aside from all the breathless reporting about “MOAR SPIKE MUTATIONS!!” i have yet to see a single report with any actual clinical evidence that the newly branded omicron variant is anything other than less dangerous than delta was.
it’s just, to steal a wonderful quote “mutational stargazing.”
this makes sense. not only are we continuing to evolve AWAY from an what looks near certain to be a lab engineered virulence optimum, but this is the natural path of viral evolution.
delta was a deeply attenuated version of prior versions. it’s original CFR was around 0.1%. this rose sharply over the summer as vaccine fade hit and this rise affected the vaccinated and the unvaccinated alike, so it appears to be a property of the virus, not of the vaccines. it was also mirrored by all cause mortality and so appears to be a real rise in fatality, not a definitional artifact.
i will still bet dollars to doughnuts that it was the vaccines themselves that, by being leaky but semi-protective, drove this inverted gradient to hotter strains.
a virus “wants” one thing: to spread. make a copy of me and pass it on. that’s the whole ballgame. harming the host and incapacitating them is maladaptive to this goal. mild viruses spread better. asymptomatic viruses spread best of all.
and that looks more and more like the case here. omicron looks milder than delta, especially than the souped up delta strains that emerged over the summer.
this is good news, not a reason for terror. the ideal outcome would be a virus with no symptoms and infinite spread that would immediately inoculate everyone.
primary symptoms appear to be lethargy. loss of taste and smell is largely absent.
as this virus looks to outcompete delta, but with lower risk, the idea that we want to keep it out seems exactly wrong. this is the variant you want. more spread, considerably less risk, mostly asymptomatic, but will generate the real, sterilizing immunity that the vaccines do not.
this is how pandemics end, not how panics should begin.
watching the west once more lose its collective mind is just pathetic.
based on the early looks, this is not even a chipmunk in the road to swerve around, it’s the shadow of a chimpunk and it’s a less dangerous strain that the one we currently have and another even lower risk bite at the immunity apple.
whether it will follow delta in terms of vaccine mediated evolution toward hotter future strains is anyone’s guess (and certainly possible) but if it is, indeed, destined to do so, then that’s all the more reason to let it spread now.
“we should panic in case it turns out we need to panic” is simply not a basis for public health.
I’m a voracious reader of Covid books but nothing could have prepared me for Scott Atlas’s A Plague Upon Our House, a full and mind-blowing account of the famed scientist’s personal experience with the Covid era and a luridly detailed account of his time at the White House. The book is hot fire, from page one to the last, and will permanently affect your view of not only this pandemic and the policy response but also the workings of public health in general.
Atlas’s book has exposed a scandal for the ages. It is enormously valuable because it fully blows up what seems to be an emerging fake story involving a supposedly Covid-denying president who did nothing vs. heroic scientists in the White House who urged compulsory mitigating measures consistent with prevailing scientific opinion. Not one word of that is true. Atlas’s book, I hope, makes it impossible to tell such tall tales without embarrassment.
Anyone who tells you this fictional story (including Deborah Birx) deserves to have this highly credible treatise tossed in his direction. The book is about the war between real science (and genuine public health), with Atlas as the voice for reason both before and during his time in the White House, vs. the enactment of brutal policies that never stood any chance of controlling the virus while causing tremendous damage to the people, to human liberty, to children in particular, but also to billions of people around the world.
For the reader, the author is our proxy, a reasonable and blunt man trapped in a world of lies, duplicity, backstabbing, opportunism, and fake science. He did his best but could not prevail against a powerful machine that cares nothing for facts, much less outcomes.
If you have heretofore believed that science drives pandemic public policy, this book will shock you. Atlas’s recounting of the unbearably poor thinking on the part of government-based “infectious disease experts” will make your jaw drop (thinking, for example, of Birx’s off-the-cuff theorizing about the relationship between masking and controlling case spreads).
Throughout the book, Atlas points to the enormous cost of the machinery of lockdowns, the preferred method of Anthony Fauci and Deborah Birx: missed cancer screenings, missed surgeries, nearly two years of educational losses, bankrupted small business, depression and drug overdoses, overall citizen demoralization, violations of religious freedom, all while public health massively neglected the actual at-risk population in long-term care facilities. Essentially, they were willing to dismantle everything we called civilization in the name of bludgeoning one pathogen without regard to the consequences.
The fake science of population-wide “models” drove policy instead of following the known information about risk profiles. “The one unusual feature of this virus was the fact that children had an extraordinarily low risk,” writes Atlas. “Yet this positive and reassuring news was never emphasized. Instead, with total disregard of the evidence of selective risk consistent with other respiratory viruses, public health officials recommended draconian isolation of everyone.”
“Restrictions on liberty were also destructive by inflaming class distinctions with their differential impact,” he writes, “exposing essential workers, sacrificing low-income families and kids, destroying single-parent homes, and eviscerating small businesses, while at the same time large companies were bailed out, elites worked from home with barely an interruption, and the ultra-rich got richer, leveraging their bully pulpit to demonize and cancel those who challenged their preferred policy options.”
In the midst of continued chaos, in August 2020, Atlas was called by Trump to help, not as a political appointee, not as a PR man for Trump, not as a DC fixer but as the only person who in nearly a year of unfolding catastrophe had a health-policy focus. He made it clear from the outset that he would only tell what he believed to be true; Trump agreed that this was precisely what he wanted and needed. Trump got an earful and gradually came around to a more rational view than that which caused him to wreck the American economy and society with his own hands and against his own instincts.
In Task Force meetings, Atlas was the only person who showed up with studies and on-the-ground information as opposed to mere charts of infections easily downloadable from popular websites. “A bigger surprise was that Fauci did not present scientific research on the pandemic to the group that I witnessed. Likewise, I never heard him speak about his own critical analysis of any published research studies. This was stunning to me. Aside from intermittent status updates about clinical trial enrollments, Fauci served the Task Force by offering an occasional comment or update on vaccine trial participant totals, mostly when the VP would turn to him and ask.”
When Atlas spoke up, it was almost always to contradict Fauci/Birx but he received no backing during meetings, only to have many people in attendance later congratulate him for speaking out. Still, he did have a convert in Trump himself, but by then it was too late: not even Trump could prevail against the wicked machine he had permissioned into operation.
It’s a Mr. Smith Goes to Washington story but applied to matters of public health. From the outset of this disease panic, policy came to be dictated by two government bureaucrats (Fauci and Birx) who, for some reason, were confident in their control over media, bureaucracies, and White House messaging, despite every attempt by the president, Atlas, and a few others to get them to pay attention to the actual science about which Fauci/Birx knew and care little.
Fortunately, we now have this book to set the record straight. It gives every reader an inside look at the workings of a system that wrecked our lives. If the book finally declines to offer an explanation for the hell that was visited upon us – every day we still ask the question why? – it does provide an accounting of the who, when, where, and what. Tragically, too many scientists, media figures, and intellectuals in general went along. Atlas’s account shows exactly what they signed up to defend, and it’s not pretty.
The cliche that kept coming to mind as I read is “breath of fresh air.” That metaphor describes the book perfectly: blessed relief from relentless propaganda. Imagine yourself trapped in an elevator with stultifying air in a building that is on fire and the smoke gradually seeps in from above. Someone is in there with you and he keeps assuring you that everything is fine, when it is obviously not.
That’s a pretty good description of how I felt from March 12, 2020 and onward. That was the day that President Trump spoke to the nation and announced that there would be no more travel from Europe. The tone in his voice was spooky. It was obvious that more was coming. He had clearly fallen sway to extremely bad advice, perhaps he was willing to push lockdowns as a plan to deal with a respiratory virus that was already widespread in the US from perhaps 5 to 6 months earlier.
It was the day that the darkness descended. A day later (March 13), the HHS distributed its lockdown plans for the nation. That weekend, Trump met for many hours with Anthony Fauci, Deborah Birx, son-in-law Jared Kushner, and only a few others. He came around to the idea of shutting down the American economy for two weeks. He presided over the calamitous March 16, 2020, press conference, at which Trump promised to beat the virus through general lockdowns.
Of course he had no power to do that directly but he could urge it to happen, all under the completely delusional promise that doing so would solve the virus problem. Two weeks later, the same gang persuaded him to extend the lockdowns.
Trump went along with the advice because it was the only advice he was fed at the time. They made it appear that the only choice that Trump had – if he wanted to beat the virus – was to wage war on his own policies that were pushing for a stronger, healthier economy. After surviving two impeachment attempts, and beating back years of hate from a nearly united media afflicted by severe derangement syndrome, Trump was finally hornswoggled.
Atlas writes: “On this highly important criterion of presidential management—taking responsibility to fully take charge of policy coming from the White House—I believe the president made a massive error in judgment. Against his own gut feeling, he delegated authority to medical bureaucrats, and then he failed to correct that mistake.”
The truly tragic fact that both Republicans and Democrats do not want spoken about is that this whole calamity did indeed begin with Trump’s decision. On this point, Atlas writes:
Yes, the president initially had gone along with the lockdowns proposed by Fauci and Birx, the “fifteen days to slow the spread,” even though he had serious misgivings. But I still believe the reason that he kept repeating his one question—“Do you agree with the initial shutdown?”—whenever he asked questions about the pandemic was precisely because he still had misgivings about it.
Large parts of the narrative are devoted to explaining precisely how and to what extent Trump had been betrayed. “They had convinced him to do exactly the opposite of what he would naturally do in any other circumstance,” Atlas writes, that is
“to disregard his own common sense and allow grossly incorrect policy advice to prevail… This president, widely known for his signature “You’re fired!” declaration, was misled by his closest political intimates. All for fear of what was inevitable anyway—skewering from an already hostile media. And on top of that tragic misjudgment, the election was lost anyway. So much for political strategists.”
There are so many valuable parts to the story that I cannot possibly recount them all. The language is brilliant, e.g. he calls the media “the most despicable group of unprincipled liars one could ever imagine.” He proves that assertion in page after page of shocking lies and distortions, mostly driven by political goals.
I was particularly struck by his chapter on testing, mainly because that whole racket mystified me throughout. From the outset, the CDC bungled the testing part of the pandemic story, attempting to keep the tests and process centralized in DC at the very time when the entire nation was in panic. Once that was finally fixed, months too late, mass and indiscriminate PCR testing became the desiderata of success within the White House. The problem was not just with the testing method:
“Fragments of dead virus hang around and can generate a positive test for many weeks or months, even though one is not generally contagious after two weeks. Moreover, PCR is extremely sensitive. It detects minute quantities of virus that do not transmit infection… Even the New York Times wrote in August that 90 percent or more of positive PCR tests falsely implied that someone was contagious. Sadly, during my entire time at the White House, this crucial fact would never even be addressed by anyone other than me at the Task Force meetings, let alone because for any public recommendation, even after I distributed data proving this critical point.”
The other problem is the wide assumption that more testing (however inaccurate) of whomever, whenever was always better. This model of maximizing tests seemed like a leftover from the HIV/AIDS crisis in which tracing was mostly useless in practice but at least made some sense in theory. For a widespread and mostly wild respiratory disease transmitted the way a cold virus is transmitted, this method was hopeless from the beginning. It became nothing but make work for tracing bureaucrats and testing enterprises that in the end only provided a fake metric of “success” that served to spread public panic.
Early on, Fauci had clearly said that there was no reason to get tested if you had no symptoms. Later, that common-sense outlook was thrown out the window and replaced with an agenda to test as many people as possible regardless of risk and regardless of symptoms. The resulting data enabled Fauci/Birx to keep everyone in a constant state of alarm. More test positivity to them implied only one thing: more lockdowns. Businesses needed to close harder, we all needed to mask harder, schools needed to stay closed longer, and travel needed to be ever more restricted. That assumption became so entrenched that not even the president’s own wishes (which had changed from Spring to Summer) made any difference.
