Dr. Mercola’s Latest Response to CNN’s Hit Piece
By Dr. Joseph Mercola | October 5, 2021
CNN reporter Randi Kaye visited my home unannounced, then tracked me down as I bicycled around my home town in August 2021. Her purpose was to publish a hit piece further labeling me as a “super-spreader of COVID-19 misinformation,”1 based primarily on the opinions of foreign agent Imran Ahmed, founding CEO Center for Countering Digital Hate (CCDH),2 which is a recently spun up front group funded by dark money.
After that story aired, she again contacted me, this time via email, to request an interview regarding my latest book, “The Truth About COVID-19: Exposing The Great Reset, Lockdowns, Vaccine Passports, and the New Normal.” Interview questions were provided via email, as were my responses. CNN ran this new story October 4, 2021.
In the interest of transparency, below I’ll post the email exchange so you can read my response to her questions firsthand. You can tell from the leading questions that this “story” isn’t true journalism but rather another hit piece manipulated to fit a preformed agenda.
CNN Interview Request for My Latest Book
August 26, 2021, Kaye emailed, “Here are the questions we would like answered about Dr. Mercola’s new book. We would welcome responses by 5pm tomorrow, please.” The questions, which are clearly accusatory, are as follows:
“You say in your book that “A large amount of data strongly suggests the COVID – 19 vaccine may be completely unnecessary, which means the global population is being bamboozled into participating in a dangerous and unprecedented experiment for no good reason whatsoever.” Can you please point us to that data that suggests the covid vaccines are unnecessary or dangerous?
You say in your book that “vaccine trials are rigged.” What proof do you have of that? Which trials? How many? Who rigged them and for what purpose?
You say in your book, “Common sense dictates that if the vaccines cannot prevent or reduce infection and transmission, hospitalization, or death, then they cannot possibly end the pandemic.” And that “There’s no telling whether they will ultimately prevent hospitalizations and deaths.”
Can you please provide us with the source and support for your statements since the CDC says vaccines are nearly 100% effective at preventing severe disease and death and greatly reduce infection.
How do you explain statements from hospitals and government officials that nearly all those who are getting sick and dying now are the unvaccinated?
Do you feel responsible for the spread of misinformation by writing a book full of conspiracy theories and false claims?
What were you paid for this book deal by the publisher?
Are you donating 100% of the earnings from your book?
If so, to which organization? Are you concerned this book will cost people their lives?”
My Response to CNN
Media organizations contact Mercola.com regularly, sometimes to challenge us on the researched, fact-checked articles we post for our readers. In CNN’s case, the information they were seeking was directly related to my book, which was the No. 1 best seller in all categories for four straight days with thousands of five-star ratings.
Much like the information on Mercola.com, the information in my book is thoroughly referenced, but Kaye, ironically, engaged in the dissemination of misinformation herself by describing my book as being “full of conspiracy theories and false claims.” My response to her questions follows:
“Many studies and other literature offer support for my position in answering several of your questions, which are combined since they can be answered with the same literature. Here are the important points that drive my book:
The vaccines are just 39% effective and waning, and the CDC’s Advisory Committee on Immunization Practices has now advised booster doses to the mRNA vaccines in immunocompromised persons. CDC’s goal is to begin offering booster doses to everyone else beginning this fall.3,4,5,6
Additionally, breakthrough infections among fully vaccinated persons are becoming more and more prevalent around the world. Evidence is beginning to mount that people with breakthrough infections can spread the Delta variant more easily.7,8,9,10,11,12,13
Most recently, researchers in Israel report that fully vaccinated persons are up to 13 times more likely to get infected than those who have had a natural COVID infection.
As explained by ScienceMag: The study “found in two analyses that people who were vaccinated in January and February were, in June, July and the first half of August, six to 13 times more likely to get infected than unvaccinated people who were previously infected with the coronavirus.
In one analysis, comparing more than 32,000 people in the health system, the risk of developing symptomatic COVID-19 was 27 times higher among the vaccinated, and the risk of hospitalization eight times higher.”14
The study also said that, while vaccinated persons who also had natural infection did appear to have additional protection against the Delta variant, the vaccinated were still at a greater risk for COVID-19-related-hospitalizations compared to those without the vaccine, but who were previously infected.
Vaccinees who hadn’t had a natural infection also had a 5.96-fold increased risk for breakthrough infection and a 7.13-fold increased risk for symptomatic disease.
“This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity,” study authors said.15
A majority of gravely ill patients in Israel are double vaccinated.16 A majority of deaths over 50 in England are also double vaccinated.17 Also, mass vaccination of the population with the highly mutating coronavirus will only evolve perfectly vaccine-resistant strains of the virus.”18
Injection Trials Included COVID-19 Infections as Successes
The next part of my response focused more specifically on the vaccine trials, which were problematic from the start since they did not include prevention of infection as an endpoint. Instead, all study endpoints required infection with SARS-CoV-2, and “successes” included subjects with confirmed COVID-19 cases. The difference measured wasn’t whether or not the vaccines prevented COVID-19 but whether, and how, they modified symptoms among those infected.19
Also problematic is the unblinding of the vaccine trials, which means the placebo groups were removed. As medical investigative journalist Jeanne Lenzer wrote in the BMJ, “The data are now likely to be scanty and less reliable given that the trials are effectively being unblinded.”20 This is the next section of my response to Kaye:
“Regarding the vaccine trials: The vaccine trials were designed specifically to succeed for profit. The public health authorities and media like CNN are utilizing fear of the virus to induce psychological stress that promotes obedience and servitude.21
Additionally, proof that the trials are “rigged” can be shown by virtue of the fact that they’ve done away with the control groups — who were getting a placebo but who were then offered the vaccine, which virtually does away with the ability to compare adverse reactions including deaths. Pfizer’s own vaccine insert for Comirnaty admits that the control group hasn’t existed since December 2020:
Section 6.1 — “Upon issuance of the Emergency Use Authorization (December 11, 2020) for COMIRNATY, participants were unblinded to offer placebo participants COMIRNATY. Participants were unblinded in a phased manner over a period of months to offer placebo participants COMIRNATY.”22
NPR has noted that removing the placebo groups from vaccine trials will prevent accurate data from long-term studies from being known.23
Additionally, the CDC is being dishonest by utilizing data from the beginning of this year when the vaccine campaign had just been initiated to conflate their claim. They are using data that were scant early in the year because so few were vaccinated, as opposed to using current information.24
Proceeding with the FDA approval of Comirnaty this week was unprecedented. No other vaccine has ever received approval this fast — and without public comment being allowed through ACIP [the CDC’s Advisory Committee on Immunization Practices] or VRBPAC [the FDA’s Vaccines and Related Biological Products Advisory Committee] before approval was issued.
The approval is unconscionable because over 600,000 adverse reactions and 6,000 deaths [now over 14,500 deaths25] have been reported in the U.S. to VAERS. A majority of these reports are filed by medical professionals.
This shows that the safety of these vaccines is not proven. Besides, the experiments are continuing through 2027 as the FDA APPROVAL requires Pfizer to submit study results analyzing risk of myocarditis and pericarditis, and risk to long-term infant development in pregnant women. Study results will be submitted to the FDA for review on Oct 31, 2025 and May 31, 2027 respectively.”26
Lifesaving Information That CNN Won’t Share
CNN and other media outlets have the power to share lifesaving information that could turn the pandemic around and save lives in the process — but they won’t. Instead, the media are ignoring the basics of healthy immune function and the importance of early COVID-19 treatment to continue to push the narrative that the only solution is to get an injection.
