The FDA wants to hide pre-licensure data until you’re dead. Now the CDC wants to hide post-licensure safety data
By Aaron Siri | Injecting Freedom | December 30, 2021
You must take this product. You cannot sue if injured. You can maybe see the clinical trial safety data in 75+ years. And the deidentified post-licensure safety data – no, you cannot see that either.
Three prior posts explained how the FDA seeks to delay for 75+ years full production of Pfizer’s pre-licensure safety data. While we have that fight, we submitted a request to the CDC, on behalf of ICAN, for the deidentified post-licensure safety data for the Covid-19 vaccines in the CDC’s v-safe system. Even though this data is available in deidentified form (meaning, it includes no personal health information), the CDC refused to produce this data claiming it is not deidentified.
So, on behalf of ICAN, we filed a federal lawsuit against the CDC and its parent entity, the U.S. Department of Health and Human Services (HHS), to force the CDC to produce this data to the public. The CDC should have no issue doing so because it has already made this data available to a private company – Oracle – in deidentified form. It is telling that Larry Ellison’s company can see the data American taxpayers paid the CDC to collect but the average American and independent scientists cannot?!
What is the v-safe system you may ask? Since rolling out the Covid-19 vaccines, the FDA and CDC have stated that their primary safety monitoring system, VAERS, is unreliable. The CDC therefore deployed a new safety monitoring system for COVID-19 vaccines called “v-safe.” V-safe is a smartphone app that allows vaccine recipients to “tell CDC about any side effects after getting the COVID-19 vaccine.” The purpose of the app “is to rapidly characterize the safety profile of COVID-19 vaccines when given outside a clinical trial setting.” With this new system, the CDC claims that these “vaccines are being administered under the most intensive vaccine safety monitoring effort in U.S. history.”
That all sounds great. And a CDC document explains that data submitted to v-safe is “collected, managed, and housed on a secure server by Oracle,” a private computer technology company, and that Oracle can access “aggregate deidentified data for reporting.” This means data submitted to v-safe is already available in deidentified form and could be immediately released to the public.
But yet, after we submitted a FOIA request to the CDC, on behalf of ICAN, to produce the deidentified v-safe data, the CDC acknowledged that “v-safe data contains approximately 119 million medical entries” but refused to produce that data by claiming that the “information in the app is not de-identified.” The CDC had apparently not read its own documentation regarding v-safe. But we had. So, we appealed this decision and submitted another request to the CDC that expressly asked only for any deidentified v-safe data, in the app or otherwise. Meaning, in the form that the CDC made the data available to Oracle. Incredibly, the CDC administratively closed this request stating it was duplicative of the original request.
Let me break that down again. The first request was denied by the CDC because it claimed the request sought data in the app that was deidentified. But then the CDC closed the second request, which made clear it is seeking only deidentified data (in the app or otherwise), by claiming the second request was duplicative of the first request! If this sounds ridiculous, it is because it is.
The public should be outraged by the CDC’s games.
The introduction to the lawsuit is copied below with a link to the entire complaint at the end. As with the pre-licensure Pfizer data, if you find what you are reading difficult to believe, that is because it is dystopian for the government to give pharmaceutical companies billions, mandate Americans to take their products, prohibit Americans from suing for harms, yet refuse to let Americans see the pre- and post-licensure safety data for these products. The lesson yet again is that civil and individual rights should never be contingent upon a medical procedure.
INTRODUCTION TO LAWSUIT AGAINST CDC FOR V-SAFE DATA
1. Between December 2020 and February 2021, the Food and Drug Administration (“FDA”) issued Emergency Use Authorizations for three COVID-19 vaccines, one of which subsequently received FDA approval in August 2021. While the FDA approved these vaccines, the Centers for Disease Control and Prevention (“CDC”), an agency within the Department of Health and Human Services (“HHS”), is charged with monitoring the safety of all vaccines, including the COVID-19 vaccines approved by the FDA. The CDC claims that these “COVID-19 vaccines are being administered under the most intensive vaccine safety monitoring effort in U.S. history[.]”
2. The federal government has mandated that millions of Americans receive these vaccine products. HHS has also given pharmaceutical companies complete immunity for injuries caused by those products. Mandating that millions of Americans inject a product for which they cannot hold the manufacturer liable if the product injures them demands complete transparency, especially when it comes to releasing the data underlying the product’s safety. FOIA exists precisely so that the American people can obtain transparency and, in this case, obtain the data which supports the CDC’s claims to intensive safety monitoring.
3. As for the pre-licensure data submitted by the pharmaceutical companies, the FDA took the position in another FOIA action that, because it needs to deidentify that data, it needs at least 75 years to produce the data to the public. As for the post-licensure data, the FDA and CDC have said that their prior primary existing safety monitoring program was incapable of determining causation and were otherwise unreliable. The CDC has, however, deployed a new safety monitoring system for the COVID-19 vaccines, v-safe, and the data within v-safe is already available in deidentified form and could be forthwith released to the public.
4. V-safe is a smartphone app that allows vaccine recipients to “tell CDC about any side effects after getting the COVID-19 vaccine.” The purpose of the app “is to rapidly characterize the safety profile of COVID-19 vaccines when given outside a clinical trial setting and to detect and evaluate clinically important adverse events and safety issues that might impact policy or regulatory decisions.”
5. Data submitted to v-safe is “collected, managed, and housed on a secure server by Oracle,” a private computer technology company. Although the CDC has “access to the individualized survey data,” Oracle can only access “aggregate deidentified data for reporting.”
6. Plaintiff asked through its instant FOIA requests that the CDC produce the deidentified data from the v-safe program in the same form that Oracle can access. Plaintiff believes that to assure transparency regarding the government’s claim that COVID-19 vaccines are “safe and effective,” the public should have immediate access to all v-safe data, in deidentified form, and therefore, once the CDC produces that data, Plaintiff intends to make it publicly available. Despite the fact that the deidentified data already exists, it is already in the hands of a private company, and the CDC has never objected to its production, the CDC has so far failed to produce it to Plaintiff or to the American public. The federal government is thereby not only failing to provide the transparency necessary to earn the American people’s trust regarding these vaccines but is also failing to comply with FOIA.
7. Plaintiff Informed Consent Action Network (“Plaintiff”) is a non-profit organization that advocates for informed consent and full transparency and disseminates information necessary for same with regard to all medical interventions. It intends to make all v-safe data immediately available to the public so that independent scientists can immediately analyze that data. It believes that we need all hands on deck, both inside and outside the government, to address serious and ongoing issues with the vaccine program, including waning immunity, adverse reactions, etc. Locking out independent scientists from addressing these issues is dangerous, irresponsible, unethical, and illegal.
8. To acquire the v-safe data, Plaintiff made three requests to the CDC pursuant to the Freedom of Information Act (5 U.S.C. § 552, as amended) (“FOIA”) seeking information regarding v-safe.
….
You can read the entire complaint here :

ICAN Sues CDC to Stop Hiding V-Safe Data from the Public
Informed Consent Action Network | December 29, 2021
The FDA and CDC have now made crystal clear that their promise of transparency with regard to COVID-19 vaccines was hogwash. As everyone now knows, the FDA has asked a federal judge to give it at least 75 years to produce the pre-authorization/licensure safety data. And we now know with certainty, federal health authorities similarly want to hide the post-authorization/licensure safety data.
The FDA and CDC have admitted their existing safety monitoring program, VAERS, was incapable of determining causation and therefore unreliable. The CDC has therefore deployed a new safety monitoring system for COVID-19 vaccines called v-safe, and now claims that these “vaccines are being administered under the most intensive vaccine safety monitoring effort in U.S. history.”
