COVID Vaccine Mandates Are Killing Aviation, Healthcare, Other Critical Services. Is It Intentional?
The Defender | October 15, 2021
The widespread hemorrhaging of experienced public- and private-sector employees — a “man-made disaster of historic proportions,” according to former U.S. Rep. Ron Paul — is hollowing out some of the most important public-facing professions in the country.
Although many factors are at play, COVID vaccine mandates are a significant contributor, with employers refusing to honor the option to refuse Emergency Use Authorization COVID vaccines that the U.S. Food and Drug Administration (FDA) supposedly guaranteed.
The result has been the threatened or actual mass firing and resignation of thousands of unvaccinated workers in critical sectors like healthcare, policing, firefighting, education and aviation, with skilled and experienced workers prepared to “leave if that’s what it comes to” rather than take the risky shots.
Even though these departures are “drastically overwhelming employers’ ability to replace them,” many of the politicians and corporate executives pushing the mandates seem weirdly at ease with their policy.
This complacency begs the question: Is the sabotage of air travel, high-quality healthcare, first-responder capability and other core services an intentional step designed to further weaken Americans’ resilience and expand authoritarian controls?
Flying the friendly skies
In one of the most widely publicized recent examples of workforce havoc, Southwest Airlines had to ground 35% of its scheduled flights this past holiday weekend, less than a week after the carrier mandated COVID vaccines for all employees.
The airline’s feeble explanation — bad weather and other problems — left many stranded passengers “confounded … because weather was clear over most of the country, particularly near airports that had lots of delays and cancellations.”
As Paul wryly noted, “the weather problems that Southwest claims to be experiencing seem unique to that carrier.”
In “methinks they doth protest too much” fashion, the airline, the pilots union and the Federal Aviation Administration (FAA) are telling the public that the flight upheaval had nothing to do with employee ire over the vaccine edict.
However, one news report indicated that on the Friday in question, only three of 35 pilots showed up for work at Southwest’s Jacksonville hub, suggesting the pilots — at least 50% of whom are unvaccinated — are “drawing a line in the sand.”
Other major airlines that have imposed mandates — JetBlue, American, United, Alaska, Frontier and Hawaiian Airlines — are also facing fierce employee pushback.
The Southwest Airlines Pilots Association has gone so far as to criticize the company’s mandate as a “bad move,” stating pilot fatigue is already at triple its historic levels, with flights “operating at a higher than normal operational risk.”
Seeking to reassure its employees, Southwest CEO Gary Kelly told ABC News in an interview after the travel kerfuffle, “we’re not going to fire any employees over this [vaccine mandates].” Kelly said Southwest would urge unvaccinated employees to “seek an accommodation.”
Certainly, further outflows of competent personnel unwilling to be jabbed would exacerbate understaffing problems — and increase airline customer risks.
Adverse events in mid-air?
Commercial airline executives and pilots would be well-advised to read the affidavit submitted in late September by Lt. Col. Colonel Theresa Long, M.D., brigade surgeon for the 1st Aviation Brigade in Ft. Rucker, Alabama. Long is “responsible for certifying the health, mental and physical ability and readiness for … nearly 4,000 individuals on flight status.”
The affidavit highlights serious concerns about vaccinated pilots’ fitness for duty in light of myocarditis and other cardiac risks linked to COVID injections — problems that potentially could cause pilots to die in mid-flight.
Military aviators, Long points out, must meet “the most stringent medical standards” in the entire military to be eligible for flight status. In the private sector, heart problems can cause pilots to lose their commercial airline license.
In Long’s view, it is highly likely that “all persons who have received a COVID-19 Vaccine are damaged in their cardiovascular system in an irreparable and irrevocable manner.”
Noting that she has ascertained development of “significant and aggressive systemic health issues” in multiple flight crew members within 48 hours of vaccination, Long described one particularly alarming case:
“I personally observed the most physically fit female soldier I have seen in over 20 years in the Army, go from collegiate-level athlete training for Ranger School, to being physically debilitated with cardiac problems, newly diagnosed pituitary brain tumor [and] thyroid dysfunction within weeks of getting vaccinated.”
Other military physician-colleagues, Long said, are also reporting “firsthand experience with a significant increase in the number of young soldiers with migraines, menstrual irregularities, cancer, suspected myocarditis and reporting cardiac symptoms after vaccination.”
For young and fit pilots, the conclusion is obvious: COVID vaccines “are more risky, harmful and dangerous than having no vaccine at all,” Long said.
Many members of the military have apparently reached similar conclusions. With only 62 deaths attributed to COVID during the entire pandemic — out of 2.1 million troops — hundreds of thousands of service members are not in compliance with the U.S. Department of Defense’s Nov. 2 deadline to be fully vaccinated.
In February, a poll found that 53% of active-duty personnel, spouses and veterans had no plans to get injected.
Long said military flight crews present “extraordinary risks,” not just to themselves, but also to others “given the equipment they operate, munitions carried thereon and areas of operation in close proximity to populated areas.”
Her recommendations? “[A]ll pilots, crew and flight personnel in the military service who … received any COVID-19 vaccination [should] be grounded” and the “[c]ompulsory SARS-CoV-2 mRNA vaccination program should be immediately suspended.”
Where are we headed?
Far from being receptive to the attempts by Long and at least 15 of her colleagues to share their disturbing observations with military superiors, the physicians say they are being ignored, rejected, ostracized or met with “threats of punishment.”
Long therefore issued her affidavit under the Military Whistleblower Protection Act, fully cognizant of the “horrific repercussions” her whistleblowing may have on her “career, [her] relationships and life as an Army doctor.”
The Ft. Rucker brass’s lack of interest in the impact of the experimental vaccines on pilot health is puzzling in light of Government Accountability Office (GAO) analyses showing there are already acute shortages of military pilots.
In late September, Texas Rep. Dan Crenshaw reminded the secretary of defense that military readiness is subpar and tweeted, “are you really willing to allow a huge exodus of experienced service members just because they won’t take the vaccine?”
With the U.S. mired in “the worst … healthcare labor crisis in memory,” the same question could be directed to hospital CEOs who seem willing to let go of sizeable proportions of employees — even if it means adopting drastic measures such as refusing patients, closing departments or leaving beds empty.
Fed up, 96% of union members working at Kaiser Permanente in California and Oregon just voted to go out on strike.
Notably, hospitals earned record windfall profits last year from COVID federal stimulus and Medicare add-ons for ventilator intervention, even as they furloughed, laid off or cut the pay of frontline health workers in the midst of a “pandemic.”
And this year, politicians like New York’s unelected governor seem blithely willing to let the experienced health workers who took those furloughs and pay cuts go, bringing in pinch-hitting National Guard members or imported foreign workers.
It may still be too soon to untangle the full array of corporate and political interests driving the counterproductive policies that are chasing out large swaths of competent health workers, first responders, aviation workers and service members — while demoralizing (or sickening via COVID injection) those who comply with mandates and remain.
One thing is for sure, however: COVID-19 vaccines increase the risk of blood clots and so does air travel, which could make flight personnel especially vulnerable. Members of the public who take to the skies would surely rather have an experienced unvaccinated pilot who is of the caliber of a Chesley “Sully” Sullenberger in the cockpit — rather than a “second-string” vaccinated pilot who could be at higher risk of dying in mid-flight.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Infection Rate in Vaccinated People in Their 40s Now More Than DOUBLE the Rate in Unvaccinated, PHE Data Shows
Vaccine Effectiveness Hits Minus-109%

By Will Jones • The Daily Sceptic • October 15, 2021
In the latest Vaccine Surveillance report from Public Health England (PHE) the infection rate in double-vaccinated people in their 40s went above 100% higher than in the unvaccinated for the first time, reaching 109%. This translates to an unadjusted vaccine effectiveness of minus-109%.
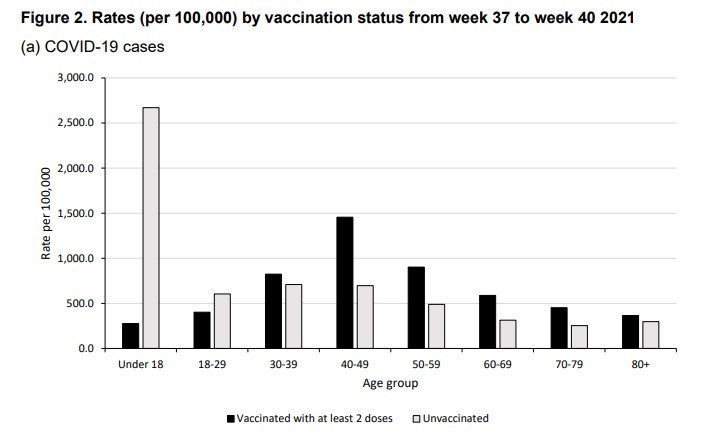
Vaccine effectiveness continues to drop fast in all over-18s (see chart at top), hitting minus-85% for those in their 50s, minus-88% for those in their 60s and minus-79% for those in their 70s. (For definitions and discussion of limitations see here.)