The last part of my response to Kaye includes empowering steps that virtually everyone can take to support their health and reduce their risk of infectious disease. This includes having supplies from the Front Line COVID-19 Critical Care Working Group (FLCCC) I-MASK+ protocol on hand in the event you do get COVID-19.
FLCCC’s I-MASK+ protocol can be downloaded in full,27 giving you step-by-step instructions on how to prevent and treat the early symptoms of COVID-19. FLCCC also has protocols for at-home prevention and early treatment, called I-MASS, which involves ivermectin, vitamin D3, a multivitamin and a digital thermometer to watch your body temperature in the prevention phase and ivermectin, melatonin, aspirin and antiseptic mouthwash for early at-home treatment.
I also recommend getting a nebulizer, and the moment you feel a sniffle or something coming on, use nebulized hydrogen peroxide. Having a pulse oximeter on hand is also wise, as it’s a noninvasive way to measure the oxygen levels in your blood, allowing you to monitor your levels and help gauge whether a trip to the ER is truly in order.
As I told Kaye, taking control of your health continues to be the “secret” that I strive to share with the masses. The remainder of my response to CNN follows:
“I am donating all proceeds to the National Vaccine Information Center. I encourage every person to fully educate themselves to make individual decisions about medical risk-taking by talking with their personal physician and comparing the risks and benefits to make an informed decision that includes all the information on how these vaccines are working (or not working) and what all the possible side effects may be.
This pandemic is a direct reflection of the health of our population: 95% of COVID deaths have multiple comorbidities. Obesity, vitamin D deficiency and metabolic dysfunction are at the core of this pandemic and can be resolved by taking control of your health by following science-based dietary and lifestyle recommendations.
Since building up your health can’t be done overnight, what you can do beginning right now is avoid linoleic acid, check to ensure your vitamin D levels are above 40ng/ml, exercise, get fresh air and proper sun exposure, and restrict your eating window to a 6- to 8-hour time frame each day.
If you do get COVID-19, early treatment is crucial. Follow the Front Line Critical Care Alliance iMASK+ or MATH+ treatment protocols.”28
Sources and References
- 1 YouTube August 5, 2021
- 2 Twitter Josh Hawley July 20, 2021
- 3 CNBC July 23, 2021
- 4 KHN Morning Briefing August 26, 2021
- 5 Contagion Live August 14, 2021
- 6 U.S. CDC, COVID-19 Vaccine Booster Shot September 1, 2021
- 7 CNBC July 30, 2021
- 8 NPR August 23, 2021
- 9 MSN August 27, 2021
- 10 Reuters August 20, 2021
- 11 CIDRAP July 29, 2021
- 12 Reuters August 25, 2021
- 13 National Geographic August 20, 2021
- 14 Science August 26, 2021
- 15 medRxiv August 25, 2021
- 16, 17 Science August 16, 2021
- 18 LiveScience August 6, 2021
- 19, 21 Forbes September 23, 2020
- 20 BMJ 2020;371:m4956
- 22 FDA, Comirnaty Highlights of Prescribing Information
- 23 NPR February 19, 2021
- 24 Undercurrents, The Lies Behind the “Pandemic of Unvaxxed”
- 25 MedAlerts September 3, 2021
- 26 thebmjopinion August 23, 2021
- 27 FLCCC Alliance, I-Mask+
- 28 FLCCC Alliance, I-Mask+ Prevention & Early Outpatient Treatment Protocol for COVID-19
Video emerges where Fauci and others plan for a “Universal mRNA Flu Vaccine” which became the “COVID-19 Vaccine”
Because People were not Afraid Enough of the Flu Virus

By Brian Shilhavy | Health Impact News | October 5, 2021
Last night Alex Jones of Infowars.com did a special broadcast regarding an October, 2019 video that they had just become aware of that was a panel discussion hosted by the Milken Institute discussing the need for a Universal Flu Vaccine.
The video clip that they played of this event was a 1 minute and 51 second dialogue between the moderator, Michael Specter, a journalist who is a New Yorker staff writer and also an adjunct professor of bioengineering at Stanford University, Anthony Fauci, the director of the National Institute of Allergy and Infectious Disease, and Rick Bright, the director of HHS Biomedical Advanced Research and Development Authority (BARDA).
In this short clip, which was extracted from the hour long panel discussion, Anthony Fauci explains that bringing a new, untested kind of vaccine like an mRNA vaccine, would take at least a decade (“if everything goes perfectly”) to go through proper trials and be approved by the FDA.
He would know, because he had been trying to do it for about a decade already by then (October, 2019), trying to develop an mRNA based vaccine for HIV.
But now they were discussing something much bigger than just a vaccine for AIDS patients. They are talking about a “Universal Flu Vaccine” that everyone would have to take – a huge market for Big Pharma!
Rick Bright, the director of HHS Biomedical Advanced Research and Development Authority (BARDA), then speaks and states that what could happen is that “an entity of excitement that is completely disruptive and is not beholden to bureaucratic strings and processes” could change that.
Here is the short clip which I put on our Bitchute and Rumble channels last night:
Alex Jones spent over 50 minutes covering this on his show last night, and it looks like he covered it on his show today as well.
I have not had a chance to watch these yet, as I went and found the original 1 hour panel discussion video, and spent the day listening to and analyzing that, so that I could supply this report to our readers.
Joining Fauci, Rick Bright, and Michael Specter at this event were:
- Margaret Hamburg, Foreign Secretary, National Academy of Medicine
- Bruce Gellin, President, Global Immunization, Sabin Vaccine Institute
- Casey Wright, CEO, FluLab
In short, this panel discussion focused on what they perceived as the need for a universal flu vaccine, but they admitted that the old way of producing vaccines was not sufficient for their purposes, and that they needed some kind of global event where many people were dying to be able to roll out a new mRNA vaccine to be tested on the public.
They all agreed that the annual flu virus was not scary enough to create an event that would convince people to get a universal vaccine.
And as we now know today, about 2 years after this event, that “terrifying virus” that was introduced was the COVID-19 Sars virus.
And so now we know why the flu just “disappeared” in the 2020-21 flu season. It was simply replaced by COVID-19, in a worldwide cleverly planned “pandemic” to roll out the world’s first universal mRNA vaccines.
This was always the goal, and previous efforts through various influenzas, AIDS, Ebola, and other “viruses” were all unsuccessful in leading to the development of a universal vaccine to inject into the entire world’s population.
Margaret Hamburg stated regarding getting a “Universal Vaccine” into the market:
“It’s time to stop talking, and it’s time to act.”
“I think it is also because we haven’t had a sense of urgency.”
Michael Specter asks:
“Do we need lots of people to die for that sense of urgency to occur?”
Hamburg replies that: “There are already lots of people dying” from the flu each year.
Bruce Gellin states that basically people just are not afraid enough of the term “the flu.”
There are so many things that are revealed about how Big Pharma and government health authorities think in this panel discussion. For example, they bemoan the fact that if they do too good of a job in public health, then they lose funding to develop products that fight viruses.
