Lewy body formation in macaques
- SARS-CoV-2 Prion-Like Domains in Spike Proteins Enable Higher Affinity to ACE2
And compare them to some of the “fact checks” which claim there are no instances in VAERS which as you can see from the queries above (which you can replicate yourself):
You decide who is telling the truth.
And note that the “fact checkers” never did a single VAERS query. Wow. That’s the first place you’d look to prove the claim is false.
Uprising in Guadeloupe

By David Montoute | Fourth World | November 23, 2021
An insurrectional situation has emerged in Guadeloupe. Roads are closed, buildings set on fire, and clashes between demonstrators and security forces are raging. Many Guadeloupeans have decided that, against dictatorship, violence is a legitimate option. It is a violence directed against the so-called ‘health pass’ and against the mandatory vaccination of careworkers imposed upon this overseas territory by Metropolitan France.
In September, France had made it compulsory for all health workers, home carers, transport staff, medical students, firefighters, and all related personnel to have the Covid vaccine. This was accompanied with the requisitioning of all Ivermectin stocks in order to force the deeply unpopular vaccine upon the people of Guadeloupe (as well as neighbouring Martinique). According to French government figures, only 33% of Guadeloupeans are vaccinated (versus 75% in Metropolitan France), with a simiar figure in Martinique.
Tensions rose in October with the arrest of two demonstrators, one of them being Claudine Maraton, the general secretary of the UTS-UGTG (the trade union section of the General Workers Union of Guadeloupe). The UGTG had taken a leading position in the political opposition to the vaccine mandate, a position that the president of the Guadeloupe region also came to echo. As the conflict sharpened, the governing En Marche party’s MP for Guadeloupe began to describe the situation on the island as “quasi-insurrectional”, with opposition to the Covid regulations showing a “weakening state authority” on the island.
The Minister of Health, Olivier Véran seemed to recognise the fragility of France’s position, and decided to push back the deadline for the vaccination mandate to November 15th. But if November 15th marked the end of the ‘health emergency’ measures in most of the overseas territories, in Guadeloupe, it marked the start of an indefinite general strike, launched by a collective of trade union and citizen organisations against the mandatory injection of careworkers and the pass sanitaire. At a press conference at the Palais de la Mutualité in Pointe-à-Pitre, Maïté Hubert M’Toumo, the new General Secretary of the UGTG had already sounded the battle-cry: “From Monday, war is declared!”
“From September, the French state decided to renew hostilities […] all doctors and nurses can receive a notice prohibiting them from working. This means that from Monday, the French state which spoke of war has just declared war on us. The situation is catastrophic. Thousands of workers are affected, whom they want to shamelessly fire, without delay of challenge. We can’t accept that. It’s not possible. The Guadeloupeans are in danger and from the moment war is declared, we are obliged to respond. From Monday, war is declared, there will be nothing that will work, we must organise ourselves so that nothing functions: Monday, Tuesday, Wednesday, Thursday… every day! We have no choice, we must come together, all social and professional classes, all Guadeloupeans. From Monday there will be two camps: the camp of the French state which has decided to defile us and defile all who oppose their plans; and the other side that wants to protect the country in order to live in freedom. The French president said that vaccines are freedom, so freedom is conditioned on a vaccine, a vaccine that is not under control, a vaccine that generates more and more serious side effects. Is this freedom? It’s not possible. So from Monday, war is declared!”
![]()
Maïté Hubert M’Toumo
The Departmental Fire and Rescue Service (SDIS), also affected by the mandatory vaccination order, had come to assume a leading role in the protests. As the strike began on the 15th, fights broke out between firefighters and the elite gendarmes, When the gendarmes charged one group, the firefighters responded with jets of water. Other incidents between strikers and police triggered a wave of arrests as the Pointe-à-Pitre prosecutor’s office complained of “repeated threats to a law enforcement officer.” Maïté Hubert M’Toumo denounced the arrests in a public statement, calling them “a serious attack on a fundamental freedom which is the right to strike” and rallying “all members and activists to strengthen the picket lines”. Even as the government sent in hundreds of police and gendarme reinforcements, the strike hardened on the following weekend, with rioting breaking out in Pointe-à-Pitre and across the Island. Several gas stations were closed by protesters, and many motorists raided those that remained open, fearing the strike would impact fuel supplies. As the demonstrations and clashes escalated, shops and pharmacies were torched and looted, while schools, post offices and courts were shut down. Reports surfaced that protestors had broken into an arms depot in the island’s capital, Pointe-à-Pitre, and stolen rifles. Col Jean Pierre, of the gendarmerie at Pointe-à-Pitre, said some of the protesters had fired upon security forces. “We just don’t know how far this will still go,” the city’s mayor, Harry Durimel, told FranceInfo radio.
