Letter to a Scientifically-Minded Friend
Case Study: The Ivermectin Disinformation Campaign
By Margaret Anna Alice | October 20, 2021
I noticed your pumpkin spice horse dewormer meme on Facebook. I didn’t react because none of the emojis captured the mixture of sadness, disappointment, and surprise I felt upon seeing it.
I am dismayed to see that you, as scientifically literate as you are, fell for the pharmaceutical corporations’ smear campaign against a Nobel-Prize–winning medication. If someone as intelligent, savvy, and rational as you could be deceived by such a brazenly undisguised disinformation campaign, what hope is there for the stupefied masses?
That said, I believe you are intellectually honest enough to consider the possibility that exceedingly lucrative lies are being peddled by the media, self-appointed mouthpieces, celebrities, politicians, and agencies lavishly paid for and wielded by BigPharma. And I would hope you would want to investigate to determine the truth for yourself rather than religiously Trusting The Science™ and attendant sound bytes being shoveled down our gullets every conscious moment.
Recall the escalating levels of duplicity, corruption, and malevolence depicted over the course of Breaking Bad—and multiply that cumulative nefariousness a thousandfold. Then add a few trillion dollars of captive, globally mandated profits, and you’ll begin to grasp why the Pharmaceutical Drug Cartel has harnessed every available mechanism of mass formation to induce hypnosis, coerce compliance, and mute the voices of scientists and medical professionals who persist in speaking the truth at grave risk to their livelihoods, reputations, and lives.
Understand that it was necessary for the pharmaceutical corporations to discredit any proven, cheap, effective alternatives to the vaccines to secure the Emergency Use Authorization that granted the manufacturers 100 percent immunity from liability—an appealing arrangement considering Pfizer was surely eager to avoid another landmark penalty like the $2.3 billion the U.S. Justice Department described as the largest health care fraud settlement in its history.
The fox is guarding the henhouse, the wolf is howling incessantly about his trustworthiness, the snake is strangling any roosters who sound the alarm, and the coyote is stringing barbed wire around the farm. Meanwhile, the Stockholm Syndrome–afflicted hens are gobbling up their feed, clucking proudly about their beloved guards, echoing every talking point, and furiously defending the predators against those who remain skeptical about their motives.
Getting back to ivermectin. As The Dude would say, “New shit has come to light.”
You probably heard the viral hit piece about the Oklahoma hospital turning away gunshot victims due to an influx of people overdosing on horse dewormer paste. You may not have heard the hospital issued a statement refuting that lie, which included the following:
“NHS Sequoyah has not treated any patients due to complications related to taking ivermectin. This includes not treating any patients for ivermectin overdose.
“All patients who have visited our emergency room have received medical attention as appropriate. Our hospital has not had to turn away any patients seeking emergency care.”
Rolling Stone was forced to issue a retraction, albeit still laden with biased language reinforcing the original unsubstantiated claims about ivermectin.
Perhaps you also heard about the Mississippi Health Department alert claiming “at least 70% of the recent calls [to the Mississippi Poison Control Center] have been related to ingestion of livestock or animal formulations of ivermectin.”
I suspect you didn’t know that, too, was bunkum. It was actually 2 percent. And out of that 2 percent (eight people), just four called with questions about ingestion of the livestock form of ivermectin—and only one was advised to seek care.
Thanks to the tenacious detective work of investigative reporters Mary Beth Pfeiffer and Linda Bonvie as described in this exposé, the New York Times, the Washington Post, The Guardian, and the Associated Press were all forced to issue corrections. (Incidentally, Mary Beth was subsequently locked out of her Twitter account for performing actual journalism instead of toeing the propaganda line.)
The New York Times appended its correction two weeks after the original article was published, casually noting, “An earlier version of this article misstated the percentage of recent calls to the Mississippi poison control center related to ivermectin. It was 2 percent, not 70 percent.”
The bogus 70-percent figure was then used by the FDA to launch its viral “You are not a horse” tweet, which raked up 23.7 million views in two days. How many of those people know that campaign was based on fallacious information? How many of those people care that they were ingesting and spreading lies about an exceptionally safe drug responsible for saving billions of lives since its genesis?
Still trust Big Media/Big Tech/the Ministry of Truth?
These are far from isolated examples of deceit. There are myriad instances of unabashed deception occurring in the pharma-funded media and technosphere. You’re right in that bots are a concern, but not in the way the propagandists are telling you. Rather, BigPharma fabrications of supposedly personal anecdotes are being propagated verbatim across thousands of social media accounts, and influencers are being paid to prop up a methodically crafted yet eminently fragile narrative that cannot survive unimpeded speech.
Also by the award-winning Mary Beth Pfeiffer, this heavily documented article dispels many of the falsehoods about ivermectin BigPharma has been cropdusting the public mind with. Here is another overview of the scientific literature by Dr. Colleen Huber, NMD.
A PubMed search of ivermectin currently returns 9,085 results. Do you think there would be more than 9,000 peer-reviewed journal articles on a horse dewormer? Antibiotics are used by veterinarians, too—who in their right mind would deny the efficacy of antibiotics for humans because of that?
Add COVID to the ivermectin PubMed search, and you get 296 results as of this writing—many documenting the extraordinary potential and success of treating COVID patients with ivermectin.1
In addition to inspecting the peer-reviewed literature, I recommend watching videos by credible scientists and medical professionals who are following the ethical demands of their profession and genuinely trying to discover the facts rather than serving as propaganda dissemination machines.
Dr. Mobeen Syed, for instance, examines the peer-reviewed literature and often draws helpful illustrations to walk viewers through the findings at a granular level. His videos are aimed at medical students, but because of that, he tends to delve deeper into the science than most. Here is Dr. Syed’s YouTube channel. You won’t find his videos on ivermectin there, though, because, as I hope you now realize, there is a media/Big Tech blackout on scientific facts that interfere with their disinformation campaigns. You can find those videos by going to his Odysee channel and typing “ivermectin” into the search. This video on Ivermectin in Action offers a quick overview to help you understand how it can be used to combat SARS-CoV-2.
This real-time analysis of more than 1,000 studies compares the effectiveness of different medications for early treatment. Ivermectin presently has the most studies (63) after hydroxychloroquine (294), and the pooled effects indicate ivermectin resulted in a 66-percent improvement in symptoms. Studies focusing on the use of ivermectin in combination with zinc, vitamin D, vitamin C, and other components of many early-treatment protocols suggest even higher efficacy levels.
This probably goes without saying, but hydroxychloroquine was subjected to the same slanderous tactics for the same reasons as ivermectin, and there are plenty of

An unwitting Goldstein, Trump played right into BigPharma’s strategy to discredit hydroxychloroquine by praising it—giving Trump Derangement Syndrome (a psychological disorder manufactured by and spread to tremendous monetary benefit and turnkey mass control by the media) sufferers the best and only reason they needed to dismiss it. They have been trained to plug their ears, cover their eyes, scream at the top of their lungs, and stamp their feet the instant any one of the Deplorables opens his mouth. One of the most effective instruments in the plutocracy’s toolkit, TDS has been brandished to misdirect the public for years, and it continues to work its magic despite Trump’s declining relevance, the embers of which the media will continue to fan as long as it pays dividends—just as Goldstein’s detested image is deployed in culturally unifying activities such as Two Minutes Hate:
In this undercover exposé featuring a Health & Human Services whistleblower, you’ll see that medical professionals at this federal facility are being threatened with loss of their jobs if they prescribe ivermectin to COVID patients (@ 10:44):
Think about this for a moment—why wouldn’t the public, the media, governments, health agencies, and everyone in the world be ecstatic about the possibility of an exceptionally cheap drug with more than four billion doses administered since 1998 and four decades’ worth of clinical data proving its safety and efficacy having the potential to save the lives of those who contract a disease people have been living in terror of for nearly two years now? What kind of contorted, harlequin world are we living in where lifesaving early-treatment protocols are being maligned as a threat? Don’t you find that suspicious?
