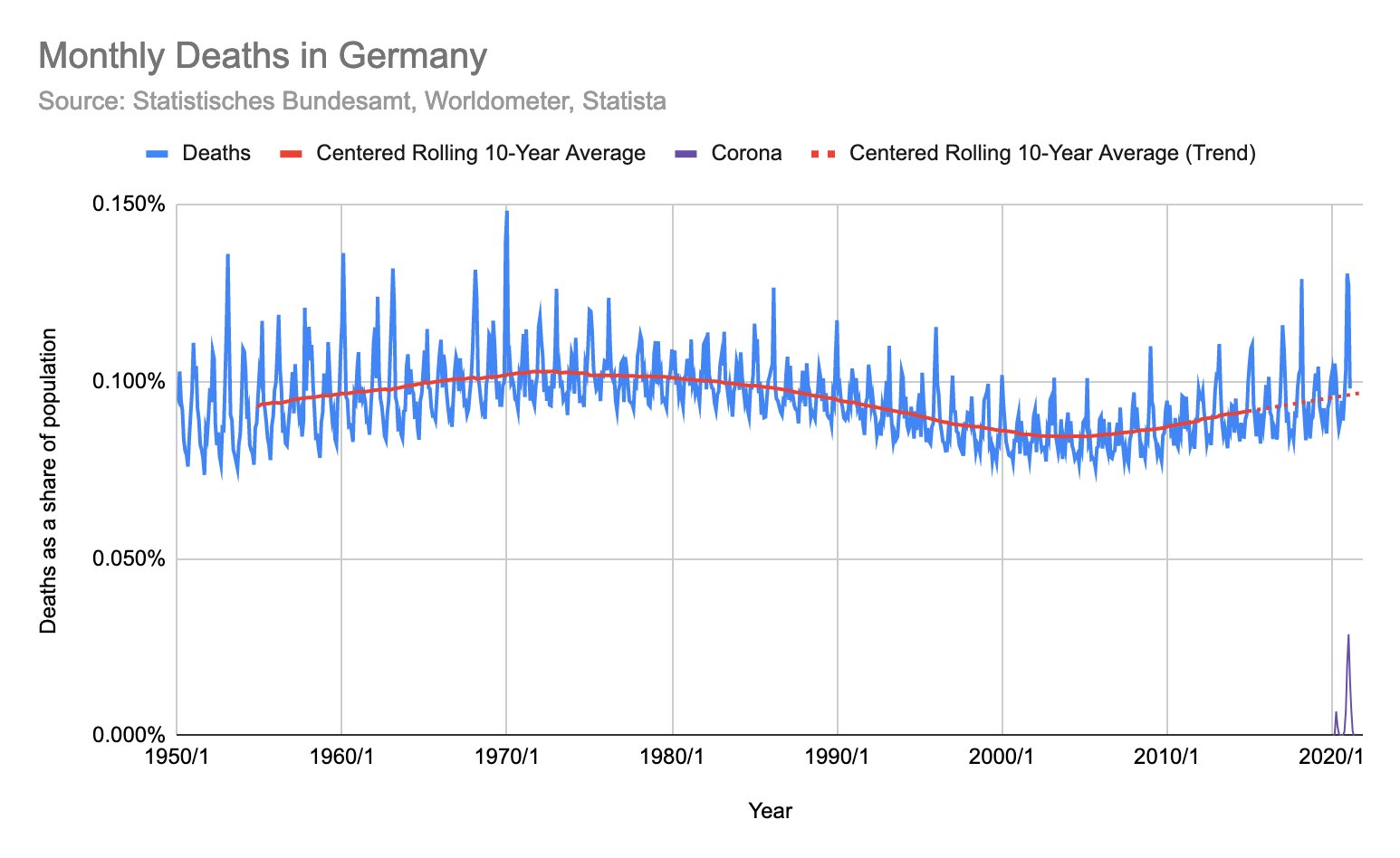
German Omicron Data
el gato malo – bad cattitude – december 31, 2021
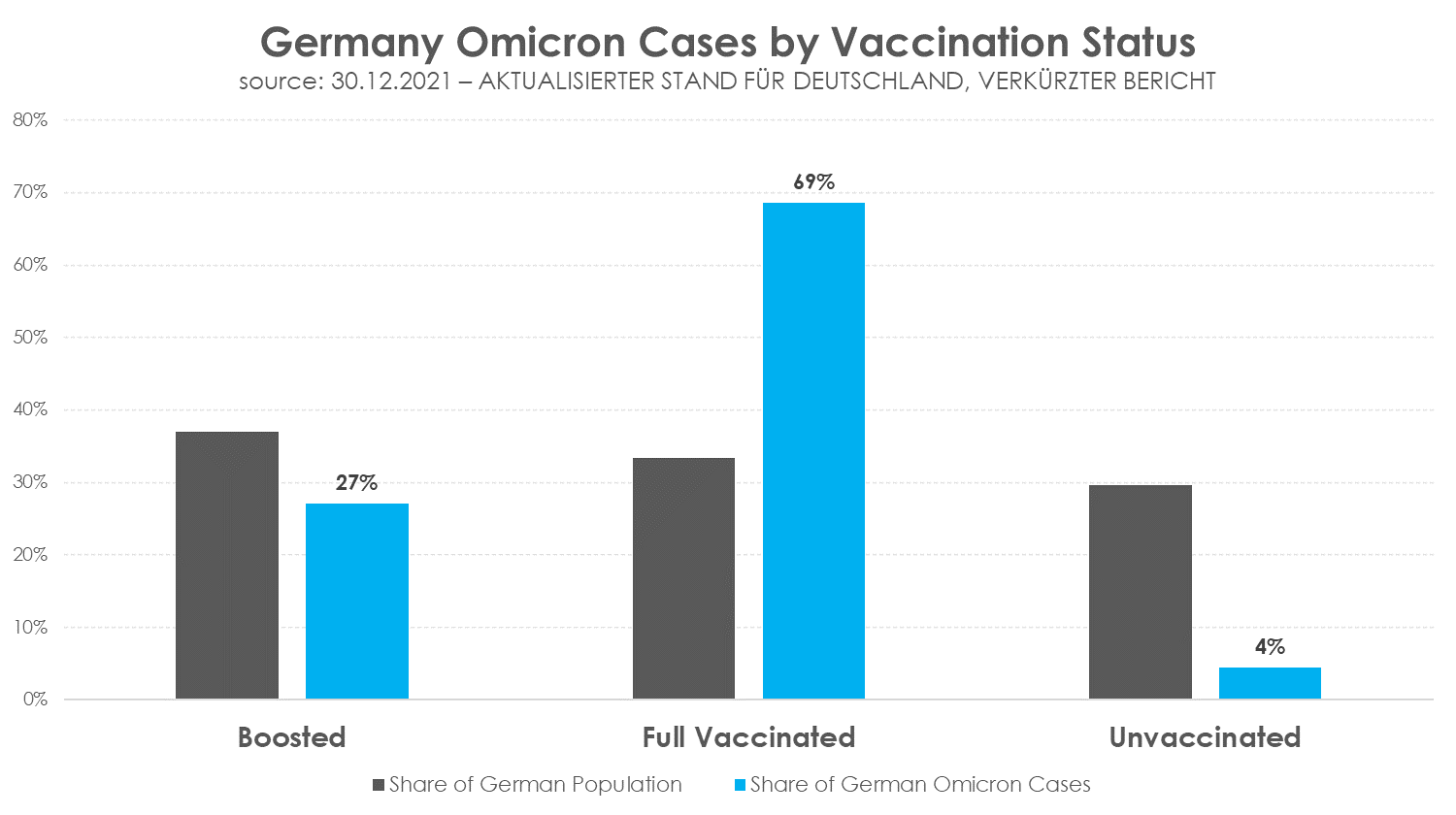
this data recently emerged from the robert koch institute in germany.
(no, this has nothing to do with the american koch brothers. it’s a common name and this is a quasi-government health agency.)
data such as this is easy to misinterpret and nearly everyone is doing it incorrectly, so i’d like to walk through why, counter to what many are claiming, this data actually shows that boosters have negative VE (vaccine efficacy).
caveat: this is a small and likely incomplete societal dataset. the sample size is possibly large enough to give us a sense of outcomes, but as with all societal data, it’s difficult to know what bias may be injected by self selection for testing and for vaccination. error bars are likely meaningful.
but we work with what we have, not what we would prefer, so let’s take a look:
this is the summarized raw data:
– 4020, ergo 95,58 % vollständig Geimpfte (1137 davon geboostert) – 186 Ungeimpfte (4,42 %)
4020 cases with 2 or more doses of vaccine, 1137 of them with boosters.
186 cases in the unvaccinated.
(unfortunately, there is no breakout for 1 dose only, so i’m presuming that group has been included in “unvaccinated”)
germany is 70.5% “full vaccinated.” (per OWID) thus, by the definitions this report uses, it is 29.5% unvaccinated.
it is 38.2% boosted as of 12/30/21. it’s not clear to me if this study is using that figure or only counting as boosted those who got their booster more than 14 days ago (as many seem to count it). if this is so, the number drops to 29.3%. i will look at it both ways to try to create some bookends for the range. (if anyone can clarify, i’d be grateful)
to see what is happening more granularly, we first need to regroup the terms:

from this one can see that the 3 groups are actually fairly similar in size, but quite divergent in outcomes.
many seem to presume that because cases in the boosted are a lower percentage of overall cases than the boosted are of the overall population that this shows vaccine efficacy.
this is not, however, correct as can be readily seen once we adjust this data to a per capita level.
that data looks like this (using 83.2mm for german population)
and this makes the issue obvious.

to calculate VE, we need to compare the vaccinated cohorts to the unvaccinated. that’s the control group. there are probably some pretty significant error bars here, but this outcome is STARK. the risk ratios for all vaccinated groups are far, far higher than control.
boosting does seem to lead to a 2/3 risk reduction vs just being double vaxxed but still leaves one at 4.7X the risk of the unvaccinated.

this risk ratio leads to VE figures that are, frankly, so bad that i suspect there must be some sort of bias here. this looks too extreme to be entirely plausible and far exceeds all other data i have seen.

one possible source of this issue is definitional. if the german study is using “boosted +14 days” as its definition, then the numbers change quite a bit as the size of the boosted group shrinks and the size of double vaxxed rises causing their risk rates to converge somewhat.


another possible source of contamination is the actual act of running a booster campaign during an outbreak.
the tendency toward transitory immune suppression created by mRNA vaccine administration is well documented.

the danes found it to be on the order of 40-100% increase in the likelihood of infection in the 2 weeks following administration (with 100% likely being a better proxy for genpop as they resemble HCW’s more than NH residents). this study was during a period of relatively low prevalence and with a less contagious variant than omicron. this needle could have moved quite a lot by now.
and all this piles up, so if you are doubling the risk of a group already showing increased risk due to vaccine escape/antigenic fixation/OAS the issue may become multiplicative. […]
Facts about Covid-19
Swiss Policy Research | Updated: December 2021
Fully referenced facts about covid-19, provided by experts in the field, to help our readers make a realistic risk assessment.
“The only means to fight the plague is honesty.” (Albert Camus, 1947)
Overview
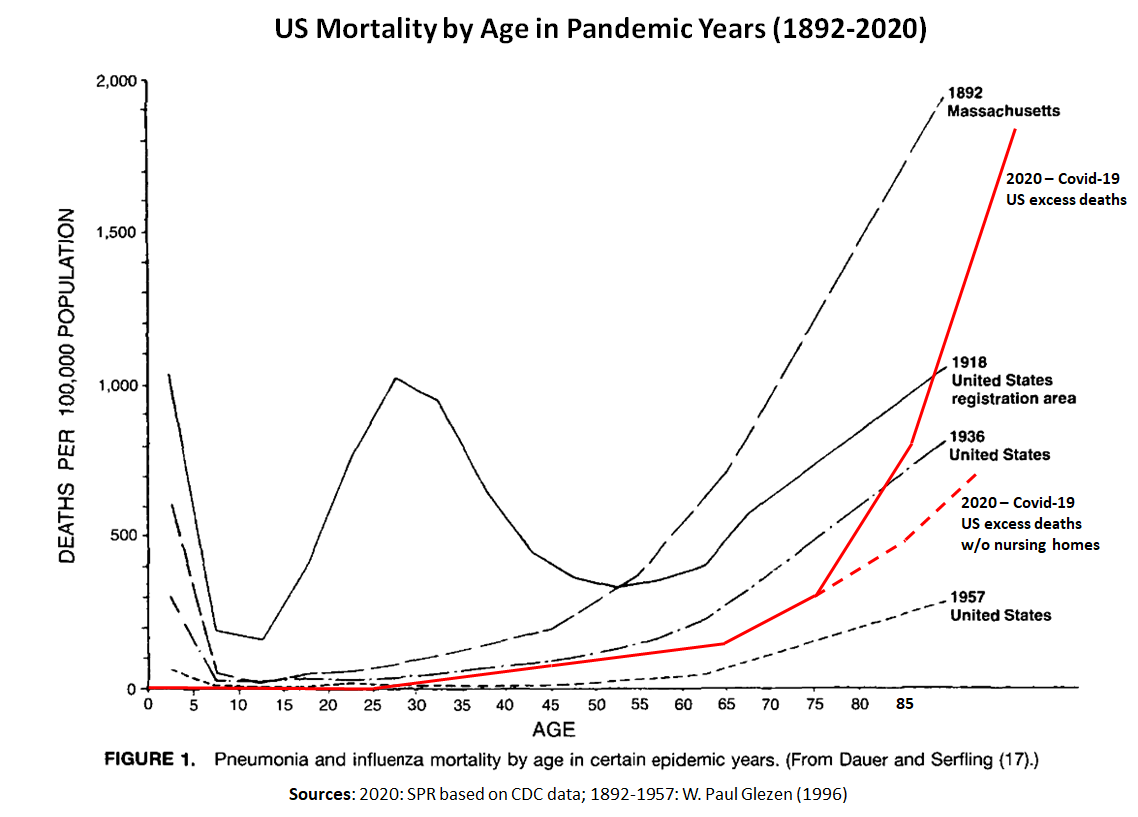
- Lethality: According to the latest immunological studies, the overall infection fatality rate (IFR) of covid in the general population is about 0.1% to 0.5% in most countries, which is most closely comparable to the medium influenza pandemics of 1936, 1957 and 1968.
- Vaccines: Real-world studies have shown a very high, but rapidly declining covid vaccine effectiveness against severe disease. Vaccination cannot prevent infection and transmission. Various severe and fatal vaccine adverse events have been reported, including in young people. A prior infection generally confers superior immunity compared to vaccination.
- Treatment: For people at high risk or high exposure, early or prophylactic treatment is essential to prevent progression of the disease. According to numerous international studies, early outpatient treatment of covid may significantly reduce hospitalizations and deaths.
- Age profile: The median age of covid deaths is over 80 years in most Western countries (78 in the US) and about 5% of the deceased had no serious preconditions. The age and risk profile of covid mortality is therefore comparable to normal mortality, but increases it proportionally.
- Nursing homes: In many Western countries, about 50% of all covid deaths have occurred in nursing homes, which require targeted and humane protection. In some cases, care home residents died not from the coronavirus, but from weeks of stress and isolation.
- Excess mortality: Overall, the pandemic has increased mortality by 5% to 25% in most Western countries. In some countries, up to 30% of additional deaths have been caused not by covid, but by indirect effects of the pandemic and lockdowns (including drug overdose deaths).
- Antibodies: By the end of 2020, between 10% and 30% of the population in most Western countries had coronavirus antibodies. In India and some Latin American countries, coronavirus infection prevalence reached up to 75% by the summer of 2021.
- Symptoms: About 30% of all infected persons show no symptoms. Overall, about 95% of all people develop at most mild or moderate symptoms and do not require hospitalization. Early outpatient treatment may significantly reduce hospitalizations.
- Long covid: Up to 10% of symptomatic people experience post-acute or long covid, i.e. covid-related symptoms that last several weeks or months. Long covid may also affect younger and previously healthy people whose initial course of disease was rather mild.
- Transmission: Indoor aerosols appear to be the main route of transmission of the coronavirus, while outdoor aerosols, droplets, as well as most object surfaces appear to play a minor role. The coronavirus season in the northern hemisphere usually lasts from November to April.
- Masks: There is still little to no scientific evidence for the effectiveness of face masks in the general population, and the introduction of mandatory masks couldn’t contain or slow the epidemic in most countries. If used improperly, masks may increase the risk of infection.
- Children and schools: In contrast to influenza, the risk of disease and transmission in children is rather low in the case of covid. There was and is therefore no medical reason for the closure of elementary schools or other measures specifically aimed at children.
- Contact tracing: A WHO study of 2019 on measures against influenza pandemics concluded that from a medical perspective, contact tracing is “not recommended in any circumstances”. Contact tracing apps on cell phones have also proven ineffective in most countries.
- PCR tests: The highly sensitive PCR test kits may in some cases produce false positive or false negative results or react to non-infectious virus fragments from a previous infection. In this regard, the so-called cycle threshold or ct value is an important parameter.
- Virus mutations: Similar to influenza viruses, mutations occur frequently in coronaviruses. Most of these mutations are insignificant, but some of them may increase the transmissibility, virulence or immune evasion of the virus to some extent.
- Lockdowns: In contrast to early border controls, lockdowns have had no significant effect on the pandemic. According to the UN, lockdowns may put the livelihood of 1.6 billion people at acute risk and may push an additional 150 million children into poverty.
- Sweden: In Sweden, covid mortality without lockdown has been comparable to a strong influenza season and somewhat below the EU average. About 50% of Swedish deaths occurred in nursing homes and the median age of Swedish covid deaths was about 84 years.
- Media: The reporting of many media has been unprofessional, has increased fear and panic in the population and has led to a hundredfold overestimation of the lethality of the coronavirus. Some media even used manipulative pictures and videos to dramatize the situation.
- Virus origin: The origin of the new coronavirus remains unknown, but the best evidence currently points to a covid-like pneumonia incident in a Chinese mine in 2012, whose virus samples were collected, stored and researched by the Wuhan Institute of Virology (WIV). Due to cooperations, some US labs may also have had access to these viruses.
- Surveillance: NSA whistleblower Edward Snowden warned that the coronavirus pandemic may be used to expand global surveillance. Many governments have restricted fundamental rights of their citizens and announced plans to introduce digital biometric vaccine passports.
Overview diagrams






