Children aged between five and 11 should get a Covid-19 jab only if there is a “high risk” of severe infection for them or for someone in their inner circle, Finland’s health watchdog has said.
Vaccination for all children aged between five and 11 cannot be recommended until there is more information available on the vaccination safety for this age group, including rare side effects, Finland’s Institute for Health and Welfare (THL) said in a statement last week, adding that relevant government decrees should be amended before a general vaccination campaign for young children could be launched.
So far, only those facing an acute risk of severe infection or who have “severely immunocompromised people” within their inner circle should get a jab, the THL said. It added that a vaccination campaign for children could start early next year provided sufficient evidence for the jabs’ safety is there.
“The main reason THL does not recommend vaccinations now for all children aged 5 to 11 is their own low incidence of the disease. Infection in children of this age is usually mild and severe symptoms are very rare, compared to other diseases that have been prevented by vaccinations,” said Hanna Nohynek, THL’s chief physician.
The health watchdog believes that vaccination of children “does not significantly slow down the epidemic” in its current form. “If a society wants to influence the course of the epidemic by vaccinating children, and … benefits are small, safety information is even more important,” Nohynek explained.
In Finland, just about 5% of children aged between five and 11 were diagnosed with Covid-19 by the end of November 2021. Only 33 children have been treated in a hospital since the start of the pandemic, THL said, adding that treatment courses lasted just one or two days on average. All vaccinations, including those against Covid-19, are voluntary when it comes to children, it added.
December 6, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine, Finland |
Leave a comment
Here I am on vitamins again. I don’t wish to give the impression that all I care about is vitamins. However, I have been thinking about them recently for various reasons.
The first thing to say is that I do find it slightly strange that we have substances which are absolutely essential for life, that we must eat., because our bodies cannot make them. It seems a design flaw. I want my money back.
Added to this absolute reliance on them, we do not get any hint that we are running out. If we become dehydrated, we feel thirsty, and we drink. If our energy supplies are running down, we feel hungry and we eat.
On the other hand, if our Vitamin B12 supplies are becoming perilously low – we might end up feeling bloody awful. In the final stages we could end up paralyzed, then dead, without knowing why. Vitamin B12 is essential for the health of neurones (amongst other things). But there is nothing that triggers our desire to forage around for foodstuffs rich in vitamin B12. Supposing we knew what they were anyway.
I presume this means that whilst we were evolving from the primeval soup, there were plenty of vitamins (and minerals) about. We had no need to seek them out specifically, because they were always present in the things we ate. In ample supply? Always …? Of course, it is not just vitamins, there are minerals we need too.
Magnesium
Most people are probably blissfully unaware they need magnesium. If you don’t have enough, how would you know? The first recognisable symptom may be … suddenly dropping dead.
Israel gives us a stark warning of what happens when magnesium goes missing, with no-one noticing. For many years, most of the water supply in Israel has been provided by desalination. This process does not just get rid of salt (NaCl), it also removes the other salts, and minerals, at the same time.
In normal circumstances people get most of the magnesium they need from drinking water. Which means there was clearly a potential for a major deficiency problem building up in Israel. As most of their water contained nothing but pure H20.
Did anyone notice? As in, did anyone say, ‘golly I feel low in magnesium today, I must go and eat a substance high in magnesium…’ Nope. Did anyone die. Yup, they did. As outlined in the paper ‘Association between exposure to desalinated sea water and ischemic heart disease, diabetes mellitus and colorectal cancer; A population-based study in Israel.’ 1
There were possibly as many as 4,000 deaths a year:
‘An estimated 4,000 Israelis die in an average year due to an inadequate amount of magnesium in their bodies – and the amount they get from natural potable water sources is increasingly declining due to the growing desalination of sea water. The figure is 10-fold the death toll from road accidents.’ 2
The population of Israel is just over nine million. The equivalent death rate in the UK would be 30,000 deaths a year, or 180,000 in the US. A silent killer indeed.
Anyway, yes, magnesium is critical stuff. It is extremely important for health, especially heart health. It is required for the correct functioning of the electrical system in your heart, and a low level increases the risk of atrial fibrillation. Here from the paper ‘Low serum magnesium and the development of atrial fibrillation in the community: the Framingham Heart Study.’
‘… individuals in the lowest quartile of serum magnesium were ~50% more likely to develop AF…compared with those in the upper quartiles.’ 3
Unfortunately, despite its importance, we don’t feel magnesium depleted. We do not crave magnesium rich foods – as if we would have any idea what they might be … I certainly don’t. The symptoms of severe deficiency are also non-specific. The first symptom might be that your heart decides to stop beating.
It’s not just Israel. Here from the paper: ‘Subclinical magnesium deficiency: a principal driver of cardiovascular disease and a public health crisis.’
‘Furthermore, because of chronic diseases, medications, decreases in food crop magnesium contents, and the availability of refined and processed foods, the vast majority of people in modern societies are at risk for magnesium deficiency.’ 4
Have you ever heard of any of this? Did you even know you had magnesium in your body – or that it did anything important? I suspect not. However, from the same paper:
‘… magnesium deficiency can lead to serious morbidity and mortality and has been implicated in multiple cardiovascular diseases such as hypertension, cardiomyopathy, cardiac arrhythmia, atherosclerosis, dyslipidaemia and diabetes. Unfortunately, the western diet is often low in magnesium due to the refining and processing of foods, and hypomagnesaemia is often underdiagnosed in hospitalised patients.’4
My advice, take a supplement. Especially if you live in an area with ‘soft’ water – which generally means not many minerals. Doubly especially if you have atrial fibrillation. It might just go away. How much do you need to take? Around 400mg a day is fine.
Back to vitamins – in this case, Vitamin(s) B
The reason for the detour is that I really wanted to make it clear that it is certainly not a given that we routinely get all the essential micro-nutrients we need from our diet.
Modern living, modern food production and farming, modern food processing … have all have a significant impact on what our food, and water, contains.
The lazy mainstream assumption that micronutrient deficiencies simply do not exist is, therefore, wrong. Try looking at Iodine deficiency in Switzerland sometime. In addition, I am extremely dubious that we truly know what the optimal intake of micronutrients may be. The research in this area is sketchy, to say the least.
This, eventually, takes us onto vitamins, more specifically, the B vitamins. There are many of them – eight, in fact.
- B1 (thiamine)
- B2 (riboflavin)
- B3 (niacin)
- B5 (pantothenic acid)
- B6 (pyridoxine)
- B7 (biotin)
- B9 (folate ak.a. folic acid)
- B12 (cobalamin)
The first question that springs to mind is the following. Where are numbers four, eight, ten and eleven? What happened to them? It’s a bit like clotting factors. We have VII, VIII, IX etc. But there is no factor one, or two. Who gets to name things in medicine anyway?
Moving on. My main interest in the B vitamins is that, if you are low in three of them, maybe four of them: three, six, nine and twelve, this can lead to an increased level of a protein in the blood called homocysteine. [I think B6 is more important than B3, but we shall let this go for now].
The reason why this is important is if you have a high level of homocysteine then this is strongly associated with an increased risk of cardiovascular disease. The mechanism of action appears to be that homocysteine is toxic to endothelial cells.
‘Elevated homocysteine (Hc) levels have a well-established and clear causal relationship to epithelial damage leading to coronary artery disease.’ 5
On the other hand, low levels of homocysteine are associated with a lower risk:
‘In observational studies, lower homocysteine levels are associated with lower rates of coronary heart disease and stroke. Folic acid and vitamins B6 and B12 lower homocysteine levels.’[i]
As you may have gathered from that short quote, if you have a high homocysteine level, and you take B vitamins, your homocysteine levels will fall. As confirmed in a study in the American Journal of Clinical Nutrition :
‘Elevated levels of homocysteine is an indication of inadequate folate and vitamin B-12 in the diet, writes lead author Giovanni Ravaglia, a researcher with University Hospital S. Orsola-Malpighi in Bologna, Italy. His paper appears in the March American Journal of Clinical Nutrition….High homocysteine levels can be treated very easily with vitamins, including folate, niacin, and B-12.’ 6
I think the connection between B vitamins, and homocysteine, were first noted by Kilmer McCully. He studied the area in detail at Harvard University. At least he did so for a while, before he was unceremoniously booted out for carrying out research that threatened to undermine the almighty cholesterol hypothesis. A sorry tale, as reported in the New York Times :
‘Thomas N. James, a cardiologist and president of the University of Texas Medical Branch who was also the president of the American Heart Association in 1979 and ’80, is even harsher [regarding the treatment of McCully]. ”It was worse than that you couldn’t get ideas funded that went in other directions than cholesterol,” he says. ”You were intentionally discouraged from pursuing alternative questions. I’ve never dealt with a subject in my life that elicited such an immediate hostile response.”