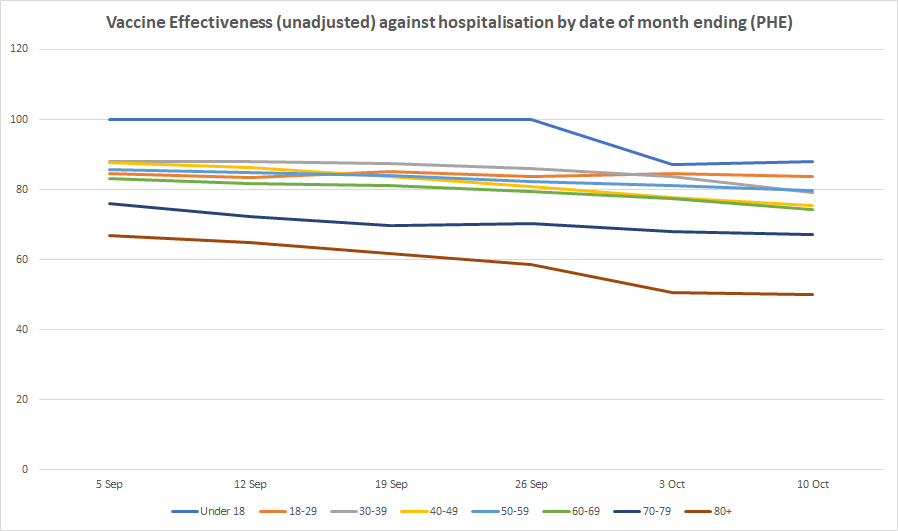
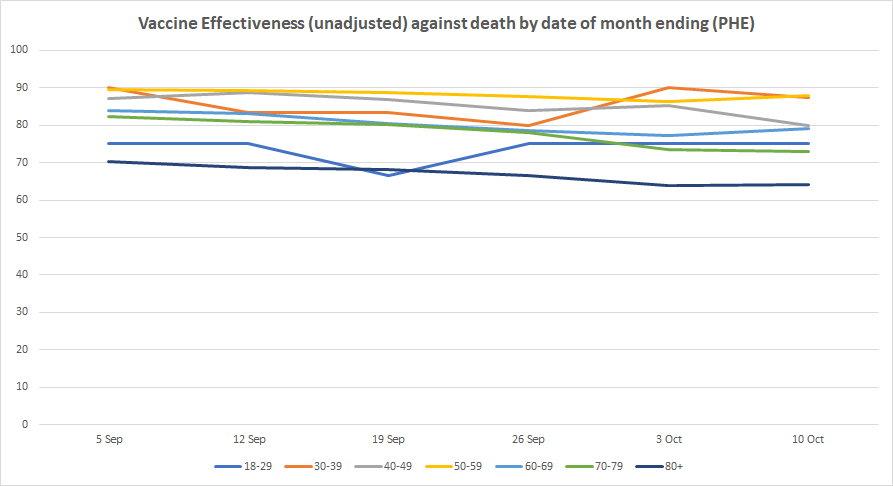
Vaccine effectiveness against hospitalisation and death continues to hold up in all age groups, though with some signs of decline, particularly among older people.
There is still nothing from Government sources acknowledging this failure of the vaccines against infection, its implications for policy and analysing what might be behind it.
Australian Doctors Are Complicit In Experimentation On The Population
By Dr. Judy Wilyman | Principia Scientific | October 16, 2021

It is the ‘education’ and regulation of doctors that is preventing doctors from practising medicine with integrity in 2020-21.
The Government Therapeutic Goods Administrator (TGA) of Drugs/Vaccines in Australia states that COVID19 vaccines are:
- Experimental and include new untested genetic technology. Hence these drugs only have provisional approval and are not full approved for use in humans.
- The vaccines are not safe. Millions of injuries have been recorded by global government regulators including – anaphylaxis, thrombosis, and coagulation disorders (blood clots), infertility, heart problems (myocarditis and pericarditis), neurological damage (cognitive decline), strokes, paralysis, convulsions, seizures and well over 100,000 deaths.
- There are on average more deaths per day due to the COVID vaccines than to COVID-19 disease itself.
- The vaccines are ineffective – they do not prevent you getting or dying from COVID-19 disease, and they do not prevent transmission of the virus in the community. Hence, they are a drug and not a ‘vaccine’ under the WHO’s definition of a vaccine.
- They have only been tested to see if they reduce the symptoms and not to see if they prevent disease.
- They are unnecessary because 99.9% of people under 70 develop immunity through mild or asymptomatic infection. Our immune system develops natural herd immunity in the community through this exposure and the most detrimental action that any government can take is to quarantine healthy asymptomatic people. This hinders the control of infectious diseases in the community. Hence, Sweden did not lockdown its population and the WHO did not provide any evidence that asymptomatic people were a risk to the community in March 2020 when they used this strategy for the first time in history.
- The injection is not specific for COVID-19 disease and the synthetic spike protein that is produced by our cells upon exposure to any coronavirus is toxic to the human body. This includes the development of autoimmune diseases, blood clots and infertility.
Did you see this information reported in the mainstream media? No. Welcome to 2021 where the medical-industry uses framed and manipulated statistics, emotional labels, and anecdotal evidence in the mainstream media to inform you about any drug that they have labelled a ‘vaccine.’
The removal of both scientific evidence and balanced discussion of vaccines in the media has occurred over decades, and we now have a situation where labels and biased information are being used to manipulate your thinking about these drugs. Drugs that are being mandated for HEALTHY people in genetically diverse populations.
This fraudulent promotion of a medical intervention was cemented in 2009 when a government board was set up in Australia to regulate doctors on the “accepted” science for vaccine promotion.
This Federal government agency is called the Australian Health Practitioners Regulatory Authority (AHPRA) and it is both a government agency and an Australian incorporated business (ABN 78 685 433 429).
In other words, this board controls the knowledge doctors can promote on vaccines and it influences the design and promotion of government vaccination policies. This board has the power to de-regulate doctors and health professionals who make a different risk assessments of vaccines to that provided by this government regulatory board.
Medication for healthy people affects their quality of life and it is doctors who are trained to assess the medical literature for risks and benefits. The AHPRA board has a serious conflict of interest in the regulation of doctors’ knowledge on vaccines, and doctors cannot speak the truth to power if they can lose their livelihoods for doing so.
The risks of vaccines associated with our genetics are now being described as “antivaccination material” and doctors are threatened with de-registration by AHPRA for providing this medical literature to their patients. This includes contraindications to vaccines that have been practiced for 40+ years but have now been arbitrarily removed.
Hence, doctors are now violating the first principle of medicine because they cannot promote their patients best interest first. That is, drugs/vaccines must be given to individuals with advice regarding their own individual circumstances and genetics. This is a key factor in health outcomes with respect to drugs and when this is violated doctors are no longer promoting health in the community. They are promoting sickness and death because many illnesses are linked to our family history and genetics.
The Australian government has now indemnified doctors to give these experimental injections to their patients – injections that are documented to cause serious known and unknown harm in patients. Taxpayers (we) will be paying for our doctors to inflict this harm (and death) on patients without fully informed consent due to government mandates that remove our jobs and right to travel if we refuse.
Over the last few decades doctors have been “educated” in pharma-funded medical schools with industry-funded science. They are taught that anyone who discusses the ingredients of vaccines (drugs) or the serious risks of vaccines, is an “antivaxxer” and a “conspiracy theorist”. This same opinion is provided to the public in the corporate-sponsored mainstream media to denigrate any scientific discussion of the risks of these drugs that are given to healthy people.
Mainstream media has always been a tool to manipulate public behaviour and when the US Congress removed liability from pharmaceutical companies for any harm caused by any drug labelled a “vaccine” in 1986 (because they were paying millions of dollars in compensation for deaths and injuries), this enabled big pharma to minimise the risks of these drugs and to exaggerate the benefits (“life-saving products”) – without providing evidence for these claims.
In 2021 this dismissive ridicule by authorities reached a new low when the Western Australian Premier, Mark McGowan, disrespectfully told ~5,000 WA parents and grandparents at a rally opposing mandatory jabs for jobs, to “Grow a brain” and he stated that “this is about medicine and saving lives”. This statement by this Premier is simply untrue when you ignore the genetics of the population.
High school science students can tell the Premier that a mandatory drug/vaccine, in a genetically diverse population, will cause death and sickness in a significant proportion of the population. Mark McGowan should be removed from his role as Premier for his contempt for the people he serves and for putting the public’s lives are risk with false health information.
Politicians, media, and doctors are using labels to convey a ‘belief’ about vaccines and to stigmatise critical thinking, and this is done without providing any supportive evidence for the implied meanings the words are given. This strategy has been used to support the expansion of national vaccination programs from 1986 – 2021.
Since 1986 ‘beliefs’ that are not evidence-based have been promoted by the media, politicians and doctors by using the following words to promote public health policy:
Vaccines – drugs that have ‘rare’ side-effects and are ‘necessary to control infectious diseases.’ Both claims are untrue.
Infectious diseases – re-labelled as ‘vaccine-preventable diseases’ since 1986 to imply that they can be prevented with a vaccine.
Vaccination programs – falsely labelled as ‘immunisation programs.’ It is known that many vaccinated people do not get immunity after a vaccine is given and they still get the disease.
Catch-Up Schedules – They are not catch-up schedules because most older Australians did not have these vaccines and were never at risk from these diseases.
Antivaxxer – a derogatory term used to describe an educated parent/professional that discusses the risk-benefit analysis of vaccines or ingredients of vaccines. Knowledge of these criteria are necessary to promote ‘healthy’ outcomes from vaccines, yet they are ridiculed.
Conspiracy Theory – derogatory term used to dismiss the serious conflicts of interest in every aspect of global health policy designed by the WHO/GAVI alliance and national vaccination policies designed by governments.
This is a political situation, and it is the influence of corporate money in the political and economic decisions of governments that has led to doctors, governments and the media collaborating to commit a serious crime against their populations by falsely advertising an experimental genetic technology as a ‘vaccine’.
People, including health professionals, are walking into their own deaths and illnesses, due to the false and misleading health information that is being provided by the powerful medical-industry complex to politicians.
