1. it is not nor will it ever be possible to be “fully vaccinated” with these vaccines.

2. almost none of this has ever worked and only serves to drive hysteria.
all we need to do to have our lives and livelihoods back is to stop pretending we ever needed to give them up.

3. continuing to play cards with an opponent who smiles at you while dealing off the bottom of the deck is the literal height of stupidity and has been since i first posted this meme over a year ago…

bonus fact:
you cannot obey your way out of tyranny or an appease an oppressor until they stop.
complying so that it will end simply ensures that it will NEVER end.
going along to get along is the interminable, grinding road to subjugation.
disobey.

December 1, 2021
Posted by aletho |
Civil Liberties, Deception, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine, Human rights |
Leave a comment

Like most parents across the land, I received a letter from the local council’s Director of Public Health this morning (forwarded by the school in an email) explaining that they have “advised [sic] schools that parents/carers/other visitors are not invited” to nativity plays this year. Not the end of the world in the grand scheme of things, of course – just another depressing example in the long litany of examples of children’s priorities being cast under a bus due to adult panic during the course of this pandemic.
Much more concerning, because of what it said about the mindset of the Director of Public Health in question, was this alarmingly blithe justification for continued restrictions in schools, buried in the body of the letter:
Much as we would all like it to be, the pandemic is not over. Whilst it is clear that the vaccination programme is effective in preventing serious disease and deaths, the vaccine is never going to stop all transmission, and resultant harm, on its own. [Emphasis added]
You couldn’t get a starker admission than this that we long ago moved beyond “flattening the curve” or staving off a dire public health emergency in a once-in-a-lifetime, never-to- be-repeated year. No: we are now in a different place altogether – one in which we must stop transmission “and resultant harm” for its own sake, forever. For how else are we supposed to interpret this statement? On what grounds will parents ever be allowed back into schools to watch nativity plays (or even properly meet their children’s teachers), if the requirement is for “all transmission and resultant harm” to end? We will never be in that position. So in what circumstance does the Director of Public Health envisage there ever will be a return to normal schooling? Ought this not to be made clear to local parents?
More broadly, this incident raises the question of how it is that something so fundamental – children’s schooling – has ended up beholden to the whim of unelected, largely unaccountable, public officials such as this. The local Director of Public Health in any given local authority cannot be voted out. They are not challenged by probing interviews in prominent media outlets. The means by which they are appointed is entirely opaque. And their policy positions, political backgrounds, and motivations are subject to essentially no public scrutiny. Yet they possess the power, at the sweep of a pen, to disrupt the lives of literally tens of thousands of people within their bailiwicks, with the only possible avenue of challenge being a prohibitively expensive and time-consuming claim for judicial review. This ought to be intolerable in a free society. Yet it is the position in which we find ourselves.
Once again, the Covid pandemic and its response have shone a harsh light on British democracy, and revealed it to be in a dilapidated state indeed.
November 29, 2021
Posted by aletho |
Civil Liberties, Science and Pseudo-Science | Covid-19, Human rights, UK |
Leave a comment

In this messed-up mixed-up world the formerly respected Fourth Estate has devolved into a collection of flat-out liars, brain-dead ideologues and unmitigated ignoramuses. Turn on any of the mainstream media channels or go to any one of hundreds of online outlets and you’ll be swamped in effluent.
The horrific murderous tragedy in Waukesha, Wisconsin in which a man deliberately and determinedly drove his SUV at a high rate of speed through a parade last week is being called a “parade crash” by the most liberal media outlets.
According to 95% of the media talking heads and their cohort, Kyle Rittenhouse is a ‘murdering white supremacist.’ Laughably, Snopes calls the three convicted felons who attacked Rittenhouse — one a domestic abuser and rapist, another a pedophile, and the third a burglar — ‘victims.’ Snopes goes further saying those three felons were there to ‘peacefully protest.’ Never mind the fires, the looting and property destruction. None of which was discussed in the vast majority of the media during Rittenhouse’s trial or after his acquittal.
Now we have a new variant of COVID-19 which the physician who first encountered and reported it says is “mild.” In a report in the Telegraph, Dr. Angelique Coetzee, a GP for thirty-three years who also chairs the South African Medical Association says, “Their symptoms were so different and so mild from those I had treated before.”
Mild illness. Zero hospitalizations. No deaths. Yet with this report, we have yet another round of wholesale fear mongering from the press and governments.
“Biden to restrict travel from South Africa and 7 other countries starting Monday” (Remember the cries and howls from the Left when Trump shut down travel when COVID first appeared? Xenophobe!)
“Boris Johnson announces ‘tighter rules’ in response to Omicron variant”
“Israel to ban entry of foreigners from all countries over Omicron”
Across the ether alleged “news” outlets are spouting nonsense about this variant that the WHO and CDC say appears to be mild and, thus far, not deadly.
MSNBC proclaims, “Omicron variant renews calls for more robust vaccination…” Why when the vaccines we currently have a) do not work against the pre-existing COVID variants and b) aren’t designed for this variant? (MSNBC’s institutional ignorance was run up the flagpole for fullest display with this story.)
“Omicron variant puts world in a ‘race against time’, says EU Commission President” is the headline quote from CNN.
MSNBC proclaims, “New covid variant: Omicron is a pandemic gut check.” They hype the “growing concern” and breathlessly report that “Omicron variant represents a ‘significant potential risk’ to its (Moderna’s) Covid-19 vaccine.” Well, DUH! Previous vaccines that didn’t work against alpha, beta or delta sure aren’t going to work against a new strain. The biggest risk is that if this is as mild or non-threatening as it seems to be thus far (zero deaths, zero hospitalizations, remember) is that the market for COVID vaccines may have just dried up.
As soon as news of this variant came out and was blasted around the world, financial and commodity markets tanked, prompting Goldman Sachs to announce, “This mutation is unlikely to be more malicious and that the existing vaccines will most likely continue to be effective in preventing hospitalizations and deaths. We do not think that the new variant is sufficient reason to make major portfolio changes.”
According to Paul Elias Alexander, PhD at the Brownstone Institute, it might be that COVID has now transformed so much that new variants might be more infectious but less deadly.
This is a brain twister of an article if you’re not accustomed to reading technical papers, but Alexander makes several key points (emphasis added):
“The virus is behaving just like how viruses behave. They are mutable and mutate and via Muller’s ratchet, we expect this to be milder and milder mutations and not more lethal ones given the pathogen seeks to infect the host and not arrive at an evolutionary dead-end.”
“For example, the (Pfizer) vaccine has failed to stop infection and spread against Delta… fully vaccinated individuals with breakthrough infections have peak viral load similar to unvaccinated cases.”
What’s most fascinating in this paper is a reference to a Swedish study of records of the nation’s entire population. The study’s findings are that efficacy of Pfizer’s BioNtech vaccine “waned progressively from 92% (effectiveness) at day 15-30 to 47% at day 121-180, and from day 211 and onwards no effectiveness could be detected.
AstraZenica’s mRNA vaccine fared even worse: “effectiveness of ChAdOx1 nCoV-19 was generally lower and waned faster, with no effectiveness detected from day 121 and onwards.”
This Swedish study is news given that governments are forcing vaccines into our bodies. Shouldn’t this be reported? Shouldn’t it be headlines? Yet nowhere is this information readily available outside the medical community. WHO isn’t reporting it; CDC and FDA aren’t reporting on it in the US, and nowhere in Europe is it being reported.
The only reason Dr. Alexander’s paper and the Swedish study are presented here is because of diligent research through many sites and noting a single reference embedded in a longer article.
The fact is, all of this COVID hysteria is being driven by the lobbyists for the pharmaceutical companies and fomented by “news” organizations and governments for power and control over us, our livelihoods and our lives.
Isn’t it about time this nonsense ends?
November 29, 2021
Posted by aletho |
Fake News, Mainstream Media, Warmongering | CNN, Covid-19, MSNBC, United States |
Leave a comment
A further three football players collapsed during play this week, bringing new interest to the question of what might be the connection between this unusually high number of on-field medical emergencies and the Covid vaccines. Football pundit Trevor Sinclair got into hot water for raising the question on-air, while scientists argued that the disturbing trend is more likely to be a consequence of Covid itself than the vaccines.
Presumably something lies behind the recent rise, which according to some analysts has involved 21 sudden deaths (most heart-related) of FIFA players so far in 2021, compared to around 4.2 in an average year (with a standard deviation of 2.0). Assuming this isn’t a reporting phenomenon, this is an extraordinary spike and highly statistically significant.
The two major unusual factors this year are the presence of SARS-CoV-2 and the Covid vaccination programme. However, only two such deaths were reported in 2020, when Covid was also around, which would seem to lend weight to a vaccine explanation.
The vaccines are known to affect the heart and cardiovascular system in some cases, which is why blood clots and heart inflammation (e.g. myocarditis) are among the side-effects listed and why a number of countries have ceased using some of the vaccines in younger age groups. This means the idea that there could be a link between an unusual spate of heart-related emergencies and the vaccines shouldn’t be dismissed out of hand.
On the other hand, some studies have shown that the risk of developing myocarditis is substantially higher following SARS-CoV-2 infection than vaccination.
A number of scientists have pointed out that insofar as cardiovascular problems arise from the effect of the SARS-CoV-2 spike protein (and there seems to be some agreement that the spike protein is a large part of the causal story here) a bout of SARS-CoV-2 exposes the body to at least as much spike protein as a course of vaccination. Against that, those who suspect that the vaccines are playing a key role say that in fact most SARS-CoV-2 infections are not systemic but remain localised to the respiratory system, so have little impact on the cardiovascular system, whereas vaccination always allows the spike protein to have a systemic impact by gaining easy access to the bloodstream.
This matter would seem to merit much closer and more urgent attention than it appears to be receiving from regulators. It should be straightforward for those with access to the relevant data (most of which unfortunately is not publicly available) to analyse cardiovascular deaths according to vaccination status and prior infection status to see if there are patterns that may be a signal of concern.
An abstract appeared in the leading journal Circulation earlier this month which concluded: “The mRNA vaccines dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy, and other vascular events following vaccination.” There was no study to accompany the abstract, however, and it has been heavily criticised by some specialists. Nonetheless, leading NHS Consultant Cardiologist Dr Aseem Malhotra stuck his neck out this week on GB News to reveal that a cardiology researcher colleague found similar results, but was not prepared to publish for fear of the repercussions for his or her career: “They aren’t going to publish their findings, they are concerned about losing research money.”
What are the wider trends in deaths?
Since July, ONS data shows there have been 20,823 excess deaths in England and Wales, with 11,531 involving Covid, leaving 9,292 excess deaths from other causes (if we make the conservative assumption that all Covid deaths are excess deaths).
