According to Centers for Disease Control and Prevention data,1 COVID-19 “cases” have trended downward since peaking during the first and second week of January 2021.
At first glance, this decline appears to be occurring in tandem with the rollout of COVID shots. January 1, 2021, only 0.5% of the U.S. population had received a COVID shot. By mid-April, an estimated 31% had received one or more shots,2 and as of July 13, 48.3% were fully “vaccinated.”3
However, as noted in a July 12, 2021, STAT News article,4 “cases” had started their downward trend before COVID shots were widely used. “Following patterns from previous pandemics, the precipitous decline in new cases of Covid-19 started well before a meaningful number of people had been vaccinated,” Robert M. Kaplan, Professor Emeritus at the UCLA Fielding School of Public Health, writes. He continues:
“Nearly 50 years ago, medical sociologists John and Sonja McKinlay examined5 death rates from 10 serious diseases: tuberculosis, scarlet fever, influenzae, pneumonia, diphtheria, whooping cough, measles, smallpox, typhoid, and polio. In each case, the new therapy or vaccine credited with overcoming it was introduced well after the disease was in decline.
More recently, historian Thomas McKeown noted6 that deaths from bronchitis, pneumonia, and influenza had begun rapidly falling 35 years before the introduction of new medicines that were credited with their conquest. These historical analyses are relevant to the current pandemic.”
‘Case’ Decline Preceded Widespread Implementation of Jab
As noted by Kaplan, COVID-19 “cases” peaked in early January 2021. January 8, more than 300,000 new positive test results were recorded on a daily basis. By February 21, that had declined to a daily new case count of 55,000. COVID-19 gene modification injections were granted emergency use authorization at the end of December 2020, but by February 21, only 5.9% of American adults had been fully vaccinated with two doses.
Despite such a low vaccination rate, new “cases” had declined by 82%. Considering health authorities claim we need 70% of Americans vaccinated in order to achieve herd immunity and stop the spread of this virus, this simply makes no sense. Clearly, the COVID shots had nothing to do with the decline in positive test results.
To be clear, reported cases mean positive test results, and we now know the vast majority of positive PCR tests have been, and still are, false positives. They’re not sick. They simply had a false “positive.” Right now, we’re also faced with yet another situation that complicates attempts at data analysis, and Kaplan understandably did not address any of these confounding factors.
But just so you’re aware, if you have been fully “vaccinated,” then the CDC recommends running the PCR test at a cycle threshold (CT) of 28 or lower, which dramatically lowers your chance of a false positive result, but if you are unvaccinated, the PCR test is recommended to be run at a CT of 40 or higher, virtually guaranteeing a false positive.
This is just one way by which the CDC is manipulating data to make the COVID shots appear more effective than they are. This also allows them to falsely claim that the vast majority of new cases are among the unvaccinated.
Naturally, if unvaccinated are tested in such a way as to maximize false positives, then they’re going to make up the bulk of the so-called caseload. In reality, though, the vast majority of them aren’t sick.
Meanwhile, those who have received the jabs only count as a COVID case if they’re hospitalized and/or die with a positive test result. These widely differing testing strategies skew the data and allow for false interpretations to be made.
Natural Immunity Explains Decline in Cases
As noted by Kaplan, the most reasonable explanation for declining rates of SARS-CoV-2 appears to be natural immunity from previous infections, which vary considerably from state to state.7 He goes on to cite a study8 by the National Institutes of Health, which suggests SARS-CoV-2 prevalence was 4.8 times higher than previously thought, thanks to undiagnosed infection.
In other words, they claim that for every reported positive test result, there were likely nearly five additional people who had the infection but didn’t get a diagnosis. To analyze this data further, Kaplan calculated the natural immunity rate by dividing the new estimated number of people naturally infected by the population of any given state. He writes:9
“By mid-February 2021, an estimated 150 million people in the U.S. (30 million times five) may have had been infected with SARS-CoV-2. By April, I estimated the natural immunity rate to be above 55% in 10 states: Arizona, Iowa, Nebraska, North Dakota, Oklahoma, Rhode Island, South Dakota, Tennessee, Utah, and Wisconsin.
At the other end of the continuum, I estimated the natural immunity rate to be below 35% in the District of Columbia, Hawaii, Maine, Maryland, New Hampshire, Oregon, Puerto Rico, Vermont, Virginia, and Washington …
By the end of 2020, new infections were already rapidly declining in nearly all of the 10 states where the majority may have had natural immunity, well before more than a minuscule percentage of Americans were fully vaccinated. In 80% of these states, the day when new cases were at their peak occurred before vaccines were available.
In contrast, the 10 states with lower rates of previous infections were much more likely to experience new upticks in Covid-19 cases in March and April … By the end of May, states with fewer new infections had significantly lower vaccination rates than states with more new infections.”
COVID Shots Cannot Eliminate COVID-19
So, SARS-CoV-2 cases were actually higher in states where natural immunity was low but vaccination rates were high. Meanwhile, in states where natural immunity due to undiagnosed exposure was high, but vaccination rates were low, the daily new caseload was also lower.
This makes sense if natural immunity is highly effective (which, historically it has always been and there’s no reason to suspect SARS-CoV-2 is any different in that regard). It also makes sense if the COVID shots aren’t really offering any significant protection against infection, which we also know is the case.
Vaccine manufacturers have already admitted these COVID shots will not provide immunity, meaning they will not prevent you from being infected. The idea behind these gene modification injections is that if/when you do get infected, you’ll hopefully experience milder symptoms, even though you’re still infectious and can spread the virus to others.
Kaplan ends his analysis by saying that COVID shots are a safer way to achieve herd immunity, and that they are “the best tool available for assuring that the smoldering fire of [COVID-19] is extinguished.” I disagree, based on two major issues.
First, and perhaps most importantly, this is an untested “vaccine” and we have no idea of the short-term let alone long-term damage it will cause, as any reasonable effort at collecting this data has been actively suppressed. Secondly, the survivability of COVID-19 outside of nursing homes is 99.74%. If you’re under the age of 40, your chance of surviving a bout of COVID-19 is 99.99%.10,11,12
You can’t really improve your chances of surviving beyond that, so COVID shots cannot realistically end the pandemic. Meanwhile, the COVID shots come with an ever-growing list of potential side effects that can take years if not decades off your natural life span. The shots are particularly unnecessary for anyone with natural immunity,13 yet that’s what the CDC recommends.14
Why Push COVID Jab on Those with Natural Immunity?
In January 2021, Dr. Hooman Noorchashm, a cardiac surgeon and patient advocate, sent a public letter15 to the U.S. Food and Drug Administration commissioner detailing the risks of vaccinating individuals who have previously been infected with SARS-CoV-2, or who have an active SARS-CoV-2 infection.
He urged the FDA to require prescreening for SARS-CoV-2 viral proteins to reduce the risk of injuries and deaths following vaccination, as the vaccine may trigger an adverse immune response in those who have already been infected with the virus. In March 2021, Fox TV host Tucker Carlson interviewed him about these risks. In that interview, Noorchashm said:16
“I think it’s a dramatic error on part of public health officials to try to put this vaccine into a one-size-fits-all paradigm … We’re going to take this problem we have with the COVID-19 pandemic, where a half-percent of the population is susceptible to dying, and compound it by causing totally avoidable harm by vaccinating people who are already infected …
The signal is deafening, the people who are having complications or adverse events are the people who have recently or are currently or previously infected [with COVID]. I don’t think we can ignore this.”
In an email to The Defender, Noorchashm fleshed out his concerns, saying:17
“Viral antigens persist in the tissues of the naturally infected for months. When the vaccine is used too early after a natural infection, or worse during an active infection, the vaccine force activates a powerful immune response that attacks the tissues where the natural viral antigens are persisting. This, I suggest, is the cause of the high level of adverse events and, likely deaths, we are seeing in the recently infected following vaccination.”
Despite being widely ignored, Noorchashm continues to push for the implementation of prevaccine screening using PCR or rapid antigen testing to determine whether the individual has an active infection, and an IgG antibody test to determine past infection.
If either test is positive, he recommends delaying vaccination for a minimum of three to six months to allow your IgG levels to wane. At that point, he recommends testing your blood IgG level and use that as a guide to decide the timing of your vaccination.
Those with Natural Immunity Have Higher Risk of Side Effects
Mere weeks after Noorchashm’s letter to the FDA, an international survey18 confirmed his concerns. After surveying 2,002 people who had received a first dose of COVID-19 vaccine, they found that those who had previously had COVID-19 experienced “significantly increased incidence and severity” of side effects, compared to those who did not have natural immunity.
The mRNA COVID-19 vaccines were linked to a higher incidence of side effects compared to the viral vector-based COVID-19 vaccines, but tended to be milder, local reactions. Systemic reactions, such as anaphylaxis, flu-like illness and breathlessness, were more likely to occur with the viral vector COVID-19 vaccines.
Like Noorchashm before them, the researchers called on health officials to reevaluate their vaccination recommendations for people who’ve had COVID-19:19
“People with prior COVID-19 exposure were largely excluded from the vaccine trials and, as a result, the safety and reactogenicity of the vaccines in this population have not been previously fully evaluated. For the first time, this study demonstrates a significant association between prior COVID19 infection and a significantly higher incidence and severity of self-reported side effects after vaccination for COVID-19.
Consistently, compared to the first dose of the vaccine, we found an increased incidence and severity of self-reported side effects after the second dose, when recipients had been previously exposed to viral antigen.
In view of the rapidly accumulating data demonstrating that COVID-19 survivors generally have adequate natural immunity for at least 6 months, it may be appropriate to re-evaluate the recommendation for immediate vaccination of this group.”
CDC Misrepresents Data to Push Jab on Those with Immunity
So far, the CDC has refused to change its stance on the matter. Instead, officials at the agency seem to have doubled down and actually go out of their way to misrepresent data in an effort to harass those with natural immunity to inappropriately take the jab, which is clearly clinically unnecessary.
In a report issued by the CDC’s Advisory Committee on Immunization Practices (ACIP) December 18, 2020, the Pfizer-BioNTech COVID-19 vaccine was said to have “consistent high efficacy” of 92% or more among people with evidence of previous SARS-CoV-2 infection.20
After looking at the Pfizer trial data, Rep. Thomas Massie — a Republican Congressman for Kentucky and an award-winning scientist in his own right — discovered that’s completely wrong. In a January 30, 2021, Full Measure report, investigative journalist Sharyl Attkisson described how Massie tried, in vain, to get the CDC to correct its error. According to Massie:21,22
“There is no efficacy demonstrated in the Pfizer trial among participants with evidence of previous SARS-CoV-2 infections and actually there’s no proof in the Moderna trial either …
It [the CDC report] says the exact opposite of what the data says. They’re giving people the impression that this vaccine will save your life, or save you from suffering, even if you’ve already had the virus and recovered, which has not been demonstrated in either the Pfizer or the Moderna trial.”
After multiple phone calls, CDC deputy director Dr. Anne Schuchat finally acknowledged the error and told Massie it would be fixed. “As you note correctly, there is not sufficient analysis to show that in the subset of only the people with prior infection, there’s efficacy. So, you’re correct that that sentence is wrong and that we need to make a correction of it,” Schuchat said in the recorded call.
January 29, 2021, the CDC issued its supposed correction, but rather than fix the error, they simply rephrased the mistake in a different way. This was the “correction” they issued:
“Consistent high efficacy (≥92%) was observed across age, sex, race, and ethnicity categories and among persons with underlying medical conditions. Efficacy was similarly high in a secondary analysis including participants both with or without evidence of previous SARS-CoV-2 infection.”
As you can see, the “correction” still misleadingly suggests that vaccination is effective for those previously infected, even though the data showed no such thing. Children of ever-younger ages are also being pushed to get the COVID jab, even though they have the absolute lowest risk of dying from COVID-19 of any group.
Data23 from the first 12 months of the pandemic in the U.K. show just 25 people under the age of 18 died from or with COVID-19.24 In all, 251 children under 18 were admitted to intensive care between March 2020 and February 2021. The absolute risk of death from COVID-19 in children is 2 in 1 million.
Vaccine Provides Far Less Protection Than Natural Immunity
While some claim vaccine-induced immunity offers greater protection against SARS-CoV-2 infection than natural immunity, historical and current real-world data simply fail to support this non-common sense assertion.
As recently reported by Attkisson25,26 and David Rosenberg 7 Israeli National News,27 recent Israeli data show those who have received the COVID jab are 6.72 times more likely to get infected than people who have recovered from natural infection.
Among the 7,700 new COVID cases diagnosed so far during the current wave of infections that began in May 2021, 39% were vaccinated (about 3,000 cases), 1% (72 patients) had recovered from a previous SARS-CoV-2 infection and 60% were neither vaccinated nor previously infected. Israeli National News notes:28
“With a total of 835,792 Israelis known to have recovered from the virus, the 72 instances of reinfection amount to 0.0086% of people who were already infected with COVID.
By contrast, Israelis who were vaccinated were 6.72 times more likely to get infected after the shot than after natural infection, with over 3,000 of the 5,193,499, or 0.0578%, of Israelis who were vaccinated getting infected in the latest wave.”
