CDC Gives Incoming Refugees Nobel Prize-Winning Ivermectin
By Kelen McBreen | InfoWars | September 3, 2021
All Middle Eastern, Asian, North African, Latin American, and Caribbean refugees entering the U.S. since 2019 have been prescribed ivermectin.
The CDC recommendation advises doctors working for the International Organization for Migration (IOM), who screen refugees in their home countries, and American doctors who treat them when they arrive to prescribe both ivermectin and albendazole.
Since the CDC guidance was released pre-Covid, naysayers will point out the ivermectin was prescribed for parasites and not for Covid-19, and presume the drug probably doesn’t work against viral infections.
Ivermectin’s creators won a Nobel Prize in Medicine in 2015 for the drug’s ability to battle infections caused by roundworm parasites.
As Tokyo, Japan’s top health official Dr. Haruo Ozaki recently explained, “In Africa, if we compare countries distributing ivermectin once a year with countries which do not give ivermectin… I mean, they don’t give ivermectin to prevent Covid, but to prevent parasitic diseases… but anyway, if we look at Covid numbers in countries that give ivermectin, the number of cases is 134.4 per 100,000, and the number of death is 2.2 in 100,000.”
He continued, “Now, African countries which do not distribute ivermectin: 950.6 cases per 100,000 and 29.3 deaths per 100,000. I believe the difference is clear.”
Several studies show ivermectin actually is effective at treating Covid-19, but what this information truly exposes is the current media and government demonization campaign against it.
Despite media cries of “people eating horse paste” and several stories about an increase in poison control calls from people misusing the drug, the CDC has been giving it to refugees for at least two years.
By the way, a Fox 9 Minnesota story lists possible symptoms of an ivermectin “overdose” as “nausea, vomiting, diarrhea, decreased consciousness, hallucinations, seizures, coma, and death.”
However, not a single person in the United States has died from a Covid-related ivermectin overdose.
Plus, the majority of people resorting to the horse version of ivermectin are doing so because the attacks on the drug have convinced many doctors and pharmacies not to prescribe or carry it.
The establishment is even upset that celebrities like top podcast host Joe Rogan and “Cheers” star Kirstie Alley have touted the drug as helping them defeat Covid.
The CDC is obviously aware that the drug is safe for people to use as its physicians prescribe it to refugees just as tens of thousands of doctors across the U.S. are now giving it to patients for Covid.
So, why is mainstream media and a government agency like the FDA scaring Americans out of a treatment that could help them with the virus?
The FDA’s website explains, “Certain animal formulations of ivermectin such as pour-on, injectable, paste, and ‘drench,’ are approved in the U.S. to treat or prevent parasites in animals. For humans, ivermectin tablets are approved at very specific doses to treat some parasitic worms, and there are topical (on the skin) formulations for head lice and skin conditions like rosacea.”
Well, no doctors are prescribing ivermectin animal formulations to their patients, and the government and media both know this.
Perhaps it’s because the FDA, which is “virtually controlled by Pfizer” according to President Trump, is currently developing their own Covid drug to be taken twice a day alongside their vaccine.
Merck, the company that produces ivermectin, is also developing a drug to treat Covid which will make them much more money than the cheap antiviral ivermectin.
On June 9, Merck revealed that the U.S. government is paying the company $1.2 billion to supply 1.7 million courses of the new drug to federal government agencies.
Or, it could be that the Covid vaccines still being used under Emergency Use Authorization would no longer have that emergency approval if a legitimate low-risk treatment were available.
Follow the money and stop paying attention to establishment media.
On child vaccines, the experts are suddenly reluctant to follow ‘the science’
By Jonathan Cook | September 4, 2021
In some of these blogs I have been trying to gently highlight what should be a very obvious fact: that “the science” we are being constantly told to follow is not quite as scientific as is being claimed.
That is inevitable in the context of a new virus about which much is still not known. And it is all the more so given that our main response to the pandemic – vaccination – while being a relatively effective tool against the worst disease outcomes is nonetheless an exceedingly blunt one. Vaccines are the epitome of the one-size-fits-all approach of modern medicine.
Into the void between our scientific knowledge and our fear of mortality has rushed politics. It is a refusal to admit that “the science” is necessarily compromised by political and commercial considerations that has led to an increasingly polarised – and unreasonable – confrontation between what have become two sides of the Covid divide. Doubt and curiosity have been squeezed out by the bogus certainties of each faction.
All of this has been underscored by the latest decision of the Joint Committee on Vaccinations and Immunisation, the British government’s official advisory body on vaccinations. Unexpectedly, it has defied political pressure and demurred, for the time being at least, on extending the vaccination programme to children aged between 12 and 15.
The British government appears to be furious. Ministers who have been constantly demanding that we “follow the science” are reportedly ready to ignore the advice – or more likely, bully the JCVI into hastily changing its mind over the coming days.
And liberal media outlets like the Guardian, which have been so careful until now to avoid giving a platform to “dissident” scientists, are suddenly subjecting the great and the good of the vaccination establishment to harsh criticism from doctors who want children vaccinated as quickly as possible.
Watching this confected “row” unfold, one thing is clear: “the science” is getting another political pummelling.
Peek behind the curtain
There are a few revealing snippets buried in the media reports of the JCVI’s reasons for delaying child vaccinations – information that challenges other parts of the vaccination narrative that have been unassailable till now.
One concerns long Covid, fear of which has probably been the main factor driving parents to push for their children to be vaccinated – given that Covid poses little immediate threat of serious illness to the vast majority of children. Of long Covid in children, the JCVI argues, according to the Guardian, that “the impact of the symptoms may be no worse than those seen in children who have not actually had Covid”.
What to make of that? We know that over the past few decades a small but growing proportion of children have been suffering from long-term chronic fatigue syndromes – often following a viral infection. This may relate to more general immunity problems in children that, like other chronic disease, doctors have been largely baffled by – and may even be contributing to.
Is long Covid another fatigue syndrome, and one that many of these children would have suffered from if they had been infected with a different virus, like flu? Don’t hold your breath waiting for a debate on that question, let alone an answer, any time soon.
Then there is this. The Guardian reports that the JCVI was concerned about “the unknown longer-term consequences of a rare side-effect [myocarditis – heart inflammation] seen with mRNA vaccines such as the Pfizer/BioNTech and Moderna shots. … What makes the JCVI uneasy is that there is little long-term follow-up on vaccinated children.”
“Unknown longer-term consequences”? A lack of “follow-up” on vaccinated children? These sound more like the criticisms of the tin-foil hat-wearers than the cautious advice of vaccination experts.
Or is it just that we have been given a fleeting peek behind the curtain of official medical debate to see an uncertainty that has been actively concealed from us. “The science” is not quite as solid as the scientists or politicians would have us believe, it seems.
Piling on the pressure
What sensible view should we, the public, take when that “scientific” consensus suddenly solidifies – possibly as soon as next week – behind exactly what the politicians are demanding.
The government and parts of the media are clearly going to keep piling the pressure on the JCVI. The committee’s efforts to avoid being drawn into a highly charged and politicised debate about vaccinating children is written all over the caveats and get-out clauses in its decision on Friday.