Analysis of cause of death data for England shows that between July 4th and November 5th 2021 there have been 3,095 excess deaths involving heart failure, of which 854 could be put down to COVID-19, leaving 2,241 from other causes; 4,460 excess deaths involving ischaemic heart diseases, of which 1,413 could be Covid, leaving 3,047 from other causes; 1,307 excess deaths involving cerebrovascular diseases, of which 489 could be Covid, leaving 818 from other causes; and 8,109 excess deaths involving ‘other circulatory diseases’, of which 3,357 could be Covid, leaving 4,752 from other causes. These categories can overlap – a death certificate can mention more than one of them – so the figures can’t simply be added to get a grand total, and the underlying cause could be recorded as something different. Nonetheless, we are talking about thousands of additional cardiovascular deaths since the summer.
Despite this, ONS data shows that deaths where the underlying cause was cardiovascular have been below average in this period. At the same time, deaths where Covid is recorded as the underlying cause account for only a fraction of cardiovascular deaths in the period. So what was the underlying cause of all these excess deaths involving cardiovascular conditions that weren’t Covid either? A query to the ONS came back suggesting that it was down to the significant excess in deaths where the underlying cause was recorded as “symptoms, signs and ill-defined conditions”. In other words, we don’t really know. So according to official data, there have been thousands of excess deaths involving cardiovascular conditions in the past four months, but the underlying cause of many of those deaths is unknown. This would seem to warrant further investigation, and since the vaccines may be implicated, without delay.
November 28, 2021
Posted by aletho |
War Crimes | Covid-19, COVID-19 Vaccine |
Leave a comment
This is an open letter to Andrew Gregory, Health Editor of the Guardian.
Dear Andrew,
We are a group of citizens dedicated to promoting a more open, democratic society. We have tried to contact you on several occasions without success, so we have published this open letter in the hope you will see it and reply.
On November 18, you published a story with the headline: ‘Mask-wearing cuts Covid incidence by 53%, says global study.’
The sub-heading was: ‘Researchers said results highlight the need to continue with face coverings, social distancing and handwashing alongside vaccine programmes’.
We were struck by this, since it goes against a substantial body of evidence that concludes that mask-wearing offers little if any protection against viruses, for example these studies https://swprs.org/face-masks-evidence/ https://www.professorhinkley.com/blog/sorry-oregon-your-mask-is-useless-according-to-the-science; https://www.city-journal.org/do-masks-work-a-review-of-the-evidence.
You did not reference the paper on which you base your article but an internet search reveals it. (Stella Talic corresponding author). You paraphrase uncritically: ‘Vaccines are safe and effective and saving lives around the world. But … it is not yet known if jabs will prevent future transmission of emerging coronavirus variants …
‘Results from more than 30 studies from around the world were analysed in detail, showing a statistically significant 53 per cent reduction in the incidence of Covid with mask wearing …’
We find it puzzling that you did not mention that ten days earlier the CATO Institute (an American libertarian think-tank) published a 61-page working paper entitled: Evidence for Community Cloth Face Masking to Limit the Spread of SARS-CoV 2: A Critical Review.
It tentatively concluded: ‘Of 16 quantitative meta-analyses, eight were equivocal or critical as to whether evidence supports a public recommendation of masks, and the remaining eight supported a public mask intervention on limited evidence, primarily on the basis of the precautionary principle.’
Given this striking incongruity, we have ten questions:
1. Have you read the Talic paper?
2. Do you agree that it is an exaggeration to describe it as a ‘global study’?
3. Have you read the associated British Medical Journal editorial?
4. Do you agree that your headline: ‘Mask-wearing cuts Covid incidence by 53%, says global study’ is misleading?
5. Were you aware of this when you chose the heading?
6. Why has the Guardian not published the results of the many studies which say there is no evidence of benefit and some evidence of harm?
7. Do you agree that professional journalism requires balance, in the public interest?
8. Would a more accurate headline be: ‘The majority of randomised controlled trials fail to establish that wearing face masks protects anyone against viruses’?
9. Is the Guardian’s policy to publish only information that supports a particular set of beliefs?
10. Are you prepared publicly to debate this matter?
Here is a little more detail about our concerns. The CATO meta-analysis states: ‘In non-healthcare settings, of the 14 RCTs (randomised control trials) identified by the authors that evaluated face mask efficacy compared to no-mask controls in protecting against respiratory infections other than Covid-19, 13 failed to find statistically significant benefits … of eight RCTs that evaluated face mask efficacy against respiratory illness transmission in non-healthcare household settings, all eight failed to find a statistically significant benefit for the use of face masks alone …’
This gives a very different picture from the one your newspaper article presented.
Talic et al claim to have screened 36,729 papers, but found only six on masks they considered eligible for inclusion. Yet an internet search reveals numerous relevant research articles. How can the authors have overlooked this, and how can their conclusion be true given the many other conflicting studies?
We dug a little deeper and found that several of the papers cited by Talic et al are telephone surveys covering multiple variables, with questionable methodology.
For example, one study investigated the effectiveness of mask-wearing in families in their homes of laboratory-confirmed Covid-19 cases in Beijing and concluded that face mask use was ’79 per cent effective in reducing transmission’.
Strangely, the paper contains a passage that seems to undermine the whole study: ‘As the compliance of UFMU (universal face mask use) would be poor in the home, there was difficulty and also no necessity for everyone to wear masks at home …’
This seems to imply that the use of face masks by family members in their households included in the study was sporadic and that therefore the study has no scientific merit.
Equally strange, one of six papers referenced in the Talic paper is the Danish RCT mask study, which the authors presumably included to support their conclusions, even though it doesn’t. In fact, the study was inconclusive (a difference of between 1.8 per cent and 2.1 per cent)
Even more peculiar, the Talic article is linked in the BMJ to an editorial published simultaneously which directly refutes the claim of a 53 per cent reduction in Covid incidence.
It says: ‘Face masks seem to have a real but small effect for wearer and source control, although final conclusions should await full reports of the trials from Bangladesh and Guinea-Bissau.
‘However, the quality of the current evidence would be graded – by GRADE (Grading of Recommendations, Assessment, Development and Evaluations) criteria – as low or very low, as it consists of mainly observational studies with poor methods (biases in measurement of outcomes, classification of PHSM – Public Health and Social Measures – and missing data), and high heterogeneity of effect size. More and better research are needed.’
How can such inconsistencies be overlooked by a senior editor of a quality broadsheet?
Signed
Professor David Seedhouse, BSc (Hons), PhD
Bruce Luffman
Sarah Goode, PhD
Alex Thorn
Simon Fletcher
Sandy French
Fiona Swan, LLB, Solicitor (Rtd.)
Monica Coyle
Daphne Havercroft, Project Management Professional (PMP)®
Phil Button, BSc, MBCS
Professor Chris Jesshope, BSc Hons (Mathematics), MSc (computer science), PhD (electronics)
Philip Morkel, Managing Director Engineering Services, Law Degree, MBA, S/W Project management
Tony Woodcock
Dr Damien Bush, MA, VetMB, Cert. SAS, MRCVS, RCVS, Recognised Advanced Practitioner Small Animal Surgery
Neil Sherry
Michael Welby
Shirley Dudfield
Maddy Conway
Peter Whitehead
Vanessa Peutherer, Author, Learning & Development Consultant (Health Care Ethics), RGN, ENG, ENB (Rtd)
Michael Philips, BSc (Hons) Mathematics
Edina Atkinson
Adam Mockett, BA (Hons)
Mike Davies, Project Manager (Rtd)
Alex Camm MPhil, CQSW
Susan James, FCILEX
Myra Forster-van Hijfte, DVM, CertVR CertSAM, DipECVIM, FRCVS
Dr. Jo-Ann van Eijck, Ph.D, Former Associate Professor at University of Hong Kong
Helen Myles, BSc (Hons) Maths and Psychology
November 28, 2021
Posted by aletho |
Deception, Fake News, Mainstream Media, Warmongering | Covid-19, The Guardian |
Leave a comment
reports from SA indicate that the virus is VERY mild
aside from all the breathless reporting about “MOAR SPIKE MUTATIONS!!” i have yet to see a single report with any actual clinical evidence that the newly branded omicron variant is anything other than less dangerous than delta was.
it’s just, to steal a wonderful quote “mutational stargazing.”
this makes sense. not only are we continuing to evolve AWAY from an what looks near certain to be a lab engineered virulence optimum, but this is the natural path of viral evolution.
delta was a deeply attenuated version of prior versions. it’s original CFR was around 0.1%. this rose sharply over the summer as vaccine fade hit and this rise affected the vaccinated and the unvaccinated alike, so it appears to be a property of the virus, not of the vaccines. it was also mirrored by all cause mortality and so appears to be a real rise in fatality, not a definitional artifact.
i will still bet dollars to doughnuts that it was the vaccines themselves that, by being leaky but semi-protective, drove this inverted gradient to hotter strains.
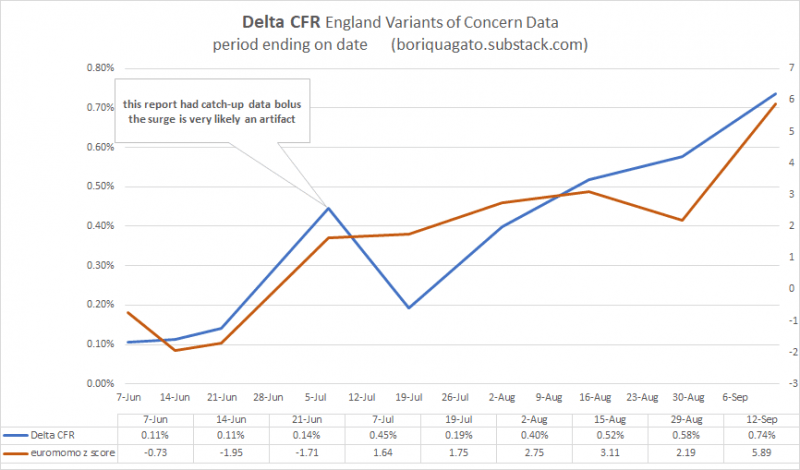
full discussion and data HERE.
a virus “wants” one thing: to spread. make a copy of me and pass it on. that’s the whole ballgame. harming the host and incapacitating them is maladaptive to this goal. mild viruses spread better. asymptomatic viruses spread best of all.
and that looks more and more like the case here. omicron looks milder than delta, especially than the souped up delta strains that emerged over the summer.
this is good news, not a reason for terror. the ideal outcome would be a virus with no symptoms and infinite spread that would immediately inoculate everyone.
primary symptoms appear to be lethargy. loss of taste and smell is largely absent.
