Another week, another Vaccine Surveillance report (now published by the U.K. Health Security Agency (UKHSA), the successor to Public Health England), and with it more worrying news on the vaccine front.
Infection rates in the double-vaccinated compared to the unvaccinated continue to rise, meaning unadjusted vaccine effectiveness continues to decline. Infection rates are now higher in the double-vaccinated compared to the unvaccinated by 124% in those in their 40s, 103% in those in their 50s and 60s and 101% in those in their 70s, corresponding to unadjusted vaccine effectiveness estimates of minus-124%, minus-103% and minus-101% respectively. For those over 80 the unadjusted vaccine effectiveness is minus-34% while for those in their 30s it is minus-27%. For 18-29 year-olds it is 25%, so still positive but low, while for under-18s it is 90%, the only age group showing high efficacy. Vaccine effectiveness against emergency hospital admission and death continues to hold up, though with some indication of gradual slide, particularly in older age groups (see below). (For definitions and limitations, see here.)
The UKHSA has continued to receive criticism for publishing this data, with claims that the figures used for the unvaccinated population are unreliable and likely too high, artificially suppressing the infection rate and vaccine effectiveness. Cambridge statistician Professor David Spiegelhalter put out a scathing tweet on these lines on Friday, but he didn’t elaborate on his claim or link to an article explaining it further.
Completely unacceptable that UKHSA put out absurd statistics showing case-rates higher in vaxxed than non-vaxxed (Fig 2), when just an artefact of using hopelessly biased NIMS popn estimates. Feeding conspiracy theorists worldwide. https://t.co/DjyhxnSm2z
Professors Norman Fenton and Martin Neil have argued that in fact the PHE/UKHSA data may underestimate the number of unvaccinated rather than overestimate them, which would have the reverse effect.
Either way though, what wouldn’t change is the fact of the large and fast decline in effectiveness against infection. This is now generally acknowledged among many scientists (likely caused by waning over time or new variants or both), though has not had the logical impact on Government policy one might have expected and hoped for of eliminating the rationale for vaccine passports and mandates.
A further point revealed for the first time in this week’s surveillance report is that the vaccines may actually hobble the body’s ability to develop the strongest immunity once infected. As noted by Alex Berenson, the report mentions (in passing) that “recent observations from U.K. Health Security Agency (UKHSA) surveillance data” show that “N antibody levels appear to be lower in individuals who acquire infection following two doses of vaccination”.
The report does not elaborate on this, but on the face of it it is a startling admission. It is basically saying that a certain kind of antibody which is not produced by the vaccines but is usually produced by infection (and hence is used by PHE/UKHSA to identify those with antibodies-from-infection) is not produced so well by those who are infected post-vaccination. Insofar as this is true it means the vaccines may actually prevent the immune system from developing the strongest form of protection against reinfection. This phenomenon of the immune system being in some way hobbled by the way it first encounters a pathogen is well-known and is referred to as original antigenic sin.
There would be a number of implications of this. It would mean that since the vaccine rollout got going the prevalence of N antibodies in the population has ceased to be a reliable measure of how many people are previously infected (which might explain why it has been rising so slowly during the Delta surge). It would also mean the vaccines may make reinfections and serious illness upon reinfection more likely. Plus likely other things as well.
This is something that should be investigated fully and the results published so that its impact can be properly assessed and understood.
Your colon, which is also known as the large intestine, plays an incredibly important role in your health. As part of the digestive tract, bacteria in the colon are responsible for the final breakdown of food material before it passes into the rectum and is excreted through the anus.1
New evidence published in Frontiers in Pharmacology show the antiparasitic medication ivermectin may have a new application in the treatment of colorectal cancer (CRC).2 Researchers are hopeful this may have a positive impact on colon cancer deaths. Colon cancer is the third leading cancer diagnosis and third cause of cancer death in the U.S.3
According to data from the National Cancer Institute,4 an estimated 149,500 new cases of colorectal cancer will be diagnosed in 2021 and an estimated 52,980 people will die. This represents 7.9% of all new cases of cancer diagnosed in 2021 and 8.7% of all cancer deaths.
There are modifiable risk factors associated with colorectal cancer.5 For example, lifestyle factors over which you have control that reduce your risk of colorectal cancer include your diet, alcohol consumption, activity level, weight and history of smoking.
In 2015, the International Agency for Research on Cancer, an arm of the World Health Organization,6 concluded that processed meat could cause colorectal cancer in humans and classified it as a Group 1 carcinogen. According to the WHO, this means:
“… there is convincing evidence that the agent causes cancer. In the case of processed meat, this classification is based on sufficient evidence from epidemiological studies that eating processed meat causes colorectal cancer.”
Ivermectin Shows Promise in Treatment of Colorectal Cancer
Wrongly vilified as a “livestock drug” by the media in the treatment of COVID-19 with “scant evidence it works,”7 researchers have found a new use for this Nobel Prize-winning medication.8 As the research team wrote in the published study, although CRC is the third most common cancer worldwide, it still lacks effective therapy.9
Past research has demonstrated that ivermectin also has anti-inflammatory, antitumor and antiviral properties. To test the influence ivermectin may have on colorectal cancer cells, the team used cancer cell lines SW48010 and SW1116.11 Both are epithelial cell lines from the large intestine in humans.
The researchers12 used multiple tests to determine cell viability and apoptosis after exposure to ivermectin. They also measured reactive oxygen species levels and cell cycle. To explore the effect on proliferation, the researchers used different concentrations of ivermectin on the cultured cells and found cell viability decreased in a dose-dependent and time-dependent manner.
The ivermectin also altered cell morphology, demonstrating a decrease in cells after just 24 hours and a loss of their original shape. Cultured cells were also exposed to concentrations of ivermectin after which cell viability and apoptosis were measured. The researchers found an increase in apoptosis indicating a dose-dependent effect.
Additionally, the researchers measured the activity of Caspase-3 that plays a vital role initiating apoptosis. They found that ivermectin increases Caspase 3/7 activity in both cell lines in a dose-dependent manner.
This information supports past studies that have suggested ivermectin has anticancer activity against cancers of the digestive system, reproductive system, brain, respiratory system, hematological and breast. The researchers concluded the data demonstrated:13
“… ivermectin may regulate the expression of crucial molecules … Therefore, current results indicate that Ivermectin might be a new potential anticancer drug for treating human colorectal cancer and other cancers.”
Current Colorectal Tumor Treatments Are Invasive and Damaging
The potential use of ivermectin in the treatment of colorectal cancer, or other cancers, offers great hope since current treatments are often invasive and damaging. Ivermectin has been prescribed successfully in humans for 40 years14 with a known side effect profile. This includes drowsiness, headache, mild skin rash, nausea, diarrhea and dizziness.15
The American Cancer Society’s16 current recommendations for treatment of colorectal cancer are based on the stage of disease at diagnosis. The treatments can include surgery, chemotherapy, radiation and targeted therapies. Targeted drugs work differently from chemotherapy and have different side effects, which can include high blood pressure, fatigue, mouth sores, bleeding and low white blood counts.17
Unfortunately, these are the best treatments that Western medicine currently has to offer people with colorectal cancer. Following chemotherapy or ionizing radiation, it is not uncommon to develop a secondary cancer after cellular damage from the treatment.18
For example, after chemotherapy, acute myelogenous leukemia is one of the most common types of cancer to develop. After radiation treatments, a solid tumor can develop near the margin of the irradiated field. Bone and soft tissue sarcomas are the most common.
Help Protect Your Gut Against Colon Cancer
There are several steps you can take to help protect yourself against colon cancer. Research published in Pharmaceutical Research19 suggested that only 5% to 10% of all cancer cases are due to genetic defects, while the rest are linked to environment and lifestyle factors.
The researchers estimated that of the environmental and lifestyle factors that contribute to cancer related deaths, nearly 30% are due to tobacco, 35% are related to diet and 20% are related to infections. The remaining 15% can be due to lack of physical activity, stress and environmental pollutants. Some of the lifestyle factors that can help reduce your risk colon cancer include:
Eating more fiber — Dietary fiber is associated with a reduced risk of colorectal cancer, specifically colorectal adenomas and distal colon cancer.20 By eating more whole foods, such as fruits and vegetables, you’ll naturally be eating more fiber from the best source.
