FDA Grants Emergency Use of Pfizer Vaccine for Kids 5 to 11, as Reports of Injuries After COVID Vaccines Near 840,000
By Megan Redshaw | The Defender | October 29, 2021
Data released Friday by the Centers for Disease Control and Prevention (CDC) showed that between Dec. 14, 2020, and Oct. 22, 2021, a total of 837,595 adverse events following COVID vaccines were reported to the Vaccine Adverse Event Reporting System (VAERS).
The data included a total of 17,619 reports of deaths — an increase of 491 over the previous week. There were 127,457 reports of serious injuries, including deaths, during the same time period — up 4,624 compared with the previous week.
Excluding “foreign reports” to VAERS, 622,743 adverse events, including 8,068 deaths and 51,532 serious injuries, were reported in the U.S. between Dec. 14, 2020, and Oct. 22, 2021.
Of the 8,068 U.S. deaths reported as of Oct. 22, 11% occurred within 24 hours of vaccination, 15% occurred within 48 hours of vaccination and 27% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 411.6 million COVID vaccine doses had been administered as of Oct. 15. This includes: 242 million doses of Pfizer, 154 million doses of Moderna and 15 million doses of Johnson & Johnson (J&J).

The data come directly from reports submitted to VAERS, the primary government-funded system for reporting adverse vaccine reactions in the U.S.
Every Friday, VAERS makes public all vaccine injury reports received as of a specified date, usually about a week prior to the release date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed.
Historically, VAERS has been shown to report only 1% of actual vaccine adverse events.
This week’s U.S. data for 12- to 17-year-olds show:
- 22,212 total adverse events, including 1,348 rated as serious and 25 reported deaths. Two of the 25 deaths were suicides.
The most recent death involves a 12-year-old girl (VAERS I.D. 1784945) who died from a respiratory tract hemorrhage 22 days after receiving her first dose of Pfizer’s vaccine.
Another recent death includes a 15-year-old male who died six days after receiving his first dose of Pfizer’s COVID vaccine. According to his VAERS report (VAERS I.D. 1764974), the previously healthy teen complained of brief unilateral shoulder pain five days after receiving his COVID vaccine. The next day he played with two friends at a community pond, swung on a rope swing, flipped into the air, and landed in the water feet first. He surfaced, laughed and told his friends “Wow, that hurt!” He then swam toward shore underwater, as was his usual routine, but did not re-emerge.
An autopsy showed no external indication of a head injury, but there was a small subgaleal hemorrhage — a rare, but lethal bleeding disorder — over the left occiput. In addition, the boy had a mildly elevated cardiac mass, increased left ventricular wall thickness and small foci of myocardial inflammation of the lateral wall of the left ventricle with myocyte necrosis consistent with myocardial infarction.
- 58 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment or resulted in death — with 96% of cases
attributed to Pfizer’s vaccine. - 539 reports of myocarditis and pericarditis (heart inflammation) with 531 cases attributed to Pfizer’s vaccine.
- 125 reports of blood clotting disorders, with all cases attributed to Pfizer.
This week’s U.S. VAERS data, from Dec. 14, 2020, to Oct. 22, 2021, for all age groups combined, show:
- 19% of deaths were related to cardiac disorders.
- 54% of those who died were male, 41% were female and the remaining death reports did not include gender of the deceased.
- The average age of death was 72.7.
- As of Oct. 22, 4,151 pregnant women reported adverse events related to COVID vaccines, including 1,296 reports of miscarriage or premature birth.
- Of the 3,065 cases of Bell’s Palsy reported, 51% were attributed to Pfizer vaccinations, 41% to Moderna and 8% to J&J.
- 685 reports of Guillain-Barré syndrome, with 41% of cases attributed to Pfizer, 31% to Moderna and 28% to J&J.
- 2,043 reports of anaphylaxis where the reaction was life-threatening, required treatment or resulted in death.
- 10,493 reports of blood clotting disorders. Of those, 4,590 reports were attributed to Pfizer, 3,766 reports to Moderna and 2,083 reports to J&J.
- 2,971 cases of myocarditis and pericarditis with 1,865 cases attributed to Pfizer, 978 cases to Moderna and 118 cases to J&J’s COVID vaccine.
FDA grants Emergency Use Authorization for Pfizer Vaccine for 5- to 11-year-olds
The U.S. Food and Drug Administration (FDA) today granted Emergency Use Authorization (EUA) for the Pfizer-BioNTech COVID vaccine for children 5 to 11 years old, The Associated Press reported.
The announcement followed Tuesday’s recommendation by the FDA’s vaccine advisory committee that the agency grant Pfizer’s request. The advisory committee vote passed with 17 in support, and one abstention.
Reporting on today’s news, STAT noted:
“The vaccine was not granted FDA approval, but instead an emergency use authorization. Emergency authorizations are used when the secretary of health and human services has declared a public health emergency to more quickly clear the use of vaccines, treatments, and diagnostic tests. These authorizations lapse when the state of emergency ends. Pfizer’s vaccine was fully approved for those age 16 and older in August, and was previously granted an emergency use authorization for use in adolescents ages 12 to 15.”
The dose for younger children will be one-third the strength given to people 12 and older, with two shots given three weeks apart. Before the shots can be rolled out, the CDC must weigh in with its own recommendations.
During Tuesday’s meeting, the Vaccines and Related Biological Products Committee heard evidence from Pfizer and regulators, and listened to concerns raised by multiple scientists and physicians.
Based on CDC data presented during the meeting, among children 5 to <12 years of age, there have been approximately 1.8 million confirmed and reported COVID cases since the beginning of the pandemic, and only 143 COVID-related deaths in the U.S. through Oct. 14.
Pfizer provided safety data on two study cohorts of children ages 5 to 11, both of roughly equal size. The first group was followed for only about two months, the second for only two-and-a-half weeks.
Pfizer said “post-vaccination myocarditis/pericarditis” in participants 5 to <12 years of age will not be studied until after the vaccine is authorized for children.
Pfizer vaccine ‘failed any reasonable risk-benefit calculus in connection with children,’ scientist says Brian Dressen, Ph.D., is one of the scientists who testified Tuesday during the FDA advisory committee’s 8-hour hearing. Dressen is also the husband of Brianne Dressen, who in 2020 developed a severe neurological injury during the Utah-based portion of the U.S. AstraZeneca COVID vaccine.
During his 3-minute testimony, Dressen, a chemist with an extensive background in researching and assessing the degree of efficacy in new technologies, told the FDA advisory panel Pfizer’s vaccine “failed any reasonable risk-benefit calculus in connection with children.”
