Following the Money on Climate Change Media Coverage
![]()
By Chris Morrison | The Daily Sceptic | February 20, 2022
The Associated Press (AP) is assigning another two dozen journalists across the world to cover ‘climate issues’. AP Senior Vice President Julie Pace described the move as a “far reaching initiative that will transform the way we cover the climate story”. Over 20 of the journalists will be new hires and they will be funded by an $8m gift from five billionaire philanthropic organisations, including the Left-wing Rockefeller Foundation. The money is just the latest in a series of such gifts and AP reports that 50 writing jobs are funded from these sources.
AP is not the only large media company to collect such hand-outs. The BBC and the Guardian regularly receive multi-million dollar contributions from the trusts of wealthy philanthropists. It is estimated that Bill Gates has given over $300 million over the last decade to a wide variety of media outlets. Faced with plummeting paid readers and advertisers, mainstream legacy media seems eager to tap a new revenue stream.
The money is spread wide across such media. This month, the Pulitzer Center on Crisis Reporting received $1.5 million from Rockefeller to “expand coverage of under-reported and/or inaccurately reported critical public health information”. The Quadrivium Foundation, run by Democrat power couple James and Kathryn Murdoch, is also paying climate wages at AP. On its website, the Foundation notes that it also invests in Climate Central, using meteorologists as “trusted messengers” of the links between extreme weather and climate change. Since it is not possible to link individual weather events to long term climate change with any scientific certainty, this aim looks to be a waste of money, or perhaps not.
‘Trusted messengers’ seems to be a phrase much in vogue around philanthropic operations. Last October, Rockefeller gave $4.5 million to Purpose Global, a non-profit company that aims to help corporate clients with their “cultural intelligence”. The money was given in support of facilitating a “communication network of trusted messengers”. This would “amplify accurate information and combat mis- and dis- information on COVID-19 vaccines”. In September 2020, the Gates Foundation gave the Guardian $3.5 million to “support” its regular reporting on global health. Likewise, the Global Health Security Team at the Telegraph is Gates-funded.
Old school journalists might be a little happier to see less of the ‘trusted messenger’ stuff and more of the requirement to investigate. But critical inquiry of climate change science has been more or less banned from many mainstream outlets. This is despite the fact that the hypothesis that humans cause all or most global warming is unproven, and many scientists look more to natural causes for long term change. Predictions – often termed evidence – of future warming, are based on climate models that have never provided an accurate forecast in the last 40 years. Global warming started to run out of steam two decades ago, and it has been at a standstill for the last seven. When Google Adsense banned the main climate web page tracking accurate satellite data showing the standstill, the interest was confined to just a few outlets, including the Daily Sceptic.
 One of the largest suppliers of cash for climate change is the Bill and Melinda Gates Foundation. Perhaps unsurprisingly, the BBC and the Guardian are two of its favourite giftees. The Guardian has received upwards of $20 million over recent years starting with £6m in 2011 to establish a “millennium Development Goals” feed that provides “compelling evidence-based content”. During the last decade, Gates has given at least $20 million to help fund the BBC World Service and $5.5 million for the Corporation’s Media Action charity.
One of the largest suppliers of cash for climate change is the Bill and Melinda Gates Foundation. Perhaps unsurprisingly, the BBC and the Guardian are two of its favourite giftees. The Guardian has received upwards of $20 million over recent years starting with £6m in 2011 to establish a “millennium Development Goals” feed that provides “compelling evidence-based content”. During the last decade, Gates has given at least $20 million to help fund the BBC World Service and $5.5 million for the Corporation’s Media Action charity.
In that time, the software tycoon, once treated with great suspicion for early monopolistic tendencies, has become a prized ‘talking head’ across the BBC for epidemics, vaccines and anti-meat diets. His recent scary tales of climate change, “How to Avoid a Climate Disaster”, was recently given five airings on prime time Radio 4.
Elsewhere, there are prizes for the best behaved – sorry – most distinguished climate journalist. Every year, the foundation of BBVA, a Spanish bank heavily involved in financing Net Zero projects, hands out €100,000 to the lucky recipient. Last year it went to Marlow Hood of Agence France-Presse, who describes himself as the “Herald of the Anthropocene”, the latter being a political renaming of the current Holocene era. In 2019, Matt McGrath of the BBC pocketed the cash, while in 2020 the award went to – no great surprise – the Guardian.
Much of the BBC money appears to support advocacy in the developing world, although the terms of specific grants are sometimes hard to understand. A letter from the Bill and Melinda Gates Foundation in August 2019 describing the purpose of a $2.03 million grant to the BBC reads as follows: “To help us learn deepen our underpinning of processes and user journeys for different sets of women’s empowerment collectives, develop use cases for where digital can help amplify effects bring efficiencies, and close gender gaps for women”.
No doubt when this non-sensical gibberish was translated into understandable English, the money was spent wisely.
Most Published Studies Exaggerated the Effects of Ocean Acidification – and Covid, Etc.
By Jennifer Marohasy | February 20, 2022
The concept of ocean acidification, and human-caused global warming more generally, could be described as containing a grain of truth embedded in a mountain of nonsense. Indeed, the projected large increase in atmospheric CO2 will at most cause a small reduction in pH – it will not turn the ocean acidic. Yet this is what is implied by the term ocean acidification. True acidification would require average pH to be reduced below 7.0, at which point seashells would indeed begin to dissolve. This is an impossible scenario, however, because of the ocean’s effectively limitless buffering capacity.
There is a newly published study by Jeff Clements and team that concludes many of the published studies on ocean acidification, especially those studies published in high impact journals and accompanied by sensational media reporting, have turned-out to be wrong, or at least exaggerated.
My colleague Peter Ridd describes the situation:
This problem with exaggeration of threats applies to many areas of science and has a name: The Decline Effect.
The Decline Effect goes like this: an early report, usually attracting huge media interest, predicts some sort of catastrophe. But when follow up work is done, usually with far better experimental procedure and far greater numbers of samples, the original report turns out to be wrong.
Jeff Clements’ team included Timothy Clark, Josefin Sundin and Frederik Jutfelt who were involved in a study last year proving that numerous reports by James Cook University’s coral reef centres on reef fish was totally wrong.
I co-authored a book chapter with John Abbot some years ago that explained:
Initial concerns about ocean acidification focused on organisms that construct their shells or skeletons from calcium carbonate. Such organisms are referred to as marine calcifiers and include not only corals, but also crabs, clams and conchs (sea snails).
Theoretically, and according to popular science magazines, all corals are already severely and negatively affected by ocean acidification. But this is not evident from methodologically sound studies undertaken at the Great Barrier Reef. A review of the growth rates of six, hard coral species at Lord Howe Island (Anderson et al. 2015) found marked variation in the growth rates of branching coral, while growth rates of the massive Porites coral were unchanged. The researchers suggested that a decline in the growth rates of the branching species could be attributable to a reduction in the calcium carbonate saturation state as a consequence of higher summer temperatures. A study measuring calcification rates for 41 long-lived Porites corals from seven reefs from the central Great Barrier Reef (D’Olivio et al. 2009), showed good recovery from the major 1998 bleaching event, with no significant trend in calcification rates for the inner reefs. Corals from the mid-shelf central Great Barrier Reef, however, did show a decline of 3.3%.