Latest updates
Basics
General
- The Covid Vaccine War (December 2021)
- The Return of the Flu (November 2021)
- The WEF and the Pandemic (October 2021)
- Global Covid Mortality (September 2021)
- Variants: What’s next? (July 2021)
- Obesity and the pandemic (June 2021)
- The failure of PCR mass testing (June 2021)
- Pre-symptomatic transmission (June 2021)
- Covid versus the flu, revisited (March 2021)
- Lockdowns in China in 2021 (February 2021)
- Why Covid-19 is a “strange pandemic” (Sept. 2020)
Vaccines
- Covid Vaccines: A Reality Check (December 2021)
- Covid vaccine adverse events (December 2021)
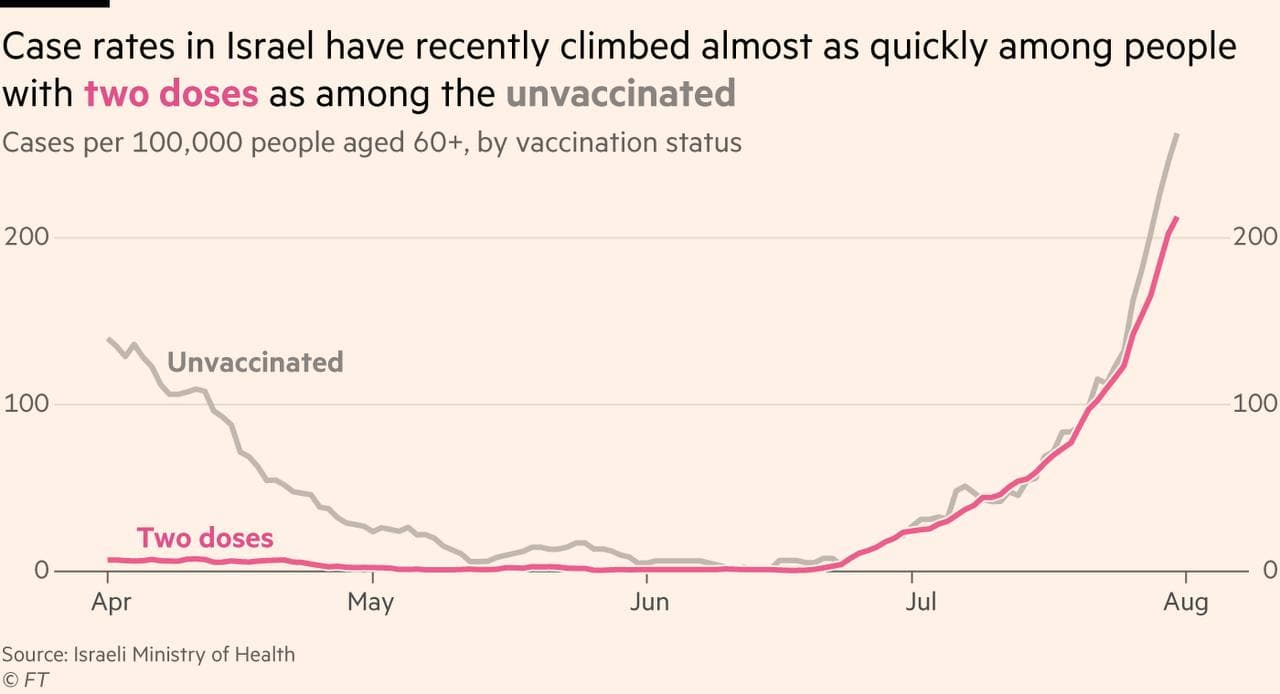
- Israel: Highest infection rate in the world (Sept. 2021)
- Israel: Why is all-cause mortality increasing? (April 2021)
- Videos: Vaccines: Successes and Controversies (Dec. 2020)
Early Treatment
- The Ivermectin Debate (July 2021)
- Covid and anti-androgens (July 2021)
- Molnupiravir: Caution (October 2021)
- Severe covid: An autoimmune attack (July 2021)
- Is budesonide really effective against covid? (April 2021)
- Remdesivir: An Epidemic Failure (October 2020)
Face masks
- The Mask Folly in Retrospect (August 2021)
- Danish Mask Study: No Benefit (November 2020)
- WHO Mask Study Seriously Flawed (September 2020)
Other topics
- Judgment day: Sweden vindicated (Dec. 2021)
- Omicron Hits the Mutation Jackpot (Nov. 2021)
- Meanwhile in Australia (June 2021)
- The Censorship Pandemic (May 2021)
- On the “people collapsing in Wuhan” (April 2021)
- Lockdowns: Fewer Suicides in 2020? (April 2021)
12 inconvenient predictions about “Covid-19 vaccines”