The government’s stated aim in wanting to vaccinate children is to avoid “disruption” to children’s education, as though this is about the well-being of pupils. But we need to be honest: the disruptions were imposed on schools by politicians and educators not for the sake of children but for the sake of adults, frightened by our own vulnerability to Covid.
The JCVI has embarrassed the government by reminding us of this fact in relation to child vaccinations. Not only have we deprived children of a proper education over a year or more and opportunities to develop physically, mentally and emotionally through their school life, clubs, trips and sport, but now, suggests the JCVI, we want to inject them with a new drug whose long-term consequences are not fully understood or, it seems, being properly investigated.
All of this will be unmentionable again as soon as the JCVI can be arm-twisted into agreeing to the government’s demands. We will be told once again to blindly “follow the science”, to obey these political dictates as we were once required to obey the spiritual dictates of our clerics.
Censoring testimony
“Follow the science” is a mantra designed to shut down all critical thinking about how we respond to the pandemic – and to justify censorship of even well-qualified dissenting scientists by corporate media and their social media equivalents.
For example, YouTube has excised the testimony of medical experts to the US Congress who have been trying to bring attention to the potential benefits of ivermectin, a safe, long-out-of-patent medicine. Instead the corporate media is derisively describing it as a “horse drug” to forestall any discussion of its use as a cheap therapeutic alternative to endless, expensive vaccine booster shots.
(And by the way, before the “follow the science” crowd work themselves into a lather, I have no particular view on the usefulness of ivermectin, I simply want experts to be allowed to discuss it in public. Watch, for example, this farcical segment below from the Hill in which the presenters are forced, while discussing the media furore about podcast star Joe Rogan’s use of ivermectin to treat his Covid, to avoid actually naming the drug at the centre of the furore for fear of YouTube censorship.)
To want more open debate, not less, about where we head next, especially as western states have vaccinated significant majorities of their populations, is often being treated as the equivalent of “Covid denial”.
Where this new authoritarian climate leads is apparent in the shaming of anyone who tries to highlight that our responses to Covid are following a familiar big-business-friendly pattern: focus all attention on expensive, short-term, resource-hungry quick fixes (in this case, vaccines) and ignore important, long-term, sustainable solutions such as improving the population’s health and immunity to this pandemic and the ones likely to follow.
An obesity epidemic – obesity is a key factor in susceptibility to severe Covid, though you would hardly know it from the media coverage – is still not being tackled, even though the obesity epidemic, unlike Covid, has been growing as a public health threat for many decades. Why? Because the corporate food industry, and more especially the fast-food and sugar industries, and the corporate health industries are financially invested in it never being tackled.
There is no serious media debate about the role of health in tackling Covid because the corporate media are invested in exactly the same consumption model as the food and health corporations – not least, they heavily depend on corporate advertising.
Which is why the media hurried to amplify attacks on Jonathan Neman, head of the salad fast-food restaurant chain Sweetgreen, for supposedly “downplaying the importance of vaccines”, as soon as he pointed out the statistical fact that 78 per cent of people admitted to hospital for Covid are obese and overweight. He asked quite reasonably:
What if we made the food that is making us sick illegal? What if we taxed processed food and refined sugar to pay for the impact of the pandemic? What if we incentivized health?
Politicians, of course, have no interest in taking action against the corporate food industry both because they depend on campaign donations from those same corporations and because they want good press from the corporate media.
Studies on immunity
Another topic that has been made all but taboo is the issue of natural immunity. A series of recent studies suggest that those who have caught and recovered from Covid have a better response to the delta variant than those who have been vaccinated only.
Those who have recovered appear to be many times less likely to get reinfected, suggesting natural immunity confers stronger and longer-lasting protection against Covid than vaccines, including preventing hospitalisation and transmission to others.
That may have significant implications for our reliance on vaccines. For instance, vaccines may be playing a part in creating new, more aggressive variants, given that the vaccinated have been wrongly encouraged to see themselves as at less risk of catching Covid but are in fact more likely than those who have recovered to transmit the disease.
If that is the case, the current orthodoxy preferring vaccines has turned reality on its head.
Perhaps, not surprisingly, these studies have received almost no coverage. They conflict with every single message the politicians, media and “follow the science” crowd have been promulgating for months.
How much that narrative has been engineered can be seen in the role the World Health Organisation played early on, as the vaccines were being rolled out, in secretly trying to rewrite medical history. Uniquely in the case of Covid, they pretended that herd immunity could only be achieved through vaccination, as though natural immunity did not count.
Highlighting this new study does not mean that letting Covid rip through the population is the best strategy, or that vaccinations do not help prevent illness and the spread of Covid.
But it does undermine the simple-minded, and novel, insistence that vaccination is the only safe way to protect against a virus, or even the best.
It does undermine the case increasingly being promoted by politicians and the media that the unvaccinated should be treated as a threat to society and accorded second-class status (watch the video below).
It does undermine the demand for vaccine passports as a prerequisite for “normal life” being restored.
And it hints at an additional reason the JCVI may have been reluctant to rush into testing a new generation of vaccines on children for a disease that is rarely serious for them and to which they will have stronger immunity if they catch it rather than being vaccinated against it.
Glaring vacuum
What these studies and others suggest is that we need a more open, honest debate about the best way forward, a more inclusive debate rather than what we have at the moment: accusations, arrogance and contempt – from both sides.
The left should not be siding with media corporations to shut down debate, even Covid denial; they should be pushing for more persuasive arguments. And the left should not be cheering on the bullying or stigmatising of people who are hesitant about taking the vaccines, either for themselves or their children.
Enforce a glaring vacuum in the public discourse, as has happened with Covid, and two things are guaranteed: that politicians and corporations will exploit that vacuum to increase their power and profits; and a significant section of the public will attribute the worst, most cynical motives to those enforcing the vacuum.
The very act of gagging anyone – but most especially experts – from conducting certain kind of conversations is bound to increase political alienation, cynicism and social polarisation. It creates no kind of consensus or solidarity. It creates only division and bitterness. Which, putting my cynic’s hat on for a moment, may be the very reason why it seems to be our leaders’ preferred course of action.
UK data tables on September 3 say delta causes less mortality and less % of admissions than alpha or beta
By Meryl Nass, MD | September 4, 2021
This briefing provides an update on previous briefings up to 20 August 2021:
Technical briefing 22, 3 September 2021
On pages 15-20 (Table 4) we see the following (I will use (I) for inclusion and (E) for exclusion, which are described below:
% admitted from the ER (E) (I) Mortality rate, overall
alpha < 50 years 1.0% 1.4% 0.1%
alpha > 50 5.3% 8.6% 4.8%
beta < 50 1.0% 1.5% 0.2%
beta. > 50 4.2% 9.0% 4.2%
delta < 50 0.7% 1.2% 0.0%
delta > 50 2.8% 6.2% 2.3%
Below are the odd inclusion and exclusion criteria. But it really doesn’t matter which you use, for delta is milder using either, both in terms of deaths and in terms of percent hospitalized from the ER.
