Australian Doctors Are Complicit In Experimentation On The Population
By Dr. Judy Wilyman | Principia Scientific | October 16, 2021

It is the ‘education’ and regulation of doctors that is preventing doctors from practising medicine with integrity in 2020-21.
The Government Therapeutic Goods Administrator (TGA) of Drugs/Vaccines in Australia states that COVID19 vaccines are:
- Experimental and include new untested genetic technology. Hence these drugs only have provisional approval and are not full approved for use in humans.
- The vaccines are not safe. Millions of injuries have been recorded by global government regulators including – anaphylaxis, thrombosis, and coagulation disorders (blood clots), infertility, heart problems (myocarditis and pericarditis), neurological damage (cognitive decline), strokes, paralysis, convulsions, seizures and well over 100,000 deaths.
- There are on average more deaths per day due to the COVID vaccines than to COVID-19 disease itself.
- The vaccines are ineffective – they do not prevent you getting or dying from COVID-19 disease, and they do not prevent transmission of the virus in the community. Hence, they are a drug and not a ‘vaccine’ under the WHO’s definition of a vaccine.
- They have only been tested to see if they reduce the symptoms and not to see if they prevent disease.
- They are unnecessary because 99.9% of people under 70 develop immunity through mild or asymptomatic infection. Our immune system develops natural herd immunity in the community through this exposure and the most detrimental action that any government can take is to quarantine healthy asymptomatic people. This hinders the control of infectious diseases in the community. Hence, Sweden did not lockdown its population and the WHO did not provide any evidence that asymptomatic people were a risk to the community in March 2020 when they used this strategy for the first time in history.
- The injection is not specific for COVID-19 disease and the synthetic spike protein that is produced by our cells upon exposure to any coronavirus is toxic to the human body. This includes the development of autoimmune diseases, blood clots and infertility.
Did you see this information reported in the mainstream media? No. Welcome to 2021 where the medical-industry uses framed and manipulated statistics, emotional labels, and anecdotal evidence in the mainstream media to inform you about any drug that they have labelled a ‘vaccine.’
The removal of both scientific evidence and balanced discussion of vaccines in the media has occurred over decades, and we now have a situation where labels and biased information are being used to manipulate your thinking about these drugs. Drugs that are being mandated for HEALTHY people in genetically diverse populations.
This fraudulent promotion of a medical intervention was cemented in 2009 when a government board was set up in Australia to regulate doctors on the “accepted” science for vaccine promotion.
This Federal government agency is called the Australian Health Practitioners Regulatory Authority (AHPRA) and it is both a government agency and an Australian incorporated business (ABN 78 685 433 429).
In other words, this board controls the knowledge doctors can promote on vaccines and it influences the design and promotion of government vaccination policies. This board has the power to de-regulate doctors and health professionals who make a different risk assessments of vaccines to that provided by this government regulatory board.
Medication for healthy people affects their quality of life and it is doctors who are trained to assess the medical literature for risks and benefits. The AHPRA board has a serious conflict of interest in the regulation of doctors’ knowledge on vaccines, and doctors cannot speak the truth to power if they can lose their livelihoods for doing so.
The risks of vaccines associated with our genetics are now being described as “antivaccination material” and doctors are threatened with de-registration by AHPRA for providing this medical literature to their patients. This includes contraindications to vaccines that have been practiced for 40+ years but have now been arbitrarily removed.
Hence, doctors are now violating the first principle of medicine because they cannot promote their patients best interest first. That is, drugs/vaccines must be given to individuals with advice regarding their own individual circumstances and genetics. This is a key factor in health outcomes with respect to drugs and when this is violated doctors are no longer promoting health in the community. They are promoting sickness and death because many illnesses are linked to our family history and genetics.
The Australian government has now indemnified doctors to give these experimental injections to their patients – injections that are documented to cause serious known and unknown harm in patients. Taxpayers (we) will be paying for our doctors to inflict this harm (and death) on patients without fully informed consent due to government mandates that remove our jobs and right to travel if we refuse.
Over the last few decades doctors have been “educated” in pharma-funded medical schools with industry-funded science. They are taught that anyone who discusses the ingredients of vaccines (drugs) or the serious risks of vaccines, is an “antivaxxer” and a “conspiracy theorist”. This same opinion is provided to the public in the corporate-sponsored mainstream media to denigrate any scientific discussion of the risks of these drugs that are given to healthy people.
Mainstream media has always been a tool to manipulate public behaviour and when the US Congress removed liability from pharmaceutical companies for any harm caused by any drug labelled a “vaccine” in 1986 (because they were paying millions of dollars in compensation for deaths and injuries), this enabled big pharma to minimise the risks of these drugs and to exaggerate the benefits (“life-saving products”) – without providing evidence for these claims.
In 2021 this dismissive ridicule by authorities reached a new low when the Western Australian Premier, Mark McGowan, disrespectfully told ~5,000 WA parents and grandparents at a rally opposing mandatory jabs for jobs, to “Grow a brain” and he stated that “this is about medicine and saving lives”. This statement by this Premier is simply untrue when you ignore the genetics of the population.
High school science students can tell the Premier that a mandatory drug/vaccine, in a genetically diverse population, will cause death and sickness in a significant proportion of the population. Mark McGowan should be removed from his role as Premier for his contempt for the people he serves and for putting the public’s lives are risk with false health information.
Politicians, media, and doctors are using labels to convey a ‘belief’ about vaccines and to stigmatise critical thinking, and this is done without providing any supportive evidence for the implied meanings the words are given. This strategy has been used to support the expansion of national vaccination programs from 1986 – 2021.
Since 1986 ‘beliefs’ that are not evidence-based have been promoted by the media, politicians and doctors by using the following words to promote public health policy:
Vaccines – drugs that have ‘rare’ side-effects and are ‘necessary to control infectious diseases.’ Both claims are untrue.
Infectious diseases – re-labelled as ‘vaccine-preventable diseases’ since 1986 to imply that they can be prevented with a vaccine.
Vaccination programs – falsely labelled as ‘immunisation programs.’ It is known that many vaccinated people do not get immunity after a vaccine is given and they still get the disease.
Catch-Up Schedules – They are not catch-up schedules because most older Australians did not have these vaccines and were never at risk from these diseases.
Antivaxxer – a derogatory term used to describe an educated parent/professional that discusses the risk-benefit analysis of vaccines or ingredients of vaccines. Knowledge of these criteria are necessary to promote ‘healthy’ outcomes from vaccines, yet they are ridiculed.
Conspiracy Theory – derogatory term used to dismiss the serious conflicts of interest in every aspect of global health policy designed by the WHO/GAVI alliance and national vaccination policies designed by governments.
This is a political situation, and it is the influence of corporate money in the political and economic decisions of governments that has led to doctors, governments and the media collaborating to commit a serious crime against their populations by falsely advertising an experimental genetic technology as a ‘vaccine’.
People, including health professionals, are walking into their own deaths and illnesses, due to the false and misleading health information that is being provided by the powerful medical-industry complex to politicians.
This corporate health model has monopolised doctors, industry-funded research institutions, politicians, and the mainstream media to educate the public with ignorance about the risks of vaccines. A situation described as agnotology in the academic literature and if doctors were not gagged by AHPRA (their government/corporate regulatory board) it would not have been possible to violate their medical ethics and commit this crime against humanity that will destroy the genetic fabric of society.
I cannot do it anymore

In an open letter, an employee of German public broadcaster ARD is critical of one and a half years of Corona coverage: Ole Skambraks has worked as an editorial assistant and editor at the public broadcaster for 12 years.
BY OLE SKAMBRAKS | multipolar magazine | 14. Oktober 2021
I can no longer remain silent. I can no longer silently watch what has been going on for a year and a half now within my organization, a public service broadcaster. Things like “balance”, “social cohesion” and “diversity” in reporting are principles embedded in the statutes and media state contracts. Today, the exact opposite is happening. There is no true discourse and exchange in which all parts of society can come together and find common ground.
From the beginning, I felt that public service broadcasting should fill precisely this space: promote dialogue between advocates of measures and critics, between people who are afraid of the virus and people who are afraid of losing their basic rights, between vaccination supporters and vaccination sceptics. For the past year and a half, however, the space for discussion has narrowed considerably.
Scientists and experts who were respected and esteemed before Covid, who were given space in public discourse, are suddenly labelled cranks, tinfoil hat wearers or Covidiots. As an oft-cited example, consider Wolfgang Wodarg, a medical specialist in several fields, an epidemiologist and a long-time health politician. Until the Covid crisis, he was also on the board of Transparency International. In 2010, as Chair of the Council of Europe Health Committee, he exposed the influence of the pharmaceutical industry in the swine flu pandemic. At that time, he was granted the opportunity to express his opinion on public service broadcasting, but in times of Covid this is no longer possible. His voice has been replaced by that of so-called fact-checkers, who seek to discredit him.
Paralysing consensus
Instead of an open exchange of opinions, a “scientific consensus” was proclaimed, that must be defended. Anyone who doubts this and demands a multidimensional perspective on the pandemic, will reap indignation and scorn.
The same pattern is at work in the newsrooms. For the last one and a half years, I have no longer been working in the daily news business, which I am pleased about. In my current position, I am not involved in decisions about which topics are treated and how. Here, I describe my impressions from editorial conferences and an analysis of the reporting. For a long time I did not dare to leave the role of observer, the supposed consensus seemed too absolute and unanimous.
For a few months, I have been venturing out onto the ice, making some critical remarks here and there in conferences. This is often followed by a shocked silence, sometimes a “thank you for pointing it out” and every so often a lecture on why it is not true. This has never resulted in any reporting.
The result of one and a half years of Covid-19 is an unparalleled division in society. Public service broadcasting has played a major role in this. It is increasingly failing in its responsibility to build bridges between the camps and to promote exchange.
It is often argued that the critics are a small, negligible minority, which, for reasons of proportionality, cannot be accommodated to any great extent. This argument should have been retired at least with the Swiss referendum on Covid-19 measures. Despite the lack of free exchange of opinions in mass media in that country too, the votes cast went only 60:40 in favour of the government. (1) With a proportion of 40%, can you talk about a small minority? It also turned out that the Swiss Government had tied Covid-related financial support to the vote, which might have influenced some to tick “Yes” on the ballot.
The developments of the Covid crisis are taking place on so many levels, affecting all parts of society, and thus we clearly need more space for a free debate – certainly not less.
In this context, it is less revealing which topics are being discussed in public service media, than what is not being discussed. The reasons for this are many and need to be subject to honest internal scrutiny. It could be helpful to look at some titles published by the media scientist and former MDR broadcasting adviser Uwe Krüger, for example his book “Mainstream – Warum wir den Medien nicht mehr trauen” (“Mainstream — why we no longer trust the media”).
In any case, it takes courage to swim against the current in conferences where such topics are discussed. Often those who can put forward their arguments in the most eloquent way will get their message across but, if in doubt, the editorial team will decide, of course. Very early on, those critical of the Government’s Covid-19 measures were labelled right-wingers. Which editor will still dare to voice similar ideas?
Open questions
Thus the list of inconsistencies and open questions, which have gone largely unreported, is very long:
- Why do we know so little about “gain of function research” (which aims at making viruses more dangerous to humans)?
- Why does the new Infection Protection Act state that the basic right to bodily integrity and the inviolability of one’s home may be restricted henceforth – even without an epidemic situation?
- Why must people who have already had Covid-19 still get the jab, even though they are at least as well protected as those who are vaccinated?
- Why are we not talking about ”Event 201” and the global pandemic exercises held shortly before the spread of SARS-CoV-2 — at all, or only in the context of conspiracy theories? (2)
- Why was the internal document from the German Federal Ministry of the Interior — a document which was known to the media and in which the authorities were asked to create a “shock effect” to underscore the impact of the Covid-19 pandemic on human society — not published in full and discussed publicly?
- Why is the study by Professor Ioannidis on survival rates (99.41% for people under 70) not featured in the headlines, while the fatally flawed, inflated figures produced by Imperial College were (in the spring of 2020, Neil Ferguson foresaw half a million Covid-19 deaths in the United Kingdom and more than 2 million in the United States)?
- Why does it say, in a document produced for the German Federal Ministry of Health, that Covid-19 patients stood for no more than 2% of the burden of hospitals during 2020?
- Why does Bremen have the by far the highest incidence (113 as at 04/10/21) and at, the same time, by far the highest vaccination rate in Germany (79%)?
- Why were payments of 4 million euro paid into a family account belonging to EU Health Commissioner Stella Kyriakides, who was responsible for concluding the first EU vaccine contracts with pharmaceutical companies? (3)
- Why are people suffering severe vaccine injury not featured to the same extent as people with severe Covid-19 disease were in 2020? (4)
- Why is no one disturbed by the irregular way of counting “breakthrough infections” in vaccinated people? (5)
- Why does the Netherlands report clearly higher volumes of side effects of the Covid-19 vaccines than other countries?
