L.A. City Council unveiled its new plan to harass its unvaccinated workers with bi-weekly COVID tests to paid for by employees.
Los Angeles City Council has announced that its police officers, firefighters and other city workers who have not yet received their experimental COVID-19 pharmaceutical gene therapy injections – will be ‘given more time’ to get their jabs under the new plan approved by the City Council.
City officials hope that a constant campaign of harassment and financial penalties waged against its workers will encourage any remaining unvaccinated employees to submit to the corporate jabs.
City workers who haven’t given up their constitutional right to bodily autonomy by Dec. 18th will face “corrective action” and punishment by the city, including legalized targeted harassment by city officials, according to their plan released yesterday.
Until then, the city’s unvaccinated workers will be required to get tested for COVID-19 twice per week, on their own time, and at a cost of $65 for each test – deducted straight from their paychecks.
California official will be studying the results of this program closely, no doubt with plans to replicate it across other sectors of society, and as a coercive instrument for businesses as well.
To review: We have now had ten months of mass vaccination against SARS-CoV-2. Nearly 7 billion doses have been administered worldwide. This unprecedented campaign has not eradicated Corona; it has not even suppressed infections. Instead, case statistics have ballooned almost everywhere. While the vaccinated appear to enjoy some protection against severe outcomes, skyrocketing transmission means most countries have seen little benefit, on balance, from their universal vaccination campaigns. The most pressing question has become, simply: What is going on?
I’ve explored a few different possibilities. First, there seems to be a Marek Effect at work. We might imagine that all viruses have an optimal level of population-wide virulence – an advantageous degree of aggression at which they can spread effectively, while not driving their hosts underground too soon. Certain Delta sub-strains, previously punished for their excessive aggression in unvaccinated populations, have likely been favoured by the vaccines, which reduce symptoms in the vaccinated without preventing infection for more than a few months. Our vaccines reduced the average virulence of SARS-2, and the virus adapted to reattain the prior, optimal balance.
But the virus and its interactions with human hosts constitute a complex system. In such systems, it is very unlikely that any effect can be put down to a single cause. The Public Health England data provide powerful reasons to suspect that the vaccines may be compromising immunity to SARS-2 via Original Antigenic Sin. This is not a crazy internet fantasy, but a well-observed limitation of human immunity. It is the primary reason that respiratory viruses like influenza return again and again. Despite multiple reinfections across the whole population, we are never quite immune to the flu, because its strategy is to exploit the way our immune systems learn.
The mechanisms of Original Antigenic Sin are not fully understood, but we have a rough idea of what might be happening. When a virus infects your body for the first time, your naive memory B cells imprint on specific virus proteins, or antigens, presented to them. These B cells then become either memory B cells or plasma cells. Forever after, they specialise in producing antibodies against those specific antigens. When a slightly mutated form of the virus arrives, these memory B-cells begin pouring forth the antibodies they learned to produce during the first infection. These antibodies bind to multiple epitopes on the virus particles, and in the process they give the slower-moving naive B-cells little chance to learn about any new, mutant virus features.
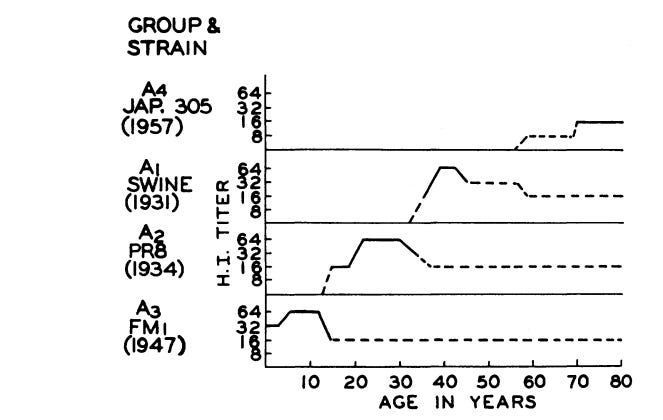
Original Antigenic Sin was most influentially described by Thomas Francis in 1960. He noted that, regardless of whatever influenza A strains were in circulation, subjects tended to have dominant antibody responses to the strains that were current in their early childhood:
The antibody of childhood is largely a response to … the virus causing the first Type A influenza infection of the lifetime. As the group grows older and subsequent infections take place, antibodies to additional families of virus are acquired. But … the antibody which is first established continues to characterize that cohort of the population throughout its life. The antibody forming mechanisms have been highly conditioned by the first stimulus, so that later infections with strains of the same type successively enhance the original antibody to maintain it at the highest level at all times in that age group. The imprint established by the original virus infection governs the antibody response thereafter. This we have called the doctrine of original antigenic sin.
An important consequence of this childhood conditioning, is that different age cohorts within the population have overlapping or layered immunity to different influenza strains. This is an important if subtle aspect of our population-wide immunity to influenza A. It looks like this:
As older cohorts die, their immunity to older strains dies with them. These old strains, long suppressed, are then positioned to return, for very few human immune systems remember them any longer. Francis believed this was the mechanism underlying periodic cycles of pandemic influenza. The 1957 influenza pandemic, for example, featured a strain of flu against which only the oldest cohorts – those in their 70s – had specific antibodies. As these “immunological veterans” disappeared, this older, long-suppressed type of influenza was free to return and cause another pandemic event.
In conclusion, Francis proposed that optimised influenza vaccines might be administered to children before their first infection. He envisioned vaccines designed to confer immunity against “known or anticipated recurrent strains” and hoped that “In this manner the original sin of infection could be replaced by an initial blessing of induced immunity.”
Strategic vaccination conferring immunity against likely future strains is of course exactly the opposite of our current efforts to give every last living human multiple vaccinations against an extinct strain of SARS-2.
*
The existence of Original Antigenic Sin has been confirmed by generations of research, and the literature is full of curious findings. A major reason flu shots don’t work, for example, is that they are powerless to redirect adult immune systems against novel influenza strains. Most people who get flu shots are adults, with immune systems long since primed by childhood infection. Hence this old Lancet case study of influenza outbreaks among boys at Christ’s Hospital in Sussex in the 1970s:
In each outbreak, the protective effect of inactivated influenza-A vaccine was limited to those boys, not already immune, who were vaccinated for the first time with the most up-to-date strain. Revaccination with the same strain did not increase the degree of protection, and revaccination with a later strain did not afford protection against subsequent challenge.
The flu vaccines, in other words, work great if you’ve never had the flu before. Otherwise they don’t do anything.
And consider these remarks, from a 2005 article in Nature Medicine:
It is often difficult to further increase antibody levels, specificity and the quality of the immune response in individuals who have been repeatedly immunized through either vaccination or recurrent exposure to infectious agents or cross-reacting microbial antigens. This has been a particular concern for aging adults in the context of the antigenic drift of influenza virus, in view of their annual exposure to antigens of new but related influenza variants through either infection or vaccination. After exposure to a new but cross-reacting antigenic variant, such individuals may respond by producing antibodies that are primarily directed at antigens characterizing influenza viruses encountered during earlier epidemics.
The authors go on to write that the “impact” of Original Antigenic Sin “on protection is far from established,” noting earlier research showing substantial all-cause mortality reductions from flu shots. Later work, though, has shown that the mortality reduction of influenza vaccines is largely an illusion of selection effects. For a variety of reasons, those most likely to die of influenza are far less likely than healthier groups to be vaccinated.