Dressen said the decision to authorize for 5- to 11-year-olds is being rushed and is based on “incomplete data from underpowered trials, insufficient to predict rates of severe and long-lasting adverse reactions.”
Dressen urged the committee to reject the EUA modification and direct Pfizer to perform trials that decisively demonstrate the benefits outweigh the risks for children.
Dressen’s wife was severely injured last November after receiving her first and only dose of a COVID vaccine administered during a clinical trial.
“Because study protocol requires two doses, she was dropped from the trial, and her access to the study app deleted,” Dressen said. “Her reaction is not described in the recently released clinical trial report — 266 participants are described as having an adverse event leading to discontinuation, with 56 neurological reactions tallied.”
CDC updates guidance allowing immunocompromised to get a fourth COVID shot
Immunocompromised adults who received a third dose of either the Pfizer-BioNTech or Moderna COVID vaccine will become eligible for a fourth booster shot six months after receiving their third dose, according to CDC guidance issued Monday.
“In such situations, people who are moderately and severely immunocompromised may receive a total of four vaccine doses,” with the fourth coming at least six months after the third, the CDC’s new guidelines said.
In August, the CDC authorized a third dose of either Pfizer-BioNTech or the Moderna mRNA vaccine — but not Johnson and Johnson’s (J&J) adenovirus vaccine — for certain immunocompromised people 18 and older.
However, a third dose is now considered part of the primary series, rather than a booster. The earliest that immunocompromised people who received a third mRNA vaccine shot can get a fourth shot as a booster would be February.
The agency said people could select that booster from any of the three COVID vaccines available in the U.S, including J&J, but specified a fourth dose of Moderna’s vaccine should be half the size of a normal dose.
Double-vaccinated can still spread the virus at home
Fully vaccinated people are catching COVID and passing it on to those they live with, warn experts in the UK. A British study published in the Lancet Oct. 29, showed individuals who have had two vaccine doses can be just as infectious as those who have not been jabbed.
Even if they are asymptomatic or have few symptoms, the chance of transmitting the virus to other unvaccinated housemates is about two in five, or 38%. This drops to one in four, or 25%, if housemates are also fully vaccinated.
“By carrying out repeated and frequent sampling from contacts of COVID-19 cases, we found that vaccinated people can contract and pass on an infection within households, including to vaccinated household members,” said Dr. Anika Singanayagam, co-lead author of the study.
“Our findings provide important insights into … why the Delta variant is continuing to cause high COVID-19 case numbers around the world, even in countries with high vaccination rates.
Vaccinated contacts who tested positive for COVID on average received their shots longer ago than those who tested negative, which the authors said was evidence of waning immunity and supported the need for booster shots.
Neil Ferguson, an Imperial epidemiologist, said the transmissibility of Delta meant that it was unlikely Britain would reach herd immunity for long.
“That may happen in the next few weeks: If the epidemic’s current transmission peaks and then starts declining, we have by definition in some sense reached herd immunity, but it is not going to be a permanent thing,” Ferguson told reporters.
16-year-old girl develops severe vulvar ulcers after second Pfizer shot
A case report published Oct. 25 in the Journal of Pediatric and Adolescent Gynecology revealed a new potential novel side effect of Pfizer’s COVID vaccine that doctors say warrant further investigation.
According to the report, a 16-year-old non-sexually active female presented to the pediatric gynecology clinic with vaginal pain six days after receiving her second dose of Pfizer’s COVID vaccine.
Within 24 hours of receiving the vaccine, the girl developed fever, fatigue, myalgias and “sores” in her vaginal area. Over the next two days, right-sided lesions in her vaginal area coalesced and became more painful. The teen went to the urgent care with a fever of 105 degrees. She was diagnosed with a Bartholin gland abscess.
Despite antibiotic therapy, her symptoms worsened and her lesions were covered in exudate with a necrotic, ring-like border. In the gynecology clinic, the patient’s lesions were exquisitely painful, resulting in difficulty with urination, defecation and walking. She had no respiratory symptoms and no history of COVID exposure.
The report said the findings “were consistent with vulvar aphthous ulcers in association with influenza-like symptoms following Pfizer BioNTech (BNT162b2) COVID-19 vaccination.”
“Our patient had typical clinical features of aphthous ulcer, including an influenza-like prodrome and characteristic dermatologic manifestations which occurred after receiving the Pfizer COVID vaccine,” the authors wrote. According to the report, the girl’s case was submitted to VAERS “due to the temporal relationship with COVID vaccine administration.”
Children’s Health Defense asks anyone who has experienced an adverse reaction, to any vaccine, to file a report following these three steps.
Megan Redshaw is a freelance reporter for The Defender. She has a background in political science, a law degree and extensive training in natural health.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Yale Epidemiologist Cautions About Child Vaccination
By Tom Woods | Principia Scientific International | October 29, 2021
The next wave of vaccination mandates will involve children. Since anyone raising concerns about this is considered an enemy of society, it’s been impossible to have a rational discussion about it.
Here’s what Harvey Risch, professor of epidemiology at the Yale School of Public Health and the Yale School of Medicine had to say about it this week.
“As far as I can tell, it’s a top-down structure, and most doctors do not get their information by going back and reading the original studies and making up their own minds. They get fed the information from pharma reps or from what they’re told from societies. The conflicts are legion. So it’s no surprise that most doctors don’t pay attention and think what they’re told…
“If the child has chronic conditions that make their risk appreciable, then there is a reason that they should be considered for vaccination. Other than that, if it were my child, I would homeschool them. Honestly, I would organize with other parents to take them out of the school and create a homeschooling environment.
There is no choice. Your child’s life is on the line.
“It’s not a high risk. Vaccination is not a high risk that’s going to kill every child by doing so. However, it’s enough of a risk that on the average the benefit is higher for homeschooling than it is for vaccination and being in school.”
Martin Kulldorff of Harvard is saying something similar:
“I don’t think children should be vaccinated for COVID. I’m a huge fan of vaccinating children for measles, for mumps, for polio, for rotavirus, and many other diseases. That’s critical. But COVID is not a huge threat to children….
“They can be infected, just like they can get the common cold, but they’re not a big threat. They don’t die from this, except in very rare circumstances. So if you want to talk about protecting children or keeping children safe, I think we can talk about traffic accidents, for example, which they are really at some risk…. And there are other things that we should make sure [of] to keep children safe. But COVID is not a big risk factor for children.”
