Data released Sept. 17 by the Centers for Disease Control and Prevention (CDC) showed that between Dec. 14, 2020 and Sept. 17, 2021, a total of 726,965 adverse events following COVID vaccines were reported to the Vaccine Adverse Event Reporting System (VAERS). The data included a total of 15,386 reports of deaths — an increase of 461 over the previous week.
There were 99,410 reports of serious injuries, including deaths, during the same time period — up 7,887 compared with the previous week.
Of the 6,981 U.S. deaths reported as of Sept. 17, 12% occurred within 24 hours of vaccination, 17% occurred within 48 hours of vaccination and 30% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 383.6 million COVID vaccine doses had been administered as of Sept. 17. This includes: 220 million doses of Pfizer, 149 million doses of Moderna and 15 million doses of Johnson & Johnson (J&J).
The data come directly from reports submitted to VAERS, the primary government-funded system for reporting adverse vaccine reactions in the U.S.
Every Friday, VAERS makes public all vaccine injury reports received as of a specified date, usually about a week prior to the release date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed.
This week’s U.S. data for 12- to 17-year-olds show:
The most recent deaths involve a 17-year old male (VAERS I.D. 1689212) with cancer who was vaccinated April 17, tested positive for COVID on July 20, was hospitalized and passed away Aug. 29; and a 16-year old female (VAERS I.D. 1694568) who died from a pulmonary embolism nine days after receiving her first Pfizer dose.
Other recent reported deaths include two patients [VAERS I.D. 1655100] who died after their second dose of Pfizer, including a 13-year old female, a 15-year-old boy (VAERS I.D. 1498080) who previously had COVID, was diagnosed with cardiomyopathy in May 2021 and died four days after receiving his second dose of Pfizer’s vaccine when he collapsed on the soccer field and went into ventricular tachycardia; and a 13-year-old girl (VAERS I.D. 1505250) who died after suffering a heart condition after receiving her first dose of Pfizer.
This flew under the radar at the time, but it’s important to shine a light on it now.
Back on August 27, 2021, the World Health Organization (WHO) quietly published a detailed directive which instructs governments around the world how to standardise and implement the digital segregation system which they are calling a ‘digital COVID-19 certificate’ aka vaccine passport, immunity passport, health pass, green pass, or digital wallet (as the EU has since renamed it).
By positioning itself in this way, the WHO has elevated itself to de facto global government status, with little or no interest in the democratic processes of individual sovereign nations and their people. Instead, they are simply pushing forward with their own globalist agenda – clearly run on behalf of the transnational pharmaceutical cartel – in concert with a cadre of billionaire elites (led by the Bill & Melinda Gates Foundation which funds the WHO to the tune of $265 million per annum) and another key unelected non-state actor, the World Economic Forum (WEF) in Davos, Switzerland.
It clearly states its primary function in guiding governments:
“The primary target audience of this document is national authorities tasked with creating or overseeing the development of a digital vaccination certificate solution for COVID-19. The document may also be useful to government partners such as local businesses, international organizations, non- governmental organizations and trade associations, that may be required to support Member States in developing or deploying a DDCC:VS solution.”
The following is taken directly from the WHO’s own website:
Digital documentation of COVID-19 certificates: vaccination status: technical specifications and implementation guidance, 27 August 2021
Overview
This is a guidance document for countries and implementing partners on the technical requirements for developing digital information systems for issuing standards-based interoperable WHO-2019-nCoV-Digital-certificates-vaccination-2021.1-eng digital certificates for COVID-19 vaccination status, and considerations for implementation of such systems, for the purposes of continuity of care, and proof of vaccination.
The Czech Republic’s vaccine roll-out has hit a wall.
It appears that state agencies are experiencing an increasingly low demand for jabs being recommended to over 60 year-olds due to multiple reports concerning possible side effects from the vaccine.
In September, only 36 new applicants came for AstraZeneca.
Irozhlasreports how the government is now dumping hundreds of thousands of doses overseas in Asia (translated):
In recent weeks, the Czechia has directly donated over 200,000 doses of AstraZenec to Asia, hundreds of thousands more vaccines have been released by the state to other countries since the summer, and these orders will not even reach the Czech Republic.
Those jabs which they can’t give away are heading for the incinerator:
Burned: 20,650. So far, this is the September account of AstraZeneca’s coronavirus vaccines …. the state must dispose of vaccines en masse. It is said that they cannot donate anymore. Tens of thousands more doses expire in October. Most of the state is likely to burn again.
At the turn of October and November, the incinerators will have their work taken care of. Another 55,000 batches, which are in stock by the distribution company Avenier and which are distributed in warehouses and pharmacies, will go.
Problems with the vaccine agenda in eastern Europe are a source of concern for Brussels as it hopes to implement its digital segregation system system commonly referred to as Vaccine Passports but codified in EU policy as a more harmless sounding “Digital Wallet.”
Last Friday, FDA’s advisory committee (VRBPAC) voted 16 to 2 against giving a license to a third Pfizer booster shot for everyone age 16 and up.
Although a second vote at Friday’s meeting had not been planned, another question was hastily developed. That question asked whether the vaccine could be licensed for a third booster dose for high risk people under the age of 65. That vote got a unanimous yes.
The panels decisions are not final. The FDA is obliged to take the panels advice into consideration, but it is not required to adopt it. So yesterday, the FDA issued a license for the Pfizer vaccine for the booster dose.
“individuals 18 through 64 years of age whose frequent institutional or occupational exposure to SARS-CoV-2 puts them at high risk of serious complications of COVID-19 including severe COVID-19.”
This is what I call weasel wording. This statement does not make sense. People whose occupation puts them at high risk of exposure to COVID are no more likely to be at high risk of serious complications or severe COVID-19 than anyone else. They are at higher risk of developing COVID, but not at higher risk of serious COVID.
What FDA did (and you know who did this: Peter Marks, head of CBER and Janet Woodcock, acting Commissioner, are the only people with the authority to come up with this BS) was to take the VRBPAC approval for people with underlying conditions that put them at high risk for severe COVID, and twist it into an approval for all health care workers, staff at schools and colleges, grocery store workers, big box employees, etc.
Why? Because a license is necessary to impose a mandate, that’s why.
It looked like the weasels had won again. However, there was a small hoop left to jump through before any mandates came down.
While FDA determines how a drug or vaccine should be licensed or authorized for use, the CDC’s ACIP committee is the group responsible for creating the recommendations for use of the vaccine in different demographic groups.
And so ACIP did what it never does. It rejected the CDC’s proposal to widen the license for the third dose to all with potential occupational exposures. the ACIP limited their approval to what the FDA advisory committee had voted for last Friday. As CNBC noted,
… Dr. Leana Wen [member of the Council on Foreign Relations and the World Economic Forum], an emergency physician and former Baltimore health commissioner, on Twitter called the CDC panel’s vote to reject boosters more widely a “mistake.”
“Really, we are not allowing healthcare workers, many of whom got vaccinated in back in December, to get a booster? What about teachers in cramped classrooms where masks aren’t required?” she tweeted, adding CDC Director Dr. Rochelle Walensky should overrule the recommendation.
… In a paper published days before an FDA advisory meeting last week, a leading group of scientists said available data showed vaccine protection against severe disease persists, even as the effectiveness against mild disease wanes over time. The authors, including two high-ranking FDA officials and multiple scientists from the World Health Organization, contended in the medical journal The Lancet that widely distributing booster shots to the general public is not appropriate at this time.
I think 2 things happened. The propaganda that the vaccines still prevent serious disease while perhaps not preventing mild disease stood in the way of approving boosters to prevent mild disease. Why give a potentially dangerous booster to prevent a cold? It doesn’t make sense.
Second, everyone on those committees knew that if the vaccine’s third dose did get approved for a huge swath of the general public, it would be mandated for themselves in no time. A third dose would have been required for every member of both FDA’s and CDC’s advisory committees. I don’t think they were ready for that. And maybe they weren’t ready for the resistance from those who took the 2 shots thinking they were done… and now, it seems they could get into a situation where they could be fired for not having a third dose. What about more and more doses?
Or maybe the large demonstrations in Australia and Europe were influencing those advisory committee members…
The Winter 2021 “AMA COVID-19 Guide: Background/Messaging on Vaccines, Vaccine Clinical Trials & Combatting Vaccine Misinformation,”1 issued by the American Medical Association (AMA) raises serious questions about the AMA’s adherence to transparency, honesty, ethics and the moral standards to which it will hold its members.
The AMA was founded in 1847 and is the largest professional association and lobbying group of physicians and medical students in the U.S. According to the AMA itself, its mission is to promote the art and science of medicine and the betterment of public health.
How then do they explain this “COVID-19 messaging guide,” which explicitly teaches doctors how to deceive their patients and the media when asked tough questions about COVID-19, treatment options and COVID shots?