Atlas’s first job, then, was to challenge this whole indiscriminate testing agenda. To his mind, testing needed to be about more than accumulating endless amounts of data, much of it without meaning; instead, testing should be directed toward a public-health goal. The people who needed tests were the vulnerable populations, particularly those in nursing homes, with the goal of saving lives among those who were actually threatened with severe outcomes. This push to test, contact trace, and quarantine anyone and everyone regardless of known risk was a huge distraction, and also caused huge disruption in schooling and enterprise.
To fix it meant changing the CDC guidelines. Atlas’s story of attempting to do that is eye-opening. He wrestled with every manner of bureaucrat and managed to get new guidelines written, only to find that they had been mysteriously reverted to the old guidelines one week later. He caught the “error” and insisted that his version prevail. Once they were issued by the CDC, the national press was all over it, with the story that the White House was pressuring the scientists at the CDC in terrible ways. After a week-long media storm, the guidelines changed yet again. All of Atlas’s work was made null.
Talk about discouraging! It was also Atlas’s first full experience in dealing with deep-state machinations. It was this way throughout the lockdown period, a machinery in place to implement, encourage, and enforce endless restrictions but no one person in particular was there to take responsibility for the policies or the outcomes, even as the ostensible head of state (Trump) was on record both publicly and privately opposing the policies that no one could seem to stop.
As an example of this, Atlas tells the story of bringing some massively important scientists to the White House to speak with Trump: Martin Kulldorff, Jay Bhattacharya, Joseph Ladapo, and Cody Meissner. People around the president thought the idea was great. But somehow the meeting kept being delayed. Again and again. When it finally went ahead, the schedulers only allowed for 5 minutes. But once they met with Trump himself, the president had other ideas and prolonged the meeting for an hour and a half, asking the scientists all kinds of questions about viruses, policy, the initial lockdowns, the risks to individuals, and so on.
The president was so impressed with their views and knowledge – what a dramatic change that must have been for him – that he invited filming to be done plus pictures to be taken. He wanted to make it a big public splash. It never happened. Literally. White House press somehow got the message that this meeting never happened. The first anyone will have known about it other than White House employees is from Atlas’s book.
Two months later, Atlas was instrumental in bringing in not only two of those scientists but also the famed Sunetra Gupta of Oxford. They met with the HHS secretary but this meeting too was buried in the press. No dissent was allowed. The bureaucrats were in charge, regardless of the wishes of the president.
Another case in point was during Trump’s own bout with Covid in early October. Atlas was nearly sure that he would be fine but he was forbidden from talking to the press. The entire White House communications office was frozen for four days, with no one speaking to the press. This was against Trump’s own wishes. This left the media to speculate that he was on his deathbed, so when he came back to the White House and announced that Covid is not to be feared, it was a shock to the nation. From my own point of view, this was truly Trump’s finest moment. To learn of the internal machinations happening behind the scenes is pretty shocking.
I can’t possibly cover the wealth of material in this book, and I expect this brief review to be one of several that I write. I do have a few disagreements. First, I think the author is too uncritical toward Operation Warp Speed and doesn’t really address how the vaccines were wildly oversold, to say nothing of growing concerns about safety, which were not addressed in the trials. Second, he seems to approve of Trump’s March 12th travel restrictions, which struck me as brutal and pointless, and the real beginning of the unfolding disaster. Third, Atlas inadvertently seems to perpetuate the distortion that Trump recommended ingesting bleach during a press conference. I know that this was all over the papers. But I’ve read the transcript of that press conference several times and find nothing like this. Trump actually makes clear that he was speaking about cleaning surfaces. This might be yet another case of outright media lies.
All that aside, this book reveals everything about the insanity of 2020 and 2021, years in which good sense, good science, historical precedent, human rights, and concerns for human liberty were all thrown into the trash, not just in the US but all over the world.
Atlas summarizes the big picture:
“in considering all the surprising events that unfolded in this past year, two in particular stand out. I have been shocked at the enormous power of government officials to unilaterally decree a sudden and severe shutdown of society—to simply close businesses and schools by edict, restrict personal movements, mandate behavior, regulate interactions with our family members, and eliminate our most basic freedoms, without any defined end and with little accountability.”
Atlas is correct that “the management of this pandemic has left a stain on many of America’s once noble institutions, including our elite universities, research institutes and journals, and public health agencies. Earning it back will not be easy.”
Internationally, we have Sweden as an example of a country that (mostly) kept its sanity. Domestically, we have South Dakota as an example of a place that stayed open, preserving freedom throughout. And thanks in large part to Atlas’s behind-the-scenes work, we have the example of Florida, whose governor did care about the actual science and ended up preserving freedom in the state even as the elderly population there experienced the greatest possible protection from the virus.
We all owe Atlas an enormous debt of gratitude, for it was he who persuaded the Florida governor to choose the path of focussed protection as advocated by the Great Barrington Declaration, which Atlas cites as the “single document that will go down as one of the most important publications in the pandemic, as it lent undeniable credibility to focused protection and provided courage to thousands of additional medical scientists and public health leaders to come forward.”
Atlas experienced the worst of the slings, arrows, and worse. The media and the bureaucrats tried to shut him up, shut him down, and body bag him professionally and personally. Cancelled, meaning removed from the roster of functional, dignified human beings. Even colleagues at Stanford University joined in the lynch mob, much to their disgrace. And yet this book is that of a man who has prevailed against them.
In that sense, it is easily the most crucial first-person account we have so far. It is gripping, revealing, devastating for the lockdowners and their vaccine-mandating successors, and a true classic that will stand the test of time. It’s simply not possible to write the history of this disaster without a close examination of this erudite first-hand account.
Jeffrey A. Tucker is Founder and President of the Brownstone Institute and the author of many thousands of articles in the scholarly and popular press and ten books in 5 languages, most recently Liberty or Lockdown.
EARLIER this month Dr Byram Bridle, a Canadian viral immunologist whose faculty at the University of Ontario has disowned him for his repeated assertion that Covid-19 vaccines are not safe, gave a remarkable off-the-cuff interview to a reporter. Bridle starts by explaining the reasons why heavily vaccinated countries are experiencing high case rates, why adverse reactions are not being reported or diagnosed and discusses the overwhelming evidence for ivermectin as an ant-viral treatment for Covid where studies have been conducted correctly.
DR BYRAM BRIDLE: A recent study came out looking at 68 different countries and they plotted on a graph the case rate for Covid-19 and the vaccination rate in the country. And the more vaccinated the country is, the more problems they’re having with Covid-19. So these people have the vaccine. Remember all the antibody titers they’re showing, that’s in the blood, but these people, on average, are quite poorly protected in their upper airways. And it’s not the virus that’s deep down in the alveoli that gets transmitted to other people because of the dead airspace when we exhale. It’s the viral particles that are in the upper airways. So that’s why the vaccinated can spread this just as efficiently as somebody who’s completely unprotected. And so these vaccines on that basis, because they don’t come close to conferring sterilising immunity, they don’t properly protect the upper respiratory tract, they only confer about four and a half months of immunity, it’s absolutely 100 per cent impossible to achieve the goal of herd immunity with these vaccines. 100 per cent impossible.
What I’ve seen way too much of – and it does cause me very serious concern – is we’re seeing people who had cancers that were in remission or that were being well-controlled, and their cancers have gone completely out of control after getting the vaccine. And what we do know with the vaccine is the vaccine causes at least a temporary drop in T-cell numbers and those T-cells are part of our immune system, and they’re the critical weapons that our immune system has to fight off cancerous cells. So there’s a potential mechanism there. And all I can say is I’ve seen . . . I’ve had people contact me with way too many of these reports for me to feel comfortable. I do feel that that’s probably, I would say, my newest major safety concern. And it’s also the one that is going to be by far the most underreported on any adverse event database. Because if somebody’s had a cancer before the vaccine, there’s no way public health officials will ever link it to the vaccine. But what we’re seeing is oncology teams that had pushed the cancers into remission or keeping them well-controlled can no longer control them after the vaccine.
So we know in Canada it’s very upsetting, because in Canada we have a system that will never, never detect problems with these vaccines – that’s why we’ve always had to rely on other countries. Like with the AstraZeneca vaccine, we told Canadians that the AstraZeneca vaccine was 100 per cent safe, despite the fact that 12 European countries had paused the programme to look for potential links to the blood clotting, potentially fatal blood clotting. And we were told as Canadians that we didn’t have to worry because ours was from a . . . they announced that the problem was associated with a single batch from a single production facility in Europe and ours was coming from India and therefore it didn’t apply to us. The European Medicines Agency will tell you that was never the case. And of course, then eventually, after there were Canadians that did die and many that did have to be treated for the blood clots, then we finally admitted that it was a problem.
And that’s how our system . . . our system is never going to work, because this is the thing. First of all, we’re not informing people when they get the vaccine that they’re to report any unusual medical condition up to eight weeks after receiving a dose of the vaccine. And then the attending physician is required to, by law, to report anything unusual. Most physicians are not. And now some of them are . . . many don’t, because they don’t want to contradict the current narrative. And the College of Physicians and Surgeons of Ontario has turned out to be incredibly tyrannical and are crushing many physicians and threatening many who don’t go with this narrow public health narrative. Many also can’t get their submissions done because they’re onerous. So, for example, British Columbia can take up to 40 minutes to submit one of these reports, and you can imagine if there’s an Emergency Room physician who sees five people in a shift that come in with problems and have recently been vaccinated, they can’t afford to spend hours on that shift, reporting it, right?
So there’s many reasons why people aren’t reporting to the physicians, and there are many reasons why the physicians aren’t reporting to the local Medical Officer of Health. And that’s the next step is, if a physician submits it, it doesn’t necessarily go into our database, it goes to the local Medical Officer of Health. This is the thing: the physicians are not supposed to make a determination of whether they think the medical condition that’s occurred after the vaccine is or is not related to the vaccine. They’re not supposed to make that determination. The local Medical Officers of Health are. And as you can imagine, with the huge bias that exists there, the majority of them, we’re seeing unusually high percentages of these reports that do get submitted being rejected at the level of the local Medical Officer of Health. And then from there, the ones that they do approve go to the Public Health Agency of Canada and then they could be filed into our adverse event database. But because of that, because of all the filtering that’s going on, this is the problem. We’re not getting accurate numbers.
So yes, a statistician, of course, could be looking for these. But if you don’t get accurate numbers reported, you can do all the analysis you want, it’s not going to be accurate, right? Your analysis is only as accurate as the data, the raw data you have to work with.
A D-dimer test is definitely a good one to do, because it can be suggestive of micro clots, which could be an indicator of blood clotting. But yeah, we’re finding that most physicians won’t do it. And we’re also finding a shortage, actually, of the blood collection tubes that are needed to do that as well.
Yeah, yeah, no, this is a virus. But ivermectin has clear-cut antiviral properties. For example, it has multiple mechanisms of action, but one is it inhibits the binding of the spike protein on the virus to these receptors that we have on the cells of our lungs. And yeah, what’s interesting is a lot of countries . . . so, that’s what’s frustrating for me as a vaccine developer, I knew that there was going to be no outlet for the vaccines if there were effective early treatment strategies. So I followed the science for the early treatment strategies, and I saw that the studies were flawed early on.
For example, a lot of the studies that were being done were being done in countries where things like ivermectin were available over the counter. So in other words, they were testing their treatment group, which was getting a defined amount of ivermectin and comparing it to a control group which had an undefined amount of ivermectin. So essentially comparing ivermectin treatment to ivermectin treatment, right? And then they showed there was no benefit. Well, of course not. If you’re comparing, you know, a treatment group to a treatment group.
And so when the science has been done properly, there’s an overwhelming [body] of scientific data showing that it works. And so even though I love vaccines, I couldn’t help but wonder why we were providing initially this authorisation for interim use, what we call emergency use in the United States, because we had clear, effective early treatments. I have worked with many physicians. These things clearly work. In fact, a lot of the countries that are having the most success, like, for example, a lot of the low income countries have had no choice. I mean, look, they’ve been left to take the leftovers for the vaccines. They can’t afford a lot of expensive treatments. So they have been relying on these effective early treatment strategies using repurposed generic drugs that are really cheap, and they’ve had a huge success.
