A Surgeon Writes…
By Toby Young • The Daily Sceptic • October 24, 2021
An NHS surgeon who’s contributed to the Daily Sceptic before has sent us an email offering us his perspective on the current NHS ‘crisis’. It’s a reminder that even though the current pressure on the NHS cannot realistically be attributed to Covid hospital admissions – which remain at around 5% of the total – that doesn’t mean that the NHS isn’t under strain.
There are various debates about whether or not the NHS is under pressure with pundits rightly pointing out that the NHS is not under pressure due to Covid-related disease. I think at this stage this is an unhelpful diversion. The fact is there is a big problem and trying to disprove it by just looking at Covid is missing the bigger picture.
The NHS is under a lot of pressure due to processes unrelated to Covid workload. While hospitals are not yet full to the brim, the overall activity levels are higher than usual for certain regions (whether this is due to the catch-up effect, neglect, the iatrogenic effect of recent non-pharmaceutical or other interventions/measures, etc.). The main crisis is related to staffing. This labour shortage has been noted in many sectors of the economy, but the staffing crisis (mainly non-doctoral) in the NHS has been chronic and worsening for years. This year tipped the balance (psychological exhaustion, physical exhaustion, sickness absence, track and trace, etc.). In our region hospitals are routinely cancelling (relatively non-essential) surgery due to lack of staff required to either run operating theatres or wards/ancillary services. Hospitals are routinely running extra activity on Saturdays to try and catch up on cancer work. This is a weekly occurrence not limited to the place I work. Factor in the very long (self-created) waiting lists and the winter (which has not even started), and the crisis could become unmanageable.
I am pessimistic. Regardless of the Covid workload, the Government may use a real crisis in the NHS to justify more pointless non-pharmaceutical interventions and vaccine passports (complete nonsense from a medical, ethical and social perspective) out of desperation, misconception, or both.
17,000+ deaths reported after COVID vaccines, including new report of 12-year-old who died after Pfizer vaccine
By Megan Redshaw | The Defender | October 23, 2021
Data released Friday by the Centers for Disease Control and Prevention (CDC) showed that between Dec. 14, 2020, and Oct. 15, 2021, a total of 818,044 adverse events following COVID vaccines were reported to the Vaccine Adverse Event Reporting System (VAERS).
The data included a total of 17,128 reports of deaths — an increase of 362 over the previous week, and a new report of a 12-year-old who died after getting the Pfizer vaccine.
There were 117,399 reports of serious injuries, including deaths, during the same time period — up 5,434 compared with the previous week.
Excluding “foreign reports” to VAERS, 612,125 adverse events, including 7,848 deaths and 50,225 serious injuries, were reported in the U.S. between Dec. 14, 2020, and Oct. 15, 2021.
Of the 7,848 U.S. deaths reported as of Oct. 15, 11% occurred within 24 hours of vaccination, 15% occurred within 48 hours of vaccination and 28% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 406.1 million COVID vaccine doses had been administered as of Oct. 15. This includes: 237 million doses of Pfizer, 154 million doses of Moderna and 15 million doses of Johnson & Johnson (J&J).

The data come directly from reports submitted to VAERS, the primary government-funded system for reporting adverse vaccine reactions in the U.S.
Every Friday, VAERS makes public all vaccine injury reports received as of a specified date, usually about a week prior to the release date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed.
Historically, VAERS has been shown to report only 1% of actual vaccine adverse events.
This week’s U.S. data for 12- to 17-year-olds show:
- 21,921 total adverse events, including 1,325 rated as serious and 25 reported deaths. Two of the 25 deaths were suicides.
The most recent death involves a 12-year-old girl (VAERS I.D. 1784945) who died from a respiratory tract hemorrhage 22 days after receiving her first dose of Pfizer’s vaccine.
Another recent death includes a 15-year-old male who died six days after receiving his first dose of Pfizer’s COVID vaccine. According to his VAERS report (VAERS I.D. 1764974), the previously healthy teen complained of brief unilateral shoulder pain five days after receiving his COVID vaccine.