AMA Teaches Doctors How to Deceive
“It is critical that physicians and patients have confidence in the safety and efficacy of COVID-19 vaccines as they become available for public use,” the “AMA COVID-19 Guide” states, adding:2
“To overcome vaccine hesitancy and ensure widespread vaccine acceptance among all demographic groups, physicians and the broader public health community must continue working to build trust in vaccine safety and efficacy, especially in marginalized and minoritized communities with historically well-founded mistrust in medical institutions.”
Indeed, the entire guide is aimed at teaching doctors how to foster confidence in the medical profession in general, as it pertains to treatment of COVID-19, but in particular as it pertains to the experimental COVID shots.
The guide provides “suggested narratives” for various engagements, such as when communicating on social media, as well as “talking points to guide external communications,” such as when being interviewed. It lists nine specific “key messages” that they want doctors to focus on when communicating about COVID-19. These key messages can be summarized as follows:
Express confidence in vaccine development
Stress the importance of vaccines
Highlight the need to combat the spread of vaccine misinformation
Adhere to updated ethical guidance for physicians and medical personnel, which says they have a moral obligation to get vaccinated themselves
Give general vaccine recommendations, such as the recommendation for everyone over the age of 6 months, including pregnant women, to get an annual flu shot
Stress the importance of eliminating nonmedical vaccine exemptions
Highlight the increased availability of flu vaccines, and the importance of getting a flu shot even if you’ve gotten a COVID injection
Highlight the importance of including minorities, both in vaccine trials and as trusted messengers who can “promote social pressure” to get minorities vaccinated and dispel historical distrust in medical institutions
Denounce scientific analyses “predicated on personal opinions, anecdote and political ideologies”
AMA Concerned About Disinformation
On page 7 of the guide, under the science narrative heading, the AMA declares it is “deeply concerned that rampant disinformation and the politicization of health issues are eroding public confidence in science and undermining trust in physicians and medical institutions,” adding that “Science should be grounded in a common understanding of facts and evidence and able to empower people to make informed decisions about their health.”3
To that end, the AMA is calling upon “all elected officials to affirm science and fact in their words and actions,” and for media to “be vigilant in communicating factual information” and to “challenge those who chose to trade in misinformation.”
AMA Then Instructs Doctors on How to Disinform
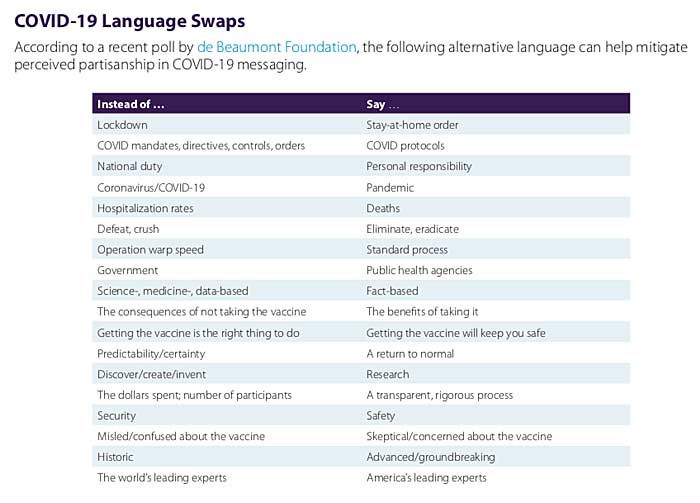
It’s a disappointment, then, to find the AMA instructing doctors on how to misinform the public using a variety of psychological and linguistic tools. Perhaps one of the most egregious examples of this is the recommended “COVID-19 language swaps” detailed on page 9.
As you can see below, the AMA explicitly instructs doctors to swap out certain words and terms for other, more narrative-affirming choices. Shockingly, this includes swapping “hospitalization rates” to “deaths” — two terms that are not even remotely interchangeable!
Another highly questionable word swap is to not address the nitty, gritty details of vaccine trials, such as the number of participants, and instead simply refer to these trials as having gone through “a transparent, rigorous process.”
Swapping the factual term “Operation Warp Speed” for “standard process” is another outrageous misdirection. The two simply aren’t interchangeable. In fact, they’re actually diametrically opposed to one another. Standard process for vaccine development includes a long process of over a decade and a large number of steps that were either omitted or drastically shortened for the COVID shots.
Following standard process is what makes vaccine development take, on average, 10 years and often longer. Operation Warp Speed allowed vaccine makers to slap together these COVID shots in about nine months from start to finish. You cannot possibly say that the two terms describe an identical process.
The Power of Language
Other language swaps are less incredible but still highlight the fact that the AMA wants its members to help push a very specific and one-sided narrative that makes power-grabbing overreaches and totalitarian tactics sound less bad than they actually are, and make questionable processes sound A-OK.
Language is a powerful tool with which we shape reality,4 because it shapes how we think about things. As noted by storyteller and filmmaker Jason Silva:5
“The use of language, the words you use to describe reality, can in fact engender reality, can disclose reality. Words are generative… We create and perceive our reality through language. We think reality into existence through linguistic construction in real-time.”
For example, “lockdown” sounds like involuntary imprisonment imposed by a totalitarian regime, which is what it is, whereas “stay-at-home order” sounds far less draconian. After all, “home” is typically associated with comfort and safety.
The same goes for using “COVID protocols” in lieu of “COVID mandates, directives, controls and orders.” “Protocols” sounds like something that is standard procedure, as if the COVID measures are nothing new, whereas “mandates, controls and orders” imply that, indeed, we’re in medical fascism territory, which we are.
How to Steer, Block, Deflect and Stall Inconvenient Questions
The AMA could have instructed its members to simply stick to the facts and be honest — and in some sections, it does do that — but it doesn’t end there. Rather, the AMA provides a full page of instructions on how to steer the conversation, and how to block, deflect and stall when faced with tough questions where an honest answer might actually break the official narrative.
Here’s a sampling of these instructions. I encourage you to read through page 8 of the guide, and pay attention to these psychological tricks when listening to interviews or reading the news.
Interviewing techniques
Steer the conversation back to the narrative by saying: “Before we leave that matter, let me add …”
Block a tough question by saying: “That’s [proprietary, confidential etc], but what I can tell you is …”
Deflect an unwanted question by saying: “That’s a common misperception but the reality is …”
Redirect away from an unwanted question, back to the official narrative by saying: “I don’t have the details on that, but what I know is …”
Stall by saying: Repeat the question asked, or acknowledge the question by saying, “I’m glad you asked …”
It’s worth noting that the AMA also stresses that: 1) Doctors are to speak for the AMA, and 2) doctors are NOT to offer their personal views. Speaking for the AMA is listed under “Your Responsibilities” when being interviewed, while not discussing personal views is listed under “Interview Don’ts.”
AMA Is Rapidly Eroding All Credibility
The AMA’s guidance isn’t all bad. Some of its advice makes perfect sense. But the inclusion of language swaps that result in false statements being made, and tools for steering, blocking, deflecting, redirecting and stalling in order to avoid direct answers do nothing but erode credibility and thus trust in the medical community.
Its direct instruction to not share personal views is another trust-eroding strategy. When people talk to their doctor, they want to hear what that doctor actually thinks, based on their own knowledge and experience.
They don’t expect their doctor — or a doctor appearing in an interview — to simply rehash a narrative dictated by the AMA. If we cannot trust our medical professionals to give their honest opinions and give direct answers, there’s little reason to even discuss our concerns with them, and that’s the opposite of what the AMA claims it seeks to achieve.
The AMA is concerned about the proliferation of misinformation and eroding trust, yet it’s telling its members to keep their professional views to themselves and lie about COVID deaths. With this guidance document, the AMA is essentially implicating itself as a source and instigator of medical misinformation that ultimately might injure patients.
In a Stew Peters Show interview (see bitchute), Dr. Bryan Ardis criticized the AMA guidance document, pointing out that while the AMA claims it put out the guidance to prevent political ideologies from dictating medicine, it is actually proving that the AMA itself is deferring to political ideology rather than medical facts.
The AMA wants its members to act as propagandists for a particular narrative — using “politically correct language” — rather than sharing information and acting in accordance with their own conscience and professional insight. As noted by Peters:
“If a doctor’s just going to repeat what the AMA tells them, why have doctors at all? You can get plenty of starving propagandists at any liberal college, but instead we want to turn our medical professionals into ideological zombies with stethoscopes.”
However, even if one restricts oneself to the narrow confines of the health narrative, 18 months of data — emerging in spite of ferocious censorship — have repeatedly illustrated that the official story is full of lies and omissions.
With this level of damage after just nine months, now is as good a time as any to reexamine “COVID math” and highlight some of the embedded falsehoods that cast serious doubt on official and corporate pronouncements about risks and benefits.