Michael Specter states: “It seems to me that one of the curses of the public health world is, if you guys do your job well, everyone goes along well and healthy.”
Hamburg: “And they cut your funding.”
Rick Bright complains that the yearly distribution of flu vaccines is inefficient in terms of collecting data, and in the process actually admits that some vaccines just don’t work well:
“We distribute 150 million doses of the seasonal (flu) vaccines every year, we don’t even know how many people are being vaccinated from the doses that are delivered to the people, which doses they got, and what the real outcome was, so that we can learn from that knowledge base on how to optimize or improve our vaccine. So there are opportunities that we have today…”
I think if we uncloaked the poorest performing vaccines in the market place today, it might be very revealing to tell us which of the technologies we have, and allow us to go deeper into those technologies to determine why they are more effective. There are vaccines licenses today that are more effective. I think that we’re just afraid to admit the truth.”
So much for the public mantra that is espoused by Big Pharma and government that the “science” of vaccines is “settled,” and that they are completely “safe and effective.”
Casey Wright repeats the mantra that was publicized every year, before COVID, about just how deadly the flu virus was: “650,000 people die every year from the flu.”
As we have documented many times over the past decade here at Health Impact News, this is simply not true. This is an estimate because actual laboratory confirmed cases of influenza each year are very small, probably less than 1000 in the U.S.
Most flu-like symptoms are never tested in a lab to determine what is causing the symptoms. They were always just classified as “flu” to inflate the numbers to justify the very profitable flu shot each year. Some of our previous coverage of this issue:
Did 80,000 People Really Die from the Flu Last Year? Inflating Flu Death Estimates to Sell Flu Shots
So as they have inflated the COVID-19 cases since last year, they are simply continuing their policy of inflating flu numbers each year in order to sell their vaccines. They obviously could not have done both last year, as the public would have quickly seen that the math doesn’t work.
And yet, so many in the public bought the lie that the COVID-19 measures got rid of the flu, but not COVID-19.
Ultimately, this panel discussion can be boiled down to: Nobody wants to fund research for a universal flu vaccine. So how do we change that? Create a pandemic of fear over the flu (but they couldn’t call it the “flu” because people are no longer afraid of influenza, and the fear over “AIDS” had also subsided.)
Fauci then addressed this “perception problem.”
There’s this perception (about the flu), if it’s so serious, how come people get the flu each year and it isn’t a catastrophe?
When you’re dealing with a disease like HIV, if you get HIV, it’s serious. Whether you’re young, whether you’re middle aged, or whether you’re old. If you get cancer, that’s bad. Whether you’re young, whether it’s intermediate… whereas if it’s influenza, some people, they go throughout life and it doesn’t impact them at all.
There isn’t anyone who is afraid of influenza. You go into a focus group and you say: Are you afraid of getting HIV if you’re at risk? Oh, absolutely.
Are you afraid of getting cancer? Absolutely. Are you afraid of the flu? Don’t bother me.
That’s the reality of how people perceive flu.
And it is going to be very difficult to change that, unless you do it from within and say, I don’t care what your perception is, we’re going to address the problem, in a disruptive way…
Specter then asks:
In the long run, over time, if the 2009 pandemic had been much more deadly, would that have ended up being a better thing for humanity?
Everyone is silent as they obviously were thinking about how to answer that, and Specter says: “Come on gang.”
Fauci ultimately answers and says “No” because there were other years that were worse than 2009 and it didn’t change a thing in terms of creating a universal vaccine.
Hamburg then states:
The sad truth is that when there is a major crisis, it focuses attention and usually resources and some significant mobilization follows.
We need, #1, this time to be different, and we also need to really organize ourselves in a way where there will be accountability for sustained action, and not just response.
Specter states:
Craig Venter, who is a controversial person, but interesting to me, has written that he thinks we ought to have a vaccine, such that, if you take off in a plane from Hong Kong, and are infected, by the time your plane lands in New York, there ought to be a vaccine assembled and deliverable to you.
How crazy is that? How far are we from that? Are we ever going to get there?
Bright replies:
I’m not going to say how far away, but I don’t think that’s too crazy.
I think that if we move towards the era of synthetic-based vaccines, I think we remove the dependencies of thinking the vaccine that has be grown into something else, an egg, a cell, or insect cell – any type of dependency embryo.
If we can move into more synthetic, the nucleic acid based, messenger RNA based, those sequences can be rapidly shared around the world.
He then goes on to talk about using a 3D printer to print out a “vaccine patch” that people use to administer the “vaccine.”
We also learn in this panel discussion why Anthony Fauci is so opposed to natural immunity, because natural immunity for influenza, according to his view, translates to an immune response against other strains of a particular influenza virus, which will interfere with what they are trying to do with the vaccines.
That is why he wants to inject infants as young as 6 months old with a universal vaccine, as he states here, to prevent that “confused” natural immunity from happening before the child grows older.
So the big question that this panel was tackling, was how do they implement their strategies, and what is holding them back?
Certainly the government/regulatory issue is a big one, and now two years later we can see exactly how they did that, by controlling the FDA and the CDC to promote the “killer virus pandemic” narrative as long as possible to justify taking emergency measures that short-cut the normal procedures for bringing novel, new drugs to the market.
It also clearly explains the vicious opposition to existing, cheap therapeutics that very easily treated what is really just the seasonal flu “virus,” which stood in their way of rolling out a universal vaccine.
Casey Wright then made a rather remarkable comment about “philanthropy” and its role in this effort:
There’s a potential role for philanthropy to play there… we are in a position to take on a little more risk (she smiles eerily as she says this), to be open to a little bit more experimentation and methods in how we do things. That’s what I think is unique about FluLab, and its unique about other philanthropies.
I think they can play a really important role there, and fund a set of bolder, maybe earlier promising concepts.
Bingo! Think Bill and Melinda Gates Foundation, the Rockefeller Foundation, and other “philanthropies” that are “unburdened” by regulatory issues as they spend their money pretty much unchecked, with no accountability, all in the name of “science” and the “greater good.”
We have seen most certainly how the Gates Foundation has done this in India by luring poor people into highly questionable ethical experimentations with vaccines, such as the Gardasil vaccine which we have covered so often over the years here at Health Impact News.
Bruce Gellin then talks about a report published by his organization that called for an “entity” that would make these decisions and bring everyone together to collaborate to create this universal vaccine, and eliminate those who oppose.
The report was published in 2019, and here is the press release.
He states:
They called for this “entity” which is the collaboration we talked about. They called for the need to infuse innovation, to find some of these people who we don’t know might be part of the problem to come into this. And to try to think about how we talk about this differently so that your stomach flu doesn’t keep us from making progress. (everyone laughs…)
I assume that this “entity” is Gellin’s group, The Sabin-Aspen Vaccine Science & Policy Group.
Today, this is the main group fighting “vaccine hesitancy” and trying to silence any dissenting voices that get in their way of rolling out this universal vaccine, which of course we now know is the COVID-19 vaccine.
Watch the entire panel discussion to learn just how arrogant these people are. This is on our Bitchute and Rumble channels… Further analysis at Health Impact News.