# Inclusion: Including cases with the same specimen and attendance dates
‡ Exclusion: Excluding cases with the same specimen and attendance dates. Cases where specimen date is the same as date of emergency care visit are excluded to help remove cases picked up via routine testing in healthcare settings whose primary cause of attendance is not COVID-19. This underestimates the number of individuals in hospital with COVID-19 but only includes those who tested positive prior to the day of their emergency care visit. Some of the cases detected on the day of admission may have attended for a diagnosis unrelated to COVID-19. ^ Total deaths in any setting (regardless of hospitalisation status) within 28 days of positive specimen date.
On page 11 the report claims that the risk of hospitalization is greater for delta (which is undermined by the data table 4 in the report) but it cites some other data set to make the point:
“The crude analysis indicates that the proportion of Delta cases who present to emergency care is greater than that of Alpha, but a more detailed analysis of 43,338 COVID-19 cases indicates that the risk of hospitalisation among Delta cases is 2.26 times greater compared to Alpha (Twohig and others, 2021 ).”
While the proportion who present to the ER with delta may be greater, this could be a function of all the fearmongering about the delta strain. The data presented, however, are very reassuring about delta mortality and hospitalization rates. The data are incredibly reassuring about young people: those under 50. Only 0.03% have died (my calculation) which is counted as 0% in Table 4. A considerably lower proportion than for alpha or beta.
I have omitted the other variants here because there were less than 500 total cases identified for each in the Table.
Madness

Philosophers-stone.info, 2020
By Richard Hugus | September 4, 2021
Looking at the last year and a half, it seems people have forgotten that evil is a significant and real force in our world. The term has religious connotations which secular societies would like to avoid, but we might do well to remember the old story of good versus evil. Evil people are not stupid. They know very well how to lie while appearing to be the soul of virtue. How could we doubt that the homely philanthropist Bill Gates, or the smiling Justin Trudeau, or Anthony Fauci with his Brooklyn accent, or the fatherly Joe Biden, could have anything but the best of intentions for us? Well, that’s how the game works. These people were chosen for their job because they are effective liars — one of the perks of selling one’s soul.
The “pandemic” is an attack on human freedom being conducted in increments. We started out with a three week quarantine to relieve supposedly overwhelmed hospitals and health care workers. Now, 18 months later, “there will be consequences” for people who refuse to get “vaccinated” says Trudeau in Canada. In Australia, people who have been under strict lockdown for months are now being told not to talk to each other or bring their children to playgrounds. Internment camps have been mentioned, and some say they are being built for those who refuse the jab. Children are being taken away from “unvaccinated” parents. If current jab rates are any indication, half the world’s population may end up in the camps, but that’s not an insanity too far for our would-be masters.
The globalists seem to care very much about getting something injected into us. They know better than we do what that is and what it is supposed to do — we can only speculate. Is it a slow-acting poison like glyphosate, promoted for many years by the same cast of characters? Is it a tool for chronic disease to keep the pharmaceutical industry and the medical establishment in business, like conventional vaccines? Is it a sterilizing agent to reduce the world population? Is it a code to genetically modify human beings? Is it the foundation of the circuitry that will connect us to 5G so that we can be completely surveilled? Or is it 6G, which will have enough bandwidth to bring us into the completely manufactured reality of The Matrix? We don’t know. But clearly there is a hidden agenda.
Some say the agenda of mass immunization is to institute “vaccine passports” to bring in totalitarian social control. But if this was the only goal, why would the clever technocrats, with all their careful planning, have chosen to inject people with a “vaccine” that doesn’t prevent or stop transmission of the alleged virus and is so harmful that not long after it was rolled out it started killing and injuring people in such large numbers that it couldn’t be covered up? The genius technocrats would have been much better off using a saline solution, then declare victory over the “pandemic” with no side effects. No, it seems that there is something important in the shot, and that the idea is to change all of humanity with it. If so, there will have been no crime more diabolical in the history of the world. While patriots thought their love of country and their guns would protect them, Klaus Schwab walked right in the front door and robbed them blind. Full-on psychological warfare of 2020 became biological warfare in 2021, and not a shot was fired. Our enemy were kindly medical personnel with syringes. Bullets don’t stop nano-scale mRNA.
In a 2017 TedX talk, Tal Zaks, the Israeli chief medical officer of Moderna, bragged about “hacking the software of life.” At this point, science revealed hubris perhaps not seen since the development of the atom bomb. We learn from Greek tragedy that there is always a reckoning when man meddles with forces he knows nothing about — in this case, the human genome. “Whom the gods would destroy, they first drive mad.” The same story goes back to the ancients.
As they go mad, the globalists are on a race to the bottom. They want to get as many people injected as they can before people realize the injections are not only not stopping disease, they are causing it. The masters of the universe have to suppress clear proof that safe conventional medicines effectively treat whatever the illness is called “covid” — how we hate the word! They want as many people as they can enrolled in their social credit system before people realize they’ve fallen into a trap. They want so much of the crime accomplished that it can no longer be reversed.
The race is desperate. New York Mayor deBlasio has declared that the 8 million people who live in the city be segregated according to their injection status, just like Jim Crow. Dictator Dan is re-enacting the Milgram experiment on the entire population of Australia. Emmanuel Macron wants the French to starve to death if they don’t get the “pass sanitaire.” Joe Biden has told employers outright to require the jab as a condition for work, since the federal government can’t legally do it. He has social media doing the same thing with censorship. Colleges and universities are making injection status a condition of enrollment, destroying careers and higher ducation. Variants of “the virus” are being hyped to create more fear, when there was never a valid test for the original. The dark ritual of masking is coming back. Children are again being muzzled in school, and our entire society is being humiliated as the most innocent and least protected among us — children — are publicly abused. The children themselves may come to see their parents and all adults as cowards for not protecting them. The “unvaccinated” are being vilified, with virtue signalers openly suggesting they deserve to be punished. All this is happening apace because so many people will be getting sick from the injections that there will be no way to cover it up. The globalists are acting more like mad scientists than confident leaders serene in their power . . . because they are mad.
We should understand that what the authorities pretend to be incompetence and unfortunate mistakes are actually intended goals. They haven’t destroyed economies or immiserated, injured, and killed thousands of people by mistake. They know what they’re doing, and they’re doing their best to cover it up. The next flu season may bring disaster, with large numbers of people getting sick because their immune systems have been seriously damaged by the jab. At that point, the plan may be so obvious that even the brainwashed will wake up.
It is up to us to put a stop to the mass injection program. If only one person changes their mind after seeing our protests, we will have made a difference. It is not too late.
Why all the fuss about Ivermectin?
By Brian C. Joondeph | American Thinker | September 3, 2021
First hydroxychloroquine, now ivermectin, is the hated deadly drug de jour, castigated by the medical establishment and regulatory authorities. Both drugs have been around for a long time as FDA-approved prescription medications. Yet now we are told they are as deadly as arsenic.