The false case for vaccinating kids
Pfizer’s CEO, veterinarian Albert Bourla, is currently drumming up buzz in anticipation of a likely decision by the U.S. Food and Drug Administration (FDA) to green-light emergency use of his company’s COVID vaccine in children ages 5-11. To buttress his arguments, Bourla claims that pediatric COVID cases are on the rise.
However, setting aside the questionable PCR testing methodology being used to identify these “cases” (that is, until the Centers for Disease Control and Prevention (CDC) retires the PCR test at the end of the year), recent studies show reported COVID-19 hospitalizations — “one of the primary metrics for tracking the severity of the coronavirus pandemic” — have been grossly inflated for children. In actuality, pediatric COVID hospitalization rates are “vanishingly small.”
One fact, especially, bears repeating: Through age 19, children and adolescents have a 99.9973% COVID-19 survival rate. This information, which has been a constant throughout the reported pandemic, is reiterated in the most recent analyses by Stanford physician, epidemiologist and statistician John Ioannidis, who has been a steadfast critic of COVID alarmism from the very beginning.
And Ioannidis’s good news does not stop with the 19-and-unders. Until people hit their seventies, all age groups have survival rates well over 99%:
0-19: 99.9973%
20-29: 99.986%
30-39: 99.969%
40-49: 99.918%
50-59: 99.73%
60-69: 99.41%
70+: 97.6% (non-institutionalized)
70+: 94.5% (institutionalized and non-institutionalized)
As Off-Guardian’s Kit Knightly wrote about another Ioannidis study this past spring, “With every new study, with every new paper, the ‘deadly’ pandemic gets less and less, well, deadly.”
At that time, Ioannidis ascertained that the global infection fatality rate was 95% lower than the one disseminated by the World Health Organization (WHO).
Risks: the example of myocarditis
Commenting on the pediatric hospital studies — in which more than half of the children entered the hospital for reasons having nothing to do with anything resembling COVID — a reporter wrote, “The implications … are enormously important, as reports of pediatric hospitalizations have regularly made headlines over the past year, greatly affecting public perceptions about risks to children.”
Those headlines and perceptions likely will prompt some parents to rush into the waiting arms of their local vaccinator.
Bourla and other Pfizer executives have remained mum about the many 12- to 17-year-olds who are ending up hospitalized and injured after taking the company’s experimental mRNA product.
Sadly, the post-jab statements made by these disabled teens and their parents share a common refrain: influenced by skewed media reports from some corners, and without the benefit of information censored in other corners, they were not aware of the risks.
What are some of those risks?
A study out of Ottawa recently estimated that one of every 625 Moderna doses administered results in myocarditis (heart inflammation), as does an estimated one in 2,500 doses of the Pfizer shot, with a “tight temporal association between receipt of mRNA vaccine and subsequent development of symptoms in a relatively short time frame afterwards.”
The Ottawa authors pointed out that their estimates — based on “direct investigation of patients” who were “largely in the vulnerable 18- 30 age category” — were tenfold higher than the incidence produced by a less rigorous study that looked only at “administrative health data.”
The authors also noted the relevance of their findings for the “ongoing public debate regarding proposals for vaccination of children under the age of 16.”
According to another new study, healthy boys between the ages of 12 and 15, with no underlying medical conditions, were four to six times more likely to be diagnosed with vaccine-related myocarditis than they were to be hospitalized with COVID.
The Ottawa study may have pointed more of a finger at the Moderna shot, but a late August CDC update on heart problems reported to the Vaccine Adverse Event Reporting System (VAERS) in the aftermath of COVID vaccination suggests the Pfizer injection may be equally treacherous, especially for young men.
Using a statistically credible estimate that VAERS data are underreporting COVID injuries by a factor of 41, Steve Kirsch (founder of the COVID-19 Early Treatment Fund) has calculated (slide #15) that roughly one in 318 boys ages 16 and 17 can be expected to develop myocarditis after two Pfizer doses, and a third booster dose of the Pfizer vaccine could escalate that risk to a frightening one in 25.
Another recent look at VAERS data by Health Impact News showed that in 2021, to date, 12- to 19-year-olds have been 50 times more likely to experience heart problems after receiving experimental COVID shots — and nearly eight times more likely to die — compared to all other FDA-approved vaccines combined.
Considering adverse events reported to VAERS over the past decade for all vaccines combined, there has been a “highly anomalous” 1,000% increase in total adverse events reported thus far for 2021.
With these kinds of findings, the pushback against giving children the shots is growing louder and stronger.
The authors of a just-published study in Toxicology Reports openly ask, “Why are we vaccinating children against COVID-19?” They warn that younger age groups could experience longer-term effects (such as myocarditis) “that, if serious, would be borne by children/adolescents for potentially decades.”
John Ioannidis’s new study shows that institutionalization negatively skews outcomes for the 70-plus age group. Whereas the survival rate is 97.5% for the community-dwelling elderly 70 or older, it falls to 94.5% when institutionalized elderly in that age group are included in the count.
Why are the institutionalized elderly faring so poorly? In the UK, reporters and undertakers have furnished one possible answer, sharing troubling on-the-ground descriptions about illegal euthanasia alleged to be taking place on a widespread basis in care homes as well as hospitals.
In the U.S., meanwhile, regulators, hospitals and pharmacies have implemented equally disturbing policies that require withholding inexpensive drugs, such as ivermectin and hydroxychloroquine — shown elsewhere to be effective and safe — while essentially forcing hospitalized COVID patients onto protocols that are not only unhelpful but murderous.
Mexico City achieved up to a 76% reduction in COVID hospitalizations by making ivermectin-based home treatment kits widely available. With evidence like this, why are U.S. hospitals stubbornly adhering to life-threatening protocols involving remdesivir (known to produce fluid in the lungs and longer hospital stays) and intubation?
One rather dark answer is that hospitals are not only immune from liability for any fatal outcomes resulting from this approach but receive hefty federal payments — including a 20% Medicare “add-on” that may sum up to as much as $40,000 for patients who spend four or more days on a ventilator.
Although hospitals may hasten to refute that these factors are at play, the growing number of hospital whistleblowers is becoming hard to ignore.
In March, Baylor University’s Dr. Peter McCullough lamented that as many as 85% of COVID deaths could have been prevented with early treatment using ivermectin and other formerly commonplace drugs disallowed by regulators and for which U.S. pharmacies will no longer fill “off-label” prescriptions.
There is international agreement with McCullough’s position that “large reductions in COVID-19 deaths are possible using ivermectin,” and the U.S.-based Front Line COVID-19 Critical Care (FLCCC) Alliance describes the drug as potentially the “global solution to the pandemic.”
However, instead of applauding these advocates of early intervention for their efforts to save lives, they have become, according to mRNA vaccine inventor Dr. Robert Malone, the focus of intense “coordinated strategies” to subject them to “derision and attacks and character assassination.”
Those ‘anomalous’ deaths
In analyses presented by Steve Kirsch to the FDA (slide #6), Kirsch summarized data showing the COVID vaccines are killing more people than they are saving — including producing six excess deaths for each life reportedly saved in nursing home residents, and five excess deaths per life saved according to Pfizer’s early clinical trial data.
In February, studies out of Israel were already showing the Pfizer shot (the only one used in Israel) was causing “mortality hundreds of times greater in young people compared to mortality from coronavirus without the vaccine, and dozens of times more in the elderly.”
Investigative journalist Corey Lynn of Corey’s Digs pointed out the CDC’s methodology for calculating COVID vaccine-related deaths is highly misleading because it is based on the number of doses administered, rather than on the number of people who receive injections.
Lynn’s analysis shows this methodology reduces the percentage of deaths almost by half, “an incredible mathematical error, surely done with intention.”
Another CDC ploy for undercounting the damage done by the COVID injections has to do with the agency’s definition of “fully vaccinated. The CDC currently considers as “unvaccinated” anyone who is not two weeks out from their second dose (in a two-dose series) or two weeks out from a single-dose vaccine. (And as Children’s Health Defense President Mary Holland recently pointed out, “unvaccinated” could “soon mean anyone who’s missing the latest booster dose,” with even more boosters likely in store down the road.)
Given that 17% of the deaths reported to VAERS have occurred within 48 hours of COVID vaccination, it is clear many U.S. vaccine deaths are being counted as “unvaccinated” deaths and misattributed to COVID-19 or other causes.
In the UK, however, public health data show that 80% of “COVID-19” deaths in August were in people who had been vaccinated, and hospitalization rates were 70% higher in the vaccinated than in the unvaccinated.
Increasingly, members of the public are not fooled by the statistical shenanigans. When a Detroit TV channel recently tried to drum up hostility against the unvaccinated by asking viewers to submit tales of recalcitrant uninjected relatives dying from COVID-19, they instead got more than 182,000 comments about loved ones who had died or been injured after receiving one or more COVID shots.