It took two years for McCully to find a new research job. His children were reaching college age; he and his wife refinanced their house and borrowed from her parents. McCully says that his job search developed a pattern: he would hear of an opening, go for interviews and then the process would grind to a stop. Finally, he heard rumors of what he calls ”poison phone calls” from Harvard. ”It smelled to high heaven,” he says.’
McCully says that when he was interviewed on Canadian television after he left Harvard, he received a call from the public-affairs director of Mass. General. ”He told me to shut up,” McCully recalls. ”He said he didn’t want the names of Harvard and Mass. General associated with my theories.’ 7
And you wonder why researchers are wary of questioning the cholesterol hypothesis? Yes, crushing scientific debate has a long and inglorious history, starting long before COVID19 first appeared over the horizon. In the world of cholesterol, it has been going on for well over sixty years.
Homocysteine, B vitamins and dementia
Now, dear reader, having just focussed on B vitamins, homocysteine and cardiovascular disease, I am going to abruptly change tack. I shall now move away from heart disease to Alzheimer’s disease. The reason for this is straightforward.
As I began to research this area in more detail, it become increasingly clear that there was a worrying association between raised homocysteine, brain damage, and dementia. This certainly attracted my attention. Because I like my brain, and I want to keep it healthy for a long as possible.
I came across papers such as this: ‘Plasma Homocysteine as a Risk Factor for Dementia and Alzheimer’s Disease.’
‘An increased plasma homocysteine level is a strong, independent risk factor for the development of dementia and Alzheimer’s disease.’ 8
There were many more such papers, but you probably get the general idea. Raised homocysteine … Bad.
At this point I already knew that the B vitamins can lower the homocysteine level – if it is high. In addition, B vitamins are well known to have vital functions in the central and peripheral nervous system.
Here, from the paper: ‘B Vitamins in the nervous system: Current knowledge of the biochemical modes of action and synergies of thiamine, pyridoxine, and cobalamin.’
Neurotropic B vitamins play crucial roles as coenzymes and beyond in the nervous system. Particularly vitamin B1 (thiamine), B6 (pyridoxine), and B12 (cobalamin) contribute essentially to the maintenance of a healthy nervous system. Their importance is highlighted by many neurological diseases related to deficiencies in one or more of these vitamins, but they can improve certain neurological conditions even without a (proven) deficiency.’ 9
So, not only do certain B vitamins lower homocysteine levels. A number of them play a critical role in the growth and support of nerve cells, and suchlike.
None of this is exactly news. It has been known for centuries that excess alcohol consumption – which blocks Vitamin B1 absorption from the gut – can cause a specific form of dementia called Korsakoff’s dementia. Because of this, people with alcohol problems are often prescribed high dose vitamin B1 (Thiamine).
Which means that it was never a stretch to suggest that giving people B vitamins might be an extremely good thing if you want to prevent, or delay, the progression of Alzheimer’s/brain shrinkage. Either through the benefits on lowering raised homocysteine, or via the critical functions of B vitamins on the structure and function of the brain.
That, anyway, was the underlying science. But does giving B vitamins actually work? Well researchers at Cambridge University certainly believed it was a splendid idea :
‘In an initial, randomized controlled study on elderly subjects with increased dementia risk, we showed that high-dose B-vitamin treatment (folic acid 0.8 mg, vitamin B6 20 mg, vitamin B12 0.5 mg) slowed shrinkage of the whole brain volume over 2 years.’ 10
In a follow-up study, this group of researchers then found that, in people with raised homocysteine levels, who already had signs of dementia, B-vitamins reduced brain destruction and slowed, even halted, the progression of Alzheimer’s. In their own words, from the paper ‘Preventing Alzheimer’s disease-related gray matter atrophy by B-vitamin treatment’:
‘… we showed that high-dose B-vitamin treatment (folic acid 0.8 mg, vitamin B6 20 mg, vitamin B12 0.5 mg) slowed shrinkage of the whole brain volume over 2 years. Here, we go further by demonstrating that B-vitamin treatment reduces, by as much as seven-fold, the cerebral atrophy in those gray matter (GM) regions specifically vulnerable to the AD (Alzheimer’s Disease) process, including the medial temporal lobe. In the placebo group, higher homocysteine levels at baseline are associated with faster GM atrophy, but this deleterious effect is largely prevented by B-vitamin treatment. We additionally show that the beneficial effect of B vitamins is confined to participants with high homocysteine.’ 11
Yes, it was all looking quite good. By the way, this study came out in 2013.
But then we need to factor in the knowledge that B vitamins are very cheap. Very cheap indeed. In addition, they cannot be patented. Which makes it extremely difficult for any pharmaceutical company to make money from them. You can, of course sell them for a small profit, but pharmaceutical companies need billions to feed the machine. They require unique, patentable, blockbuster drugs. Drugs my precious.
Had any drug shown such a significant effect on brain shrinkage, I am one hundred per cent certain that the finding would have been shouted from the rooftops. We would be looking at a massive blockbuster. Probably the biggest selling drug in the world – ever.
As it was, the research from Cambridge was passed over in virtual silence … I suspect you never heard anything about it. Then, with a certain inevitability, the findings were, effectively squashed.
How was this done?
It was done through the power of the meta-analysis. A meta-analysis is a fancy term describing an attempt to bring together all the relevant trials that have been done in a therapeutic area. In order to construct a ‘meta’ study, or meta-analysis.
They can be a very useful way to bring together all of the relevant research, where there have been a large number of different studies done. In an attempt to establish the definitive answer to a medical question. Does drug x, or intervention y, actually work. If so, what are the true benefits? Assuming that the trials have all showed subtle, or not so subtle, differences in their effects.
Meta-analyses are often treated as though they are the very pinnacle of medical research. Tablets of stone handed down by Gods. In realty, they need to be treated with a very large pinch of salt, and a healthy dose of scepticism.
This is because meta-analyses often ram together studies with very different populations, using different doses of drugs, or vitamins. Or completely different drugs or vitamins, for different lengths of time.
Just to add to the potential messiness, studies can be included that have completely unrelated outcomes. You end up comparing apples and bananas, in order to decide if pomegranates actually work. In computing it would be called garbage in, garbage out – GIGO.
Moving on, in 2014, the year after the Cambridge study, a whole number of different studies on B-vitamins were brought together in a ‘meta-analysis.’ I use the term meta-analysis very loosely here. It was called: ‘Effects of homocysteine lowering with B vitamins on cognitive aging: meta-analysis of 11 trials with cognitive data on 22,000 individuals.’ 12
Sounds good, so far. In fact, the total number of individuals they looked at was 20,431 – which is a lot nearer to twenty thousand than twenty-two thousand. But, hey ho, what’s sixteen hundred or so people between friends? Having said this deliberate figure inflation is an important indication of researchers trying to ‘big up’ their findings – in my book.
Here’s another thing. A number of the studies had absolutely nothing to do with cognitive function … at all. One of the studies included was HOPE-2. Here is the background to the study.
‘In observational studies, lower homocysteine levels are associated with lower rates of coronary heart disease and stroke. Folic acid and vitamins B6 and B12 lower homocysteine levels. We assessed whether supplementation reduced the risk of major cardiovascular events in patients with vascular disease.’ 13
Yes HOPE-2 was a study on cardiovascular disease. It has absolutely nothing to do with Alzheimer’s, or any other form of dementia. The title of HOPE-2 was ‘Homocysteine Lowering with Folic Acid and B Vitamins in Vascular Disease.’ Cognition, or brain function, was not measured. Yet, it was still included in a meta-analysis of ‘11 trials with cognitive data on 22,000 individuals.’ [20,431 individuals, actually].
Moving on, and this is perhaps more mission critical. In only just over seven thousand of the individuals studied did anyone measure cognitive function at the start of the trial and then again, at the end. Leaving aside such studies as HOPE-2 where it was not measured at all. Which, straight off, means that the vast bulk of this meta-analysis is utterly meaningless.
How can you possibly know what happened to anyone’s cognitive state, if you only measured it once? Did it improve, did it worsen – not the faintest. In two thirds of the individuals included in this meta-analysis we have no idea what happened to cognitive function – at all.
It doesn’t stop here. There were others who felt that this was not meta-analyses finest hour:
‘First and foremost, this meta-analysis excluded trials on mild cognitive impairment (MCI) and Alzheimer’s disease. As a possible consequence, most of the trials included in this meta-analysis either did not see any significant cognitive change (between the start and the end of the trial) in the placebo group or did not look at such change.14
Yes, they specifically excluded people with existing cognitive impairment, or Alzheimer’s, which would be, by far, most important group to study. As they actually have the condition you are interested in.
