Good news from Japan: Ivermectin works
By Joel S Hirschhorn | December 30, 2021
This is from a recent news story:
“The Pandemic in Japan was going out of control, yet the Japanese government was smart enough to look beyond vaccines in its COVID-19 containment efforts.
In September, Japan deployed Ivermectin and legalising the use of the anti-parasitic drug has helped people recover from COVID-19 with more durable and long-lasting immunity. Caseloads have come down rapidly without the need for booster vaccination doses. In Tokyo, there were around 6,000 cases in the middle of August, but the number has now dropped down to below one hundred.
Japan is now overcoming the Coronavirus, with the number of COVID tests dropping from 25% in the fag end of August to just 1% mid-October.
Ivermectin use is thus helping Japan permanently beat the COVID-19 Pandemic. If and when vaccine efficacy wanes, Japan will have a choice- using an anti-parasitic medicine as a permanent cure to ensure speedy recovery of infected patients with durable immunity. Japan has thus crushed Big Pharma with a small move- deploying the use of Ivermectin.”
This is from another news story:
“Ivermectin was allowed as a treatment on August 13 and after 2 weeks the cases started to come down. In fact, they are now down 99 percent from the peak.
In Japan, doctors can now prescribe it without restrictions, and people can buy it legally from India. Japan is a country where 72.5 percent of the inhabitants are fully vaccinated.”
And here is an article on how the media lied about Japan not using ivermectin successfully. Many of us got fooled by big media lies.
Check out the following two graphs that tell the true story. The first shows how Japan has recently done very well by using ivermectin.

The following graph shows how the US compares to three countries that have used ivermectin successfully. It plots COVID deaths per million people versus date.

Omicron in the Spotlight
Fewer severe cases, vaccine failure, rapid spread, murky origins.

Swiss Policy Research | December 31, 2021
Covid severity
Data from South Africa indicated that the impact of the omicron wave was much lower than previous covid. However, South Africa had already a total infection rate of about 80%, indcluding about 200,000 covid deaths in 60 million people, i.e. a population fatality rate of about 0.3%.
Thus, it was not immediately clear if the lower impact in South Africa was due to prior immunity or lower intrinsic virulence of the omicron variant. Early data from Europe remained ambiguous, too, as omicron primarily affected young people and travelers.
But recent data from Denmark, Norway, Britain and Canada, although still preliminary, appear to show that omicron really causes fewer severe cases of covid, regardless of vaccination and immunity status.
For instance, a preprint study from Ontario with about 15,000 people found that the risk of hospitalization or death was about 50% lower among omicron cases compared to delta cases (see chart above; the 95% confidence interval ranges from 25% to 75%).
The latest official data from Denmark also shows a ~50% lower hospitalization rate with omicron compared to delta (1.1% vs. 0.6%). An analysis by Imperial College London estimates that the hospitalization rate of omicron is about 25% to 50% lower compared to delta.
The somewhat lower virulence of omicron will be especially important for people at high risk of severe covid, whereas the general population may not notice much of a difference. Indeed, case studies of (vaccinated) omicron outpatients describe symptoms very similar to previous coronavirus variants, including chest pain or shortness of breath in 20% to 40% of cases (see “7 boosted Germans go to South Africa” (table 2) and “33 boosted nurses have a party in the Faroe islands” (table 1)).
Omicron in South Africa:

Omicron in South Africa (FT)
Why is omicron milder?
Preliminary cell culture studies and animal studies show that, while omicron achieves very high viral loads in the upper airways – explaining its rapid spread and short incubation period –, it appears to achieve lower viral loads in the lungs. In addition, omicron appears to induce much less cell fusion, thus causing less tissue damage.
Omicron: Lower viral load in the lungs and lower cell fusion:

Omicron: Lower viral loads in the lung

Omicron: Less cell fusion

Omicron: Less lung tissue damage in hamsters
Vaccine protection
Several studies have shown that existing covid vaccines, which are still based on the original Wuhan coronavirus strain, achieve almost no neutralization against omicron. Protection against infection, even after a booster, appears to be 30% to 50% at most and is waning within weeks.