Kulldorff points to the experience of his native Sweden. Beginning with the first wave in the spring of 2020, Sweden “decided to keep daycare and schools open for all children ages 1 to 15.
And there are 1.8 million such children who got through the first wave without vaccines, of course, without masks, without any sort of distancing in schools.
If a child was sick, they were told to stay home. But that was basically it. And you know how many of those 1.8 million children died from COVID? Zero. Only a few hospitalizations. So this is not a risky disease for children.”
He concludes: “If you’re a child, even if you haven’t had COVID, the risk of serious disease or death is minuscule … So it’s not at all clear that the benefits outweigh the risks for children.”
Try discussing this with friends and relatives on social media, and you run the risk of being silenced.
We are not even allowed to discuss these things. And when in our lifetimes has free discussion been more urgently needed?
There’s no censorship in my group, the Tom Woods Show Elite.
Here we discuss important matters like adults.
If you’re in a position where you don’t need such a thing, you are among the lucky few.
New York City’s New ‘Public Health’ Plan: Let Garbage Pile Up on the Sidewalks

By Adam Dick | Ron Paul Institute | October 29, 2021
In the name of “public health,” the New York City government this week has been telling city employees to take the experimental coronavirus “vaccine” shots by Friday at 5 p.m. or be fired, or as the city government terms it, “placed on leave without pay.” Plenty of city workers of all types upset by this attack on their freedom have been taking to the streets in large numbers to protest, often admirably joined by leaders of their unions.
Apparently, New York City garbagemen upset with their mistreatment have chosen to skip days of work as well. The result, detailed in a Thursday article by Jean Lee at NBC News is trash piling up in parts of the city as regularly scheduled trash collection fails to occur.
What to expect after the Friday deadline? Continued piling up of trash on New York City sidewalks, right next to where millions of people in the densely populated city live, work, shop, and play each day is a good bet. Lee quotes the president of the Sanitation Officers Association:
Joseph Mannion, president of the Sanitation Officers Association, fears the trash pileups might foreshadow a possible worker shortage on Monday if vaccination rates among sanitation workers don’t increase by Friday. He said that the sanitation department has been moving to snow season shifts — 12 hours instead of eight — in anticipation of a possible worker shortage.
‘Prepare for the worst and hope for the best,’ Mannion said.
But Mannion is skeptical and said that he knows many sanitation workers are “hardened in their beliefs” and will refuse vaccination, even if it means being put on unpaid leave.
‘I know more people are getting vaccinated, but is it going to change around 60 percent to 80 percent?’ asked Mannion. ‘I don’t know. I don’t think so.’
More and more people in New York City must be asking themselves which is a healthier, and more pleasant, option: (A) letting trash continue to pile up on sidewalks while 100 percent of garbagemen are confirmed to have taken the experimental coronavirus vaccine shots, or (B) having trash regularly cleared from sidewalks while letting garbagemen choose whether they take the shots? My guess is that most people will choose option B, especially if the trash keeps piling up for weeks or even months on end.
Nov. 3: Join the ‘Worldwide Walkout,’ a Global Protest Against Government Overreach
Children’s Health Defense
Children’s Health Defense (CHD) on Nov. 3 will join organizations and individuals in “Worldwide Walkout” by calling in sick or taking a personal day to protest the unprecedented loss of freedom that has occurred the world over since the COVID pandemic began.
Parents will also pull their children out of school for the day to protest the many restraints that have applied directly to children.
“No government in history has ever surrendered power in the absence of a demand,” said Robert F. Kennedy, Jr., CHD chairman and chief legal counsel. “We need to tell these governments and their friends in the technocracy, the Silicon Valley billionaire boys club, the mainstream media and the pharmaceutical industry that we will no longer tolerate their trampling of citizens’ rights.”
Emboldened by reports of a recent walkout of Southwest employees — which led the airline’s management to drop plans to put unvaccinated employees on unpaid leave — nurses, doctors, teachers, police officers, firefighters and other workers are expected to participate in the protest.
“Coercive mandates of shoddily tested medical products and segregationist passports violate international human rights law,” said CHD President and General Counsel Mary Holland.
Holland added:
“We need brave citizens to peacefully refuse to comply with unlawful and unethical edicts that for the past year-and-a-half have been allowed to trump individual rights and freedoms. Those days are over. There will be no business as usual until segregationist and coercive medical policies advanced by government authorities end once and for all.”
Organizers announced the protest after the Vaccines and Related Biological Products Advisory Committee (VRBPAC), which advises the U.S. Food and Drug Administration, on Tuesday recommended the agency authorize Pfizer’s Emergency Use Authorization COVID vaccine for children 5 to 11 years old.
The vote to recommend authorization of this vaccine, despite evidence that COVID does not pose a threat to young people, is causing even more unrest among those concerned with the safety of COVID vaccines in all age groups.
From mid-December 2020 through Oct. 15, 2021, the Vaccine Adverse Events Reporting System (VAERS) received 818,044 reports of injury following COVID vaccination, including 17,128 deaths.
“This vote by VRBPAC to put young children at risk of serious injury, and even death, is one more reason people need to stand up to tyranny, and let businesses and governments know we will no longer comply with reckless decisions that threaten the health of our children,” said CHD Executive Director Laura Bono.
CHD chapters, coalition partners and local community organizers are planning mass gatherings of people in peaceful noncompliance to take place in high-exposure areas in many cities and states. Visit “Worldwide Walkout” for locations and details. If you don’t see one for your area, reach out to others in your community to plan an event. Choose a location that is easy to get to and can be seen by many.
Once your date, location and time are in place, tell us your plans so we can help amplify your message.
CHD.TV will carry live coverage of the day’s events.
The Covid vaccine victims who will not be silenced

By Kathy Gyngell | TCW Defending Freedom | October 28, 2021
IT’S hard to tell sometimes whether the mainstream media is ingenuous and stupid, or disingenuous and malign. Their across-the-board, uncritical and almost adulatory reporting of Israel’s ‘first out of the traps’ mass vaccination programme prompts this observation. Check out Israel on Google: however many pages you search, you won’t find one critical article on the Israeli vaccination programme’s efficacy or ethics.
Had it been an unmitigated success there’d be no cause for surprise. But the truth is otherwise. Despite its early roll-out and achieving rates of vaccination in vulnerable groups upwards of 90 per cent, it’s no secret that over the summer the country experienced another wave of the virus that vaccination proved no barrier to. By early August the vaccinated (not the unvaccinated) in Israel were reported by a leading Israeli health official to account for 95 per cent of severe and 90 per cent of new hospitalisations for Covid-19. Significant ‘excess’ deaths in non-Covid vulnerable age groups also raised serious questions about the vaccines’ safety. In addition, this pre-print study (un-peer reviewed) published in August found natural immunity conferred longer lasting and stronger protection against the disease and hospitalisation caused by the Delta variant than the vaccine.