Businesses push back against Scotland’s vaccine passport
By Ken Macon | Reclaim The Net | October 5, 2021
Resistance to the introduction of vaccine passes, based on various grounds and gaining momentum for different reasons – is not present only among the general population and customers. In Scotland, owners of businesses have joined those who are opposed to a mandated COVID passport system by announcing a weekend boycott of the program.
Their argument is that the scheme Scotland launched via an app is so technically flawed that it is causing chaos and harming their businesses, as it keeps customers and visitors to places like night clubs and football stadiums away by simply not working.
This seems to be yet another in UK’s botched schemes rolled out over the course of the pandemic, and besides being riddled with technical problems, another thing these have in common is that they cost a lot of taxpayers’ money – although the latest Scottish “omnishambles” as some are calling the app is “cheap” compared to some other UK COVID fiascos – it cost a “mere” £600,000 ($816,520) to develop, although that’s probably £600,000 too much, considering that it doesn’t appear to work.
The first to defiantly pull out of the scheme once it became apparent it was useless were football clubs, who have been hard-hit by COVID restrictions that kept fans out of stadiums and seriously undermined their revenues for months on end.
The app was officially put in practice last Friday morning, with the SNP-led government announcing people would need to show proof of vaccination to be let into this type of venue. But the very same day, realizing the app wasn’t working, Aberdeen FC simply abandoned this requirement for its fans to attend the game upcoming on Sunday.
“Nobody will be asked to show proof of vaccine,” the club announced on Friday, reacting to fans being unable to buy tickets because the app could not be used to prove their vaccination status. Other Scottish clubs, like Rangers and Hearts, soon followed suit, while owners of nightclubs and others in the hospitality industry did the same, saying the confusion was “farcical.”
What followed was Health Secretary Humza Yousaf having to reverse previous policy, saying that “nobody should be denied entry this weekend if they failed to show proof of vaccination, and admitted the widespread technical problems may take ‘days’ to fix,” the Telegraph reported.
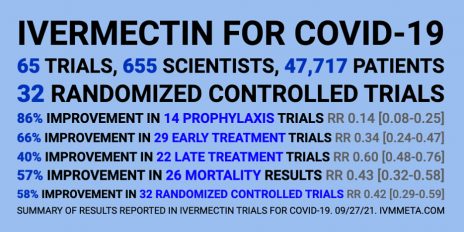
The Research Is Clear: Ivermectin Is a Safe, Effective Treatment for COVID. So Why Isn’t It Being Used?
By Elizabeth Mumper, M.D., FAAP | The Defender | October 4, 2021
A patient with Type 1 diabetes called to tell me the pharmacist at our local Walgreens refused to fill the prescription I had written for ivermectin, so I called to ask why.
The young pharmacist, a few years out of pharmacy school, informed me he did not understand why I was using ivermectin for early treatment of COVID because “SARS-CoV-2 does not have an exoskeleton.”
I explained I was not using ivermectin as an anti-parasitic medication, but that it had impressive data as an anti-inflammatory and anti-viral.
Furthermore, as a pediatrician, I have more than 40 years of experience managing multiple viral illnesses. There is value in treating viruses early, often with inexpensive natural remedies, rather than “staying at home until you have problems breathing then go to the hospital” as U.S. public officials have advised for COVID.
The pharmacist was not buying my initial explanation. “I am not going to fill prescriptions for ivermectin that are used in pseudo vaccine doses,” he told me.
I was surprised a young pharmacist was able to override an experienced physician’s prescription, effectively removing an inexpensive prevention and treatment option for selected patients in the middle of a pandemic.
The medical educator in me kicked in. “I would be happy to send you some references about the use of ivermectin for treatment and prevention. There are impressive studies from Argentina, Peru, Africa and India that suggest much better outcomes than we are achieving here in the U.S. with our single-minded focus on vaccines.”
He told me the U.S. Food and Drug Administration (FDA) did not recommend ivermectin for COVID. I asked to see the documentation and he agreed to fax it to me.
I hand-delivered 93 references and a great review article to the Walgreens.
The pharmacist faxed back a post from March 5, on the FDA website entitled “Why You Should Not Use Ivermectin to Treat or Prevent COVID-19.”
The next day, I received notice that a pharmacy in Northern Virginia would not fill any prescriptions for ivermectin if the diagnosis code mentioned COVID.
I had written an ivermectin prescription for a patient who has a history of bad reactions to vaccines and significant autoimmune illness. His adolescent age means that he is at very low risk of death from COVID itself.
Based on my experience as his doctor for over a decade, I was worried about potential adverse events if he got the COVID vaccine. I dug into the data about ivermectin, and it seemed like a great option for him to have on hand for early treatment of COVID if he got sick.
A pharmacist in a drug store, who never examined my patient or learned his extensive medical history, got to trump my best medical judgment by refusing to fill the prescription.
The same day, in a conversation with a compounding pharmacy, we learned of a case in which a patient’s family had to take a hospital to court to obtain treatment with ivermectin.
Bear in mind that the safety profile for ivermectin is excellent and the drug is spectacularly less expensive than the vast majority of hospital interventions.
Three days later, on a zoom call with a colleague whose parents live in Colorado, I learned that a pharmacist at a major drugstore was not only refusing to fill ivermectin for 86- and 87-year-old patients who held valid prescriptions, but the pharmacist was taking the initiative to remind the other King Soopers pharmacies in the state not to fill those prescriptions either.
My analysis of the medical literature is that ivermectin has an impressive safety record and there are multiple studies from around the globe suggesting it can decrease morbidity and mortality from COVID 19.
Two doctors who were actually in the ICU treating real patients, Dr. Paul Marik and Dr. Pierre Kory, looked at their prior experience with similarly sick patients and reviewed treatment strategies to determine what could be helpful.
As Dr. Anthony Fauci advised us to “stay home and wait for the vaccine,” frontline doctors took care of the patients before them, learning valuable lessons about what worked and what did not.
Let’s hit the highlights, quoting directly from the review paper by Kory et al, Jan 2021:
- Since 2012, multiple in vitro studies have demonstrated that ivermectin inhibits the replication of many viruses, including influenza, Zika, Dengue and others (Mastrangelo et al., 2012; Wagstaff et al., 2012; Tay et al., 2013; Götz et al., 2016; Varghese et al., 2016; Atkinson et al., 2018; Lv et al., 2018; King et al., 2020; Yang et al., 2020).
- ivermectin inhibits SARS-CoV-2 replication and binding to host tissue via several observed and proposed mechanisms (Caly et al., 2020a).
- ivermectin has potent anti-inflammatory properties with in vitro data demonstrating profound inhibition of both cytokine production and transcription of nuclear factor-κB (NF-κB), the most potent mediator of inflammation (Zhang et al., 2008; Ci et al., 2009; Zhang et al., 2009).
- ivermectin significantly diminishes viral load and protects against organ damage in multiple animal models when infected with SARS-CoV-2 or similar coronaviruses (Arevalo et al., 2020; de Melo et al., 2020).
- ivermectin prevents transmission and development of COVID-19 disease in those exposed to infected patients (Behera et al., 2020; Bernigaud et al., 2020; Carvallo et al., 2020b; Elgazzar et al., 2020; Hellwig and Maia, 2020; Shouman, 2020).