In many countries, infection rates among vaccinated people are currently higher than among unvaccinated people, perhaps because there are already more recovered people among the unvaccinated people, or because recently vaccinated/boosted people have a higher infection risk (post-vaccination spike in infection risk).
At any rate, vaccination no longer provides any meaningful protection against infection with omicron, and “vaccine passports” have become entirely useless or counterproductive.
There are some indications that vaccination still provides some protection against severe disease; it has been argued that this might be due to a broader T cell response or immune memory. Previous infection also provides good protection (50%-60%) against severe disease, but it can no longer prevent reinfection (i.e. many previously infected people will get re-infected).
On the positive side, there are first antibody neutralization results showing that an infection with omicron provides protection against the delta variant, too.
Vaccines: Zero protection after 45-90 days, negative after >90 days.

Vaccines: Zero protection after 45-90 days, negative after >90 days. (Denmark)
Rapid spread
Omicron has already taken over from delta in parts of Europe and the US, or is currently in the process of doing so. In many countries, and also at the global level, coronavirus infections have reached a new all-time record.
Despite a hospitalization rate that is 25% to 50% lower (see above), omicron has already significantly increased hospital and ICU admissions and even deaths in places like Denmark, England and New York City (see next charts). It is true that some of these hospitalization are not “due to covid”, but in-hospital transmission is not a positive thing, either.
Therefore, early treatment of high-risk patients should remain a top priority.