None of this evidence caused Israel’s government even a pause for thought. Au contraire the country was first off the mark again – this time with ‘booster’ third and fourth jabs all endorsed by the MSM with articles crediting it with powers its predecessors strangely lacked:
‘ . . . third doses are highly effective at preventing people from becoming infected with Delta, among those who are willing to be vaccinated,’ one enthusiastic professor opined. He said they not only dramatically reduce a person’s susceptibility to infection, they create a barrier to the onward transmission and spread of the virus.
The message from Israel for the UK is clear, or so the i newspaper would also have us believe. The booster is the way forward that our Government must follow with all speed.
It’s not just the politicos and the MSM mouthing the mantra. The Brookings Institute has opined tortuously that despite Israel’s ‘successful’ vaccination programme, its mounting cases make ‘the booster shot of the Covid-19 vaccine more necessary than ever’.
No academic looking for a living, breathing example of cognitive dissonance could find a better one.
This is the theory we’ve explained more than once in these pages. It accounts for the unaccountable – in this case for vaccine enthusiasts’ (do more) irrational response to the vaccines’ failure to deliver; for the ‘doubling down’ phenomenon – anything rather than acknowledge they may have got it wrong or placed too much reliance on what was always uncertain.
Faithful to the theory, they claim in face of negative data that their actions were successful in averting the worst, going further into denial with professions that had they not acted it would have been worse; thus setting up a canny ‘heads-we-win, tails-you-lose’ interpretation of things.
Festinger, the originator of this particular theory of human behaviour, explains it as ‘a psychic condition of tension and discomfort brought about by a palpable contradiction in an individual’s mental world’. It is an unease that must be eliminated: ‘Accordingly, something in the individual’s conscious awareness has to be invented, altered, ignored or denied.’
What is undoubtedly being denied by the authorities and their propagandists is the other side of the story – not only the inconvenient data but the human testimonies of those who have fallen foul of the experimental vaccine. This is the ultimate denial, keeping invisible the very real victims and survivors of the vaccines whose accounts are too threatening to the official narrative for the authorities to acknowledge.
Thank God then for the The Testimonies Project from Israel … to make sure their voices are heard, since they are not being heard in the Israeli media.
It’s a project that needs replicating worldwide to ensure that the millions of Covid vaccine victims are not airbrushed out of history and that there will be record of the human suffering that politicians can and must be brought to account for.
You can watch it here.
Trucking Alliance warns of looming “disaster” if vaccine passports are introduced
The proposals would not only be an attack on civil liberties, it would cause further disruption to supply chains.
By Ken Macon | Reclaim The Net | October 27, 2021
The Canadian Trucking Alliance (CTA) has warned of substantial “supply chain disruptions” if the US enforces vaccine passports at the border.
A few weeks ago, the US Department of Homeland Security announced a vaccine mandate for all international travel including truck drivers that will take effect in January. The announcement has been heavily criticized by cross-border truckers. According to Transportation Network, one executive in the Canadian trucking industry warned that the mandate would lead to a “disaster.”
This week, the CTA warned that the mandate would increase supply chain disruptions. Trucks facilitate about 70% of the $650 billion trade between Canada and the US. About 40,000 US drivers and 120,000 Canadian drivers operate in the cross-border trade between the two countries.
The CTA said that about 20% of drivers will stop cross-border operations once the vaccine mandate is enforced.
“CTA conservatively estimates that 20 percent of Canadian truck drivers crossing the border (22,000), and 40 percent of U.S. truck drivers (16,000), would almost immediately exit the Canada-US trade system should the vaccination mandate take effect in January 2022,” the organization said.
It called on both the US and Canadian governments to “reexamine appropriate mandate timelines for cross-border truck drivers.”
The group also argued that more time is needed to create a “seamless mutual system of identification for drivers” to avoid delays when drivers are showing proof of vaccination.
However, the Biden administration appears to be disregarding the warnings of “dire consequences” from leading truck organizations by proceeding with the vaccine passport plans.
The Leaky Vaccine Breakthrough Variant Is Here
By Dr. Joseph Mercola | October 26, 2021
It was only a matter of time before a vaccine-resistant strain of COVID-19 would surface, and that time has already come to pass. As reported by The Conservative Treehouse October 3, 2021:1
“What this study2 finds is exactly what vaccine developer Geert Vanden Bossche (Belgium) has been predicting. The predominance of antibody-resistant SARS-Cov-2 variants in vaccine breakthrough cases from the San Francisco Bay Area, California …
Dr. Vanden Bossche has been using Israeli data and showing3 how the widespread vaccination rates were creating pressure on the virus to mutate into variants with higher levels of contagion.
The unvaccinated group has been keeping the pressure down by defeating the virus and carrying natural immunity. However, as the unvaccinated population is increasingly made smaller, the pressure on the virus to mutate increases. Subsequently, these mutations stay at higher or more effective levels of infection.”
Vaccine-Evading Variants Are Emerging
The study, posted on the preprint server medRxiv, August 25, 2021, concluded that those who are fully “vaccinated” against COVID-19 are in fact more susceptible to COVID variant infections than unvaccinated people.
Vanden Bossche’s theory was that vaccine antibodies would suppress natural antibody responses, allowing variants to slip through, and this seems to be what’s happening. As explained by The Conservative Treehouse October 3, 2021:4
“Among vaccinated individuals, a COVID variant virus is not recognized by the specialized antibodies provided by the vaccine, and the natural antibodies have been programmed to stand down.”
According to the authors of the study:5
“Associations between vaccine breakthrough cases and infection by SARS coronavirus 2 (SARS-CoV-2) variants have remained largely unexplored. Here we analyzed SARS-CoV-2 whole-genome sequences and viral loads from 1,373 persons with COVID-19 from the San Francisco Bay Area from February 1 to June 30, 2021, of which 125 (9.1%) were vaccine breakthrough infections.
Fully vaccinated were more likely than unvaccinated persons to be infected by variants carrying mutations associated with decreased antibody neutralization (78% versus 48%), but not by those associated with increased infectivity (85% versus 77%) …
These findings suggest that vaccine breakthrough cases are preferentially caused by circulating antibody-resistant SARS-CoV-2 variants, and that symptomatic breakthrough infections may potentially transmit COVID-19 as efficiently as unvaccinated infections, regardless of the infecting lineage.”