Original Antigenic Sin has been famously implicated in dengue fever. This is considered to be an extreme case of the phenomenon, with “considerable bearing on vaccine strategies.” Here the conclusions are ominous and full of implications for our own situation:
Once a response has been established, it is unlikely that repeat boosting will be able to change its scope, meaning that balanced responses against the four virus serotypes will need to be established with the first vaccine dose.
The danger is that immunity to one strain alone may lead to permanently impaired immune response to the three other serotypes, causing worse and longer illness.
*
Influenza had been infecting humans for generations before anybody came up with the notion of influenza vaccines. Despite the efforts of public health authorities everywhere, most people catch the flu before they are ever vaccinated, and so flu shots have little opportunity to undermine population-wide immunity to influenza A.
The complex system constituted by SARS-CoV-2 and its interactions with the human immune system, on the other hand, remains barely understood. In chasing an empty fantasy of herd immunity, authorities are denying human populations everywhere the opportunity to develop the layered, population-wide resistance against successive SARS-2 strains that is the foundation of our immunity against other respiratory viruses. Aside from the minority that have managed to recover from natural infection before the vaccinators got to them, most humans will have their crucial, primary immune response conditioned by the spike protein of SARS-2 in its vintage 2020 configuration.
It is a near certainty that this immunity will attenuate antibody responses to the spike protein of current and future variants, forever. Mutant spike proteins will increasingly escape vaccine-conferred immunity, and breakthrough infections will elicit only partial response to the new epitopes. Insofar as the data also suggest that our vaccines will attenuate immunity to other virus proteins beyond spike, mass vaccination will lead to ever more volatile waves of infection – in exchange for limited and fading protection against severe outcomes.
The most dangerous thing to do, at this point, would be to vaccinate children. The virus is not a threat to them, and if they are infected by the new forms of SARS-2 that are sure to emerge every winter, we will begin to establish – through them and the as yet unvaccinated – the layered immunity that is the only way of coming to terms with SARS-2 in the longer term. As long as the vaccinators are permitted to continue their radical and increasingly insane campaign, though, nothing will improve. Indeed, their policies threaten to bring about a semi-permanent pandemic state for generations to come.
Mortality data tells us information about deaths in Australia and is usually released every 6 weeks. For an unexplained reason, the latest data is over 15 weeks overdue.
As Government becomes more and more powerful, anyone who challenges the current policies is smeared and censored. The legacy media happily parrots the propaganda, afraid of losing government funding.
Unreliable, intermittent wind and solar energy will leave Australian families sitting in the dark without coal-fired power to back them. ‘Renewables’ only farm taxpayer money, not energy.
Where to even begin with the FDA’s preposterous risk-benefit analysis of Pfizer’s mRNA COVID-19 “vaccine” in children ages 5 to 11?
Let’s start with my bona fides. I have a year of undergraduate statistics at one of the best liberal arts colleges in America (Swarthmore). I have a year of graduate statistics at the masters program rated #1 for policy analysis (UC Berkeley). And I have a Ph.D. in political economy from one of the top universities in the world (University of Sydney). My research focus is on corruption in the pharmaceutical industry so I’ve read scientific studies in connection with vaccines nearly every day for 5 years. Earlier in my career I worked professionally tearing apart shoddy cost-benefit analyses prepared by corporations that were trying to get tax breaks, contracts, and other concessions from local government. Suffice it to say I’ve thought a lot about risk-benefit analysis and I’m better equipped than most to read one of these documents.
The FDA’s risk-benefit analysis in connection with Pfizer’s Emergency Use Authorization (EUA) application to inject children ages 5 to 11 with their COVID-19 vaccine is one of the shoddiest documents I’ve ever seen.
Let’s take it from the top:
🚩 COVID-19 rates in children ages 5 to 11 are so low that there were ZERO cases of severe COVID-19 and ZERO cases of death from COVID in either the treatment (n= 1,518) or control group (n= 750). So any claims you see in the press about the Pfizer vaccine being “90% effective” in children are meaningless because they are referring to mild cases from which children usually recover quickly (and then have robust broad spectrum immunity). So there is literally no emergency in this population for which one could apply for Emergency Use Authorization. Pfizer’s application should be dead on arrival if the FDA actually followed the science and their own rules. We will return to this topic below.
🚩 Pfizer’s clinical trial in kids was intentionally undersized to hide harms. This is a well known trick of the pharmaceutical industry. The FDA even called them out on it earlier this summer and asked Pfizer to expand the trial and Pfizer just ignored them because they can. (Pfizer fudged it by importing data from a different study but this other study only monitored adverse outcomes for 17 days so if anything the new data polluted rather than clarified outcomes). To put it simply, if the rate of particular adverse outcome in kids as a result of this shot is 1 in 5,000 and the trial only enrolls 1,518 in the treatment group then one is unlikely to spot this particular harm in the clinical trial. Voilà “Safe & Effective(TM)”.
🚩 Pfizer only enrolled “participants 5-11 years of age without evidence of prior SARS-CoV-2 infection.” Does the Pfizer mRNA shot wipe out natural immunity and leave one worse-off than doing nothing as shown in this data from the British government? Pfizer has no idea because children with prior SARS-CoV-2 infection were excluded from this trial. This was by design. Toxic polluters have learned to not ask questions that they do not want the answers to, lest they wind up staring at their own smoking gun in a future court case.
“What the British are saying is they are now finding the vaccine interferes with your body’s innate ability after infection to produce antibodies against not just the spike protein but other pieces of the virus. Specifically, vaccinated people don’t seem to be producing antibodies to the nucleocapsid protein, the shell of the virus, which are a crucial part of the response in unvaccinated people. This means vaccinated people will be far more vulnerable to mutations in the spike protein EVEN AFTER THEY HAVE BEEN INFECTED AND RECOVERED ONCE (or more than once, probably). It also means the virus is likely to select for mutations that go in exactly that direction because those will essentially give it an enormous vulnerable population to infect. And it probably is still more evidence the vaccines may interfere with the development of robust long-term immunity post-infection.”
🚩 Did Pfizer LOSE CONTACT with 4.9% of their clinical trial participants? The FDA risk-benefit document states: “Among Cohort 1 participants, 95.1% had safety follow-up ≥2 months after Dose 2 at the time of the September 6, 2021 data cutoff.” So what happened with those 4.9% who did not have safety follow-up 2 months after Dose 2? Were they in the treatment or control group? We have no idea because Pfizer isn’t saying. Given the small size of the trial, failing to follow up with 4.9% of the participants potentially skews the results.
🚩 The follow up period was intentionally too short. This is another well-know trick of the pharmaceutical industry designed to hide harms. Cohort 1 appears to have been followed for 2 months, cohort 2 was only monitored for adverse events for 17 days. Many harms from vaccines including cancer and autoimmune disorders take much longer to show up. As the old saying goes, “you can have it quick or you can have it done right, but you cannot have both.” Pfizer chose quick.
🚩 The risk-benefit model created by the FDA only looks at one known harm from the Pfizer mRNA shot — myocarditis. But we know that the real world harms from the Pfizer mRNA shot go well beyond myocarditis and include anaphylaxis, Bell’s Palsy, heart attack, thrombocytopenia/ low platelet, permanent disability, shingles, and Guillain-Barré Syndrome (GBS) to name a few. Cancer, diabetes, endocrine disruption, and autoimmune disorders may show up later. But the FDA does not care about any of that because they have a vaccine to sell so they just ignore all of those factors in their model.