At the global level, a clock-like 120-day coronavirus infection cycle has been observed in the last two years; the current global cycle should peak around January 3, but it is also possible that omicron will break this cycle and continue its expansion.
Denmark (cases, hospital admissions, ICU patients, deaths):

Omicron in Denmark (OWD)
England (hospital admissions):

Omicron in England (Covid Actuary)
New York City (hospital and ICU patients):
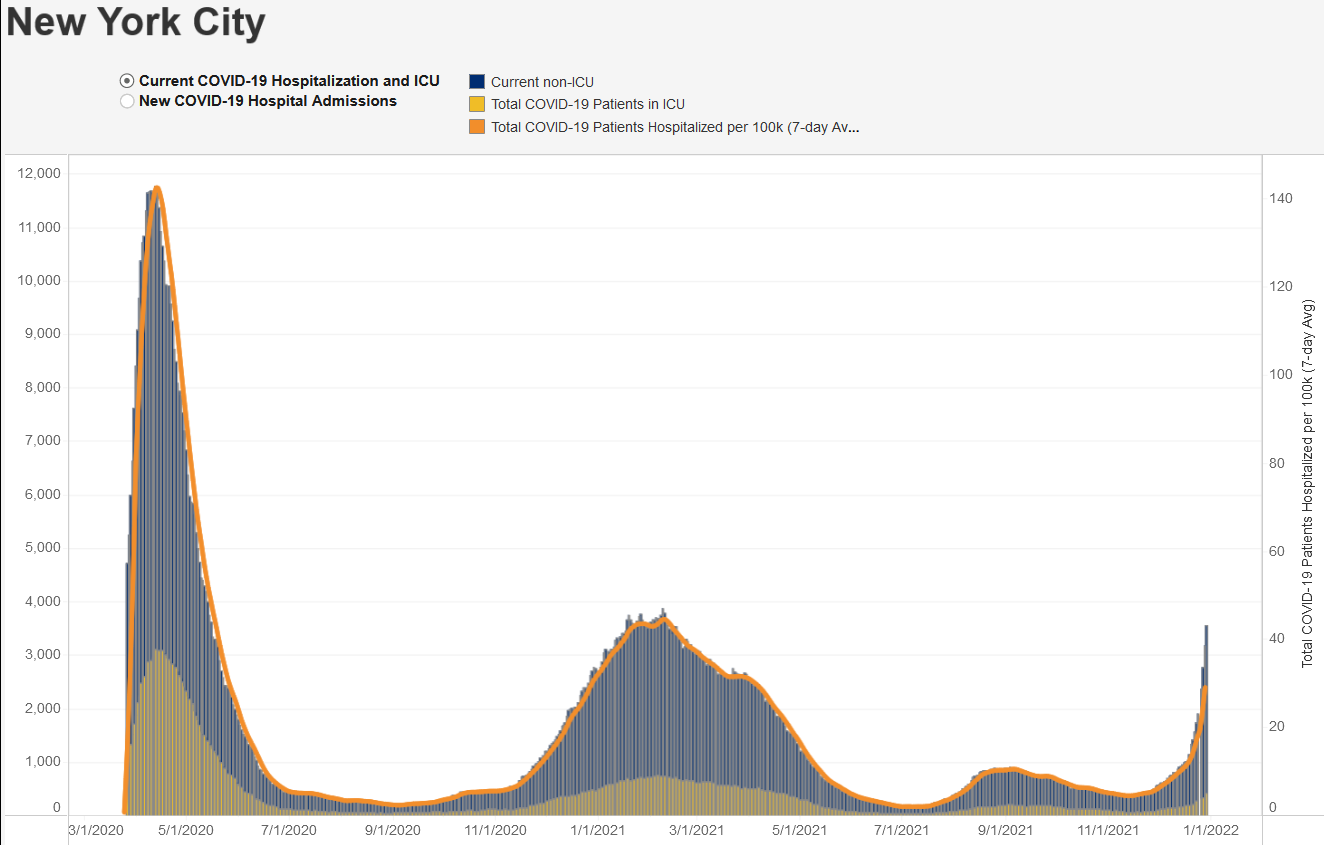
New York City (hospital and ICU patients) (New York)
Australia (infections):

Omicron in Australia (Ian MSC)
Murky origins
The origins of the omicron variant, probably in South Africa, remain very murky. First, the last known ancestor of omicron dates back to March-June 2020 (!). Second, the extreme imbalance between synonymous and non-synonymous mutations (non-changing vs. changing amino acids) indicates an unnatural origin (i.e. not via evolution, not even in mice).
This currently points to either some lab experiment (e.g. during vaccine development or immune escape research, which was performed in some South African labs), or possibly to a mutation induced during the molnupiravir drug trial in South Africa (i.e. the Merck pill that induces a very high rate of mutations).
Meanwhile, Taiwan confirmed that in late November, a scientist in a BSL-3 lab got infected by the delta variant of the coronavirus during lab work.
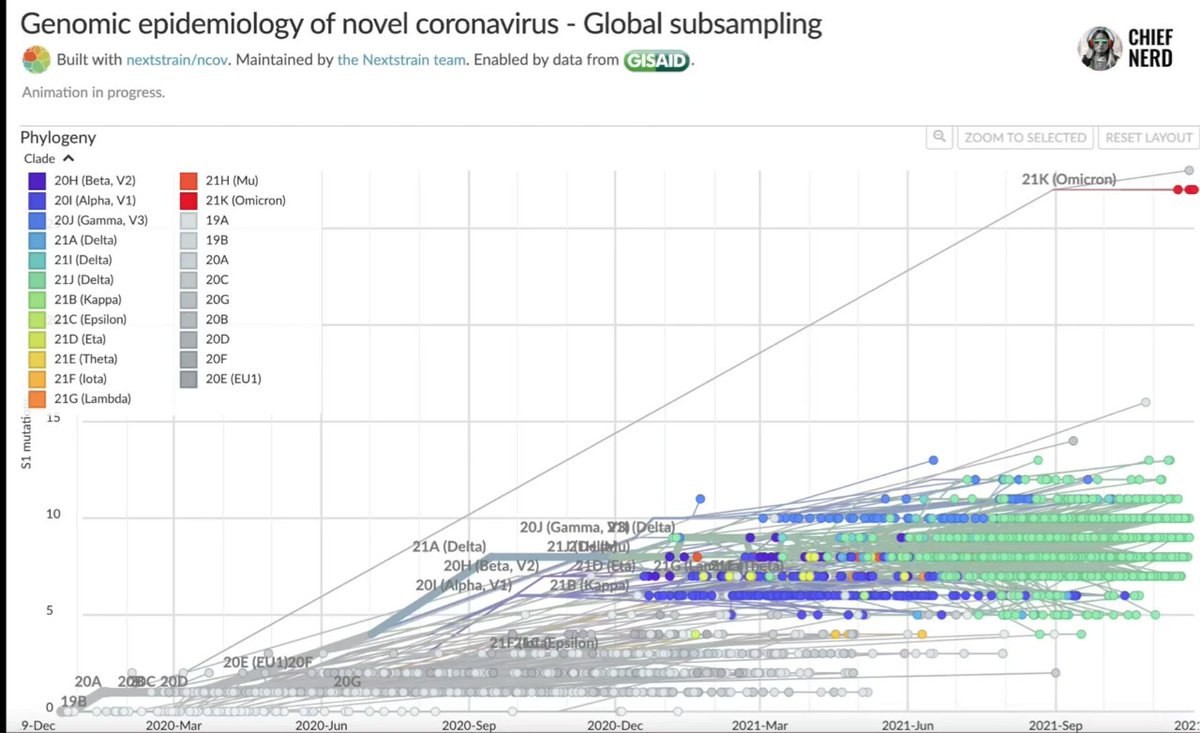
Omicron origin (Twitter/Nextstrain)
See also
No, 500 Children were NOT admitted to hospital with Covid this week
OffGuardian | December 30, 2021
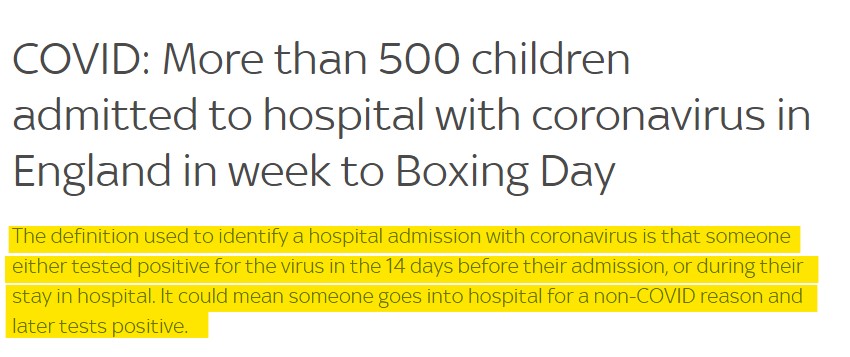
Two days ago Sky News reported that, in the week from December 20th to Boxing Day (December 26th, for our non-UK readers), over 500 British children had been admitted to hospital with Covid19.
The story has been picked up by other outlets too, with the Metro headlining:
More than 500 children admitted to hospital with Covid in Christmas week