This corporate health model has monopolised doctors, industry-funded research institutions, politicians, and the mainstream media to educate the public with ignorance about the risks of vaccines. A situation described as agnotology in the academic literature and if doctors were not gagged by AHPRA (their government/corporate regulatory board) it would not have been possible to violate their medical ethics and commit this crime against humanity that will destroy the genetic fabric of society.
I cannot do it anymore

In an open letter, an employee of German public broadcaster ARD is critical of one and a half years of Corona coverage: Ole Skambraks has worked as an editorial assistant and editor at the public broadcaster for 12 years.
BY OLE SKAMBRAKS | multipolar magazine | 14. Oktober 2021
I can no longer remain silent. I can no longer silently watch what has been going on for a year and a half now within my organization, a public service broadcaster. Things like “balance”, “social cohesion” and “diversity” in reporting are principles embedded in the statutes and media state contracts. Today, the exact opposite is happening. There is no true discourse and exchange in which all parts of society can come together and find common ground.
From the beginning, I felt that public service broadcasting should fill precisely this space: promote dialogue between advocates of measures and critics, between people who are afraid of the virus and people who are afraid of losing their basic rights, between vaccination supporters and vaccination sceptics. For the past year and a half, however, the space for discussion has narrowed considerably.
Scientists and experts who were respected and esteemed before Covid, who were given space in public discourse, are suddenly labelled cranks, tinfoil hat wearers or Covidiots. As an oft-cited example, consider Wolfgang Wodarg, a medical specialist in several fields, an epidemiologist and a long-time health politician. Until the Covid crisis, he was also on the board of Transparency International. In 2010, as Chair of the Council of Europe Health Committee, he exposed the influence of the pharmaceutical industry in the swine flu pandemic. At that time, he was granted the opportunity to express his opinion on public service broadcasting, but in times of Covid this is no longer possible. His voice has been replaced by that of so-called fact-checkers, who seek to discredit him.
Paralysing consensus
Instead of an open exchange of opinions, a “scientific consensus” was proclaimed, that must be defended. Anyone who doubts this and demands a multidimensional perspective on the pandemic, will reap indignation and scorn.
The same pattern is at work in the newsrooms. For the last one and a half years, I have no longer been working in the daily news business, which I am pleased about. In my current position, I am not involved in decisions about which topics are treated and how. Here, I describe my impressions from editorial conferences and an analysis of the reporting. For a long time I did not dare to leave the role of observer, the supposed consensus seemed too absolute and unanimous.
For a few months, I have been venturing out onto the ice, making some critical remarks here and there in conferences. This is often followed by a shocked silence, sometimes a “thank you for pointing it out” and every so often a lecture on why it is not true. This has never resulted in any reporting.
The result of one and a half years of Covid-19 is an unparalleled division in society. Public service broadcasting has played a major role in this. It is increasingly failing in its responsibility to build bridges between the camps and to promote exchange.
It is often argued that the critics are a small, negligible minority, which, for reasons of proportionality, cannot be accommodated to any great extent. This argument should have been retired at least with the Swiss referendum on Covid-19 measures. Despite the lack of free exchange of opinions in mass media in that country too, the votes cast went only 60:40 in favour of the government. (1) With a proportion of 40%, can you talk about a small minority? It also turned out that the Swiss Government had tied Covid-related financial support to the vote, which might have influenced some to tick “Yes” on the ballot.
The developments of the Covid crisis are taking place on so many levels, affecting all parts of society, and thus we clearly need more space for a free debate – certainly not less.
In this context, it is less revealing which topics are being discussed in public service media, than what is not being discussed. The reasons for this are many and need to be subject to honest internal scrutiny. It could be helpful to look at some titles published by the media scientist and former MDR broadcasting adviser Uwe Krüger, for example his book “Mainstream – Warum wir den Medien nicht mehr trauen” (“Mainstream — why we no longer trust the media”).
In any case, it takes courage to swim against the current in conferences where such topics are discussed. Often those who can put forward their arguments in the most eloquent way will get their message across but, if in doubt, the editorial team will decide, of course. Very early on, those critical of the Government’s Covid-19 measures were labelled right-wingers. Which editor will still dare to voice similar ideas?
Open questions
Thus the list of inconsistencies and open questions, which have gone largely unreported, is very long:
- Why do we know so little about “gain of function research” (which aims at making viruses more dangerous to humans)?
- Why does the new Infection Protection Act state that the basic right to bodily integrity and the inviolability of one’s home may be restricted henceforth – even without an epidemic situation?
- Why must people who have already had Covid-19 still get the jab, even though they are at least as well protected as those who are vaccinated?
- Why are we not talking about ”Event 201” and the global pandemic exercises held shortly before the spread of SARS-CoV-2 — at all, or only in the context of conspiracy theories? (2)
- Why was the internal document from the German Federal Ministry of the Interior — a document which was known to the media and in which the authorities were asked to create a “shock effect” to underscore the impact of the Covid-19 pandemic on human society — not published in full and discussed publicly?
- Why is the study by Professor Ioannidis on survival rates (99.41% for people under 70) not featured in the headlines, while the fatally flawed, inflated figures produced by Imperial College were (in the spring of 2020, Neil Ferguson foresaw half a million Covid-19 deaths in the United Kingdom and more than 2 million in the United States)?
- Why does it say, in a document produced for the German Federal Ministry of Health, that Covid-19 patients stood for no more than 2% of the burden of hospitals during 2020?
- Why does Bremen have the by far the highest incidence (113 as at 04/10/21) and at, the same time, by far the highest vaccination rate in Germany (79%)?
- Why were payments of 4 million euro paid into a family account belonging to EU Health Commissioner Stella Kyriakides, who was responsible for concluding the first EU vaccine contracts with pharmaceutical companies? (3)
- Why are people suffering severe vaccine injury not featured to the same extent as people with severe Covid-19 disease were in 2020? (4)
- Why is no one disturbed by the irregular way of counting “breakthrough infections” in vaccinated people? (5)
- Why does the Netherlands report clearly higher volumes of side effects of the Covid-19 vaccines than other countries?
- Why has the efficacy description of the Covid-19 vaccines published on the Paul-Ehrlich-Institut website been changed three times in the last few weeks? From “Covid-19 vaccines protect against infection with the SARS-CoV-2 virus” (on 15 August 2021), via “Covid-19 vaccines protect against severe forms of infection with the SARS-CoV-2 virus” (on 7 September 2021), to, finally, “Covid-19 vaccines are indicated for active immunization to prevent the Covid-19 disease caused by the SARS-CoV-2 virus” (on 27 September 2021). (6)
A couple of these points warrant a closer look.
“Gain of function” and “Lab leak”
As for “gain of function research” — research aiming at making viruses more dangerous, as was done at the Institute of Virology in Wuhan, China, and financed by the United States — so far, I have not heard or read anything substantial. This type of research is done in so-called Biosafety Level 4 Laboratories, where work has been carried out for decades to see how animal viruses can be altered to make them dangerous to humans as well. So far, ARD and ZDF have given this topic a wide berth — despite the obvious need for a debate. One question worth exploring could be: Do we, as a society, want such research to be carried out?
There are numerous reports on the “lab leak theory” – the assumption that SARS-CoV-2 originated in a lab. It is worth noting that last year, this idea was immediately labelled a conspiracy myth. Alternative media investigating this were banned from social media such as YouTube and Twitter and the information was deleted. Scientists who supported this theory found themselves under massive attack. Today, the “lab leak theory” is at least as plausible as the bat transmission theory. The American investigative journalist Paul Thacker published the results of his meticulous research in the British Medical Journal. Commenting on this, Dr. Ingrid Mühlhauser, professor of health sciences at Hamburg University writes:
“Step by step, he [Thacker] reveals how members of an American lab group deliberately concocted a conspiracy theory to disguise their lab accident at Wuhan as a conspiracy theory. This myth is supported by respected journals such as The Lancet. Science journalists and fact-checker services accept the information without any reflection. Participating scientists keep mum, either out of fear, or to avoid running the risk of losing their standing or research grants. For more than a year now, Facebook has blocked posts that question the natural origin of SARS-CoV-2. If the lab accident theory is confirmed, then ZDF and other media will have defended conspiracy theories.”
Ivermectin and alternatives to vaccination
For months now, it has been clear that effective and cheap treatments do exist for Covid-19, but their use is not allowed. The data on this is unequivocal. But the pseudoscientific disinformation campaigns against these medications are indicative of the state of medicine today. Hydroxychloroquine is a drug known for decades and used routinely against malaria and rheumatic disorders. Last year, the drug was suddenly deemed dangerous. The statement by then-President Donald Trump that hydroxychloroquine would be a “game changer” did the rest to discredit the medication. The political reasoning no longer allowed a scientific debate on HCQ.
In the spring, the catastrophic situation in India caused by the spread of the Delta variant was widely reported in the media (then still referred to as the Indian variant). But the fact that India rather quickly brought the situation under control, and that the use of Ivermectin in large states such as Uttar Pradesh had a decisive role in this, was not deemed newsworthy. (7)
Ivermectin was granted a temporary authorisation in the Czech Republic and Slovakia for treating Covid-19 patients. This was at least reported by the MDR, albeit with a negative slant.
In its report on possible medications, Bayerischer Rundfunk failed to even mention Ivermectin. As for hydroxychloroquine, only negative studies were cited, omitting all studies with positive results.
In the summer of 2020, lab tests showed that the molecule Clofoctol was also effective against SARS-CoV-2. Until 2005, the antibiotic drug was sold in France and Italy under the commercial names of Octofene and Gramplus. The French authorities repeatedly blocked the Pasteur Institute in Lille from launching a study with Covid-19 patients. At the beginning of September, after several attempts, the first patients were recruited.