So, for example, Egypt is a good example. Egypt, you know, Egypt has a three per cent vaccination rate. Three per cent of their eligible population is double vaccinated compared with Canada, which is at around 64 or 66 per cent. And they have 14 cases of Covid-19 per 100,000 people per day on average, whereas we have about 570 cases per day, so vastly higher.
And this is what people are seeing. A recent study came out looking at 68 different countries, and they plotted on a graph the case rate for Covid-19 and the vaccination rate in the country. And the more vaccinated the country is, the more problems they’re having with Covid-19. And when you look at these countries that have low vaccination rates, they’ve been relying on effective early treatment strategies.
So for example, with Egypt, I didn’t realise, but I asked that question to my collaborators, ‘What is Egypt doing right that we’re not doing here in North America?’ They sent me the official treatment protocol for Covid-19. Do you know what the number one thing is that they go to first? [It] is hydroxychloroquine and number two is ivermectin.
And if you look at Israel – Israel has the highest vaccination rate in the world, right? And the Delta variant is completely out of control, which is why they’ve been administering the third dose, why they’ve committed to a fourth dose. And with these numbers I was telling you, so they have the highest vaccination rates. So again, keep this in mind so as to understand – Egypt: three per cent vaccination rate, 14 cases per 100,000 of the population per day. Israel is at over an 80 per cent vaccination rate and has over 5,000 cases right now per day.
So these things work best as an early treatment strategy, so they should be administered. The sooner you administer them, the better the outcome. So we’ve had physicians – and I know these people and they’re good friends of mine – who have been absolutely destroyed for using ivermectin with their patients, and they’ve kept their patients out of the hospital, they’ve kept them out of the ICU. I find this exceptionally frustrating because I keep getting criticised for raising my concerns about the vaccines and harms, and I have physicians coming at me and saying, ‘Well, if only you saw on the front lines what happens to people who die from Covid and how terrible it is.’ And yes, it’s awful, and I feel terrible for all of them. But the other thing that I point out is it’s estimated that more than half the people that have died in this pandemic would be alive today if we had accepted these early treatment strategies. That’s the reality, and I’ve seen it with every physician who has administered this. They talk about our ICUs being overrun, but every physician that I have worked with – and I’ve worked with many who have used these effective treatment strategies – they’ve kept their patients out of the ICU. They don’t go to the ICU and they don’t die.
Do you realise that the way we’ve been treating patients is they go to the hospital and if they aren’t sick enough to go on a respirator, they typically get sent home and it’s, you know, take fluids and some of these other . . . maybe some aspirin. It’s basically what were they like to call in medicine, ‘watchful waiting’, which means, ‘we’re going to do nothing’, right? And you literally have to wait till you’re sick enough to come in and basically be put in the ICU and put on a respirator.
That’s not how you treat disease, right? The earlier you intervene, the better the outcome. And we have these early treatment strategies, and I think it’s no coincidence the only one we’ve approved in Canada is called remdesivir. It does have genuine safety issues and does virtually nothing for Covid-19. But it’s on patent and there’s tons of money that can be made. These other ones are dirt cheap. Ivermectin, you can treat somebody for about a dollar a day. So they’ve been using it to great effect in all these low income countries. But in North America, we’ve refused to adopt these strategies.
And you have to understand, and they even talk about safety issues. Well, one of the things is, so, there’s rare cases of safety issues associated with using the veterinary form, and that’s simply because of calculation errors – people making simple mathematical errors when trying to convert to the human dose. And the reality is that ivermectin is on the list for the World Health Organisation of one of the 50 most needed drugs in the entire world, has an unbelievable safety record. It’s used worldwide to effectively treat all these parasitic diseases. It was approved by Health Canada in 2018 to treat exotic parasitic diseases when Canadians are travelling. And so there’s absolutely no excuse.
…
Dr Bridle: My own physician, honestly, criticised me, saying I’m giving out this messaging, talking about patients of hers that died.
I respectfully pointed out that I’m also on the front lines and I’m trying to deal on a daily basis with family members of people who have died from the Covid-19 vaccines. And so I’m seeing these horrible deaths as well on the other side.
And the difference to me is, had they not rejected these effective early treatment strategies, at least half of the patients that died in their practices would be alive today.
So I’m sorry, I don’t have a lot of patience for these physicians. And I’m just going to point out one thing as well that’s important for the general public to know. I usually don’t ever, ever criticise anybody’s expertise in their particular area of work. But we’re in unique times. And so I think the public needs to be aware.
We put a lot of faith in our physicians. The average family physician knows almost nothing about immunology and certainly about vaccines. People forget vaccinology is a sub-discipline of immunology. The average family physician in Canada gets between five and ten lectures in their first year on immunology, of which a tiny fraction of that is going to be dealing with vaccines.
They are not immunologists, they are not vaccinologists and they’re ignoring the vaccinologist here in Canada. They are promoting the vaccines and the reality is they don’t understand the science, and they do not have a deep enough understanding, on average, to understand the science and to understand the debates that are going on.
Interviewer: If information has been deliberately suppressed about these treatments, that would be a crime, seeing that people are dying?
Dr Bridle: Yes. Yes.
Interviewer: Doctor, will we see a national debate, like with top scientists on this subject ever in Canada? Like their side for pro, and our side? Do you think we’ll ever see that in Canada?
Dr Bridle: I and my colleagues have been open to that for months, many months. I would love to see it done. The public should be insisting on it, like the old-fashioned good scientific debates.
I would argue scientists can talk about the science. We can put aside our emotions. We can talk about it respectfully. I would argue what I would like to see happen is have a team – if it’s too big, it gets a little unwieldy – so I’d say between three and five scientists and/or physicians who want to debate both aspects of the Covid-19 policies and then have it moderated by somebody. And it has to be very public.
And that’s what I keep pointing out to the public. People who keep arguing that those of us who have legitimate concerns are wrong, providing misinformation, that we’re lying and that we don’t know what we’re talking about, have to keep asking themselves why then are many of us standing there in the arena like the gladiators of old? We’re standing in the arena, we’re waiting. None of their champions will step forward. None. We’ve tried it.
So we tried this in Ontario with (their Premier) Doug Ford. It was attempted in Alberta. It was attempted in Saskatchewan, where their premiers were also invited to have these open scientific discussions.
Nobody so far – and I know I’ve issued invitations. Every single person who attacks me I invite them to come on and talk publicly. I was even being interviewed once and live in the chat somebody was trolling the whole talk.
It was interesting. The person who was interviewing me stopped and invited the person to come on. They logged off pretty quickly. And that’s what we’re seeing over and over again. It’s remarkable.
I’ve asked thousands of people, not one person, not even one, in all these months has been willing to talk openly, publicly about the science and medicine underlying Covid-19. It’s exceptionally frustrating.
Even my own colleagues at the university who have attacked me, there are 83 of them, about that number, who signed a letter to the public saying that I was lying to the public, providing misinformation.
Do you realise some of these individuals were just down the hallway from me, in the same hallway, just a few doors down? None, not one of them, not one of those people was ever willing to talk to me on the phone, in a Zoom meeting or come to my office – and I have an open door policy and I invited many of them to do so – not one person.
And then, even after they signed that off, saying that I was giving misinformation, I had written a scientific document to outline the science that I’d been talking about, because this was birthed from a short interview that I gave on the radio, where I expressed concerns that the messenger RNA vaccines might be linked to the heart inflammation that was occurring in young people. And then I was attacked on that.
I wrote a document with all the science because, of course, I was not able to deliver all of my scientific arguments in that short interview.
People argued to the public, ‘You realise he only told you half the story.’ And I laugh about that because I say, ‘Well, you’re giving me far too much credit because I didn’t even get to deliver one per cent of the story.’
They’re trying to mean that I didn’t get to the other side of the story. No, there was so much more science, so many more mechanisms of action, of potential harm of these things.
And after I wrote that document, this letter was written by my colleagues. You realise that of those who I was able to get a straight answer from, none of them had even read my science. None of them had even bothered to see what my arguments were for my position. This is what’s happening right now, and the censorship is extreme it’s really unbelievable.
Interviewer: Some of your colleagues, they also said that it doesn’t alter DNA. Would you care to comment on that?
Dr Bridle: Yeah. So when it comes to the DNA, there isn’t sufficient data to … my personal opinion is that it’s not substantially altering the DNA.
All I can tell you is it was thought that human cells did not have a type of protein that’s needed to convert the messenger RNA in the vaccine into DNA. It turns out we do actually have these types of proteins present. So it’s theoretically possible.
Personally, I would think that it’s probably not a substantial issue, but theoretically possible. So as this is theoretically possible, I would argue as a scientist that it would be worthwhile investigating that – doing the research just to alleviate our concerns, people’s concerns, about that.
That’s the thing, people ask these questions and as you see that there’s theoretical possibilities for these happening, that used to be the scientific basis for then conducting the research and definitively answering people’s questions. So many of the questions that you have, I can’t definitively answer because we’ve lost this whole concept of conducting research to address the tough questions.
Interviewer: What I find interesting with what you’re saying is what I’m seeing, very clearly, is you’re confronting a talking point, not a science. And let me illustrate what I mean by that.
You ask a doctor about all this and what’s their answer if you really push them? ‘Well, we’re following the advice of x, y, z and they’re following the science that we trusted?’ Right? You go to the level above them, same thing. You go to the level above them, same thing.
Dr Bridle: We’ve tried, as scientists …
Interviewer: I understand that. You guys will talk to science because you’re working with it. The other side is purposely convoluting science from a talking point.
Dr Bridle: Yes.
Interviewer: I honestly wonder if they have a science. My wife and I survived …
Dr Bridle: Well, at this point I can tell you, as a scientist – that’s why I’m willing to debate anybody on it – they don’t have the science on their side. That’s very clear. And in fact, you no longer need to understand the science, you just need to understand the contradictions that are coming.
Because, this is the thing, the reason why people like Dr Palmer and myself can stand up and talk off the cuff without any script here is because we’re speaking the truth. We’re speaking based on our knowledge, and we don’t have to keep track of a story when we’re speaking the truth.
We don’t have to make sure that what we’re saying today matches what we said at last week’s rally or the one before that. But the public health narrative has become so discombobulated now that they’re constantly contradicting themselves.
And there’s so many examples that I could give you. But let’s take one, for example. I encourage people now to start taking headlines from the mainstream media from months ago, which had people like myself censored, and line them up side-by-side with headlines that they have today.
‘So a great example is this whole issue of the vaccine mandate and the fact that, you know, what are we telling people right now? If you have one dose of the vaccine, you’re lumped in with the unvaccinated. You’re dangerous, you’re the same as somebody who has been unvaccinated, you’re unprotected and you’re going to kill everybody else, right?
We know from the very get-go, the two-dose regimen was proclaimed to have 95 per cent effectiveness. So, this is the thing, a lot of people who are accepting this current messaging about the ‘one dose doesn’t count’ have forgotten about the one-dose summer.
Remember when Trudeau (the Canadian Prime Minister) was pushing and all we were hearing about was the one-dose summer? So in Canada, the world was watching us in bewilderment and wondering what the basis was for us going from the approved three or four-week interval, depending on whether it was the Pfizer or Moderna vaccine, to a four-month interval.
And if you recall, the reason why we could go for the one-dose summer and not worry about getting people two doses is because we were told one dose was 95 per cent effective.
‘A lot of you don’t realise this. If you don’t believe me, you can go on the Health Canada website right now and look. They will have on there that the one dose of the Pfizer vaccine is 95 per cent effective.
So now you have to start asking yourself, using their own messaging: If one dose is 95 per cent effective and two doses is 95 per cent effective, then why are the people with one dose being lumped in with those who are unvaccinated? Why was that OK then, when trying to justify going to a four-month interval, which had no scientific basis?