The Mirror went with:
More than 500 children admitted to hospital with Covid in week leading up to Boxing Day
Going on to say [our emphasis]:
A record number of new Covid infections were reported today with the easily transmissible Omicron strain being named as the driving force for the surge – now the variant is having an unprecedented impact on Britain’s younger population
Other publications cited “concerning data” that 50 babies had been admitted to hospital with Covid on Christmas day alone.
But is any of this true?
In short, no. It is a meaningless number created by deliberately misleading statistical definitions.
This is actually the easiest fact-check we’ve ever done, because Sky literally fact-checked themselves in their own subheading:
Let’s repeat that with some added emphasis:
The definition used to identify a hospital admission with coronavirus is that someone either tested positive for the virus in the 14 days before their admission, or during their stay in hospital. It could mean someone goes into hospital for a non-COVID reason and later tests positive.
So no, 512 children were not admitted to hospital for Covid infection, 512 children were admitted to hospital for potentially “non-COVID reasons”, and either tested positive while they were in hospital or had tested positive sometime in the previous two weeks.
We’ve gone over this many times before.
The official definition of a “Covid death” is death by any cause, in someone who tested positive in the month preceding their death.
The official definition of a “covid hospitalisation” is anyone who is admitted to hospital for any reason after testing positive, or tests positive while they are already in hospital for something else.
We don’t need to explain, yet again, how meaningless the resultant statistics will be if you use these definitions.
But if they keep lying about the figures, we will keep correcting them.