While most ocean acidification research has been focused on physiological processes, in particular calcification, there have also been studies on three common hard corals to look at their fertilisation, embryonic development, larval survivorship, and metamorphosis (Chua et al. 2013a; Chua et al. 2013b). These studies have found the early life-history stages were unaffected by reduced pH; there was no consistent effect of elevated CO2 alone, nor in combination with temperature.
Studies of the effect of very high CO2 levels (up to 2,850 ppm) on molluscs – including oysters, clams, scallops and conchs – have shown that these species will generally build their shells more slowly as CO2 levels increase (Ries et al. 2009). This same study showed that crabs and lobsters respond quite differently to the same elevated CO2 levels, showing a general increase in calcification rates.
This chart shows how quickly scientists could meet the demand for commentary in the new area of ocean acidification, including to support the theory of human-caused global warming.
The varied responses among different organisms reflect their differing abilities to regulate pH at the site of calcification, and:
- the extent to which their outer shell layer is protected by an organic covering
- the solubility of their shell, or skeletal mineral
- the extent to which they use photosynthesis (Ries et al. 2009).
Of course, many marine organisms are not calcifiers, and some of these organisms have also been tested for a response to ocean acidification.
When seagrasses collected from three locations in the Great Barrier Reef region – Cockle Bay, Magnetic Island, and Green Island – were exposed to four different CO2 concentration levels for two weeks – with water temperature and salinity in the experimental tanks near-constant throughout – all three seagrass species exhibited enhanced photosynthetic responses (Ow et al. 2015). That is growth rates, observed after two weeks of exposure to an enriched CO2 environment in an indoor aquarium, were higher. This suggests that ocean acidification could mean more seagrass, which would be good for large marine mammals like dugongs (dugongs are vulnerable to extinction because of issues unrelated to changing ocean chemistry).
Also, contrary to expectations, laboratory investigations into the effects of three different CO2 treatments on anemonefish (commonly known as the clownfish) found that higher CO2 levels stimulated breeding activity (Miller et al. 2013). The breeding pairs from the fringing reefs of Orpheus Island on the Great Barrier Reef, where they are exposed to the highest CO2 levels, produced double the number of clutches per breeding pair, and 67% more eggs per clutch than the control. However, young anemonefish that were bred in high CO2 levels and high temperatures showed decreases in their length, weight, condition, and survival (Miller et al. 2012). Though these effects were absent or reversed when their parents also experienced the higher concentrations (Miller et al. 2013).

We concluded:
Most studies have been on single species in contrived laboratory conditions. They have been of short duration, and they have not considered the potential for adaptation. In the few instances where adaptation has been considered, it has been shown to significantly modify the impact of varying pH as a consequence of elevated levels of CO2.
All of this needs to be assessed against the reality that along the length and breadth of the Great Barrier Reef there are naturally occurring large daily fluctuations in pH, and that it is unclear as to what extent the current trends of apparent pH decline are part of existing natural cycles.
Most of the articles describe the effects of changes of pH on biological organisms; many of the claims are based exclusively on laboratory experiments (Riebesell & Gattuso 2015). However, a problem with laboratory experiments is that they cannot capture the complexities of the real world, not even the tremendous natural variability in ocean pH – which is a measure of ocean acidification.
Statistician John P.A. Ioannidis published a review of medical research back in 2005 entitled ‘Why most published research findings are false’ (Plos Medicine ). It included a comment that:
The majority of modern biomedical research is operating in areas with very low pre- and post-study probability for true findings.
The review by John Ioannidis is a devastating critic of the sad state of biomedical research. It is this same profession, biomedical research, that concluded we should fear Covid-19 and get vaccinated – with the results from the Pfizer trials withheld while emergency approvals were granted for the mass vaccination of citizens across the world against Covid-19.
We will no doubt have better insights, when studies like those by Jeff Clements into ocean acidification, are undertaken into the recent Covid-19 vaccine research. We may then be in a position to judge whether the apparent ineffectiveness of these particular Covid-19 vaccines, despite all the promises, can be best explained by corporate greed and mendacity, or simply flaws in the scientific method. Certainly there was pressure on medical researchers to find a quick cure, that could be administered as part of a global public health response, to what appeared in the beginning to be a deadly new virus much worse than the seasonal flu.
The British Medical Journal in an editorial dated 19thJanuary includes commentary that we don’t know enough about Covid-19 vaccines.
‘Today, despite the global rollout of Covid-19 vaccines and treatments, the anonymised participant-level data underlying the trials for these new products remain inaccessible to doctors, researchers, and the public—and are likely to remain that way for years to come,’ the editorial states. ‘This is morally indefensible for all trials, but especially for those involving major public health interventions.’
The editorial also accuses pharmaceutical companies of ‘reaping vast profits without adequate independent scrutiny of their scientific claims,’ pointing to Pfizer, whose Covid vaccine trial was ‘funded by the company and designed, run, analysed, and authored by Pfizer employees’.
Of course, Peter Ridd lost his job at James Cook University for speaking truth to power. Those who continue to publish studies on ocean acidification, especially those studies published in high impact journals and accompanied by sensational media reporting, have most recently been rewarded by the Australian government with an additional $1billion in funding. Some of this money will end-up funding more nonsense ocean acidification projects at James Cook University. It is unlikely that any of this grant money will be used to ensure that there is some quality assurance of the same research.
How a false hydroxychloroquine narrative was created, and more

Meryl Nass, MD
Alliance for Human Research Protection | June 28, 2020
Below, Dr. Meryl Nass reviews a long list of corrupt practices that undermine the integrity of medical science and the practice of medicine during the current medical crisis. The coronavirus crisis has been made significantly worse by stakeholders who are preventing doctors from prescribing for their patients, existing, safe and effective medicines, because the stakeholders are invested on garnering projected future profits from not-yet-developed vaccines and “countermeasures” specifically developed against COVID-19.
The stakeholders who influence and issue medical practice guidelines, include public health officials, global public health institutions, government advisory committees, and clinical trialists who design trials to provide commercially beneficial results. Editors of prestigious high impact, medical journals contribute to the corruption of medicine by publishing fraudulent studies, and reports of clinical trials that were designed to cause foreseeable deaths, The focus of Dr. Nass’ J’Accuse post are clinical trials that deliberately subjected some patients to toxic doses of Hydroxychloroquine. [Dr. Nass is a longtime member of the AHRP Board of Directors].
These collaborators engaged in an orchestrated effort to prevent physicians from utilizing an existing, off-patent, cheap and affordable drug, that thousands of clinicians attest to its therapeutic benefit.
- The problem with Hydroxychloroquine, a drug with a 70-year safety track record, is that there is no profit to be made from this cheap, off-patent drug!
*****************
It is remarkable that a series of events taking place over the past 3 months produced a unified message about hydroxychloroquine, and produced similar policies about the drug in the US, Canada, Australia, NZ and western Europe. The message is that generic, inexpensive hydroxychloroquine is dangerous and should not be used to treat a potentially fatal disease, Covid-19, for which there are no (other) reliable treatments.
- Hydroxychloroquine had been used safely for 65 years in millions of patients. And so the message was crafted that the drug is safe for its other uses, but dangerous when used for Covid-19. It doesn’t make sense, but it seems to have worked.
Were these acts carefully orchestrated? You decide.
Might these events have been planned to keep the pandemic going? To sell expensive drugs and vaccines to a captive population? Could these acts result in prolonged economic and social hardship, eventually transferring wealth from the middle class to the very rich? Are these events evidence of a conspiracy?