But now those same people who are sitting with one dose are told, ‘No, no, no. It’s not 95 per cent effective, it’s the equivalent of being unvaccinated altogether.’
This is where we’re getting to. So on that basis alone, that’s what I’m saying is, it’s become blatantly obvious. You don’t have to understand the science. They are not following the science, they’re contradicting themselves over and over and over again.
…
DR BYRAM BRIDLE: There’s been a remarkable number of young people who have died for no apparent reason. And in many cases, we can’t confirm their vaccination status. But I’ve been particularly concerned about the number of varsity athletes at our universities who have been dying completely unexpectedly and suddenly. And the only thing that I can tell you – and I don’t know whether they were or were not vaccinated – well, actually, I can’t tell you when they were vaccinated. What I can tell you is that no varsity athlete in Ontario can participate in a varsity team without being vaccinated. They weren’t allowed exemptions.
INTERVIEWER: My point on that example was simply this: if you’re following the science, that first statement that that head doc released would never be said.
BRIDLE: Yes.
INTERVIEWER: You would say, ‘We don’t know.’
BRIDLE: Exactly. That’s exactly, yes.
INTERVIEWER: But that’s the way they’re reporting it tells you . . .
BRIDLE: As you heard from me, yeah.
INTERVIEWER: . . . their complete agenda.
BRIDLE: As you heard from me. I won’t say definitively that it’s because of the vaccine. I’m a scientist, I’m open to that possibility that there is some other underlying condition with any individual case. But there’s too many of these to not investigate properly. Absolutely.
INTERVIEWER: And if anybody’s paying attention, that whole approach should really put your guard up.
BRIDLE: Yes.
INTERVIEWER: You should realise there’s something drastically wrong with public health officials who would talk with that kind of language.
BRIDLE: Yeah, well, look at the language. So, another contradiction is . . . so, for example, at my university, our president hosted the local Medical Officer of Health who declared the whole reason why the vaccine mandate made so much sense is that there is essentially no such thing as a breakthrough infection. And that’s still being claimed by many, although their ability to claim that continues to be eroded. But that was the idea, and they cited like a 0.003 per cent breakthrough infection rate, so essentially zero, meaning you’re completely protected.
And when our President was asked about that recently, she actually created quite a furore on our campus, because she completely contradicted the messaging that they had just given. Well, the reason why, of course, they still have to mask and physically distance is because, hey, you know, it’s well known that people who are vaccinated can still get infected, still get Covid and transmit the virus. And in fact, there’s very good immunological reasons why people who are vaccinated can still transmit the virus and the scientific data that is emerging is showing that they can transmit at least as efficiently as somebody who has no immunity whatsoever.
And the reason is, is because when we put the vaccine in the shoulder, we’re tricking our bodies into thinking that it’s what we call systemic infection. And so, the problem is that is where your body wants to protect the most is the blood, because if a pathogen gets into the blood it can disseminate throughout the whole body. And so we got all these antibodies in the blood.
So, the one place in our respiratory system where these antibodies will spill over into, if you’re trying to protect against a systemic infection, are the lower airways. And that’s because you just think about gas exchange. There’s barely a physical barrier between the alveolar space and the blood vessels to allow that ready air exchange, which also means it’s very easy for a pathogen that gets deep into the lungs – so that would be what we call pneumonia – for that pathogen to get into the blood. So we put antibodies in the lower airways if we think we have a systemic infection. But we aren’t getting proper antibody protection in the upper airways like we would if we were naturally infected. So these people that have the vaccine, yeah, remember all the antibody titers they’re showing, that’s in the blood. But these people, on average, are quite poorly protected in their upper airways. And it’s not the virus that’s deep down the alveoli that gets transmitted to other people, because of the dead airspace when we exhale, it’s the viral particles that are in the upper airways. So that’s why the vaccinated can spread this just as efficiently as somebody who’s completely unprotected.
And so these vaccines, on that basis, because they don’t come close to conferring sterilising immunity, they don’t properly protect the upper respiratory tract. They only confer about four and a half months of immunity. It’s absolutely 100 per cent impossible to achieve the goal of herd immunity with these vaccines. 100 per cent impossible. For these companies it would be such a quick and easy and cheap study to do, and they could definitively rule this problem in or out. And whenever there’s such easy to do research to be done and they won’t do it, that for me is always a red flag.
INTERVIEWER: Yeah, exactly why isn’t that happening?
DR BYRAM BRIDLE: Yes. All I can say is, again, we’re not being provided with accurate data. So it’s hard to answer any of these questions to do with, you know, what’s actually due to COVID, what’s due to other things? And how we’re defining these things is crazy. Like I said, we’re not even defining somebody who’s vaccinated until they’re 14 days out from their second dose. The second dose is serving as a booster, right? And so typically, the immune response would be peaking actually about five to ten days after receiving that. So we’re actually taking people who would theoretically be at the absolute peak of a vaccine-induced immunity, and we’re calling them not fully vaccinated, for example.
And so for example, if people were to die in that time frame, even if it was linked to the vaccine, it’d be linked as somebody who was not fully vaccinated having died. So it’s very difficult with all these kind of nuances that are going on. All I can say really is what we do know is that the problem of Covid, the number of cases has been dramatically overestimated, but to an unknown degree, because of the way we’ve misused the PCR test. And we know that the problems associate with the vaccines have been grossly underestimated, but to an unknown degree.
And so until we have accurate numbers for these – which I can’t see we’re going to have at any time soon unless we completely change the way we’re monitoring these things – we’re not going to be able to come up with accurate assessments as scientists of . . . you know, with these kind of questions. But the issue was at the beginning, or the problem was, people kept arguing that this could have between a 1 and 10 per cent fatality rate, infection fatality rate, meaning for every 100 people who were infected with the virus between 1 and 10 would die. But the thing is, as we never knew what the proper denominator was, how many people were getting infected – we still don’t know, because again, like I mentioned, there’s many of us . . . well, in fact, just right here, there was an individual who has gone now, but showed me his test result. He had had a positive Covid test result almost a year and a half ago, when he showed me his antibody response for the spike protein, it’s higher, way higher than the average person who’s been vaccinated at the peak, at the peak of their antibody response. So there’s somebody who clearly acquired immunity naturally. And we’re not tracking these people at all, because in many cases where people have actually been infected they didn’t even know it and have natural immunity.
We’re running this clinical trial where we’re evaluating natural acquisition of immunity. We’re finding a huge number of people who never realised that they were sick have clear evidence of immunity against this virus. So that means that for those individuals they were infected but this was not a pathogen for them and they recovered without, you know, without developing disease. And so we have no idea – and we now know this is much more common than we accepted at the beginning – but we have no idea just how common, right?
So the point is, we still don’t know the full extent of the denominator. But when it was updated in February, what was published at that time was that the infection fatality rate was 0.15 – so not even 1 per cent like we were being told, but 0.15 per cent – and that was for the entire population. And if you took out those who were 70 years and older, it dropped to 0.05 per cent. So, just to put that into perspective, a bad flu season would be at 0.1 per cent.
So again, if you go out of the high risk, the highest risk demographic, those over 70. And we’re actually dealing with a problem that is less fatal than the annual flu. And especially when we start talking about children – we’ve had one infant in BC who died. We’re, you’re talking about taking these vaccines down now, in the next phase, to five-year-olds and then all the way down to six months of age. And when you start getting down to under ten years of age, virtually nobody has died. And when you look at the flu, it’s far more dangerous for these individuals.
And if you want to look at another one, respiratory syncytial virus, which we live with – far more dangerous to young people. And this is where even pregnant or breastfeeding women are being told, encouraged, to get vaccinated to protect their infants. It’s crazy. It’s all based on this . . . it’s easy to make people feel that infants are very fragile, very fragile human beings, which in some ways they are. But when it comes to SARS-CoV-2, this was presented today: the younger you are, the fewer receptors you express in your respiratory system that this virus can use to latch on to your cells. And in fact, when you get down into the infants, they’re quite resistant to infection with this virus. And that’s why we haven’t been seeing deaths among that population.
So it’s very unusual, with any other infectious disease you always have two peaks: the frail elderly and the very young. And it’s very clear why, because the frail elderly . . . well, as we get older, our immunological function declines so we in essence become somewhat immunosuppressed as we get older. And then on the very young side, our immune systems don’t fully mature until we’re 16 years old. Still, some components of the immune system maturing as young teenagers. So we’re dealing with less mature immune systems, immune systems that aren’t fully mature as we get into the youngest population. So that’s why we usually see these peaks in the oldest and the youngest. But SARS-CoV-2 is not like that, it’s very unusual in the sense that, yes, infants are relatively immature in terms of their immunological functioning, but they’re physically very resistant to infection with this virus.
So this is all crazy to be encouraging breastfeeding women to be vaccinated, to protect their infants. Their infants are already naturally protected. And as we go down and we start vaccinating six-month-old breastfeeding infants, what we’re doing is we’re bypassing the natural protection they have from the virus when we inject these vaccines, where we start getting their body to manufacture the spike protein. And again, I can’t emphasise enough. The spike protein is not the inert target that we were hoping it would be for the immune system. It has all kinds of biological activities in our bodies that can potentially be harmful.
And what people have to understand is that the receptor that that spike protein can bind to in our children and infants is expressed at the same concentration internally as in adults. And that’s because that protein doesn’t exist to serve as a receptor for the virus, it actually exists to serve basic physiological processes such as regulating blood pressure and so on. So, they’re naturally protected from infection from SARS-CoV-2, but when we put the vaccines in, they’re at least as susceptible as adults to all the harms.
BMJ notes we will NEVER have the evidence, vaccine makers structured the trials to avoid proving an all-cause mortality benefit since they know it’s negative
If you are are still in doubt as to whether we are being hoodwinked on the safety and efficacy of the COVID vaccines, this Editorial in the BMJ today should remove all doubt. We are being hoodwinked. And it’s not going to get better. Ever. So we are stuck with a vaccine that is being mandated where most people have no fu*&($#ing clue as to whether it works or not.
Those of us who know how to interpret the safety data from VAERS and other similar systems know full well what is going on, but when we try to warn people, we are being marginalized as spreaders of misinformation. Who’s lying? Well, suffice it to say that no self-proclaimed VAERS expert will agree to a debate.
Note: For those of you upset about the headline, sure, they can argue that the COVID vaccines saved people from dying from COVID. I concede that. But the all-cause mortality (ACM) rate (which nobody is looking at), has always been far greater than the COVID lives saved.
Strategic Group, a major rental housing provider in Alberta, Canada, announced that all new tenants need to show a vaccine passport to live in its properties. Critics claim the renter’s vaccine mandate sets a dangerous precedent.
“Vaccination of everyone in our community is the only way we are going to get through this pandemic and back to a sense of normalcy,” said Riaz Mamdani, founder and CEO of Strategic Group, in an October 28 press release.
“The safety of our team and our residents is a top priority, so ensuring full vaccination across the board is the least we can do.”
The press release said that “all employees, residents, and prospective residents” have to be vaccinated. Existing tenants will have to show proof of vaccination. Anyone “unable to be vaccinated (i.e., children under the age of 12) is exempt until able to receive the vaccine.”
“These rules apply to all of Strategic Group’s residential communities in Alberta.”
The renter owns more than 100 1 and 2-bedroom units in Edmonton and Calgary.
The Canadian Pressreported that the Strategic Group COO Tracey Steman said that the company was “very proud” of the mandatory vaccination policy.
“And we’d like to see other landlords implement the same policy… It will help to end this pandemic,” Steman continued. “We’ve had really good feedback from our tenants.”
According to the company’s CEO, residents inspired the new policy as they were saying that “they value knowing that all their neighbors are vaccinated – they feel even safer in their own homes.”
Eva Chipiuk of the Justice Center for Constitutional Freedoms (JCCF) told LifeSiteNews that Strategic Group’s vaccine mandate for tenants “sets a dangerous precedent in Alberta and in Canada.”
