Biden praises Southwest Covid vaccine mandate amid cancelation chaos, says it will help ‘eliminate this disease’

© REUTERS/Leah Millis
RT | October 14, 2021
In an address from the White House, President Joe Biden praised companies like Southwest Airlines enforcing his Covid-19 vaccine mandate, despite the CEO seemingly rebuking the requirement the day before.
Addressing the government’s effort to battle the coronavirus pandemic on Thursday through vaccine mandates, Biden praised private companies that have already been “stepping up” to combat misinformation about the Covid-19 vaccine and the implementation of their vaccine mandates.
“Southwest Airlines … the head of the pilots’ union and its CEO dismissed critics who claim vaccination mandates contributed to flight disruptions,” Biden said, referring to mass cancelations at Southwest Airlines that peaked on Sunday, shortly after the company began enforcing the vaccine mandate put forth by the president.
The company and the White House have denied the mandate and ensuing staffing shortages caused them to delay a third of their flights in the US. White House Press Secretary Jen Psaki even deemed the mandates “good for the economy” following the cancelations and speculation by critics.
In his address, Biden went on to praise school board members, doctors, and other healthcare workers for battling “misinformation” about vaccines.
“All of these efforts,” Biden said of the companies and individuals facing “misinformation” about vaccines and mandates, “are going to help us continue moving the dial to eliminate this disease.”
Biden’s comments came shortly after Southwest CEO Greg Kelly appeared to distance himself from the mandate, despite the company saying there was no connection between their scheduling troubles and the requirement.
The CEO told CNBC he had never “been in favor of corporations imposing that kind of a mandate,” though adding again it has nothing to do with the cancelations.
Biden pushed back against the divisive response his vaccine mandates have received from the public, saying mandates “should not be another issue that divides us” and is only part of the larger effort to battle the virus and get the still lagging, according to the president, vaccination rate up.
“Mandates work,” the president said, and companies like Southwest that have already implemented them prove that, he added.
The Department of Labor will be requiring all businesses with 100 or more employees to require Covid vaccinations, an order multiple companies have already said they will defy.
Go Fund Me Takes Down Fundraising Campaign for Litigation Over Vaccine Mandate
By Jonathan Turley | October 12, 2021
We previously discussed how GoFundMe has joined social media sites in censoring opposing viewpoints on subjects from critical race theory to vaccines to election fraud. The site once offered a neutral site for those seeking to support others with similar views or interests. The company now insists that it will only allow people to gather on the site if it believes their views are true and correct. However, it was still surprising to see the site take down a fundraising account for litigation against vaccine mandates. The effort of former nurse Jennifer Bridges was simply to get such matters before the courts, which can be the ultimate authority on what is “misinformation.” GoFundMe however blocked people from contributing to the litigation.
Bridges is a former registered nurse at Houston Methodist hospital who was fired after refusing to comply with the hospital’s vaccine requirement. She raised more than $180,000 for her lawsuit before being shutdown under the company’s “misinformation” policy. Heidi Hagberg, a spokesperson for GoFundMe, said in a statement to Business Insider that “when our team initially reviewed the fundraiser, it was within our terms of service as the funds were for legal fees to fight vaccine mandates. The fundraiser has since been updated to include misinformation which violates our terms of service.”
What is striking about this latest ban is that the courts are the place for such claims to be weighed in a neutral and dispassionate forum. “Misinformation” can be addressed by judges after both sides are allowed to present evidence. Bridges’ lawsuit was dismissed in June, Bridges’ attorneys appealed the decision. We should all favor such reviews. Indeed, if GoFundMe believes that Bridges is wrong, it should invite further judicial review to establish a clear record on such issues.
GoFundMe admits to have taken down “hundreds” of fundraisers that included statements of “misinformation related to vaccines.”
I do not agree with the arguments against the vaccine. I and my family are vaccinated. However, I am equally concerned with avoiding the growing virus of censorship. In the last few years, we have seen an increasing call for private censorship from Democratic politicians and liberal commentators. Faculty and editors are now actively supporting modern versions of book-burning with blacklists and bans for those with opposing political views. The most chilling aspect of this story is how many on the left applaud such censorship. A new poll shows roughly half of the public supporting not just corporate censorship but government censorship of anything deemed “misinformation.”
Free speech can be its own disinfectant for bad speech. GoFundMe is a private company and can impose such rules on users. However, it is an act of censorship and it is a denial of free speech by a corporation. In this case, the company is preventing its site from being used to raise money to allow courts to review the factual and legal basis for these claims — a curious effort for a company that claims to be fighting “misinformation.”
Southwest Airlines pilots and staff are flying in the face of corporate and government vaccine mandates
By R. M. Huffman | RT | October 12, 2021
Southwest Airlines’ top brass can deny the massive delays they’ve been experiencing have anything to do with their insistence staff take Covid shots or lose their job till they are blue in the face… but no one is buying it.
Southwest is experiencing turbulence. Over the weekend, the Texas-based airline canceled over 1,800 flights. Monday was no better: almost 400 more flights were canceled. A corporate spokesman, Alan Kasher, blamed the catastrophic interruption in business on bad weather in Florida and “issues” with air traffic control.
His claim was met with immediate disbelief, as the Federal Aviation Administration countered that no ATC staffing shortages were reported over the weekend, and competitor airlines flying in the same regions only canceled a tiny fraction of their own flights. The real reason for the cancellations is an open secret, despite Kasher’s reticence in acknowledging it. Southwest’s pilots and crews have been given a vaccine mandate, and they’re simply not having it.
Just today, on Good Morning America, Southwest CEO Gary Kelly spun the bad news like a turbine, citing “no evidence” that his company’s disastrous past few days had any connection with the vaccine ultimatum he’d handed down to his workforce. It does, of course, and Kelly knows it.
Here’s what’s actually happening. On September 9, Joe Biden announced his intention to force every company that employs more than 100 people to give their employees a vaccine mandate. Southwest Airlines subsequently relayed a missive to its employees, pilots, and crew members: “Southwest Airlines will be required to comply with the federal government’s directive for Employees of federal contractors to be fully vaccinated against COVID-19.” The deadline was set for December 8: get the vaccine, hope for an exemption, or be fired.
Many of these employees had already contracted and beaten the disease, enjoying an effective natural immunity. Others remained concerned about reports of adverse effects, including thrombosis (for which the Johnson & Johnson jab was pulled from market) and myocarditis (for which the Moderna shot was pulled as well). Many were also aware that vaccinations, while decreasing hospitalizations and deaths, don’t completely stop breakthrough infections and have demonstrated a diminishing efficacy.
Whatever the individual reasons, a mandate mutiny began brewing. It’s manifested now, asserting itself over these last few days in a way that can’t be ignored. Pilots save up paid sick days, often accumulating months’ worth, even years. As their concerns have gone unheard by executives and, faced with the ignominy of sacrificing bodily autonomy for corporate compliance, or being fired and losing their careers – including all those saved hours they’ve earned – pilots are simply calling in sick and cashing in their paid leave.
The union for Southwest’s 9,000 pilots denies an organized protest, sick-out, or shutdown, and that’s true. These individuals acting out of conscience are a loose confederation of colleagues at best. They’ve been told by Southwest suits that “the federal directive gives little latitude for input or choice.”They rejected that assertion, are rejecting it, and will continue to reject it.
Perhaps the most baffling aspect of the entire scenario is the fact that there isn’t even a rule with which Southwest Airlines is complying. When President Biden delivered his ultimatum in September, lawmakers and legal scholars were dubious. Many wondered how Biden intended to give teeth to his speech, as he’s not a part of any legislative body. His answer: use the Occupational Safety and Health Administration (OSHA) to define vaccination as a workplace safety concern and issue a rule accordingly.
Regardless of the small agency’s legal standing to accomplish such a legislative workaround, or its ability to subsequently enforce it, a more foundational problem remains for Southwest and other employers: OSHA has not yet made such a rule, much less navigated the legal challenges already being made.
Unsuccessful with his carrots, Biden has picked up a stick; legally, this stick would be fragile in the best case, but at the moment it remains a complete mirage. It’s hard to believe that Southwest is so willing to infuriate both stranded customers and disgruntled pilots to avoid being beaten with it.
It is natural that airline executives would want to stay in the government’s good graces. After all, they’ve multiple times gone begging to Congress, cap in hand, lamenting the looming layoffs of their “valued employees” and asking for taxpayer bailout dollars. They’ve received them, to the tune of billions, as well as millions in compensation for themselves. Government contracts, at risk if the company doesn’t impose a vaccine mandate, make up a mere 3% of Southwest’s business, yet a hard line has been drawn over all objections of pilots and crews. How could Southwest’s employees not question where their CEO’s loyalty really lies?
Customers stranded at airports and dealing with canceled flights can’t be blamed for being frustrated, but their ire ought not be aimed at Southwest pilots, any more than the many tea enthusiasts among the American colonials should have been angry at the men who tossed the tea shipments into Boston Harbor. Economic disruption can be powerful, both as a symbol and as a practical protest method (although sometimes it’s mostly property destruction and looting, to which this current action bears no resemblance).
Perhaps even more so than the nurses and doctors once held up as heroes and now fired for refusing the jab, these pilots and crew members are showing concerned Americans, Europeans, Australians, and all free citizens, a potential way forward through this miserable morass of mandates. In Western democracies, government is designed to represent the people, not rule them. At some point, our elected officials decided that they would prefer to be masters rather than servants, entangling themselves with corporate leadership in a moldering rat king of stifling bureaucratic fiat and decree.
Just tell them no.
American corporations exist at the whim of their customers and through the willingness of their employees.
The United States government serves only with the consent of the governed.
Neither is the king of anybody. It’s high time they stop behaving as if they are.
Southwest Airlines’ goodwill is gone. Its executives now have a choice: hold firm to a specious vaccine mandate and watch its customers and employees fly away or, find a spine, and tell the federal government that it won’t play the willing stooge to Biden’s bullying tactics.
It’s time for corporate vaccine mandates to crash and burn.
R. M. Huffman is a physician, author, and observer of culture.
We need a Covid champion to defy Big Pharma like the thalidomide heroine
By Mary McGreechin | TCW Defending Freedom | October 13, 2021
IN 1960, Frances Oldham Kelsey prevented thousands of American babies from facing a life of severe disability.