These replies provide compelling evidence that what we are now experiencing is a “pandemic of the vaccinated.”
New York’s first female governor Kathy Hochul, who took the reins in the Empire State after her predecessor and former boss, Andrew Cuomo, finally resigned, is showing the state’s recalcitrant healthcare workers just how understanding and progressive she can be.
During a press briefing with reporters in Rochester Wednesday, Hochul told a group of reporters that she hoped all unvaccinated workers would meet Monday’s deadline to get the jab, or lose their jobs.
For those who continue to resist – including nearly 20% of the state’s hospital and nursing-home workers – they will be replaced. Possibly by foreign workers.
Faced with this, it makes sense to wonder how NY State, which has no immigration-related authority, could even credibly make such a threat? But Hochul says there have been conversations with the Department of State (albeit on a “limited basis”) about the possibility of doling out emergency visas to foreign workers.
“To those who won’t, we’ll be replacing people. And I have a plan that’s going to be announced very shortly,” she said.
“We’ve identified a whole range of opportunities we have to help supplement them.”
Hochul said state officials were “working closely with various hospital systems to find out where we can get other individuals to come in and supplement places like nursing homes.”
“We’re also reaching out to the Department of State to find out about visas for foreign workers, on a limited basis, to bring more nurses over here,” she said.
Per the Department of Health’s records, 19% of the state’s hospital workers remained unvaccinated as of Sept. 15, and 18% of nursing home employees remained unvaccinated as of Wednesday.
Starting Monday, employers can fire unvaccinated workers who don’t have a “valid medical exemption” (though employees who claim religious exemption are also immune until Oct. 12 due to a temporary injunction issued by a federal judge in Utica).
The plaintiffs in that case, almost all of them Catholic, oppose vaccines because they “employ aborted fetus cell lines in their testing, development, or production.”
Though the US Conference of Bishops says it’s okay for Catholics to take these vaccines if no alternatives are available, and Pope Francis has of course spoken out in favor of vaccination.
Circling back to the situation in New York, while Hochul is probably reveling in her first opportunity to play “hardball” – a game for which her predecessor was famous – New York health workers can probably rest easy – at least when it comes to the foreign worker threat. The State Department couldn’t process all those SIVs for Afghan collaborators in a timely manner. What makes you think they’ll be able to dole them out to foreign workers, who probably also haven’t been vaccinated. Where does Hochul think these foreign workers are going to come from? Europe?
We get a lot of e-mails and private messages along these lines “do you have a source for X?” or “can you point me to mask studies?” or “I know I saw a graph for mortality, but I can’t find it anymore”. And we understand, it’s been a long 18 months, and there are so many statistics and numbers to try and keep straight in your head.
So, to deal with all these requests, we decided to make a bullet-pointed and sourced list for all the key points. A one-stop-shop.
Here are key facts and sources about the alleged “pandemic”, that will help you get a grasp on what has happened to the world since January 2020, and help you enlighten any of your friends who might be still trapped in the New Normal fog (click links to skip):
1. The survival rate of “Covid” is over 99%. Government medical experts went out of their way to underline, from the beginning of the pandemic, that the vast majority of the population are not in any danger from Covid.
Almost all studies on the infection-fatality ratio (IFR) of Covid have returned results between 0.04% and 0.5%. Meaning Covid’s survival rate is at least 99.5%.
*
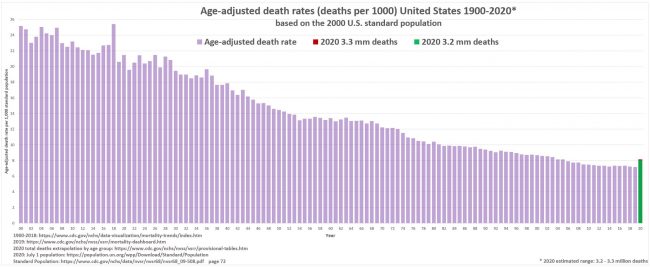
2. There has been NO unusual excess mortality. The press has called 2020 the UK’s “deadliest year since world war two”, but this is misleading because it ignores the massive increase in the population since that time. A more reasonable statistical measure of mortality is Age-Standardised Mortality Rate (ASMR):
By this measure, 2020 isn’t even the worst year for mortality since 2000, In fact since 1943 only 9 years have been better than 2020.
Similarly, in the US the ASMR for 2020 is only at 2004 levels:
For a detailed breakdown of how Covid affected mortality across Western Europe and the US click here. What increases in mortality we have seen could be attributable to non-Covid causes [facts 7, 9 & 19].
*
3. “Covid death” counts are artificially inflated. Countries around the globe have been defining a “Covid death” as a “death by any cause within 28/30/60 days of a positive test”.
Removing any distinction between dying of Covid, and dying of something else after testing positive for Covid will naturally lead to over-counting of “Covid deaths”. British pathologist Dr John Lee was warning of this “substantial over-estimate” as early as last spring. Other mainstream sources have reported it, too.
Considering the huge percentage of “asymptomatic” Covid infections [14], the well-known prevalence of serious comorbidities [fact 4] and the potential for false-positive tests [fact 18], this renders the Covid death numbers an extremely unreliable statistic.
*
4. The vast majority of covid deaths have serious comorbidities. In March 2020, the Italian government published statistics showing 99.2% of their “Covid deaths” had at least one serious comorbidity.
These included cancer, heart disease, dementia, Alzheimer’s, kidney failure and diabetes (among others). Over 50% of them had three or more serious pre-existing conditions.
5. Average age of “Covid death” is greater than the average life expectancy. The average age of a “Covid death” in the UK is 82.5 years. In Italy it’s 86. Germany, 83. Switzerland, 86. Canada, 86. The US, 78, Australia, 82.
As such, for most of the world, the “pandemic” has had little-to-no impact on life expectancy. Contrast this with the Spanish flu, which saw a 28% drop in life expectancy in the US in just over a year. [source]
*
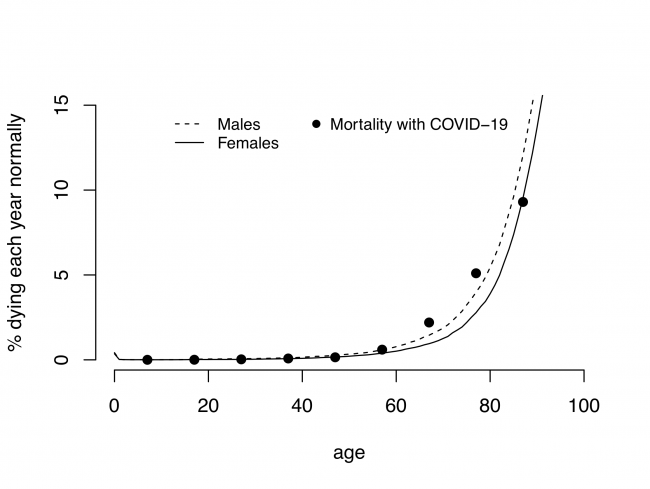
6. Covid mortality exactly mirrors the natural mortality curve.Statistical studies from the UK and India have shown that the curve for “Covid death” follows the curve for expected mortality almost exactly:
The small increase for some of the older age groups can be accounted for by other factors.[facts 7, 9 & 19]
*
7. There has been a massive increase in the use of “unlawful” DNRs. Watchdogs and government agencies have reported huge increases in the use of Do Not Resuscitate Orders (DNRs) over the last twenty months.
In the UK there was an “unprecdented” rise in “illegal” DNRs for disabled people, GP surgeries sent out letters to non-terminal patients recommending they sign DNR orders, whilst other doctors signed “blanket DNRs” for entire nursing homes.
A study done by Sheffield Univerisity found over one-third of all “suspected” Covid patients had a DNR attached to their file within 24 hours of hospital admission.
Blanket use of coerced or illegal DNR orders could account for any increases in mortality in 2020/21.[Facts 2 & 6]
*
PART II: LOCKDOWNS
8. Lockdowns do not prevent the spread of disease. There is little to no evidence lockdowns have any impact on limiting “Covid deaths”. If you compare regions that locked down to regions that did not, you can see no pattern at all.
“Covid deaths” in Florida (no lockdown) vs California (lockdown)
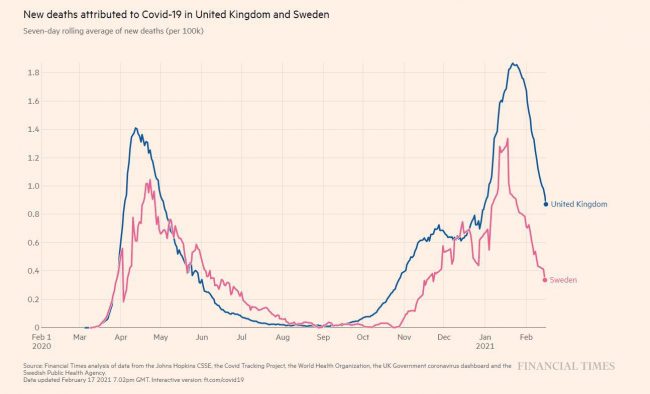
“Covid deaths” in Sweden (no lockdown) vs UK (lockdown)
*
9. Lockdowns kill people. There is strong evidence that lockdowns – through social, economic and other public health damage – are deadlier than the “virus”.