As a physician, I am certainly aware of ivermectin but don’t recall ever writing a prescription for it in my 30+ years’ medical career. Ivermectin is an anthelmintic, meaning it cures parasitic infections. In my world of ophthalmology, it is used on occasion for rare parasitic or worm infections in the eye.
Ivermectin was FDA approved in 1998 under the brand name Stromectol, produced by pharmaceutical giant Merck, approved for several parasitic infections. The product label described it as having a “unique mode of action,” which “leads to an increase in the permeability of the cell membrane to chloride ions.” This suggests that ivermectin acts as an ionophore, making cell membranes permeable to ions that enter the cell for therapeutic effect.
Ivermectin is one of several ionophores, others including hydroxychloroquine, quercetin, and resveratrol, the latter two available over the counter. These ionophores simply open a cellular door, allowing zinc to enter the cell, where it then interferes with viral replication, providing potential therapeutic benefit in viral and other infections.
This scientific paper reviews and references other studies demonstrating antibacterial, antiviral, and anticancer properties of ivermectin. This explains the interest in this drug as having potential use in treating COVID.
Does ivermectin work in COVID? I am not attempting to answer that question, instead looking at readily available information because this drug has been the focus of much recent media attention. For the benefit of any reader eager to report this article and author to the medical licensing boards for pushing misleading information, I am not offering medical advice or prescribing anything. Rather, I am only offering commentary on this newsworthy and controversial drug.
What’s newsworthy about ivermectin? A simple Google search of most medications describes uses and side effects. A similar search of ivermectin provides headlines of why it shouldn’t be taken and how dangerous it is.

YouTube screen grab
The Guardian describes ivermectin as horse medicine reminding readers considering taking the drug, “You are not a horse. You are not a cow”, saying it’s a medicine meant for farm animals. The FDA echoed that sentiment in a recent tweet, adding “Seriously, y’all. Stop it,” their word choice making it obvious who the tweet was directed to.
Perhaps the FDA didn’t realize that Barack and Michelle Obama often used the term “y’all” and that some might construe the FDA tweet as racist.
The FDA says ivermectin “can be dangerous and even lethal,” yet they approved it in 1998 and have not pulled it from the market despite it being “dangerous and lethal.” Any medication can be “dangerous and lethal” if misused. People have even overdosed on water.
It is true that ivermectin is also used in animals, as are many drugs approved for human use. This is a list of veterinary drugs with many familiar names of antibiotics, antihypertensives, and anesthetics commonly used by humans. Since these drugs are used in farm animals, should humans stop taking them? That seems a rather unscientific argument against ivermectin, especially coming from the FDA.
And healthcare professionals are not recommending or prescribing animal versions of ivermectin as there is an FDA-approved human formulation.
Does ivermectin work against COVID? That is the bigger question and worthy of investigation, rather than reminding people that they are not cows.
A study published several months ago in the American Journal of Therapeutics concluded,
Meta-analyses based on 18 randomized controlled treatment trials of ivermectin in COVID-19 have found large, statistically significant reductions in mortality, time to clinical recovery, and time to viral clearance. Furthermore, results from numerous controlled prophylaxis trials report significantly reduced risks of contracting COVID-19 with the regular use of ivermectin. Finally, the many examples of ivermectin distribution campaigns leading to rapid population-wide decreases in morbidity and mortality indicate that an oral agent effective in all phases of COVID-19 has been identified.
To my knowledge, these 18 studies have not been retracted, unlike previous studies critical of hydroxychloroquine which were ignominiously retracted by prestigious medical journals like The Lancet and the New England Journal of Medicine.
Yet the medical establishment refuses to even entertain the possibility of some benefit from ivermectin, castigating physicians who want to try it in their patients. 18 studies found benefit. Are they all wrong?
Podcaster Joe Rogan recently contracted COVID and recovered within days of taking a drug cocktail including ivermectin. Was it his drug cocktail, his fitness, or just good luck? Impossible to know but his experience will keep ivermectin in the news.
Highly unvaccinated India had a surge in COVID cases earlier this year which abruptly ended following the widespread use of ivermectin, over the objections and criticism of the WHO. In the one state, Tamil Nadu, that did not use ivermectin, cases tripled instead of dropping by 97 percent as in the rest of the country.
This is anecdotal and could have other explanations but the discovery of penicillin was also anecdotal and observational. Good science should investigate rather than ignore such observations.
The Japanese Medical Association recently endorsed ivermectin for COVID. The US CDC cautioned against it.
There is legal pushback as an Ohio judge ordered a hospital to treat a ventilated COVID patient with ivermectin. After a month on the ventilator, this patient is likely COVID free and ivermectin now will have no benefit, allowing the medical establishment to say “see I told you so” that it wouldn’t help.
By this point, active COVID infection is not the issue; instead, it is weaning off and recovery from long-term life support. The early hydroxychloroquine studies had the same flaw, treating patients too late in the disease course to provide or demonstrate benefit.
These drugs have been proposed for early outpatient treatment, not when patients are seriously ill and near death. Looking for treatment benefits in the wrong patient population will yield expected negative results.
Given how devastating COVID can be and how, despite high levels of vaccination in countries like the US, UK, and Israel, we are seeing surging cases and hospitalizations among the vaccinated, we should be pulling out all the stops in treating this virus.
Medical treatment involves balancing risks and benefits. When FDA-approved medications are used in appropriate doses for appropriate patients, prescribed by competent physicians, the risks tend to be low, and any benefit should be celebrated. Instead, the medical establishment, media, and regulatory authorities are taking the opposite approach. One has to wonder why.
Journal Nature: COVID lockdowns are key to begin ‘personal carbon allowances’
Restrictions on individuals… that were unthinkable only 1 year before’ have us ‘more prepared to accept tracking & limitations’ to ‘achieve a safer climate’
Nature Sustainability |
Authors argue COVID restrictions, smart meters & tracking apps can be used as a stepping stone for a personal carbon allowance:
Journal article urges for “the need for a low-carbon recovery from the COVID-19 crisis” by using “personal carbon allowances (PCAs).”
“A PCA scheme would entail all adults receiving an equal, tradable carbon allowance that reduces over time in line with national targets… encompassing individuals’ carbon emissions relating to travel, space heating, water heating and electricity.” …
“Allowances were envisioned to be deducted from the personal budget with every payment for transport fuel, home-heating fuels and electricity bills. People in shortage would be able to purchase additional units in the personal carbon market from those with excess to sell. New, more ambitious PCA proposals include economy-wide emissions, encompassing food, services and consumption-related carbon emissions, for example.”