- Why has the efficacy description of the Covid-19 vaccines published on the Paul-Ehrlich-Institut website been changed three times in the last few weeks? From “Covid-19 vaccines protect against infection with the SARS-CoV-2 virus” (on 15 August 2021), via “Covid-19 vaccines protect against severe forms of infection with the SARS-CoV-2 virus” (on 7 September 2021), to, finally, “Covid-19 vaccines are indicated for active immunization to prevent the Covid-19 disease caused by the SARS-CoV-2 virus” (on 27 September 2021). (6)
A couple of these points warrant a closer look.
“Gain of function” and “Lab leak”
As for “gain of function research” — research aiming at making viruses more dangerous, as was done at the Institute of Virology in Wuhan, China, and financed by the United States — so far, I have not heard or read anything substantial. This type of research is done in so-called Biosafety Level 4 Laboratories, where work has been carried out for decades to see how animal viruses can be altered to make them dangerous to humans as well. So far, ARD and ZDF have given this topic a wide berth — despite the obvious need for a debate. One question worth exploring could be: Do we, as a society, want such research to be carried out?
There are numerous reports on the “lab leak theory” – the assumption that SARS-CoV-2 originated in a lab. It is worth noting that last year, this idea was immediately labelled a conspiracy myth. Alternative media investigating this were banned from social media such as YouTube and Twitter and the information was deleted. Scientists who supported this theory found themselves under massive attack. Today, the “lab leak theory” is at least as plausible as the bat transmission theory. The American investigative journalist Paul Thacker published the results of his meticulous research in the British Medical Journal. Commenting on this, Dr. Ingrid Mühlhauser, professor of health sciences at Hamburg University writes:
“Step by step, he [Thacker] reveals how members of an American lab group deliberately concocted a conspiracy theory to disguise their lab accident at Wuhan as a conspiracy theory. This myth is supported by respected journals such as The Lancet. Science journalists and fact-checker services accept the information without any reflection. Participating scientists keep mum, either out of fear, or to avoid running the risk of losing their standing or research grants. For more than a year now, Facebook has blocked posts that question the natural origin of SARS-CoV-2. If the lab accident theory is confirmed, then ZDF and other media will have defended conspiracy theories.”
Ivermectin and alternatives to vaccination
For months now, it has been clear that effective and cheap treatments do exist for Covid-19, but their use is not allowed. The data on this is unequivocal. But the pseudoscientific disinformation campaigns against these medications are indicative of the state of medicine today. Hydroxychloroquine is a drug known for decades and used routinely against malaria and rheumatic disorders. Last year, the drug was suddenly deemed dangerous. The statement by then-President Donald Trump that hydroxychloroquine would be a “game changer” did the rest to discredit the medication. The political reasoning no longer allowed a scientific debate on HCQ.
In the spring, the catastrophic situation in India caused by the spread of the Delta variant was widely reported in the media (then still referred to as the Indian variant). But the fact that India rather quickly brought the situation under control, and that the use of Ivermectin in large states such as Uttar Pradesh had a decisive role in this, was not deemed newsworthy. (7)
Ivermectin was granted a temporary authorisation in the Czech Republic and Slovakia for treating Covid-19 patients. This was at least reported by the MDR, albeit with a negative slant.
In its report on possible medications, Bayerischer Rundfunk failed to even mention Ivermectin. As for hydroxychloroquine, only negative studies were cited, omitting all studies with positive results.
In the summer of 2020, lab tests showed that the molecule Clofoctol was also effective against SARS-CoV-2. Until 2005, the antibiotic drug was sold in France and Italy under the commercial names of Octofene and Gramplus. The French authorities repeatedly blocked the Pasteur Institute in Lille from launching a study with Covid-19 patients. At the beginning of September, after several attempts, the first patients were recruited.
Why are the health authorities taking such a strong stand against treatments, which have been available since the beginning of the pandemic? I would have liked to see some investigative research by the ARD here! It has been made clear that the new Covid vaccines could qualify for emergency use authorisation (EUA) only because there was no officially recognised treatment for SARS-CoV-2.
This is not about celebrating any one Covid miracle drug. My aim is to highlight facts which have not been given due consideration. From the outset, the message given in public discourse was that vaccination was the only way out. The WHO even went so far as to change the definition of “herd immunity”, implying that it can only be achieved by vaccination and no longer by previous infection, as was previously the case.
What about if the road chosen is a dead end?
Questions on vaccine efficacy
Data from countries with a particularly high vaccination rate show that infection with SARS-CoV-2 also in fully vaccinated people is more rule than exception. Dr. Kobi Haviv, Director of the Herzog Hospital in Jerusalem, reports that between 85% and 90% of severe cases in his intensive care unit are patients who have had two jabs. (8)
As regards Israel as a whole, the journal Science writes: “On 15 August, 514 Israelis were admitted to hospital with severe or critical Covid-19 disease … out of these 514 persons, 59% were fully vaccinated. Out of those vaccinated, 87% were 60 years or older.” Science quotes an Israeli government adviser, who explains: “One of the great stories coming out of Israel [is]: ‘The vaccines work, but not well enough’.”
It is also now evident that, with the Delta variant, vaccinated people carry (and spread) the same viral load as unvaccinated people.
What has this data situation brought about in Germany? — A lockdown specifically for unvaccinated people or, put somewhat euphemistically: the “2G rule”. In fact, society is being divided into two classes. Vaccinated people regain their freedom (as they do not risk endangering others), whereas unvaccinated people (who do risk endangering others) must undergo tests, and pay for them out of their pocket, and will no longer receive sick pay if quarantined. Moreover, employment bans and dismissals on the grounds of vaccination status are no longer out of the question, and health insurance funds may impose less favourable rates on the unvaccinated in the future. Why this pressure on unvaccinated people? This has no foundation in science and is damaging to our society.
Antibodies produced by vaccination wane after only a few months. A look at Israel shows that after the second jab, there will be a third for the whole population, and then a fourth as recently announced. Those who fail to get a booster shot after six months will lose their status as immune and thus their “Green Pass” (the digital Covid-19 pass introduced in Israel). In the United States, President Joe Biden is talking about Covid-19 booster shots every 5 months. Marion Pepper, immunologist at the University of Washington, questions this strategy, explaining to The New York Times that repeated stimulation of the innate immune response can lead to a phenomenon called “immune fatigue”.
It is a little discussed fact that natural infection allows a person to develop clearly stronger immunity. “Ultrapotent antibodies” or ”super immunity” have been found in people who were infected with SARS-CoV-2 during the last year. These antibodies react against more than 20 different mutations of the virus and remain for longer than antibodies acquired via vaccination.
After all, Health Minister Jens Spahn has now declared that proof of antibodies is also to be accepted. But to be officially recognized as immune you still have to be vaccinated. Who can understand this logic? A CNN interview with Dr. Anthony Fauci, Director of NIAID (under the NIH, the National Health Institutes) clearly illustrates the absurdity of the situation. People with natural immunity are still not a consideration in the minds of the politicians!
I know a physician who is desperately trying to get an answer from the health authorities and the RKI to this problem: One of her patients presents an IgG antibody titer value of 400 AU/ml — clearly more than many vaccinated people. As her Covid-19 infection occurred more than six months ago, she has lost her immune status. The answer was: “Give her the jab!” — which the physician will not do, considering the titer value.
A lack of basic journalistic understanding
The way out of the pandemic touted by our politicians and the media turns out to be a permanent vaccine subscription. Scientists advocating a different Covid approach are not able to reach out via public service media, as demonstrated again by the sometimes defamatory reporting on the video action #allesaufdentisch. Instead of discussing the content of the videos with the parties concerned, experts were sought out to discredit the campaign. By doing this, public service commit the very same error which they hold against #allesaufdentisch.
Der Spiegel journalist Anton Rainer opined in the SWR interview about the video action, that these are not interviews in a classical sense: “In principle you see two people agreeing with each other.” Listening to the reporting by my broadcaster gave me stomach pains, and I was very annoyed by the lack of basic journalistic understanding of the need to let those with opposing views have their say. (9) I made my concerns known to those concerned and the editorial team by email.
A typical comment in conferences is that a topic has “already been covered”. For example, when I brought up the high likelihood of underreporting of vaccine side effects. Yes, sure, the topic was discussed with in-house experts, who – no surprises here – concluded that there was no underreporting. “Opposing views” will be discussed here and there, but are rarely given a human face in such a way that broadcasters actually speak with people who hold critical views.
Critics under pressure
The most vocal critics must count on house searches, prosecution, account suspensions, transfers or dismissal, or even referral to psychiatric care. Even if they hold opinions you do not share — this has no place in a state subject to the rule of law.
In the United States, it is already being discussed whether criticising science should be labelled a hate crime. The Rockefeller Foundation has announced a grant of 13.5 million dollars to censor misinformation in the health field.
WDR television broadcasting director Jörg Schönenborn declared that “facts are facts and they hold true”. If that was so, how is it then possible that scientists behind closed doors argue incessantly and even strongly disagree on some quite basic issues? As long as we are not making that clear, any assumption of supposed objectivity will lead to a dead end. We can only hope to edge closer to “reality” – and that is only possible with open exchange of ideas and scientific knowledge.
What is happening now is no honest fight against “fake news”. Rather, we are left with the impression that any information, evidence, or discussion deviating from the official narrative is suppressed.
A recent example is the factual and scientifically transparent video by IT specialist Marcel Barz. By analysing raw data, Barz was able to establish that the actual figures on excess deaths, hospital occupancy rates as well as infections did not correspond to those gleaned from the media and politicians in the last year and a half. He also demonstrates how you can present a perfect image of a pandemic using such data, and explains why he feels this is dishonest. After three days and 145,000 views, the video was deleted from YouTube (and reinstated only Barz after objected, and many others protested). The stated reason: “medical misinformation”. This begs the question: Who decided this, and on what grounds?
The fact-checker from Volksverpetzer dismissed Marcel Barz as “fake”. The verdict by Correctiv was a bit milder (Barz has given a public and detailed reply). He is proved right by the document produced for the German Federal Ministry of Health, which shows that Covid-19-Patienten stood for no more than 2% of the hospital burden during 2020. Barz went to the press with his analysis but was ignored. In a functioning discourse, our media would invite him for a debate.
Covid-related content has been deleted countless times, as shown by journalist Laurie Clarke in The British Medical Journal. Facebook and similar media are private companies and are thus free to decide what may be published on their platforms. But in doing so, are they also allowed to steer the discourse?
Public service broadcasting could have an important balancing role, by offering an open exchange of opinion. Not so, unfortunately!
Digital vaccine passes and surveillance
The Gates and Rockefeller Foundations drafted and financed the WHO guidelines for digital vaccine passes. These passes are now being rolled out everywhere. Only with these passes will public life be possible – whether you want to take the tram, have a coffee or get medical treatment. An example from France shows that this digital pass will stay even after the pandemic ends. MP Emanuelle Ménard demanded the following addition to the legal text: The digital vaccine pass shall end when the virus spread no longer presents a level of danger which justifies its use. Her proposed amendment was rejected. Thus we are but a small step away from global population control or even a surveillance state via projects such as ID2020.
Australia is currently testing a facial recognition app, to ensure that people stay at home when in quarantine. In Israel, electronic wristbands are used for this purpose. In one Italian city, drones are being tested to measure the temperature of beachgoers, and in France, the law is changed to allow large-scale drone surveillance.
All these topics must be subject to intensive and critical scrutiny within our society. This is not happening to a sufficient extent in the reporting by our broadcasting organisations and, indeed, was not an election campaign issue.
Blinkered vision
The way in which public discourse has been curtailed is indicative of the “gatekeeper of information”. A current example comes from Jan Böhmermann, who demanded that virologists Hendrik Streeck and Professor Alexander S. Kekulé be deprived of their opportunity to speak out, claiming that they were not competent to do so.
Even though the two physicians have very impressive CVs, Böhmermann has thus narrowed the field of vision even more. So, now we cannot even listen to people who present their criticism of government policy wearing kid gloves?
Public discourse has been curtailed so much that Bayerischer Rundfunk has more than once refrained from broadcasting speeches by members of state parliaments who take a critical view of the measures during parliamentary debates.
Is that what the new understanding of democracy looks like in public service broadcasting? Alternative media platforms thrive first and foremost because the established platforms fail to do their job as a democratic corrective.