December 31, 2021 |
One Year Ago | Today |
| 1. The vaccinated can contaminate others | Conspiracy Theory | TRUE |
| 2. The vaccinated can get infected | Conspiracy Theory | TRUE |
| 3. The vaccines can cause adverse reactions | Conspiracy Theory | TRUE |
| 4. Third and fourth doses | Conspiracy Theory | TRUE |
| 5. A new shot every 6 months | Conspiracy Theory | TRUE |
| 6. Vaccination for little children | Conspiracy Theory | TRUE |
| 7. Lockdown for the unvaccinated | Conspiracy Theory | TRUE |
| 8. Difficulty for the unvaccinated to work | Conspiracy Theory | TRUE |
| 9. Classified contracts between Pfizer and governments | Conspiracy Theory | TRUE |
| 10. The vaccines don’t stop infection | Conspiracy Theory | TRUE |
| 11. Restrictions even for the vaccinated | Conspiracy Theory | TRUE |
| 12. Proof of vaccination required (“vaccine passports”) | Conspiracy Theory | TRUE |
| Source: https://t.me/PIUSIAMOPRIMANEUSCIAMO (in Italian) | ||
The FDA wants to hide pre-licensure data until you’re dead. Now the CDC wants to hide post-licensure safety data
By Aaron Siri | Injecting Freedom | December 30, 2021
You must take this product. You cannot sue if injured. You can maybe see the clinical trial safety data in 75+ years. And the deidentified post-licensure safety data – no, you cannot see that either.
Three prior posts explained how the FDA seeks to delay for 75+ years full production of Pfizer’s pre-licensure safety data. While we have that fight, we submitted a request to the CDC, on behalf of ICAN, for the deidentified post-licensure safety data for the Covid-19 vaccines in the CDC’s v-safe system. Even though this data is available in deidentified form (meaning, it includes no personal health information), the CDC refused to produce this data claiming it is not deidentified.
So, on behalf of ICAN, we filed a federal lawsuit against the CDC and its parent entity, the U.S. Department of Health and Human Services (HHS), to force the CDC to produce this data to the public. The CDC should have no issue doing so because it has already made this data available to a private company – Oracle – in deidentified form. It is telling that Larry Ellison’s company can see the data American taxpayers paid the CDC to collect but the average American and independent scientists cannot?!
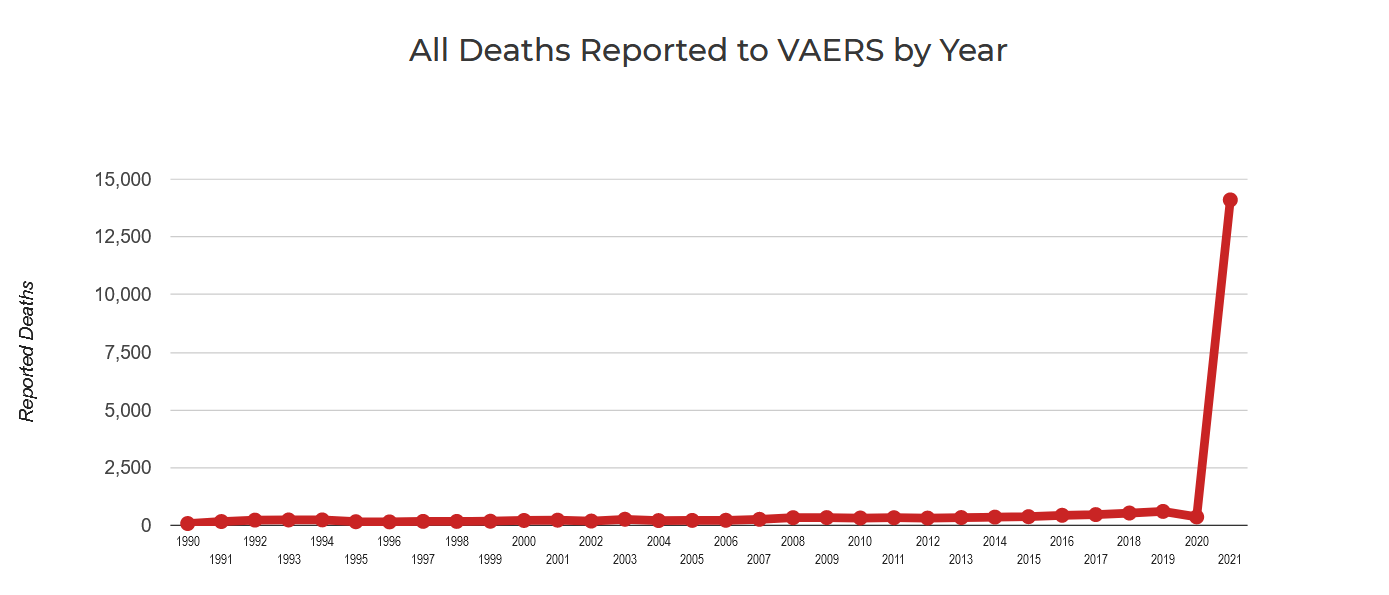
What is the v-safe system you may ask? Since rolling out the Covid-19 vaccines, the FDA and CDC have stated that their primary safety monitoring system, VAERS, is unreliable. The CDC therefore deployed a new safety monitoring system for COVID-19 vaccines called “v-safe.” V-safe is a smartphone app that allows vaccine recipients to “tell CDC about any side effects after getting the COVID-19 vaccine.” The purpose of the app “is to rapidly characterize the safety profile of COVID-19 vaccines when given outside a clinical trial setting.” With this new system, the CDC claims that these “vaccines are being administered under the most intensive vaccine safety monitoring effort in U.S. history.”
That all sounds great. And a CDC document explains that data submitted to v-safe is “collected, managed, and housed on a secure server by Oracle,” a private computer technology company, and that Oracle can access “aggregate deidentified data for reporting.” This means data submitted to v-safe is already available in deidentified form and could be immediately released to the public.
But yet, after we submitted a FOIA request to the CDC, on behalf of ICAN, to produce the deidentified v-safe data, the CDC acknowledged that “v-safe data contains approximately 119 million medical entries” but refused to produce that data by claiming that the “information in the app is not de-identified.” The CDC had apparently not read its own documentation regarding v-safe. But we had. So, we appealed this decision and submitted another request to the CDC that expressly asked only for any deidentified v-safe data, in the app or otherwise. Meaning, in the form that the CDC made the data available to Oracle. Incredibly, the CDC administratively closed this request stating it was duplicative of the original request.
Let me break that down again. The first request was denied by the CDC because it claimed the request sought data in the app that was deidentified. But then the CDC closed the second request, which made clear it is seeking only deidentified data (in the app or otherwise), by claiming the second request was duplicative of the first request! If this sounds ridiculous, it is because it is.
The public should be outraged by the CDC’s games.