In particular, during the COVID-19 pandemic, restrictions on individuals for the sake of public health, and forms of individual accountability and responsibility that were unthinkable only one year before, have been adopted by millions of people. People may be more prepared to accept the tracking and limitations related to PCAs to achieve a safer climate and the many other benefits (for example, reduced air pollution and improved public health) associated with addressing the climate crisis.Sustainable Development Goals (SDGs)
Other lessons that could be drawn relate to the public acceptance in some countries of additional surveillance and control in exchange for greater safety… Recent studies show how COVID-19 contact-tracing apps were successfully implemented with mandatory schemes in several East Asian countries, such as China, Taiwan and South Korea… Recent advances in smarter home and transport options make it possible to easily track and manage a large share of individuals’ emissions. Evidence from the roll-out of smart meters and informative displays can be used to design feedback that is highly effective in engaging individuals to reduce their energy-related emissions… In terms of implementation platforms, while in the 2000s carbon allowances were expected to be managed by a card, in the 2020s high ownership would make smartphones the preferred option for accounting and trading (while providing alternative options for the few without smartphones).
The State That Doesn’t Care If You Live Or Die

By Tom Woods | Principia Scientific | September 3, 2021
Ask the average person in whatever country you choose what his chances of hospitalization with or death from COVID are and the answers will shock you. Nearly everyone you speak to is completely uninformed.
Naturally it is impossible to make rational decisions amidst this degree of ignorance.
Now is as good a time as any for some perspective.
The survival rate for people in the 0-19 age group is 99.997 percent. For 20-29 it’s 99.986 percent. You can find all the figures in the graphic below.
The data come from a recent paper by Stanford’s Cathrine Axfors and John Ioannidis, “Infection fatality rate of COVID-19 in community-dwelling populations with emphasis on the elderly: An overview.” Here’s how it breaks down:

A person under 50 is therefore at greater risk of death from drowning, choking on food, sunstroke, or from a sharp object.
This is not to say that we’re not dealing with a nasty virus for some people who contract it. But do you think the average person has any idea that the numbers for survival are this high?
In the UK, the Daily Mail just published an article called, “Is it time to stop obsessing over Covid figures? Statistics reveal virus is NOT the biggest killer — with heart disease, dementia and cancer each claiming four times as many lives in an average week last month.”
“Even before the rollout of the vaccine,” the article notes, “fewer than one per cent of people who caught Covid died. Now, scientists say that figure is ten times smaller.”
They included this graphic, for perspective:

Much as I welcome this, it’s pretty rich for the British press (or indeed any press) to publish an article and a chart like that, though, scratching their heads as to why people are obsessed about COVID, when they themselves are directly responsible for the misinformation that brought about that obsession.
Remember when the Washington Post called Iowa the “state that doesn’t care if you live or die” when that state removed its COVID restrictions? That was seven months ago.
Here’s the chart. Think we’re going to hear any apologies, or any “gee, I guess I don’t understand this virus as well as I thought,” or…?

That’s enough perspective for one day.
No Animal Studies for the Vaccines
By Martin Armstrong | ArmstrongEconomics | September 2, 2021
I find it extremely unbelievable that nobody will investigate this entire scam for what it is. The people behind the vaccines should be dragged in to testify what is going on. Moderna has admitted it took them only 2 days to create the vaccine. In Texas, they are trying to launch a criminal investigation. The FDA is no longer trustworthy, for the normal time to get anything approved is 12 years. What has been released in less than one year with no animal studies? There has been NO TESTING to determine side effects on pregnancy, fertility, or lactation.
It is just stunning that we have politicians REFUSING to look at anything, probably because they are too busy counting their bribes. The White House said under NO condition would they ever fire Fauci, meaning under NO condition will they investigate anyone.
Meanwhile, even the notorious corrupt Snopes had to admit this is TRUE. Despite demanding everyone gets vaccinated, the White House said its own staff DOES NOT need to be vaccinated provided they are routinely checked. So why is the White House the entire exception? Even the military is demanding 100% compliance. Meanwhile, the White House has demanded everyone else receive vaccinations or lose their job.
The fact that they have skipped animal trials is very disturbing. When the government is part of the conspiracy against the public, we will NEVER know the truth about anything. Jack Dorsey has been especially protective of the narrative. Nobody is allowed to question the government no matter what.

Then there are studies revealing that natural immunity to COVID is 13 times better than the vaccines. They try to bury such studies, and they also try to ensure that they are not peer-reviewed in order to discredit them. The Science journalist Alex Berenson was permanently suspended from Twitter one day after his tweets that reported an Israeli study that making this finding that natural immunity from a prior Covid-19 infection is 13 times more effective than vaccines against the delta variant. Twitter is now acting against the very basis of free speech, which is threatening people’s lives. I would love to see Twitter taken down, for they are clearly now responsible for the deaths of many people from vaccine injuries.

To show that this is one giant cover-up, OSHA has instructed employers NOT TO REPORT vaccine injuries suffered by employees if they only “recommend” the shots. Many employers with more than 10 employees are required to keep a record of serious work-related injuries and illnesses. Nobody should volunteer to be vaccinated to satisfy an employer, for you will not be covered for any injury or loss of pay, and you could be fired for not showing up to work for a period of time. However, if employers mandate vaccines to work, then the vaccine injuries should become subject to reporting, lawsuits, and workman’s comp claims.
Ivermectin Metaanalysis
By Meryl Nass, MD | September 3, 2021
Tess Lawrie’s group’s metaanalysis of ivermectin research papers, published in June, has received a great deal of positive attention. It was, as expected, carefully done. The authors graded the quality of the papers they reviewed.
The abstract noted:
“Therapeutic Advances: Meta-analysis of 15 trials found that ivermectin reduced risk of death compared with no ivermectin (average risk ratio 0.38, 95% confidence interval 0.19–0.73; n 5 2438; I2 5 49%; moderate-certainty evidence)…” This means that using only evidence of moderately good quality (high quality is often hard to come by, especially using observational data), if 100 people sick enough with Covid to die are given ivermectin, only 38 will die, and 62% will be saved.
“Low-certainty evidence found that ivermectin prophylaxis reduced COVID-19 infection by an average 86% (95% confidence interval 79%–91%).”
More doctors are using the drug. More patients are hearing about it. I have been getting more calls from patients who want to know about it. The NY Times said pharmacists are filling 88,000 scripts a week now.
Covid death rates, compared to the number of cases diagnosed, are way down compared to 2020 and last winter. While the NYT says there are 100,000 Covid patients in hospital now, only 1,500 are dying daily, or 1.5%, a much lower percentage than previous waves.
This is probably due to lower virulence of current variants, some benefit from vaccination, less use of ventilators and more use fo effective therapeutics.
And so now the CDC is coming down hard and many pharmacist have decided to stop filling the scripts in the past week. More on this in my next post.
Top Misinformation Article Attributed to Chicago Tribune
By Dr. Joseph Mercola | September 2, 2021
According to Facebook’s content transparency report for the first quarter of 2021, released in mid-August 2021, the most popular article shared on the platform between January 2021 and March 2021 was about a 56-year-old Miami, Florida, obstetrician who died two weeks after his first Pfizer injection.1
The story initially ran in the South Florida Sun Sentinel 2 April 8, 2021, and was republished by the Chicago Tribune that same day.3 The doctor, Dr. Gregory Michael, received his first dose December 18, 2020.
Three days later, he developed small spots on his hands and feet, which prompted him to go to the emergency room, where they found he had an abnormally low blood count. Platelets stop bleeding by clotting, and when platelets drop too low, internal bleeding can occur, resulting in what looks like blood blisters on the skin.