If, after honestly examining the extensive scientific evidence demonstrating the value of ivermectin as a therapeutic against COVID—uncolored by the blinding biases that have been implanted in your consciousness to deter you from questioning, thinking for yourself, and researching the claims made in press releases issued from on high and regurgitated by talking heads, bots, and the unthinking public—you do come to realize they’ve been lying to you about ivermectin, ask yourself, What else are they lying about? Why would you believe anything they say, including their relentless efforts to demolish all who have the moral fortitude, intellectual prowess, and chutzpah to reveal the Big Lies being inflicted on the eagerly submissive populace?
And then consider this—what kind of next-level psychopaths would purposely sully the reputation of a drug that has the potential to drastically reduce mortality rates in COVID-19 patients? Again I ask, Why would you trust their credibility on any other aspect of the narrative they’ve concocted to drag us toward their rapacious and tyrannical ends?
Are you with me? Instead of permitting those malefactors to define your perception of reality, unplug from the Matrix (television, newspapers, radio, mainstream sources), detox from social media, and start conducting your own independent research outside the confines of what Big Brother allows you to see.
Scientific inquiry requires transparency, freedom from fear of reprisal, the liberal exchange of ideas, and encouragement of the pursuit of scientific truth—none of which are present in today’s COVID-1984 climate.
I realize this lengthy letter may seem like an overblown reaction to a meme intended to serve as light humor. When you understand that the vilification of a lifesaving medication has likely caused innumerable unnecessary deaths and will continue to do so if we serve as purveyors of such lethal smears, you might begin to fathom why I am responding this way.

If you want to understand the full scope of the mass subterfuge that has been staged since the beginning of this fiasco, you’ll need to venture off the trodden path and into the forest, where the free exchange of information is still permitted. You’ll need to shed the psychological barriers the cult leaders have installed to make you fear transgressing the perimeters they’ve defined for your mind.
They’ve lied about the people questioning the narrative. The people out here, in the forest, are nothing like what you’ve been bamboozled into believing. I am one of them. We are scientists; doctors; nurses; medical professionals; psychotherapists; professors; engineers; journalists; attorneys; writers; artists; musicians; filmmakers; truckers; teachers; construction workers; retirees; and creatives, independent thinkers, researchers, laborers, and ordinary folks of all stripes and colors. Some are Nobel Laureates; one knowingly risked a Nobel Prize.
We are the Book People of François Truffaut’s Fahrenheit 451:
You will find we share many of your values—especially your respect for science, your commitment to truth, your critical thinking skills, and your concern for humanity. It is for all those reasons and many more that we are standing against this new religion masquerading as science, its self-appointed priests, their colluders, and the tyranny they are facilitating.
People of every political persuasion and philosophy can be found here. What unites us above the superficial partisan partitions is a sincere desire for truth, justice, and freedom to prevail. We are anti-propaganda, anti-oppression, anti-censorship, and anti-corruption—basically, we are aligned with those who have opposed totalitarianism throughout history.
I understand it can be unnerving departing from the comfort zone mapped out for you, but it is also exceptionally liberating to take ownership of your own knowledge and to begin awakening from the mass psychosis that has befallen the globe.
You will be astonished at how evident the puppet strings become on others once you’ve severed your own. You will be able to observe the puppetry from afar, with a clarity of vision that renders the manipulation laughably apparent. And you will have freed your mind from their control, having begun the arduous yet infinitely rewarding process of recovery from menticide.
If you have questions about any aspect of the COVID narrative, please don’t hesitate to ask. While you will need to follow your own path to discovery, I can point you to resources I have found helpful along the way. I have invested thousands of hours’ worth of research into nearly every aspect of this phenomenon, having gotten well over a year’s head start. Yes, you have a lot of catching up to do when it comes to deprogramming from the Covidian cult beliefs and discovering the genuine science that has been censored, but you can also benefit from hindsight and the revelations that have emerged in the meantime.
For example, this well-documented crib sheet covers 30 basic facts you may be unaware of due to BigPharma/Big Media/Big Tech’s suppression efforts.
Since my blog is aimed at awakening people precisely like you, perusing past posts may answer some of your questions. I suggest starting with my first article, A Primer for the Propagandized: Fear Is the Mind-Killer, and working your way forward. You will also find a surfeit of resources in my Recommendations Roundups (e.g., Recommendations Roundup #1 and the subsequent Down Under Edition).
Here are a few Einstein quotes to inspire you on your journey of discovery:
“Science can flourish only in an atmosphere of free speech.”
“The important thing is not to stop questioning. Curiosity has its own reason for existence.”
“Unthinking respect for authority is the greatest enemy of truth.”
“A man should look for what is, and not for what he thinks should be.”
“The world is in greater peril from those who tolerate or encourage evil than from those who actually commit it.”
Finally, understand that I am saying all this because I respect and care for you. I have faith in your integrity, critical thinking skills, reasoning capacities, and willingness to explore content untainted by dubious funding and conflicts of interest.
I firmly believe that if you detach from the immersive, mind-controlling mainstream media; start reading and listening to the voices of the thousands of silenced scientists, medical professionals, and other individuals of profound knowledge and conscience speaking out; and start formulating your own conclusions based on scientific evidence instead of the illogical and constantly fluctuating baby food taradiddles being spooned into the public’s gaping mouth, the scales will fall from your eyes and you will recognize the catastrophic depth and breadth of the fraud that has been wreaked on the world. When that happens, you will switch allegiance from the tyrants to the people, adding your talents to the growing phalanx of conscientious objectors doing everything within our capacity to resist the totalitarian technocratic dystopia the compliant have been sleepwalking toward like hens to the fox.
Is Aspirin the New Horse Dewormer?
By Brian C. Joondeph, MD | American Thinker | October 18, 2021
Aspirin is one of those drugs that has been around forever. It is commonly used as a pain reliever, anti-inflammatory, and blood thinner. Surprisingly it may also have benefits in treating COVID.
A paper in Anesthesia and Analgesia published last spring titled, “Aspirin use is associated with decreased mechanical ventilation, intensive care unit admission, and in-hospital mortality in hospitalized patients with coronavirus disease 2019.”
This was a retrospective, observational study of adult patients admitted to multiple hospitals in the U.S. between March and July 2020, in the early days of COVID. The primary outcome addressed by the researchers from George Washington University was the need for mechanical ventilation, which then, and still now, carries an extremely high chance of never leaving the ICU alive.
This was not a gold standard randomized prospective clinical trial. That would not be feasible in this situation since study patients were already hospitalized and critically ill. Remember in the early days, one needed to be extremely ill before even being admitted to the hospital rather than being sent home until sick enough to return and go straight to the ICU.
But the results were impressive. As reported last week by the Jerusalem Post,
The team investigated more than 400 COVID patients from hospitals across the United States who take aspirin unrelated to their COVID disease, and found that the treatment reduced the risk of several parameters by almost half: reaching mechanical ventilation by 44%, ICU admissions by 43%, and overall in-hospital mortality by 47%.