Dr David Nabarro, World Health Organization special envoy for Covid-19 described lockdowns as a “global catastrophe” in October 2020:
We in the World Health Organization do not advocate lockdowns as the primary means of control of the virus[…] it seems we may have a doubling of world poverty by next year. We may well have at least a doubling of child malnutrition […] This is a terrible, ghastly global catastrophe.”
Unemployment, poverty, suicide, alcoholism, drug use and other social/mental health crises are spiking all over the world. While missed and delayed surgeries and screenings are going to see increased mortality from heart disease, cancer et al. in the near future.
The impact of lockdown would account for the small increases in excess mortality [Facts 2 & 6]
*
10. Hospitals were never unusually over-burdened. the main argument used to defend lockdowns is that “flattening the curve” would prevent a rapid influx of cases and protect healthcare systems from collapse. But most healthcare systems were never close to collapse at all.
As part of their Covid policy, the NHS announced in Spring of 2020 that they would be “re-organizing hospital capacity in new ways to treat Covid and non-Covid patients separately” and that “as result hospitals will experience capacity pressures at lower overall occupancy rates than would previously have been the case.”
This means they removed thousands of beds. During an alleged deadly pandemic, they reduced the maximum occupancy of hospitals. Despite this, the NHS never felt pressure beyond your typical flu season, and at times actually had 4x more empty beds than normal.
11. PCR tests were not designed to diagnose illness. The Reverse-Transcriptase Polymerase Chain Reaction (RT-PCR) test is described in the media as the “gold standard” for Covid diagnosis. But the Nobel Prize-winning inventor of the process never intended it to be used as a diagnostic tool, and said so publicly:
PCR is just a process that allows you to make a whole lot of something out of something. It doesn’t tell you that you are sick, or that the thing that you ended up with was going to hurt you or anything like that.”
*
12. PCR Tests have a history of being inaccurate and unreliable. The “gold standard” PCR tests for Covid are known to produce a lot of false-positive results, by reacting to DNA material that is not specific to Sars-Cov-2.
As early as February of 2020 experts were admitting the test was unreliable. Dr Wang Cheng, president of the Chinese Academy of Medical Sciences told Chinese state television “The accuracy of the tests is only 30-50%”. The Australian government’s own website claimed“There is limited evidence available to assess the accuracy and clinical utility of available COVID-19 tests.” And a Portuguese court ruled that PCR tests were “unreliable” and should not be used for diagnosis.
You can read detailed breakdowns of the failings of PCR tests here, here and here.
*
13. The CT values of the PCR tests are too high. PCR tests are run in cycles, the number of cycles you use to get your result is known as your “cycle threshold” or CT value. Kary Mullis said: “If you have to go more than 40 cycles[…]there is something seriously wrong with your PCR.”
Dr Juliet Morrison, virologist at the University of California, Riverside, told the New York Times: Any test with a cycle threshold above 35 is too sensitive…I’m shocked that people would think that 40 [cycles] could represent a positive…A more reasonable cutoff would be 30 to 35″.
In the same article Dr Michael Mina, of the Harvard School of Public Health, said the limit should be 30, and the author goes on to point out that reducing the CT from 40 to 30 would have reduced “covid cases” in some states by as much as 90%.
Based on what we know about the CT values, the majority of PCR test results are at best questionable.
*
14. The World Health Organization (Twice) Admitted PCR tests produced false positives. In December 2020 WHO put out a briefing memo on the PCR process instructing labs to be wary of high CT values causing false positive results:
when specimens return a high Ct value, it means that many cycles were required to detect virus. In some circumstances, the distinction between background noise and actual presence of the target virus is difficult to ascertain.
Then, in January 2021, the WHO released another memo, this time warning that “asymptomatic” positive PCR tests should be re-tested because they might be false positives:
Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology.
*
15. The scientific basis for Covid tests is questionable. The genome of the Sars-Cov-2 virus was supposedly sequenced by Chinese scientists in December 2019, then published on January 10th 2020. Less than two weeks later, German virologists (Christian Drosten et al.) had allegedly used the genome to create assays for PCR tests.
They wrote a paper, Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR, which was submitted for publication on January 21st 2020, and then accepted on January 22nd. Meaning the paper was allegedly “peer-reviewed” in less than 24 hours. A process that typically takes weeks.
Since then, a consortium of over forty life scientists has petitioned for the withdrawal of the paper, writing a lengthy report detailing 10 major errors in the paper’s methodology.
They have also requested the release of the journal’s peer-review report, to prove the paper really did pass through the peer-review process. The journal has yet to comply.
The Corman-Drosten assays are the root of every Covid PCR test in the world. If the paper is questionable, every PCR test is also questionable.
It is literally impossible to tell the difference between an “asymptomatic case” and a false-positive test result.
*
17. There is very little evidence supporting the alleged danger of “asymptomatic transmission”. In June 2020, Dr Maria Van Kerkhove, head of the WHO’s emerging diseases and zoonosis unit, said:
From the data we have, it still seems to be rare that an asymptomatic person actually transmits onward to a secondary individual,”
… limited evidence to suggest the importance of [asymptomatic] transmission. The role of asymptomatic or presymptomatic influenza-infected individuals in disease transmission may have been overestimated…”
Given the known flaws of the PCR tests, many “asymptomatic cases” may be false positives.[fact 14]
*
PART V: VENTILATORS
18. Ventilation is NOT a treatment for respiratory viruses. Mechanical ventilation is not, and never has been, recommended treatment for respiratory infection of any kind. In the early days of the pandemic, many doctors came forward questioning the use of ventilators to treat “Covid”.
Writing in The Spectator, Dr Matt Strauss stated:
Ventilators do not cure any disease. They can fill your lungs with air when you find yourself unable to do so yourself. They are associated with lung diseases in the public’s consciousness, but this is not in fact their most common or most appropriate application.
German Pulmonologist Dr Thomas Voshaar, chairman of Association of Pneumatological Clinics said:
When we read the first studies and reports from China and Italy, we immediately asked ourselves why intubation was so common there. This contradicted our clinical experience with viral pneumonia.
Despite this, the WHO, CDC, ECDC and NHS all “recommended” Covid patients be ventilated instead of using non-invasive methods.
This was not a medical policy designed to best treat the patients, but rather to reduce the hypothetical spread of Covid by preventing patients from exhaling aerosol droplets.
*
19. Ventilators killed people. Putting someone who is suffering from influenza, pneumonia, chronic obstructive pulmonary disease, or any other condition which restricts breathing or affects the lungs, will not alleviate any of those symptoms. In fact, it will almost certainly make it worse, and will kill many of them.
Mechanical ventilation is also damaging to the physical structure of the lungs, resulting in “ventilator-induced lung injury”, which can dramatically impact quality of life, and even result in death.
According to the “undercover nurse”, ventilators were being used so improperly in New York, they were destroying patients’ lungs:
This policy was negligence at best, and potentially deliberate murder at worst. This misuse of ventilators could account for any increase in mortality in 2020/21 [Facts 2 & 6]
*
PART VI: MASKS
20. Masks don’t work. At least a dozen scientific studies have shown that masks do nothing to stop the spread of respiratory viruses.
One meta-analysis published by the CDC in May 2020 found “no significant reduction in influenza transmission with the use of face masks”.
Another study with over 8000 subjects found masks “did not seem to be effective against laboratory-confirmed viral respiratory infections nor against clinical respiratory infection.”
There are literally too many to quote them all, but you can read them: [1][2][3][4][5][6][7][8][9][10] Or read a summary by SPR here.
The WHO commissioned their own meta-analysis in the Lancet, but that study looked only at N95 masks and only in hospitals. [For full run down on the bad data in this study click here.]
Aside from scientific evidence, there’s plenty of real-world evidence that masks do nothing to halt the spread of disease.
