Fauci and the Great AIDS Swindle
A Partial Review of Robert F. Kennedy, Jr., THE REAL ANTHONY FAUCI

BY LAURENT GUYÉNOT • UNZ REVIEW • NOVEMBER 27, 2021
Robert F. Kennedy, Jr.’s new book, The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health is not the book of a politician seeking attention. It is the book of a man determined to stake his own life in the resistance against the unfolding bio-terrorist assault on humankind by governments captive of the pharmaceutical industry. He is calling for mass insurrection, and his last word is: “I’ll see you on the barricades.” The book begins like this:
I wrote this book to help Americans—and citizens across the globe—understand the historical underpinnings of the bewildering cataclysm that began in 2020. In that single annus horribilis, liberal democracy effectively collapsed worldwide. The very governmental health regulators, social media eminences, and media companies that idealistic populations relied upon as champions of freedom, health, democracy, civil rights, and evidence-based public policy seemed to collectively pivot in a lockstep assault against free speech and personal freedoms. Suddenly, those trusted institutions seemed to be acting in concert to generate fear, promote obedience, discourage critical thinking, and herd seven billion people to march to a single tune, culminating in mass public health experiments with a novel, shoddily tested and improperly licensed technology so risky that manufacturers refused to produce it unless every government on Earth shielded them from liability. … Conscientious objectors who resisted these unwanted, experimental, zero-liability medical interventions faced orchestrated gaslighting, marginalization, and scapegoating. American lives and livelihoods were shattered by a bewildering array of draconian diktats imposed without legislative approval or judicial review, risk assessment, or scientific citation. So-called Emergency Orders closed our businesses, schools and churches, made unprecedented intrusions into privacy, and disrupted our most treasured social and family relationships.
 Kennedy is not a newcomer to this frightening dystopia. “My 40-year career as an environmental and public health advocate,” he writes, “gave me a unique understanding of the corrupting mechanisms of ‘regulatory capture,’ the process by which the regulator becomes beholden to the industry it’s meant to regulate.” From the time he entered the vaccine debate in 2005, he realized that “the pervasive web of deep financial entanglements between Pharma and the government health agencies had put regulatory capture on steroids.” The Centers for Disease Control and Prevention (CDC), for example, owns 57 vaccine patents and spent $4.9 billion in 2019 buying and distributing vaccines. The Food and Drug Administration (FDA) receives 45 percent of its budget from the pharmaceutical industry. The National Institutes of Health (NIH), with its $42 billion budget, owns hundreds of vaccine patents and often profits from the sale of products it supposedly regulates. High-level officials receive yearly emoluments of up to $150,000 in royalty payments on products that they help develop and then usher through the approval process.
Kennedy is not a newcomer to this frightening dystopia. “My 40-year career as an environmental and public health advocate,” he writes, “gave me a unique understanding of the corrupting mechanisms of ‘regulatory capture,’ the process by which the regulator becomes beholden to the industry it’s meant to regulate.” From the time he entered the vaccine debate in 2005, he realized that “the pervasive web of deep financial entanglements between Pharma and the government health agencies had put regulatory capture on steroids.” The Centers for Disease Control and Prevention (CDC), for example, owns 57 vaccine patents and spent $4.9 billion in 2019 buying and distributing vaccines. The Food and Drug Administration (FDA) receives 45 percent of its budget from the pharmaceutical industry. The National Institutes of Health (NIH), with its $42 billion budget, owns hundreds of vaccine patents and often profits from the sale of products it supposedly regulates. High-level officials receive yearly emoluments of up to $150,000 in royalty payments on products that they help develop and then usher through the approval process.
Dr. Anthony Fauci, “America’s reigning health commissar,” stands at the summit of that Leviathan. From 1968, he occupied various posts at the National Institute of Allergy and Infectious Diseases (NIAID), a sub-agency of NIH, of which he became director in 1984. With a $417,608 annual salary, he is the highest paid of all federal employees, including the President. “His experiences surviving 50 years as the panjandrum of a key federal bureaucracy, having advised six Presidents, the Pentagon, intelligence agencies, foreign governments, and the WHO, seasoned him exquisitely for a crisis that would allow him to wield power enjoyed by few rulers and no doctor in history.” He has nurtured a complex web of financial entanglements that has transformed the NIH into a subsidiary of Big Pharma. Reaching into the deep pockets of the Clinton and Gates Foundations, he has used his $6 billion annual budget to achieve dominance and control over many agencies, including the World Health Organization (WHO). He can make and break careers, enrich or punish university research centers, and dictate the outcome of scientific research across the globe, consistently prioritizing pharmaceutical industry profits over public health.
Kennedy’s book documents Fauci’s “two-decade strategy of promoting false pandemics as a scheme for promoting novel vaccines,” as well as “his actions to conceal widespread contamination in blood and vaccines, his destructive vendettas against scientists who challenge the Pharma paradigm, [and] his deliberate sabotaging of patent-expired remedies against infectious diseases.”
But of course, Kennedy’s book is not about a man: it is about an irremediably corrupt and predatory system created in the U.S. and exported worldwide. Ultimately, however, the system is built and run by humans, and focusing on its most emblematic representative shows its very soul.
Kennedy’s book puts the current crisis in historical perspective. But it doesn’t tell the story chronologically. It starts with a very long first chapter on the current Covid crisis—a book by itself—, then goes back, from chapter 3, to the 1980s and the search for the AIDS vaccine, the template for today’s pharmaceutical coup. In this review, I will focus on the AIDS episode, because it is the least familiar part of a history covering fifty years, and it helps make sense of what is happening today. It is an incredible story, that I would have had difficulty believing just three years ago, but that our current enslavement now makes utterly credible.
The thirty-year decampment of journalistic scrutiny means that there is still no coherent public narrative chronicling Dr. Fauci’s futile quest for his “inevitable” AIDS vaccine, much less accountability. Industry and government scientists have instead shrouded the scandalous saga in secrecy, subterfuge, and prevarication, obscuring a thousand calamities and a sea of tears deserving its own book. Every meager effort to research the debacle—on Google, PubMed, news sites, and published clinical trial data—yields only shocking new atrocities—a grim, repetitive parade of horribles: heartbreaking tragedies, entrenched institutional arrogance and racism, broken promises, vast expenditures of squandered treasure, and the recurring chicanery of Anthony Fauci, Bob Gallo, and Bill Gates.
Kennedy deserves praise and gratitude for his courage to bring this controversy out into the open, in a clear and well-documented exposé. His book is destined to become a landmark in the struggle for Life and Truth—and in the Kennedy heroic saga. This article reflects only a fraction of what can be learned from its 480 pages packed with data and references. Since page numbers in the kindle edition (recommended for its thousand hyperlinks) differ from those in the printing book, I have dispensed with them.
In the Beginning
In the first lines of his 2014 book Thimerosal: Let the Science Speak (documenting an astonishing 1,135 percent higher rate of autism among children who took hepatitis B vaccines), Kennedy prudently claimed to be “pro-vaccine” and to “believe that vaccines have saves the lives of hundreds of millions of humans over the past century.” Kennedy makes no such disclaimer in his new book. Rather, he sides with the critics of the popular dogma that vaccines played the key role in abolishing mortal contagious illnesses in North America and Europe, citing a 2000 study by CDC and Johns Hopkins scientists that concluded: “nearly 90 percent of the decline in infectious disease mortality among US children occurred before 1940, when few antibiotics or vaccines were available.” The main causes of the dramatic 74 percent decline in infectious disease mortality in the first half of the twentieth century were improved nutrition and sanitation.

From Kennedy, The Real Anthony Fauci, 2021
This revisionist but objective perspective explains why Fauci and Gates’s obsession with vaccine-preventable diseases has caused negative overall impacts on public health in Africa and Asia, by proportionally reducing assistance streams for nutrition, clean water, transportation, hygiene, and economic development. Gates and Fauci have actually hijacked WHO’s public health agenda away from the projects that are proven to curb infectious diseases, and diverted international aid to wedge open emerging markets for their multinational partners.
To understand their craze for vaccines, Kennedy reminds us of the pioneering influence of the Rockefeller Foundation. In 1911, after the Supreme Court ruled that Standard Oil constituted an “unreasonable monopoly” and splintered it into thirty-four companies, John D. Rockefeller inaugurated what Bill Gates would later call “philanthrocapitalism.” He provided large grants to scientists for synthesizing and patenting chemical versions of the molecules identified in traditional medicine. The Foundation provided almost half of the initial budget for the League of Nations’ Health Organization (LNHO) in 1922, and populated its ranks with its veterans and favorites. It imbued the League with its technocratic philosophy of health, inherited by its successor body, the WHO, in 1948.
The Rockefeller Foundation launched a “public-private partnership” with pharmaceutical companies called the International Health Commission, which first set about inoculating the hapless populations of the colonized tropics with a yellow fever jab. By the time John D. Rockefeller, Jr. disbanded it in 1951, the International Health Commission had spent billions of dollars on tropical disease campaigns in almost 100 countries and colonies. These projects had a hidden agenda, according to a 2017 report, U.S. Philanthrocapitalism and the Global Health Agenda: they allowed the Rockefeller family to open developing world markets for oil, mining, banking and other profitable trades, including pharmaceutical profits that grew tremendously when, in the 1970s:
a wave of new technologies, including PCR and super powerful electron microscopes, had opened windows on teeming new worlds containing millions of species of previously unknown viruses to scientists. … The lure of fame and fortune ignited a chaotic revolution in virology as ambitious young PhDs scrambled to inculpate newly discovered microbes as the cause of old malignancies. … Under this new rubric, every theoretical breakthrough, every find, became potentially the basis for a new generation of drugs.
By the mid-1970s, the CDC was seeking to justify its existence by tracking small outbreaks of rabies. “Drumming up public fear of periodic pandemics was a natural way for NIAID and CDC bureaucrats to keep their agencies relevant. Dr. Fauci’s immediate boss and predecessor as NIAID Director, Richard M. Krause, helped pioneer this new strategy in 1976.” That year the fake swine flu epidemic was concocted. The experimental vaccine was so fraught with problems that the Health and Human Services (HHS) discontinued the jab after vaccinating 49 million Americans. According to news accounts, the incidence of flu was seven times greater among the vaccinated than the unvaccinated. Furthermore, the vaccine caused some 500 cases of the degenerative nerve disease Guillain-Barré Syndrome, 32 deaths, more than 400 paralyzations, and as many as 4,000 other injuries. Injured plaintiffs filed 1,604 lawsuits. By April 1985, the government had paid out $83,233,714 and spent tens of millions of dollars adjudicating and processing those claims.
Another scandal broke in 1983, when a NIH-funded UCLA study found that the DTP vaccine developed by Wyeth—now Pfizer—was killing or causing severe brain injury, including seizures and death, in one in every 300 vaccinated children. While protecting children against diphtheria, tetanus, and pertussis, the DTP vaccine had ruined their immune systems, making them vulnerable to a wide range of other deadly infections.
The resultant lawsuits caused the collapse of insurance markets for vaccines and threatened to bankrupt the industry. Wyeth claimed to be losing $20 in downstream liability for every dollar it earned on vaccine sales, and induced Congress to pass in 1986 the National Childhood Vaccine Injury Act, which shielded vaccine makers from liability. (This incentive for unrestricted greed was strengthened in 2005 when George W. Bush signed into law the Public Readiness and Emergency Preparedness Act).