Something has gone wrong
For a long time, I could say with pride and joy that I work in public service broadcasting. ARD, ZDF and Deutschlandradio have generated outstanding research, formats, and content. The quality standards are extremely high and thousands of staff members are doing great work despite increasing cost pressure and savings targets. But with Covid-19, something has gone wrong. Suddenly, I have become aware of tunnel vision, blinkers and a supposed consensus which is no longer questioned. (10)
The Austrian broadcaster Servus TV is proof that another way is possible. In the programme “Corona-Quartett” / “Talk im Hanger 7” proponents and critics are given equal space. Why is that not possible in German television? (11) “You cannot let every crank take the stage”, is the quick retort. The false balance, giving serious and dubious opinions an equal chance to be heard, must be avoided. — A killer argument, which also happens to be unscientific. The basic principle of science is doubt, questioning, checking. If this does not happen, then science has become a religion.
Yes, there is actually a false balance. It is the blind spot in our heads, which no longer allows true debate. We are throwing around apparent facts, but can no longer listen to each other. Contempt replaces understanding, fighting the opposing view replaces tolerance. The basic values of our society are thrown overboard, just like that. Here we go: People who do not want to get the jab are crazy, there we go: “Shame on the sleeping sheep”.
While we are busy fighting, we fail to notice that the world around us is changing at breakneck speed. Virtually all areas of our lives are being transformed. How this develops is essentially determined by our capacity for cooperation, compassion and awareness of ourselves and our words and deeds. For our spiritual wellbeing, we would do well to open the space for debate – while being mindful, respectful and with understanding of different perspectives. (12)
Writing this, I feel like a heretic — someone who commits high treason and must reckon with being punished. Maybe this is not the case. Maybe I am not actually risking my job, and maybe freedom of opinion and pluralism are not under threat. I really hope so and I look forward to constructive exchange with my colleagues.
Ole Skambraks
ole.skambraks@protonmail.com
About the author: Ole Skambraks, born in 1979, studied Political Science and French at Queen Mary University in London, as well as Media Management at the ESCP Business School in Paris. He was a Moderator, Reporter and Writer at Radio France Internationale, Online Editor and Community Manager at cafebabel.com, Programme Manager of the MDR Sputnik morning show and Editor at WDR Funkhaus Europa / Cosmo. He is currently working as an Editor in Programme Management/Sound Design at SWR2.
Further information from the author
PS: For fact-checkers and people interested in a multi-perspective, here are the counter-positions to the points discussed in the text:
Prof. John Ioannidis
https://www.faz.net/aktuell/wissen/forscher-john-ioannidis-verharmlost-corona-und-provoziert-17290403.html
https://sciencebasedmedicine.org/what-the-heck-happened-to-john-ioannidis/
Imperial College Modelling
https://blogs.bmj.com/bmj/2020/10/07/covid-19-modelling-the-pandemic/
Gain of function research
https://www.gavi.org/vaccineswork/next-pandemic/nipah-virus
Hydroxychloroquin / Ivermectin
https://www.br.de/nachrichten/wissen/corona-malaria-mittel-hydroxychloroquin-bei-covid-19-unwirksam,RtghbZ4
https://www.who.int/publications/i/item/WHO-2019-nCoV-therapeutics-2021.2
Immunity of the vaccinated
https://www.biorxiv.org/content/10.1101/2021.08.23.457229v1
Immunity of the recovered
https://science.orf.at/stories/3208411/?utm_source=pocket-newtab-global-de-DE
Vaccination breakthroughs / Pandemic of the non-vaccinated
https://www.spektrum.de/news/corona-impfung-wie-viele-geimpfte-liegen-im-krankenhaus/1921090#Echobox=1631206725
https://www.mdr.de/wissen/covid-corona-impfdurchbrueche-sind-selten-100.html
Pseudo-experts / Science Denial / PLURV-Principle
https://www.ndr.de/nachrichten/info/82-Coronavirus-Update-Die-Lage-ist-ernst,podcastcoronavirus300.html#Argument
Notes:
(1) The exception was the coverage of the referendum, during which Swiss television was obliged to give both parties the same broadcasting slot.
(2) More Pandemic-Emergency exercises were “Clade X“ (2018), “Atlantic Storm“ (2005), “Global Mercury“ (2003) and “Dark Winter“ (2001). These exercises were always about information management.
(3) Panorama reported on the payments, but did not clearly portray Kyriakides’ role regarding the Corona vaccine contracts. Otherwise, the issue has not had much prominence in the media.
(4) For example, there was hardly any coverage on public radio of the British musician Eric Clapton, who developed violent reactions after vaccination and now regrets it.
(5) According to the RKI, a vaccination breakthrough is when a vaccinated person can show both a positive test and symptoms – for the unvaccinated, a positive test is sufficient. In this way, the unvaccinated are statistically more significant.
(6) Each under the heading “List of approved vaccines”; previous PEI website editions accessible via the Internet archive Wayback Machine.
(7) The WHO has even praised the Indian state of Uttar Pradesh for its corona policy, but without mentioning ivermectin. The vaccination rate in Uttar Pradesh is below 10 %.
(8) See also FDA meeting of 17 September 2021, at 5:47:25
(9) The fairest reporting comes from BR, although here too it was about and not with the makers. MDR offers a comprehensive and differentiated analysis on its media portal.
(10) I would not like to speak of an actual “unified opinion” of the public broadcasters. There have always been critical contributions and course corrections in reporting. But it is always a question of context, broadcasting time and scope how a topic is treated. My colleagues have also confirmed my observations.
(11) Fresh formats like ZDF’s “Auf der Couch” (On the Couch) give hope, even if I don’t think a Karina Reiß or a Wolfgang Wodarg will be taking a seat there any time soon.
The truth is still in lockdown
The first cross-party report says we didn’t lockdown early enough. The truth is, lockdowns don’t work.
By Laura Dodsworth | October 15, 2021
We now move, work, socialise, worship and meet around the UK with relative freedom.* Sadly, truth remains in strict lockdown.
Information is infectious and its transmissibility must be suppressed if it is deemed inconvenient, even if truthful. If it escapes, it can travel faster on social media than an airborne virus and must be captured, quarantined and sanitised to prevent onward infection. Most recently, in a long list of examples, a speech made by MP David Davis about vaccine passports was temporarily suspended from Youtube. Many videos and articles from reputable sources have been labelled misinformation if they run counter to WHO or governmental policy. Social media giants, governments and public health authorities are petrified of outbreaks of misinformation and even, sometimes, the truth.
So it was no surprise that the first cross-party report into the management of the epidemic in the UK, Coronavirus: lessons learned to date was unwilling to tackle certain truths.
One of the main inferences is that lockdown should have been implemented earlier. The truth is that lockdowns don’t work and cause great harm.
The report’s conclusions are assumptions. Opinions are not backed up with evidence. There is an unwillingness to interrogate the modelling that provides the foundations for the conclusions. The only thing that matters in this report is Covid and deaths by Covid. It is almost as if there are no other societal losses to put in the balance. There is no quantifiable cost benefit analysis of lockdown.
I spoke to Professor Simon Wood, Chair of Computational Studies at the School of Mathematics at the University of Edinburgh about the report. Wood authored a peer-reviewed paper published in Biometrics, which found that Covid-19 levels were probably falling before each of the three lockdowns. A separate paper, with colleague Ernst Wit, came to the same conclusion for the first two lockdowns, by the alternative approach of re-doing Imperial College’s major modelling study of the epidemic.
In summary he told me,
“The whole report is written within the framework that the only thing that counts is avoiding deaths from Covid, and that full lockdowns were essential. Evidence for the latter seems to be entirely absent. The closest we seem to get to actual evidence on lockdown efficacy is Neil Ferguson’s opinion in paragraph 77. The extent to which the committee is really able to weigh scientific evidence, as opposed to opinion, is questionable if paragraph 94 is any guide. This is such a gross misrepresentation of what the cited paper said, that it could have appeared on Twitter, rather than a parliamentary report.”
I asked him what he thought about the reliance on modelling throughout the epidemic. There are multiple flaws (expanded on in more detail in my book A State of Fear, and it’s appendix, “Lockdowns Don’t Work” and in many articles and papers online, some listed here) but one key flaw is that the Infection Fatality Rate in the initial modelling was 0.9%. By autumn 2020, a peer-reviewed paper by the WHO had put the IFR at 0.23%, and in the UK it is currently (albeit post-vaccination) at 0.096%. Wood generously told me it was,
“difficult to get the IFR right at the outset. We did the analysis thinking Imperial were very on the high side, but it in fact it wouldn’t have been assessed as less than 0.6% at the outset.” He went on: “The main error is to put too much emphasis on modelling not on measuring. Often models are being used for prediction purposes they were not designed or validated for.”
I put it to Wood that, in circular and fallacious reasoning, the modelling is being used to measure the success of lockdown by deaths ‘saved’ against those predicted by the unsubstantiated and flawed simulated forecasts of the modelling. He agreed: “the post hoc justification for the measures using modelling often looks like bending the model to the conclusion you want to achieve.”
There is a growing body of evidence that light interventions and voluntary behaviour changes – ie not lockdowns – are sufficient to reduce the R. Real world examples support this, namely Sweden, South Dakota and Florida. Conversely, as economist Professor David Paton reported, early and strict lockdowns did not always work. Czechia’s did not stop subsequent surges of the virus and further lockdowns. Czechia currently has the sixth highest death rate per million in the world. Peru, another country which enforced very strict and early lockdown, has the worst death rate in the world.
The report’s authors state we should learn lessons internationally, but fail to explain what they think happened in Sweden, for instance. In science it’s generally a good idea to have a control treatment and, to a limited extent, Sweden provided that. Surely it deserves some discussion if weighing up the evidence on what should have happened. It seems the report’s accusation of “British exceptionalism” only travels in one direction.
When data proves that lockdowns cannot be credited with controlling the virus, why does the argument persist? Why is truth still locked down?
Ironically, the authors accuse the government of groupthink, but they might still be under its sway themselves. It will be hard for the enactors and supporters of the lockdown to admit it was a brutal, ineffective and harmful policy. Far easier to assert the main problem is that it wasn’t imposed early and hard enough.
The harms of lockdown only get passing mentions. I can’t weight this article with the full burden of harms, but in brief: In the first year of lockdown the government borrowed £229 billion, the highest figure since records began in 1946. The pain of broken tax pledges, fiscal drag, inflation, and unemployment won’t be felt in full for months and years to come. The NHS waiting list is now 5.74 million and 7.5 million fewer people were referred for routine hospital care between January 2020 and July 2021.
These problems should not appear unexpected – they were foretold by the UK’s most eminent disaster and recovery planners.
In this 145 page report, the world “children” is mentioned a mere three times, but the impact of the lockdown on them is not mentioned at all. On World Mental Health Day, the ONS released data on children’s mental health and the impact of restrictions. A quarter of 11 to 16 year olds with a probable mental disorder in 2021 said Covid restrictions had made their lives much worse. And the number of young people aged 0 to 18 years old referred to mental health services between April and June 2021 increased by 93% from the same period in 2020, and 41% on 2019 in England.
Another word that is only mentioned three times is “obesity” alongside the other pre-existing health conditions which are known to be associated with poor outcomes for Covid-19. This really is the elephant in the room. The truth is, Covid-19 death rates are ten times higher in countries where more than half the adult population is overweight. In that sense, perhaps our pandemic preparedness should have started many years earlier with better health and dietary advice. Not only does lockdown not tackle the underlying chronic co-morbidities which lead to severe Covid-19 illness and deaths, but lockdown caused British people to gain weight, cease normal exercise and drink more alcohol.
The UK had multiple pandemic plans, including for SARS/MERS outbreaks. The authors of this report claim that we didn’t abandon the plans earlier in the crisis because of “groupthink”. This is a bizarre subversion – crisis management plans are not supposed to be abandoned during a crisis. If the government were guilty of groupthink, it was in following other countries in implementing an experimental policy. As Professor Ferguson put it,
“It’s a communist one party state, we said. We couldn’t get away with it in Europe, we thought. And then Italy did it. And we realised we could.”
The report does not mention Exercise Alice, a pandemic simulation exercise for MERS that has only been released after persistent Freedom of Information requests. It’s not clear that the authors are aware of it.
We will need a more wide-ranging inquiry that establishes whether lockdowns work, if they are sensible, proportionate and moral. Essentially, we must be truthful about what the costs are. We need to balance the losses.
Truth is infectious. Eventually it will peek around the doorframe, dare to stroll outside, evade quarantine and someone will catch a glimpse. Then another. Soon, everyone will be queueing up to greet our old friend Truth with hail-fellow-well-met and a hearty slap on the back. Then we must clutch Truth to us and never again lock it down.
* Although mandatory vaccine passports are a concerning development in Scotland and Wales.