Optimizing your vitamin D level — A vitamin D deficiency is a risk factor for colorectal cancer.21 One study22 showed people with higher blood levels of vitamin D were less likely to develop colorectal tumors. It’s important to monitor your vitamin D levels to ensure you stay within a healthy range.23
Avoiding processed meats — These include pastrami, ham, bacon, pepperoni, hot dogs, some sausages and hamburgers preserved with salt or chemical additives. The nitrates found in processed meats are frequently converted into nitrosamine,24 which are clearly associated with an increased risk of certain cancers.
Exercising — There is evidence that regular exercise can significantly impact and reduce your risk of colon cancer.25,26,27 Exercise helps drive down insulin levels and it has also been suggested that apoptosis is triggered by exercise.28 Exercise also improves circulation of immune cells which improves the efficiency of your immune system.
Maintaining a normal weight and control belly fat — According to one NIH study,29 obesity is more closely associated with colon cancer than diet. Hyperinsulinemia, which occurs in type 2 diabetes, and linked to obesity, is an important factor in the development of colon cancer.30
According to the National Cancer Institute,31 results from the NHANES in 2011 to 2014 nearly 70% of people in the U.S. over 20 were overweight or obese. It’s not just how much weight you carry, but where it’s carried. One study32 showed that visceral fat has a positive association with the prevalence of colorectal cancers. The prevalence increased significantly as the measurement of visceral fat increased.
Limiting alcohol and eliminating smoking — Although smoking is more frequently associated with lung cancer, research has shown there is a link between smoking tobacco and a greater risk of colon cancer.33 Data published in 2020,34 demonstrated a dose-dependent relationship between cigarette smoking and CRC.
Alcohol intake is also associated with a higher risk of colorectal cancers. One study35 found a differentiation between the types of alcohol and the effect on the colon and rectum. Another published in 2018,36 found the relationship between excess alcohol intake was linked not only to the alcohol but also to the predisposition to a poor diet low in fiber.
Eating garlic — There is evidence demonstrating garlic can kill cancer cells in vitro. Several studies have analyzed the effects that dietary garlic may have on the development of colorectal cancer. One study37 did not find a significant reduction in risk.
A second published in January 2020,38 did find evidence that garlic could reduce the risk of CRC. One study39 published in the Asia Pacific Journal of Clinical Oncology revealed the odds of getting CRC were 79% lower in those who a diet high in allium vegetables, which include garlic, leeks and onions.
Optimizing Mitochondrial Health Lowers Metabolic Disease Risk
In 2016, Thomas Seyfried, Ph.D., was the recipient of my Game Changer Award for his work on cancer as a metabolic disease. Later, his work was heavily featured in Travis Christofferson’s excellent book “Tripping Over the Truth: The Metabolic Theory of Cancer.”
In November 2018,40 Dr Peter Attia, who focuses interviewed Seyfried in a detailed discussion about why cancer cells grow and how conventional medicine has it mostly wrong when it comes to treatment. During the interview Seyfried talked about important principles in cancer treatment including biopsies, surgical intervention, radiation and chemotherapy.
As I have discussed in the past,41 Seyfried and others have shown cancer is primarily a metabolic disease and that normal mitochondria can suppress cancer growth. In other words, for cancer cells to proliferate, they must have dysfunctional mitochondria. Seyfried’s research demonstrates cancer can be managed when you move from using glucose and glutamine for fuel to primarily ketone bodies in a ketogenic diet.
The take-home message from Seyfried’s work is keeping your mitochondria healthy significantly reduces the risk for any type of cancer. By primarily avoiding toxic environmental factors and implementing healthy lifestyle strategies you can reduce the risk of mitochondrial dysfunction. This is the sole focus of the program detailed in my book “Fat for Fuel.” Topping my list of strategies to optimize mitochondrial health are:
•Cyclical nutritional ketosis — The divergence from an ancestral diet, including the prevalence of processed and unnatural foods replete with added sugars, net carbs and industrial fats, is responsible for most of the damage to your mitochondria. A foundational strategy to optimize health is to eat the right fuel.
•Calorie restriction — By limiting the amount of fuel available to your body, you reduce mitochondrial free radical production. Calorie restriction is consistently shown to have many therapeutic benefits.
•Meal timing — When you eat late in the evening, your body stores the energy instead of using it. This creates a buildup of ATP and ultimately an excessive amount of free radical formation.
•Normalizing your iron level — High levels of iron enhances oxidation and creates reactive oxygen species and free radicals. Contrary to popular belief, excess iron is more prevalent in the population than iron deficiency. Fortunately, this is very easy to address.
Simply checking your iron level with a serum ferritin test will reveal if your level is high. You can correct high levels by donating blood two or three times a year to maintain a healthy level.
•Exercise — In addition to the evidence discussed above related to colorectal cancer, exercise also upregulates PCG1 alpha and Nrf2. These are genes that promote mitochondrial efficiency, helping them to grow and divide if actively. Simply put, by increasing the energy demand on yourself during physical activity, it signals your body to create more mitochondria to meet the energy demand.
On July 28, the Wall Street Journal ran our article “Why Is the FDA Attacking a Safe, Effective Drug?” In it, we outlined the potential value of the antiparasitic drug ivermectin for Covid-19, and we questioned the FDA’s vigorous attack on ivermectin. Many people praised us and many criticized us. We had clearly covered a sensitive subject. It didn’t help that one of the studies we referenced was retracted shortly before we submitted our article. Within hours of learning that fact, we sent a mea culpa to the Journal’s editors. They acted quickly, adding a note at the end of the electronic version and publishing our letter. It’s important to address two criticisms of our work. The first is that we exaggerated the FDA’s warning on ivermectin. The second is that Merck’s stance on ivermectin proved that even the company that developed ivermectin thought that it doesn’t work for Covid-19.
First, we didn’t exaggerate the FDA’s warning on ivermectin. Instead, the agency changed its website after our article was published, probably to reflect the points we made. Second, Merck had two incentives to downplay ivermectin’s usefulness against the novel coronavirus. We’ll explain both points more fully.
Ivermectin was developed and marketed by Merck & Co. while one of us (Hooper) worked there years ago. Dr. William C. Campbell and Professor Satoshi Omura were awarded the 2015 Nobel Prize for Physiology or Medicine. They earned it for discovering and developing avermectin. Later Campbell and some associates modified avermectin to create ivermectin. Merck & Co. has donated four billion doses of ivermectin to prevent river blindness and other diseases in areas of the world, such as Africa, where parasites are common. The ten doctors who are in the Front Line Covid-19 Critical Care Alliance call ivermectin “one of the safest, low-cost, and widely available drugs in the history of medicine.” Ivermectin is on the WHO’s List of Essential Medicines and ivermectin has been used safely in pregnant women, children, and infants.
Ivermectin is an antiparasitic, but it has shown, in cell cultures in laboratories, the ability to destroy 21 viruses, including SARS-CoV-2, the cause of Covid-19. Further, ivermectin has demonstrated its potential in clinical trials for the treatment of Covid-19 and in large-scale population studies for the prevention of Covid-19.
Contradicting these positive results, the FDA issued a special statement warning that “you should not use ivermectin to treat or prevent Covid-19.” The FDA’s warning, which included language such as, “serious harm,” “hospitalized,” “dangerous,” “very dangerous,” “seizures,” “coma and even death,” and “highly toxic,” might suggest that the FDA was warning against pills laced with poison. In fact, the FDA had already approved the drug years ago as a safe and effective anti-parasitic. Why would it suddenly become dangerous if used to treat Covid-19? Further, the FDA claimed, with no scientific basis, that ivermectin is not an antiviral, notwithstanding its proven antiviral activity.
Interestingly, at the bottom of the FDA’s strong warning against ivermectin was this statement: “Meanwhile, effective ways to limit the spread of COVID-19 continue to be to wear your mask, stay at least 6 feet from others who don’t live with you, wash hands frequently, and avoid crowds.” Was this based on the kinds of double-blind studies that the FDA requires for drug approvals? No.
After some critics claimed that we overstated or overreacted to the FDA’s special warning, we reviewed the FDA’s website and found that it had been changed, and there was no mention of the changes nor any reason given. Overall, the warnings were watered down and clarified. We noticed the following changes:
The false statement that “Ivermectin is not an anti-viral (a drug for treating viruses)” was removed.