🚩 Pfizer intentionally wipes out the control group as soon as they can by vaccinating all of the kids who initially got the placebo. They claim that they are doing this for “ethical reasons”. But everyone knows that Pfizer’s true aim is to wipe out any comparison group so that there can be no long term safety studies. Wiping out the control group is a criminal act and yet Pfizer, Moderna, J&J, and AZ do this as standard practice with the blessing of the FDA/CDC.
🚩 Given all of the above, how on earth did the FDA claim any benefits at all from this shot? You should probably sit down for this part because it’s a doozy! Here’s the key sentence:
Vaccine effectiveness was inferred by immunobridging SARS-CoV-2 50% neutralizing antibody titers (NT50, SARS-CoV-2 mNG microneutralization assay).
Wait, what!? I’ll explain. There were ZERO cases of severe COVID-19 in the clinical trial of children ages 5 to 11. So Pfizer and the FDA just ignored all of the actual health outcomes (they had to, there is no emergency, so the application is moot). INSTEAD Pfizer switched to looking at antibodies in the blood. In general, antibodies are a poor predictor of immunity. And the antibodies in the blood of these 5 to 11 year old children tell us nothing because again, there were zero cases of severe COVID-19 in this study (none in the treatment group, none in the control group). So Pfizer had to get creative! What they came up with is “immuno-bridging”. Pfizer looked at the level of antibodies in the bloodwork of another study, this one involving people 16 to 25 years old, figured out the level of antibodies that seems to be protective in that population, then figured out how many kids ages 5 to 11 had similar levels of antibodies in their blood, and then came up with a number for how many cases, hospitalizations, ICU admissions, and deaths would be prevented by this shot in the 5 to 11 population in the future, based on the antibody levels and health outcomes from the 16 to 25 year old population. If your head hurts from that tortured logic, it should, because such chicanery is unprecedented in a risk-benefit analysis.
So when the FDA uses this tortured logic at the beginning of their briefing document, all of the calculations that stem from this will be flat out wrong. Not just wrong but preposterous and criminally wrong.
The whole ballgame comes down to Table 14 on page 34 of the FDA’s risk-benefit document. And there the red flags come fast and furious.
🚩 The FDA model only assesses the benefits of vaccine protection in a 6-month period after completion of two doses. Furthermore it assumes constant vaccine efficacy during that time period. This is problematic on several counts.
First, reducing mild cases in children is not a desired clinical outcome. As Dr. Geert Vanden Bossche points out, mass vaccination turns kids into shedders of more infectious variants.
“Under no circumstances should young and healthy people be vaccinated as it will only erode their protective innate immunity towards Coronaviruses (CoV) and other respiratory viruses. Their innate immunity normally/ naturally largely protects them and provides a kind of herd immunity in that it dilutes infectious CoV pressure at the level of the population, whereas mass vaccination turns them into shedders of more infectious variants. Children/ youngsters who get the disease mostly develop mild to moderate disease and as a result continue to contribute to herd immunity by developing broad and long-lived immunity. If you are vaccinated and get the disease, you may develop life-long immunity too but why would you take the risk of getting vaccinated, especially when you’re young and healthy? Firstly, there is the risk of potential side effects; secondarily, there is the ever increasing risk that your vaccinal antibodies will no longer be functional while still binding to the virus, thereby increasing the likelihood of ADE or even severe disease….”
Second, we know that vaccine efficacy in the month after the first dose is negative because it suppresses the immune system and it begins to wane after 4 months so all of the FDA’s estimates of vaccine efficacy are inflated.
Third, the harms of myocarditis from these shots will likely unfold over the course of years. Robert Malone, the inventor of mRNA technology notes that the FDA is admitting that children will be injected twice a year forever (hence the six month time frame in the FDA risk-benefit model). But the risks of “adverse events such as cardiomyopathy will be cumulative.” So any model that only looks at a six month time frame is hiding the true adverse event rate.
🚩 The FDA/Pfizer play fast and loose with their estimates of myocarditis. First they estimate “excess” (read: caused by the shot) myocarditis using data from the private “Optum health claim database” instead of the public VAERS system (p. 32). So it’s impossible for the public to verify their claims. Then, when it comes to estimating how many children with vaccine-induced myocarditis will be hospitalized and admitted to the ICU they use the Vaccine Safety Datalink (see page 33). Why switch to a different database for those estimates? Finally, there is no explanation for how they calculated “excess” myocarditis deaths, so they just put 0. Red flag, red flag, red flag.
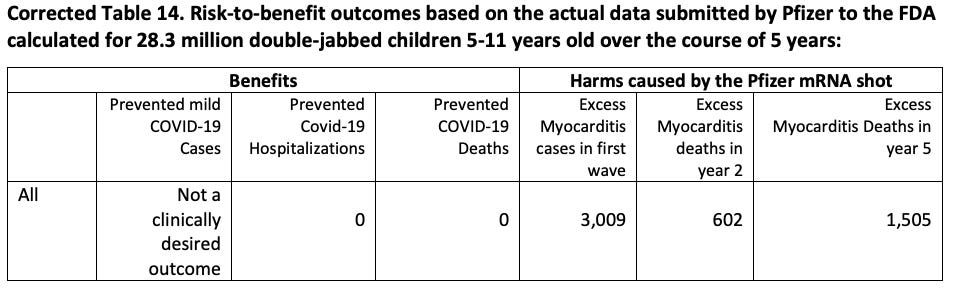
The FDA estimates that there will be 106 extra myocarditis cases per 1 million double-jabbed children 5-11. There are 28,384,878 children ages 5 to 11 in the U.S. The Biden administration wants to inject Pfizer mRNA shots into all of them and has already purchased enough doses to do just that (even though only 1/3rd of parents want to jab their kids with this shot). So (if the Biden administration has its way) 106 excess myocarditis cases per 1 million x 28.38 million people would be 3,009 excess myocarditis cases post-vaccination if the Pfizer vaccine is approved.
And over the course of several years many of those children will die.
Dr. Anthony Hinton (“Consultant Surgeon with 30 years experience in the NHS”) points out that myocarditis has a 20% fatality rate after 2 years and a 50% fatality rate after 5 years:
Viral myocarditis results in 2 in 10 people dead after 2 years and 5 in 10 after 5 years. It’s not mild. It’s dead heart muscle. https://t.co/ixRmk48rja
So the FDA has it exactly backwards — they want to prevent mild COVID in children which reduces herd immunity and they just flat out lie about the harms from myocarditis.
I’ve taken the liberty to correct the FDA’s Table 14 with actual real world data and extended it over 5 years. It looks like this:
A study by Harvard Pilgrim Healthcare for the U.S. Department of Health and Human Services estimated that VAERS only captured 1% of actual vaccine injuries. Steve Kirsch has done elaborate modeling that puts the Under-Reporting Factor of COVID-19 vaccine deaths at 41 (so multiply the above numbers by 41). And myocarditis is just one of a multitude of possible harms from COVID-19 vaccines. Dr. Jessica Rose recently calculated an Under-Reporting Factor of 31 for all severe adverse events following vaccination.