The WEF and the Pandemic
How is the Davos World Economic Forum involved in the coronavirus pandemic?
Swiss Policy Research | October 6, 2021
The Davos World Economic Forum (WEF) is a premier forum for governments, global corporations and international entrepreneurs. Founded in 1971 by engineer and economist Klaus Schwab, the WEF describes its mission as “shaping global, regional and industry agendas” and “improving the state of the world”. According to its website, “moral and intellectual integrity is at the heart of everything it does.”
The WEF has been involved in the coronavirus pandemic in several ways.
First, the WEF was, together with the Gates Foundation, a sponsor of the prescient “Event 201” coronavirus pandemic simulation exercise, held in New York City on October 18, 2019 – the same day as the opening of the Wuhan Military World Games, seen by some as “ground zero” of the global pandemic. China itself has argued that US military athletes may have brought the virus to Wuhan.
Second, the WEF has been a leading proponent of digital biometric identity systems, arguing that they will make societies and industries more efficient, more productive and more secure. In July 2019, the WEF started a project to “shape the future of travel with biometric-enabled digital traveler identity management”. In addition, the WEF collaborates with the ID2020 alliance, which is funded by the Gates and Rockefeller foundations and runs a program to “provide digital ID with vaccines”. In particular, ID2020 sees the vaccination of children as “an entry point for digital identity.”
Third, WEF founder Klaus Schwab is the author of the book COVID-19: The Great Reset, published in July 2020, which argues that the coronavirus pandemic can and should be used for an “economic, societal, geopolitical, environmental and technological reset”, including, in particular, advancing global governance, accelerating digital transformation, and tackling climate change.
Finally, the WEF has been running, since 1993, a program called “Global Leaders for Tomorrow”, rebranded, in 2004, as “Young Global Leaders”. This program aims at identifying, selecting and promoting future global leaders in both business and politics. Indeed, quite a few “Young Global Leaders” have later managed to become Presidents, Prime Ministers, or CEOs (see below).
During the coronavirus pandemic, several WEF Global Leaders and Global Shapers (a junior program of the Global Leaders) have played prominent roles, typically promoting zero-covid strategies, lockdowns, mask mandates, and ‘vaccine passports’. This may have been a (largely failed) attempt to protect public health and the economy, or it may have been an attempt to advance the global transformation agenda outlined above, or perhaps both.
In this regard, some notable Young Leaders include Jeffrey Zients (US White House Coronavirus Response Coordinator), Stéphane Bancel (CEO of Moderna), Jeremy Howard (founder of influential lobby group “Masks for All”), Leana Wen (zero-covid CNN medical analyst), Eric Feigl-Ding (zero-covid Twitter personality), Gavin Newsom (Governor of California, selected in 2005), Devi Sridhar (British zero-covid professor), Jacinda Ardern (Prime Minister of New Zealand), French President Emanuel Macron (selected one year prior to his election in 2017), Austrian Chancellor Sebastian Kurz, German Chancellor Angela Merkel (selected back in 1993), German Health Minister Jens Spahn, and former British Prime Minister Tony Blair (a leading proponent of ‘global vaccine passports’).
To get a full overview of their members, see Global Leaders for Tomorrow and Young Global Leaders on WikiSpooks (a Wiki focusing on covert power structures) as well as the official Young Global Leaders website. For an overview of some notable members in politics and the media, see below.
In conclusion, the Davos World Economic Forum has indeed been involved in the strategic management of the coronavirus pandemic, with a major emphasis on using the pandemic as a catalyst for digital transformation and the global introduction of digital identity systems.
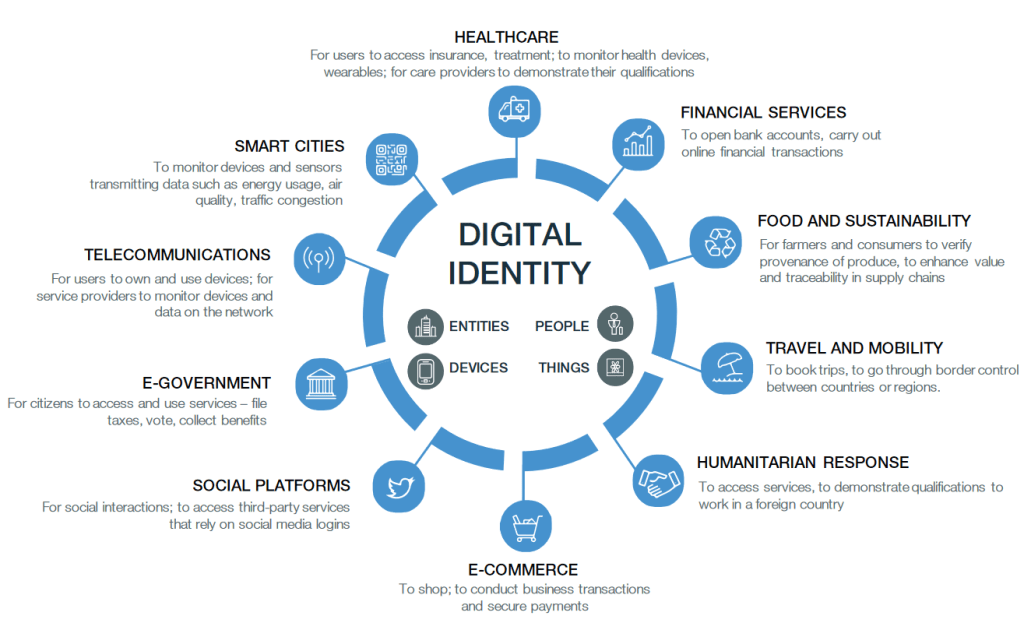
Digital Identity: The vision of the World Economic Forum (WEF, 2018)
WEF “Young Global Leaders”
An overview of some WEF Young Global Leaders (2005-2021) and Global Leaders for Tomorrow (1993-2003) in politics and the media. The list is not exhaustive.
Sources: Global Leaders for Tomorrow and Young Global Leaders on WikiSpooks.
United States
Politics and Policy
Jeffrey Zients (White House Coronavirus Response Coordinator since 2021, selected in 2003), Jeremy Howard (co-founder of lobby group “masks for all”, selected in 2013), California Governor Gavin Newsom (selected in 2005), Pete Buttigieg (selected in 2019, candidate for US President in 2020, US secretary of transportation since 2021), Chelsea Clinton (Clinton Foundation board member), Huma Abedin (Hillary Clinton aide, selected in 2012), Nikki Haley (US ambassador to the UN, 2017-2018), Samantha Power (US ambassador to the UN, 2013-2017, USAID Administrator since 2021), Ian Bremmer (founder of Eurasia Group), Bill Browder (initiator of the Magnitsky Act), Jonathan Soros (son of George Soros), Kenneth Roth (director of “Human Rights Watch” since 1993), Paul Krugman (economist, selected in 1995), Lawrence Summers (former World Bank Chief Economist, former US Treasury Secretary, former Harvard University President, selected in 1993), Alicia Garza (co-founder of Black Lives Matter, selected in 2020), Stéphane Bancel (Moderna CEO).
Media
CNN medical analyst Leana Wen (selected in 2018), CNN chief medical correspondent Sanjay Gupta, Covid Twitter personality Eric Feigl-Ding (a ‘WEF Global Shaper‘ since 2013), Andrew Ross Sorkin (New York Times financial columnist), Thomas Friedman (New York Times columnist, selected in 1995), George Stephanopoulos (ABC News, 1993), Lachlan Murdoch (CEO of Fox Corporation).
Technology and Social Media
Microsoft founder Bill Gates (1993), former Microsoft CEO Steven Ballmer (2000-2014, selected in 1995), Amazon founder Jeff Bezos (1998), Google co-founders Sergey Brin and Larry Page (2002/2005), former Google CEO Eric Schmidt (2001-2017, selected in 1997), Wikipedia co-founder Jimmy Wales (2007), PayPal co-founder Peter Thiel (2007), eBay co-founder Pierre Omidyar (1999), Facebook founder and CEO Mark Zuckerberg (2009), Facebook COO Sheryl Sandberg (2007).
Great Britain, Canada, New Zealand
Professor Devi Sridhar (a leading ‘zero covid’ proponent, selected in 2020/21), former British Prime Ministers Tony Blair and Gordon Brown (both selected in 1993), BBC World Service journalist Dawood Azami, Lynn Forester de Rothschild (co-owner of The Economist), Nathaniel Rothschild (son of Lord Rothschild), historian Niall Ferguson (selected in 2005), William Hague (Foreign Secretary, 2010-2014), Charles Allen (CEO of ITV, 2004-2007; Chairman of EMI, 2008-2010).
New Zealand Prime Minister Jacinda Ardern (since 2017, selected in 2014), Canadian Deputy Prime Minister Chrystia Freeland (selected in 2001; former managing director of Reuters). Canadian Prime Minister Justin Trudeau is a WEF participant, but is not a confirmed Young Global Leader.
Germany
Chancellor Angela Merkel (selected in 1993, 12 years before becoming Chancellor), current Health Minister Jens Spahn and former Health Ministers Philipp Roesler and Daniel Bahr, current co-chair of the Green Party and failed Chancellor candidate Annalena Baerbock (selected in 2020), former co-chair of the Green Party Cem Özdemir (selected in 2002), media mogul and Axel Springer CEO Mathias Doepfner (selected in 2001), talk show host Sandra Maischberger, late Foreign Minister and Vice Chancellor Guido Westerwelle (1997), former German President Christian Wulff (selected in 1995, 15 years before becoming President), Reto Francioni (former CEO of Deutsche Boerse).
European Union
EU Commission Presidents Jose Manuel Barroso (2004-2014, selected in 1993) and Jean-Claude Juncker (2014-2019, selected in 1995), French President Emanuel Macron (since 2017, selected in 2016), former French President Nicolas Sakozy (2007-2012, selected in 1993), Austrian Chancellor Sebastian Kurz, former Italian Prime Minister Matteo Renzi (2014-2016, selected in 2012), former Spanish Prime Minister Jose Maria Aznar (1996-2004, selected in 1993), Klaus Regling (CEO of the European Financial Stability Mechanism since 2012), Guy Verhofstadt (former Belgian Prime Minister, Chair of the Brexit Steering Group), Danish Minister for the Environment Lea Wermelin, Finnish Prime Minister Sanna Marin, former Finnish Prime Minister Alexander Stubb, and Mark Leonard (founding director of the Soros-funded European Council on Foreign Relations).
Switzerland
Natalie Rickli (Director of Health of the Canton of Zurich, selected in 2012), former Presidents of the Swiss National Council Christa Markwalder (selected in 2011) and Pascale Bruderer-Wyss (selected in 2009), Geneva politician Pierre Maudet (selected in 2013), NZZ media group CEO Felix R. Graf (selected in 2007), former Swiss Justice Minister Ruth Metzler (selected in 2002), former Swiss television CEO Roger de Weck (2011-2017, selected in 1994), former UBS CEOs Peter Wuffli (selected in 1994) and Marcel Rohner (selected in 2003), former Credit Suisse CEO Tidjane Tiam (1998).
Video Annex
1) Bill Gates demanding “digital immunity proof” in March 2020
2) Edward Snowden warning of the “destruction of rights” (March 2020)
3) The Chinese “social credit” system (May 2019)
Further reading
- All Roads Lead to Dark Winter (Whitney Webb, April 2020)
See also
BMJ Publishes Belated Attack on the Great Barrington Declaration, but It Doesn’t Hit the Target
By Noah Carl • The Daily Sceptic • October 13, 2021
The Great Barrington Declaration, which advocates a focused protection strategy for dealing with COVID-19, was published in October last year – before many countries around the world imposed their winter lockdowns.
Recently, The BMJ Opinion – a journalistic offshoot of the well-known medical journal – published a very belated hit piece against the authors. As you might expect, it’s light on scientific arguments and heavy on tactics like ad hominem, guilt by association and appeals to authority.
The authors, David Gorski and Gavin Yamey, really don’t mince words. For example, they describe the Declaration (which has been signed by hundreds of scientists and healthcare professionals) as a “well-funded sophisticated science denialist campaign based on ideological and corporate interests”.
Not exactly a respectful way to talk about your colleagues. But it’s hardly the first time the Declaration’s critics have sunk to this level. Just last month, Jay Bhattacharya became the subject of a censorious petition which claimed that he “sows mistrust of policies designed to protect the public health”.
Gorski and Yamey begin their article by criticising the Declaration’s authors for collaborating with the American Institute for Economic Research, which they claim is a “libertarian, climate-denialist, free market think tank”.