The next day he played with two friends at a community pond, swung on a rope swing, flipped into the air, and landed in the water feet first. He surfaced, laughed and told his friends “Wow, that hurt!” He then swam toward shore underwater, as was his usual routine, but did not re-emerge.
An autopsy showed no external indication of a head injury, but there was a small subgaleal hemorrhage — a rare, but lethal bleeding disorder — over the left occiput. In addition, the boy had a mildly elevated cardiac mass, increased left ventricular wall thickness and small foci of myocardial inflammation of the lateral wall of the left ventricle with myocyte necrosis consistent with myocardial infarction.
- 57 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment or resulted in death — with 96% of cases attributed to Pfizer’s vaccine.
- 535 reports of myocarditis and pericarditis (heart inflammation) with 527 cases attributed to Pfizer’s vaccine.
- 119 reports of blood clotting disorders, with all cases attributed to Pfizer.
This week’s U.S. VAERS data, from Dec. 14, 2020, to Oct. 15, 2021, for all age groups combined, show:
- 19% of deaths were related to cardiac disorders.
- 54% of those who died were male, 42% were female and the remaining death reports did not include gender of the deceased.
- The average age of death was 72.7.
- Of the 3,014 cases of Bell’s Palsy reported, 51% were attributed to Pfizer vaccinations, 41% to Moderna and 8% to J&J.
- 666 reports of Guillain-Barré syndrome, with 40% of cases attributed to Pfizer, 31% to Moderna and 28% to J&J.
- 2,010 reports of anaphylaxis where the reaction was life-threatening, required treatment or resulted in death.
- 10,290 reports of blood clotting disorders. Of those, 4,488 reports were attributed to Pfizer, 3,709 reports to Moderna and 2,040 reports to J&J.
- 2,878 cases of myocarditis and pericarditis with 1,815 cases attributed to Pfizer, 939 cases to Moderna and 114 cases to J&J’s COVID vaccine.
Illinois Sheriffs Reject Mayor Lightfoot’s Urgent Plea To Cover Police Shortage In Crime-Hit Chicago
By Tyler Durden | Zero Hedge | October 22, 2021
As hundreds of Chicago police are being put on “no-pay leave” over their refusal to submit their personal Covid vaccination status with the city, Chicago Mayor Lori Lightfoot appears to have fewer and fewer allies as she desperately tries to fill the gap of officer shortages due to the vax order. Area county sheriffs are refusing to send additional manpower that’s she requesting to urgently cover the gaps, telling her that’s it’s a problem of the mayor’s own making.
“Chicago Mayor Lori Lightfoot received a rude awakening after multiple sheriffs in nearby jurisdictions refused her request to fill the gap in police manpower after she threatened to fire 3,000 local officers for not complying with the city’s COVID-19 vaccine mandate,” The Washington Examiner reports on the latest developments. “DuPage County Sheriff James Mendrick and Kane County Sheriff Ron Hain said they’ve helped Lightfoot in the past, but her latest request is a self-inflicted wound that could have been avoided. They said they would only step in and help the Chicago Police Department if city officers were in distress or under duress.”
Sheriff Hain had this to say, echoing recent criticisms of the Chicago police union which has cited terrible communication and heavy-handedness in place of requests for dialogue on the issue: “[The Illinois Law Enforcement Alarm System] typically responds to emergency situations where there is no opportunity for planning,” Hain said. “This situation to me is much different.”
Despite sheriff’s offices shutting the door on the mayor’s request to cover Chicago PD officer shortages, police continue to reportedly be summoned to headquarters where they are given one last on the spot ultimatum: submit to last week’s vaccine status order or be relieved from duty without pay.
So far the city says it’s not yet going after street patrol officers, which is obviously on fears of a coming crime wave that will hit an already understaffed notoriously high-crime city.
BBC has compiled recent statistics as the standoff over the vax mandate continues:
Chicago, a city of nearly three million people, has seen more than 1,600 sexual assaults, nearly 3,000 shootings and 649 murders this year – a 14% increase over last.