Why would aspirin be helpful for COVID, a respiratory disease? What if COVID is more than simply a lung disease or pneumonia? COVID is actually thought to be a microvascular disease causing blood clots, as described in the medical journal Circulation,
Although most patients with coronavirus disease 2019 (COVID-19) present with a mild upper respiratory tract infection and then recover, some infected patients develop pneumonia, acute respiratory distress syndrome, multi-organ failure, and death. Clues to the pathogenesis of severe COVID-19 may lie in the systemic inflammation and thrombosis observed in infected patients. We propose that severe COVID-19 is a microvascular disease in which coronavirus infection activates endothelial cells, triggering exocytosis, a rapid vascular response that drives microvascular inflammation and thrombosis.
Note the thrombosis aspect, blood clots forming in the lungs and elsewhere in the body. Aspirin, as a blood thinner, reduces the risk of blood clots, explaining its potential benefit for COVID.

YouTube screen grab
For the same reason, the American Heart Association recommends,
If you have had a heart attack or stroke, your doctor may want you to take a daily low dose of aspirin to help prevent another. Aspirin is part of a well-established treatment plan for patients with a history of heart attack or stroke.
Add the appropriate caveat, which I would echo, “You should not take daily low-dose aspirin on your own without talking to your doctor. The risks and benefits vary for each person.”
How did aspirin get its start? Over 3,500 years ago, willow bark, known as “nature’s aspirin,” was used as a painkiller and antipyretic by ancient Egyptians and Greeks, and in a chemical synthesis by a Bayer chemist in 1897.
Aside from pain relief, it was found to have anti-platelet and anti-cancer effects. It’s also on the World Health Organization’s list of essential medicines, along with another familiar drug, ivermectin. The Harvard-based physicians’ health study in the 1980s found that low-dose aspirin reduced the risk of heart attack by 44 percent.
A recently published Israeli study found, “Aspirin use is associated with better outcomes among COVID-19 positive patients.” This included a lower likelihood of infection, disease duration, and hospital survival. In other words, aspirin works as both a preventative and as a treatment.
Aspirin is another potential therapeutic, along with hydroxychloroquine and ivermectin, which is inexpensive, readily available, and relatively safe, and could save countless lives when used appropriately for COVID. An editorial in Anesthesia and Analgesia described aspirin for COVID as, “An old, low-cost therapy with a strong rationale.” And right on cue, it’s time for aspirin-bashing to commence.
At the same time as these papers showing potential benefits of aspirin for COVID hit the news, the U.S. Preventative Services Task Force, on Oct. 12, posted draft recommendations saying that, “Once people turn 60 years old, they should not consider starting to take aspirin because the risk of bleeding cancels out the benefits of preventing heart disease.” What curious timing.
Certainly, aspirin has potential side effects including an increased risk of bleeding. All medications have side effects and one can even die from drinking too much water. It always comes down to medical decision-making, balancing risks and benefits, in consultation with one’s healthcare provider.
The media wasted no time in using the suddenly released and new aspirin recommendations at the same time as news reports on aspirin benefits for COVID hit the news.
NBC reported, “Most adults shouldn’t take daily aspirin to prevent heart attack, panel says.” The New York Times echoed, “Daily low-dose aspirin no longer recommended by doctors, if you’re healthy.” Healthline went further, “Doctors warn daily aspirin use can be dangerous.” Driving or walking across the street can be dangerous too.
Sound familiar? How many adults have been taking low-dose aspirin daily for many years, based on the decades-old Harvard study? I have as I have a family history of cardiovascular disease and my internist and I agree that the benefits outweigh the risks, despite the new recommendations.
Similarly how many patients have been taking hydroxychloroquine for years or decades for arthritis or lupus, without dying from the drug as Fox News crank Neil Cavuto warned last year? How many take ivermectin to prevent parasitic infections? Now we can add aspirin to the list of once safe and effective medications — that’s now on par with cyanide or strychnine.
It seems the medical establishment and the media want to squash any potential COVID therapeutic, especially the inexpensive ones, instead pushing vaccines and extremely pricey medicines like Merck’s new $712 COVID drug.
The media described ivermectin as horse dewormer or animal paste, seemingly unaware that it is an FDA-approved medication for human use and was once honored with a Nobel Prize. Watch Joe Rogan put CNN’s medical mouthpiece, Dr. Sanjay Gupta, in a virtual chokehold until he tapped out and admitted to CNN’s irresponsible reporting and lying about ivermectin.
Aspirin also has non-medical uses including as a stain remover, garden enhancer, and dandruff remedy. I would love to hear President Trump mention the potential benefits of aspirin for COVID and see the news headlines of Trump recommending people ingest detergent, fertilizer, or shampoo to treat COVID.
Welcome to simple aspirin, the media’s new horse dewormer.
Brian C. Joondeph, M.D., is a physician and writer.
Propaganda, Character Assassination & the Campaign Against Prof David Miller
By Dr Piers Robinson | OffGuardian | October 19, 2021
On October 1st 2021, the University of Bristol decided to buckle in the face of a near 3 year-long pro-Israel lobby campaign and fire Professor David Miller.
I have worked with David for many years now, co-published work on the theory of propaganda, researched and written about the UK FCO propaganda operation (ongoing) that has sought to overthrow the Syrian government, and developed the fledgling Organisation for Propaganda Studies.
David was, is, and will continue to be, a major intellectual force with respect to our understanding of propaganda, and his integrity, particularly in relation to the Israel-Palestine issue, is now cemented in history. He became a voice for the Palestinians, highlighting the ways in which propaganda has worked in order to simultaneously suppress public understanding of the nefarious actions of the Israeli government against them and erase awareness of their plight.
Inevitably and predictably he became an essential target for the pro-Israel lobby and the implementation of a remarkably sustained and aggressive campaign designed to falsely smear him as ‘anti-Semitic’ and have him fired.
I also have a relationship with the University of Bristol. I studied for my MSc in International Relations back in 1996-97 (funded by the Economic and Social Research Council [ESRC]) and continued in 1997 to undertake a PhD (also ESRC funded) under the supervision of Professor Eric Herring. I left at the end of the 2nd year of the PhD to take up my first full-time academic post at the University of Liverpool, School of Politics and Communication Studies. My PhD was awarded in 2000 from the University of Bristol.
Smear campaigns and character assassination are a core feature of contemporary propaganda and our ‘democratic’ landscape. There is even an academic Handbook on the tactic, titled The Routledge Handbook of Character Assassination and Reputation Management, whilst US investigative journalist Sharyl Atkinson has provided a powerful account detailing how legitimate political views are stifled through nefarious attempts to destroy reputations.
I have witnessed this tactic first hand through my experience researching propaganda and the war on Syria.
For the ‘thought crime’ of questioning and researching UK government-linked ‘influence operations’ in that war, in particular the controversy over the OPCW (Organisation for the Prohibition of Chemical Weapons) and the alleged chemical weapon attack in Douma 2018, myself and other colleagues (including David), have been subjected to aggressive and continuous smearing some of which is documented here.
Even when OPCW whistleblower scientists emerged and corroborated what we had been saying, those attacking us have simply continued with accusations of our being ‘conspiracy theorists’, ‘war crime deniers’ and agents of ‘disinformation’. That smear campaign also now incorporates OPCW whistleblowers with attempts to blacken their reputations.
What we see today is not completely new and David’s experience is not an isolated one.
In an earlier era, scientists such as Professor Steven Jones were smeared and pushed from their positions when raising perfectly objective, evidence-based and rational questions regarding 9/11. Chemist and laboratory director Kevin Ryan was fired for blowing the whistle on his own company which had obfuscated evidence related to the building collapses that occurred on 9/11.