This weekend, Paris authorities began sending elite police and counterterrorism officers with armoured vehicles to Guadeloupe in a bid to stamp out the uprising. The police reinforcements set about dismantling protesters’ road barricades while the island’s authorities imposed a dusk-to-dawn curfew until Tuesday morning. By Monday the police had arrested at least 38 people charged with looting and smashing shops.
Over the weekend, the main UGTG trade union called for continued protests. Meanwhile, Martinique has followed its neighbour’s example and gone on general strike against the measures dictated by Paris.
The cultural rejection
Guadeloupe – like Martinique – has a deep-rooted history of anti-vaccine sentiment linked to distrust of the Paris government. Political scientist Pamela Obertan, who is helping to organise anti-mandate protests explains that Guadeloupeans “are descendants of slaves, and for us, control over our bodies is really important… The government wants to impose on us a medical experiment. We are still medical experiments.”
For decades, agriculture workers in Guadeloupe and Martinique were exposed to an endocrine-disrupting, carcinogenic pesticide called chlordecone. Around 95% of the population in these two islands is known to register chlordecone in their blood. Studies have linked the pesticide to prostate cancer, and, significantly, Guadeloupe and Martinique have the highest prostate cancer rates in the world. Yet nothing has been done about real health emergencies such as this one. And this goes a long way to explain the distrust towards the metropolis that is felt in the French Antilles. It is this context that has empowered vaccination-refusal, which is now turning into a nationalist and patriotic cause.
Accompanying this development, there is a longstanding usage and trust in folk medicine. As Guadeloupe’s University Hospital director lamented, the vaccine refusniks are “pushing Guadeloupian pharmacology.” From the start of the aggressive push for ”Covid” vaccination, sales of Virapic, a syrup based on the local jackass bitters herb, skyrocketed. This tropical shrub (Neurolaena lobata) is traditionally used for treatment of fever and flu symptoms, wounds and infections, and a variety of parasitic ailments such as malaria, ringworm, and amoebiasis. The plant has found a local champion in pharmacist Henry Joseph, co-founder of the laboratory Phytobokaz. Joseph, claims to have proven the plant’s efficacy against emerging RNA viruses and thus its relevance to ‘Covid-19′.
Whatever comes of such research, the island’s distrust in vaccines is unlikely to abate any time soon. The metropolitan government’s refusal to negotiate, together with the local suppression of data on vaccine deaths will continue to antagonise an already rebellious populace. According to lawyer Maître Ellen Bessis, the University Hospital Center (CHU) of Guadeloupe never declares vaccination status amongst any hospitalisations. This, she says allows them to register vaccinated deaths in Guadeloupe’s hospitals as unvaccinated, which is what she says is happening. Bessis’ claim is based on the extensive testimony of firefighters who, in Guadeloupe, share the job of transporting emergency cases to hospital. As the civil liberties organisation Rester Libre ! says, “If this information were verified, it would be an absolute scandal: a statistical lie designed to hide the dangerousness of the vaccine. It would create a crisis of absolute confidence with the public authorities, and, therefore, all the figures, all the data, could be called into question.”
It is difficult to imagine how the execrable Macron government could possibly backtrack in this conflict, or provide any concessions for Guadeloupe. For to do so would undermine the mandate policy in metropolitan France. Yet the rebellion of the island population can only deepen, as Ellen Bessis affirms.
