The transmission of respiratory viruses is poorly understood. However, the models used by SAGE to justify draconian restrictions are far too simplistic – they are based on a handful of assumptions that have not been adjusted in the light of real world evidence, despite numerous forecasting failures. First, they assume that every individual is equally susceptible to every variant. SAGE therefore assumes that each outbreak will lead to uncontrolled, exponential viral spread unless there is a material reduction in human interactions.
Why haven’t lockdowns worked? There are broadly two types of respiratory virus. There are those that spread person to person – like measles – in a continuous chain of transmission, uninterrupted by season and with every susceptible contact falling ill. Then there are those we do not understand so well, like influenza, which are much more complex. Instead of the simplistic close contact model, which assumes Covid spreads like measles, we should perhaps consider an alternative more sophisticated model based on influenza. The influenza virus model is unusual – it is predicated on the majority being exposed to a particular airborne virus but, oddly, only a minority appear to be susceptible to each year’s variant. To complicate matters further, influenza can also spread person to person.
The spread of influenza is difficult to model and the cause of the surges in transmission seen each winter is not fully understood. However, influenza has been measured for centuries, enabling interesting patterns to be discerned. Spread does appear to occur person-to-person but only a trickle of cases occur in the summer months before there is sudden exponential growth leading to a winter surge. This annual surge also happens in autumn in milder climates like Australia and California.
Each winter between 5 per cent and 15 per cent of the population somehow become susceptible to the new circulating influenza ‘variant’ (aka strain) – and to date no one can explain why the percentage is so small. Spending an hour in indoor environments in winter is sufficient to expose everyone inside to an infectious dose of influenza, but the majority remain uninfected – perhaps because they are not susceptible. After the 5-15 per cent cohort of susceptible individuals in a particular year are infected, a temporary quasi-herd immunity is reached. Cases therefore fall, reaching negligible levels until the next winter. Clear Gompertz curves are seen, although only affecting part of the population.
The following winter, those who were previously infected remain immune but a further 5-15 per cent become susceptible, somehow. No-one understands what exactly causes these people to become susceptible in winter when they were not the previous winter nor in the summer. A novel influenza virus can take up to eleven winters before full herd immunity is reached for that particular type of influenza virus.
The poorly understood winter trigger that precipitates an influenza surge actually occurs twice each winter and usually the second half sees a different ‘variant’ surge and predominate. Influenza was present for the first half of winter 2019/20 but disappeared globally for the second half at the exact time that SARS-CoV-2 surged, 3 weeks earlier in Italy than in Sweden and the UK. Although these are quite different viruses, the fact that SARS-CoV-2 surged at the exact time that we would have expected a new influenza variant to rise suggests that the influenza transmission model is a viable candidate to examine further for COVID.
The critical point is that many more people are exposed to influenza every year than are infected, because it is airborne and infuses throughout indoor enclosed spaces. The majority are protected by their immune system and the remainder succumb. Vaccination is generally thought to have had an impact on influenza associated hospitalisations and mortality but the evidence it has significantly reduced transmission and infection is weak.
Comparing the transmission of SARS-CoV-2 to influenza is not the equivalent of dismissing COVID as being like ‘flu. In a certain subset, COVID causes more hospitalisations than influenza and results in greater demand for intensive care. However, how we respond to it is predicated on understanding how it transmits, so considering the influenza model is important.
Although we do have evidence of significant person-to-person close contact transmission of SARS-CoV-2, there are many areas of ambiguity such that this cannot be the only route of transmission, once again supporting the ‘influenza spread’ hypothesis to explain the spread of COVID.
The person-to-person close contact model cannot explain certain oddities of influenza transmission. For hundreds of years there have been reports of outbreaks of influenza in boats that have been at sea for weeks with no human contact. It is now clear that SARS-CoV-2 can be transmitted as aerosols through the air, like influenza, and it has been isolated from hospital ventilation systems. In addition, there is a growing body of evidence of numerous viruses present in the troposphere (four to 12 miles above us) which fall to ground level under the right environmental conditions. For decades the simultaneous appearance of genetically identical influenza virus around the world could not be explained, but tropospheric spread may explain this phenomenon.
The simplistic person-to-person close contact model cannot explain certain oddities of Covid either. There was an outbreak of a thousand cases diagnosed within two days of each other in a garment factory in Sri Lanka, without a super-spreader, at a time when there was minimal community Covid. An Argentinian fishing vessel had an outbreak after five weeks at sea, despite everyone testing negative before setting sail. There have been several occasions when Australian authorities have struggled to understand the source of Delta variant infections in the community at times of very low prevalence. Canada publish their test and trace data and 40 per cent of COVID cases in Canada, even at low prevalence, never have an identified source of transmission.
SAGE has never explained how key workers, including hospital staff, who have been continually exposed, could remain unaffected by the original and Alpha variants only to succumb to the Delta variant months later. The household transmission rate for SARS-CoV-2 is around one in 10 – is this because of good luck, or because the other nine in 10 people sharing living quarters with an infected person are not susceptible to that particular variant?
The influenza model of transmission is a hypothesis that requires testing, which could start by interviewing those on the Diamond Princess to see how many have been infected with subsequent variants.
Real world evidence has repeatedly shown that the simplistic approach adopted by SAGE – and others – has failed. No explanations have been offered for the lack of correlation between changes in human behaviour and viral prevalence. Early models were always more likely to be inaccurate but as more data has appeared the refusal to adjust the models becomes less forgivable. Numerous scientists have been pointing out the faults in the SAGE models for well over a year. Rather than SAGE listening, debating and adjusting their hypothesis, in a scientific way, dissenting voices have been quashed. The latest failures of the SAGE models must be a reality check. Other hypotheses, including the influenza model, need to be given due consideration and overly simplistic models, which fail to explain the patterns in real world data, must be discarded for good.
Dr Craig (@ClareCraigPath) has been a pathologist since 2001 – she worked in the NHS and reached consultant level in 2009. She specialised in cancer diagnostics including diagnostic testing for cancer within mass screening programmes, and was the day-to-day pathology lead for the cancer arm of the 100,000 Genomes Project. Subsequently she has worked on artificial intelligence for cancer diagnostics.
October 8, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | Covid-19, UK |
Leave a comment
A study published Sept. 30, in the peer-reviewed European Journal of Epidemiology Vaccines found “no discernible relationship” between the percentage of population fully vaccinated and new COVID cases.
In fact, the study found the most fully vaccinated nations had the highest number of new COVID cases, based on the researchers’ analysis of emerging data during a seven-day period in September.
The authors said the sole reliance on vaccination as a primary strategy to mitigate COVID-19 and its adverse consequences “needs to be re-examined,” especially considering the Delta (B.1.617.2) variant and the likelihood of future variants.
They wrote:
“Other pharmacological and non-pharmacological interventions may need to be put in place alongside increasing vaccination rates. Such course correction, especially with regards to the policy narrative, becomes paramount with emerging scientific evidence on real-world effectiveness of the vaccines.”
As part of the study, researchers investigated the relationship between the percentage of population fully vaccinated and new COVID cases across 68 countries and 2,947 U.S. counties that had second dose vaccine, and available COVID case data.
For seven days preceding Sept. 3, researchers computed COVID cases per one million people for each country, as well as the percentage of population that was fully vaccinated.

Relationship between cases per 1 million people (last 7 days) and percentage of population fully vaccinated across 68 countries as of September 3, 2021
Notably, Israel with more than 60% of its population fully vaccinated, had the highest COVID cases per 1 million people during the seven-day period.
Iceland and Portugal, with more than 75% of their populations fully vaccinated, had more COVID cases per 1 million people than countries such as Vietnam and South Africa, where only about 10% of the population is fully vaccinated.
Across U.S. counties, the median new COVID cases per 100,000 people during the seven-day period was similar across the categories of percentage of population fully vaccinated.

Percentage of counties that had an increase of cases between two consecutive 7-day time periods by percentage of population fully vaccinated across 2947 counties as of Sept. 2, 2021
The researchers found a substantial county variation in new COVID cases within categories of percentage of population fully vaccinated. There also appeared to be no significant signaling of COVID cases decreasing in counties where a higher percentages of the population was fully vaccinated.
Of the top five counties with the highest percentage of population fully vaccinated (99.9% – 84.3%), the Centers for Disease Control and Prevention (CDC) identified four as “high” transmission counties.
Three of the four counties classified as “high” transmission had fully vaccinated rates of 90% or higher. Conversely, of the 57 counties classified as “low” transmission by the CDC, 15 had fully vaccinated rates of 20% or lower.
The findings also showed no discernible association between COVID cases and fully vaccinated rates when a one-month lag was considered, to account for the 14-day period it takes for a vaccine to be considered effective.
The authors suggested a correction to the policy narrative is warranted, as increasing vaccination rates is not enough. “Such course correction, especially with regards to the policy narrative, becomes paramount with emerging scientific evidence on real-world effectiveness of the vaccines,” they wrote.