V-safe is a smartphone app that allows vaccine recipients to “tell CDC about any side effects after getting the COVID-19 vaccine.” The purpose of the app “is to rapidly characterize the safety profile of COVID-19 vaccines when given outside a clinical trial setting.” Data submitted to v-safe is “collected, managed, and housed on a secure server by Oracle,” a private computer technology company. Although the CDC has “access to the individualized survey data,” Oracle can only access “aggregate deidentified data for reporting.” Meaning, based on the CDC’s own documentation, the data submitted to v-safe is already available in deidentified form (with no personal health information) and could be immediately released to the public.
ICAN, through its attorneys, therefore asked in three FOIA requests that the CDC produce the deidentified data from the v-safe program in the same form in which Oracle can currently access it. The agency acknowledged that “v-safe data contains approximately 119 million medical entries” but denied producing that data because the “information in the app is not de-identified.” The CDC had apparently not read its own documentation regarding v-safe. But ICAN’s attorneys had and so they administratively appealed this decision and, at the same time, to leave no doubt what was being requested, submitted another request to the CDC that sought all data deidentified after it was submitted to the v-safe app (in other words, in the form that the agency made known that Oracle has the data). Incredibly, the CDC administratively closed this request stating it was duplicative of the original request.
Meaning, the first request was denied by the CDC because the CDC claimed it requested data that was deidentified when entered into the app, but then the CDC closed the second request (which was identical to the first request except for making clear it was seeking data deidentified at any point – before or after it was entered into the app) by claiming the second request was duplicative of the first request! The CDC is plainly playing games. It clearly does not want the v-safe data released.
The public should have immediate access to all v-safe data in deidentified form. Despite the fact that this deidentified data already exists, that it is already in the hands of a private company, and that the CDC has never objected to its production, the CDC has so far failed to produce it to ICAN or to the American public – the same people being mandated to take this liability-free product. But don’t worry, ICAN will not rest until this data is made public and so today has commenced a lawsuit against the CDC and HHS demanding that a court compel them to release this data.
You can read this lawsuit here.
Ivermectin and the Price of Life
By Justus R. Hope, MD | The Desert Review | December 13, 2021
What is your life worth? More to the point, what is your loved one’s life worth? What value would you place on your child, your mother, father, or spouse?
When the world experienced an average of nearly 15,000 COVID deaths per day, Dr. Andrew Hill decided on the price of a human life. Dr. Hill made that calculation during a conversation with Dr. Tess Lawrie, in January of 2021, during the peak of the Winter Surge.
In a zoom conversation between Dr. Tess Lawrie, nicknamed the “Conscience of Medicine,” and Dr. Andrew Hill, then the most influential Ivermectin advocate in the world, Dr. Hill chose dollars over human lives.
Hill’s parent institution, the University of Liverpool, had just received a 40 million dollar donation from UNITAID four days before Hill’s Ivermectin paper was published, and Dr. Hill’s conclusion was changed 180 degrees from his position just a few weeks earlier.
Andrew Hill admitted that his sponsors (UNITAID) pressured him to alter his conclusion. Hill explained, “I think I’m in a very sensitive position here.”
Dr. Lawrie called Hill out. She stated, “Lots of people are in sensitive positions; they’re in hospital, in ICUs dying, and they need this medicine.”
Lawrie criticized Hill, “This is what I don’t get, you know, because you’re not a clinician. You’re not seeing people dying every day. And this medicine prevents deaths by 80%. So 80 percent of those people who are dying today don’t need to die because there’s Ivermectin.”
Hill responded that the NIH would not agree to recommend IVM.
Dr. Tess Lawrie fired back, “Yeah, because the NIH is owned by the vaccine lobby…This is bad research. So at this point, I am really, really worried about you.”
Hill answered, “Okay. Yeah. I mean, it’s a difficult situation.”
Lawrie responded, “No, you might be in a difficult situation. I’m not because I have no paymaster. I can tell the truth… How can you deliberately try and mess up…you know? So, how long are you going to let people carry on dying unnecessarily – up to you? What is the timeline you’ve allowed for this, then?”
Andrew Hill reacted, “Well, I think… I think that it goes to WHO and the NIH, and the FDA, and the EMEA. And they’ve got to decide when they think enough is enough.”
Dr. Lawrie pointed out the obvious, “You’d rather… risk loads of people’s lives. Do you know if you and I stood together on this, we could present a united front and we could get this thing. We could make it happen. We could save lives; we could prevent people from getting infected. We could prevent the elderly from dying…
I’m a doctor, and I’m going to save as many lives as I can. And I’m going to do that through getting the message [out] on Ivermectin…Okay. Unfortunately, your work is going to impair that, and you seem to be able to bear the burden of many, many deaths, which I cannot do.”
Dr. Lawrie demanded to know the identity of the unknown UNITAID author who changed Dr. Hill’s conclusions, the person whose influence was to cause so many preventable deaths.
“So who is it in UNITAID, then? Who is giving you opinions on your evidence?”
Hill answered, “Well, it’s just the people there. I don’t…”
Dr. Lawrie pressed Hill, “Could you please give me a name of someone in UNITAID I could speak to, so that I can share my evidence and hope to try and persuade them to understand it?
Dr. Hill evaded, “Oh, I’ll have to think about who to, to offer you with a name… But I mean this is very difficult because I’m, you know, I’ve got this role where I’m supposed to produce this paper and we’re in a very difficult, delicate balance… Yeah, it’s a very strong lobby…”
The conversation concludes with Dr. Hill promising to do everything in his power to get Ivermectin approved if she could give him six more weeks.
Dr. Lawrie, “So, how long do you think the stalemate will go on for?”
Dr. Hill, “From my side. Okay… I think end of February, we will be there in six weeks.”
Dr. Tess Lawrie, “How many people die every day?”
Dr. Andrew Hill, “Oh, sure. I mean, you know, 15,000 people a day.”
Dr. Tess Lawrie, “Fifteen thousand people a day times six weeks… Because at this rate, all other countries are getting Ivermectin except the UK and the USA, because the UK and the USA and Europe are owned by the vaccine lobby.”
Dr. Andrew Hill, “My goal is to get the drug approved and to do everything I can to get it approved so that it reaches the maximum…”
Dr. Tess Lawrie, The Conscience of Medicine, concluded with this, “You’re not doing everything you can, because everything you can would involve saying to those people who are paying you, ‘I can see this prevents deaths. So I’m not going to support this conclusion anymore, and I’m going to tell the truth.’”
Finally, Dr. Lawrie added, “Well, you’re not going to get it approved the way you’ve written that conclusion. You’ve actually shot yourself in the foot, and you’ve shot us all in the foot. All of… everybody trying to do something good. You have actually completely destroyed it… I don’t know how you sleep at night, honestly.”
The fact that Dr. Andrew Hill allowed another person to change his paper’s conclusion has been known for more than six months and was published in the book, Ivermectin for the World.
“However, he [Dr. Andrew Hill] was reigned in before more damage [to the vaccine lobby] was done:
- He was invited to the NIH, along with Dr. Marik, probably to give the appearance of propriety.
- He was given a gag order and told not to speak to any more press until The WHO made an official decision on Ivermectin. It turned out that this decision would go against the drug despite Dr. Hill’s findings.
- Dr. Hill’s conclusion would be changed by someone else, and the rest is history.”
What was not known, until the transcript of the zoom conference between Dr. Hill and Dr. Lawrie was leaked, were the specifics of the quid pro quo. It turns out that the height of the COVID-19 Winter surge, when about 15,000 people per day were dying, was precisely the same time as the zoom conference, held on January 18, 2021. Moreover, it was days after Andrew Hill’s University of Liverpool took the $40 million payoff.