Michael remained in intensive care for two weeks, but no matter what they did, his platelet count refused to budge. During the night of January 3, 2021, he died of a massive stroke. According to the coroner, the COVID injection could not be ruled out as a contributing or causative factor.
In a Facebook post, Michael’s widow stated he’d been “very healthy” and that he’d been a COVID-19 vaccine advocate. His death caused her to question the safety of the shot, however.
“I believe that people should be aware that side effects can happen, that the vaccine is not good for everyone and in this case destroyed a beautiful life, a perfect family and has affected so many people in this community.” she wrote. “Please do not let his death be in vain please save more lives my making this information news.”4
Even Viral Content Has Minor Reach
According to The New York Times,5 Facebook held off on publishing the first-quarter report for fear the findings might “look bad for the company.” Executives decided they wanted to make some “key fixes to the system” before releasing it. That’s why it wasn’t published until August.
Interestingly, the report reveals that even when something goes viral, the total number of views is still a tiny fraction of the overall content. Even the biggest accounts make up but a small portion of overall content views. Combined, the top 20 accounts with the most views during the first quarter — which included UNICEF, The Dodo and LADbible — accounted for only 1.18% of all U.S. content views.
As noted in the report, this “shows that, even though it may seem like a page or post has extensive reach on the platform, that isn’t the case when measured against the total amount of content available on the platform.”
Facebook Calls Out CCDH for Manufacturing ‘Faulty Narrative’
As you may know, an obscure one-man organization funded by dark money called the Center for Countering Digital Hate (CCDH) has published several reports, including “The Anti-Vaxx Playbook,”6 “The Disinformation Dozen”7 and “Disinformation Dozen: The Sequel,”8 in which the founder, Imran Ahmed — an unregistered foreign agent — claims to have identified the top most influential “anti-vaxxers” in the U.S.
In a completely unexpected turn of events, Facebook is now calling out the CCDH for having manufactured a faulty narrative without evidence against the 12 individuals targeted in its reports (myself included).9
This is important, seeing how the CCDH reports have been the primary “reference” source of authority used by media and government officials to smear, threaten and infringe on American citizens’ right to free speech.
The U.S. Department of Homeland Security even lists promulgating “false narratives” around COVID-19 as a top national security threat, which basically puts a “domestic terrorist” target on the backs of those of us who have been identified by the CCDH as the most prolific “superspreaders” of COVID misinformation.
As reported by GreenMed Info :10
“Google now shows an astounding 84,700 search results for CCDH’s defamatory phrase ‘disinformation dozen. ’Amazingly, this includes 16,000 news stories within the international press, approximately 100% of which are word-for-word amplifications of CCDH’s claims/defamatory statements and reported uncritically as fact.
In addition, the Surgeon General Vivek Murthy, the White House Press Secretary Jen Psaki, and president Biden all used CCDH’s report as the sole source for their own defamatory accusations, reaching a dangerous rhetorical climax on July 20th when Biden stated that these 12 individuals are literally “killing people” [by spreading misinformation].”
No Evidence to Support ‘Misinfo Superspreader’ Claim
In an August 18, 2021, Facebook report, Monika Bickert, vice president of Facebook content policy, sets the record straight, and in the process, demolishes the CCDH’s claims:11
“In recent weeks, there has been a debate about whether the global problem of COVID-19 vaccine misinformation can be solved simply by removing 12 people from social media platforms. People who have advanced this narrative contend that these 12 people are responsible for 73% of online vaccine misinformation on Facebook. There isn’t any evidence to support this claim …
That said, any amount of COVID-19 vaccine misinformation that violates our policies is too much by our standards — and we have removed over three dozen Pages, groups and Facebook or Instagram accounts linked to these 12 people, including at least one linked to each of the 12 people, for violating our policies.
We have also imposed penalties on nearly two dozen additional Pages, groups or accounts linked to these 12 people, like moving their posts lower in News Feed so fewer people see them or not recommending them to others. We’ve applied penalties to some of their website domains as well so any posts including their website content are moved lower in News Feed.
The remaining accounts associated with these individuals are not posting content that breaks our rules, have only posted a small amount of violating content, which we’ve removed, or are simply inactive.
In fact, these 12 people are responsible for about just 0.05% of all views of vaccine-related content on Facebook. This includes all vaccine-related posts they’ve shared, whether true or false, as well as URLs associated with these people.”
It’s worth restating the key point in this quote: Combined, the top 12 individuals and organizations identified by the CCDH as being responsible for a whopping 73% of vaccine misinformation on Facebook, are in fact only responsible for 0.05% of vaccine-related content — 1,460 times lower than the CCDH’s outrageous claim. That’s no small discrepancy.
CCDH Claims Blasted as Unjustified and Biased
Bickert goes on to refer directly to the CCDH report “The Disinformation Dozen,”12 stating:
“The report13 upon which the faulty narrative is based analyzed only a narrow set of 483 pieces of content over six weeks from only 30 groups, some of which are as small as 2,500 users.
They are in no way representative of the hundreds of millions of posts that people have shared about COVID-19 vaccines in the past months on Facebook.
Further, there is no explanation for how the organization behind the report identified the content they describe as ‘anti-vax’ or how they chose the 30 groups they included in their analysis. There is no justification for their claim that their data constitute a ‘representative sample’ of the content shared across our apps.”
CCDH Meets Definition of ‘Hateful Extremists’
Ironically, while the CCDH claims to “counter hate” online, and Ahmed sits on the Steering Committee of the U.K. Commission on Countering Extremism, CCDH itself actually meets the Commission’s definition of hateful extremists.14 In the 2019 Commission document, “Challenging Hateful Extremism,” the term is defined as:15
“Behaviours that can incite and amplify hate, or engage in persistent hatred, or equivocate about and make the moral case for violence; And that draw on hateful, hostile or supremacist beliefs directed at an out-group who are perceived as a threat to the wellbeing, survival or success of an in-group; And that cause, or are likely to cause, harm to individuals, communities or wider society.”
In addition, in the forward of the report, lead commissioner Sara Khan notes that “Hateful extremists seek to restrict individual liberties and curtail the fundamental freedoms that define our country.”
All of these definitions and clarifications of what hateful extremism is fit the CCDH to a T. Ahmed manufactured data to create a false narrative that 12 individuals pose a threat to the well-being and survival of the whole world, and then used that narrative to incite hate against us and curtail our freedom of speech.
Who Fact Checks the Fact Checkers?
In related news, the self-appointed arbiter of factual truths, NewsGuard, has had to backpedal in recent months and issue dozens of corrections to “fact checks” in which they’ve labeled the Wuhan lab leak theory as a debunked conspiracy theory with no basis in fact.
Since the beginning of the COVID pandemic, NewsGuard has wrongly down-rated 225 websites for articles mentioning the lab leak theory.16 In reality, there’s far more evidence to support the lab leak theory than any other theory, but it took over a year before the weight of this evidence became too obvious for the media to ignore.