“Be careful around vaccinated people, because they can carry a more resistant form of COVID-19,” The Conservative Treehouse warns, adding that the narrow protection you get from the COVID shot will inevitably necessitate a booster shot for each emerging new variant that is resistant to the shots.
UK Data Show Increased COVID Mortality Among Fully Vaxxed
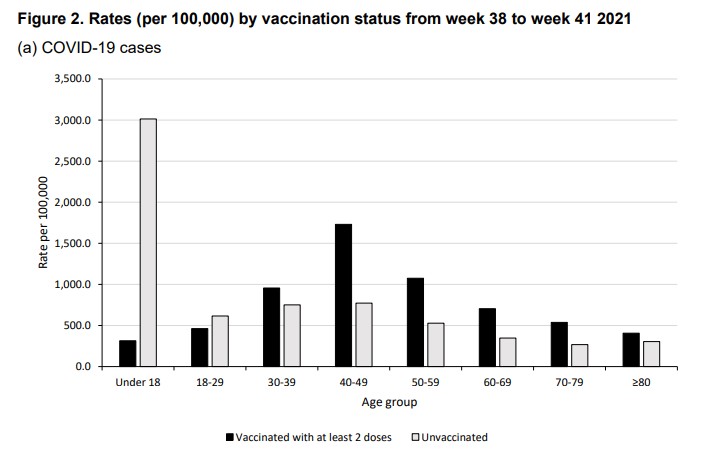
British data also raise serious questions about the wisdom of this injection campaign. In its Technical Briefing 23,6 published September 17, 2021, Public Health England reveals data showing the COVID death toll is actually higher among the fully vaccinated compared to the unvaccinated.
Between February 1, 2021, and September 12, 2021, 157,400 fully vaccinated patients (26.52% of total cases) were diagnosed with a Delta variant. Among the unvaccinated, there were 257,357 Delta variant cases (43.36% of total cases).
However, while Delta infections were far more prevalent among the unvaccinated, these patients also had better outcomes. In all, 63.5% of those who died from COVID-19 within 28 days of a positive test were fully vaccinated (1,613 compared to 722 in the unvaccinated group).
More Signs of Antibody-Dependent Enhancement
In a letter to the editor of the Journal of Infection,7 published August 9, 2021, three researchers point out that “infection-enhancing anti-SARS-CoV-2 antibodies recognize both the original Wuhan/D614G strain and Delta variants,” which suggests antibody-dependent enhancement (ADE) is emerging. According to the authors:8
“Antibody dependent enhancement (ADE) of infection is a safety concern for vaccine strategies. In a recent publication, Li et al. (Cell 184 :4203–4219, 2021) have reported that infection-enhancing antibodies directed against the N-terminal domain (NTD) of the SARS-CoV-2 spike protein facilitate virus infection in vitro, but not in vivo.
However, this study was performed with the original Wuhan/D614G strain. Since the Covid-19 pandemic is now dominated with Delta variants, we analyzed the interaction of facilitating antibodies with the NTD of these variants … [W]e show that enhancing antibodies have a higher affinity for Delta variants than for Wuhan/D614G NTDs …
As the NTD is also targeted by neutralizing antibodies, our data suggest that the balance between neutralizing and facilitating antibodies in vaccinated individuals is in favor of neutralization for the original Wuhan/D614G strain.
However, in the case of the Delta variant, neutralizing antibodies have a decreased affinity for the spike protein, whereas facilitating antibodies display a strikingly increased affinity. Thus, ADE may be a concern for people receiving vaccines based on the original Wuhan strain spike sequence (either mRNA or viral vectors).”
As noted by independent journalist Sharyl Attkisson,9 “Despite the fact that multiple medical authorities predicted, told us, and hoped, ADE would not impact Covid-19 vaccines, data from the study indicates it has done just that.”
Antibody Levels Decrease After Second Dose
While you’re not considered “fully vaccinated” until 14 days after your first dose of Janssen’s or AstraZeneca’s shot, or second dose of Moderna’s or Pfizer’s, a recent Israeli study found antibody levels actually decrease after the second dose of Pfizer’s COVID shot. The findings were reported by The Jerusalem Post, October 7, 2021:10
“Antibody levels decrease rapidly after two doses of the Pfizer coronavirus vaccine, a study11 by researchers at the Sheba Medical Center published … in the New England Journal of Medicine …
The research also showed the probability that different groups of individuals — based on age and general health status — will find themselves below a certain antibody threshold after a period of six months.”
In all, 4,868 staff members at the Sheba Medical Center participated in the study,12 undergoing monthly serological tests to measure their antibodies for up to six months after their second Pfizer shot.
Everyone, regardless of age or gender, saw a rapid decline in their antibodies after the second dose. IgG antibodies — which are part of your humoral immune response — decreased at a consistent rate over time, whereas the neutralizing antibodies rapidly decreased during the first three months, and then slowed down thereafter. According to the authors:13
“Although IgG antibody levels were highly correlated with neutralizing antibody titers (Spearman’s rank correlation between 0.68 and 0.75), the regression relationship between the IgG and neutralizing antibody levels depended on the time since receipt of the second vaccine dose …
The highest titers after the receipt of the second vaccine dose (peak) were observed during days 4 through 30, so this was defined as the peak period.
The expected geometric mean titer (GMT) for IgG for the peak period, expressed as a sample-to-cutoff ratio, was 29.3. A substantial reduction in the IgG level each month, which culminated in a decrease by a factor of 18.3 after 6 months, was observed.
Neutralizing antibody titers also decreased significantly, with a decrease by a factor of 3.9 from the peak to the end of study period 2, but the decrease from the start of period 3 onward was much slower, with an overall decrease by a factor of 1.2 during periods 3 through 6. The GMT of neutralizing antibody, expressed as a 50% neutralization titer, was 557.1 in the peak period and decreased to 119.4 in period 6 …
Six months after receipt of the second dose, neutralizing antibody titers were substantially lower among men than among women, lower among persons 65 years of age or older than among those 18 to less than 45 years of age, and lower among participants with immunosuppression than among those without immunosuppression.”
COVID-19 Unrelated to Jab in 68 Countries, 2,947 US Counties
The Israeli findings above can help explain the findings of a study14 published September 30, 2021, in the European Journal of Epidemiology, which found no relationship between COVID-19 cases and levels of vaccination in 68 countries worldwide and 2,947 counties in the U.S. If anything, areas with high vaccination rates had slightly higher incidences of COVID-19. According to the authors:15
“[T]he trend line suggests a marginally positive association such that countries with higher percentage of population fully vaccinated have higher COVID-19 cases per 1 million people.”