AIDS and AZT
In 1984, when Fauci became director of NIAID, the AIDS crisis was spiraling out of control. That proved “a redemptive juncture for NIAID and the launch pad for Dr. Fauci’s stellar rise.” In an April 1984 press conference, NIH scientist Robert Gallo linked AIDS to the virus that was soon to be named HIV. Dr. Fauci then moved aggressively to claim jurisdiction for his agency over the National Cancer Institute (NCI), another sub-agency of NIH. “As the nation’s newly appointed AIDS czar, Dr. Fauci was now a gatekeeper for almost all AIDS research … parroting NCI’s vows to cure cancer, Dr. Fauci promised Congress that he would quickly produce drugs and vaccines to banish AIDS.”
At the same time, he was deliberately spreading contagion terror, warning in a 1983 fear-mongering article that “the scope of the syndrome may be enormous”, since “routine close contact, as within a family household, can spread the disease”—despite the fact that AIDS was almost exclusive to intravenous drug users and male homosexuals. A year later, Fauci was forced to concede that health officials had never detected a case of the disease spread through “casual contact.” Nevertheless, Dr. Fauci’s systematic response was “to amplify the widespread panic of dreaded pestilence that would naturally magnify his power, elevate his profile, and expand his influence. Amplifying terror of infectious disease was already an ingrained knee-jerk institutional response at NIAID.”
Having seized control over AIDS research, Fauci captured the new flood of congressional AIDS appropriations flowing to NIH through the lobbying of a newly organized gay community. By 1990, NIAID’s annual AIDS budget reached $3 billion. In the ensuing decades, the federal government spent over half a trillion dollars in the quest for an elusive vaccine that never materialized. Dr. Fauci pumped up taxpayers’ money into nearly 100 vaccine candidates, with no other result than “massive transfers of public lucre to Dr. Fauci’s Pharma partners,” and a sea of tears for millions of unfortunate human guinea pigs.
NIAID’s lack of in-house drug development capacity meant that Fauci had to farm out drug research to a network of so-called “principal investigators” (PIs), academic physicians and researchers controlled by pharmaceutical companies and acting as liaisons, recruiters and spokespersons.
PIs are pharmaceutical industry surrogates who play key roles promoting the pharmaceutical paradigm and functioning as high priests of all its orthodoxies, which they proselytize with missionary zeal. They use their seats on medical boards and chairmanships of university departments to propagate dogma and root out heresy. … They are the credentialed and trusted medical experts who prognosticate on television networks—now helplessly reliant on pharmaceutical ad revenue—to push out Pharma content.
Dr. Fauci’s choice to transfer virtually all of NIAID’s budget to pharmaceutical PIs for drug development was an abdication of the agency’s duty to find the source and eliminate the explosive epidemics of allergic and autoimmune disease that began under his watch around 1989. … NIAID money effectively became a giant subsidy to the blossoming pharmaceutical industry to incubate a pipeline of profitable new drugs targeted to treat the symptoms of those very diseases.
In the late 80s and early 90s, PIs received every year between 4 and 5 billions of dollars from NIH’s budget. But “legalized bribes” from drug companies and royalty payments from drug products often dwarfed their government funding. Celia Farber’s 2006 Harper’s article, “Out of Control: AIDS and the Destruction of Medical Science,” laid bare the culture of squalor, corruption, and vendetta at Fauci’s AIDS Branch, the Division of Acquired Immunodeficiency Syndrome (DAIDS).
Despite his miserable track record at reducing illness over the previous decade, Fauci persuaded President Bill Clinton, in May 1997, to set a new national goal for science. In a speech delivered at Morgan State University, Clinton—perhaps not without cryptic irony— imitated Kennedy’s May 25, 1961 moonshot promise, saying, “Today let us commit ourselves to developing an AIDS vaccine within the next decade.”
A year later, Bill Gates, who had just founded his International Aids Vaccine Initiative (IAVI), sealed a deal with Fauci. “Over the next two decades, that partnership would metastasize to include pharmaceutical companies, military and intelligence planners, and international health agencies all collaborating to promote weaponized pandemics and vaccines and a new brand of corporate imperialism rooted in the ideology of biosecurity.” The story of Gates’ involvement in the vaccine business, of his murderous experiments in Africa and India, and of his rise as the unofficial top sponsor of the WHO (ordering in 2011: “All 193 member states, you must make vaccines a central focus of your health systems”), is told in chapters 9 and 10 of Kennedy’s book.
When Dr. Fauci became head of NIAID, azidothymidine, known as AZT, was the only candidate as an AIDS remedy. AZT is a “DNA chain terminator,” randomly destroying DNA synthesis in reproducing cells. It had been developed in 1964 for cancer, but abandoned as too toxic even for short-term therapy. It was deemed so worthless that it was not even patented. In 1985, Samuel Broder, head of the National Cancer Institute (NCI), claimed having found that AZT killed HIV in test tubes. The British company Burroughs Wellcome then patented it as an AIDS remedy. “Recognizing financial opportunity in the desperate terror of young AIDS patients facing certain death, the drug company set the price at up to $10,000/year per patient—making AZT one of the most expensive drugs in pharmaceutical history. Since Burroughs Wellcome could manufacture AZT for pennies per dose, the company anticipated a bonanza.”
Fauci gave Burroughs Wellcome a monopoly control over the government’s HIV response. But all did not go smoothly. “AZT’s horrendous toxicity hobbled researchers struggling to design study protocols that would make it appear either safe or effective.” Another problem is that community-based doctors were achieving promising results with cheap, off-label therapeutic drugs. Dr. Fauci refused to test any of those repurposed drugs that had no Pharma patrons. When he did put on trial AL721, an antiviral that was far less toxic than AZT, he rigged the studies to fail, and abruptly cancelled Phase 2.
Meanwhile, he accelerated testing of AZT, skipping animal testing and allowing Burroughs Wellcome to proceed directly to human trials. In March 1987, Fauci’s team declared the human trials a success after only four months, and Fauci congratulated himself in front of the press. However, when in July 1987, the official report of Burroughs Wellcome’s Phase 2 trial was published, European scientists complained that raw data showed no benefit in reducing symptoms. FDA conducted its own investigation eighteen months later, but kept its results secret, until investigative journalist John Lauritsen obtained some of them by using the Freedom of Information Act; the documents showed that the Fauci/Burroughs Wellcome research teams had engaged in widespread data tampering. More than half of the AZT patients suffered adverse reactions so deadly that they needed multiple blood transfusions just to keep them alive. Nevertheless, Fauci kept on lying himself to the top of the world, with little scrutiny from mainstream media.
A key and enduring legacy of the AZT battle was Dr. Fauci’s emergence as the alpha wolf of HHS [Health and Human Services]. His enormous budget, and multiplying contacts on Capitol Hill, the White House, and the medical industry, thereafter allowed him to influence or ignore a succession of politically appointed HHS directors and to bully, manipulate, and dominate HHS’s other sister agencies, most notably FDA.
AZT was not the only subject of interest to Fauci. By June 2003, NIH was running 10,906 clinical trials on new antiviral concoctions in some four hundred clinical trials in ninety countries. Some of those trials seemed pulled out of Dickens’ worst nightmares. The Alliance for Human Research Protection (AHRP), a medical industry watchdog organization, has documented that between 1985 and 2005, NIAID conscripted at least 532 infants and children from foster care in New York City as subjects of clinical trials testing experimental AIDS drugs and vaccines. AHRP’s investigation revealed that many of those children were perfectly healthy and may not even have been HIV-infected. Yet 80 of them died. In 2004, journalist Liam Scheff chronicled Dr. Fauci’s secretive experiments on foster children at Incarnation Children’s Center (ICC) in New York City and numerous sister facilities between 1988 and 2002. These disclosures, comments Kennedy, beg many questions:
From what moral wilderness did the monsters who devised and condoned these experiments descend upon our idealistic country? How have they lately come to exercise such tyrannical power over our citizens? What sort of nation are we if we allow them to continue? Most trenchantly, does it not make sense that the malevolent minds, the elastic ethics, the appalling judgment, the arrogance, and savagery that sanctioned the barbaric brutalization of children at the Incarceration Convent House, and the torture of animals for industry profit, could also concoct a moral justification for suppressing lifesaving remedies and prolonging a deadly epidemic? Could these same dark alchemists justify a strategy of prioritizing their $48 billion vaccine project ahead of public health and human life? Did similar hubris—that deadly human impulse to play God—pave the lethal path to Wuhan and fuel the reckless decision to hack the codes of Creation and fabricate diabolical new forms of life—pandemic superbugs—in a ramshackle laboratory with scientists linked to the Chinese military?
Indeed, Kennedy shows in his final chapter, “Germ Games,” that Fauci’s investments in so-called “gain of function” experiments to engineer pandemic superbugs raise “the ironic possibility that Dr. Fauci may have played a role in triggering the global contagion that two US presidents entrusted him to manage.”
Africa is “the venue of choice for companies seeking cooperative government officials, compliant populations, the lowest per-patient enrollment costs, and lax oversight by media and regulatory officials.” In the early 1990s, African dictators rolled out the red carpet for Pharma, cashing in on the lucrative business of farming out their citizens for the booming clinical trial business. And on January 29, 2003, President George W. Bush announced at his State of the Union speech his Emergency Plan for AIDS Relief (PEPFAR), Fauci’s new swindle:
On the continent of Africa, nearly 30 million people have the AIDS virus. … Yet across that continent, only 50,000 AIDS victims—only 50,000—are receiving the medicine they need. … I ask the Congress to commit $15 billion over the next five years, including nearly $10 billion in new money, to turn the tide against AIDS in the most afflicted nations of Africa and the Caribbean.
Does HIV Cause AIDS?
Kennedy’s chapter 5, “The HIV Heresies,” opens up with the following note:
I hesitated to include this chapter because any questioning of the orthodoxy that HIV is the sole cause of AIDS remains an unforgivable—even dangerous—heresy among our reigning medical cartel and its media allies. But one cannot write a complete book about Tony Fauci without touching on the abiding—and fascinating—scientific controversy over what he characterizes as his “greatest accomplishment” and his “life’s work.”
The controversy illustrates how pharmaceutical industries and health agencies, acting in concert, engineer consensus on incomplete or fraudulent theories, and ruthlessly suppress dissent from even the most gifted recognized scientists. “From the outset,” Kennedy insists, “I want to make clear that I take no position on the relationship between HIV and AIDS.” However, there seems little doubt that his basic point is correct:
During the thirty-six years since Dr. Fauci and his colleague, Dr. Robert Gallo, first claimed that HIV is the sole cause of AIDS, no one has been able to point to a study that demonstrates their hypothesis using accepted scientific proofs. … Even today, incoherence, knowledge gaps, contradictions, and inconsistencies continue to bedevil the official dogma.
The success story of the HIV-AIDS dogma shows “many of the tactics Dr. Fauci has pioneered to dodge debate—bedazzling and bamboozling the press into ignoring legitimate inquiry of the credo, and undermining, gaslighting, punishing, bullying, intimidating, marginalizing, vilifying, and muzzling critics.” One of Fauci’s victims was Dr. Peter Duesberg, who in 1987 was still recognized as the world’s most accomplished retrovirologist. Duesberg argues that HIV does not cause AIDS but is essentially a “free rider” common to high-risk populations who suffer immune suppression due to environmental exposures. HIV, he says, is a harmless passenger virus that has almost certainly coexisted in humans for thousands of generations without causing diseases. While HIV may be sexually transmittable, Duesberg claims, AIDS is not.
Duesberg published his views in a groundbreaking 1987 article, then in a 724-page book, Inventing the AIDS Virus. Kennedy finds that “Duesberg’s rationales appear so clean, so elegantly crafted, and so compelling that, in reading them, it seems impossible that the entire [orthodox] hypothesis did not instantly collapse under the smothering weight of relentless logic.” But Fauci and Gallo never attempted to reply to Duesberg. Blaming AIDS on a virus was the gambit that had allowed NIAID to claim the jurisdiction—and cash flow—away from NCI, and Duesberg was severely punished for endangering this.