Breakthrough Infections Are on the Rise
Other Israeli data also suggest the limited protection offered by the COVID shot is rapidly eroding. August 1, 2021, director of Israel’s Public Health Services, Dr. Sharon Alroy-Preis, announced half of all COVID-19 infections were among the fully vaccinated.29 Signs of more serious disease among fully vaccinated are also emerging, she said, particularly in those over the age of 60.
Even worse, August 5, Dr. Kobi Haviv, director of the Herzog Hospital in Jerusalem, appeared on Channel 13 News, reporting that 95% of severely ill COVID-19 patients are fully vaccinated, and that they make up 85% to 90% of COVID-related hospitalizations overall.30
Other areas where a clear majority of residents have been vaccinated are also seeing spikes in breakthrough cases. In Gibraltar, which has a 99% COVID jab compliance rate, COVID cases have risen by 2,500% since June 1, 2021.31
US Outbreak Shatters ‘Pandemic of Unvaccinated’ Narrative
An investigation by the CDC32,33 also dispels the narrative that we’re in a “pandemic of the unvaccinated.” An outbreak in Barnstable County, Massachusetts, resulted in 469 new COVID cases among residents who had traveled into town between July 3 and July 17, 2021.
Of these cases, 74% were fully vaccinated, as were 80% of those requiring hospitalization.Most, but not all, had the Delta variant of the virus. The CDC also found that fully vaccinated individuals who contract the infection had as high a viral load in their nasal passages as unvaccinated individuals who got infected.34 This means the vaccinated are just as infectious as the unvaccinated. According to Attkisson:35
“CDC’s newest findings on so-called ‘breakthrough’ infections in vaccinated people are mirrored by other data releases. Illinois health officials recently announced36 more than 160 fully-vaccinated people have died of Covid-19, and at least 644 been hospitalized; 10 deaths and 51 hospitalizations counted in the prior week …
In July, New Jersey reported 49 fully vaccinated residents had died of Covid; 27 in Louisiana; 80 in Massachusetts … Nationally, as of July 12, CDC said it was aware of more than 4,400 people who got Covid-19 after being fully vaccinated and had to be hospitalized; and 1,063 fully vaccinated people who died of Covid.”
It is important to note this data is over 1 month old now and it is likely that many thousands of fully “vaccinated” have now died from COVID-19.
Natural Immunity Appears Robust and Long-Lasting
An argument we’re starting to hear more of now is that even though natural immunity after recovery from infection appears to be quite good, “we don’t know how long it’ll last.” This is rather disingenuous, seeing how natural immunity is typically lifelong, and studies have shown natural immunity against SARS-CoV-2 is at bare minimum longer lasting than vaccine-induced immunity.
Here’s a sampling of scholarly publications that have investigated natural immunity as it pertains to SARS-CoV-2 infection. There are several more in addition to these:
Science Immunology October 202038 found that “RBD-targeted antibodies are excellent markers of previous and recent infection, that differential isotype measurements can help distinguish between recent and older infections, and that IgG responses persist over the first few months after infection and are highly correlated with neutralizing antibodies.”
The BMJ January 202139 concluded that “Of 11, 000 health care workers who had proved evidence of infection during the first wave of the pandemic in the U.K. between March and April 2020, none had symptomatic reinfection in the second wave of the virus between October and November 2020.”
Science February 202140 reported that “Substantial immune memory is generated after COVID-19, involving all four major types of immune memory [antibodies, memory B cells, memory CD8+ T cells, and memory CD4+ T cells]. About 95% of subjects retained immune memory at ~6 months after infection. Circulating antibody titers were not predictive of T cell memory.
Thus, simple serological tests for SARS-CoV-2 antibodies do not reflect the richness and durability of immune memory to SARS-CoV-2.” A 2,800-person study found no symptomatic reinfections over a ~118-day window, and a 1,246-person study observed no symptomatic reinfections over 6 months.
A February 2021 study posted on the prepublication server medRxiv41 concluded that “Natural infection appears to elicit strong protection against reinfection with an efficacy ~95% for at least seven months.”
An April 2021 study posted on medRxiv42 reported “the overall estimated level of protection from prior SARS-CoV-2 infection for documented infection is 94.8%; hospitalization 94.1%; and severe illness 96·4%. Our results question the need to vaccinate previously-infected individuals.”
Another April 2021 study posted on the preprint server BioRxiv43 concluded that “following a typical case of mild COVID-19, SARS-CoV-2-specific CD8+ T cells not only persist but continuously differentiate in a coordinated fashion well into convalescence, into a state characteristic of long-lived, self-renewing memory.”
A May 2020 report in the journal Immunity 44 confirmed that SARS-CoV-2-specific neutralizing antibodies are detected in COVID-19 convalescent subjects, as well as cellular immune responses. Here, they found that neutralizing antibody titers do correlate with the number of virus-specific T cells.
A May 2021 Nature article45 found SARS-CoV-2 infection induces long-lived bone marrow plasma cells, which are a crucial source of protective antibodies. Even after mild infection, anti-SARS-CoV-2 spike protein antibodies were detectable beyond 11 months’ post-infection.
A May 2021 study in E Clinical Medicine 46 found “antibody detection is possible for almost a year post-natural infection of COVID-19.” According to the authors, “Based on current evidence, we hypothesize that antibodies to both S and N-proteins after natural infection may persist for longer than previously thought, thereby providing evidence of sustainability that may influence post-pandemic planning.”
Cure-Hub data47 confirm that while COVID shots can generate higher antibody levels than natural infection, this does not mean vaccine-induced immunity is more protective. Importantly, natural immunity confers much wider protection as your body recognizes all five proteins of the virus and not just one. With the COVID shot, your body only recognizes one of these proteins, the spike protein.
A June 2021 Nature article48 points out that “Wang et al. show that, between 6 and 12 months after infection, the concentration of neutralizing antibodies remains unchanged. That the acute immune reaction extends even beyond six months is suggested by the authors’ analysis of SARS-CoV-2-specific memory B cells in the blood of the convalescent individuals over the course of the year.
These memory B cells continuously enhance the reactivity of their SARS-CoV-2-specific antibodies through a process known as somatic hypermutation. The good news is that the evidence thus far predicts that infection with SARS-CoV-2 induces long-term immunity in most individuals.”
Another June Nature paper concluded that “In the absence of vaccination antibody reactivity [to the receptor binding domain (RBD) of SARS-CoV-2], neutralizing activity and the number of RBD-specific memory B cells remain relatively stable from 6 to 12 months.” According to the authors, the data suggest “immunity in convalescent individuals will be very long lasting.”
What Makes Natural Immunity Superior?
The reason natural immunity is superior to vaccine-induced immunity is because viruses contain five different proteins. The COVID shot induces antibodies against just one of those proteins, the spike protein, and no T cell immunity. When you’re infected with the whole virus, you develop antibodies against all parts of the virus, plus memory T cells.
This also means natural immunity offers better protection against variants, as it recognizes several parts of the virus. If there are significant alternations to the spike protein, as with the Delta variant, vaccine-induced immunity can be evaded. Not so with natural immunity, as the other proteins are still recognized and attacked.
Not only that but the COVID jabs actually actively promote the production of variants for which they provide virtually no protection at all, while those with natural immunity do not cause variants and are nearly universally protected against them.
If we are to depend on vaccine-induced immunity, as public health officials are urging us to do, we’ll end up on a never-ending booster treadmill. Boosters will absolutely be necessary, as the shot offers such narrow protection against a single protein of the virus. Already, Moderna has publicly stated that the need for additional boosters is expected.
Ultimately It’s About Wealth Transfer, Power and Control
Government agencies typically don’t issue recommendations without ulterior motives. Since current recommendations make absolutely no sense from a medical and scientific standpoint, what might the reason be for these illogical and reprehensibly unethical recommendations to inject people who don’t need it with experimental gene modification technology?
Why are they so hell-bent on getting a needle in every arm? And why are they refusing to perform any kind of risk-benefit analysis?
Data already indicate these COVID-19 injections could be the most dangerous medical product we’ve ever seen, and a June 24, 2021, peer-reviewed study published in the medical journal Vaccines warned we are in fact killing nearly as many with the shots as would die from COVID-19 itself.50
Using data from a large Israeli field study and two European drug reactions databases, they recalculated the NNTV for Pfizer’s mRNA shot. To prevent one case of COVID-19, anywhere between 200 and 700 had to be injected. To prevent a single death, the NNTV was between 9,000 and 50,000, with 16,000 as a point estimate.
Meanwhile, the number of people reporting adverse reactions from the shots was 700 per 100,000 vaccinations. For serious side effects, there were 16 reports per 100,000 vaccinations, and the number of fatal side effects was 4.11 per 100,000 vaccinations.
The final calculation suggested that for every three COVID-19 deaths prevented, two died from the shots. “This lack of clear benefit should cause governments to rethink their vaccination policy,” the authors concluded.
As has become the trend, a letter expressing “concern” about the study was published June 28, 2021, resulting in the paper being abruptly retracted July 2, 2021, against the authors’ objections. They disagreed with the accusation that their data and subsequent conclusion were misrepresentative, but the paper was retracted before they had time to publish a rebuttal.
Based on everything we’ve discovered so far, it seems a pandemic virus industrial complex is running the show, with a goal to eliminate medical rights and personal freedoms in order to centralize power, control and wealth.
By the looks of things, the COVID-19 mass psychosis and loss of any rational thinking by nearly half the population will continue to persist as long as the propaganda continues. Fear will continue and if need be, other engineered viruses may be released, for which they’ll create even more gene modification injections.
I believe the truth will eventually be so overwhelming, it’ll sweep away the confusion and the lies.
Renowned physician and professor of medicine Dr. Peter McCullough describes early treatment protocols for COVID-19 that have saved countless lives… and the forces that have aligned themselves against their widespread adoption.
Below are resources for early outpatient treatment:
In June 2021, the U.S. National Security Council released a new “National Strategy for Countering Domestic Terrorism” document.1 While it’s being largely framed as a tool to fight White supremacy and political extremism, the definition of what constitutes a “domestic terrorist” is incredibly vague and based on ideologies rather than specific behaviors.
It’s not difficult to imagine this policy being used to silence political opposition simply by labeling anyone who disagrees with the government as a domestic terrorist and charging them with a hate crime.
We’re already seeing signs suggesting that this is the path we’re on. July 28, 2021, Dr. Peter Hotez published a paper2 in PLOS Biology titled “Mounting Antiscience Aggression in the United States,” in which he suggests criticizing Dr. Anthony Fauci and other scientists ought to be labeled a “hate crime.” Commenting on the paper, Paul Joseph Watson at Summit News writes:3
“This is yet another transparent effort to dehumanize anti-lockdown protesters and demonize people who merely want to exercise bodily autonomy while elevating Fauci and his ilk to Pope-like status. Science isn’t supposed to be a religious dogma that is set in stone, it’s an ever-evolving knowledge base that changes and improves thanks to dissent and skepticism.”
Science Depends on Questioning and Challenging Assumptions
Attorney Jonathan Turley also responded to Hotez’s paper in an August 4, 2021, blog post, saying:4
“’Religion is a culture of faith; science is a culture of doubt.’ Feynman’s statement captures how science depends upon constant questioning and challenging of assumptions …
[T]here remain important debates over not just the underlying science relation to Covid-19 but the implications for such science for public policies. Criminalizing aspects of that debate would ratchet up the threats against those with dissenting views, including some scientists. That would harm not just free speech but science in the long run.”
Should We Have Protected Classes That Cannot Be Questioned?
Turley also points out how making scientists a protected class (and one would assume only those with specific political leanings) is a slippery slope that will likely have unwieldy ramifications:5
“The federal hate crime laws focus on basis of a person’s characteristics of race, religion, ethnicity, nationality, gender, sexual orientation, and gender identity. We have seen calls for adding professions like police officers, which I also opposed.
As with police officers, the inclusion of such professions would have a direct and inimical impact on free speech in our society. Indeed, it would create a slippery slope as other professions demand inclusion from reporters to ministers to physicians. Hate crimes would quickly apply to a wide array of people due to their occupations.”
Will America Accept No-Fly List for Unvaccinated?
Writing for The Atlantic,6 former assistant secretary for Homeland Security Juliette Kayyem posits that people who do not want to be part of the COVID injection experiment “need to bear the burden” when it comes to preventing the spread of SARS-CoV-2.
“The number of COVID-19 cases keeps growing, even though remarkably safe, effective vaccines are widely available,” Kayyem writes.7 “Many public agencies are responding by reimposing masking rules on everyone.
But at this stage of the pandemic, tougher universal restrictions are not the solution to continuing viral spread. While flying, vaccinated people should no longer carry the burden for unvaccinated people.
The White House has rejected a nationwide vaccine mandate … but a no-fly list for unvaccinated adults is an obvious step that the federal government should take.
It will help limit the risk of transmission at destinations where unvaccinated people travel — and, by setting norms that restrict certain privileges to vaccinated people, will also help raise the stagnant vaccination rates that are keeping both the economy and society from fully recovering.”