“Taking a drug for an unapproved use can be very dangerous. This is true of ivermectin, too” was changed to the less alarming “Ivermectin has not been shown to be safe or effective for these indications.” (Indications is the official term used in the industry to denote new uses for a drug, such as new diseases or conditions, and/or new patient populations.)
The statement, “If you have a prescription for ivermectin for an FDA-approved use, get it from a legitimate source and take it exactly as prescribed,” was changed to, “If your health care provider writes you an ivermectin prescription, fill it through a legitimate source such as a pharmacy, and take it exactly as prescribed.” This more clearly acknowledges that reasonable physicians may prescribe ivermectin for non-FDA-approved uses, such as Covid-19.
The ending statement about masks, spacing, hand washing, and avoiding crowds was replaced with one that recommended getting vaccinated and following CDC guidelines.
The reasonable statement “Talk to your health care provider about available COVID-19 vaccines and treatment options. Your provider can help determine the best option for you, based on your health history” was added at the end.
The new warning from the FDA is more correct and less alarming than the previous one.
In a statement from February, Merck, the company that originated and still sells ivermectin, agreed with the FDA that ivermectin should not be used for Covid-19. “We do not believe that the data available support the safety and efficacy of ivermectin beyond the doses and populations indicated in the regulatory agency-approved prescribing information.”[2]
To some, this appeared to be a smoking gun. Merck wants to make money, they reason, and people are interested in using ivermectin for Covid-19, therefore, Merck would warn against such usage only if the scientific evidence were overwhelming. But that’s not how the pharmaceutical industry works.
Here’s how the FDA-regulated pharmaceutical industry really works.
The FDA judges all drugs as guilty until proven, to the FDA’s satisfaction, both safe and efficacious. By what process does this happen? The FDA waits for a deep-pocketed sponsor to present a comprehensive package that justifies the approval of a new drug or a new use of an existing drug. For a drug like ivermectin, long since generic, a sponsor may never show up. The reason is not that the drug is ineffective; rather, the reason is that any expenditures used to secure approval for that new use will help other generic manufacturers that haven’t invested a dime. Due to generic drug substitution rules at pharmacies, Merck could spend millions of dollars to get a Covid-19 indication for ivermectin and then effectively get zero return. What company would ever make that investment?
With no sponsor, there is no new FDA-approved indication and, therefore, no official recognition of ivermectin’s value. Was the FDA’s warning against ivermectin based on science? No. It was based on process. Like a typical bureaucrat, the FDA won’t recommend the use of ivermectin because, while it might help patients, such a recommendation would violate its processes. The FDA needs boxes checked off in the right order. If a sponsor never shows up and the boxes aren’t checked off, the FDA’s standard approach is to tell Americans to stay away from the drug because it might be dangerous or ineffective. Sometimes the FDA is too enthusiastic and these warnings are, frankly, alarming. Guilty until proven innocent.
There are two reasons that Merck would warn against ivermectin usage, essentially throwing its own drug under the bus.
Once they are marketed, doctors can prescribe drugs for uses not specifically approved by the FDA. Such usage is called off-label. Using ivermectin for Covid-19 is considered off-label because that use is not specifically listed on ivermectin’s FDA-approved label.
While off-label prescribing is widespread and completely legal, it is illegal for a pharmaceutical company to promote that use. Doctors can use drugs for off-label uses and drug companies can supply them with product. But heaven forbid that companies encourage, support, or promote off-label prescribing. The fines for doing so are outrageous. During a particularly vigorous two-year period, the Justice Department collected over $6 billion from drug companies for off-label promotion cases. Merck’s lawyers haven’t forgotten that lesson.
Another reason for Merck to discount ivermectin’s efficacy is a result of marketing strategy. Ivermectin is an old, cheap, off-patent drug. Merck will never make much money from ivermectin sales. Drug companies aren’t looking to spruce up last year’s winners; they want new winners with long patent lives. Not coincidentally, Merck recently released the clinical results for its new Covid-19 fighter, molnupiravir, which has shown a 50% reduction in the risk of hospitalization and death among high-risk, unvaccinated adults. Analysts are predicting multi-billion-dollar sales for molnupiravir.[3]
While we can all be happy that Merck has developed a new therapeutic that can keep us safe from the ravages of Covid-19, we should realize that the FDA’s rules give companies an incentive to focus on newer drugs while ignoring older ones. Ivermectin may or may not be a miracle drug for Covid-19. The FDA doesn’t want us to learn the truth.
The FDA spreads lies and alarms Americans while preventing drug companies from providing us with scientific explorations of existing, promising, generic drugs.
David R. Henderson is a Senior Fellow with the American Institute for Economic Research.
He is also a research fellow with the Hoover Institution at Stanford University and emeritus professor of economics with the Naval Postgraduate School, is editor of The Concise Encyclopedia of Economics.
David was previously the senior economist for health policy with President Reagan’s Council of Economic Advisers.
***
Charles L. Hooper is President and co-founder of Objective Insights, Inc. He is also the author of Would the FDA Reject Itself? (Chicago Park Press, 2021), currently available as an ebook on Apple Books and Amazon Kindle. A paper version is forthcoming.
Prior to forming Objective Insights in 1994, he worked at Merck & Co., Syntex Labs, and NASA.
He is a former visiting fellow at the Hoover Institution at Stanford University.
His experience is in decision analysis, economics, product pricing, forecasting, and modeling.
A deleted government report exploring how to make the public alter its behavior to accept the new ‘green economy’ reveals how COVID-19 restrictions have created a population with a “deep set reverence” for authority and a “powerful tendency to conform.”
The report was inadvertently published by the British government before being hastily pulled down, but numerous journalists were able to retrieve its contents.
The document explored how to weaponize behavioral psychology to ‘nudge’ the public into supporting measures and adopting behavior without them explicitly knowing they’re being manipulated.
The investigation found that the same techniques the government used to force people into accepting lockdown could be used to make them change their lifestyles in the name of preventing climate change.
Under the heading “principles for successful behaviour,” the paper noted;
“Government statements, actions and laws powerfully shape perceptions of normative and acceptable behaviour. For instance, even with public criticism being high, many still perceived government approval as the yardstick for safe behaviour during COVID-19 ‘we’re allowed to do this now [so must be safe]…’. This reveals, for many, a deep set reverence for legitimate government authority, regardless of one’s personal political views.”
While PR stunts such as having officials vaccinated live on television worked to convince people of the narrative, elite hypocrisy (public officials violating lockdown rules) was found to cause significant damage to public trust.
“Perceived hypocrisy can do a lot to undermine efforts to build public engagement and support. This was observed during the COVID-19 pandemic when prominent authority figures broke guidelines, leading to measurable reductions in public compliance as well as shifting attitudes.”
“Green politics has similar deep-seated reputational issues with elite hypocrisy,” notes Breitbart. “A common feature of climate change summits has been high-profile attendees arriving by private or government jet, a disconnect between word and deed that seems unlikely to vanish in the near term.”
The paper concluded that people can be rather easily “nudged” into changing their behavior in response to government announcements and “have a powerful tendency to conform.”
The investigation also found that even if enforced changes to lifestyle are not wanted by the public, most tend to fall in line with the new status quo rather quickly anyway.
The report was prepared by the Behavioural Insights Team (BIT), a quasi-government body that was part of the effort to use “totalitarian” and “unethical” methods of instilling fear into the population as a means of scaring them into complying with lockdown rules.
A related group, the Scientific Pandemic Insights Group on Behaviours team, warned at the start of the first lockdown that a “substantial number of people still do not feel sufficiently personally threatened [by Covid-19].”
“The perceived level of personal threat needs to be increased among those who are complacent, using hard-hitting emotional messaging,” the group added, leading to numerous lurid propaganda campaigns that exaggerated the threat of COVID to bully the public into total submission.
In summary, the public is largely unthinking, compliant and docile and can be made to go along with just about anything so long as they’re bombarded with the right propaganda.
Kevin Galalae has published his research in a document titled: PCR Tests and the Depopulation Program. He concludes “the coronavirus blamed for countless deaths real and imagined is a political fiction. The symptoms attributed to Covid are caused by a deliberate three-pronged attack on our health and lives by our own national and international authorities.”