Dr. Fauci summoned the entire upper clergy of his HIV orthodoxy—and all of its lower acolytes and altar boys—to unleash a storm of fierce retribution on the Berkeley virologist and his followers. … the AIDS establishment, down to its lowliest doctor, publicly reviled Duesberg, NIH defunded him, and academia ostracized and exiled the brilliant Berkeley professor. The scientific press all but banished him. He became radioactive.
Surprisingly, however, Dr. Luc Montagnier, whose discovery of HIV Gallo had in fact stolen—as he admitted in 1991 after years of litigation—, became Duesberg’s most embarrassing convert, declaring at the San Francisco International AIDS Conference in June 1990, that “the HIV virus is harmless and passive, a benign virus.” He added that, according to his findings, HIV becomes dangerous only in the presence of a second organism, a bacteria-like bug called a mycoplasma. Montagnier, in fact, had never claimed that HIV was the only factor in AIDS, and grew increasingly skeptical of that theory. His repeated questioning of the establishment paradigm signaled the beginning of his vilification, for which his Nobel Prize hardly protected him.
Gallo’s “proof” that the cause of AIDS was a virus—as opposed to toxic exposures— provided the critical foundation stone of Dr. Fauci’s career. It allowed Fauci to capture the AIDS program and launch NIAID as the leading federal partner of the drug-production industry. This explains why Fauci never funded any study to explore whether HIV actually caused AIDS, and took vigorous preemptive action against any such study.
Kennedy cites other dissenting voices on AIDS epidemiology. Dr. Shyh-Ching Lo, the Chief Researcher in charge of AIDS programs for the Armed Forces Institute of Pathology, was shocked by Anthony Fauci’s unconventional claim that antibodies, normally the sign of a robust immune response, should, with HIV, be the signal for impending death. Since “HIV tests” do not in reality detect the elusive virus but only antibodies, there seems to be an Orwellian inversion at work. Kennedy also quotes Dr. David Rasnick, a PhD biochemist who has worked for thirty years in the pharmaceutical biotech field:
Fauci’s fundamental conundrum is that he has told everybody to diagnose AIDS based on the presence of HIV antibodies. With every other disease, the presence of antibodies is the signal that the patient has vanquished the disease. With AIDS, Fauci and Gallo, and now Gates, claim it’s a sign you’re about to die. Think about it; if the objective of an AIDS vaccine is to stimulate antibody production, then success would mean that every vaccinated person would also have an AIDS diagnosis. I mean, this is fodder for a comedy bit. It’s like someone gave the Three Stooges an annual billion-dollar budget!
The nature of AIDS—a syndrome, not a disease—is itself subject to questions, since it was made to encompass a galaxy of some thirty separate well-known diseases, all of which occur in individuals who have no HIV infection. “In the hands of Dr. Fauci’s opportunistic PIs, AIDS became an amorphous malady subject to ever-changing definitions, encompassing a multitude of old diseases in hosts who test positive for HIV.” Nobel Laureate Kary Mullis, the inventor of the PCR tests, pointed out that the PCR was capable of finding HIV signals in large segments of the population who suffered no AIDS symptoms. On the other hand, AIDS commonly occurs in people who test HIV negative, as Geoffrey Cowley documented in a 1992 Newsweek article, followed by Steve Heimoff in the Los Angeles Times.
These very inconsistencies were not a problem for Fauci and his standing army of pharmaceutical mercenaries. Quite the opposite: they opened up Africa’s AIDS bonanza. Researchers funded by Fauci, using PCR tests and murky statistical models, declared that up to 30 million Africans were suffering from AIDS, nearly half the adult population in some nations. While in Western nations, AIDS continued to be a disease of drug addicts and homosexual “poppers” (consumers of the amyl nitrite vasodilator providing relaxation of the anal musculature, packaged into the “popper” container patented by Burroughs Wellcome and advertised in the gay press throughout the AIDS epidemic), mysteriously, in Africa, 59 percent of AIDS cases were women, and 85 percent were heterosexuals.
But in the early 1990s, the character of AIDS changed dramatically with the proliferation of AZT. As they started to give AZT to people who were in fact not even sick but simply positive on the HIV test, AIDS started to look increasingly like AZT poisoning. And the death rate climbed precipitously. According to the Duesbergians, the vast majority of “AIDS deaths” after 1987 were actually caused by AZT. The medication that Dr. Fauci was prescribing to treat AIDS patients actually did what the virus could not: it caused AIDS itself. In 1988, the average survival time for patients taking AZT was four months. In 1997, recognizing the lethal effect of AZT, health officials lowered the dose; the average lifespan of AZT patients then rose to twenty-four months. According to Dr. Claus Köhnlein, a German oncologist, “We virtually killed a whole generation of AIDS patients without even noticing it because the symptoms of the AZT intoxication were almost indistinguishable from AIDS.”
Conclusion
In July 2019, Dr. Fauci made a surprise announcement: he finally had a working HIV vaccine, the potential “nail in the coffin” for the epidemic. He conceded that his new vaccine didn’t prevent transmission of AIDS, but predicted that those who took the jab would find that when they did get AIDS, the symptoms would be much reduced. Kennedy comments:
So confident was Dr. Fauci of the media’s slavish credulity that he assumed, correctly, that he’d never need to answer the many questions raised by this feverish gibberish. That entire odd proposition received zero critical press commentary. His success at slapping lipstick on this donkey and selling it to the world as a Thoroughbred may have emboldened his ruse—a year later—of placing similar cosmetics on the COVID vaccines that, likewise, neither prevent disease nor preclude transmission.
By 2019, the AIDS rope started to wear out. Who still cared about AIDS anyway? The “Covid-19 Pandemic” came as the perfect opportunity for a reset and an update in the pharmaceutical racket. As Winston Churchill reportedly said, “Never let a good crisis go to waste”. With complicit corporate media blacking out the scandalous track record of his white-coat mafia, Fauci emerged, again, as the good doctor, the savior.
“Is it fair to blame Dr. Fauci for a crisis that, of course, has many authors?” asks Kennedy. To some extent, it is.
Under Dr. Fauci’s leadership, the allergic, autoimmune, and chronic illnesses which Congress specifically charged NIAID to investigate and prevent, have mushroomed to afflict 54 percent of children, up from 12.8 percent when he took over NIAID in 1984. Dr. Fauci has offered no explanation as to why allergic diseases like asthma, eczema, food allergies, allergic rhinitis, and anaphylaxis suddenly exploded beginning in 1989, five years after he came to power. On its website, NIAID boasts that autoimmune disease is one of the agency’s top priorities. Some 80 autoimmune diseases, including juvenile diabetes and rheumatoid arthritis, Graves’ disease, and Crohn’s disease, which were practically unknown prior to 1984, suddenly became epidemic under his watch. Autism, which many scientists now consider an autoimmune disease, exploded from between 2/10,000 and 4/10,000 Americans when Tony Fauci joined NIAID, to one in thirty-four today. Neurological diseases like ADD/ADHD, speech and sleep disorders, narcolepsy, facial tics, and Tourette’s syndrome have become commonplace in American children. The human, health, and economic costs of chronic disease dwarf the costs of all infectious diseases in the United States. By this decade’s end, obesity, diabetes, and pre-diabetes are on track to debilitate 85 percent of America’s citizens. America is among the ten most over-weight countries on Earth. The health impacts of these epidemics—which fall mainly on the young—eclipse even the most exaggerated health impacts of COVID-19.
Dr. Fauci has done nothing to advance NIAID’s core obligation of researching the causes of chronic allergic and autoimmune diseases that have mushroomed under his tenure. Instead, Fauci has “reshaped NIAID into the leading incubator for new pharmaceutical products, many of which, ironically, profit from the cascading chronic disease pandemic.” Instead of researching the causes of Americans’ failing health, Dr. Fauci funnels the bulk of his $6 billion budget to the research and development of new drugs and vaccines that are largely responsible for weakening our natural immunity. “Of late, he has played a central role in undermining public health and subverting democracy and constitutional governance around the globe and in transitioning our civil governance toward medical totalitarianism.”
I was reminded of Dr. Knock, the central character of Jules Romains’s famous novel Knock or the Triumph of Medicine, written in 1923. Dr. Knock is a shady medical doctor of dubious competence who professes that “health” is an obsolete and unscientific concept, and that all men are sick and need to be informed about it by their doctor. To advance his plan of converting a whole town into permanent patients, he enlists the help of the school teacher and of the pharmacist, who suddenly sees his clientele booming (watch unforgettable moments of Guy Lefranc’s 1951 film adaptation with Louis Jouvet here and here).

Louis Jouvet as Dr. Knock in 1951
To some extent, however, Fauci is himself the product of a civilizational orientation that could only, in the long run, lead to the tyrannical medical technocracy that is now trying to enslave us. Rather than a new Dr. Frankenstein, Fauci is our own monster coming back after us. Kennedy hints at this vast aspect of the question, pointing to the need for deep questioning. The way Americans and Westerners in general have come to view health care has been shaped by the philosophy of the Rockefeller Foundation: “a pill for an ill.” In the debate between the “miasma theory”—that emphasizes preventing disease by fortifying the immune system through nutrition and by reducing exposures to environmental toxins and stresses—versus the “germ theory”—which blames disease on microscopic pathogens—we have unambiguously opted for the latter. We have signed up for an approach to disease that requires to identify the culpable germ and tailor a poison to kill it. The choice was not forced upon us. We have surrendered responsibility for our health to medical experts and insurance brokers.
As Dr. Claus Köhnlein and Torsten Engelbrecht observe in their book Virus Mania (2007) quoted by Kennedy: “The idea that certain microbes—above all fungi, bacteria, and viruses—are our great opponents in battle, causing certain diseases that must be fought with special chemical bombs, has buried itself deep into the collective conscience.” It is a warlike paradigm, perfectly suited for manufacturing consent on the way to dictatorship. As Kennedy wrote in his preface to Dr. Joseph Mercola and Ronni Cummins, The Truth About Covid-19 (2021), “demagogues must weaponize fear to justify their demands for blind obedience.”
Government technocrats, billionaire oligarchs, Big Pharma, Big Data, Big Media, the high-finance robber barons, and the military industrial intelligence apparatus love pandemics for the same reasons they love wars and terrorist attacks. Catastrophic crises create opportunities of convenience to increase both power and wealth.
Laurent Guyénot, PhD, is the author of The Unspoken Kennedy Truth and of a film on the same subject.
This perverse ban on ivermectin, cheap and proven to work
By Kathy Gyngell | TCW Defending Freedom | November 23, 2021
GIVEN the feared winter resurgence of Covid infection despite, or because of, the government’s mass vaccination programme, the continued ban on ivermectin in this country becomes ever more perverse.
It beggars belief that the British public is still denied access to this proven prophylactic and treatment. If the public health authorities are genuinely worried about pressure on hospitals, why have not the Medicines and Health products Regulatory Agency (MHRA), Public Health England, the NHS and Department of Health all gone flat out over this last year to approve ivermectin with the same zeal they gave emergency authorisation to the limited trialled, novel gene therapy, Covid vaccines?
The answer is widespread misinformation from the top down. Put ‘ivermectin’ into the Google search box and what do you come up with? Topping the list is a warning from the US Food and Drug Administration (FDA) why it should NOT be used to treat or prevent Covid-19. Their reason? It’s as simple as the fact that they have not approved it and, because they have not approved, it cannot be used. Trials are ongoing they say. Maybe some are. But plenty have been completed, as Dr Pierre Kory’s paper (he was the lead author) ‘Review of the Emerging Evidence Demonstrating the Efficacy of Ivermectin in the Prophylaxis and Treatment of Covid-19’, published by the American Journal of Therapeutics earlier this year, made quite clear.