A medical officer with the US Food and Drugs Administration (FDA), Kelsey refused to buckle under relentless pressure from the pharmaceutical company Merrell to approve the drug thalidomide for use as a sedative and, off-label, as a treatment for morning sickness.
From 1957, the drug had been used in Europe to ease extreme nausea in the early stages of pregnancy. But by 1961, mounting reports from concerned doctors revealed devastating birth defects in the babies of women who had taken thalidomide.
Determined to break into the lucrative American drug market, Merrell had claimed stringent testing showed the drug to be safe as well as efficacious.
Kelsey, however, was suspicious of incomplete data and the omission of tests on the drug’s prolonged use and refused to give her approval. Despite harassment and intimidation by the company – ‘most of the things they called me you wouldn’t print’ – Kelsey had remained resolute.
Today, as the Covid agenda aims to vaccinate every man, woman and child, minimising, or ignoring, often fatal side-effects, we need a Frances Kelsey to say: ‘No.’ Or even: ‘Not yet.’ Despite some courageous voices within the medical community speaking out at great personal cost, no influential figure has voiced the level of dissent needed to halt this programme.
Medical advances have, undeniably, delivered life-enhancing and life-saving treatments. Yet countless lawsuits against the pharmaceutical industry demonstrate that medicine can have an iatrogenic (illness-causing), as well as a therapeutic, effect. In the US alone, billions of dollars are paid annually in damages by pharmaceutical companies.
The industry has sought to temper such negative perceptions by cultivating a philanthropic image, portraying itself as a benevolent entity driven by altruism rather than a competitive industry whose investors salivate at ever-increasing share prices.
Despite these endeavours, it is astonishing that a large proportion of the public have failed to be concerned that drug companies which have been fined astronomical sums in multiple lawsuits have been granted liability immunity on Covid vaccines. With pharmaceutical firms typically afforded limited liability protection, this indemnity has been described as ‘very rare.’
Should we be surprised at the lack of public suspicion? The NHS has been elevated to such a degree that any condemnation of this behemoth is considered blasphemy. A 2020 Ipsos MORI poll revealed that more than 90 per cent of Britons trusted doctors and nurses ‘to tell the truth.’
Yet medics may be untruthful, or unaware of the full facts behind the medicine they prescribe. UK doctors believed thalidomide could be given ‘with complete safety to pregnant women and nursing mothers without adverse effect on mother or child’, yet it was later acknowledged that no tests were done involving pregnant women.
The effect of Covid vaccines on fertility and the unborn child are unknown. However, more than 30,000 women have, at present, reported changes in their menstrual cycle post-vaccination.
The vice-president of the Royal College of Obstetricians and Gynaecologists stated: ‘We support calls for more research to understand why women may be experiencing changes to their menstrual cycle after having the vaccine.’ Stable door, horse and bolted come to mind.
And whilst pregnant women were excluded from the Covid vaccine trials, the Journal of the American Medical Association (JAMA) had these reassuring words to ‘pregnant people’: ‘Reproductive toxicity studies with the Moderna vaccine in rats haven’t uncovered any worrisome signals.’
Are we to place our trust in pharmaceutical companies whose employees’ emails reveal such statements as:
‘I am not 100 per cent comfortable with this data being made publicly available.’
‘Thus far we have buried trials 15, 31, 56 … how do we face the outside world when they begin to criticise us for suppressing data?’
‘Lisa has done a great “smoke and mirrors” job.’
All this correspondence was made public when litigation against AstraZeneca’s anti-psychotic drug Seroquel began. The company, now most famously known for the development and production of Covid vaccines, faced a major lawsuit in 2009 brought by thousands of Seroquel users who claimed they had developed diabetes whilst taking the drug.
The damning emails proved the pharmaceutical giant had been aware of the risk a decade earlier. Moreover, AstraZeneca had suppressed research which showed its earlier anti-psychotic treatment, Haloperidol, was more effective, and much cheaper, than Seroquel.
Employee John Tumas messaged concerns to colleagues that ‘our own analysis supports the “view out there” that we are less effective than Haloperidol.’
Promoting expensive treatments over cheaper alternatives has also caused debate regarding Covid-19. Those advocating for the use of Ivermectin, more commonly used as an anti-parasitic in animals, to treat the virus, have been relentlessly mocked. But studies have shown the drug can provide ‘an increase in clinical recovery … and a decrease in mortality rates even when used in patients with severe Covid-19.’
Yet a trial conducted on those with mild symptoms concluded it had little effect. Doctor Eduardo Lopez-Medina published his findings in JAMA, maintaining that Ivermectin had delivered negligible benefits.
However, a ‘conflict of interest disclosure’ revealed Dr Lopez-Medina was in receipt of grants and ‘personal fees’ from pharmaceutical giants GlaxoSmithKline, Janssen and Sanofi Pasteur – all involved in the production of Covid-19 vaccines.
Countless stories have emerged in the past 18 months which should raise serious questions over transparency and truthfulness within the medical field – from doctors wrongly claiming intensive care units are full of unvaccinated 20 and 30-year-olds on ventilators, to hospital matrons inventing stories of children’s wards full of Covid patients.
And yet we are expected to have faith that such medics, and the pharmaceutical industry, have our best interests at heart in their pursuit of global vaccination against Covid-19.
Like Frances Oldham Kelsey, we should remain steadfast against coercion and duress. We should ask more questions and seek more answers. If we do not like the answers we find, then we must hold the line. For our own sake and that of our children.
Ex-Pfizer Employee Warns Vaccine Increases COVID By Over 300%
By Lance D Johnson | Humans Are Free | October 1, 2021
The fraudulence of covid-19 vaccines is on full display, and the evidence is sitting right out in the open. The full FDA approval for Pfizer’s COMIRNATY vaccine contained clinical proof that the inoculation increases COVID infection by over 300 percent!

Varitage.com
A former Pfizer employee named Karen Kingston is blowing the whistle on her former employer. Kingston is currently a pharmaceutical marketing expert and biotech analyst. When she scrutinized the full FDA approval for COMIRNATY, she found blatant fraud in Pfizer’s clinical studies.
FDA Approves Pfizer’s Covid-19 Vaccine, Even Though It Increases Infection By 300 Percent
Kingston brought forth a Briefing Document from the FDA’s advisory committee meeting that took place on September 17, 2021. The title of the document is, “Application for licensure of a booster dose for COMIRNATY (COVID-19 Vaccine, mRNA).” The document includes clinical studies conducted by Pfizer. These studies track the durability of immunity offered by the COMIRNATY vaccine and compare it to immunity observed in unvaccinated people.
“If you get the Pfizer vax, you’re more likely to get COVID” said Kingston, “So, when they weren’t injected, their infection rate was 1.3% and when they got injected, it was 4.34%. It went up by over 300%.” How could the FDA have glossed over this evidence and approved blatant fraud?
Since the vaccine was officially approved, the federal government started applying pressure on businesses across the US, threatening them with extortion and fines if they do not impose vaccine mandates on their employees.
The covid-19 vaccines have been injected almost 225 million times into the arms of Americans, causing severe injury and death along the way. Real world observations also support clinical data showing that the vaccines increase one’s susceptibility to covid-19.
In fact, the vaccines increase viral load in the nostrils of the vaccinated. An August 26 article by Dr. Peter McCullough shows that the covid vaccines allow the vaccinated to carry 251 times the viral load of covid-19 in their nostrils, turning them into the asymptomatic super spreaders they once feared.
Pfizer Studies Show That Being Unvaccinated Offers Greater Protection
Medical freedom rights attorney, Thomas Renz, went public with the Pfizer fraud. The Pfizer study involved over 36,000 people. Those who were injected earlier in the study were more likely to come down with covid infections later on, showing a clear trend of waning immunity. Those put in “high priority” groups, who were vaccinated earlier on, have a 36 percent greater chance of infection, compared to the group that vaccinated later on.
The group that vaccinated later on went unvaccinated for 5.1 months longer than the group that got vaccinated early on. This placebo group did not have high rates of infection while they were unvaccinated, even though they went longer without any “protection.”
Because of this, Kingston stated that the vaccinated group “have an even higher chance of being infected with COVID-19 than the 36 percent difference indicated by this portion of the study.”
The study even admitted in its conclusion: “An additional analysis appears to indicate that incidence of COVID-19 generally increased in each group of study participants with increasing time post-Dose 2.” Kingston clarified that infection rates “increase over time” when people get two doses of Pfizer mRNA.
Most shocking was the data on the placebo group. In the first four months, the placebo group had “no vaccine protection” and recorded an infection rate of 12.6 cases per 1,000 person-years. The infection rate for the unvaccinated was a meager 1.3 percent.
After their placebo period, the group got “fully vaccinated.” In just a few months, this group became more infectious and showed 43.4 cases per 1,000 person-years. Their infection rate went UP by over 300 percent to a 4.34% infection rate. Mrs. Kingston called this “super alarming.”
“They had less infection when they had no protection. So, that’s a problem,” she said.
References:
Are leaky vaccines driving delta variant evolution and making it more deadly?
by el gato malo – bad cattitude – october 10, 2021
one of the great fears in any vaccination campaign is that the vaccine can wind up becoming the driver viral evolution and making the virus more dangerous. this is a special concern around imperfect (so called “leaky”) vaccines that are non-sterilizing. such vaccines do not stop spread or contagion of the virus. this means the virus will have lots of chances to replicate.
when you combine this with a vaccine that reduces severity of cases and prevents deaths in the vaccinated, it’s a bit of a perfect storm. you get full spread but break the evolutionary gradient towards mildness that viruses tend to follow (and that protects humanity from them).
all a virus wants is to replicate. “make a copy of me and pass it on.” that’s the biological imperative of the selfish gene. excel at it, you win. fail, you disappear. simple as that.
killing or harming the host is maladaptive to viral spread. it’s like burning down your own house with your car in the garage. now you have nowhere to live and no way to get around. that’s not a recipe for reproductive fitness.
this is a property of the world, not of the viruses themselves. so it applies to all of them, evolved and lab hotwired alike.
so viruses evolve to become less, not more virulent. they do not want to kill you. ideally, they’d like to help you. figure out how to be a useful symbiote, and you get a huge boost in propagation. (mitochondria were probably bacteria that were so useful, all our cells incorporated them.) so seeing case fatality rate (CFR) rise in a variant of a virus is like watching water flow uphill. it’s not supposed to do that and when it does, you need to suspect some external force acting on it.
and we’re seeing water flow uphill here.