I’m not sure why this is a ‘gotcha’. Lockdown is about as un-libertarian a policy as you could imagine, so it’s not really surprising that a libertarian think tank would oppose it. And in any case, the Declaration’s website clearly states that the document was “was written and signed at the American Institute for Economic Research”.
Martin Kulldorff has since clarified that the AIER president and board did not know about the Declaration until after it was published. But even if they had done, so what? As Kulldorff notes, universities like Duke and Stanford have received money from the Koch brothers. Should we therefore completely disregard what their academics have to say?
Gorski and Yamey’s next move is to cite social media censorship of lockdown sceptics as evidence that their arguments constitute ‘misinformation’. (Incidentally, that term – which basically means ‘information that’s missing from the mainstream narrative’ – appears no fewer than six times in the article.)
However, this argument relies on circular logic: ‘Something was censored on social media? Therefore, it’s misinformation. How do we know? Well, misinformation is what social media companies censor.’ In reality, of course, the fact that something was censored is no indication whatsoever that it’s factually incorrect.
The authors then allege that when Sunetra Gupta and Carl Heneghan met Boris Johnson in September of last year, they were successful in “persuading him to delay” a ‘circuit breaker’ lockdown, which could have forestalled the second wave of infections.
As historian Phil Magness has already noted, this argument is deficient on two counts. It’s not clear that Gupta and Heneghan did persuade the Prime Minister to shelve the ‘circuit breaker’ idea. But even if they did, there’s no reason to believe that policy would’ve prevented a large number of deaths.
Finally, Gorski and Yamey compare lockdown sceptics to ‘climate science deniers’, insofar as both groups “argue that evidence-based public health measures do not work”. They call for experts to push back against the Great Barrington Declaration by highlighting “scientific consensus”, citing the John Snow Memorandum.
Of course, the pro-lockdown John Snow Memorandum is just another public statement signed by scientists and health professionals. If it constitutes “scientific consensus”, then so does the Great Barrington Declaration. I’m only aware of one attempt to gauge overall expert opinion on focused protection: the survey by Daniele Fanelli.
He asked scientists who’d published at least one relevant paper, “In light of current evidence, to what extent do you support a ‘focused protection’ policy against COVID-19, like that proposed in the Great Barrington Declaration?” Of those who responded, more than 50% said “partially”, “mostly” or “fully”.
Regardless of the exact number of experts who support focused protection, claiming there is a “scientific consensus” against it is simply false. Long before the Declaration itself was published, many scientists had proposed some version of precision shielding. In fact, this was basically the U.K.’s plan until the middle of March, 2020.
On March 5th, Chris Whitty told the Health and Social Care Committee that we are “very keen” to “minimise economic and social disruption”, and mentioned that “one of the best things we can do” is “isolate older people from the virus”.
Another prominent scientist who has argued in favour of focused protection is Sir David Spiegelhalter. In an article published on May 29th, he and George Davey Smith said that we ought to “stratify shielding according to risk” because lockdown is “seriously damaging many aspects of people’s lives”.
They noted that this would require “a shift away from the notion that we are all seriously threatened by the disease, which has led to levels of personal fear being strikingly mismatched to objective risk of death”.
Among the ad hominems, appeals to authority and repeated uses of ‘misinformation’, finding a scientific argument in Gorski and Yamey’s article is not easy. And given that the content’s almost a year out of date, I’m not sure why the authors felt the need to publish it.
SPECIAL BROADCAST: DR. ROBERT MALONE ON HIS MRNA CREATION
STEW PETERS | OCTOBER 13, 2021
Stew Peters sat down with Dr. Robert Malone, the creator of the mRNA technology being used in the shots being falsely referred to as “vaccines”, which have proven to be dangerous, and in many cases DEADLY.
House of Commons Covid Report Gets Some Things Right, Most Things Wrong
By Toby Young • The Daily Sceptic • October 12, 2021
On Monday evening two House of Commons select committees – the Science and Technology Committee and the Health and Social Care Committee – published a joint report on the Government’s handling of the COVID-19 pandemic that was predictably damning. It was published in time to make the following day’s front pages – “Britain must learn from ‘big mistakes’ on Covid, says report”, reported the Times on its front page – but not in time for newspaper reporters or broadcast journalists to properly assess its findings. Not that that stopped all the usual suspects from using it as a stick to beat the Government with. For instance, Labour’s Shadow Health Secretary Jonathan Ashworth told the BBC that the “damning” findings showed that “monumental errors” had been made and called for the public inquiry – scheduled for next spring – to be brought forward.
The authors of the report say in the Executive Summary that the reason they’ve published it now, when there are still a large number of ‘known unknowns’ as well as ‘unknown unknowns’, is because we urgently need to learn from what the Government got right and what it got wrong so we are better prepared for the next pandemic, which might come along at any moment. But if it’s too soon to say what was a mistake and what wasn’t, that argument collapses. Indeed, a premature report that draws the wrong conclusions, e.g. that the Government didn’t lock down in March of last year early enough, which is one of the main findings of this report, is worse than useless since it may encourage future Governments to repeat the same mistakes.
I’ve now read the report – yes, all 145 pages – so you don’t have to.
What the report gets right
- It criticises the Government for discharging elderly patients from hospitals into care homes without testing them first to see if they had COVID-19 and without putting any measures in place in care homes to mitigate the impact of that policy, as well as for the lack of PPE in care homes. The report says these errors “led to many thousands of deaths which could have been avoided”. Hard to argue with that, although one of the oddities of the report is that it criticises the lack of infection control in care homes, but not in hospitals. Weird, given that ~20% of cases over the course of the U.K.’s epidemic have been hospital-acquired infections.
- The authors praise the RECOVERY trial for carrying out large randomised control trials of different COVID-19 treatments and identifying dexamethasone as an effective treatment. That too seems right.
- The report highlights the disproportionately high Covid death rates among black, Asian and minority ethnic populations and acknowledges that part of the explanation for that may be biological differences between those populations and the white British population. Even acknowledging that genetic factors may be part of the reason for these disparities makes a refreshing change. Unfortunately, the report goes on to play down these biological differences and claims that social, economic and health inequalities are much bigger factors.
- It criticises hospitals and care homes for issuing ‘Do Not Attempt CPR’ notices to patients/clients with learning disabilities and autism, often without the consent of their families. No argument there.
- Rather than blame Boris and other senior members of the Government for the decision not to lock down before March 23rd 2020, the report emphasises that they were just following the recommendations they were being given by their scientific advisors. As I’ve pointed out before, that is correct.
- The report is at least ambivalent about how effective a two-week ‘circuit breaker’ would have been in England in September of 2020.
It is impossible to know whether a circuit breaker in the early autumn of 2020 would have had a material effect in preventing a second lockdown given that the Kent (or Alpha) variant may already have been prevalent. Indeed such an approach was pursued in Wales, which still ended up having further restrictions in December 2020.
Unfortunately, having written this, the authors then go on to say:
It is likely that a “circuit break” of temporary lockdown measures if introduced in September 2020, and earlier lockdown measures during the winter, could have impeded the rapid seeding and spread of the Kent variant.
Make up your mind guys!
What the report gets wrong
- The report claims that the U.K.’s Pandemic Preparedness Strategy wasn’t fit for purpose because it prepared us for “an influenza-like pandemic” rather than a more serious infectious disease that was spread, in part, by asymptomatic transmission. Professor Devi Sridhar, who gave evidence to the joint committees, is quoted as saying the mistake our Government made was to assume COVID-19 was “just like a bad flu”. In fact, it was like a bad flu, as judged by the latest estimates of the infection fatality rate, and the jury’s still out on whether asymptomatic people who test positive for Covid are infectious.
- One of the reasons the Government didn’t lock down before March 23rd, according to the authors, is because its scientific advisors were guilty of following the flawed playbook of the Pandemic Preparedness Strategy. In particular, the initial advice was to try to ‘manage’ the spread of the virus through the general population rather than to suppress it altogether, which the authors believe would have been the correct strategy. They claim the Government didn’t realise this sooner because it had failed to learn the lessons of the SARS, Swine Flu and MERS pandemics and embed those lessons in its strategy. But, surely, one of the lessons of those pandemics is that national lockdowns aren’t necessary to contain pandemics – and that advice was embedded in the U.K. Government’s strategy document. The mistake the Government made was not to initially follow that advice; the mistake was to stop following it on March 23rd. The only time a government has tried quarantining entire regions as a strategy to mitigate the impact of a viral outbreak prior to 2020 was in Mexico in 2009 when something like a lockdown was imposed on April 27th in Mexico City, the State of Mexico and the State of San Luis Potosí. That was policy abandoned on May 6th because of the mounting social and economic costs.
- Bizarrely, the authors of the report claim the reason the British Government didn’t abandon the Pandemic Preparedness Strategy sooner was because of “groupthink”. But, surely, the reason for putting a carefully thought out strategy document in place, incorporating the lessons from the mistakes made during previous pandemics, was precisely to avoid Government decisions being influenced by groupthink. And that approach was successful until mid-March, at which point Boris Johnson and his closest political allies abandoned it and decided to copy what other Western leaders were doing, i.e. lockdown. In other words, it was groupthink that was responsible for the disastrous U-turn, not the comparatively sensible initial approach.
- One of the main conclusions of the report is that the Government should have locked down earlier than it did – that’s one of the “big mistakes” in all the headlines – and they quote Professor Neil Ferguson to that effect:
The initial U.K. policy was to take a gradual and incremental approach to introducing non-pharmaceutical interventions. A comprehensive lockdown was not ordered until March 23rd 2020 – two months after SAGE first met to consider the national response to COVID- 19. This slow and gradualist approach was not inadvertent, nor did it reflect bureaucratic delay or disagreement between Ministers and their advisers. It was a deliberate policy – proposed by official scientific advisers and adopted by the Governments of all of the nations of the United Kingdom. It is now clear that this was the wrong policy, and that it led to a higher initial death toll than would have resulted from a more emphatic early policy. In a pandemic spreading rapidly and exponentially every week counted. The former SAGE participant Professor Neil Ferguson told the Science and Technology Committee that if the national lockdown had been instituted even a week earlier “we would have reduced the final death toll by at least a half”.
- In fact, it’s far from clear that “this was the wrong policy” or that it “led to a higher initial death toll”. The authors of this report take it for granted that – in the words of Professor David Paton – “governments can turn infections on or off like a tap by imposing or lifting restrictions”, when all the real-world data we’ve accumulated in the past 18 months suggests that is hopelessly naive (see these 30 studies, for instance). Governments around the world, including ours, have been guilty of wildly over-estimating the impact of non-pharmaceutical interventions on the spread of the virus.
- In the British case, there’s no reason to believe that locking down earlier would have reduced the final death toll at all, let alone by half. As David Paton points out, the Czech Republic locked down on March 16th, imposed hard border controls and rolled out the first national mask mandate in Europe. Yet it had a second surge in the Autumn of 2020, prompting it to lock down again, and then an even bigger one in December, leading to a third lockdown. Cases surged again in Czechia in February and March of this year and, six months ago, it had the second-highest per capita Covid death toll in the world, according to Reuters.
More damning still is the comparison with Sweden, which didn’t lock down at all in 2020 and, as of today, is ranked 50th in Worldometers’ table ranking countries according to per capita deaths. The U.K., by contrast, is ranked 25th.

- There are only three mentions of Sweden in this report, two of them in a single footnote. Any assessment of the U.K. Government’s response to the pandemic that fails to compare it with that of the Swedish Government – particularly one advocating we should have locked down sooner and for longer – doesn’t deserve to be taken seriously.
- The report’s authors take at face value the “reasonable worst-case” scenarios that various modellers (including a sidekick of Dominic Cummings’) came up with in mid-March to show that if the Government continued to follow Plan A, i.e. the Pandemic Preparedness Strategy, the NHS was on track to become overwhelmed many times over. Here is Matt Hancock giving evidence on June 8th 2021, appealing to a prediction of “slightly below” 820,000 deaths, absent a lockdown:
I asked for a reasonable worst-case scenario planning assumption. I was given the planning assumption based on Spanish flu, and it was signed off at Cobra on January 31st. That was a planning assumption for 820,000 deaths. […]
In the week beginning March 9th, what happened is that the data started to follow the reasonable worst-case scenario. By the end of that week, the updated modelling showed that we were on the track of something close to that reasonable worst-case scenario. I think the numbers were slightly below that, but they were of a scale that was unconscionable.