Conclusion
The Pfizer vaccine fails any honest risk-benefit assessment in connection with its use in children ages 5 to 11. The FDA’s risk-benefit analysis of Pfizer’s mRNA vaccine in children ages 5 to 11 is shoddy. It used tortured logic (that would be rejected by any proper academic journal) in order to reach a predetermined result that is not based in science. The FDA briefing document is a work of fiction and it must be withdrawn immediately. If the FDA continues with this grotesque charade it will cause irreparable harms to children and the FDA leadership will one day be prosecuted for crimes against humanity.
The rediscovery of a series of grisly experiments on beagle puppies has galvanized social media users into demanding the arrest of “America’s doctor” Anthony Fauci. But where was everyone when his work was harming humans?
Images of a sad pair of beagle puppies, their heads encased in square cages as they lie hopelessly on a table, have yanked at America’s heartstrings since they were shoved back into the national spotlight by White Coat Waste Project, a group that calls out US government labs for animal cruelty and other misuse (and abuse) of citizens’ money.
Millions of taxpayer dollars were used to essentially torture the puppies to death in labs in and out of the US, according to the organization, which unearthed evidence of the cruelty in the form of over $21 million spent on a total of four experiments – none of which was medically necessary. One involved severing 44 puppies’ vocal cords so that their pained barking and whining wouldn’t bother the scientists; another deliberately infected them with sand flies over the course of 22 months, restricting their movements by locking their heads in boxes so that they could not even swat the insects away as they were being eaten alive.
It’s horrific stuff by any measure, beyond cartoonish levels of evil. Indeed, even Texas Senator Ted Cruz (R) claimed he thought the tweets he’d read about Fauci “literally ‘torturing puppies’” had to be “metaphorical.”
But while the outrage is justified, it’s also old news. One could ask why the masses have turned against Fauci only now, when his National Institute for Allergies and Infectious Diseases has been funding the torture of puppies for years, with one of the horrific experiments dating from 2016. The most recent grant dated from 2020, meaning Fauci’s agency was vivisecting helpless furry animals at the University of Georgia even while he was being worshiped as America’s Doctor™ and posing for photos with other people’s dogs.
Even White Coat Waste Project refers to its own revelations as “Fauci’s other international scandal,” implying knowledge of a better-known episode in the fame-hungry doctor’s life.
One must ask why the popular outrage against Fauci over animal cruelty is not matched by an equal (if not more forceful) outrage over the doctor’s crimes against humanity. From his enthusiastic support of gain-of-function studies to his efforts to sideline a cheap, effective drug that could have saved thousands of lives during the AIDS epidemic in favor of a highly toxic alternative, Fauci’s hands are covered in the blood of humans as well as that of canines.
Indeed, Fauci’s behavior during the Covid-19 outbreak – trashing cheap but effective treatments in favor of expensive alternatives lacking proof of efficacy – eerily mirrors his actions during the early years of AIDS. Thousands of people have died in both cases after Fauci pushed deadly or ineffective medications – most notably the failed cancer drug AZT in the 1980s and the failed Ebola drug remdesivir in the last two years – while safer and more efficacious remedies sat on the shelf.
Discoveries that members of the National Institutes of Health, parent of Fauci’s NIAID, had hefty investments in Gilead, maker of remdesivir, as well as in Moderna, one of the manufacturers of an mRNA vaccine for Covid-19, have only raised more questions about Fauci’s motives during the coronavirus pandemic.
Fauci has also been caught lying repeatedly about his involvement in gain-of-function research aimed at making bat coronaviruses more infectious in humans. Despite his profuse denials of even funding such research in recent months, he previously defended the work by arguing that any knowledge gained from bolstering the infectious potential of such pathogens was “worth the risk” of unleashing a pandemic. Whether or not his NIAID-funded research played a part in the Covid-19 outbreak has not been proven, but Fauci’s furious tap-dancing around any questions regarding the Wuhan lab or gain-of-function research in general does him no favors.
Yet, somehow, none of this elicits anything like the howls of rage coming from dog-lovers on social media. The same outrage-on-demand contingent who demand countries like China and Vietnam stop eating dog meat, signing a petition with one hand while biting into a well-done burger with the other, insist on the closure of “barbaric” wet markets like the one we were told spawned the novel coronavirus in late 2019. This group’s problem is less animal cruelty than being reminded of that cruelty. They’d rather wait until their meat is shrink-wrapped and frozen in a supermarket than pick out the tastiest-looking chicken in the bunch and have it slaughtered then and there.
Ultimately, Fauci being arrested is an endpoint that animal rights activists, human rights activists, and the normally comatose members of Congress – 24 of whom actually signed a letter demanding answers from the once-untouchable Coronavirus Pope – should see eye-to-eye on. But the diminutive doctor must not be permitted to skate on his real crimes – whether it’s pandemic profiteering, bankrolling gain-of-function research in China that was at the time illegal to perform in the US, or allegedly perjuring himself in congressional testimony. Fauci has much to answer for. Dozens of dead puppies are just the tip of the iceberg.
Unfortunately, like other gleeful architects of the Covid-19 police state who’ve been caught in the midst of scandal – former New York Governor Andrew Cuomo, for example – arresting Fauci on the basis of popular rage over dead puppies is likely to close the book on further prosecution, no matter how heinous his “real” crimes.
Just as Cuomo is unlikely to ever be held to account for the thousands of elderly New Yorkers who died because of his nursing-home order to house Covid-positive patients with the helpless elderly, Fauci will be permitted to enjoy his retirement – and big fat pension – in peace. Americans who have lost everything to his mismanagement of the Covid-19 pandemic must not let that happen.
Helen Buyniski is an American journalist and political commentator at RT. Follow her on Telegram
This is the 15th of the round-ups of Covid vaccine safety reports and news compiled by a group of medical doctors who are monitoring developments but prefer to remain anonymous in the current climate (find the 14th one here).
By no means is this part of an effort to generate alarm about the vaccines or dissuade anyone from getting inoculated. It should be read in conjunction with the Daily Sceptic‘s other posts on vaccines, which include both encouraging and not so encouraging developments. At the Daily Sceptic we report all the news about the vaccines whether positive or negative and give no one advice about whether they should or should not take them. Unlike with lockdowns, we are neither pro-vaccine nor anti-vaccine; we see our job as reporting the facts, not advocating for or against a particular policy. The vaccine technology is novel and the vaccines have not yet fully completed their trials, which is why they’re in use under temporary and not full market authorisation. This has been done on account of the emergency situation and the trial data was largely encouraging on both efficacy and safety. For a summary of that data, see this preamble to the Government’s page on the Yellow Card reporting system. (Dr Tess Lawrie in June wrote an open letter to Dr June Raine, head of the MHRA, arguing that: “The MHRA now has more than enough evidence on the Yellow Card system to declare the COVID-19 vaccines unsafe for use in humans,” a claim that has been ‘fact checked’ here.) Boris Johnson has now said that the vaccine “doesn’t protect you against catching the disease, and it doesn’t protect you against passing it on”. We publish information and opinion to inform public debate and help readers reach their own conclusions about what is best for them, based on the available data.
Dr Scott McLachlan reports an excessive number of healthy babies born to mothers who’ve had the vaccine during pregnancy dying within 48-72 hours of birth.