“According to this renter’s policy, you do not deserve a roof over your head unless you have taken an experimental injection,” said Chipiuk.
“Such a policy, utterly unthinkable two years ago, is now frighteningly announced with pride,” she added.
“Under what authority is this policy being made?”
Chipiuk noted that the laws banning smoking indoors were discussed in “government housing.”
“This is not the same. These rental companies are taking the law into their own hands. If we allow this to happen, what will be next and who will find themselves without a place to live?” the lawyer asked.
In an article on The Lawyers Daily, landlord-tenant lawyer Caryma Sa’d explained why it is illegal for landlords to enforce vaccine passport mandates for tenants. Sa’d noted that refusing a potential client because of their vaccination status is discrimination.
Also, “landlords cannot simply make unilateral changes to the terms of the agreement, which would include imposing proof of vaccination as a condition of the tenancy.”
“This would prevent a landlord from attempting to evict a tenant based on vaccination status, unless it can be established that the tenant is substantially interfering with the reasonable enjoyment of others within the unit or otherwise causing serious problems at the residential complex because of their vaccination status,” the lawyer continued.
The president of the Canadian Federation of Apartment Associations John Dickie told the Canadian Press that it was “possible” for some landlords to follow Strategic Group’s lead and implement a vaccine passport mandate, but that was not likely to be “very widespread.”
“We’re not the health police,” said Dickie.
“Rental housing providers realize people need housing. We’re not in the habit of inquiring into people’s political views.”
In case you were beginning to feel like your world was becoming a cliché dystopian movie script, don’t feel bad. It appears that at least some of the villains agree with you.
Not happy with unsatisfying stories, scripts and narratives that shape our disorganized zeitgeist, Klaus Schwab and other creepy dungeon masters trying to manage the post-covid world have called for a ‘New Narrative’ to shape our 21st century and beyond. Schwab described the World Economic Forum’s Great Narrative Initiative announced on November 11 as a “collaborative effort of the world’s leading thinkers to fashion longer-term perspectives and co-create a narrative that can help guide the creation of a more resilient, inclusive and sustainable vision for our collective future.”
It is no question that this new project is bone chilling, but can it work? Does it have any basis in reality or is the oligarchical high priesthood stage managing this shit show intoxicated by their own self-induced narratives and completely incapable of seeing the seeds of self-destruction they have created for themselves?
Let’s examine this question in a bit of detail.
As far back as we look, recorded history demonstrates myths and stories that shape each culture’s subjective experience trying to make sense of the objective world and the many tenuous challenges that are tossed into our path.
Deep Structure Narratives
An ice age comes to an end and sea levels rise hundreds of feet drowning millions while wiping out coastal cities. As a consequence, flood myths appear across various cultures of the world.
Fires from the sky reflect terrible asteroids striking the earth wrecking havoc on ecosystems and perhaps even inducing volcanism and vast weather anomalies. As a consequence, more myths are created featuring heroes, villains, angels and Gods punishing sinners and rewarding those with virtue.
Throughout history, countless stories have been created by shamans, priests, and poets which have attempted to infuse meaning onto traumatic events induced by either nature or geopolitical strategies. Some classical stories may have even exposed geopolitical evils under the safer terrain of fiction when literal truths were impossible. One instance of this latter case can be found in the Olympian Gods of Homer’s stories who were in all likelihood representative of actual oligarchical families who manipulated never ending wars and exploited the folly and corruption of their chosen chess pieces on the Great Game of ancient Greece.
These stories are a part of the human condition and for the most part, perfectly natural.
However, in our supposedly enlightened secular era, these forms of myths are discarded as the foolish practices of simpler unscientific times.
Science has taught us to believe in logic. Not faith in God or the health of our immaterial souls.
The medieval myths of sea monsters and flat earths beyond which unsuspecting voyagers would meet a terrible fate were superseded for a new set of narratives during the enlightenment period. During this period, pure logic and empiricism were placed upon the new altars where religion once stood and we were told to worship new godheads by the names such as Kant, Locke, Hegel, Bacon and Newton. When Nietzsche proclaimed God to be dead, this was the current of thinkers that supposedly killed him.
The Indian poet Rabindranath Tagore referred to those suffering from this disease of metastasized logic saying: “A mind all logic is like a knife all blade. It makes the hand bleed that uses it.”
When the foundation of enlightenment logic began to break down under the pressure of reality over a century ago, new narratives taking the form of the Standard Model quantum mechanics began teaching modern man that what appears to be living is in truth, just made up of non living atoms and chemical interactions… and what appears to be ordered form operating with purpose is merely the stochastic motion of atoms devoid of purpose, beauty or even objective truth. We were told that all of this was held together only by a mix of luck (statistical probability) and four fundamental forces created 13.7 billion years ago. All behavior in human life or in nature thus explained away by Darwinian models of survival of the fittest and random mutations. The rise of modern monstrosities like eugenics, and neo-Malthusianism were the sick children of these ghoulish assumptions.
The more we probe behind the impressive veneer of these popular narratives, the more we discover that myths spun by modern day high priests on behalf of political interests have not only continued into our present age, but have continuously adopted new costumes to adapt to our changing world. Those brilliant minds whose discoveries actually overturned old narratives by leaping beyond the domains of inductive/deductive thinking are carefully obscured under mathematical formulas devoid of the spirit and personality of these exceptional individuals (1).
The Political Consequences of False Macro-Narratives
Some political expressions of today’s secular narratives were seen as neocons trotted out in front of cameras broadcasting the message that the two hijacked planes which destroyed three towers on 9/11 was orchestrated by angry Muslims in caves who hated our freedom.
We were told that covid-19 arose from a badly cooked mammal that kissed a bat requiring a total abolition of our constitutional freedoms.
We were told that the protest on January 6, 2021 in Washington D.C. was an insurrection worse than anything the U.S. had seen since the Civil War when 500,000 Americans slaughtered each other for four years.
We are continuously told that Russia has ambitions to undermine democratic elections across the entire free world while China is aiming to subvert western values and impose a global communist government through its imperial New Silk Road.
I could obviously go on for quite some time here, but needless to say, political myth making is an ugly part of life. But while each lie certainly does grave damage, our susceptibility to falling for these falsities is in no way disconnected from our acceptance of those higher meta narratives embedded in those scientific myths that shape HOW our minds move. Every high priest knows that controlling HOW people think is always infinitely more powerful than controlling WHAT they think about any particular thing. This is how the neocon rot grew in the U.S.A over a few generations leading us to today’s multifaceted systemic breakdown crisis.
One of the fathers of the mutant that became neoconservatism was a narrative-building master named Leo Strauss.
Leo Strauss’ Neocon Monstrosity
Working closely with Fabian Society and Frankfurt School agents throughout his career as a teacher in Columbia, New School and the University of Chicago, Strauss preached a perverse interpretation of Plato’s Republic to tens of thousands of devoted students spread across several decades.
Among the highest lessons contained in Strauss’s teachings (at least for a select few among his students) was the idea of the Noble Lie developed by Plato in Book 3 of the Republic. Strauss taught his students that this Noble Lie was the greatest weapon and rightful tool of anyone who found themselves in a position of power to rule over the weak at any time in history.
In true Nietzschean fashion, the narrow definition of “power” as the subordination of the weak to the strong was the only definition permitted by Strauss who taught his students that while Plato preached love of wisdom to the masses, he secretly held a different teaching for those elite among his Academy who would control political power. To these elite few, he gave the name ‘gentlemen’ and ‘Guardians’.
Strauss taught that Plato’s Guardians would control the shadows cast on the cave wall which the plebs shackled to their senses, would believe were the only reality possible. The mandate of these perverse neo-Platonists was to live the ideal not of Socrates, but rather of Thrasymachus whose immoral doctrine Socrates annihilated in the first book of the Republic. Those young neocons learning from their master were taught that the true ‘secret Socrates’ believed, like Thrasymachus, or Callicles (student of Gorgias), was that the highest purpose in life is to attain power, satisfy our lusts and control the shadows in the cave.
While I adore Plato, I would never deny that he was a myth maker.
The stories showcased in his dialogues from the Timaeus, Critias, Theaetetus, Sophist, Statesman, Meno, Laws, Phaedo, Apology, Gorgias, Republic etc… have shaped the minds of some of the greatest historic figures across 2400 years of world history. Renaissance figures like St. Augustine, Ibn Sina, Erasmus, Shakespeare, Benjamin Franklin, Lincoln, Moses Mendelsohn, Pushkin, Martin Luther King Jr., and countless other brilliant souls had their wits sharpened on the stories and lessons contained in Plato’s writings.
But was Plato truly the tyrannical double-speaker portrayed by Strauss and his followers who preached morality for the weak and vice for those who would control the shadows?
To be a true Guardian in Plato’s world meant more than simply getting out of the cave to see with the light of the sun (symbolic for creative reason) and then lord over the masses.
While Nietzscheans like Strauss stop reading at this moment and choose to dominate the slaves using a higher power of thinking reserved only for a select few of the golden collar elite… Plato made it very clear in his Republic and other writings, that the TRUE philosopher (and implicitly true guardian) was obliged to return back into the cave at risk of his or her life in order to help liberate their fellow captives.
Narratives for Freedom or Slavery?
“Every artist, every scientist, every writer must decide now where he stands. The artist must take sides. He must elect to fight for freedom or for slavery. I have made my choice”
-Paul Robeson, 1937
The question can now be posed: how do we know which narratives are designed to enslave us, which empower us, and which are benign (like a child’s belief in the tooth fairy or the toy-bearing fat guy who trades gifts for good behavior)?
Since each person’s internal universe interfaces with the external reality through the filter of both logic, senses, imagination, and free will, is it possible that some narratives can uplift and inspire us to be more than we are in the face of impossible odds? Can certain stories sharpen our wisdom and free us from the shackles of sense perception as we are taught to see ever more through the eye of reason and a developed imagination?
When George Washington led a small force of farmers against the world’s largest mercenary force in 1776, was it purely logic that guided them in this statistically impossible fight, or were stories of Christ’s passion animating this seeming irrational drive for freedom? When Syria was beset with foreign sponsored Jihadists and teetered on the brink of the abyss, did stories of the Prophet Mohammed animate their hearts to do the impossible when an easier albeit more slavish road awaited their surrender?
Certainly, history has proven time and again, that a certain type of poetic story can empower us to leap beyond our limitations and gain insights into the deeper truths of the human condition and universal reality itself. Even Shakespeare’s “fictional” stories offer the sensitive soul great universal lessons into humanity and real politic which has served great statesmen for centuries.
A Last Look at Today’s Oligarchical Narrative Builders
Although we can affirm with certainty that some narratives can be good and others evil, is it possible that the oligarchs managing today’s Great Narrative project wish humanity no harm?
Perhaps Lynn Forrester de Rothschild is completely genuine when she launched the Council for Inclusive Capitalism alongside Prince Charles, Mark Carney and a handful of Davos Billionaires representing tens of trillions of dollars of capital in 2014. Helping to transform capitalism into a green, eco friendly, more inclusive system that treats everyone equally is a good thing isn’t it?
When this Council merged with the Vatican in December 2020, Lynn de Rothschild described the event as “a historic new partnership between some of the world’s largest investment and business leaders and the Vatican… joining moral and market imperatives to reform capitalism into a powerful force for the good of humanity.”
This council is even led by “a core group of world leaders” who even call themselves “Guardians” following the title used by Plato 2400 years ago.
These guardians include the CEOs of powerful organizations as State Street, Bank of America, Johnson and Johnson, Rockefeller Foundation, Ford Foundation, Merck, British Petroleum, and the Rothschild banking houses. Not exactly the most morally advanced coterie of political heavy weights one could imagine, but still maybe the evil that they have been a part for decades has all been arranged for the sake of a higher good that only the elite may be permitted to know…
Unfortunately for the Davos Guardians, the reality of the New Great Narrative is a world devoid of those very principles that humanity requires to survive and thrive within our creative, reasonable universe. Wielding the power to control a shadow land of dumbed down slaves within a cave might seem impressive for some, but when juxtaposed with the active, creative multipolar paradigm now rising to become a global force for scientific and technological progress, controlling cave dwellers becomes little more than a bleak and pitiful ambition.