Just as violent crimes have risen, though, thousands of the city’s police force may not show up to work.
… Nearly one-third of Chicago’s almost 13,000-member police department have so far refused to register their vaccination status, putting them on track for dismissal. Twenty-one have been officially removed from active duty so far, but some officials have warned that the mandate could leave Chicago’s police force dangerously depleted.
Adding fuel to the fire of the crisis, President Joe Biden during his CNN Town Hall remarks Thursday night continued pushing his view that emergency responders should be fired for defying local vaccine mandates.
The president even appeared to mock those rejecting vaccine mandates on the basis of “freedom”…
“I have the freedom to kill you with my COVID,” Biden said, mocking what he sees as the attitude of mandate opponents. “No, I mean, come on, freedom.”
Meanwhile the head of Chicago’s largest police union, John Catanzara, is still urging officers to hold the line, despite a weekend gag order imposed on him by the city.
“It is the city’s clear attempt to force officers to ‘Chicken Little, the sky is falling’ into compliance,” he’s recently urged the union’s 11,000 members. “Do not fall for it. Hold the line.”
Millions Of Americans Are Getting Fired For Not Taking A Jab That’s Now 3% Effective
By Chris Menahan | InformationLiberation | October 19, 2021
CNN is reporting that a new study involving over 600,000 veterans has found that Johnson & Johnson’s covid vaccine’s protection “fell from 88% in March to 3% in August.”
“A study published Thursday reported a steep decline in vaccine effectiveness against infection by August of this year, especially for people who received the J&J vaccine,” CNN reported over the weekend. “The researchers found that among more than 600,000 veterans, J&J’s vaccine’s protection fell from 88% in March to 3% in August.”
As there are no requirements (yet) that people be triple-jabbed — or double-jabbed in the case of J&J’s shot — this means millions of Americans are getting fired for not having taken a shot that’s now 3% effective.
On the flip side, we know from another Israeli study that “vaccinated individuals had 27 times higher risk of symptomatic COVID infection compared to those with natural immunity from prior COVID disease,” as epidemiologist Martin Kulldorff noted.
That Israeli study, which was done between June 1 and August 14, involved only Pfizer recipients.
The new study of vets in America showed that Pfizer’s effectiveness declined to 50% in August from 91% and Moderna’s fell to 64% from 92%. That suggests natural immunity is now more than a hundred times more effective than J&J’s vaccine, yet the federal government and most companies do not even recognize natural immunity as a justification not to get vaxxed.
They insist you take some experimental jab — any jab at all now that the FDA has endorsed mixing and matching vaccines for “boosters” — or get fired from your job.
Meanwhile, the FDA is approving the rollout of boosters despite little to no data showing their effectiveness based off “gut feeling” rather than data.


CDC Director: We may need to update our definition of ‘fully vaccinated’
By Kit Knightly | OffGuardian | October 23, 2021
Yesterday, in a press conference, the director of the CDC warned that they may have to “update” the definition of “fully vaccinated”.
At the virtual presser accompanying the approval of “mix-and-match” booster jabs, Dr Rochelle Walensky told reporters that:
We will continue to look at this. We may need to update our definition of ‘fully vaccinated’ in the future,
The “updated” definition would potentially mean only people who have had the third “booster” shot would be considered “fully vaccinated”, while people who have had the two original shots are no longer “fully vaccinated”.
Whilst the warning might just be a ploy to scare people into getting their “booster” without forcing them to, it should be noted a revised definition of “fully vaccinated” has already been adopted in other countries.
For example, it is already policy in Israel where, in early September they “updated what it means to be vaccinated,”. You now need a third shot, or else you are no longer considered vaccinated.
We wrote about it at the time, and predicted it would likely spread to the rest of the world.
In fact, figures in the alternate media have been predicting this for a while. See this clip from YouTuber WhatsHerFace back in August:
As for the potential purpose of any “updated definition”, well it would be twofold.
Firstly, it would allow them to maintain control. Forcing people to jump through hoops just to “get back” rights they once took for granted creates an atmosphere that normalises state tyranny.