- ivermectin hastens recovery and prevents deterioration in patients with mild to moderate disease treated early after symptoms (Carvallo et al., 2020a; Elgazzar et al., 2020; Gorial et al., 2020; Khan et al., 2020; Mahmud, 2020; Morgenstern et al., 2020; Robin et al., 2020).
- ivermectin hastens recovery and avoidance of ICU admission and death in hospitalized patients (Elgazzar et al., 2020; Hashim et al., 2020; Khan et al., 2020; Niaee et al., 2020; Portmann-Baracco et al., 2020; Rajter et al., 2020; Spoorthi V, 2020).
- ivermectin reduces mortality in critically ill patients with COVID-19 (Elgazzar et al., 2020; Hashim et al., 2020; Rajter et al., 2020).
- ivermectin leads to striking reductions in case-fatality rates in regions with widespread use (Chamie, Juan, 2020).
- The safety, availability, and cost of ivermectin is nearly unparalleled given its near nil drug interactions along with only mild and rare side effects observed over almost 40 years of use and billions of doses administered (Kircik et al., 2016).
- ivermectin was successful at controlling several diseases which blighted the lives of billions living in poverty in the tropics.
- ivermectin’s discoverers were awarded the Nobel Prize in Medicine in 2015.
- ivermectin is included in the World Health Organization’s “List of Essential Medicines.” It has been widely distributed in countries like India for pennies a day. The out-of-pocket cost of ivermectin at my Walgreen’s is more than$1,000.
Kory and Marik compiled eight studies (three randomized controlled studies and five observational controlled studies) demonstrating efficacy in prevention of COVID-19 with significant decreased transmission.
They found 19 controlled studies that showed significant impacts on time to recovery, hospital stay, decrease in viral loads, reductions in duration of cough and decreased mortality.
In medical history pre-COVID, this body of research about ivermectin would be applauded for bringing value in the midst of a pandemic. In the medical era pre-COVID, the judgment and experience of clinicians at the patient’s bedside counted for something.
Pre-COVID, we taught medical students to use keen observational skills and keep accurate records of whether the patient improved or deteriorated after the treatment strategies used.
In the Age of COVID, pharmacists who chide doctors that “COVID does not have an exoskeleton” deny patients ivermectin — a safe, cheap, effective and potentially life-saving early treatment.
If you or your patients are having trouble getting ivermectin prescriptions filled for COVID 19 prevention or treatment, see this excellent resource from the Front Line COVID 19 Critical Care Alliance.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Winter is coming, and so are the nudges.
The UK government’s Winter Plan is rife with nudges
By Laura Dodsworth | October 4, 2021
There’s a chill in the air. Not from the changing seasons, it’s still beautifully balmy, but because the behavioural scientists’ fingertips have traced a hoar frost of psychocratic nudge on the government’s “Autumn and Winter Plan”.
The UK government’s Winter Plan plan contained some welcome news. The most draconian schedules of the Coronavirus Act will be revoked, including the powers to close schools, allow potentially infectious people to be detained, and restrictions on gatherings and events. The language around the plan’s launch was thankfully more cool-headed. The times are “challenging” but it is no longer claimed that Covid is the “biggest threat this country has faced in peacetime history”.
But the plan is also rife with “nudges” – sneaky ways to prime, prepare and prod you into the desired mindset and course of action.
The contents are freighted with the sunk cost fallacy; we’ve come so far, we mustn’t allow our good work to be undone. This also taps into people’s innate sensitivity to loss.
The trigger from Plan A to Plan B will be “unsustainable pressure” on the NHS rather than deaths. It’s under serious pressure every winter so consider yourselves to be put on notice.
There are other indications of the inevitability of Plan B. I spoke to behavioural scientist Patrick Fagan, who observed that:
“the Plan A / Plan B approach is a classic example of the foot-in-the-door technique. Firstly it makes us accept Plan A because, compared to Plan B, it looks more reasonable; then, once we have accepted and acclimatised to Plan A, we are more likely to then accept Plan B, because it is just one extra step on top of the commitment we’ve already made. The announcement of Plan B may also be an example of the mere exposure effect: simply by talking about the measures (even if, ironically, saying they won’t be implemented), the government makes them more familiar and therefore more psychologically acceptable.”
Bizarrely, after 18 months we’re trapped in a Groundhog Day of modelling and worst case scenarios. Almost a year ago, on the 21st September, Chris Whitty and Patrick Vallance warned of infections hitting 50,000 per day by mid-October in their “Shock and Awe” presentation. When the day arrived, the moving average was 16,228.
According to the doom-mongers at SAGE, up to 7,000 people could be hospitalised per day within the month. And this September the modellers were wrong once again – hospitalisations peaked at about a 1,000 a day and are now falling.
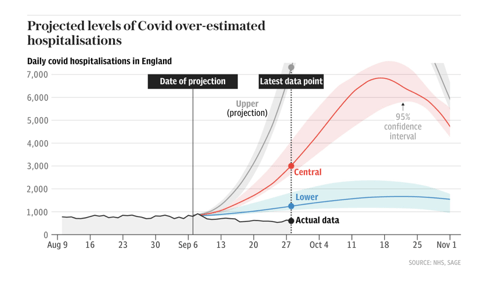
Source: The Telegraph
The big numbers both fuel the policies and justify them. It doesn’t matter that there are more optimistic scenarios, or that the modelling has limitations, because the first supine headline sticks in the brain. The behavioural psychology principle of “salience” draws your attention to what is novel and risky.
Dr Alex De Figueiredo, who conducts mathematical and statistical analyses for the Vaccine Confidence Project, told me that:
“Since the beginning of the pandemic it seems many modelling assumptions, such as the infection fatality rate, have been quite pessimistic. I think this has been why many of the predictions — such as hospitalisations and deaths — have been overstated. It also appears there has been little effort to validate forecasts out-of-sample, such as applying the models to Sweden or Florida, who have had far fewer restrictions.”
There are no quantifiable measures for what justifies each step from Plan A to Plan B. The parameters are fluid, unspecified. This creates confusion and stress, which infantilises people and makes them look to the government for direction. Essentially, confusion increases compliance.
The threat of lockdown hangs like a Sword of Damocles. Will we, or won’t we? It seems unlikely that the public and businesses could be persuaded again. Regardless, the threat of lockdown might be leveraged to justify the introduction of Covid Passports, in what is known as a “reciprocation nudge” – we appear to be given a concession in return for reduced resistance to another option.
Covid Passports have been vigorously opposed by MPs and civil liberties groups, and there hasn’t been a vote in Parliament yet. Despite this, they squat in Plan B as a fait accompli, in the denouement of the “door in the face” technique. This is when a huge request is made, then refused, to be followed by a second smaller request, in this case relegation to Plan B and for limited venues only. Boris Johnson said that it’s “not sensible to rule out this kind of option now when it might still make the difference between keeping businesses open or not.” But why would it be sensible when the Public Administration and Constitutional Affairs Committee produced a damning report against them and found the government could make no scientific case in their favour?
Covid Passports appear to be a behavioural science tool, used to increase vaccine uptake. This may backfire. ‘A Cross-Sectional Study in the UK and Israel on Willingness to Get Vaccinated against COVID-19’ found that vaccine passports deter a significant minority of people who want autonomy over their bodies. This also chimes with the research conducted by De Figueiredo and colleagues at The Vaccine Confidence Project. The bullying and resultant mistrust may impact Covid-19 vaccine uptake as well as other public health initiatives.