ARTICLE
as this virus looks to outcompete delta, but with lower risk, the idea that we want to keep it out seems exactly wrong. this is the variant you want. more spread, considerably less risk, mostly asymptomatic, but will generate the real, sterilizing immunity that the vaccines do not.
this is how pandemics end, not how panics should begin.
watching the west once more lose its collective mind is just pathetic.
based on the early looks, this is not even a chipmunk in the road to swerve around, it’s the shadow of a chimpunk and it’s a less dangerous strain that the one we currently have and another even lower risk bite at the immunity apple.
whether it will follow delta in terms of vaccine mediated evolution toward hotter future strains is anyone’s guess (and certainly possible) but if it is, indeed, destined to do so, then that’s all the more reason to let it spread now.
“we should panic in case it turns out we need to panic” is simply not a basis for public health.
pandemics can and do end themselves and it’s become manifestly obvious that the vaccines developed here and pushed endlessly as panacea are of little to no help in that regard and quite a strong case to be made that they have made it, overall, worse for everyone, including the vaccinated.
boosters, lockdowns, and travel bans are not the way out. the generation of low risk natural herd immunity is.
it is long past time we stopped playing these stupid games.
the prizes we stand to win are not going to get any less stupid this time…
November 28, 2021
Posted by aletho |
Science and Pseudo-Science | Covid-19, COVID-19 Vaccine |
Leave a comment
I’m a voracious reader of Covid books but nothing could have prepared me for Scott Atlas’s A Plague Upon Our House, a full and mind-blowing account of the famed scientist’s personal experience with the Covid era and a luridly detailed account of his time at the White House. The book is hot fire, from page one to the last, and will permanently affect your view of not only this pandemic and the policy response but also the workings of public health in general.
Atlas’s book has exposed a scandal for the ages. It is enormously valuable because it fully blows up what seems to be an emerging fake story involving a supposedly Covid-denying president who did nothing vs. heroic scientists in the White House who urged compulsory mitigating measures consistent with prevailing scientific opinion. Not one word of that is true. Atlas’s book, I hope, makes it impossible to tell such tall tales without embarrassment.
Anyone who tells you this fictional story (including Deborah Birx) deserves to have this highly credible treatise tossed in his direction. The book is about the war between real science (and genuine public health), with Atlas as the voice for reason both before and during his time in the White House, vs. the enactment of brutal policies that never stood any chance of controlling the virus while causing tremendous damage to the people, to human liberty, to children in particular, but also to billions of people around the world.
For the reader, the author is our proxy, a reasonable and blunt man trapped in a world of lies, duplicity, backstabbing, opportunism, and fake science. He did his best but could not prevail against a powerful machine that cares nothing for facts, much less outcomes.
If you have heretofore believed that science drives pandemic public policy, this book will shock you. Atlas’s recounting of the unbearably poor thinking on the part of government-based “infectious disease experts” will make your jaw drop (thinking, for example, of Birx’s off-the-cuff theorizing about the relationship between masking and controlling case spreads).
Throughout the book, Atlas points to the enormous cost of the machinery of lockdowns, the preferred method of Anthony Fauci and Deborah Birx: missed cancer screenings, missed surgeries, nearly two years of educational losses, bankrupted small business, depression and drug overdoses, overall citizen demoralization, violations of religious freedom, all while public health massively neglected the actual at-risk population in long-term care facilities. Essentially, they were willing to dismantle everything we called civilization in the name of bludgeoning one pathogen without regard to the consequences.
The fake science of population-wide “models” drove policy instead of following the known information about risk profiles. “The one unusual feature of this virus was the fact that children had an extraordinarily low risk,” writes Atlas. “Yet this positive and reassuring news was never emphasized. Instead, with total disregard of the evidence of selective risk consistent with other respiratory viruses, public health officials recommended draconian isolation of everyone.”
“Restrictions on liberty were also destructive by inflaming class distinctions with their differential impact,” he writes, “exposing essential workers, sacrificing low-income families and kids, destroying single-parent homes, and eviscerating small businesses, while at the same time large companies were bailed out, elites worked from home with barely an interruption, and the ultra-rich got richer, leveraging their bully pulpit to demonize and cancel those who challenged their preferred policy options.”
In the midst of continued chaos, in August 2020, Atlas was called by Trump to help, not as a political appointee, not as a PR man for Trump, not as a DC fixer but as the only person who in nearly a year of unfolding catastrophe had a health-policy focus. He made it clear from the outset that he would only tell what he believed to be true; Trump agreed that this was precisely what he wanted and needed. Trump got an earful and gradually came around to a more rational view than that which caused him to wreck the American economy and society with his own hands and against his own instincts.
In Task Force meetings, Atlas was the only person who showed up with studies and on-the-ground information as opposed to mere charts of infections easily downloadable from popular websites. “A bigger surprise was that Fauci did not present scientific research on the pandemic to the group that I witnessed. Likewise, I never heard him speak about his own critical analysis of any published research studies. This was stunning to me. Aside from intermittent status updates about clinical trial enrollments, Fauci served the Task Force by offering an occasional comment or update on vaccine trial participant totals, mostly when the VP would turn to him and ask.”
When Atlas spoke up, it was almost always to contradict Fauci/Birx but he received no backing during meetings, only to have many people in attendance later congratulate him for speaking out. Still, he did have a convert in Trump himself, but by then it was too late: not even Trump could prevail against the wicked machine he had permissioned into operation.
It’s a Mr. Smith Goes to Washington story but applied to matters of public health. From the outset of this disease panic, policy came to be dictated by two government bureaucrats (Fauci and Birx) who, for some reason, were confident in their control over media, bureaucracies, and White House messaging, despite every attempt by the president, Atlas, and a few others to get them to pay attention to the actual science about which Fauci/Birx knew and care little.
Fortunately, we now have this book to set the record straight. It gives every reader an inside look at the workings of a system that wrecked our lives. If the book finally declines to offer an explanation for the hell that was visited upon us – every day we still ask the question why? – it does provide an accounting of the who, when, where, and what. Tragically, too many scientists, media figures, and intellectuals in general went along. Atlas’s account shows exactly what they signed up to defend, and it’s not pretty.
The cliche that kept coming to mind as I read is “breath of fresh air.” That metaphor describes the book perfectly: blessed relief from relentless propaganda. Imagine yourself trapped in an elevator with stultifying air in a building that is on fire and the smoke gradually seeps in from above. Someone is in there with you and he keeps assuring you that everything is fine, when it is obviously not.
That’s a pretty good description of how I felt from March 12, 2020 and onward. That was the day that President Trump spoke to the nation and announced that there would be no more travel from Europe. The tone in his voice was spooky. It was obvious that more was coming. He had clearly fallen sway to extremely bad advice, perhaps he was willing to push lockdowns as a plan to deal with a respiratory virus that was already widespread in the US from perhaps 5 to 6 months earlier.
It was the day that the darkness descended. A day later (March 13), the HHS distributed its lockdown plans for the nation. That weekend, Trump met for many hours with Anthony Fauci, Deborah Birx, son-in-law Jared Kushner, and only a few others. He came around to the idea of shutting down the American economy for two weeks. He presided over the calamitous March 16, 2020, press conference, at which Trump promised to beat the virus through general lockdowns.
Of course he had no power to do that directly but he could urge it to happen, all under the completely delusional promise that doing so would solve the virus problem. Two weeks later, the same gang persuaded him to extend the lockdowns.
Trump went along with the advice because it was the only advice he was fed at the time. They made it appear that the only choice that Trump had – if he wanted to beat the virus – was to wage war on his own policies that were pushing for a stronger, healthier economy. After surviving two impeachment attempts, and beating back years of hate from a nearly united media afflicted by severe derangement syndrome, Trump was finally hornswoggled.
Atlas writes: “On this highly important criterion of presidential management—taking responsibility to fully take charge of policy coming from the White House—I believe the president made a massive error in judgment. Against his own gut feeling, he delegated authority to medical bureaucrats, and then he failed to correct that mistake.”
The truly tragic fact that both Republicans and Democrats do not want spoken about is that this whole calamity did indeed begin with Trump’s decision. On this point, Atlas writes:
Yes, the president initially had gone along with the lockdowns proposed by Fauci and Birx, the “fifteen days to slow the spread,” even though he had serious misgivings. But I still believe the reason that he kept repeating his one question—“Do you agree with the initial shutdown?”—whenever he asked questions about the pandemic was precisely because he still had misgivings about it.
Large parts of the narrative are devoted to explaining precisely how and to what extent Trump had been betrayed. “They had convinced him to do exactly the opposite of what he would naturally do in any other circumstance,” Atlas writes, that is
“to disregard his own common sense and allow grossly incorrect policy advice to prevail… This president, widely known for his signature “You’re fired!” declaration, was misled by his closest political intimates. All for fear of what was inevitable anyway—skewering from an already hostile media. And on top of that tragic misjudgment, the election was lost anyway. So much for political strategists.”
There are so many valuable parts to the story that I cannot possibly recount them all. The language is brilliant, e.g. he calls the media “the most despicable group of unprincipled liars one could ever imagine.” He proves that assertion in page after page of shocking lies and distortions, mostly driven by political goals.
I was particularly struck by his chapter on testing, mainly because that whole racket mystified me throughout. From the outset, the CDC bungled the testing part of the pandemic story, attempting to keep the tests and process centralized in DC at the very time when the entire nation was in panic. Once that was finally fixed, months too late, mass and indiscriminate PCR testing became the desiderata of success within the White House. The problem was not just with the testing method:
“Fragments of dead virus hang around and can generate a positive test for many weeks or months, even though one is not generally contagious after two weeks. Moreover, PCR is extremely sensitive. It detects minute quantities of virus that do not transmit infection… Even the New York Times wrote in August that 90 percent or more of positive PCR tests falsely implied that someone was contagious. Sadly, during my entire time at the White House, this crucial fact would never even be addressed by anyone other than me at the Task Force meetings, let alone because for any public recommendation, even after I distributed data proving this critical point.”
The other problem is the wide assumption that more testing (however inaccurate) of whomever, whenever was always better. This model of maximizing tests seemed like a leftover from the HIV/AIDS crisis in which tracing was mostly useless in practice but at least made some sense in theory. For a widespread and mostly wild respiratory disease transmitted the way a cold virus is transmitted, this method was hopeless from the beginning. It became nothing but make work for tracing bureaucrats and testing enterprises that in the end only provided a fake metric of “success” that served to spread public panic.
Early on, Fauci had clearly said that there was no reason to get tested if you had no symptoms. Later, that common-sense outlook was thrown out the window and replaced with an agenda to test as many people as possible regardless of risk and regardless of symptoms. The resulting data enabled Fauci/Birx to keep everyone in a constant state of alarm. More test positivity to them implied only one thing: more lockdowns. Businesses needed to close harder, we all needed to mask harder, schools needed to stay closed longer, and travel needed to be ever more restricted. That assumption became so entrenched that not even the president’s own wishes (which had changed from Spring to Summer) made any difference.