“We wonder what is going on in the mind of the government!” says Jocelyn Zou, of the fire department’s union. “We Guadeloupeans have a notion of freedom. But they impose compulsory vaccination on us when alternative solutions exist. We have every motivation to fight to the end!”
France to send special forces to Guadeloupe after looting, arson:
RELATED: Martinique and Guadeloupe: Ivermectin stocks are requisitioned to force vaccination
What is happening in Australia’s Aboriginal communities?
OffGuardian | November 26, 2021
The last few days we have heard some alarming reports about how the Northern Territories of Australia are treating their indigenous communities.
Tweets and videos have emerged claiming aboriginal people are being removed from their land and sent to “quarantine centres”, allegedly to protect them from the virus.
Some representatives of the community have sent out videos asking for “international aid”, and claiming Aboriginal communities are being placed under “martial law” and people are being removed from their homes “at gunpoint”
At a protest against the measures, one aboriginal elder was violently arrested by officers witnesses claim were not wearing ID badges.
Another elder, June Mills, posted a video to facebook expressing concern about how difficult it is to get information out of the locked down communities. She says she has heard that the army is “removing people against their will”, ending with the emotive cry “they are killing us!”
Australia has been so rapidly descending into a fascist hellhole that none of this, if true, would be at all surprising. The very fact they have a huge quarantine camp they unironically refer to as “The Centre for National Resilience” should be a massive red flag for everyone.
Michael Gunner, Chief Minister of the Northern Territories, was a caricature of wide-eyed zealotry in a recent press conference. When asked whether vaccine mandates might alienate some people, even those already vaccinated he said:
If you support or give comfort to anybody who argues against the vaccine, you are an anti-vaxxer, I don’t care what your personal vaccination status is.”
The phrase “give comfort too” should alarm people, because it’s only ever used in warlike settings, discussing treason and collusion. “Giving comfort to the enemy“.
In another press conference, Gunner also announced a “hard lockdown” in aboriginal communities, meaning people are not allowed to leave their homes except for medical treatment or if required by law. Adding that people are being “removed” to quarantine centres in military trucks. Not just people diagnosed with “covid”, but “close contacts” too:
Police are going door to door in Aboriginal communities to “intensively engage” with those who do not want the “vaccine”.
All this is being sold in the mainstream as “concern” for communities which could be “extra vulnerable”.
Voices on social media – who are totally real, and not at all shills there to control the narrative – are claiming strict measures are necessary to protect indigenous Australians from Covid, because it would rip through their communities “like syphilis did to the Native Americans”. There is, so far, very little evidence to support this fear-mongering.
However, written statements, allegedly from people detained, are emerging online saying they are being well taken care of, and that “irresponsible” social media posts are “hurting people”.
Amnesty UK issued a press release condemning the moves, but this was swiftly countermanded by Amnesty Australia, and dismissed as “disinformation” in the press and by Michael Gunner as “conspiracy theorising” from “tinfoil hat-wearing tossers”.
Some other Australian states are already building quarantine camps specifically for Aboriginal communities.
South Australia announced a tender for these camps last week, with press coverage underlining they would be only for those people who are “unable to isolate at home”.
Whether genuinely well-intentioned or not, it can certainly be argued this is an example of massive governmental overreach, especially for a virus that is at worst a bad seasonal flu.
It’s a convoluted and complex situation, with the real facts being hard to establish. Whatever the reality, it’s a situation that bears close watching.
Are We Overreacting to Omicron?
BY PAUL ELIAS ALEXANDER | BROWNSTONE INSTITUTE | NOVEMBER 26, 2021
With natural exposure immunity and early outpatient treatment and when combined with no reports of increased lethality, the WHO’s reaction of generating panic toward “Omicron” is causing needless fear and panic. So too with the Biden administration’s newly imposed travel restrictions, which will achieve nothing and will once again disrupt trade and violate human rights.
The WHO has said that the Omicron variant can spread more quickly than other variants. Likely true. The virus is behaving just like how viruses behave. They are mutable and mutate and via Muller’s ratchet, we expect this to be milder and milder mutations and not more lethal ones given the pathogen seeks to infect the host and not arrive at an evolutionary dead-end.