And like any parasite which can do naught but kill the very host it needs to suckle on for its very survival, those Davos guardians are likely to meet the same fate as that encountered by Edgar Poe’s impotent, nihilistic oligarch Roderick Usher as his castle crumbled into an abyss.
Note
(1) Some exemplary names of these exceptional individuals include Leonardo Da Vinci, Luca Pacioli, Pierre Fermat, Christian Huygens, Johannes Kepler, Gottfried Leibniz, Max Planck, and Dimitry Mendeleyev (to name but a few).
Twitter suspended my account (likely forever since there is no appeal) due to one post on prion diseases. Here’s the information they wanted to make sure you NEVER find out.
Summary
There is no doubt the mRNA vaccines are causing prion diseases. People didn’t have these diseases before the shot and suddenly they develop them after the shot. There is no other explanation for this. None of the “fact checkers” can explain the cause of the excess rates. Prion diseases are incurable and always fatal. You can die as soon as 6 weeks after COVID vaccination (see within 6 weeks and within 6 months examples).
However, Twitter believes this is not true, but they refuse to tell anyone why they think that. Other fact checkers who have checked this out never did a VAERS query and are unable to explain away the “excess” number of reports other than doing a blanket dismissal that everything in VAERS is fraudulent without providing any evidence of that claim (other than one report out of 1.6M reports).
None of the fact checkers will debate on this to set the record straight.
On November 24, 2021 I posted the following message on Twitter:
Twitter suspended my account hours later. There is no appeal available. All content over the last 12 years was removed. All my 75K followers were zeroed. My messages were removed. There was no opportunity to download my content.
The only thing left: that my Twitter ID was @stkirsch.
Twitter refuses to tell us what I said that was misleading?
Twitter won’t tell me that!!! They are deliberately withholding their definitive analysis on this extremely important scientific issue. Why???
I really want to know. Obviously, Twitter fact-checkers (all of whom I presume must have PhD degrees or MD degrees to be able to assess my claims) were able to quickly read all the medical literature and determine without a doubt I made an error and should be terminated for making a mistake. But they won’t tell me the mistake!!
If they want to fight misinformation, why aren’t they posting a link to their research proving me wrong when they terminate the account. They obviously invested hours of time in the research before they terminated me. Why not provide a link to that research so everyone can learn from it including me??
Here’s the evidence for my claim
Back in May 2021 when Professor Byram Bridle was disclosing the FOIA request on the Pfizer vaccine bio-distribution data he mentioned that the spike protein was associated with Lewy body formation which is linked to prion diseases. He expressed concern that the vaccines could cause prion diseases like dementia, Alzheimer’s, and Creutzfeldt-Jakob disease (CJD).
What do you know. He was right. Now we have proof.
Check out these VAERS query results. These searches are over all 30 years of VAERS and all 70+ vaccines. See anything unusual? Yeah, for less than 1 year of the COVID vaccines, the results are off the charts.
And for CJD which is extremely rare:
Remember, these are 30 year searches for all vaccines. Clearly there are excess reports. And we know VAERS isn’t being “over-reported” this year which I’ve shown many times before (events not caused by the vaccine are reported at rates comparable to other vaccines).
If it wasn’t the COVID vaccines causing this, what was the cause?
Nobody can answer that question, not even the Twitter fact checkers!
And compare them to some of the “fact checks” which claim there are no instances in VAERS which as you can see from the queries above (which you can replicate yourself):
An insurrectional situation has emerged in Guadeloupe. Roads are closed, buildings set on fire, and clashes between demonstrators and security forces are raging. Many Guadeloupeans have decided that, against dictatorship, violence is a legitimate option. It is a violence directed against the so-called ‘health pass’ and against the mandatory vaccination of careworkers imposed upon this overseas territory by Metropolitan France.
In September, France had made it compulsory for all health workers, home carers, transport staff, medical students, firefighters, and all related personnel to have the Covid vaccine. This was accompanied with the requisitioning of all Ivermectin stocks in order to force the deeply unpopular vaccine upon the people of Guadeloupe (as well as neighbouring Martinique). According to French government figures, only 33% of Guadeloupeans are vaccinated (versus 75% in Metropolitan France), with a simiar figure in Martinique.
Tensions rose in October with the arrest of two demonstrators, one of them being Claudine Maraton, the general secretary of the UTS-UGTG (the trade union section of the General Workers Union of Guadeloupe). The UGTG had taken a leading position in the political opposition to the vaccine mandate, a position that the president of the Guadeloupe region also came to echo. As the conflict sharpened, the governing En Marche party’s MP for Guadeloupe began todescribe the situation on the island as “quasi-insurrectional”, with opposition to the Covid regulations showing a “weakening state authority” on the island.
The Minister of Health, Olivier Véran seemed to recognise the fragility of France’s position, and decided to push back the deadline for the vaccination mandate to November 15th. But if November 15th marked the end of the ‘health emergency’ measures in most of the overseas territories, in Guadeloupe, it marked the start of an indefinite general strike, launched by a collective of trade union and citizen organisations against the mandatory injection of careworkers and the pass sanitaire. At a press conference at the Palais de la Mutualité in Pointe-à-Pitre, Maïté Hubert M’Toumo, the new General Secretary of the UGTG had already sounded the battle-cry: “From Monday, war is declared!”
“From September, the French state decided to renew hostilities […] all doctors and nurses can receive a notice prohibiting them from working. This means that from Monday, the French state which spoke of war has just declared war on us. The situation is catastrophic. Thousands of workers are affected, whom they want to shamelessly fire, without delay of challenge. We can’t accept that. It’s not possible. The Guadeloupeans are in danger and from the moment war is declared, we are obliged to respond. From Monday, war is declared, there will be nothing that will work, we must organise ourselves so that nothing functions: Monday, Tuesday, Wednesday, Thursday… every day! We have no choice, we must come together, all social and professional classes, all Guadeloupeans. From Monday there will be two camps: the camp of the French state which has decided to defile us and defile all who oppose their plans; and the other side that wants to protect the country in order to live in freedom. The French president said that vaccines are freedom, so freedom is conditioned on a vaccine, a vaccine that is not under control, a vaccine that generates more and more serious side effects. Is this freedom? It’s not possible. So from Monday, war is declared!”
Maïté Hubert M’Toumo
The Departmental Fire and Rescue Service (SDIS), also affected by the mandatory vaccination order, had come to assume a leading role in the protests. As the strike began on the 15th, fights broke out between firefighters and the elite gendarmes, When the gendarmes charged one group, thefirefighters responded with jets of water. Other incidents between strikers and police triggered a wave of arrests as the Pointe-à-Pitre prosecutor’s office complained of “repeated threats to a law enforcement officer.” Maïté Hubert M’Toumo denounced the arrests in a public statement, calling them “a serious attack on a fundamental freedom which is the right to strike” and rallying “all members and activists to strengthen the picket lines”. Even as the government sent in hundreds of police and gendarme reinforcements, the strike hardened on the following weekend, with rioting breaking out in Pointe-à-Pitre and across the Island. Several gas stations were closed by protesters, and many motorists raided those that remained open, fearing the strike would impact fuel supplies. As the demonstrations and clashes escalated, shops and pharmacies were torched and looted, while schools, post offices and courts were shut down. Reports surfaced that protestors had broken into an arms depot in the island’s capital, Pointe-à-Pitre, and stolen rifles. Col Jean Pierre, of the gendarmerie at Pointe-à-Pitre, said some of the protesters had fired upon security forces. “We just don’t know how far this will still go,” the city’s mayor, Harry Durimel, told FranceInfo radio.
This weekend, Paris authorities began sending elite police and counterterrorism officers with armoured vehicles to Guadeloupe in a bid to stamp out the uprising. The police reinforcements set about dismantling protesters’ road barricades while the island’s authorities imposed a dusk-to-dawn curfew until Tuesday morning. By Monday the police had arrested at least 38 people charged with looting and smashing shops.
Over the weekend, the main UGTG trade union called for continued protests. Meanwhile, Martinique has followed its neighbour’s example and gone on general strike against the measures dictated by Paris.
— United Together Against Chronic Endocrine Ailments (@UAilments) November 26, 2021
The cultural rejection
Guadeloupe – like Martinique – has a deep-rooted history of anti-vaccine sentiment linked to distrust of the Paris government. Political scientist Pamela Obertan, who is helping to organise anti-mandate protests explains that Guadeloupeans “are descendants of slaves, and for us, control over our bodies is really important… The government wants to impose on us a medical experiment. We are still medical experiments.”
For decades, agriculture workers in Guadeloupe and Martinique were exposed to an endocrine-disrupting, carcinogenic pesticide called chlordecone. Around 95% of the population in these two islands is known to register chlordecone in their blood. Studies have linkedthe pesticide to prostate cancer, and, significantly, Guadeloupe and Martinique have the highest prostate cancer rates in the world. Yet nothing has been done about real health emergencies such as this one. And this goes a long way to explain the distrust towards the metropolis that is felt in the French Antilles. It is this context that has empowered vaccination-refusal, which is now turning into a nationalist and patriotic cause.
Accompanying this development, there is a longstanding usage and trust in folk medicine. As Guadeloupe’s University Hospital director lamented, the vaccine refusniks are “pushing Guadeloupian pharmacology.” From the start of the aggressive push for ”Covid” vaccination, sales of Virapic, a syrup based on the local jackass bitters herb, skyrocketed. This tropical shrub (Neurolaena lobata) is traditionally used for treatment of fever and flu symptoms,wounds and infections, and a variety of parasitic ailments such as malaria, ringworm, and amoebiasis. The plant has found a local champion in pharmacist Henry Joseph, co-founder of the laboratory Phytobokaz. Joseph, claims to have proven the plant’s efficacy against emerging RNA viruses and thus its relevance to ‘Covid-19′.
Whatever comes of such research, the island’s distrust in vaccines is unlikely to abate any time soon. The metropolitan government’s refusal to negotiate, together with the local suppression of data on vaccine deaths will continue to antagonise an already rebellious populace. According to lawyer Maître Ellen Bessis, the University Hospital Center (CHU) of Guadeloupe never declares vaccination status amongst any hospitalisations. This, she says allows them to register vaccinated deaths in Guadeloupe’s hospitals as unvaccinated, which is what she says is happening. Bessis’ claim is based on the extensive testimony of firefighters who, in Guadeloupe, share the job of transporting emergency cases to hospital. As the civil liberties organisation Rester Libre !says, “If this information were verified, it would be an absolute scandal: a statistical lie designed to hide the dangerousness of the vaccine. It would create a crisis of absolute confidence with the public authorities, and, therefore, all the figures, all the data, could be called into question.”
It is difficult to imagine how the execrable Macron government could possibly backtrack in this conflict, or provide any concessions for Guadeloupe. For to do so would undermine the mandate policy in metropolitan France. Yet the rebellion of the island population can only deepen, as Ellen Bessis affirms.
“We wonder what is going on in the mind of the government!” says Jocelyn Zou, of the fire department’s union. “We Guadeloupeans have a notion of freedom. But they impose compulsory vaccination on us when alternative solutions exist. We have every motivation to fight to the end!”
France to send special forces to Guadeloupe after looting, arson:
The last few days we have heard some alarming reports about how the Northern Territories of Australia are treating their indigenous communities.
Tweets and videos have emerged claiming aboriginal people are being removed from their land and sent to “quarantine centres”, allegedly to protect them from the virus.
Some representatives of the community have sent out videos asking for “international aid”, and claiming Aboriginal communities are being placed under “martial law” and people are being removed from their homes “at gunpoint”
🆘BREAKING NEWS🆘 Representatives of the Aboriginal Community in Australia issue International Plea for help over tyrannical Australian coercion & control.