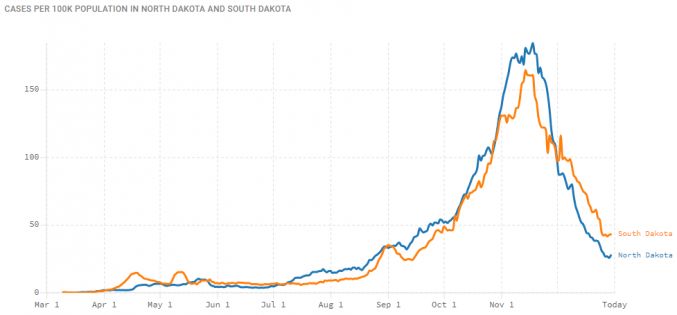
For example, North Dakota and South Dakota had near-identical case figures, despite one having a mask-mandate and the other not:
21. Masks are bad for your health. Wearing a mask for long periods, wearing the same mask more than once, and other aspects of cloth masks can be bad for your health. A long study on the detrimental effects of mask-wearing was recently published by the International Journal of Environmental Research and Public Health
Dr. James Meehan reported in August 2020 he was seeing increases in bacterial pneumonia, fungal infections, facial rashes .
Masks are also known to contain plastic microfibers, which damage the lungs when inhaled and may be potentially carcinogenic.
The report goes on to warn these masks (and other medical waste) will clog sewage and irrigation systems, which will have knock on effects on public health, irrigation and agriculture.
A study from the University of Swansea found “heavy metals and plastic fibres were released when throw-away masks were submerged in water.” These materials are toxic to both people and wildlife.
*
PART VII: VACCINES
23. Covid “vaccines” are totally unprecedented. Before 2020 no successful vaccine against a human coronavirus had ever been developed. Since then we have allegedly made 20 of them in 18 months.
While traditional vaccines work by exposing the body to a weakened strain of the microorganism responsible for causing the disease, these new Covid vaccines are mRNA vaccines.
mRNA (messenger ribonucleic acid) vaccines theoretically work by injecting viral mRNA into the body, where it replicates inside your cells and encourages your body to recognise, and make antigens for, the “spike proteins” of the virus. They have been the subject of research since the 1990s, but before 2020 no mRNA vaccine was ever approved for use.
*
24. Vaccines do not confer immunity or prevent transmission. It is readily admitted that Covid “vaccines” do not confer immunity from infection and do not prevent you from passing the disease onto others. Indeed, an article in the British Medical Journal highlighted that the vaccine studies were not designed to even try and assess if the “vaccines” limited transmission.
The vaccine manufacturers themselves, upon releasing the untested mRNA gene therapies, were quite clear their product’s “efficacy” was based on “reducing the severity of symptoms”.
*
25. The vaccines were rushed and have unknown longterm effects. Vaccine development is a slow, laborious process. Usually, from development through testing and finally being approved for public use takes many years. The various vaccines for Covid were all developed and approved in less than a year. Obviously there can be no long-term safety data on chemicals which are less than a year old.
Pfizer even admit this is true in the leaked supply contract between the pharmaceutical giant, and the government of Albania:
the long-term effects and efficacy of the Vaccine are not currently known and that there may be adverse effects of the Vaccine that are not currently known
26. Vaccine manufacturers have been granted legal indemnity should they cause harm. The USA’s Public Readiness and Emergency Preparedness Act (PREP) grants immunity until at least 2024.
The UK went even further, granting permanent legal indemnity to the government, and any employees thereof, for any harm done when a patient is being treated for Covid19 or “suspected Covid19”.
Again, the leaked Albanian contract suggests that Pfizer, at least, made this indemnity a standard demand of supplying Covid vaccines:
Purchaser hereby agrees to indemnify, defend and hold harmless Pfizer […] from and against any and all suits, claims, actions, demands, losses, damages, liabilities, settlements, penalties, fines, costs and expenses
*
PART VIII: DECEPTION & FOREKNOWLEDGE
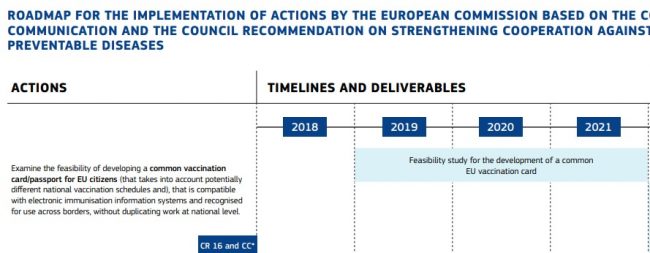
27. The EU was preparing “vaccine passports” at least a YEAR before the pandemic began. Proposed COVID countermeasures, presented to the public as improvised emergency measures, have existed since before the emergence of the disease.
These documents were combined into the 2019 “Vaccination Roadmap”, which (among other things) established a “feasibility study” on vaccine passports to begin in 2019 and finish in 2021:
This report’s final conclusions were released to the public in September 2019, just a month before Event 201 (below).
*
28. A “training exercise” predicted the pandemic just weeks before it started. In October 2019 the World Economic Forum and Johns Hopkins University held Event 201. This was a training exercise based on a zoonotic coronavirus starting a worldwide pandemic. The exercise was sponsored by the Bill and Melinda Gates Foundation and GAVI the vaccine alliance.
The exercise published its findings and recommendations in November 2019 as a “call to action”. One month later, China recorded their first case of “Covid”.
*
29. Since the beginning of 2020, the Flu has “disappeared”. In the United States, since February 2020, influenza cases have allegedly dropped by over 98%.
Meanwhile, a new disease called “Covid”, which has identical symptoms and a similar mortality rate to influenza, is supposedly sweeping the globe.
*
30. The elite have made fortunes during the pandemic. Since the beginning of lockdown the wealthiest people have become significantly wealthier. Forbes reported that 40 new billionaires have been created “fighting the coronavirus”, with 9 of them being vaccine manufacturers.
These are the vital facts of the pandemic, presented here as a resource to help formulate and support your arguments with friends or strangers. Thanks to all the researchers who have collated and collected this information over the last twenty months, especially Swiss Policy Research.
While the UK is supposedly dropping their vaccine passport idea (for now), things are looking bleak in country after country as people all around the world are facing the threat of vaccine mandates. Today on #SolutionsWatch James explores the array of solutions that are on the table to thwart this threat.
Dalek-like cries of ‘Vaccinate! Vaccinate!’ are everywhere, and yet many reputable doctors and scientists have warned for months of existing hazards from the jab, including deaths and injuries linked to its unique and experimental mode of action, and future risks that may be even more dire. (See also here and here.)
I have written some 35 articles on Covid over the past year, first for Lockdown Sceptics, now renamed The Daily Sceptic, and then for The Conservative Woman, now renamed TCW Defending Freedom. Both these daily newsletters, with associated websites, run largely by volunteers, are doing a far better job than any of the well-funded mainstream media or indeed academic journals in consistently questioning and challenging Covid orthodoxy, from a strong ethical as well as factual basis. It is a dynamic field, and they have risen to the challenge magnificently.
With some sadness, I have decided I must step back from the controversy for a while. As with ‘HIV’/Aids, another scientific nonsense which I covered as a journalist but which survived for decades because it suited so many powerful interests, Covid-19 has gripped the public imagination and discourse in such a way that facts, reason and ethics are playing little part in the global response to the crisis.
To see a recent example of how crazy things have become, please watch this five-minute video by Julie Ponesse, a professor of ethics at the University of Western Ontario. She recorded it for first-year students, having been threatened with dismissal after 20 years because ‘I will not submit to having an experimental vaccine injected into my body’.
‘My job is to think critically,’ she says. ‘To ask questions. Questions like, Says who? Who is the authority giving this order? Should I trust them with my body?
‘As a professor, I don’t have to watch the news to find out if the Covid vaccines are safe. I read medical journals, and I consult my colleagues who are professors of science and medicine. I’ve learned from doctors that there are serious questions about how safe these vaccines really are. There are questions about how well they work. Nobody is promising that I won’t get Covid, or transmit Covid, if I get the vaccine.
‘But ultimately, none of that matters to me. Because I am a professor of ethics, and I am a Canadian. I’m entitled to make choices about what does and does not enter my body, regardless of my reasons.
‘If I’m allowed back into my university, it’s my job to teach my students that this is wrong. It is ethically wrong to impose an experimental medical procedure as a condition of employment. This is my first, and potentially my last, lesson of the year.’
On September 7, Ponesse was dismissed. Now Joe Biden is threatening 80million unvaccinated Americans with mandatory jabs – more than he is threatening the Taliban, as a Fox News commentator put it.
Most of my former medical and science correspondent colleagues, and indeed the social media giants such as Facebook and Google (whose ad department has just de-platformed TCW Defending Freedom), have been drawn into the false belief that we are in a war that can be won only if everyone gets the jab.
That belief has been supported and promoted from the start by a scientific establishment seeking to assuage its guilt over the fact that science itself gave us SARS-CoV-2. The virus was clearly a product of genetic engineering by American and Chinese scientists, but a high-level decision was taken to try to hide this fact from the public.