Which leads on to the next obvious problem:
… people included in these trials included in the meta-analysis were healthy and did not show any cognitive decline, whether they received B-vitamin treatment or not. So, B-vitamins could hardly prevent or slow down something not happening in the first place.’ 14
Just to make this point a little clearer, in the minority of studies, where they bothered to measure cognitive function at the start, and also at the end, they found that almost no individuals developed any degree of cognitive impairment – in either group. Not in the treatment group, or the placebo groups. As virtually nothing happened to anyone, nothing could have been proved one way or another.
Attempting to study the progress of dementia, in people who do not have dementia, and who may never get dementia, nor have any signs of cognitive decline … is like doing a blood pressure lowering study on people who do not have a raised blood pressure.
Then, on finding there was no difference in cardiovascular event in either arm of the trial, you proceed to claim that blood pressure lowering does not work. Because there was no difference between those given the drug, and those taking the placebo. Do you think this makes any sense? Answers on a postcard, that should be sent to the Willie Wonka chocolate factory. Care of A.N. Idiot.
Despite begin riddled with fatal flaws, this analysis was greeted as though it was the definitive study. B-vitamins have no effect on cognitive decline, end of. This is what the head of Alzheimer’s Research UK had to say:
‘Although one trial in 2010 showed that for people with high homocysteine, B vitamins had some beneficial effect on the rate of brain shrinkage, this comprehensive review of several trials shows that B vitamins have not been able to slow mental decline as we age, nor are they likely to prevent Alzheimer’s. While the outcome of this new and far-reaching analysis is not what we hoped for, it does underline the need for larger studies to improve certainty around the effects of any treatment.
New and far-reaching analysis. Comprehensive review … ho hum. If I were given the job of marking this meta-analysis, I would hand it back in a rather grumpy fashion. ‘I asked you to look at the benefit of lowering homocysteine, using B-vitamins, in people with cognitive problems, or early-stage Alzheimer’s. Yet, you have not even bothered to look at these groups. In fact, you deliberately excluded them.
In addition, you included trials where the researchers failed to measure mental decline. Added to this, in most of these trials, no-one even had a high homocysteine level to start with, so they cannot – by definition – have had low levels of B-vitamins. So, how could vitamin B supplementation possible have been of any benefit … I am most disappointed. Please try again, and this time READ the brief.’
One of the trials lasted for four months, another for six months. What measurable different in cognitive function can anyone possibly expect to see in those timescales… This was not a flawed meta-analysis. It was simply gibberish.
There was a time when I would have questioned my own sanity in reading a meta-analysis such as this. Surely, I had got it wrong. Researchers would never put together such a steaming pile. If they did, then no-one would publish it. Nowadays I find myself far more in agreement with Drummond Rennie: deputy editor of the Journal of the American Medical Association :
‘There seems to be no study too fragmented, no hypothesis too trivial, no literature citation too biased or too egotistical, no design too warped, no methodology too bungled, no presentation of results too inaccurate, too obscure, and too contradictory, no analysis too self-serving, no argument too circular, no conclusions too trifling or too unjustified, and no grammar and syntax too offensive for a paper to end up in print.’ 15
A famous quote… in certain circles.
As it turns out, this analysis was done by exactly the same people who rule the research world of cholesterol lowering, known as the Cholesterol Treatment Triallists Collaboration (CTT) in Oxford. This paper came under the banner of the ‘B-vitamin treatment triallists collaboration’. Who knew such a group existed? One wonders exactly why they exist? Does the world really require such an organisation?
They sure as hell slammed the door shut on vitamin B/homocysteine research in cognitive function. Which was, some may say, possibly whey they were set up in the first place.
In my opinion, you can either believe the B-vitamin treatment triallists collaboration from Oxford with their meta-analysis. Which some would call complete and utter rubbish. Not me, of course. Personally, I have never seen a more detailed and error free research paper. I can hardly praise it highly enough.
Or, you can believe the Cambridge researchers, who demonstrated a seven-fold reduction in cerebral atrophy with B-vitamins – in those with raised homocysteine levels. The choice is entirely up to you.
1: https://pubmed.ncbi.nlm.nih.gov/29982150/
2: https://www.jpost.com/business-and-innovation/health-and-science/4000-israelis-die-annually-due-to-lack-of-magnesium-479184
3: https://pubmed.ncbi.nlm.nih.gov/23172839/
4: https://openheart.bmj.com/content/5/1/e000668
5: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5359933/#:~:text=Elevated%20homocysteine%20(Hc)%20levels%20have,II%20diabetes%20mellitus%20(T2DM)
6: https://www.webmd.com/alzheimers/news/20030228/elderly-dementia-linked-to-homocysteine#:~:text=A%20new%20study%20suggests%20that,researcher%20with%20University%20Hospital%20S
7: https://www.nytimes.com/1997/08/10/magazine/the-fall-and-rise-of-kilmer-mccully.html
8: https://www.nejm.org/doi/full/10.1056/nejmoa011613
9: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6930825/
10: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3677457/
11: https://pubmed.ncbi.nlm.nih.gov/23690582/
12: https://academic.oup.com/ajcn/article/100/2/657/4576556
13: https://www.nejm.org/doi/full/10.1056/nejmoa060900
14: https://www.alzheimersresearchuk.org/blog/b-vitamins-and-alzheimers-disease/
15: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3005733/
December 6, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular |
Leave a comment
many of you are probably too young to remember the AIDS panic of the 80’s.
but when it came out, the NIH, with tony fauci leading the charge, was getting literally everything wrong.
they pushed a narrative of fear, vilified the infected, interfered with the development and adoption of effective treatments, and completely misrepresented spread and mitigation.
it’s how we wound up with absolute garbage like this ad:

it’s probably pretty jarring to see, but this is because you now have perspective. at the time, A LOT of people believed this. fear of getting AIDS from public toilet seats was a very real thing. fear of getting AIDS from casual contact or sharing dining or cooking facilities was a very real thing. people worried they might be sitting near a gay person on a bus. the “moral majority” of dingbat tele-evangelists thundered about it daily.
and then, as now, one jumped up bureaucrat with no idea what he was talking about was running around like chicken little screaming of falling skies and grandstanding about non-existent risks to children.
the fact that it was literally the same guy who is still at it should deeply embarrass us all.
i urge you to watch the video and hear him, in his own words. because this is who tony fauci was, and he has not gotten better. he’s just become more powerful and more nastily manipulative and narcissistic.

the appalling inaccuracy and vicious othering of the AIDS campaign is still his bread and butter play. it’s what tony does. only the scale and scope of power has changed.
one day, 20 years from now, people will look back on these rushed and slipshod vaccine approvals and mandates for products that are not at all suited to task and claims about masks and lockdowns and feel sick to their stomachs.
they will not be able to believe how such pseudoscience and rapacious world wrecking doctrine not only got foisted upon the world, but accepted and cheer led by it.
they will, in the light of perspective, marvel that the same man who convinced us that our kids would get AIDS from being near a gay teacher was allowed to generate pretext to close the schools to “protect” children from a disease that poses them almost no risk, a disease they do not contract nor spread serious cases of.
they will be appalled by the suggestion that a non-sterilizing vaccine was forced on them even after the fact that the vaccine does not mitigate spread was known and despite a towering and dangerous adverse events profile that rendered it a clearly of negative benefit to cost proposition to the young and healthy.
in short, they’ll feel just like you probably did looking at that AIDS ad.
think very carefully about just who you are choosing to trust here.
these “experts” do not have track records of being correct or even of being honest.
check the date on this:

they told you not only that these vaccines would stop spread, but that they literally changed the definition of “herd immunity” so that it could ONLY be achieved by vaccines.
then the vaccines failed to stop spread, likely made it worse, and they doubled down on “you need to get vaxxed” in spite of this, pivoting to this bizarre new take of “you need to get vaxxed to save hospital space” which, of course, is ALSO not working. now they want boosters. soon it will be “variant boosters.” if you don’t think annual covid shots are coming, you probably fell for the “did you know the word gullible is not in the dictionary?” trick. twice.
this is not “changing your views when new facts arise” this is “finding new justifications for doing the same thing despite the facts being 180 degrees opposite to what you claimed.”
this is not science, it’s scientology.
it’s the same people making the same mess.
isn’t it about time we broke this cycle?
food for thought.
December 6, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular, Video | Covid-19, COVID-19 Vaccine, United States |
Leave a comment
By now, many have seen the recent segment with cardiologist Dr. Aseem Malhotra which aired on GB News last week. Here he is again, this time speaking with Maajid Nawaz on LBC radio about the article in the American Heart Association’s prestigious journal ‘Circulation’. The findings in this study should disturb everyone.
What is stated in this prestigious peer reviewed medical journal ties in with the numerous reports in recent weeks of young healthy people – including many of top-flight athletes – all suddenly suffering from serious cardiac incidents, and in many cases, dying. How many of these casualties are a result of the experimental mRNA COVID-19 vaccines?