When my book A State of Fear: how the UK government weaponised fear during the Covid-19 pandemic was published some people believed, quite quaintly, that public health measures and messaging were unrelated to behavioural science. I think that the book and the writings of other academics and journalists have moved the dial. Once nudge is seen it can’t be unseen. The public increasingly see the nudge. If the behavioural scientists have been dazzling people with card tricks they have over-played their hand.
As such, there is more honesty about the purpose Covid Passports serve. Nicola Sturgeon, Scotland’s First Minister, said that the passport scheme
“will not eradicate transmission completely but it will help reduce it in some higher risk settings, and it will maximise protection against serious illness. And we believe – as we have seen already in some other countries – it will help encourage take-up of the vaccine.”
Similarly, Linda Bauld, Professor of Public Health and Interim Social Policy Adviser to the Scottish Government, also admitted that Covid Passports are “to increase uptake in vaccination” and the “rationale” is that it particularly boosts vaccination in 18 to 29 year olds.
While Covid Passports are in Plan B, Ministers say different things about them each day. Within the space of a week, Sajid Javid scrapped them but also didn’t rule them out for pubs. Javid admitted there’s “no evidence” for them but Boris Johnson called them “sensible”. Does the left hand not know what the right hand is doing? Or maybe a big behavioural science brain lurks in between. The epidemic management is reminiscent of the uncertainty created by Vladislav Surkov in the Soviet Union to deliberately turn politics into a performance of confusion – you don’t know what’s real anymore.
There are never-ending question marks over travel, although double-vaccinated travellers will no longer need expensive and inconvenient PCR tests. The double-jabbed will delight in the news, and it sounds sensible on the surface. However, this is not about “following the science”, since the previously infected do not benefit from the exemption. This is an incentive, a classic nudge, to encourage jabs. The vaccinated are rewarded and the unvaccinated are punished. Bearing in mind that negative tests and prior infection could suffice, this decision reeks of disdain for personal autonomy.
Vaccines for 12 to 15 year olds have been authorised. Politicians have stirred up debate amongst all corners regarding whether children should be jabbed with their parents’ consent or not. This utilises what Patrick Fagan calls “the leapfrog effect”. He says,
“it leapfrogs one stage of the debate and in doing so, sets the baseline assumptions which become accepted implicitly. Specifically, by having people debate whether or not parents’ consent should be sought, they are establishing the unspoken assumption that children should receive the jab in the first place. Those who think they are debating the government, arguing that parents’ consent is needed, are actually accepting its true goal, to jab kids.”
The government might be more in control of the narrative than many people like to believe. (Of course, chaos and confusion are alternatives…)
Worryingly, can teens truly provide informed consent? Throughout 2020 they were exhorted not to “kill granny”, which would provoke fear, shame and stress. Ads on Tiktok tell youngsters that the way to get back to normal is to take the vaccine. The vaccine will be rolled out in schools which will create peer pressure, in a particularly egregious use of “norms”. Finally, if the JCVI found the decision difficult, how is a 12 year old supposed to weigh up the evidence? (Nudging teens is the subject matter of my next article.)
Since the Cabinet reshuffle, Michael Gove has been informally dubbed the ‘Minister for Christmas’. Boris Johnson joked that he “didn’t want to have to cancel Christmas again”. Did you know Christmas might be cancelled and needs saving? You do now, the idea has been “seeded”.
Although it is ostensibly supply chains which threaten Christmas, the joke draws a comparison with last year’s Covid reasons. Again, you are put on notice. The nudges are still focussed on increasing vaccination, for now, but the threat to Christmas might hint at the beginning of a behavioural science approach to meet green targets.
We must be good boys and girls if we want Santa to come. And be aware, the nudgers are drafting our collective New Year’s Resolutions.
Twitter backtracks after censoring a mother’s obituary

By Cindy Harper | Reclaim The Net | October 4, 2021
Twitter’s fact-checkers appended a “misleading” alert to an obituary about a young woman who allegedly died after contracting a rare blood-clotting condition provoked by the COVID-19 vaccine.
After being accused of going so far with its censorship that it would resort to censoring an obituary, Twitter relented to the backlash and reversed the censorship.
The woman in question, Jessica Berg Wilson, a 37-year-old mother of two, died in the first week of September from Vaccine-Induced Thrombotic Thrombocytopenia, a rare blood disorder in which small clots grow throughout the body, damaging platelets and preventing blood from reaching key organs. According to her obituary, Wilson’s greatest life ambition was to “be the best mother possible” to her daughters Bridget and Clara.
“She had been vehemently opposed to taking the vaccine, knowing she was in good health and of a young age and thus not at risk for serious illness. In her mind, the known and unknown risks of the unproven vaccine were more of a threat,” it read.
Kelly Bee, a Twitter user, posted Jessica Berg Wilson’s obituary with the statement, “an ‘exceptionally healthy and vibrant 37-year-old young mother with no underlying health conditions,’ passed away from COVID Vaccine-Induced Thrombotic Thrombocytopenia. She did not want to get vaccinated.”
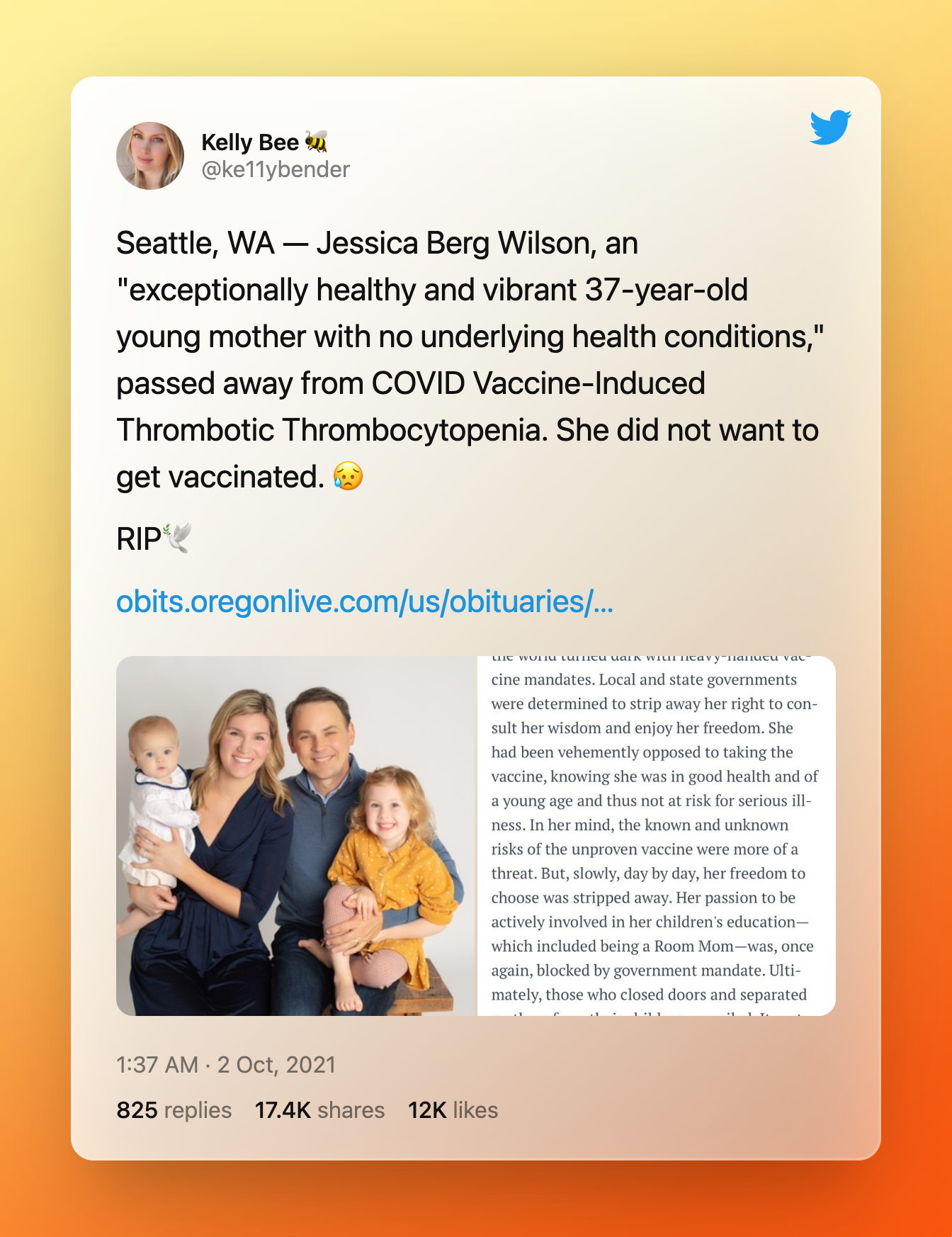
However, Twitter flagged the post as “misleading” and blocked it from being replied to, shared, or liked.