Here is a list of what happened, in no special order. Please help add to this list if you know of additional acts I should include. This will be a living document. I have penned this as if it is the “to do” list of items to be carried out by those who pull the strings. The items on the list have already been carried out. One wonders what else might be on their list, yet to be carried out, for this pandemic.
1. You stop doctors from using the drug in ways it is most likely to be effective (in outpatients at onset of illness). You prohibit use outside of situations you can control.
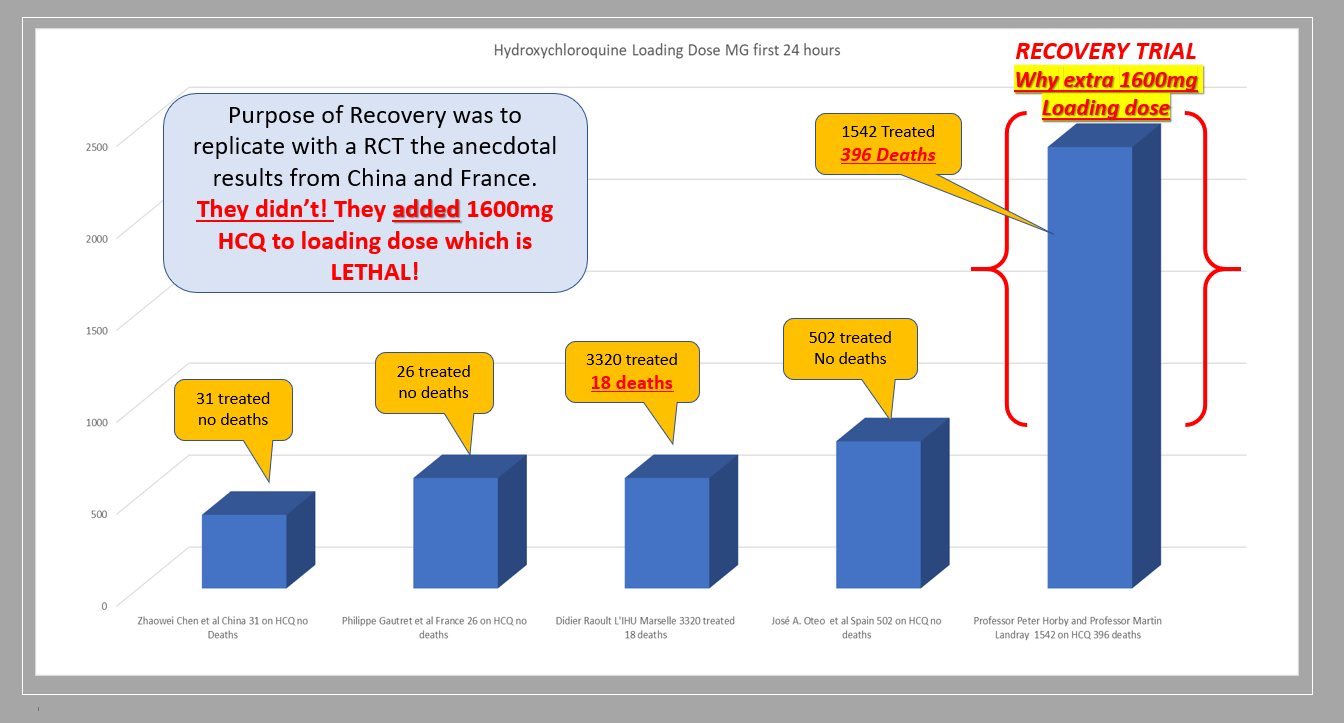
Situations that were controlled to show no benefit included 3 large, randomized, multi-center clinical trials (Recovery, Solidarity and REMAP-Covid), which are generally believed to yield the most reliable evidence. However, each of them used excessive doses that were known to be toxic; see my previous articles here and here.
2. You prevent or limit use in outpatients by controlling the supply of the drug, using different methods in different countries and states. In NY state, by order of the governor, hydroxychloroquine could only be prescribed for hospitalized patients. France has issued a series of different regulations to limit prescribers from using it. France also changed the drugs’ status from over-the-counter to a drug requiring a prescription.
3. You play up the danger of the drug, emphasizing side effects that are very rare when the drug is used correctly. You make sure everyone has heard about the man who died after consuming hydroxychloroquine in the form of fish tank cleaner.
4. You limit clinical trials to hospitalized patients, instead of testing the drug in outpatients, early in the illness, when it is predicted to be most effective.
5. You design clinical trials to give much too high a dose, ensuring the drug will cause harm in some subjects, sufficient to mask any possible beneficial effect. You make sure that dozens of trials in dozens of countries around the world use these dangerous doses.
6. You design clinical trials to collect almost no safety data, so any cause of death due to drug toxicity will be attributed to the disease instead of the drug.
7. You issue rules for use of the drug based on the results of the unethical, overdosing Recovery study.
8. You publish, in the world’s most-read medical journal, the Lancet, an observational study from a huge worldwide database that says use of chloroquine drugs caused significantly increased mortality. You make sure that all major media report on this result. Then 3 European countries announce they will not allow doctors to prescribe the drug. And Sanofi announces it will no longer supply the drug for use with Covid, and will halt its own clinical trials, based on a fabricated study.
9. Even after hundreds of people renounce this observational study due to easily identified fabrications–which, as James Todaro, MD, wrote was a “study out of thin air“–the Lancet held firm for two weeks, serving to muddy the waters about the trial, until finally 3 of its 4 coauthors (but not the journal) retracted the study. You make sure few media report that the data were fabricated and the “study” a fraud. You let people believe the original story: that hydroxychloroquine routinely kills.
10. You ensure federal agencies like FDA and CDC hew to your desired policies. For example, FDA advised use only in hospitalized patients (too late) or in clinical trials (which are limited, are difficult to enroll in, or use excessive doses). As of mid June, FDA now advises patients and doctors to only use the drug in a clinical trial!
Another example: you have FDA make unsubstantiated and false claims, such as: “Hospitalized patients were likely to have greater prospect of benefit (compared to ambulatory patients with mild illness)” and claim the chloroquine drugs have a slow onset of action. If that were really true, they would not be used for acute attacks of malaria or in critically ill patients with Covid. (Disclosure: I once dosed myself with chloroquine for an acute attack of P. vivax malaria, and it worked very fast.). Providing no other treatment advice, CDC refers clinicians to the NIH guidelines, discussed below.
11. You make sure to avoid funding/encouraging clinical trials that test drug combinations like hydroxychloroquine with zinc, with azithromycin, or with both, although there is ample clinical evidence that such combinations provide a cumulative benefit to patients.
12. You have federal and UN agencies make false, illogical claims based on models rather than human data. For example, you have the FDA state on June 15 that the dose required to treat Covid is so high it is toxic, after the Recovery and Solidarity trials have been exposed for toxic dosing. This scientific double-speak gives some legal cover to the clinical trials that overdosed their patients.
According to Denise Hinton, RN, the FDA’s Chief Scientist, or a clumsy FDA wordsmith:
”Under the assumption that in vivo cellular accumulation is similar to that from the in vitro cell-based assays, the calculated free lung concentrations that would result from the EUA suggested dosing regimens are well below the in vitro EC50/EC90 values, making the antiviral effect against SARS-CoV-2 not likely achievable with the dosing regimens recommended in the EUA. The substantial increase in dosing that would be needed to increase the likelihood of an antiviral effect would not be acceptable due to toxicity concerns.”