Top UK scientists, including Sir Jeremy Farrar of the Wellcome Trust and Sir Patrick Vallance, former president of research and development at global pharmaceutical company GlaxoSmithKline and now chief scientific adviser to the Government, took part in secret talks the day after Covid-19 was declared a global health emergency to decide how to respond.
Bibles of the scientific world such as Nature and The Lancet vigorously promoted the idea that the virus jumped across to humans from an animal host, and I believed them myself at first, in common with most reporters.
For all this time, since the pandemic began, it has been left to individual ‘maverick’ researchers – often barred from official channels of communication – to demonstrate that years of laboratory work brought about the modifications which turned a bat virus into a danger for humans.
Yet nearly 18 months ago, an Anglo-Norwegian team of vaccine researchers using electron microscopy described six ‘unique fingerprints . . . indicative of purposive manipulation’ in the virus’s spike protein, enabling it to enter a wide range of human cells. They warned that the protein in itself was hazardous and that specific precautions would be needed when using it in any vaccine candidate.
Their report was suppressed, and even today the scientific community continues to avoid considering its devastating implications, which include an explanation for the blood clotting belatedly acknowledged as an adverse effect from vaccines based on the spike.
Was Covid a plandemic? High-level, international pandemic scenario planning did precede the arrival of SARS-CoV-2, but the evident panic in China when the first cases emerged, and attempted cover-up of British and American involvement, speak more to an accidental escape than a planned crisis.
However, immensely influential foundations, whose own financial interests and investments are served as they fund campaigns for so-called ‘global health security’ and ‘pandemic preparedness’ (see for example here, here, here and here) have contributed to the crisis. They have helped bring into being the very threats they were supposed to counter. Unless and until these influences are exposed, and the malign consequences acknowledged, we look set to perpetuate the mistakes.
At least in the UK, ministers may be realising that lockdowns intended to ‘save’ our NHS had the opposite result. The service is on its knees, with many staff dispirited, and millions are awaiting care and treatment. Children and old people have especially suffered.
Yet public opinion has been whipped into such a frenzy of fear that there is widespread acquiescence in the face of proposals for more punishing controls, especially surrounding Covid vaccines.
This is despite a lack of clear evidence as to whether Covid vaccination is truly ‘safe and effective’, as we are constantly assured by government scientists, or may actually be doing more harm than good. The issue has become so political that it is difficult to sort out facts from propaganda, but I believe that Public Health England, while promoting vaccine passports and ‘no jab, no job’ policies, has its head in the sand over evidence that we may face a disaster of unimaginable proportions.
It tries to justify lives lost to the jab by plucking huge numbers of ‘lives saved’ and ‘infections avoided’ out of thin air. Data showing declining vaccine effectiveness and a need for booster shots tell us that these claims are at best, huge overestimates. The latest experience of highly vaccinated Israel (see here and here) is discouraging, to say the least.
Before I learned of the toxicity of the spike protein and the way it is carried through the blood and distributed throughout the body, accumulating especially in the ovaries and potentially damaging fertility, I admired the ingenuity of the RNA vaccines and hoped they would work.
Today, however, despite being aged 77, I would far prefer to take my chances with the virus, which we now know is dealt with successfully by most people’s natural immune mechanisms, than with the jab, which is designed to bypass the body’s first defences.
The human body has astonishing resilience and intelligence, and I am sure most of the millions who have received and recovered from the jab, usually without more than a day or two of discomfort, will be fine.
Yet now the NHS is gearing up to roll out the jab for 12- to 15-year-olds, and teachers’ leaders are all for it. Objections by experts who know that healthy children are at essentially zero risk from the virus, while the jab itself can injure or kill, have been acknowledged, but set aside, by the UK’s four chief medical officers. This is despite heartfelt pleas such as from the UK Medical Freedom Alliance.
Vaccinating 12-year-olds with an experimental jab of certain toxicity, even against their parents’ wishes? How could we have reached a state of such stupidity as even to contemplate such measures?
And it won’t necessarily end there. Pfizer and Moderna are both seeking authorisation to extend the jab drive to 5-11-year-olds.
An element that has surprised and distressed me is the almost complete lack of Parliamentary oversight of the handling of the crisis. It is as if our elected representatives have been reduced to a single party, and even that party has been dancing to the tune of unelected advisers and officials.
I wondered about writing to Labour leaders to urge them to challenge the Government much more strongly, but then read a long essay, The Unions and the U-turns, which provides an important piece of the puzzle as to why ministers have stumbled along so disastrously for so long, usually with cries of ‘Too late!’ or ‘Hit harder!’ from the Opposition.
Written by philosopher, author and campaigner Ben Irvine, it describes the driving role that public sector unions have played, largely behind the scenes, in what Irvine calls the ‘coronapanic debacle’ in Britain. Understanding the role of socialists in pushing the Prime Minister into repeated U-turns on Covid policy, he writes, ‘is key to unlocking this whole sorry mess’.
For instance, you may not know that the first lockdown was set in motion the day after the largest teaching union threatened unilateral schools closures. Or that numerous teaching unions refused to return to work during the first lockdown. Or that in the summer of 2020 a transport workers’ union threatened to strike unless the government mandated masks on trains. Or that in the same summer a retail workers’ union threatened to strike unless the government mandated masks in shops. Or that the third lockdown happened the day after there was a colossal teaching mutiny with hundreds of thousands of teachers refusing to return to work in January 2021. Or that the reason why children have been cruelly masked in schools was that mutinous teaching unions demanded it.
In the time I now intend to take out, I want to explore what is missing in the human spirit that makes us vulnerable to such madness.
Greed plays a part. It is obvious that Big Pharma, with its friends in government and the World Health Organisation, has been well placed to capitalise on the crisis.
How much better it would have been if the incredible £400billion cost to the nation of the UK’s handling of the crisis to date had been spent on strengthening immunity to the virus through nutritional and social support structures, rather than poured into furlough schemes, mass testing with dodgy kits, and untested vaccines.
But the discovery that powerful unions helped amplify the disaster makes me realise it is not just scientific embarrassment, and capitalist greed, driving the policy errors, but also the false compassion to which those on the Left seem especially vulnerable. ‘Save Lives – Stop Living’ is one of my favourite slogans from these Orwellian times.
In the early years of Aids, I joined media colleagues in raising the alarm about a virus that we were told put all sexually active people at risk because of a long time lag between infection and illness. We were happy to feel we were contributing to the public health effort.
But thanks to the work of ‘dissident’ scientists in the USA and Australia, I gradually learned that ‘HIV’ was not a genuine pathogen. ‘HIV/Aids’ was a concept, marketed with skill and urgency by American government scientists with support from colleagues in the UK and elsewhere, after a period in which the plight of early Aids victims had been cruelly neglected.
The virus theory democratised the illness and brought compassion in place of condemnation. Gay Lib leaders had fought for years to end discriminatory laws and attitudes and when Aids came along, its early characterisation as a ‘gay plague’ linked to promiscuous anal sex and heavy drug use threatened to derail the movement.
Then big money, combined with political correctness, created a monolithic belief system, never fully dismantled, that caused enormous harm. Under the leadership of the US ‘Aids czar’ Anthony Fauci, now playing a similar role with Covid, HIV/Aids became a business worth hundreds of billions of dollars, supporting countless well-meaning NGOs as well as science journals and researchers.
The use of unvalidated test kits bequeathed poor African countries with a false belief that the continent was in the grip of a terrible epidemic. A lethal, hugely expensive, US government-sponsored drug marketed by Burroughs Wellcome killed and tortured thousands of gay men, as well as ‘HIV’-positive children, and patients with the blood clotting disorder haemophilia. (SeePoIson By Prescription – The AZT Story, by John Lauritsen, published by Asklepios, New York, 1990.) A futile search for a vaccine to a non-existent virus continues to this day – 35 years on!
The scientific community fiercely resisted challenge and never owned up to the mistakes at the heart of the HIV paradigm, which I have summarised here.
When the then Sunday Times editor Andrew Neil persisted in publishing Aids heresies, the response was censorship, suppression and ridicule. Other mass media, notably the BBC, Guardian, Independent and Observer, bayed for our blood. The Health Education Council started an Aids journalism award specifically in our dishonour. The science journal Nature contemplated picketing the ST offices.
This was despite challenges from top scientists, including Nobel laureates such as Kary Mullis, inventor of the PCR test widely used in Aids research and now (grossly misused) in purportedly diagnosing Covid, who insisted there was zero scientific evidence of HIV being the cause of the collapse of the immune system seen in the syndrome.
I learned at that time that the bigger the evidence vacuum, the greater the intolerance of dissenting views and the tighter the attempted mind control.
Doctors who sought to treat aids by means other than the official drug, called AZT, were struck off the medical register or otherwise hounded out of the profession. Scientists who advocated different ways of tackling Aids were unable to publish.