The majority of critics were outraged that Twitter was censoring an obituary and they responded by urging their followers to help the tweet go viral in violation of the company’s warning. Twitter has since removed the “misleading” designation and revoked the shadowban.
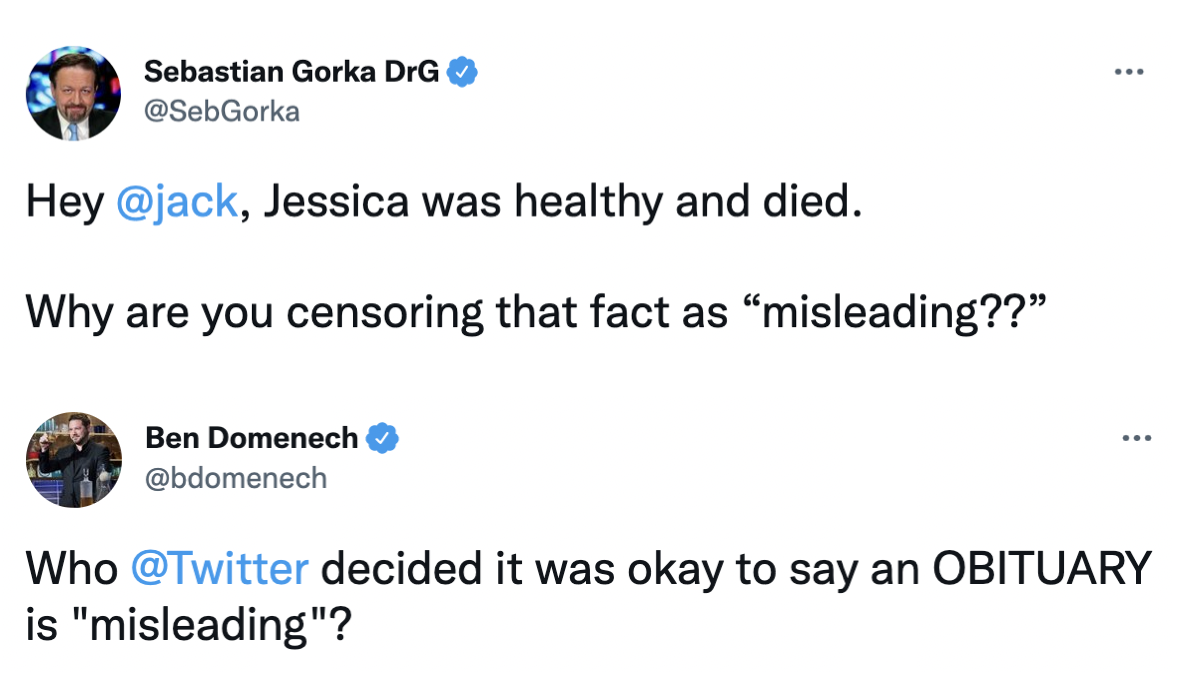
Additionally, several bloggers, including Ben Domenech of The Federalist, retweeted the obituary. Ben’s tweet reads: Who @Twitter decided it was okay to say an OBITUARY is ‘misleading’ ?”
Another tweet said “Twitter is now censoring obituaries,” – posted by Sean Davis.
Furthermore, Sebastian Gorka, who worked in the Trump administration’s Department of Defense, tagged Twitter CEO Jack Dorsey in a tweet asking what aspect of the obituary was incorrect or “misleading.”
“Hey @jack, Jessica was healthy and died. Why are you censoring that fact as ‘misleading??” he said.
“My name is Bill Gates, King of Kings”

Source: The next outbreak? We’re not ready | Bill Gates | INTIDOMAIN
By Richard Hugus | October 4, 2021
My name is Ozymandias, King of Kings,
Look on my Works, ye Mighty, and despair!
— Percy Bysshe Shelley, Ozymandias
The evidence is in. Gene-manipulating injections advertised as a “vaccine for covid 19” have killed and injured many thousands of people. Instead of providing immunity to an alleged virus, the shots actually harm the immune system and turn it against us. The spike proteins created by the shots spread out to attack major organs in the body, leading to a thousand and one different health problems, including heart attacks, myocarditis, pericarditis, strokes, blood clots, spontaneous abortions, neurological disorders, depression, and death. Yet the medical establishment is urging everyone, including pregnant women and children, to get the jab. The ghost standing in as US President recently decreed that if people refuse the shot they will lose their job. This is coercion to accept a medical intervention known to be a danger to human health — a crime against humanity. Half the population of the country is now facing this coercion.
This only makes sense if we reason that the authorities want to harm us, or that there is something so important in the injection that they don’t mind harming us, as long as we get the injection. Bill Gates said early in 2020 that everyone on the planet should be “vaccinated.” Perhaps his dream was that when that is accomplished there will be no one left who will not be genetically modified (to Gates’s secret specifications) and thus no one left to hold him to account.
One of the most insidious arguments put forward by the authorities is that we are facing a health crisis so serious that individual freedom must be sacrificed for the common good, and therefore no one has a moral right to refuse the Frankenshot. This argument quickly comes down to whether human beings have inalienable rights — rights given to us by God, which the state does not have the power to take away or overrule. To accept or reject any substance being given to us is obviously such a right. And after this we can discuss the details — that the purpose of the “vaccine” is unclear, that its contents are unknown, that it has proven harmful to thousands of people, that we were not informed of adverse effects, that natural immunity should be recognized, that tests establishing the alleged disease were fraudulent, that there is no emergency, that there are safe alternative treatments, et cetera. But if we understand that the state is a lesser power, then we understand that it does not have the authority to order substances injected into our bodies.