Secondly, and more cynically, it would allow them to artificially manipulate statistics to flatter the vaccines’ effectiveness whilst hiding any damage they might do.
We already know that, in the US and others, you’re not considered “vaccinated” if you’re only single-jabbed, or double-jabbed for less than two weeks. So any patient infected with “Covid” in that time is considered “unvaccinated”, NOT a “breakthrough infection”.
By redefining “fully vaccinated”, they can turn millions of double-jabbed people back into “unvaccinated” people and stop them from becoming potential “breakthrough infections” and hurting the vaccine effectiveness stats.
This will, in turn, camouflage any excess mortality in those who have had the vaccine, for example due to antibody-dependent enhancement, because all those who die will officially be “not fully vaccinated”.
They’ll likely push it through soon, before this winter’s flu season hits, so any flu deaths can be “unvaccinated covid deaths”.
And for anybody out there who got double-jabbed thinking they were buying their life back, we’re sorry, but we did warn you this would happen.
As Infection Rates for Vaccinated Aged 40-79 Hit Double the Rates in the Unvaccinated, the U.K. Health Security Agency Suggests that Vaccines May Hobble the Immune Response on Infection

By Will Jones • The Daily Sceptic • October 23, 2021
Another week, another Vaccine Surveillance report (now published by the U.K. Health Security Agency (UKHSA), the successor to Public Health England), and with it more worrying news on the vaccine front.
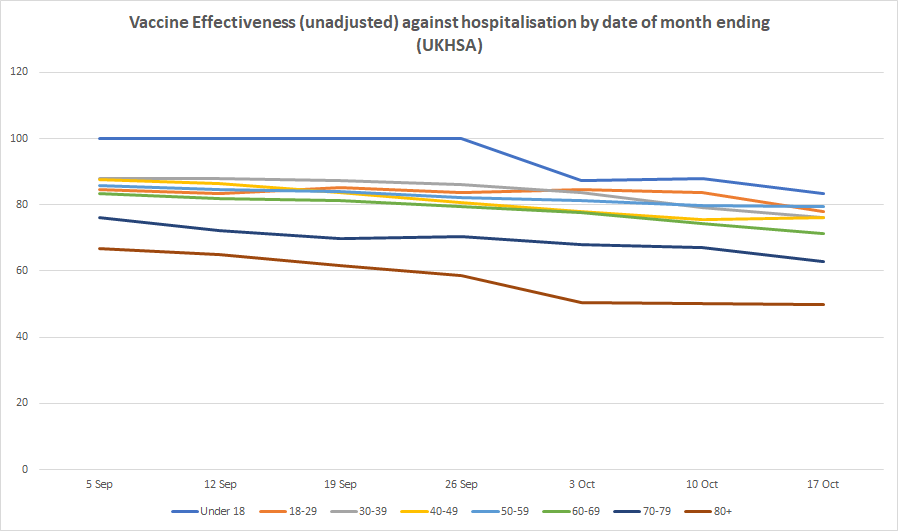
Infection rates in the double-vaccinated compared to the unvaccinated continue to rise, meaning unadjusted vaccine effectiveness continues to decline. Infection rates are now higher in the double-vaccinated compared to the unvaccinated by 124% in those in their 40s, 103% in those in their 50s and 60s and 101% in those in their 70s, corresponding to unadjusted vaccine effectiveness estimates of minus-124%, minus-103% and minus-101% respectively. For those over 80 the unadjusted vaccine effectiveness is minus-34% while for those in their 30s it is minus-27%. For 18-29 year-olds it is 25%, so still positive but low, while for under-18s it is 90%, the only age group showing high efficacy. Vaccine effectiveness against emergency hospital admission and death continues to hold up, though with some indication of gradual slide, particularly in older age groups (see below). (For definitions and limitations, see here.)