By contrast with this detailed review of the evidence the FDA’s substantive concern appears to rest on random reports of harms deriving from self-medication with ivermectin.
The BBC not to be behindhand entered the fray with its customary selective and biased take on ‘the science’. Its recent report entitled ‘How false science created a Covid ‘miracle’ drug‘ made not even the most minimal of checks on the veracity of their assertions, which are pulled apart here. A letter sent to a programme journalist in response to their request for information (in advance of transmission) by Dr Tess Lawrie, the Director of the British Ivermectin Recommendation Development Group (BIRD), an advocacy group of clinicians and scientists from around the world, setting out the science behind the case for authorising it, was completely ignored. Her letter can be found here.
How the BBC came not to ask how it was that remdesivir – a standard medication for Covid in the UK – was approved on the basis of one study when ivermectin, with 63 studies, of them 31 Randomised Controlled Trials (RCT), 7 meta-analyses, 32 Observational Controlled Trials (OCT), multiple country case studies, expert opinion, patient testimony ALL pointing in favour of the medication, was not, is inexplicable.
This is the news source the public is still told to trust.
A blog posted on BIRD last week asked whether there are indeed any genuine gripes about the quality of the evidence, as the FDA and others suggest?
No, there are not. The author argues it is down to a misinformation campaign based on misleading information produced by high profile public health agencies, like the World Health Organisation, itself a victim of disinformation tactics, that has been ‘perpetrated by a minority of corporations to manipulate and delay government action on matters that would adversely affect their income and profit’. Speculation of course. But every indication points that way.
As reported extensively in TCW Defending Freedom, for example here, the WHO is subject to the huge financial influence of the Bill and Melinda Gates Foundation, the organisation’s second biggest donor. Since one of the BMGF’s long-term interest is in delivering vaccines, why would they show any interest in promoting the use of cheap, old repurposed medications in the treatment and prevention of Covid-19? It’s for the very same reason that ivermectin has proved of so little interest to Big Pharma -it’s hardly the money spinner that indemnified world-wide vaccination is.
Worse perhaps than what these big interests have not done is what they have actively done to discredit ivermectin. The BIRD blog relays an analysis by Dr Kory setting out what the WHO ‘did’ with the ivermectin evidence. He says it:
· Failed to publish a pre-established protocol for data exclusion
· Excluded two ‘quasi-randomised’ controlled trials (RCTs) with lower mortality
· Excluded two RCTs that compared ivermectin to or gave it together with other medications, all reporting lower mortality
· Excluded seven other available ivermectin RCT results
· Excluded all RCTs and observational controlled trials (OCTs) investigating ivermectin in the prevention of Covid-19
· Excluded 13 OCTs, more than 5,500 patients, that showed reductions in mortality
· Excluded numerous published and pre-print epidemiologic studies.
The bottom line, however, remains – if ivermectin is good enough and provenly effective for the more than 20 lower-income countries which do distribute it and also benefit from lower Covid rates, why are the populations of wealthier nations and individuals still being denied?
It’s a point that clearly has bothered the chairman of the Tokyo Medical Association, Dr Haruo Ozaki, who would recommend ivermectin for Covid patients, noting that the parts of Africa that use ivermectin to control parasites have a Covid death rate of just 2.2 per 100,000 population, compared with 13 times that death rate among African countries that do not use ivermectin.
‘I would like,’ said Dr Ozaki, ‘the government to consider treatment at the level of the family doctor’ with the informed consent of the patient. So would we.
New VAERS analysis reveals hundreds of serious adverse events that the CDC and FDA never told us about
Serious adverse events that are more elevated than myocarditis. New VAERS analysis by Albert Benavides blows the “safe and effective” narrative away.
By Steve Kirsch | November 9, 2021
The CDC and FDA have said the vaccines are “safe and effective.” They haven’t found any serious issues with the COVID vaccines. Zero. Zip. Nada. It was the DoD that found myocarditis.
The evidence in plain sight shows that they are either lying or incompetent. Or both. But of course, the medical community is never going to call them on this.
So that’s where our team of vaccine safety experts comes in; to reveal the truth about what is really going on.
In a brand new VAERS data analysis performed by our friend Albert Benavides (aka WelcomeTheEagle88), we found hundreds of serious adverse events that were completely missed by the CDC that should have been mentioned in the informed consent document that are given to patients. And we found over 200 symptoms that occur at a higher relative rate than myocarditis (relative to all previous vaccines over the last 5 years). All together, there were over 4,000 VAERS adverse event codes that were elevated by these vaccines by a factor of 10 or more over baseline that the CDC should have warned people about.
As of November 1, 2021, there have been more adverse events reported for the COVID vaccines than for all 70+ vaccines combined since they started tracking adverse events 30 years ago. That’s a stunning statistic, nobody can deny it, but nobody in the mainstream medical community (or mainstream media) seems to care much. It’s not even worth noting in passing. Wow.
Here’s what the evidence shows:
- The COVID vaccines are the most dangerous vaccines in human history. They are 800 times more deadly than the smallpox vaccine which was the previous record holder. The vaccines have killed over 150,000 Americans and permanently disabled even more. They don’t make sense for anyone of any age. The younger you are, the worse it gets. For kids, it is estimated that we kill 117 kids for every COVID death we prevent.
- The Pfizer 6 month trial showed the drug can save 1 life for every 22,000 people vaccinated. It also appeared from the trial that the drug killed more people than it saved (there were 20 deaths in the treatment group vs. 14 in placebo after unblinding). So we are “saving” fewer than 10,000 lives at the expense of over 150,000 deaths. In short, we kill 15 people to save 1. That’s incredibly stupid. But nobody in the Biden administration wants to meet with our team. They basically don’t want to hear the truth. Instead, they focus on deplatforming and censoring us which are techniques that are effective when the data doesn’t work out for you.
- Both the FDA and CDC have proven inept in spotting safety signals. They can’t even compute the VAERS URF which is a number that is required for any serious risk-benefit analysis. So the FDA and CDC outside committee members are all flying blind in approving the vaccines. Even after this deficiency is pointed out in the public comments by yours truly (and direct emails to the committee members), it makes no difference. We are ignored. The CDC safety monitoring is so bad that they even admitted at the last ACIP meeting that it was the DoD that spotted the myocarditis signal. So the FDA and CDC have basically been batting .000 in terms of spotting safety signals that have been sitting in plain sight the entire time.
- They can’t admit that they missed the signals now because that would be an admission they missed them before. So they will try to discredit this article with ad hominem attacks (this is a technique used to win an argument when you cannot win on the evidence).
- The serious events we highlight below are all consistent with the mechanism of action that Robert Malone and I first described in the Darkhorse podcast. Namely, that the spike protein that is produced in response to the delivery of the mRNA is cytotoxic and results in blood clots, inflammation and scarring throughout your body which then creates a wider range of severe adverse events than any vaccine in human history.
- The medical community is trained by the CDC to believe the vaccines are safe, so they interpret all the adverse events as not vaccine related. But if it wasn’t the vaccine that caused all these events, what was it? What’s worse is they tell their patients, “this is all in your head” or that “your baby died because you had a genetic defect.”
- In general, patients believe their doctors and never figure out where to get a cytokine panel to discover that they are vaccine injured (go to www.covidlonghaulers.com to get the cytokine panel and IncellDx to get the spike protein assay). So people never learn how to rid their body of the spike protein either (see my article on vaccine treatment for the drugs they use to do this) which is the first step in the road to recovery.
- The high adverse event rates aren’t “excess reporting.” It is due to excess events. For example, one neurologist had 0 cases of vaccine adverse events in her entire career, but this year, she has 2,000. Another physician I know has had 0 events in 29 years in his 700 patients. This year he needs to report 25 events. Physicians themselves have experienced stunningly higher incidence rates of reproductive, neurological, and cardiac events since the vaccines rolled in 2021. We couldn’t find a single cardiologist who actually had fewer cases of myocarditis after the vaccines rolled out as the members of the FDA and CDC claim.
- The serious events are primarily centered around menstruation, blood clots, inflammation and scarring, cardiovascular damage, and neurological damage, just as we predicted in the podcast in June of 2021.
- There are hundreds of serious adverse events that are caused by these vaccines. This of course is shocking to people since the CDC has repeatedly said you can’t ascribe causality to data in VAERS. Not true. The VAERS data analysis (temporal data, the dose dependency, and the elevated reporting rates compared to baseline) provide ample signal to enable us to show causality on all of these events using the five Bradford-Hill criteria applicable to vaccines.
- Nicki Minaj was right to complain about elevated rates of testicular swelling, impotence (erectile dysfunction), and orchitis. Every world authority who opined on the matter belittled her and said she was wrong, but all the symptoms she talked about are strongly elevated as you’ll see from the data below. None of these so-called experts of course ever looks at the data; it’s all based on arguing from their belief system rather than the scientific evidence. And even if those authorities disagreed with the VAERS data, it was irresponsible not to have pointed out the raw data to people and then explain why they totally ignored the elevated signal in the VAERS data. Today, we do science based on our belief system rather than the old-fashioned way of looking at what the data actually says. Our team is old-fashioned.
- There is a pretty good chance that the vaccines don’t really work at all and never did. We know the Pfizer Phase 3 trials were gamed in many ways. There is no doubt that the vaccines elevate antibodies, but it seems that it is quite possible that the immunity they confer is actually the result of killing off (or excluding as in the case of the trials) people with weaker immune systems. The people who are left are thus more resistant to the virus. Mathew Crawford will be coming out shortly with an analysis that makes a compelling case for this novel hypothesis. Subscribe to his substack here.
- It is unlikely that anyone in the world will want to debate us publicly on any of the claims above (or on any of my articles or on any of Mathew’s articles), but if you are a prominent supporter of the false narrative and want a public debate, we are here for you. Our team would be thrilled to accept the challenge as we have no desire to spread misinformation. If we got it wrong, we are happy to correct our mistakes if you can explain to us clearly the mistake we made and the correction you suggest (e.g., the “right” answer). Yet even with multiple million dollar incentives (listed in this article), nobody seems to be interested in showing how we got it wrong. Everyone talks about how bad the vaccine misinformation problem is, but nobody is willing to do anything to show that we got it wrong. For example, I’ve asked any prominent scientist in America who disagrees with my analysis (showing eight different ways to validate that over 150,000 Americans have been killed by the vaccines) to let me see their “correct” analysis showing the “correct” number, but nobody will. They won’t even come on a recorded call to show us how we got it wrong. It’s baffling. They all want to do it in slow motion via documents because that way it’s easier to obfuscate the truth and they can avoid answering questions. The latter is key.
- It’s really easy to tell who is telling you the truth here. John Su is the CDC expert on VAERS. If he’s wrong, the entire narrative falls apart. I personally attacked Dr. Su in a widely read article accusing him of being corrupt. I offered to publish his response in the article. He said nothing. I offered to debate him. No dice. TrialSiteNews tried to interview him. He refused to reply. Seriously? If the CDC gave us 2 hours to ask John Su questions, we would destroy his credibility and the credibility of the CDC. That’s why he’s not talking and that’s why the CDC will never let him talk to anyone on our team. Because we don’t ask softball questions like what John gets at the ACIP meetings. We play hardball.
What we found in the VAERS analysis below can be verified by anyone because it is all publicly accessible. Albert spent only a few hours to produce the tables. So the CDC should have been able to do the same work Albert did.
You can easily verify any entry yourself via manual queries to any VAERS interface (my favorite is MedAlerts, but others such as openvaers and the HHS site give the same results).