Why are the health authorities taking such a strong stand against treatments, which have been available since the beginning of the pandemic? I would have liked to see some investigative research by the ARD here! It has been made clear that the new Covid vaccines could qualify for emergency use authorisation (EUA) only because there was no officially recognised treatment for SARS-CoV-2.
This is not about celebrating any one Covid miracle drug. My aim is to highlight facts which have not been given due consideration. From the outset, the message given in public discourse was that vaccination was the only way out. The WHO even went so far as to change the definition of “herd immunity”, implying that it can only be achieved by vaccination and no longer by previous infection, as was previously the case.
What about if the road chosen is a dead end?
Questions on vaccine efficacy
Data from countries with a particularly high vaccination rate show that infection with SARS-CoV-2 also in fully vaccinated people is more rule than exception. Dr. Kobi Haviv, Director of the Herzog Hospital in Jerusalem, reports that between 85% and 90% of severe cases in his intensive care unit are patients who have had two jabs. (8)
As regards Israel as a whole, the journal Science writes: “On 15 August, 514 Israelis were admitted to hospital with severe or critical Covid-19 disease … out of these 514 persons, 59% were fully vaccinated. Out of those vaccinated, 87% were 60 years or older.” Science quotes an Israeli government adviser, who explains: “One of the great stories coming out of Israel [is]: ‘The vaccines work, but not well enough’.”
It is also now evident that, with the Delta variant, vaccinated people carry (and spread) the same viral load as unvaccinated people.
What has this data situation brought about in Germany? — A lockdown specifically for unvaccinated people or, put somewhat euphemistically: the “2G rule”. In fact, society is being divided into two classes. Vaccinated people regain their freedom (as they do not risk endangering others), whereas unvaccinated people (who do risk endangering others) must undergo tests, and pay for them out of their pocket, and will no longer receive sick pay if quarantined. Moreover, employment bans and dismissals on the grounds of vaccination status are no longer out of the question, and health insurance funds may impose less favourable rates on the unvaccinated in the future. Why this pressure on unvaccinated people? This has no foundation in science and is damaging to our society.
Antibodies produced by vaccination wane after only a few months. A look at Israel shows that after the second jab, there will be a third for the whole population, and then a fourth as recently announced. Those who fail to get a booster shot after six months will lose their status as immune and thus their “Green Pass” (the digital Covid-19 pass introduced in Israel). In the United States, President Joe Biden is talking about Covid-19 booster shots every 5 months. Marion Pepper, immunologist at the University of Washington, questions this strategy, explaining to The New York Times that repeated stimulation of the innate immune response can lead to a phenomenon called “immune fatigue”.
It is a little discussed fact that natural infection allows a person to develop clearly stronger immunity. “Ultrapotent antibodies” or ”super immunity” have been found in people who were infected with SARS-CoV-2 during the last year. These antibodies react against more than 20 different mutations of the virus and remain for longer than antibodies acquired via vaccination.
After all, Health Minister Jens Spahn has now declared that proof of antibodies is also to be accepted. But to be officially recognized as immune you still have to be vaccinated. Who can understand this logic? A CNN interview with Dr. Anthony Fauci, Director of NIAID (under the NIH, the National Health Institutes) clearly illustrates the absurdity of the situation. People with natural immunity are still not a consideration in the minds of the politicians!
I know a physician who is desperately trying to get an answer from the health authorities and the RKI to this problem: One of her patients presents an IgG antibody titer value of 400 AU/ml — clearly more than many vaccinated people. As her Covid-19 infection occurred more than six months ago, she has lost her immune status. The answer was: “Give her the jab!” — which the physician will not do, considering the titer value.
A lack of basic journalistic understanding
The way out of the pandemic touted by our politicians and the media turns out to be a permanent vaccine subscription. Scientists advocating a different Covid approach are not able to reach out via public service media, as demonstrated again by the sometimes defamatory reporting on the video action #allesaufdentisch. Instead of discussing the content of the videos with the parties concerned, experts were sought out to discredit the campaign. By doing this, public service commit the very same error which they hold against #allesaufdentisch.
Der Spiegel journalist Anton Rainer opined in the SWR interview about the video action, that these are not interviews in a classical sense: “In principle you see two people agreeing with each other.” Listening to the reporting by my broadcaster gave me stomach pains, and I was very annoyed by the lack of basic journalistic understanding of the need to let those with opposing views have their say. (9) I made my concerns known to those concerned and the editorial team by email.
A typical comment in conferences is that a topic has “already been covered”. For example, when I brought up the high likelihood of underreporting of vaccine side effects. Yes, sure, the topic was discussed with in-house experts, who – no surprises here – concluded that there was no underreporting. “Opposing views” will be discussed here and there, but are rarely given a human face in such a way that broadcasters actually speak with people who hold critical views.
Critics under pressure
The most vocal critics must count on house searches, prosecution, account suspensions, transfers or dismissal, or even referral to psychiatric care. Even if they hold opinions you do not share — this has no place in a state subject to the rule of law.
In the United States, it is already being discussed whether criticising science should be labelled a hate crime. The Rockefeller Foundation has announced a grant of 13.5 million dollars to censor misinformation in the health field.
WDR television broadcasting director Jörg Schönenborn declared that “facts are facts and they hold true”. If that was so, how is it then possible that scientists behind closed doors argue incessantly and even strongly disagree on some quite basic issues? As long as we are not making that clear, any assumption of supposed objectivity will lead to a dead end. We can only hope to edge closer to “reality” – and that is only possible with open exchange of ideas and scientific knowledge.
What is happening now is no honest fight against “fake news”. Rather, we are left with the impression that any information, evidence, or discussion deviating from the official narrative is suppressed.
A recent example is the factual and scientifically transparent video by IT specialist Marcel Barz. By analysing raw data, Barz was able to establish that the actual figures on excess deaths, hospital occupancy rates as well as infections did not correspond to those gleaned from the media and politicians in the last year and a half. He also demonstrates how you can present a perfect image of a pandemic using such data, and explains why he feels this is dishonest. After three days and 145,000 views, the video was deleted from YouTube (and reinstated only Barz after objected, and many others protested). The stated reason: “medical misinformation”. This begs the question: Who decided this, and on what grounds?
The fact-checker from Volksverpetzer dismissed Marcel Barz as “fake”. The verdict by Correctiv was a bit milder (Barz has given a public and detailed reply). He is proved right by the document produced for the German Federal Ministry of Health, which shows that Covid-19-Patienten stood for no more than 2% of the hospital burden during 2020. Barz went to the press with his analysis but was ignored. In a functioning discourse, our media would invite him for a debate.
Covid-related content has been deleted countless times, as shown by journalist Laurie Clarke in The British Medical Journal. Facebook and similar media are private companies and are thus free to decide what may be published on their platforms. But in doing so, are they also allowed to steer the discourse?
Public service broadcasting could have an important balancing role, by offering an open exchange of opinion. Not so, unfortunately!
Digital vaccine passes and surveillance
The Gates and Rockefeller Foundations drafted and financed the WHO guidelines for digital vaccine passes. These passes are now being rolled out everywhere. Only with these passes will public life be possible – whether you want to take the tram, have a coffee or get medical treatment. An example from France shows that this digital pass will stay even after the pandemic ends. MP Emanuelle Ménard demanded the following addition to the legal text: The digital vaccine pass shall end when the virus spread no longer presents a level of danger which justifies its use. Her proposed amendment was rejected. Thus we are but a small step away from global population control or even a surveillance state via projects such as ID2020.
Australia is currently testing a facial recognition app, to ensure that people stay at home when in quarantine. In Israel, electronic wristbands are used for this purpose. In one Italian city, drones are being tested to measure the temperature of beachgoers, and in France, the law is changed to allow large-scale drone surveillance.
All these topics must be subject to intensive and critical scrutiny within our society. This is not happening to a sufficient extent in the reporting by our broadcasting organisations and, indeed, was not an election campaign issue.
Blinkered vision
The way in which public discourse has been curtailed is indicative of the “gatekeeper of information”. A current example comes from Jan Böhmermann, who demanded that virologists Hendrik Streeck and Professor Alexander S. Kekulé be deprived of their opportunity to speak out, claiming that they were not competent to do so.
Even though the two physicians have very impressive CVs, Böhmermann has thus narrowed the field of vision even more. So, now we cannot even listen to people who present their criticism of government policy wearing kid gloves?
Public discourse has been curtailed so much that Bayerischer Rundfunk has more than once refrained from broadcasting speeches by members of state parliaments who take a critical view of the measures during parliamentary debates.
Is that what the new understanding of democracy looks like in public service broadcasting? Alternative media platforms thrive first and foremost because the established platforms fail to do their job as a democratic corrective.
Something has gone wrong
For a long time, I could say with pride and joy that I work in public service broadcasting. ARD, ZDF and Deutschlandradio have generated outstanding research, formats, and content. The quality standards are extremely high and thousands of staff members are doing great work despite increasing cost pressure and savings targets. But with Covid-19, something has gone wrong. Suddenly, I have become aware of tunnel vision, blinkers and a supposed consensus which is no longer questioned. (10)
The Austrian broadcaster Servus TV is proof that another way is possible. In the programme “Corona-Quartett” / “Talk im Hanger 7” proponents and critics are given equal space. Why is that not possible in German television? (11) “You cannot let every crank take the stage”, is the quick retort. The false balance, giving serious and dubious opinions an equal chance to be heard, must be avoided. — A killer argument, which also happens to be unscientific. The basic principle of science is doubt, questioning, checking. If this does not happen, then science has become a religion.