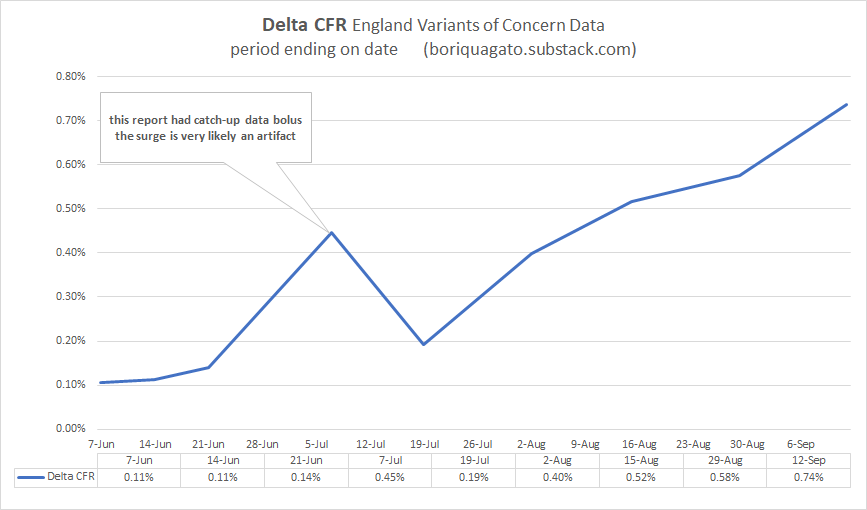
i started with the england variants of concern (VoC) data. it’s the best quality and the best broken out. (the US data is just plain broken. it’s being deliberately scrubbed to prevent analysis like this.) because this data is always aggregated from feb to current period, it does not provide good temporal snapshots, but this can be fixed by subtracting the penultimate report from the current one etc. you subtract report 22’s totals from report 23 and you get just what happened in the last 2 weeks (it used to be a weekly report, now it’s bi-weekly)
what we see is not what one would expect from a virus. none of the other variants (pre vaccine) worked like this. none saw CFR rise like this. and no jump from major variant to variant saw a statistically significant rise in deadliness.
this IS however what one would expect if a virus were undergoing vaccine mediated evolution (as mareks disease did in chickens) and selecting for hotter strains because vaccinated people can carry and spread them and not die.
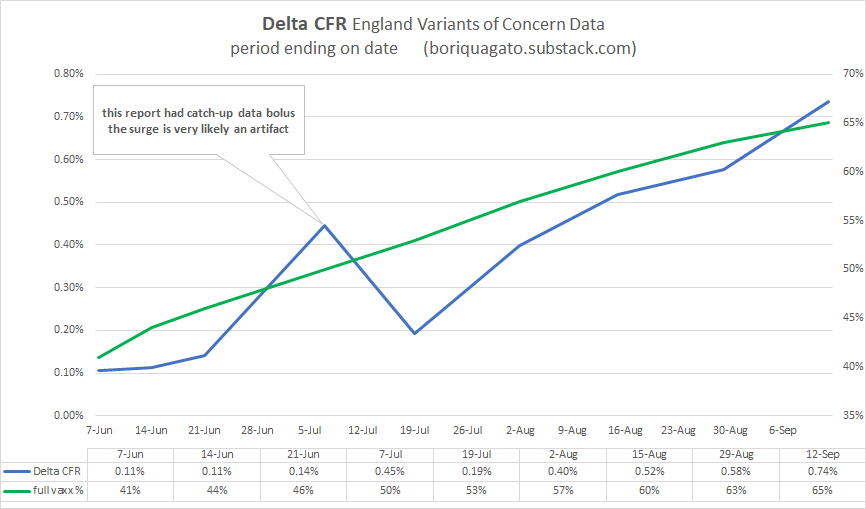
experienced CFR on delta is nearly 7X what it was in the beginning of june and has been galloping since the middle of july.
(note that pretty much all this data has a large artifact in it from the 21 june report (VoC 17). there was a “data-dump” in it where they caught up on a bolus of past data. it’s an artifact, not a signal. best to ignore it. i suspect the curve from mid june to mid july was smooth.)
put simply: this is not good.
delta is rapidly approaching alpha (1.1%) in terms of CFR whereas it used to be 90% lower. (it also means that the reports on delta CFR in these VoC updates are FAR too low because they are a blend of all cases and deaths back to feb, so they are averaging in the low CFR past and are slow to respond to current dynamics)
this is consistent with, but not proof of vaccines mediated evolution. to get there, we need to do better.
so now we need to start ruling things out and validating this claim to see if it’s meaningful.
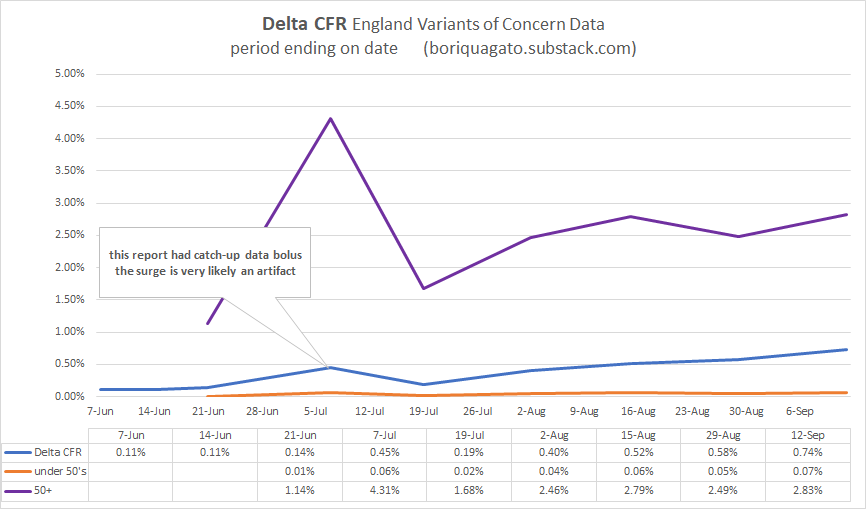
first, it’s not a simpson’s paradox in age data. CFR is rising in over and under 50’s. it’s not mix shift alone. CFR in over 50’s is up 2.5X. it’s up 4-7X in under 50’s.
we’re at about a 3X rise in CFR overall in delta since the summer once we adjust for shifts in age. not as worrying as 7, but still worrying.
and the deaths are real. it’s not made up counting. this can be clearly seen when we comp CFR to the euro-momo Z scores (thoughtfully provided by frequent gato collaborator ben m at USmortality.com. z score is just a measure of deviation from expected all cause deaths. (explained HERE)
alignment is quite strong.
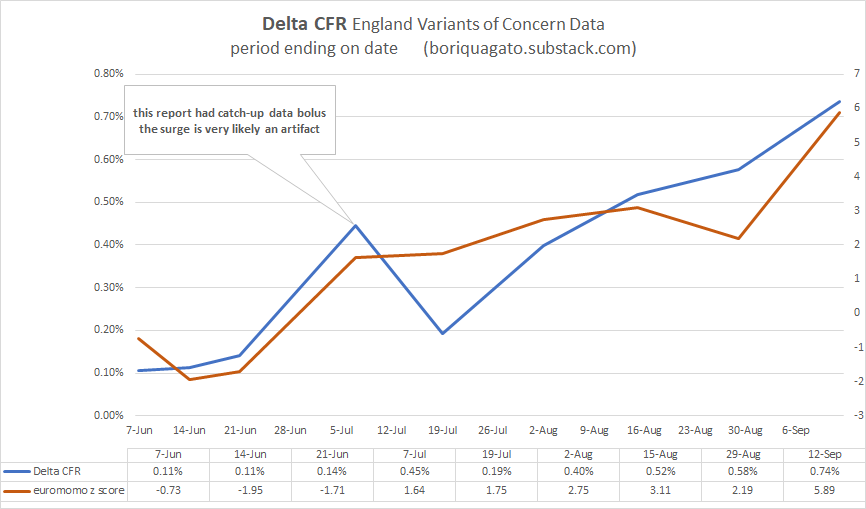
z score was trending negative and spiked to high levels just as CFR really started to ramp up.
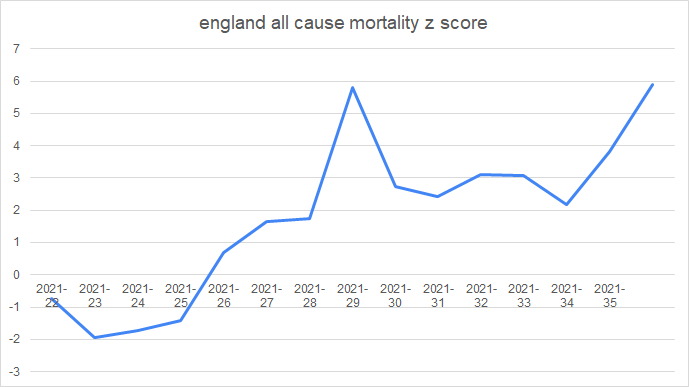
z score for the year can be seen here. starting in wk 22 (may 31) (numbers after the year are weeks)
and given that we know that vaccines DO work to stop deaths in the UK (seemingly in the 50-60% range) it’s even more unexpected that CFR would be rising like this. but it is and the rise in the vaxx rate is not hampering it.
(the precise alignment here is more chart crime than signal, so i’d caution against inferring too much from it)
none of this is what one would expect. not remotely. it bucks evolution, it bucks the other variants, and it flies in the face of late stage pandemic dynamics like increase in acquired immunity (which IS sterilizing), depletion of high risk cohorts, improvements in treatment, etc. all these should be pushing CFR down.
instead, water is flowing uphill.
the question is “why?”
the other day, i discussed ADE (antibody dependent enhancement) where antibodies wind up acting as passkeys for a virus to enter cells and also the fetchingly biblically named OAS (original antigenic sin) whereby preferential training to one antibody response leads to its use against new variants of a pathogen and thereby prevents adaptation to more effective modalities.
note that these two phenomena are by no means mutually exclusive and are actually strongly synergistic.
but are they driving this issue?
i do not not think so.