In this recent interview with Dr. Malhotra, the so-called “fact checkers” are exposed as mouthpieces of government agencies, the WHO, and a wildly corrupt corporate pharmaceutical cartel determined to promote their experimental mRNA gene therapy jabs at all costs. Who benefits? This informative segment offers some answers to these questions.
December 6, 2021
Posted by aletho |
Full Spectrum Dominance, Science and Pseudo-Science, Video | COVID-19 Vaccine |
Leave a comment
ICYMI, here’s a chart from a recent post by my good friend Mathew Crawford. It basically shows, the more you vaccinate, the more cases and deaths you get.

Critics would argue, “it’s confounded! more elderly are vaccinated.” But the same critics cannot show us this is false. They can only do “hand-waving” arguments that it must be wrong. Not very convincing.
Governments won’t release the data to show vaccinations are safe. I wonder why?
However, we actually agree with the critics that it is confounded but here’s why: governments don’t release the breakdowns publicly so we can’t do any better than this. If the vaccines are so safe, why don’t they release the data to the public to show this?
Is this just a fluke? I don’t think so. Watch this video starting at 7:00. The line goes the wrong way. The more you vaccinate, the worse it gets.
The health authorities are never going to figure this out because it would discredit them. So they have to keep on singing the same tune: “Safe and effective.”
December 5, 2021
Posted by aletho |
Science and Pseudo-Science | Covid-19, COVID-19 Vaccine |
Leave a comment
What happened to Joe Biden could have happened to anyone. In fact, it happens all the time. Throughout human history. He (presumably) caught a cold from his one-and-half-year-old grandson. His theory is that his grandson “likes to kiss his pop.” As a result, he got a “frog in his throat.”
It’s just a cold! No reason to freak out!
Biden’s spokesperson says that he has taken recourse to therapeutics. He “is taking some over-the-counter medication and probably some cough drops and some tea, but otherwise he’s proceeding with his schedule,” said Jen Psaki.
It’s all so normal. So much part of life. There is no way to know if Biden is correct in his casual contact tracing. He might not have gotten the cold from his grandson but he could have. Any parent will tell you that the first child comes with a full year of household sniffles and sickness. The second one is not so bad because the parents have built up immunity. And so on.
But maybe Biden should not have been letting his grandson kiss on him? That’s absurd. He would gladly risk infection in exchange for which he obtains and grants affection. It’s part of the deal we have all made with pathogens: we do a dangerous dance with them in order to experience love, freedom, choice, and human rights.
So far there is nothing I’ve written above that is unusual. It’s the way we’ve always lived. No one thinks the grandson should be punished for passing on a cold – which by the way can be a Rhinovirus or a Coronavirus. No one thinks that Biden should have avoided all contact with his family. There is no moral panic here. No one accuses anyone of aggression. It’s just life as we’ve always known it. Our immune systems have evolved to make it all possible.
So too with Deborah Birx’s desire to see her mother and take a trip, during the exact time last year when she was demanding that everyone cease all travel. The problem here is not the normal desire to see family. The problem is the hypocritical compulsion imposed on everyone else.
Biden’s behavior here is a beautiful illustration of the implicit and endogenous social contract under which we have all agreed to live. We live in the presence of pathogens, regrettable to be sure, but just what we’ve come to deal with. The payoff from the normal exposure to disease that we experience in the course of life is that we get stronger and more resistant to disease – plus we get to live normal lives.
When we do get sick, we reach for the things that make us better. We take cough drops. We sleep more. We have chicken soup. We starve a cold and feed a fever – or maybe it is the reverse, I forget. Whatever, we try to get well so that we can go on with life.
My apologies that this article is dreadfully boring so far. But boring is striking because, for some reason, we decided to forget all of this for the last two years in dealing with a new virus that is associated with a 99.8% survival rate, the victims of which tend to die at an age at which people normally die.
In short, we decided to panic ourselves into abolishing rights and liberties, while throwing out all inherited wisdom about infection, immunity, therapeutics, and viruses in general, not to mention all rights and traditional law. Talk of therapeutics for Covid was all-but banned. In short, we went utterly crazy, causing tremendous harm to public health, and the social and cultural fabric.
What strikes me about Biden and the frog in his throat is how casually and quickly he and his administration take recourse to traditional wisdom about viruses, even as the same administration is promoting the upending of life as we’ve known it all for a virus that is a near cousin of the very thing he caught from his grandson. And yet his spokesperson draws on what we’ve always known in order to calm people down.
I don’t blame Biden or his defenders for their common sense regarding infection. I blame them for not applying this traditional wisdom consistently for other viruses.
Still, the response to Biden’s infection should give us all hope that we can get back to normal, stop stigmatizing the sick, stop calling people who recover from Covid “survivors,” stop avoiding each other as if the human person is nothing but a vector of disease spread, and stop with this incredible cruel demand that every person separate from everyone else in the name of controlling a virus.
How many children have been forcibly kept from seeing grandma and grandpa over the last two years? How many lovers have been prevented from being together because they live in different disease jurisdictions? How many families have been shattered by Deborah Birx’s preposterous demand that we all live in separation from everyone else? How many people have been arrested for violating curfew? How many writers have been censored merely for saying that this Coronavirus should be treated like a normal pathogen?
Millions. Tens of millions. Billions across the world. We’ve paid a ghastly price for freaking out in all the ways in which Biden himself has not during his bout with a cold.
Nonetheless, this should give us hope that the old wisdom is not entirely extinguished. Some things are more important than disease avoidance, even for old people. We all need connection, and with that comes some risk. Our biology has evolved to deal with it. Indeed, the more exposure we experience (whether that means slobbering kids or mixing with people from all over the world in the commercial marketplace), the stronger we get and the longer the lives we live.
Freedom and human choice – plus affection, love, family, and normal life, even art, play, sports, and crowds – are all possible in the presence of infectious disease. Indeed, all these things are essential, else life is not worth living. That’s the real lesson here. May Biden’s throat frog – likely contracted through exposure – teach us at least this much.
Jeffrey A. Tucker is Founder and President of the Brownstone Institute and the author of many thousands of articles in the scholarly and popular press and ten books in 5 languages, most recently Liberty or Lockdown.
December 5, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | Covid-19, Human rights |
Leave a comment
An investigation of official ONS data has revealed that since the Covid-19 vaccine was offered and administered to kids in England and Wales there has been a 54% rise in deaths among male children compared to the same period in 2020.
The UK’s Medicine and Healthcare product Regulatory Agency (MHRA) have openly admitted that they suspect myocarditis and pericarditis are potential side effects of the Pfizer and Moderna Covid-19 vaccines, especially among young males. A suspicion that has been strong enough for the UK Medicine Regulator to officially add warnings about myocarditis and pericarditis to the safety labels of the Covid-19 vaccines.
Myocarditis is inflammation of the heart muscle, whereas pericarditis is inflammation of the protective sacs surrounding the heart. Both are extremely serious conditions due to the vital role the heart plays in keeping a person alive, and the fact that the heart muscle cannot regenerate. Serious myocarditis can lead to cardiac arrest and knock years off a persons life.

The UK Government have now also admitted in official documents that a high percentage of all hospitalised children are presenting to hospital with Myocarditis following Covid-19 vaccination.

This fact adds greater concern for data published by Public Health England on the number of 999 calls made requesting an ambulance due to cardiac arrest. The stats show that they have skyrocketed against the expected average since young adults and teens began receiving the Covid-19 vaccine.

Chris Whitty advised the UK Government to roll-out the Pfizer Covid-19 vaccine to all children over the age of 12 in week 37 of 2021. Thanks to preparations already being made by the NHS to intrude on education in schools and administer the jab to children, the roll-out got underway the following week (week 38).
The 2020 edition of ‘Deaths registered weekly in England and Wales, which can be downloaded here, and accessed on the ONS website here shows the number of deaths registered weekly by age group.

The ONS data shows that between September 18th and November 13th 2020 a total of 24 deaths occurred among male children aged between 10 and 14.
However, the 2021 edition of ‘Deaths registered weekly in England and Wales, which can be downloaded here, and accessed on the ONS website here, shows a significantly higher number of deaths have occurred among male children in 2021 following Chris Whitty’s decision to offer them the Covid-19 vaccine.
The data shows that between week 38 (week beginning 18th September) and week 46 (week ending 19th November) of 2021, a total of 37 deaths occurred among male children aged between 10 and 14.

This shows that since the Covid-19 vaccines began being given to kids over the age of 12, deaths among male children have increased by 54% compared to the same period in 2020.
We compiled the following graph on ONS figures so that we were able to easily compare the number of deaths per week among male children in 2020 and 2021.