Yes, there is actually a false balance. It is the blind spot in our heads, which no longer allows true debate. We are throwing around apparent facts, but can no longer listen to each other. Contempt replaces understanding, fighting the opposing view replaces tolerance. The basic values of our society are thrown overboard, just like that. Here we go: People who do not want to get the jab are crazy, there we go: “Shame on the sleeping sheep”.
While we are busy fighting, we fail to notice that the world around us is changing at breakneck speed. Virtually all areas of our lives are being transformed. How this develops is essentially determined by our capacity for cooperation, compassion and awareness of ourselves and our words and deeds. For our spiritual wellbeing, we would do well to open the space for debate – while being mindful, respectful and with understanding of different perspectives. (12)
Writing this, I feel like a heretic — someone who commits high treason and must reckon with being punished. Maybe this is not the case. Maybe I am not actually risking my job, and maybe freedom of opinion and pluralism are not under threat. I really hope so and I look forward to constructive exchange with my colleagues.
Ole Skambraks
ole.skambraks@protonmail.com
About the author: Ole Skambraks, born in 1979, studied Political Science and French at Queen Mary University in London, as well as Media Management at the ESCP Business School in Paris. He was a Moderator, Reporter and Writer at Radio France Internationale, Online Editor and Community Manager at cafebabel.com, Programme Manager of the MDR Sputnik morning show and Editor at WDR Funkhaus Europa / Cosmo. He is currently working as an Editor in Programme Management/Sound Design at SWR2.
Further information from the author
PS: For fact-checkers and people interested in a multi-perspective, here are the counter-positions to the points discussed in the text:
Prof. John Ioannidis
https://www.faz.net/aktuell/wissen/forscher-john-ioannidis-verharmlost-corona-und-provoziert-17290403.html
https://sciencebasedmedicine.org/what-the-heck-happened-to-john-ioannidis/
Imperial College Modelling
https://blogs.bmj.com/bmj/2020/10/07/covid-19-modelling-the-pandemic/
Gain of function research
https://www.gavi.org/vaccineswork/next-pandemic/nipah-virus
Hydroxychloroquin / Ivermectin
https://www.br.de/nachrichten/wissen/corona-malaria-mittel-hydroxychloroquin-bei-covid-19-unwirksam,RtghbZ4
https://www.who.int/publications/i/item/WHO-2019-nCoV-therapeutics-2021.2
Immunity of the vaccinated
https://www.biorxiv.org/content/10.1101/2021.08.23.457229v1
Immunity of the recovered
https://science.orf.at/stories/3208411/?utm_source=pocket-newtab-global-de-DE
Vaccination breakthroughs / Pandemic of the non-vaccinated
https://www.spektrum.de/news/corona-impfung-wie-viele-geimpfte-liegen-im-krankenhaus/1921090#Echobox=1631206725
https://www.mdr.de/wissen/covid-corona-impfdurchbrueche-sind-selten-100.html
Pseudo-experts / Science Denial / PLURV-Principle
https://www.ndr.de/nachrichten/info/82-Coronavirus-Update-Die-Lage-ist-ernst,podcastcoronavirus300.html#Argument
Notes:
(1) The exception was the coverage of the referendum, during which Swiss television was obliged to give both parties the same broadcasting slot.
(2) More Pandemic-Emergency exercises were “Clade X“ (2018), “Atlantic Storm“ (2005), “Global Mercury“ (2003) and “Dark Winter“ (2001). These exercises were always about information management.
(3) Panorama reported on the payments, but did not clearly portray Kyriakides’ role regarding the Corona vaccine contracts. Otherwise, the issue has not had much prominence in the media.
(4) For example, there was hardly any coverage on public radio of the British musician Eric Clapton, who developed violent reactions after vaccination and now regrets it.
(5) According to the RKI, a vaccination breakthrough is when a vaccinated person can show both a positive test and symptoms – for the unvaccinated, a positive test is sufficient. In this way, the unvaccinated are statistically more significant.
(6) Each under the heading “List of approved vaccines”; previous PEI website editions accessible via the Internet archive Wayback Machine.
(7) The WHO has even praised the Indian state of Uttar Pradesh for its corona policy, but without mentioning ivermectin. The vaccination rate in Uttar Pradesh is below 10 %.
(8) See also FDA meeting of 17 September 2021, at 5:47:25
(9) The fairest reporting comes from BR, although here too it was about and not with the makers. MDR offers a comprehensive and differentiated analysis on its media portal.
(10) I would not like to speak of an actual “unified opinion” of the public broadcasters. There have always been critical contributions and course corrections in reporting. But it is always a question of context, broadcasting time and scope how a topic is treated. My colleagues have also confirmed my observations.
(11) Fresh formats like ZDF’s “Auf der Couch” (On the Couch) give hope, even if I don’t think a Karina Reiß or a Wolfgang Wodarg will be taking a seat there any time soon.
The truth is still in lockdown
The first cross-party report says we didn’t lockdown early enough. The truth is, lockdowns don’t work.
By Laura Dodsworth | October 15, 2021
We now move, work, socialise, worship and meet around the UK with relative freedom.* Sadly, truth remains in strict lockdown.
Information is infectious and its transmissibility must be suppressed if it is deemed inconvenient, even if truthful. If it escapes, it can travel faster on social media than an airborne virus and must be captured, quarantined and sanitised to prevent onward infection. Most recently, in a long list of examples, a speech made by MP David Davis about vaccine passports was temporarily suspended from Youtube. Many videos and articles from reputable sources have been labelled misinformation if they run counter to WHO or governmental policy. Social media giants, governments and public health authorities are petrified of outbreaks of misinformation and even, sometimes, the truth.
So it was no surprise that the first cross-party report into the management of the epidemic in the UK, Coronavirus: lessons learned to date was unwilling to tackle certain truths.
One of the main inferences is that lockdown should have been implemented earlier. The truth is that lockdowns don’t work and cause great harm.
The report’s conclusions are assumptions. Opinions are not backed up with evidence. There is an unwillingness to interrogate the modelling that provides the foundations for the conclusions. The only thing that matters in this report is Covid and deaths by Covid. It is almost as if there are no other societal losses to put in the balance. There is no quantifiable cost benefit analysis of lockdown.
I spoke to Professor Simon Wood, Chair of Computational Studies at the School of Mathematics at the University of Edinburgh about the report. Wood authored a peer-reviewed paper published in Biometrics, which found that Covid-19 levels were probably falling before each of the three lockdowns. A separate paper, with colleague Ernst Wit, came to the same conclusion for the first two lockdowns, by the alternative approach of re-doing Imperial College’s major modelling study of the epidemic.
In summary he told me,
“The whole report is written within the framework that the only thing that counts is avoiding deaths from Covid, and that full lockdowns were essential. Evidence for the latter seems to be entirely absent. The closest we seem to get to actual evidence on lockdown efficacy is Neil Ferguson’s opinion in paragraph 77. The extent to which the committee is really able to weigh scientific evidence, as opposed to opinion, is questionable if paragraph 94 is any guide. This is such a gross misrepresentation of what the cited paper said, that it could have appeared on Twitter, rather than a parliamentary report.”
I asked him what he thought about the reliance on modelling throughout the epidemic. There are multiple flaws (expanded on in more detail in my book A State of Fear, and it’s appendix, “Lockdowns Don’t Work” and in many articles and papers online, some listed here) but one key flaw is that the Infection Fatality Rate in the initial modelling was 0.9%. By autumn 2020, a peer-reviewed paper by the WHO had put the IFR at 0.23%, and in the UK it is currently (albeit post-vaccination) at 0.096%. Wood generously told me it was,
“difficult to get the IFR right at the outset. We did the analysis thinking Imperial were very on the high side, but it in fact it wouldn’t have been assessed as less than 0.6% at the outset.” He went on: “The main error is to put too much emphasis on modelling not on measuring. Often models are being used for prediction purposes they were not designed or validated for.”
I put it to Wood that, in circular and fallacious reasoning, the modelling is being used to measure the success of lockdown by deaths ‘saved’ against those predicted by the unsubstantiated and flawed simulated forecasts of the modelling. He agreed: “the post hoc justification for the measures using modelling often looks like bending the model to the conclusion you want to achieve.”
There is a growing body of evidence that light interventions and voluntary behaviour changes – ie not lockdowns – are sufficient to reduce the R. Real world examples support this, namely Sweden, South Dakota and Florida. Conversely, as economist Professor David Paton reported, early and strict lockdowns did not always work. Czechia’s did not stop subsequent surges of the virus and further lockdowns. Czechia currently has the sixth highest death rate per million in the world. Peru, another country which enforced very strict and early lockdown, has the worst death rate in the world.
The report’s authors state we should learn lessons internationally, but fail to explain what they think happened in Sweden, for instance. In science it’s generally a good idea to have a control treatment and, to a limited extent, Sweden provided that. Surely it deserves some discussion if weighing up the evidence on what should have happened. It seems the report’s accusation of “British exceptionalism” only travels in one direction.
When data proves that lockdowns cannot be credited with controlling the virus, why does the argument persist? Why is truth still locked down?
Ironically, the authors accuse the government of groupthink, but they might still be under its sway themselves. It will be hard for the enactors and supporters of the lockdown to admit it was a brutal, ineffective and harmful policy. Far easier to assert the main problem is that it wasn’t imposed early and hard enough.
The harms of lockdown only get passing mentions. I can’t weight this article with the full burden of harms, but in brief: In the first year of lockdown the government borrowed £229 billion, the highest figure since records began in 1946. The pain of broken tax pledges, fiscal drag, inflation, and unemployment won’t be felt in full for months and years to come. The NHS waiting list is now 5.74 million and 7.5 million fewer people were referred for routine hospital care between January 2020 and July 2021.