The introduction to the lawsuit is copied below with a link to the entire complaint at the end. As with the pre-licensure Pfizer data, if you find what you are reading difficult to believe, that is because it is dystopian for the government to give pharmaceutical companies billions, mandate Americans to take their products, prohibit Americans from suing for harms, yet refuse to let Americans see the pre- and post-licensure safety data for these products. The lesson yet again is that civil and individual rights should never be contingent upon a medical procedure.
INTRODUCTION TO LAWSUIT AGAINST CDC FOR V-SAFE DATA
1. Between December 2020 and February 2021, the Food and Drug Administration (“FDA”) issued Emergency Use Authorizations for three COVID-19 vaccines, one of which subsequently received FDA approval in August 2021. While the FDA approved these vaccines, the Centers for Disease Control and Prevention (“CDC”), an agency within the Department of Health and Human Services (“HHS”), is charged with monitoring the safety of all vaccines, including the COVID-19 vaccines approved by the FDA. The CDC claims that these “COVID-19 vaccines are being administered under the most intensive vaccine safety monitoring effort in U.S. history[.]”
2. The federal government has mandated that millions of Americans receive these vaccine products. HHS has also given pharmaceutical companies complete immunity for injuries caused by those products. Mandating that millions of Americans inject a product for which they cannot hold the manufacturer liable if the product injures them demands complete transparency, especially when it comes to releasing the data underlying the product’s safety. FOIA exists precisely so that the American people can obtain transparency and, in this case, obtain the data which supports the CDC’s claims to intensive safety monitoring.
3. As for the pre-licensure data submitted by the pharmaceutical companies, the FDA took the position in another FOIA action that, because it needs to deidentify that data, it needs at least 75 years to produce the data to the public. As for the post-licensure data, the FDA and CDC have said that their prior primary existing safety monitoring program was incapable of determining causation and were otherwise unreliable. The CDC has, however, deployed a new safety monitoring system for the COVID-19 vaccines, v-safe, and the data within v-safe is already available in deidentified form and could be forthwith released to the public.
4. V-safe is a smartphone app that allows vaccine recipients to “tell CDC about any side effects after getting the COVID-19 vaccine.” The purpose of the app “is to rapidly characterize the safety profile of COVID-19 vaccines when given outside a clinical trial setting and to detect and evaluate clinically important adverse events and safety issues that might impact policy or regulatory decisions.”
5. Data submitted to v-safe is “collected, managed, and housed on a secure server by Oracle,” a private computer technology company. Although the CDC has “access to the individualized survey data,” Oracle can only access “aggregate deidentified data for reporting.”
6. Plaintiff asked through its instant FOIA requests that the CDC produce the deidentified data from the v-safe program in the same form that Oracle can access. Plaintiff believes that to assure transparency regarding the government’s claim that COVID-19 vaccines are “safe and effective,” the public should have immediate access to all v-safe data, in deidentified form, and therefore, once the CDC produces that data, Plaintiff intends to make it publicly available. Despite the fact that the deidentified data already exists, it is already in the hands of a private company, and the CDC has never objected to its production, the CDC has so far failed to produce it to Plaintiff or to the American public. The federal government is thereby not only failing to provide the transparency necessary to earn the American people’s trust regarding these vaccines but is also failing to comply with FOIA.
7. Plaintiff Informed Consent Action Network (“Plaintiff”) is a non-profit organization that advocates for informed consent and full transparency and disseminates information necessary for same with regard to all medical interventions. It intends to make all v-safe data immediately available to the public so that independent scientists can immediately analyze that data. It believes that we need all hands on deck, both inside and outside the government, to address serious and ongoing issues with the vaccine program, including waning immunity, adverse reactions, etc. Locking out independent scientists from addressing these issues is dangerous, irresponsible, unethical, and illegal.
8. To acquire the v-safe data, Plaintiff made three requests to the CDC pursuant to the Freedom of Information Act (5 U.S.C. § 552, as amended) (“FOIA”) seeking information regarding v-safe.
….
You can read the entire complaint here :