The transcript of this conference call appeared in Robert F. Kennedy Jr.s’ book, The Real Anthony Fauci, and in this article published by The Defender newsletter:
https://childrenshealthdefense.org/defender/ivermectin-big-pharma-rfk-jr-the-real-anthony-fauci/
World daily COVID deaths were averaging around 15,000 per day on January 18, 2021, and six weeks later were averaging some 9,700. Currently, the world is seeing about 7,500 per day die.
80% of these or more could have been prevented with Ivermectin, a statement with which Dr. Hill would likely agree.
Overall, since that fateful decision of Andy Hill to allow his sponsor to “change” his paper’s conclusion, 2.475 million people [11 months x 30 days per month x 7500 deaths per day] have died, 80% of them could have been saved had Ivermectin been approved. So precisely 1.98 million lives were lost as a result of the betrayal.
The price per life?
Forty million dollars was the value of the donation made to the University of Liverpool by UNITAID. This sum comes out to 20 dollars and 20 cents per life. That is what we are all worth in the calculus of the vaccine lobby.
UNITAID bills itself as a “global health agency” hosted by the World Health Organization and supported by the vaccine lobby.
The Bill and Melinda Gates Foundation contributed hundreds of millions to UNITAID. In October, they committed $120 million more to the new expensive Merck drug molnupiravir, a costly and genotoxic competitor of Ivermectin.
Some experts say it will stimulate the emergence of viral mutants and worsen the pandemic.
https://uk.news.yahoo.com/covid-pill-being-rolled-among-121237206.html
If that prospect is not concerning enough, consider this: One dose of Remdesivir, a drug that does not save lives, but one that is widely used on most United States ICU COVID cases, costs $3,100 per dose, or to put it bluntly, one dose of Remdesivir is worth roughly 153 lives. Yet, the worst drug earned the FDA’s approval while the best one, Ivermectin, was suppressed for money.
Ivermectin, a drug that has nearly eradicated River Blindness in much of the world, a safe drug already given to humans in over 4 billion doses, can be purchased mail-order from India at 1,000 12mg tablets for $163. That comes out to 16.3 cents per dose.
Dr. Alan Bain recently saved the life of 71-year-old Sun Ng thanks to a court order issued by Judge Paul Fullerton. Following the hospital’s initial refusal, Ng’s family sued Edward-Elmhurst Health and Sun Ng was administered the Ivermectin for five days. After the treatment, Ng “removed his breathing tube” and was taken out of ICU.

Sun Ng’s Recovery with Ivermectin
Dr. Bain, unable to get a local pharmacy to fill the prescription for Ivermectin, obtained the mail-order version and saved Ng’s life.
https://patch.com/illinois/naperville/covid-patient-given-ivermectin-edward-improving-report
Thus, five 12 mg doses cost about 82 cents but are worth more than the 20 dollar value placed by the vaccine lobby and Andrew Hill on a human life because pennies were all it took to purchase the Ivermectin that saved Sun Ng.
Ivermectin has 27 randomized controlled studies involving tens of thousands of patients showing reduced time to viral clearance, hastened recovery time, and reduced mortality. On the other hand, the vaccine lobby’s choice, Remdesivir, was rejected by the WHO as a drug that failed to improve survival and other outcomes.
https://covid19criticalcare.com/wp-content/uploads/2021/08/SUMMARY-OF-THE-EVIDENCE-BASE-FINAL.pdf
One thousand doses of Ivermectin can be purchased online for $163. Yet, UNITAID paid $40 million to change Dr. Hill’s conclusions to call for more studies [delaying Ivermectin approval], essentially condemning millions of human beings to death from COVID-19. So while 82 cents may be the price of life, it seems that twenty pieces of silver remains the price of death.
Dr. Justus R. Hope, writer’s pseudonym, graduated summa cum laude from Wabash College where he was named a Lilly Scholar. He attended Baylor College of Medicine where he was awarded the M.D. degree. He completed a residency in Physical Medicine & Rehabilitation at The University of California Irvine Medical Center. He is board-certified and has taught at The University of California Davis Medical Center in the departments of Family Practice and Physical Medicine & Rehabilitation. He has practiced medicine for over 35 years and maintains a private practice in Northern California.
FDA Should Need Only ‘12 Weeks’ to Release Pfizer Data, Not 75 Years, Plaintiff Calculates
By Seth Hancock | The Defender | December 17, 2021
U.S. Food and Drug Administration (FDA) officials skipped the start of oral arguments Tuesday as a federal district court weighed whether the agency can take 75 years to fully release documents on Pfizer’s Comirnaty COVID vaccine, according to a lawyer representing plaintiffs who sued the FDA for the documents.
A U.S. Department of Justice lawyer representing the FDA told the U.S. District Court for the Northern District of Texas the agency will produce more than 329,000 related documents as fast as it can, while safeguarding personally identifiable information and Pfizer trade secrets.
Public Health and Medical Professionals for Transparency (PHMPT), the group behind the Freedom of Information Act (FOIA) request and subsequent lawsuit, is seeking safety and effectiveness data, adverse reaction reports and a list of active and inactive vaccine ingredients.
PHMPT is a group of more than 30 scientists, medical professionals, international public health professionals and journalists. The group’s lawsuit argues the FDA is overestimating the time needed and understaffing the job.
“Assuming a low average of 50 pages per hour per person, even to review the hundreds of thousands of pages the FDA estimates, the agency would need just 19 reviewers to work full-time for 12 weeks to review and produce these documents — which is a tiny fraction of its approximately 18,000 employees,” said PHMPT in a legal brief filed Monday.
The day before oral arguments, the FDA released 14 document files, the largest file including 2,030 pages. PHMPT posted an updated list which shows documents released since Nov. 17.
FOIA does not mandate any particular processing schedule, only that the agency process requests “as soon as practicable,” the FDA said in a legal brief filed Monday.
“The bottom-line issue still remains what processing schedule is ‘practicable’ for the agency,” the FDA said.
At the agency’s proposed rate of 500 documents per month, the last documents would be released in 2096.
A quote from Business Intelligence Associates, an e-discovery company, estimated 400,000 pages could be produced within six to eight weeks at a cost of $132,000, according to PHMPT.
PHMPT wants the FDA documents released within 108 days. That’s the same amount of time the FDA spent reviewing the responsive documents for “the far more intricate task” of licensing Pfizer’s vaccine, the group said in its lawsuit.
Attorney Aaron Siri, who represents PHMPT, said:
“Americans must routinely produce documents, pay fines, and otherwise expend resources to comply with the law. Courts don’t inquire as to the ability or financial resources to comply with the law — they must comply.
“In fact, it would be laughable if a billionaire defendant came before a court and claimed poverty to escape making a document production, but that is the FDA’s position.”
The FDA budget for fiscal year 2019 was $6.1 billion.
In the FDA’s 64-page briefing, the agency argued it needed the full 75 years to redact and release the documents out of “fairness” to other FOIA requesters.
PHMPT defined fairness differently in its responding brief:
“Fairness would be giving millions of Americans who are mandated to receive this liability-free vaccine today assurance regarding the FDA’s review by allowing independent scientists access to the same data the FDA reviewed, without making them wait decades.
“Fairness would be allowing Americans injured by the vaccine today, who cannot sue Pfizer or anyone else for the harm, hope that independent scientists with access to that data can more readily develop treatments for their ailments.
“Fairness would be our federal health authorities allocating more than one person spending a few hours each month to review Pfizer’s documents for public disclosure after having given Pfizer over $17 billion of taxpayer money to develop and market the product.
“That would be fair to the American people.”
Siri noted that no decision has been made by the court and that a transcript of this week’s hearing should be released soon.
U.S. Rep. Ralph Norman (R-S.C.) earlier this month introduced a bill that would force the FDA to release them in 100 days.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
The FDA approves boosters for minors – without testing boosters on minors
Age group testing? Zero.