Victoria government lied about who had access to Covid contact tracing data

By Didi Rankovic | Reclaim The Net | December 28, 2021
The government of the Australian state of Victoria not only decided to deliberately keep citizens in the dark about court rulings exposing the fact the privacy of their data collected by contact tracing apps can be compromised – but is now doubling down.
And the way the state’s Acting Premier Jacinta Allan, who has currently taken over while Premier Dan Andrews is being investigated for “concealing treason and fraud,” chose to defend the failure to inform people about matters pertaining to sensitive private information about them was to say the government was – shielding them from misinformation.
Australian media say the attempts to hide the truth have been made repeatedly, and Allan’s logic in defending the move is that if revealed, the Supreme Court’s secret ruling that said the data was not “absolutely protected” would have given rise to a “baseless scare campaign” as media reporting the facts would have caused “fear and misinformation.”
She did not clarify what type of “misinformation and fear” was expected to arise from the truth.
“The decision was taken in the balance of providing confidence in the Victorian community that this wasn’t a matter that needed to have that level of misinformation spread about it,” Allan said on Tuesday of the way the multiple levels of deceit had been handled.
This Supreme Court finding came to light after the Herald Sun reported that despite explicit promises of information safety, and its use only for health purposes, this was a lie – and one ongoing for two years.
Instead of making contact tracing data available only in order to fight the epidemic, it was also available to law enforcement, and authorities like the WorkCover agency.
It was precisely that agency’s demands to be given access to tracing app data that launched the legal case, when the Department of Health asked the court to order WorkCover to stop.
Another revelation is that the state’s Covid commander Jeroen Weimar petitioned the court to keep the case secret for five years. He tried to persuade the court that maintaining Victorians’ trust in the tracing system was what really matters – at the same time downplaying the importance of the citizens’ right to know their data can be shared, despite assurances from Covid tracers that this was not possible.
Asked if it was right to hide from the public the truth about the safety of their data – and the fact a court case was unfolding financed by their tax money, Allan said, “They don’t deserve a fear campaign, they don’t deserve misinformation,” and added that their data “will be protected.”
Shadow Attorney-General Matt Bach sees the scandal differently:
“People should be shocked and appalled. We should never become accustomed to this level of dishonesty.”
Biggest pandemic lie: PCR tests accurately detect cases and deaths
By Joel S Hirschhorn | December 28, 2021
As of this Friday, December 31 the ubiquitous and infamous PCR test used universally by the public health and medical establishments is gone, according to a CDC declaration issued last July.
To all of the propaganda victims of the pandemic collusion mafia, now is the time (belatedly) to face facts. A huge fraction of all the fear-producing data in COVID cases, hospitalizations and deaths are sheer crap. From the very beginning in early 2020 there were experts who said that the PCR test should not have been so used universally as a way to detect and document COVID infection and disease.
You may have noticed that there has been no coverage of this rather important act by CDC in the leftist mainstream media. Why not? Because now they have to admit that massive false positive results from PCR tests have produced totally unreliable data. These PCR tests had the capability of calling the common flu or cold COVID. And so much of the time they were run at very high cycles to create false positives.
FDA has other approved tests for COVID that will be used.
The larger point after two pandemic years is that the public should better appreciate just how easy it has been for public health, medical and public policy establishments to totally lie about virtually all aspects of the pandemic.
It started with PCR testing and continues to this day with COVID vaccines. If you were stupid enough to trust testing, then you probably remain stupid enough to trust everything said about vaccines and boosters as ways to curb the pandemic. And add on masking, lockdowns and school closings to the BIG LIES endlessly promoted by Big Media, Big Government and Big Pharma.
And now keep believing, if you remain gullible, that omicron is a huge health threat.
Starting with my book Pandemic Blunder I have worked endlessly to be a truth-teller. But it is not easy to combat the disinformation and lies from all the powerful forces determined to instill fear so that governments can coerce and control the public.
Though I prefer to focus on COVID deaths, there are reasons why these data are also problematic. So many have died with COVID but not from COVID.
Hospitals have utterly failed to effectively prevent COVID related deaths, now over 830,000 and that will surely reach 1 million by the end of March. Why? Because severely ill, late-stage COVID patients in ICUs are not being saved by current hospital protocols. Those patients got to that point because the government prevented wide use of generic medicines for early home treatment and even now for late-stage COVID.