Travel Ban Identified as Effective Coercion Strategy
According to Kayyem, traveling in general and flying in particular is not a human right, and putting unvaccinated individuals on a no-fly list is a matter of national security, in the sense that the country needs to protect itself from people capable of spreading this dangerous virus.
She makes no mention of the scientifically confirmed fact that none of the COVID shots actually prevent you from getting infected, and that “vaccinated” individuals carry the same viral load as the unvaccinated,8,9 which means they’re just as infectious. The main difference is that vaccinated individuals might not realize that they’re carriers, as the primary effect when the injections do work is lessening symptoms of infection.
Kayyem also cites a New York Times and Kaiser Family Foundation poll in which 41% of unvaccinated respondents had said prohibition on airline travel would sway their decision, including 11% of those “adamantly opposed” to vaccination. In other words, where free doughnuts and million-dollar lotteries have failed to coerce people to get the shot, an airline travel ban might do the trick.
Despite her former position within government, she makes no mention of laws forbidding coercion of medical volunteers, such as the U.S. Code of Federal Regulations 45 CFR 46 (subpart A, the Belmont report),10 the International Covenant on Civil and Political Rights treaty,11 the Declaration of Helsinki12 or the Nuremberg Code.13 Supreme court rulings have also clarified that Americans have the right to choose their own health care in general.14,15
Reframing to Confuse the Issue
Kayyem suggests circumventing such basic human rights by reframing the issue. She writes:16
“The public debate about making vaccination a precondition for travel, employment, and other activities has described this approach as vaccine mandates, a term that … suggests that unvaccinated people are being ordered around arbitrarily.
What is actually going on, mostly, is that institutions are shifting burdens to unvaccinated people … rather than imposing greater burdens on everyone.
Americans still have a choice to go unvaccinated, but that means giving up on certain societal benefits. Nobody has a constitutional right to attend The Lion King on Broadway or work at Disney or Walmart … People who still want to wait and see about the vaccines can continue doing so. They just can’t keep pushing all the costs on everyone else.”
As pointed out by Swift Headline,17 the owner of Atlantic magazine, Laurene Powell Jobs, the billionaire widow of Steve Jobs, owns two private jets herself, giving her the freedom to fly around the world at will, regardless what vaccine mandates might be in place. Many other ultra-rich individuals would also be able to ignore the rules due to wealth alone, essentially turning them into a protected class. Swift Headline points out this projection:18
“The Atlantic went on to say unvaccinated people who are exercising their individual rights as free Americans ‘do not deserve’ to be a ‘protected class’ …
Jobs’s wealth and class status is detailed in Breitbart News’ Editor-in-Chief Alex Marlow’s book, ‘Breaking the News: Exposing the Establishment Media’s Hidden Deals and Secret Corruptions,’ which ‘exposes the hidden connections between the establishment media and the activist left.’
As Marlow details, Jobs’s past is a privileged one … Jobs ‘married well and inherited a lot of money, and her wealth is tied up in some of world’s biggest companies,’ Marlow continues. ‘She is the establishment.’”
The Price of Admission to Society
August 2, 2021, the San Francisco Chronicle also published an opinion piece19 by the Chronicle editorial board, in which they suggested we ought to “Make vaccination the price of admission to society.” One way to evaluate the reasonableness of such a proposition is to replace COVID “vaccination” with anything else. How about: “Make proof of contraception use the price of admission to bars and nightclubs.”
“Make clear skin the price of admission to gyms and public swimming pools.” “Make being taller than 5’ 9” the price of admission to theme parks.” “Make having a BMI below 25 the price of admission to airline flights.” “Make proof of not having an illness the price of admission to in-hospital care.”
According to the Chronicle editorial board, “the unvaccinated account for over 95% of hospitalizations and deaths.”20 The board does not cite where it got that data from, so let’s review the source of that data.
In an August 5, 2021, video statement, Centers for Disease Control and Prevention director Dr. Rochelle Walensky noted that this statistic was obtained by looking at hospitalization and mortality data from January through June 2021 — a timeframe during which the vast majority of the United States population were unvaccinated.
When you look at more recent data, the trend is swinging in the opposite direction.
January 1, 2021, only 0.5% of the U.S. population had received a COVID shot. By mid-April, an estimated 31% had received one or more shots,21 and as of June 15, 48.7% were fully “vaccinated.”22
The CDC has also pointed out that you are not considered “fully vaccinated” until two weeks after your second dose (in the case of Pfizer or Moderna), which is given six weeks after your first shot.23 This means that if you receive your first dose on June 1, you won’t be “fully vaccinated” until eight weeks later, around August 1.
So, the narrative that we’re in a “pandemic of the unvaccinated” was created by using statistics from a time period when the U.S. as a whole was largely unvaccinated. When you look at more recent data, the trend is swinging in the opposite direction.
Vaccinated Now Comprise the Bulk of Hospitalizations
For example, August 1, 2021, Dr. Sharon Alroy-Preis, director of Israel’s Public Health Services, announced half of all COVID-19 infections were among the fully vaccinated.24
A few days later, August 5, Dr. Kobi Haviv, director of the Herzog Hospital in Jerusalem, appeared on Channel 13 News, reporting that 95% of severely ill COVID-19 patients are fully vaccinated, and that they make up 85% to 90% of COVID related hospitalizations overall.25
In Scotland, official data on hospitalizations and deaths show 87% of those who have died from COVID-19 in the third wave that began in early July were vaccinated,26 and in Gibraltar, which has a 99% COVID jab compliance rate, COVID cases have risen by 2,500% since June 1, 2021.27
A CDC investigation of an outbreak in Barnstable County, Massachusetts between July 6 through July 25, 2021, found 74% of those who received a diagnosis of COVID19, and 80% of hospitalizations, were among the fully vaccinated.28,29 Most, but not all, had the Delta variant.
“What the breakthrough cases appear to show is that the delta variant of the coronavirus is more easily carried and transmitted by vaccinated people than its predecessors,” the Chronicle editorial board writes.30
“In any case, the greater apparent transmissibility of the variant makes it that much more important to protect as many people as possible from severe COVID by increasing inoculation rates.”
What the board appears to be saying is that unvaccinated people must be protected against severe infection, against their will, if need be, and the best way to do that is to discriminate against them and treat them like second-class citizens.
Again, a simple way to check the reasonableness of this argument is to swap out the COVID reference for something else. How about, “It’s important to protect as many people as possible from dying in car accidents by raising car prices so fewer people can get behind the wheel.”
Can ‘Big Brother’ Save You From a Virus?
As early as April 2020, The Times in the U.K. weighed in with similar suggestions, stating “We need Big Brother to beat this virus.”31 Clare Foges, the author of the piece in question, went on to say, “Don’t let the civil liberties lobby blind us to the fact that greater state surveillance, including ID cards, is required.”
The argument that Big Brother can protect us from infection is ludicrous on its face, because no amount of people surveillance can prevent microscopic viruses from circulating.
The No. 1 place of viral spread is in institutions, such as nursing homes and hospitals, yet the staff within them are among the most well-trained in pathogenic control. If trained hospital staff can’t prevent the spread of viruses, how can government officials do it?
Importantly, the argument that we need vaccine passports to prove we’re “clean” enough to participate in society immediately falls apart when you take into account the fact that the COVID shots do not provide immunity. You can still be infected, carry the virus and spread it to others.
We’ve already seen several examples of situations where 100% of people were fully “vaccinated” against COVID-19 yet an outbreak occurred. We’ve even seen over 100 fully COVID injected people die from COVID in one state alone, Massachusetts,32 so it is likely there are now many thousands of fully “vaccinated” who have died from COVID.
Even a 100% Vaccination Rate Cannot Eliminate COVID
Most recently, Carnival cruise lines experienced an outbreak despite every last person on that ship having proof of COVID “vaccination.”33 The cruise liner had even intentionally reduced capacity from 4,000 to 2,800 to provide ample social distancing capability. None of the measures worked. People got sick anyway, which makes perfect sense if you remember that the shot doesn’t provide immunity, only symptom reduction.
Cases such as these clearly reveal that even if everyone gets the shot, SARS-CoV-2 will mutate and continue to circulate, taking people out here and there. To think that giving up basic rights and freedoms is the answer simply isn’t logical. Taking responsibility for your own health is, and that includes deciding if and how you want to protect yourself from SARS-CoV-2.
Nebulized hydrogen peroxide can also be used for prevention and treatment of COVID-19, as detailed in Dr. David Brownstein’s case paper34 and Dr. Thomas Levy’s free e-book, “Rapid Virus Recovery.” And if there’s effective treatment, there’s little need to risk permanent side effects from an experimental gene technology that can only provide a narrow range of protection in the first place.
According to the most recent stats released by the CDC this past Saturday, August 14, 2021, their Vaccine Adverse Event Reporting System (VAERS) now has recorded more than twice as many deaths following the non-FDA approved experimental COVID-19 shots during the past 8 and a half months, than deaths recorded following ALL FDA approved vaccines for the past 30 years.
This has to be the most censored information in the U.S. right now, even though these statistics come directly from the CDC.
They have now recorded 12,791 deaths, 16,044 permanent disabilities, 70,667 emergency room visits, 51,242 hospitalizations, 13,139 life threatening events, among 682,873 reported injuries from 571,831 cases.
The CDC’s official response to these statistics is that they are basically coincidences, and are not related to the experimental COVID-19 shots.
Reports of adverse events to VAERS following vaccination, including deaths, do not necessarily mean that a vaccine caused a health problem. A review of available clinical information, including death certificates, autopsy, and medical records, has not established a causal link to COVID-19 vaccines. (Source.)
Trusting in the CDC for COVID-19 safety information is quite obviously deadly. Because it is widely known that these statistics that they admit to are but a fraction of actual cases, as very few medical professionals are willing to classify an injury or death as caused by COVID-19 injections.
By way of contrast, deaths following all FDA-approved vaccines for the 30 years prior to the emergency use authorizations of the COVID-19 shots total 6,068 over 30 years according to the CDC.
What are NOT included in these 12,791 deaths the CDC is reporting following COVID-19 shots, are the number of fetal deaths following COVID-19 injections into pregnant women, which now numbers 1,360 deaths according to the CDC.
The Big Pharma cartel is now fully in control of just about every aspect of our lives. They own the corporate media which is not reporting any of these statistics from VAERS, and they control the health agencies like the NIH, the CDC, and the FDA.
Anthony Fauci did the Sunday talk show tour yesterday, and stated that Americans need to surrender their liberties (yes, he actually said that) because we are all fighting a common enemy, “the virus.”
In addition, the Department of Homeland Security has now issued a bulletin declaring that anyone who questions COVID-19 measures like masks and “vaccines” are potential “domestic terrorists.”
They are using a bogus COVID-19 “outbreak” called the “Delta variant,” and the CDC has already been caught lying about who are actually being hospitalized right now, falsely stating that the “unvaccinated” are filling up hospitals, when almost the exact opposite is happening around the world.
The latest IPCC report on climate change was released last week, and has signalled a sea-change in the ongoing “big issue”. The Pandemic was fun while it lasted, but it’s time it faded back and we got on with the next stage.
That’s not just my interpretation either, they are quite literally saying it themselves.
Usually, when there’s a big narrative shift looming, you can find one key article that tells you everything you need to know about the plan. For the IPCC report, it’s this iNews article by Andrew Marr. Where he literally uses the phrase “hinge to climate from Covid” several times:
“There is a great turn coming, a change in the terms of political debate, a period of hinge. We are swinging from the many months of coronavirus obsession into an autumn which will be dominated, rightly, by the climate emergency. But much of what we have learned from Covid-19 – about the state, authority, journalism and civil society – is directly applicable to what’s coming next.”
The media have, naturally, been full of headlines on the IPCC report, with varying degrees of alarmism and insanity.
But none of them outline just what the next few months have in store for us better than Marr. The goblinoid face of the establishment, who nauseatingly cheered on Blair in Iraq, can always be relied upon to keep on message. He’s always right there saying the right thing at the right time. And this piece is no exception.
He headlines “Treat people like grown-ups and they will fight climate change like Covid-19”, adding [our emphasis]:
“Education works. We are following the science and as we continue to do so, we will successfully tackle climate-change issues in the same way we faced down the coronavirus.”
He never outright states what this “same way” is, exactly, but it’s not really hard to imagine what he means. His article isn’t about the future, anyway, it’s all about the past.
It’s tracking the tools deployed during the “pandemic”, and how effective they were. A performance review for the politicians and “journalists” who have successfully parlayed a “virus” that poses almost zero danger to the general public into a full-fledged remodelling of society.
He points out how politicians under-estimated how willingly people would leverage their freedoms:
“To begin with [Western leaders] worried that voters would not accept restrictions on their liberties for the greater good. By and large, they were wrong. […] This shaped how Germans, Americans, the French and British – and many more – responded, and allowed societies to change direction faster than anyone would have predicted.”
How easily the media were able to spread misinformation that controlled public opinion:
“The media, so often blamed for almost everything, found new ways to explain complex scientific arguments in ways that most people understood.”