These problems should not appear unexpected – they were foretold by the UK’s most eminent disaster and recovery planners.
In this 145 page report, the world “children” is mentioned a mere three times, but the impact of the lockdown on them is not mentioned at all. On World Mental Health Day, the ONS released data on children’s mental health and the impact of restrictions. A quarter of 11 to 16 year olds with a probable mental disorder in 2021 said Covid restrictions had made their lives much worse. And the number of young people aged 0 to 18 years old referred to mental health services between April and June 2021 increased by 93% from the same period in 2020, and 41% on 2019 in England.
Another word that is only mentioned three times is “obesity” alongside the other pre-existing health conditions which are known to be associated with poor outcomes for Covid-19. This really is the elephant in the room. The truth is, Covid-19 death rates are ten times higher in countries where more than half the adult population is overweight. In that sense, perhaps our pandemic preparedness should have started many years earlier with better health and dietary advice. Not only does lockdown not tackle the underlying chronic co-morbidities which lead to severe Covid-19 illness and deaths, but lockdown caused British people to gain weight, cease normal exercise and drink more alcohol.
The UK had multiple pandemic plans, including for SARS/MERS outbreaks. The authors of this report claim that we didn’t abandon the plans earlier in the crisis because of “groupthink”. This is a bizarre subversion – crisis management plans are not supposed to be abandoned during a crisis. If the government were guilty of groupthink, it was in following other countries in implementing an experimental policy. As Professor Ferguson put it,
“It’s a communist one party state, we said. We couldn’t get away with it in Europe, we thought. And then Italy did it. And we realised we could.”
The report does not mention Exercise Alice, a pandemic simulation exercise for MERS that has only been released after persistent Freedom of Information requests. It’s not clear that the authors are aware of it.
We will need a more wide-ranging inquiry that establishes whether lockdowns work, if they are sensible, proportionate and moral. Essentially, we must be truthful about what the costs are. We need to balance the losses.
Truth is infectious. Eventually it will peek around the doorframe, dare to stroll outside, evade quarantine and someone will catch a glimpse. Then another. Soon, everyone will be queueing up to greet our old friend Truth with hail-fellow-well-met and a hearty slap on the back. Then we must clutch Truth to us and never again lock it down.
* Although mandatory vaccine passports are a concerning development in Scotland and Wales.
27,247 Deaths 2,563,768 Injuries Following COVID Shots in European Database

By Brian Shilhavy | Health Impact News | October 15, 2021
The European Union database of suspected drug reaction reports is EudraVigilance, and they are now reporting 27,247 fatalities, and 2,563,768 injuries, following COVID-19 injections.
A Health Impact News subscriber from Europe reminded us that this database maintained at EudraVigilance is only for countries in Europe who are part of the European Union (EU), which comprises 27 countries.
The total number of countries in Europe is much higher, almost twice as many, numbering around 50. (There are some differences of opinion as to which countries are technically part of Europe.)
So as high as these numbers are, they do NOT reflect all of Europe. The actual number in Europe who are reported dead or injured following COVID-19 shots would be much higher than what we are reporting here.
The EudraVigilance database reports that through September 25, 2021 there are 27,247 deaths and 2,563,768 injuries reported following injections of four experimental COVID-19 shots:
- COVID-19 MRNA VACCINE MODERNA (CX-024414)
- COVID-19 MRNA VACCINE PFIZER-BIONTECH
- COVID-19 VACCINE ASTRAZENECA (CHADOX1 NCOV-19)
- COVID-19 VACCINE JANSSEN (AD26.COV2.S)
From the total of injuries recorded, almost half of them (1,222,818) are serious injuries.
“Seriousness provides information on the suspected undesirable effect; it can be classified as ‘serious’ if it corresponds to a medical occurrence that results in death, is life-threatening, requires inpatient hospitalisation, results in another medically important condition, or prolongation of existing hospitalisation, results in persistent or significant disability or incapacity, or is a congenital anomaly/birth defect.”
A Health Impact News subscriber in Europe ran the reports for each of the four COVID-19 shots we are including here. It is a lot of work to tabulate each reaction with injuries and fatalities, since there is no place on the EudraVigilance system we have found that tabulates all the results.
Since we have started publishing this, others from Europe have also calculated the numbers and confirmed the totals.*
Here is the summary data through October 9, 2021.
Total reactions for the mRNA vaccineTozinameran (code BNT162b2,Comirnaty) from BioNTech/ Pfizer: 12,835 deaths and 1,124,072 injuries to 09/10/2021
- 30,454 Blood and lymphatic system disorders incl. 177 deaths
- 32,024 Cardiac disorders incl. 1,894 deaths
- 296 Congenital, familial and genetic disorders incl. 24 deaths
- 15,348 Ear and labyrinth disorders incl. 10 deaths
- 943 Endocrine disorders incl. 5 deaths
- 17,445 Eye disorders incl. 30 deaths
- 97,494 Gastrointestinal disorders incl. 528 deaths
- 291,182 General disorders and administration site conditions incl. 3,649 deaths
- 1,271 Hepatobiliary disorders incl. 63 deaths
- 11,416 Immune system disorders incl. 66 deaths
- 40,375 Infections and infestations incl. 1,269 deaths
- 14,956 Injury, poisoning and procedural complications incl. 201 deaths
- 28,358 Investigations incl. 404 deaths
- 7,934 Metabolism and nutrition disorders incl. 231 deaths
- 145,368 Musculoskeletal and connective tissue disorders incl. 159 deaths
- 922 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 91 deaths
- 195,566 Nervous system disorders incl. 1,394 deaths
- 1,495 Pregnancy, puerperium and perinatal conditions incl. 44 deaths
- 177 Product issues incl. 1 death
- 20,700 Psychiatric disorders incl. 164 deaths
- 3,873 Renal and urinary disorders incl. 209 deaths
- 30,210 Reproductive system and breast disorders incl. 4 deaths
- 48,955 Respiratory, thoracic and mediastinal disorders incl. 1,504 deaths
- 53,542 Skin and subcutaneous tissue disorders incl. 116 deaths
- 2,209 Social circumstances incl. 17 deaths
- 1,318 Surgical and medical procedures incl. 36 deaths
- 30,241 Vascular disorders incl. 545 deaths
Total reactions for the mRNA vaccine mRNA-1273(CX-024414) from Moderna: 7,322 deaths and 328,594 injuries to 09/10/2021
- 6,545 Blood and lymphatic system disorders incl. 69 deaths
- 10,153 Cardiac disorders incl. 787 deaths
- 130 Congenital, familial and genetic disorders incl. 3 deaths
- 4,082 Ear and labyrinth disorders incl. 3 deaths
- 279 Endocrine disorders incl. 3 deaths
- 4,949 Eye disorders incl. 22 deaths
- 27,956 Gastrointestinal disorders incl. 286 deaths
- 88,398 General disorders and administration site conditions incl. 2,715 deaths
- 540 Hepatobiliary disorders incl. 30 deaths
- 2,817 Immune system disorders incl. 11 deaths
- 10,710 Infections and infestations incl. 562 deaths
- 7,148 Injury, poisoning and procedural complications incl. 134 deaths
- 6,185 Investigations incl. 130 deaths
- 3,158 Metabolism and nutrition disorders incl. 170 deaths
- 40,736 Musculoskeletal and connective tissue disorders incl. 149 deaths
- 407 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 48 deaths
- 56,868 Nervous system disorders incl. 735 deaths
- 629 Pregnancy, puerperium and perinatal conditions incl. 8 deaths
- 65 Product issues incl. 2 deaths
- 6,131 Psychiatric disorders incl. 129 deaths
- 1,898 Renal and urinary disorders incl. 131 deaths
- 5,644 Reproductive system and breast disorders incl. 6 deaths
- 14,462 Respiratory, thoracic and mediastinal disorders incl. 743 deaths
- 17,687 Skin and subcutaneous tissue disorders incl. 65 deaths
- 1,480 Social circumstances incl. 28 deaths
- 1,131 Surgical and medical procedures incl. 74 deaths
- 8,406 Vascular disorders incl. 279 deaths
Total reactions for the vaccine AZD1222/VAXZEVRIA (CHADOX1 NCOV-19) from Oxford/ AstraZeneca: 5,633 deaths and 1,027,132 injuries to 09/10/2021
- 12,420 Blood and lymphatic system disorders incl. 227 deaths
- 17,765 Cardiac disorders incl. 638 deaths
- 169 Congenital familial and genetic disorders incl. 7 deaths
- 12,102 Ear and labyrinth disorders incl. 1 death
- 545 Endocrine disorders incl. 4 deaths
- 18,094 Eye disorders incl. 27 deaths
- 99,247 Gastrointestinal disorders incl. 294 deaths
- 270,596 General disorders and administration site conditions incl. 1,355 deaths
- 892 Hepatobiliary disorders incl. 54 deaths
- 4,190 Immune system disorders incl. 26 deaths
- 28,330 Infections and infestations incl. 359 deaths
- 11,689 Injury poisoning and procedural complications incl. 162 deaths
- 22,549 Investigations incl. 132 deaths
- 11,969 Metabolism and nutrition disorders incl. 83 deaths
- 153,909 Musculoskeletal and connective tissue disorders incl. 82 deaths
- 554 Neoplasms benign malignant and unspecified (incl cysts and polyps) incl. 18 deaths
- 212,950 Nervous system disorders incl. 884 deaths
- 483 Pregnancy puerperium and perinatal conditions incl. 10 deaths
- 174 Product issues incl. 1 death
- 19,153 Psychiatric disorders incl. 56 deaths
- 3,848 Renal and urinary disorders incl. 56 deaths
- 14,092 Reproductive system and breast disorders incl. 2 deaths
- 36,247 Respiratory thoracic and mediastinal disorders incl. 673 deaths
- 47,145 Skin and subcutaneous tissue disorders incl. 42 deaths
- 1,361 Social circumstances incl. 6 deaths
- 1,240 Surgical and medical procedures incl. 24 deaths
- 25,419 Vascular disorders incl. 410 deaths
Total reactions for the COVID-19 vaccine JANSSEN (AD26.COV2.S) from Johnson & Johnson: 1,457 deaths and 83,970 injuries to 09/10/2021
- 786 Blood and lymphatic system disorders incl. 36 deaths
- 1,428 Cardiac disorders incl. 137 deaths
- 30 Congenital, familial and genetic disorders
- 805 Ear and labyrinth disorders incl. 1 death
- 52 Endocrine disorders incl. 1 death
- 1,140 Eye disorders incl. 6 deaths
- 7,423 Gastrointestinal disorders incl. 66 deaths
- 21,965 General disorders and administration site conditions incl. 381 deaths
- 104 Hepatobiliary disorders incl. 9 deaths
- 347 Immune system disorders incl. 7 deaths
- 2,564 Infections and infestations incl. 102 deaths
- 791 Injury, poisoning and procedural complications incl. 16 deaths
- 4,223 Investigations incl. 88 deaths
- 502 Metabolism and nutrition disorders incl. 34 deaths
- 12,777 Musculoskeletal and connective tissue disorders incl. 34 deaths
- 41 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 2 deaths
- 16,999 Nervous system disorders incl. 160 deaths
- 31 Pregnancy, puerperium and perinatal conditions incl. 1 death
- 21 Product issues
- 1,143 Psychiatric disorders incl. 13 deaths
- 325 Renal and urinary disorders incl. 16 deaths
- 1,356 Reproductive system and breast disorders incl. 5 deaths
- 2,985 Respiratory, thoracic and mediastinal disorders incl. 167 deaths
- 2,565 Skin and subcutaneous tissue disorders incl. 5 deaths
- 258 Social circumstances incl. 4 deaths
- 606 Surgical and medical procedures incl. 45 deaths
- 2,703 Vascular disorders incl. 121 deaths

*These totals are estimates based on reports submitted to EudraVigilance. Totals may be much higher based on percentage of adverse reactions that are reported. Some of these reports may also be reported to the individual country’s adverse reaction databases, such as the U.S. VAERS database and the UK Yellow Card system. The fatalities are grouped by symptoms, and some fatalities may have resulted from multiple symptoms.