- Rather than just take those projections at face value, couldn’t the House of Commons committees have interrogated the models a little bit? The report’s most damning criticism – that the Government’s delay in imposing the first lockdown resulted in thousands of unnecessary deaths – is contingent on not questioning those forecasts. In light of SAGE’s over-estimate of the likely uptick in cases following the easing of restrictions on July 19th of this year, as well as its more recent over-estimate of hospitalisations this autumn, wouldn’t it have been prudent to scrutinise those models? That’s a particularly glaring omission, given that the authors of the report criticise members of the Government for not challenging the scientific advice they were given: “Those in Government have a duty to question and probe the assumptions behind any scientific advice given, particularly in a national emergency, but there is little evidence sufficient challenge took place.” Why do “those in Government” have a duty to do this, but not those serving on select committees who are supposed to be holding the Government to account?
- In case further evidence is required that the authors of the report have credulously lapped up the doom-mongering of SPI-M and others, consider this passage:
It seems astonishing looking back that – despite the documented experiences of other countries; despite the then Secretary of State referring to data with a Reasonable Worst Case Scenario of 820,000 deaths; despite the raw mathematics of a virus which, if it affected two-thirds of the adult population and if one percent of people contracting it died would lead to 400,000 deaths – it was not until March 16th that SAGE advised the Government to embark on a full lockdown (having said on March 13th that “it was unanimous that measures seeking to completely suppress the spread of COVID-19 will cause a second peak”) and not until March 23rd that the Government announced it.
- Note the appeal to an IFR of 1% when even Neil Ferguson’s team at Imperial College, which predicted 510,000 deaths if the Government stuck with Plan A in its famous March 16th paper, assumed an IFR of 0.9%. In fact, a WHO bulletin put the IFR at 0.23% as long ago as October 2020.
- This unwillingness to interrogate the modelling data that underpins the report’s conclusions is particularly odd, given that the authors acknowledge the limitations of modelling elsewhere – “Models can be useful and informative to policymakers, but they come with limitations” – and at one point try to blame the delay in lockdown down on an “overreliance on specific mathematical models”! Again it’s a case of one rule for me and another for thee.
- The report compares the response of the British government in the first months of the pandemic unfavourably to that of various East Asian and South East Asian governments, but overlooks the fact that many Asian countries that successfully suppressed infection by closing borders at the beginning of 2020, and rolling out successful test, trace and isolate programmes, are now in the grip of devastating waves in spite of having vaccinated large swathes of their populations. That suggests their non-pharmaceutical interventions only succeeded in postponing the impact of SARS-CoV-2, not avoiding it. (It also fails to note that these supposed role models didn’t issue stay-at-home orders, close schools or shutter businesses in their initial responses to the pandemic.)
- The report criticises the Government for stopping community testing in March 2020 due to PHE’s lack of testing capacity and praises Matt Hancock for setting the 100,000 tests a day target to galvanise the system into massively ramping up that capacity. Indeed, the authors claim that had a proper test-and-trace system been in place at the beginning of 2020, the initial lockdown might have been avoided. That, too, is a shaky assumption. After all, the Government has spent £37 billion and counting on a ‘world-beating’ test, trace and isolate programme but that didn’t stop us locking down for a second and third time. The authors of the report acknowledge this point, but blame Baroness Harding for not doing a better job of running NHS Test and Trace. That seems a tad harsh, particularly as the authors repeatedly say – Uriah Heap-like – that it’s not their intention to apportion blame for the mistakes they’ve identified.
- The report praises the speed at which the Nightingale hospitals were created, although it acknowledges that, for the most part, they weren’t used. But the reason they weren’t used is partly because the NHS lacked the trained employees to staff them with – ICU nurses, for instance. Perhaps if they’d been built with less speed – at a cost to the taxpayer of roughly half a billion pounds, don’t forget – the Government would have had time to spot this obvious flaw in the plan. Or, more realistically, those aware of it from the start would have had more time to organise and obstruct this expensive PR stunt.
- The authors praise the Government – and the NHS – for at no point running out of ICU beds and becoming overwhelmed, as the health system did in some parts of Italy during the first phase of the pandemic. But given the enormous cost of protecting the NHS – both in terms of seriously ill people who were either discharged or went untreated, as well as the collateral damage inflicted by the lockdowns on the economy, education, family life, mental health, etc. – it’s impossible to say whether prioritising the NHS at the expense of absolutely everything else was in fact the right strategy. To bottom that out you need to do some cost-benefit analysis, of which there is precisely none in this report.
- The report concludes by praising the Vaccine Taskforce under the leadership of Kate Bingham and highlights the ‘success’ of the U.K.’s vaccine programme – “one of the most effective in Europe and, for a country of our size one of the most effective in the world”. But they ignore the fact that the efficacy of the Covid vaccines is much less impressive than the initial trial data indicated and looks less impressive with each passing week, something Dr. Will Jones has been meticulously documenting for the Daily Sceptic. So was the massive Government expenditure on the development and trialling of home grown vaccines, as well as procuring hundreds of millions of vaccines manufactured overseas, worth it? One notable omission from the report is any acknowledgement of the risks associated with a fast-tracked vaccine approval process – it just breathlessly praises the speed with which vaccines were made available to the public and expresses the hope that “in the future this could be conducted in much shorter time still”.
Conclusion
This is a pretty feeble document that seems to have been written with an eye on getting Jeremy Hunt and Greg Clark – the chairs of the two select committees involved – on the BBC news rather than making a serious contribution to understanding what the Government got right and what it got wrong over the past 18 months. It’s hard to argue with some of its findings, but its headline conclusion – that the Government should have locked down earlier – isn’t based on any serious analysis, let alone a careful consideration of the evidence that seems to point in the opposite direction. Talk about groupthink!
I hope the official inquiry, when it comes, is a bit more intellectually weighty than this.
Are leaky vaccines driving delta variant evolution and making it more deadly?
by el gato malo – bad cattitude – october 10, 2021
one of the great fears in any vaccination campaign is that the vaccine can wind up becoming the driver viral evolution and making the virus more dangerous. this is a special concern around imperfect (so called “leaky”) vaccines that are non-sterilizing. such vaccines do not stop spread or contagion of the virus. this means the virus will have lots of chances to replicate.
when you combine this with a vaccine that reduces severity of cases and prevents deaths in the vaccinated, it’s a bit of a perfect storm. you get full spread but break the evolutionary gradient towards mildness that viruses tend to follow (and that protects humanity from them).
all a virus wants is to replicate. “make a copy of me and pass it on.” that’s the biological imperative of the selfish gene. excel at it, you win. fail, you disappear. simple as that.
killing or harming the host is maladaptive to viral spread. it’s like burning down your own house with your car in the garage. now you have nowhere to live and no way to get around. that’s not a recipe for reproductive fitness.
this is a property of the world, not of the viruses themselves. so it applies to all of them, evolved and lab hotwired alike.
so viruses evolve to become less, not more virulent. they do not want to kill you. ideally, they’d like to help you. figure out how to be a useful symbiote, and you get a huge boost in propagation. (mitochondria were probably bacteria that were so useful, all our cells incorporated them.) so seeing case fatality rate (CFR) rise in a variant of a virus is like watching water flow uphill. it’s not supposed to do that and when it does, you need to suspect some external force acting on it.
and we’re seeing water flow uphill here.
i started with the england variants of concern (VoC) data. it’s the best quality and the best broken out. (the US data is just plain broken. it’s being deliberately scrubbed to prevent analysis like this.) because this data is always aggregated from feb to current period, it does not provide good temporal snapshots, but this can be fixed by subtracting the penultimate report from the current one etc. you subtract report 22’s totals from report 23 and you get just what happened in the last 2 weeks (it used to be a weekly report, now it’s bi-weekly)
what we see is not what one would expect from a virus. none of the other variants (pre vaccine) worked like this. none saw CFR rise like this. and no jump from major variant to variant saw a statistically significant rise in deadliness.
this IS however what one would expect if a virus were undergoing vaccine mediated evolution (as mareks disease did in chickens) and selecting for hotter strains because vaccinated people can carry and spread them and not die.
experienced CFR on delta is nearly 7X what it was in the beginning of june and has been galloping since the middle of july.
(note that pretty much all this data has a large artifact in it from the 21 june report (VoC 17). there was a “data-dump” in it where they caught up on a bolus of past data. it’s an artifact, not a signal. best to ignore it. i suspect the curve from mid june to mid july was smooth.)
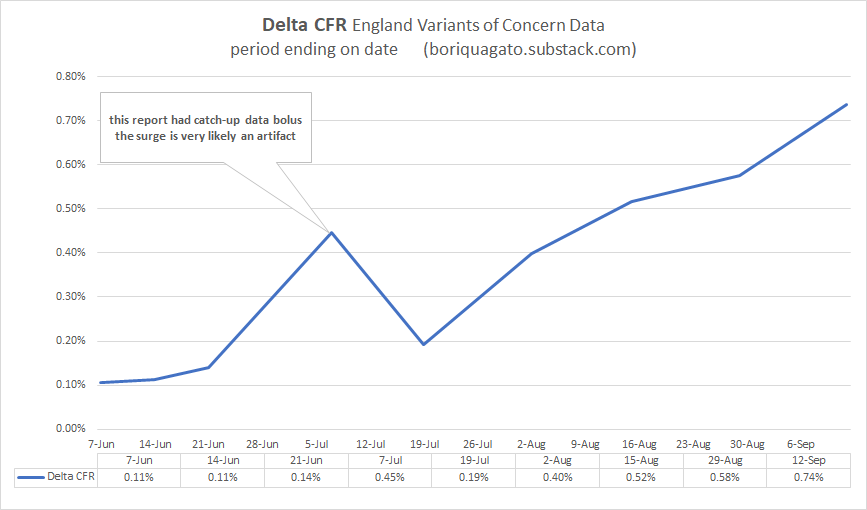
put simply: this is not good.
delta is rapidly approaching alpha (1.1%) in terms of CFR whereas it used to be 90% lower. (it also means that the reports on delta CFR in these VoC updates are FAR too low because they are a blend of all cases and deaths back to feb, so they are averaging in the low CFR past and are slow to respond to current dynamics)
this is consistent with, but not proof of vaccines mediated evolution. to get there, we need to do better.
so now we need to start ruling things out and validating this claim to see if it’s meaningful.
first, it’s not a simpson’s paradox in age data. CFR is rising in over and under 50’s. it’s not mix shift alone. CFR in over 50’s is up 2.5X. it’s up 4-7X in under 50’s.
we’re at about a 3X rise in CFR overall in delta since the summer once we adjust for shifts in age. not as worrying as 7, but still worrying.
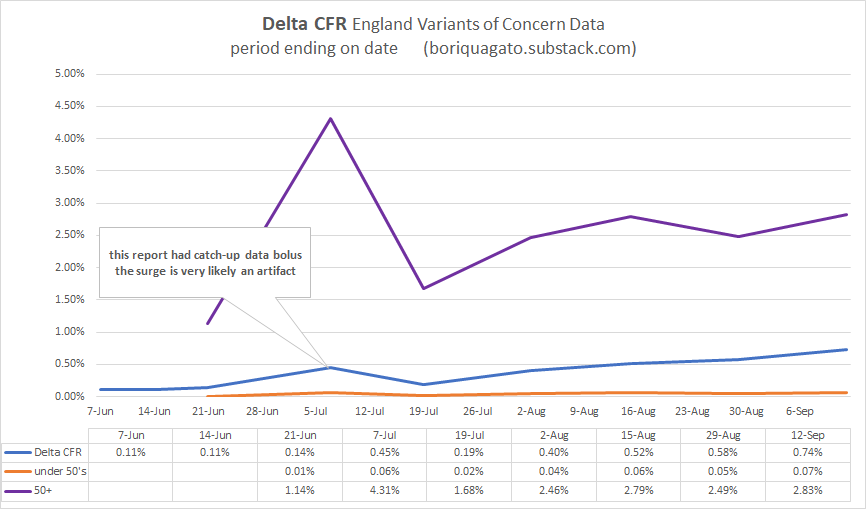
and the deaths are real. it’s not made up counting. this can be clearly seen when we comp CFR to the euro-momo Z scores (thoughtfully provided by frequent gato collaborator ben m at USmortality.com. z score is just a measure of deviation from expected all cause deaths. (explained HERE)
alignment is quite strong.