And how these lessons can be applied to messaging on climate change going forward:
“This is a core lesson that needs to be learned, as we hinge from Covid to climate. Public understanding of science has become a security issue. Without it, there will be no public support for the hard decisions on transport, heating and land use.”
The whole thing reads that way, like a cross between a press release and a progress report. Appearing a blithe opinion piece to the uninitiated, but having a clear second layer of meaning to those who know how to read it.
There are throwaway lines propping up globalism (“how little nature notices national borders”), and brief praise for China’s authoritarian government vs the West’s “slapdash” approach and “tardy lockdowns”, but those are B plots.
The story here is “hey guys, this all worked much better than we thought it would, we could do the same thing for climate change”.
DOES THIS MEAN THAT THE PANDEMIC IS OVER?
Not “over”, but certainly on the decline. It’s obvious that the press are prepping the groundwork to leave Covid behind, and turn their focus to the next stage of the Great Reset.
But, all that said, it will be a difficult sell. Harder than Covid, in some ways, because people are so much more used to climate alarm calls. For want of a better word, they have become somewhat immune to it.
What’s more, the establishment clearly knows this, because they’re keeping the pandemic warm on the backburner. Ready to bring it back to the boil should the need arise.
The pandemic is becoming a new forever war, akin to the war on terror. We won’t ever win it, but it will disappear from headlines until they need to shock or distract people.
Marr, for example, doesn’t declare the pandemic over, instead he says:
“The pandemic is not, of course, yet over. It will end raggedly and slowly; and politicians who proclaim victory will quickly sound foolish[…]it will probably feel as if we have beaten this thing.”
Before adding the ubiquitous riders that will keep the “threat” of the Covid alive in the public imagination:
“The Delta variant may be the most contagious virus ever [and] can reinfect the double-vaccinated […] Britain is going to face a period of “bumpiness” in transmission rates and uncertainty about the near future […] the winter may be tough […] Booster jabs will become routine.”
There’s clearly a plan in place. He practically spells it out, claiming Covid19 will be pushed off the front pages…
“Though not every day… this will be bumpy. There will be sudden scares about the emergence of a possible new variant somewhere unexpected; and urgent questions about biosecurity at Heathrow. There will be stories about outbreaks in care homes, or a sudden spike in infections in particular age or ethnic groups.”
Do you see what he’s saying yet?
The pandemic isn’t over, it will just “feel” like it is, while they fill the front pages with big red numbers about climate change.
If people don’t respond to those big red numbers the way they should… well, there just might be another variant. Maybe a racist one.
The pandemic has served its purpose, but they won’t end it yet. Not until they’re sure everyone is good and scared of something else.
SO WHAT COMES NEXT?
It’s not hard to see exactly where this all leads. Mostly because they’re telling us.
“nothing short of transforming society will avert catastrophe”
This isn’t new. This has been bubbling along in the background for months (I have already written two articles about it), but the message is being refined into a simple three-step process:
Point out all the ways Covid and climate change are similar.
“The interesting thing is that so much of the world’s experience during the pandemic relates quite closely to the climate crisis – our human interrelatedness, the importance of effective governance, the centrality of science and its communication.”
Followed by the “covid is worse” [my emphasis]:
“Of course, the two challenges are different. So far, a little over 4.3 million people have died from Covid. Australian and Chinese academics estimate that around five million people are dying each year from the effects of climate change […] Suffice it to say that even if the Delta variant is the most infectious disease mankind has so far faced, the climate emergency is at another level – a reshaper of geography, highly unpredictable and, in short, existential for the planet and its inhabitants.”
Patrick Vallance does the same in his article in the Guardian, and then again in The Times. There are several others along the same lines, such as this one from the Hill, or this one from the International Monetary Fund.
So, the way they’re going to talk about (or should we say say “market”?) climate change action is fairly clear. But what are these hypothetical actions going to be?
Are we seeing any hints as to what this “transformation of society” might entail? Or what these “tough decisions” could be?
Well, there were whispers of climate lockdowns, but they have died away since the outraged reaction. There’s always talk of other schemes, like limiting flights, outlawing beef and “personal carbon allowances”, but these are hardly new.
Andrew Marr’s article contains a couple of hints. But the only specific policy he mentions is forcing households to replace their boilers (“at a high cost to millions of families”), and this somewhat creepy allusion to the importance of the Deep State:
“A final lesson is that Westminster and the state are two very different things. The state includes the NHS, national science labs, networks of experts […] I now feel we should spend less time on the distracting national puppet show and more time thinking about what I might delicately call the deeper sources of authority.”
Mostly, though, the mainstream voices are being very quiet on specifics. I suspect partly to stop the spread of what Marr calls “an outbreak of conspiracy theories in new media”, but mostly because they’re not sure exactly what they want to do yet, and they don’t believe the majority mentally prepared enough.
The COP26 Climate Summit in Glasgow, this November, will be something to keep an eye on. Expect a lot of scary stories in the weeks leading up to it, and then a lot of “policy recommendations” in its wake.
We’re pivoting to climate change guys. Great Reset Phase II is upon us.
According to the Centers for Disease Control and Prevention, the White House and most mainstream media, what we have now is a “pandemic of the unvaccinated.”1
According to the official narrative, 99% of COVID-19 deaths and 95% of COVID-related hospitalizations are occurring among the unvaccinated. In a July 16, 2021, White House press briefing,2 CDC director Dr. Rochelle Walensky claimed “over 97% of people who are entering the hospital right now are unvaccinated.”
But as reported by Fox News anchor Laura Ingraham on “The Ingraham Angle,” “that statistic is grossly misleading,”3 and in an August 5, 2021, video statement, Walensky inadvertently revealed how that 95% to 99% statistic was created.
Grossly Misleading Data Manipulation
As it turns out, to achieve those statistics, the CDC included hospitalization and mortality data from January through June 2021. It does not include more recent data or data related to the Delta variant, which is now the most prevalent strain in circulation. The problem is, the vast majority of the United States population was unvaccinated during that timeframe.
January 1, 2021, only 0.5% of the U.S. population had received a COVID shot. By mid-April, an estimated 31% had received one or more shots,4 and as of June 15, 48.7% were fully “vaccinated.”5 Keep in mind that you’re not “fully vaccinated” until two weeks after your second dose (in the case of Pfizer or Moderna), which is given six weeks after your first shot. This is according to the CDC.6
So, those receiving an initial dose in June, for example, won’t be “fully vaccinated” until eight weeks later, sometime in July or August.
By using statistics from a time period when the U.S. as a whole was largely unvaccinated, the CDC is now claiming we’re in a “pandemic of the unvaccinated,” in an effort to demonize those who still have not agreed to receive this experimental gene modification injection.
Selective Pressure Promotes Emergence of New Variants
Here’s what Canadian viral immunologist and vaccine researcher Dr. Byram Bridle told Ingraham about the claim that we’re in a pandemic of the unvaxxed, and that the unvaccinated are hotbeds for dangerous variants:
“Absolutely, it’s untrue to be calling this a pandemic of the unvaccinated. And it’s certainly untrue … that the unvaccinated are somehow driving the emergence of the novel variants. This goes against every scientific principle that we understand.
The reality is, the nature of the vaccines we are using right now, and the way we’re rolling them out, are going to be applying selective pressure to this virus to promote the emergence of new variants. Again, this is based on sound principles.
We have to look no further than … the emergence of antibiotic resistance … The principle is this: If you have a biological entity that is prone to mutation — and the SARS-CoV-2, like all coronaviruses is prone to mutation — and you apply a narrowly focused selective pressure that is nonlethal, and you do this over a long period of time, this is the recipe for driving the emergence of novel variants.
This is exactly what we’re doing. Our vaccines are focused on a single protein of the virus, so the virus only has to alter one protein, and the vaccines don’t come close to providing sterilizing immunity.
People who are vaccinated still get infected, it only seems particularly good at blunting the disease, and what that tells you therefore is that these vaccines in the vast majority of people are applying a nonlethal pressure, narrowly focused on one protein, and the vaccine rollout is occurring over a long period of time. That’s the recipe for driving variants.”
Natural Immunity Offers Far Superior Protection
Bridle also explains why natural immunity offers robust protection against all variants, whereas vaccine-induced immunity can’t. When you acquire the infection naturally, your body develops antibodies against ALL of the viral proteins whereas the COVID shots only trigger antibodies against one, namely the spike protein.
As mentioned above, when you have antibodies against just one of the viral proteins, the virus only needs to mutate that one protein in order to evade your immune system. When you have natural immunity, on the other hand, your antibodies will recognize all parts of the virus, so even if the spike protein is mutated, your body will recognize other parts of the virus and mount an attack against those.
That SARS-CoV-2 works the same way other viruses do was shown in a Nature Reviews Immunology study7 by Alessandro Sette and Shane Crotty, published in October 2020. The study, “Cross-Reactive Memory T Cells and Herd Immunity to SARS-CoV-2” argued that naturally-acquired immunity against SARS-CoV-2 is potent, long-lasting and very broad in scope, as you develop both antibodies and T cells that target multiple components of the virus and not just one.
If we are to depend on vaccine-induced immunity, as public health officials are urging us to do, we’ll end up on a never-ending booster treadmill. Boosters will absolutely be necessary, as the shot offers such narrow protection against a single protein of the virus. Already, data around the world show vaccine-induced protection is waning rapidly in the face of new variants, and Moderna has publicly stated that the need for additional boosters is expected.8
How Dangerous Is the Delta Variant?
According to Dr. Anthony Fauci, the Delta variant is both more transmissible and more dangerous than the original virus and previous variants. July 4, 2021, he told NBC News:9
“It is more effective and efficient in its ability to transmit from person to person. And studies that we’ve seen where they have been the variant that’s dominated in other countries, it’s clear that it appears to be more lethal in the sense of more serious — allow you to get more serious disease leading to hospitalization, and in some cases leading to deaths.”
In a June 29, 2021, interview,10 Fauci called the Delta variant “a game-changer” for unvaccinated people, warning it will devastate the unvaccinated population while vaccinated individuals are protected against it.
Remember, Fauci is not a clinician and has never treated someone infected with SARS-CoV-2. Other health experts and practicing physicians who treat COVID-19 patients disagree with Fauci’s claims, arguing that not only is the Delta variant not more dangerous, it’s certainly not more dangerous for the unvaccinated.
As reported by Ingraham in June 2021 (video above), there’s an evolutionary genetics theory called Muller’s Ratchet, which states that as an outbreak starts to peter out, the virus tends to mutate into a more transmissible form, but at the same time it grows weaker, causing far less serious infection. According to epidemiologist and cardiologist Dr. Peter McCullough, this is exactly what we’re seeing. He told Ingraham:
“The good news is on the 18th of June, the United Kingdom presented their 16th report11 on the mutations — and they’re doing a great job, much better than our CDC — and what they demonstrated is that the Delta is more contagious but it’s far less deadly, far less worrisome. In fact, it’s a much weaker virus than both the U.K. [Alpha] and the South African [Beta] variants.”
Spike Mutations Render Vaccinated Vulnerable to Delta
Importantly, the Delta variant contains three different mutations, all in the spike protein. This, McCullough explains, allows this variant to evade the immune responses in those who have received the COVID jabs — but not those who have natural immunity which, again, is much broader. In a June 30, 2021, appearance on Fox News, McCullough stated:12
“It is very clear from the UK Technical Briefing13 that was published June 18th that the vaccine provides no protection against the Delta variant. It’s a very mild variant.
Whether you get the vaccine or not, patients will get some very mild symptoms like a cold and they can be easily managed … Patients who have severe symptoms or at high risk, we can use simple drug combinations at home and get them through the illness. So, there’s no reason now to push vaccinations.”
Children’s Health Defense chief scientific officer Brian Hooker, Ph.D., has echoed McCullough’s sentiments. The Defender quotes Hooker:14
“What we’re seeing is virus evolution 101. Viruses like to survive, so killing the host (i.e. the human who is infected) defeats the purpose because killing the host kills the virus, too. For this reason, new variants of viruses that circulate widely through the population tend to become more transmissive but less pathogenic. In other words, they will spread more easily from person to person, but they will cause less damage to the host.
The vaccine focuses on the spike protein, whereas natural immunity focuses on the entire virus.
Natural immunity — with a more diverse array of antibodies and T-cell receptors — will provide better protection overall as it has more targets in which to attack the virus, whereas vaccine-derived immunity only focuses on one portion of the virus, in this case, the spike protein. Once that portion of the virus has mutated sufficiently, the vaccine no longer is effective.”
Real-World Data Show Most of Infected are Fully ‘Vaccinated’
Real-world data from areas with high COVID jab rates show the complete converse of what media, the CDC and White House officials are telling us. In addition to the British Technical Briefing No. 16,15 cited above, we have additional data from Israel, Scotland, Massachusetts and Gibraltar:
•August 1, 2021, director of Israel’s Public Health Services, Dr. Sharon Alroy-Preis, announced half of all COVID-19 infections were among the fully vaccinated.16 Signs of more serious disease among fully vaccinated are also emerging, she said, particularly in those over the age of 60.