COVID-19 Shots Continue to Kill and Injure People Worldwide
The true number of people dying and becoming crippled worldwide following the COVID-19 shots is unknown, since the adverse reaction systems used in most countries are passive systems, and there is tremendous pressure to NOT relate a disability or death to the COVID shots.
US Treasury deputy sec warns unvaxxed Americans that shortages will continue until EVERYONE is jabbed
RT | October 15, 2021
The deputy secretary at the US Treasury has put Americans on notice that the only way to end the plague of empty shelves around the country is for every resident to be vaccinated. The frank warning came off as a threat to many.
Wally Adeyemo, the Biden administration’s second-highest official in the Treasury Department, appeared to publicly blackmail the still-sizable portion of Americans who have not been vaccinated against Covid-19 during a Thursday ABC interview, seemingly blaming them for the ongoing shortages of consumer goods that have led many to mock the president as ‘Empty Shelves Joe’.
Despite viral photos depicting thousands of cargo ships lined up at the Port of Los Angeles ready to unload their goods, Adeyemo claimed that the supply chain issues plaguing so many US retailers are an international issue and will only let up when a sufficient percentage of the country has been vaccinated.
Describing the disastrous economic conditions as “an economy that’s in transition,” Adeyemo acknowledged that “we are seeing high prices for some of the things that people have to buy.” While he praised the administration’s stimulus payments, he also pinned the blame squarely on the unvaccinated.
“The reality is that the only way we’re going to get to a place where we work through this transition is if everyone in America and everyone around the world gets vaccinated.”
While the ABC reporter repeatedly suggested that the country’s shortages of toilet paper and other panic-buy items could be traced to international supply chain disruptions, a growing number of Americans are demanding answers regarding the weirdly specific nature of certain products missing from store shelves. Some have even voiced doubt concerning whether the shortages are being introduced deliberately, either to gin up hatred against the unvaccinated or keep Americans economically off-balance as they grow accustomed to the wild disruptions of the pandemic.
Adeyemo did the Biden cabinet no favors by adding fuel to the conspiratorial fire, explaining the primary reason Biden continued to push for everyone to be vaccinated was that only then could the White House “provide the resources the American people need to make it to the other side” of the supply chain problem.
Despite blaming the international shipping industry for empty shelves in the US, the media establishment has acknowledged that the ports of Los Angeles and Long Beach – which together process 40% of the nation’s imports – had their busiest years on record last year, giving the lie to the notion that the products missing from American shelves simply don’t exist. However, many truckers working for shipping companies have balked at the idea of mandatory vaccination, leaving their firms’ fleets woefully understaffed, and others have gone on strike to demand better working conditions.
The Biden administration has attempted to address the supply chain problem by calling for the Port of Los Angeles to run 24 hours, but while he praised his own promised move as a “game changer,” the executive director of the port has made it clear that there is no timetable in place for the promised schedule shift. Meanwhile, Biden’s cabinet has come across as woefully out of touch – White House Chief of Staff Ron Klain, for example, pooh-poohed the issue of empty shelves as a “high class” problem earlier this week, eliciting criticism from both Left and Right. And Transportation Secretary Pete Buttigieg has been quietly vacationing on paternity leave since mid-August, leaving the country without even a semblance of logistical oversight as the cargo clog shows no signs of dissipating.
Labor shortages are being felt far beyond the US, though often for similar reasons. In Italy, thousands of protesters turned out to block cargo ships from unloading their bounty earlier this week. The demonstrators were outraged over the country’s adoption of a mandatory vax-to-work policy similar to that threatened by the Biden administration. And the UK government has begged lorry drivers to return to work, even luring foreign drivers in with temporary visas as the country frets over its own empty shelves issues.
Australian ‘truckies’ have united with other unions to exert pressure on the government, which has kept cities like Melbourne under lockdown for months despite vanishingly few reported cases of Covid-19. The government was already floating policies like ‘no jab, no job’ over a year ago and has led the way in leveraging the pandemic to turn Five Eyes ‘democracies’ into police states.
More stories about staffing problems and lawsuits over the mandates
By Meryl Nass, MD | October 14, 2021
Massachusetts may lose 40-50% of its corrections officers to the mandate, and the governor is talking about bringing in the National Guard. The Guard is already driving school buses. Massachusetts is possibly the bluest state in the nation. It was the only state that voted for McGovern in 1972.
Massachusett’s State Police union has filed for an injunction against the clot shot mandate. So has the corrections officers’ union.
If this is what is happening in the bluest state, just think how many clot shot refusers there are everywhere else. The society can’t run if the workers can’t work. Are the bosses trying to create chaos as a pretext for something else, or are they only trying to bluff and coerce us into submission?
———————
Dr. Peter McCullough said doctors are now being hunted for refusing to go along. One day after an affidavit I wrote was filed in court in Maine against our health department’s mandate for healthcare workers, I got a letter from the secretary of the medical board telling me I had to respond to a complaint. What was the complaint? Someone who never met me and does not know any of my patients didn’t like a video interview he saw, and said so to the board. Not a single specific complaint or allegation was made against anything I said.
I will keep you all updated regarding this business. I am dismayed but simultaneously amused at how a medical board or its secretary can ask me to defend myself against a charge of being disliked. Is this America’s COVID jurisprudence?
UK: CHALLENGING VACCINATION POLICIES AT WORK
UK Freedom Project | August 31, 2021
The UK Government has played a duplicitous game over recent months regarding COVID-19 vaccines and proof of vaccination status.
Early in 2021, in response to a petition calling for the government to commit to not implementing COVID-19 vaccine passports that received over 375,000 signatures, the Vaccines Minister repeatedly stated that mandating vaccines and implementing a passport system would be discriminatory and a dangerous first step onto a very slippery slope.
Yet here we are at the end of August with a vaccine mandate in place for care home workers and the government allowing, and indeed enabling, private businesses to set their own policies regarding vaccination and vaccine status for both employees and customers.
While many employers are jumping on the bandwagon and are either making COVID-19 vaccination a condition of continued employment or are implementing various discrimination measures such as segregating non-vaccinated staff from the rest of the workforce, most have failed to appreciate that there is already well established law in effect that protects the rights of employees (and human beings in general) and prevents employers enacting such policies.
If you are faced with loss of employment, change of duties or are being treated differently as a result of your choice not to have a COVID-19 vaccine, then the law is on your side.
We have collaborated with a solicitor to put together a letter that you can send to your immediate line manager (and your HR department and employer) that states your position, your rights and the law.
It is important that all employees take a stand. Employers will only get away with this if employees cave in and either accept changes to their employment or leave of their own volition to find alternative work.
As well as the letter, we have compiled a set of explanatory notes to give to your employer, so that they (and you) fully understand the various pieces of domestic and international legislation that their actions and attitudes are breaching.
Please use the buttons below to download
- the letter in Word format (which you will need to personalise by adding your name and address, the date and the name and address of your line manager/employer
- the explanatory notes in PDF format (which need to accompany the letter for completeness),
You should keep a copy of both documents for your own records.
Hand the letter to your line manager and ask for it to be placed on your personnel records.