Iceland and Portugal, for example, where more than 75% of their populations are fully vaccinated, had more COVID-19 cases per 1 million people than Vietnam and South Africa, where only about 10% of the populations are fully vaccinated.16
Data from U.S. counties showed the same thing. New COVID-19 cases per 100,000 people were “largely similar,” regardless of the percentage of a state’s population that was fully vaccinated.
“There … appears to be no significant signaling of COVID-19 cases decreasing with higher percentages of population fully vaccinated,” the authors wrote.17 Notably, out of the five U.S. counties with the highest vaccination rates — ranging from 84.3% to 99.9% fully vaccinated — four of them were on the U.S. Centers for Disease Control and Prevention’s “high transmission” list. Meanwhile, 26.3% of the 57 counties with “low transmission” have vaccination rates below 20%.
The study even accounted for a one-month lag time that could occur among the fully vaccinated, since it’s said that it takes two weeks after the final dose for “full immunity” to occur. Still, “no discernable association between COVID-19 cases and levels of fully vaccinated” was observed.18
Key Reasons Why Reliance on Jabs Should Be Reexamined
The study summed up several reasons why the “sole reliance on vaccination as a primary strategy to mitigate COVID-19” should be reevaluated. For starters, the jab’s effectiveness is rapidly waning.
“A substantial decline in immunity from mRNA vaccines six months’ post immunization has … been reported,” the researchers noted, adding that even severe hospitalization and death from COVID-19, which the jabs claim to protect against, have increased from 0.01% to 9% and 0% to 15.1%, respectively, among the fully vaccinated from January 2021 to May 2021.19
If the jabs work as advertised, why haven’t these rates continued to rise instead of fall? “It is also emerging,” the researchers noted, “that immunity derived from the Pfizer-BioNTech vaccine may not be as strong as immunity acquired through recovery from the COVID-19 virus.”20
For instance, a retrospective observational study published August 25, 2021, revealed that natural immunity is superior to immunity from COVID-19 jabs. According to the authors:21
“This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity.”
Reinfection Is Very Rare
The fact is, while breakthrough cases continue among those who have gotten one or more COVID-19 injections, it’s extremely rare to get COVID-19 after you’ve recovered from the infection. How rare? Researchers from Ireland conducted a systematic review including 615,777 people who had recovered from COVID-19, with a maximum duration of follow-up of more than 10 months.22
“Reinfection was an uncommon event,” they noted, “with no study reporting an increase in the risk of reinfection over time.” The absolute reinfection rate ranged from 0% to 1.1%, while the median reinfection rate was just 0.27%.23,24,25
Another study revealed similarly reassuring results. It followed 43,044 SARS-CoV-2 antibody-positive people for up to 35 weeks, and only 0.7% were reinfected. When genome sequencing was applied to estimate population-level risk of reinfection, the risk was estimated at 0.1%.26
There was no indication of waning immunity over seven months of follow-up, unlike with the COVID-19 injection, which led the researchers to conclude that “Reinfection is rare. Natural infection appears to elicit strong protection against reinfection with an efficacy >90% for at least seven months.”27
All Risk for No Reward?
The purpose of informed consent is to give people all of the data related to a medical procedure so they can make an educated decision before consenting. In the case of COVID-19 injections, such data initially weren’t available, given their emergency authorization, and as concerning side effects became apparent, attempts to share them publicly were suppressed.
In August 2021, a large study from Israel28 revealed that the Pfizer COVID-19 mRNA jab is associated with a threefold increased risk of myocarditis,29 leading to the condition at a rate of one to five events per 100,000 persons.30 Other elevated risks were also identified following the COVID-19 jab, including lymphadenopathy (swollen lymph nodes), appendicitis and herpes zoster infection.31
Dr. Peter McCullough, an internist, cardiologist and epidemiologist, is among those who have warned that COVID-19 injections are not only failing but putting lives at risk.32
According to McCullough, by January 22, 2021, there had been 186 deaths reported to the Vaccine Adverse Event Reporting System (VAERS) database following COVID-19 injection — more than enough to reach the mortality signal of concern to stop the program.
“With a program this size, anything over 150 deaths would be an alarm signal,” he said. The U.S. “hit 186 deaths with only 27 million Americans jabbed.” McCullough believes if the proper safety boards had been in place, the COVID-19 jab program would have been shut down in February 2021 based on safety and risk of death.33
Now, with data showing no difference in rates of COVID-19 cases among the vaxxed and unvaxxed, it appears more and more likely that the injections have a high level of risk with very little reward, especially among certain populations, like youth.
Mass Vaccination Drives Mutations
It’s well-known that if you put living organisms like bacteria or viruses under pressure, via antibiotics, antibodies or chemotherapeutics, for example, but don’t kill them off completely, you can inadvertently encourage their mutation into more virulent strains. Those that escape your immune system end up surviving and selecting mutations to ensure their further survival.
Many have warned about immune escape due to the pressure being placed upon the COVID-19 virus during mass vaccination,34 and according to one mathematical model,35 a worst-case scenario can develop when a large percentage of a population is vaccinated but viral transmission remains high, such as it is now. This is a prime scenario for the development of resistant mutant strains.36
At this point, COVID-19 injection failures and serious jab-related health risks are both apparent. We now also have data showing that having a high vaccination rate does nothing to lower COVID-19 incidence.
It might actually increase it slightly, as we’re seeing in India. In Kerala, India, which boasts a 93% vaccination rate, more than half of all new COVID cases are fully vaccinated, as are 57% of COVID-related deaths.37 With all data pointing in the same direction, it’s clear that COVID shots aren’t the answer. As noted in the European of Journal of Epidemiology :38
“Stigmatizing populations can do more harm than good. Importantly, other non-pharmacological prevention efforts (e.g., the importance of basic public health hygiene with regards to maintaining safe distance or handwashing, promoting better frequent and cheaper forms of testing) needs to be renewed in order to strike the balance of learning to live with COVID-19 in the same manner we continue to live a 100 years later with various seasonal alterations of the 1918 Influenza virus.”
If You’re ‘Vaccinated’ You May Be High-Risk for COVID
As predicted from the very beginning of the mass vaccination campaign, we’re now starting to see evidence of ADE, which makes people more prone to serious illness rather than less.