The latest U.K. Covid figures by vaccination status, up to week 41 (17th October), report higher cases of Covid per 100,000 people in double-vaccinated than unvaccinated.
Sweden has suspended the Moderna jab indefinitely after vaccinated patients developed myocarditis, whilst a case of Pfizer vaccine-associated-myocarditis is reported as the cause of death in a 22 year old man in Korea.
VAERS – the American version of the Yellow Card reporting system – released new data on October 15th bringing the total to 818.044 reports of adverse events following Covid vaccines, including 17,128 deaths and 122,833 serious injuries.
DAEN Australia – the equivalent of the Yellow Card reporting system – has logged (up to October 10th) 67,063 reports of adverse events, including 589 deaths. Australia has recorded 1,432 Covid deaths to date.
Children (Under 18) Adverse Events U.K. – up to October 13th, MHRA report a total of 1,297 adverse event reports, comprising 1,056 Pfizer, 233 AstraZeneca, 5 Moderna and 3 unspecified. Myocarditis reports remain 10 in a million for this age group. No information is provided on fatalities.
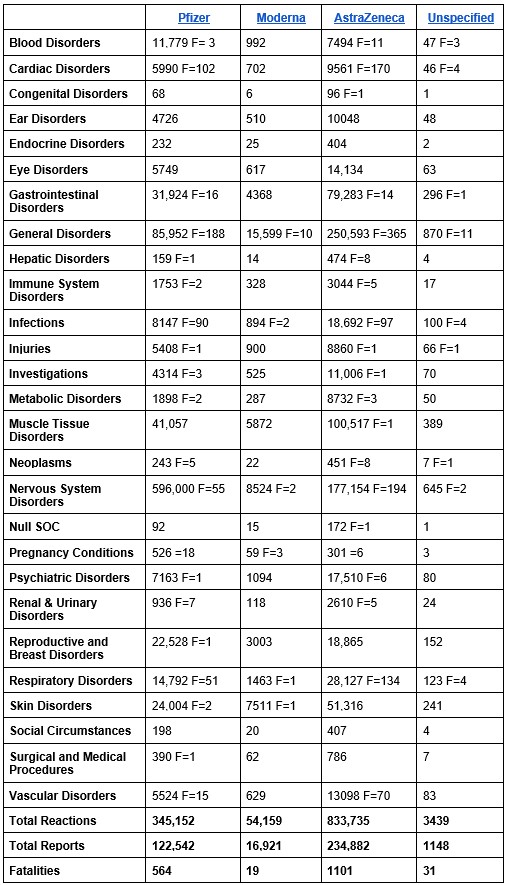
Summary of Adverse Events in the U.K.
According to an updated report published on October 21st, the MHRA Yellow Card reporting system has recorded a total of 1,236,485 events based on 375,493 reports. The total number of fatalities reported is 1,715.
Pfizer (22.9 million first doses, 19.9 million second doses) now has one Yellow Card in 187 people vaccinated. Deaths: 1 in 40,603 people vaccinated (564).
AstraZeneca (24.9 million first doses, 24.1 million second doses) has one Yellow Card in 106 people vaccinated. Deaths: 1 in 22,616 people vaccinated (1,101).
Moderna (1.5 million first doses, 1.2 million second doses) has one Yellow Card in 89 people vaccinated. Deaths: 1 in 78,947 people vaccinated (19).
Overall, one in every 131 people vaccinated (0.76%) have experienced a Yellow Card adverse event. The MHRA has previously estimated that the Yellow Card reporting rate may be approximately 10% of actual figures.
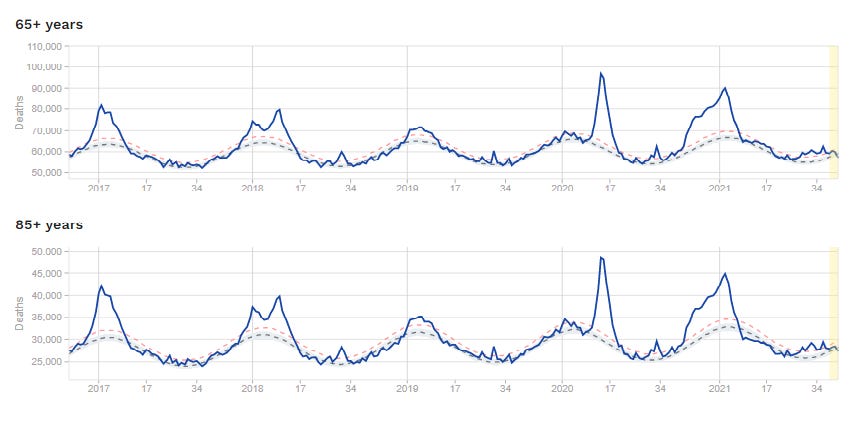
It wouldn’t take much to push a population of such elderly and frail people into a life-threatening situation. Lock them up for months on end. Deny them human contact on pain of arrest and fines they couldn’t hope to pay. Withdraw medical treatment. Quarantine their carers. Terrorise them with propaganda about a civilisation-ending disease. Order them to stay at home and avoid the contact of other people like the plague. Tell them hospitals standing empty are on the verge of being overwhelmed. Turn medical centres into places to fear, the breeding grounds of a deadly new disease. That should be more than enough. It has been more than enough.
To preserve the elderly, the world has used the young – who suffered no pandemic – as a shield.
The young have lost their jobs, their childhoods, their right to breathe air freely, their right to say no to experimental medicine they do not need.
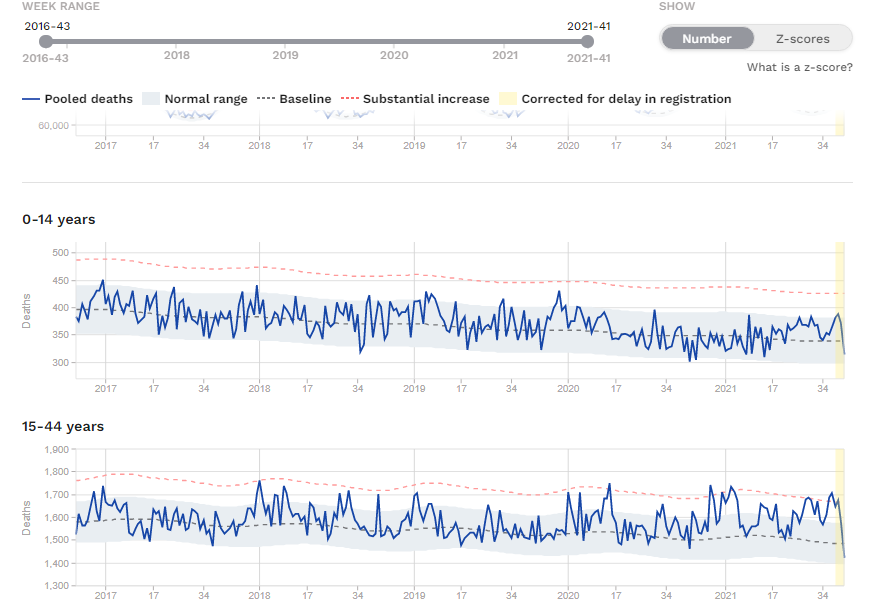
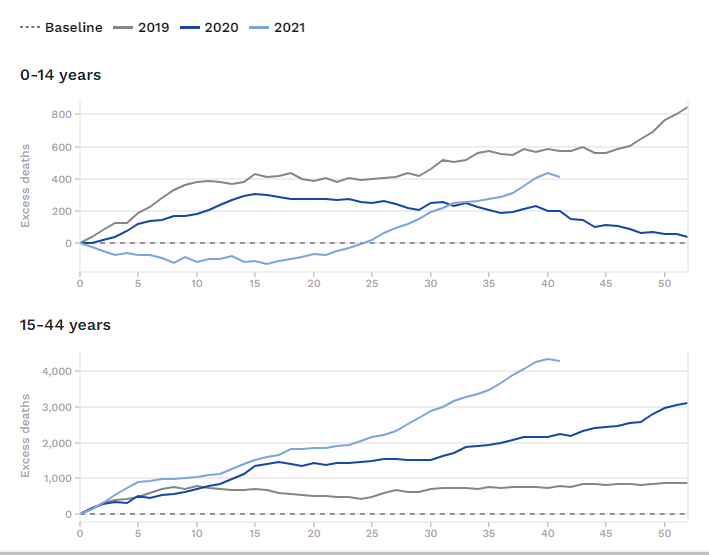
And now they appear to be dying for the elderly too:
Please can somebody explain why deaths are rising so steeply in European youth?