- if they were, we’d be seeing the CFR rise in the vaccinated but not in the unvaccinated and if it were ALL antibodies, we’d be seeing the previously infected getting hit too. but they are not.
- we’d also likely be seeing low or negative vaccine efficacy (VE) for deaths. but we aren’t. it’s clear the vaccinated are doing better.
CFR is (and has been) much better in the vaccinated than the unvaxxed in UK over 50’s (the highest risk category). trends are similar, but absolute values durably disparate.
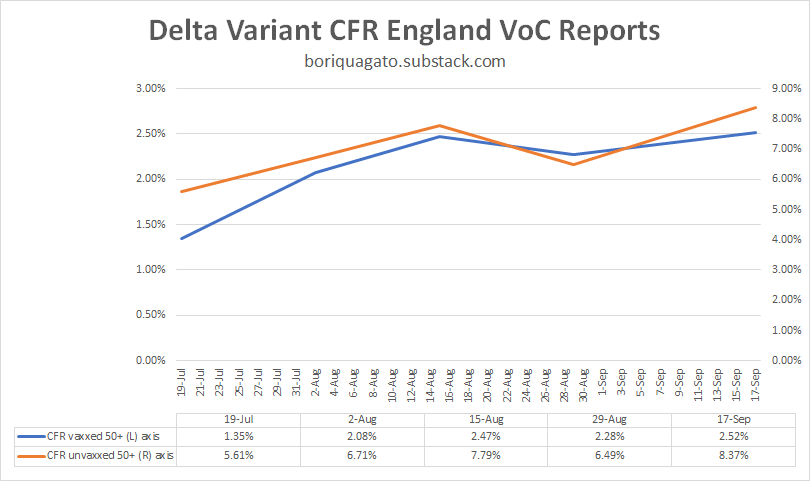
whether and to what extent this is real vaccine efficacy vs cohort bias in a place where 90% of this demographic is vaccinated remains an open issue. it may simply be that only those with the weakest/most compromised immunes systems have not gotten the jab. but this is not really material here.
what IS material is the fact that CFR in the unvaxxed is trending up significantly and so is CFR in the vaxxed. but we’re not seeing many cases of re-infection and almost none of those are serious. this does not look like ADE or OAS as a major driver. if it were, there’s no reason the CFR in the unvaccinated would be rising too.
what this IS consistent with is a variant heating up and getting more and more deadly because it is not checked by normal biological limitations. vaccine mediated evolution (VME) would be very bad news for us.
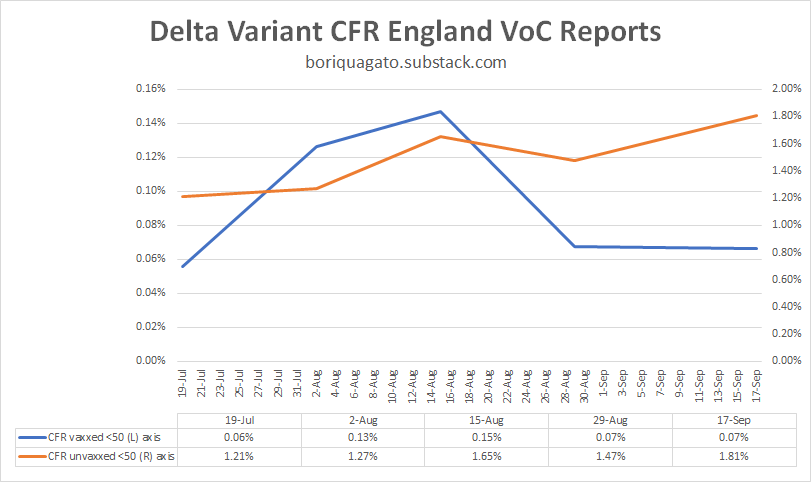
we can see similar in the under 50’s, though the data here is a bit of a mess as during this period, so many very low risk under 50’s (those under 18) got vaccinated that it moved a material risk profile reduction from unvaxxed to vaxxed. i suspect that is why “CFR vaxxed” dropped. it was not vaccines working, it was the vaccinated category being “salted” with large number of the lowest risk folks around. (it also means that group left the unvaxxed, so you get an effect on both)
so i view this data as much lower quality than over 50’s, but it still looks like VME, not ADE or OAS.
this is EXACTLY what leaky vaccines did in chickens.
(read these links. THIS in particular. it’s important.)
such vaccines change the evolutionary gradient for a virus. instead of becoming less virulent/deadly, they can tend the other way because the maladaptiveness of killing the host is mitigated in the vaccinated population. this is what happened with marek’s disease in chickens.
not only is it now more lethal to them than ebola is to humans, making it one of if not THE hottest persistent disease known (killing 100% of unvaxxed birds in 10 days), but, it’s now a disease so hot that an unvaccinated chicken cannot spread it. they die too quickly. only the vaccinated birds spread the nasty strains of mareks. they’re the only ones who live long enough to shed virus.
“Previously, a hot strain was so nasty, it wiped itself out. Now, you keep its host alive with a vaccine, then it can transmit and spread in the world,” Read said. “So it’s got an evolutionary future, which it didn’t have before.”

this is an awful lot of puzzle pieces snapping together and i think we’re really starting to see what this is a picture of.
leaky vaccines that stop severe illness and death but not spread look to be affecting the evolution of the covid 19 virus.
this is an established, predictable, and well supported risk from such vaccines.
this has become my leading hypothesis.
it also explains why we’re seeing such a large rise in deaths relative to cases and deaths and hospitalization overall in so many places. it’s the virus adapting to a stressor we put on it and becoming much more dangerous as a result.
the CFR is a function of the virus, but the virus has become a function of the leaky vaccines.
and it also means the vaccine is protecting no one. yes, it seems to have 50-60% protection against death. but what good is that against a CFR that’s up 300% or more (and rising)? everyone is worse off.

negative VE’s on spread are accelerating cases and this is multiplicative with higher CFR. this is the nightmare scenario and no one is left better off as a result. the CFR among the high risk vaccinated groups is way up too.
everyone is harmed but the brunt is borne by the unvaccinated which perversely winds up looking like better vaccine efficacy. the very fact that vaccines made everyone worse off but spread the misery unevenly makes it look like vaccines are a good idea.
it’s just simple math. if we do something to one group that makes their death rate rise from 1 to 2 per 100 but that also makes the death rate in another group rise from 1 to 4 per 100, that looks like a VE of 50%. in reality, it’s killing 100% more vaxxed people and 300% more of the unvaxxed.
mistaking that gas pedal for the brake and pushing ever harder when you fail to slow would represent an accelerating disaster curve.
that’s the problem with relative measures that ignore absolute changes. you can hide all manner of calamity in such analyses.
it’s still, of course, possible that i’m wrong, but this is looking more and more like it has to be the answer. i can find nothing else fits the facts and the facts themselves are weird enough that “it’s just normal” does not look like a satisfying explanation either and we have enough features here that we can really start testing our puzzle pieces. this one aligns in an AWFUL lot of places.
for something this odd to happen, it takes a truly uncommon exogenous stressor.
i’m just not seeing what else it could be than vaccine mediated selection for hotter variants driving pernicious delta evolution.
so, i’m putting this out to you all to see if you can find some other explanation for what’s going on that fits these facts.
looking forward to the peer review as, honestly, i hope i’m wrong here. this is not an outcome that anyone wants. it’s the nightmare scenario both as a pandemic and as a political horror in the making as if this was an “own-goal”, what would the experts and politicians that pushed this plan not be willing to do to avoid accepting the blame?
because this is career or pharma franchise polonium, and that’s if you’re lucky.
let’s keep at this. one way or the other, we need to know.
the facts do not care about our feelings and epidemiology data is a lousy fabric from which to spin a wubbie to hide under.
we need to get at the truth.
(even if it makes us make a face like this)

Australia Building Quarantine Camps For “Ongoing Operations”

By Paul Joseph Watson | Summit News | October 12, 2021
Despite some states tentatively beginning to lift lockdown restrictions, Australian authorities are building quarantine camps that won’t be completed until next year in order to prepare for “ongoing operations” and to house those “who have not had access to vaccination.”
According to ABC Australia, one such 1,000-bed quarantine facility at Wellcamp Airport outside Toowoomba will be fully completed by the end of March 2022.
“At this stage, the cabins will be used by domestic travellers returning from COVID hotspots,” states the report.
However, it also makes clear that the camp will be used for “ongoing operations” and will be a source of employment for the local area.
The camps is split into different zones and accommodates singles, doubles, and family rooms while being patrolled by police and security guards 24/7.
Citing new strains of COVID and people “who have not had access to vaccination,” Queensland Deputy Premier Steven Miles told the media outlet, “We anticipate there to be a continuing need for quarantine facilities.”
The government is leasing the land on which the camp is being built from the Wagner Corporation for 12 months with an option for a further 12 months after that.
Another 1,000-bed quarantine facility is also being built on a 30-hectare Army barracks site in the industrial area of Pinkenba, near Brisbane Airport.
“Why anyone who had left Australia would come back again is unclear,” writes Dave Blount. “It is possibly the most repressive country in the world regarding Covid tyranny.”
As we previously highlighted, state authorities in America are also constructing new “quarantine facilities” for Americans who are “unable to quarantine at home.”
As we reported last year, Authorities in Quebec City, Canada announced they will isolate “uncooperative” citizens in a coronavirus facility, the location of which remains a secret.
New Zealand also announced plans to place COVID infectees and their family members in “quarantine facilities.”
Back in January, German authorities also announced they would hold COVID dissidents who repeatedly fail to properly follow the rules in what was described as a ‘detention camp’ located in Dresden.
The figures that show the real risk of Covid vaccine in pregnancy
By Sally Beck | TCW Defending Freedom | October 12, 2021
SINCE February, the BBC have been urging pregnant women to take the Covid vaccination despite the fact that no manufacturer will complete a trial in expectant mothers before December this year. Instead, British health chiefs have relied on information from women in the US who accidentally found themselves pregnant after taking the Covid jab, and reported the results of their pregnancy to the V-safe app. V-safe is hosted by the US Centers for Disease Control (CDC) but it is not a scientific study.