The virus will mutate downward so that it can use the host (us) to propagate itself via our cellular metabolic machinery. The Delta has shown us this: it is very infectious and mostly non-lethal. Especially for children and healthy people. So is the WHO panicking the globe needlessly? Is this Covid-19 February 2020 once again?
The problem with South Africa as is with Australia and New Zealand and even island nations like Trinidad is that it has low natural immunity to SAR-Cov-2. This is because, as we witnessed over the last year and more, if you lock down your society too long and too hard, you deny the nation and population from inching closer to population-level herd immunity. And you have no economy or society from which to reemerge. You devastate your society for a pathogen that is largely harmless to the vast majority of people especially children.
Moreover, governments asked us for two weeks to flatten the curve to help prepare hospitals so that they can tend to surges and other non-Covid illnesses. We as societies gave our governments 2 weeks, not 21 months. They failed to tend to the non-Covid illnesses and we locked down the healthy and well (children and young and middle aged healthy persons) while failing to properly protect the vulnerable and high-risk persons such as the elderly. We failed and it was like killing fields in our nursing homes.
This failure rests on public health messaging and government. Additionally, what did our governments in the US, Canada, UK, Australia etc. do with the tax money for the hospitals and PPE etc.? Hospitals must be prepared by now. Governments have failed! Not the people. The Task Forces have failed, not the people.
These nations thought that they could stay locked down and wait for a vaccine. This is a reasonable view though I was against lockdowns as they would and did cause crushing harms on especially poor persons and children. The problem is there was an opportunity cost because the vaccine we were waiting on was suboptimally developed without the proper safety testing or assessment of effectiveness.
We have data that the Pfizer vaccine loses 40% of antibodies per month, meaning in 3 months post-shot, you have low effective vaccinal immunity. We see it clearly playing out now whereby you got to tamp down spread with the draconian lockdowns, but you did it at the cost of natural immunity. That is the opportunity cost. So we spent on getting the vaccine and it cost us natural immunity and thus herd immunity.
For example, the vaccine has failed to stop infection and spread against Delta. We have research findings by Singanayagam et al. (fully vaccinated individuals with breakthrough infections have peak viral load similar to unvaccinated cases and can efficiently transmit infection in household settings, including to fully vaccinated contacts), by Chau et al. (viral loads of breakthrough Delta variant infection cases in vaccinated nurses were 251 times higher than those of cases infected with prior strains early 2020), and by Riemersma et al. (no difference in viral loads when comparing unvaccinated individuals to those who have vaccine “breakthrough” infections and if vaccinated individuals become infected with the delta variant, they may be sources of SARS-CoV-2 transmission to others) that reveal the vaccines have very suboptimal efficacy.
This situation of the vaccinated being infectious and transmitting the virus has also emerged in seminal nosocomial outbreak papers by Chau et al. (HCWs in Vietnam), the Finland hospital outbreak (spread among HCWs and patients), and the Israel hospital outbreak (spread among HCWs and patients). These studies have also revealed that the PPE and masking were essentially ineffective within the healthcare setting. All of the HCWs were double-vaccinated yet there was extensive spread to themselves and their patients.
In addition, Nordström et al. (vaccine effectiveness of Pfizer against infection waned progressively from 92% day 15-30 to 47% day 121-180, and from day 211 and onwards no effectiveness), Suthar et al. (a substantial waning of antibody responses and T cell immunity to SARS-CoV-2 and its variants, at 6 months following the second immunization), Yahi et al. (with Delta variant, neutralizing antibodies have a decreased affinity for the spike protein, whereas facilitating antibodies display a strikingly increased affinity), Juthani et al. (higher numbers of patients with severe or critical illness in those who received the Pfizer vaccine), Gazit et al. (SARS-CoV-2-naïve vaccinees had a 13-fold increased risk for breakthrough infection with the Delta variant, and substantially elevated risk of symptomatic Covid and hospitalization), and Acharya et al. (no significant difference in cycle threshold values between vaccinated and unvaccinated, asymptomatic and symptomatic groups infected with Delta) collectively reveal the poor efficacy and even negative efficacy of the Covid vaccines. Levine-Tiefenbrun et al. reports that the viral load reduction effectiveness declines with time after vaccination, “significantly decreasing at 3 months after vaccination and effectively vanishing after about 6 months.”