13. You have a WHO report claim toxic doses are needed. This of course is nonsense since
a) CDC researchers showed strong effects against SARS-1 at safely achievable concentrations,
b) the drug at normal doses is being tested in over 30 different medical conditions (see clinicaltrials.gov), and
c) reports from many different countries say that the drug is effective for Covid-19 at normal doses, while
a high dose chloroquine treatment arm was halted in Brazil and a preprint of the study was posted April 11, after finding the toxic effects were causing ventricular arrhythmias and deaths.
- Toxicity was noted after only 3 days of treatment, during which 3.6 grams of chloroquine were administered. But the Solidarity (3.2 grams of hydroxychloroquine in 3 days), Recovery (3.6 grams of hydroxychloroquine in 3 days) and REMAP-Covid trials (3.6 grams of hydroxychloroquine in 3 days) continued overdoing patients until June, despite Brazil’s evidence of deaths by overdose.
- Tellingly, JAMA editor Gordon Rubenfeld wrote about the Brazilian study, “if you are prescribing HCQ after these JAMA results, do yourself and your defense lawyer a favor. Document in your medical record that you informed the patient of the potential risks of HCQ including sudden death and its benefits (???).”
14. You create an NIH Guideline committee for Covid treatment recommendations, in which 16 members have or had financial entanglements with Gilead, maker of Remdesivir. The members were appointed by the CoChairs. Two of the three CoChairs are themselves financially entangled with Gilead. Are you surprised that their guidelines recommend specifically against the use of hydroxychloroquine and in favor of Remdesivir, and that they deem this the new “standard of care”?
15. You frighten doctors so they don’t prescribe hydroxychloroquine, if prescribing it is even allowed in their jurisdiction, because prescribing outside the “standard of care” leaves them open to malpractice lawsuits. You further tell them (through the FDA) they need to monitor a variety of lab parameters and EKG when using the drug, although this was never advised before, which makes it very difficult to use the drug in outpatients. You have the European Medicines Agency issue similar warnings.
16. You manage to control the conduct of most trials around the world by designing the WHO-managed Solidarity trials, currently conducted in 35 countries. WHO halted hydroxychloroquine clinical trials around the world, twice.
The first time, May 25, WHO claimed it was in response to the (fraudulent) Lancet study.
The second time, June 17, WHO claimed the stop was in response to the Recovery trial results.
Recovery used highly toxic doses of hydroxychloroquine in over 1500 patients, of whom 396 died.
You stop the trial before the data safety monitoring board has looked at your data, a move that is unlikely to be consistent with trial protocol. WHO’s trial in over 400 hospitals overdosed patients with 2.0 g hydroxychloroquine in the first 24 hours.
WHO’s trial in over 400 hospitals was unlikely to provide useful results, as it too overdosed patients with hydroxychloroquine. The trial was halted days after the toxic doses were exposed.
17. You have the WHO pressure governments to stop doctors prescribing hydroxychloroquine.
18. You have the WHO pressure professional societies to stop doctors prescribing hydroxychloroquine.
19. You make sure that the most-consulted medical encyclopedia, UptoDate, provides bad guidance to physicians, advising them to restrict hydroxychloroquine to only patients in clinical trials, citing the above sources of information.

Anthony Fauci, MD
20. You have the head of the Coronavirus Task Force, Dr. Tony Fauci, insist the drug cannot be used in the absence of strong evidence… while he insisted exactly the opposite in the case of the MERS coronavirus outbreak several years ago, when he recommended an untested drug combination for use… which had been developed for that purpose by his agency.
And while he was bemoaning the lack of evidence, he was refusing to pay for trials to study hydroxychloroquine. And he was changing the goalposts on the Remdesivir trial, not once but twice, to make Remdesivir show just a tiny bit of benefit, but no mortality benefit. And don’t forget, Fauci was thrilled to sponsor a trial of a Covid vaccine in humans before there was any data from animal trials. So much for requiring high quality evidence before risking use of drugs and vaccines in humans!
21. You convince the public that the crisis will be long-lasting. You have the 2nd richest man in the world, and biggest funder of the WHO, Bill Gates, keep repeating to the media megaphone that we cannot go back to normal until there is a vaccine. (The Gates Foundation helped design the WHO clinical trials, and Gates is heavily invested in pharmaceuticals and vaccines.)

Bill Gates
- You have CDC (with help from FDA) prevent the purchase of coronavirus test kits from Germany, China, WHO, etc, and fail to produce a valid test kit themselves. The result was that during January and February, US cases could not be reliably identified, and for several months thereafter insufficient and unreliable test kits made it impossible to track the epidemic and stop the spread.
- You have trusted medical spokesmen lie to the public about the pandemic’s severity, so precautions weren’t taken when they might have been more effective and less long-lasting. Congress was repeatedly briefed about the pandemic in January and February, which scared several Congress members enough that they sold off large amounts of stock, risking insider trading charges. Senator Burr is one of them, currently under investigation for major stock sales on February 13.
Yet Dr. Fauci told USA Today on February 17 that Americans should worry more about the flu than about coronavirus, the danger of which was “just miniscule.” Then on February 28, Drs. Fauci and Robert Redfield (CDC Director) wrote in the New England Journal :
“… the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively.”
 You destroy the reputation of respected physicians who stand in your way. Professor Didier Raoult and his team in Marseille have used hydroxychloroquine on over 4,000 patients, reporting a mortality rate of about 0.8%. (The mortality rate of patients given hydroxychloroquine in the Recovery trial was 25.7%.) Raoult is very famous for discovering over 100 different microorganisms, and finding the long-sought cause of Whipple’s Disease. With this reputation, Raoult apparently thought he could treat patients as he saw fit, which he has done, under great duress. Raoult was featured in a New York Times Magazine article, with his photo on the cover, May 12, 2020. After describing his accomplishments, the Times very unfavorably discussed his personality, producing a detailed hit piece. He is now considered an unreliable crank in the US.
You destroy the reputation of respected physicians who stand in your way. Professor Didier Raoult and his team in Marseille have used hydroxychloroquine on over 4,000 patients, reporting a mortality rate of about 0.8%. (The mortality rate of patients given hydroxychloroquine in the Recovery trial was 25.7%.) Raoult is very famous for discovering over 100 different microorganisms, and finding the long-sought cause of Whipple’s Disease. With this reputation, Raoult apparently thought he could treat patients as he saw fit, which he has done, under great duress. Raoult was featured in a New York Times Magazine article, with his photo on the cover, May 12, 2020. After describing his accomplishments, the Times very unfavorably discussed his personality, producing a detailed hit piece. He is now considered an unreliable crank in the US.
- You have social media platforms ban content that does not agree with the desired narrative. As YouTube CEO and ex-wife of Google founder Sergey Brin, Susan Wojcicki said,
“YouTube will ban any content containing medical advice that contradicts World Health Organisation (WHO) coronavirus recommendations. Anything that would go against World Health Organisation recommendations would be a violation of our policy.”
- When your clinical trials are criticized for overdosing patients, you have Oxford-affiliated, Wellcome Trust-supported scientists at Mahidol University publish papers (a literature review with modeling and a modeling study) purporting to show that the doses used were not toxic. You develop a new method to measure hydroxychloroquine in a handful of Recovery patients who were not poisoned. However, there are 2 problems you forgot with this approach:
- The Brazilian data, including 16 deaths, extensive clinical information and documented ventricular arrhythmias, are much more valuable than theoretical models of what might be happening in the body.