Everywhere I look I see widespread dishonesty, incompetence and corruption. These have produced widespread suffering in all aspects of lives. Time for the revolution. If you have enough critical thinking capability to see all the many lies from the powerful, especially the evil Fauci.
Kennedy’s Fauci revelations – Part Two
By Sally Beck | TCW Defending Freedom | December 22, 2021
This is the second of two parts. The first appeared yesterday.
THE revelations in Robert F Kennedy Jnr’s book about Anthony Fauci’s handling of the Covid crisis are damning. That is putting it politely.
He illustrates how the United States chief medical adviser, in charge of healthcare for the American people for over 40 years, presided over the worst coronavirus death rate in the world, nearly double that of many countries. The US suffered 2,107 deaths per 100,000 citizens, while Sweden, who accidentally became the world’s control group by ignoring damaging lockdown and mask mandates, had 1,444 deaths per 100,000.
Fauci is blinkered to affordable treatments, and inexplicably banned them. The rest of the world followed suit with the result that thousands who tested positive for SARS-CoV-2 were left to deteriorate at home until gasping for breath, when they were finally admitted to hospital and ventilated. Many never came home.
RFK Jnr, 67, son of assassinated US attorney general Bobby Kennedy and nephew of assassinated President John F Kennedy, began his legal career as an environment lawyer. Time.com named him ‘hero for the planet’. These days he is accused of being an antivaxxer, but like most activists in this arena he is simply pro-vaccine safety.
As he says at the beginning of his book The Real Anthony Fauci: Bill Gates, Big Pharma and the Global War on Democracy and Public Health: ‘Complex scientific and moral problems are not resolved through censorship of dissenting opinions, deleting content from the Internet, or defaming scientists and authors who present information challenging to those in power. Censorship leads instead to greater distrust of both government institutions and large corporations.’
Many formerly respected medics, as well as RFK Jnr, now find they are victims of cancel culture, while those in power are able to dictate undemocratic, unproven and draconian measures with the capability to destroy our lives and economies without censure or challenge.
Here is an edited extract from chapter 1:
‘Peer-reviewed science offered anaemic if any support for masking, quarantines and social distancing, and Dr Fauci offered no citations or justifications to support his diktats. Both common sense and the weight of scientific evidence suggest that all these strategies, and unquestionably shutting down the global economy, caused far more injuries and deaths than they averted.
‘During a speech to HHS [Health and Human Services] regulators, Fauci explained the fruitlessness of masking asymptomatic people. “The one thing historically people need to realise, that even if there is some asymptomatic transmission, in all the history of respiratory borne viruses of any type, asymptomatic transmission has never been the driver of outbreaks. The driver of outbreaks is always a symptomatic person. Even if there’s a rare asymptomatic person that might transmit, an epidemic is not driven by asymptomatic carriers.”
‘Dr Fauci observed in March 2020 that a mask’s only real efficacy may be in “making people feel a little better”. Perhaps he recognised that what masking lacked in efficacy against contagion, it compensated for with powerful psychological effects. These symbolic powers demonstrated strategic benefits for the larger enterprise of encouraging public compliance with draconian medical mandates. Dr Fauci’s switch to endorsing masks after first recommending against them came at a time of increasing political polarisation, and masks quickly became important tribal badges – signals of rectitude for those who embraced Dr Fauci, and the stigmata of blind obedience to undeserving authority among those who balked. Moreover, masking, by amplifying everyone’s fear, helped inoculate the public against critical thinking.
‘By serving as persistent reminders that each of our fellow citizens was a potentially dangerous and germ-infected threat to us, masks increased social isolation and fostered divisions and fractionalisation – thereby impeding organised political resistance.
‘The impact of masking on the national psyche reminded me of the subtle contribution of the “duck and cover drills” of my youth, drills that sustained and cemented the militaristic ideology of the Cold War. Those futile exercises reinforced what my uncle John F Kennedy’s Defense Secretary, Robert McNamara, called “National Mass Psychosis”. By suggesting to Americans that full-scale nuclear war was possible, but also survivable, ruinous investments in that project were justified. For the government and mandarins of the Military Industrial Complex, this absurd narrative yielded trillions in appropriations.