The deliberate three-pronged attack is summarised as follows:
damage the epithelium of the nasopharyngeal cavity with PCR test swabs to bring down the immune defences that protect our brain
create a closed loop between the mouth and the nose, thus between outgoing and incoming air, by forcing us to wear face masks throughout the day
increase damage to the brain by subjecting us to chemicals and neurotoxins that could never reach the brain had they not destroyed the blood-brain barrier
Kevin Galalae is a Canadian human rights activist, author, journalist and historian. He has authored numerous books including Killing Us Softly: The Global Depopulation Policy. As an activist, Galalae has many notable accomplishments including matters in the United Kingdom, European Union and United Nations and is an ardent defender of a free World Wide Web.
Galalae is also an expert on the topic of the global depopulation policy – also known as Agenda 21, Agenda 2030 or population control. His biography makes interesting reading and, as downloaded from The EveryDay Concerned Citizen, is attached below.
The creator of the PCR test, Dr. Kary Mullis, has stated clearly and on many occasions that the results of the PCR tests can be easily misinterpreted to mean anything. The PCR testing methodology does not distinguish if positive results are infectious.
Given their invasive nature and the fact that they were never meant for diagnostic but for research purposes, why are they being used as often as possible on the same individuals and on as many people as possible? “Well, now I know how the system is misusing them!” Galalae exclaims and gives his explanation, with links to scientific research, in his twelve-page document: PCR Tests and the Depopulation Program (see attached below).
“The long swab inserted into the nasopharyngeal cavity all the way to the roof of the nose … damages the fascicles of the olfactory nerve, which, as it turns out, has dire consequences for human health and lifespan because the olfactory nerve is one of only two windows in the cranium through which viruses and bacteria can move from nose to brain, thus can cross the blood-brain barrier, the other one being the trigeminal nerve.” – PCR Tests and the Depopulation Program
The olfactory nerve contains sensory nerve fibres relating to the sense of smell. It is the only cranial nerve that has stem cells – called olfactory ensheathing cells – which enable it to continually regenerate throughout life. They are the cells that protect the olfactory nerve and aid its regeneration in case of damage through age or injury. These cells are so unique that doctors have recently begun using them to successfully repair spinal cord injuries and to treat brain diseases.
Additionally, the olfactory ensheathing cells assist in innate immunity because they are phagocytic and, as such, ingest bacteria. The innate immune system includes all our body’s first line defences such as the physical barriers lining the nose, throat, lungs and gut, as well as the skin. Innate immunity provides broad protection and is quick to react to any threat. The olfactory ensheathing cells are thus a crucial part of the protection provided to the brain.
For adults aged between 57 and 85 years, once the olfactory ensheathing cells lose their ability to regenerate the chance of dying within five years is four times higher.
The PCR tests serve two important roles for the depopulation program.
In the short-term, by repeatedly damaging the olfactory nerve with nasal swabs the incidence of viral and bacterial infections is rapidly raised. This helps governments create and sustain the impression of a pandemic. The more people are tested the more people are damaged and left defenceless against various infections that are then mislabelled en masse as Covid infections. And, by simply raising the number of cycles in the thermal cycler the authorities get the percentage of positive results they want.
“And in the long-term, by periodically damaging the olfactory nerve it will lose its ability to regenerate and this helps governments prematurely kill countless people ages 57 to 85, the very age groups governments of the developed world want dead to ease the old-age burden and prevent economic collapse.” – PCR Tests and the Depopulation Program
The trigeminal nerve is a nerve responsible for sensation in the face and motor functions. If the test swab is inserted at the wrong angle and it touches this nerve it can affect the sense of taste and even sight.
“But even inserted at the correct angle, the mucosa of the nasopharyngeal cavity is damaged irrespective of the angle at which the swab is inserted at so long as it is inserted as deeply and rotated as vigorously as required by the PCR testing procedure, especially when the swabs are designed to do as much damage as possible by having serrated tips capable of scratching and damaging as much epithelium as possible” – PCR Tests and the Depopulation Program
Ethylene oxide, a well-known cancer-causing substance, is used to sterilize the PCR test swabs. “And since the swabs smear this mutagenic chemical on the mucosa of the nose, which is hypersensitive, it damages our health in unknown ways.” – PCR Tests and the Depopulation Program
Face Masks
“By mandating mask wearing indoors and outdoors, knowing that exhaled air contains numerous bacteria and viruses, the planners are subjecting billions of people to inhale pathogens that the body exhaled from the respiratory tract … Hundreds of studies show that the inside of surgical masks contain greatly increased loads of bacteria and fungi after prolonged wearing and are a source of contamination not only for those wearing them but also for those around them.” – PCR Tests and the Depopulation Program
The latest and most comprehensive study has found that mask wearing by the general population leads to: a drop in oxygen; fatigue; rise in carbon dioxide; respiratory impairment; headache; and, temperature rise and moisture under the mask.
How do the test swabs and masks work together towards the same aim?
Galalae surmises that the test swabs damage the immune defences of the brain leaving it exposed to pathogens. And then, the masks subject the brain to asphyxiation by depriving it of oxygen and bombarding it with carbon dioxide. The respiratory center of the brain – which controls minute-to-minute breathing – begins to malfunction and as a result, people have trouble breathing. “The breathlessness (dyspnoea) associated with Covid is therefore not due to lung lesions but to damage to neural processing, thus due to brain damage.” – PCR Tests and the Depopulation Program
Chemicals And Toxins
“The general population has been subjected to an onslaught of dangerous chemicals through hand sanitisers, whose use medical authorities have mandated for the most mundane activities ever since the plandemic has been started. Methanol is probably the most dangerous and most often found chemical in hand sanitisers … It is known to cause metabolic acidosis, visual disturbances and neurological deficit.” – PCR Tests and the Depopulation Program
Galalae then goes on to explain how the adult population is subjected to neurotoxins – most likely isodecanes and mycotoxins – hidden in body care products, food and drinks (especially beer).
Summary
Galalae ends with “this explains, among other things,” and he lists a number of points the below being a few of them, why:
incidences of illness increase as PCR testing increases;
the pathology attributed to Covid is so wide-ranging and so far removed from any other viral infection of the respiratory tract;
the pandemic disappears and reappears;
vaccine passports are only given to people who are either vaccinated or have had positive PCR tests, but never to those who show that they have naturally acquired antibodies; there is no pharmacological treatment for Covid; and,
governments continue to insist on subjecting as many people as possible as often as possible to an intrusive medical test that can be easily done by analysing saliva.
The unrelenting opposition to using ivermectin to treat and prevent COVID-19 is stronger than ever. This has resulted from a gigantic increase in demand for IVM by much of the public.
Despite big media tirades against IVM, the truth about its effectiveness (together with failure of COVID vaccines) has reached the public through many articles on alternative news websites and truth-tellers on countless podcasts. Its success has forced Big Pharma to create expensive copies of it.
Monthly IVM prescriptions increased 72 percent from 39,864 in 2019 to 68,428 in 2021 (through May). Just when COVID vaccination started to be pushed in January 2021 prescriptions hit a high of 97,192. A number of medical specialties greatly increased off-label use of IVM for fighting COVID in this period: anesthesiology, 1,319%; pulmonology, 1,167%; cardiology, 741%, for example. Strong support by physicians for IVM to cure and prevent COVID.
And in my book Pandemic Blunder I made the case with data that using cheap, safe and effective generics like IVM and hydroxychloroquine would save 80% or more of COVID deaths. Esteemed physician Peter McCollough later said 85%. For the US, that means some 600,000 lives could have been saved, and globally over 4 million lives. Meanwhile, hundreds of thousands of people worldwide have also died from COVID vaccines, the failed solution to the pandemic.
Merck, a maker of IVM, is getting much positive press coverage for its forthcoming prescription oral antiviral (molnupiravir). It is designed to replace IVM that they cannot make big money from. FDA will soon give it emergency use authorization because of the emerging clarity that COVID vaccines do NOT work effectively or safely.
That the Washington Post says that what Merck has created is the “first covid-fighting pill” illustrates how awful big media has been in ignoring the proven benefits of the IVM and HCQ generics. And ignoring the many failures of COVID vaccines. In its October 2 front-page story on the new Merck pill, it did not even mention IVM or present any data showing IVM as proven even more effective than the new expensive drug tested on only hundreds of people for a short period.
In contrast, IVM has been used successfully on hundreds of thousands of people to treat and prevent COVID.