A few days later, August 5, Dr. Kobi Haviv, director of the Herzog Hospital in Jerusalem, appeared on Channel 13 News, reporting that 95% of severely ill COVID-19 patients are fully vaccinated, and that they make up 85% to 90% of COVID-related hospitalizations overall.17 As of August 2, 2021, 66.9% of Israelis had received at least one dose of Pfizer’s injection, which is used exclusively in Israel; 62.2% had received two doses.18
•In Scotland, official data on hospitalizations and deaths show 87% of those who have died from COVID-19 in the third wave that began in early July were vaccinated.19
•A CDC investigation of an outbreak in Barnstable County, Massachusetts, between July 6 through July 25, 2021, found 74% of those who received a diagnosis of COVID19, and 80% of hospitalizations, were among the fully vaccinated.20,21 Most, but not all, had the Delta variant of the virus.
The CDC also found that fully vaccinated individuals who contract the infection have as high a viral load in their nasal passages as unvaccinated individuals who get infected.22 This means the vaccinated are just as infectious as the unvaccinated.
•In Gibraltar, which has a 99% COVID jab compliance rate, COVID cases have risen by 2,500% since June 1, 2021.23
While those who benefit from keeping the pandemic going would like you to cower in fear at the thought of the Delta variant, there’s really no evidence that it’s any worse than the original. It’s more transmissible, yes, but far less dangerous, as its primary symptoms are that of a regular cold.
According to Harvard and Stanford professors, the actual number of Americans dying from or with COVID-19 are actually at an all-time low, so alarmism is uncalled for.24
And, as for viral social media posts by doctors and nurses claiming hospitals are overflowing with unvaccinated COVID patients, don’t believe them. Most are bots. We’ve repeatedly seen evidence that fearmongering is being spread not by real people but by fake accounts run by artificial intelligence. This includes blue check accounts. Here’s a sampling of recent bot farm tweets trying to scare everyone:25
Don’t Fear It, Just Treat It
In closing, remember there are several different treatment protocols for COVID-19 that appear just as effective for variants as for the original virus, including the following:
Nebulized hydrogen peroxide for prevention and treatment of COVID-19, as detailed in Dr. David Brownstein’s case paper26 and Dr. Thomas Levy’s free e-book, “Rapid Virus Recovery.” Levy believes nebulized hydrogen peroxide can also be an invaluable strategy for combating spike protein toxicity27 because, in addition to being a powerful antiviral, it will also augment and speed up cellular healing, in part by improving oxygenation
More than seven months have passed since an unarmed protester named Ashli Babbitt was shot dead inside the US Capitol while attempting to climb through an opening in a glass door.
Six months after her death, her killer – a police officer who apparently shot her without warning, and certainly without having made any effort to stop her short of putting a fatal bullet through her chest – has never been publicly identified, let alone charged or disciplined.
During those same seven months – during which every self-respecting liberal demanded a criminal penalty for the policeman who killed George Floyd – Ashli Babbitt, the victim of an equally questionable police killing, has been the target of an orgy of media character assassination.
When Donald Trump recently mentioned her death as “a terrible thing” (hardly a radical assessment), New York Magazine’s response seethed with victim-blaming outrage, insisting that the unarmed Babbitt, with no criminal history of any kind:
was leading the mob [inside the Capitol] violently forward toward its goal of threatening or killing officials.”
There’s no evidence that Babbitt intended to kill anyone, let alone that she actually tried to. And there’s plenty of reason to believe that her fatal shooting was illegal. But facts about Ashli Babbitt have never counted for much in liberal media.
For the press, the top priority has been to ensure that in any story told about the 2020 election, Donald Trump and his supporters are the ones who tried to destroy American democracy, while Joe Biden’s Democratic Party heroically came to its rescue.
In this respect, New York’s slander is altogether typical. Refracted through the editors’ invective, in which (among other things) Republican politicians are, weirdly, accused as the real culprits in Babbitt’s death, the underlying message emerges as an ideological tautology: Ashli Babbitt had to die because she joined the wrong sort of protest.
No wonder New York concluded that the hapless 35-year-old was killed “for a very good reason.”
The January 6 demonstration in which she participated has been as relentlessly demonized in the press as Babbitt herself.
According to mainstream media, the men and women who marched to the Capitol to protest the machinations by which Biden ousted Trump from the White House were – take your pick – “fascists” (PBS), “white supremacists” (CNN), “terrorists” (MSNBC), or a violent “mob” bent on paralyzing the United States government (USA Today), while virtually every mainstream media outlet still insists – against all evidence – that, collectively, the demonstrators staged an armed “insurrection” that only just failed to turn the United States into a right-wing dictatorship.
And anyone who imagined that, after seven months of this, the slanders against Ashli Babbitt couldn’t get any more venomous reckoned without the inflammatory effect of mass media Trump-hatred.
When, on July 12, the former President suggested that Babbitt’s killer should at least be publicly identified, the New Republic swung into anti-Republican overdrive, claiming in a hysterical screed that the unarmed Babbitt was a monster who had hoped for “the mass execution of Democratic politicians and prominent liberals” when she went to Washington to be killed on January 6.
Merciful heavens, the woman was so freaking bloodthirsty that she actually used to watch – Tucker Carlson!
Even that wasn’t all. The same rant that accused Ashli Babbitt of harboring dreams of mass murder described the January 6 protest as “a mob of thousands who…rampaged through the halls of Congress,” when in fact only a small fraction of the protesters entered the Capitol at all, and only a handful of those have been accused of possessing “weapons” (most of which seem to have been flagpoles); with a single exception, not one of the charged “insurrectionists” even thought to bring a gun to the coup. (The lone protester facing criminal charges who did carry a pistol into the Capitol never drew it, according to police.)
But hey, fantasy breeds fantasy: for liberals like the TNR editors, where there are Trump supporters, there’s just got to be mayhem.
Lest I be accused of playing an after-the-fact role in the “insurrection” myself, let me emphasize that I do not share Ashli Babbitt’s politics, and that I do not approve of the actions of the protesters who broke into the Capitol on January 6. Nor do I regard the 2020 presidential election as having been “stolen,” at least not in the sense that many of the protesters evidently believed it was – of which more presently.
But whether Ashli Babbitt was right about Donald Trump or about the 2020 election is ultimately beside the point. The plain truth is that as far as anyone can tell she was the victim of an extrajudicial execution – an execution made even more heinous by the fact that Babbitt’s actual offenses inside the Capitol involved no violence and placed no one in jeopardy.
It is an outrage that in the United States of America a police officer can shoot a woman dead for trespassing. And it is doubly an outrage that so few ostensible civil libertarians have been willing to say so.
Scores of liberals, politicians, op-ed writers and public moralists demanded a full-scale investigation into the fatal police shooting of Breonna Taylor. Why couldn’t one of them utter a single word of protest about the lethally trampled civil rights of Ashli Babbitt?
The smear campaign against Babbitt is more than the product of a pernicious double standard. It also serves to distract the public from the very real issues that spurred the protest in the first place.
I repeat: I don’t credit stories about the ghost of Hugo Chavez rising from the grave to manipulate secretly-programmed voting machines on Election Day. (In fact, I suspect these “theories” have been amplified in popular media precisely because they’re relatively easy to refute.)
But the January 6 protesters did have excellent reasons to be angry about the electoral process that put an end to Trump’s term of office. And since the popular press refuses to discuss the protesters’ legitimate grievances, allow me to enumerate three of the most important ones.
1. The balloting procedures used in key jurisdictions were probably illegal.
In several closely contested states – Georgia, Illinois, Michigan and Pennsylvania among them – state executives made unilateral changes in the election laws in order to facilitate voting by mail rather than at polling booths, citing the “killer virus” as a pretext. Yet in every such case, the applicable state constitution assigns questions of public policy – including the extent to which people can vote by mail – to the state’s legislators rather than the executive branch; these matters cannot legally be determined by gubernatorial fiat except in strictly defined “emergencies.”
Nor can it be claimed that COVID19 posed such an emergency. Even Atlantic Magazine, one of the most sedulous organs of coronavirus hysteria, conceded barely a month before the presidential election that “voting with a mask on is no more dangerous than going to a grocery store with a mask on – something millions of Americans do every week.”
That means that the balloting procedures used in several important states were fundamentally flawed – not only violating the relevant state constitutions but probably transgressing the “due process of law” requirement of the Fourteenth Amendment to the US Constitution itself. And while there’s no way to know whether these wrongly altered procedures actually changed the outcome of the election, Trump voters had every right to condemn them.
2. The election was effectively decided by mass media misinformation.
It is ironic that so much recent propaganda accuses Trump and his supporters of circulating “misinformation.” In fact, one of the most consequential misinformation campaigns of modern times was largely responsible for Trump’s defeat.
Post-election observers are in general agreement that Joe Biden – that mumbling mummy – would have stood little chance of besting Trump had it not been for the popular press’ relentless stoking of coronavirus hysteria.
Of particular impact was the claim – repeated in various forms in more venues than I can count – that Trump was “personally responsible for tens of thousands of deaths,” as one typical hit piece insisted in the run-up to the election.
But was he? For all the huffing and puffing, no one has presented any real evidence to support the accusation. Yes, the man in the bad wig behaved as anyone familiar with his record might have expected: he made some foolish remarks, picked needless feuds with Democratic governors, hogged the spotlight, reversed himself without acknowledgment, and took credit for things that would have happened just as well without him.
But the fact remains that presidential action had little effect on the virus or its consequences; nearly all the important decisions – including the disastrous lockdowns and small business closures, not to mention the suspension of representative democracy and the attacks on education, public worship and the arts – were made at the state level.
In all of this, the White House was largely irrelevant. Trump’s most culpable act – in my opinion – was backing the Food and Drug Administration as it cut the corners of the testing procedures that should have been required for the COVID19 “vaccines” and granted the manufacturers blanket legal immunity for any adverse medical consequences.
But on that point, remember, Trump was supported by the “experts” and even by his political opponents. Legitimate criticism never figured in the media blitz against the former President. Instead, he was blindsided over claims so vague they couldn’t even be specified, with dire-sounding but meaningless words like “downplaying” or “mishandling” repeated so often that eventually they seemed to prove themselves. It was an impressive display of emotion-churning propaganda. It contained little or no truth.
Did the avalanche of misinformation violate any election laws? Alas, no. But that fact certainly did not deprive angry voters of their right to protest.
3. Biden’s election guaranteed the worsening of the coronavirus coup.
The protesters’ conviction that Trump actually won the election probably won’t stand the test of time. But in one important sense, they did know perfectly well what they were fighting for – and so did we.
Joe Biden has never made a secret of his fondness for attacks on freedom in the name of “health” regulation. Less than two months into his term, Biden was openly mulling an executive fiat that would require the muzzling and six-foot separation of all American workers, even those who have submitted to the “vaccines.”
He has also suggested that anyone who declines to be a guinea pig for Big Pharma is unpatriotic, and has announced a plan to have “local health leaders” hawk the scantily-tested drugs from door to door to add even more pressure to the vaccination campaign – even as the unprecedented “gene therapy” has already figured in more than 5,300 deaths nationwide.
And this is clearly just the beginning.
Each passing week sees the lockdown-lovers flaunting still more contempt for the Bill of Rights. Mandatory muzzling has been reintroduced in Los Angeles County. Geraldo Rivera, a media stalking horse for the administration, has endorsed Jim Crow restrictions for the “unvaccinated” that would bar them from grocery stores and nearly all public places.
The US Surgeon General is publicly calling for still more censorship on social media (where dozens of accounts have already been canceled for disseminating information the authorities don’t like).
The nastiest aspect of all these police-state tactics is the growing intensity of the hate speech aimed at dissenters. “Look, the only pandemic we have is among the unvaccinated,” Biden insisted (falsely) on July 16.
Rochelle Walensky, head of the Centers for Disease Control and Prevention, took the incitement a step farther, blaming even infections among vaccinated Americans on “outbreaks of cases in parts of the country that have low vaccination coverage.” In other words: if you get sick, you can thank those dastardly freethinkers who still imagine they’re entitled to civil rights.
It’s a dangerous and divisive strategy. And anyone unsure where it leads need only look to Italy, France and Greece, where officials are already forcing health care workers to submit to vaccinations on pain of losing their livelihoods.
French President Emmanuel Macron, not even bothering to seek parliamentary approval, is mandating “vaccine passports” for anyone who wants to eat at a restaurant or to travel by train.
And these strong-arm tactics are doubtless intended to prepare us for worse still to come. Anthony Fauci himself has declared that COVID19 vaccination should be compulsory in as many places as possible – even though federal law holds otherwise, since the drugs have only been granted “emergency use” authorization – because he thinks it “horrifying” that people should decide the fate of their own bodies. (The good doctor sings a different tune on the question of legalized abortion, but since when have our ruling mandarins been consistent?)
In short, to say that a lot was at stake in the 2020 presidential election would be putting it very mildly. Liberal pundits have expressed shock at the willingness of thousands of people to converge on Washington to denounce the election results that effectively intensified the coronavirus coup. I think it would have been shocking had they not done so.