Atlas’s first job, then, was to challenge this whole indiscriminate testing agenda. To his mind, testing needed to be about more than accumulating endless amounts of data, much of it without meaning; instead, testing should be directed toward a public-health goal. The people who needed tests were the vulnerable populations, particularly those in nursing homes, with the goal of saving lives among those who were actually threatened with severe outcomes. This push to test, contact trace, and quarantine anyone and everyone regardless of known risk was a huge distraction, and also caused huge disruption in schooling and enterprise.
To fix it meant changing the CDC guidelines. Atlas’s story of attempting to do that is eye-opening. He wrestled with every manner of bureaucrat and managed to get new guidelines written, only to find that they had been mysteriously reverted to the old guidelines one week later. He caught the “error” and insisted that his version prevail. Once they were issued by the CDC, the national press was all over it, with the story that the White House was pressuring the scientists at the CDC in terrible ways. After a week-long media storm, the guidelines changed yet again. All of Atlas’s work was made null.
Talk about discouraging! It was also Atlas’s first full experience in dealing with deep-state machinations. It was this way throughout the lockdown period, a machinery in place to implement, encourage, and enforce endless restrictions but no one person in particular was there to take responsibility for the policies or the outcomes, even as the ostensible head of state (Trump) was on record both publicly and privately opposing the policies that no one could seem to stop.
As an example of this, Atlas tells the story of bringing some massively important scientists to the White House to speak with Trump: Martin Kulldorff, Jay Bhattacharya, Joseph Ladapo, and Cody Meissner. People around the president thought the idea was great. But somehow the meeting kept being delayed. Again and again. When it finally went ahead, the schedulers only allowed for 5 minutes. But once they met with Trump himself, the president had other ideas and prolonged the meeting for an hour and a half, asking the scientists all kinds of questions about viruses, policy, the initial lockdowns, the risks to individuals, and so on.
The president was so impressed with their views and knowledge – what a dramatic change that must have been for him – that he invited filming to be done plus pictures to be taken. He wanted to make it a big public splash. It never happened. Literally. White House press somehow got the message that this meeting never happened. The first anyone will have known about it other than White House employees is from Atlas’s book.
Two months later, Atlas was instrumental in bringing in not only two of those scientists but also the famed Sunetra Gupta of Oxford. They met with the HHS secretary but this meeting too was buried in the press. No dissent was allowed. The bureaucrats were in charge, regardless of the wishes of the president.
Another case in point was during Trump’s own bout with Covid in early October. Atlas was nearly sure that he would be fine but he was forbidden from talking to the press. The entire White House communications office was frozen for four days, with no one speaking to the press. This was against Trump’s own wishes. This left the media to speculate that he was on his deathbed, so when he came back to the White House and announced that Covid is not to be feared, it was a shock to the nation. From my own point of view, this was truly Trump’s finest moment. To learn of the internal machinations happening behind the scenes is pretty shocking.
I can’t possibly cover the wealth of material in this book, and I expect this brief review to be one of several that I write. I do have a few disagreements. First, I think the author is too uncritical toward Operation Warp Speed and doesn’t really address how the vaccines were wildly oversold, to say nothing of growing concerns about safety, which were not addressed in the trials. Second, he seems to approve of Trump’s March 12th travel restrictions, which struck me as brutal and pointless, and the real beginning of the unfolding disaster. Third, Atlas inadvertently seems to perpetuate the distortion that Trump recommended ingesting bleach during a press conference. I know that this was all over the papers. But I’ve read the transcript of that press conference several times and find nothing like this. Trump actually makes clear that he was speaking about cleaning surfaces. This might be yet another case of outright media lies.
All that aside, this book reveals everything about the insanity of 2020 and 2021, years in which good sense, good science, historical precedent, human rights, and concerns for human liberty were all thrown into the trash, not just in the US but all over the world.
Atlas summarizes the big picture:
“in considering all the surprising events that unfolded in this past year, two in particular stand out. I have been shocked at the enormous power of government officials to unilaterally decree a sudden and severe shutdown of society—to simply close businesses and schools by edict, restrict personal movements, mandate behavior, regulate interactions with our family members, and eliminate our most basic freedoms, without any defined end and with little accountability.”
Atlas is correct that “the management of this pandemic has left a stain on many of America’s once noble institutions, including our elite universities, research institutes and journals, and public health agencies. Earning it back will not be easy.”
Internationally, we have Sweden as an example of a country that (mostly) kept its sanity. Domestically, we have South Dakota as an example of a place that stayed open, preserving freedom throughout. And thanks in large part to Atlas’s behind-the-scenes work, we have the example of Florida, whose governor did care about the actual science and ended up preserving freedom in the state even as the elderly population there experienced the greatest possible protection from the virus.
We all owe Atlas an enormous debt of gratitude, for it was he who persuaded the Florida governor to choose the path of focussed protection as advocated by the Great Barrington Declaration, which Atlas cites as the “single document that will go down as one of the most important publications in the pandemic, as it lent undeniable credibility to focused protection and provided courage to thousands of additional medical scientists and public health leaders to come forward.”
Atlas experienced the worst of the slings, arrows, and worse. The media and the bureaucrats tried to shut him up, shut him down, and body bag him professionally and personally. Cancelled, meaning removed from the roster of functional, dignified human beings. Even colleagues at Stanford University joined in the lynch mob, much to their disgrace. And yet this book is that of a man who has prevailed against them.
In that sense, it is easily the most crucial first-person account we have so far. It is gripping, revealing, devastating for the lockdowners and their vaccine-mandating successors, and a true classic that will stand the test of time. It’s simply not possible to write the history of this disaster without a close examination of this erudite first-hand account.
Jeffrey A. Tucker is Founder and President of the Brownstone Institute and the author of many thousands of articles in the scholarly and popular press and ten books in 5 languages, most recently Liberty or Lockdown.
November 28, 2021
Posted by aletho |
Book Review, Civil Liberties, Economics, Science and Pseudo-Science, Timeless or most popular | Covid-19, Florida, Human rights, United States |
Leave a comment
EARLIER this month Dr Byram Bridle, a Canadian viral immunologist whose faculty at the University of Ontario has disowned him for his repeated assertion that Covid-19 vaccines are not safe, gave a remarkable off-the-cuff interview to a reporter. Bridle starts by explaining the reasons why heavily vaccinated countries are experiencing high case rates, why adverse reactions are not being reported or diagnosed and discusses the overwhelming evidence for ivermectin as an ant-viral treatment for Covid where studies have been conducted correctly.
You can watch the full video below.
DR BYRAM BRIDLE: A recent study came out looking at 68 different countries and they plotted on a graph the case rate for Covid-19 and the vaccination rate in the country. And the more vaccinated the country is, the more problems they’re having with Covid-19. So these people have the vaccine. Remember all the antibody titers they’re showing, that’s in the blood, but these people, on average, are quite poorly protected in their upper airways. And it’s not the virus that’s deep down in the alveoli that gets transmitted to other people because of the dead airspace when we exhale. It’s the viral particles that are in the upper airways. So that’s why the vaccinated can spread this just as efficiently as somebody who’s completely unprotected. And so these vaccines on that basis, because they don’t come close to conferring sterilising immunity, they don’t properly protect the upper respiratory tract, they only confer about four and a half months of immunity, it’s absolutely 100 per cent impossible to achieve the goal of herd immunity with these vaccines. 100 per cent impossible.
What I’ve seen way too much of – and it does cause me very serious concern – is we’re seeing people who had cancers that were in remission or that were being well-controlled, and their cancers have gone completely out of control after getting the vaccine. And what we do know with the vaccine is the vaccine causes at least a temporary drop in T-cell numbers and those T-cells are part of our immune system, and they’re the critical weapons that our immune system has to fight off cancerous cells. So there’s a potential mechanism there. And all I can say is I’ve seen . . . I’ve had people contact me with way too many of these reports for me to feel comfortable. I do feel that that’s probably, I would say, my newest major safety concern. And it’s also the one that is going to be by far the most underreported on any adverse event database. Because if somebody’s had a cancer before the vaccine, there’s no way public health officials will ever link it to the vaccine. But what we’re seeing is oncology teams that had pushed the cancers into remission or keeping them well-controlled can no longer control them after the vaccine.
So we know in Canada it’s very upsetting, because in Canada we have a system that will never, never detect problems with these vaccines – that’s why we’ve always had to rely on other countries. Like with the AstraZeneca vaccine, we told Canadians that the AstraZeneca vaccine was 100 per cent safe, despite the fact that 12 European countries had paused the programme to look for potential links to the blood clotting, potentially fatal blood clotting. And we were told as Canadians that we didn’t have to worry because ours was from a . . . they announced that the problem was associated with a single batch from a single production facility in Europe and ours was coming from India and therefore it didn’t apply to us. The European Medicines Agency will tell you that was never the case. And of course, then eventually, after there were Canadians that did die and many that did have to be treated for the blood clots, then we finally admitted that it was a problem.
And that’s how our system . . . our system is never going to work, because this is the thing. First of all, we’re not informing people when they get the vaccine that they’re to report any unusual medical condition up to eight weeks after receiving a dose of the vaccine. And then the attending physician is required to, by law, to report anything unusual. Most physicians are not. And now some of them are . . . many don’t, because they don’t want to contradict the current narrative. And the College of Physicians and Surgeons of Ontario has turned out to be incredibly tyrannical and are crushing many physicians and threatening many who don’t go with this narrow public health narrative. Many also can’t get their submissions done because they’re onerous. So, for example, British Columbia can take up to 40 minutes to submit one of these reports, and you can imagine if there’s an Emergency Room physician who sees five people in a shift that come in with problems and have recently been vaccinated, they can’t afford to spend hours on that shift, reporting it, right?
So there’s many reasons why people aren’t reporting to the physicians, and there are many reasons why the physicians aren’t reporting to the local Medical Officer of Health. And that’s the next step is, if a physician submits it, it doesn’t necessarily go into our database, it goes to the local Medical Officer of Health. This is the thing: the physicians are not supposed to make a determination of whether they think the medical condition that’s occurred after the vaccine is or is not related to the vaccine. They’re not supposed to make that determination. The local Medical Officers of Health are. And as you can imagine, with the huge bias that exists there, the majority of them, we’re seeing unusually high percentages of these reports that do get submitted being rejected at the level of the local Medical Officer of Health. And then from there, the ones that they do approve go to the Public Health Agency of Canada and then they could be filed into our adverse event database. But because of that, because of all the filtering that’s going on, this is the problem. We’re not getting accurate numbers.
So yes, a statistician, of course, could be looking for these. But if you don’t get accurate numbers reported, you can do all the analysis you want, it’s not going to be accurate, right? Your analysis is only as accurate as the data, the raw data you have to work with.