Speaking as someone who is using IVM as a prophylactic, here is what I have seen in recent times. Though getting a prescription for it is very difficult and stressful it can be done through a number of websites. But then the battle just begins. Many pharmacies, especially big chain ones, will not fill IVM prescriptions if there is any evidence that it is being used to fight COVID.
And then you will likely discover, as I did, that virtually no pharmacy (typically small community ones) that will fill such prescriptions has any IVM. That’s right. There is a national shortage of IVM because of huge demand in recent months and because US makers have not escalated production.
Probably, millions of vaccine resisters are using IVM, especially those resisting booster shots.
Can you still get it? Yes, and even without a prescription. It will have to come from India, with many makers of IVM. It can take many weeks to get it. But the cost is a tiny fraction of what US pharmacies have been charging when they did have it in stock. Rather than $4 or $5 for a 3 mg pill, you can buy 12 mg pills for way under $1 a pill.
But there is more to the IVM story.
There is absolutely no doubt whatsoever that there is massive medical science data showing absolute reliable data that IVM is safe and effective for both treating and preventing COVID. This is what should be a bold large headline in newspapers if we had honest big media: IVM SAFE AND EFFECTIVE ALTERNATIVE TO COVID VACCINES.
But instead, there is a constant barrage of articles and statements from government agencies asserting IVM should not be used to fight COVID. They argue it is unsafe and ineffective. Both are lies aimed solely at protecting the mass vaccination effort and the profits of big drug companies. And now protecting the new Big Pharma market for antiviral pills.
FDA has issued very strong warnings against using IVM for COVID. Nothing it has said follows the true science and mountains of data supporting safe and effective IVM use. Like other IVM opponents, it has conflated personal IVM use with the use of IVM products designed for animals.
This is even more infuriating. Merck, despite being a maker of IVM discredited its use for COVID by irresponsibly stating, “We do not believe that the data available support the safety and efficacy of ivermectin beyond the doses and populations indicated in the regulatory agency-approved prescribing information.”
Clearly, Merck, Pfizer and other vaccine makers are developing their own oral antivirals to directly compete with the cheap and effective IVM. These antivirals, unlike cheap generic IVM, would be patented so expensive pills could be sold worldwide. They will find some ingenious ways to copy IVM but make enough changes to get patents.
Already, Merck has begun production of its new pill to be taken twice daily for five days. Even more significant: The US government has made an advance purchase of 1.7 million treatment courses for $1.2 billion! That is over $700 per treatment. So much more profitable than making IVM. Forget the billions of dollars spent on vaccines that are injuring and killing many people.
I am confident in predicting that as more and more bad news about the ineffectiveness and dangerous side effects of COVID vaccines become increasingly known to more of the public, the big drug companies will increasingly switch from vaccines to prescription antiviral medicines. This is what smart corporate business strategic planning is all about. With Merck, it has already started. And FDA, CDC and NIH will go along with this strategic switch.
This will preserve a trillion-dollar market for pharmaceutical companies. How the government and public health establishment weasel word their switch from COVID vaccines to antiviral pills will be a marvelous magical trick to watch. Do you think that they will admit that millions of people worldwide have lost their health and lives from vaccine use? Of course not. Expensive antiviral pills will simply be sold as a better solution.
Be clear about the science explaining why IVM and HCQ have worked. They both (along with zinc) interfere at the earliest stage of COVID infection with viral replication. Stops infection in its tracks. They work as prophylactics for the same reason. If you keep a modest amount of IVM and HCQ in your body (and take zinc, vitamins C and D, and quercetin) any virus that enters your body can be stopped before major viral replication. The new prescription medicines coming from Merck and other Big Pharma are designed to serve the same function as the cheap generics.
This is the big truth coming to fruition: All the emerging information on COVID vaccine ineffectiveness and dangerous and often lethal side effects is forcing a major strategic shift to antivirals.
Congressman Louie Gohmert has recently made a number of solid observations about IVM:
“Almost 4 billion doses of ivermectin have been prescribed for humans, not horses, over the past 40 years. In fact, the CDC recommends all refugees coming to the U.S. from the Middle East, Asia, North Africa, Latin America, and the Caribbean receive this so-called dangerous horse medicine as a preemptive therapy. Ivermectin is considered by the World Health Organization (WHO) to be an ‘essential medicine.’ The Department of Homeland Security’s ‘quick reference’ tool on COVID-19 mentioned how this life-saving drug reduced viral shedding duration in a clinical trial.”
“To date, there are at least 63 trials and 31 randomized controlled trials showing benefits to the use of ivermectin to fight COVID-19 prophylactically as well as for early and late-stage treatment. Ivermectin has been shown to inhibit the replication of many viruses, including SARS-CoV-2. It has strong anti-inflammatory properties and prevents transmission of COVID-19 when taken either before or after exposure to the virus.”
“Ivermectin also speeds up recovery and decreases hospitalization and mortality in COVID-19 patients. It has been FDA approved for decades and has very few and mild side effects. It has an average of 160 adverse events reported every year, which indicates ivermectin has a better safety record than several vitamins. In short, there is no humane, logical reason why it should not be widely used to fight against the China Virus should a patient and doctor decide it is appropriate to try in that patient’s case.” And that small number of adverse events pales in comparison to hundreds of thousands for COVID vaccines.
A new, comprehensive report noted that 63 studies have confirmed the effectiveness of IVM in treating COVID-19. This is a great website to see positive IVM data.
And consider what former Director of Intellectual Property at Gilead Pharmaceuticals, Brian Remy, said about the necessity of implementing Ivermectin. “It is simple – use what works and is most effective – period. Ivermectin used in combination with other therapeutics is a no-brainer and should be the standard of care for COVID-19.
Not only would this be good for business and help avoid the criticism and bad PR, and potential civil/criminal liability for censorship, scientific misconduct, etc. for misrepresentation of Ivermectin and other generics, but most importantly it would save countless lives and end the pandemic for good.” Amen.
Want even more positive facts? Consider the India experience. In India’s deadly second pandemic surge, Ivermectin obliterated their crisis. Within weeks after adopting IVM cases were down 90%. Those states with more aggressive IVM use were down more dramatically. Daily cases in Goa, Uttarakhand, Uttar Pradesh, and Delhi were down 95%, 98%, 99%, 99%, respectively.
And appreciate this: Dr. Kory and the FLCCC published a narrative review in May 2021, showing the massive effectiveness of IVM against COVID-19 in reducing death and cases. They concluded that it must be adopted globally immediately. Yet big media without respect for public health waged war against IVM. Now it is going crazy in support of the expensive Merck antiviral pill.
To sum up: The IVM story is far from over. We now have a pandemic of the vaccinated. From all over the world the fractions of people said to have died from COVID who were fully vaccinated are very high, often 80 percent. Many people with breakthrough COVID infections die. Blame those deaths on the vaccines. Big media suppresses all the negative information on the vaccines and all the positive information on IVM.
This double whammy is pure evil.
It is designed to pave the way for the new, expensive generation of antiviral pills once the medical and public health establishments backtrack from their vaccine advocacy and coercion.
About the author: Dr. Joel S. Hirschhorn, author of Pandemic Blunder and many articles on the pandemic, worked on health issues for decades. As a full professor at the University of Wisconsin, Madison, he directed a medical research program between the colleges of engineering and medicine. As a senior official at the Congressional Office of Technology Assessment and the National Governors Association, he directed major studies on health-related subjects; he testified at over 50 US Senate and House hearings and authored hundreds of articles and op-ed articles in major newspapers. He has served as an executive volunteer at a major hospital for more than 10 years. He is a member of the Association of American Physicians and Surgeons, and America’s Frontline Doctors.
A concerned Physician Assistant, Deborah Conrad, convinced her hospital to carefully track the Covid-19 vaccination status of every patient admitted to her hospital. The result is shocking.
As Ms. Conrad has detailed, her hospital serves a community in which less than 50% of the individuals were vaccinated for Covid-19 but yet, during the same time period, approximately 90% of the individuals admitted to her hospital were documented to have received this vaccine.
These patients were admitted for a variety of reasons, including but not limited to COVID-19 infections. Even more troubling is that there were many individuals who were young, many who presented with unusual or unexpected health events, and many who were admitted months after vaccination.