Even if your risk for ADE is small (and we have no data on prevalence as of yet), the data we do have suggest the shots aren’t ending outbreaks, and indeed can’t, end them, as it’s the vaccinated who are facilitating the emergence of vaccine-evading variants. The real answer is natural herd immunity, as natural immunity protects against most variants and not just one.
To be on the safe side, I recommend considering yourself “high-risk” for severe COVID if you’ve received one or more shots, and implement known effective treatment at the first sign of a respiratory infection.
Options include the Zelenko protocol,39 the MATH+ protocols40 and nebulized hydrogen peroxide, as detailed in Dr. David Brownstein’s case paper.41 Whichever treatment protocol you use, make sure you begin treatment as soon as possible, ideally at first onset of symptoms.
Sources and References
- 1, 4 Conservative Treehouse October 3, 2021
- 2, 5 medRxiv August 25, 2021, DOI: 10.1101/2021.08.19.21262139
- 3 YouTube Vejon Health Vanden Bosche and Robert Malone interview
- 6 Public Health England Technical Briefing 23, September 17, 2021
- 7, 8 Journal of Infection Letter to the Editor August 9, 2021
- 9 Sharyl Attkisson August 17, 2021
- 10 The Jerusalem Post October 7, 2021
- 11, 12, 13 NEJM October 6, 2021 DOI: 10.1056/NEJMoa2114583
- 14, 15, 16, 17, 18, 19, 20, 38 European Journal of Epidemiology September 30, 2021
- 21 medRxiv August 25, 2021
- 22, 23 Rev Med Virol. 2021;e2260
- 24 The Blaze July 14, 2021
- 25 News Rescue July 15, 2021
- 26, 27 medRxiv January 15, 2021
- 28, 30, 31 The New England Journal of Medicine August 25, 2021
- 29 MedPage Today August 25, 2021
- 32 BitChute, Episode 20 of Perspectives on the Pandemic: The Dangers of the Injections, August 26, 2021
- 33, 34 BitChute, Episode 20 of Perspectives on the Pandemic, ‘This Interview Could Save Your Life’ Part Two: The Dangers of the Injections, August 26, 2021
- 35, 36 Scientific Reports July 30, 2021
- 37 Onmanorama.com October 12, 2021
- 39 Zelenko protocol
- 40 Covid19criticalcare.com
- 41 Science, Public Health Policy and The Law July 2020; 1: 4-22 (PDF)
Pressure Mounts on the UKHSA to Stop Publishing Data Showing Infection Rates Higher in the Vaccinated
By Will Jones | The Daily Sceptic | October 27, 2021
The Prime Minister may have acknowledged reality and stated that being double vaccinated “doesn’t protect you against catching the disease, and it doesn’t protect you against passing it on” but others appear to remain in denial.
On Sunday I asked whether now that the PM had let the cat out of the bag the media would start reporting properly on the UKHSA data showing higher infection rates in the vaccinated than the unvaccinated. It appears the answer is no, at least if the Times‘s Tom Whipple is any indication.
In a typically mean-spirited piece – in which anyone who doesn’t agree with his favoured scientist of the hour is smeared as a conspiracy theorist and purveyor of misinformation – Whipple quotes Cambridge statistician Professor David Spiegelhalter, who heaps opprobrium on the U.K. Health Security Agency (the successor to PHE) for daring to publish data that contradicts the official vaccine narrative. Spiegelhalter says of the UKHSA vaccine surveillance reports:
This presentation of statistics is deeply untrustworthy and completely unacceptable… I cannot believe that UKHSA is putting out graphics showing higher infection rates in vaccinated than unvaccinated groups, when this is simply an artefact due to using clearly inappropriate estimates of the population. This has been repeatedly pointed out to them, and yet they continue to provide material for conspiracy theorists around the world.
This is the graphic he is presumably referring to.
If Professor Spiegelhalter has a source for his claim that higher infection rates in the vaccinated are “simply an artefact” of erroneous population estimates then he doesn’t provide it.
Whipple says the data has been “seized upon around the world”.
The numbers have been promoted by members of HART, a U.K. group that publishes vaccine misinformation. They have also been quoted on the Joe Rogan Experience podcast in the US, which reaches 11 million people.
Appearing on that podcast, Alex Berenson, a U.S. journalist now banned from Twitter, specifically referenced the source to show it was reliable.
The UKHSA is adamant that it is doing nothing wrong. The Times quotes Dr Mary Ramsay, head of immunisation at the UKHSA, explaining: “Immunisation information systems like NIMS are the internationally recognised gold standard for measuring vaccine uptake.”
So Professor Spiegelhalter thinks that the gold standard gives “clearly inappropriate estimates of the population”, and using it is “deeply untrustworthy and completely unacceptable”? That may be his view, but the UKHSA can hardly be criticised for following the recognised standards for its work.
A more measured criticism is provided by Colin Angus, a statistician from the University of Sheffield, who the Times quotes saying that using NIMS data makes sense but the “huge uncertainty” in the population estimates should be clearer.
Whipple, however, goes further and claims that “using population data from other official sources shows, instead, shows that the protection of vaccines continues”. Yet he does not provide those sources or go into any detail about how they back up his claim.
For now, the UKHSA is defending its report (we’ll see how long it holds out for). But even so, Dr Ramsay is adamant that the report rules out using the data to estimate vaccine effectiveness: “The report clearly explains that the vaccination status of cases, inpatients and deaths should not be used to assess vaccine effectiveness and there is a high risk of misinterpreting this data because of differences in risk, behaviour and testing in the vaccinated and unvaccinated populations.”
This defence somewhat misses Professor Spiegelhalter’s criticism about population estimates. But it’s also misleading in that the report doesn’t “clearly” explain that its data “should not be used to assess vaccine effectiveness”. What it says is it is “not the most appropriate method to assess vaccine effectiveness and there is a high risk of misinterpretation”. But, as explained before, using population-based data on infection rates in vaccinated and unvaccinated is certainly a valid method of estimating unadjusted vaccine effectiveness, which is defined as the reduced infection rate in the vaccinated versus the unvaccinated. While a complete study would then adjust those raw figures for potential systemic biases (with varying degrees of success), we shouldn’t necessarily expect those adjustments to be large or change the picture radically. Indeed, when a population-based study from California (which showed vaccine effectiveness against infection declining fast), carried out these adjustments the figures barely changed at all.