The authors cited data from the Ministry of Health in Israel showing the effectiveness of two doses of Pfizer’s COVID vaccine against preventing SARS-CoV-2 infection was reported to be 39% — substantially lower than the reported trial efficacy of 96%.
Emerging research also shows immunity derived from Pfizer’s COVID vaccine may not be as strong as natural immunity acquired through infection.
A substantial decline in immunity from mRNA vaccines six months post immunization has also been reported along with an increasing number of breakthrough cases among the fully vaccinated, the researchers said.
The authors said stigmatizing populations over vaccines can do more harm than good, and non-pharmacological prevention efforts need to be renewed in order to learn to live with COVID “in the same manner we continue to live 100 years later with various seasonal alterations of the 1918 Influenza virus.”
Breakthrough cases significantly underreported as FDA reviews booster data
The number of vaccinated people testing positive for COVID is on the rise, and doctors in Ohio are reporting more breakthrough cases across hospital systems.
However, only certain types of COVID breakthrough cases are reported at both the state and federal level, leaving patients with mild cases underreported.
“We estimate anywhere from two to 10 times as many positives that are being reported is the real situation,” said Dr. David Margolius, division director of internal medicine at MetroHealth in Cleveland.
“It’s still rare, but I get a dozen COVID positive cases a day in my basket, and usually three or four of them have been vaccinated,” said Margolius.
The Ohio Department of Health and the CDC only report breakthrough cases in patients requiring hospital admission, or cases that resulted in death.
The CDC said it made the change in May in order to “maximize the quality of data collected on cases of greatest clinical and public importance.”
As of Sept. 27, the CDC had received reports from 50 U.S. states and territories of 22,115 patients with COVID vaccine breakthrough infection who were hospitalized or died.
The CDC said the number of COVID vaccine breakthrough infections reported to the agency are an undercount of all SARS-CoV-2 infections among fully vaccinated persons, especially of asymptomatic or mild infections.
In addition, national surveillance relies on passive and voluntary reporting, and data are not complete or representative, according to the CDC.
Massachusetts health officials on Tuesday reported nearly 4,000 new breakthrough cases over the past week, and 46 more deaths, according to NBC Boston.
In the last week, 3,741 new breakthrough cases were reported, with 125 more vaccinated people hospitalized.
This brings the total number of breakthrough cases in Massachusetts to 40,464 — out of 4.63 million vaccinated people — and the death toll among people with breakthrough infections to 300.
According to the Vermont Daily Chronicle, which cited statistics from Vermont’s Department of Health, 76% of the state’s COVID fatalities in September were breakthrough cases, with just eight of the 33 Vermonters who died being unvaccinated.
As of Tuesday, 88% of all eligible Vermonters age 12 and over had been vaccinated with at least one shot.
Health Department spokesperson Ben Truman said most of the vaccine “breakthrough” fatalities were elderly. Because they were among the first vaccinated, Vermont’s elderly “have had more time to potentially become a vaccine breakthrough case,” he said.
According to The Washington Post, Dr. Peter Marks, director of the U.S. Food and Drug Administration’s (FDA) Center for Biologics Evaluation and Research, said Tuesday updated data might make a strong case in support of everyone 18 and older being eligible for COVID vaccine boosters, but the agency will have to see whether its outside advisers agree.
The remarks from Marks came during a webinar as the FDA prepares to meet Oct. 14 and 15 with its outside advisers to discuss authorizing Moderna and Johnson & Johnson COVID booster shots.
Megan Redshaw is a freelance reporter for The Defender. She has a background in political science, a law degree and extensive training in natural health.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
October 8, 2021
Posted by aletho |
Science and Pseudo-Science | Covid-19, COVID-19 Vaccine, European Union, United States |
Leave a comment
GAINESVILLE, Florida – Florida Gov. Ron DeSantis announced on Friday that the city of Gainesville has withdrawn a COVID-19 vaccine mandate for workers after pressure from his administration and a court ruling against the policy last month.
“We are not going to allow our first responders and government employees, many of whom have been on the front lines for over a year and a half, to be cast aside by local politicians’ mandates,” DeSantis said in a press release. “This reversal by the City of Gainesville is a victory for liberty.”
According to the press release, the Florida Department of Health (FDOH) received a letter from Gainesville last week informing the department that city commissioners “voided” a recent vaccination mandate for all public employees.
The FDOH had written to Gainesville mayor Lauren Poe days earlier, threatening to enforce a law signed by DeSantis in May that bans government entities, schools, and businesses from demanding COVID vaccination status. The law, S.B. 2006, allows up to $5,000 in fines per violation.
Gainesville told the health department in response that there are now “zero employees who are subject to a City COVID-19 employer vaccination requirement.”
“Please be advised that on September 23, 2021, the City Commission of the City of Gainesville took action to rescind their August 5th action related to COVID-19,” city manager Lee Feldman wrote, adding that the vaccine rules “have been voided.”
The day before the FDOH notice, a Florida judge temporarily halted Gainesville’s vaccine mandate following a lawsuit brought by city workers and backed by the DeSantis administration.
“The city failed to put on any evidence that the Vaccine Mandate serves a compelling state interest or that the Vaccine Mandate was the least restrictive means to accomplish that interest,” Circuit Judge Monica Brasington ruled September 22. Gainesville, in fact, “did not put on any evidence, at all, at the injunction hearing,” she noted.
The City Commission of Gainesville voted to rescind the rule the next day.
More than 200 city workers, including police officers, firefighters, and other first responders, sued to block the mandate, with the backing of Florida Attorney General Ashley Moody, a Republican who filed a brief in support of the workers in September.
Last month, Gov. DeSantis announced that Florida would move to penalize violations of the state’s ban on COVID-19 vaccine requirements, such as those in Gainesville, with “millions of dollars” in fines.
“If a government agency in the state of Florida forces a vaccine as a condition to employment, that violates Florida law, and you will face a $5,000 fine for every single violation,” the governor declared at a press conference near Gainesville. “If you look at places here in Alachua County, like the city of Gainesville, I mean, that’s millions and millions of dollars potentially in fines.”
“We will certainly move to impose the fines as the law requires when we see people that are denied access,” he said.
The DeSantis administration continues to fight local vaccine mandates in multiple counties, including Leon County, where city officials confirmed this weekend that they fired 14 employees who refused to disclose their vaccination status by Friday, in violation of S.B. 2006.
The FDOH had warned the county last week that it must “immediately rescind” the coercive vaccine policy and “refrain from terminating any employees who decline to produce proof of vaccination.”
“Fines may be assessed based on each employee who was required to submit proof of vaccination as a condition of continued employment,” wrote Doug Woodlief, FDOH division director for Emergency Preparedness and Community Support. Those fines could cost Leon County over $3.5 million, according to the Tallahassee Democrat.
Orange County also faces potential fines due to an ongoing COVID vaccine mandate, which prompted a lawsuit from dozens of firefighters last week, local news reported. The county downgraded the mandate days after Gov. DeSantis’ press conference last month, but has harassed unvaccinated employees and impeded them from being promoted, firefighters have said.
The Gainesville workers’ victory against compulsory COVID vaccination follows similar recent successes in other states. In Arizona, the city of Tucson backed down on a vaccine mandate last month after Republican Attorney General Mark Brnovich threatened to withhold up to $175 million in funding from the city, citing state laws enacted by Republicans earlier this year.
October 7, 2021
Posted by aletho |
Civil Liberties, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine, United States |
Leave a comment
Three US medical certifying boards have warned doctors that they risk losing their certification and licence if they spread covid vaccine misinformation.
Internists, family doctors, and paediatricians received an email on 9 September that quoted a warning from the Federation of State Medical Boards in July1 which read: “Providing misinformation about the covid-19 vaccine contradicts physicians’ ethical and professional responsibilities, and therefore may subject a physician to disciplinary actions, including suspension or revocation of their medical licence.”2
Richard Baron, president and chief executive of the American Board of Internal Medicine (ABIM), told The BMJ that the move was an attempt to establish a standard of care. “As standard setting organisations, we thought it was important to be on record, in a public way, to make clear that putting out flagrant misinformation is unethical and dangerous during a pandemic.” Baron said that the statement has been well received—“4 to 1 positive.” But community physicians contacted by The BMJ thought differently.
“When I got that email I thought I’d better not put anything on social media about vaccines,” said Shveta Raju, a community physician in the Atlanta, Georgia, area, who has treated covid patients and led the vaccination effort at her outpatient clinic.
“The email was sent more as a veiled threat to keep doctors on the official, established narrative, and that’s what I find chilling,” said a paediatrician who pseudonymously blogs under the name Elizabeth Bennett. “Pandemic or no, there is a problem with having an ill defined concept of misinformation that’s tied to public health messaging that hasn’t been consistent. How are physicians supposed to figure out what is misinformation when public health messaging swings so wildly?” Bennett asked.
Undefined offence
Baron said that the statement was also intended to signal the certifying boards’ support for physicians “trying to do the right thing.”
“We wanted to support that group and say ‘hey, we do have a standard of care here and you are doing the right thing when you uphold it,’” he said.