One would think that after an association was identified by a healthcare professional, our health authorities would at least review this finding, right? Sadly, when Ms. Conrad reached out to health authorities herself, she was ignored. My firm then sent a letter to the CDC and FDA on July 19, 2021 on Ms. Conrad’s behalf (see letter below), yet neither agency has responded. Even worse, when doctors came to Ms. Conrad for assistance with filing VAERS report for their patients, the hospital prohibited her from filing these reports.
That the CDC and FDA failed to respond is arguably not surprising – they have been cheerleading this vaccine for months. Admitting almost any harm now would be akin to asking them to turn a gun on themselves.
This again highlights the importance of never permitting government coercion and mandates when it comes to medical procedures.
Full letter to the CDC and FDA:
Letter exchange with the hospital:
In-depth interview with Ms. Conrad on the Highwire:
Sometimes it pays to step back in history to understand exactly how something monumental was created. This is the story of how one Big Lie turned our world upside down and ruined the lives of millions of people.
Hard to believe that one Big Lie could have created all the pandemic controls, especially lockdowns, school closings and quarantines, that devastated our lives, our economy and our society. But it happened.
A very powerful, influential person told the world in early 2020 that the new China virus that leads to COVID-19 infection was especially lethal. It quickly pushed a fast, enormous response to protect public health. Was the truth was being told? It was not. There was an exaggeration of the new virus lethality for the entire population.
In truth, it was only severe for the oldest age category. Helped by corrupt data from CDC, overstatement of COVID lethality continues today to maintain public fear.
But first it is important to discuss the meaning of critically important terms. What the Big Lie was all about had to do with the fatality or death rate of what early in 2020 was seen as an invading new virus coming from China. How should we think about the fatality rate of a virus?
Terminology
One simple and correct way is how many people die from the infection caused by the virus: the Infection Fatality Rate (IFR). But another possible way would be to invoke the Case Fatality Rate (CFR); the fraction of documented cases of people with the virus that resulted in death.
How can you know how many people are infected? A lot of testing would be necessary. For our COVID pandemic there has been, surprisingly, very little wide blood testing across the whole population. Many people with infections have no symptoms or just mild ones and do not seek testing or medical attention. The CDC has done a terrible job of getting good data on infection numbers.
As to cases ascribed to COVID, there are reasons why that number surely underestimates how many people are really infected. Why? Because only some people, usually with symptoms, get tested and if found positive become a case. On the other side, the PCR test method most widely used has often been implemented in a way to get false positive results.
Mainly because the number of cycles the test is run is far too high (above 25) and picks up fragments of the virus (or any coronavirus) that does not document real COVID infection. Thus, the CFR is not a reliable or accurate measure of the real death rate despite widely published case numbers.
Key Moment In History
During a March 11, 2020 hearing of the House Oversight and Reform Committee on coronavirus preparedness, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Disease, put it plainly: “The seasonal flu that we deal with every year has a mortality of 0.1 percent,” he told the congressional panel, whereas coronavirus is “10 times more lethal than the seasonal flu,” per STAT news. [0.1 percent also expressed as .001]
He also said: “The bottom line: It is going to get worse.” And this: “The stated mortality, overall, of [the coronavirus], when you look at all the data including China, is about 3 percent.”
That figure of 3 percent, far from reliable, is 30 times greater than the figure given for the seasonal flu. Fauci exaggerated to create a crisis. Simply by implying great lethality for everyone infected by the new COVID virus.
And it should be noted that CDC has found the flu IFR ranged from 0.1 percent (the figure cited by Fauci) to 0.17 percent [.0017] from 2014 to 2019, because seasonal deaths vary significantly.
What Fauci said put the country, with the help of big media, into convulsions. It created the foundation for authoritarian contagion controls driving a spike into the lives of Americans. Fauci intentionally created the pandemic by creating fear.
New York City Analysis
An interesting analysis was made for IFR for New York City at the height of the pandemic in May 2020. It illustrates how both death and infection data can be fine-tuned to get an IFR. As to deaths, blood testing found that 19.9 percent of people had antibodies indicating infection, yielding a number of 1,671,351 infected. As to deaths from COVID, there were three components: 13,156 confirmed, 5,126 probable, and 5,148 excess for a total of 23,430, that may have overstated deaths.
Probable meant likely COVID death but not confirmed through testing. Excess meant the number above expected seasonal baseline level. Using the total deaths divided by total infected produces an IFR of .014. Higher than the usual quoted flu value [.001] for the height of the pandemic in high density New York City.
And without consideration of variations among most vulnerable groups. A high rate of fatality for elderly people would cause a deceptive high value for IFR for the entire population.
Deaths certainly have declined significantly in the past year and more (even as high transmissivity delta variant has probably maintained high levels of infections). Why? Because of far better actions in hospitals and because infected people have surely learned a lot about home treatments to catch COVID infection early after initial symptoms and possibly a positive test. Cutting the deaths in half for the same number of infected people results in an IFR of .007, probably a more realistic figure for today.
World Health Organization
At an October 2020 meeting of the World Health organization, Dr Michael Ryan, the Head of Emergencies revealed that they believe roughly 10 percent of the world has been infected with Sars-Cov-2. This is their “best estimate.” This figure was based on the average results of all the broad seroprevalence (blood) studies done around the world. The message was that the virus is nothing as deadly as everyone predicted.
At the time the global population was roughly 7.8 billion people, if 10 percent have been infected that is 780 million infections. The global death toll then attributed to Sars-Cov-2 infections was seen as 1,061,539. That’s an infection fatality rate of roughly or 0.14 percent [.0014]. Consistent with seasonal flu and the predictions of many experts from around the world. And inconsistent with the dire picture given by Fauci.
Great Analysis
Now consider the detailed analysis “Public Health Lessons Learned From Biases in Coronavirus Mortality Overestimation” by Ronold B. Brown published in August 2020. He has doctoral degrees in public health and organizational behavior.
Here are highlights from this article that focused on what Fauci said.
“The validity of this estimation could benefit from vetting for biases and miscalculations. The main objective of this article is to critically appraise the coronavirus mortality estimation presented to Congress.”
[What Fauci said] “helped launch a campaign of social distancing, organizational and business lockdowns, and shelter-in-place orders.”
“Previous to the Congressional hearing, a less severe estimation of coronavirus mortality appeared in a February 28, 2020 editorial released by NIAID [Fauci’s department] and the Centers for Disease Control and Prevention (CDC). Published online in the New England Journal of Medicine (NEJM.org), the editorial stated: ‘…the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1 percent).’
Almost as a parenthetical afterthought, the NEJM editorial inaccurately stated that 0.1 percent is the approximate case fatality rate of seasonal influenza. By contrast, the World Health Organization (WHO) reported that 0.1 percent or lower is the approximate influenza infection fatality rate, not the case fatality rate.“
Brown correctly hit the key semantic issue: CFR versus IFR.
“IFRs are estimated following an outbreak, often based on representative samples of blood tests of the immune system in individuals exposed to a virus. Estimation of the IFR in COVID-19 is urgently needed to assess the scale of the coronavirus pandemic.“ [Now, over a year later this has not happened.]
Brown correctly emphasized “it is imperative to not confuse fatality rates [CFR and IFR] with one another; else misleading calculations with significant consequences could result.” [That is exactly what Fauci engineered.]
Brown said the 1 percent figure in the testimony was consistent with the “coronavirus CFR of 1.8-3.4 percent (median, 2.6 percent) reported by the CDC.” [As I write this data in The Washington Post shows a CFR of 1.6 percent. This substantiates that the health care system has made progress in curbing COVID deaths. But this current CFR is still 16 times higher than the IFR figure for the seasonal flu. IFR remains the issue.]
Now Brown gets to the heart of the problem: “A comparison of coronavirus and seasonal influenza CFRs may have been intended during Congressional testimony, but due to misclassifying an IFR as a CFR, the comparison turned out to be between an adjusted coronavirus CFR of 1 percent and an influenza IFR of 0.1 percent.”
[Did Fauci, the widely lauded expert, not know what he was doing? Hard to believe this. If he knew, then we have the explanation for the Big Lie.]
By May 2020 “it was clear that the coronavirus mortality total for the season would be nowhere near 800,000 deaths inferred from the 10-fold mortality overestimation reported to Congress [emphasis added].