As an example, the Swedish study (retrospective with 842,974 pairs (N=1,684,958) is particularly alarming for it shows that while the vaccine provides temporary protection against infection, the efficacy declines below zero and then to negative efficacy territory at approximately 7 months, underscoring that the vaccinated are highly susceptible to infection and eventually become highly infected (more so than the unvaccinated). A further example emerges from Ireland whereby reporting suggests that the Waterford city district has the State’s highest rate of Covid-19 infections, while the county also boasts the highest rate of vaccination in the Republic (99.7% vaccinated). Reports are that the U.S. Covid-19 deaths for 2021 surpassed the deaths from 2020, leading some to state that “more people have died from COVID-19 in 2021, with most adults vaccinated and nearly all seniors), than in 2020 when nobody was vaccinated.”
Thus these nations that locked down and stayed that way are in a quandary for they do not know what to do now. If you open you will get surges in infection. Where is the money that was to go to hospital preparation? Did governments embezzle and steal and misappropriate the money for the hospitals remain still not prepared?
We have a lot of natural immunity in the US, e.g. near 65-70% of the population. The open states (those that did not lock down too long and too hard and opened quickly) will likely do very well with this Omicron or any new variant. This also is the power of natural immunity.
And we need not forget the potency of the overlooked ‘innate’ immunity with the innate antibodies and innate natural killer cellular compartment. This innate response is particularly potent in children (our first line of defense against pathogens) and is what has spared children from Covid and how children typically stave off pathogens, especially young children still laying down immunological memory.
Moreover, there is no reporting of increased virulence/lethality of this new Omicron variant. As yet this will remain the case based on Delta and prior variants. There are no guarantees but we operate based on risk and all things point to the same for this new variant.
Just because there is a wave in SA does not mean that there will be waves in the US or Israel or other places with greater natural immunity. This was the prize of letting people enjoy day-to-day living. The nations that have ended lockdowns are likely to move past this new variant scare, and be fine. This is more of an overreaction by the WHO and governments and much ado about nothing.
Dr Alexander holds a PhD. He has experience in epidemiology and in the teaching clinical epidemiology, evidence-based medicine, and research methodology. Dr Alexander is a former Assistant Professor at McMaster University in evidence-based medicine and research methods; former COVID Pandemic evidence-synthesis consultant advisor to WHO-PAHO Washington, DC (2020) and former senior advisor to COVID Pandemic policy in Health and Human Services (HHS) Washington, DC (A Secretary), US government; worked/appointed in 2008 at WHO as a regional specialist/epidemiologist in Europe’s Regional office Denmark, worked for the government of Canada as an epidemiologist for 12 years, appointed as the Canadian in-field epidemiologist (2002-2004) as part of an international CIDA funded, Health Canada executed project on TB/HIV co-infection and MDR-TB control (involving India, Pakistan, Nepal, Sri Lanka, Bangladesh, Bhutan, Maldives, Afghanistan, posted to Kathmandu); employed from 2017 to 2019 at Infectious Diseases Society of America (IDSA) Virginia USA as the evidence synthesis meta-analysis systematic review guideline development trainer; currently a COVID-19 consultant researcher in the US-C19 research group
With Low Vaccination Rates, Africa’s Covid Deaths Remain Far below Europe and the US
By Ryan McMaken | MISES WIRE | November 23, 2021
 Since the very beginning of the covid panic, the narrative has been this: implement severe lockdowns or your population will experience a bloodbath. Morgues will be overwhelmed, the death total toll will be astounding. On the other hand, we were assured those jurisdictions that do lock down would see only a fraction of the death toll.
Since the very beginning of the covid panic, the narrative has been this: implement severe lockdowns or your population will experience a bloodbath. Morgues will be overwhelmed, the death total toll will be astounding. On the other hand, we were assured those jurisdictions that do lock down would see only a fraction of the death toll.