To this day, and as Dr David Hughes has recently detailed in an academic journal, mainstream academia continues to self-censor and avoid substantial analysis of 9/11.
Today, with Covid-19, we now appear to be seeing an unprecedented level of attacks on academics who have raised what are, again, perfectly objective, evidence-based and rational questions regarding the efficacy of lockdowns and the drive toward coerced/mandated injections.
High profile and leading academics such as Sunetra Gupta (University of Oxford) and even Professor Robert Malone, inventor of mRNA technology used in the current Covid-19 injection, have had to battle concerted drives to discredit them, with, for example, Gupta being accused of being a ‘conspiracy theorist’.
Professor Sucharit Bhakdi, an early critic of lockdown, has been accused of anti-Semitism in what appears to be a wildly ill-founded and crude attempt to discredit his expertise.
The assault on professional autonomy appears to be accelerating rapidly with Professor Robert Malone declaring in October 2021 that:
[p]hysicians who speak out are being actively hunted via medical boards and the press. They are trying to delegitimize and pick us off one by one…This is happening globally.”
Something is indeed ‘rotten in the state of Denmark’.

In David’s case we have seen how powerful actors, in this case the pro-Israel lobby and the Israeli government, have worked to organize and influence in order to build sufficient pressure on the University of Bristol so that they would take the extreme step of firing him.
The campaign has been huge and drawn upon both mainstream media and celebrity influencers, as well as student bodies, in order to relentlessly misrepresent his work as anti-Semitic when, in truth, David’s views and work are based on a clear commitment against racism and discrimination.
It is worth noting that an independent report from a QC, commissioned by the University of Bristol, concluded that Professor Miller’s comments did not constitute unlawful speech and had also explicitly determined his remarks were not anti-Semitic. And, in all of this controversy, the progressive destruction of the Palestinian people and the illegal actions of the state of Israel government continue unabated.
Of course, it is this wider issue that those attacking David most want us all to forget. By allowing itself to play along with a nefarious campaign to smear and cancel David, the University of Bristol has become an important element in what are widely acknowledged to be crimes and atrocities. In doing so the University has clearly placed itself on the wrong side of history.
Smear campaigns and character assassination, then, are nothing new; but they are now intensified to the point that academics such as David are being fired, and high-profile scientists even from the medical sciences are targeted. Freedom of speech and freedom of expression cannot flourish in this environment and nor can academia, especially when rational debate is being supplanted with propaganda and politicized science.
Our ability to evaluate, debate, and speak truth to power are being fundamentally undermined and, along with that, so is any pretence that we live in a functioning democracy. That the University of Bristol has become an active participant in these nefarious processes should be a source of shame for all those who work there. For sure, the memories of my time there are forever tarnished and I will never again think fondly of my postgraduate days at Bristol nor speak in positive terms about the institution.
David’s experience is part of a wider process across democracies whereby power has sought to wrestle control of both professional classes and publics. We will now see, in the coming years, who will prevail.
Trust in institutions, whether government, mainstream media or academia, is likely to decline and rapidly so. And we are now living in an era when there are unprecedented opportunities for the development of new institutions in which freedom of expression and speaking truth to power are cherished, promoted and protected.
The vibrant independent media scene and increasingly discredited mainstream media are good examples of these dynamics although, as Glen Greenwald explains here, there is a concerted drive by political power and corporate media to regain control; I doubt they will ever succeed.
The pro-Israel lobby and the University of Bristol might think that they have secured a major victory in their campaign to silence critical debate on Israel, but they will not have the last word and, certainly, they will not have succeeded in silencing Professor Miller nor putting a stop to his essential work.
Despite the personal loss, and unlike the University of Bristol, Professor Miller will emerge stronger and more influential than ever.
A petition in support of Professor Miller can be signed here.
Dr Piers Robinson is co-Director of the Organisation for Propaganda Studies, convenor of the Working Group on Syria, Media and Propaganda and associated researcher with the Working Group on Propaganda and the 9/11 ‘Global War on Terror.
Vaccine Safety Update
By Will Jones • The Daily Sceptic • October 19, 2021
This is the 14th of the round-ups of Covid vaccine safety reports and news compiled by a group of medical doctors who are monitoring developments but prefer to remain anonymous in the current climate (find the 13th one here).
By no means is this part of an effort to generate alarm about the vaccines or dissuade anyone from getting inoculated. It should be read in conjunction with the Daily Sceptic‘s other posts on vaccines, which include both encouraging and not so encouraging developments. At the Daily Sceptic we report all the news about the vaccines whether positive or negative and give no one advice about whether they should or should not take them. Unlike with lockdowns, we are neither pro-vaccine nor anti-vaccine; we see our job as reporting the facts, not advocating for or against a particular policy. The vaccine technology is novel and the vaccines have not yet fully completed their trials, which is why they’re in use under temporary and not full market authorisation. This has been done on account of the emergency situation and the trial data was largely encouraging on both efficacy and safety. For a summary of that data, see this preamble to the Government’s page on the Yellow Card reporting system. (Dr Tess Lawrie in June wrote an open letter to Dr June Raine, head of the MHRA, arguing that: “The MHRA now has more than enough evidence on the Yellow Card system to declare the COVID-19 vaccines unsafe for use in humans,” a claim that has been ‘fact checked’ here.) We publish information and opinion to inform public debate and help readers reach their own conclusions about what is best for them, based on the available data.
- On October 7th, the deaths reported as adverse events from vaccination in Taiwan overtook the number of deaths following Covid infection.
- Infection rates in England in vaccinated people aged 40-49 is now more than double the rate in the unvaccinated. Evidence now suggests that vaccinated people can spread the Delta variant and a study has shown that six months after the second dose of the Pfizer vaccine, antibody levels in healthcare workers had decreased substantially.
- The first case of vaccine induced thrombotic thrombocytopaenia following the J&J vaccine outside of the USA was documented.
- Sweden, Denmark, Iceland and Finland have temporarily halted the use of Moderna’s COVID-19 vaccine for people under the age of 30 due to heart risks.
- There has been a case of reactivation of hepatitis C infection following the Pfizer vaccination.
- A large number of studies are increasingly showing evidence of robust natural immunity from natural Covid infection.
- There have been calls for clearer ONS data on the rise in deaths of young males in England and Wales. Investigation of official ONS data indicates that since the Covid vaccine has been rolled out to teens, there has been a significant increase in deaths in this age group.
- The Senate in France voted against making the Covid vaccine mandatory.
- EudraVigilance – the equivalent of the Yellow Card reporting system in the EU – has logged (up to October 9th) 1,038,776 reports of 2,536,526 adverse events, including 27,242 deaths.
- DAEN Australia – the equivalent of the Yellow Card reporting system – has logged (up to September 29th) 63,672 reports of 204,746 adverse events, including 566 deaths.
Summary of Adverse Events in the U.K.
According to an updated report published on October 14th, the MHRA Yellow Card reporting system has recorded a total of 1,228,991 events based on 372,878 reports. The total number of fatalities reported is 1,719.
- Pfizer (22.7 million first doses, 19.8 million second doses) now has one Yellow Card in 188 people vaccinated. Deaths: 1 in 40,391 people vaccinated (562).
- AstraZeneca (24.9 million first doses, 24 million second doses) has one Yellow Card in 106 people vaccinated. Deaths: 1 in 22,514 people vaccinated (1,106).
- Moderna (1.5 million first doses, 1.2 million second doses) has one Yellow Card in 90 people vaccinated. Deaths: 1 in 75,000 people vaccinated (20).