It’s not just that our government – and its tame mouthpieces in the press – is using the pretext of “health regulation” to demonize those citizens who choose to exercise their right not to be injected with an untested drug. The entire vaccine-blackmail program is premised on a lie.
The campaign necessarily assumes that the COVID19 “vaccines” prevent transmission of the virus from one person to another. They do no such thing.
The manufacturers have acknowledged, and the FDA has explicitly confirmed, the absence of any evidence that the new “vaccines” prevent either infection or transmission of SARS-CoV-2. The argument that vaccination is necessary to “protect the public” against COVID19 is simply fraudulent.
Not only does the fear-mongering about “the unvaccinated” falsely assume that the “vaccines” prevent transmission, it completely ignores the presence of genuine immunity among those who have already been exposed. As with any respiratory virus, exposure to SARS-CoV-2 triggers the development of antibodies and T-cells that serve to prevent future infections and, therefore, to block the virus’ transmissibility.
In October 2020, the prominent Oxford University epidemiologist Sunetra Gupta estimated that “three months, maybe six is sufficient time for enough immunity to accumulate…that the vulnerable could resume normal lives” in the United States. More than nine months have now passed since Gupta’s assessment.
Even if her estimate turns out to have been overly optimistic, there can be no doubt that enough natural immunity exists in the general population to have a profound effect on the transmissibility of COVID19, with or without the experimental drugs the government wants us to use. Any “analysis” that omits that obvious fact is patently dishonest.
And suppose, for argument’s sake, that one overlooks all this and accepts the “case” numbers peddled by the CDC. Even so, the statistical basis for all the shrieking about “a pandemic of the unvaccinated” is riddled with too many inconsistencies to be taken seriously.
The southern states of Mississippi and Arkansas, for instance, are both at the low end of the vaccination-level range, at 33.6% and 35.2% respectively.
If the Biden-Walensky propaganda were correct, those states would be inundated in comparable outbreaks of new COVID19 infections.
In fact, after adjusting for the small difference in population size, Arkansas’ most recent 7-day average for “new cases” is nearly 2.5 times higher than Mississippi’s. Such a disparity in the official numbers clearly cannot be explained on the basis of COVID19 vaccination rates.
And things are no different at the high end of the vaccination spectrum. Maryland has “fully vaccinated” 57.6% of its population, while New York lags just slightly behind at 55.8%. Yet, after adjustment for the different population sizes of the two states, New York still has nearly 2.5 times the 7-day average number of new “cases” of COVID19 that Maryland has – as big a gap as that between Mississippi and Arkansas.
Or consider the wildly different “case” levels to be found in California, which has a “fully vaccinated” rate of 51.5%, and in Pennsylvania, where the rate is 51.1%. Again, after adjusting for population, California’s latest “new case” average is well over double that of Pennsylvania’s – even though the vaccination level in the two states is virtually identical. Anomalies like these make nonsense of any argument that the US is experiencing a “pandemic of the unvaccinated.”
And what about the “vaccinated”? Here, too, the propaganda doesn’t withstand even cursory scrutiny. Recently, six “fully vaccinated” people at a single wedding – held in a “large, open-air tent” – all came down with COVID19. Of those six, two were hospitalized and one died.
In a rather desperate brush-off typical of mainstream media, Insider’s Hilary Brueck described this as a “small outbreak that underscores how effective vaccines are against even variants of the virus.”
Ah, how nimbly propagandists put about in a changing wind! A year ago, six symptomatic cases of COVID19 would have marked the ceremony where they originated as a dreaded “superspreader event” – it would have been touted as proof that anyone selfish enough to invite guests to a wedding ought to be treated as a public menace.
And if, on top of that, fully a third of those infected had been hospitalized, and over 16% of them had dropped dead – well, I will leave it to the reader to imagine the hysterical headlines that would have erupted about that. Are we really supposed to chant hosannas now that the identical evils are showing up in the wake of COVID19 “vaccinations”?
But let us return to January 6 and the conspiracy of silence surrounding the killing of Ashli Babbitt.
Apart from her violent death – the only one that occurred in the Capitol on January 6 – the incidents of that day were strikingly incommensurate with the media’s horrified depictions of the “storming” of Congress.
Yes, there were scuffles with police, but such things were hardly unprecedented in Washington. And the media’s obsessive use of the phrase “deadly riot” misrepresents the unfortunate but nonviolent deaths (other than Babbitt’s) that occurred during or immediately after the protest.
Brian Sicknick, the Capitol Police officer who died the following day, and whose death – as we were assured by the New York Times on the basis of “anonymous” reports – resulted from being clubbed over the head with a fire extinguisher by one of the “insurrectionists,” actually died of natural causes (as did two of the older protesters).
The only other supposedly “violent” death, that of protester Rosanne Boyland, was determined by the D.C. medical examiner’s office last April to be the consequence of “acute amphetamine intoxication,” though that didn’t prevent the Times from offering its readers back in January a gorily detailed – and false – account of how Boyland was “trampled” and “crushed” to death by “the mob.”
(By the way, I am not aware that the ostensibly meticulous fact-checkers at the Times have ever printed a directretraction of either of these two bogus articles. Innocent errors do sometimes merit a correction at the Paper of Record; malicious errors almost never do.)
The threat allegedly posed by the demonstrators to members of Congress seems also to have been greatly exaggerated. Despite the media’s early insistence that the “insurrection” was led by sinister “right-wing extremists,”only a handful of those who breached the Capitol had any ties to the Proud Boys, Oath Keepers, Three Percenters or Aryan Nations.
“More than four-fifths” of those charged for their actions on January 6 “come from various backgrounds, from business owners to white-collar professionals,” the BBC reported in February. The claim that the “rioters” brought zip-tie handcuffs to use on Democratic politicians turned out to be another falsification: the one protester photographed holding the “restraints” actually found them on a table inside the Capitol. The police had brought them there.
And frankly, I find it a little hard to believe the stories of lawmakers who say they feared for their lives during the “siege” when one of them, a Democrat from the Virgin Islands, could generate straight-faced media reports by claiming that she preferred a “possible confrontation with the insurrectionist mob” to sharing a “secure location” with some Republicans who were – gasp – not wearing masks!
True, her insistence that masks on the Republicans would have protected her, while her own would not, is part of the magical thinking we’ve all been asked to swallow throughout the propaganda campaign.
But would anyone who genuinely thought she was running from a lynch mob refuse a safe haven just because “I wouldn’t be able to see the virus as it was coming toward me” from a few un-muzzled legislators across the room? What was evidently meant to sound like a horror story reads, to me, much more like farce.
So it turns out that anyone genuinely concerned about “deadly violence” during the January 6 protest can have only one real subject to investigate: Ashli Babbitt. And the more one investigates her death, and the circumstances surrounding it, the less justifiable the whole scenario appears.
Just how, for instance, did protesters manage to enter the Capitol in the first place?
No one in power has offered any convincing answer to that question.
Federal government buildings in Washington are normally among the most zealously guarded in the world. And everyone knew that a large political protest was planned for January 6, the day Joe Biden’s election as President was to be officially certified.
Why couldn’t Capitol police use tear gas to stop the unarmed demonstrators as soon as they breached the entrances, especially since “tear gas munitions were used by other federal police agencies against protesters in front of Lafayette Park” just a few months earlier? And assuming the local police force was somehow unable to handle the crowd, where was the vaunted National Guard?
Some of the protesters believe that they were deliberately entrapped. As one of them later told the FBI, “law enforcement purposefully did not have enough resources there so that supporters of the former president could overrun the Capitol and be subsequently labeled as ‘intruders.’” I cannot prove this theory correct – but I also cannot dismiss it as implausible.
As early as February 4, Time Magazine’s Molly Ball reported that a “conspiracy” involving “an informal alliance between left-wing activists and business titans” had orchestrated a “vast, cross-partisan campaign” to ensure Biden’s smooth entry into office.
This “conspiracy” was so effective that it “got states to change voting systems” and, on the day of the January 6 protest itself, saw to it that the protesters who converged on the Capitol “were met by virtually no counterdemonstrators” who might otherwise “be blamed for any mayhem.”
Surely a cabal capable of that much could also arrange for the protest to get just far enough out of hand to guarantee media images that would discredit Donald Trump with the nation’s political elites – which, of course, is exactly what happened. Or was it all just coincidence?
Along similar lines, the strange absence of the National Guard on January 6 has been widely reported – but only as an inexplicable blunder.
Yet couldn’t this, like the parallel absence of counter-demonstrations, have been deliberate?
We know that the deployment of National Guard or military personnel to the Capitol would have required the consent of the Joint Chiefs of Staff. And we know that the Chairman of the Joint Chiefs was General Mark Milley, a man who (according to a soon-to-be-published book) told his aides that Trump reminded him of Hitler, and whose determination to ensure that Biden was installed as President – “come hell or high water” – went so far that he “informally planned for different ways to stop Trump” after the election, including private telephone conversations with (Democratic) House Speaker Nancy Pelosi.
In fact, credible reports maintain (though he denies it) that General Walter Piatt, director of Army staff, specifically refused to send National Guard troops to the Capitol on January 6 because “it wouldn’t look good.”
An honest press – if we had one – would be taking a hard look into the possibility that the “deadly riot” was really political theater, organized not by the protesters but by the very democracy-haters the protesters came to challenge. That would make Babbitt’s killing an even uglier miscarriage of justice.
Meanwhile, the refusal of the media, the pundits, the civil rights organizations, the politicians – just about everyone in power – to give Ashli Babbitt’s death the attention it deserves is more than a wrong in itself. It is part of a larger pattern of political gaslighting by which the victors in the 2020 election, while accusing Trump & Co. of an attempted “coup,” continue to advance a coup of their own.
Today the coup marches under the name “Delta variant.” But this is only a temporary phase. Specific terrors will vary from month to month, but there will always be some reason for whittling down our remaining freedoms. This latest scare is entirely typical.
Notwithstanding the ballyhoo, there’s no real evidence that the “Delta variant” is particularly dangerous – not even the CDC has attempted to make that case – and as a general rule, subsequent variants of a respiratory virus are less severe than those they follow.
(As a matter of fact, there’s only sketchy evidence that the new “variant” is even more transmissible than the original version, despite popular media’s insistence on this as a matter of fact: the CDC cites only one study about the alleged contagiousness of the “Delta variant,” which is based entirely on manifestly unreliable public “test” data. It’s also rife with anomalies, such as the finding that the variant spreads more rapidly among Asians than among white people, while among blacks it actually appears to be less transmissible. Go figure.)
In other words, like nearly everything the “experts” have claimed about COVID19 for the last seventeen months, the “deadly Delta” story is much less about facts than it is about maintaining public hysteria.
And the motive for the fear porn is perfectly clear. The Biden administration never intended to give the public anything more than a brief honeymoon from coronavirus terror.
True, there had to be some kind of reward for voting Donald Trump out of office. But now it’s time to get back to business – “business” being the deepening confinement of the American public.
“The carefree Covid season is over,” barked CNN on July 17. And the network was quick to identify the next targets of the crackdown: conservative media, for encouraging “vaccine hesitancy,” and “Republican-led states” that “have tried to outdo each other in limiting the power of cities and counties to impose Covid restrictions in case of a new outbreak.”
It’s a short step from condemning defenders of basic liberties to uprooting the liberties themselves. So if you thought this was all about roasting a TV commentator like Tucker Carlson or a politician like Ron DeSantis, think again: you ain’t seen nothing yet.
Can we still pry our country loose from the grip of the fear campaign? I hope so, believing as I do in the aspirations to which our political system is dedicated, and still more in the value of the human lives that have grown up under the influence of those ideals.
But if we want each life to matter, we have to prove that Ashli Babbitt’s life mattered too. We need to demand more from the federal Justice Department than the cynical conclusion that there was:
no evidence to establish that, at the time the officer fired a single shot at Ms. Babbitt, the officer did not reasonably believe that it was necessary to do so in self-defence or in defense of the Members of Congress and others evacuating the House Chamber.”
We need to seek an explanation for the fact that “the officer,” unlike Derek Chauvin – currently behind bars for killing George Floyd – has never faced charges of any kind for gunning down an unarmed woman under circumstances that placed no one in serious danger.
We must ask why there are no crowds in the streets to support the Babbitt family’s lawsuit against the Capitol police, as there would be if she had been killed by a cop during a Black Lives Matter rally.
It must be clear by now that the coronavirus coup isn’t going away of its own accord. If we don’t demand an end to it, there will be no end.
There will only be more fear porn, more manipulated elections, more wrecked livelihoods, more attacks on freedom – and more tragedies like the killing of Ashli Babbitt, who believed that by taking her protest to the seat of government she could make a difference.
Whether she was right about that is no longer up to her. It’s up to us.
Michael Lesher is an author, poet and lawyer whose legal work is mostly dedicated to issues connected with domestic abuse and child sexual abuse. His latest nonfiction book is Sexual Abuse, Shonda and Concealment in Orthodox Jewish Communities (McFarland & Co., 2014)
The country of Belarus, which imposed no legal lockdown at all throughout the entire pandemic, has released COVID mortality figures which are broadly in line with other nearby countries which imposed draconian lockdowns.