The UKHSA has continued to receive criticism for publishing this data, with claims that the figures used for the unvaccinated population are unreliable and likely too high, artificially suppressing the infection rate and vaccine effectiveness. Cambridge statistician Professor David Spiegelhalter put out a scathing tweet on these lines on Friday, but he didn’t elaborate on his claim or link to an article explaining it further.
Professors Norman Fenton and Martin Neil have argued that in fact the PHE/UKHSA data may underestimate the number of unvaccinated rather than overestimate them, which would have the reverse effect.
Either way though, what wouldn’t change is the fact of the large and fast decline in effectiveness against infection. This is now generally acknowledged among many scientists (likely caused by waning over time or new variants or both), though has not had the logical impact on Government policy one might have expected and hoped for of eliminating the rationale for vaccine passports and mandates.
A further point revealed for the first time in this week’s surveillance report is that the vaccines may actually hobble the body’s ability to develop the strongest immunity once infected. As noted by Alex Berenson, the report mentions (in passing) that “recent observations from U.K. Health Security Agency (UKHSA) surveillance data” show that “N antibody levels appear to be lower in individuals who acquire infection following two doses of vaccination”.
The report does not elaborate on this, but on the face of it it is a startling admission. It is basically saying that a certain kind of antibody which is not produced by the vaccines but is usually produced by infection (and hence is used by PHE/UKHSA to identify those with antibodies-from-infection) is not produced so well by those who are infected post-vaccination. Insofar as this is true it means the vaccines may actually prevent the immune system from developing the strongest form of protection against reinfection. This phenomenon of the immune system being in some way hobbled by the way it first encounters a pathogen is well-known and is referred to as original antigenic sin.
There would be a number of implications of this. It would mean that since the vaccine rollout got going the prevalence of N antibodies in the population has ceased to be a reliable measure of how many people are previously infected (which might explain why it has been rising so slowly during the Delta surge). It would also mean the vaccines may make reinfections and serious illness upon reinfection more likely. Plus likely other things as well.
This is something that should be investigated fully and the results published so that its impact can be properly assessed and understood.
White House, CDC Readying COVID Vaccination for 5- to 11-Year-Olds Prior to FDA Authorization
‘This Is Politics, Not Science’
By Megan Redshaw | The Defender | October 20, 2021
The White House today unveiled plans to roll out COVID vaccines for children ages 5 to 11, even though vaccine safety experts — who advise U.S. drug regulators and review safety and efficacy data — have not met to discuss whether Pfizer’s COVID vaccine should be authorized for use in the pediatric age group.
The Biden administration said it will secure enough vaccine doses to vaccinate the 28 million children ages 5 to 11 who would become eligible if the vaccine is authorized for that age group, CNN reported.
The White House will also help equip more than 25,000 pediatric and primary care offices, hundreds of community health centers and rural health clinics as well as tens of thousands of pharmacies to administer the shot.
Jeff Zients, White House COVID-19 response director, said 15 million doses will be ready to ship within a week after the vaccine is authorized, with millions of additional shots coming each week thereafter.
“We know millions of parents have been waiting for [a] COVID-19 vaccine for kids in this age group,” Zients told reporters during a COVID briefing. “And should the FDA and (U.S. Centers for Disease Control and Prevention) authorize the vaccine, we will be ready to get shots in arms.”
Zients said kids have different needs than adults and “our operational planning is geared to meet those specific needs, including by offering vaccinations in settings that parents and kids are familiar with and trust.”
The administration said it is launching a partnership with the Children’s Hospital Association “to work with over 100 children’s hospital systems across the country to set up vaccination sites in November and through the end of the calendar year.”
The administration plans to make vaccination available at school and other “community-based sites” with help from Federal Emergency Management Agency funding.
The U.S. Department of Health and Human Services (HHS) will also carry out a national public education campaign “to reach parents and guardians with accurate and culturally responsive information about the vaccine and the risks that COVID-19 poses to children.”
As has been the case for adult vaccinations, the administration believes trusted messengers — educators, doctors and community leaders — will be vital to encouraging vaccinations, according to U.S. News & World Report.