This fact has been ignored, notably by Lucy Chappell, Professor in Obstetrics at King’s College London, and the BBC, to tell women it is safe to go ahead and get the jab.
If that were the case, there would be no related adverse reactions reported to the Medicines and Healthcare products Regulatory Agency (MHRA), the drug company-funded government body collating information on Covid vaccination safety.
But it is there in black and white: miscarriages, stillbirths and one foetal death have been reported, 590 to date, 12 last week alone. Pfizer have one third more reports than AstraZeneca and Moderna, primarily because the AZ jab has been suspended for under-40s and the Moderna has been in use only since April, while the Pfizer has been available since December 2020. Women in their 30s were invited to receive the jab in May so those of child-bearing age have officially been receiving the vaccine for around four months.
The MHRA is not concerned about the figures and says: ‘The numbers of reports of miscarriage and stillbirth are low in relation to the number of pregnant women who have received Covid-19 vaccines to date (more than 92,000 up to end of August 2021) and how commonly these events occur in the UK outside of the pandemic. There is no pattern from the reports to suggest that any of the Covid-19 vaccines used in the UK, or any reactions to these vaccines, increase the risk of miscarriage or stillbirth.’ No further detail is provided so it is not possible to scrutinise the figures.
This sounds reassuring, but when American investigative journalist Jefferey Jaxen analysed a study by 21 authors analysing data from V-safe published in the prestigious New England Journal of Medicine, he discovered they had manipulated the figures. He was not the only one and Dr Hong Sun PhD, from Dedalus Healthcare, Antwerp, Belgium, complained to the NEJM editor.
The published figures showed a rate of 12.6 per cent miscarriage in women 20 weeks pregnant and under, which is similar to pre-Covid figures and raises no red flags. They did not include 700 reports of miscarriage in women over 20 weeks pregnant. Once those figures were added, the miscarriage rate increased to 82 per cent.
As always, the devil is in the detail, and without additional detail from the MHRA or Big Pharma, it is impossible to tell whether British women should be worried.
Latest Yellow Card scheme figures are published below with 1,698 fatalities reported. That’s an increase of 66 deaths in the three weeks since we published the last figures from September 9.
Updated report published October 7, 2021
MHRA Yellow Card Reporting up to September 29, 2021
• Pfizer BioNTech: 22.5million people – 42.1m doses – Yellow Card reporting rate 1 in 189 people impacted
• Oxford/AstraZeneca: 24.9m people – 48.9m doses – Yellow Card reporting rate 1 in 106 people impacted
• Moderna: 1.4m people – 2.6m doses – Yellow Card reporting rate 1 in 84 people impacted
Overall, 1 in 132 people injected experiences and reports a Yellow Card Adverse Event. A significant proportion require urgent medical care, and the effects may be life-changing or long-lasting. The MHRA says as few as 10 per cent of reactions may be reported.
Reactions – 335,344 (Pfizer) + 830,818 (AZ) + 53,032 (Moderna) + 3,372 (Unknown) = 1,222,566
Reports – 118,970 (Pfizer) + 233,904 (AZ) + 16,582 (Moderna) + 1118 (Unknown) = 370,574 people impacted
Fatal – 552 (Pfizer) + 1097 (AZ) + 19 (Moderna) + 30 (Unknown) = 1,698
Blood Disorders – 11,342 (Pfizer) + 7474 (AZ) + 972 (Moderna) + 47 (Unknown) = 19,835
Anaphylaxis – 486 (Pfizer) + 820 (AZ) + 40 (Moderna) + 1 (Unknown) = 1,347
Acute Cardiac – 5,734 (Pfizer) + 9,474 (AZ) + 671 (Moderna) + 42 (Unknown) = 15,921
Pericarditis/Myocarditis (Heart inflammation) – 560 (Pfizer) + 288 (AZ) + 126 (Moderna) + 2 (Unknown) = 976
Infections – 7,902 (Pfizer) + 18,572 (AZ) + 883 (Moderna) + 96 (Unknown) = 27,453
Herpes – 1,666 (Pfizer) + 2,524 (AZ) + 93 (Moderna) + 15 (Unknown) = 4,298
Headaches & Migraines – 26,145 (Pfizer) + 92,289 (AZ) + 3610 (Moderna) + 266 (Unknown) = 122,310
Eye Disorders – 5,562 (Pfizer) + 14,044 (AZ) + 601 (Moderna) + 62 (Unknown) = 20,269
Blindness – 107 (Pfizer) + 292 (AZ) + 16 (Moderna) + 4 (Unknown) = 419
Deafness – 205 (Pfizer) + 372 (AZ) + 17 (Moderna) + 2 (Unknown) = 596
Spontaneous Abortions – 346 + 8 stillbirth/foetal death (Pfizer) + 207 + 3 stillbirth (AZ) + 35 + 1 foetal death (Moderna) + 2 (Unknown) = 590 + 12
Skin Disorders – 23,303 (Pfizer) + 51,098 (AZ) + 7,418 (Moderna) + 238 (Unknown) = 82,057
Psychiatric Disorders – 6,970 (Pfizer) + 17,425 (AZ) + 1,070 (Moderna) + 77 (Unknown) = 25,542
Facial Paralysis incl. Bell’s Palsy – 757 (Pfizer) + 913 (AZ) + 58 (Moderna) + 7 (Unknown) = 1,735
Strokes and CNS haemorrhages – 525 (Pfizer) + 2094 (AZ) + 19 (Moderna) + 10 (Unknown) = 2,648
Guillain-Barré Syndrome – 53 (Pfizer) + 428 (AZ) + 3 (Moderna) + 5 (Unknown) = 489
Nervous System Disorders – 57,975 (Pfizer) + 176,644 (AZ) + 8,321 (Moderna) + 633 (Unknown) = 243,573
BCG Scar Reactivation – 46 (Pfizer) + 35 (AZ) + 30 (Moderna) + 1 (Unknown) = 112
Respiratory Disorders – 14,352 (Pfizer) + 29,009 (AZ) + 1420 (Moderna) + 120 (Unknown) = 43,901
Pulmonary Embolism & Deep Vein Thrombosis – 618 (Pfizer) + 2,806 (AZ) + 23 (Moderna) + 20 (Unknown) = 3,467
Seizures – 789 (Pfizer) + 1,926 (AZ) + 140 (Moderna) + 12 (Unknown) = 2,867
Paralysis – 327 (Pfizer) + 786 (AZ) + 42 (Moderna) + 6 (Unknown) = 1,161
Nosebleeds – 782 (Pfizer) + 2242 (AZ) + 82 (Moderna) + 9 (Unknown) = 3,115
Dizziness – 9,123 (Pfizer) + 24,486 (AZ) + 1654 (Moderna) + 91 (Unknown) = 35,354
Renal/Urinary Disorders – 915 (Pfizer) + 2,590 (AZ) + 116 (Moderna) + 23 (Unknown) = 3,644
Vomiting – 3,609 (Pfizer) + 11,423 (AZ) + 657 (Moderna) + 42 (Unknown) = 15,731
Reproductive/Breast Disorders – 21,797 (Pfizer) + 18,593 (AZ) + 2893 (Moderna) + 149 (Unknown) = 43,432
Sen. Ron Johnson Shares COVID-19 Data from Public Health England, Refutes “Pandemic of The Unvaccinated” Narrative
The Last Refuge | October 3, 2021
Senator Ron Johnson (R-Wisconsin) used his time on the Senate floor to discuss recently released COVID-19 data from Public Health England in the U.K. [DATA pdf Here]
Ironically, Senator Johnson is forced to use the Senate floor to share the information in an effort to stop government and Big Tech censorship of the discussion. Unlike the rest of the nation, the House and Senate chamber rules create a free speech zone that prohibits anyone from censoring congressional debate and discussion.
Senator Johnson outlines data from the U.K. clearly showing the vaccines offer no protection from the claimed Delta variant. COVID-19 is carried and shed by vaccinated individuals. The subsequent rate of COVID-19 hospitalization and COVID-19 death appears unaffected by the vaccine itself. WATCH:
As Senator Johnson notes: 63% of the deaths in the U.K. during the 7 month period being discussed were among the vaccinated population.
The data Ron Johnson is sharing is available HERE in pdf form
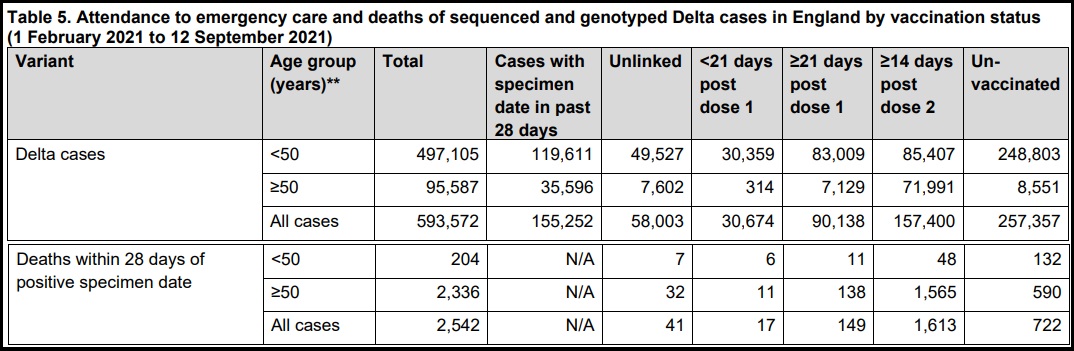
SOURCE: Page 19, 20 – Table 5

Natural Immunity and Covid-19: Twenty-Nine Scientific Studies to Share with Employers, Health Officials, and Politicians
BROWNSTONE INSTITUTE | OCTOBER 10, 2021
From the beginning of the March 2020 lockdowns for the SARS-CoV-2 virus, the subject of natural immunity (also called post-infection immunity) has been neglected. Once the vaccination became widely available, what began with near silence at the beginning turned nearly into a complete blackout of the topic.