The censorship was absolute. At one point, a major paper deconstructing the HIV theory was accepted by a well-respected journal. But the defenders of the HIV/Aids faith got to hear of it, the editor was removed, and his successor withdrew the paper from the publication pipeline. Even patients who dared question the orthodoxy were viciously lied against and abused, sometimes with lethal results.
It took 25 years for the WHO to acknowledge that there was no world pandemic among heterosexuals, although it continued to maintain that sub-Saharan Africa was being devastated by the disease. That too was untrue, as I learned in 1993 during several weeks reporting from supposed Aids hotspots in Africa. I found that scarce resources were being misdirected to an imaginary epidemic created by the unvalidated ‘HIV’ test. The scientific and medical establishments went into a frenzy over these reports but they were never refuted.
Unlike ‘HIV’/Aids, Covid-19 is all too real. For reasons that are not well understood, the disease comes in definite though generally short-lived waves, and it can be lethal in people who are already near death’s door through other illnesses or because of old age.
I am sure that those who knew of its genetically engineered status when it first escaped from the Wuhan lab feared the worst, and that was why a global alert was sounded.
However it has been known since late last year that overall the proportion of virus-infected patients who die is less than 0.2 per cent, not much more than in a bad year for flu, and far lower than was initially thought.
By that time, though, full-scale fearmongering propaganda was under way. An uncalibrated diagnostic test had been rushed out, giving the false impression that ‘cases’ were rampant when in fact many of those who tested positive were in good health.
Deaths among the elderly were reclassified as Covid even when from cancer or heart disease or inappropriate drug use (see this funeral director’s report for a moving account of this scandal).
Just as with ‘HIV’/Aids, cheap treatment approaches such as vitamin D and ivermectin that were being used by some doctors to keep patients out of hospital were officially rubbished and even banned.
Mask mandates, lockdowns and enforced separations were used indiscriminately, and largely without scientific justification, to bring about a completely disproportionate fear.
Now, in what seems to me to be a continuing effort to divert attention from the laboratory-induced, chimeric status of the Covid virus, scientists are telling us there are many more like SARS-CoV-2, jumping from animals into humans all the time and potentially causing new pandemics.
They also talk up the threat posed by genetic changes in the virus, when in fact the variations are generally insignificant and natural, as explained here by Oxford University’s Professor Sunetra Gupta.
They ignore evidence that ‘natural immunity not only confers robust, durable and high-level protection against Covid, but also provides better protection than vaccine-induced immunity’.
And meanwhile, the so-called variants provide a convenient excuse for the failure of the existing vaccines and an argument for booster shots which could become the basis of a never-ending bonanza for the pharmaceutical companies.
Is there any hope that we may come to our senses sooner with Covid than with Aids?
Government agencies worldwide, including the UK’s (Bill Gates and Big Pharma funded) Medicines and Healthcare products Regulatory Agency (MHRA), have been supine in the face of a huge range of adverse effects potentially related to the Covid jab. More than 1,500 deaths and thousands of injuries have been reported under the UK’s ‘yellow card’ scheme, and many thousands more in the US, but the regulators have shown extreme reluctance to acknowledge the harm being caused.
One big difference from the ‘HIV’/Aids era is that the internet has enabled critics of Covid orthodoxy to post challenging data and opinion, despite online censorship.
When celebrity rapper Nicki Minaj, with 22.6million followers, tweeted that her cousin’s friend became impotent through swollen testicles after receiving the Covid vaccine, she was almost universally mocked. But as analyst Steve Kirsch reported in TrialSite News, Minaj was right and all the world’s experts wrong: there are more than 60 cases of testicular swelling on the US database of adverse reactions to the Covid jab.
Information that could end the ‘vaccine dystopia’ is out there. It is present in a multitude of sources, including the UK’s own TCW Defending Freedom and The Daily Sceptic, but is still largely withheld from the wider public by governments, their advisers, and the mainstream media.
I do not share the view that there is a depopulation agenda at work, or that super-prisons are being built to house the unvaccinated, or that microchips are to be implanted in us by crazed technocrats. But I can understand how such theories gain credence while top scientists who funded the work that created the virus remain in denial about what they have done, and world leaders who were informed of SARS-CoV-2’s laboratory origin remain in the panic mode that brought such a disastrous response.
Our leaders, both scientific and political, have barricaded themselves behind a wall that is preventing them from seeing and hearing the reality. This time, unlike in the tragic ‘HIV’/Aids story, perhaps the fourth estate will soon recognise that it can step back from its own well-intentioned panic stations, and bring that wall down.
A doctor, who is also the owner of a diagnostic lab has found a 20 times increase in cancers since the COVID-19 vaccine rollout. Explaining his findings he said that the vaccines seem to be causing serious autoimmune issues, in a way he described as a “reverse HIV” response.
On March 18, Dr. Ryan Cole, a board-certified pathologist and owner and operator of a diagnostics lab, reported to the public in a video produced by Idaho state government’s “Capitol Clarity” project, that he is seeing a massive ‘uptick’ in various autoimmune diseases and cancers in patients who have been vaccinated.
“Since January 1, in the laboratory, I’m seeing a 20 times increase of endometrial cancers over what I see on an annual basis,” reported Dr. Cole in the video clip shared on Twitter.
“I’m not exaggerating at all because I look at my numbers year over year, I’m like ‘Gosh, I’ve never seen this many endometrial cancers before’,” he continued.
Explaining his findings at the March 18 event, Cole told Idahoans that the vaccines seem to be causing serious autoimmune issues, in a way he described as a “reverse HIV” response.
Cole explained that two types of cells are required for adequate immune system function: “Helper T-cells,” also called “CD4 cells,” and “killer T-cells,” often known as “CD8 cells.”
According to Cole, in patients with HIV, there is a massive suppression of “helper T-cells” which cause immune system functions to plummet, and leave the patient susceptible to a variety of illnesses.
Similarly, Cole describes, “post-vaccine, what we are seeing is a drop in your killer T-cells, in your CD8 cells,”
“And what do CD8 cells do? They keep all other viruses in check,” he continued.
Much like HIV causes immune system disruption by suppressing CD4 “helper” cells, the same thing happens when CD8 “killer” cells are suppressed. In Dr. Cole’s expert view, this is what seems to be the case with the COVID-19 jabs.
Cole goes on to state that as a result of this vaccine-induced “killer T-cell” suppression, he is seeing an “uptick” of not only endometrial cancer, but also melanomas, as well as herpes, shingles, mono, and a “huge uptick” in HPV when “looking at the cervical biopsies of women.”
This is not the first time the COVID-19 vaccines have been linked to serious issues regarding women’s health.
Recently, according to VAERS data a breastfeeding baby died of blood clots and inflamed arteries weeks after his mother was given the Pfizer COVID-19 vaccine.
Dr. Cole states in his video that, not only are melanomas showing up more frequently, like endometrial cancers, the melanomas are also developing more rapidly, and are more severe in younger people, than he has ever previously witnessed.
“Most concerning of all, there is a pattern of these types of immune cells in the body keeping cancer in check,” stated the doctor.
“I’m seeing invasive melanomas in younger patients; normally we catch those early, and they are thin melanomas, [but] I’m seeing thick melanomas skyrocketing in the last month or two,” he added.
Cole came into prominence in January of 2021 when the Idaho government put in place an effort called “Capitol Clarity,” with the stated goal of keeping Idahoans informed about the facts surrounding COVID-19.
Capitol Clarity has since hosted Dr. Ryan Cole multiple times to provide information to the public about vaccine safety and COVID-19 measures more broadly.
The videos of Dr. Cole at these events, which were originally posted on YouTube, have since been deleted by the Google owned video platform in a continual effort of censorship by Big Tech.
In a Highwire exclusive, Deborah Conrad, a hospitalist physician’s assistant on the frontlines of the pandemic, pulls back the curtain on the complete lack and disregard in her hospital for reporting Covid vaccine injury to VAERS, this country’s only mechanism to track the safety of these rushed-to-market, mandated products.
In riveting detail, including emails & recorded phone conversations, Conrad exposes the internal push to turn a blind eye to injuries and “tow the company line” that this vaccine is safe.
A while ago, I received an email from a friend who asked:
How can many, many respected, competitive, independent science folks be so wrong about [global warming] (if your [skeptical] premise is correct). I don’t think it could be a conspiracy, or incompetence. … Has there ever been another case when so many ‘leading’ scientific minds got it so wrong?
The answer to the second part of my friend’s question—“Has there ever been another case where so many ‘leading’ scientific minds got it so wrong?”—is easy. Yes, there are many such cases, both within and outside climate science. In fact, the graveyard of science is littered with the bones of theories that were once thought “certain” (e.g., that the continents can’t “drift,” that Newton’s laws were immutable, and hundreds if not thousands of others).
Science progresses by the overturning of theories once thought “certain.” … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.