Even after adjusting for the effect of successful mitigation measures that may have slowed down the rate of coronavirus transmission, it seems unlikely that so many deaths were completely eliminated by a nonpharmaceutical intervention such as social distancing, which was only intended to contain infection transmission, not suppress infections and related fatalities.”
As to getting good data to determine IFR, Brown noted: “A revised version of a non–peer-reviewed study on COVID-19 antibody seroprevalence in Santa Clara County, California, found that infections were many times more prevalent than confirmed cases.
As more serosurveys are conducted throughout the country, a nationally coordinated COVID-19 serosurvey of a representative sample of the population is urgently needed, which can determine if the national IFR is low enough to expedite an across-the-board end to restrictive mitigating measures.”
[In other words, with systematic blood testing, if we have an IFR for COVID similar to the IFR for the seasonal flu, then the many disruptive and costly actions by the public health establishment are not justified. And they never were! ]
Another Analysis
The title of this September 2020 article by Len Cabrera is “Mistake or Manipulation.” An initial point made was: “A review of the early events mentioned in Dr. Brown’s paper and the lack of any corrections to the record suggest that the misstatement [by Fauci] before Congress was not a mistake.” If not a mistake, then it was intentional.
This point was dead on: “In his testimony, Dr. Fauci claimed the mortality of flu was 0.1 percent and that the case fatality rate of COVID was 3 percent but could be as low as 1 percent with asymptomatic cases. This is an apples-to-oranges comparison of the flu’s infection fatality rate (IFR) to COVID-19’s case fatality rate (CFR).”
And this critical point was made: “All cases are infections, but not all infections are confirmed cases, so the number of infections always exceeds the number of cases, making IFR less than CFR.” In other words, if the number of deaths is the same, then a lower denominator for calculating CFR compared to that for getting the IFR results in a higher number for CFR.
Are we to believe that the esteemed Fauci did not know this? Or is it reasonable to conclude that Fauci knew exactly what he was doing, namely using some simple data to create a pandemic crisis that required massive authoritarian government actions? Fauci set the stage for his wait-for-the-vaccine pandemic strategy that he sold to President Trump.
This required that the government establish blocks to wide use of the safe, cheap, effective and FDA approved generic medicines already found to cure COVID in early 2020, namely ivermectin and hydroxychloroquine. Details about these early treatment protocols are given in Pandemic Blunder.
Here is another point made: “A careful viewing of the testimony suggests the line [COVID being 10 times worse than flu] was not a mistake.
Dr. Fauci was specifically asked if COVID was less lethal than H1N1 or SARS. Rather than refer to his own NEJM article saying SARS had a case fatality rate of 9-10 percent (3 to 10 times worse than COVID), Dr. Fauci said, “Absolutely not… the 2009 pandemic of H1N1 was even less lethal than regular flu… this is a really serious problem that we have to take seriously.”
He repeated that COVID’s “mortality is 10 times that [of influenza]” and concluded with, “We have to stay ahead of the game in preventing this.”
This also was a prescient view: ”This was a perfect series of switches: IFR to CFR, voluntary isolation for the sick to mandatory isolation for everyone, two weeks to flatten the curve to indefinite lockdown until there’s a vaccine. (If you think it will be voluntary, you’re not paying attention.)”
Add this to the quest for truth: “A study in France looked at all-cause mortality data from 1946 to 2020 and concluded that ‘SARS-CoV-2 is not an unusually virulent viral respiratory disease pathogen” because there is no significant increase in mortality. Of the deaths in 2020, the study said, ‘unprecedented strict mass quarantine and isolation of both sick and healthy elderly people, together and separately, killed many of them.’”
Here is the article’s correct conclusion: “Sadly, many politicians were duped and went along with the recommendations for lockdowns and masks that followed from Dr. Fauci’s 10-times-deadlier testimony. Don’t expect them to admit their mistakes, either. Perhaps the only thing harder for a politician than telling the whole truth is admitting a mistake.”
What Is The Truth?
If you listen to many experts, you hear this truth based on CDC data: 99.8 or 99.9 percent of people across all ages who get infected by COVID do not die. That means that the IFR overall is .001 or .002. In other words, not so terribly worse than the flu IFR, but it does vary with age.
In September 2020 these CDC age related data were reported:
Updated survival rates and IFR by age group:
0-19: 99.997 percent, IFR .003 percent
20-49: 99.98 percent, IFR .02 percent
50-69: 99.5 percent, IFR .5 percent
70+: 94.6 percent, IFR 5.4 percent
Note that through age 49 the IFR is less than the average for flu of 0.1 percent, but higher for older people. And only for the 70+ group is the IFR more than 10 times greater. In other words, only for the oldest group is what Fauci said in his congressional testimony accurate. What if Fauci had said something in tune with that reality? The vaccine program he pushed should have focused on the elderly, not the entire population.
From the important recent report “COVD-19: Restoring Public Trust During A Global Health Crisis” are age data and COVID CFR [through Feb. 16, 2021]. Note these are Case Facility Rate data, meaning that the figures are very exaggerated because the number of infected are very much higher than the number of cases: probably 100 million more infections than cases. Thus, the total across all age groups of 1.701 percent, [.01701] should be corrected to .289 percent [.00289]; this is about three times higher than the cited flu IFR, not the 10 times higher given by Fauci. And it would be much lower for the less than 70 population.
A very recent article said this: “While estimates of COVID-19’s infection fatality rate (IFR) range from study to study, the expert consensus does indeed place the death rate at below 1 percent for most age groups.” Fauci did indeed overhype COVID for all but the very elderly. This supports the view of the eminent Dr. Peter McCollough that a wise COVID vaccine strategy would have been to target the elderly, not the entire population.
The widely acclaimed medical researcher John P. Ioannidis of Stanford University has examined IFR for COVID in considerable detail,
In October 2020 he said this: “The infection fatality rate of COVID-19 can vary substantially across different locations and this may reflect differences in population age structure and case-mix of infected and deceased patients and other factors. The inferred infection fatality rates tended to be much lower than estimates made earlier in the pandemic.”
At that time, he said:” Across 51 locations, the median COVID-19 infection fatality rate was 0.27 percent (corrected 0.23 percent).” Higher than the Fauci quoted value for the flu (0.1 percent), but not 10 times greater.
A new report from the defense department gives data on 5.6 million fully vaccinated Medicare participants age 65 and older. There were 161,000 recent breakthrough COVID infections and the IFR was 0.021. It noted an IFR for this group of0 .12 (about five times greater) during the March to December 2020 period when there was far less effective hospital care and no mass vaccination.
Both IFRs for elderly Americans are greater than the quoted typical flu value, but far from a very lethal viral infection.
Recently, it was reported that according to CDC work “More than 39 million Americans have been diagnosed with coronavirus infection since the pandemic started in 2020.” Using that figure, that may be too low because only 1.4 million blood samples were tested, together with the current CDC value of about 700,000 COVID fatalities results in an average IFR of 0.018.
Why is 39 million infected people low? Because many medical experts have said that there are probably some 100 million Americans with natural immunity resulting from COVID infection.
The key word to question in what CDC did is “diagnosed.” In other words, people who were tested and found positive. But clearly a large fraction of asymptomatic and mildly symptomatic people did not get tested. So, what if you add 100 million to the 39 million figure and then use that as the denominator, with 700,000 deaths in the numerator, and calculate the IFR?
You get an IFR of 0.005. Not ten times higher than the flu value cited by Fauci in his congressional testimony [actually 3 times higher than the high end of flu IFR values].
Podcaster Jack Murphy, who founded Liminal Order, deduced that because the CDC said there were twice as many people who were infected with COVID, then it automatically meant that the lethality rate must be cut in half, commenting that the virus that had killed 646,000 Americans in the last 19 months is “far less lethal than already known.”
Murder Motivation
To accept the entire argument for a Big Lie it is necessary to explain the motivation for Fauci to intentionally tell the public that the new China virus was extremely lethal. So much worse than seasonal flu. So awful that extreme government action was needed.
It is relevant to note that in January 2017 Fauci warned the Trump administration, in a public talk, that no doubt there would be a “surprise outbreak” of a new infectious disease pandemic. “The thing we’re extraordinarily confident about is that we’re going to see this in the next few years,” he said. He got what he wanted.
Maybe all the talk about a “plandemic” was spot on. And maybe Fauci had insights because he was funding the work at the Wuhan Laboratory to develop extremely toxic viruses.