‘Social distancing mandates also rested on a dubious scientific footing. In September 2021, former FDA Commissioner Dr Scott Gottlieb admitted that the six-foot distancing rule that Dr Fauci and his HHS colleagues imposed upon Americans was “arbitrary,” and not, after all, science-backed. The process for making that policy choice, Gottlieb continued, “is a perfect example of the lack of rigour around how CDC made recommendations”.
‘Finally, the lockdowns of the healthy were so unprecedented that the World Health Organisation’s official pandemic protocols recommended against them. Some WHO officials were passionate on the topic, among them Professor David Nabarro, Senior Envoy on Covid-19, a position reporting to the Director General.
‘On October 8, 2020, he said, “We in the World Health Organisation do not advocate lockdowns as a primary means of controlling this virus. We may well have a doubling of world poverty by next year. We’ll have at least a doubling of child malnutrition because children are not getting meals at school and their parents in poor families are not able to afford it. This is a terrible, ghastly, global catastrophe, actually, and so we really do appeal to all world leaders: Stop using lockdown as your primary control method . . . lockdowns just have one consequence that you must never ever belittle – and that is making poor people an awful lot poorer.”
‘Dr Fauci and other officials made no inquiry or claims as to whether lockdowns would cause more harm and death than they averted. Subsequent studies have strongly suggested that lockdowns had no impact in reducing infection rates. There is no convincing difference in Covid infections and deaths between laissez-faire jurisdictions and those that enforced rigid lockdowns and masks. Dr Fauci’s mask deceptions were among several “noble lies” that, his critics complained, revealed a manipulative and deceptive disposition undesirable in an even-handed public health official. Dr Fauci explained to the New York Times that he had upgraded his estimate of the vaccine coverage needed to insure “herd immunity” from 70 per cent in March to 80-90 per cent in September not based on science, but rather in response to polling that indicated rising rates of vaccine acceptance.
‘He supported Covid jabs for previously infected Americans, defying overwhelming scientific evidence that post-Covid inoculations were both unnecessary and dangerous.’
Under questioning on September 9, 2021, Dr Fauci conceded he could cite no scientific justification for this policy.
‘In September 2021, in a statement justifying Covid vaccine mandates to school children, Dr Fauci dreamily recounted his own grade-school measles and mumps vaccines – an unlikely memory, since those vaccines weren’t available until 1963 and 1967, and Dr Fauci [who is 80 years old] attended grade school in the 1940s. Dr Fauci’s little perjuries about masks, measles, mumps, herd immunity, and natural immunity attest to his dismaying willingness to manipulate facts to serve a political agenda.’
New York Democrat introduces new social media censorship bill
The bill aims to curb people’s speech by targeting platforms
By Didi Rankovic | Reclaim The Net | December 27, 2021
If a state senator got his way, the state of New York could soon get a new law aimed at regulating what content can appear on social media. The bill is designed to circumvent existing federal-level solutions in some instances and is reportedly inspired by internal documents leaked by former Facebook employee Frances Haugen.
But many legal experts believe that the bill, if passed, would eventually be overturned as unconstitutional for preventing dissemination of protected content.
The bill sponsored by state Senator Brad Hoylman wants to tackle what’s referred to as unlawful online content such as “misinformation” (particularly around Covid/vaccines), and posts that might allegedly lead users to develop eating disorders or engage in self-harm.
Envisaged in the bill is an amendment to New York’s penal code that lets citizens, the state attorney general and city corporation councils sue tech companies behind social media networks, or individuals, if they are suspected of “contributing” to spread of misinformation in a manner that’s “knowing or reckless.”
And while the bill is worded in a way that states content seen as endangering people’s safety or health should be clamped down on if it is “promoted” – including (but not exclusively) by means of algorithms and other methods of recommendation, experts say the distinction between that and any post created by users is not clear enough to stand up to legal scrutiny.
“The distinction between ‘hosting’ and ‘amplifying’ content is incoherent,” Santa Clara University School of Law professor Eric Goldman has told the New York Post, adding that Hoylman has taken that “incoherent” idea – “and embraced its most censorial option.”