The data is there now for the authorities to see, a 54% increase in deaths of male children compared to 2020 since they started to be given the Covid-19 vaccine, they must investigate this and cease the roll-out of the jabs to kids immediately.
December 4, 2021
Posted by aletho |
Science and Pseudo-Science, War Crimes | COVID-19 Vaccine, UK |
Leave a comment
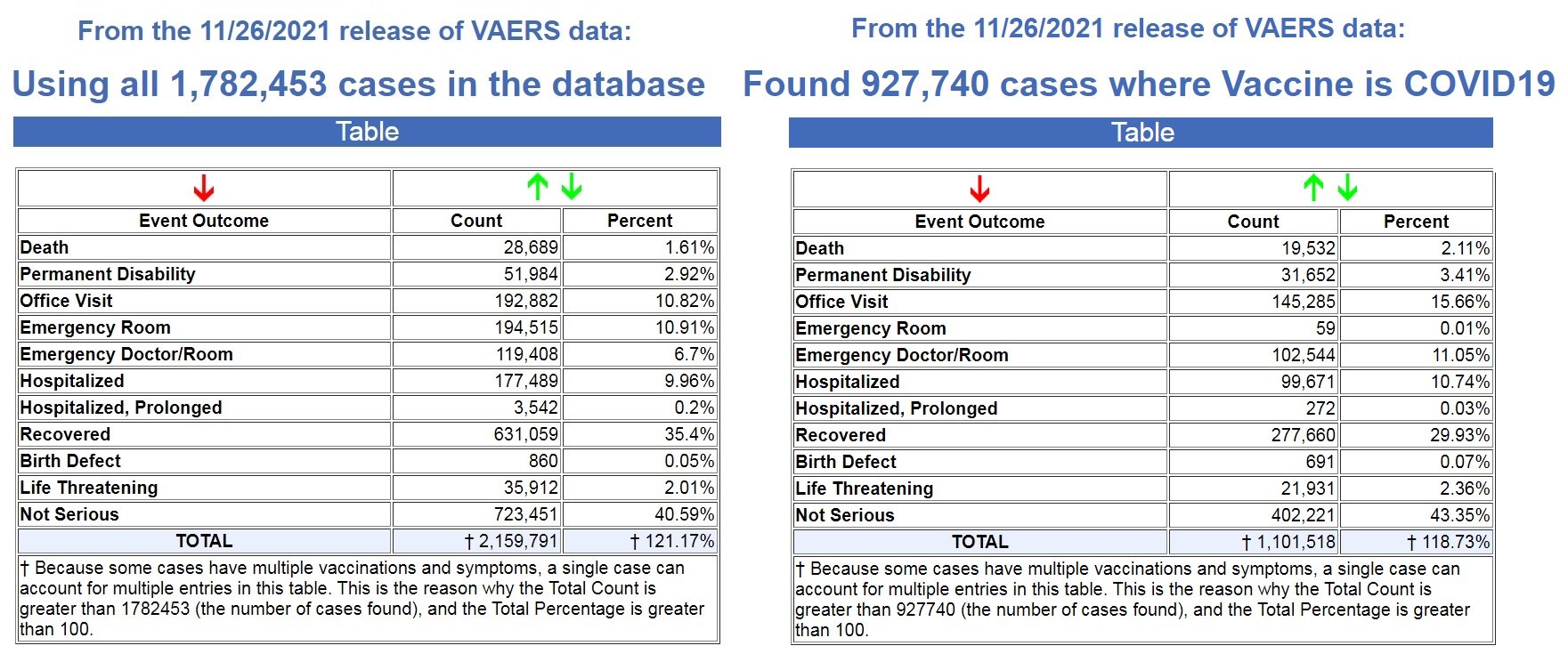
The latest data dump into the U.S. Government’s Vaccine Adverse Events Reporting System (VAERS) happened yesterday (12/3/21) and covers data through 11/26/2021.
There are now 927,740 cases reported to VAERS following COVID-19 shots for the past 11 months, out of the total of 1,782,453 cases in the entire VAERS database filed for the past 30+ years.
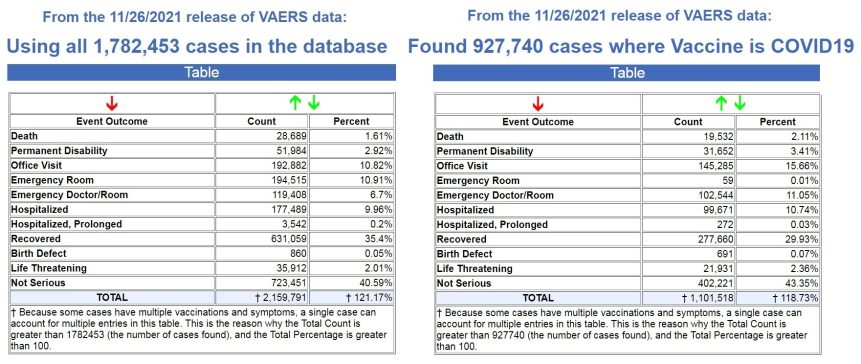
That means that 52% off ALL vaccine adverse reaction cases in VAERS for the past 30+ years have been reported in the last 11 months following the COVID-19 shots.
In addition, 68% of all deaths following vaccines reported in VAERS for the past 30+ years have been reported in the last 11 months following the COVID-19 shots.
We are on pace to see 21,307 deaths reported in the first year following the experimental COVID-19 shots, while the average yearly deaths reported after FDA-approved vaccines for the past 30+ years is 305 deaths.
That is an astounding 86% increase in reported deaths following the COVID-19 shots, a 70X increase over the average reported deaths following vaccinations for the past 30+ years!
- FDA-approved vaccines: 305 deaths per year
- COVID-19 EUA shots: 21,307 deaths per year
And as Dr. Jessica Rose has previously reported, the under-reporting factor in VAERS for the COVID-19 shots is 41X, as a conservative number, which means that at least 800,812 people have now died following COVID-19 shots based on the VAERS data.
Most, if not all, of those deaths are being reported in the pharma-owned corporate media as “COVID” deaths, as there are now more recorded “COVID deaths” for the first 11 months of 2021 than there were for the entire year in 2020, when there were no COVID vaccines until December. (Source.)

Record Number of Fetal Deaths Following COVID-19 Shots
As of this most recent update in VAERS, we have now found 2,809 fetal deaths following COVID-19 shots injected into pregnant and child-bearing women for the past 11 months. (Source.)
By way of contrast, using the exact same search parameters in VAERS, but excluding the COVID-19 shots, we found 2,168 fetal deaths following all FDA-approved vaccines for the past 30+ years. (Source.)
That’s an average of 72 fetal deaths per year following all FDA-approved vaccines for the past 30+ years, compared to what is on pace to be 3064 fetal deaths in 1 year following COVID-19 shots.
- FDA-approved vaccines: 72 fetal deaths per year
- COVID-19 EUA shots: 3064 fetal deaths per year
That is an 80% increase in fetal deaths recorded in VAERS following the COVID-19 shots. And yet, the CDC and FDA continue to recommend these EUA shots for pregnant women and nursing mothers.
Not only do they recommend these shots for pregnant women, we now have ample evidence that they have known since earlier this year that these shots are dangerous to pregnant women, and causing fetal deaths.
In a March 4, 2021 Advisory Commission on Childhood Vaccines (ACCV) meeting, the CDC submitted a report that contained a section titled: Maternal vaccination safety summary (starting on p. 39).
They stated (emphasis mine – my comments in red):
* Pregnant women were not specifically included in pre-authorization clinical trials of COVID-19 vaccines
– Post-authorization safety monitoring and research are the primary ways to obtain safety data on COVID-19 vaccination during pregnancy
* Larger than expected numbers of self-reported pregnant women have registered in v-safe
* The reactogenicity profile and adverse events observed among pregnant women in v-safe did not indicate any safety problems (based on what criteria???)
* Most reports to VAERS among pregnant women (73%) involved non-pregnancy specific adverse events (e.g., local and systemic reactions)
* Miscarriage was the most frequently reported pregnancy-specific adverse event to VAERS; numbers are within the known background rates based on presumed COVID-19 vaccine doses administered to pregnant women (no supporting evidence to backup these claims)
It is important to note through all of this reporting by the CDC that these are based on self-reporting data from pregnant women.
We know that it is politically incorrect to blame any health issue on a COVID-19 “vaccine,” and that doctors and nurses are pressured to NOT report these, so how many pregnant women had an adverse reaction, like a miscarriage, and never even thought to link it to their COVID-19 shot?
So back in March of this year (2021), there were already major concerns about the effects of the shots on pregnant women, as “larger than expected” pregnant women were reporting adverse reactions, and “the most frequently reported pregnancy-specific adverse event to VAERS” was “miscarriage.”
Then in August of this year (2021), the CDC presented a “new study” with “new data.”