They did not suffer from historically excess death in the middle of the pandemic.
Why are they dying now?
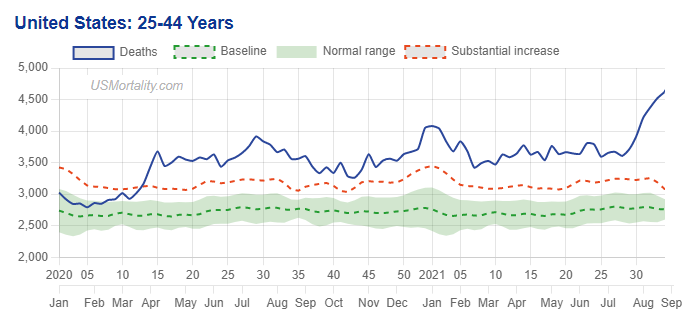
And it is not only them – US young people are suffering the same fate:
PHARMACOVIGILANCE: the practice of monitoring the effects of medical drugs after they have been licensed for use, especially in order to identify and evaluate previously unreported adverse reactions.
Pages 34-35 of the FDA review of Pfizer’s data for the 5-11 year olds provides the pretense of truly caring about identifying and quantifying adverse events from the vaccine. Just look at all the “activities” Pfizer and its partner must do. Well, of course they have to do them, since their clinical trial was so underpowered (not enough subjects) and only ran 2 months for about half the kids and 2.5 weeks for the rest. Duh?
Not only that, but Pfizer presented its data to FDA on October 6, and FDA already had completed its review and written its 39 page report by October 23, 17 days later. Fast work. But then again, we are only talking about the health of 28 million elementary school kids. And millions more overseas whose countries follow FDA advice.
And lest I forget, we are also talking about their education, because it seems they won’t be able to attend school soon, if unjabbed. Gavin Newsome said so. And a bill is being introduced in the District of Columbia for the same purpose.
Clearly, the stakes are pretty low, so a pretend Pfizer clinical trial and a pretend FDA review are good enough, right?
Below is part of FDA’s presentation. What is missing is the most important information, revealed in an Aug 23 letter from FDA. And that is, that the trials FDA demands Pfizer undertake to find out how dangerous its vaccines actually are, will not be reported to FDA until 2024 and 2025–presumably after most of the world’s children have already received 2 or 4 or 6 or 8 doses.
9 PHARMACOVIGILANCE ACTIVITIES
Pfizer submitted a revised Pharmacovigilance Plan (PVP) to monitor safety concerns that could be associated with BNT162b2 in individuals 5-11 years of age. The PVP includes the following safety concerns:
• Important Identified Risks: anaphylaxis, myocarditis, and pericarditis
• Important Potential Risks: Vaccine-associated enhanced disease (VAED), including vaccine-associated enhanced respiratory disease (VAERD).
Pfizer-BioNTech plans to conduct passive and active surveillance to monitor the postauthorization safety for the Pfizer-BioNTech COVID-19 Vaccine, including: 35
• Mandatory reporting by the Sponsor under the EUA for the following events to VAERS within 15 days: SAEs (irrespective of attribution to vaccination); COVID-19 disease resulting in hospitalization or death; multisystem inflammatory syndrome (MIS)
• Adverse event reporting in accordance with regulatory requirements for the licensed vaccine, COMIRNATY
• Additionally, following approval of COMIRNATY, the Sponsor was also asked to submit reports of myocarditis and pericarditis as 15-day reports to VAERS.
• Periodic safety reports containing an aggregate review of safety data including assessment of AEs; vaccine administration errors, whether or not associated with an AE; and newly identified safety concerns.
• Post-authorization observational studies, that would be modified to encompass the evaluation of children 5-11 years of age include active surveillance safety studies using large health insurance claims and/or electronic health record database(s):
– Study C4591009: A non-interventional post-approval safety study of the Pfizer-BioNTech COVID-19 mRNA Vaccine in the United States
Objective: To assess the occurrence of safety events of interest, including myocarditis and pericarditis, in the general U.S. population of all ages, pregnant women, the immunocompromised, and persons with a prior history of COVID-19 within selected data sources participating in the U.S. Sentinel System.
– Study C4591021: Post-conditional approval active surveillance study among individuals in Europe receiving the Pfizer-BioNTech Coronavirus Disease 2019 (COVID-19) Vaccine
Objective: To assess the potential increased risk of AESIs, including myocarditis/pericarditis, after being vaccinated with at least one dose of the PfizerBioNTech COVID-19 Vaccine.
– Study C4591021 Substudy: Substudy to describe the natural history of myocarditis and pericarditis following administration of COMIRNATY
Objective: To describe the natural history of post-vaccination myocarditis/pericarditis, including recovery status, risk factors, and/or identification of serious cardiovascular outcomes within one year of myocarditis/pericarditis diagnosis among individuals vaccinated with BNT162b2 as well as individuals not vaccinated with a COVID-19 vaccine.
– Study C4591036: Prospective cohort study with at least 5 years of follow-up for potential long-term sequelae of myocarditis after vaccination (in collaboration with Pediatric Heart Network [PHN]). Working title: Myocarditis/pericarditis follow-up study within the Pediatric Heart Network
Objective: To characterize the clinical course, risk factors, resolution, long-term sequelae, and quality of life in children and young adults <21 years with acute postvaccine myocarditis/pericarditis. Pfizer-BioNTech also plans to include vaccine effectiveness analyses among individuals 5-11 years of age in Study C4591014 entitled “Pfizer-BioNTech COVID-19 BNT162b2 Vaccine Effectiveness Study Kaiser Permanente Southern California.”
1. We cannot vaccinate ourselves out of the Covid problem. Mass vaccination is forcing the virus to produce variants, which escape any protection provided by the jab (see here for a report covering 68 countries). Instead, the vaccine should be offered only to those most vulnerable, such as the very elderly.
2. It is especially wrong to give it to children. They are at almost zero risk from Covid but subject to a real risk of damage from this particular vaccine, unrecognised during its development.