Then, once vaccines became available, the narrative was modified to “Get shots in arms and then covid will stop spreading. Those countries without vaccines, on the other hand, will continue to face mass casualties.”
The lockdown narrative, of course, has already been thoroughly overturned. Jurisdictions that did not lock down or adopted only weak and short lockdowns ended up with covid death tolls that were either similar to—or even better than—death tolls in countries that adopted draconian lockdowns. Lockdown advocates said locked-down countries would be overwhelmingly better off. These people were clearly wrong.
Undaunted by the increasing implausibility of the lockdown narrative, the global health bureaucrats are nonetheless doubling down on forced vaccines—as we now see in Austria—and we continue to be assured that only countries with high vaccination rates can hope to avoid disastrous covid outcomes.
Yet, the experience in sub-Saharan Africa calls both these narratives into question: Africa’s numbers have been far, far lower than the experts warned would be the case.
For example, the AP reported this week that in spite of low vaccination rates, Africa has fared better than most of the world:
[T]here is something “mysterious” going on in Africa that is puzzling scientists, said Wafaa El-Sadr, chair of global health at Columbia University. “Africa doesn’t have the vaccines and the resources to fight COVID-19 that they have in Europe and the U.S., but somehow they seem to be doing better,” she said….
Fewer than 6% of people in Africa are vaccinated. For months, the WHO has described Africa as “one of the least affected regions in the world” in its weekly pandemic reports.
Yet disaster for Africa has long been predicted for several reasons even beyond the availability of vaccines. For instance, it is known that lockdowns are especially impractical in the poorest parts of the world. This is because populations in places with undeveloped economies can’t simply sit at home and live off savings or debt. Rather, these people must go out into the world and earn a living on a day-to-day basis. Starvation is the alternative. Moreover, much of this work is done in the informal economy, so enforcing lockdowns becomes especially difficult.

Source: Our World in Data (Confirmed Deaths per Million, November 19, 2021; Share of People Vaccinated against Covid-19, November 19, 2021).
It was also assumed covid would be especially deadly in Africa due to the fact many large households live in small housing units.
But that “conventional wisdom” flies in the face of the reality of covid in Africa, which is that there have been fewer deaths.
The “experts” have groped around, looking for possible explanations.
Some sources, for example, insist that the low death totals are only an artifact of incomplete reporting on covid infections and that “a lack of good qualitative data was the issue.”
But Richard Wamai at Northeastern University rejects the claim it’s all about case reporting, and says that “local systems for reporting deaths in Africa make it difficult to hide COVID-19 casualties.” In a paper for the International Journal of Environmental Research and Public Health, Wamai and his coauthors conclude, “[T]here is no evidence that COVID-19 mortality data is less accurately reported in Africa than elsewhere” and “While the true picture of infections and mortality in the continent has yet to fully emerge, the quality of data for other diseases, such as HIV/AIDS, indicates that Africa has the capacity to collect and report valid disease surveillance data.”
In any case, the World Health Organization reports that covid deaths in Africa make up only 2.9 percent of covid deaths, while Africa’s population is 16 percent of the global total. Africa’s covid total could double or triple, and Africa would still be faring far better than Europe and the Americas.
Wamai et al. also note that at this point “[i]t is likely that SARS-CoV-2 has already been widely disseminated through Africa… If so, widespread infection is likely to also result in widespread natural immunity.”
In other words, continued claims by health officials—both in Africa and elsewhere—that mass death is right around the corner with the “next wave” look increasingly implausible.
It looks increasingly likely that the lack of covid mortality in Africa is not due to a data issue nor a situation in which covid has been “contained” up until now. So then why is Africa doing so much better than the wealthy West?
Naturally, the advocates of forced lockdowns and coerced vaccines would prefer to ignore this issue altogether, but the undeniable reality of Africa’s experience has forced mainstream researchers to publicly admit the many ways that many factors can explain covid’s prevalence beyond vaccination rates and mask mandates.