Even now, there is an absence of open discussion, presumably in the interests of promoting universal vaccination and required documentation of such vaccination as a condition of participating in public life and even the jobs marketplace. Still, the science exists. Many studies exist. Their authors deserve credit, recognition, and to have their voices heard.
These studies demonstrate what was and is already known: natural immunity for a SARS-type virus is robust, long-lasting, and broadly effective even in the case of mutations, generally more so than vaccines. In fact, a major contribution of 20th-century science has been to expand upon and further elucidate this principle that has been known since the ancient world. Every expert presumably knew this long before the current debates. The effort to pretend otherwise is a scientific scandal of the highest order, especially because the continued neglect of the topic is affecting the rights and freedoms of billions of people.
People who have contracted the virus and recovered deserve recognition. For that matter, people who prefer an exposure risk to the virus in order to gain robust immunity deserve the freedom to make that choice. The realization that natural immunity – which pertains now to perhaps half of the US population and billions around the world – is effective in providing protection should have a dramatic effect on vaccine mandates.
Individuals whose livelihoods and liberties are being deprecated and deleted need access to the scientific literature as it pertains to this virus. They should send a link to this page far and wide. The scientists have not been silent; they just haven’t received the public attention they deserve. The preparation of this list was assisted by links provided by Paul Elias Alexander and Rational Ground’s own cheat sheet on natural immunity, which also includes links to popular articles on the topic.
1. One-year sustained cellular and humoral immunities of COVID-19 convalescents, by Jie Zhang, Hao Lin, Beiwei Ye, Min Zhao, Jianbo Zhan, et al. Clinical Infectious Diseases, October 5, 2021. “SARS-CoV-2-specific IgG antibodies, and also NAb can persist among over 95% COVID-19 convalescents from 6 months to 12 months after disease onset. At least 19/71 (26%) of COVID-19 convalescents (double positive in ELISA and MCLIA) had detectable circulating IgM antibody against SARS-CoV-2 at 12m post-disease onset. Notably, the percentages of convalescents with positive SARS-CoV-2-specific T-cell responses (at least one of the SARS-CoV-2 antigen S1, S2, M and N protein) were 71/76 (93%) and 67/73 (92%) at 6m and 12m, respectively. Furthermore, both antibody and T-cell memory levels of the convalescents were positively associated with their disease severity.”
2. Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections, by Sivan Gazit, Roei Shlezinger, Galit Perez, Roni Lotan, Asaf Peretz, Amir Ben-Tov, Dani Cohen, Khitam Muhsen, Gabriel Chodick, Tal Patalon. MedRxiv, August 25, 2021. “Our analysis demonstrates that SARS-CoV-2-naïve vaccinees had a 13.06-fold increased risk for breakthrough infection with the Delta variant compared to those previously infected, when the first event (infection or vaccination) occurred during January and February of 2021. The increased risk was significant for a symptomatic disease as well…. This analysis demonstrated that natural immunity affords longer lasting and stronger protection against infection, symptomatic disease and hospitalization due to the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity.”
3. Shedding of Infectious SARS-CoV-2 Despite Vaccination, by Kasen K. Riemersma, Brittany E. Grogan, Amanda Kita-Yarbro, Gunnar E. Jeppson, David H. O’Connor, Thomas C. Friedrich, Katarina M. Grande, MedRxiv, August 24, 2021. “The SARS-CoV-2 Delta variant might cause high viral loads, is highly transmissible, and contains mutations that confer partial immune escape. Outbreak investigations suggest that vaccinated persons can spread Delta. We compared RT-PCR cycle threshold (Ct) data from 699 swab specimens collected in Wisconsin 29 June through 31 July 2021 and tested with a qualitative assay by a single contract laboratory. Specimens came from residents of 36 counties, most in southern and southeastern Wisconsin, and 81% of cases were not associated with an outbreak. During this time, estimated prevalence of Delta variants in Wisconsin increased from 69% to over 95%. Vaccination status was determined via self-reporting and state immunization records.”
4. Necessity of COVID-19 vaccination in previously infected individuals, by Nabin K. Shrestha, Patrick C. Burke, Amy S. Nowacki, Paul Terpeluk, Steven M. Gordon, MedRxiv, June 5, 2021. “Individuals who have had SARS-CoV-2 infection are unlikely to benefit from COVID-19 vaccination, and vaccines can be safely prioritized to those who have not been infected before.”
5. Large-scale study of antibody titer decay following BNT162b2 mRNA vaccine or SARS-CoV-2 infection, by Ariel Israel, Yotam Shenhar, Ilan Green, Eugene Merzon, Avivit Golan-Cohen, Alejandro A Schäffer, Eytan Ruppin, Shlomo Vinker, Eli Magen. MedRxiv, August 22, 2021. “This study demonstrates individuals who received the Pfizer-BioNTech mRNA vaccine have different kinetics of antibody levels compared to patients who had been infected with the SARS-CoV-2 virus, with higher initial levels but a much faster exponential decrease in the first group.”
6. Discrete Immune Response Signature to SARS-CoV-2 mRNA Vaccination Versus Infection, by Ellie Ivanova, Joseph Devlin, et al. Cell, May 2021. “While both infection and vaccination induced robust innate and adaptive immune responses, our analysis revealed significant qualitative differences between the two types of immune challenges. In COVID-19 patients, immune responses were characterized by a highly augmented interferon response which was largely absent in vaccine recipients.”
7. SARS-CoV-2 infection induces long-lived bone marrow plasma cells in humans, by Jackson S. Turner, Wooseob Kim, Elizaveta Kalaidina, Charles W. Goss, Adriana M. Rauseo, Aaron J. Schmitz, Lena Hansen, Alem Haile, Michael K. Klebert, Iskra Pusic, Jane A. O’Halloran, Rachel M. Presti, Ali H. Ellebedy. Nature, May 24, 2021. “This study sought to determine whether infection with SARS-CoV-2 induces antigen-specific long-lived BMPCs in humans. We detected SARS-CoV-2 S-specific BMPCs in bone marrow aspirates from 15 out of 19 convalescent individuals, and in none from the 11 control participants…. Overall, our results are consistent with SARS-CoV-2 infection eliciting a canonical T-cell-dependent B cell response, in which an early transient burst of extrafollicular plasmablasts generates a wave of serum antibodies that decline relatively quickly. This is followed by more stably maintained levels of serum antibodies that are supported by long-lived BMPCs.”
8. Longitudinal analysis shows durable and broad immune memory after SARS-CoV-2 infection with persisting antibody responses and memory B and T cells, by Kristen W. Cohen, Susanne L. Linderman, Zoe Moodie, Julie Czartoski, Lilin Lai, Grace Mantus, Carson Norwood, Lindsay E. Nyhoff, Venkata Viswanadh Edara, et al. MedRxiv, April 27, 2021. “Ending the COVID-19 pandemic will require long-lived immunity to SARS-CoV-2. We evaluated 254 COVID-19 patients longitudinally from early infection and for eight months thereafter and found a predominant broad-based immune memory response. SARS-CoV-2 spike binding and neutralizing antibodies exhibited a bi-phasic decay with an extended half-life of >200 days suggesting the generation of longer-lived plasma cells. In addition, there was a sustained IgG+ memory B cell response, which bodes well for a rapid antibody response upon virus re-exposure.”
9. Incidence of Severe Acute Respiratory Syndrome Coronavirus-2 infection among previously infected or vaccinated employees, by N Kojima, A Roshani, M Brobeck, A Baca, JD Klausner. MedRxiv, July 8, 2021. “Previous SARS-CoV-2 infection and vaccination for SARS-CoV-2 were associated with decreased risk for infection or re-infection with SARS-CoV-2 in a routinely screened workforce. The was no difference in the infection incidence between vaccinated individuals and individuals with previous infection. Further research is needed to determine whether our results are consistent with the emergence of new SARS-CoV-2 variants.”
10. Single cell profiling of T and B cell repertoires following SARS-CoV-2 mRNA vaccine, by Suhas Sureshchandra, Sloan A. Lewis, Brianna Doratt, Allen Jankeel, Izabela Ibraim, Ilhem Messaoudi. BioRxiv, July 15, 2021. “Interestingly, clonally expanded CD8 T cells were observed in every vaccinee, as observed following natural infection. TCR gene usage, however, was variable, reflecting the diversity of repertoires and MHC polymorphism in the human population. Natural infection induced expansion of larger CD8 T cell clones occupied distinct clusters, likely due to the recognition of a broader set of viral epitopes presented by the virus not seen in the mRNA vaccine. Our study highlights a coordinated adaptive immune response where early CD4 T cell responses facilitate the development of the B cell response and substantial expansion of effector CD8 T cells, together capable of contributing to future recall responses.”
11. mRNA vaccine-induced T cells respond identically to SARS-CoV-2 variants of concern but differ in longevity and homing properties depending on prior infection status, Jason Neidleman, Xiaoyu Luo, Matthew McGregor, Guorui Xie, Victoria Murray, Warner C. Greene, Sulggi A. Lee, Nadia R. Roan. BioRxiv, July 29, 2021. “In infection-naïve individuals, the second dose boosted the quantity and altered the phenotypic properties of SARS-CoV-2-specific T cells, while in convalescents the second dose changed neither. Spike-specific T cells from convalescent vaccinees differed strikingly from those of infection-naïve vaccinees, with phenotypic features suggesting superior long-term persistence and ability to home to the respiratory tract including the nasopharynx. These results provide reassurance that vaccine-elicited T cells respond robustly to emerging viral variants, confirm that convalescents may not need a second vaccine dose, and suggest that vaccinated convalescents may have more persistent nasopharynx-homing SARS-CoV-2-specific T cells compared to their infection-naïve counterparts.”
12. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection, Jennifer M. Dan, Jose Mateus, Yu Kato, Kathryn M. Hastie, et al., Science, January 6, 2021. “Understanding immune memory to SARS-CoV-2 is critical for improving diagnostics and vaccines, and for assessing the likely future course of the COVID-19 pandemic. We analyzed multiple compartments of circulating immune memory to SARS-CoV-2 in 254 samples from 188 COVID-19 cases, including 43 samples at ≥ 6 months post-infection. IgG to the Spike protein was relatively stable over 6+ months. Spike-specific memory B cells were more abundant at 6 months than at 1 month post symptom onset. SARS-CoV-2-specific CD4+ T cells and CD8+ T cells declined with a half-life of 3-5 months. By studying antibody, memory B cell, CD4+ T cell, and CD8+ T cell memory to SARS-CoV-2 in an integrated manner, we observed that each component of SARS-CoV-2 immune memory exhibited distinct kinetics.”