In 20 Years of Practicing Medicine, ‘I’ve Never Witnessed So Many Vaccine-Related Injuries’
The Defender | October 13, 2021
In a letter dated Sept. 28 to officials at the U.S. Food and Drug Administration (FDA) and Centers for Disease Control and Prevention (CDC), an ICU physician detailed her concerns about the adverse reactions, including deaths, she witnessed in people who had received a COVID vaccine.
Dr. Patricia Lee, a licensed physician in California, said her experience with patients harmed by the vaccine “does not comport with claims made by federal health authorities regarding the safety of COVID-19 vaccines.”
In the letter, Lee described observing “entirely healthy individuals suffering serious, often fatal, injuries,” including transverse myelitis, resulting in quadriplegia, pneumocystis pneumonia, multi-system organ failure, cerebral venous sinus thrombosis, postpartum hemorrhagic shock and septic shock.
Lee, a practicing physician for more than 20 years, said she “never witnessed so many vaccine-related injuries until this year.”
Lee told Dr. Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research, and Dr. Tom Shimabukuro with the CDC’s COVID-19 Vaccine Task Force Vaccine Safety Team, that while “causation is difficult to prove definitively, it is my clinical judgment that each of these injuries were caused by a COVID-19 vaccine, because there was no other plausible explanation for these injuries other than the fact that the patients had recently been vaccinated.”
Lee acknowledged that her report reflects the experience of a single physician. However, she wrote, it appears “statistically improbable” that any one physician should witness this many COVID-19 vaccine injuries if the federal health authority claims regarding the vaccines’ safety were accurate.
“I can no longer silently accept the serious harm being caused by the COVID-19 vaccines,” Lee concluded. “It is my sincere hope that the reaction to this letter will not be to focus on me, but rather to focus on addressing the serious safety issues with these products that, without doubt, you have either missed or are choosing to ignore.”
Since the issuing of the original letter, Lee’s attorneys sent another letter to the CDC and FDA saying that the agencies’ “failure to respond is highly concerning,” adding that they are seeking a response so they can “arrange a discussion and information gathering session between Dr. Lee and the appropriate representatives at the CDC and FDA.”
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
SPECIAL BROADCAST: DR. ROBERT MALONE ON HIS MRNA CREATION
STEW PETERS | OCTOBER 13, 2021
Stew Peters sat down with Dr. Robert Malone, the creator of the mRNA technology being used in the shots being falsely referred to as “vaccines”, which have proven to be dangerous, and in many cases DEADLY.
Deaths Following Vaccination Reported in Taiwan Exceed Nation’s COVID Death Total
BY BLUEAPPLES | ZERO HEDGE | OCTOBER 14, 2021
Since the onset of the COVID-19 pandemic, few nations have been lauded as much for their management of the disease as Taiwan has. Since the first cases of COVID-19 in the country were reported in February 2020, only 16,313 infections and 846 deaths have been recorded. Despite how successfully the nation had managed the outbreak, it still enrolled itself in the World Health Organization-led COVAX exchange program and began its first wave of vaccinations on March 22, 2021. While the nation hadn’t had even a dozen deaths attributed to COVID-19 by the time the first vaccine was administered, 836 of the 846 deaths attributed to COVID-19 have occurred since the vaccination program began. In an even more dubious display concerning the safety and effectiveness of the vaccines administered in Taiwan, the nation’s Central Epidemic Command Center (“CECC”) has stated that 850 deaths have been reported as adverse events following vaccinations. That totally eclipses the number of fatalities attributed to the virus itself.
Taiwan’s vaccination campaign began much later than many other nations, a lag which many blame on political interference from China which was best illustrated by the island nation’s difficulties procuring orders of Pfizer-BioNTech’s mRNA vaccines. Despite these hurdles, the country was at first able to procure 117,000 doses of AstraZeneca’s vaccines. Additional deliveries of 200,000 and 400,000 doses from the same manufacturer arrived the following two months before another 150,000 vaccines from Moderna were delivered in May 2021. It gave emergency approval to a domestically engineered alternative made by Medigen Vaccine Biologics Corporation with shipments from Pfizer-BioNTech and Johnson & Johnson soon following. As of October 11, 4.48 million Taiwanese, about 19% of the population, have been fully vaccinated and 13.7 million, or about 59% of population, have received one dose. The country has stated that it seeks to have 70% of its population fully vaccinated.

Yet, by the time Taiwan had approved those five vaccines for emergency use, an alarming trend began appearing. The highest seven-day average of new cases of COVID-19 observed in Taiwan before its first vaccines were deployed was just 3. By May 28, 2021, that seven-day average exploded to 597. As the rest of the world grappled with an increase in cases despite the global advancement of vaccination efforts, most those countries had recorded their all-time highs for new cases and deaths before any vaccines were available. One exception to that rule was seen in Israel, where the record for a highest single-day case count was recorded following the beginning of the nation’s campaign to administer third doses of the Pfizer-BioNTech vaccines in the wake of concerns of the delta variant’s impact of the efficacy of vaccines. Yet, even though Israel did surpass its previous one-day high, the amount by which it exceeded that paled in comparison to Taiwan. The seven-day average in Taiwan would not fall under 10 new cases again until September 2021. Since then, despite the increase in vaccinations, that national average has never managed to reach its pre-vaccination levels. The lowest seven-day average Taiwan has seen since it began vaccinating its citizens was recorded at 5 on September 5, 2021.

While the increase in viral transmission since March will likely be attributed to mutations like the delta variant, it could also be indicative of the antibody dependent enhancement onset from vaccines that has been forewarned about by scientists and physicians such as Dr. Robert Malone, one of the scientists behind the development of mRNA technology. Though not all vaccines used in Taiwan utilize mRNA technology, the viral vector-based vaccines like AstraZeneca’s still predicate their promotion of antibodies by exposing the immune system of vaccinated patients to the spike protein of SARS-CoV-2. Antibodies based on the genetic fragment of the spike protein alone opposed to a whole genetic sequence of a viral particle are suspected to be less capable of warding off infection. Scientists like Dr. Michael Yeadon, formerly of Pfizer, attest that these inadequate antibodies actually facilitate viral entry because they don’t possess the necessary protein structures, or paratopes, to the corresponding protein structures on the viral particles, called epitopes. This phenomenon was observed in clinical trials of mRNA vaccines aimed at combating the coronavirus which caused Middle Eastern Respiratory Syndrome. Advocates of that theory warning against that risk have expressed concerns that this same outcome of the potential deficiencies in COVID-19 vaccines has been overlooked by a hurried regulatory process.
As far as the 850 deaths reported to the Taiwanese CECC following vaccinations are concerned, 643 have been attributed to patients receiving AstraZeneca doses, 183 received Moderna doses, and just 22 received Taiwan’s own Medigen vaccine. Despite being recorded as adverse events following vaccination, many Taiwanese officials have responded to the CECC report by stating that these deaths may not be inherently due to the vaccines. The CECC has previously affirmed its position that reactions from the Moderna vaccine have resulted in fatal adverse events. As the seven-day average of COVID-19 deaths continues to hover between 0 and 1 as it has over the last several weeks, it’s possible that deaths reported to the Taiwanese CECC following vaccination will continue to exceed those attributed to viral infection for some time.
Featured Video

Fear Is the Mind Killer
or go to
Aletho News Archives – Video-Images
From the Archives
Alarmist climate science as a textbook example of groupthink
By Paul MacRae | May 1, 2012
A while ago, I received an email from a friend who asked:
How can many, many respected, competitive, independent science folks be so wrong about [global warming] (if your [skeptical] premise is correct). I don’t think it could be a conspiracy, or incompetence. … Has there ever been another case when so many ‘leading’ scientific minds got it so wrong?
The answer to the second part of my friend’s question—“Has there ever been another case where so many ‘leading’ scientific minds got it so wrong?”—is easy. Yes, there are many such cases, both within and outside climate science. In fact, the graveyard of science is littered with the bones of theories that were once thought “certain” (e.g., that the continents can’t “drift,” that Newton’s laws were immutable, and hundreds if not thousands of others).
Science progresses by the overturning of theories once thought “certain.” … continue
Blog Roll
 Aletho News
Aletho News- Military aid to Ukraine vital for ‘US hegemony’ – Republican senator
- Zelensky’s favorite drone company at center of Ukrainian corruption alert
- The Broken Contract
- US CENTCOM’s Request for Dark Eagle Missiles Shows Shortage of Weapons and Limited Options
- Iran consolidates Strait of Hormuz control in post-war power shift, leaving US in dark
- A pause, not a ceasefire: Washington stalls, Tehran recalibrates
- US blockade crumbles as Iran turns to overland routes
- Hidden costs of US Iran war push total far beyond $25bn Pentagon claim
- Iran Will Respond With Long-Term Strikes to US Attack, Even If It Is Short-Term – IRGC
- Fear Is the Mind Killer
- If Americans Knew
- Former Tik Tok official describes massive pressure from Israel lobby
- Amid ceasefire violations and genocide, Israel commits piracy – Daily Update
- Five Laws and Standards That Require the US Cut Off Weapons to Israel
- Israel’s diabolical killing machine and how it targets journalists.
- The Global Sumud Flotilla to Gaza — A cry at sea to the world’s dormant conscience
- Politico’s powerful parent company tells Politico they must support Israeli narrative
- How Tony Dokoupil Became the Face of ‘Zionist Fanatic’ Bari Weiss’s CBS
- Far Right Israeli Settler Movement Enters Syria in a Push for “Greater Israel”
- ‘People Have the Right to Be Buried’: In Gaza, Thousands of Palestinians Remain Trapped Under Rubble
- Born during Israel’s genocide: Gaza’s child survivors bear the scars of war
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