Raju responded, “If that was their intent, they should have defined misinformation. By leaving it undefined, the message was that we can’t talk about this at all.” She said that physicians are, by and large, a conservative group. “If they’re not sure what can be deemed misinformation, physicians would rather be quiet.”
Bennett concurred: “The thing I find most alarming is that they don’t define misinformation, but if they strip you of your board certification, you would lose your means of earning a living.”
Doctors spreading misinformation?
Official and social media company efforts to target “vaccine misinformation” predate the pandemic.3 But the new statement from ABIM, the American Board of Family Medicine, and the American Board of Paediatrics is one of several recent statements putting doctors in the spotlight for the first time.
In Canada, warnings about physician information began earlier, when in April the College of Physicians and Surgeons of Ontario declared that physicians “have a professional responsibility not to communicate anti-vaccine, anti-masking, anti-distancing, and anti-lockdown statements or promote unsupported, unproven treatments for covid-19.”4
The Canadian statement triggered an outcry, leading to a clarification that the statement was “not intended to stifle a healthy public debate about how best to address aspects of the pandemic.” But concerns continued. In June, a Canadian member of parliament held a press conference on censorship of Canadian clinicians and scientists. YouTube removed the video of the meeting.56
The BMJ asked ABIM about the size of the problem of board certified physicians spreading misinformation.
“We don’t have a sense of numbers of physicians spreading misinformation,” Baron said. “We’re at the beginning.” He believed it was only a “small number of doctors.” The medical boards opted to send the statement to all doctors, he said, because focusing on just the offending individuals would “miss the impact they’re having because of how much their voices are being amplified.”
As an example of “unprofessional or unethical behaviour,” Baron cited the case of a Florida doctor offering medical exemptions from mask wearing for $50 (£37; €43).7
Personalised medicine—or one-size-fits-all?
The BMJ asked whether physicians expressing doubt about the need for booster doses or vaccination of patients with natural immunity—two matters that have been the subject of debate and changing official guidance—would qualify as misinformation.8 “I don’t think we have concerns with doctors wrestling with areas where the science is unclear,” Baron said, “but there is no debate about whether people should get a primary vaccination series.”
Raju worries about the impact on personalised care. “The job of physicians is to take guidelines and apply them to the patient in front of them.” But now “physicians are basically being told that when it comes to covid vaccines it’s one-size-fits-all.”
Baron said, “We’re not trying to stifle conversations between doctors and patients. We understand that different people may look at evidence in different ways, but when you have an overwhelming preponderance of medical consensus in a certain area, you need at least to tell patients that there is an overwhelming professional consensus here.”
Cautious approach
Jeffrey Flier, former dean of Harvard Medical School, said that in the context of the pandemic, he was “not opposed to certain levels of misinformation triggering a decision to question somebody’s licence.” He said, “I can see this being an appropriate remedy at a time of public health emergency.
“But this is not how the system for licensure and certification has traditionally worked, and creates many opportunities for mistaken judgment about what is and is not misinformation, and those decisions would have to be rendered with extreme caution.”
Flier added, “We have to remember that there are legitimate areas of debate, and such matters should not fall within the scope of disciplinary actions.”
“There are reasons to be concerned that state boards might be unprepared for these kinds of decisions at a time when so many aspects of covid policy have been enmeshed with political views.”
Footnotes
-
This article was updated on 4 October to make clear that it was medical certifying boards, rather than licensing boards, that emailed physicians. The email quoted an earlier warning from the Federation of State Medical Boards.
-
Competing interests: PD gave a public statement at a 17 September 2021 FDA advisory committee to discuss covid-19 vaccines, where he highlighted the joint statement. The views and opinions expressed here are those of the author and do not necessarily reflect official policy or position of the University of Maryland.
-
Provenance: commissioned; not externally peer reviewed.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usage
View Abstract
October 7, 2021
Posted by aletho |
Deception, Full Spectrum Dominance, Science and Pseudo-Science, War Crimes | Canada, Covid-19, COVID-19 Vaccine, Human rights, United States |
Leave a comment
Imagine you’re a doctor. You go into work every day for long hours and figure out how to treat Covid. You are saving lives and doing so patient by patient. Each patient has individual needs that sometimes require custom care, but you know early treatment works.
Suddenly, faraway bureaucrats demand that you abandon your best practices and fall into line around their grand plan. Suddenly your patients can’t get what you prescribe. Media apparatchiks diminish, invalidate or mock everything you’ve learned and are doing.
And all of it is being carried out in the name of “science.”
The Physicians’ Rebellion
More than 10,000 physicians and medical scientists have signed onto a Declaration that accuses public health authorities of, well, doing it wrong–and to devastating effect.
“WHEREAS, public policy makers have chosen to force a “one size fits all” treatment strategy, resulting in needless illness and death, rather than upholding fundamental concepts of the individualized, personalized approach to patient care which is proven to be safe and more effective;”
The Declaration goes on to assert that “thousands of physicians are being prevented from providing treatment to their patients, as a result of barriers put up by pharmacies, hospitals, and public health agencies” and that “These policies may actually constitute crimes against humanity.”
Local Knowledge
Such statements might strike non-physicians as hyperbolic. But consider that many of these doctors, such as Dr. Brian Tyson have each saved thousands of lives through early intervention and best practices developed in the field through trial-and-error, observation, and active communication among peers.
“We started seeing inflammation, so we used anti-inflammatories,” Dr. Tyson explains.
“We saw blood clots, so we used anticoagulants. We saw patients having trouble breathing, so we used asthma medications… It wasn’t just one drug. It was the art of what we see and how those patients responded to what we gave them.”
Despite treating more than 6,000 patients, Tyson can count the patients he’s lost to Covid on three fingers. And yet non-practicing officials are interfering with the work of doctors like Tyson.
The physicians and medical scientists who have signed the Declaration are also frustrated with the authoritarian measures supported by career bureaucrats such as Anthony Fauci. Indeed as more information trickles out, more and more observers suspect Fauci approved funding for dangerous research at the Wuhan Institute of Virology and then colluded with the bioethically disturbed Peter Daszak to propagate the unlikely “natural origins” theory.
Barriers to Treatment
Public health authorities have erected huge barriers to early treatment by:
- Putting pressure on major pharmacies not to fill essential prescriptions,
- Putting pressure on insurers not to cover proven therapies, and
- Putting pressure on Big Tech giants to censor and suppress eminent physicians such as cardiologist Peter A. McCullough, who has expressed concerns about vaccinating children.
Declaration signatories include physicians who figured out how to successfully reduce the death toll while public health authorities dithered and delayed their grand plan to roll out mRNA vaccines for everyone — including, apparently, low-risk populations.
All the doctors agree that greater access to early treatment could have saved thousands of lives–and could save thousands more. The Declaration suggests that public health authorities are trying to steamroll over clinical practitioners when these camps should complement each other.
“We are in a pandemic of undertreatment,” said intensive care specialist Pierre Kory, M.D., winner of the British Medical Association’s President’s Choice Award.
“Everything else that we’ve discovered, everything that’s in our protocols is because we have used good clinical sense, lots of experience, and we’ve used trial and error using our best judgments of risks and benefits.”
Clinicians or “Experts?”
Why should anyone trust thousands of doctors and medical researchers over public health authorities and other so-called experts trotted out in media campaigns?
- Physicians figured out how to save lives and control Covid by talking to each other and developing best practices.
- Physicians have more local knowledge and more direct experience with real patients.
- Physicians are not as beholden to pharmaceutical companies as public health authorities, particularly as these authorities have gone as far as mandating pharma products for millions.
- Physicians have learned to scale up their practices, including telemedicine, to avoid ‘hospital overwhelm.’
- Physicians have learned that early treatment and natural immunity is an effective way to reduce the dangers of a pandemic whose virus was probably funded by… public health authorities.
It’s no wonder these doctors are in open rebellion against authoritarian public health bodies who seek to implement monolithic mass behavioral control in place of a dynamic multi-pronged approach that includes clinical best practices.
Intimate, repeated, in-person care, which includes both observational and randomized control studies, has an underappreciated advantage over armchair analysis and “exciting, soul-capturing abstractions,” which have “extended themselves over the perception of world and self like plastic pillowcases.” And yet the doctors of the Physicians Declaration soldier on.
Nevermind. Fall into line. The government is here to help.
Note: The Declaration by the International Physicians and Medical Researchers is not affiliated with The Great Barrington Declaration hosted by AIER. Yet there are striking similarities in that each group represents a groundswell of opposition to authoritarian public health policies worldwide.
Max Borders is author of After Collapse: The End of America and the Rebirth of Her Ideals and The Social Singularity: A Decentralist Manifesto.
October 7, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular, War Crimes | Covid-19 |
Leave a comment

Dr. Rochagné Kilian
OWEN SOUND, Ontario – Dr. Rochagné Kilian recently resigned as an emergency room and family practice physician due to her concerns that the Ontario health system and Grey Bruce Health Services (GBHS) crossed ethical lines throughout the pandemic.