13. Persistence of neutralizing antibodies a year after SARS-CoV-2 infection, by Anu Haveri, Nina Ekström, Anna Solastie, Camilla Virta, Pamela Österlund, Elina Isosaari, Hanna Nohynek, Arto A. Palmu, Merit Melin. MedRxiv, July 16, 2021. “We assessed the persistence of serum antibodies following wild-type SARS-CoV-2 infection six and twelve months after diagnosis in 367 individuals of whom 13% had severe disease requiring hospitalization. We determined the SARS-CoV-2 spike (S-IgG) and nucleoprotein IgG concentrations and the proportion of subjects with neutralizing antibodies (NAb).”
14. Quantifying the risk of SARS‐CoV‐2 reinfection over time, by Eamon O Murchu, Paula Byrne, Paul G. Carty, et al. Rev Med Virol. 2021. “Reinfection was an uncommon event (absolute rate 0%–1.1%), with no study reporting an increase in the risk of reinfection over time. Only one study esti- mated the population‐level risk of reinfection based on whole genome sequencing in a subset of patients; the estimated risk was low (0.1% [95% CI: 0.08–0.11%]) with no evidence of waning immunity for up to 7 months following primary infection. These data suggest that naturally acquired SARS‐CoV‐2 immunity does not wane for at least 10 months post‐infection. However, the applicability of these studies to new variants or to vaccine‐induced immunity remains uncertain.”
15. SARS-CoV-2 antibody-positivity protects against reinfection for at least seven months with 95% efficacy, by Laith J. Abu-Raddad, Hiam Chemaitelly, Peter Coyle, Joel A. Malek. The Lancet, July 27, 2021. “Reinfection is rare in the young and international population of Qatar. Natural infection appears to elicit strong protection against reinfection with an efficacy ~95% for at least seven months.”
16. Natural immunity against COVID-19 significantly reduces the risk of reinfection: findings from a cohort of sero-survey participants, by Bijaya Kumar Mishra, Debdutta Bhattacharya, Jaya Singh Kshatri, Sanghamitra Pati. MedRxiv, July 19, 2021. “These findings reinforce the strong plausibility that development of antibody following natural infection not only protects against re-infection by the virus to a great extent, but also safeguards against progression to severe COVID-19 disease.”
17. Protection of previous SARS-CoV-2 infection is similar to that of BNT162b2 vaccine protection: A three-month nationwide experience from Israel, by Yair Goldberg, Micha Mandel, Yonatan Woodbridge, Ronen Fluss, Ilya Novikov, Rami Yaari, Arnona Ziv, Laurence Freedman, Amit Huppert, et al.. MedRxiv, April 24, 2021. “Similarly, the overall estimated level of protection from prior SARS-CoV-2 infection for documented infection is 94·8% (CI:[94·4, 95·1]); hospitalization 94·1% (CI:[91·9, 95·7]); and severe illness 96·4% (CI:[92·5, 98·3]). Our results question the need to vaccinate previously-infected individuals.”
18. Immune Memory in Mild COVID-19 Patients and Unexposed Donors Reveals Persistent T Cell Responses After SARS-CoV-2 Infection, by Asgar Ansari, Rakesh Arya, Shilpa Sachan, Someshwar Nath Jha, Anurag Kalia, Anupam Lall, Alessandro Sette, et al. Front Immunol. March 11, 2021. “Using HLA class II predicted peptide megapools, we identified SARS-CoV-2 cross-reactive CD4+ T cells in around 66% of the unexposed individuals. Moreover, we found detectable immune memory in mild COVID-19 patients several months after recovery in the crucial arms of protective adaptive immunity; CD4+ T cells and B cells, with a minimal contribution from CD8+ T cells. Interestingly, the persistent immune memory in COVID-19 patients is predominantly targeted towards the Spike glycoprotein of the SARS-CoV-2. This study provides the evidence of both high magnitude pre-existing and persistent immune memory in Indian population.”
19. Live virus neutralisation testing in convalescent patients and subjects vaccinated against 19A, 20B, 20I/501Y.V1 and 20H/501Y.V2 isolates of SARS-CoV-2, by Claudia Gonzalez, Carla Saade, Antonin Bal, Martine Valette, et al, MedRxiv, May 11, 2021. “ No significant difference was observed between the 20B and 19A isolates for HCWs with mild COVID-19 and critical patients. However, a significant decrease in neutralisation ability was found for 20I/501Y.V1 in comparison with 19A isolate for critical patients and HCWs 6-months post infection. Concerning 20H/501Y.V2, all populations had a significant reduction in neutralising antibody titres in comparison with the 19A isolate. Interestingly, a significant difference in neutralisation capacity was observed for vaccinated HCWs between the two variants whereas it was not significant for the convalescent groups.”
20. Highly functional virus-specific cellular immune response in asymptomatic SARS-CoV-2 infection, by Nina Le Bert, Hannah E. Clapham, Anthony T. Tan, Wan Ni Chia, et al, Journal of Experimental Medicine, March 1, 2021. “Thus, asymptomatic SARS-CoV-2–infected individuals are not characterized by weak antiviral immunity; on the contrary, they mount a highly functional virus-specific cellular immune response.”
21. SARS-CoV-2-specific T cell memory is sustained in COVID-19 convalescent patients for 10 months with successful development of stem cell-like memory T cells, Jae Hyung Jung, Min-Seok Rha, Moa Sa, Hee Kyoung Choi, Ji Hoon Jeon, et al, Nature Communications, June 30, 2021. “In particular, we observe sustained polyfunctionality and proliferation capacity of SARS-CoV-2-specific T cells. Among SARS-CoV-2-specific CD4+ and CD8+ T cells detected by activation-induced markers, the proportion of stem cell-like memory T (TSCM) cells is increased, peaking at approximately 120 DPSO. Development of TSCM cells is confirmed by SARS-CoV-2-specific MHC-I multimer staining. Considering the self-renewal capacity and multipotency of TSCM cells, our data suggest that SARS-CoV-2-specific T cells are long-lasting after recovery from COVID-19, thus support the feasibility of effective vaccination programs as a measure for COVID-19 control.”
22. Antibody Evolution after SARS-CoV-2 mRNA Vaccination, by Alice Cho, Frauke Muecksch, Dennis Schaefer-Babajew, Zijun Wang, et al, BioRxiv, et al, BioRxiv, July 29, 2021. “We conclude that memory antibodies selected over time by natural infection have greater potency and breadth than antibodies elicited by vaccination. These results suggest that boosting vaccinated individuals with currently available mRNA vaccines would produce a quantitative increase in plasma neutralizing activity but not the qualitative advantage against variants obtained by vaccinating convalescent individuals.” Newer version reads: “These results suggest that boosting vaccinated individuals with currently available mRNA vaccines will increase plasma neutralizing activity but may not produce antibodies with breadth equivalent to those obtained by vaccinating convalescent individuals.”
23. Differential effects of the second SARS-CoV-2 mRNA vaccine dose on T cell immunity in naïve and COVID-19 recovered individuals, by Carmen Camara, Daniel Lozano-Ojalvo, Eduardo Lopez-Granados. Et al., BioRxiv, March 27, 2021. “While a two-dose immunization regimen with the BNT162b2 vaccine has been demonstrated to provide a 95% efficacy in naïve individuals, the effects of the second vaccine dose in individuals who have previously recovered from natural SARS-CoV-2 infection has been questioned. Here we characterized SARS-CoV-2 spike-specific humoral and cellular immunity in naïve and previously infected individuals during full BNT162b2 vaccination. Our results demonstrate that the second dose increases both the humoral and cellular immunity in naïve individuals. On the contrary, the second BNT162b2 vaccine dose results in a reduction of cellular immunity in COVID-19 recovered individuals, which suggests that a second dose, according to the current standard regimen of vaccination, may be not necessary in individuals previously infected with SARS-CoV-2.”
24. COVID-19 natural immunity: Scientific Brief. World Health Organization. May 10, 2021. “Available scientific data suggests that in most people immune responses remain robust and protective against reinfection for at least 6-8 months after infection (the longest follow up with strong scientific evidence is currently approximately 8 months). Some variant SARS-CoV-2 viruses with key changes in the spike protein have a reduced susceptibility to neutralization by antibodies in the blood. While neutralizing antibodies mainly target the spike protein, cellular immunity elicited by natural infection also target other viral proteins, which tend to be more conserved across variants than the spike protein.”
25. SARS-CoV-2 re-infection risk in Austria, by Stefan Pilz, Ali Chakeri, John Pa Ioannidis, et al. Eur J Clin Invest. April 2021. “We recorded 40 tentative re-infections in 14 840 COVID-19 survivors of the first wave (0.27%) and 253 581 infections in 8 885 640 individuals of the remaining general population (2.85%) translating into an odds ratio (95% confidence interval) of 0.09 (0.07 to 0.13). We observed a relatively low re-infection rate of SARS-CoV-2 in Austria. Protection against SARS-CoV-2 after natural infection is comparable with the highest available estimates on vaccine efficacies. Further well-designed research on this issue is urgently needed for improving evidence-based decisions on public health measures and vaccination strategies.”
26. Anti-spike antibody response to natural SARS-CoV-2 infection in the general population, by Jia Wei, Philippa C. Matthews, Nicole Stoesser, et al, MedRxiv, July 5, 2021. “We estimated antibody levels associated with protection against reinfection likely last 1.5-2 years on average, with levels associated with protection from severe infection present for several years. These estimates could inform planning for vaccination booster strategies.”
27. SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: a large, multicentre, prospective cohort study (SIREN), by Victoria Jane Hall, FFPH, Sarah Foulkes, MSc, Andre Charlett, PhD, Ana Atti, MSc, et al. The Lancet, April 29, 2021. “A previous history of SARS-CoV-2 infection was associated with an 84% lower risk of infection, with median protective effect observed 7 months following primary infection. This time period is the minimum probable effect because seroconversions were not included. This study shows that previous infection with SARS-CoV-2 induces effective immunity to future infections in most individuals.”