Techno Fog | December 14, 2021
Late last week, on December 9, the FDA approved the Emergency Use Authorization (EUA) for the Pfizer COVID-19 vaccine, “authorizing the use of a single booster dose for administration to individuals 16 and 17 years of age.” The booster is to be given at least 6 months after vaccination.
Before we get to the data the FDA cited in the booster for kids aged 16-17, let’s go through the facts:
COVID-19 is not a threat to teenagers aged 16-17. On October 25, we warned that the FDA was about to approve an experimental COVID-19 vaccine for children. It seemed unnecessary to give the EUA Pfizer vaccine to minors, as CDC data showed that for children aged 5-11 years-old, there have been 1.8 million COVID-19 cases and only 138 deaths. For older kids, from our own calculations, there have been approximately 3 million COVID-19 infections for those aged 12-18 years, leading to approximately 400 COVID-19 deaths in those ages. Children who get COVID-19 (including the age range approved for the latest booster) generally have less severe symptoms. Even the CDC concedes that “children are less likely to develop severe illness or die from COVID-19.”
The Pfizer vaccine is particularly dangerous for young men aged 16-17. As we observed back in October, teenage boys are especially at risk for heart problems – like myocarditis – after getting the Pfizer vaccine:
“Boys between 16 and 19 years of age had the highest incidence of myocarditis after the second dose . . . The risk of heart problems in boys of that age was about nine times higher than in unvaccinated boys of the same age.” New York Times.
The risk of myocarditis for boys 16 – 19 years old is higher after the Pfizer second dose. What happens after the third dose??
That’s a good question.
One would rightly assume that the third dose might present more danger of heart problems than the second dose. But FDA doesn’t have the answer to this question. And why doesn’t it have the answer?
Because the FDA didn’t look.
Because the FDA decided against holding an advisory meeting to discuss the decision.
Because the FDA required ZERO tests in this age bracket before approving the latest Pfizer booster for this age bracket.
Instead, the FDA relied on prior (old) booster data from a study of “200 participants, 18 through 55 years of age.” Choosing to ignore the long-term data for the efficacy of the Pfizer booster shot, the FDA instead reviewed the old data showing “the antibody response against the SARS-CoV-2 virus one month after a booster dose of the vaccine.”
That’s it. That’s the rigorous studies that now meet FDA standards. Given the self-imposed and purposeful limitations the FDA has placed on its own own information, it has the audacity to conclude:
“The benefits of a single booster dose of the Pfizer-BioNTech COVID-19 Vaccine or Comirnaty outweigh the risks of myocarditis and pericarditis in individuals 16 and 17 years of age to provide continued protection against COVID-19 and the associated serious consequences that can occur including hospitalization and death.”
This is the FDA making a cost/benefit calculation without knowing the costs or benefits. It doesn’t know the real risks because it didn’t study the potential for adverse reactions in kids aged 16 – 17 years. It doesn’t know the real benefits because it chose a shitty study that was limited to one month efficacy data.
This robust FDA cost/benefit calculation might sound familiar to our loyal readers. That would be because the Government did the same thing when recommending the COVID-19 vaccines for “people who are pregnant.”
FDA Colludes with US Postal Service to Destroy Ivermectin Shipments
InfoWars | December 15, 2021
The US Food and Drug Administration is colluding with the US Postal Service to intercept inbound international shipments of Covid wonder drug ivermectin, reports circulating on social media claim.
According to letters from the FDA being shared online, the federal regulatory agency blocked shipments of ivermectin from reaching their intended recipients as they came through ports of entry.
“A shipment addressed to you from a foreign country is being held by the post office at the request of the US Food and Drug Administration,” reads one letter shared by attorney Aaron Siri.
According to the letter, the package containing 200 tablets of “Iverheal ivermectin tablets” was intercepted at the JFK Airport Port of Entry on November 9, 2021.
In another letter, the FDA intercepted 300 tablets of “Iverpac12” back in August, which they said were “subject to refusal of admission into the United States and are subject to administrative destruction.”
News of the FDA’s collusion with the US Postal Service comes as more people seek the effective drug and other preventative early treatments to remedy Covid-19 symptoms.
Meanwhile, the FDA has continued it’s fear-mongering campaign advising Americans not to consume the “horse dewormer” drug to treat Covid, as it has not been formally approved [for COVID use].
Comirnaty, liability, and how the HHS lies, cheats and steals
By Meryl Nass, MD | December 12, 2021
I checked the Federal Register and there has been no notice that Comirnaty has been added to the National Childhood Vaccine injury Program (NVICP). I confirmed this by checking whether Comirnaty had been added to the childhood schedule, and according to the HRSA, which manages both compensation programs, it has not.
So, if you receive the licensed Comirnaty vaccine, correctly labeled as the brand-name product and not the vaccine being fobbed off as licensed product, and you are injured, you are free to sue the manufacturer for your injury. Could this be why Pfizer wrote, “Pfizer does not plan to produce any product with these new [Comirnaty National Drug Codes] and labels over the next few months while EUA authorized product is still available and being made available for U.S. distribution.”
If, however, you receive the Pfizer-BioNTech vaccine under Emergency Use Authorization, or the Moderna or J and J vaccine, you can’t sue anyone. You have the right to beg HRSA for compensation of lost wages and unpaid medical bills, period. So far, HRSA and the Countermeasures Injury Compensation Program it administers have not paid out one dime for the approximately one million injuries and 20,000 deaths reported to VAERS for any COVID vaccine.
In other words, the federal government (DHHS) has not admitted a single injury was caused by a COVID vaccine. CDC says it has not linked a single death to a COVID vaccine–not even when the patient walked into the vaccination center but got carried out to the morgue. FDA doesn’t know much about myocarditis, Bell’s Palsy, thrombosis, thrombocytopenia, pulmonary emboli, etc. There are no black box warnings on any of the COVID vaccines.
HRSA, FDA, CDC and NIH are all agencies within the federal Department of Health and Human Services. They have all gotten their stories straight. They know nothing and they are just following orders. Heil HHS!
They can’t find a doggone problem in the 20 or so databases they are spending many $millions of your money to “study.”
Want to know the biggest conspiracy in the US right now? It is the HHS.
FDA has access to a bunch of electronic databases it has termed the “BEST” Initiative, and it published a plan to use them to study heart attacks, pulmonary embolism, thrombocytopenia, etc. back in July. Where are the results, FDA? What are you waiting for? (According to CDC, “More than 459 million doses of COVID-19 vaccines were administered in the United States from December 14, 2020, through November 29, 2021.”). It seems clear that we aren’t supposed to be informed of FDA’s findings until everyone possible has been vaccinated, at which point the results will be irrelevant.
In October 2020, FDA’s Steve Anderson told us there were even more databases that would be studied.
On August 23, 2021, FDA announced its databases were inadequate to assess myocarditis, so BioNTech would have to do it for them. Here is what FDA wrote about its inability to use VAERS and its many other databases:
- As noted above, the FDA acknowledges that “We have determined that an analysis of spontaneous postmarketing adverse events reported under section 505(k)(1) of the FDCA [in other words, VAERS–Nass] will not be sufficient to assess known serious risks of myocarditis and pericarditis and identify an unexpected serious risk of subclinical myocarditis.
- Furthermore, the pharmacovigilance system that FDA is required to maintain under section 505(k)(3) of the FDCA [in other words, FDA’s many other databases that cost the taxpayer zillions–Nass] is not sufficient to assess these serious risks.”
NOT SUFFICIENT???
Unsaid, but implied, is that if FDA is incapable of studying thousands of reported cases of myocarditis, it probably cannot study the other serious adverse events that have been reported in conjunction with COVID vaccines.