In a virtual meeting that included GBHS CEO Gary Sims and other staff members, Dr. Kilian asked Sims a series of questions about what she believes is unethical behaviour on behalf of the Ontario health system at all levels. Sims appeared to be unprepared for difficult questions pertaining to the ongoing rollout of vaccination mandates and vaccine segregation restrictions the Ontario heath system is championing.
Kilian estimated that 80 percent of the patients she saw in the ER during the past month who had inexplicable symptoms were “double vaxxed.”
Dr. Kilian relocated to Owen Sound – a small city in Grey County, Ontario – from South Africa after previously working in British Columbia. When she resettled in Owen Sound with her family, she expressed to a local paper how happy she was to live there: “Our recruitment to Owen Sound might have been by chance, but our choice to settle here was definitely not. Our four months in Owen Sound have been blessed. A little town with lots of soul, surrounded by beautiful landscapes, filled with welcoming residents and businesses, and exciting festivals, programs and activities. We truly feel fortunate to raise a family here.”
The first issue that Dr. Kilian brought up during the meeting was informed consent regarding the COVID jab and what she considered to be a coercive mentality of pressuring people to accept medications that she pointed out are still in “clinical trials.”
An GBHS administrator did not answer her question directly, but instead passed the buck to the provincial government and stated they do not have “oversight or input” regarding consent mechanisms presented to patients.
Kilian added that having more input into what patients are consenting to is something that GBHS “should consider,” especially in light of enacting the government-recommended vaccination mandates with their own staff.
Referring to informed consent and mandating experimental vaccines that been linked to thousands of deaths and injuries, Sims explained that because of the “pandemic,” certain procedural normalities will not take place.
“In a pandemic, some of those pieces that you think would be there [mechanisms of informed consent from the government] when you have lots of time to review stuff … in a pandemic, they’re going to pass mandates, and they’re going to pass laws, and they’re going to pass directives as needed to manage that pandemic,” he said. “And some of the things … will feel like they’re infringing on or taking short cuts … they are doing that directly to save lives.”
Sims then stated that there is a “massive scientific group” that has reviewed all the issues pertaining to the vaccines and their usage and rollout. This meeting took place August 23. Since then, the Ontario government has admitted that at least one of the vaccines pushed on the public has caused serious heart problems in young men, who are at virtually no statistical risk of suffering severely from COVID.
Dr. Kilian pressed Sims about claims that protocols of informed consent can be skirted due to an emergency, and clarified that the Tri-Council Policy Statement stipulates that an emergency situation does not warrant skirting protocols that protect the population from being put at risk due to medical experimentation. The Tri-Council Policy Statement is a Canadian guideline for the ethical conduct of research involving humans and/or human biological materials. As the vaccinations are still technically under experimental trial, they are being implemented under a research-based framework on the population.
It was Kilian’s opinion that the ethical framework is being ignored, thus health workers and citizens are being forced to take something against their will that is not proven to be safe or effective in the long term, as a result of vaccination mandates.
Sims reacted sharply to Kilian and said, “Nobody is forcing you to do this, you have a right to say no, but the reality is the government has the right to say that you’re not employed.”
“When the law looks at it, the law is saying you have the right to do it [enforcing vaccine mandates],” he added.
Dr. Byram Bridle, a University of Guelph professor, recently released a letter he sent to the president of his university that called into question the legitimacy of vaccine mandates, both from a medical and legal perspective. He stated in the letter that he is “confident there will be lawyers willing to test this in court.”
Dr. Kilian asked a final question in the virtual meeting about the claims that Sims and others at GBHS have made about the majority of COVID-associated cases in the region being among the unvaccinated. She asked if there was a detailed database that could be shared to prove this point. Sims stated that the vaccination status of the individuals who have been admitted in his region could not be released due to privacy reasons, but that the provincial government would have the information.
He then claimed that provincially, “less than 0.7 percent of people who ended up in ICUs were vaccinated.”
He referred to the “third wave” of COVID in Ontario that he said was due to the Delta variant, and stated that “it was all unvaccinated” who fell seriously ill at that time. The third wave in Ontario is reported to have happened in April and May. The vast majority of Ontarians had not received their second dose of any COVID jab by that point, and the province has made it clear in numerous places that a person only counts as “full vaccinated” for clinical purposes after 14 days have passed since they have received their second dose.
During the month of May in the Grey Bruce region, there were a total three confirmed hospitalizations with COVID-19. Five people in the region died that month with a COVID-positive diagnosis, and two of the deaths were residents who died outside of the county.
Sims said on the call that a minimum “80 percent” and up to “97 percent” of ICU patients with COVID across the province were unvaccinated. It is impossible to reach that number given the Grey Bruce statistics because there are too few people for calculations to be mathematical doable.
He then intimated that there will be great fears among pediatric physicians regarding autumn COVID numbers “if children start to die.” There is no evidence to suggest that COVID is dangerous to children in any statistically significant way.
Dr. Kilian resigned from her position while on the call with GBHS administration and spoke about her situation on the The Strong and Free TruthCast, where she criticized the state of health care in Canada. She expressed that care for the individual patient has gone by the wayside during the “farce that we have been living through.”
She said that throughout the entire time that the pandemic has been declared, she has only admitted two patients to the ICU that tested positive for COVID. She then clarified that this did not mean they were in the ICU due to COVID, but only that they had tested positive. She stated that her emergency department was “dead” throughout all of the declared waves of COVID, and that she took pictures of the official numbers to prove that they “had nothing to do” with lack of patients.
Dr. Kilian added that since the rollout of COVID jabs, she has seen a striking uptick in patients who have been admitted with heart issues and do not fit risk categories. She stated that as more and more people have received the jab, she has seen a host of strange events in her patients. She spoke of “people coming with newly diagnosed high blood-pressure, diabetics that was controlled that are no longer controlled – their sugars are either through the roof or they’re down in the ground … The only factor … constant that changed in their life was the injection of an experimental biologic.”
October 7, 2021
Posted by aletho |
Civil Liberties, War Crimes | Canada, Covid-19, COVID-19 Vaccine, Human rights |
Leave a comment
How many people have died of COVID-19? The media is reporting CDC data that the death toll is about 640,000 in the U.S., but the answer is nobody knows. Health officials like Dr. Anthony Fauci claim that there are likely far more COVID-19 deaths than have been reported, meaning that such deaths are being undercounted.1
Evidence of this, however, is lacking and many believe the opposite is true — that COVID-19 deaths have been overreported, in some cases by as much as 500%. In a Full Measure investigation, host and investigative journalist Sharyl Attkisson revealed their findings from around the U.S., which found that “in some documented cases, news that COVID was the cause of death was greatly exaggerated.”2
Meanwhile, the U.S. Centers for Disease Control and Prevention has made startling changes in how they track COVID-19 cases, which is muddling the data and making it virtually impossible to track infections among those who have received a COVID-19 injection.3
Homicide, Suicide Counted as COVID Deaths
Grand County, Colorado, has a population of just 15,717 people.4 It’s the type of rural area where coroner Brenda Bock is able to keep tabs on each and every death, including those from COVID-19 — of which, she said, there were none in 2020.5 COVID-19 deaths, however, were recorded in the area, highlighting the problems with how such casualties are counted. Bock told Attkisson:6
“I had a homicide-suicide the end of November, and the very next day it showed up on the state website as Covid deaths. And they were gunshot wounds. And I questioned that immediately because I had not even signed off the death certificates yet, and the state was already reporting them as Covid deaths.”
The reasoning behind counting the homicide-suicide deaths as COVID-19 casualties was that they were listed in a database of people who had tested positive for COVID-19 within 28 days of their death. According to Full Measure:7
“Because there had been no Covid deaths within the geographic boundaries of Grand County in 2020, Bock was in a unique position to challenge the state’s accounting. In many cities and counties, the numbers are too big and the coroners would never know about discrepancies.”
There were other instances in Grand County as well. Bock investigated two “COVID-19 deaths,” which turned out to be people who were still alive. “They just got put in there by accident,” Bock said.8 Attkisson also spoke with Dr. James Caruso, chief medical examiner and coroner for Denver, who said he had also heard from coroners in rural counties that trauma deaths were being counted as COVID-19 casualties:9
“[A]t some level — maybe the state level, maybe the federal level — there’s a possibility that they were cross-referencing Covid tests. And that people who tested positive for Covid were listed as a Covid-related death, regardless of their true cause of death. And I believe that’s very erroneous, and not the way the statistics needed to be accumulated.”
Dying ‘of’ COVID or ‘With’ COVID
The distinction comes down to some tricky wording: deaths “among” COVID-19 cases and deaths “due to” COVID-19, or dying “of” COVID or “with” COVID. Someone who died with COVID-19 may be counted as a death among COVID-19 cases, even if the virus had nothing to do with their death.
When a death is said to be “due to” COVID-19, this is intended when COVID-19 caused or significantly contributed to the death. According to the Colorado Department of Public Health and Environment:10
“The number of deaths due to COVID-19 are not necessarily included in the number of deaths among people with COVID-19. After review, at either the state or national level, some deaths may not be counted as COVID-19 deaths. This is rare, and the expectation is that in the end the numbers will closely align.”