Overall, one in every 132 people vaccinated (0.76%) have experienced a Yellow Card adverse event. The MHRA has previously estimated that the Yellow Card reporting rate may be approximately 10% of actual figures.
- Thrombosis & Embolism (all types) = 7,072
- Anaphylaxis = 1,353
- Acute Cardiac = 16,092
- Pericarditis/Myocarditis (Heart inflammation) = 1,000
- Herpes = 4,322
- Headaches & Migraines = 122,717
- Blindness = 424
- Deafness = 599
- Spontaneous Abortions = 593 miscarriages + 13 foetal deaths/stillbirths
- Facial Paralysis incl. Bell’s Palsy = 1,752
- Strokes and CNS haemorrhages = 2,662
- Guillian Barre Syndrome = 491
- Pulmonary Embolism & Deep Vein Thrombosis = 3,502
- Seizures = 2,872
- Paralysis = 1,173
- Nosebleeds = 3,120
- Dizziness = 35,509
- Vomiting = 15,807
- Reproductive/Breast Disorders= 43,969
Further analysis can be found via the UK Freedom Project.

Source: Pfizer; Moderna; AstraZeneca; Unspecified. “F” denotes fatal.
Official Government Reports Show Vaccinated Lost 40% Of Their Immunity
THE EXPOSÉ • OCTOBER 10, 2021
Latest UK PHE Vaccine Surveillance Report figures on Covid cases show that doubly vaccinated 40-70 year olds have lost 40% of their immune system capability compared to unvaccinated people.
Their immune systems are deteriorating at around 5% per week (between 2.7% and 8.7%). If this continues then 30-50 year olds will have 100% immune system degradation, zero viral defence by Christmas and all doubly vaccinated people over 30 will have lost their immune systems by March next year.
The 5 PHE tables below from their excellent Vaccine Surveillance Report, separated by 4 weeks, clearly show the progressive damage that the vaccines are doing to the immune system’s response.
People aged 40-69 have already lost 40% of their immune system capability and are losing it progressively at 3.3% to 6.4% per week.
Weekly Decline in doubly vaccinated immune system performance compared to unvaccinated people…

Everybody over 30 will have lost 100% of their entire immune capability (for viruses and certain cancers) within 6 months.
30-50 year olds will have lost it by Christmas. These people will then effectively have full blown acquired immunodeficiency syndrome and destroy the NHS.
The vaccine booster shots have to be the same as the vaccines themselves, because it takes forever to do clinical trials and get approval for something different. So if you take a booster shot, these figures show that you are giving yourself an even faster progressive form of acquired immunodeficiency syndrome (after a couple of months of effectiveness).
Table 2. COVID-19 cases by vaccination status…
Cases reported by specimen date between week 32 and week 35 2021 – https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1016465/Vaccine_surveillance_report_-_week_36.pdf

Cases reported by specimen date between week 33 and week 36 2021 – https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1018416/Vaccine_surveillance_report_-_week_37_v2.pdf

Cases reported by specimen date between week 34 and week 37 2021 – https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1019992/Vaccine_surveillance_report_-_week_38.pdf

Cases reported by specimen date between week 35 and week 38 2021 – https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1022238/Vaccine_surveillance_report_-_week_39.pdf

Cases reported by specimen date between week 36 and week 39 2021 – https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1023849/Vaccine_surveillance_report_-_week_40.pdf

Pfizer originally claimed a 95% efficiency for their vaccine (calculated as in the last column above). The figures above indicate that their figures may well have been correct immediately after vaccination (the younger age groups have had the vaccine for the shortest time).
But the figures above also show that the vaccines do NOT merely lose efficiency over time down to zero efficiency, they progressively damage the immune system until a negative efficiency is realised. They presently leave anybody over 30 in a worse position than they were before vaccination. For more see here.
Lockdown: Where Did ‘The Science’ Come From?
By Noah Carl • The Daily Sceptic • October 19, 2021
In a previous post, I looked at where ‘The Science’ of community masking came from. Here I’ll do the same thing for lockdowns.
As many lockdown sceptics (including myself) have noted, lockdowns represent a radical departure from conventional forms of pandemic management. There is no evidence that, before 2020, they were considered an effective way to deal with influenza pandemics.
In a 2006 paper, four leading scientists (including Donald Henderson, who led the effort to eradicate smallpox) examined measures for controlling pandemic influenza. Regarding “large-scale quarantine”, they wrote, “The negative consequences… are so extreme” that this measure “should be eliminated from serious consideration”.
Likewise, a WHO report published mere months before the COVID-19 pandemic classified “quarantine of exposed individuals” as “not recommended under any circumstances”. The report noted that “there is no obvious rationale for this measure”.
And we all know what the U.K.’s own ‘Pandemic Preparedness Strategy’ said, namely: “It will not be possible to halt the spread of a new pandemic influenza virus, and it would be a waste of public health resources and capacity to attempt to do so.”
As an additional exercise, I searched the pandemic preparedness plans of all the English-speaking Western countries (U.K., Ireland, U.S., Canada, Australia and New Zealand) for mentions of ‘lockdown’, ‘lock-down’ ‘lock down’ or ‘curfew’.
Only ‘curfew’ was mentioned, and only once – in Ireland’s plan. The relevant sentence was: “Mandatory quarantine and curfews are not considered necessary.” None of the lockdown strings were mentioned in any of the countries’ plans.
So where did ‘The Science’ of controlling Covid using lockdowns come from? As everyone knows, China implemented the first lockdown (of Hubei province) in January of 2020. Yet it wasn’t until March that lockdowns became part of ‘The Science’.