A D-dimer test is definitely a good one to do, because it can be suggestive of micro clots, which could be an indicator of blood clotting. But yeah, we’re finding that most physicians won’t do it. And we’re also finding a shortage, actually, of the blood collection tubes that are needed to do that as well.
Yeah, yeah, no, this is a virus. But ivermectin has clear-cut antiviral properties. For example, it has multiple mechanisms of action, but one is it inhibits the binding of the spike protein on the virus to these receptors that we have on the cells of our lungs. And yeah, what’s interesting is a lot of countries . . . so, that’s what’s frustrating for me as a vaccine developer, I knew that there was going to be no outlet for the vaccines if there were effective early treatment strategies. So I followed the science for the early treatment strategies, and I saw that the studies were flawed early on.
For example, a lot of the studies that were being done were being done in countries where things like ivermectin were available over the counter. So in other words, they were testing their treatment group, which was getting a defined amount of ivermectin and comparing it to a control group which had an undefined amount of ivermectin. So essentially comparing ivermectin treatment to ivermectin treatment, right? And then they showed there was no benefit. Well, of course not. If you’re comparing, you know, a treatment group to a treatment group.
And so when the science has been done properly, there’s an overwhelming [body] of scientific data showing that it works. And so even though I love vaccines, I couldn’t help but wonder why we were providing initially this authorisation for interim use, what we call emergency use in the United States, because we had clear, effective early treatments. I have worked with many physicians. These things clearly work. In fact, a lot of the countries that are having the most success, like, for example, a lot of the low income countries have had no choice. I mean, look, they’ve been left to take the leftovers for the vaccines. They can’t afford a lot of expensive treatments. So they have been relying on these effective early treatment strategies using repurposed generic drugs that are really cheap, and they’ve had a huge success.
So, for example, Egypt is a good example. Egypt, you know, Egypt has a three per cent vaccination rate. Three per cent of their eligible population is double vaccinated compared with Canada, which is at around 64 or 66 per cent. And they have 14 cases of Covid-19 per 100,000 people per day on average, whereas we have about 570 cases per day, so vastly higher.
And this is what people are seeing. A recent study came out looking at 68 different countries, and they plotted on a graph the case rate for Covid-19 and the vaccination rate in the country. And the more vaccinated the country is, the more problems they’re having with Covid-19. And when you look at these countries that have low vaccination rates, they’ve been relying on effective early treatment strategies.
So for example, with Egypt, I didn’t realise, but I asked that question to my collaborators, ‘What is Egypt doing right that we’re not doing here in North America?’ They sent me the official treatment protocol for Covid-19. Do you know what the number one thing is that they go to first? [It] is hydroxychloroquine and number two is ivermectin.
And if you look at Israel – Israel has the highest vaccination rate in the world, right? And the Delta variant is completely out of control, which is why they’ve been administering the third dose, why they’ve committed to a fourth dose. And with these numbers I was telling you, so they have the highest vaccination rates. So again, keep this in mind so as to understand – Egypt: three per cent vaccination rate, 14 cases per 100,000 of the population per day. Israel is at over an 80 per cent vaccination rate and has over 5,000 cases right now per day.
So these things work best as an early treatment strategy, so they should be administered. The sooner you administer them, the better the outcome. So we’ve had physicians – and I know these people and they’re good friends of mine – who have been absolutely destroyed for using ivermectin with their patients, and they’ve kept their patients out of the hospital, they’ve kept them out of the ICU. I find this exceptionally frustrating because I keep getting criticised for raising my concerns about the vaccines and harms, and I have physicians coming at me and saying, ‘Well, if only you saw on the front lines what happens to people who die from Covid and how terrible it is.’ And yes, it’s awful, and I feel terrible for all of them. But the other thing that I point out is it’s estimated that more than half the people that have died in this pandemic would be alive today if we had accepted these early treatment strategies. That’s the reality, and I’ve seen it with every physician who has administered this. They talk about our ICUs being overrun, but every physician that I have worked with – and I’ve worked with many who have used these effective treatment strategies – they’ve kept their patients out of the ICU. They don’t go to the ICU and they don’t die.
Do you realise that the way we’ve been treating patients is they go to the hospital and if they aren’t sick enough to go on a respirator, they typically get sent home and it’s, you know, take fluids and some of these other . . . maybe some aspirin. It’s basically what were they like to call in medicine, ‘watchful waiting’, which means, ‘we’re going to do nothing’, right? And you literally have to wait till you’re sick enough to come in and basically be put in the ICU and put on a respirator.
That’s not how you treat disease, right? The earlier you intervene, the better the outcome. And we have these early treatment strategies, and I think it’s no coincidence the only one we’ve approved in Canada is called remdesivir. It does have genuine safety issues and does virtually nothing for Covid-19. But it’s on patent and there’s tons of money that can be made. These other ones are dirt cheap. Ivermectin, you can treat somebody for about a dollar a day. So they’ve been using it to great effect in all these low income countries. But in North America, we’ve refused to adopt these strategies.
And you have to understand, and they even talk about safety issues. Well, one of the things is, so, there’s rare cases of safety issues associated with using the veterinary form, and that’s simply because of calculation errors – people making simple mathematical errors when trying to convert to the human dose. And the reality is that ivermectin is on the list for the World Health Organisation of one of the 50 most needed drugs in the entire world, has an unbelievable safety record. It’s used worldwide to effectively treat all these parasitic diseases. It was approved by Health Canada in 2018 to treat exotic parasitic diseases when Canadians are travelling. And so there’s absolutely no excuse.
…
Dr Bridle: My own physician, honestly, criticised me, saying I’m giving out this messaging, talking about patients of hers that died.
I respectfully pointed out that I’m also on the front lines and I’m trying to deal on a daily basis with family members of people who have died from the Covid-19 vaccines. And so I’m seeing these horrible deaths as well on the other side.
And the difference to me is, had they not rejected these effective early treatment strategies, at least half of the patients that died in their practices would be alive today.
So I’m sorry, I don’t have a lot of patience for these physicians. And I’m just going to point out one thing as well that’s important for the general public to know. I usually don’t ever, ever criticise anybody’s expertise in their particular area of work. But we’re in unique times. And so I think the public needs to be aware.
We put a lot of faith in our physicians. The average family physician knows almost nothing about immunology and certainly about vaccines. People forget vaccinology is a sub-discipline of immunology. The average family physician in Canada gets between five and ten lectures in their first year on immunology, of which a tiny fraction of that is going to be dealing with vaccines.
They are not immunologists, they are not vaccinologists and they’re ignoring the vaccinologist here in Canada. They are promoting the vaccines and the reality is they don’t understand the science, and they do not have a deep enough understanding, on average, to understand the science and to understand the debates that are going on.
Interviewer: If information has been deliberately suppressed about these treatments, that would be a crime, seeing that people are dying?
Dr Bridle: Yes. Yes.
Interviewer: Doctor, will we see a national debate, like with top scientists on this subject ever in Canada? Like their side for pro, and our side? Do you think we’ll ever see that in Canada?
Dr Bridle: I and my colleagues have been open to that for months, many months. I would love to see it done. The public should be insisting on it, like the old-fashioned good scientific debates.
I would argue scientists can talk about the science. We can put aside our emotions. We can talk about it respectfully. I would argue what I would like to see happen is have a team – if it’s too big, it gets a little unwieldy – so I’d say between three and five scientists and/or physicians who want to debate both aspects of the Covid-19 policies and then have it moderated by somebody. And it has to be very public.
And that’s what I keep pointing out to the public. People who keep arguing that those of us who have legitimate concerns are wrong, providing misinformation, that we’re lying and that we don’t know what we’re talking about, have to keep asking themselves why then are many of us standing there in the arena like the gladiators of old? We’re standing in the arena, we’re waiting. None of their champions will step forward. None. We’ve tried it.
So we tried this in Ontario with (their Premier) Doug Ford. It was attempted in Alberta. It was attempted in Saskatchewan, where their premiers were also invited to have these open scientific discussions.
Nobody so far – and I know I’ve issued invitations. Every single person who attacks me I invite them to come on and talk publicly. I was even being interviewed once and live in the chat somebody was trolling the whole talk.
It was interesting. The person who was interviewing me stopped and invited the person to come on. They logged off pretty quickly. And that’s what we’re seeing over and over again. It’s remarkable.
I’ve asked thousands of people, not one person, not even one, in all these months has been willing to talk openly, publicly about the science and medicine underlying Covid-19. It’s exceptionally frustrating.
Even my own colleagues at the university who have attacked me, there are 83 of them, about that number, who signed a letter to the public saying that I was lying to the public, providing misinformation.
Do you realise some of these individuals were just down the hallway from me, in the same hallway, just a few doors down? None, not one of them, not one of those people was ever willing to talk to me on the phone, in a Zoom meeting or come to my office – and I have an open door policy and I invited many of them to do so – not one person.
And then, even after they signed that off, saying that I was giving misinformation, I had written a scientific document to outline the science that I’d been talking about, because this was birthed from a short interview that I gave on the radio, where I expressed concerns that the messenger RNA vaccines might be linked to the heart inflammation that was occurring in young people. And then I was attacked on that.
I wrote a document with all the science because, of course, I was not able to deliver all of my scientific arguments in that short interview.
People argued to the public, ‘You realise he only told you half the story.’ And I laugh about that because I say, ‘Well, you’re giving me far too much credit because I didn’t even get to deliver one per cent of the story.’
They’re trying to mean that I didn’t get to the other side of the story. No, there was so much more science, so many more mechanisms of action, of potential harm of these things.
And after I wrote that document, this letter was written by my colleagues. You realise that of those who I was able to get a straight answer from, none of them had even read my science. None of them had even bothered to see what my arguments were for my position. This is what’s happening right now, and the censorship is extreme it’s really unbelievable.
Interviewer: Some of your colleagues, they also said that it doesn’t alter DNA. Would you care to comment on that?
Dr Bridle: Yeah. So when it comes to the DNA, there isn’t sufficient data to … my personal opinion is that it’s not substantially altering the DNA.
All I can tell you is it was thought that human cells did not have a type of protein that’s needed to convert the messenger RNA in the vaccine into DNA. It turns out we do actually have these types of proteins present. So it’s theoretically possible.
Personally, I would think that it’s probably not a substantial issue, but theoretically possible. So as this is theoretically possible, I would argue as a scientist that it would be worthwhile investigating that – doing the research just to alleviate our concerns, people’s concerns, about that.
That’s the thing, people ask these questions and as you see that there’s theoretical possibilities for these happening, that used to be the scientific basis for then conducting the research and definitively answering people’s questions. So many of the questions that you have, I can’t definitively answer because we’ve lost this whole concept of conducting research to address the tough questions.