Again, this “data” is dependent on pregnant women “self-reporting” adverse reactions, so we know these reports will be well below what was actually happening in the population, as it is politically incorrect to report any adverse reactions related to the experimental COVID-19 shots. To do so is to be branded an “anti-vaxxer” and shame you for life.
The August update admitted that 13% of the pregnant women who had received a COVID-19 shot reported a miscarriage. The CDC brushed this aside by stating “miscarriage typically occurs in about 11-16% of pregnancies.”
But of course ALL miscarriages are reported somewhere in the medical files, which is why they can even come up with a number range like this. So this figure is based on 100% of the reported data, while the COVID-19 related miscarriages are only based on what was self-reported, and we have no idea how many women never reported their miscarriages because they never related it to their COVID-19 shot.
One the main studies the CDC allegedly relied upon to declare that COVID-19 shots were safe for pregnant women, was a study published in the New England Journal of Medicine on June 17, 2021.
But on October 14, 2021, they issued a statement stating that some of their data was wrong in the June 17th study. (Source.) It dealt specifically with pregnancies in their 20th week or earlier.
“No denominator was available to calculate a risk estimate for spontaneous abortions, because at the time of this report, follow-up through 20 weeks was not yet available for 905 of the 1224 participants vaccinated within 30 days before the first day of the last menstrual period or in the first trimester. Furthermore, any risk estimate would need to account for gestational week–specific risk of spontaneous abortion.” (Source.)
Full article
December 4, 2021
Posted by aletho |
Deception, Science and Pseudo-Science, War Crimes | CDC, COVID-19 Vaccine, FDA, United States |
Leave a comment
Medical evidence strongly justifies a proactive approach for using vitamin D
There seems to be an endless refusal by the public health establishment to fight the pandemic with the best science-based tools. Instead, they keep pushing vaccines.
Great German research provides unequivocal medical evidence that the government should be strongly advocating two actions: 1. Take vitamin D supplements and 2. Have your blood tested for vitamin D.
The title for this October 2021 journal article says it all: “COVID-19 Mortality Risk Correlates Inversely with Vitamin D3 Status, and a Mortality Rate Close to Zero Could Theoretically Be Achieved at 50 ng/mL 25(OH)D3: Results of a Systematic Review and Meta-Analysis.” [25(OH)D3 refers to metabolite of the vitamin in blood]
In other words, there is clear evidence that the lower your vitamin D level the greater your risk of dying from COVID infection. Moreover, the data clearly show that you need a blood level of at least 50 ng/mL.
Odds are, however, that very, very few people have been tested for their vitamin D level. This is a situation where waiting for testing is not the prudent approach. Vitamin D pills are pretty cheap and it is perfectly safe to take a healthy daily dose to maintain a good immune system. I take 4,000 IUs twice daily.
Here are a number of highlights from this research and other sources; the discussion is aimed at informing people with information not provided by Big Media, Big Government and Big Pharma.
Vitamin D is an accurate predictor of COVID infection. Its deficiency is just as significant, and perhaps more so, than more commonly discussed underlying medical conditions, including obesity.
To be clear, there is a level of vitamin D for an effective strategy at the personal and population level to prevent or mitigate new surges and outbreaks of COVID that are related to reduced vaccine effectiveness and new variants.
In the German study, fifteen other studies were cited that showed low vitamin D levels were related to cases of severe COVID infection, and seven studies that found positive results from treating ill patients with the vitamin.
The German study noted: “The finding that most SARS-CoV-2 patients admitted to hospitals have vitamin D3 blood levels that are too low is unquestioned even by opponents of vitamin D supplementation.” The German study “followed 1,601 hospitalized patients, 784 who had their vitamin D levels measured within a day after admission and 817 whose vitamin D levels were known before infection. And the researchers also analyzed the long-term average vitamin D3 levels documented for 19 countries. The observed median vitamin D value over all collected study cohorts was 23.2 ng/mL, which is clearly too low to work effectively against COVID.”
Why does this vitamin work so well? The German study explained: A main cause of a severe reaction from COVID results from a “cytokine storm.” This refers to the body’s immune system releasing too many toxic cytokines as part of the inflammatory response to the virus. Vitamin D is a main regulator of those cells. A low level of the vitamin means a greater risk for a cytokine storm. This is especially pertinent for lung problems from COVID.
Other studies
On a par with the German study was an important US medical article from May 2021: Vitamin D and Its Potential Benefit for the COVID-19 Pandemic. It noted: “Experimental studies have shown that vitamin D exerts several actions that are thought to be protective against coronavirus disease (COVID-19) infectivity and severity. … There are a growing number of data connecting COVID-19 infectivity and severity with vitamin D status, suggesting a potential benefit of vitamin D supplementation for primary prevention or as an adjunctive treatment of COVID-19. … there is no downside to increasing vitamin D intake and having sensible sunlight exposure to maintain serum 25-hydroxyvitamin D at a level of least 30 ng/mL and preferably 40 to 60 ng/mL to minimize the risk of COVID-19 infection and its severity.” This confirms the German study and its finding of a critical vitamin level of 50 ng/mL.
Daniel Horowitz has made this correct observation about vitamin D supplementation: “An endless stream of academic research demonstrates that not only would such an approach have worked much better than the vaccines, but rather than coming with sundry known and unknown negative side effects.“
There are now 142 studies vouching for the near-perfect correlation between higher vitamin D levels and better outcomes in COVID patients.
From Israel came work that showed 25% of hospitalized COVID patients with vitamin D deficiency died compared to just 3% among those without a deficiency. And those with a deficiency were 14 times more likely to end up with a severe or critical condition.
Also from Israel, data on 1,176 patients with COVID infection admitted to the Galilee Medical Center, 253 had vitamin D levels on record and half were vitamin D-deficient. This was the conclusion: “Among hospitalized COVID-19 patients, pre-infection deficiency of vitamin D was associated with increased disease severity and mortality.”
Several studies have come from the University of Chicago. One found that a vitamin D deficiency (less than 20 ng/ml) may raise the risk of testing positive for COVID-19, actually a 7.2% chance of testing positive for the virus. And that more than 80% of patients diagnosed with COVID-19 were vitamin D deficient. And Black individuals who had levels of 30 to 40 ng/ml had a 2.64 times higher risk of testing positive for COVID-19 than people with levels of 40 ng/ml or greater.
On the good news side is a new study from Turkish researchers. They focused on getting people’s levels over 30 ng/mL with supplements. At that level there was success compared to people without supplementation. This was true even if they had comorbidities. They were able to achieve that blood level within two weeks. Those with no comorbidities and no vitamin D treatment had 1.9-fold increased risk of having hospitalization longer than 8 days compared with cases with both comorbidities and vitamin D treatment.
Another option
Some people may have absorption problems. The solution is to use the active form of D – either calcifediol or calcitriol – to raise their levels more quickly. This bypasses the liver’s metabolic process very effectively. Studies have shown that people hospitalized with low levels but given the active form of D did not progress to the ICU. Places that sell vitamin D often sell the concentrated active form.
I have a supply of cholecalciferol pills that provide 50,000 IUs, compared to ordinary D pills typically with 2,000 IUs. A reasonable use of the high concentration pills is in the event of coming down with a serious COVID infection. This may be a sensible strategy for those who do not know what their level is or have not taken the normal pills for some period. It can take months to raise a very low level to above the critical level the German study found necessary for the best protection.
Deficiency
Aside from dealing with COVID, two pertinent questions are: Is there an optimal level of vitamin D and are Americans deficient in it? For the first, this has been said: “While blood levels of 30 ng/mL or higher are considered normal, the optimal blood level of vitamin D has not yet been established.” From the Cleveland Clinic is this: “Normal vitamin D levels are usually between 20-80 NG/ML. If supplementation is recommended, remember to take it with a meal and on a full stomach to help absorption. Unfortunately, about 42% of the US population is vitamin D deficient with some populations having even higher levels of deficiency.”
A Mayo Clinic study said this: “Vitamin D deficiency is more common than previously thought. The Centers for Disease Control and Prevention has reported that the percentage of adults achieving vitamin D sufficiency as defined by 25(OH)D of at least 30 ng/mL has declined from about 60% in 1988-1994 to approximately 30% in 2001-2004 in whites and from about 10% to approximately 5% in African Americans during this same time. Furthermore, more people have been found to be severely deficient in vitamin D [ <10 ng/mL]. Even when using a conservative definition of vitamin D deficiency, many patients routinely encountered in clinical practice will be deficient in vitamin D.”
Clearly, personal deficiency can only be determined by a blood test that prudent people will request their doctors to order for a lab test.
Conclusions
Seeing vitamin D as crucial to surviving COVID is supported by solid medical research. There is good data to support a desired level of 50 ng/mL. Whether a person has this level requires a blood test for the vitamin, not something that most physicians normally call for when ordering blood tests for other reasons.