VAERS has operated for 30 years, collecting reports of vaccine adverse events. It averaged under 100 cases of myocarditis reported yearly until this year. Through November, CDC reports it received 1949 reports of myocarditis and pericarditis, in those under 30. CDC didn’t say what the total number of reports for all ages was.
Somehow, these HHS don’t seem all that concerned that the admitted reporting rate of myocarditis is over 20 times the average during the past 30 years. Why?
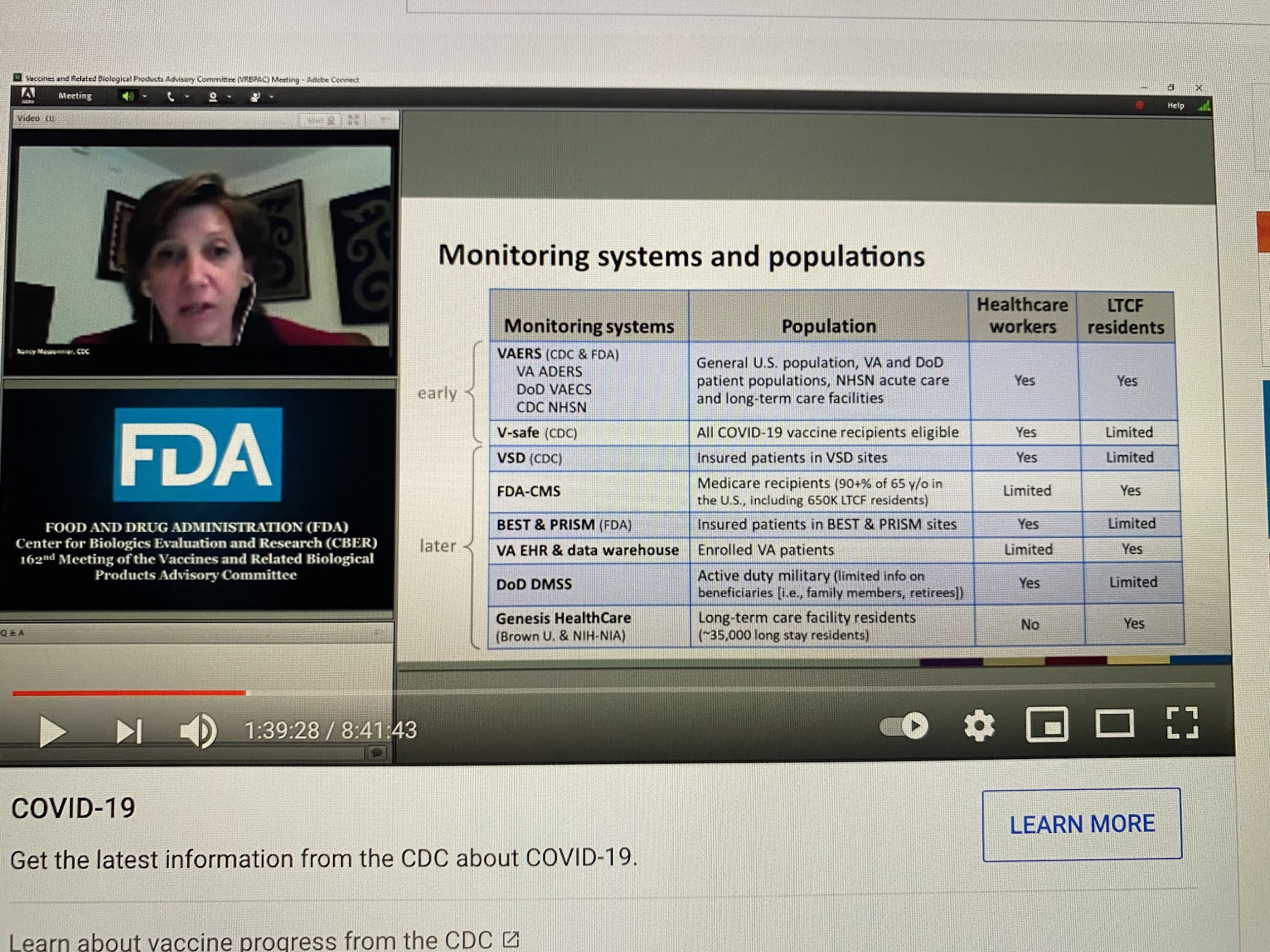
CDC has been even more shady in its analyses of safety as FDA, if that is even possible. Below, Nancy Messonier, then head of Immunizations and Respiratory Diseases at CDC, presented this list of databases that CDC would be using in the evaluation of COVID vaccine safety, on December 10, 2020. Apart from the V-safe (which they stopped talking about last January), VSD (which somehow can’t find any problems, not even myocarditis) and VAERS, all these other databases have been MIA.
NIH, whose job has never been to issue treatment guidelines, but instead to do and fund research, suddenly took over the treatment guidelines for COVID early in 2020. It formed a committee of internal and eternal “experts” to make up the guidelines. How were they chosen? That is not clear, but what is clear is that 16 of these so-called experts had current or recent financial entanglements with Gilead, the maker of remdesivir. NIH and the US Army also owned pieces of remdesivir. A number of other had financial conflicts with Merck. While NIH is the biggest single funder of medical research in the world, I cannot recall seeing a single study it funded on the safety of COVID vaccines. But somehow vaccines are its number one recommendation.
But it is not even clear that the committee is functional. The NIH has been sued to learn whether a vote was even taken by the committee regarding its ivermectin guidelines, which fly in the face of the evidence on ivermectin. How was NIH somehow authorized to issue guidelines in the first place?
Here is what has obviously occurred. All these agencies were told they had to keep quiet on vaccine problems (and perhaps problems of other COVID treatments), and they had to fiddle with their data or their analytic methods, or both, to get the required results. And there was to be NO BAD NEWS, no matter what. And no good news regarding generic treatments.
As we have seen, the so-called scientists and physicians working as bureaucrats in these agencies all caved, sucked it up, did the dirty work, kept their jobs, and betrayed their oaths and the trust of the people of the USA and the world.
Disclosing Pfizer vaccine data ‘may take until 2096’
RT | December 9, 2021
The US Food and Drug Administration is cooperating with a Freedom of Information Act request for clinical data associated with Pfizer’s Covid-19 vaccine, but may require 75 years to do so – even longer than a prior estimate.
The FDA has insisted it cannot commit to a faster release of the medical data associated with the approval of the Pfizer-BioNTech coronavirus vaccine, according to a legal brief filed on Tuesday in response to the FOIA request. The agency reiterated that after processing 12,000 pages in about a two-month period, it will only be able to process 500 pages per month going forward. With tens of thousands of additional files up for review, plaintiffs fear the process may drag on two decades longer than the previous 55-year estimate.
Lawyer Aaron Siri sued the FDA on behalf of a group of doctors calling themselves Public Health and Medical Professionals for Transparency, who had previously complained the FDA wasn’t supplying the data they had requested in a timely fashion. Having pointed out last month that the FDA had looked through Pfizer’s documents in a mere 108 days in order to license the vaccine, Siri questioned why the agency now required a whopping 20,000 days to make the same documents public.
Approximately 451,000 pages regarding the clinical trials for a vaccine millions of Americans are being mandated to take will remain floating in legal limbo for up to 75 years if the agency has its way, Siri warned. He called it “dystopian” for the government to pay Pfizer billions of dollars, shield it from lawsuits and require citizens to be injected with its product, only to refuse access to the documents used to grant its licensure in the first place.
The FDA has justified the unusual timetable by pointing out its Center for Biologics Evaluation and Research – the body tasked with reviewing the records – only has 10 staffers, two of whom are “new.” The FDA also complained that stepping up the pace would divert “significant resources away from the processing of other FOIA requests that are also in litigation.”