Interviewer: What I find interesting with what you’re saying is what I’m seeing, very clearly, is you’re confronting a talking point, not a science. And let me illustrate what I mean by that.
You ask a doctor about all this and what’s their answer if you really push them? ‘Well, we’re following the advice of x, y, z and they’re following the science that we trusted?’ Right? You go to the level above them, same thing. You go to the level above them, same thing.
Dr Bridle: We’ve tried, as scientists …
Interviewer: I understand that. You guys will talk to science because you’re working with it. The other side is purposely convoluting science from a talking point.
Dr Bridle: Yes.
Interviewer: I honestly wonder if they have a science. My wife and I survived …
Dr Bridle: Well, at this point I can tell you, as a scientist – that’s why I’m willing to debate anybody on it – they don’t have the science on their side. That’s very clear. And in fact, you no longer need to understand the science, you just need to understand the contradictions that are coming.
Because, this is the thing, the reason why people like Dr Palmer and myself can stand up and talk off the cuff without any script here is because we’re speaking the truth. We’re speaking based on our knowledge, and we don’t have to keep track of a story when we’re speaking the truth.
We don’t have to make sure that what we’re saying today matches what we said at last week’s rally or the one before that. But the public health narrative has become so discombobulated now that they’re constantly contradicting themselves.
And there’s so many examples that I could give you. But let’s take one, for example. I encourage people now to start taking headlines from the mainstream media from months ago, which had people like myself censored, and line them up side-by-side with headlines that they have today.
‘So a great example is this whole issue of the vaccine mandate and the fact that, you know, what are we telling people right now? If you have one dose of the vaccine, you’re lumped in with the unvaccinated. You’re dangerous, you’re the same as somebody who has been unvaccinated, you’re unprotected and you’re going to kill everybody else, right?
We know from the very get-go, the two-dose regimen was proclaimed to have 95 per cent effectiveness. So, this is the thing, a lot of people who are accepting this current messaging about the ‘one dose doesn’t count’ have forgotten about the one-dose summer.
Remember when Trudeau (the Canadian Prime Minister) was pushing and all we were hearing about was the one-dose summer? So in Canada, the world was watching us in bewilderment and wondering what the basis was for us going from the approved three or four-week interval, depending on whether it was the Pfizer or Moderna vaccine, to a four-month interval.
And if you recall, the reason why we could go for the one-dose summer and not worry about getting people two doses is because we were told one dose was 95 per cent effective.
‘A lot of you don’t realise this. If you don’t believe me, you can go on the Health Canada website right now and look. They will have on there that the one dose of the Pfizer vaccine is 95 per cent effective.
So now you have to start asking yourself, using their own messaging: If one dose is 95 per cent effective and two doses is 95 per cent effective, then why are the people with one dose being lumped in with those who are unvaccinated? Why was that OK then, when trying to justify going to a four-month interval, which had no scientific basis?
But now those same people who are sitting with one dose are told, ‘No, no, no. It’s not 95 per cent effective, it’s the equivalent of being unvaccinated altogether.’
This is where we’re getting to. So on that basis alone, that’s what I’m saying is, it’s become blatantly obvious. You don’t have to understand the science. They are not following the science, they’re contradicting themselves over and over and over again.
…
DR BYRAM BRIDLE: There’s been a remarkable number of young people who have died for no apparent reason. And in many cases, we can’t confirm their vaccination status. But I’ve been particularly concerned about the number of varsity athletes at our universities who have been dying completely unexpectedly and suddenly. And the only thing that I can tell you – and I don’t know whether they were or were not vaccinated – well, actually, I can’t tell you when they were vaccinated. What I can tell you is that no varsity athlete in Ontario can participate in a varsity team without being vaccinated. They weren’t allowed exemptions.
INTERVIEWER: My point on that example was simply this: if you’re following the science, that first statement that that head doc released would never be said.
BRIDLE: Yes.
INTERVIEWER: You would say, ‘We don’t know.’
BRIDLE: Exactly. That’s exactly, yes.
INTERVIEWER: But that’s the way they’re reporting it tells you . . .
BRIDLE: As you heard from me, yeah.
INTERVIEWER: . . . their complete agenda.
BRIDLE: As you heard from me. I won’t say definitively that it’s because of the vaccine. I’m a scientist, I’m open to that possibility that there is some other underlying condition with any individual case. But there’s too many of these to not investigate properly. Absolutely.
INTERVIEWER: And if anybody’s paying attention, that whole approach should really put your guard up.
BRIDLE: Yes.
INTERVIEWER: You should realise there’s something drastically wrong with public health officials who would talk with that kind of language.
BRIDLE: Yeah, well, look at the language. So, another contradiction is . . . so, for example, at my university, our president hosted the local Medical Officer of Health who declared the whole reason why the vaccine mandate made so much sense is that there is essentially no such thing as a breakthrough infection. And that’s still being claimed by many, although their ability to claim that continues to be eroded. But that was the idea, and they cited like a 0.003 per cent breakthrough infection rate, so essentially zero, meaning you’re completely protected.
And when our President was asked about that recently, she actually created quite a furore on our campus, because she completely contradicted the messaging that they had just given. Well, the reason why, of course, they still have to mask and physically distance is because, hey, you know, it’s well known that people who are vaccinated can still get infected, still get Covid and transmit the virus. And in fact, there’s very good immunological reasons why people who are vaccinated can still transmit the virus and the scientific data that is emerging is showing that they can transmit at least as efficiently as somebody who has no immunity whatsoever.
And the reason is, is because when we put the vaccine in the shoulder, we’re tricking our bodies into thinking that it’s what we call systemic infection. And so, the problem is that is where your body wants to protect the most is the blood, because if a pathogen gets into the blood it can disseminate throughout the whole body. And so we got all these antibodies in the blood.
So, the one place in our respiratory system where these antibodies will spill over into, if you’re trying to protect against a systemic infection, are the lower airways. And that’s because you just think about gas exchange. There’s barely a physical barrier between the alveolar space and the blood vessels to allow that ready air exchange, which also means it’s very easy for a pathogen that gets deep into the lungs – so that would be what we call pneumonia – for that pathogen to get into the blood. So we put antibodies in the lower airways if we think we have a systemic infection. But we aren’t getting proper antibody protection in the upper airways like we would if we were naturally infected. So these people that have the vaccine, yeah, remember all the antibody titers they’re showing, that’s in the blood. But these people, on average, are quite poorly protected in their upper airways. And it’s not the virus that’s deep down the alveoli that gets transmitted to other people, because of the dead airspace when we exhale, it’s the viral particles that are in the upper airways. So that’s why the vaccinated can spread this just as efficiently as somebody who’s completely unprotected.
And so these vaccines, on that basis, because they don’t come close to conferring sterilising immunity, they don’t properly protect the upper respiratory tract. They only confer about four and a half months of immunity. It’s absolutely 100 per cent impossible to achieve the goal of herd immunity with these vaccines. 100 per cent impossible. For these companies it would be such a quick and easy and cheap study to do, and they could definitively rule this problem in or out. And whenever there’s such easy to do research to be done and they won’t do it, that for me is always a red flag.
INTERVIEWER: Yeah, exactly why isn’t that happening?
DR BYRAM BRIDLE: Yes. All I can say is, again, we’re not being provided with accurate data. So it’s hard to answer any of these questions to do with, you know, what’s actually due to COVID, what’s due to other things? And how we’re defining these things is crazy. Like I said, we’re not even defining somebody who’s vaccinated until they’re 14 days out from their second dose. The second dose is serving as a booster, right? And so typically, the immune response would be peaking actually about five to ten days after receiving that. So we’re actually taking people who would theoretically be at the absolute peak of a vaccine-induced immunity, and we’re calling them not fully vaccinated, for example.
And so for example, if people were to die in that time frame, even if it was linked to the vaccine, it’d be linked as somebody who was not fully vaccinated having died. So it’s very difficult with all these kind of nuances that are going on. All I can say really is what we do know is that the problem of Covid, the number of cases has been dramatically overestimated, but to an unknown degree, because of the way we’ve misused the PCR test. And we know that the problems associate with the vaccines have been grossly underestimated, but to an unknown degree.
And so until we have accurate numbers for these – which I can’t see we’re going to have at any time soon unless we completely change the way we’re monitoring these things – we’re not going to be able to come up with accurate assessments as scientists of . . . you know, with these kind of questions. But the issue was at the beginning, or the problem was, people kept arguing that this could have between a 1 and 10 per cent fatality rate, infection fatality rate, meaning for every 100 people who were infected with the virus between 1 and 10 would die. But the thing is, as we never knew what the proper denominator was, how many people were getting infected – we still don’t know, because again, like I mentioned, there’s many of us . . . well, in fact, just right here, there was an individual who has gone now, but showed me his test result. He had had a positive Covid test result almost a year and a half ago, when he showed me his antibody response for the spike protein, it’s higher, way higher than the average person who’s been vaccinated at the peak, at the peak of their antibody response. So there’s somebody who clearly acquired immunity naturally. And we’re not tracking these people at all, because in many cases where people have actually been infected they didn’t even know it and have natural immunity.
We’re running this clinical trial where we’re evaluating natural acquisition of immunity. We’re finding a huge number of people who never realised that they were sick have clear evidence of immunity against this virus. So that means that for those individuals they were infected but this was not a pathogen for them and they recovered without, you know, without developing disease. And so we have no idea – and we now know this is much more common than we accepted at the beginning – but we have no idea just how common, right?
So the point is, we still don’t know the full extent of the denominator. But when it was updated in February, what was published at that time was that the infection fatality rate was 0.15 – so not even 1 per cent like we were being told, but 0.15 per cent – and that was for the entire population. And if you took out those who were 70 years and older, it dropped to 0.05 per cent. So, just to put that into perspective, a bad flu season would be at 0.1 per cent.
So again, if you go out of the high risk, the highest risk demographic, those over 70. And we’re actually dealing with a problem that is less fatal than the annual flu. And especially when we start talking about children – we’ve had one infant in BC who died. We’re, you’re talking about taking these vaccines down now, in the next phase, to five-year-olds and then all the way down to six months of age. And when you start getting down to under ten years of age, virtually nobody has died. And when you look at the flu, it’s far more dangerous for these individuals.
And if you want to look at another one, respiratory syncytial virus, which we live with – far more dangerous to young people. And this is where even pregnant or breastfeeding women are being told, encouraged, to get vaccinated to protect their infants. It’s crazy. It’s all based on this . . . it’s easy to make people feel that infants are very fragile, very fragile human beings, which in some ways they are. But when it comes to SARS-CoV-2, this was presented today: the younger you are, the fewer receptors you express in your respiratory system that this virus can use to latch on to your cells. And in fact, when you get down into the infants, they’re quite resistant to infection with this virus. And that’s why we haven’t been seeing deaths among that population.