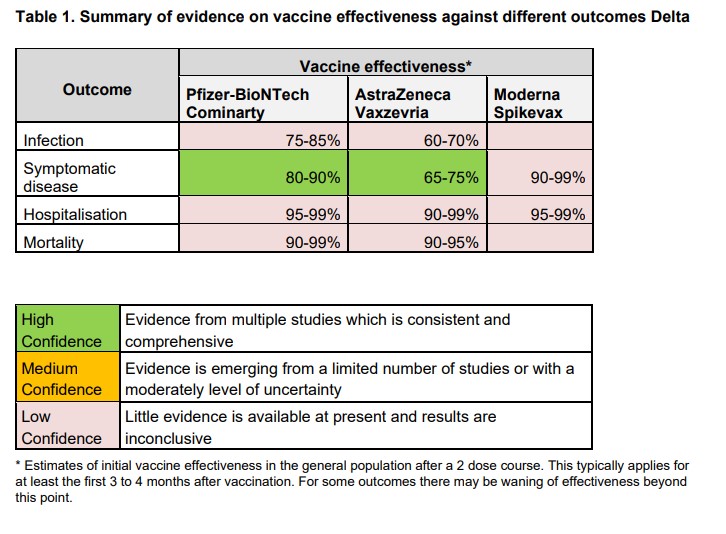
The UKHSA report adds that: “Vaccine effectiveness has been formally estimated from a number of different sources and is described earlier in this report.” In fact, though, most of those estimates are reported as low confidence (see below), which means: “Little evidence is available at present and results are inconclusive.” While it claims high confidence for its estimates against symptomatic disease, a footnote explains that this only holds for 12-16 weeks: “This typically applies for at least the first three to four months after vaccination. For some outcomes there may be waning of effectiveness beyond this point.”
It is precisely this “waning of effectiveness” that the latest real-world data is giving us insight into. Rather than trying to discredit that data and those who report it by throwing around general, unquantified criticisms, scientists and academics like Professor Spiegelhalter should be redoubling efforts to provide constructive analysis to get to the bottom of what’s really going on with the vaccines. If there are issues with the population estimates then those need to be looked at, and if there are biases that need adjusting for then those need to be quantified. But do, please, get on with it – and lay off the smearing of those who raise the questions.
FDA Panel Backs Pfizer Shot For Kids: “We’re never going to learn about how safe this vaccine is unless we start giving it”
By Chris Menahan | InformationLiberation | October 26, 2021
An FDA vaccine advisory panel on Tuesday voted unanimously 17-0 in favor shooting up kids aged 5-11 with Pfizer’s experimental mRNA injection with panelist Dr Eric Rubin stating, “we’re never going to learn about how safe this vaccine is unless we start giving it.”
Full context:
https://twitter.com/politicalwilli/status/1453082309201117199?ref_src=twsrc%5Etfw%7Ctwcamp%5Etweetembed%7Ctwterm%5E1453082309201117199%7Ctwgr%5E%7Ctwcon%5Es1_&ref_url=https%3A%2F%2Fwww.informationliberation.com%2F%3Fid%3D62628
“We’re never going to learn about how safe this vaccine is unless we start giving it,” Dr Rubin said, urging other panelists to vote for it. “That’s just the way it goes.”
The panel voted in favor of experimenting on tens of millions of helpless children with zero long-term data on side effects because 94 children between 5 and 11 have died with COVID-19 (they claimed “of”) and “all have names. All of them had mothers,” to quote the emotional gobbledegook uttered by panelist Patrick S. Moore.
From The Washington Post :
“To me, it seems that it is a hard decision but a clear one,” said Patrick S. Moore, a University of Pittsburgh microbiologist and committee member. He noted that 94 children between 5 and 11 have died of covid-19, and “all have names. All of them had mothers.”
As the WSJ reported:
Members of the FDA’s vaccine-advisory panel supported Moderna’s booster dose even though the evidence for it was from a small study and had mixed results.
“It’s more a gut feeling rather than based on really truly serious data,” said Patrick Moore, a member of the committee and a professor of molecular genetics and biochemistry at the University of Pittsburgh School of Medicine. “The data itself is not strong, but it is certainly going in the direction that is supportive of this vote.”
This is how they “follow the science.”
Featured Video

Fear Is the Mind Killer
or go to
Aletho News Archives – Video-Images
From the Archives
Alarmist climate science as a textbook example of groupthink
By Paul MacRae | May 1, 2012
A while ago, I received an email from a friend who asked:
How can many, many respected, competitive, independent science folks be so wrong about [global warming] (if your [skeptical] premise is correct). I don’t think it could be a conspiracy, or incompetence. … Has there ever been another case when so many ‘leading’ scientific minds got it so wrong?
The answer to the second part of my friend’s question—“Has there ever been another case where so many ‘leading’ scientific minds got it so wrong?”—is easy. Yes, there are many such cases, both within and outside climate science. In fact, the graveyard of science is littered with the bones of theories that were once thought “certain” (e.g., that the continents can’t “drift,” that Newton’s laws were immutable, and hundreds if not thousands of others).
Science progresses by the overturning of theories once thought “certain.” … continue
Blog Roll
 Aletho News
Aletho News- US blockade crumbles as Iran turns to overland routes
- Hidden costs of US Iran war push total far beyond $25bn Pentagon claim
- Iran Will Respond With Long-Term Strikes to US Attack, Even If It Is Short-Term – IRGC
- Fear Is the Mind Killer
- Israeli strikes kill 10 in southern Lebanon, including 3 rescue workers
- Israeli military ‘failed on all fronts’: Poll
- US at a crossroads: Iran’s firm positions leave Trump no option but to capitulate
- Iran signals decisive response to end US maritime bullying, piracy
- Trump eager for off-ramp in war on Iran, but Netanyahu has him trapped: Former official
- Trump’s ‘Golden Dome’ offers ‘limited’ shield against ballistic missiles: Defense official
- If Americans Knew
- How Tony Dokoupil Became the Face of ‘Zionist Fanatic’ Bari Weiss’s CBS
- Far Right Israeli Settler Movement Enters Syria in a Push for “Greater Israel”
- ‘People Have the Right to Be Buried’: In Gaza, Thousands of Palestinians Remain Trapped Under Rubble
- Born during Israel’s genocide: Gaza’s child survivors bear the scars of war
- Who are the women and girls behind Gaza war’s horrific casualty toll?
- Beloved Gaza doctor detained “indefinitely” without charge – Daily Update
- By Week’s End, Trump’s War Will Be Plainly Illegal
- CBS News Reportedly Ousts London Bureau Chief Over Differences With Bari Weiss Over Gaza Coverage
- State Department Says US Is in Conflict With Iran ‘At the Request’ of Israel
- What ceasefire? Israel won’t stop killing in Gaza, Lebanon – Daily Update
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