But according to Bock, the inflated numbers could hurt the region’s economy, which is largely dependent on tourism:11
“It’s absurd that they would even put that on there. Would you want to go to a county that has really high death numbers? Would you want to go visit that county because they are contagious? You know I might get it, and I could die if all of a sudden one county has a high death count. We don’t have it, and we don’t need those numbers inflated.”
Caruso told Attkisson that he voiced his concerns about deaths being wrongly attributed to COVID-19 to the Colorado Department of Public Health in April 2020. A coroner from Montezuma County also complained after an alcohol death was deemed a COVID death. Colorado ended up adding categories to their death counts, stating a person died “Of” COVID or “With” COVID, but the counts were still off.
For instance, Bock’s murder-suicide cases were still being counted under “With COVID,” even though they shouldn’t have been tallied at all. According to Bock:12
“And that’s what I complained about. And then when I did talk to the Governor, he told me he didn’t believe it was right, but he wasn’t going to have them remove it from the count because all the other states were doing it that way so we were going to also.”
Full Measure’s investigation found that of the 13,845 COVID-related deaths in Colorado, about half were among people who died “among” or “with” COVID. The media is also contributing to the confusion. In one instance The New York Times inflated the number of people who died from COVID-19 in Grand County by at least 500%.13
This raises questions about COVID deaths being reported nationwide. There have been reports, for instance, of traffic accident fatalities,14 cancer15 and nursing home or hospice deaths16 being attributed to COVID-19. And in Alameda County, California, when they removed deaths that’s weren’t directly caused by COVID-19 from their official count, the number of “COVID” deaths dropped by 25%.17 Attkisson said:18
“The obvious implications are huge. If such a significant number of Colorado’s “Covid deaths” weren’t directly caused by Covid, or even related at all in some cases, and if that bears out in other states, it means the national totals we’ve heard since the start of the pandemic could be largely misleading.”
CDC Isn’t Tracking Most Cases Among the Vaccinated
Media reports keep referring to the pandemic as a crisis of the unvaccinated, which is simply inaccurate, since COVID-19 continues to affect and spread among those who have been vaccinated. The CDC’s Morbidity and Mortality Weekly Report (MMWR) posted online July 30, 2021, details an outbreak of COVID-19 that occurred in Barnstable County, Massachusetts — 74% of the cases occurred in fully vaccinated people.19
So-called “breakthrough infections,” which used to be known as vaccine failures, were reported by the CDC far earlier, though, including in their May 28 MMWR, which documented 10,262 breakthrough infections reported January 1, 2021, to April 23, 2021, across 46 states.20
This, they believed, was “likely a substantial undercount,” but rather than continuing to assess the situation, they stopped monitoring most COVID-19 infections among vaccinated people:21
“Beginning May 1, 2021, CDC transitioned from monitoring all reported COVID-19 vaccine breakthrough infections to investigating only those among patients who are hospitalized or die, thereby focusing on the cases of highest clinical and public health significance.”
ProPublica detailed the case of Meggan Ingram, a 37-year-old who is fully vaccinated but tested positive for COVID-19. She became sick enough to require oxygen and intravenous steroids in a hospital for three hours, but wasn’t admitted. Her case won’t be counted among the official count, and neither will the seven other people in her household who also tested positive — five of them fully vaccinated.22
The end result is that there’s no way to know how many people have been infected, including among the vaccinated, and how the virus is spreading. As Dr. Randall Olsen, medical director of molecular diagnostics at Houston Methodist Hospital in Texas, told ProPublica, “They are missing a large portion of the infected. If you’re limiting yourself to a small subpopulation with only hospitalizations and deaths, you risk a biased viewpoint.”23
Injection Effectiveness Is Dropping
It’s possible the CDC stopped tracking most COVID-19 cases among the vaccinated in order to obscure just how commonly the vaccines are failing. According to CDC data, the overall COVID-19 vaccine effectiveness declined from 91.8% in May to 75% in July.24 Among nursing home residents, the vaccines are similarly failing, dropping from an effectiveness rate of 74.7% in March-May 2021 to 53.1% in June-July.25
“The vaccinated are not as protected as they think. They are still in jeopardy,” Dr. Eric Topol, director of the Scripps Research Translational Institute, told ProPublica.26 As for why the CDC abruptly stopped tracking most breakthrough cases, the agency said it was because the more targeted data collection would be more useful for “response research, decisions, and policy.”27
However, it’s resulted in a lack of consistency and access to the full data for the U.S. public, with each state varying in what data it’s gathering and whether or not to share it. U.S. Sen. Edward Markey, D-Mass., has called on the CDC to track and share information on COVID-19 breakthrough cases. In a letter to CDC director Dr. Rochelle Walensky, he said:28
“The American public must be informed of the continued risks posed by COVID-19 and variants, and public health and medical officials, as well as health care providers, must have robust data and information to guide their decisions on public health measures.”
In July 2021, he asked to CDC to respond to a series of questions, including whether vaccine-derived immunity is decreasing in light of the breakthrough cases and what action they’re taking to monitor breakthrough cases among people who aren’t hospitalized. As of September 2021, he had still received no response, and many remain puzzled over the CDC’s sudden refusal to track such crucial health data.29
“I was shocked,” Dr. Leana Wen, a physician and visiting professor of health policy and management at George Washington University, told ProPublica. “I have yet to hear a coherent explanation of why they stopped tracking this information.”30
Sources and References
October 7, 2021
Posted by aletho |
Deception | Covid-19, New York Times, United States |
Leave a comment
Yesterday I noted that, 18 months after the start of the pandemic, a sizeable chunk of Americans still dramatically overestimate the risks of Covid. In a recent poll, more than one third said the risk of being hospitalised if you’re not vaccinated is at least 50%.
Of course, you’d expect some people to get the answer wrong just because we’re dealing with a small quantity, and there’s always going to be some degree of overestimation. But many people were off by a factor more than 10. What accounts for this?
Interestingly, Democrat voters’ guesses were much higher than Republican voters’ – about twice as many Democrats said the risk of being hospitalised if you’re not vaccinated is at least 50%. This suggests a role for ideology.
Throughout the pandemic, the ‘Democrat position’ has been to support restrictions and mandates, whereas the ‘Republican position’ has been to oppose such measures. This is clearly visible in a plot of U.S. states by average stringency index. Almost all the ‘red’ states are on the left-hand side, while almost all the ‘blue’ states are on the right.
Given that partisans (on all sides) like to avoid cognitive dissonance, they tend to adopt beliefs that are consistent with their party’s platform. Since Democrat politicians have been busy imposing all sorts of restrictions and mandates, Democrat voters have adopted beliefs that imply those measures were justified.
Most survey respondents don’t know numbers like ‘the risk of hospitalisation for people who aren’t vaccinated’ off the top of their head. Instead, they probably make a guess based on all the relevant information they can recall.
Democrat voters, who’ve spent the pandemic consuming media like MSNBC, CNN and NPR, will recall numerous incidents of pundits saying that Covid is extremely dangerous, and we have to do whatever we can to stop the spread.
They will also recall that they were locked down for months, that their kids’ schools were closed, and that they had to wear a mask whenever they went to the grocery store.
Putting all this information together, they will tend to assume that the risk of being hospitalised from Covid is extremely high. ‘Why else,’ they might ask, ‘would there have been so many restrictions?’
Note: Republicans also overestimated the risk of being hospitalised from Covid, albeit to a lesser extent than Democrats. This indicates that people’s skewed risk perceptions cannot be blamed solely on the content of left-wing media (or the policies implemented in ‘blue’ states).
The psychological quirk that may account for people’s skewed risk perceptions has a name in psychology: the availability heuristic. As Steven Pinker notes, “people estimate the probability of an event or the frequency of a kind of thing by the ease with which instances come to mind”.
Because plane crashes always make the news, people tend to overestimate the risks of air travel. And they may overestimate the risks of Covid for the same reason.
Since the start of the pandemic, we’ve been treated to morbid ‘daily death numbers’ – but for only one cause of death. Perhaps if these figures had been reported for all causes of death, people’s risk perceptions would be slightly less skewed. (Or perhaps they’d just be terrified of everything…)
During a pandemic, we obviously do want people to take precautions; we don’t want them nonchalantly walking into a care home when they have a high fever and a nasty cough. Yet – contrary to what some in government seem to believe – we don’t want people to be utterly terrified either.
There’s been so much attention on people claiming Covid is “just the flu” that the media has largely ignored the other end of the spectrum: people who believe Covid is the bubonic plague!
We can agree it’s bad if people underestimate the risks. But it’s also bad if they overestimate the risks. We want them to have the right risk perceptions. That way, they can make informed decisions.