Another elder, June Mills, posted a video to facebook expressing concern about how difficult it is to get information out of the locked down communities. She says she has heard that the army is “removing people against their will”, ending with the emotive cry “they are killing us!”
Australia has been so rapidly descending into a fascist hellhole that none of this, if true, would be at all surprising. The very fact they have a huge quarantine camp they unironically refer to as “The Centre for National Resilience” should be a massive red flag for everyone.
Michael Gunner, Chief Minister of the Northern Territories, was a caricature of wide-eyed zealotry in a recent press conference. When asked whether vaccine mandates might alienate some people, even those already vaccinated he said:
If you support or give comfort to anybody who argues against the vaccine, you are an anti-vaxxer, I don’t care what your personal vaccination status is.”
Australia 🇦🇺: "If you are against the vaccine mandate, you are an anti-vaxxer, even if you are personally vaccinated"
Some people are evil. Some people are stupid. But what's really dangerous is the combination of both 👇 _pic.twitter.com/ifQPBASza7
The phrase “give comfort too” should alarm people, because it’s only ever used in warlike settings, discussing treason and collusion. “Giving comfort to the enemy“.
In another press conference, Gunner also announced a “hard lockdown” in aboriginal communities, meaning people are not allowed to leave their homes except for medical treatment or if required by law. Adding that people are being “removed” to quarantine centres in military trucks. Not just people diagnosed with “covid”, but “close contacts” too:
This is an absolutely appalling breach of human rights.. 38 indigenous Australians in the Northern Territory have been hauled into quarantine camps by the army. pic.twitter.com/VBrCAg3ZdP
All this is being sold in the mainstream as “concern” for communities which could be “extra vulnerable”.
Voices on social media – who are totally real, and not at all shills there to control the narrative – are claiming strict measures are necessary to protect indigenous Australians from Covid, because it would rip through their communities “like syphilis did to the Native Americans”. There is, so far, very little evidence to support this fear-mongering.
However, written statements, allegedly from people detained, are emerging online saying they are being well taken care of, and that “irresponsible” social media posts are “hurting people”.
Amnesty UK issued a press release condemning the moves, but this was swiftly countermanded by Amnesty Australia, and dismissed as “disinformation” in the press and by Michael Gunner as “conspiracy theorising” from “tinfoil hat-wearing tossers”.
Some other Australian states are already building quarantine camps specifically for Aboriginal communities.
South Australia announced a tender for these camps last week, with press coverage underlining they would be only for those people who are “unable to isolate at home”.
Whether genuinely well-intentioned or not, it can certainly be argued this is an example of massive governmental overreach, especially for a virus that is at worst a bad seasonal flu.
It’s a convoluted and complex situation, with the real facts being hard to establish. Whatever the reality, it’s a situation that bears close watching.
With natural exposure immunity and early outpatient treatment and when combined with no reports of increased lethality, the WHO’s reaction of generating panic toward “Omicron” is causing needless fear and panic. So too with the Biden administration’s newly imposed travel restrictions, which will achieve nothing and will once again disrupt trade and violate human rights.
The WHO has said that the Omicron variant can spread more quickly than other variants. Likely true. The virus is behaving just like how viruses behave. They are mutable and mutate and via Muller’s ratchet, we expect this to be milder and milder mutations and not more lethal ones given the pathogen seeks to infect the host and not arrive at an evolutionary dead-end.
The virus will mutate downward so that it can use the host (us) to propagate itself via our cellular metabolic machinery. The Delta has shown us this: it is very infectious and mostly non-lethal. Especially for children and healthy people. So is the WHO panicking the globe needlessly? Is this Covid-19 February 2020 once again?
The problem with South Africa as is with Australia and New Zealand and even island nations like Trinidad is that it has low natural immunity to SAR-Cov-2. This is because, as we witnessed over the last year and more, if you lock down your society too long and too hard, you deny the nation and population from inching closer to population-level herd immunity. And you have no economy or society from which to reemerge. You devastate your society for a pathogen that is largely harmless to the vast majority of people especially children.
Moreover, governments asked us for two weeks to flatten the curve to help prepare hospitals so that they can tend to surges and other non-Covid illnesses. We as societies gave our governments 2 weeks, not 21 months. They failed to tend to the non-Covid illnesses and we locked down the healthy and well (children and young and middle aged healthy persons) while failing to properly protect the vulnerable and high-risk persons such as the elderly. We failed and it was like killing fields in our nursing homes.
This failure rests on public health messaging and government. Additionally, what did our governments in the US, Canada, UK, Australia etc. do with the tax money for the hospitals and PPE etc.? Hospitals must be prepared by now. Governments have failed! Not the people. The Task Forces have failed, not the people.
These nations thought that they could stay locked down and wait for a vaccine. This is a reasonable view though I was against lockdowns as they would and did cause crushing harms on especially poor persons and children. The problem is there was an opportunity cost because the vaccine we were waiting on was suboptimally developed without the proper safety testing or assessment of effectiveness.
We have data that the Pfizer vaccine loses 40% of antibodies per month, meaning in 3 months post-shot, you have low effective vaccinal immunity. We see it clearly playing out now whereby you got to tamp down spread with the draconian lockdowns, but you did it at the cost of natural immunity. That is the opportunity cost. So we spent on getting the vaccine and it cost us natural immunity and thus herd immunity.
For example, the vaccine has failed to stop infection and spread against Delta. We have research findings by Singanayagam et al. (fully vaccinated individuals with breakthrough infections have peak viral load similar to unvaccinated cases and can efficiently transmit infection in household settings, including to fully vaccinated contacts), by Chau et al. (viral loads of breakthrough Delta variant infection cases in vaccinated nurses were 251 times higher than those of cases infected with prior strains early 2020), and by Riemersma et al. (no difference in viral loads when comparing unvaccinated individuals to those who have vaccine “breakthrough” infections and if vaccinated individuals become infected with the delta variant, they may be sources of SARS-CoV-2 transmission to others) that reveal the vaccines have very suboptimal efficacy.
This situation of the vaccinated being infectious and transmitting the virus has also emerged in seminal nosocomial outbreak papers by Chau et al. (HCWs in Vietnam), the Finland hospital outbreak (spread among HCWs and patients), and the Israel hospital outbreak (spread among HCWs and patients). These studies have also revealed that the PPE and masking were essentially ineffective within the healthcare setting. All of the HCWs were double-vaccinated yet there was extensive spread to themselves and their patients.
In addition, Nordström et al. (vaccine effectiveness of Pfizer against infection waned progressively from 92% day 15-30 to 47% day 121-180, and from day 211 and onwards no effectiveness), Suthar et al. (a substantial waning of antibody responses and T cell immunity to SARS-CoV-2 and its variants, at 6 months following the second immunization), Yahi et al. (with Delta variant, neutralizing antibodies have a decreased affinity for the spike protein, whereas facilitating antibodies display a strikingly increased affinity), Juthani et al. (higher numbers of patients with severe or critical illness in those who received the Pfizer vaccine), Gazit et al. (SARS-CoV-2-naïve vaccinees had a 13-fold increased risk for breakthrough infection with the Delta variant, and substantially elevated risk of symptomatic Covid and hospitalization), and Acharya et al. (no significant difference in cycle threshold values between vaccinated and unvaccinated, asymptomatic and symptomatic groups infected with Delta) collectively reveal the poor efficacy and even negative efficacy of the Covid vaccines. Levine-Tiefenbrun et al. reports that the viral load reduction effectiveness declines with time after vaccination, “significantly decreasing at 3 months after vaccination and effectively vanishing after about 6 months.”
As an example, the Swedish study (retrospective with 842,974 pairs (N=1,684,958) is particularly alarming for it shows that while the vaccine provides temporary protection against infection, the efficacy declines below zero and then to negative efficacy territory at approximately 7 months, underscoring that the vaccinated are highly susceptible to infection and eventually become highly infected (more so than the unvaccinated). A further example emerges from Ireland whereby reporting suggests that the Waterford city district has the State’s highest rate of Covid-19 infections, while the county also boasts the highest rate of vaccination in the Republic (99.7% vaccinated). Reports are that the U.S. Covid-19 deaths for 2021 surpassed the deaths from 2020, leading some to state that “more people have died from COVID-19 in 2021, with most adults vaccinated and nearly all seniors), than in 2020 when nobody was vaccinated.”
Thus these nations that locked down and stayed that way are in a quandary for they do not know what to do now. If you open you will get surges in infection. Where is the money that was to go to hospital preparation? Did governments embezzle and steal and misappropriate the money for the hospitals remain still not prepared?
We have a lot of natural immunity in the US, e.g. near 65-70% of the population. The open states (those that did not lock down too long and too hard and opened quickly) will likely do very well with this Omicron or any new variant. This also is the power of natural immunity.
And we need not forget the potency of the overlooked ‘innate’ immunity with the innate antibodies and innate natural killer cellular compartment. This innate response is particularly potent in children (our first line of defense against pathogens) and is what has spared children from Covid and how children typically stave off pathogens, especially young children still laying down immunological memory.
Moreover, there is no reporting of increased virulence/lethality of this new Omicron variant. As yet this will remain the case based on Delta and prior variants. There are no guarantees but we operate based on risk and all things point to the same for this new variant.
Just because there is a wave in SA does not mean that there will be waves in the US or Israel or other places with greater natural immunity. This was the prize of letting people enjoy day-to-day living. The nations that have ended lockdowns are likely to move past this new variant scare, and be fine. This is more of an overreaction by the WHO and governments and much ado about nothing.
Dr Alexander holds a PhD. He has experience in epidemiology and in the teaching clinical epidemiology, evidence-based medicine, and research methodology. Dr Alexander is a former Assistant Professor at McMaster University in evidence-based medicine and research methods; former COVID Pandemic evidence-synthesis consultant advisor to WHO-PAHO Washington, DC (2020) and former senior advisor to COVID Pandemic policy in Health and Human Services (HHS) Washington, DC (A Secretary), US government; worked/appointed in 2008 at WHO as a regional specialist/epidemiologist in Europe’s Regional office Denmark, worked for the government of Canada as an epidemiologist for 12 years, appointed as the Canadian in-field epidemiologist (2002-2004) as part of an international CIDA funded, Health Canada executed project on TB/HIV co-infection and MDR-TB control (involving India, Pakistan, Nepal, Sri Lanka, Bangladesh, Bhutan, Maldives, Afghanistan, posted to Kathmandu); employed from 2017 to 2019 at Infectious Diseases Society of America (IDSA) Virginia USA as the evidence synthesis meta-analysis systematic review guideline development trainer; currently a COVID-19 consultant researcher in the US-C19 research group
Hundreds of articles published in peer reviewed journals are being retracted after scammers exploited the processes for publishing special issues to get poor quality papers—sometimes consisting of complete gibberish– into established journals.
In some cases, fraudsters posed as scientists and offered to guest edit issues that they then filled with sham papers. (1)
Elsevier is withdrawing 165 articles currently in press and plans to retract 300 more that have been published as part of 6 special issues in one of its journals, and Springer Nature is retracting 62 articles published in a special issue of one journal.