After authorities in Belarus refused to put their citizens under lockdown, the global media had a collective hissy fit, with one headline declaring, “One leader looks hell-bent on turning COVID-19 into a catastrophe for his country.”
However, while managing to avoid all the negative impacts of lockdown, the outcome of Belarus’ no lockdown policy is far from a “catastrophe.”
Newly released overall death statistics from the start of the pandemic up to March 2021 show that the death rate is similar to neighboring countries such as Latvia, Russia and Ukraine which imposed full lockdowns.
Indeed, when compared to Poland, which imposed a particularly harsh lockdown, Belarus’ mortality rate in March 2021 was significantly lower.
Belarus is similar to Sweden, which has suffered fewer than 15,000 COVID deaths despite refusing to impose a lockdown. Figures show that cases and deaths tend to fall in waves whether a lockdown is imposed or not, proving that lockdowns are totally pointless.
The strict lockdown in the UK🇬🇧 was so effective that it stopped the spread of Covid in Sweden🇸🇪 as well 💪 pic.twitter.com/M12KVBibw5
“Alongside places like South Dakota, Florida, Sweden and Tanzania, Belarus is an important illustration of what can be expected from COVID-19 when restrictions aren’t imposed. Like those places, we see that the outcome is basically the same as similar places where restrictions are imposed,” writes Will Jones.
“It simply isn’t the case that a whole country becomes infected if the virus is given largely free reign, as Belarus, like other no-restriction jurisdictions, shows. Even without lockdowns and vaccines the epidemic is self-limiting and comes to an end at around the same point having infected a similar number of people. Until our leaders and their advisers grasp this crucial fact about COVID-19, they will keep pursuing pointless and ineffective but deeply harmful policies.”
Don’t expect any of this to be highlighted by the mainstream media, which has parroted the provable falsehood that repeated lockdowns were to thank for ending each “wave” of COVID.
IN his post forTCW Defending Freedom yesterday, Neville Hodgkinson drew our attention to possibly the most courageous and clear thinking of the doctors to take on the official Covid narrative. Painstaking and meticulous, Peter McCullough has the clarity and capacity to get the simple heart of the matter.
For those doubling down in the establishment and officialdom who find themselves beset with ever more uncomfortable evidence to accommodate in their commitment to coercive and mandatory vaccination, his truths must be very disconcerting.
This, I have no doubt, is why the only references to him you’ll find in a Google search attempt to vilify or discredit him.
Apparently it is not sufficient to cancel this persistent thorn in the side. Baylor Scott & White, a medical centre and health company with which Dr McCullough was once affiliated, have taken it upon themselves to sue him, ostensibly for his references to his prior affiliation with BSW. It is hard to see the action as motivated other than by an intent to discredit him.
Two of his horrified colleagues have written a detailed and heartfelt letter in support of him and condemning the action of BSW. You can read it here.
In April and June of 2020 I wrote about something I referred to as LOKIN 20. In a series of articles I was among those in the so called “alternative media” who tried to highlight that lockdowns and other response measures, created by the Coronavirus Act, increased the risks to the most vulnerable.
This was entirely contrary to the rationale we were given for these new laws and subsequent policies. The response was promoted to the public as a “plan” to protect the most vulnerable. It was certainly a plan but increasing, rather than decreasing, the risks appears to have been the objective.
I reported the removal the safeguards put in place following the Shipman Inquiry and Francis Report (Mid Staffs). I pointed to statistical evidence from the Office of National Statistics and the concerns raised, by people like Professor Carl Heneghan and David Spiegelhalter, that a dangerous withdrawal of healthcare was contributing toward unnecessary increased mortality among the most vulnerable.
I am not claiming any great insight or deductive powers. I was just one, among many others, in the inappropriately named alternative media who were reporting the obvious dangers inherent to government policy.
It is important to stress that the increased mortality risk from the policies, rather than COVID 19, was abundantly clear at the time. Many people tried to warn the public but they were widely dismissed and labelled as “COVID deniers.”
A year later a number of mainstream media (MSM) articles have emerged confirming, what appears to have been, a policy that would inevitably maximise the risks to the most vulnerable. As usual, the possibility of deliberate policy intent is never broached in any of these MSM pieces. Their reports uncritically cite statements by politicians and consistently assume that these policies were mistakes and promote the notion that lessons need to be learned.
Speaking in June 2020 about the high risk discharge of 25,000 vulnerable patients into care setting, where they received neither medical care nor adequate social care, the former Health Secretary and chairman of the Health Select Committee, Jeremy Hunt, was unquestioningly reported as saying:
“It seems extraordinary that no one appeared to consider the clinical risk to care homes despite widespread knowledge that the virus could be carried asymptomatically”
Leaving aside the clear scientific proof that there is no such thing as asymptomatic transmission of SARS-CoV-2, the evidence suggests that these were neither mistakes nor failures. Yet all we see from the mainstream media is a free pass for the politicians and a blanket refusal to ever question their deceitful statements.
We face a huge sociopolitical problem. Despite the mountain of historical and contemporaneous evidence that governments can and do intentionally harm us, it seems we are collectively incapable of grasping the reality of democide. We wrongly assume that every policy is intentionally benign.
We must overcome this flawed and naive belief. Until we recognise that there are those within government, and its wider partnership networks, that wish us ill we will remain unable to address the threat they pose to all of us.
The UK government not only created the legislation to enable healthcare providers to increase the risks to the most vulnerable, they fully understood those risks. They had previously identified them in training exercises and had extensively modelled those risks.
Contrary to Hunt’s statement, there were many in the UK government who did “consider the clinical risk to care homes.” When the claimed pandemic arrived, rather than respond to limit and reduce the known dangers, the government, of which Hunt is a leading member, appeared to intentionally exacerbate them.
Section 14 of the Coronavirus Act removed the crucial NHS obligations under the NHS (standards) Framework. The NHS did not have to comply with clause 21(2)(a) and 21(12) of the 2012 Regulations.
The NHS no longer had a duty to assess a patient’s “eligibility for NHS Continuing Healthcare” before discharging them. In addition, no relevant body needed to have any “regard to the National Framework.” It is important to recognise what this meant within the context of a supposed global pandemic.
On 19th March 2020 the HCID group of Public Health England and the Advisory Committee on Dangerous Pathogens (ACDP) unanimously agreed to downgrade COVID 19, from a High Consequence Infectious Disease, due to low mortality. The UK government issued instructions to the NHS that they must discharge as many patients as possible on the same day.
With no duty to assess a patient’s continuing healthcare needs, the government set very unsafe assessment criteria and compelled hospitals to discharge them. Unless they were in intensive care, receiving oxygen, on intravenous fluids or imminently close to death, the government decreed:
“Every patient on every general ward should be reviewed on a twice daily board round to determine the following. If the answer to each question is ‘no’, active consideration for discharge to a less acute setting must be made.”
This is worth reiterating. During an allegedly unprecedented health crisis the UK government removed the NHS duty to assess a patient’s health status (and conditions) before discharging them from hospital. They then issued instructions compelling the NHS to discharge as many patients as possible.
The government and the NHS accepted that this would mean discharging patients with an active COVID 19 infection into the community. COVID patients, and people with a range of potentially life threatening conditions, were shipped into care settings where other vulnerable adults, who may not not have had any infection, were supposedly “shielding.”
There is no doubt that untested and COVID 19 positive patients entered the care system via this route. Both during the first and second “waves.” It is entirely reasonable to suspect that this policy, combined with others we are about to discuss, caused the said “waves.”
An August 2020 study by the Queen’s Nursing Institute found the following practices commonly operating in Care Homes during the spring 2020 outbreak. We should note the element of compulsion:
“Having to accept patients from hospitals with unknown Covid-19 status, being told about plans not to resuscitate residents without consulting families, residents or care home staff… 21% of respondents said that their home accepted people discharged from hospital who had tested positive for Covid-19… a substantial number found it difficult to access District Nursing and GP services… 25% in total reporting it somewhat difficult or very difficult during March-May 2020.”
“These settings are admitting people who are discharged from hospital with a COVID-positive test who will be moving or going back into a care home setting.”
Even a few isolated voices in the mainstream media pointed out what they referred to as culpable neglect. Some of the UK’s leading charities for vulnerable people including the Alzheimer’s Society, Marie Curie, Age UK, Care England and Independent Age contributed toward an open letter to the UK government. Written on 14th April 2020 they highlighted a litany of policy “failures:”
“Instead of being allowed hospital care, to see their loved ones and to have the reassurance that testing allows; and for the staff who care for them to have even the most basic of PPE, they are told they cannot go to hospital, routinely asked to sign Do Not Resuscitate orders.”
The policies operated both by the NHS and the care homes, as a consequence of Coronavirus Act’s “legislative easement,” did not protect the most vulnerable. Rather they maximised their clinical risk. Not just of COVID 19, but of every condition that rendered them vulnerable in the first place.
From the 17th March 2020 the NHS were discharging vulnerable patients into care homes without assessing their “eligibility for healthcare.” On 2nd April 2020 the NHS combined this with instructions that care home residents should not be conveyed to hospital. On the 6th April they issued guidance to GP’s which stated:
“All patients should be triaged remotely… Remote consultations should be used when possible. Consider the use of video consultations when appropriate.”
So called “first wave” mortality peaked on the 11th of April and the UK government published its COVID 19 Action Plan on the 15th April. This seemingly insane policy agenda was deemed “necessary” by the UK state to create “capacity” in the NHS:
“The UK Government with the NHS set out its plans on the 17th March 2020 to free up NHS capacity via rapid discharge into the community and reducing planned care… We can now confirm we will move to institute a policy of testing all residents prior to admission to care homes.”
There was no commitment to improve the situation from the UK government, just a plan to move toward one. We know from the observations of the CQC that they continued these high risk policies during the subsequent virus “waves.” There is no evidence that any of these policies were designed to reduce the risks of the most vulnerable. They all, consistently tended to increase them.
It is not tenable for politicians to now claim that they didn’t know what was happening. They constructed and enabled all of the policies that made this dangerous negligence possible. Nor is it credible to simply blame the medical profession. The widespread use of Hospital Trust gagging orders (non disclosure agreements) was also in place. Doctors who did speak out were disciplined or sacked. This was systemic policy initiative which physicians were expected to abide by.
Once the vulnerable were trapped in abandoned care homes, which were knowingly understaffed, the remaining, unprotected staff were then left to deal with both their own safety fears and the mounting mortality. The government decided this was an opportune moment to suspend all safety inspections in both hospital and care settings. This was supposed to “limit infections,” although every other decision they made appeared to increase them. Yet again, ending inspections raised the mortality risk for the most vulnerable.
At the same time, Do Not Resuscitate (DNAR) notices were being attached to vulnerable people’s care plans, often without their consent or even their knowledge. This coincided with a massive increase in orders for the potentially life ending medication midazolam.
In March 2020 the NHS purchased the equivalent of two years worth of supply. French suppliers were then given regulatory approval by the MHRA to sell additional stock to the NHS. This was then distributed for out of hospital use in the community.
This benzodiazepine (midazolam) is a sedative/anaesthetic that suppresses respiration and the central nervous system (CNS). The British National Formulary (BNF) recommends its use for sedation of anxious or agitated terminally ill patients using a mechanised syringe pump in doses of 30–200 micrograms/kg/hour. It is not recommended for conscious sedation in higher doses due to the following risks:
“CNS (central nervous system) depression; compromised airway; severe respiratory depression.”
Therefore a frail, eight stone (50 kg) adult could receive an initial dose of up to 2.5mg followed by a total incremental dose of another 2.5mg over a 24hr period. The purpose of this would be to ease their anxiety and agitation if they were experiencing the frightening sensation of intense respiratory difficulty.
Midazolam becomes a conscious anaesthetic for use in intensive and palliative care when given in higher doses. The British Association for Palliative Medicine recommend:
“Start with 2.5-5 milligrams – if necessary, increase progressively to 10 milligrams – maintain with 10-60 milligrams / 24h in a syringe pump”
Ten milligrams is twice the BNF recommended dose to ease anxiety (for an 8 stone vulnerable adult.) Therefore it is extremely concerning that NHS Clinical Guideline for Symptom Control for patients with COVID-19 recommended 10mg of Midazolam for patients with “distressing breathlessness at rest.” This risks a rapid deterioration of the symptoms causing them that distress.
Police are still investigating an estimated 15,000 deaths that occurred at Gosport War Memorial Hospital between 1987 and 2001. An inquiry has already found that at least 456 people’s lives were “shortened” through the unwarranted use of unnecessary medication. Many suspect that the true figure is in the thousands. The independent panel into the malpractice at Gosport War Memorial Hospital found:
“There was a disregard for human life and a culture of shortening the lives of a large number of patients by prescribing and administering “dangerous doses” of a hazardous combination of medication not clinically indicated or justified… they were, in effect, put on a terminal care pathway… The risk of using them in combination has been consistently documented in the BNF. In particular, it has long been known that when given together, opioids and midazolam cause enhanced sedation, respiratory depression and lowered blood pressure.”