As the US approaches 800,000 COVID related deaths it is reasonable to believe that perhaps hundreds of thousands of lives could have been saved if the government had strongly supported vitamin D blood testing and supplementation if needed. But in the absence of such a COVID policy, people have good reasons to use D supplements if they are not routinely exposed to sunlight without using sunscreen products.
Many physicians have issued protocols for preventing and treating COVID that include vitamin D supplements. For example, the esteemed Dr. Zelenko uses the following: 5,000 IU 1 time a day for 7 days for low risk patients, and for high risk patients: 10,000 IU once a day for 7 days or 50,000 IU once a day for 1-2 days.
However, continuing its stupidity, NIH maintains that “There is insufficient evidence to recommend either for or against the use of vitamin D for the prevention or treatment of COVID-19.” This too was said: “Vitamin D deficiency (defined as vitamin D ≤20 ng/mL) is common in the United States, particularly among persons of Hispanic ethnicity and Black race. These groups are also overrepresented among cases of COVID-19 in the United States. Vitamin D deficiency is also more common in older patients and patients with obesity and hypertension; these factors have been associated with worse outcomes in patients with COVID-19.” Sounds smart to fight deficiency for avoiding COVID health impacts.
Sadly, we cannot count on the public health establishment to take a science-based, aggressive policy on using vitamin D supplements as an alternative to COVID vaccines or expensive medicines. Its up to individuals to protect their own lives by being well informed and proactive.
December 4, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | Covid-19, Vitamin D |
Leave a comment
Hiding part of the data leads to wrong conclusions
There have been numerous papers published showing how well the vaccines protect people after the second dose. Some of this effect is an illusion. The effect happens as a result of inaccurate measuring and a phenomenon called survivorship bias.
Survivorship bias happens when a group is compared at two time points, but the members of the group change between the time points. It would be like assessing the quality of a swimming school which favours the technique of throwing people into the middle of the ocean, leaving them for a couple of hours and claiming credit for how well the remaining students can swim. After two hours, the only people left would be the ones who could already swim and possibly a few who learnt to swim the hard way! The poor souls who drowned in the interim don’t even make the count. Attributing the remaining people’s swimming ability to the coach who turned up 2 hours later would obviously give a very misleading picture. Pointing out that no-one drowned in later lessons would be equally misleading in determining the success of the ‘teaching technique’.
With covid vaccination there is a two week period after vaccination that is not included in the data. The rationale given for this is that vaccines take a while to induce antibodies and therefore the first two weeks’ data are not relevant. Obviously this is flawed. What if the vaccines have deleterious effects that are visible straightaway, that have nothing to do with antibody production? An example is the high rate of shingles seen after covid vaccination, suggesting there is a problem with viral reactivation. This may explain why Sars-CoV-2 infection rates are actually higher in the vaccinated than in the unvaccinated in the first two weeks after vaccination.
The effect of eliminating the first two weeks is a misleading data bias. If people become infected and are dying during that period, this needs to be included. The possibility that the vaccine itself may exert an effect on infection rate cannot be overlooked and the entire dataset needs to be included in order to accurately assess effectiveness. By only measuring the period after the higher risk of infection (0-14 days) it is possible to be deceived. Any signal would be missed.
Aside from it being nonsensical in terms of individual risk to remove this period of time, there will also be an impact on the wider community. If the vaccine in fact causes a spike in infections during the first two weeks, this will inevitably increase spread and will lead to an increased number of infections in that community during that time. Therefore, the assessment of the impact of the vaccination programme must include not only the effect on the individual, but the impact on the wider community.
This point is of particular relevance for close-knit communities where many are being vaccinated at the same time, such as schools and in particular communities with a high number of vulnerable people such as care homes and hospitals. What we are effectively doing is ‘speeding up’ the wave of infections (and deaths). Ultimately at the end of the viral season, the same number of people died. Because of excluding the earlier deaths (1-14 days), we are misled into thinking that the vaccines were more effective than they actually were. By only looking at the later period and seeing fewer deaths during that time, the illusion was created that lives were saved. This is evident in data from many countries following vaccine roll-out. The graph below showing the UK versus Europe illustrates this point, as the UK was the fastest to roll out the vaccine. The total number of deaths, represented by the area under the curve, was similar to other countries, but is just compressed into a shorter time period.
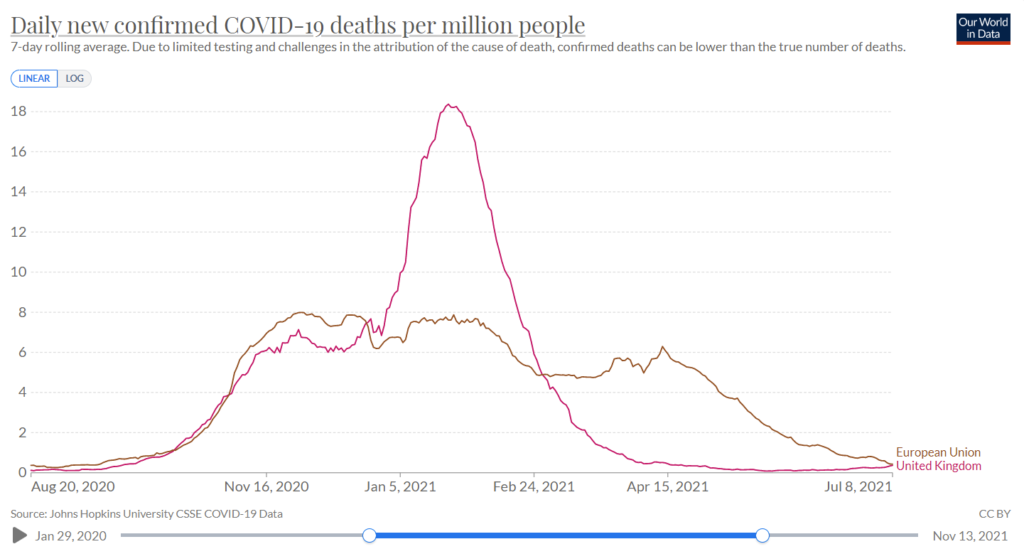
Figure 1: Covid Deaths in winter in UK and the European Union
Let’s now examine some specific examples, e.g. this study of nursing home residents in the United States. The results show that over the course of the study 6.8% of the vaccinated population were infected and 6.8% of the unvaccinated population were infected. However, by deciding that the first 14 days after vaccination should be excluded, the grey area for the vaccinated group is compared to the black and grey area combined for the unvaccinated. Doing so could lead to the claim of 66% vaccine efficacy against infection. The authors of this study were honest enough to share the raw data and did not claim 66% efficacy.
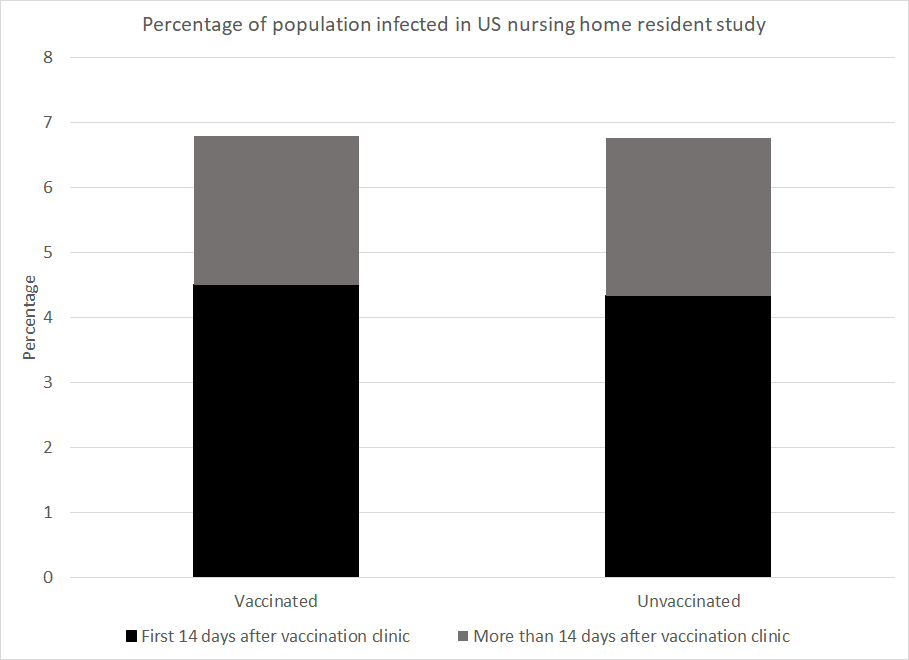
Figure 2: Data from US paper showing the percentage of the nursing home population to be infected by time after the clinic came to their home and by vaccination status
However, numerous studies have relied on this trick to make claims of vaccine efficacy. The most obvious examples of this are the original Pfizer trial study and the AstraZeneca trial.