October 6, 2021
Posted by aletho |
Mainstream Media, Warmongering, Science and Pseudo-Science, Timeless or most popular | Covid-19 |
Leave a comment
Because People were not Afraid Enough of the Flu Virus

Last night Alex Jones of Infowars.com did a special broadcast regarding an October, 2019 video that they had just become aware of that was a panel discussion hosted by the Milken Institute discussing the need for a Universal Flu Vaccine.
The video clip that they played of this event was a 1 minute and 51 second dialogue between the moderator, Michael Specter, a journalist who is a New Yorker staff writer and also an adjunct professor of bioengineering at Stanford University, Anthony Fauci, the director of the National Institute of Allergy and Infectious Disease, and Rick Bright, the director of HHS Biomedical Advanced Research and Development Authority (BARDA).
In this short clip, which was extracted from the hour long panel discussion, Anthony Fauci explains that bringing a new, untested kind of vaccine like an mRNA vaccine, would take at least a decade (“if everything goes perfectly”) to go through proper trials and be approved by the FDA.
He would know, because he had been trying to do it for about a decade already by then (October, 2019), trying to develop an mRNA based vaccine for HIV.
But now they were discussing something much bigger than just a vaccine for AIDS patients. They are talking about a “Universal Flu Vaccine” that everyone would have to take – a huge market for Big Pharma!
Rick Bright, the director of HHS Biomedical Advanced Research and Development Authority (BARDA), then speaks and states that what could happen is that “an entity of excitement that is completely disruptive and is not beholden to bureaucratic strings and processes” could change that.
Here is the short clip which I put on our Bitchute and Rumble channels last night:
Alex Jones spent over 50 minutes covering this on his show last night, and it looks like he covered it on his show today as well.
I have not had a chance to watch these yet, as I went and found the original 1 hour panel discussion video, and spent the day listening to and analyzing that, so that I could supply this report to our readers.
Joining Fauci, Rick Bright, and Michael Specter at this event were:
- Margaret Hamburg, Foreign Secretary, National Academy of Medicine
- Bruce Gellin, President, Global Immunization, Sabin Vaccine Institute
- Casey Wright, CEO, FluLab
In short, this panel discussion focused on what they perceived as the need for a universal flu vaccine, but they admitted that the old way of producing vaccines was not sufficient for their purposes, and that they needed some kind of global event where many people were dying to be able to roll out a new mRNA vaccine to be tested on the public.
They all agreed that the annual flu virus was not scary enough to create an event that would convince people to get a universal vaccine.
And as we now know today, about 2 years after this event, that “terrifying virus” that was introduced was the COVID-19 Sars virus.
And so now we know why the flu just “disappeared” in the 2020-21 flu season. It was simply replaced by COVID-19, in a worldwide cleverly planned “pandemic” to roll out the world’s first universal mRNA vaccines.
This was always the goal, and previous efforts through various influenzas, AIDS, Ebola, and other “viruses” were all unsuccessful in leading to the development of a universal vaccine to inject into the entire world’s population.
Margaret Hamburg stated regarding getting a “Universal Vaccine” into the market:
“It’s time to stop talking, and it’s time to act.”
“I think it is also because we haven’t had a sense of urgency.”
Michael Specter asks:
“Do we need lots of people to die for that sense of urgency to occur?”
Hamburg replies that: “There are already lots of people dying” from the flu each year.
Bruce Gellin states that basically people just are not afraid enough of the term “the flu.”
There are so many things that are revealed about how Big Pharma and government health authorities think in this panel discussion. For example, they bemoan the fact that if they do too good of a job in public health, then they lose funding to develop products that fight viruses.
Michael Specter states: “It seems to me that one of the curses of the public health world is, if you guys do your job well, everyone goes along well and healthy.”
Hamburg: “And they cut your funding.”
Rick Bright complains that the yearly distribution of flu vaccines is inefficient in terms of collecting data, and in the process actually admits that some vaccines just don’t work well:
“We distribute 150 million doses of the seasonal (flu) vaccines every year, we don’t even know how many people are being vaccinated from the doses that are delivered to the people, which doses they got, and what the real outcome was, so that we can learn from that knowledge base on how to optimize or improve our vaccine. So there are opportunities that we have today…”
I think if we uncloaked the poorest performing vaccines in the market place today, it might be very revealing to tell us which of the technologies we have, and allow us to go deeper into those technologies to determine why they are more effective. There are vaccines licenses today that are more effective. I think that we’re just afraid to admit the truth.”
So much for the public mantra that is espoused by Big Pharma and government that the “science” of vaccines is “settled,” and that they are completely “safe and effective.”
Casey Wright repeats the mantra that was publicized every year, before COVID, about just how deadly the flu virus was: “650,000 people die every year from the flu.”
As we have documented many times over the past decade here at Health Impact News, this is simply not true. This is an estimate because actual laboratory confirmed cases of influenza each year are very small, probably less than 1000 in the U.S.
Most flu-like symptoms are never tested in a lab to determine what is causing the symptoms. They were always just classified as “flu” to inflate the numbers to justify the very profitable flu shot each year. Some of our previous coverage of this issue:
Did 80,000 People Really Die from the Flu Last Year? Inflating Flu Death Estimates to Sell Flu Shots
So as they have inflated the COVID-19 cases since last year, they are simply continuing their policy of inflating flu numbers each year in order to sell their vaccines. They obviously could not have done both last year, as the public would have quickly seen that the math doesn’t work.
And yet, so many in the public bought the lie that the COVID-19 measures got rid of the flu, but not COVID-19.
Ultimately, this panel discussion can be boiled down to: Nobody wants to fund research for a universal flu vaccine. So how do we change that? Create a pandemic of fear over the flu (but they couldn’t call it the “flu” because people are no longer afraid of influenza, and the fear over “AIDS” had also subsided.)
Fauci then addressed this “perception problem.”
There’s this perception (about the flu), if it’s so serious, how come people get the flu each year and it isn’t a catastrophe?
When you’re dealing with a disease like HIV, if you get HIV, it’s serious. Whether you’re young, whether you’re middle aged, or whether you’re old. If you get cancer, that’s bad. Whether you’re young, whether it’s intermediate… whereas if it’s influenza, some people, they go throughout life and it doesn’t impact them at all.
There isn’t anyone who is afraid of influenza. You go into a focus group and you say: Are you afraid of getting HIV if you’re at risk? Oh, absolutely.
Are you afraid of getting cancer? Absolutely. Are you afraid of the flu? Don’t bother me.
That’s the reality of how people perceive flu.
And it is going to be very difficult to change that, unless you do it from within and say, I don’t care what your perception is, we’re going to address the problem, in a disruptive way…
Specter then asks:
In the long run, over time, if the 2009 pandemic had been much more deadly, would that have ended up being a better thing for humanity?
Everyone is silent as they obviously were thinking about how to answer that, and Specter says: “Come on gang.”
Fauci ultimately answers and says “No” because there were other years that were worse than 2009 and it didn’t change a thing in terms of creating a universal vaccine.
Hamburg then states:
The sad truth is that when there is a major crisis, it focuses attention and usually resources and some significant mobilization follows.
We need, #1, this time to be different, and we also need to really organize ourselves in a way where there will be accountability for sustained action, and not just response.
Specter states:
Craig Venter, who is a controversial person, but interesting to me, has written that he thinks we ought to have a vaccine, such that, if you take off in a plane from Hong Kong, and are infected, by the time your plane lands in New York, there ought to be a vaccine assembled and deliverable to you.
How crazy is that? How far are we from that? Are we ever going to get there?
Bright replies:
I’m not going to say how far away, but I don’t think that’s too crazy.
I think that if we move towards the era of synthetic-based vaccines, I think we remove the dependencies of thinking the vaccine that has be grown into something else, an egg, a cell, or insect cell – any type of dependency embryo.
If we can move into more synthetic, the nucleic acid based, messenger RNA based, those sequences can be rapidly shared around the world.
He then goes on to talk about using a 3D printer to print out a “vaccine patch” that people use to administer the “vaccine.”
We also learn in this panel discussion why Anthony Fauci is so opposed to natural immunity, because natural immunity for influenza, according to his view, translates to an immune response against other strains of a particular influenza virus, which will interfere with what they are trying to do with the vaccines.
That is why he wants to inject infants as young as 6 months old with a universal vaccine, as he states here, to prevent that “confused” natural immunity from happening before the child grows older.
So the big question that this panel was tackling, was how do they implement their strategies, and what is holding them back?
Certainly the government/regulatory issue is a big one, and now two years later we can see exactly how they did that, by controlling the FDA and the CDC to promote the “killer virus pandemic” narrative as long as possible to justify taking emergency measures that short-cut the normal procedures for bringing novel, new drugs to the market.
It also clearly explains the vicious opposition to existing, cheap therapeutics that very easily treated what is really just the seasonal flu “virus,” which stood in their way of rolling out a universal vaccine.
Casey Wright then made a rather remarkable comment about “philanthropy” and its role in this effort:
There’s a potential role for philanthropy to play there… we are in a position to take on a little more risk (she smiles eerily as she says this), to be open to a little bit more experimentation and methods in how we do things. That’s what I think is unique about FluLab, and its unique about other philanthropies.