This report was published in September 2018. In 2020 the NHS treatment guidelines for COVID 19 patients, who were deemed to be “agitated,” was:
“Start with Morphine 20mg and Midazolam 20mg”
This is precisely the mechanical syringe combination used at Gosport War Memorial to “shorten” thousands of peoples lives. There are numerous reasons to suspect that the huge increase in midazolam ordered by the NHS, with the full knowledge of the government, was intended for this purpose.
In April 2020 the Health and Social Care Committee, chaired by Jeremy Hunt, heard submissions from medical professionals as they considered the government response to the global pandemic. In Q377 Dr Luke Evans (MP fror Hinckley and Bosworth) asked then Health Secretary about NHS provisions for “a good death.” This is medical shorthand for assisted dying or euthanasia. Dr Evans (MP) asked:
“The syringe drivers are used to deliver medications such as midazolam and morphine. Do you have any precautions in place to ensure that we have enough of those medications?”
To which Matt Hancock replied:
“Yes. We have a big project to make sure that the global supply chains for those sorts of medications… are clear. In fact, those medicines are made in a relatively small number of factories around the world, so it is a delicate supply chain and we are in contact with the whole supply chain.”
Hancock was clearly referring to the huge midazolam order and MHRA approval of the French supply chain. The UK government had already passed the Coronavirus Act, removing the NHS Framework duties, and had ordered them to discharge patients en masse. The NHS had instructed care homes not to send sick patients to hospital and GP support from the care homes had effectively been withdrawn.
Jeremy Hunt was chairing this discussion. For him to claim two months later that no one had “appeared to consider the clinical risk to care homes” smacks of vile obfuscation. The best we can say about this statement is that he was wrong. We now have the documentation which shows that the clinical risk in care homes was very carefully considered and the withdrawal of care was planned.
In 2016 the UK government ran Exercise Cygnus. The training scenario was prepared by Professor Neil Ferguson and his team at Imperial College London (ICL). It simulated a flu outbreak and was a Command Post Exercise (CPX) designed to test the UK’s pandemic preparedness. Nearly a thousand key officials took part from central and local government departments, the NHS, public health bodies from across UK, as well as local emergency response planners.
Some of the Cygnus Report recommendations were implemented in response to COVID 19 and others not. For example, it recommended legislative easements. The Coronavirus Act certainly eased the legislation surrounding the death registration process and the NHS duty of care. The legal requirements for inquests, post-mortems and cremations were also relaxed.
Exercise Cygnus also highlighted a number of deficiencies. It identified inadequate numbers of critical, general and acute care beds, which the government then proceeded to reduce further; it warned that whole sections of the NHS may have to be shut, which is exactly what the government did during the “pandemic;” it highlighted that the most vulnerable could be denied care, just as they were, and that the health service would have to be set on a war footing just to be able to cope.
These were warnings not policy suggestions. The UK government’s adoption of some of the Cygnus recommendations and determination not to address Gygnus alarms appears to have been their policy response to COVID 19.
COVID 19 healthcare strategies were seemingly set in 2016. The Cygnus scenario, modelled by Ferguson and ICL differed from their COVID 19 “models” only by virtue of being based upon influenza rather than a coronavirus.
Perhaps this explains why Exercise Cygnus was kept secret, reportedly for reasons of “national security.” When the report was released, after being exposed, it was heavily redacted and all the names of the senior officials involved were hidden.
The official explanation for this is that it was just too terrifying for the public to withstand. We might ask, terrifying for whom? Using the media to terrorise the public during the alleged pandemic was recommended by Spi-B (SAGE.)
It is reasonable to assume that many of those redacted names would have been people working for Ferguson’s ICL team and current members of SAGE. If so, this indicates that those involved in planning the response to COVID 19 not only understood what the risks were, they then provided the claimed “scientific” justification for policies which they knew would increase them.
One of the senior officials involved in Cygnus reportedly said:
“These exercises are supposed to prepare government for something like this – but it appears they were aware of the problem but didn’t do much about it.”
Again, we see the assumption that everything must be explained away as error or unfortunate oversight. This stretches credibility beyond breaking point when we understand that Gygnus ultimately produced a plan to deny healthcare during a pandemic. This policy of increasing the risks of the most vulnerable was evidently operating during the first alleged pandemic wave. It also seems likely that it continued beyond that point.
Based upon the Cygnus conclusions, in September 2017, the NHS Surge and Triage briefing paper was made available to senior health and government officials. It discussed something called population triage:
“The purpose of this paper is to provide an update to Chief Medical Officer (CMO) and the Chief Scientific Advisor (CSA) on continuing refinement of the knowledge and understanding behind the potential decision that may be required in a future extreme pandemic influenza scenario to move to a state of population triage across the country..”
Population triage means the potential denial of healthcare:
“The majority of the detail in this paper will not be replicated in any publically available documentation… Difficult decisions will be needed about maintaining patient access to care.. There is significant discussion in the paper about ceasing or changing care to patients in the HRG (Healthcare Resource Croups)… Patients would be assessed on probability of survival rather than clinical need and higher level services would no longer be provided… Total excess death rate would be in excess of 7,806 per week of the peak of the pandemic if all these services were stopped… So in the peak six weeks of a pandemic… 46,836 excess deaths could be expected”
Between 7th March and 8th May 2020, there were 47,243 excess deaths in England and Wales. According to the Cygnus predictions this was slightly higher than the numbers envisaged to result directly from the withdrawal of healthcare. However, nearly all of these deaths were attributed to COVID 19. We should ask where, in the claimed COVID 19 mortality figures, the anticipated deaths from the denial of healthcare are.
In November 2017 a number of English stakeholders also met to discuss the a pandemic briefing paper for Adult Social and Community Care. This too was a product of Exercise Gygnus. Once again the intention was to keep the report secret.
“The majority of the detail in this paper will not be replicated in any publically available documentation… Whilst demand will increase, capacity, which is already under pressure because of recruitment challenges, will also reduce because of staff absences… Adult social care will have an increased role in supporting rapid discharge from hospital.. In a severe pandemic, only those services that are life-critical will be maintained… More patients could be supported by a greater focus on telecare/tele-monitoring.”
It is known, from the reports of the CQC and national charities and other NHS documents cited in this article, that primary healthcare was withdrawn from care settings and the community. The staff shortages identified in 2016 became chronic and then severe during the pandemic. This was entirely predictable and was a known outcome of the track and trace and self isolation polices of the UK government.
The briefing paper spoke about which services could be “reduced or deferred.” Crucially these included assessment of care needs, mobility support, personal care support, maintaining family connections and access to medical treatment.
During the “first wave”approximately 25,000 vulnerable people were discharged into care homes to face the extremely high risk environment created for them by the UK government. At the same time potentially life ending drugs were being liberally prescribed.
This was the COVID 19 policy response and we were told the intention was to “protect the most vulnerable”. All of it was predicted on the assumption that hospital were struggling to cope with the “surge” in COVID 19 patients. According to the UK government, patients needed to be discharged to free up capacity in the NHS.
At the height of the so called first wave, on the 13th of April 2020, the Health Service Journal reported that hospital bed occupancy was at a record low, with 4 times more beds available that usual for the time of year. There were 37,500 available beds.
The HSJ stated that the reason for this spare capacity was the discharge policy operated by NHS at the behest of the government. What they didn’t mention is that these figures show the high risk discharge of the most vulnerable people in our society was entirely unnecessary.
You may not like it but is not “unthinkable” that this was deliberate, coordinated policy designed to increase the mortality statistics. Many have questioned the claimed severity of the alleged pandemic. If you wish to give the impression of a high mortality disease then you need the deaths to back up your claim.
It is feasible that all of these risk heightening factors happened to perfectly coalesce to increase mortality, but is it plausible? A refusal to contemplate the possibility of a intentional act does not rule it out. Only a thorough, truly independent investigation can.
While this system was in operation, the UK government encouraged widespread adoption of the Clap for Carers, often referred to as “clap for the NHS.” During lockdowns, as the whole nation was told to self isolate indoors and avoid all unnecessary congregation, between the 26th March and the 28th May, we were “allowed” to simultaneously congregate on the streets and show our appreciation by clapping, banging pots and pans and ringing bells.
Meanwhile vulnerable people were being discharged into unsafe care homes where access to medical care was withdrawn and essential social care removed. Clapping for this was obscene. The government clearly used this ploy both as a distraction and as propaganda. This does not suggest that doctors, nurses and carers do not deserve our support. Any medical professional or carer who blows the whistle is almost certainly making a career ending decision.
Given the evidence we have discussed, if we consider ourselves to be responsible citizens who live in a democracy, it is unconscionable for us to simply ignore what appears to have been a deliberate and illegal government policy of large scale euthanasia in the UK. We must seek answers from policy makers and malfeasance in office must be prosecuted wherever it is identified.
I doubt these professors have anything to fear from a food tax
By Eric Worrall | Watts Up With That? | November 19, 2016
A group of researchers in Oxford University, England have suggested that imposing a massive tax on carbon intensive foods – specifically protein rich foods like meat and dairy – could help combat climate change. […]
This proposal, from a group of people who have probably never missed a meal in their lives, is totally obscene. High income countries often have a lot of poor people who would be hard hit by increases in the price of food.
Needlessly exacerbating the risk poor people don’t get enough to eat, especially children and pregnant mothers, who are especially vulnerable to adverse health impacts from lack of protein in their diet – if this ghastly proposal is ever implemented, future generations will look upon it as a crime against humanity. – Read full article
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.
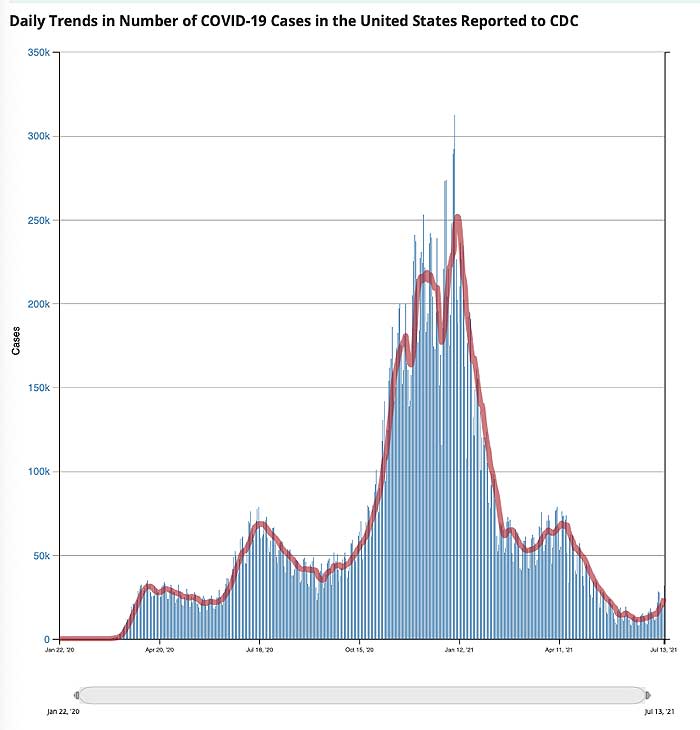



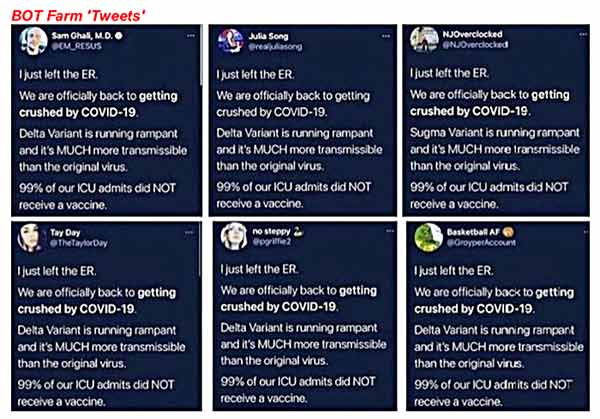
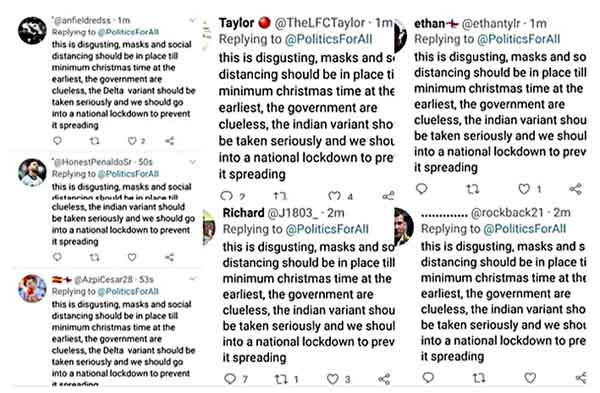
 More than seven months have passed since an unarmed protester named Ashli Babbitt was
More than seven months have passed since an unarmed protester named Ashli Babbitt was 