Tony Blair is the real idiot here

By Will Jones | The Daily Sceptic | December 30, 2021
Tony Blair was quoted recently as saying: “If you’re not vaccinated at the moment you’re not just irresponsible, you’re an idiot.”
Before the Covid vaccine was rolled out PHE published data that showed those aged 80 years or over were seventy times more likely to die than those under 40. Earlier this year, before young adults and children were vaccinated, the JVCI said that the incidence of severe outcomes from Covid in children and young people was very low and that Covid disease in children was typically mild or asymptomatic. COVID-19 has killed fewer children than seasonal flu in a normal year according to data compiled by the U.S. Centers for Disease Control and Prevention. The data was clear even in 2020 that if you were under 50 and in good health your risk of serious harm or death from the disease was vanishingly small.
For valid consent to be obtained for vaccination, not only would it be necessary to have a good perspective of Covid risk for that particular individual, it would also be essential to know whether naturally acquired immunity conferred as good or better protection and if remaining unvaccinated increased the risk to others. A former vaccine taskforce chief and many scientists involved in the Covid vaccine manufacture have stated that they were never designed to end transmission and this has now become clear for all to see. A recent Danish study confirms natural immunity is better.
For the above reasons it was refreshing to hear the Japanese Government declare: “Do not discriminate against the unvaccinated.”
Another factor that is important for valid informed consent and the decision on whether to be vaccinated or not is to look at the history of medicine. When new medical ideas or treatments were embarked upon how risky were they and how accomplished were healthcare professionals in providing that treatment?
In February this year the BMJ produced an article estimating 237 million or more medication errors are made every year in the U.K.
A few of the biggest medical scandals in history include thalidomide in the 50s and 60s, the HIV tainted blood scandal in the 80s and the PIP silicone implants more recently.
Are sceptical patients idiots? Are cautious people, including parents of young children, who have diligently assessed their risk profiles, done their own research, and shunned all the coercion, ‘idiots’?
Finally, it is also important in making the vaccination decision to ask ourselves how much we trust those in power and how often they can get big things wrong.
Galileo spent his last years in house arrest, was tried and forced to retract his perfectly correct position about the solar system being centred around the Sun, instead of around the Earth. Was he an idiot?
Were those who questioned the presence of weapons of mass destruction or the alleged guilt of the U.K. sub-postmasters all idiots?
Mr Blair, you later said: “Possibly I was a little too undiplomatic in my use of language.” No, Mr Blair, you were being arrogant and discriminatory. You do not acknowledge the deficiencies in the Covid vaccination programme’s ability to prevent infections over time without continual boosters; the evidence now clearly demonstrating the superiority of naturally acquired immunity for all but the extremely vulnerable; the unknown consequences of a novel strategy that attempts to control an airborne virus and its very real limitations in preventing transmission. You neglect to discuss medical ethics in relation to informed consent and how your comment can stigmatise people and thereby coerce them into being vaccinated.
Worst of all, Mr Blair, is that you made such a remark without submitting yourself to the challenge of fair scrutiny. Have you said this face-to-face to those I refer to above? Have you openly debated this one-on-one with scientists that say the opposite? Would you be prepared to be interviewed by such scientists, or would that scare you into thinking that you might look like an… unwise person?
Three more studies show negative vaccine efficacy. When will health authorities face up to what the data is telling us?