The White House began laying the groundwork with states earlier this month, asking governors to enroll pediatricians and other providers in vaccination programs so they could start administering shots as soon as they were ready.
“In the era of Delta, children get infected as readily as adults do, and they transmit the infection as readily as the adults do,” Dr. Anthony Fauci, White House chief medical advisor, told reporters Wednesday. “We may not appreciate that, because about 50% of the infections in children are asymptomatic.”
According to the American Academy of Pediatrics, less than 2% of children known to be infected by the coronavirus are hospitalized, and less than 0.03% of those infected die.
As The Defender reported in June, experts testifying before the FDA, when it was considering authorizing Pfizer’s vaccine for 12- to 15-year-olds, argued the risks did not outweigh the benefits, even for that older age group.
Vaccinating children for the benefit of adults is an “unproven hypothetical benefit,” Peter Doshi, Ph.D., associate professor University of Maryland School of Pharmacy and senior editor of The BMJ, told the FDA.
Doshi reminded FDA officials they cannot authorize or approve a medical product in a population unless the benefits outweigh the risks in that same population.
“If the FDA does not have a high bar for EUAs [Emergency Use Authorization] and licensing, the point of regulation is lost,” Doshi said.
Vaccine advisers to the FDA aren’t scheduled to meet until Oct. 26 to consider Pfizer’s request to authorize its vaccine for children ages 5 to 11. In the meeting, the advisers will review the companies’ data and FDA’s own assessment, then vote on whether the FDA should grant EUA.
The CDC will convene its committee of independent vaccine experts on Nov. 2 and 3 to set official recommendations for the vaccine’s use.
If authorized, this would be the first COVID vaccine for younger children. The Pfizer-BioNTech vaccine is currently approved for people age 16 and older and has emergency authorization for children ages 12 to 15.
CDC issues guidance on administering Pfizer-BioNTech vaccine to kids ahead of meeting
The White House isn’t alone in making plans to vaccinate 5- to 11-year-olds official in advance of the vaccine being authorized for that age group. The CDC last week issued guidance outlining key aspects of a COVID vaccination program for children younger than 12 years old “designed to inform jurisdictional planning under the assumption of FDA authorization and CDC recommendations of at least one COVID-19 vaccine product for children of this age.”
The CDC’s “Pediatric COVID-19 Vaccination Operational Planning Guide” includes details about the anticipated Pfizer-BioNTech vaccine — though it may be updated as other manufacturers submit applications for FDA review — and is based on “current facts and planning assumptions.”
In the document, the CDC lays out the differences between the pediatric vaccine and adult vaccine, gives detailed product configuration and provides a distribution strategy.
In addition, the CDC informed providers the Public Readiness and Emergency Preparedness (PREP) Act and PREP Act Declaration issued by the HHS Secretary “authorize and provide liability protections to licensed providers and others identified in the declaration to administer COVID-19 vaccines authorized by FDA, including COVID-19 vaccines authorized for administration to children.”
Beginning Oct. 20, states and other jurisdictions will be able to preorder doses of the Pfizer-BioNTech COVID vaccine formulated for children ages 5 to 11, according to the CDC’s federal planning document. The orders are in anticipation of a rollout that could begin as early as Nov. 3.
The CDC said jurisdictions should be ready to vaccinate children 5–11 years old shortly thereafter pending FDA authorization and CDC recommendation.
“By the White House already purchasing 65 million pediatric doses of the Pfizer-BioNTech vaccine, and the CDC putting out guidelines ahead of FDA authorization — let alone, a recommendation by its own Advisory Committee on Immunization and Practices — these actors are revealing the whole vaccine regulatory process to be a complete sham,” said Mary Holland, president of Children’s Health Defense in an email to The Defender.
“There could be no better way to undermine public confidence than to make it clear that this is politics, not science.”
Megan Redshaw is a freelance reporter for The Defender. She has a background in political science, a law degree and extensive training in natural health.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
FDA and CDC Ignore Damning Report that over 90% of a Hospital’s Admissions were Vaccinated for Covid-19
By Aaron Siri | October 17, 2021
A concerned Physician Assistant, Deborah Conrad, convinced her hospital to carefully track the Covid-19 vaccination status of every patient admitted to her hospital. The result is shocking.