As this chart taken from the paper by David Rozado shows, major Western media outlets did not start mentioning ‘lockdown’ frequently until March:
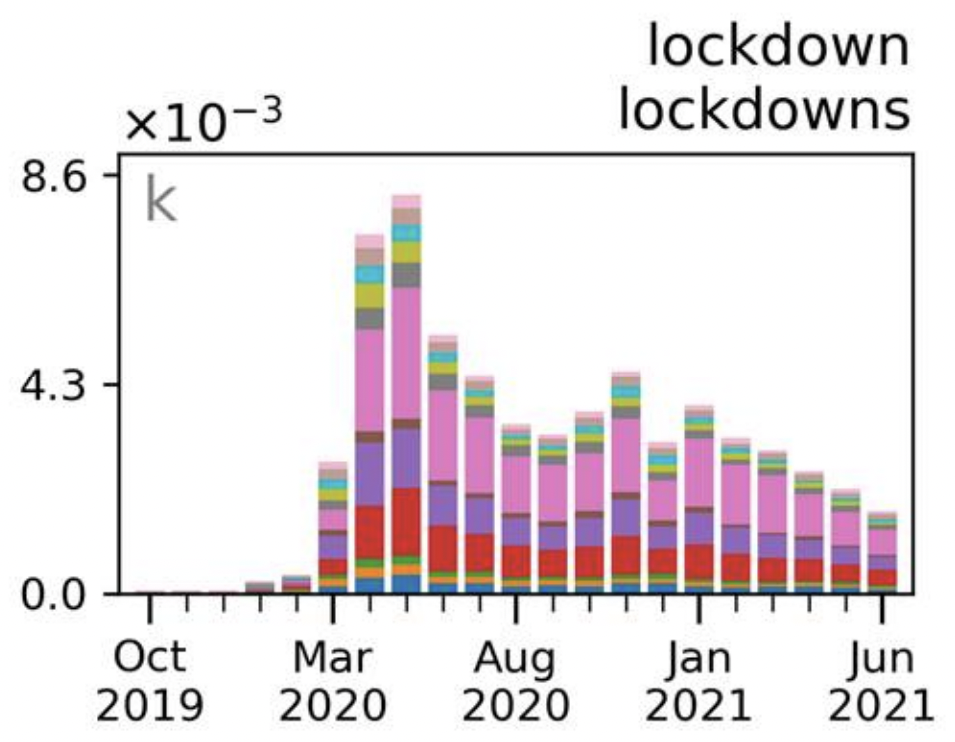
And this chart confirms that worldwide Google search interest for ‘lockdown’ was essentially nil until 8th March 2020:
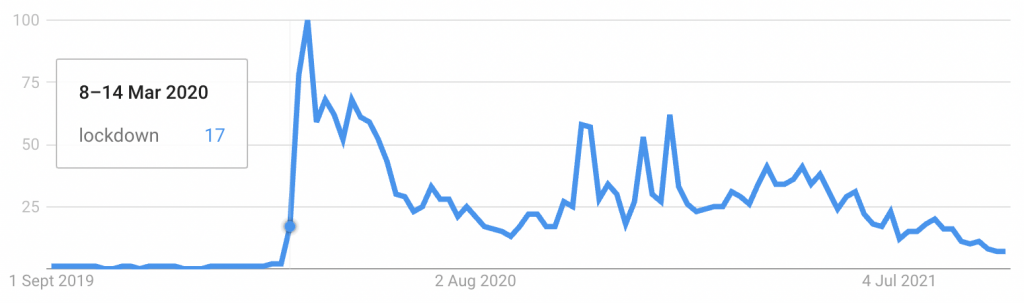
So what happened in early March? Well, Italy was the first Western country to lock down – on 9th March last year. And as Michael Senger argues, its decision appears to have been prompted by the WHO’s report of 24th February, which gave a glowing evaluation of China’s lockdown. (Senger’s piece is well worth reading.)
Other Western countries then followed suit. The next most important event, following Italy’s decision to lock down, was the publication of a report by Neil Ferguson’s team on 16th March.
This report has been described as the “catalyst for policy reversal”. Up until then, the U.K. had been more or less following its pandemic preparedness plan. As late as March 5th, Chris Whitty told the Health and Social Care Committee that “what we’re very keen to do is minimise social and economic disruption”.
Although other, similar reports had already been published, the analysis by Neil Ferguson’s team was seen as particularly authoritative. According to the New York Times, the report “also influenced the White House to strengthen its measures”.
On March 17th, Neil Ferguson and his colleagues held a press conference after returning from Downing Street. They confirmed that Britain would be adopting a new strategy. “The aim is not to slow the rate of growth of cases but actually pull the epidemic into reverse,” Ferguson said.
As to why the U.K. was changing tack, Ferguson noted, “We have had bad news from Italy and from early experience in UK hospitals”. However, subsequent revelations suggest that “bad news” was less important than the shifting of the Overton window.
In an interview with the Times published in December last year, Ferguson noted that “people’s sense of what is possible in terms of control changed quite dramatically between January and March”. Referring to China’s lockdown, he elaborated, “We couldn’t get away with it in Europe, we thought… And then Italy did it. And we realised we could”.
After China’s initial response in Hubei, it took two months for lockdowns to go from ‘unprecedented’ to ‘unavoidable’. They received two major doses of intellectual credibility: first from the WHO, and then from Neil Ferguson’s team. Italy set the all-important precedent for Western countries.
As to whether one should trust ‘The Science’ on lockdowns, a reasonable answer would be, ‘Do you mean the pre or the post-Covid science?’
Nebraska AG Says Doctors Can Legally Prescribe Ivermectin, HCQ for COVID, Calls Out FDA, CDC, Fauci, Media for ‘Fueling Confusion and Misinformation’
By Megan Redshaw | The Defender | October 18, 2021
Few subjects have been more controversial than ivermectin and hydroxychloroquine — two long-established, inexpensive medications widely and successfully used in many parts of the world for the prevention and treatment of COVID.
By contrast, the use of both medications against COVID has been largely suppressed in the U.S, where doctors have been threatened and punished for prescribing them.
On Oct. 15, Nebraska Attorney General (AG) Doug Peterson issued a legal opinion that Nebraska healthcare providers can legally prescribe off-label medications like ivermectin and hydroxychloroquine for the treatment of COVID, so long as they obtain informed consent from the patient.
However, if they did neglect to obtain consent, deceive, prescribe excessively high doses or other misconduct, they could be subject to discipline, Peterson wrote.
The AG’s office emphasized it was not recommending any specific treatment for COVID. “That is not our role,” Peterson wrote. “Rather, we address only the off-label early treatment options discussed in this opinion and conclude that the available evidence suggests they might work for some people.”
Peterson said allowing physicians to consider early treatments will free them to evaluate additional tools that could save lives, keep patients out of the hospital and provide relief for our already strained healthcare system.
The opinion, based on an assessment of relevant scientific literature, was rendered in response to a request by Dannette Smith, CEO of the Nebraska Department of Health and Human Services.
Smith asked the AG’s office to look into whether doctors could face discipline or legal action under Nebraska’s Uniform Credential Act (UCA) — meant to protect public health, safety and welfare — if they prescribed ivermectin or hydroxychloroquine.
“After receiving your question and conducting our investigation, we have found significant controversy and suspect information about potential COVID-19 treatments,” Peterson wrote.
For example, a paper published in the Lancet — one of the most prestigious medical journals in the world — denounced hydroxychloroquine as dangerous, yet the statistics were flawed and the authors refused to provide analyzed data.
The paper was retracted, but not before countries stopped using the drug and trials were cancelled or interrupted.
“The Lancet’s own editor-in-chief admitted that the paper was a ‘fabrication,’ a ‘monumental fraud’ and a ‘shocking example of research misconduct’ in the middle of a global health emergency,” Peterson wrote in the opinion.
A recently published paper on COVID recognized that “for reasons that are yet to be clarified,” early treatment has not been emphasized despite numerous U.S. healthcare providers advocating for early treatment and “scores of treating and academic physicians” — who have published papers in well respected journals — urging early interventions.
Peterson cited numerous studies showing ivermectin and hydroxychloroquine reduced mortality by up to 75% or more when used as a preventative or prophylaxis for COVID, suggesting hundreds of thousands of lives could have been saved had the drugs been widely used in America.
“Every citizen — Democrat or Republican — should be grateful for Doug Peterson’s thoughtful and courageous counteroffensive against the efforts of Big Pharma, its captive federal regulators, and its media and social media allies to silence doctors and deny Americans life-saving treatments,” Robert F. Kennedy Jr., chairman of Children’s Health Defense, told The Defender via email.
“We finally have a leader who puts constitutional rights, peer-reviewed science and human health above industry profits. Doug Peterson is uncowed and unbowed — a genuine hero on horseback for all Americans.” Kennedy said.
Children’s Health Defense President Mary Holland agreed. “This Nebraska AG opinion lets doctors get back to being doctors — without being second-guessed by government, pharmacists and others interfering in the crucial doctor-patient relationship,” Holland said.
Although the AG’s office did not rule out the possibility that other off-label drugs might show promise — either now or in the future — as a prophylaxis or treatment against COVID, it confined its opinion to ivermectin and hydroxychloroquine for the sake of brevity.