3. Cheap and effective treatment is available which keeps the vast majority of patients out of hospital. Health officials and regulators should support doctors who want to use these treatments, and to educate patients in how to strengthen their responses to the virus.*
4. Lockdowns and official fear-inducing propaganda have blighted the lives of millions, especially children, and must never be repeated.
The discussion is a must view for concerned individuals. It offers a completely different perspective from that of the NHS chiefs now calling for booster jabs and the return of Covid restrictions.
These edited contributions give a flavour of the discussion:
Dr Robert Malone, key architect of the mRNA technology that made possible the most commonly used Covid vaccines: ‘The virus is evolving very rapidly. This is akin to what happens if you overuse antibiotics. With universal vaccination, we’re driving towards an endpoint of vaccine-resistant mutants. The vaccines need to be used intelligently.
‘This set of vaccines that we have right now are gene therapy-based, and they have a common problem: they only have one antigen. It’s the spike antigen. When they were developing them, they didn’t realise the spike was biologically active. No fault of theirs. Everybody was in a rush.
‘But now it’s time to take a breath and say, “Hey, does this really make sense?” We don’t have to be just Left or Right, pro- or anti-vaccine. There’s a middle ground. We, as a community, need to protect people at high risk, not just here in our community, in our states; in my opinion, we need to protect the elders throughout the world. We don’t need to hoard all the vaccine for people that don’t really need it.
‘I’m not an anti-vaxxer, I’m a guy who’s spent the majority of my adult life developing vaccines. This is a technology platform that has enormous promise. And right now it’s in its infancy. The safety of the underlying technology is not yet fully demonstrated.
‘People did what they did in good faith and focused on a protein that they thought was fully safe – spike. But now, over a year later, we know that in the virus, this protein is responsible for much of the disease – the pathology in your vascular endothelial cells [blood vessel linings], the coagulation. And it’s unfortunate that this particular protein, in what appears to be a biologically active form, was used in these vaccines.’
Dr Richard Urso, ophthalmologist, Texas: ‘When people say, “They died of Covid”, they died of an inflammatory, thrombotic disease. They didn’t die from the virus running through their body. There’s a bunch of drugs that can be used for the purpose of inflammation in this disease. There’s a bunch of drugs for thrombosis. Hopefully at some point we’ll have a really good, early treatment that’s directed to the virus itself. Right now we have other, very effective treatments.
‘About 330 children have died of Covid in a year and a half [under-19s in the US]. Typically, about 50,000 children a year die – many from drownings, from car accidents. You need to look at that as you look at the risk to children. And do they spread? – No, at least seven different studies show that children spreading to adults is close to zero.’
Dr Brian Tyson, family doctor, California, who has successfully treated more than 6,000 Covid patients and now finds children are getting sick from typical winter illnesses, rather than Covid: ‘With treatment started from day 1 to 7, I have had zero deaths. From treatment started from day 7 to 14, I have four – two died the same day they showed up at the clinic, and two died in hospital.
‘Under that data Dr Urso was talking about, not one healthy child died from Covid-19. It was children who had four or five risk factors – morbid obesity being number one, diabetes number two, weakened immune system number three; kids on chemotherapy and things like that. So yes, they’re going to have opportunistic infections, but that’s no different than would normally take out these kids anyway, unfortunately.’
Dr Heather Gessling, family doctor, Missouri: ‘My numbers exactly match up with Brian’s. I’ve treated about 1,500 and I’ve had one death, because there was some delay in treatment.’
Dr Mark McDonald, child psychiatrist, Los Angeles: ‘Fear has been the driving force of this pandemic from the very beginning. What’s driving the fear now is propaganda. I see kids all day long. The developmental stage that children need to go through – babies, toddlers, young adults – is being foreclosed on them.
‘Brown University department of paediatrics published a study that found babies born after January 1, 2020, have an IQ drop of 20 points. Why? They don’t see faces. They don’t play. They don’t have exposure to friends. They don’t go to school. They’re basically locked in their homes, looking at their parents for a year and a half. And their brains have not developed.
‘My concern is that we are building a generation of young people who are so traumatised that they will never fully recover. They’re always going to be scarred emotionally.
‘I don’t mean to be depressing. I mean to be alarming, so everyone can finally say, “Stop!” We’ve got to stop the damage, and then figure out what to do about it.’
Dr Gessling: ‘I think “Stop the damage!” means to acknowledge what we have done wrong. We should reverse all the measures that have been implemented. Patients, families, parents, should take it upon themselves to feel empowered. We need to get back to the basics, because we’ve done this wrong for so long.
‘One of the books we all had in medical school was Harrison’s Principles of Internal Medicine. This is what we have forgotten: “Many specific host factors influence the likelihood of acquiring an infectious disease: age, immunisation history, prior illnesses, level of nutrition, pregnancy status, coexisting illnesses and perhaps emotional state – all have some impact on the risk of infection after exposure to a potential pathogen.” All we have done is focus on one of those: immunisation history.
‘The ability to provide early, effective treatment should make us feel empowered. We should not feel afraid any more.’
Dr Pierre Kory, pulmonary and critical care specialist; founding member and president, the Front Line Covid-19 Critical Care Alliance; co-author of two Covid prevention and treatment protocols: ‘My hopes are that more and more attention is going to be paid to early treatment strategies, especially now the vaccinated are getting sick. Many people were led to believe that if you get your vaccine, we’re going to end this thing, you don’t have to worry about it, you can carry on with your lives.
‘But guess what? My colleagues are talking about even scarier variants that are coming. And so we need more tools to fight this. The positive message is, we have them, and they can handle any variant that comes at us. We just need to get that message out. I don’t believe anybody has died who’s had effective early treatment.’
Dr John Littell, family doctor, Florida: ‘What we’re seeing now is that patients are getting early treatment with ivermectin, hydroxychloroquine and a host of other medications, because of this free exchange of ideas in this group of physicians and others around the world.
‘Dr Tyson, Dr Gessling and myself are family physicians, OK? So we’re the folks who have been in those front lines getting the phone calls in the middle of the night from concerned parents. And what you’ve just heard from Dr Kory and from us is that is that if you take the right preventive treatment, you’re approaching zero per cent mortality.’
Dr Kory: ‘If we have effective treatments, why aren’t they being recognised and disseminated across the world? I think we’re up against two forces.
‘The first is that in general, our health agencies are suffering what’s called regulatory capture. They’re largely driven by financial interests that are making sure that the solution to the pandemic is one that is profitable. Vaccines are profitable.
‘The other, somewhat overlapping challenge is that in academia, in the last ten years, there’s been this increasing belief that the only proof of efficacy of a drug has to come out of a large, double-blind, randomised controlled trial. You have to make the diagnosis – everyone has to have a positive test; they have to have symptoms; they have to be enrolled, consented, randomised, and then the drug is delivered. Each one of those steps takes time. So it’s often very delayed, and under-dosed – they’re using doses that I was using six months ago.’
Dr Ryan Cole, medical director, Cole Diagnostics, Idaho, who has done more than 100,000 Covid tests in the past year: ‘Covid is a clotting disease. When we give a spike protein [through the vaccine], that is an active biologic molecule. We chose the wrong molecule, which causes disease.
‘So what do I see under the microscope? We see clotting under the skin, in the lungs, in the blood vessels, in the brain – not from the virus, but from the spike from the vaccine itself.