For instance, mentioning that obesity is an important factor in covid mortality has in the past been likely to get one savaged in the media for “fat shaming.” Yet the Africa situation has forced the well informed to admit that yes, obese populations clearly suffer more from covid. In Africa, not surprisingly, we find that obesity rates are far below those found in North America and Europe.
Other possible explanations forwarded as reasons for Africa’s situation include past exposure to other coronaviruses, youthful populations, fewer patients lacking zinc and vitamin D, past use of the Bacillus Calmette-Guérin vaccination, climate, genetic background, and parasite load. In addressing the African “enigma” one group of researchers in the journal Colombia medica dared even suggest it’s possible—although not conclusively shown at this point—that “a mass public health preventive campaign against COVID-19 may have taken place, inadvertently, in some African countries with massive community ivermectin use.”

Source: “Global Obesity Levels,” ProCon.org, last modified March 27, 2020; Our World in Data (Share of People Vaccinated against Covid-19, November 19, 2021).
In the West, however, the media drumbeat around covid has consistently been “Shut up, stay home, get jabbed, and stop doubting the experts on forced vaccines.” Fortunately, however, the African situation has forced many researchers to ask inconvenient questions.
In fact, it’s amazing Africa has not been overcome by mass death considering that covid lockdowns and covid “mitigation” measures have contributed to the impoverishment and mass starvation on the continent. Or as Germany’s DW News puts it, “Measures put in place to slow the spread of the novel coronavirus are pushing millions of people in Africa into severe hunger.” And as Wamai notes, “[S]ome of the excess deaths in Africa “can be attributed not to the disease, but to lockdown measures that cut off access to medical care for other illnesses.”
But Africa hasn’t gotten the bloodbath that was promised, and as one Nigerian put it, “They said there will be dead bodies on the streets and all that, but nothing like that happened.”
Featured Video

Fear Is the Mind Killer
or go to
Aletho News Archives – Video-Images
From the Archives
Infertility: A Diabolical Agenda
Dr. Joseph Mercola | July 9, 2022
“Infertility: A Diabolical Agenda,” is the fourth vaccine-related documentary by Dr. Andrew Wakefield. It tells the story of an intentional infertility vaccine program conducted on African women, without their knowledge or consent.
While it’s been brushed off as a loony conspiracy theory for years, there’s compelling evidence showing it did, in fact, happen, and there’s nothing to prevent it from happening again. … continue
Blog Roll
 Aletho News
Aletho News- Israeli strikes kill 10 in southern Lebanon, including 3 rescue workers
- Israeli military ‘failed on all fronts’: Poll
- US at a crossroads: Iran’s firm positions leave Trump no option but to capitulate
- Iran signals decisive response to end US maritime bullying, piracy
- Trump eager for off-ramp in war on Iran, but Netanyahu has him trapped: Former official
- Trump’s ‘Golden Dome’ offers ‘limited’ shield against ballistic missiles: Defense official
- Ukraine Seeks to Provoke a Nuclear Conflict: Zakharova
- US squares up to China over Panama Canal
- Monroe Doctrine 2.0: ‘Great Reset’ for US Imperialism?
- Nuclear Apartheid: Iran’s Rise Exposes the NPT Fraud and the West’s Israel Exception
- If Americans Knew
- How Tony Dokoupil Became the Face of ‘Zionist Fanatic’ Bari Weiss’s CBS
- Far Right Israeli Settler Movement Enters Syria in a Push for “Greater Israel”
- ‘People Have the Right to Be Buried’: In Gaza, Thousands of Palestinians Remain Trapped Under Rubble
- Born during Israel’s genocide: Gaza’s child survivors bear the scars of war
- Who are the women and girls behind Gaza war’s horrific casualty toll?
- Beloved Gaza doctor detained “indefinitely” without charge – Daily Update
- By Week’s End, Trump’s War Will Be Plainly Illegal
- CBS News Reportedly Ousts London Bureau Chief Over Differences With Bari Weiss Over Gaza Coverage
- State Department Says US Is in Conflict With Iran ‘At the Request’ of Israel
- What ceasefire? Israel won’t stop killing in Gaza, Lebanon – Daily Update
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