- Either the drug is too toxic to use for a life-threatening disease, or even extremely high doses are safe. You can’t have it both ways.
Oxford is the institution running the Recovery trial, and invented a Covid vaccine that already has 400 million doses on order. The Wellcome Trust funded the Recovery trial.
- You change your trial’s primary outcome measures after the trials have started, in order to prevent detection of drug-induced deaths (Recovery) or to make your drug appear to have efficacy (NIAID Remdesivir trial).
- You stop manufacturers from supplying the drug. Shortly after the fraudulent Lancet paper came out, Sanofi announced it would no longer supply the drug for use with Covid, and would halt its two hydroxychloroquine clinical trials. One of the cancelled Sanofi trials was expected to test 210 outpatients early in the course of disease. The trial remains suspended at the time of writing, while the Lancet paper was retracted 13 days after publication.
- You surely don’t want a trial of hydroxychloroquine treatment early in the disease, since it might show an excellent effect.
FDA Executive Officer: “Almost a Billion Dollars a Year Going into FDA’s Budget from the People we Regulate”
Health Impact News | February 17, 2022
Project Veritas published Part Two of its series on the FDA on Wednesday night which featured FDA Executive Officer, Christopher Cole, speaking about the inner workings of the agency including the FDA’s conflicts of interest, overspending, and why it’s hard for those within the agency to speak out on such abuses.
https://www.bitchute.com/video/WT4CuKhKW6N9/
In the footage, Cole talks about the impact that pharmaceutical companies have on the agency including the process for approving drugs.
“A long time ago, Congress approved user fees for [the] FDA. Basically, we charge the industry millions of dollars in order to hire more drug reviewers and vaccine reviewers, which will speed up the approval process, so they make more money,” Cole says in the hidden camera footage.
He then reveals that the FDA tones down the impact that these user fees have on the agency’s operations because, “they’re dependent on the drug companies, and the vaccine companies and these other companies for their agency to operate.”
The incendiary footage, which features Cole talking about how the additional money the FDA brings in “gets banked” to be spent on “whatever you can, whether it’s right or wrong,’’ also features Cole discussing reasons why it’s difficult for anyone in government to speak out about practices he sees as “probably excessive.”
“I don’t think there’s enough people saying they’re, like, ‘Look, that’s fine, but that’s not right. So, we’re not going to charge that.’ You don’t want to be that person. You’re not going to have a long shelf life in the agency if you’re always that person,” Cole said.
“There’s not an incentive to speak out in government, surprisingly. You would think there would be, but there’s not. It’s better just to just not say anything and just ignore it. The whistleblower, well, it’s high-profile whistleblower statutes and everything, that’s kind of ridiculous,” Cole said before adding “it’s better to just stay quiet and accept.”
Cole’s LinkedIn page lists him as an Executive Officer within the agency’s Countermeasures Initiatives, which plays a critical role in ensuring that drugs, vaccines, and other measures to counter infectious diseases and viruses are safe. He made these revelations on a hidden camera to an undercover Project Veritas reporter.
A spokesperson for FDA issued a statement yesterday saying, “The person purportedly in the video does not work on vaccine matters and does not represent the views of the FDA.”
This statement appears to contradict a phone call released Wednesday afternoon by Project Veritas wherein Cole reiterated, during the conversation with Project Veritas Founder and CEO, James O’Keefe, that he is “a manager in the office that helps oversee the approval of the COVID vaccines for emergency approval.”
See also: Part One
FDA official reveals Biden plan for Covid jabs — Project Veritas
Even toddlers will eventually be required to get annual Covid-19 jabs, an FDA official said in the undercover clip

© Project Veritas
RT | February 16, 2022
Investigative outlet Project Veritas has released footage of a Food and Drug Administration (FDA) executive claiming that annual Covid-19 vaccine jabs are on the way, even for children under five.
In part one of a two-part undercover video series, Christopher Cole, an executive officer with the FDA and head of the agency’s Countermeasures Initiatives, told a Project Veritas reporter he is involved in the “approval process for the various” Covid vaccines. In the video released on Tuesday, Cole claimed more jabs are in the pipeline for everyone and acknowledged the “money incentive” for companies like Pfizer to promote more vaccination.
“It’ll be a recurring fountain of revenue. It might not be that much initially, but it’ll be recurring… if they can get every person required at an annual vaccine, that is a recurring return of money going into their company,” Cole said of vaccine manufacturers. At another point in the footage, the FDA official also admitted that the very companies the FDA regulates dump “almost a billion dollars a year” into its budget.
Cole said even toddlers would be included in this annual shot requirement, though he conceded that there hasn’t been enough testing on the long-term effects of the vaccines on various groups, including young children and pregnant women. Asked how he knew such a mandate could be coming, he said: “Just from everything I’ve heard, [the FDA] are not going to not approve it.”
The annual jab would be “just like the flu shot,” Cole said, and required as the effectiveness of vaccines “wanes.”
The FDA released a statement responding to Veritas’ video on Wednesday, saying Cole “does not work on vaccine matters” and “does not represent the views of the FDA.”
US President Joe Biden has not endorsed an annual vaccine jab, but Cole said the president “wants to inoculate as many people as possible.” Biden’s health officials have also floated the idea of regular jabs. White House health adviser Dr. Anthony Fauci has been open in recent talks to the idea of booster shots being needed regularly, though he has not endorsed annual shots for everyone.
“It will depend on who you are,” he told the Financial Times last week. “But if you are a normal, healthy, 30-year-old person with no underlying conditions, you might need a booster only every four or five years.”
ICAN-Obtained Email Shows Alliance Between White House, Facebook, and Pharma
Informed Consent Action Network | February 14, 2022
A White House email, obtained on behalf of ICAN, shows Facebook, Merck, and the CDC Foundation, whose corporate partners includes Pfizer, have formed an alliance “to use social media and digital platforms to build confidence in and drive uptake of vaccines.” No conflict there.
On August 12, 2021, ICAN, through its attorneys, submitted a Freedom of Information Act request for communications between White House staff and Facebook, Google, and YouTube. In response to this request, ICAN received a June 15, 2021 email sent by Facebook’s then-Public Policy Manager, Nkechi “Payton” Iheme, to several White House employees.
In it, Iheme announces a new initiative, the “Alliance for Advancing Health Care,” between Facebook and several major companies and organizations, including Merck, the Vaccine Confidence Project, the Sabin Vaccine Institute, and the CDC Foundation. Significantly, one of the CDC Foundation’s corporate partners is Pfizer. In the email, Iheme explains that the Alliance is “focused on advancing public understanding of how social media and behavioral sciences can be leveraged to improve the health of communities around the world” and states that its first project is to “provide grants to researchers and organizations for projects that explore how to use social media and digital platforms to build confidence in and drive uptake of vaccines.” Facebook announced this new initiative on June 9, 2021 here.
The conflict of interest is astonishing. This email shows without a doubt that, through the CDC Foundation created “to support the [CDC’s] work,” the federal government, which is in charge of ensuring the safety of vaccines, has teamed up with Big Pharma and Big Tech to push a liability-free product on the world, while attempting to stomp out anyone who questions this arrangement.
Just as the pharmaceutical companies will never rest when it comes to promoting and selling their vaccine products, and the federal government will not rest in its efforts to assist them, we will never rest in exposing the truth regarding these products or in demanding full transparency and full informed consent for any and all vaccines.