Before we get to Albert’s analysis of the VAERS data, let’s do a little background.
The Darkhorse Podcast
On June 10, 2021, my friend Robert Malone and I appeared on Bret Weinstein’s Darkhorse Podcast to tell the world what we had learned about the COVID vaccines. You can watch the 3 hour version here or the condensed 1 hour version here if you haven’t already seen it. I highly recommend the whole thing; I know a lot of people who watched it multiple times and raved about it.
Basically, we said the COVID vaccines were super dangerous, they had killed a lot of people at the time, the Pfizer bio-distribution data that Dr. Byram Bridle obtained from the Japanese government using a FOIA request showed the lipid nanoparticles delivered a very substantial dose of mRNA to female ovaries, and that the spike protein that is subsequently produced causes blood clots, inflammation, and scarring leading to a large number of cardiovascular and neurological symptoms, a number of which would be irreversible. Robert in particular noted that we had no clue about the amount, dose, and duration of the spike protein that is produced (we still don’t) because this testing was never done in animals (they looked only at the distribution of the nanoparticles which is not the same thing). Bret referenced a very long article I had written on May 25, 2021 for TrialSiteNews entitled “Should you get vaccinated?”
For reference, here is the bio-distribution graph that Bret showed in that podcast:

See anything wrong? Note that we deliberately omitted areas of the body where the vaccine was expected to accumulate in order to highlight areas of the body where it wasn’t supposed to go. Naturally, those supporting the mainstream narrative that the vaccines are safe and effective went into overdrive to suppress the episode and discredit what we said. They said we were dishonest not to include everything in the chart. YouTube censored the video after nearly 1M views. Wikipedia accused both of us of spreading misinformation and then blocked me when I tried to point out that the scientific evidence supported what I said. Wikipedia relies on fact checks for science.
We were right about everything we said in the podcast, and now, thanks to the work Albert did, it’s now easier to see we were telling the truth: the top elevated events were neurological, cardiovascular, and related to the female reproductive system, just like we said. I was stunned at the sheer number of menstrual events that made it to the very top of the list. That was a surprise to me.
Openvaers has been highlighting the damaging effects on both male and female reproductive systems for months with a page dedicated to reproductive health, but the medical community, Congress, and mainstream press wasn’t paying any attention at all. These event counts are not normal, but nobody really seems to care. President Biden not only doesn’t care; he wants to force all our kids to be vaccinated with the most dangerous vaccine in human history.

With the new analysis, the counts are much easier to interpret because instead of being just raw counts, they are numbers relative to a baseline rate so we can instantly see what symptoms are “abnormal” meaning 10X or more higher than “expected.” The answer: over 4,000 adverse events.
The X factor analysis (November 7, 2021)
Before I give you the link to the spreadsheet of VAERS symptoms sorted by X factor, you need to know a few things to properly interpret the data.
First, let’s address the myth that is promoted by the FDA that the VAERS database is “over reported.” As we said above, there are more events this year than any previous year, so that’s why the events are up. But there still could be a component of overreporting as well, i.e., that people this year are more likely to make a report on an event compared to last year since everyone is so “highly aware” of the vaccines. Nice theory. No data to back it up. Nobody making that argument has ever included any data to back up their assertion. We call that a hand-waving argument. Doctor surveys we’ve done show that, if anything, they are less likely to report an adverse event this year for a variety of reasons (hospital frowns on it, no time, still too frustrating, too many events to report). The other way we can tell is to look at the rates of events that are not comorbidities or causal. We find that events like Musculoskeletal pain, Screaming, Head banging, Local reaction, Diet refusal, Croup infectious, Hepatitis A, Eyelid oedema, and more occur at pretty much the same rate this year as in previous years.
Now let’s tackle the columns:
Symptom
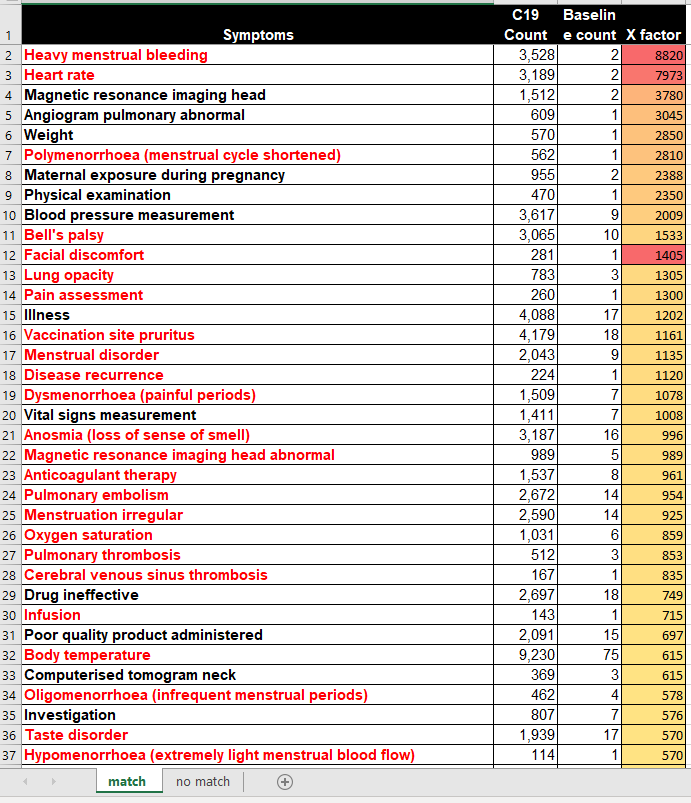
This is the VAERS symptom name. These are coded by HHS upon receipt of the report based on the contents of the report. Some of these symptoms are tests that are ordered. An elevation of a test is a good signal something is amiss. Other symptoms are not causal, but are comorbidities. For example, it might be that diabetes is there more often not because it makes diabetes worse, but because diabetic people are more likely to report symptoms. So for these symptoms, we have to be careful about the analysis. But for many of these symptoms such as cancer, herpes zoster (shingles), diabetes and more, these are all exacerbated by the vaccine as we know from talking directly to doctors. Finally, some symptoms like “rib fracture” or “suicide” are elevated because they are caused by the vaccine. For example, the vaccine can make you lose consciousness and fall and fracture your hip. The vaccine can give you tinnitus which is so bad that you want to kill yourself. So we have to be extremely careful to examine each one of these symptoms carefully because in most cases, we’ll find that they are indeed caused by the vaccine. I’ve coded a bunch of symptoms red that I thought were serious/interesting. I’m not done yet, so the redness coding was only methodically done on the first 100 symptoms and sporadically after that. When I get more time, I’ll go through them and update the file. Note that myocarditis is located on row 274, i.e., way way down.
Also, when looking at deaths, we never look at a “symptom” of death since death is coded in a separate field. So the event count for the “death” symptom (6,487) is lower than the over 8,000 domestic deaths.
Guillain-Barre syndrome is only elevated by a factor of 6 from baseline, likely because other vaccines also elevate GBS; this vaccine elevates it even more.
C19 count
This is the raw number of VAERS events in 2020 and 2021 due to the COVID vaccines for that symptom. The key here is that this count should be multiplied by 41 (known as the underreporting factor or URF to estimate the absolute number of events that occurred). See this article for how that is computed.
Baseline count
The baseline rate is the # of incidents occurring in a 5 year period from 2015-2019 for all vaccines given in that time period.
X-factor
The X-factor is the (C19 count*5/Baseline count). This is because the baseline is 5 years so we compare the COVID counts in a year vs. the average count in a typical year. So an X-factor of 10 or more would mean that the symptom is very likely to be caused by the vaccine since it is highly elevated from the “normal” rate.
Now let’s tackle the tabs. There are two tabs:
match tab
On the match tab are symptoms where the baseline count !=0
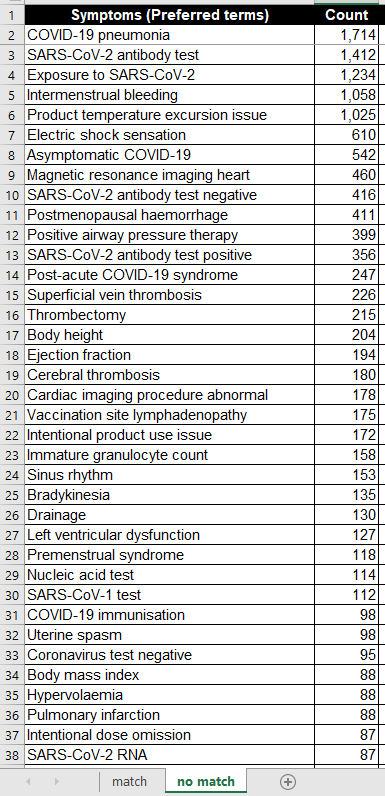
no match tab
On the “no match” tab are symptoms where the baseline count=0. So these are quite extraordinary since these symptoms are not typically seen even once in 5 years. So here, even a small value in the “count” field is very significant, e.g., 2 or more would be comparable to a 10X or more on the “match tab.”
Now here are some screenshots of the first page of the two tabs:
And the no match tab:
What the data tells us
Here are a few quick observations from the complete data set (see next section for downloading):
- Female reproductive issues top the list. These are strongly elevated by these vaccines. Many of the top symptoms are all related to the menstrual process.
- There are an enormous number of cardiovascular and neurological events that are strongly elevated, many of them serious.
- Fibrin D dimer increased is #53 on the list, elevated by a factor of over 400x above baseline. Charles Hoffe discovered D-dimer was elevated in over 60% of the patients he measured. This is very serious as D-dimer is a lagging indicator of blood clots.
- Troponin increased was #130, elevated by a factor of 205. Troponin indicates heart damage and it is elevated to extreme levels (10X heart attack levels or more) and can stay elevated for months at a time (with a heart attack, the levels start returning back to normal immediately after the incident)
- Death as a symptom (which is pretty unusual coding since it isn’t a symptom), is #433 and elevated by 96X. Hardly a “safe” vaccine.
- Brain herniation at #405 is elevated by a factor of 100X over baseline. However, this is not considered a big deal at the CDC (perhaps because many people there don’t use their brain).
- Cardiac arrest at #450 is elevated by 93X. This is when your heart stops. This is a relatively serious condition since you don’t last for too long after that. It’s a bit surprising that the CDC missed that one. Perhaps because they don’t have a heart?
- Pulmonary embolism #24 is elevated by 954 times normal. How the CDC can miss that one is simply astonishing! This was the cause of death of 2 of the 14 kids that the CDC looked at in their death analysis. Mainstream press will never ask them that question as to why the CDC would not find causality here. They wrote: “CDC reviewed 14 reports of death after vaccination. Among the decedents, four were aged 12–15 years and 10 were aged 16–17 years. All death reports were reviewed by CDC physicians; impressions regarding cause of death were pulmonary embolism (two), …” 954 times normal is hard to explain, isn’t it? So no causality? That’s hard to explain, so they didn’t. They just moved on as if there is nothing to see.
- Intracranial haemorrhage (their spelling) is at #604 and is elevated by 79X. Two of the 14 kids from the CDC analysis died from that. How could that not be causal? They never explained that.
- Tinnitus at #362 is elevated by 105X. This can be so bad that people can kill themselves from this alone. One of the people who work at Vaccine Safety Research Foundation (VSRF) had to talk a friend out of suicide.
- There are many many more issues to be concerned with, but I wanted to get the list out quickly so there can be more eyes on this.
- For months, I’ve offered to discuss our data and analyses to both the FDA and CDC outside committees as well as the CDC and FDA themselves, but nobody wanted to see it. Most hit delete on my emails. A few told me to wait for the public comment period and submit it then (which I’ve done). Nobody followed up.