So it’s very unusual, with any other infectious disease you always have two peaks: the frail elderly and the very young. And it’s very clear why, because the frail elderly . . . well, as we get older, our immunological function declines so we in essence become somewhat immunosuppressed as we get older. And then on the very young side, our immune systems don’t fully mature until we’re 16 years old. Still, some components of the immune system maturing as young teenagers. So we’re dealing with less mature immune systems, immune systems that aren’t fully mature as we get into the youngest population. So that’s why we usually see these peaks in the oldest and the youngest. But SARS-CoV-2 is not like that, it’s very unusual in the sense that, yes, infants are relatively immature in terms of their immunological functioning, but they’re physically very resistant to infection with this virus.
So this is all crazy to be encouraging breastfeeding women to be vaccinated, to protect their infants. Their infants are already naturally protected. And as we go down and we start vaccinating six-month-old breastfeeding infants, what we’re doing is we’re bypassing the natural protection they have from the virus when we inject these vaccines, where we start getting their body to manufacture the spike protein. And again, I can’t emphasise enough. The spike protein is not the inert target that we were hoping it would be for the immune system. It has all kinds of biological activities in our bodies that can potentially be harmful.
And what people have to understand is that the receptor that that spike protein can bind to in our children and infants is expressed at the same concentration internally as in adults. And that’s because that protein doesn’t exist to serve as a receptor for the virus, it actually exists to serve basic physiological processes such as regulating blood pressure and so on. So, they’re naturally protected from infection from SARS-CoV-2, but when we put the vaccines in, they’re at least as susceptible as adults to all the harms.
November 28, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular, Video | Canada, Covid-19, COVID-19 Vaccine |
Leave a comment
The last few days we have heard some alarming reports about how the Northern Territories of Australia are treating their indigenous communities.
Tweets and videos have emerged claiming aboriginal people are being removed from their land and sent to “quarantine centres”, allegedly to protect them from the virus.
Some representatives of the community have sent out videos asking for “international aid”, and claiming Aboriginal communities are being placed under “martial law” and people are being removed from their homes “at gunpoint”
At a protest against the measures, one aboriginal elder was violently arrested by officers witnesses claim were not wearing ID badges.
Another elder, June Mills, posted a video to facebook expressing concern about how difficult it is to get information out of the locked down communities. She says she has heard that the army is “removing people against their will”, ending with the emotive cry “they are killing us!”
Australia has been so rapidly descending into a fascist hellhole that none of this, if true, would be at all surprising. The very fact they have a huge quarantine camp they unironically refer to as “The Centre for National Resilience” should be a massive red flag for everyone.
Michael Gunner, Chief Minister of the Northern Territories, was a caricature of wide-eyed zealotry in a recent press conference. When asked whether vaccine mandates might alienate some people, even those already vaccinated he said:
If you support or give comfort to anybody who argues against the vaccine, you are an anti-vaxxer, I don’t care what your personal vaccination status is.”
The phrase “give comfort too” should alarm people, because it’s only ever used in warlike settings, discussing treason and collusion. “Giving comfort to the enemy“.
In another press conference, Gunner also announced a “hard lockdown” in aboriginal communities, meaning people are not allowed to leave their homes except for medical treatment or if required by law. Adding that people are being “removed” to quarantine centres in military trucks. Not just people diagnosed with “covid”, but “close contacts” too:
Police are going door to door in Aboriginal communities to “intensively engage” with those who do not want the “vaccine”.
All this is being sold in the mainstream as “concern” for communities which could be “extra vulnerable”.
Voices on social media – who are totally real, and not at all shills there to control the narrative – are claiming strict measures are necessary to protect indigenous Australians from Covid, because it would rip through their communities “like syphilis did to the Native Americans”. There is, so far, very little evidence to support this fear-mongering.
However, written statements, allegedly from people detained, are emerging online saying they are being well taken care of, and that “irresponsible” social media posts are “hurting people”.
Amnesty UK issued a press release condemning the moves, but this was swiftly countermanded by Amnesty Australia, and dismissed as “disinformation” in the press and by Michael Gunner as “conspiracy theorising” from “tinfoil hat-wearing tossers”.
Some other Australian states are already building quarantine camps specifically for Aboriginal communities.
South Australia announced a tender for these camps last week, with press coverage underlining they would be only for those people who are “unable to isolate at home”.
Whether genuinely well-intentioned or not, it can certainly be argued this is an example of massive governmental overreach, especially for a virus that is at worst a bad seasonal flu.
It’s a convoluted and complex situation, with the real facts being hard to establish. Whatever the reality, it’s a situation that bears close watching.
November 26, 2021
Posted by aletho |
Civil Liberties, Science and Pseudo-Science | Australia, Covid-19, COVID-19 Vaccine, Human rights |
Leave a comment
With natural exposure immunity and early outpatient treatment and when combined with no reports of increased lethality, the WHO’s reaction of generating panic toward “Omicron” is causing needless fear and panic. So too with the Biden administration’s newly imposed travel restrictions, which will achieve nothing and will once again disrupt trade and violate human rights.
The WHO has said that the Omicron variant can spread more quickly than other variants. Likely true. The virus is behaving just like how viruses behave. They are mutable and mutate and via Muller’s ratchet, we expect this to be milder and milder mutations and not more lethal ones given the pathogen seeks to infect the host and not arrive at an evolutionary dead-end.
The virus will mutate downward so that it can use the host (us) to propagate itself via our cellular metabolic machinery. The Delta has shown us this: it is very infectious and mostly non-lethal. Especially for children and healthy people. So is the WHO panicking the globe needlessly? Is this Covid-19 February 2020 once again?
The problem with South Africa as is with Australia and New Zealand and even island nations like Trinidad is that it has low natural immunity to SAR-Cov-2. This is because, as we witnessed over the last year and more, if you lock down your society too long and too hard, you deny the nation and population from inching closer to population-level herd immunity. And you have no economy or society from which to reemerge. You devastate your society for a pathogen that is largely harmless to the vast majority of people especially children.
Moreover, governments asked us for two weeks to flatten the curve to help prepare hospitals so that they can tend to surges and other non-Covid illnesses. We as societies gave our governments 2 weeks, not 21 months. They failed to tend to the non-Covid illnesses and we locked down the healthy and well (children and young and middle aged healthy persons) while failing to properly protect the vulnerable and high-risk persons such as the elderly. We failed and it was like killing fields in our nursing homes.
This failure rests on public health messaging and government. Additionally, what did our governments in the US, Canada, UK, Australia etc. do with the tax money for the hospitals and PPE etc.? Hospitals must be prepared by now. Governments have failed! Not the people. The Task Forces have failed, not the people.
These nations thought that they could stay locked down and wait for a vaccine. This is a reasonable view though I was against lockdowns as they would and did cause crushing harms on especially poor persons and children. The problem is there was an opportunity cost because the vaccine we were waiting on was suboptimally developed without the proper safety testing or assessment of effectiveness.
We have data that the Pfizer vaccine loses 40% of antibodies per month, meaning in 3 months post-shot, you have low effective vaccinal immunity. We see it clearly playing out now whereby you got to tamp down spread with the draconian lockdowns, but you did it at the cost of natural immunity. That is the opportunity cost. So we spent on getting the vaccine and it cost us natural immunity and thus herd immunity.
For example, the vaccine has failed to stop infection and spread against Delta. We have research findings by Singanayagam et al. (fully vaccinated individuals with breakthrough infections have peak viral load similar to unvaccinated cases and can efficiently transmit infection in household settings, including to fully vaccinated contacts), by Chau et al. (viral loads of breakthrough Delta variant infection cases in vaccinated nurses were 251 times higher than those of cases infected with prior strains early 2020), and by Riemersma et al. (no difference in viral loads when comparing unvaccinated individuals to those who have vaccine “breakthrough” infections and if vaccinated individuals become infected with the delta variant, they may be sources of SARS-CoV-2 transmission to others) that reveal the vaccines have very suboptimal efficacy.
This situation of the vaccinated being infectious and transmitting the virus has also emerged in seminal nosocomial outbreak papers by Chau et al. (HCWs in Vietnam), the Finland hospital outbreak (spread among HCWs and patients), and the Israel hospital outbreak (spread among HCWs and patients). These studies have also revealed that the PPE and masking were essentially ineffective within the healthcare setting. All of the HCWs were double-vaccinated yet there was extensive spread to themselves and their patients.
In addition, Nordström et al. (vaccine effectiveness of Pfizer against infection waned progressively from 92% day 15-30 to 47% day 121-180, and from day 211 and onwards no effectiveness), Suthar et al. (a substantial waning of antibody responses and T cell immunity to SARS-CoV-2 and its variants, at 6 months following the second immunization), Yahi et al. (with Delta variant, neutralizing antibodies have a decreased affinity for the spike protein, whereas facilitating antibodies display a strikingly increased affinity), Juthani et al. (higher numbers of patients with severe or critical illness in those who received the Pfizer vaccine), Gazit et al. (SARS-CoV-2-naïve vaccinees had a 13-fold increased risk for breakthrough infection with the Delta variant, and substantially elevated risk of symptomatic Covid and hospitalization), and Acharya et al. (no significant difference in cycle threshold values between vaccinated and unvaccinated, asymptomatic and symptomatic groups infected with Delta) collectively reveal the poor efficacy and even negative efficacy of the Covid vaccines. Levine-Tiefenbrun et al. reports that the viral load reduction effectiveness declines with time after vaccination, “significantly decreasing at 3 months after vaccination and effectively vanishing after about 6 months.”
As an example, the Swedish study (retrospective with 842,974 pairs (N=1,684,958) is particularly alarming for it shows that while the vaccine provides temporary protection against infection, the efficacy declines below zero and then to negative efficacy territory at approximately 7 months, underscoring that the vaccinated are highly susceptible to infection and eventually become highly infected (more so than the unvaccinated). A further example emerges from Ireland whereby reporting suggests that the Waterford city district has the State’s highest rate of Covid-19 infections, while the county also boasts the highest rate of vaccination in the Republic (99.7% vaccinated). Reports are that the U.S. Covid-19 deaths for 2021 surpassed the deaths from 2020, leading some to state that “more people have died from COVID-19 in 2021, with most adults vaccinated and nearly all seniors), than in 2020 when nobody was vaccinated.”
Thus these nations that locked down and stayed that way are in a quandary for they do not know what to do now. If you open you will get surges in infection. Where is the money that was to go to hospital preparation? Did governments embezzle and steal and misappropriate the money for the hospitals remain still not prepared?
We have a lot of natural immunity in the US, e.g. near 65-70% of the population. The open states (those that did not lock down too long and too hard and opened quickly) will likely do very well with this Omicron or any new variant. This also is the power of natural immunity.