Fraudsters have been caught several times in recent years while trying to use special issues as a way to get low quality papers published in legitimate journals—but the number of affected paper seems to be increasing. In some cases the evidence points to an organized network that tries to infiltrate scientific journals with the objective of easily publishing manuscripts from pseudo-scientists or less productive researchers who want to appear in respectable journals. (1)
This leads to the topic of predatory journals which are becoming a serious nuisance in science. They actively masquerade as legitimate journals, often with similar layouts and names—although they very likely have essentially zero threshold for publication, despite typically claiming to operate with rigorous peer review processes. These predatory journals are undermining the credibility of scientific publishing because the research they publish appears to be largely unvetted. (2)
Predatory Journal Examples
Big Birds
Assistant zoology professor Daniel Baldassarre at SUNY Oswego published a paper in a supposedly scientific journal, The Scientific Journal of Research and Reviews (Iris Publishing), with the following abstract:
“Many people wonder: what’s the deal with birds? This is a common query. Birds are pretty weird. I mean, they have feathers. Most other animals don’t have feathers. To investigate this issue, I looked at some birds. I looked at a woodpecker, a parrot, and a penguin. They were all pretty weird! In conclusion, we may never know the deal with birds, but further study is warranted.” The paper’s acknowledgments: “We thank Big Bird from Sesame Street for comments on the manuscript. Several trained monkeys transcribed videos.” (3)
Iris Publishing is part of a much larger problem of journals that publish low-quality research for exorbitant fees. These journals will often spam scientists with requests for submissions or asking them to be on their editorial boards.
Ottawa Citizen Experience
In the three years since the Ottawa Citizen started covering fake science publishers, the constant question had been: how bad can they get?
Then, the Indian company OMICS (a giant company, 700 online journals, in Hyderabad) set a new low. It published meaningless garbage submitted as a test by the Ottawa Citizen the previous fall, then got exposed for it, but then once again accepted the same garbage all over again. Verbatim. (4)
Jerry Seinfeld’s Disease
John McCool submitted a paper on Jerry Seinfeld’s imaginary disease, ‘uromycitsis poisoning’. It was accepted for publication even though a simple Google search for ‘uromycitisis’ returns thousands of references to Seinfeld. (5)
Fake Editor-In-Chief
Polish researchers created a profile of a fictitious scientist named Anna O. Szust and applied on her behalf to the editorial boards of 360 journals. Oszust is the Polish word for ‘a fraud.’ They gave her fake scientific degrees and credited her with spoof book chapters. In many cases, they received a positive response within days of application and often within hours. Four titles immediately appointed Szust editor-in-chief. Forty predatory and eight directory of open access journals appointed her as an editor. (6)
Concluding Comments
The number of predatory journals has increased at an alarming rate. By 2015, more than half a million papers had been published in predatory journals, and at the end of 2016, the number of predatory journals approached about 10,000. Predatory publishing is becoming an organized industry. As of June 2020, there were 13,000.
Gary Lewis reports, “In a nutshell, predatory journals are contaminating the scientific literature by providing ostensibly rigorous reports of studies that in reality are often far from acceptable. Work published in such journals is occasionally used in serious public debates, such as climate change. They present a serious credibility for science.” (2)
Scientists are trying to make others aware of these journals. Daniel Baldassarre hopes that papers like his will spread awareness of the existence of these predatory journals and what they look lie, and hopefully get people to stop publishing in them. (3)
References
1. Holly Else, “Scammers impersonate guest editors to get sham papers published,,” nature.com, November, 20212.
2. Gary Lewis, “I got a hoax paper published about how politicians wipe their butts,” realclearscience.com, July 23, 2018
3. Ryan F. Mandelbaum, “Sketchy science journal publishes article titled – What’s the deal with birds?” gizmodo.com, April 17, 2020
4. Tom Spears, “Fake science publisher accepts (again) a paper already exposed as a ‘pile of dung’”, ottawacitizen.com, June 1, 2017
5. John H. McCool, “Opinion: why I published in a predatory journal,” The Scientist, April 6, 2017
6. Piotr Sorokowski et al, “Predatory journals recruit fake editor,” Nature, 543, 481-483 (2017)
Since the very beginning of the covid panic, the narrative has been this: implement severe lockdowns or your population will experience a bloodbath. Morgues will be overwhelmed, the death total toll will be astounding. On the other hand, we were assured those jurisdictions that do lock down would see only a fraction of the death toll.
Then, once vaccines became available, the narrative was modified to “Get shots in arms and then covid will stop spreading. Those countries without vaccines, on the other hand, will continue to face mass casualties.”
The lockdown narrative, of course, has already been thoroughly overturned. Jurisdictions that did not lock down or adopted only weak and short lockdowns ended up with covid death tolls that were either similar to—or even better than—death tolls in countries that adopted draconian lockdowns. Lockdown advocates said locked-down countries would be overwhelmingly better off. These people were clearly wrong.
Undaunted by the increasing implausibility of the lockdown narrative, the global health bureaucrats are nonetheless doubling down on forced vaccines—as we now see in Austria—and we continue to be assured that only countries with high vaccination rates can hope to avoid disastrous covid outcomes.
Yet, the experience in sub-Saharan Africa calls both these narratives into question: Africa’s numbers have been far, far lower than the experts warned would be the case.
For example, the APreported this week that in spite of low vaccination rates, Africa has fared better than most of the world:
[T]here is something “mysterious” going on in Africa that is puzzling scientists, said Wafaa El-Sadr, chair of global health at Columbia University. “Africa doesn’t have the vaccines and the resources to fight COVID-19 that they have in Europe and the U.S., but somehow they seem to be doing better,” she said….
Fewer than 6% of people in Africa are vaccinated. For months, the WHO has described Africa as “one of the least affected regions in the world” in its weekly pandemic reports.
Yet disaster for Africa has long been predicted for several reasons even beyond the availability of vaccines. For instance, it is known that lockdowns are especially impractical in the poorest parts of the world. This is because populations in places with undeveloped economies can’t simply sit at home and live off savings or debt. Rather, these people must go out into the world and earn a living on a day-to-day basis. Starvation is the alternative. Moreover, much of this work is done in the informal economy, so enforcing lockdowns becomes especially difficult.
It was also assumed covid would be especially deadly in Africa due to the fact many large households live in small housing units.
But that “conventional wisdom” flies in the face of the reality of covid in Africa, which is that there have been fewer deaths.
The “experts” have groped around, looking for possible explanations.
Some sources, for example, insist that the low death totals are only an artifact of incomplete reporting on covid infections and that “a lack of good qualitative data was the issue.”
But Richard Wamai at Northeastern University rejects the claim it’s all about case reporting, and says that “local systems for reporting deaths in Africa make it difficult to hide COVID-19 casualties.” In a paper for the International Journal of Environmental Research and Public Health, Wamai and his coauthors conclude, “[T]here is no evidence that COVID-19 mortality data is less accurately reported in Africa than elsewhere” and “While the true picture of infections and mortality in the continent has yet to fully emerge, the quality of data for other diseases, such as HIV/AIDS, indicates that Africa has the capacity to collect and report valid disease surveillance data.”
In any case, the World Health Organization reports that covid deaths in Africa make up only 2.9 percent of covid deaths, while Africa’s population is 16 percent of the global total. Africa’s covid total could double or triple, and Africa would still be faring far better than Europe and the Americas.
Wamai et al. also note that at this point “[i]t is likely that SARS-CoV-2 has already been widely disseminated through Africa… If so, widespread infection is likely to also result in widespread natural immunity.”
In other words, continued claims by health officials—both in Africa and elsewhere—that mass death is right around the corner with the “next wave” look increasingly implausible.
It looks increasingly likely that the lack of covid mortality in Africa is not due to a data issue nor a situation in which covid has been “contained” up until now. So then why is Africa doing so much better than the wealthy West?
Naturally, the advocates of forced lockdowns and coerced vaccines would prefer to ignore this issue altogether, but the undeniable reality of Africa’s experience has forced mainstream researchers to publicly admit the many ways that many factors can explain covid’s prevalence beyond vaccination rates and mask mandates.
For instance, mentioning that obesity is an important factor in covid mortality has in the past been likely to get one savaged in the media for “fat shaming.” Yet the Africa situation has forced the well informed to admit that yes, obese populations clearly suffer more from covid. In Africa, not surprisingly, we find that obesity rates are far below those found in North America and Europe.
In the West, however, the media drumbeat around covid has consistently been “Shut up, stay home, get jabbed, and stop doubting the experts on forced vaccines.” Fortunately, however, the African situation has forced many researchers to ask inconvenient questions.
In fact, it’s amazing Africa has not been overcome by mass death considering that covid lockdowns and covid “mitigation” measures have contributed to the impoverishment and mass starvation on the continent. Or as Germany’s DW News puts it, “Measures put in place to slow the spread of the novel coronavirus are pushing millions of people in Africa into severe hunger.” And as Wamai notes, “[S]ome of the excess deaths in Africa “can be attributed not to the disease, but to lockdown measures that cut off access to medical care for other illnesses.”
But Africa hasn’t gotten the bloodbath that was promised, and as one Nigerian put it, “They said there will be dead bodies on the streets and all that, but nothing like that happened.”
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.

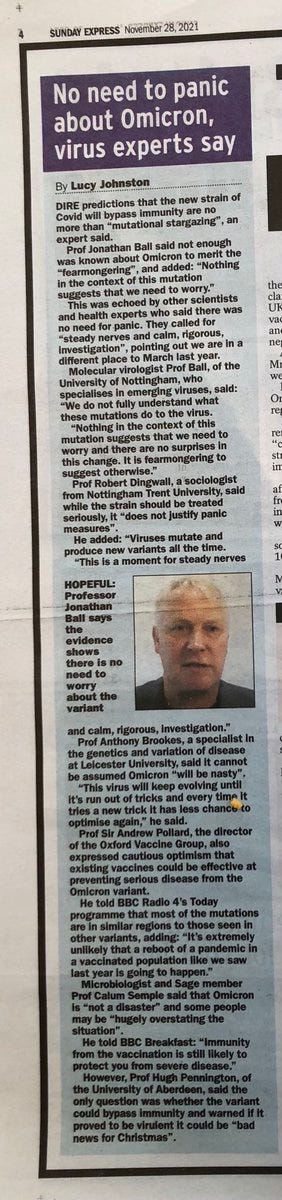
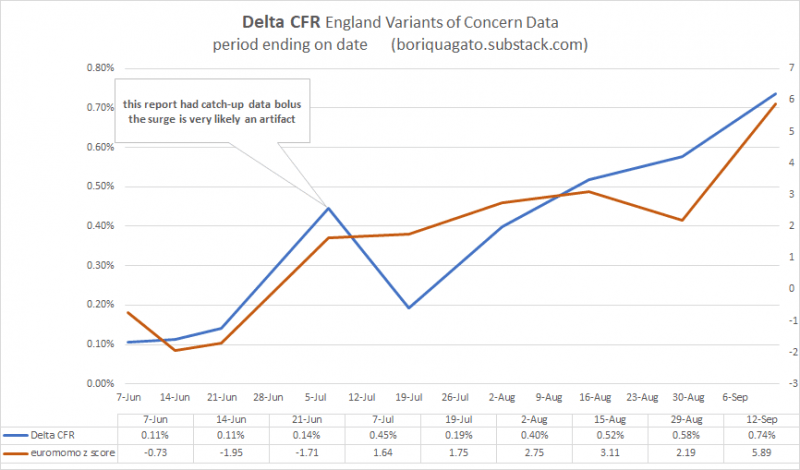

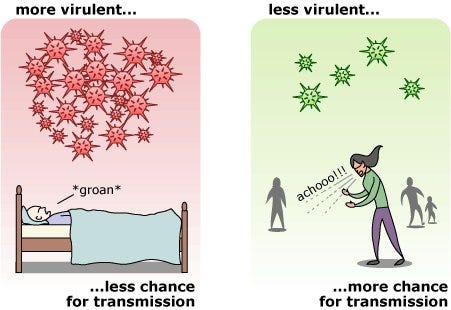





 Since the very beginning of the covid panic, the narrative has been this: implement severe lockdowns or your population will experience a bloodbath. Morgues will be overwhelmed, the death total toll will be astounding. On the other hand, we were assured those jurisdictions that do lock down would see only a fraction of the death toll.
Since the very beginning of the covid panic, the narrative has been this: implement severe lockdowns or your population will experience a bloodbath. Morgues will be overwhelmed, the death total toll will be astounding. On the other hand, we were assured those jurisdictions that do lock down would see only a fraction of the death toll.


 Aletho News
Aletho News