The Excel file with the full results
I’m trying to increase the number of paying subscribers I have as this supports the substack community. All proceeds will go to paying the salaries of people working for the Vaccine Safety Research Foundation (vacsafety.org) as well as buying ads so we can get the message out.
You can find the full Excel file and Albert’s analysis in this article.
What is the Number Needed to Vaccinate to prevent a single COVID fatality in kids 5 to 11 based on Pfizer’s EUA application?
And what are the risks that go along with injecting that many kids?
By Toby Rogers | October 31, 2021
Number Needed to Vaccinate (NNTV), the standard policy tool that Pharma, the FDA, & CDC no longer want to talk about
A funny thing happened this afternoon. Not funny as in “haha”. More like funny as in, “ohhhhh that’s how the FDA rigs the process.”
I was reading the CDC’s “Guidance for Health Economics Studies Presented to the Advisory Committee on Immunization Practices (ACIP), 2019 Update” and I realized that the FDA’s woeful risk-benefit analysis in connection with Pfizer’s EUA application to jab children ages 5 to 11 violates many of the principles of the CDC’s Guidance document. The CDC “Guidance” document describes 21 things that every health economics study in connection with vaccines must do and the FDA risk-benefit analysis violated at least half of them.
Today I want to focus on a single factor: the Number Needed to Vaccinate (NNTV). In four separate places the CDC Guidance document mentions the importance of coming up with a Number Needed to Vaccinate (NNTV). I did not recall seeing an NNTV in the FDA risk-benefit document. So I checked the FDA’s risk-benefit analysis again and sure enough, there was no mention of an NNTV.
Because the FDA failed to provide an NNTV, I will attempt to provide it here.
First a little background. The Number Needed to Treat (NNT) in order to prevent a single case, hospitalization, ICU admission, or death, is a standard way to measure the effectiveness of any drug. It’s an important tool because it enables policymakers to evaluate tradeoffs between a new drug, a different existing drug, or doing nothing. In vaccine research the equivalent term is Number Needed to Vaccinate (NNTV, sometimes also written as NNV) in order to prevent a single case, hospitalization, ICU admission, or death (those are 4 different NNTVs that one could calculate).
Pharma HATES talking about NNTV and they hate talking about NNTV even more when it comes to COVID-19 vaccines because the NNTV is so ridiculously high that this vaccine could not pass any honest risk-benefit analysis.
Indeed about a year ago I innocently asked on Twitter what the NNTV is for coronavirus vaccines.
Pharma sent a swarm of trolls in to attack me and Pharma goons published hit pieces on me outside of Twitter to punish me for even asking the question. Of course none of the Pharma trolls provided an estimate of the NNTV for COVID-19 shots. That tells us that we are exactly over the target.
Various health economists have calculated a NNTV for COVID-19 vaccines.
- Ronald Brown, a health economist in Canada, estimated that the NNTV to prevent a single case of coronavirus is from 88 to 142.
- Others have calculated the NNTV to prevent a single case at 256.
- German and Dutch researchers, using a large (500k) data set from a field study in Israel calculated an NNTV between 200 and 700 to prevent one case of COVID-19 for the mRNA shot marketed by Pfizer. They went further and figured out that the “NNTV to prevent one death is between 9,000 and 100,000 (95% confidence interval), with 16,000 as a point estimate.”
You can see why Pharma hates this number so much (I can picture Pharma’s various PR firms sending out an “All hands on deck!” message right now to tell their trolls to attack this article). One would have to inject a lot of people to see any benefit and the more people who are injected the more the potential benefits are offset by the considerable side-effects from the shots.
Furthermore, the NNTV to prevent a single case is not a very meaningful measure because most people, particularly children, recover on their own (or even more quickly with ivermectin if treated early). The numbers that health policy makers should really want to know are the NNTV to prevent a single hospitalization, ICU admission, or death. But with the NNTV to prevent a single case already so high, and with significant adverse events from coronavirus vaccines averaging about 15% nationwide, Pharma and the FDA dare not calculate an NNTV for hospitalizations, ICU, and deaths, because then no one would ever take this product (bye bye $93 billion in annual revenue).
Increased all cause mortality in the Pfizer clinical trial of adults
As Bobby Kennedy noted in personal correspondence with me, Pfizer’s clinical trial in adults showed alarming increases in all cause mortality in the vaccinated :
In Pfizer’s 6 month clinical trial in adults — there was 1 covid death our of 22,000 in the vaccine (“treatment”) group and 2 Covid deaths out of 22,000 in the placebo group (see Table s4). So NNTV = 22,000. The catch is there were 5 heart attack deaths in the vaccine group and only 1 in placebo group. So for every 1 life saved from Covid, the Pfizer vaccine kills 4 from heart attacks. All cause mortality in the 6 month study was 20 in vaccine group and 14 in placebo group. So a 42% all cause mortality increase among the vaccinated. The vaccine loses practically all efficacy after 6 months so they had to curtail the study. They unblinded and offered the vaccine to the placebo group. At that point the rising harm line had long ago intersected the sinking efficacy line.
Former NY Times investigative reporter Alex Berenson also wrote about the bad outcomes for the vaccinated in the Pfizer clinical trial in adults (here). Berenson received a lifetime ban from Twitter for posting Pfizer’s own clinical trial data.
Pfizer learned their lesson with the adult trial and so when they conducted a trial of their mRNA vaccine in children ages 5 to 11 they intentionally made it too small (only 2,300 participants) and too short (only followed up for 2 months) in order to hide harms.
Estimating an NNTV in children ages 5 to 11 using Pfizer’s own clinical trial data
All of the NNTV estimates above are based on data from adults. In kids the NNTV will be even higher (the lower the risk, the higher the NNTV to prevent a single bad outcome). Children ages 5 to 11 are at extremely low risk of death from coronavirus. In a meta-analysis combining data from 5 studies, Stanford researchers Cathrine Axfors and John Ioannidis found a median infection fatality rate (IFR) of 0.0027% in children ages 0-19. In children ages 5 to 11 the IFR is even lower. Depending on the study one looks at, COVID-19 is slightly less dangerous or roughly equivalent to the flu in children.
So how many children would need to be injected with Pharma’s mRNA shot in order to prevent a single hospitalization, ICU admission, or death?
Let’s examine Pfizer’s EUA application and the FDA’s risk-benefit analysis. By Pfizer’s own admission, there were zero hospitalization, ICU admissions, or deaths, in the treatment or control group in their study of 2,300 children ages 5 to 11.
So the Number Needed to Vaccinate in order to prevent a single hospitalization, ICU admission, or death, according to Pfizer’s own data, is infinity. ∞. Not the good kind of infinity as in God or love or time or the universe. This is the bad kind of infinity as in you could vaccinate every child age 5 to 11 in the U.S. and not prevent a single hospitalization, ICU admission, or death from coronavirus according to Pfizer’s own clinical trial data as submitted to the FDA. Of course Pfizer likes this kind of infinity because it means infinite profits. [Technically speaking the result is “undefined” because mathematically one cannot divide by zero, but you get my point.]
Estimating an NNTV and risk-benefit model in children ages 5 to 11 using the limited data that are available
Everyone knows that Pfizer was not even trying to conduct a responsible clinical trial of their mRNA shot in kids ages 5 to 11. Pfizer could have submitted to the FDA a paper napkin with the words “Iz Gud!” written in crayon and the VRBPAC would have approved the shot. They are all in the cartel together and they are all looking forward to their massive payoff/payday.
But let’s not be like Pharma. Instead, let’s attempt to come up with a best guess estimate based on real world data. Over time, others will develop a much more sophisticated estimate (for example, Walach, Klement, & Aukema, 2021 estimated an NNTV for 3 different populations based on “days post dose”). But for our purposes here I think there is a much easier way to come up with a ballpark NNTV estimate for children ages 5 to 11.
Here’s the benefits model:
- As of October 30, 2021, the CDC stated that 170 children ages 5 to 11 have died of COVID-19-related illness since the start of the pandemic. (That represents less than 0.1% of all coronavirus-related deaths nationwide even though children that age make up 8.7% of the U.S. population).
- The Pfizer mRNA shot only “works” for about 6 months (it increases risk in the first month, provides moderate protection in months 2 through 4 and then effectiveness begins to wane, which is why all of the FDA modeling only used a 6 month time-frame). So any modeling would have to be based on vaccine effectiveness in connection with the 57 (170/3) children who might otherwise have died of COVID-related illness during a 6-month period.
- At best, the Pfizer mRNA shot might be 80% effective against hospitalizations and death. That number comes directly from the FDA modeling (p. 32). I am bending over backwards to give Pfizer the benefit of considerable doubt because again, the Pfizer clinical trial showed NO reduction in hospitalizations or death in this age group. So injecting all 28,384,878 children ages 5 to 11 with two doses of Pfizer (which is what the Biden administration wants to do) would save, at most, 45 lives (0.8 effectiveness x 57 fatalities that otherwise would have occurred during that time period = 45).
- So then the NNTV to prevent a single fatality in this age group is 630,775 (28,384,878 / 45). But it’s a two dose regimen so if one wants to calculate the NNTV per injection the number doubles to 1,261,550. It’s literally the worst NNTV in the history of vaccination.
If you inject that many children, you certainly will have lots and lots of serious side effects including disability and death. So let’s look at the risk side of the equation.
Here’s the risk model:
- Because the Pfizer clinical trial has no useable data, I have to immuno-bridge from the nearest age group.
- 31,761,099 people (so just about 10% more people than in the 5 to 11 age bracket) ages 12 to 24 have gotten at least one coronavirus shot.
- The COVID-19 vaccine program has only existed for 10 months and younger people have only had access more recently (children 12 to 15 have had access for five months; since May 10) — so we’re looking at roughly the same observational time period as modeled above.
- During that time, there are 128 reports of fatal side effects following coronavirus mRNA injections in people 12 to 24. (That’s through October 22, 2021. There is a reporting lag though so the actual number of reports that have been filed is surely higher).
- Kirsch, Rose, and Crawford (2021) estimate that VAERS undercounts fatal reactions by a factor of 41 which would put the total fatal side effects in this age-range at 5,248. (Kirsch et al. represents a conservative estimate because others have put the underreporting factor at 100.)
- With potentially deadly side effects including myo- and pericarditis disproportionately impacting youth it is reasonable to think that over time the rate of fatal side effects from mRNA shots in children ages 5 to 11 might be similar to those in ages 12 to 24.
So, to put it simply, the Biden administration plan would kill 5,248 children via Pfizer mRNA shots in order to save 45 children from dying of coronavirus.
For every one child saved by the shot, another 117 would be killed by the shot.
The Pfizer mRNA shot fails any honest risk-benefit analysis in children ages 5 to 11.
Even under the best circumstances, estimating NNTV and modeling risk vs. benefits is fraught. In the current situation, with a new and novel bioengineered virus, where Pfizer’s data are intentionally underpowered to hide harms, and the FDA, CDC, & Biden Administration are doing everything in their power to push dangerous drugs on kids, making good policy decisions is even more difficult.
If the FDA or CDC want to calculate a different NNTV (and explain how they arrived at that number) I’m all ears. But we all know that the FDA refused to calculate an NNTV not because they forgot, but because they knew the number was so high that it would destroy the case for mRNA vaccines in children this age. Your move CDC — your own Guidance document states that you must provide this number.
FDA approves Pfizer jab for kids, but even they don’t seem sure it’s safe
By Helen Buyniski | RT | November 1, 2021
American children have no choice but to act as experimental test subjects for the Pfizer Covid-19 vaccine to determine the jab’s safety, the Food and Drug Administration has apparently concluded. Good luck, kids!