‘Now consider the numerator and the denominator. Are most people going to be fine? Yes. And I want to emphasise that.
‘[But] in our data from around the world, from the United States, from the UK, from EudraVigilance in Europe, we have seen more death and damage from this one medical product than all other vaccines combined in the last several decades, in just a short, eight-month window of time. It has done more damage than any other medical product, therapy, shot, modality, of anything we’ve ever allowed to stay on the market to this point.
‘Do I mean to sound alarmist? No, I’m being factual. And when I look at it under the microscope and I see the parts of people – or people that are no longer with us – the damage and the disease is caused by that spike protein. It is present.
‘A virus is a humanitarian issue. When we divide ourselves in thought and don’t listen to science any more, we’re going down the wrong paths.
‘We are forgetting what our amazing immune system does. How many of you had chickenpox when you were a kid? And how many of you have ever had it again? Did you need a shot? No. Grandma had measles – has grandma ever had it again? No, because her immune system works.
‘Half of kids in the US have already had Covid. We’re not antibody testing – we’re treating everybody with this terrible oppression of, “You’ve got to wear a mask . . . you’ve got to stay home if somebody in your classroom tests positive.” It denies basic science.
‘Under age 50 with no co-morbidities, your chances of dying from this disease are about nil, and if you get early treatment they are even closer to nil. So if you are a Covid recoverer, you don’t need a shot.
‘The shot can damage the hearts of children. There are more children who’ve had myocarditis – and there’s never such a thing as mild myocarditis. That’s inflammation of the heart. Once you get inflammation, you get scarring. Those kids’ hearts are damaged for life. Kids have died of heart attacks after the shot, and there are more kids that have had myocarditis than have died from Covid. Kids aged zero to 18 survive this virus at a statistical 100 per cent – 99.997 per cent. So why are we punishing kids for a virus they survive?’
*For up-to-date guides to home treatment of Covid, see here and here.
IT’S OFFICIAL: Most of the UK’s vaccinated population are suffering far higher rates of infection than the unvaccinated, and it is getting worse by the day.
The UK’s Health Security Agency publishes detailed Covid statistics, which, for the last 7 weeks, have been tabulated by age-group and vaccination status. This now allows important questions to be answered.
The Agency says most vaccinated suffer substantially higher rates of infection, and their latest chart provides a snap-shot:
All of the UK’s 30-and-over vaccinated now endure far higher rates of infection than their unvaccinated counterparts. But as a snap-shot, this tells us nothing of how this arose, or how it may yet develop. Here we re-present the agency’s data in a time-series, to promote better understanding of the trends and implications.
The UK has vaccinated its population mostly in age order, from oldest to youngest, and very recently began vaccinating its under-18-year-old cohort. Being the UK’s most freshly vaccinated, they exhibit a very high degree of resistance to Covid infection: –
This very recently vaccinated cohort benefits from a 90% improvement in their infection rates, meaning their case incidence is 10 times better than that of their unvaccinated counterparts. This is impressive, and leads us to ask how long this high degree of protection might last?
The answer, unfortunately, seems to be not very long:
The previous UK age-group to be vaccinated was the 18–29-year-old cohort, of which half was fully vaccinated by some 9 weeks ago. While still doing better than the unvaccinated of their age, they have nevertheless lost the greater part of their relative resistance to infection. If they continue their trajectory, week 12 will see that benefit completely gone.
The earlier vaccinated age-group was the 30–39 cohort. Half was fully vaccinated around week 27, and by week 39 (again some 12 weeks later) had lost their enhanced infection resistance. For at least for these two cohorts, it would seem their vaccine induced resistance reduced to zero in under 3 months.
Unfortunately, it does not stop there; Following the data shows the vaccinated descend well into negative territory, which may prompt us to ask how all earlier vaccinated cohorts are now doing?
In terms of vulnerability to infection, the answer is not so well:
The entire 40-79 vaccinated cohort is deeply negative, now below minus 50%, meaning they suffer more than double the infection rate of their unvaccinated counterparts, and there is no obvious end in sight; Given the consistent and strongly negative continuing trend for all adult cohorts, it is impossible to guess where or when these trajectories might bottom out.
But does the trend result from increased vulnerability amongst the vaccinated, or is improved resistance developing amongst the unvaccinated? The answer appears to be both:
Unvaccinated adults are enjoying significantly lowered infection rates, but the vaccinated are very clearly headed in the opposite direction:
This begs the question: Why should the vaccinated suffer mounting infection rates, while case-rates of the unvaccinated both declined and are lower? Surely, we should expect the vaccinated to do better – certainly no worse?
Yet, for all but one adult cohort, the exact opposite is true, and even for them, it seems likely for not much longer:
It has been suggested infection amongst the unvaccinated has induced robust natural immunity leading towards their herd-immunity. That may well be a factor, but, as we have seen, the vaccinated have similarly been infected, and at least for the 40-79 cohort, at much higher rates. Why should this not benefit the vaccinated as well?
Are we to understand infection after vaccination may not produce similar broad immunity?
Vaccination is intended to alter subsequent immune response to infection, which is, of course, the whole point; It is conceivable this altered response may mute the development of broad long-lasting immunity that otherwise typically results from natural infection. That might then leave the vaccinated more open to re-infection, and might help explain these results. But this remains speculation, we simply do not know today.
What we do know from the UK data, is that anyone vaccinated more than few months ago is at greatly higher risk of Covid infection, and is therefore greatly more likely to be infected than their unvaccinated counterparts.
Much has been said and written to show the vaccinated are equally capable of transmitting Covid. But because their symptoms are often muted, they are also more likely to be out and about; add this to escalating infection rates, and there can be little doubt the vaccinated now constitute by far the greatest Covid transmission risk.
In light of this, vaccine passports are clearly senseless; They are nothing more than an invitation to infection, for which no justification can now possibly remain.
Here come jabs in schools without parental consent.
“Bonnie J. Fraser Henry OBC FRCPC is a Canadian physician who is the Provincial Health Officer for British Columbia, the first woman in this position. Henry is also a clinical associate professor at the University of British Columbia. She was a family doctor and is a specialist in public health and preventive medicine.”
In fact, the politicians have worked on this for years, and enshrined it in legislation, she says.
Looks like you can garner lots of awards when your heart is a stone, Bonnie.
And, like Presidential wannabe Governor Cuomo, she even had time to write a book about her leadership in the pandemic, titled Be Kind, Be Calm, Be Safe. Do these people know what they are, or are they high on their own supply?
Here someone collected her telling the truth about masks last year and flip-flopping later:
Thousands of California Parents pulled their children from schools across the state Monday, as part of a massive protest against Covid vaccine mandates.
A while ago, I received an email from a friend who asked:
How can many, many respected, competitive, independent science folks be so wrong about [global warming] (if your [skeptical] premise is correct). I don’t think it could be a conspiracy, or incompetence. … Has there ever been another case when so many ‘leading’ scientific minds got it so wrong?
The answer to the second part of my friend’s question—“Has there ever been another case where so many ‘leading’ scientific minds got it so wrong?”—is easy. Yes, there are many such cases, both within and outside climate science. In fact, the graveyard of science is littered with the bones of theories that were once thought “certain” (e.g., that the continents can’t “drift,” that Newton’s laws were immutable, and hundreds if not thousands of others).
Science progresses by the overturning of theories once thought “certain.” … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.