Giant Ukrainian US lobbying campaign revealed
RT | February 13, 2022
Ukrainian lobbyists contacted US congressional offices, think tanks, and media figures over 10,000 times last year, according to an analysis of Foreign Agents Registration Act (FARA) filings reported by the Quincy Institute for Responsible Statecraft on Friday.
The Quincy report pointed to the “extraordinary” scale of Ukraine’s lobbying campaign, noting that the lobbying efforts of Saudi Arabia – known as one of the largest foreign lobbies in Washington DC – pales in comparison.
According to the report, most of Kiev’s persuasive efforts focused on members of Congress, who were deluged with over 8,000 contacts – emails, phone calls, and meetings – in an effort to convince them of the need to block the Nord Stream 2 pipeline, among other issues.
The Ukrainian Federation of Employers of the Oil and Gas Industry (UFEOGI), the country’s largest energy trade group, would reportedly cite Ukraine’s PM, arguing that the pipeline was “no less an existential threat” to Ukraine’s “security and democracy” than “Russian troops on the border.” The pipeline, which is completed but still has to receive the green light from German regulators, would allow Russia to export gas directly to Europe without having to pay Kiev billions for the transfer of gas.
UFEOGI lobbyists apparently centered their efforts on Senator Ted Cruz (R-Texas), who took just several days to channel the Ukrainian PM on social media. In his own message, Cruz likewise referred to the Russian pipeline as an “existential threat.”
The trade group also sought to reach out to senators who had previously backed legislation to thwart the completion of the pipeline, including several members of the Foreign Relations Committee with a history of anti-Russian votes. Cruz, Tom Cotton (R-Arkansas), John Barrasso (R-Wyoming), Ron Johnson (R-Wisconsin), and Jeanne Shaheen (D-New Hampshire) were all contacted at least 100 times last year, with some of these contacts resulting in their staffers meeting directly with Ukrainian energy lobbyists, the report claims.
The bill proposed by Cruz would have imposed bans on doing business with US companies for those involved with the Nord Stream 2 project, in addition to travel restrictions and asset freezes. It failed to pass, however.
A separate legislative proposal, put forth by Senator Bob Menendez (D-New Jersey) and dubbed “the mother of all sanctions,” would punish senior Russian officials and banks in the event of an invasion of Ukraine. The Quincy report noted that one of Menendez’s former staffers, Brittany Beaulieu, now represents UFEOGI, as well as the ‘Civil Movement for a Just Ukraine’.
Apart from the US lawmakers, Ukrainian lobbyists also reportedly courted pro-NATO think tank the Atlantic Council, contacting it hundreds of times. The report noted that one of the richest men in Ukraine, Victor Pinchuk, is also one of the Atlantic Council’s international advisers, while his foundation is a major contributor to the think tank.
Ukrainian lobbyists also targeted the Heritage Foundation, which has been advocating selling more US weapons to Ukraine and ramping up US financial assistance to Kiev. The lobbyists reached out 180 times to high-ranking figures in the organization, including its VP, throughout 2021, according to the report.
The lobbyists also did not overlook the US media, contacting the Wall Street Journal’s newsroom at least 147 times last year, the report said, citing Quincy’s analysis of the interactions.
Russia has repeatedly denied plans to invade its neighbor, dismissing reports to the contrary as fake news. US media outlets, nevertheless, have attempted to predict the outbreak of hostilities down to the very day, citing anonymous government sources. Numerous US officials have argued that the invasion was looming, with National Security Advisor Jake Sullivan saying on Friday that it could begin “any time.”
On Saturday, however, Ukrainian President Volodymyr Zelensky called on the Americans to share the evidence they supposedly have of Russia’s intentions after having previously warned that reports of an imminent war risk destabilizing his country.
Telling the truth in the age of sponsored science why so many scientific studies refute their own conclusions
el gato malo – bad cattitude – february 13, 2022
in the age of government sponsored science driven by grants, sinecure, and sponsorship, scientists face a difficult set of choices.
they must, if they wish to continue receiving the largess of the gold-givers toe the party line of state or commercially sponsored science. he who has paid the piper demands to call the tune and producing work that does not suit “the narrative” is career suicide. your funding will dry up. so may your position, your prospects for advancement, and even your tenure. you will not be asked to join committees, interviewed for articles, citied, or supported. you may be outright attacked. i discuss this in more depth HERE.
but scientists also face another constraint: they need to be accurate. they need to run good experiments, collect good data, and relay it faithfully. if they do not, they will get called out and revealed as incompetents or frauds. this too will end one’s career as it means that not only are you doing no useful work (apart from to propogandists) but will reveal that you have sold out integrity for lucre and that is the end of peers taking you seriously. you play for team lysenko now.
the need to thread this needle and appease and please both demands has led to an odd practice:
many times, the claims made in the abstract or in the conclusions are not supported by the actual data.
i know this sounds a little bizarre, but as someone who reads perhaps 1000 such papers a year, allow me to assure you, it is stunningly common in any politically loaded sphere. (and you would be amazed how many are politically loaded. it need not be government pushing it. watching geneticists tie their conclusions in knots to claim that you can breed horses for speed and endurance or dogs for intelligence but that of course there is no such thing as eugenics in humans because that would be unspeakable despite your having just proved that there is in fact, eugenics in humans is really quite something. they go to astounding lengths in the introductions of their books to disavow what they are about to prove.)
this odd compromise sort of works, but mostly, it doesn’t.
it gives those who fund studies and the journals who curate them for ideological purity their bone. the abstract says “X means Y.” this is what they want for the press releases and for waving around.
it also puts the actual data out into the world. this is what researchers, both those who did the work and those who will read it in detail, actually need. they can see the facts and will not be gulled in by the claims in the conclusion as they are adept at drawing their own conclusions.
this leads to the weird outcome of the public and the politicians frequently having one idea about what a study says and the experts in the field having more or less the opposite take.
the “experts” all know what the data means and why they are not allowed to say it. it works a bit like the foils used by renaissance dialogue writers to ape at being fools while presenting the actual case being made while the “authorities” presented the “narrative” and were made fools of by those able to read between the lines.
in the age of the internet, this sets up a bizarre and deeply frustrating conflict: those who can and do really read studies are constantly having to pick them apart and explain to the “google and spam” crowd who just selectively confirm their biases and skim the lead paragraph of a study why the study they just cited does not, in fact, say what they are claiming it does.
and, of course, trying to convince someone that the authors deliberately misstated the facts in the summary is like trying to teach a new trick to the very oldest of dogs. they are just not having it.
this has created a rancorous and dangerously stupid level of debate and an impossible burden for any one individual to carry. it takes 10 seconds to search, skim, and spam with a study you never read and start yelling “peer review!” over and over as if that means something.
it can take hours to pick the study apart and see if it really does support the conclusions stated in the summary and then hours more to convince someone who has not even read it (and probably does not know how). that’s unwinnable. it’s like sisyphus getting and additional rock to push back up the hill every time he reaches the top. pretty soon it’s 20 boulders and nothing is going anywhere.
fortunately, the internet age has produced a large group of folks interested in picking these studies apart and publishing their takes. and we form communities and help one another. so no one has to do ALL the work when the CDC publishes yet more self refuting “wave around” data.
this is, in fact, what real peer review is. it’s supposed to be hostile and to pick holes.
the upshot here is that you should be very careful taking studies you have not actually read at face value.
you need to read them. thoroughly. waving them around as if you did when you have not is a recipe for being wrong.