Nebraska AG highlights science on ivermectin
In his legal opinion, Peterson concluded evidence showed ivermectin demonstrated striking effectiveness in preventing and treating COVID, and any side effects were primarily minor and transient. “Thus, the UCA does not preclude physicians from considering ivermectin for the prevention or treatment of COVID,” Peterson wrote.
In the decade leading up to the COVID pandemic, Peterson found numerous studies showing ivermectin’s antiviral activity against several RNA viruses by blocking the nuclear trafficking of viral proteins, adding to 50 years of research confirming ivermectin’s antiviral effects.
In addition, safety data for ivermectin showed side effects were “vanishingly small.” The latest statistics available through VigiAccess reported only 5,674 adverse drug reactions to ivermectin between 1992 and October 13, 2021, an “incredibly low” number given that 3.7 billion doses have been administered since the 1980s, Peterson wrote.
Peterson cited several studies showing ivermectin led to improvement of COVID outcomes when used in early treatment or as a prophylaxis, while noting many studies with negative findings about ivermectin “excluded most available evidence,” cherry picked data within studies, misreported data, made unsupported assertions of adverse reactions to ivermectin and had “conclusions that did follow from evidence.”
Peterson also found that epidemiological evidence for ivermectin’s effectiveness, derived by analyzing COVID-related data from various states, countries or regions is instructive in the context of a global pandemic.
In one instance, a group of scholars analyzed data comparing COVID rates of countries that routinely administer ivermectin as a prophylaxis and countries that did not. The research showed “countries with routine mass drug administration of prophylactic … ivermectin have a significantly lower incidence of COVID-19.”
“This ‘highly significant’ correlation manifests itself not only ‘in a worldwide context’ but also when comparing African countries that regularly administer prophylactic ‘ivermectin against parasitic infections’ and African countries that do not,” Peterson wrote. “Based on these results, the researchers surmised that these results may be connected to ivermectin’s ability to inhibit SARS-CoV-2 replication, which likely leads to lower infection rates.”
Nebraska AG calls out FDA, Fauci on hypocrisy on ivermectin
Many U.S. health agencies have now addressed the use of ivermectin for COVID. The National Institutes of Health (NIH) has adopted a neutral position, choosing not to recommend for or against the use of ivermectin — a change from its position in January 2021 where it discouraged use of the drug for treatment of COVID.
Peterson wrote:
“The reason for the change is the NIH recognized several randomized trials and retrospective cohort studies of ivermectin use in patients with COVID-19 have been published in peer-reviewed journals. And some of those studies reported positive outcomes, including shorter time to resolution of disease manifestations that were attributed to COVID-19, greater reduction in inflammatory marker levels, shorter time to viral clearance, [and] lower mortality rates in patients who received ivermectin than in patients who received comparator drugs or placebo.”
Yet, on Aug. 29, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases within the NIH, went on CNN and announced “there is no clinical evidence” that ivermectin works for the prevention or treatment of COVID. Fauci went on to reiterate that “there is no evidence whatsoever” that it works.
“This definitive claim directly contradicts the NIH’s recognition that ‘several randomized trials … published in peer-reviewed journals’ have reported data indicating that ivermectin is effective as a COVI D-19 treatment,” Peterson wrote.
In March 2021, the FDA posted a webpage, “Why You Should Not Use lvermectin to Treat or Prevent COVID-19.”
“Although the FDA’s concern was stories of some people using the animal form of ivermectin or excessive doses of the human form, the title broadly condemned any use of ivermectin in connection with COVID-19,” Peterson wrote. “Yet, there was no basis for its sweeping condemnation.”
Peterson wrote:
“Indeed, the FDA itself acknowledged on that very webpage (and continued to do so until the page changed on September 3, 2021) that the agency had not even ‘reviewed data to support use of ivermectin in COVID-19 patients to treat or to prevent COVID-19.’ But without reviewing the available data, which had long since been available and accumulating, it is unclear what basis the FDA had for denouncing ivermectin as a treatment or prophylaxis for COVID-19.
“On that same webpage, the FDA also declared that ‘[i]vermectin is not an anti-viral (a drug for treating viruses).’ It did so while another one of its webpages simultaneously cited a study in Antiviral Research that identified ivermectin as a medicine ‘previously shown to have broad-spectrum anti-viral activity.’”
“It is telling that the FDA deleted the line about ivermectin not being ‘anti-viral’ when it amended the first webpage on September 3, 2021,” Peterson noted.
Peterson said the FDA’s most controversial statement on ivermectin was made on Aug. 21, when it posted a link on Twitter to its “Why You Should Not Use lvermectin” webpage with this statement: “You are not a horse. You are not a cow. Seriously, y’all. Stop it.”
“This message is troubling not only because it makes light of a serious matter but also because it inaccurately implies that ivermectin is only for horses or cows,” Peterson wrote.
Peterson said the FDA has assailed ivermectin’s safety while ignoring the fact that physicians routinely prescribe medications for off-label use and that ivermectin is a “particularly well-tolerated medicine with an established safety record.”
Peterson added the FDA is ignoring several randomized controlled trials and at least one metaanalysis suggesting ivermectin is effective against COVID. He pointed out the Centers of Disease Control and Prevention has adopted a similar stance — unsupported by scientific evidence — and the media has fueled confusion and misinformation on the drug.
Peterson questions professional associations’ stance on ivermectin
Professional associations in the U.S. and internationally have adopted conflicting positions on ivermectin and COVID. The American Medical Association (AMA), American Pharmacists Association (APhA) and American Society of Health-System Pharmacists (ASHP) issued a statement in September strongly opposing the ordering, prescribing or dispensing of ivermectin to prevent or treat COVID outside of a clinical trial.
But their statement relied solely on the FDA’s and CDC’s suspect positions.
The AMA, APhA and ASHP also mentioned a statement by Merck — the original patent-holder — opposing the use of ivermectin for COVID because of a “concerning lack of safety data in the majority of studies.”
“But Merck, of all sources, knows that ivermectin is exceedingly safe, so the absence of safety data in recent studies should not be concerning to the company,” Peterson wrote.
Peterson called into question the objectivity of Merck in providing an opinion on ivermectin that U.S. health agencies are relying upon. “Why would ivermectin’s original patent holder go out of its way to question this medicine by creating the impression that it might not be safe?” Peterson asked. “There are at least two plausible reasons.”
Peterson explained:
“First, ivermectin is no longer under patent, so Merck does not profit from it anymore. That likely explains why Merck declined to ‘conduct clinical trials’ on ivermectin and COVID-19 when given the chance.
“Second, Merck has a significant financial interest in the medical profession rejecting ivermectin as an early treatment for COVID-19. [T]he U.S. government has agreed to pay [Merck] about $1.2 billion for 1.7 million courses of its experimental COVID-19 treatment, if it is proven to work in an ongoing large trial and authorized by U.S. regulators.”
Merck’s treatment is known as “molnupiravir,” and aims to stop COVID from progressing when given early in the course of disease. When Merck announced Oct. 1, that preliminary studies indicated molnupiravir reduced hospitalizations and deaths by half, the drug maker’s stock price immediately jumped to 12.3%.
“Thus, if low-cost ivermectin works better than, or even the same as molnupiravir, that could cost Merck billions of dollars,” Peterson wrote.
Peterson takes on science of hydroxychloroquine
Peterson said based on his review of the evidence, his office did not find clear and convincing evidence that would warrant disciplining physicians who prescribe hydroxychloroquine for the prevention or early treatment of COVID after first obtaining informed patient consent.
Peterson pointed to similar findings with hydroxychloroquine — a less toxic derivative of a medicine named chloroquine — widely used since it was approved by the FDA in 1955 for treatment of malaria.