What Fauci said about high lethality set in motion an onerous set of government actions justified on the basis of protecting public health. Why would anyone want to overstate the lethality of the new COVID-19 virus? It was the only way to use onerous pandemic control and management methods that Fauci favored. It was necessary to set in motion a COVID vaccine program. Most of all, his strategy was used to create very high levels of FEAR in the public so that they would accept his favored government actions.
Understand this. Fauci is not a trained public health expert, nor a trained epidemiologist or virologist. He was a plain physician who over many decades as a top NIH bureaucrat accumulated enormous power. He never did what true public health experts have an ethical obligation to do. That is to tell the public both the positives and negatives of public health policies and actions.
The point is this: By pushing the need for pandemic actions to address a very lethal virus a host of government actions produced so much economic, social and personal hardships and dislocations. And many analyses have concluded that more Americans died from the government actions than from the COVID virus.
Perversely, pandemic public health actions actually harmed public health. But with widespread mainstream media support Fauci got away with everything.
Hundreds of thousands of Americans died unnecessarily. Fauci is guilty of criminally negligent homicide stemming from his initial and very public overstatement of the lethality of the COVID virus. Those who have screamed for his prosecution have a valid case.
With his power he created policies that created data to support this lethality claim. One big action was to create a testing protocol using the PCR technology in ways that created very high case levels. The inventor of that technology said it was inappropriate for diagnosing the viral infection. Millions of COVID cases resulted from running PCR equipment at very high cycle rates [high than 25]. Meanwhile the government never did widespread blood testing to get data for knowing the IFR.
The other major way to keep up public support for pandemic controls was to ensure high numbers of COVID deaths. This was done through directives on how death certificates should be filled out and through financial incentives for hospitals to certify deaths as COVID ones.
Recent analysis that in March 2020 CDC changed guidelines on how death certificates were to be filled out. Different than the procedure used for 17 years prior to this change.
This study found a COVID fatality figure of 161,392 with the new reporting versus 9,684 for the older procedure. There is little doubt that COVID death data, even accounting for some overcounting because of people dying not from any COVID influence, have been too high. This means that IFR data have been too high.
The combination of false high levels of cases and deaths helped maintain public fear of a very lethal virus. That is not correct for nearly all people younger than 70 years old.
Conclusions
To sum up: COVID was intentionally over hyped by Fauci as a very deadly disease to justify the most extreme public health actions. This was the Big Lie. Most valid data now show COVID lethality is similar to that for seasonal flu for the vast majority of people. But accepting that truth would not have justified the array of excessive government actions used for the false pandemic.
Yes, many people have died from COVID, but deaths have been overreported and infections underreported. And most deaths – at least 85% – could have been prevented by using generic medicines, such as ivermectin. There is no doubt that a great many people die with COVID but not FROM COVID, also arguing for a low IFR. At one point CDC said that only 6% of deaths resulted only from COVID, making the IFR much lower than the flu IFR.
Finally, recognizing the true lower IFR for COVID the whole rationale for mass vaccination collapses, especially in view of very high levels of adverse effects and deaths from the vaccines themselves.
Which makes perfect sense if you appreciate that the COVID IFR is now similar to the flu IFR for most people. Especially if you recognize that CDC has found the flu IFR ranged from 0.1 percent (the figure cited by Fauci) to 0.17 percent from 2014 to 2019.
Understanding that the lethality of COVID is far from the terrible picture painted by Fauci at the very beginning of the pandemic is key to weighing the risk/benefit ratio when deciding to get vaccinated. For most people the risk from the vaccine is greater than the benefit. Only the elderly have a good reason to get the shot.
Some 81 percent of COVID deaths are for people over 65. As has been pointed out by many people, the average age of most COVID deaths for elderly victims have been consistently higher than average life expectancy ages.
A new article has made important observations. The main one is that countries with low vaccination levels have been doing better than those with mass vaccination programs, like the US. The results are consistent with a widely accepted understanding that the vaccines do not effectively stem virus infection or transmission. More vaccination equated to more viral spreading.
The new study ended with advice to learn “to live with COVID-19 in the same manner we continue to live a 100 years later with various seasonal alterations of the 1918 Influenza virus.”
Dr. Joel S. Hirschhorn is the author of Pandemic Blunder and many articles on the pandemic, worked on health issues for decades. As a full professor at the University of Wisconsin, Madison, he directed a medical research program between the colleges of engineering and medicine. As a senior official at the Congressional Office of Technology Assessment and the National Governors Association, he directed major studies on health-related subjects; he testified at over 50 US Senate and House hearings and authored hundreds of articles and op-ed articles in major newspapers. He has served as an executive volunteer at a major hospital for more than 10 years. He is a member of the Association of American Physicians and Surgeons, and America’s Frontline Doctors.
We seek answers from the so-called “authorities” about what defines Covid Misinformation…
Also I will blow the lid on the publicly released TVNZ emails leading to my sacking as a TV show presenter.
It’s unscripted comedy at it’s best!
Homes that switch to heat pumps risk being switched off for weeks at a time, according to a new paper from the Global Warming Policy Foundation. That’s because the government’s heat strategy fails to address the fundamental problem of intermittency.
According to the report’s author, Andrew Montford, without any means of storing electricity in bulk, grid managers will be forced to switch down appliances like heat pumps and EV chargers when the wind doesn’t blow. In a long wind lull, homes will have to be switched off entirely. Second-generation smart meters, currently being installed across the country, will allow the grid to control appliances remotely.
Montford explains that the technologies that are widely thought to help with intermittency are in fact only marginally useful: “We don’t have enough suitable pumped hydro sites, and batteries and hydrogen are far too expensive”, he says. “The only technology that can help us here are based around fossil fuels, and the government has ruled those out”.
Moreover, it is not just a wind lull that will mean appliances have to be switched off. The distribution grid, which moves electricity around at street level, was designed for much lower loads than will be necessary in a Net Zero world. That means when too many people require power, grid managers will again have to ration demand.
GWPF director, Dr Benny Peiser, says that the report is a warning to politicians: “Leaving families cold and in the dark will lead to some very unhappy constituents. It will not end well”.
The report, entitled Survival of the Richest: Smart Meters and Energy Rationing, can be downloaded here.
… At every corner, we are urged to simply believe what we are told. Whether it is about believing Porton Down and MI6 about “novichok”, or believing the White Helmets about Sarin, or believing the FBI about “collusion”, we are presented with no facts, just assertions from authority. Those who question those assertions are deemed “bots” at best or “traitors” at worst.
Well here, fellow traitors, are the Top Ten reasons to question anything and everything the CIA – or any intelligence agency – has ever told you. … Read full article
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.


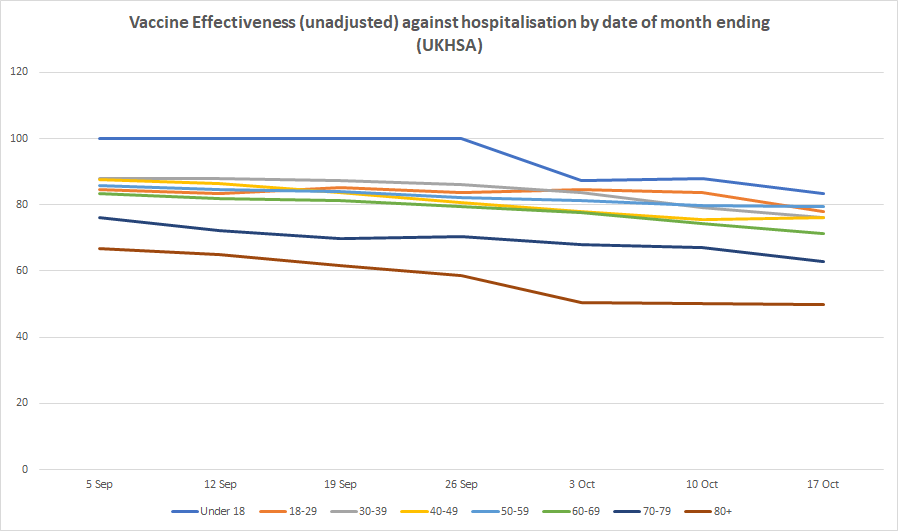







 Aletho News
Aletho News