let’s take a simple and straightforward recent example:

this article is being used to push boosters. this is because the authors said this:

i have not spoken to them. perhaps they believe this, perhaps they do not but felt they had to say it or be pariahs. i have no special insight there. but i can read data.
so let’s see what the data says.
this was a big study, but also a retrospective study with post facto matching. the matching was by age, sex, and municipality. it is tainted by the ever present “we counted no one as vaccinated until 14 days post dose 2” issue which will inevitably deeply favor vaccine efficacy through a mathematical rig job (especially in the short run) and can even produce it from zero VE and looks to have had large effects in canadian data.
so we have some ingrained bayesian issues with our cohorts that may inject serious bias toward making vaccines look effective.
the data itself was rendered quite challenging to read. (heavy text, few graphics)
it was also truncated in a somewhat misleading fashion.
if you read it closely, you’ll see that even the longest follow ups on infection data were lumped after 210 days, several were 180 (before it really gets bad) others were 120.
this is just typical bayesian datacrime and presentation bias as we’ve seen so many times before. and it does not really speak to the interesting issue of “are the vaccines preventing severity?”
this is, in fact, omitted from the study. but they did collect the data, they just made it REALLY difficult to find. you need to go HERE to the supplemental materials page. you then need to download the actual PDF as the data is not on the webpage. then you need to go to the very last page of that supplement.
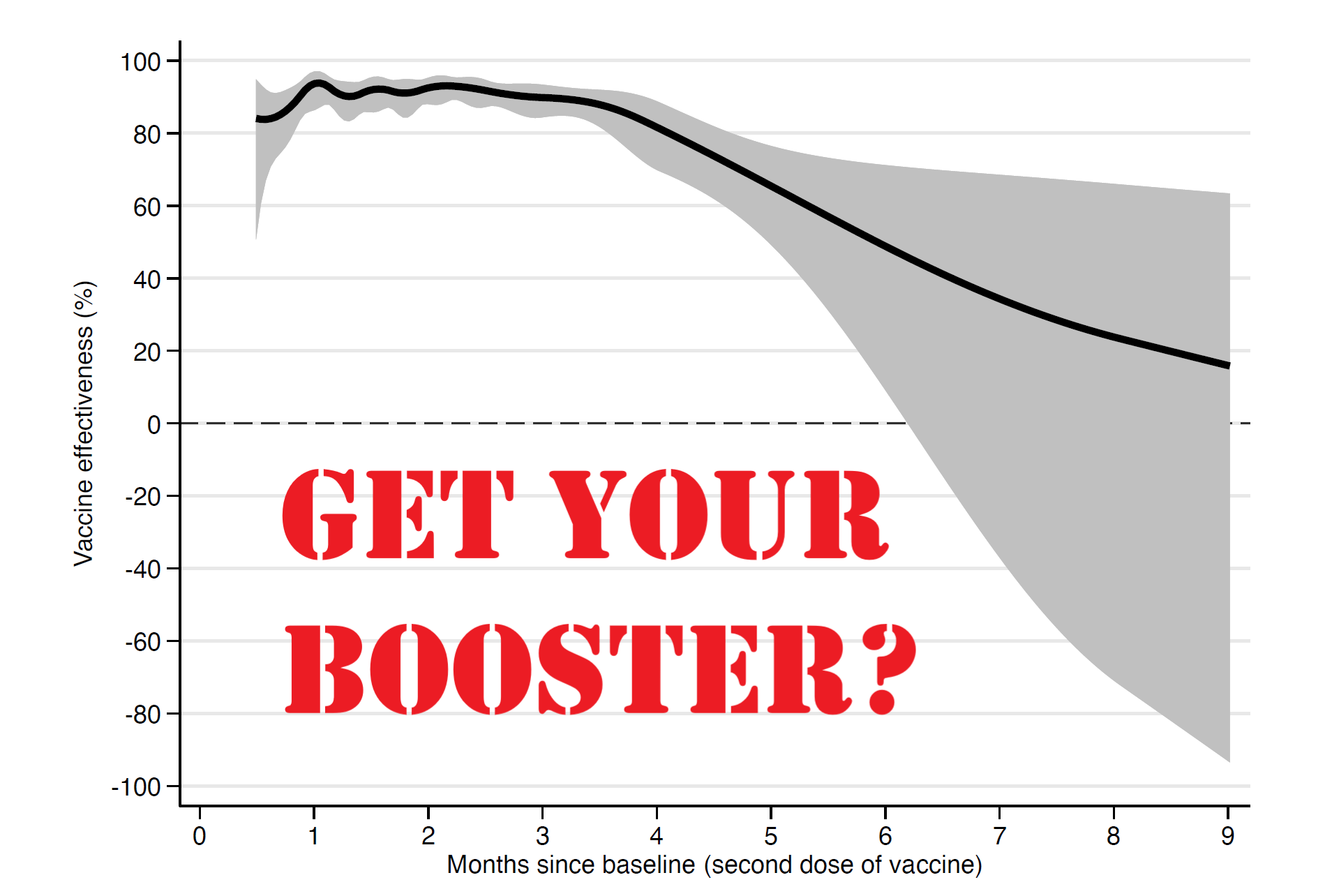
those who do so (and i’m guessing we’re down to a very few folks by then) will be rewarded with this graph:

and this one has profound and powerful implications.
- it shows that efficacy against severe outcomes like hospitalization and death also wanes very rapidly
- it shows that this efficacy keeps waning over time
- it shows that it could easily be strongly negative based on the huge downside bias to the error range (gray shaded area)
- and it shows that this data is of very low quality in terms of error magnitude.
at 9 months, midline expectation is ~15% reduction. (i’m eyeballing) but look at the confidence interval: it runs from (ballpark) +63% to -90%. that is not a useful range upon which to base anything. it implies that there is a very strong chance that vaccination is associated with greatly increased risk of severe outcomes for a great many people.
this pattern implies that boosters are likely, at best, a treadmill that will need constant refreshing, likely 3X a year or so, if you want to sustain efficacy. vaccine fade after 4 months degrades rapidly. (and frankly, the first 4 could well be an illusory halo generated by the dose 2 +14 vaccinated definition as linked above)
given the adverse events profile and the lack of severity of omicron this seems a truly odious proposition that looks likely to fail for most people on any sort or risk/benefit analysis. it is telling that the researchers here did not even attempt to take risk reward into account before claiming:
“The results strengthen the evidence-based rationale for administration of a third vaccine dose as a booster.”
what is also telling is the other part of the data required to make this claim:
do boosters work? do they refresh clinical immunity and mitigate severity? could they ever have done so and is this data even relevant with the emergence of omicron that seems to be at least an escape variant and far more likely a full blown hoskins effect/OAS variant that is enhanced, not mitigated by the vaccines.
because the evidence there looks quite persuasive that they do not.
note that all this data is from before oct 4th 2021, so it has no omicron impact whatsoever in it. claiming it bolsters the case for boosters without presenting evidence of booster efficacy on this new variant makes their claim feel like a rote bolt on, placed there to mollify and placate patrons and authorities.
there is absolutely no data here to validate that point.
the study does not even speak to the data that would be needed to make such a claim.
“efficacy wanes, so boost” is not a valid argument unless we know that boosters work, yet any evidence that boosters actually do anything to help is absent and all past data shows such rapid fade on efficacy vs severity as to make boosters a poor appearing proposition.
there is no data whatsoever on the new variant.