And we need not forget the potency of the overlooked ‘innate’ immunity with the innate antibodies and innate natural killer cellular compartment. This innate response is particularly potent in children (our first line of defense against pathogens) and is what has spared children from Covid and how children typically stave off pathogens, especially young children still laying down immunological memory.
Moreover, there is no reporting of increased virulence/lethality of this new Omicron variant. As yet this will remain the case based on Delta and prior variants. There are no guarantees but we operate based on risk and all things point to the same for this new variant.
Just because there is a wave in SA does not mean that there will be waves in the US or Israel or other places with greater natural immunity. This was the prize of letting people enjoy day-to-day living. The nations that have ended lockdowns are likely to move past this new variant scare, and be fine. This is more of an overreaction by the WHO and governments and much ado about nothing.
Dr Alexander holds a PhD. He has experience in epidemiology and in the teaching clinical epidemiology, evidence-based medicine, and research methodology. Dr Alexander is a former Assistant Professor at McMaster University in evidence-based medicine and research methods; former COVID Pandemic evidence-synthesis consultant advisor to WHO-PAHO Washington, DC (2020) and former senior advisor to COVID Pandemic policy in Health and Human Services (HHS) Washington, DC (A Secretary), US government; worked/appointed in 2008 at WHO as a regional specialist/epidemiologist in Europe’s Regional office Denmark, worked for the government of Canada as an epidemiologist for 12 years, appointed as the Canadian in-field epidemiologist (2002-2004) as part of an international CIDA funded, Health Canada executed project on TB/HIV co-infection and MDR-TB control (involving India, Pakistan, Nepal, Sri Lanka, Bangladesh, Bhutan, Maldives, Afghanistan, posted to Kathmandu); employed from 2017 to 2019 at Infectious Diseases Society of America (IDSA) Virginia USA as the evidence synthesis meta-analysis systematic review guideline development trainer; currently a COVID-19 consultant researcher in the US-C19 research group
November 26, 2021
Posted by aletho |
Science and Pseudo-Science | Australia, Covid-19, COVID-19 Vaccine, New Zealand, South Africa, United States |
Leave a comment
 Since the very beginning of the covid panic, the narrative has been this: implement severe lockdowns or your population will experience a bloodbath. Morgues will be overwhelmed, the death total toll will be astounding. On the other hand, we were assured those jurisdictions that do lock down would see only a fraction of the death toll.
Since the very beginning of the covid panic, the narrative has been this: implement severe lockdowns or your population will experience a bloodbath. Morgues will be overwhelmed, the death total toll will be astounding. On the other hand, we were assured those jurisdictions that do lock down would see only a fraction of the death toll.
Then, once vaccines became available, the narrative was modified to “Get shots in arms and then covid will stop spreading. Those countries without vaccines, on the other hand, will continue to face mass casualties.”
The lockdown narrative, of course, has already been thoroughly overturned. Jurisdictions that did not lock down or adopted only weak and short lockdowns ended up with covid death tolls that were either similar to—or even better than—death tolls in countries that adopted draconian lockdowns. Lockdown advocates said locked-down countries would be overwhelmingly better off. These people were clearly wrong.
Undaunted by the increasing implausibility of the lockdown narrative, the global health bureaucrats are nonetheless doubling down on forced vaccines—as we now see in Austria—and we continue to be assured that only countries with high vaccination rates can hope to avoid disastrous covid outcomes.
Yet, the experience in sub-Saharan Africa calls both these narratives into question: Africa’s numbers have been far, far lower than the experts warned would be the case.
For example, the AP reported this week that in spite of low vaccination rates, Africa has fared better than most of the world:
[T]here is something “mysterious” going on in Africa that is puzzling scientists, said Wafaa El-Sadr, chair of global health at Columbia University. “Africa doesn’t have the vaccines and the resources to fight COVID-19 that they have in Europe and the U.S., but somehow they seem to be doing better,” she said….
Fewer than 6% of people in Africa are vaccinated. For months, the WHO has described Africa as “one of the least affected regions in the world” in its weekly pandemic reports.
Yet disaster for Africa has long been predicted for several reasons even beyond the availability of vaccines. For instance, it is known that lockdowns are especially impractical in the poorest parts of the world. This is because populations in places with undeveloped economies can’t simply sit at home and live off savings or debt. Rather, these people must go out into the world and earn a living on a day-to-day basis. Starvation is the alternative. Moreover, much of this work is done in the informal economy, so enforcing lockdowns becomes especially difficult.

It was also assumed covid would be especially deadly in Africa due to the fact many large households live in small housing units.
But that “conventional wisdom” flies in the face of the reality of covid in Africa, which is that there have been fewer deaths.
The “experts” have groped around, looking for possible explanations.
Some sources, for example, insist that the low death totals are only an artifact of incomplete reporting on covid infections and that “a lack of good qualitative data was the issue.”
But Richard Wamai at Northeastern University rejects the claim it’s all about case reporting, and says that “local systems for reporting deaths in Africa make it difficult to hide COVID-19 casualties.” In a paper for the International Journal of Environmental Research and Public Health, Wamai and his coauthors conclude, “[T]here is no evidence that COVID-19 mortality data is less accurately reported in Africa than elsewhere” and “While the true picture of infections and mortality in the continent has yet to fully emerge, the quality of data for other diseases, such as HIV/AIDS, indicates that Africa has the capacity to collect and report valid disease surveillance data.”
In any case, the World Health Organization reports that covid deaths in Africa make up only 2.9 percent of covid deaths, while Africa’s population is 16 percent of the global total. Africa’s covid total could double or triple, and Africa would still be faring far better than Europe and the Americas.
Wamai et al. also note that at this point “[i]t is likely that SARS-CoV-2 has already been widely disseminated through Africa… If so, widespread infection is likely to also result in widespread natural immunity.”
In other words, continued claims by health officials—both in Africa and elsewhere—that mass death is right around the corner with the “next wave” look increasingly implausible.
It looks increasingly likely that the lack of covid mortality in Africa is not due to a data issue nor a situation in which covid has been “contained” up until now. So then why is Africa doing so much better than the wealthy West?
Naturally, the advocates of forced lockdowns and coerced vaccines would prefer to ignore this issue altogether, but the undeniable reality of Africa’s experience has forced mainstream researchers to publicly admit the many ways that many factors can explain covid’s prevalence beyond vaccination rates and mask mandates.
For instance, mentioning that obesity is an important factor in covid mortality has in the past been likely to get one savaged in the media for “fat shaming.” Yet the Africa situation has forced the well informed to admit that yes, obese populations clearly suffer more from covid. In Africa, not surprisingly, we find that obesity rates are far below those found in North America and Europe.
Other possible explanations forwarded as reasons for Africa’s situation include past exposure to other coronaviruses, youthful populations, fewer patients lacking zinc and vitamin D, past use of the Bacillus Calmette-Guérin vaccination, climate, genetic background, and parasite load. In addressing the African “enigma” one group of researchers in the journal Colombia medica dared even suggest it’s possible—although not conclusively shown at this point—that “a mass public health preventive campaign against COVID-19 may have taken place, inadvertently, in some African countries with massive community ivermectin use.”

In the West, however, the media drumbeat around covid has consistently been “Shut up, stay home, get jabbed, and stop doubting the experts on forced vaccines.” Fortunately, however, the African situation has forced many researchers to ask inconvenient questions.
In fact, it’s amazing Africa has not been overcome by mass death considering that covid lockdowns and covid “mitigation” measures have contributed to the impoverishment and mass starvation on the continent. Or as Germany’s DW News puts it, “Measures put in place to slow the spread of the novel coronavirus are pushing millions of people in Africa into severe hunger.” And as Wamai notes, “[S]ome of the excess deaths in Africa “can be attributed not to the disease, but to lockdown measures that cut off access to medical care for other illnesses.”
But Africa hasn’t gotten the bloodbath that was promised, and as one Nigerian put it, “They said there will be dead bodies on the streets and all that, but nothing like that happened.”
November 26, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | Africa, Covid-19, COVID-19 Vaccine |
Leave a comment
Ed Humpherson, Director of U.K. Statistics Authority the Office for Statistics Regulation (OSR), has written to Emma Rourke, Director of Health Analysis at the Office for National Statistics (ONS) to criticise the agency for a report it put out in October claiming that: “Between January 2nd and September 24th 2021, the age-adjusted risk of deaths involving coronavirus (COVID-19) was 32 times greater in unvaccinated people than in fully vaccinated individuals.”
As James Wells, a statistician who served as head of the ONS UK trade team until 2019, pointed out when he wrote to the OSR to complain about the report earlier this month, this statistic uses data from January 2nd to September 24th 2021, which includes the bulk of the winter deaths at a time when almost no one was vaccinated. This skews the implied vaccine effectiveness, as a fair comparison would only include periods when a significant proportion of the country was vaccinated.
In Mr Humpherson’s letter to Ms Rourke he wrote:
The headline in the publication is the age adjusted risk of deaths involving COVID-19 for vaccinated and unvaccinated groups for the period January 2nd to September 24th. This was also the key message in the main tweet associated with the publication. Focusing on the headline figure has been unhelpful and has undermined the more helpful analysis provided later in the report. The headline figure is based on a time period driven by data availability. While the age-standardised mortality rates for deaths involving COVID-19 are consistently lower for people who have received two vaccinations, the size of the difference varies enormously depending on the time frame chosen. The data cover a period when very few people had two doses of vaccination, to a period when the majority of the adult population had two doses (data taken from gov.uk on 24 November 2021 show second dose uptake for age 12 and over in England was 0.8% on January 10th 2021 and 77.4% by September 24th 2021). It also covers a period when case rates varied significantly as well as the levels of natural immunity in the population…
Given the analysis carried out, more should have been done to highlight the uncertainty associated with the headline figure… I would urge you to take the focus off the headline figure in any future publications.
The truth is that statistics are being spun like this all the time by Government and others during the pandemic to bolster the preferred narrative. It’s just on this occasion the effort was so egregious and prominent that it couldn’t be ignored.
November 26, 2021
Posted by aletho |
Deception, Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine, UK |
Leave a comment


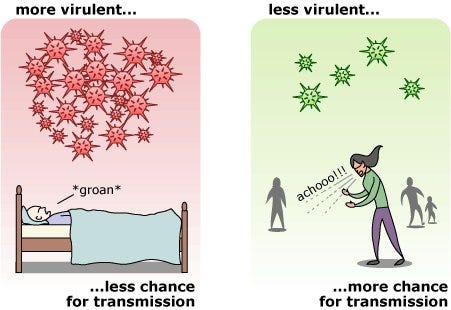

 Aletho News
Aletho News
{kind=link}