I think they can play a really important role there, and fund a set of bolder, maybe earlier promising concepts.
Bingo! Think Bill and Melinda Gates Foundation, the Rockefeller Foundation, and other “philanthropies” that are “unburdened” by regulatory issues as they spend their money pretty much unchecked, with no accountability, all in the name of “science” and the “greater good.”
We have seen most certainly how the Gates Foundation has done this in India by luring poor people into highly questionable ethical experimentations with vaccines, such as the Gardasil vaccine which we have covered so often over the years here at Health Impact News.
Bruce Gellin then talks about a report published by his organization that called for an “entity” that would make these decisions and bring everyone together to collaborate to create this universal vaccine, and eliminate those who oppose.
The report was published in 2019, and here is the press release.
He states:
They called for this “entity” which is the collaboration we talked about. They called for the need to infuse innovation, to find some of these people who we don’t know might be part of the problem to come into this. And to try to think about how we talk about this differently so that your stomach flu doesn’t keep us from making progress. (everyone laughs…)
I assume that this “entity” is Gellin’s group, The Sabin-Aspen Vaccine Science & Policy Group.
Today, this is the main group fighting “vaccine hesitancy” and trying to silence any dissenting voices that get in their way of rolling out this universal vaccine, which of course we now know is the COVID-19 vaccine.
Watch the entire panel discussion to learn just how arrogant these people are. This is on our Bitchute and Rumble channels… Further analysis at Health Impact News.
October 5, 2021
Posted by aletho |
Deception, Timeless or most popular, Video | Covid-19, COVID-19 Vaccine, Gates Foundation, Rockefeller Foundation |
Leave a comment
A patient with Type 1 diabetes called to tell me the pharmacist at our local Walgreens refused to fill the prescription I had written for ivermectin, so I called to ask why.
The young pharmacist, a few years out of pharmacy school, informed me he did not understand why I was using ivermectin for early treatment of COVID because “SARS-CoV-2 does not have an exoskeleton.”
I explained I was not using ivermectin as an anti-parasitic medication, but that it had impressive data as an anti-inflammatory and anti-viral.
Furthermore, as a pediatrician, I have more than 40 years of experience managing multiple viral illnesses. There is value in treating viruses early, often with inexpensive natural remedies, rather than “staying at home until you have problems breathing then go to the hospital” as U.S. public officials have advised for COVID.
The pharmacist was not buying my initial explanation. “I am not going to fill prescriptions for ivermectin that are used in pseudo vaccine doses,” he told me.
I was surprised a young pharmacist was able to override an experienced physician’s prescription, effectively removing an inexpensive prevention and treatment option for selected patients in the middle of a pandemic.
The medical educator in me kicked in. “I would be happy to send you some references about the use of ivermectin for treatment and prevention. There are impressive studies from Argentina, Peru, Africa and India that suggest much better outcomes than we are achieving here in the U.S. with our single-minded focus on vaccines.”
He told me the U.S. Food and Drug Administration (FDA) did not recommend ivermectin for COVID. I asked to see the documentation and he agreed to fax it to me.
I hand-delivered 93 references and a great review article to the Walgreens.
The pharmacist faxed back a post from March 5, on the FDA website entitled “Why You Should Not Use Ivermectin to Treat or Prevent COVID-19.”
The next day, I received notice that a pharmacy in Northern Virginia would not fill any prescriptions for ivermectin if the diagnosis code mentioned COVID.
I had written an ivermectin prescription for a patient who has a history of bad reactions to vaccines and significant autoimmune illness. His adolescent age means that he is at very low risk of death from COVID itself.
Based on my experience as his doctor for over a decade, I was worried about potential adverse events if he got the COVID vaccine. I dug into the data about ivermectin, and it seemed like a great option for him to have on hand for early treatment of COVID if he got sick.
A pharmacist in a drug store, who never examined my patient or learned his extensive medical history, got to trump my best medical judgment by refusing to fill the prescription.
The same day, in a conversation with a compounding pharmacy, we learned of a case in which a patient’s family had to take a hospital to court to obtain treatment with ivermectin.
Bear in mind that the safety profile for ivermectin is excellent and the drug is spectacularly less expensive than the vast majority of hospital interventions.
Three days later, on a zoom call with a colleague whose parents live in Colorado, I learned that a pharmacist at a major drugstore was not only refusing to fill ivermectin for 86- and 87-year-old patients who held valid prescriptions, but the pharmacist was taking the initiative to remind the other King Soopers pharmacies in the state not to fill those prescriptions either.
My analysis of the medical literature is that ivermectin has an impressive safety record and there are multiple studies from around the globe suggesting it can decrease morbidity and mortality from COVID 19.
Two doctors who were actually in the ICU treating real patients, Dr. Paul Marik and Dr. Pierre Kory, looked at their prior experience with similarly sick patients and reviewed treatment strategies to determine what could be helpful.
As Dr. Anthony Fauci advised us to “stay home and wait for the vaccine,” frontline doctors took care of the patients before them, learning valuable lessons about what worked and what did not.
Let’s hit the highlights, quoting directly from the review paper by Kory et al, Jan 2021:
- Since 2012, multiple in vitro studies have demonstrated that ivermectin inhibits the replication of many viruses, including influenza, Zika, Dengue and others (Mastrangelo et al., 2012; Wagstaff et al., 2012; Tay et al., 2013; Götz et al., 2016; Varghese et al., 2016; Atkinson et al., 2018; Lv et al., 2018; King et al., 2020; Yang et al., 2020).
- ivermectin inhibits SARS-CoV-2 replication and binding to host tissue via several observed and proposed mechanisms (Caly et al., 2020a).
- ivermectin has potent anti-inflammatory properties with in vitro data demonstrating profound inhibition of both cytokine production and transcription of nuclear factor-κB (NF-κB), the most potent mediator of inflammation (Zhang et al., 2008; Ci et al., 2009; Zhang et al., 2009).
- ivermectin significantly diminishes viral load and protects against organ damage in multiple animal models when infected with SARS-CoV-2 or similar coronaviruses (Arevalo et al., 2020; de Melo et al., 2020).
- ivermectin prevents transmission and development of COVID-19 disease in those exposed to infected patients (Behera et al., 2020; Bernigaud et al., 2020; Carvallo et al., 2020b; Elgazzar et al., 2020; Hellwig and Maia, 2020; Shouman, 2020).
- ivermectin hastens recovery and prevents deterioration in patients with mild to moderate disease treated early after symptoms (Carvallo et al., 2020a; Elgazzar et al., 2020; Gorial et al., 2020; Khan et al., 2020; Mahmud, 2020; Morgenstern et al., 2020; Robin et al., 2020).
- ivermectin hastens recovery and avoidance of ICU admission and death in hospitalized patients (Elgazzar et al., 2020; Hashim et al., 2020; Khan et al., 2020; Niaee et al., 2020; Portmann-Baracco et al., 2020; Rajter et al., 2020; Spoorthi V, 2020).
- ivermectin reduces mortality in critically ill patients with COVID-19 (Elgazzar et al., 2020; Hashim et al., 2020; Rajter et al., 2020).
- ivermectin leads to striking reductions in case-fatality rates in regions with widespread use (Chamie, Juan, 2020).
- The safety, availability, and cost of ivermectin is nearly unparalleled given its near nil drug interactions along with only mild and rare side effects observed over almost 40 years of use and billions of doses administered (Kircik et al., 2016).
- ivermectin was successful at controlling several diseases which blighted the lives of billions living in poverty in the tropics.
- ivermectin’s discoverers were awarded the Nobel Prize in Medicine in 2015.
- ivermectin is included in the World Health Organization’s “List of Essential Medicines.” It has been widely distributed in countries like India for pennies a day. The out-of-pocket cost of ivermectin at my Walgreen’s is more than$1,000.
Kory and Marik compiled eight studies (three randomized controlled studies and five observational controlled studies) demonstrating efficacy in prevention of COVID-19 with significant decreased transmission.
They found 19 controlled studies that showed significant impacts on time to recovery, hospital stay, decrease in viral loads, reductions in duration of cough and decreased mortality.
In medical history pre-COVID, this body of research about ivermectin would be applauded for bringing value in the midst of a pandemic. In the medical era pre-COVID, the judgment and experience of clinicians at the patient’s bedside counted for something.
Pre-COVID, we taught medical students to use keen observational skills and keep accurate records of whether the patient improved or deteriorated after the treatment strategies used.
In the Age of COVID, pharmacists who chide doctors that “COVID does not have an exoskeleton” deny patients ivermectin — a safe, cheap, effective and potentially life-saving early treatment.