28. SARS-CoV-2 Natural Antibody Response Persists for at Least 12 Months in a Nationwide Study From the Faroe Islands, by Maria Skaalum Petersen, Cecilie Bo Hansen, Marnar Fríheim Kristiansen, et al, Open Forum Infectious Diseases, Volume 8, Issue 8, August 2021. “Although the protective role of antibodies is currently unknown, our results show that SARS-CoV-2 antibodies persisted at least 12 months after symptom onset and maybe even longer, indicating that COVID-19-convalescent individuals may be protected from reinfection. Our results represent SARS-CoV-2 antibody immunity in nationwide cohorts in a setting with few undetected cases, and we believe that our results add to the understanding of natural immunity and the expected durability of SARS-CoV-2 vaccine immune responses. Moreover, they can help with public health policy and ongoing strategies for vaccine delivery.
29. Associations of Vaccination and of Prior Infection With Positive PCR Test Results for SARS-CoV-2 in Airline Passengers Arriving in Qatar, by Roberto Bertollini, MD, MPH1; Hiam Chemaitelly, MSc2; Hadi M. Yassine. JAMA Research Letter, June 9, 2021. “Of 9180 individuals with no record of vaccination but with a record of prior infection at least 90 days before the PCR test (group 3), 7694 could be matched to individuals with no record of vaccination or prior infection (group 2), among whom PCR positivity was 1.01% (95% CI, 0.80%-1.26%) and 3.81% (95% CI, 3.39%-4.26%), respectively. The relative risk for PCR positivity was 0.22 (95% CI, 0.17-0.28) for vaccinated individuals and 0.26 (95% CI, 0.21-0.34) for individuals with prior infection compared with no record of vaccination or prior infection.”
Articles in the popular media
Why COVID-19 Vaccines Should Not Be Required for All Americans, by Marty Makary, US News, August 21, 2021
Having SARS-CoV-2 once confers much greater immunity than a vaccine—but vaccination remains vital, by Meredith Wadson, Science, August 26, 2021
Natural infection vs vaccination: Which gives more protection? By David Rosenberg, Israeli National News, July 13, 2021.
Flu survivors still immune after 90 years, by Ed Yong, National Geographic, August 17, 2008.
Rescind Vaccine Mandates: Open Letter to Medical Societies, Hospitals, Clinics, and Other Healthcare Facilities, Association of American Physicians and Surgeons, August 31, 2021.
University Vaccine Mandates Violate Medical Ethics, By Aaron Kheriaty and Gerard V. Bradley, Wall Street Journal, June 14, 2021.
Immunity to the Coronavirus May Last Years, New Data Hint, by Apoorva Mandavilli, New York Times, November 17, 2020.
COVID-19 induces lasting antibody protection, Tamari Bhandara, Washington University School of Medicine, May 24, 2021.
The World Health Organization Oversold the Vaccine and Deprecated Natural Immunity, by Jeffrey Tucker, Brownstone Institute, August 29, 2021.
Why Does the CDC Recognize Natural Immunity for Chicken Pox but Not Covid? By Paul Elias Alexander, Brownstone Institute, September 17, 2021.
Rand Paul and Xavier Becerra Square Off on Natural Immunity, with Devastating Results, by Brownstone Institute, October 2, 2021.
Lockdowns, Mandates, and Natural Immunity: Kulldorff vs. Offit, by Brownstone Institute, October 6, 2021.
Hospitals Should Hire, Not Fire, Nurses with Natural Immunity, by Martin Kulldorff, October 1, 2021.
The Strange Neglect of Natural Immunity, by Jayanta Bhattacharya, Brownstone Institute, July 28, 2021.
The Brownstone Institute for Social and Economic Research is a nonprofit organization conceived of in May 2021 in support of a society that minimizes the role of violence in public life.
Critics love Fauci’s new documentary, but audience hate it and accuse Rotten Tomatoes of ‘hiding’ low score

RT | October 11, 2021
Critics have almost universally praised the new documentary on Dr. Anthony Fauci, but audiences have seemingly hated it, even accusing review aggregator Rotten Tomatoes of trying to hide the movie’s unpopularity.
National Geographic’s ‘Fauci’ has been playing in select cinemas since September 10 and premiered on the Disney Plus streaming service last week. Trailers for the film focus heavily on Fauci and his work combating Covid-19, during which time he has become one of the more controversial figures in American politics.
The film, however, takes a positive look at Fauci and focuses more on tales about the health figure from his family, as well as public figures the infectious disease expert has worked with in the past, such as U2 frontman Bono and former President George W. Bush.
On Rotten Tomatoes, which aggregates reviews from selected critics and then gives a ‘rotten’ or ‘fresh’ score, the film holds a 91% positive rating, based on 30 positive reviews and three negative. The rating from audience members, however, was conspicuously missing from the website until Monday. As of Sunday, only one review, which was negative, had been posted despite the film being out for weeks.
The site was accused of ‘hiding’ the audience score in an effort to spin the movie’s increasingly negative coverage.
On Monday, an audience score did appear, and it showed valleys of difference in opinion from critics to the audience, with users awarding the film a 2% average from over 250 ratings (though it began with a 4% rating that has continually dropped). Despite the average now showing, there is still a lack of actual user reviews on the site, though many users may have chosen to simply drop a rating instead of writing a review.
“Two Americas,” writer Josh Jordan tweeted, including a screenshot of the ‘Tomatometer’ for ‘Fauci’ along with the recently-released comedy special from Dave Chappelle, which has been labeled transphobic by critics, but has been a popular title on Netflix. Critics on Rotten Tomatoes gave the movie a ‘rotten’ score of 33% while audiences awarded a near perfect score.
Fauci critics were quick to mock the film’s near-universal panning from audience members.
The Rotten Tomatoes score for ‘Fauci’ is just the tip of the iceberg when it comes to negative reviews. On IMDB, the movie has a 1.5 rating from over 6000 users.
Trailers for the movie on YouTube haven’t fared much better. One posted by National Geographic has over 100,000 ‘dislikes’ and less than 8000 ‘likes’, as of this writing.
A Disney Plus trailer, on the other hand, has just over 1000 ‘likes’ and over 20,000 ‘dislikes’.
Rotten Tomatoes has been accused of bias in the past, and the company has often chalked up near-universal negative reactions from audiences to trolls’ review-bombing.
In 2019, the company disabled pre-release comments and removed their ‘Want to See’ function – which allowed ratings based on how excited users were for a film – in response to early backlash against franchise pictures accused by critics of going ‘woke’, such as ‘Star Wars: The Last Jedi’ and ‘Captain Marvel’.
Two years before that decision, debate around Rotten Tomatoes and the political influence the audience can have was still a heated debate. Outspoken liberal and comedian Amy Schumer claimed in 2017 that her comedy special ‘The Leather Special’ was review-bombed by the “alt-right” over her comments on Donald Trump and other Republicans (50% critic rating/4% audience). At the time, the site responded again by limiting user functions by removing a five-star system in favor of a positive or negative rating from audiences.
On the opposite end of the spectrum, conservative artists have often pointed to the fact that films aimed at right-leaning audiences often score much lower with critics than audiences as proof the company is more open to ‘certifying’ liberal critics than right-of-center or conservative ones.
Producer John Aglialoro blamed near-universal bad reviews from “hateful” critics on Rotten Tomatoes for his 2011 film ‘Atlas Shrugged: Part I’ struggling to find an audience in theaters (he would go on to produce two sequels covering the last two thirds of Ayn Rand’s influential novel).
Featured Video

Fear Is the Mind Killer
or go to
Aletho News Archives – Video-Images
From the Archives
Alarmist climate science as a textbook example of groupthink
By Paul MacRae | May 1, 2012
A while ago, I received an email from a friend who asked:
How can many, many respected, competitive, independent science folks be so wrong about [global warming] (if your [skeptical] premise is correct). I don’t think it could be a conspiracy, or incompetence. … Has there ever been another case when so many ‘leading’ scientific minds got it so wrong?
The answer to the second part of my friend’s question—“Has there ever been another case where so many ‘leading’ scientific minds got it so wrong?”—is easy. Yes, there are many such cases, both within and outside climate science. In fact, the graveyard of science is littered with the bones of theories that were once thought “certain” (e.g., that the continents can’t “drift,” that Newton’s laws were immutable, and hundreds if not thousands of others).
Science progresses by the overturning of theories once thought “certain.” … continue
Blog Roll
 Aletho News
Aletho News- Military aid to Ukraine vital for ‘US hegemony’ – Republican senator
- Zelensky’s favorite drone company at center of Ukrainian corruption alert
- The Broken Contract
- US CENTCOM’s Request for Dark Eagle Missiles Shows Shortage of Weapons and Limited Options
- Iran consolidates Strait of Hormuz control in post-war power shift, leaving US in dark
- A pause, not a ceasefire: Washington stalls, Tehran recalibrates
- US blockade crumbles as Iran turns to overland routes
- Hidden costs of US Iran war push total far beyond $25bn Pentagon claim
- Iran Will Respond With Long-Term Strikes to US Attack, Even If It Is Short-Term – IRGC
- Fear Is the Mind Killer
- If Americans Knew
- Former Tik Tok official describes massive pressure from Israel lobby
- Amid ceasefire violations and genocide, Israel commits piracy – Daily Update
- Five Laws and Standards That Require the US Cut Off Weapons to Israel
- Israel’s diabolical killing machine and how it targets journalists.
- The Global Sumud Flotilla to Gaza — A cry at sea to the world’s dormant conscience
- Politico’s powerful parent company tells Politico they must support Israeli narrative
- How Tony Dokoupil Became the Face of ‘Zionist Fanatic’ Bari Weiss’s CBS
- Far Right Israeli Settler Movement Enters Syria in a Push for “Greater Israel”
- ‘People Have the Right to Be Buried’: In Gaza, Thousands of Palestinians Remain Trapped Under Rubble
- Born during Israel’s genocide: Gaza’s child survivors bear the scars of war
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