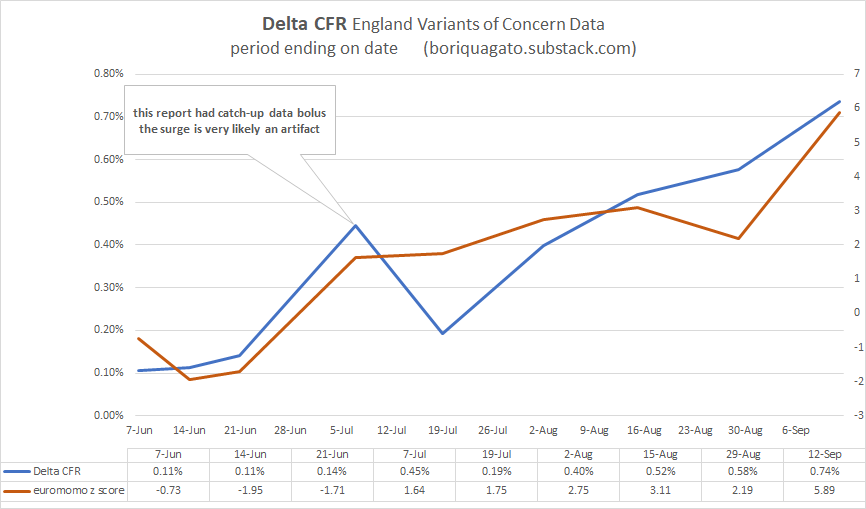
z score was trending negative and spiked to high levels just as CFR really started to ramp up.
z score for the year can be seen here. starting in wk 22 (may 31) (numbers after the year are weeks)
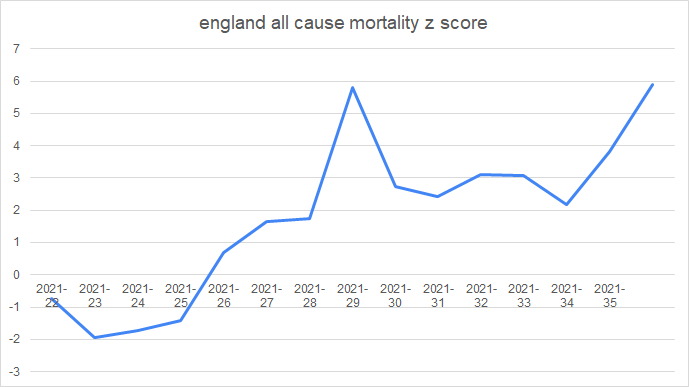
and given that we know that vaccines DO work to stop deaths in the UK (seemingly in the 50-60% range) it’s even more unexpected that CFR would be rising like this. but it is and the rise in the vaxx rate is not hampering it.
(the precise alignment here is more chart crime than signal, so i’d caution against inferring too much from it)
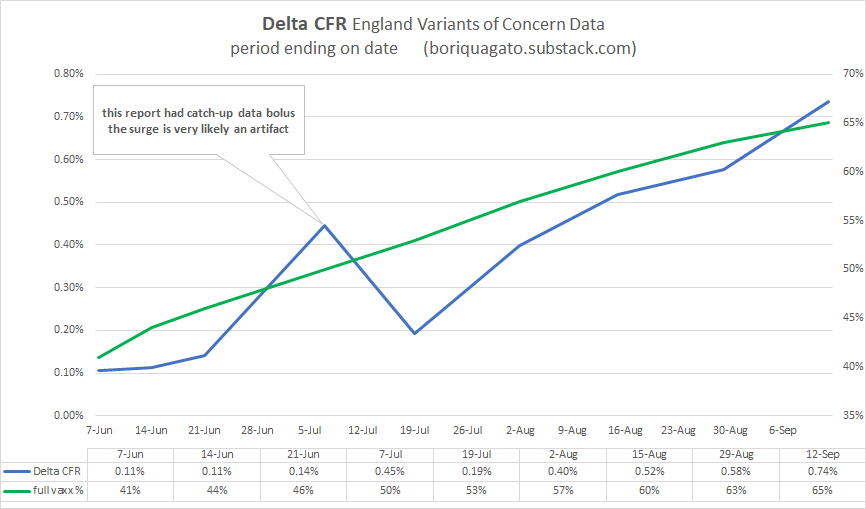
none of this is what one would expect. not remotely. it bucks evolution, it bucks the other variants, and it flies in the face of late stage pandemic dynamics like increase in acquired immunity (which IS sterilizing), depletion of high risk cohorts, improvements in treatment, etc. all these should be pushing CFR down.
instead, water is flowing uphill.
the question is “why?”
the other day, i discussed ADE (antibody dependent enhancement) where antibodies wind up acting as passkeys for a virus to enter cells and also the fetchingly biblically named OAS (original antigenic sin) whereby preferential training to one antibody response leads to its use against new variants of a pathogen and thereby prevents adaptation to more effective modalities.
note that these two phenomena are by no means mutually exclusive and are actually strongly synergistic.
but are they driving this issue?
i do not not think so.
- if they were, we’d be seeing the CFR rise in the vaccinated but not in the unvaccinated and if it were ALL antibodies, we’d be seeing the previously infected getting hit too. but they are not.
- we’d also likely be seeing low or negative vaccine efficacy (VE) for deaths. but we aren’t. it’s clear the vaccinated are doing better.
CFR is (and has been) much better in the vaccinated than the unvaxxed in UK over 50’s (the highest risk category). trends are similar, but absolute values durably disparate.
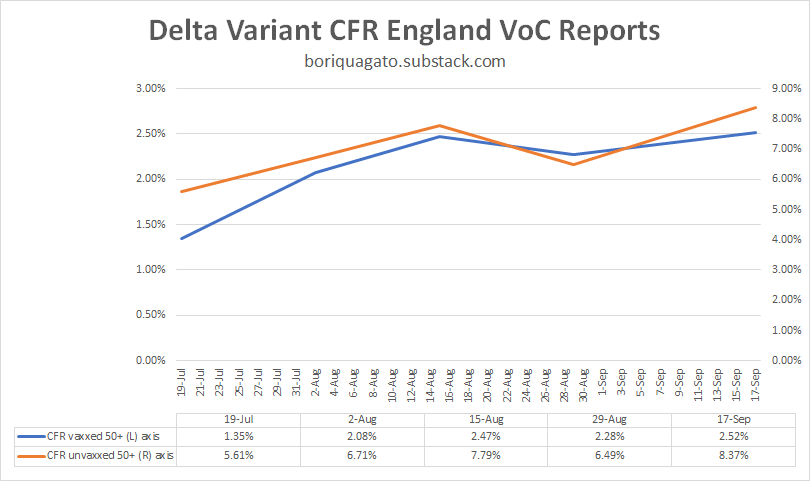
whether and to what extent this is real vaccine efficacy vs cohort bias in a place where 90% of this demographic is vaccinated remains an open issue. it may simply be that only those with the weakest/most compromised immunes systems have not gotten the jab. but this is not really material here.
what IS material is the fact that CFR in the unvaxxed is trending up significantly and so is CFR in the vaxxed. but we’re not seeing many cases of re-infection and almost none of those are serious. this does not look like ADE or OAS as a major driver. if it were, there’s no reason the CFR in the unvaccinated would be rising too.
what this IS consistent with is a variant heating up and getting more and more deadly because it is not checked by normal biological limitations. vaccine mediated evolution (VME) would be very bad news for us.
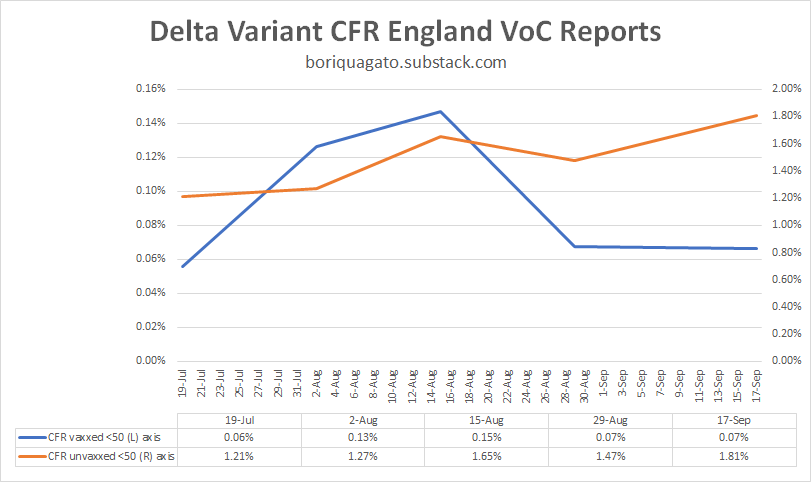
we can see similar in the under 50’s, though the data here is a bit of a mess as during this period, so many very low risk under 50’s (those under 18) got vaccinated that it moved a material risk profile reduction from unvaxxed to vaxxed. i suspect that is why “CFR vaxxed” dropped. it was not vaccines working, it was the vaccinated category being “salted” with large number of the lowest risk folks around. (it also means that group left the unvaxxed, so you get an effect on both)
so i view this data as much lower quality than over 50’s, but it still looks like VME, not ADE or OAS.
this is EXACTLY what leaky vaccines did in chickens.
(read these links. THIS in particular. it’s important.)
such vaccines change the evolutionary gradient for a virus. instead of becoming less virulent/deadly, they can tend the other way because the maladaptiveness of killing the host is mitigated in the vaccinated population. this is what happened with marek’s disease in chickens.
not only is it now more lethal to them than ebola is to humans, making it one of if not THE hottest persistent disease known (killing 100% of unvaxxed birds in 10 days), but, it’s now a disease so hot that an unvaccinated chicken cannot spread it. they die too quickly. only the vaccinated birds spread the nasty strains of mareks. they’re the only ones who live long enough to shed virus.
“Previously, a hot strain was so nasty, it wiped itself out. Now, you keep its host alive with a vaccine, then it can transmit and spread in the world,” Read said. “So it’s got an evolutionary future, which it didn’t have before.”

this is an awful lot of puzzle pieces snapping together and i think we’re really starting to see what this is a picture of.
leaky vaccines that stop severe illness and death but not spread look to be affecting the evolution of the covid 19 virus.
this is an established, predictable, and well supported risk from such vaccines.
this has become my leading hypothesis.
it also explains why we’re seeing such a large rise in deaths relative to cases and deaths and hospitalization overall in so many places. it’s the virus adapting to a stressor we put on it and becoming much more dangerous as a result.
the CFR is a function of the virus, but the virus has become a function of the leaky vaccines.
and it also means the vaccine is protecting no one. yes, it seems to have 50-60% protection against death. but what good is that against a CFR that’s up 300% or more (and rising)? everyone is worse off.

negative VE’s on spread are accelerating cases and this is multiplicative with higher CFR. this is the nightmare scenario and no one is left better off as a result. the CFR among the high risk vaccinated groups is way up too.
everyone is harmed but the brunt is borne by the unvaccinated which perversely winds up looking like better vaccine efficacy. the very fact that vaccines made everyone worse off but spread the misery unevenly makes it look like vaccines are a good idea.
it’s just simple math. if we do something to one group that makes their death rate rise from 1 to 2 per 100 but that also makes the death rate in another group rise from 1 to 4 per 100, that looks like a VE of 50%. in reality, it’s killing 100% more vaxxed people and 300% more of the unvaxxed.
mistaking that gas pedal for the brake and pushing ever harder when you fail to slow would represent an accelerating disaster curve.
that’s the problem with relative measures that ignore absolute changes. you can hide all manner of calamity in such analyses.
it’s still, of course, possible that i’m wrong, but this is looking more and more like it has to be the answer. i can find nothing else fits the facts and the facts themselves are weird enough that “it’s just normal” does not look like a satisfying explanation either and we have enough features here that we can really start testing our puzzle pieces. this one aligns in an AWFUL lot of places.
for something this odd to happen, it takes a truly uncommon exogenous stressor.
i’m just not seeing what else it could be than vaccine mediated selection for hotter variants driving pernicious delta evolution.
so, i’m putting this out to you all to see if you can find some other explanation for what’s going on that fits these facts.
looking forward to the peer review as, honestly, i hope i’m wrong here. this is not an outcome that anyone wants. it’s the nightmare scenario both as a pandemic and as a political horror in the making as if this was an “own-goal”, what would the experts and politicians that pushed this plan not be willing to do to avoid accepting the blame?
because this is career or pharma franchise polonium, and that’s if you’re lucky.
let’s keep at this. one way or the other, we need to know.
the facts do not care about our feelings and epidemiology data is a lousy fabric from which to spin a wubbie to hide under.
we need to get at the truth.
(even if it makes us make a face like this)

Australia Building Quarantine Camps For “Ongoing Operations”

By Paul Joseph Watson | Summit News | October 12, 2021
Despite some states tentatively beginning to lift lockdown restrictions, Australian authorities are building quarantine camps that won’t be completed until next year in order to prepare for “ongoing operations” and to house those “who have not had access to vaccination.”
According to ABC Australia, one such 1,000-bed quarantine facility at Wellcamp Airport outside Toowoomba will be fully completed by the end of March 2022.
“At this stage, the cabins will be used by domestic travellers returning from COVID hotspots,” states the report.
However, it also makes clear that the camp will be used for “ongoing operations” and will be a source of employment for the local area.