“We’re never going to learn about how safe the vaccine is unless we start giving it,” editor of the New England Journal of Medicine and Harvard adjunct professor Eric Rubin argued last week, his words buried within the eight-hour barrage of presentations and discussions that swirled around the FDA advisory panel’s approval of the mRNA jab for children aged five to 11.
The FDA followed up on the advisory panel’s 17-0 recommendation with approval, as it typically does, on Friday. If the Centers for Disease Control and Prevention follows suit, some 28 million American children will be quickly served up as fresh-faced fodder for a smaller dose of the Covid-19 vaccine already poised to inject some 100 million American adults. That is, as soon as President Joe Biden is able to whip up a legally-binding demand he can submit to the Occupational Safety and Health Administration.
Friday’s FDA approval means only the CDC stands between American children and a warp-speed rollout of the Pfizer jab. However, the rush to approval doesn’t necessarily mean there are no concerns. A disturbingly large portion of the FDA committee’s members are connected to Pfizer in some way or another, leading vaccine skeptics to cry foul. Meanwhile, a growing portion of the country continues to denounce the mandates in general, insisting everyone should be able to make their own decision regarding whether or not they wish to get injected.
Echoing the newly-reanimated pro-choice slogan, mandate protesters recently swarmed the Brooklyn Bridge declaring ‘My body, my choice’ as New York City employees faced the potential loss of their jobs as firefighters, police officers, sanitation handlers, and corrections officers due to Mayor Bill de Blasio’s insistence that all municipal employees get vaxxed or be relegated to the purgatory of open-ended unpaid leave.
The FDA’s effort to put the cart so far in front of the horse mirrored the words of House Speaker Nancy Pelosi during the congressional tug-of-war over Obamacare in 2010. Faced with a phonebook-sized, dubiously-legal bill unlike anything Congress had passed before and no realistic timeframe to wrangle with the details, Pelosi suggested Congress would have to “pass the bill to find out what’s in it, away from the fog of controversy.”
Since then, legislation by brute force has only grown as the means by which laws are passed in the US, as ever-more-polarized parties refuse to give an inch and betray the appearance of weakness. Allowing the ‘other side’ to be seen as achieving even the slightest victory is unconscionable, and that framework remains in place in the vaccination arena – where it makes less sense than anywhere else.
After all, it was former President Donald Trump’s Operation Warp Speed that brought the world the Pfizer shot, even if the jab itself wasn’t rolled out until shortly (some would say deliberately) after the 2020 election and vaccine mandates have since become a cause celebre of the Democratic Party.
With half the US up in arms about the other half’s supposed refusal to roll up its sleeves and submit to an intensely politicized needle, anyone who hesitates is denounced posthaste in a 21st-century witch hunt – to be fired, if not set on fire; outfitted with the scarlet A for anti-vaxxer, not adulteress; and otherwise chased out of the public square – deplatformed from Twitter, YouTube and Facebook, if not chased physically with pitchforks and torches. Similar divisions have erupted across Europe, and countries like Italy and France have pushed the issue even further, barring the unvaccinated from so much as entering grocery stores to buy food.
While the US study of the Pfizer vaccine’s effects on children five to 11 failed to turn up any deadly side effects, critics argued its population size was too small to be effective for such a purpose. Parents of some jab recipients have observed disturbing symptoms in their offspring in the hours and days following the shots and filmed heartbreaking testimonials describing their downfall from healthy children to pain-wracked perma-patients experiencing near-constant seizures, facial distortions, debilitating heart problems, or other dire health issues.
Another doctor on the FDA committee, Michael Kurilla of the National Institutes of Health, abstained from voting on recommending Pfizer-BioNTech’s vaccine entirely, citing a lack of evidence that all children need the shot, and while Kurilla, an infectious disease and pathology expert, was the only panel member to abstain from voting, he was not the only member to openly express misgivings about doling out the jab to young Americans. His colleague, Dr. Cody Meissner of Tufts University, suggested that it would be an “error” to mandate the jab for children to return to school until there was more hard data.
“We simply don’t know what the side effects are going to be,” he said, acknowledging the shot – like its adult equivalent – probably wouldn’t prevent transmission of the virus. While he was not opposed to administering the shot to certain vulnerable subgroups inside the 5-11 age group, Meissner was concerned approving the shot for everyone in that category would lead to a heavy-handed mandate the likes of which is currently being wielded against American adults.
Children who receive the Pfizer-BioNTech jab may actually get less immunity and face more risk than supplied by getting and recovering from a current strain of Covid-19, Kurilla told the Daily Mail, referring to the Delta variant and other current strains of Covid-19 circulating among the population. “The question really becomes, does this vaccine offer any benefits to them at all?” he asked rhetorically during the FDA committee meeting. He would have voted ‘yes’ if the FDA had merely proposed opening up access to the vaccine to a ‘subset’ of those ages five to 11, but he disagreed with administering it to all children within that age group.
Two other panel members voted to approve despite their misgivings. Meissner argued that a “very small percent of otherwise healthy six-to-11-year-old children…might derive some benefit,” while President and CEO of Meharry Medical College James Hildreth agreed that “vaccinating all of the children…seems a bit much for me,” pointing to the relatively low risk of hospitalization and near-zero risk of death by Covid-19 for children.
Speaking up against the jab, even circumstantially, has become the kiss of death in the medical community, with even medical rock stars like Robert Malone, one of the inventors of mRNA as a drug, cast into the dustbin of history for expressing skepticism that his invention was being incorrectly used to deliver the Covid-19 vaccine.
However, governments worldwide are setting themselves up for civil war as populations are forced to choose one ‘side’ or another. Even many of the vaccinated have acknowledged that the jab should not be forced on anyone, while entire industries like shipping, air travel, defense, and the like grind to a halt as mandates run up against the stubborn will of their employees. Southwest Airlines was allegedly forced to cancel thousands of flights earlier this month, due to a reported mass ‘sickout’ by air traffic controllers unwilling to get vaxxed, though the airline itself has denied this, and rumors of trucker strikes from Australia to America have food sellers panicking at the thought of empty shelves.
As it stands, parents who were willing to submit themselves to experimental shots in the name of convenience and retaining employment may not be so willing to offer up their children as sacrifices to a company once denounced by the US Justice Department as the worst fraudster in the pharmaceutical industry.
Governments that have shown themselves as profoundly untrustworthy throughout the Covid-19 pandemic are unlikely to change their behavior at the last minute, and parents are wise to take care in where they place their trust.
Scientist Whose Wife Was Injured by COVID Vaccine Tells FDA: ‘Please Do Not Give This to Kids’
By Megan Redshaw | The Defender | October 27, 2021
The U.S. Food and Drug Administration’s (FDA) advisory committee on Tuesday endorsed Pfizer’s COVID vaccine for children ages 5 to 11, despite strong objections raised during the meeting by multiple scientists and physicians.
Brian Dressen, Ph.D., is one of the scientists who testified during the 8-hour hearing.
Dressen is also the husband of Brianne Dressen, who developed a severe neurological injury during the Utah-based portion of the U.S. AstraZeneca COVID vaccine trial in 2020. After being injured by the first dose, Brianne withdrew from the trial.
During his 3-minute testimony, Dressen, a chemist with an extensive background in researching and assessing the degree of efficacy in new technologies, told the FDA advisory panel Pfizer’s vaccine “failed any reasonable risk-benefit calculus in connection with children.”
Dressen said:
“Your decision is being rushed, based on incomplete data from underpowered trials, insufficient to predict rates of severe and long-lasting adverse reactions. I urge the committee to reject the EUA [Emergency Use Authorization] modification and direct Pfizer to perform trials that will decisively demonstrate that the benefits outweigh the risks for children. I understand firsthand the impact that you will or will not have with the decision you’re going to make today.”
Dressen told the FDA how his wife was severely injured last November by a single dose of a COVID vaccine administered during a clinical trial. He said:
“Because study protocol requires two doses, she was dropped from the trial, and her access to the study app deleted. Her reaction is not described in the recently released clinical trial report — 266 participants are described as having an adverse event leading to discontinuation, with 56 neurological reactions tallied.”
He said he and his wife have since met participants from other vaccination trials — including Pfizer’s trial for 12- to 15-year-olds — who suffered similar reactions and fate.
Dressen said:
“Injured support groups are growing. Memberships number into at least the tens of thousands. We must do better. Those injured in a trial are a critical piece of vaccine safety data. They are being tossed aside and forgotten. The FDA has known first-hand about her case and thousands of others. The FDA has also stated that their own systems are not identifying this issue and that VAERS is not designed to identify any multi-symptom signals. The system is broken.”
Dressen said his family’s lives have changed forever. “The clinical trials are not appropriately evaluating the data,” he said. “The FDA, Centers for Disease Control and Prevention (CDC) and the drug companies continue to deflect the persistent and repeated cries for help and acknowledgment, leaving the injured as collateral damage.”
He added:
“Until we appropriately care for those already injured, acknowledge the full scope of injuries that are happening to adults, please do not give this to kids. You have a very clear responsibility to appropriately assess the risks and benefits to these vaccines. It is obvious that isn’t happening.
“The suffering of thousands continues to repeatedly fall on deaf ears at the FDA. Each of you hold a significant responsibility today and know that without a doubt, when you approve this for the 5 to 11-year-old’s, you are signing innocent kids and uninformed parents to a fate that will undoubtedly rob some of them of their life.”
In an interview with KUTV on Tuesday, Brianne said her kids will not receive a COVID-19 vaccine if approved. “I will react to the vaccine regardless of the brand, and so if my kids have this same genetic makeup, there is the high potential now that the same thing could happen to them,” she said.
Since his wife’s injury — diagnosed by doctors at the National Institutes of Health — the Dressens have met with other trial participants and families with children who also believe they were injured by the COVID vaccines. They formed a support group and website called, C19 Vax Reactions, to share their stories of vaccine injuries.
On June 26, Sen. Ron Johnson (R-Wis.) held a news conference to discuss adverse reactions related to the COVID vaccines — giving individuals, including Brianne, who have been “repeatedly ignored” by the medical community a platform to share their stories.
According to KUTV, the group continues to push the FDA and CDC for answers and help. Largely ignored, they reached out to Utah Senator Mike Lee, who wrote a letter to the CDC and FDA on their behalf.
Megan Redshaw is a freelance reporter for The Defender. She has a background in political science, a law degree and extensive training in natural health.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
FDA Panel Endorse Pfizer Shots for 5- to 11-Year-Olds, Experts Say it’s ‘Unnecessary and Will Do More Harm Than Good’
By Megan Redshaw | The Defender | October 26, 2021
The U.S. Food and Drug Administration’s (FDA) advisory committee today endorsed Pfizer’s COVID vaccine for children ages 5 to 11, despite strong objections raised during the meeting by multiple scientists and physicians.
The vote passed with 17 supporting it and one abstention.
Before the shots can be rolled out, the FDA will have to formally authorize the vaccine, and the Centers for Disease Control and Prevention (CDC) must also weigh in with its own recommendations — but the Biden administration’s announcement last week that it has already ordered 68 million doses of the pediatric vaccine suggests Pfizer’s request will sail through.
During today’s meeting, the Vaccines and Related Biological Products Committee (VRBPAC) heard evidence from Pfizer and regulators, and listened to concerns from numerous experts.
According to the FDA website, as of Oct. 25, the agency had received 139,470 comments from the public prior to today’s meeting — a number federal officials described as strikingly high.
As he opened the meeting, Dr. Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research (CBER), said, “I want to acknowledge the fact that there are strong feelings that have clearly been expressed by members of the public both for and against” authorization.