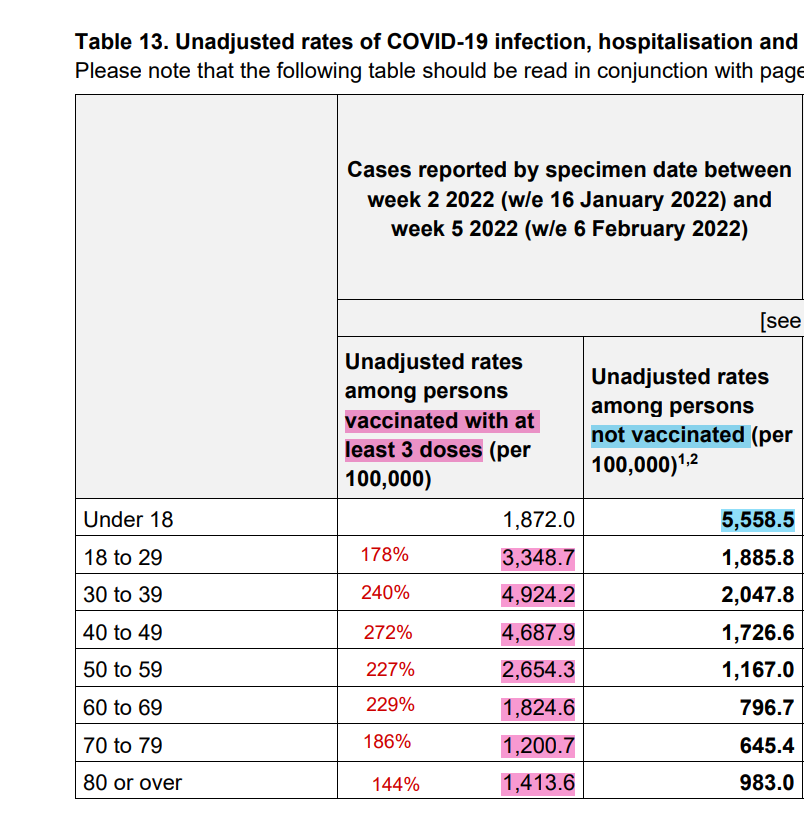
and boosters are sure not seeming to help in the UK. omi is driving rates of infection in the boosted at roughly double the rate of the unvaxxed.
the swedish study uses possibly irrelevant data and not only fails to prove out the ostensible interpretation, but winds up far more consistent with the conclusion that boosters are a waste of time and will provide ephemeral, at best, protection.
having seen this, go back and read the “interpretation” again.
now do you see my point about “the abstract says one thing while the data says another?”
i mean, they literally buried the lede at the very end of a hard to find supplement. it’s like putting the actual object of a video game inside of an easter egg.
most vexing, this easter egg also shows that vaccines may be making immunity to severe covid outcomes significantly worse.
call me mister suspicious, but i have a hunch that’s WHY they put it there.
let’s explore that a bit further:
what would be REALLY interesting is to see how this population distribution looks.
if it barbells then we likely have a serious confound going on. we really have no idea what the prior incidence of covid was in those who got vaccinated. one could expect it to be quite meaningful.
if vaccines look like they are working well in some and are strongly negative in others with not much in the middle (this is suggested but not proven by the skew in the confidence interval) then i would posit that the most likely explanation is that what looks like VE is actually naturally acquired immunity.
if you had covid then got vaxxed, vaccines look like they work, especially as the high risk groups got vaxxed more and these same groups likely had higher risk of prior infection. this gets magnified by the 2 week worry window of TLR suppression post vaccination that results in well documented decreases in immune function and a doubling of the rate of covid contraction in that period vs unvaxxed.
but if you got vaxxed without having had covid, it could be acting as an immunosuppressant or driving hoskins effect/OAS antigenic fixation that makes you more vulnerable.
this, along with all cause deaths in vaxxed vs unvaxxed measured from the moment you got your first jab is some data i’d really like to see.
it’s continuing non-availability certainly frustrating and likely telling. this data absolutely exists.
why we are not getting to see it is fast becoming a question too big to ignore.
Featured Video

Iran Walks Out On Peace Deal Due To Trump’s Threats
or go to
Aletho News Archives – Video-Images
From the Archives
Neocons confess: “We did 9/11-anthrax”
By Kevin Barrett | Press TV | September 6, 2014
As the 13th anniversary of the crimes of September, 2001 approaches, the neoconservatives are shrieking from the rooftops – and effectively confessing that they were the real perpetrators of the 9/11-Anthrax false flag operation. (The neocons, you may recall, openly called for a “new Pearl Harbor” in September, 2000 – and got one exactly one year later.)
Every year at this time, the neocons orchestrate and hype a series of public relations stunts designed to magnify fears of “radical Islam” and reinforce their crumbling 9/11-Anthrax cover story. But this year’s propaganda campaign is so extreme that it represents a tacit confession: The neocons know that the truth about the 9/11-Anthrax operation is slowly closing in on them; so they are over-reacting by desperately trying to stoke the dying embers of the so-called War on Terror, in order to maintain the myth that Muslims (rather than neoconservative Zionists) attacked America in the autumn of 2001.
When a hysterical person exhibits guilty demeanor by trying too hard to blame a crime on someone else, that person is almost certainly the real perpetrator. As the neocons try much too hard to blame Islam for 9/11 and “terrorism” in general, their hysteria inadvertently reveals their own culpability. Like Shakespeare’s Lady MacBeth, the neoconservative movement has blood on its hands and “doth protest too much.” … continue
Blog Roll
 Aletho News
Aletho News- IRAN WALKS OUT ON PEACE DEAL DUE TO TRUMP’S THREATS – w/ Prof. Seyed Mohammad Marandi
- Moderna’s mRNA Flu Vaccine Gets Unanimous Thumbs-Up Despite Risks, Low Efficacy
- UK Speech Regulator’s Telegram Questions Point Toward Private Chats
- Cuban FM blasts Rubio for ‘chronically lying’ about US fuel blockade
- Al-Jazeera demands punishment for Israeli officials following latest assassination of cameraman
- Iran opens hundreds of legal cases over US, Israeli aggression: Prosecutor general
- Iran delegation protests Trump’s threat at Switzerland talks, weighs ‘proper’ response: Source
- Terms of US capitulation to Iran presage new era for the region
- Strategic Oil Reserve Nears Collapse… US Must Choose: Guns or Butter
- The Story the Media — and the Government — Don’t Want You to Hear
- If Americans Knew
- JNS Policy Summit to kick off in Israel
- Fatalities From Israel’s Vast Gaza Genocide Deliberately Undercounted
- ‘Reproductive genocide’ in Gaza; death toll in Lebanon tops 4,000 (during a ceasefire) – Daily Update
- Israelis Invaded Lebanon And Then Cried Victim When Their Soldiers Got Killed
- FARA Docs: Israel is Spying On Millions Of Christian Americans In Their Churches
- Why US presidents from both parties end up cursing Benjamin Netanyahu
- Israel Asked Facebook to Censor Iran War Content, Internal Documents Show
- Deaths in Gaza undercounted, possibly by 100s of thousands; “Psychopath” Ben-Gvir talks trash – Daily Update
- UNICEF: “Trauma is woven into the very fabric of childhood in Gaza”
- 15 articles a day: The extent of the Israeli army’s media interference
- No Tricks Zone
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