Peterson noted that as early as 2004, a lab study revealed chloroquine was “an effective inhibitor of the replication of the severe acute respiratory syndrome coronavirus (SARS-CoV) in vitro” and should “be considered for immediate use in the prevention and treatment of SARS-CoV infections.”
In 2005, another study showed chloroquine had strong antiviral effects on SARS-CoV infection and was effective in preventing the spread of SARS-CoV in cell cultures.
Other studies showed hydroxychloroquine exhibited antiviral properties that can inhibit SARS-CoV-2 virus entry, transmission and replication, and contains anti-inflammatory properties that help regulate pro-inflammatory cytokines.
Peterson wrote, “many large observational studies suggest that hydroxychloroquine significantly reduces the risk of hospitalization and death when administered to particularly high-risk outpatients as part of early COVID-19 treatment.”
Peterson said the drug is considered to be so safe it can be prescribed for pregnant women, yet during the pandemic, the FDA raised questions about hydroxychloroquine and adverse cardiac events.
These concerns prompted one group of researchers to conduct a systematic review of the hydroxychloroquine safety literature pre-COVID. Their review indicated people taking hydroxychloroquine in appropriate doses “are at very low risk of experiencing cardiac [adverse events], particularly with short-term administration” of the drug.
Researchers noted COVID itself can cause cardiac problems, and there was no reason “to think the medication itself had changed after 70 years of widespread use,” Peterson wrote.
Peterson said one piece of key flawed data had substantially contributed to safety concerns surrounding the drug — the admittedly fraudulent Lancet study that falsely claimed hydroxychloroquine increased frequency of ventricular arrhythmias when used for treatment of COVID.
The findings were so startling that major drug trials involving hydroxychloroquine “were immediately halted” and the World Health Organization pressured countries like Indonesia that were widely using hydroxychloroquine to ban it. Some countries, including France, Italy and Belgium, stopped using it for COVID altogether.
Peterson wrote:
“The problem, however, is that the study was based on false data from a company named Surgisphere, whose founder and CEO Sapan Desai was a co-author on the published paper.
“The data were so obviously flawed that journalists and outside researchers began raising concerns within days of the paper’s publication. Even the Lancet’s editor in chief, Dr. Richard Horton, admitted that the paper was a fabrication, a monumental fraud and a shocking example of research misconduct in the middle of a global health emergency.”
Despite calls for the Lancet to provide a full expansion of what happened, the publication declined to provide details for the retraction.
As with ivermectin, the FDA and NIH adopted positions against the use of hydroxychloroquine for COVID — making assertions that were unsupported by data. The AMA, APhA and ASHP, which opposed ivermectin, also resisted hydroxychloroquine for the treatment of COVID.
By contrast, the Association of American Physicians and Surgeons, and other physician groups, support the use of both ivermectin and hydroxychloroquine as an early treatment option for COVID. Peterson cited an article co-authored by more than 50 doctors in Reviews in Cardiovascular Medicine who advocated an early treatment protocol that includes hydroxychloroquine as a key component.
Governing law allows physicians to prescribe ivermectin and hydroxychloroquine, AG says
Neb. Rev. Stat. § 38-179 generally defines unprofessional conduct as a “departure from or failure to conform to the standards of acceptable and prevailing practice of a profession or the ethics of the profession, regardless of whether a person, consumer or entity is injured, or conduct that is likely to deceive or defraud the public or is detrimental to the public interest.”
The regulation governing physicians states that unprofessional conduct includes:
“[c]onduct or practice outside the normal standard of care in the State of Nebraska which is or might be harmful or dangerous to the health of the patient or the public, not to include a single act of ordinary negligence.”
Peterson said healthcare providers do not violate the standard of care when they choose between two reasonable approaches to medicine.
“Regulations also indicate that physicians may utilize reasonable investigative or unproven therapies that reflect a reasonable approach to medicine so long as physicians obtain written informed patient consent,” Peterson wrote.
“Informed consent concerns a doctor’s duty to inform his or her patient, and it includes telling patients about the nature of the pertinent ailment or condition, the risks of the proposed treatment or procedure and the risks of any alternative methods of treatment, including the risks of failing to undergo any treatment at all.”
Peterson said this applies to prescribing medicine for purposes other than uses approved by the FDA, and that doing so falls within the standard of care repeatedly recognized by the courts.
Peterson said the U.S. Supreme Court has also affirmed that “off-label usage of medical devices” is an “accepted and necessary” practice, and the FDA has held the position for decades that “a physician may prescribe [a drug] for uses or in treatment regimens or patient populations that are not included in approved labeling.”
Peterson said the FDA has stated “healthcare providers generally may prescribe [a] drug for an unapproved use when they judge that it is medically appropriate for their patient, and nothing in the federal Food, Drug and Cosmetic Act (“FDCA”) limit[s] the manner in which a physician may use an approved drug.”
In a statement to KETV NewsWatch 7, Nebraska’s Department of Health and Human Services said:
“The Department of Health and Human Services appreciates the AG’s office delivering an opinion on this matter. The document is posted and available to medical providers as they determine appropriate course of treatment for their patients.”
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Featured Video

“Trump’s presidency is at risk of being destroyed” Col Douglas Macgregor
or go to
Aletho News Archives – Video-Images
From the Archives
Infertility: A Diabolical Agenda
Dr. Joseph Mercola | July 9, 2022
“Infertility: A Diabolical Agenda,” is the fourth vaccine-related documentary by Dr. Andrew Wakefield. It tells the story of an intentional infertility vaccine program conducted on African women, without their knowledge or consent.
While it’s been brushed off as a loony conspiracy theory for years, there’s compelling evidence showing it did, in fact, happen, and there’s nothing to prevent it from happening again. … continue
Blog Roll
 Aletho News
Aletho News- Israeli strikes kill 10 in southern Lebanon, including 3 rescue workers
- Israeli military ‘failed on all fronts’: Poll
- US at a crossroads: Iran’s firm positions leave Trump no option but to capitulate
- Iran signals decisive response to end US maritime bullying, piracy
- Trump eager for off-ramp in war on Iran, but Netanyahu has him trapped: Former official
- Trump’s ‘Golden Dome’ offers ‘limited’ shield against ballistic missiles: Defense official
- Ukraine Seeks to Provoke a Nuclear Conflict: Zakharova
- US squares up to China over Panama Canal
- Monroe Doctrine 2.0: ‘Great Reset’ for US Imperialism?
- Nuclear Apartheid: Iran’s Rise Exposes the NPT Fraud and the West’s Israel Exception
- If Americans Knew
- How Tony Dokoupil Became the Face of ‘Zionist Fanatic’ Bari Weiss’s CBS
- Far Right Israeli Settler Movement Enters Syria in a Push for “Greater Israel”
- ‘People Have the Right to Be Buried’: In Gaza, Thousands of Palestinians Remain Trapped Under Rubble
- Born during Israel’s genocide: Gaza’s child survivors bear the scars of war
- Who are the women and girls behind Gaza war’s horrific casualty toll?
- Beloved Gaza doctor detained “indefinitely” without charge – Daily Update
- By Week’s End, Trump’s War Will Be Plainly Illegal
- CBS News Reportedly Ousts London Bureau Chief Over Differences With Bari Weiss Over Gaza Coverage
- State Department Says US Is in Conflict With Iran ‘At the Request’ of Israel
- What ceasefire? Israel won’t stop killing in Gaza, Lebanon – Daily Update
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