The camps is split into different zones and accommodates singles, doubles, and family rooms while being patrolled by police and security guards 24/7.
Citing new strains of COVID and people “who have not had access to vaccination,” Queensland Deputy Premier Steven Miles told the media outlet, “We anticipate there to be a continuing need for quarantine facilities.”
The government is leasing the land on which the camp is being built from the Wagner Corporation for 12 months with an option for a further 12 months after that.
Another 1,000-bed quarantine facility is also being built on a 30-hectare Army barracks site in the industrial area of Pinkenba, near Brisbane Airport.
“Why anyone who had left Australia would come back again is unclear,” writes Dave Blount. “It is possibly the most repressive country in the world regarding Covid tyranny.”
As we previously highlighted, state authorities in America are also constructing new “quarantine facilities” for Americans who are “unable to quarantine at home.”
As we reported last year, Authorities in Quebec City, Canada announced they will isolate “uncooperative” citizens in a coronavirus facility, the location of which remains a secret.
New Zealand also announced plans to place COVID infectees and their family members in “quarantine facilities.”
Back in January, German authorities also announced they would hold COVID dissidents who repeatedly fail to properly follow the rules in what was described as a ‘detention camp’ located in Dresden.
The Great New Normal Purge
By CJ Hopkins | The Consent Factory | October 12, 2021
So, the Great New Normal Purge has begun … right on cue, right by the numbers.
As we “paranoid conspiracy theorists” have been warning would happen for the past 18 months, people who refuse to convert to the new official ideology are now being segregated, stripped of their jobs, banned from attending schools, denied medical treatment, and otherwise persecuted.
Relentless official propaganda demonizing “the Unvaccinated” is being pumped out by the corporate and state media, government leaders, health officials, and shrieking fanatics on social media. “The Unvaccinated” are the new official “Untermenschen,” an underclass of subhuman “others” the New Normal masses are being conditioned to hate.
But it isn’t just a purge of “the Unvaccinated.” Anyone deviating from the official ideology is being systematically demonized and persecuted. In Germany, Australia, and other New Normal countries, protesting the New Normal is officially outlawed. The New Normal Gestapo is going around to people’s homes to interrogate them about their anti-New Normal Facebook posts. Corporations are openly censoring content that contradicts the official narrative. New Normal goon squads roam the streets, checking people’s “vaccination” papers.
And it’s not just governments and corporations carrying out the New Normal Purge. Friends are purging friends. Wives are purging husbands. Fathers are purging children. Children are purging parents. New Normals are purging old normal thoughts. Global “health authorities” are revising definitions to make them conform to New Normal “science.”
And so on … a new official “reality” is being manufactured, right before our eyes. Anything and anyone that doesn’t conform to it is being purged, unpersoned, memory-holed, erased.
None of which should come as a surprise.
Every nascent totalitarian system, at some stage of its takeover of society, launches a purge of political opponents, ideological dissidents, and other “anti-social deviants.” Such purges can be brief or open-ended, and they can take any number of outward forms, depending on the type of totalitarian system, but you cannot have totalitarianism without them.
The essence of totalitarianism — regardless of which costumes and ideology it wears — is a desire to completely control society, every aspect of society, every individual behavior and thought. Every totalitarian system, whether an entire nation, a tiny cult, or any other form of social body, evolves toward this unachievable goal … the total ideological transformation and control of every single element of society (or whatever type of social body it comprises). This fanatical pursuit of total control, absolute ideological uniformity, and the elimination of all dissent, is what makes totalitarianism totalitarianism.
Thus, each new totalitarian system, at some point in its evolution, needs to launch a purge of those who refuse to conform to its official ideology. It needs to do this for two basic reasons: (1) to segregate or otherwise eliminate actual political opponents and dissidents who pose a threat to the new regime; and (2) and more importantly, to establish the ideological territory within which the masses must now confine themselves in order to avoid being segregated, or eliminated.
The purge must be conducted openly, brutally, so that the masses understand that the rules of society have changed, forever, that their former rights and freedoms are gone, and that from now on any type of resistance or deviation from official ideology will not be tolerated, and will be ruthlessly punished.
The purge is usually launched during a “state of emergency,” under imminent threat from some official “enemy” (e.g., “communist infiltrators,” “counter-revolutionaries,” or … you know, a “devastating pandemic”), such that the normal rules of society can be indefinitely suspended “for the sake of survival.” The more terrified the masses can be made, the more willing they will be to surrender their freedom and follow orders, no matter how insane.
The lifeblood of totalitarianism is fear … fear of both the system’s official enemy (which is constantly stoked with propaganda) and of the totalitarian system itself. That the brutality of the system is rationalized by the threat posed by the official enemy doesn’t make it any less brutal or terrifying. Under totalitarian systems (of any type or scale) fear is a constant and there is no escape from it.
The masses’ fear is then channeled into hatred … hatred of the official “Untermenschen,” whom the system encourages the masses to scapegoat. Thus, the purge is also a means of allowing the masses to purge themselves of their fear, to transform it into self-righteous hatred and unleash it on the “Untermenschen” instead of the totalitarian system, which, obviously, would be suicidal.
Every totalitarian system — both the individuals running it and the system, structurally — instinctively understands how all this works. New Normal totalitarianism is no exception.
Just reflect on what has happened over the last 18 months.
Day after day, month after month, the masses have been subjected to the most destructive psychological-terror campaign in the history of psychological terror. Sadly, many of them have been reduced to paranoid, anus-puckering invalids, afraid of the outdoors, of human contact, afraid of their own children, afraid of the air, morbidly obsessed with disease and death … and consumed with hatred of “the Unvaccinated.”
Their hatred, of course, is utterly irrational, the product of fear and propaganda, as hatred of “the Untermenschen” always is. It has absolutely nothing to do with a virus, which even the New Normal authorities admit. “The Unvaccinated” are no more of a threat to anyone than any other human being … except insofar as they threaten the New Normals’ belief in their delusional ideology.
No, we are way past rationality at this point. We are witnessing the birth of a new form of totalitarianism. Not “communism.” Not “fascism.” Global-capitalist totalitarianism. Pseudo-medical totalitarianism. Pathologized totalitarianism. A form of totalitarianism without a dictator, without a definable ideology. A totalitarianism based on “science,” on “fact,” on “reality,” which it creates itself.
I don’t know about you, but, so far, it has certainly made quite an impression on me. So much so that I have mostly set aside my satirical schtick to try to understand it … what it actually is, why it is happening, why it is happening now, where it is going, and how to oppose it, or at least disrupt it.
The way I see it, the next six months will determine how successful the initial stages of the roll-out of this new totalitarianism will be. By April of 2022, either we’ll all be showing our “papers” to the New Normal Gestapo to be able to earn a living, attend a school, dine at a restaurant, travel, and otherwise live our lives, or we will have thrown a monkey wrench into the machinery. I do not expect GloboCap to abandon the roll-out of the New Normal over the longer term — they are clearly committed to implementing it — but we have the power to ruin their opening act (which they’ve been planning and rehearsing for quite some time).
So, let’s go ahead and do that, shall we? Before we get purged, or unpersoned, or whatever. I’m not sure, as I haven’t seen a “fact-check” yet, but I believe there are some commercial airline pilots in the USA who are showing us the way.
#
Sen. Ron Johnson Shares COVID-19 Data from Public Health England, Refutes “Pandemic of The Unvaccinated” Narrative
The Last Refuge | October 3, 2021
Senator Ron Johnson (R-Wisconsin) used his time on the Senate floor to discuss recently released COVID-19 data from Public Health England in the U.K. [DATA pdf Here]
Ironically, Senator Johnson is forced to use the Senate floor to share the information in an effort to stop government and Big Tech censorship of the discussion. Unlike the rest of the nation, the House and Senate chamber rules create a free speech zone that prohibits anyone from censoring congressional debate and discussion.
Senator Johnson outlines data from the U.K. clearly showing the vaccines offer no protection from the claimed Delta variant. COVID-19 is carried and shed by vaccinated individuals. The subsequent rate of COVID-19 hospitalization and COVID-19 death appears unaffected by the vaccine itself. WATCH:
As Senator Johnson notes: 63% of the deaths in the U.K. during the 7 month period being discussed were among the vaccinated population.
The data Ron Johnson is sharing is available HERE in pdf form
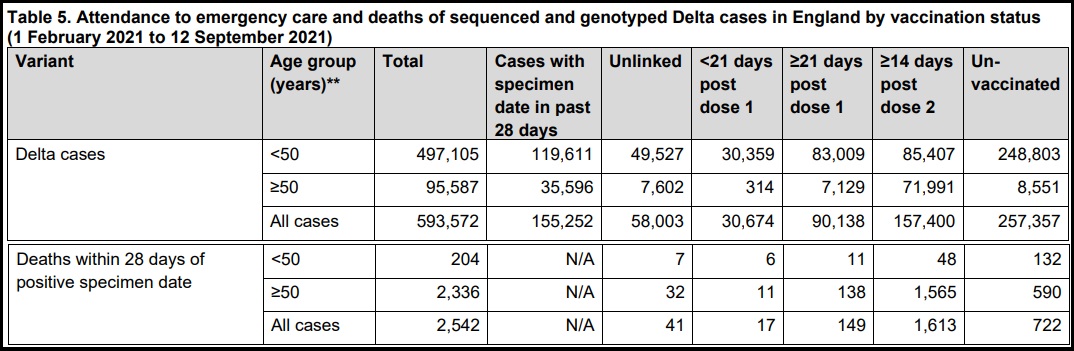
SOURCE: Page 19, 20 – Table 5

Featured Video
MIT Professsor Ted Postol: Patriot Missile Capabilties
or go to
Aletho News Archives – Video-Images
From the Archives
Neocons confess: “We did 9/11-anthrax”
By Kevin Barrett | Press TV | September 6, 2014
As the 13th anniversary of the crimes of September, 2001 approaches, the neoconservatives are shrieking from the rooftops – and effectively confessing that they were the real perpetrators of the 9/11-Anthrax false flag operation. (The neocons, you may recall, openly called for a “new Pearl Harbor” in September, 2000 – and got one exactly one year later.)
Every year at this time, the neocons orchestrate and hype a series of public relations stunts designed to magnify fears of “radical Islam” and reinforce their crumbling 9/11-Anthrax cover story. But this year’s propaganda campaign is so extreme that it represents a tacit confession: The neocons know that the truth about the 9/11-Anthrax operation is slowly closing in on them; so they are over-reacting by desperately trying to stoke the dying embers of the so-called War on Terror, in order to maintain the myth that Muslims (rather than neoconservative Zionists) attacked America in the autumn of 2001.
When a hysterical person exhibits guilty demeanor by trying too hard to blame a crime on someone else, that person is almost certainly the real perpetrator. As the neocons try much too hard to blame Islam for 9/11 and “terrorism” in general, their hysteria inadvertently reveals their own culpability. Like Shakespeare’s Lady MacBeth, the neoconservative movement has blood on its hands and “doth protest too much.” … continue
Blog Roll
 Aletho News
Aletho News- MIT Professsor Ted Postol: Patriot Missile Capabilties
- Israel Brings The War Rhetoric Towards Türkiye
- The Swiss summit of imperial humiliation
- Iran to continue IAEA cooperation under existing framework, SNSC decision: Baghaei
- Report highlights US munitions crisis: Missiles cannot be replenished quickly even with al the money in the world
- Iran’s Oil Spigot Could Open Soon But Hurdles Remain
- Trump’s Attempt to End the Iran War Infuriates the Uniparty
- First round of Swiss-hosted Iran-US talks ends with 5 key agreements
- What Is Hay Fever?
- IRAN WALKS OUT ON PEACE DEAL DUE TO TRUMP’S THREATS – w/ Prof. Seyed Mohammad Marandi
- If Americans Knew
- The Republican & Democratic Politicians Trying to Scuttle Iran Agreement
- Israel’s continued targeting of civilians in Lebanon renders ceasefire meaningless
- U.S. intelligence warns Israel is likely to undermine Iran peace deal, officials say
- In Gaza, Fathers Can’t Promise Their Children Food, Safety, or Even Survival
- This baby joins thousands of Gazans in need of medical evacuation
- Israel Kills Al Jazeera Journalist & Beloved Ecologist: 2 Articles
- Promoters of Israel: Leo Terrell, Ghana, Floyd Mayweather, Van Jones
- Gaza Soccer Player Who Dreamed of Competing in World Cup Can Now Barely Watch It
- Gaza baby loses mom and a leg; Palestinian prisoner tortured to death – Daily Update
- JNS Policy Summit to kick off in Israel
- No Tricks Zone
- 3 New Studies Find Increasing Trends In Solar Radiation Since The 1980s – Easily Explaining Warming
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