Remember when the FDA’s top vaccine regulator said even a moderately effective Covid shot could produce herd immunity if 70 percent of people got it?
By Alex Berenson | December 7, 2021
In late July 2020, Dr. Peter Marks, who oversees vaccines for the Food and Drug Administration, spoke for an FDA-produced podcast about the Covid vaccines.
At the time, the big mRNA vaccine trials were just beginning, and the two-part interview was fairly straightforward. It opened with Marks explaining what a vaccine is.
Later, though, Marks explained how an effective vaccine might end the epidemic:
What we also know is that once one reaches a certain level of protection, roughly 70 percent, and if 70 percent of the population gets that vaccine, you start to get to a place where the infectious disease that you’re trying to prevent, in this case, let’s read COVID-19 into that, it doesn’t have anywhere to go and you start to be able to help wipe that infectious disease out…
70 percent protection by 70 percent of the population equals (basically) no more Covid. Got it, doc!
The next week, Marks again explained the importance of 70 percent protection – and this time, he used the magic h-word:
That’s the concept of herd immunity that you have enough people in the population that can’t get the disease, that the disease has nowhere to go if it shows up. That’s exactly what we’d like to ultimately see with a really effective vaccine, one that might have, I think, we estimate at least 70 percent efficacy…
This might be a good time to remind you that much of Western Europe hit Marks’s magic number months ago. In countries like Britain, 70 percent (okay, 69.3!) of people – not adults, the entire population – is fully vaccinated. And about 30 percent of Britons have now received a third dose.
So how come a vaccine that was supposedly 95 percent effective at preventing infection (and supposedly even better at stopping severe disease) in clinical trials has completely failed to stop the epidemic?
Or, put another way, if the vaccines work, what’s going on?
Oh well. We’ll figure it out next pandemic. Meantime, get yer free booster today!
SOURCE: https://www.fda.gov/news-events/fda-insight/fda-insight-vaccines-covid-19-part-1
https://www.fda.gov/news-events/fda-insight/fda-insight-vaccines-covid-19-part-2
2,809 Dead Babies in VAERS Following COVID Shots as New Documents Prove Pfizer, the FDA, and the CDC Knew the Shots Were Not Safe for Pregnant Women
By Brian Shilhavy | Health Impact News | December 4, 2021
The latest data dump into the U.S. Government’s Vaccine Adverse Events Reporting System (VAERS) happened yesterday (12/3/21) and covers data through 11/26/2021.
There are now 927,740 cases reported to VAERS following COVID-19 shots for the past 11 months, out of the total of 1,782,453 cases in the entire VAERS database filed for the past 30+ years.
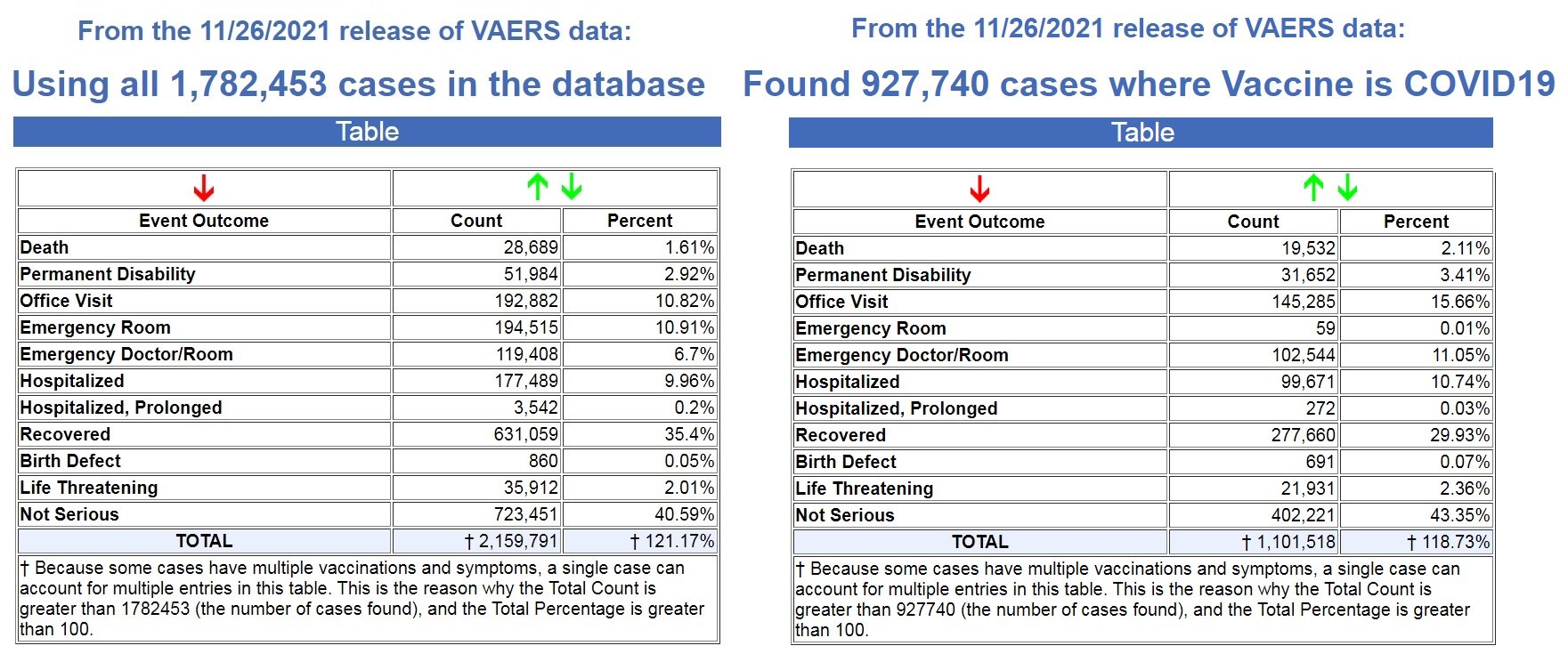
Left image source, Right image source.
That means that 52% off ALL vaccine adverse reaction cases in VAERS for the past 30+ years have been reported in the last 11 months following the COVID-19 shots.
In addition, 68% of all deaths following vaccines reported in VAERS for the past 30+ years have been reported in the last 11 months following the COVID-19 shots.
We are on pace to see 21,307 deaths reported in the first year following the experimental COVID-19 shots, while the average yearly deaths reported after FDA-approved vaccines for the past 30+ years is 305 deaths.
That is an astounding 86% increase in reported deaths following the COVID-19 shots, a 70X increase over the average reported deaths following vaccinations for the past 30+ years!
- FDA-approved vaccines: 305 deaths per year
- COVID-19 EUA shots: 21,307 deaths per year
And as Dr. Jessica Rose has previously reported, the under-reporting factor in VAERS for the COVID-19 shots is 41X, as a conservative number, which means that at least 800,812 people have now died following COVID-19 shots based on the VAERS data.
Most, if not all, of those deaths are being reported in the pharma-owned corporate media as “COVID” deaths, as there are now more recorded “COVID deaths” for the first 11 months of 2021 than there were for the entire year in 2020, when there were no COVID vaccines until December. (Source.)

Record Number of Fetal Deaths Following COVID-19 Shots
As of this most recent update in VAERS, we have now found 2,809 fetal deaths following COVID-19 shots injected into pregnant and child-bearing women for the past 11 months. (Source.)
By way of contrast, using the exact same search parameters in VAERS, but excluding the COVID-19 shots, we found 2,168 fetal deaths following all FDA-approved vaccines for the past 30+ years. (Source.)