By Will Jones | The Daily Sceptic | December 28, 2021
The last two weeks have brought three new studies finding negative efficacy for two vaccine doses, meaning the vaccinated are more likely to be infected than the unvaccinated. These are study findings, not raw data, so have been adjusted for various biases and confounders, making it harder to dismiss them as anomalous or skewed.
The first is a pre-print study from Denmark, published on December 23rd, which looked at nearly all PCR-positive SARS-CoV-2 infections in Denmark from November 20th to December 12th and investigated them to see if they were likely to be the Omicron variant. By comparing the vaccination status of those infected, the researchers found a vaccine effectiveness against the Omicron variant of minus-76.5% for Pfizer and minus-39.3% for Moderna three months after double vaccination (see chart above), meaning the double-vaccinated were considerably more likely to be infected than the unvaccinated. They found the vaccine effectiveness against Omicron was significantly lower than against Delta, with Pfizer vaccine effectiveness at 53.8% and Moderna at 65% against Delta after three months. They reported that a third dose of Pfizer got vaccine effectiveness against Omicron back up to 54.6%, at least for a month. The full results are in the table below.

Hansen et al
The latest vaccine effectiveness study from the UKHSA confirms these results. Against Omicron, the UKHSA reports zero or negative vaccine effectiveness from a double-dose of all three vaccines (AstraZeneca, Pfizer and Moderna) after five months. The third dose takes it up again, but only into the 40-60% range, and dropping fast.

AstraZeneca

Pfizer

Moderna
A new study in Eurosurveillance from Norway also backs up the observation of negative vaccine effectiveness against Omicron, with a higher proportion of those who tested positive in the particular outbreak in the study being double-vaccinated than those who did not test positive (98% versus 93%).
Some studies had already found negative vaccine effectiveness against Delta, in line with the unadjusted figures from the UKHSA, though many people had dismissed these results as anomalous or biased. With Omicron, the reports of negative efficacy are becoming impossible to ignore, with even the UKHSA publishing graphs showing it after three months on two doses. At some point, health authorities are going to need to grapple with what the data is showing on this and stop pretending it isn’t there.
After Thousands Of Parents Refused To Comply, California School District Reverses Child Jab Mandate
By Matt Agorist | The Free Thought Project | December 23, 2021
San Diego, CA — Forgoing any legal democratic processes, multiple school districts in California began mandating the COVID-19 vaccination for children earlier this year. Set to go into effect in January, any child, 16 and older, who did not get the jab, was banned from campus in all San Diego public schools.
This authoritarian move caused a mass of backlash and thousands of children and parents refused to comply. The refusal to get vaccinated set the stage for a showdown that was to unfold on January 24 when the children would be kicked out of school for non compliance.
There will be no showdown, however, as a San Diego judge struck down the mandate this week, accurately pointing out that a school district has no authority to mandate medical procedures for children.
CBS 7 reports that Superior Court Judge John S. Meyer granted a writ of mandate for a lawsuit filed by the group “Let Them Choose,” which sought to keep the school district‘s COVID-19 vaccine mandate from going into effect by arguing it did not comply with state law.
Meyer noted in the ruling that the school district‘s COVID-19 vaccine mandate cannot move forward because it conflicts with state law, which says any decision to mandate vaccines must be made at the state level and must also include a “personal belief exemption” if the mandate is not imposed by the state Legislature.
San Diego Unified’s policy did not contain this exemption.
“SDUSD‘s Roadmap appears to be necessary and rational, and the district’s desire to protect its students from COVID-19 is commendable. Unfortunately, the field of school vaccine mandates has been fully occupied by the State, and the Roadmap directly conflicts with state law,” the judge wrote in a tentative ruling.
Naturally, the school district disagreed and claimed they have the right to dictate what children can and can’t be injected with. For now, however, their objection is meaningless and the children and parents who did not want to take the vaccination, will no longer be forced to do so.
“I am overjoyed. We knew that our legal argument was strong, and we brought this case on behalf of thousands of concerned parents and students and to hear the judge say no student should be coerced into getting this vaccine was just a wonderful thing to hear,” said Sharon McKeeman, founder of the group behind Let Them Choose.
As TFTP reported earlier this month, the Los Angeles Unified School District (LAUSD) — which is the second largest school district in the country — made a similar move and mandated shots for all children aged 12 and older.
Students were told they would be banned from campus on January 10, 2022 if they failed to comply and take the shot.
NBC4 spoke to an attorney who is following these cases, Jennifer Kennedy, who explained that school districts do not have the authority to mandate medical procedures. Just like the San Diego school district did not have the authority to mandate the jabs, the LAUSD did not have it either.
“These grotesque contests and displays of treatment and candy and gifts and favors, raffles and cash prizes inducing the kids to the vaccination…. Here is the problem, kids in California cannot consent to vaccination.”
She added, “The LAUSD does not have the power to add a vaccine to the California school schedule,” she said. “You couldn’t do it if you were a po-dunk school district and you can’t do it if you’re LAUSD, the second largest district in the nation. You don’t have that legal authority.”
Several parents of students filed lawsuits against the LAUSD over the mandate and thousands of children remained unvaccinated in LAUSD. This line in the sand forced the school district to postpone their mandate last week after a whopping 28,000 children refused the jab.
It is only through resistance that the change we seek will come. As history shows us, one cannot comply their way out of tyranny.
Twitter Suspends mRNA Inventor Dr. Robert Malone