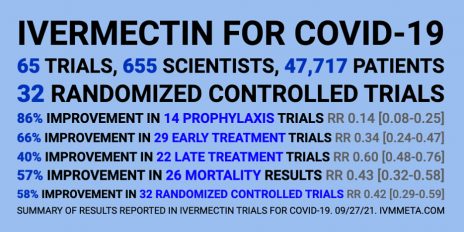
If you or your patients are having trouble getting ivermectin prescriptions filled for COVID 19 prevention or treatment, see this excellent resource from the Front Line COVID 19 Critical Care Alliance.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
October 5, 2021
Posted by aletho |
Science and Pseudo-Science | Covid-19, COVID-19 Vaccine, Ivermectin, United States |
Leave a comment
The UK government’s Winter Plan is rife with nudges
There’s a chill in the air. Not from the changing seasons, it’s still beautifully balmy, but because the behavioural scientists’ fingertips have traced a hoar frost of psychocratic nudge on the government’s “Autumn and Winter Plan”.
The UK government’s Winter Plan plan contained some welcome news. The most draconian schedules of the Coronavirus Act will be revoked, including the powers to close schools, allow potentially infectious people to be detained, and restrictions on gatherings and events. The language around the plan’s launch was thankfully more cool-headed. The times are “challenging” but it is no longer claimed that Covid is the “biggest threat this country has faced in peacetime history”.
But the plan is also rife with “nudges” – sneaky ways to prime, prepare and prod you into the desired mindset and course of action.
The contents are freighted with the sunk cost fallacy; we’ve come so far, we mustn’t allow our good work to be undone. This also taps into people’s innate sensitivity to loss.
The trigger from Plan A to Plan B will be “unsustainable pressure” on the NHS rather than deaths. It’s under serious pressure every winter so consider yourselves to be put on notice.
There are other indications of the inevitability of Plan B. I spoke to behavioural scientist Patrick Fagan, who observed that:
“the Plan A / Plan B approach is a classic example of the foot-in-the-door technique. Firstly it makes us accept Plan A because, compared to Plan B, it looks more reasonable; then, once we have accepted and acclimatised to Plan A, we are more likely to then accept Plan B, because it is just one extra step on top of the commitment we’ve already made. The announcement of Plan B may also be an example of the mere exposure effect: simply by talking about the measures (even if, ironically, saying they won’t be implemented), the government makes them more familiar and therefore more psychologically acceptable.”
Bizarrely, after 18 months we’re trapped in a Groundhog Day of modelling and worst case scenarios. Almost a year ago, on the 21st September, Chris Whitty and Patrick Vallance warned of infections hitting 50,000 per day by mid-October in their “Shock and Awe” presentation. When the day arrived, the moving average was 16,228.
According to the doom-mongers at SAGE, up to 7,000 people could be hospitalised per day within the month. And this September the modellers were wrong once again – hospitalisations peaked at about a 1,000 a day and are now falling.
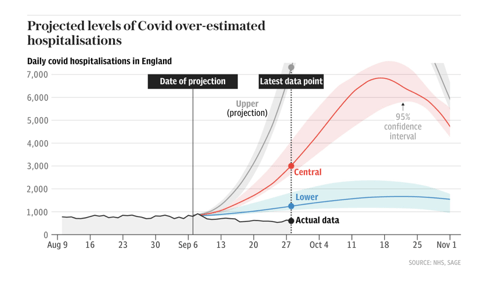
Source: The Telegraph
The big numbers both fuel the policies and justify them. It doesn’t matter that there are more optimistic scenarios, or that the modelling has limitations, because the first supine headline sticks in the brain. The behavioural psychology principle of “salience” draws your attention to what is novel and risky.
Dr Alex De Figueiredo, who conducts mathematical and statistical analyses for the Vaccine Confidence Project, told me that:
“Since the beginning of the pandemic it seems many modelling assumptions, such as the infection fatality rate, have been quite pessimistic. I think this has been why many of the predictions — such as hospitalisations and deaths — have been overstated. It also appears there has been little effort to validate forecasts out-of-sample, such as applying the models to Sweden or Florida, who have had far fewer restrictions.”
There are no quantifiable measures for what justifies each step from Plan A to Plan B. The parameters are fluid, unspecified. This creates confusion and stress, which infantilises people and makes them look to the government for direction. Essentially, confusion increases compliance.
The threat of lockdown hangs like a Sword of Damocles. Will we, or won’t we? It seems unlikely that the public and businesses could be persuaded again. Regardless, the threat of lockdown might be leveraged to justify the introduction of Covid Passports, in what is known as a “reciprocation nudge” – we appear to be given a concession in return for reduced resistance to another option.
Covid Passports have been vigorously opposed by MPs and civil liberties groups, and there hasn’t been a vote in Parliament yet. Despite this, they squat in Plan B as a fait accompli, in the denouement of the “door in the face” technique. This is when a huge request is made, then refused, to be followed by a second smaller request, in this case relegation to Plan B and for limited venues only. Boris Johnson said that it’s “not sensible to rule out this kind of option now when it might still make the difference between keeping businesses open or not.” But why would it be sensible when the Public Administration and Constitutional Affairs Committee produced a damning report against them and found the government could make no scientific case in their favour?
Covid Passports appear to be a behavioural science tool, used to increase vaccine uptake. This may backfire. ‘A Cross-Sectional Study in the UK and Israel on Willingness to Get Vaccinated against COVID-19’ found that vaccine passports deter a significant minority of people who want autonomy over their bodies. This also chimes with the research conducted by De Figueiredo and colleagues at The Vaccine Confidence Project. The bullying and resultant mistrust may impact Covid-19 vaccine uptake as well as other public health initiatives.
When my book A State of Fear: how the UK government weaponised fear during the Covid-19 pandemic was published some people believed, quite quaintly, that public health measures and messaging were unrelated to behavioural science. I think that the book and the writings of other academics and journalists have moved the dial. Once nudge is seen it can’t be unseen. The public increasingly see the nudge. If the behavioural scientists have been dazzling people with card tricks they have over-played their hand.
As such, there is more honesty about the purpose Covid Passports serve. Nicola Sturgeon, Scotland’s First Minister, said that the passport scheme
“will not eradicate transmission completely but it will help reduce it in some higher risk settings, and it will maximise protection against serious illness. And we believe – as we have seen already in some other countries – it will help encourage take-up of the vaccine.”
Similarly, Linda Bauld, Professor of Public Health and Interim Social Policy Adviser to the Scottish Government, also admitted that Covid Passports are “to increase uptake in vaccination” and the “rationale” is that it particularly boosts vaccination in 18 to 29 year olds.
While Covid Passports are in Plan B, Ministers say different things about them each day. Within the space of a week, Sajid Javid scrapped them but also didn’t rule them out for pubs. Javid admitted there’s “no evidence” for them but Boris Johnson called them “sensible”. Does the left hand not know what the right hand is doing? Or maybe a big behavioural science brain lurks in between. The epidemic management is reminiscent of the uncertainty created by Vladislav Surkov in the Soviet Union to deliberately turn politics into a performance of confusion – you don’t know what’s real anymore.
There are never-ending question marks over travel, although double-vaccinated travellers will no longer need expensive and inconvenient PCR tests. The double-jabbed will delight in the news, and it sounds sensible on the surface. However, this is not about “following the science”, since the previously infected do not benefit from the exemption. This is an incentive, a classic nudge, to encourage jabs. The vaccinated are rewarded and the unvaccinated are punished. Bearing in mind that negative tests and prior infection could suffice, this decision reeks of disdain for personal autonomy.
Vaccines for 12 to 15 year olds have been authorised. Politicians have stirred up debate amongst all corners regarding whether children should be jabbed with their parents’ consent or not. This utilises what Patrick Fagan calls “the leapfrog effect”. He says,
“it leapfrogs one stage of the debate and in doing so, sets the baseline assumptions which become accepted implicitly. Specifically, by having people debate whether or not parents’ consent should be sought, they are establishing the unspoken assumption that children should receive the jab in the first place. Those who think they are debating the government, arguing that parents’ consent is needed, are actually accepting its true goal, to jab kids.”
The government might be more in control of the narrative than many people like to believe. (Of course, chaos and confusion are alternatives…)
Worryingly, can teens truly provide informed consent? Throughout 2020 they were exhorted not to “kill granny”, which would provoke fear, shame and stress. Ads on Tiktok tell youngsters that the way to get back to normal is to take the vaccine. The vaccine will be rolled out in schools which will create peer pressure, in a particularly egregious use of “norms”. Finally, if the JCVI found the decision difficult, how is a 12 year old supposed to weigh up the evidence? (Nudging teens is the subject matter of my next article.)
Since the Cabinet reshuffle, Michael Gove has been informally dubbed the ‘Minister for Christmas’. Boris Johnson joked that he “didn’t want to have to cancel Christmas again”. Did you know Christmas might be cancelled and needs saving? You do now, the idea has been “seeded”.
Although it is ostensibly supply chains which threaten Christmas, the joke draws a comparison with last year’s Covid reasons. Again, you are put on notice. The nudges are still focussed on increasing vaccination, for now, but the threat to Christmas might hint at the beginning of a behavioural science approach to meet green targets.
We must be good boys and girls if we want Santa to come. And be aware, the nudgers are drafting our collective New Year’s Resolutions.
October 5, 2021
Posted by aletho |
Book Review, Deception, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine, UK |
Leave a comment