That’s an average of 72 fetal deaths per year following all FDA-approved vaccines for the past 30+ years, compared to what is on pace to be 3064 fetal deaths in 1 year following COVID-19 shots.
- FDA-approved vaccines: 72 fetal deaths per year
- COVID-19 EUA shots: 3064 fetal deaths per year
That is an 80% increase in fetal deaths recorded in VAERS following the COVID-19 shots. And yet, the CDC and FDA continue to recommend these EUA shots for pregnant women and nursing mothers.
Not only do they recommend these shots for pregnant women, we now have ample evidence that they have known since earlier this year that these shots are dangerous to pregnant women, and causing fetal deaths.
In a March 4, 2021 Advisory Commission on Childhood Vaccines (ACCV) meeting, the CDC submitted a report that contained a section titled: Maternal vaccination safety summary (starting on p. 39).
They stated (emphasis mine – my comments in red):
* Pregnant women were not specifically included in pre-authorization clinical trials of COVID-19 vaccines
– Post-authorization safety monitoring and research are the primary ways to obtain safety data on COVID-19 vaccination during pregnancy
* Larger than expected numbers of self-reported pregnant women have registered in v-safe
* The reactogenicity profile and adverse events observed among pregnant women in v-safe did not indicate any safety problems (based on what criteria???)
* Most reports to VAERS among pregnant women (73%) involved non-pregnancy specific adverse events (e.g., local and systemic reactions)
* Miscarriage was the most frequently reported pregnancy-specific adverse event to VAERS; numbers are within the known background rates based on presumed COVID-19 vaccine doses administered to pregnant women (no supporting evidence to backup these claims)
It is important to note through all of this reporting by the CDC that these are based on self-reporting data from pregnant women.
We know that it is politically incorrect to blame any health issue on a COVID-19 “vaccine,” and that doctors and nurses are pressured to NOT report these, so how many pregnant women had an adverse reaction, like a miscarriage, and never even thought to link it to their COVID-19 shot?
So back in March of this year (2021), there were already major concerns about the effects of the shots on pregnant women, as “larger than expected” pregnant women were reporting adverse reactions, and “the most frequently reported pregnancy-specific adverse event to VAERS” was “miscarriage.”
Then in August of this year (2021), the CDC presented a “new study” with “new data.”
Again, this “data” is dependent on pregnant women “self-reporting” adverse reactions, so we know these reports will be well below what was actually happening in the population, as it is politically incorrect to report any adverse reactions related to the experimental COVID-19 shots. To do so is to be branded an “anti-vaxxer” and shame you for life.
The August update admitted that 13% of the pregnant women who had received a COVID-19 shot reported a miscarriage. The CDC brushed this aside by stating “miscarriage typically occurs in about 11-16% of pregnancies.”
But of course ALL miscarriages are reported somewhere in the medical files, which is why they can even come up with a number range like this. So this figure is based on 100% of the reported data, while the COVID-19 related miscarriages are only based on what was self-reported, and we have no idea how many women never reported their miscarriages because they never related it to their COVID-19 shot.
One the main studies the CDC allegedly relied upon to declare that COVID-19 shots were safe for pregnant women, was a study published in the New England Journal of Medicine on June 17, 2021.
But on October 14, 2021, they issued a statement stating that some of their data was wrong in the June 17th study. (Source.) It dealt specifically with pregnancies in their 20th week or earlier.
“No denominator was available to calculate a risk estimate for spontaneous abortions, because at the time of this report, follow-up through 20 weeks was not yet available for 905 of the 1224 participants vaccinated within 30 days before the first day of the last menstrual period or in the first trimester. Furthermore, any risk estimate would need to account for gestational week–specific risk of spontaneous abortion.” (Source.)
It’s not surprising that the FDA wants to slow-walk the release of COVID jab reaction data
By Dr. Joseph Mercola | December 2, 2021
It took the U.S. Food and Drug Administration 108 days to review all the data Pfizer/BioNTech submitted in order to gain FDA approval for its Comirnaty COVID shot, which was licensed August 3, 2021.
Considering the agency claims there are 329,000 pages of data, the fact that they were able to read, analyze and draw conclusions about its safety and effectiveness in just 108 days — about 80,000 pages a month — is no small miracle. They must employ some very efficient speed readers.
And that is why the FDA’s claim that it now needs half a century to review the documents before they can release them to the public doesn’t seem very credible. Even Reuters has expressed shock, and its former CEO is on the board of Pfizer.1
Expedited FOIA Request for Comirnaty Data
In September 2021, a group called Public Health and Medical Professionals for Transparency (PHMPT) filed a Freedom of Information Act (FOIA) request with the FDA to obtain the documentation used to approve Comirnaty.
This includes safety and effectiveness data, adverse reaction reports and lists of active and inactive ingredients. Approximately 400 additional FOIA requests by other individuals for all or part of this information have also been filed.2
In their FOIA application, the PHMPT asked the agency to expedite release of the documents — a reasonable request, considering we have no raw data and the shots are being pushed on children as young as 5.
FOIA guidelines include two conditions upon which a request may be expedited. One is “if the lack of expedited treatment could reasonably be expected to pose a threat to someone’s life or physical safety,” which one could easily argue is the case here.
The second condition is “if there is an urgency to inform the public about an actual or alleged federal government activity, if made by a person who is primarily engaged in disseminating information.” This too is clearly applicable.
“During a time when COVID-19 vaccine mandates are being implemented over the objection of those that have questions about the data and information supporting the safety and efficacy of the Pfizer Vaccine, and individuals with these questions are being expelled from employment, school, transportation, and the military, the public has an urgent and immediate need to have access to this data,” the PHMPT said in its request.3
FDA Now Wants 55 Years to Release COVID Jab Data
When, after a month, the FDA still had not responded to the FOIA request, the PHMPT sued.4 The FDA is now asking a federal judge to allow them to delay the full release of all documents until 2076 — 55 years from now.
According to the U.S. Department of Justice (DOJ) attorney who represents the FDA in this case, the agency will be able to “provide more pages to more requesters” if allowed to stick to a rolling schedule of 500 pages per month, “thus avoiding a system where a few large requests monopolize finite processing resources.”
They claim they only have 10 employees assigned to FOIA releases, and before material can be released, an FDA official has to go through them and redact any information that might reveal personal information about clinical trial participants and any confidential business or trade secret information.
The 1967 FOIA law requires federal agencies to respond to FOIAs within 20 days unless “unusual circumstances” exist that prevent a timely release. Circumstances that might warrant an extended release schedule include:
- Instances where response records must be searched for and collected from an entity other than the office processing the request
- Situations involving “voluminous” amounts of records that must be compiled, and
- Instances requiring consultation with another federal agency that has a substantial interest in the information
The DOJ attorney points out that the court has allowed for a 500-page maximum per month release schedule in other cases, and should allow the FDA the same leeway here.
Plaintiffs, on the other hand, argue the agency should be able to release everything by early March 2022, noting the FDA employs 18,000 people and has an annual budget of $6 billion. Between 2008 and 2017, the agency processed 114,938 FOIA requests, of which it granted 72.4%, either fully or partially.
Of those, 39.8% were designated as “complex,” and 81.5% of these complex FOIA requests were granted in 61 days or more. Considering these historical statistics, a backlog of 400 FOIA requests doesn’t appear excessively burdensome.
FDA’s Foot-Dragging Is Suspicious
Then there’s the sticky issue that it has already proven its capacity for rapid review. Aaron Siri of the law firm Siri & Glimstad wrote in the PHMPT’s court filing:5,6,7,8
“This 108-day period is the same amount of time it took the FDA to review the responsive documents for the far more intricate task of licensing Pfizer’s COVID-19 vaccine …
It took the FDA precisely 108 days from when Pfizer started producing the records for licensure to when the FDA licensed the Pfizer vaccine. Taking the FDA at its word, it conducted an intense, robust, thorough, and complete review and analysis of those documents in order to assure that the Pfizer vaccine was safe and effective for licensure.