By Tyler Durden | Zero Hedge | December 29, 2021
After months of providing valuable Covid-19 information that runs counter to the official narrative, Twitter has finally banned Dr. Robert Malone, inventor of mRNA technology.
Malone, who will appear on the Joe Rogan show Thursday according to associate Ed Dowd (one of four contributors to the Malone doctrine), had more than 520,000 followers. He has been an outspoken critic of both mRNA vaccines, as well as the abysmal failures of policymakers worldwide in responding to the pandemic.
He was not warned or provided an opportunity to delete any offending tweets – instead he was “just suspended,” Dowd continued.
Here’s Malone’s last tweet – sharing an article which claims that the Pfizer Covid-19 vaccine does ‘more harm than good.’
Malone can still be followed via his substack page.
How to manipulate a research study
Top tips on ensuring vaccine success (and for other treatment failure)
Health Adisory and Recovery Team | December 29, 2021
There are ways to ensure any trial will give you the results you want. Here are the top six methods used to manipulate covid research results.
1. Carry out the study when cases are falling
A favourite trick that has been used repeatedly throughout the pandemic.
Vaccination is a process that takes time. At the beginning of the study all participants are enrolled as unvaccinated. People move into the vaccinated cohort over time. The result is that the unvaccinated are exposed at periods of higher prevalence and for a longer time. The vaccinated are only exposed from a period later on and further down the curve. The vaccinated will therefore be less likely to catch covid and the vaccine can be made to look like it worked.
The ONS recently deployed this trick to claim a 32 fold lower mortality among the vaccinated. It was extreme data manipulation whereby they included the majority of deaths in winter prior to vaccination instead of starting from spring when a fairer comparison could have been made. The Office for Statistics Regulation has upheld a complaint about the ONS’s manipulation of data in this case.
2. Don’t include meaningful outcome measures like death
The vaccine trials have not demonstrated prevention of death.
Death from covid was too uncommon for the trials to be able to show an effect. Among 44,000 participants in the Pfizer trial, for example, there were a total of
29 deaths before the placebo group were themselves vaccinated. 15 of these were in the vaccinated including one of the three covid deaths. There were only 20 severe covid cases reported in the Pfizer submission to the FDA for Emergency Use Authorisation, including those that did not need hospital care.
Instead of using outcomes which are hard to distort, like death, the outcomes used were based on test results.
3. Only measure outcomes for part of the time after vaccination
Vaccinated people are at increased risk of covid infection in the first two weeks after vaccination. After the first two weeks the susceptible will have acquired natural immunity. By ignoring the first two weeks, a distorted picture of the overall impact of vaccinations can be presented. If all the vaccines are doing is causing the susceptible to have their infections earlier then the whole period from the date of vaccination needs to be included in assessing any benefit.
4. Use modelled data
The most reliable scientific papers ensure that the population being studied is representative of the population as a whole. Sometimes that is hard to achieve and adjustments need to be made afterwards to account for any differences e.g. the sample may be younger than the population as a whole. These adjustments are a reasonable thing to do to correct for small problems in the sample.
However, if the sample is so different to the general population that massive adjustments need to be made then effectively the study is no longer based on real world evidence. Instead it has become yet another prediction based on modelled data.
For example, this CDC study claimed, contrary to all other evidence, that people with a prior infection were 5 times more likely to become infected than those who had been double vaccinated. The actual results from the study showed a 70% higher rate but their adjustments made this into 500%. There were other serious flaws in the study which makes even the 70% claim highly dubious.
5. Ignore a crucial subgroup
If the findings are equivocal in most of the population then modelling might be enough to get the result you want. However, if there is a subgroup which has clearly contrary results then they can be left out entirely. When trying to calculate the impact of vaccination on transmission in winter the most obvious group to study would have been the heavily vaccinated care home residents. PHE omitted this group from their paper with no reason given. The consequence was that the overall household transmission rate was much higher in the real world (see figure 1) than in the study. Using published data on mean national transmission rates each week the expected rates in the study would have been 12.4% in the unvaccinated (who were overrepresented when transmission rates were highest) and 11.7% in the vaccinated cohorts. However, the study reported a rate of only 10.1% in the unvaccinated and only 6% in the vaccinated. The population excluded from the PHE study clearly contributed to the much higher real world transmission rates for both the unvaccinated and the vaccinated.

Figure 1: Real world transmission rates as measured by the proportion of contacts that become infected, the secondary attack rate.
6. Use the wrong dose of the drug
A drug can be discredited in a trial where the protocol is deliberately designed to give a drug at an inappropriate time or dose. For example, the RECOVERY trial was said to show that hydroxychloroquine treatment was not helpful in covid. The trial design used a dose of hydroxychloroquine that was in the toxic range and may well have been responsible for the deaths of participants in the treatment arm of the trial. Hydroxychloroquine doses over 1500mg are associated with cardiovascular and neurological harms that can be potentially fatal. The trial used a dose of 2000mg in the first 18 hours and 400mg every 12 hours thereafter.
Conclusion
Scientists are human and are under pressure to produce results in their papers as that increases the chances of publication which is needed for career progression and securing funding for research. There are numerous ways in which data can be altered to tell a story and many of them have been put to use during the pandemic. Dramatic results have become headline grabbing news but often the truth was far more mundane. If a result sounds too good to be true, don’t believe it.
Featured Video

“Trump’s presidency is at risk of being destroyed” Col Douglas Macgregor
or go to
Aletho News Archives – Video-Images
From the Archives
Mutually Assured Delusion (MAD)
By Judith Curry | Climate Etc. | November 5, 2013
Groupthink: A pattern of thought charaterized by self-deception, forced manufacture of consent, and conformity to group values and ethics.
Groupthink: Collective Delusions in Organizations and Markets, by Roland Benabou, published in the Review of Economic Studies. Benabou also has a talk (ppt slides) on this subject.
First, a definition of groupthink (from the ppt slides):
Janis (1972)’s eight symptoms [of groupthink]:
- illusion of invulnerability
- collective rationalization
- belief in inherent morality
- stereotyped views of out-groups
- direct pressure on dissenters
- self-censorship
- illusion of unanimity
- self-appointed mind guards
Sound like any groups that we know? … continue
Blog Roll
 Aletho News
Aletho News- “Trump’s presidency is at risk of being destroyed” Col Douglas Macgregor
- Iran has legal right to act in Hormuz, holds US responsible for disruptions: UN mission
- Sudan’s RSF leaders build Dubai property empire with UAE backing: Investigative group
- West losing leadership position to Global South: Russia’s president
- How Cognitive Science Explains Our Looming Nuclear Crisis
- Have the US and Israel killed non-proliferation?
- Moscow, Tehran to support each other amid US aggression: Russia’s defense minister
- Iran says EU’s insistence on sanctions hastens its ‘embarrassing descent into irrelevance’
- Argentina’s Javier Milei sells out his country for Israel
- Putting Nukes in Finland Won’t Make Country Safer, Finnish Politician Cautions
- If Americans Knew
- By Week’s End, Trump’s War Will Be Plainly Illegal
- CBS News Reportedly Ousts London Bureau Chief Over Differences With Bari Weiss Over Gaza Coverage
- State Department Says US Is in Conflict With Iran ‘At the Request’ of Israel
- What ceasefire? Israel won’t stop killing in Gaza, Lebanon – Daily Update
- Palestinians in Gaza Want to Rebuild Food Systems. Israel Isn’t Letting Them.
- Under Trump, Green Card Seekers Face New Scrutiny for Views on Israel
- Sheep Theft Sent Shockwaves Through a Palestinian Village. Then, a 12-year-old Boy Was Shot Dead
- Trump alum helps Israel mount AI influence campaign
- Dispatches From Catastrophe
- Despite Denials, AIPAC Is Now Funding Campaign of Ala Stanford In Philadelphia
- No Tricks Zone
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