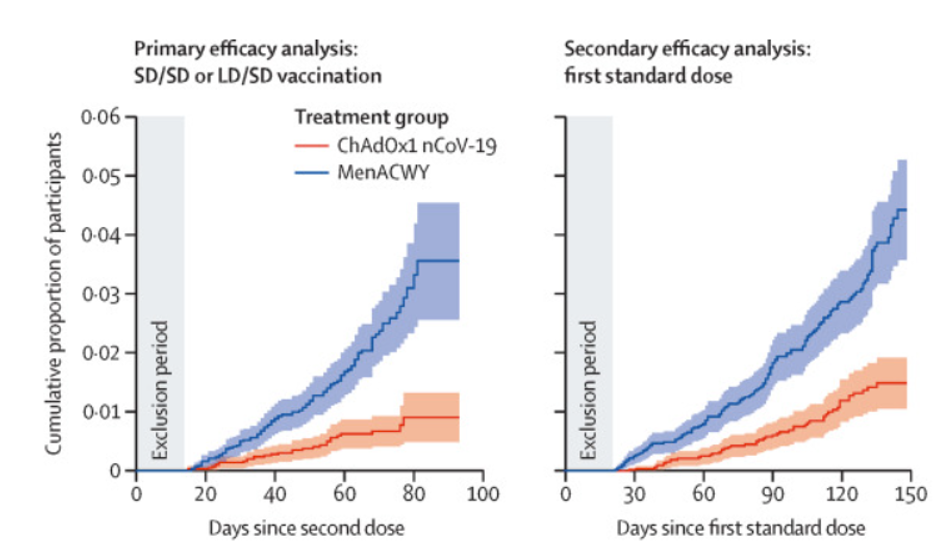
Figure 3: Graph from AstraZeneca trial showing censorship of early period (‘Exclusion Period’)
To take a second example, a Danish paper measured infection numbers in healthcare workers and care home residents. Prior to the beginning of the vaccination programme 4.8% of the healthcare workers had been infected and 3.8% of the care home residents had been. The study ended at the end of the Danish winter wave after 95% of the care home residents had been vaccinated and 28% of the healthcare workers had been. Given the worse position at the start and the lower vaccination rate in healthcare workers you might expect that they were worse off overall. However, the percentage infected by the end of the wave was 7.0% among healthcare workers but 7.7% among care home residents.
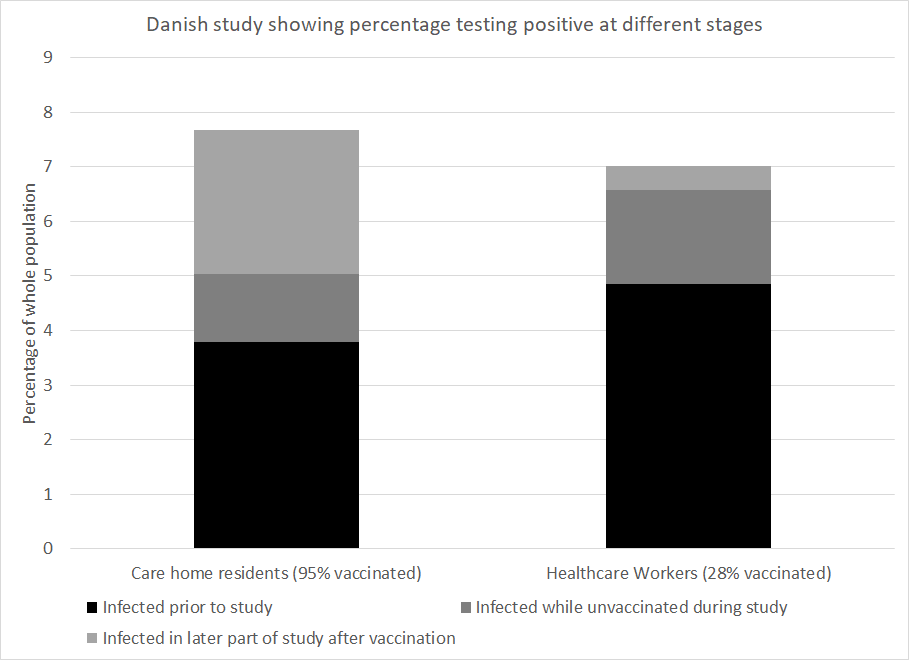
Figure 4: Data from Danish paper showing percentage of population infected among care home residents and healthcare workers
How much of the vaccine efficacy reported in covid research is really a measure of survivorship bias coupled with naturally acquired immunity? This is a critical question. No claim of vaccine efficacy should be made without first addressing this.
December 4, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine |
Leave a comment
Looking at the viral evolution of SARS-CoV-2, researchers from the prestigious universities Harvard and MIT have found that the virus not only will continue to mutate and create new variants in the future, but will become resistant to the vaccines as it adapts to humans.
Their study, published December 2, 2021, in the journal Science, shows that the mutations serve as bridges to conferring resistance to neutralizing antibodies. “The severity of the phenotypes we observed in vitro suggest that further evolved variants will more adeptly escape therapeutic antibody neutralization than currently circulating variants of concern, with potential resistance to two-component antibody cocktails,” the study authors wrote.
The scientists urged that “proactively examining the consequences of further viral evolution before the next highly antibody resistant strain emerges is of utmost importance.”
December 4, 2021
Posted by aletho |
Science and Pseudo-Science | Covid-19, COVID-19 Vaccine |
Leave a comment
In my column in the Spectator this week I’ve highlighted an egregious assault on free speech in New Zealand that was brought to my attention by the NZ Free Speech Union, which has issued a statement about it. A distinguished biochemist, Professor Garth Cooper, is being subjected to a disciplinary investigation by the Royal Society of New Zealand that could result in his expulsion. Here’s an extract:
Why is this distinguished scientist at risk of being expelled from New Zealand’s most prestigious academic society? Several months ago he was one of seven signatories to a letter in the New Zealand Listener that took issue with a proposal by a government working group that schools should give the same weight to Maori mythology as they do to science in the classroom. That is, the Maori understanding of the world — that all living things originated with Rangi and Papa, the sky mother and sky god, for instance — should be presented as just as valid as the theories of Galileo, Newton and Darwin.
The authors of the letter, “In Defence of Science“, were careful to say that indigenous knowledge was “critical for the preservation and perpetuation of culture and local practices, and plays key roles in management and policy” and should be taught in New Zealand’s schools. But they drew the line at treating it as on a par with physics, chemistry and biology: “In the discovery of empirical, universal truths, it falls far short of what we can define as science itself.”
In a rational world, this letter would have been regarded as uncontroversial. Surely the argument about whether to teach schoolchildren scientific or religious explanations for the origins of the universe and the ascent of man was settled by the Scopes trial in 1925? Apart from the obvious difficulty of prioritising one religious viewpoint in an ethnically diverse society like New Zealand (what about Christianity, Islam and Hinduism?), there is the problem that Maori schoolchildren, already among the least privileged in the country, will be at an even greater disadvantage if their teachers patronise them by saying there’s no need to learn the rudiments of scientific knowledge. Knowing about Rangi and Papa won’t get you into medical school.
But the moment this letter was published all hell broke loose. The views of the authors, who were all professors at Auckland, were denounced by the Royal Society, the New Zealand Association of Scientists, and the Tertiary Education Union, as well as by their own vice-chancellor, Dawn Freshwater. In a hand-wringing, cry-bullying email to all staff at the university, she said the letter had “caused considerable hurt and dismay among our staff, students and alumni” and said it pointed to ‘major problems with some of our colleagues’.
Two of Professor Cooper’s academic colleagues, Dr Siouxsie Wiles and Dr Shaun Hendy, issued an ‘open letter’ condemning the heretics for causing “untold harm and hurt”. They invited anyone who agreed with them to add their names to the ‘open letter’, and more than 2,000 academics duly obliged. Before long, five members of the Royal Society had complained and a panel was set up to investigate.
Worth reading in full.
If you’re a scholar in the sciences or the humanities and want to defend Professor Cooper you should write to Roger Ridley, the Chief Executive of the Royal Society of New Zealand, at roger.ridley@royalsociety.org.nz. He could use your help.
Stop Press: You can read more about this scandal here.
“Science is helping us battle worldwide crises such as Covid, global warming, carbon pollution, biodiversity loss and environmental degradation” … “Putting science on a pedestal gets us no further in the solution of these crises.”
December 4, 2021
Posted by aletho |
Progressive Hypocrite, Science and Pseudo-Science, Timeless or most popular | New Zealand |
Leave a comment


 Aletho News
Aletho News