As Ms. Conrad has detailed, her hospital serves a community in which less than 50% of the individuals were vaccinated for Covid-19 but yet, during the same time period, approximately 90% of the individuals admitted to her hospital were documented to have received this vaccine.
These patients were admitted for a variety of reasons, including but not limited to COVID-19 infections. Even more troubling is that there were many individuals who were young, many who presented with unusual or unexpected health events, and many who were admitted months after vaccination.
One would think that after an association was identified by a healthcare professional, our health authorities would at least review this finding, right? Sadly, when Ms. Conrad reached out to health authorities herself, she was ignored. My firm then sent a letter to the CDC and FDA on July 19, 2021 on Ms. Conrad’s behalf (see letter below), yet neither agency has responded. Even worse, when doctors came to Ms. Conrad for assistance with filing VAERS report for their patients, the hospital prohibited her from filing these reports.
That the CDC and FDA failed to respond is arguably not surprising – they have been cheerleading this vaccine for months. Admitting almost any harm now would be akin to asking them to turn a gun on themselves.
This again highlights the importance of never permitting government coercion and mandates when it comes to medical procedures.
Full letter to the CDC and FDA:

Letter exchange with the hospital:

In-depth interview with Ms. Conrad on the Highwire:

Featured Video

Fear Is the Mind Killer
or go to
Aletho News Archives – Video-Images
From the Archives
Alarmist climate science as a textbook example of groupthink
By Paul MacRae | May 1, 2012
A while ago, I received an email from a friend who asked:
How can many, many respected, competitive, independent science folks be so wrong about [global warming] (if your [skeptical] premise is correct). I don’t think it could be a conspiracy, or incompetence. … Has there ever been another case when so many ‘leading’ scientific minds got it so wrong?
The answer to the second part of my friend’s question—“Has there ever been another case where so many ‘leading’ scientific minds got it so wrong?”—is easy. Yes, there are many such cases, both within and outside climate science. In fact, the graveyard of science is littered with the bones of theories that were once thought “certain” (e.g., that the continents can’t “drift,” that Newton’s laws were immutable, and hundreds if not thousands of others).
Science progresses by the overturning of theories once thought “certain.” … continue
Blog Roll
 Aletho News
Aletho News- Iran consolidates Strait of Hormuz control in post-war power shift, leaving US in dark
- A pause, not a ceasefire: Washington stalls, Tehran recalibrates
- US blockade crumbles as Iran turns to overland routes
- Hidden costs of US Iran war push total far beyond $25bn Pentagon claim
- Iran Will Respond With Long-Term Strikes to US Attack, Even If It Is Short-Term – IRGC
- Fear Is the Mind Killer
- Israeli strikes kill 10 in southern Lebanon, including 3 rescue workers
- Israeli military ‘failed on all fronts’: Poll
- US at a crossroads: Iran’s firm positions leave Trump no option but to capitulate
- Iran signals decisive response to end US maritime bullying, piracy
- If Americans Knew
- Politico’s powerful parent company tells Politico they must support Israeli narrative
- How Tony Dokoupil Became the Face of ‘Zionist Fanatic’ Bari Weiss’s CBS
- Far Right Israeli Settler Movement Enters Syria in a Push for “Greater Israel”
- ‘People Have the Right to Be Buried’: In Gaza, Thousands of Palestinians Remain Trapped Under Rubble
- Born during Israel’s genocide: Gaza’s child survivors bear the scars of war
- Who are the women and girls behind Gaza war’s horrific casualty toll?
- Beloved Gaza doctor detained “indefinitely” without charge – Daily Update
- By Week’s End, Trump’s War Will Be Plainly Illegal
- CBS News Reportedly Ousts London Bureau Chief Over Differences With Bari Weiss Over Gaza Coverage
- State Department Says US Is in Conflict With Iran ‘At the Request’ of Israel
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