While it can conduct that intense review of Pfizer’s documents in 108 days, it now asks for over 20,000 days to make these documents available to the public …
The entire purpose of the FOIA is to assure government transparency. It is difficult to imagine a greater need for transparency than immediate disclosure of the documents relied upon by the FDA to license a product that is now being mandated to over 100 million Americans under penalty of losing their careers, their income, their military service status, and far worse.”
Shocking Revelations in First Batch of FOIA Docs
Two months after the lawsuit against it was filed, the FDA released a batch of 91 pages,9 and if this batch is any indication, it’s not surprising that the FDA wants to slow-walk the release of the rest. In a November 21, 2021, substack article, Kyle Becker cites directly from the released documents:10
“’It is estimated that approximately [REDACTED] doses of BNT162b2 were shipped worldwide from the receipt of the first temporary authorization for emergency supply on 01 December 2020 through 28 February 2021,’ the document states. ‘Cumulatively, through 28 February 2021, there was a total of 42,086 case reports (25,379 medically confirmed and 16,707 non-medically confirmed) containing 158,893 events …
Most cases (34,762) were received from United States (13,739), United Kingdom (13,404) Italy (2,578), Germany (1913), France (1506), Portugal (866).’ Below is a General Overview of the reported outcomes to the Adverse Events:

The chart lists 1,223 fatal outcomes in the Relevant Cases. Interestingly, the age range with the most relevant cases was 31-50 years old, which is not the age group considered to be at high risk from COVID-19.”
It’s worth noting that by redacting the specified number of doses shipped, it becomes more difficult to assess the potential ratio of injury. Still, even without that, 42,086 reports of injury, including 1,223 fatalities, are a significant signal in and of itself, especially when you consider that the 1976 swine flu vaccine was pulled after 25 deaths.
Glaring Disregard for Life
It’s even more disturbing when you consider that those 42,086 reports were received by Pfizer in just the first 2.5 months of the shot being rolled out. Pfizer even acknowledges the abnormal rate of injuries, but then sweeps it aside as being of no consequence. As noted by Siri, in a November 19, 2021 substack article, in which he discusses this first batch of documents:11
“Pfizer explains, on page 6, that ‘Due to the large numbers of spontaneous adverse event reports received for the product, [Pfizer] has prioritized the processing of serious cases…’
Pfizer ‘has also taken a [sic] multiple actions to help alleviate the large increase of adverse event reports’ including ‘increasing the number of data entry and case processing colleagues’ and ‘has onboarded approximately [REDACTED] additional fulltime employees (FTEs).’
Query why it is proprietary to share how many people Pfizer had to hire to track all of the adverse events being reported shortly after launching its product …
But no cause for alarm since Pfizer explains to the FDA: ‘The findings of these signal detection analyses are consistent with the known safety profile of the vaccine.’ So, if they knew these issues were going to arise, then why didn’t they appear to have enough staff to process this expected volume of reports?
The grand conclusion by Pfizer to the FDA: ‘The data do not reveal any novel safety concerns or risks requiring label changes and support a favorable benefit risk profile of to the BNT162b2 vaccine.’ Nothing to see here.”
Clearly, there’s plenty to be seen in the hundreds of thousands of documents Pfizer/BioNTech submitted to the FDA. The fact that the FDA is stonewalling and wants 55 years to redact them before they’re fit for public view is telling in and of itself.
You don’t need a fanciful imagination to comprehend what they might be hiding. It almost seems they want to make sure the responsible parties are all dead by the time the full data set is out in the open and people can be held to account for their decisions. Let’s hope the judge is more interested in public health than protecting the FDA’s dirty secrets.
Sources and References
- 1 ZeroHedge November 23, 2021
- 2, 7 Daily Mail November 19, 2021, Updated November 20, 2021
- 3, 4 The Defender November 19, 2021
- 5 US District Court Northern District of Texas Case 4:21-cv-01058-P
- 6 US District Court Northern District of Texas Case 4:21-cv-01058-P Second Joint Report
- 8 The Vaccine Reaction November 21, 2021
- 9 PHMPT.org Pfizer documents
- 10 thekylebecker.substack.com November 21, 2021
- 11 aaronsiri.substack.com November 19, 2021
Featured Video
NO DUST NO DEAL, Seems Like We’re Closer to Hot War w/Iran
or go to
Aletho News Archives – Video-Images
Villains of Judea
Abe Foxman
Foxman left a legacy of surveillance scandals, political vendettas, and selective outrage.

José Niño Unfiltered | May 24, 2026
When Abraham Foxman died on May 10, 2026, tributes poured in from presidents, prime ministers, and Jewish leaders worldwide, yet his legacy remains defined as much by controversy as by accomplishment.
Foxman described himself as “a passionate supporter of the State of Israel” and spent his career building the ADL into a roughly $60 million per year organization that defined mainstream American Jewish advocacy on antisemitism, civil rights, and the Jewish state. … continue
Blog Roll
 Aletho News
Aletho News- Col Doug Macgregor NO DUST NO DEAL, Seems Like We’re Closer to Hot War w/Iran
- Meet the Convicted Jewish Felon Who Scammed Floyd Mayweather
- Ex-Mossad chief threatened ICC prosecutor over Israel war crimes probe
- Trump advances his Arctic strategy
- Senior MP reveals Russia’s strategy for strikes on Kiev
- Germany Embarked on Unprecedented Military Buildup – Expert
- Moscow demands release of Russian Orthodox bishop detained by NATO state
- When Our Word is No Longer Good
- ‘Unacceptable’: Islamabad won’t normalize with Israel, defense minister says despite Trump’s push
- The Disasters of War. Trump’s “Peace Through Strength” Doctrine Conducive to Worldwide Famines…
- If Americans Knew
- Netanyahu Stresses The Need For More Propaganda As Israel’s Hasbara Budget Soars
- As Israel Heads to Elections, Netanyahu Needs War
- Conflict escalations everywhere: Gaza, Lebanon, Iran – Daily Update
- How AIPAC channels millions through shell PACs ahead of US midterms
- Israel has no mercy on Gaza, Lebanon; Trump throws a curveball into Iran negotiations – Daily Update
- Israel escalates attacks in Gaza, as it demands total disarmament – Daily Update
- Flotilla activists’ allegations of rape, sexual assault multiply – Daily Update
- Israel’s long record of using banned incendiary weapons on civilians
- How Jeffrey Goldberg weaponized Jewish trauma to pave the way for war with Iran
- ISRAELI MEDIA: They Were Children During the Nakba. This Is What They Remember 78 Years Later
- No Tricks Zone
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
- Germany’s AfD Party Calls Debunked Climate Scenarios “Greatest Fraud In Human History”
- Researchers Find Rapid Global Warming Phase At End Of Last Ice Age (Ca.18,000 Years Ago)
- Even The DNA Of Single-Celled Plankton Can Upend Alarmist Arctic Sea Ice Melt Claims
- Scandal: Although Climate Panic Is Canceled By IPCC, Europe’s Policymakers Continue With Their Crushing Policies
- How Once Hardcore Climate Alarmist Lucy Biggers Realized It Was All A Scam, Brainwashing
- German Expert: “No Climate Crisis” …”Warming Generally Better For Humanity”
- New Paleo Research: Modern ‘Climate Change’ Has Had No Apparent Impact On Precipitation Patterns
- 90% Subsidized… Bielefeld Germany’s €7 Million Hydrogen Garbage Truck Fleet Sits Idle