NewsGuard’s erroneous fact checks were recently highlighted in an August 11, 2021, report by the American Institute for Economic Research (AIER).17
AIER decided to take a closer look at NewsGuard after receiving a request for comments on a NewsGuard fact check article regarding AIER and the Great Barrington Declaration — a statement written by public health experts from Harvard, Stanford and Oxford that calls on government to implement focused protection rather than lockdowns and self-isolation. AIERS investigation found that:18
“… NewsGuard falls far short of the very same criteria for accuracy and transparency that it claims to apply to other websites. Most of the company’s fact checkers lack basic qualifications in the scientific and social-scientific fields that they purport to arbitrate.
NewsGuard’s own track record of commentary — particularly on the Covid-19 pandemic — reveals a pattern of unreliable and misleading claims that required subsequent corrections, and analysis that regularly conflates fact with opinion journalism in rendering a judgement on a website’s content.
Furthermore, the company’s own practices fall far short of the transparency and disclosure standards it regularly applies to other websites … NewsGuard’s staff primarily evaluates scientific claims by appealing to the authority of public figures who they designate as ‘experts’ on the subject in question.
Their approach generally avoids direct examination of the evidence surrounding contested claims, and instead cherry-picks a figure to treat as an authoritative final word … many of their preferred authorities are political officeholders rather than persons trained in scientific or social-scientific methods.
By selectively curating cherry-picked political authorities rather than evaluating evidence directly, NewsGuard’s approach to fact-checking effectively sidesteps the scientific method. This strategy is rendered even more problematic by the general lack of scientific expertise within NewsGuard’s team of writers.
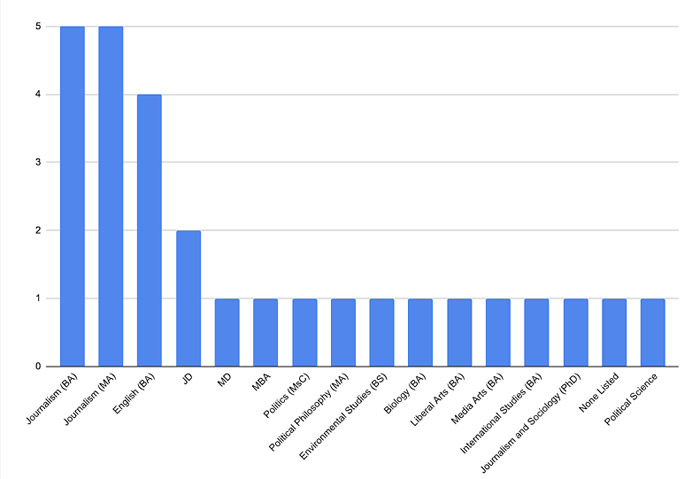
We examined the educational credentials, including the highest degree listed, for 28 publicly identified staff members on NewsGuard’s website. The company’s staff page reveals shockingly little expertise in either the hard sciences such as medicine or social sciences such as public policy, economics, and related fields …
Most NewsGuard articles on Covid-19 topics and policies are written by [NewsGuard Deputy Editor for Health, John] Gregory, whose only identified qualification is a bachelor’s degree in Media Arts … Gregory would not qualify as an expert in most of the fields he is responsible for fact-checking …
Of course, non-experts have every right to offer opinions on scientific and social-scientific matters. Whether or not they should be taken seriously as fact checkers or act as arbiters of scientific disputes is another question entirely.”
NewsGuard Staff by Field and Highest Degree Attained
NewsGuard Apologizes for Erroneous Fact Checks
After being confronted about its erroneous fact checks on the lab leak theory, NewsGuard offered the following apology in a statement sent to AIER:19
“NewsGuard either mischaracterized the sites’ claims about the lab leak theory, referred to the lab leak as a ‘conspiracy theory,’ or wrongly grouped together unproven claims about the lab leak with the separate, false claim that the COVID-19 virus was man-made without explaining that one claim was unsubstantiated, and the other was false.
NewsGuard apologizes for these errors. We have made the appropriate correction on each of the 21 labels.”
AIER commented on the apology:20
“Gregory and his colleagues appear to have simply decided that their own premature dismissal of the lab leak hypothesis equated to ‘fact’ and proceeded to penalize other sites not for factual errors, but rather for diverging from NewsGuard’s own editorial position on the same subject.
When this position turned out to be mistaken, NewsGuard pivoted to remove the errors — albeit in non-transparent ways that downplay the significance or pervasiveness of their mistake.”
NewsGuard Fails to Fulfill Its Own Credibility Criteria
In their report, AIER goes on to apply the criteria NewsGuard uses to evaluate a website’s credibility to NewsGuard itself. It’s ranking? A paltry 36.25 out of 100. According to AIER:21
“This website fails to adhere to several basic journalistic standards, and should be used with extreme caution as a source for verifying the reliability of the websites it purports to rate …
When we see fact checkers like NewsGuard, who not only fail to uphold their high-sounding principles but even publicly encourage working with the government to suppress speech, we should raise red flags.”
The NewsGuard ratings are meant to influence the reader, instructing them to disregard content with cautionary colors and cautions. That it would serve as the thought police of the technocratic establishment that seeks to silence dissent and bury information that doesn’t help move the Great Reset agenda forward is no surprise.
Especially considering its primary startup capital came from Publicis Groupe,22 a PR group that represents most of Big Pharma, including vaccine makers, and Big Tech. NewsGuard is also backed by Microsoft23 and Google.
The Publicis Groupe has been manipulating what people think about commercial products for nearly a century. Over that century, this advertising and communications firm bought or partnered with targeted advertising avenues, beginning with newspapers, followed by radio, TV, cinema and the internet.
With revenue avenues secured, Publicis’ clients and partners built a global presence that dominated the advertising world. Be it tobacco or sugar, Publicis Groupe found a way to promote and strengthen big industries. Publicis was recently sued24 for its deadly and illegal marketing of Purdue Pharma’s opioid products.
When you consider that Publicis describes its business model approach as putting clients and their needs and objectives at the center of all they do so their clients can “win and grow,” it’s easy to see what’s driving NewsGuard.
Overall, NewsGuard is just another big business aimed at keeping the chemical, drug and food industries, as well as mainstream media, intact by discrediting and eliminating unwanted competitors and analysts who empower you with information that runs counter to any given industry’s agenda.
If you’re as disturbed by censorship as I am, be sure to contact your local library today to find out if they’re one of the more than 700 libraries using NewsGuard. If they are, then ask them if they’re aware of NewsGuard’s censorship of truthful news that is now encroaching on scientific freedom and threatening the very roots of our democracy.
If your local library is using NewsGuard, it would be helpful to start a campaign to get it removed. Contact your neighbors and let them know what is happening so they can kick out this public health threat. Likewise, whenever you see someone referencing reports by the CCDH, call them out on it.