We hold these truths to be self-evident, that all men are created equal, that they are endowed by their Creator with certain unalienable Rights, that among these are Life, Liberty and the pursuit of Happiness.
-U.S. Declaration of Independence
The cabal behind the medical tyranny we are facing doesn’t believe we have God-given rights because they don’t believe there’s a God in the first place. They apparently think that since they are billionaires, and billionaires have a lot of weight to throw around, that they can be gods. They also seem to believe there is nothing they are forbidden to do to other people because other people do not have souls — they are just biological entities evolved through random nature which the rich, by virtue of their power, are free to manipulate and improve upon. To technocrats, nothing is sacred. So it makes sense to them to risk injuring pregnant women and children and even experiment on the whole human race (beside their chosen few). Those who resist are now being segregated and punished, like Palestinians in their own land. Perhaps occupied Palestine is the oligarchs’ model for our future.
The ultimate goal may be the power that previous master-slave relationships were not able to achieve — a “read/write” capability in which the master has full surveillance power over the slaves and gives the orders for them to follow. Subtracted from the slave population, of course, will be those few billion dissidents and “useless eaters” who don’t fit in with the plan. They will be terminated. From this point of view it also follows that the genetic makeup of any living thing is just software which today’s sophisticated scientists can splice, delete, modify, or re-create as the masters see fit. From this point of view humans are no different than GM corn, soy, or cotton. GM humans can be used to bring in a nice profit as well because the masters will own their patents. Perhaps Monsanto agribusiness is another model for our future.
Taken to its logical extreme, reality itself is in the hands of our would-be masters. With proper control of the media, people can be made to believe anything, like that an illness similar to the flu is a “pandemic,” or that someone who has no symptoms of illness is actually sick, or that the unvaccinated are selfishly threatening everyone else with death, or that anyone who strays from the narrative is spreading “misinformation,” or that if someone goes into convulsions directly after getting jabbed it is not due to the poison that was just injected into them, or that a serum that injures and kills is “safe and effective.” In this world, the truth is what the powerful say it is, regardless of the facts. The powerful are a locomotive big enough to just run past any anomalies and contradictions, leaving us bewildered.
However, the ambitiousness of this insane program foretells its failure. History is full of great tyrants with grand plans who came in with spectacular fame but suddenly fell in disgrace, erased by time. The oligarchs’ main weakness is their lack of any sense of limits. Gaining some power, they then want it all. They reach too far, too soon, and expose themselves in the process. And then common humanity — always patient to a fault — finally decides to stand up and become a locomotive itself, running back over the entire plan and returning us to sanity.
If the world is going to see a great reset, it will not be the one Klaus Schwab and his Davos gangsters had in mind.
We should take heart. So much has been revealed! It’s as if the world’s worst criminals burst into the courtroom and offered up a horrendous public confession.
Another Study Links Low Vitamin D to Risk of COVID
By Dr. Joseph Mercola | October 4, 2021
Another preprint study, published September 25, 2021, shows the correlation between low vitamin D levels and the risk of getting COVID-19.
In this retrospective examination of one population study and seven clinical studies where vitamin D3 levels were measured on the day of hospitalization, researchers said, “The two datasets provide strong evidence that low D3 is a predictor rather than a side effect of the infection.”
They suggested that it may be possible to “prevent or mitigate” new COVID outbreaks by simply raising people’s vitamin D3 levels to 50 ng/ml or above. Even though they said they believe vaccination is part of the fight against COVID, they added that the ongoing evidence of the part vitamin D plays in the risk for contracting the infection is especially important because the virus continues to mutate, which challenges the effectiveness of the vaccines.
New Zealand Abandons Controversial ‘Zero COVID’ Policy
But lockdowns will remain until 90% of population is vaxxed

By Paul Joseph Watson | Summit News | October 4, 2021
New Zealand has announced it is dropping its controversial ‘zero COVID’ policy after numerous critics pointed out that such an approach to eliminating the virus was impossible.
Prime Minister Jacinda Ardern made the announcement earlier today during a press conference in which she acknowledged, “The return to zero has been extremely difficult.”
“What we have called a long tail has been more like a tentacle that has been difficult to shake,” she added, noting that the delta variant of the virus forced a change in policy.
Critics had repeatedly asked how the country expected to maintain a ‘zero COVID’ policy given the emergence of new variants of the virus and decreasing efficacy of the initial round of vaccinations.
However, with 48% of the population fully vaccinated, no return to normal is expected anytime soon given that Ardern has said 90% will need to be fully vaxxed before the lockdowns will end.
Kiwis have faced continuous lockdown measures almost as brutal as their Aussie neighbors since the beginning of the pandemic.
As we highlighted in August, Ardern mimicked Australia’s top public health official by telling citizens, “Don’t talk to your neighbors,” after the country went into full lockdown as a result of just a single COVID case being detected.
Authorities also previously announced that they would put all coronavirus infectees and their close family members in “quarantine facilities” even if they refuse.
Featured Video

Fear Is the Mind Killer
or go to
Aletho News Archives – Video-Images
From the Archives
Alarmist climate science as a textbook example of groupthink
By Paul MacRae | May 1, 2012
A while ago, I received an email from a friend who asked:
How can many, many respected, competitive, independent science folks be so wrong about [global warming] (if your [skeptical] premise is correct). I don’t think it could be a conspiracy, or incompetence. … Has there ever been another case when so many ‘leading’ scientific minds got it so wrong?
The answer to the second part of my friend’s question—“Has there ever been another case where so many ‘leading’ scientific minds got it so wrong?”—is easy. Yes, there are many such cases, both within and outside climate science. In fact, the graveyard of science is littered with the bones of theories that were once thought “certain” (e.g., that the continents can’t “drift,” that Newton’s laws were immutable, and hundreds if not thousands of others).
Science progresses by the overturning of theories once thought “certain.” … continue
Blog Roll
 Aletho News
Aletho News- Why don’t UK media mention the Israel lobby?
- New US shipment of 6,500 tons of military aid arrives in Israel
- Military aid to Ukraine vital for ‘US hegemony’ – Republican senator
- Zelensky’s favorite drone company at center of Ukrainian corruption alert
- The Broken Contract
- US CENTCOM’s Request for Dark Eagle Missiles Shows Shortage of Weapons and Limited Options
- Iran consolidates Strait of Hormuz control in post-war power shift, leaving US in dark
- A pause, not a ceasefire: Washington stalls, Tehran recalibrates
- US blockade crumbles as Iran turns to overland routes
- Hidden costs of US Iran war push total far beyond $25bn Pentagon claim
- If Americans Knew
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- Israel’s top Jewish religious body ‘refuses to condemn’ smashing of Jesus statue
- Nun assaulted in Jerusalem amid ‘pattern’ of anti-Christian attacks by Israelis
- Former Tik Tok official describes massive pressure from Israel lobby
- Amid ceasefire violations and genocide, Israel commits piracy – Daily Update
- Five Laws and Standards That Require the US Cut Off Weapons to Israel
- Israel’s diabolical killing machine and how it targets journalists.
- The Global Sumud Flotilla to Gaza — A cry at sea to the world’s dormant conscience
- Politico’s powerful parent company tells Politico they must support Israeli narrative
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