According to Goldman, content that Hoylman’s bill takes aim at, such as, but not limited to, what’s considered false or harmful information that concerns Covid or political issues is in fact protected free speech under the First Amendment.
And for that reason, this expert believes, the draft legislation is unconstitutionally overbroad.
Commenting on the bill, David Greene of the Electronic Frontier Foundation concurred that the law would face First Amendment hurdles, and noted that because of the rapidly changing official guidance regarding the pandemic, it is very hard to even define what qualifies for Covid misinformation (when so much “expert” information has turned out to be false.)
“It’s really very difficult to impose liability in an environment where the truth can be hard to grasp at any point in time,” this attorney remarked.
Featured Video

Iran Walks Out On Peace Deal Due To Trump’s Threats
or go to
Aletho News Archives – Video-Images
From the Archives
Neocons confess: “We did 9/11-anthrax”
By Kevin Barrett | Press TV | September 6, 2014
As the 13th anniversary of the crimes of September, 2001 approaches, the neoconservatives are shrieking from the rooftops – and effectively confessing that they were the real perpetrators of the 9/11-Anthrax false flag operation. (The neocons, you may recall, openly called for a “new Pearl Harbor” in September, 2000 – and got one exactly one year later.)
Every year at this time, the neocons orchestrate and hype a series of public relations stunts designed to magnify fears of “radical Islam” and reinforce their crumbling 9/11-Anthrax cover story. But this year’s propaganda campaign is so extreme that it represents a tacit confession: The neocons know that the truth about the 9/11-Anthrax operation is slowly closing in on them; so they are over-reacting by desperately trying to stoke the dying embers of the so-called War on Terror, in order to maintain the myth that Muslims (rather than neoconservative Zionists) attacked America in the autumn of 2001.
When a hysterical person exhibits guilty demeanor by trying too hard to blame a crime on someone else, that person is almost certainly the real perpetrator. As the neocons try much too hard to blame Islam for 9/11 and “terrorism” in general, their hysteria inadvertently reveals their own culpability. Like Shakespeare’s Lady MacBeth, the neoconservative movement has blood on its hands and “doth protest too much.” … continue
Blog Roll
 Aletho News
Aletho News- IRAN WALKS OUT ON PEACE DEAL DUE TO TRUMP’S THREATS – w/ Prof. Seyed Mohammad Marandi
- Moderna’s mRNA Flu Vaccine Gets Unanimous Thumbs-Up Despite Risks, Low Efficacy
- UK Speech Regulator’s Telegram Questions Point Toward Private Chats
- Cuban FM blasts Rubio for ‘chronically lying’ about US fuel blockade
- Al-Jazeera demands punishment for Israeli officials following latest assassination of cameraman
- Iran opens hundreds of legal cases over US, Israeli aggression: Prosecutor general
- Iran delegation protests Trump’s threat at Switzerland talks, weighs ‘proper’ response: Source
- Terms of US capitulation to Iran presage new era for the region
- Strategic Oil Reserve Nears Collapse… US Must Choose: Guns or Butter
- The Story the Media — and the Government — Don’t Want You to Hear
- If Americans Knew
- JNS Policy Summit to kick off in Israel
- Fatalities From Israel’s Vast Gaza Genocide Deliberately Undercounted
- ‘Reproductive genocide’ in Gaza; death toll in Lebanon tops 4,000 (during a ceasefire) – Daily Update
- Israelis Invaded Lebanon And Then Cried Victim When Their Soldiers Got Killed
- FARA Docs: Israel is Spying On Millions Of Christian Americans In Their Churches
- Why US presidents from both parties end up cursing Benjamin Netanyahu
- Israel Asked Facebook to Censor Iran War Content, Internal Documents Show
- Deaths in Gaza undercounted, possibly by 100s of thousands; “Psychopath” Ben-Gvir talks trash – Daily Update
- UNICEF: “Trauma is woven into the very fabric of childhood in Gaza”
- 15 articles a day: The extent of the Israeli army’s media interference
- No Tricks Zone
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