Sources and References
- 1 USA Today August 23, 2021
- 2 Sun Sentinel April 8, 2021
- 3 Facebook Heidi Neckelmann
- 4 Chicago Tribune April 8, 2021
- 5 New York Times August 20, 2021 (Archived)
- 6 The Anti-Vaxx Playbook (PDF)
- 7, 12, 13 CCDH, The Disinformation Dozen
- 8 Misinformation Dozen: The Sequel
- 9, 11 Facebook August 18, 2021
- 10 GreenMed Info August 19, 2021
- 14 Greenmed Info March 25, 2021
- 15 Challenging Hateful Extremism 2019
- 16, 17, 18, 19, 20, 21 AIER August 11, 2021
- 22 Washington Post March 3, 2018
- 23 axios.com August 23, 2018, NewsGuard Launches First Product With Help From Microsoft
- 24 Reuters May 6, 2021
Named, shamed and fined – the maskless marauders

By Frederick Edward | TCW Defending Freedom | September 2, 2021
MAGISTRATES have been busy enforcing the laws of Covid-land, with more than 20 miscreants in Northamptonshire fined last week for failing to abide by the rules. They are named and shamed in the Northamptonshire Telegraph, the digital equivalent of the village stocks.
There are a few things to glean from the list of those convicted. We have a small insight, firstly, into the demographic shifts that are happening in the small towns of England such as Corby, Kettering and Wellingborough, with M Jatczak, K Marjani and P Blaga making an appearance.
The relative youth of those who found themselves in court is telling. J Ayre, 22, went to an outdoor gathering of more than two souls, for which he must pay £248. C Hulse, also 22, went to an indoor gathering of more than two. She has to pay £344.
While we do not know the circumstances of these individuals, it is a reminder of the price the youth have been made to pay throughout the last 18 months or so. Stuck in small accommodation or at home with their parents, they have suffered a disproportionate impact from restriction on movement. Moreover, the fines are not insignificant for those unlikely to have much disposable income.
Those caught refusing to abide by Covid regulations include:
U Aurica, 51, fined £344 for being in a corner shop without a mask;
C Oxlade, 21, found maskless in Budgens, as was E McIlreavy, 29, at Asda. Both fined £344;
L Stachura, 29, fined £344 for not wearing a face mask in a pizza takeaway.
R Gilderleft, 26, ‘left his home . . . without reasonable excuse’. He must pay £344.
The local paper website does not make it clear, but the prosecutions are likely to have been under the Coronavirus Act and Health Protection Regulations. Both pieces of legislation were passed in March 2020, the former without a vote in the Commons and the latter presented to the House only after it had come into force.
This is just a snapshot of cases involving Covid-19 rules. The Crown Prosecution Service reported in May 2021 – more than one year into the pandemic – that more than 1,800 had been brought to court, though a high proportion were subsequently identified as incorrectly charged. Indeed, between March 2020 and March 2021, all charges brought under the Coronavirus Act were incorrect, with not a single prosecution resulting from this large expenditure of police and court time.
Around 80 per cent of prosecutions brought under the Health Protection (Coronavirus, Restrictions) Regulations were correctly charged: it is under this legislation, which includes restrictions on leaving home, social gatherings and the enforcement of mask-wearing, that our Northamptonshire rebels were probably charged.
That a man living in England can be sentenced for leaving his own home is a sign of how far down the path of illiberalism we have strayed: never before in our history have we accepted such perverse rules, a fact made all the more unconscionable by their disproportionality.
What concerns me doubly is that they are enforced with such officiousness and subsequently reported so eagerly by an unquestioning and uncritical press. The Northamptonshire Telegraph says sanctimoniously: ‘The defendants were the latest to be convicted after violating emergency rules – which were designed to slow the spread of coronavirus – between January and April. Many of them were punished after failing to stick to the laws in January or February, at a time when many thousands died as the virus spiraled [sic] out of control.’
In any society which abandons the precepts of freedom, there will be a large group of people who willingly become the enforcers of the new regime. Intoxicated with power, they thrive amid a sea of petty regulations.
Naturally, one will not find names such as Matt Hancock of Neil Ferguson on the lists of those convicted. While the man on the street has the book thrown at him for daring to venture into a supermarket without a mask or seeing some friends, those in the right places and with the right connections can carry out their assignations without repercussion.
We can be convicted and fined for going to a takeaway without a mask, while our elites philander and jet around the world.
How much longer will we tolerate these glaring double standards?
Featured Video

BEN-GVIR: “ALL OF LEBANON MUST BURN” — w/ Mouin Rabbani
or go to
Aletho News Archives – Video-Images
From the Archives
UK Researchers: Tax Food to Reduce Climate Change

I doubt these professors have anything to fear from a food tax
By Eric Worrall | Watts Up With That? | November 19, 2016
A group of researchers in Oxford University, England have suggested that imposing a massive tax on carbon intensive foods – specifically protein rich foods like meat and dairy – could help combat climate change. […]
This proposal, from a group of people who have probably never missed a meal in their lives, is totally obscene. High income countries often have a lot of poor people who would be hard hit by increases in the price of food.
Needlessly exacerbating the risk poor people don’t get enough to eat, especially children and pregnant mothers, who are especially vulnerable to adverse health impacts from lack of protein in their diet – if this ghastly proposal is ever implemented, future generations will look upon it as a crime against humanity. – Read full article
Blog Roll
 Aletho News
Aletho News- The West’s Post-Soviet ‘Democracy’ Playbook
- UK suppressed intel on Sudan genocide to protect UAE ties: Report
- Starmer’s exit exposes dirty secret: UK can’t afford Ukraine War
- Putin Warns the West: Russia Is Ready
- BEN-GVIR: “ALL OF LEBANON MUST BURN” — w/ Mouin Rabbani
- There Are No Budget Constraints In New York City: “Coastal Resiliency” Edition
- The UN’s plan to levy taxes on global trade is a sinister power grab
- Is there a future for the U.S. strategy in the Arctic?
- UN inquiry finds Israel ‘intentionally’ targeting Palestinian children in Gaza, occupied West Bank
- Citizens Around the World Demand Israel’s Expulsion From the United Nations
- If Americans Knew
- ‘His only crime is that he is a Palestinian doctor’
- ‘Killed pursuing her dream’: Gaza girl on her way to school dies in Israeli drone strike
- Unbelievable pressure on Gaza from Israel, “Board of Peace” – Daily Update
- UN: Israel Continues to Commit Genocide and Other Atrocity Crimes by Deliberately Targeting Palestinian Children
- Bari Weiss, Free-Speech Fraud & Zionism Promoter, Would Rather Deport Than Debate
- ‘Doctor of the Poor’: Israeli Occupation Arrests Prominent Palestinian Physician
- Search for Your Church (and see if it has been targeted by the Israeli gov’t)
- Mark Levin Flying to Israel as Netanyahu Reportedly Seeks to ‘Leverage’ Levin to Trash Trump’s Iran Deal
- Watch: Zionist Brags about Israel’s Power to Get the World to Do What Israel Wants
- In Gaza, another senseless death on what should have been a joyous day – Daily Update
- No Tricks Zone
- 3 New Studies Find Increasing Trends In Solar Radiation Since The 1980s – Easily Explaining Warming
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