Marks stressed the only question before the experts was whether shots should be allowed, not whether to mandate them, the New York Times reported.
The dose for younger children would be one-third the strength given to people 12 and older, with two shots given three weeks apart.
Based on CDC data presented during the meeting, among children 5 to <12 years of age, there have been approximately 1.8 million confirmed and reported COVID cases since the beginning of the pandemic, and only 143 COVID-related deaths in the U.S. through Oct. 14.
In this same age group, there were 8,622 COVID-related hospitalizations through Sept 18.
“This translates to cumulative incidence rates of approximately 6,000 and 30 per 100,000 for confirmed COVID cases and COVID-related hospitalizations, respectively, among children 5 to <12 years of age,” Pfizer’s application said.
Children with underlying medical conditions, such as asthma, diabetes and obesity, made up two-thirds of severe COVID cases.
Pfizer provided safety data on two study cohorts of children ages 5 to 11, both of roughly equal size. The first group was followed only for about two months, the second for only two-and-a-half weeks.
The two-month cohort included 2,268 children ages 5 to 11. Of the 2,268 children, 1,518 received the vaccine and 750 received a placebo. Each received two shots spaced three weeks apart.
Pfizer’s study found its vaccine was about 91% effective against symptomatic COVID in children, based on 16 cases of COVID in the placebo group and three cases in the vaccinated group over the brief follow-up period.
Most side effects occurred within a couple of days and included pain at the injection site, fatigue, headache, muscle pains and chills, Pfizer said.
According to Pfizer, the number of participants in the current clinical development program was “too small to detect any potential risks of myocarditis associated with vaccination.”
Long-term safety of Pfizer’s COVID-19 vaccine “to evaluate long-term sequelae of post-vaccination myocarditis/pericarditis” in participants 5 to <12 years of age will not be studied until after the vaccine is authorized for children,” Pfizer’s application noted.
Pfizer data insufficient, kids’ risk of vaccine injury greater than COVID risk, experts say
Experts raised concerns over the lack of safety and efficacy data presented by Pfizer for use of its COVID vaccine in younger children, and they pointed to increasing safety signals based on reports to the Vaccine Adverse Event Reporting System (VAERS).
They also questioned the need to vaccinate children — whose risk of dying from COVID is “almost nil” — at all.
According to Dr. Meryl Nass, member of the Children’s Health Defense Scientific Advisory Panel, Pfizer once again did not use all of the children who participated in the trial in their safety study.
“Three thousand children received Pfizer’s COVID vaccine, but only 750 children were selectively included in the company’s safety analysis,” Nass said. “Studies in the 5-11 age group are essentially the same as the 12-15 group — in other words, equally brief and unsatisfying, with inadequate safety data and efficacy data, with no strong support for why this type of immuno-bridging analysis is sufficient.”
Nass said, “All serious adverse events were considered unrelated to the vaccine.”
During the meeting and in its FDA application, Pfizer argued children should be vaccinated to prevent SARS-CoV-2 transmission, yet the company did not assess asymptomatic transmission.
Dr. Ofer Levy, a VRBPAC member, asked for evidence that Pfizer’s vaccine prevents transmission.
Dr. William Gruber, senior vice president of Pfizer Vaccine Clinical Research and Development, said they did not assess whether the vaccine prevents transmission, but said there is evidence the vaccine prevents transmission in adults.
When questioned further, Gruber was unable to cite specific evidence to back his assertion.
Steve Kirsch, founder of the COVID-19 Early Treatment Fund, asked the panel how they could do a risk-benefit analysis with Pfizer’s COVID vaccine if they did not know the CDC’s VAERS under-reporting factor (URF).
Kirsch asked:
“How can you do a risk-benefit of analysis of COVID vaccines if you don’t know the URF? This is extremely, extremely important. You have been assuming it has been one. It is not one. Using a URF of 41, which is calculated using CDC methodology, we find over 300,000 excess deaths in VAERS. If the vaccine didn’t kill these people, what did?”
“How many Americans have to die before you pull the plug?” Kirsch asked.
Kirsch also questioned the panel on why Maddie de Garay’s severe adverse reaction to the Pfizer vaccine, which left her paralyzed, was not reported by the company to the FDA.
Dr. Jessica Rose, viral immunologist and biologist, told the panel EUA of biological agents requires the existence of an emergency and the nonexistence of alternate treatment.
“There is no emergency and COVID-19 is exceedingly treatable,” Rose said.
In a peer-reviewed study co-authored by Rose, myocarditis rates were significantly higher in people 13 to 23 years old within eight weeks of the COVID vaccine rollout.
In 12- to15-year-olds, Rose said, reported cases of myocarditis were 19 times higher than background rates.
“In an act of censorship, this paper has been temporarily removed and it has now been killed without criticism of the work,” Rose said, noting the timing of the removal was strange.
Rose said tens of thousands of reports have been submitted to VAERS for children ages 0 to 18.
Rose explained:
“In this age group, 60 children have died — 23 of them were less than 2 years old. It is disturbing to note that “product administered to patient of inappropriate age was filed 5,510 times in this age group. Two children were inappropriately injected, presumably by a trained medical professional, and subsequently died.”
Dr. Josh Guetzkow, a senior lecturer at the Hebrew University of Jerusalem, said expanding the EUA to children is unnecessary, premature and will do more harm than good.
Guetzkow said there is no emergency for children, especially healthy ones whose risk of severe illness and death is “almost nil.”

Guetzkow said kids with pre-existing conditions and prior COVID infections were not included in Pfizer’s study, so including them in the EUA is negligence.
“Pfizer’s trial is woefully underpowered to detect specific safety concerns, such as myocarditis, just like the adolescent study was, and if they weren’t able to detect an unexpected safety concern there, they wouldn’t be able to here,” Guetzkow said.
Guetzkow said:
“In Pfizer’s study, only .5% of controls were dropped due to important protocol violations, versus 3% in the treatment group. The odds of that happening by chance are 1 in 10,000. This deviation is poorly explained with no ITT analysis. The study is not double-blind and may be subject to bias. Most VSD safety monitoring programs have not reported results, why not wait?”
Guetzkow said, “from CDC reports, we can expect that for every 18 child hospitalizations prevented, at least 43 will end up in the hospital for all causes following vaccination,” yet, the “FDA’s risk-benefit analysis only counts myocarditis hospitalization.”
“Why ignore the V-safe data, and shouldn’t FDA verify Pfizer’s efficacy and immunobridging analysis first?” he asked.
Guetzkow said VAERS shows alarming safety signals, which cannot be attributed to increased vaccination, simulated reporting or COVID infections.
“We calculated the ratio of adverse events reported per million Pfizer vaccinations to reports per million flu vaccinations among teenagers to see what to expect in children. Serious events are reported 51% more often for Pfizer, deaths 47 times, life-threatening conditions 49 times,” Guetzkow said.
Guetzkow asked the panel to look at the data on COVID vaccines compared to flu vaccines. Pointing to the data on reproductive organs, Guetzkow asked, “why would we expect children to take these risks to protect adults?”
There are more than 900 types of adverse events reported after Pfizer vaccination that have never been reported after flu vaccines, including 11 cases of multisystem-inflammatory syndrome (MS-C) that occurred without previous history of COVID infection, Guetzkow said.
He added that if the panel was considering authorizing Pfizer’s COVID vaccine to prevent MS-C — as Pfizer’s application suggested as one of the reasons they should — the panel should reconsider.
During another part of the meeting, Julia Barnes-Weise, director of the Global Healthcare Innovation Alliance Accelerator, said pharmaceutical companies have concerns.
“One of them is, especially for a not-yet-approved vaccine, that they could be held liable for any injury that that vaccine seems to have caused,” Barnes-Weise said.
In a preliminary analysis last week, FDA reviewers said protection would “clearly outweigh” the risk of a very rare side effect in almost all scenarios of the pandemic, PBS News Hour reported.
Children’s Health Defense (CHD) said yesterday it would take legal action against the FDA if it granted EUA for the Pfizer-BioNTech vaccine for children 5- to 11- years old.
In a letter signed by Robert F. Kennedy, Jr., CHD chairman and chief legal counsel, and Nass, Kennedy and Nass wrote:
“CHD will seek to hold you accountable for recklessly endangering this population with a product that has little efficacy but which may put them, without warning, at risk of many adverse health consequences, including heart damage, stroke, and other thrombotic events and reproductive harms.”
Megan Redshaw is a freelance reporter for The Defender. She has a background in political science, a law degree and extensive training in natural health.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Featured Video
NO DUST NO DEAL, Seems Like We’re Closer to Hot War w/Iran
or go to
Aletho News Archives – Video-Images
Villains of Judea
Abe Foxman
Foxman left a legacy of surveillance scandals, political vendettas, and selective outrage.

José Niño Unfiltered | May 24, 2026
When Abraham Foxman died on May 10, 2026, tributes poured in from presidents, prime ministers, and Jewish leaders worldwide, yet his legacy remains defined as much by controversy as by accomplishment.
Foxman described himself as “a passionate supporter of the State of Israel” and spent his career building the ADL into a roughly $60 million per year organization that defined mainstream American Jewish advocacy on antisemitism, civil rights, and the Jewish state. … continue
Blog Roll
 Aletho News
Aletho News- Col Doug Macgregor NO DUST NO DEAL, Seems Like We’re Closer to Hot War w/Iran
- Meet the Convicted Jewish Felon Who Scammed Floyd Mayweather
- Ex-Mossad chief threatened ICC prosecutor over Israel war crimes probe
- Trump advances his Arctic strategy
- Senior MP reveals Russia’s strategy for strikes on Kiev
- Germany Embarked on Unprecedented Military Buildup – Expert
- Moscow demands release of Russian Orthodox bishop detained by NATO state
- When Our Word is No Longer Good
- ‘Unacceptable’: Islamabad won’t normalize with Israel, defense minister says despite Trump’s push
- The Disasters of War. Trump’s “Peace Through Strength” Doctrine Conducive to Worldwide Famines…
- If Americans Knew
- Netanyahu Stresses The Need For More Propaganda As Israel’s Hasbara Budget Soars
- As Israel Heads to Elections, Netanyahu Needs War
- Conflict escalations everywhere: Gaza, Lebanon, Iran – Daily Update
- How AIPAC channels millions through shell PACs ahead of US midterms
- Israel has no mercy on Gaza, Lebanon; Trump throws a curveball into Iran negotiations – Daily Update
- Israel escalates attacks in Gaza, as it demands total disarmament – Daily Update
- Flotilla activists’ allegations of rape, sexual assault multiply – Daily Update
- Israel’s long record of using banned incendiary weapons on civilians
- How Jeffrey Goldberg weaponized Jewish trauma to pave the way for war with Iran
- ISRAELI MEDIA: They Were Children During the Nakba. This Is What They Remember 78 Years Later
- No Tricks Zone
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
- Germany’s AfD Party Calls Debunked Climate Scenarios “Greatest Fraud In Human History”
- Researchers Find Rapid Global Warming Phase At End Of Last Ice Age (Ca.18,000 Years Ago)
- Even The DNA Of Single-Celled Plankton Can Upend Alarmist Arctic Sea Ice Melt Claims
- Scandal: Although Climate Panic Is Canceled By IPCC, Europe’s Policymakers Continue With Their Crushing Policies
- How Once Hardcore Climate Alarmist Lucy Biggers Realized It Was All A Scam, Brainwashing
- German Expert: “No Climate Crisis” …”Warming Generally Better For Humanity”
- New Paleo Research: Modern ‘Climate Change’ Has Had No Apparent Impact On Precipitation Patterns
- 90% Subsidized… Bielefeld Germany’s €7 Million Hydrogen Garbage Truck Fleet Sits Idle
